
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Nephrol. , 13 November 2024
Sec. Critical Care Nephrology
Volume 4 - 2024 | https://doi.org/10.3389/fneph.2024.1470926
 Sergi Codina1,2
Sergi Codina1,2 Laia Oliveras1,2Eva Ferreiro1Aroa Rovira3Ana Coloma1
Laia Oliveras1,2Eva Ferreiro1Aroa Rovira3Ana Coloma1 Nuria Lloberas2Edoardo Melilli1Miguel Hueso1,2Fabrizio Sbraga4Enric Boza5José M. Vazquez6José L. Pérez-Fernández7Joan Sabater7
Nuria Lloberas2Edoardo Melilli1Miguel Hueso1,2Fabrizio Sbraga4Enric Boza5José M. Vazquez6José L. Pérez-Fernández7Joan Sabater7 Josep M. Cruzado1,2*
Josep M. Cruzado1,2* Nuria Montero1,2*
Nuria Montero1,2*Introduction: Cardiac surgery-associated acute kidney injury (CSA-AKI) is a well-known complication that increases morbidity and mortality rates. The objective of this study was to reduce CSA-AKI through nephrologist intervention in patients awaiting cardiac surgery.
Methods: We performed a single center, open-label, randomized clinical trial including 380 patients who underwent scheduled cardiac surgery at the Hospital de Bellvitge between July 2015 and October 2019. A total of 184 patients were evaluated by the same Nephrologist one month before the surgery to minimize the risk factors for AKI. In addition to assessments at the outpatient clinic, we also collected clinical data during hospitalization and during the first year.
Results: Despite the intervention, no differences were observed between the groups in the incidence of CSA-AKI (intervention group 26.37% vs. standard of care 25.13%, p=0.874), mortality (3.91% vs. 3.59%, p=0.999), length of Intensive Care Unit (ICU) stay (10 days [7.00;15.0] for both groups, p=0.347), or renal function after one year of follow-up (estimated glomerular filtration rate (eGFR) by CKD-EPI: 74.5 ml/min (standard deviation 20.6) vs 76.7 (20.8) ml/min, respectively, p=0.364). A reduction in the need for blood transfusion was observed in the intervention group, although the difference was not statistically significant (37.22% vs. 45.03%, p =0.155).
Conclusion: In this clinical trial, nephrologist intervention in the entire population on the cardiac surgery waiting list did not show a nephroprotective benefit.
Clinical trial registration: ClinicalTrials.gov, identifier (NCT02643745).
Acute kidney injury (AKI) is a common complication of cardiac surgery. In the literature, the incidence varies from 7 to 44% depending on the study. There are different definitions used: AKIN classification (Acute Kidney Injury Network), RIFLE criteria (Risk, Injury, Failure, Loss, End-Stage Kidney Disease), or KDIGO (Kidney Disease Improving Global Outcomes) criteria based on serum creatinine and urine output (1–4). The presence of AKI has a clinical impact because it is associated with longer hospitalization, progression to end-stage renal disease (ESRD), and even increased mortality (2). The mortality risk in patients who develop acute renal dysfunction after cardiac surgery increases by approximately 40%, ranging from 2% to 19% according to the series (5).
There are some well-known risk factors associated with AKI, including baseline patient characteristics (age and comorbidities), need for perioperative blood transfusion, and the presence of earlier chronic kidney disease (6, 7). For many years, different interventions designed to prevent post-surgical AKI have been attempted without success (8). In contrast, a holistic approach during the post-operative period, guided by the implementation of the Kidney Disease Improving Global Outcomes (KDIGO) bundle of care in patients at high risk of AKI, has shown a reduction in AKI incidence, especially a decrease in moderate and severe AKI (9).
However, the prevention of AKI related to surgery should begin prior to the operation since most risk factors are modifiable. According to the ADQI (Acute Disease Quality Initiative), all patients undergoing cardiac surgery should undergo routine clinical assessment of AKI risk to implement preventive strategies (10).
The aim of this randomized clinical trial was to assess whether nephrology intervention before cardiac surgery can reduce the postoperative incidence of AKI.
We conducted a single-center, open-label, randomized clinical trial that included patients on the waiting list for cardiac surgery. Eligible patients were adults aged > 18 years who were awaiting scheduled cardiac surgery. Exclusion criteria were requirement for renal replacement therapy (RRT) before surgery, need for urgent surgery, or participation in another clinical trial. Informed consent to participate in the study was obtained from all participants.
The Clinical Research Ethics Committee of the Hospital de Bellvitge approved this study before its initiation. We followed the CONSORT guidelines to report this RCT study, and the protocol was published at clinicaltrials.gov (NCT02643745).
Patients were randomly assigned to the nephrology-intervention or control group (1:1) using a computer random number generator. Eligible patients were distributed using sequentially numbered opaque sealed envelopes during the first visit of the cardiac surgeon.
The patients assigned to the nephrologist intervention group (intervention group) had a preoperative and protocolized study that included blood and urine tests, bioimpedance at consultation and before surgery, and an outpatient clinic visit with a nephrologist who performed a detailed anamnesis, detected risk factors, and improved the overall patient’s condition (Supplementary Table 2). Patients assigned to the no-intervention group (standard of care) followed the usual routine care and did not receive any other consultation by a nephrologist, cardiologist or cardiac surgeon before surgery. Bioimpedance was performed in a subgroup of patients before surgery.
After hospital discharge, all patients visited the Nephrology Department. Clinical and analytical assessments were performed at discharge and 6 and 12 months after surgery. All consultations were conducted by the same nephrologist.
The primary endpoint was the presence of cardiac surgery-associated AKI (CSA-AKI). We defined according to the KDIGO criteria (Supplementary Table 1) (11). The secondary endpoints were mortality (in the first year), hospitalization days, length of stay in (Intensive Care Unit (ICU), need for RRT, anemia, need for blood transfusion, metabolic disorder control (diabetes, dyslipidemia), and renal function using the estimated glomerular filtration rate (eGFR) calculated by the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI).
We collected clinical data at randomization, before and after surgery, during hospitalization, and 6 and 12 months after surgery. Data were collected from the medical records. It included: baseline characteristics (age, ethnicity, gender, body mass index (BMI), comorbidities, and treatments); blood and urine analysis (serum creatinine (SCr), albuminuria (using urine albumin-to-creatinine ratio (ACR) in a spot urine sample), and proteinuria (using protein-to-creatinine ratio (PCR) in a spot urine sample), urinary ionogram, ferritin, transferrin saturation index, albumin, prealbumin, cholesterol levels (low-density lipoprotein (LDL), high-density lipoprotein (HDL), and total), fibrinogen, fasting blood glucose, HbA1c and hemoglobin, venous blood gasometry); spectroscopic bioimpedance analysis measuring: lean tissue index (LTI), fat tissue index (FTI), normohydrated weight, and the distribution of fluids in the body (total body water (TBW), extracellular water (ECW) and intracellular water (ICW) using BCM-Body Composition Monitor (Fresenius)); surgery characteristics (type of surgery, individual severity risk, off-pump time surgery, clamp time, need of post-operative pacemaker, intraoperative hemodynamics, drug use, fluid balance, and need of transfusions); and post-operative evolution (need of post-operative pacemaker, hemodynamics, drug use, fluid balance, the need of transfusion and type and duration of RRT if needed).
We aimed to detect a clinical difference of 5% reduction in the incidence of AKI between the study groups, with an expected rate of 12.2% AKI in the control group. A total of 550 subjects per group were required to have 80% power to reject the null hypothesis that the AKI rate was the same in the experimental and control groups. The type I error probability associated with this test was 5%. The investigators planned interim analyses after 25, 50%, and 75% of the trial participants completed their 1-year follow-up. However, after the 410 patients were randomized, it became apparent that the rate of the primary outcome was higher than expected in both groups. This made the trial underpowered to detect a 5% reduction in AKI rate. In fact, the trial would only be powered to detect differences of > 10%. An effect that was considered unattainable with an intervention such as that planned in our trial. Therefore, the trial monitoring committee decided to stop the trial in October 2019.
We performed an intention-to-treat analysis considering the results of the patient in the first assigned group. Continuous variables were compared between groups using the Student’s t-test or Wilcoxon rank test according to distribution. Categorical variables were compared using the X2 or Fisher’s exact test, when appropriate. We performed subgroup analysis for patients at risk based on the presence of eGFR ≤ 45 ml/min/1.73 m2. Univariate and multivariate logistic regression models were used to estimate factors associated with AKI. Results are reported as odds ratios (OR) and 95% confidence intervals (CIs). All analyses were performed with a two-sided significance level of 0.05 and were conducted with SPSS software and R software version 4.1.0 [The Comprehensive R Archive Network. Available from: https://cran.r-project.org/].
From July 2015 to October 2019, 410 patients who underwent cardiac surgery at the Hospital de Bellvitge were included in the clinical trial. A total of 203 participants were assigned to the intervention group and 207 to the standard care group. After excluding 30 patients, 380 were finally analyzed: 184 in the intervention group and 196 in the standard care group (n=196, Figure 1). The baseline characteristics of both groups did not differ significantly, except for more smokers (7.27% vs. 1.68%), chronic obstructive pulmonary disease (21.9% vs. 13%), and vascular disease (13.1% vs. 7.7%) in the intervention group (Table 1). Most surgeries were of one isolated valve (65.3%). There were no significant differences between the groups in terms of surgery type or perioperative management of volume or drugs (Table 1). At the time of surgery, no differences were observed in spectroscopic bioimpedance analysis parameters (Supplementary Table 2).
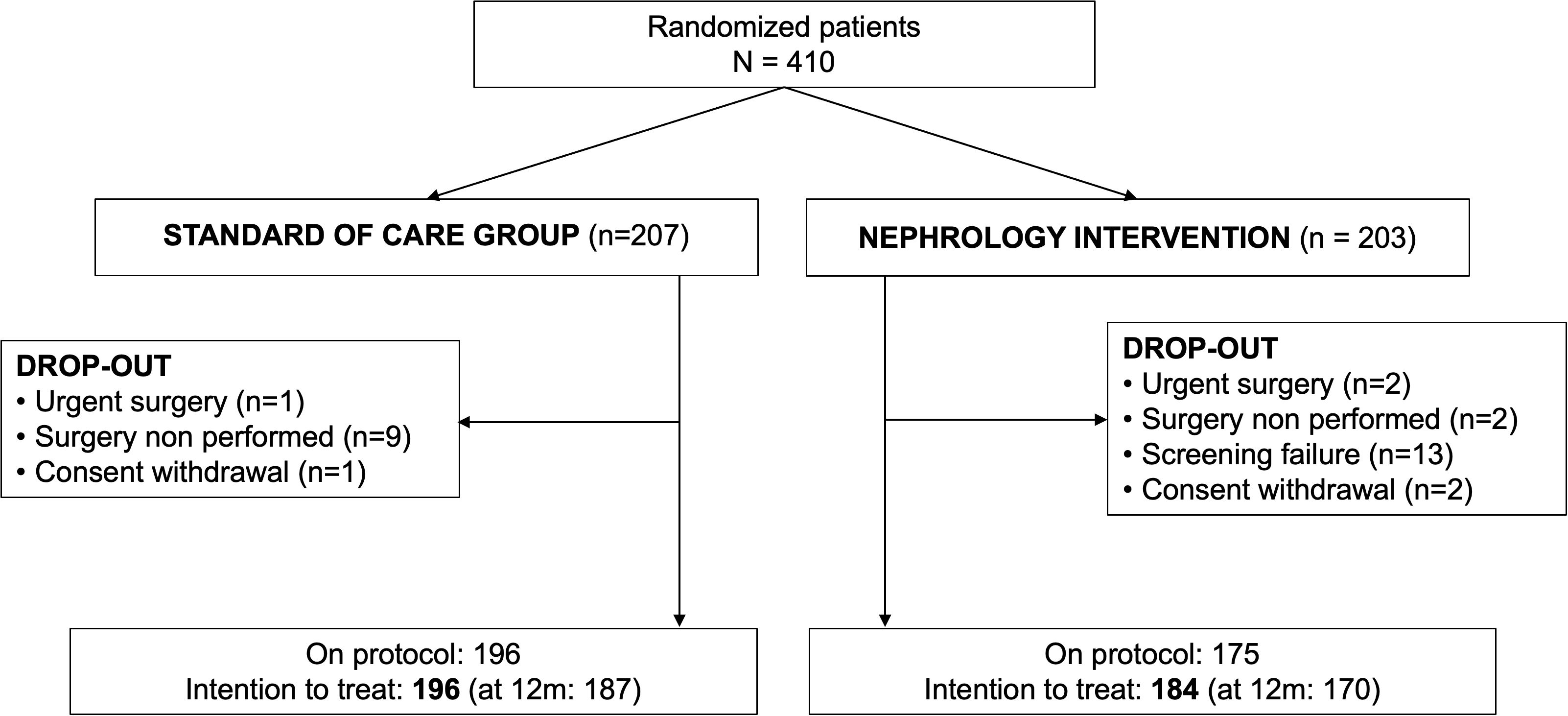
Figure 1. Flowchart of included patients.
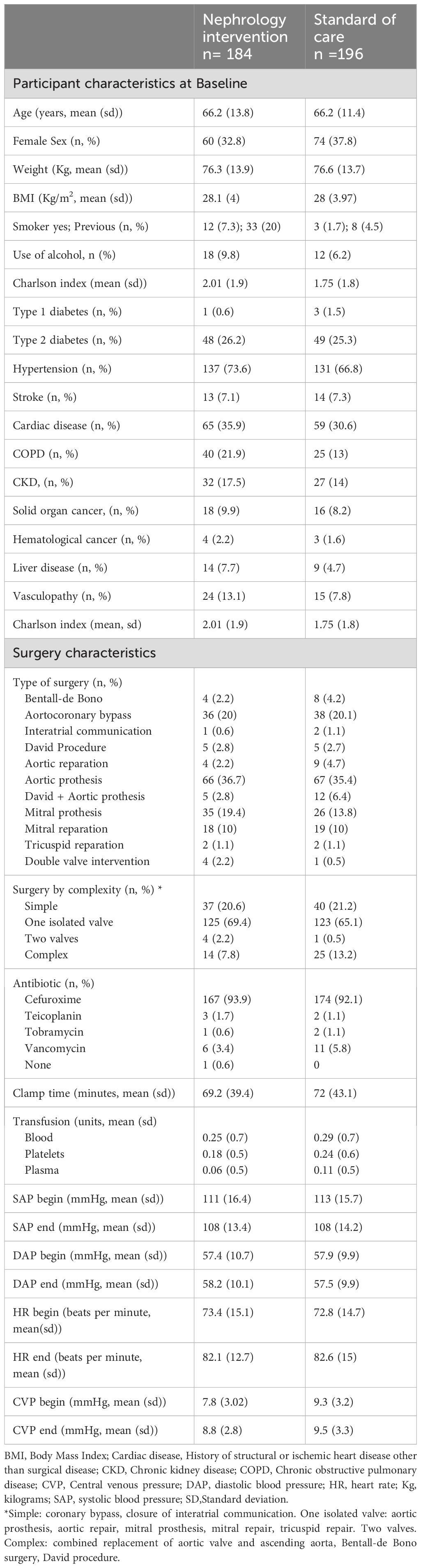
Table 1. Characteristics of the participants and surgery, according to Group.
In the 184 patients randomized into the intervention group, the nephrology consultant indicated interventions in 15 distinct categories related to renal health following the KDIGO guidelines for AKI (Table 2; Supplementary Table 3). This Nephrology Intervention was performed a minimum of one month before surgery (median 54 days; interquartile range 31.75-82). The most common interventions were the reduction of caloric intake (n=71), diuretic and antihypertensive treatment adjustment (n=29, n=41), and iron correction (n=32). Intervention achievement was evaluated at patient admission before surgery and 6 and 12 months after surgery. The median number of interventions indicated was 2 per patient (interquartile range IQR 1-3) with a mean global achievement per patient of 70.3 ± 36.1%. Despite a good accomplishment rate, no differences were observed in those variables that could be measured at the time of randomization with respect to the time of admission to the hospital between the standard-of-care and Nephrology Intervention Groups (Supplementary Table 4).
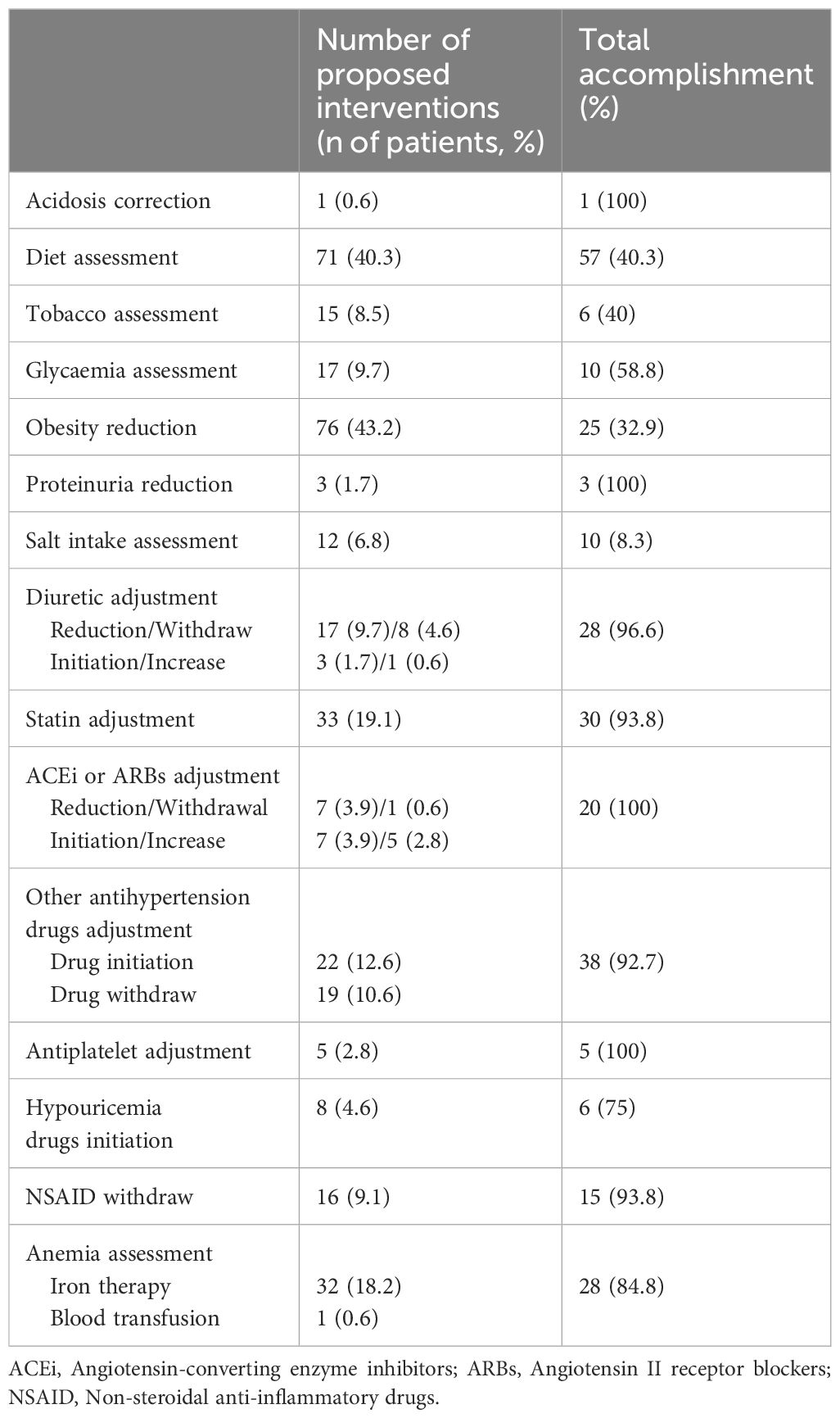
Table 2. Nephrology interventions and accomplishment.
The overall incidence of CSA-AKI was 25.73%, without differences between the groups (26.37% in intervention vs. 25.13% in standard-of-care, p=0.874). Most episodes of CSA-AKI were staged as AKI 1 (18.6% vs. 17.4%). In contrast, stage 3 AKI was marginal in both groups (3.83% and 1.54%, respectively). Although AKI stage 2 was less frequent in the intervention group, the difference was irrelevant (3.83% vs. 6.15%).
In the univariate analysis, the risk factors associated with CSA-AKI were age (odds ratio (OR) 1.05; 95% confidence interval (CI) 1.03 to 1.08; p<0.001), BMI (OR 1.06; 95% CI 1.00 to 1.13; p=0.034), clamp time (OR 1.01, 95% CI 1.00 to 1.01; p=0.026), and previous chronic kidney disease (OR 3.50; 95% CI 1.96 to 6.26; p<0.001). The factors associated with a lower risk of CSA-AKI were diastolic pressure at the beginning of surgery (OR 0.97; 95% CI 0.95 to 0.99; p=0.009), diastolic pressure at the end of the clamp (OR 0.96; 95% CI 0.94 to 0.99; p=0.004), and hemoglobin levels at hospital admission (OR 0.98; 95% CI 0.97 to 1.00; p=0.019, Table 3). In multivariate analysis, age, BMI, previous chronic kidney disease, and clamp time remained significant (Table 4).
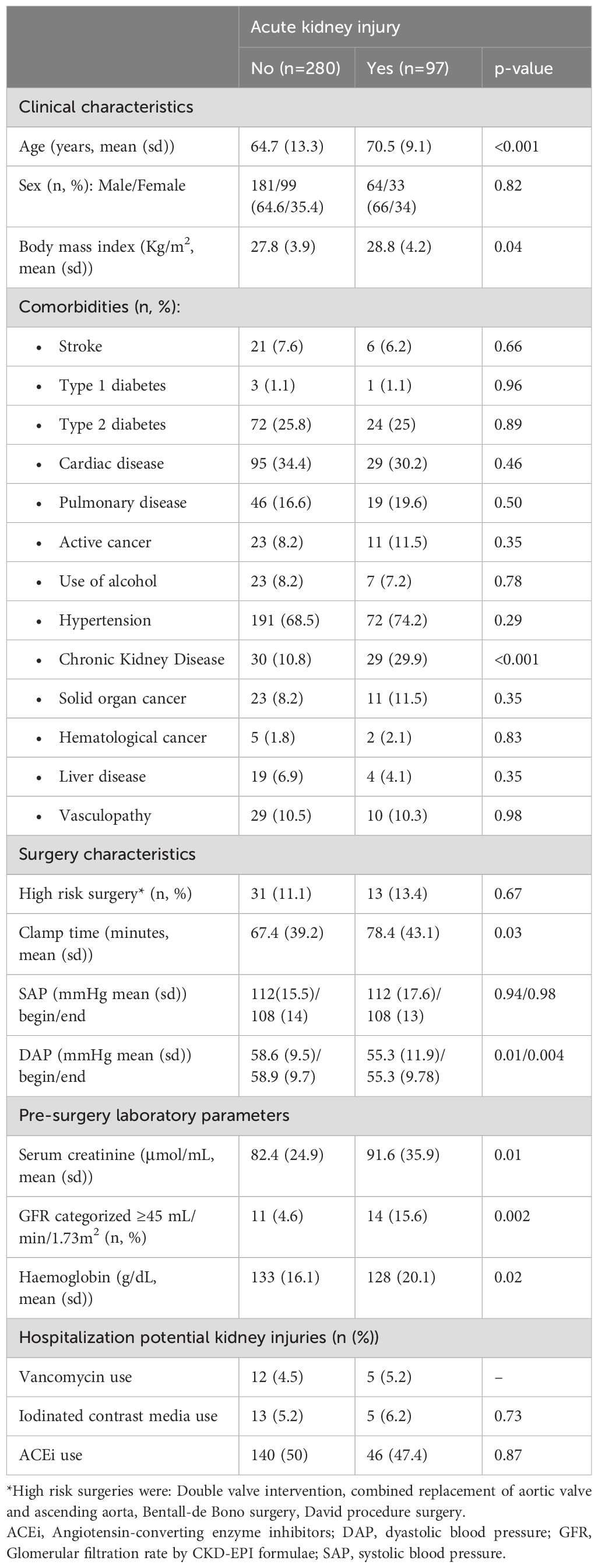
Table 3. Association of main clinical, analytical and surgery characteristics with acute kidney injury.
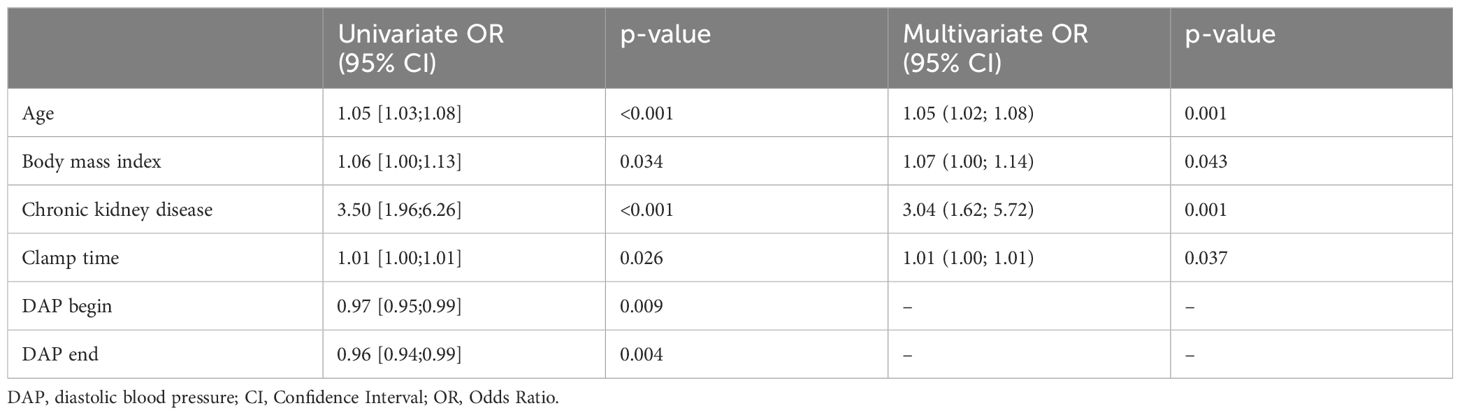
Table 4. Risk factors associated with acute kidney injury.
We then evaluated whether the nephrologist intervention had any impact on a selected group of patients at risk of CSA-AKI based on the presence of eGFR ≤ 45 ml/min/1.73 m2. In the high-risk patients randomized to the intervention group (n=13), we found a lower incidence of AKI (46.15% vs. 66.67%), although the differences did not reach statistical significance (p=0.53), probably because of the low number of high-risk patients (n=25). When the selection of patients at risk of CSA-AKI was analyzed according to the type of surgery (high versus low risk), no differences were observed in either group (high risk surgery 27.78% vs 30.77%, low risk surgery 26.22% vs 24.26%).
Regarding secondary outcomes, there were no differences in terms of mortality between the groups, neither during admission (2.17% vs. 2.04%, p =0.999) nor in the first year after surgery (3.91% vs. 3.59%, p=0.999). A reduction in the need for blood transfusion was observed in the intervention group, although the difference was not statistically significant (37.22% vs. 45.03%, p =0.155). Only four patients required RRT (intervention group, n=3; control group, n=1). The median length of hospitalization was 10 days [range, 7–15] days) in both the groups (p=0.347).
When long-term outcomes were evaluated, we did not find any differences in eGFR between the intervention group and the standard care group (74.5 ± 20.6 ml/min vs 76.7 ± 20.8 ml/min respectively, p=0.364).
No differences were observed in blood cholesterol levels at 6 months after surgery (4.32 ± 0.98 vs 4.44 ± 1.09 mmol/L; p=0.524) and after 12 months (4.53 ± 1.01 vs 4.49 ± 1.16 mmol/L; p=1), neither in glycosylated hemoglobin levels (at 6 months: 5.69 ± 0.75 vs 5.7 ± 0.72%, p=0.903 and at 12 months: 6.19 ± 1.17 vs 6.24 ± 1.08%, p=0.748).
In this randomized controlled trial, a nephrology intervention to avoid acute kidney injury after cardiac surgery did not show any benefit at the clinical level.
These results are surprisingly contrary to earlier findings. Recent studies have shown that the application of the KDIGO bundle of care protocols in early ICU hospitalization prevents moderate-to-severe AKI (9). Nevertheless, according to the ADQI (Acute Disease Quality Initiative), as many of the risk factors are modifiable, all patients undergoing cardiac surgery should undergo routine clinical assessment of AKI risk to implement preventive strategies before the operation (10). However, in our study, a nephrologist intervention focused on the correction of these potential AKI risk factors one month before surgery was not associated with the prevention of AKI and did not support these recommendations.
It is worth noting that the incidence of CSA-AKI in our cohort was lower than that previously described in some series in the literature. For example, in the PrevAKI study (9) the incidence of AKI was 55% and 71%, while in our cohort, the incidence was approximately 25% for both groups. In a study by Silva et al (12), the incidence of AKI was 43% and was associated with increased mortality, regardless of the grade of AKI. Howitt et al (2) study, the incidence of AKI can reach up to 36.1%. Many other recently published case series reported incidences of CSA-AKI similar to those observed in our study (13–16). Even in the TRIBE-AKI study (17), the incidence was only 30%, although the design of the study selected high-risk patients with CSA-AKI. It is important to note that these differences may be due to the different diagnostic criteria for AKI, which can vary significantly depending on the definition used because some only assess serum creatinine and others also take into account urine output criteria (1).
From our point of view, the differences observed in terms of CSA-AKI are related to the quality of post-operative care, especially in the first few hours in the ICU. In fact, the “intervention” that demonstrates benefits in the PrevAKI study (9) is nothing more than applying good clinical practices for the care of renal function. All these practices (consisting of avoidance of nephrotoxic agents, discontinuation of angiotensin-converting enzyme inhibitors and angiotensin receptor blockers for the first 48 h after surgery, close monitoring of serum creatinine and urine output, avoidance of hyperglycemia for the first 72 h after surgery, consideration of alternatives to radiocontrast agents, and close hemodynamic monitoring using a prespecified algorithm) should be part of routine clinical practice in all ICUs that treat patients with this high level of complexity.
AKI staging has a significant impact on the subsequent outcomes (2, 18). In our case, for example, most AKI episodes were classified as AKI stage I (70%); therefore, we did not observe a significant deterioration in renal function one year after the surgery in these patients, consistent with that previously reported (18, 19). Based on our results, we must assume that the current state of CSA-AKI is as follows: the incidence of AKI-CSA is approximately 25% in most cases associated with mild stages of AKI (stage II) that do not represent significant differences in mortality or subsequent CKD development.
The risk factors for CSA-AKI seen in our population have also been described in previous reports: the presence of earlier chronic kidney disease, older age, higher clamp time, and lower hemoglobin levels at hospitalization.
Contrary to what is recommended by the Acute Disease Quality Initiative (10), in our case, a nephrological intervention implemented in almost 200 patients did not result in a significant change in subsequent renal outcomes (CSA-AKI in the intervention group: 26.37% vs. 25.13% in the control group). On the other hand, it has meant an increase in work at the nephrologist’s office, which leads to an increase in hospital costs.
The aim of the intervention was to control the main AKI risk factors previously described (6, 7), and the median achievement of the interventions was 70.3%, which we considered positive. However, our intervention did not have a clinically significant impact. For example, at the nephrologist visit, an assessment was made of the degree of anemia and iron deficiency of the patients, given the relationship between iron metabolism and the risk of CSA-AKI (20, 21). This intervention achieved a decrease in the need for transfusion of red blood cell concentrates, but this difference did not reach statistical significance, and it did not impact the main outcome either. Therefore, we do not believe that the absence of differences observed in the study is due to the design or execution of the nephrological intervention, but to the low current impact of CSA-AKI on clinical outcomes in the general population compared to what was expected.
Currently, there is a trend towards the development of predictive tools for CSA-AKI either through “machine learning” tools (14, 22), scores based on clinical data (13) or the discovery of pre- or post-operative biomarkers (15, 17, 20, 23, 24). The general objective of these lines of research is to identify, as accurately as possible, subgroups of the population at a higher risk of AKI and post-surgical complications. For example, in a study by our group, we described how previous chronic kidney disease conferred a pro-inflammatory state that meant an increased susceptibility to the risk of developing CSA-AKI (25).
Arguably, the presence of higher comorbidity in the nephrology intervention group could have masked the study results. However, we believe that the impact of the observed differences in comorbidities (smokers, COPD, vascular disease) should be small as they have little impact on the Charlson index. In addition, it is possible that a thorough anamnesis by an expert nephrologist may have helped to unmask some diagnoses and slightly explain some of the differences found.
The main limitation of our study was the inability to reach the initial sample size, mainly due to the low incidence of CSA-AKI. However, our study features a number of strengths, in particular, our study is the first randomized clinical trial that applies a systematized pre-surgical nephrology intervention with the aim of reducing CSA-AKI in a final cohort of more than 400 patients. The current work provides novel insights by providing a clear message: with a good follow-up of the clinical guidelines, it is not necessary for all patients to be visited by a nephrologist.
Although we advise against the routine evaluation of all patients before cardiac surgery, in the future, it will be possible to consider an intervention only for a selected high-risk subgroup of patients, either in the pre- or post-surgical period. Indeed, we observed a trend toward minimization of CSA-AKI when we evaluated high-risk patients, even though the study was not designed for this purpose and there was not enough sample size to show a significant result.
Performing a Nephrological Intervention on all patients on the cardiac surgery waiting list has not shown a benefit in reducing CSA-AKI, partly because of the low impact of this entity on these patients when good clinical practices are applied. The identification of groups at increased risk of CSA-AKI may provide an opportunity to carry out personalized interventions in this specific group of patients.
The original contributions presented in the study are included in the article. Further inquiries can be directed to the corresponding authors.
The Clinical Research Ethics Committee of the Hospital de Bellvitge approved the study on July 10th, 2014 (ref PR103/14). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
SC: Data curation, Investigation, Methodology, Visualization, Writing – original draft, Writing – review & editing. LO: Data curation, Writing – review & editing. EF: Investigation, Writing – review & editing. AR: Data curation, Writing – review & editing. AC: Writing – review & editing. NL: Writing – review & editing. EM: Writing – review & editing. MH: Conceptualization, Methodology, Writing – review & editing. FS: Data curation, Writing – review & editing. EB: Data curation, Writing – review & editing. JV: Conceptualization, Methodology, Writing – review & editing. JP-F: Conceptualization, Methodology, Writing – review & editing. JS: Conceptualization, Methodology, Writing – review & editing. JC: Conceptualization, Methodology, Project administration, Supervision, Writing – review & editing. NM: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This research was supported by a grant from the SENEFRO Foundation (Spanish Society of Nephrology) (15PSJ013) and a Spanish Government Instituto de Salud Carlos III (ISCIII) Grant RICORS 2040 RD21/0005/0021 under the auspices of European Union – NextGenerationEU funds, Mecanismo para la Recuperación y la Resiliencia (MRR). We thank CERCA Programme/Generalitat de Catalunya for institutional support.
We would like to thank Rosa Maria Pérez-Garzón for her assistance in data retrieval and during the selection and recruitment process.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fneph.2024.1470926/full#supplementary-material
1. Englberger L, Suri RM, Li Z, Casey E, Daly R, Dearani J, et al. Clinical accuracy of RIFLE and Acute Kidney Injury Network (AKIN) criteria for acute kidney injury in patients undergoing cardiac surgery. Crit Care. (2011) 15(1). doi: 10.1186/cc9960
2. Howitt SH, Grant SW, Caiado C, Carlson E, Kwon D, Dimarakis I, et al. The KDIGO acute kidney injury guidelines for cardiac surgery patients in critical care: A validation study. BMC Nephrol. (2018) 19(1):149. doi: 10.1186/s12882-018-0946-x
3. Bastin AJ, Ostermann M, Slack AJ, Diller GP, Finney SJ, Evans TW. Acute kidney injury after cardiac surgery according to Risk/Injury/Failure/Loss/End-stage, Acute Kidney Injury Network, and Kidney Disease: Improving Global Outcomes classifications. J Crit Care. (2013) 28:389–96. doi: 10.1016/j.jcrc.2012.12.008
4. Robert AM, Kramer RS, Dacey LJ, Charlesworth D, Leavitt B, Helm R, et al. Cardiac surgery-associated acute kidney injury: A comparison of two consensus criteria. Ann Thorac Surg. (2010) 90:1939–43. doi: 10.1016/j.athoracsur.2010.08.018
5. Coppolino G, Presta P, Saturno L, Fuiano G. Acute kidney injury in patients undergoing cardiac surgery. J Nephrol. (2013) 26:32–40. doi: 10.5301/jn.5000215
6. Brown JR, Kramer RS, MacKenzie TA, Coca SG, Sint K, Parikh CR. Determinants of acute kidney injury duration after cardiac surgery: An externally validated tool. Ann Thorac Surg. (2012) 93:570–6. doi: 10.1016/j.athoracsur.2011.11.004
7. Molnar AO, Parikh CR, Sint K, Coca S, Koyner J, Patel U, et al. Association of postoperative proteinuria with AKI after cardiac surgery among patients at high risk. Clin J Am Soc Nephrol. (2012) 7:1749–60. doi: 10.2215/CJN.13421211
8. Schaubroeck HAI, Vargas D, Vandenberghe W, Hoste EAJ. Impact of AKI care bundles on kidney and patient outcomes in hospitalized patients: a systematic review and meta-analysis. BMC Nephrol. (2021) 22:335. doi: 10.1186/s12882-021-02534-4
9. Meersch M, Schmidt C, Hoffmeier A, Van Aken H, Wempe C, Gerss J, et al. Prevention of cardiac surgery-associated AKI by implementing the KDIGO guidelines in high risk patients identified by biomarkers: the PrevAKI randomized controlled trial. Intensive Care Med. (2017) 43:1551–61. doi: 10.1007/s00134-016-4670-3
10. Nadim MK, Forni LG, Bihorac A, Hobson C, Koyner J, Shaw A, et al. Cardiac and vascular surgery-associated acute kidney injury: The 20th International Consensus Conference of the ADQI (Acute Disease Quality Initiative) Group. J Am Heart Assoc. (2018) 7(11):e008834. doi: 10.1161/JAHA.118.008834
11. Mehta RL, Kellum JA, Shah SV, Molitoris B, Ronco C, Warnock D, et al. Acute Kidney Injury Network: Report of an initiative to improve outcomes in acute kidney injury. Crit Care. (2007) 11:1–8. doi: 10.1186/cc5713
12. Marco PS, Nakazone MA, Maia LN, MaChado MN. Cardiac surgery-associated acute kidney injury in patients with preserved baseline renal function. Braz J Cardiovasc Surg. (2022) 37:613–21. doi: 10.21470/1678-9741-2022-0108
13. Demirjian S, Bashour CA, Shaw A, Schold J, Simon J, Anthony D, et al. Predictive accuracy of a perioperative laboratory test-based prediction model for moderate to severe acute kidney injury after cardiac surgery. JAMA - J Am Med Assoc. (2022) 327:956–64. doi: 10.1001/jama.2022.1751
14. Tseng PY, Chen YT, Wang CH, Chiu K, Peng Y, Hsu S, et al. Prediction of the development of acute kidney injury following cardiac surgery by machine learning. Crit Care. (2020) 24(1):478. doi: 10.1186/s13054-020-03179-9
15. Perry Wilson F, Martin M, Yamamoto Y, Partridge C, Moreira E, Arora T, et al. Electronic health record alerts for acute kidney injury: Multicenter, randomized clinical trial. BMJ. (2021) 372:1–10. doi: 10.1136/bmj.m4786
16. Alhulaibi AA, Alruwaili AM, Alotaibi AS, Alshakhs FN, Alramadhan HS, Koudieh MS. Validation of various prediction scores for cardiac surgery-associated acute kidney injury. J Saudi Hear Assoc. (2022) 34:222–31. doi: 10.37616/2212-5043.1322
17. Vasquez-Rios G, Moledina DG, Jia Y, McArthur E, Mansour S, Thiessen-Philbrook H, et al. Pre-operative kidney biomarkers and risks for death, cardiovascular and chronic kidney disease events after cardiac surgery: the TRIBE-AKI study. J Cardiothorac Surg. (2022) 17:1–12. doi: 10.1186/s13019-022-02066-4
18. Choe SH, Cho H, Bae J, Ji S, Yoon H, Lee H, et al. Severity and duration of acute kidney injury and chronic kidney disease after cardiac surgery. J Clin Med. (2021) 10(8):1556. doi: 10.3390/jcm10081556
19. Ishani. The magnitude of acute serum creatinine increase after cardiac surgery and the risk of chronic kidney disease, progression of kidney disease, and death (Archives of Internal Medicine. Arch Intern Med. (2011) 171:1919. doi: 10.1001/archinternmed.2011.527
20. Zhao L, Yang X, Zhang S, Zhou X. Iron metabolism-related indicators as predictors of the incidence of acute kidney injury after cardiac surgery : a meta-analysis. Ren Fail. (2023) 45(1). doi: 10.1080/0886022X.2023.2201362
21. Karkouti K. Transfusion and risk of acute kidney injury in cardiac surgery. Br J Anaesth. (2012) 109:i29–38. doi: 10.1093/bja/aes422
22. Zhang H, Wang Z, Tang Y, Chen X, You D, Wu Y, et al. Prediction of acute kidney injury after cardiac surgery: model development using a Chinese electronic health record dataset. J Transl Med. (2022) 20:1–15. doi: 10.1186/s12967-022-03351-5
23. Menez S, Moledina DG, Garg AX, Thiessen-Philbrook H, McArthur E, Jia Y, et al. Post-operative Biomarkers and risk of chronic kidney disease after cardiac surgery: The TRIBE-AKI Study. Kidney Int. (2021) 99(3):716–24. doi: 10.1016/j.kint.2020.06.037.Post-Operative
24. Wu B, Chen J, Yang Y. Biomarkers of acute kidney injury after cardiac surgery: A narrative review. BioMed Res Int. (2019) 2019. doi: 10.1155/2019/7298635
Keywords: acute kidney injury, cardiac surgery, nephrology intervention, clinical trials, intensive care
Citation: Codina S, Oliveras L, Ferreiro E, Rovira A, Coloma A, Lloberas N, Melilli E, Hueso M, Sbraga F, Boza E, Vazquez JM, Pérez-Fernández JL, Sabater J, Cruzado JM and Montero N (2024) Nephrology intervention to avoid acute kidney injury in patients awaiting cardiac surgery: randomized clinical trial. Front. Nephrol. 4:1470926. doi: 10.3389/fneph.2024.1470926
Received: 26 July 2024; Accepted: 09 October 2024;
Published: 13 November 2024.
Edited by:
Jill Moser, University Medical Center Groningen, NetherlandsReviewed by:
Casper Franssen, University Medical Center Groningen, NetherlandsCopyright © 2024 Codina, Oliveras, Ferreiro, Rovira, Coloma, Lloberas, Melilli, Hueso, Sbraga, Boza, Vazquez, Pérez-Fernández, Sabater, Cruzado and Montero. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Nuria Montero, bnVyaWFtb250ZXJvcGVyZXpAZ21haWwuY29t; Josep M. Cruzado, am1jcnV6YWRvQGJlbGx2aXRnZWhvc3BpdGFsLmNhdA==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.