 Anika Lucas1,2Jeanette Rutledge2
Anika Lucas1,2Jeanette Rutledge2 Richard Sloane3Katherine Hall3,4Ciara Green2Carl Pieper3Cathleen Colón-Emeric3,4,5
Richard Sloane3Katherine Hall3,4Ciara Green2Carl Pieper3Cathleen Colón-Emeric3,4,5 Rasheeda Hall1,2,3*
Rasheeda Hall1,2,3*- 1Durham Veterans Affairs Healthcare System, Renal Section, Durham, NC, United States
- 2Department of Medicine, Division of Nephrology, Duke University, Durham, NC, United States
- 3Center for the Study of Aging and Human Development, Duke University, Durham, NC, United States
- 4Durham Veterans Affairs Healthcare System, Geriatric Research Education and Clinical Center, Durham, NC, United States
- 5Department of Medicine, Division of Geriatrics, Duke University, Durham, NC, United States
Background: Physical resilience, or the ability to recover after a physical stressor, declines with aging. Efforts to preserve physical resilience in the older dialysis population are critically needed; however, validated, patient-centered measures that are sensitive to change are also needed. Our objective was to assess accelerometer-derived step count variability, or a measure of intra-individual variation in physical activity, as a potential measure of physical resilience among older adults receiving hemodialysis.
Methods: Community-dwelling ambulatory older adults receiving in-center hemodialysis were prospectively enrolled. Participants wore wrist accelerometers during daytime hours on both dialysis and non-dialysis days up to 14 days, and the feasibility of accelerometer use was assessed from wear time. We used accelerometer data to compute step counts in 4-hour blocks and step count variability. Physical function was assessed with the Short Physical Performance Battery (SPPB which includes gait speed test), grip strength, activities of daily living (ADLs) instruments, and life space mobility. We assessed interval fatigue (subjective rating from 0 to 10) on dialysis and non-dialysis days and self-reported recovery time. We assessed the correlations of step count variability with measures of physical function and step count and interval fatigue.
Results: Of 37 enrolled participants, 29 had sufficient accelerometer data for analyses. Among the 29 participants, mean (SD) age was 70.6(4.8) years, and 55% (n=16) were male and 72% (n=21) were Black race. Participants were largely sedentary with median (Q1-Q3) self-reported total kilocalories per week of 200 (36–552). Step count variability was positively correlated with measures of physical function: SPPB (r=0.50, p<0.05), gait speed (r=0.59, p<0.05), handgrip strength (r=0.71, p<0.05), Instrumental ADLs (r=0.44, p<0.05) and life space mobility (r=0.54, p<0.05).There was a weak inverse correlation between post-dialysis step counts (4-hour blocks after a dialysis session) and post-dialysis interval fatigue [r=-0.19 (n=102, p=0.06).
Conclusions: Physical activity assessment via accelerometer is feasible for older adults receiving hemodialysis. Step count variability correlated with physical function, so it may be a novel measure of physical resilience. Further studies are needed to validate this measure.
Introduction
Among older adults receiving hemodialysis, nearly 40% experience a decline in physical function in a given year (1). The remaining 60% maintain or improve their physical function. This heterogeneity is likely in part explained by variations in physical resilience (2). Physical resilience encompasses the ability to maintain or recover functioning after a physical stressor (2). Studies of physical resilience in older dialysis patients may elucidate clues for maintaining physical function and quality of life (3, 4). However, there is no unifying understanding of physical resilience or validated measures of physical resilience in older adults receiving hemodialysis.
Physical resilience for a hemodialysis patient can manifest as an individual’s ability to recover after the hemodynamic and pro-inflammatory stress imposed by each hemodialysis session (5). We hypothesized that physical resilience, or degree of recovery, would be reflected by how activity patterns recover to baseline following a hemodialysis session. Accelerometry has been used to assess activity patterns through step counts in hemodialysis patients in prior studies (6–8). Therefore, step count variability, or a measure of intra-individual variation in step counts in discrete time intervals, could reflect recovery after hemodialysis. For example, a patient with higher step count variability would have wider shifts in physical activity across intervals because they spent more time in a day active than resting. As in prior studies of dynamical systems (e.g. heart rate variability, inflammatory response) (9, 10), higher step count variability reflects higher physiological complexity, or an individual’s ability to demonstrate physiological adaptations after a stressor, which is considered a hallmark of successful aging (11–13). Understanding if step count variability can provide information suggestive of physical resilience is valuable for development of resilience measures for older adults receiving hemodialysis.
The primary objective of this study was to determine the role of physical activity assessment via accelerometer in physical resilience. To achieve this objective, we conducted a prospective cohort study in older adults receiving hemodialysis to assess the feasibility of accelerometer use and the relationship between step count variability and physical function. Because accelerometer use can be impractical, we also explored additional measures (e.g., serial measures of fatigue, self-reported recovery time) and their relationship with physical activity to identify potential alternative measures.
Materials and methods
This was a prospective, longitudinal feasibility study that aimed to evaluate physical activity as a potential measure of physical resilience in older patients receiving in-center hemodialysis. We recruited a convenience sample of 37 older adults (≥ 65 years) receiving hemodialysis sessions from 2017 to 2018. Exclusion criteria included individuals who were not ambulatory, those who did not exhibit independence in all ADLs (e.g., long-term care residents), those with advanced dementia, non-English speaking individuals, and those in hospice. All subject screening, recruitment, and consent occurred at outpatient dialysis clinics within 32 miles of Duke University Hospital. This protocol was approved by the Duke IRB (Pro 00075802), and all patients provided written informed consent.
Physical activity
Participants underwent home physical activity monitoring for 14 consecutive days using a wrist-mounted Actigraph accelerometer (models GT3X and GT3X+; Pensacola, FL). The Actigraph triaxial accelerometer has been widely validated as a reliable instrument to estimate daily physical activity (14).
Activity monitors and instructions were given to participants during an initial study visit on a typical dialysis session day. Study personnel demonstrated wrist placement and explained the accelerometer to the participants using a standardized script. Participants wore the device during day-time hours, except at times when there was a possibility of the device becoming wet. The accelerometer was worn on non-access wrist (a wrist that does not have a functional arteriovenous access for dialysis) attached to a wrist band.
Alternative measures of physical resilience
We postulated that alternative measures of physical resilience would include interval fatigue and self-reported recovery time (15). As in other studies evaluating fatigue variability in the dialysis population (16, 17), interval fatigue was assessed during the period of home physical activity monitoring. Study personnel called and/or texted participants at three regular intervals throughout each weekday (e.g., 10AM, 2PM, and 6PM) to ask participants to report their fatigue score at that moment on a numeric rating scale (0–10). A score of 0 indicated “no fatigue” and a score of 10 “fatigue as bad as you can imagine.” (18) We also assessed self-reported recovery time by asking the following validated question: “How long does it take for you to recover from a dialysis session?” (19)
Additional measures
To obtain a baseline assessment of physical function, we administered the following measures in the dialysis unit (before dialysis on a mid-week dialysis day): Short Physical Performance Battery (SPPB), [SPPB includes assessments of gait speed, time to complete 5 chair stands, and balance. All tests in the SPPB are scored 0-4, for a total score of 0-12, with higher scores indicating better function], handgrip strength (as measured using a dynamometer), Lawton (20) and Katz (21) ADLs, and Life-Space Mobility (22). We also collected demographics, comorbidities using the Charlson Comorbidity Index, and length of time on dialysis. Participants were also asked to complete the Low Physical Activity Questionnaire, an instrument that converts survey responses about physical activity into total kilocalories(kcal)/week (23).
Statistical analyses
Using ActiLife v6.12 data processing software, accelerometer physical activity data was processed into step counts (24). Only individuals who had ≥ 10 hours of valid wear time on 3 or more days were retained for analyses (25). To assess changes in step counts over an interdialytic period, participants had to have at least 3 days of data that included both dialysis and non-dialysis days. Step counts were summed in 4-hour (4-hr) blocks. With knowledge of each participant’s dialysis schedule, each participant’s hemodialysis session was represented in one 4-hr block (see blue dots in Figure 1). Then, all other 4-hr blocks, or non-dialysis blocks, were assigned relative to the participant’s hemodialysis 4-hr block. In an approach similar to heart rate variability (9, 26), step count variability was estimated from the difference in step counts from one 4-hr block to another (each dot in Figure 1). Each participant had a series of step count differences determined over all of their 4-hr blocks, and step count variability for each participant was calculated as the standard deviation of the absolute value of all of the step count differences (formula in Figure 1). Similar to heart rate variability, higher step count variability reflects higher physiological complexity which is essential for recovery from a stressor (9).

Figure 1 Schematic of Step Count Variability Measure Using a Participant’s Data. Here is an example of a subset of 4-hour blocks (blue indicates dialysis block, and red indicates non-dialysis block) between two consecutive dialysis sessions for one participant. Step count differences between each 4-hour block were calculated for each participant. Then, the step count variability was calculated as the standard deviation of the series of step count differences for each participant.
Analyses were conducted using data from participants with sufficient step count data. Summary statistics are presented as mean ± SD or median (Q1-Q3) for continuous data and presented as proportions for categorical data. To assess feasibility of accelerometer use, we calculated the average time participants wore it out of the expected 14 days. We assessed feasibility of interval fatigue assessment from the proportion of participants with any missing interval fatigue data. Assumptions allowing the use of parametric analysis were largely met in order to perform a Pearson correlation to assess the relationship between step counts and step count variability (measured in 4-hr blocks). We visualized the relationship between step count variability by tertiles and step count during hemodialysis and post-dialysis 4-hr blocks over three consecutive dialysis days. To assess step count variability as a measure of physical resilience, we assessed Pearson correlations between step count variability and physical function (SPPB total score, gait speed, hand grip strength, ADLS, and life space mobility). These correlations were conducted using both Pearson and Spearman correlations, with similar results for both. For ease of interpretation we are presenting the Pearson correlation results.
We assessed correlations of physical activity and alternative measures of physical resilience including fatigue. Because fatigue was not normally distributed, Spearman’s correlation was used to assess the association between step count (measured in 4-hr blocks) and interval fatigue for both post-dialysis 4-hr blocks and for all other 4-hr blocks. We assessed the correlation between step count variability and self-reported recovery time and total kcal/week (derived from the Low Physical Activity Questionnaire). All statistical analyses were performed using SAS (version 9.4, SAS Inc., Cary NC).
Results
Cohort characteristics
Of 37 participants, 8 were excluded from analyses for insufficient data (wearing accelerometer < 3 days, or only on dialysis days (n=6), or study withdrawal due to illness (n=2)) (Figure 2). Among the 29 participants in the analytic cohort, mean (SD) age was 70.6 (4.8) years, 55% (n=16) were men, and 72% (n=21) were Black race (Table 1). Participants had mean (SD) SPPB 6.3 (3.2), mean (SD) life-space mobility score 21.8 (8.4) and self-reported caloric expenditure was median (Q1-Q3) 200 (36-552) total kcal/week. While participants generally had preserved basic ADLs, instrumental ADLs, and handgrip strength (28); there was heterogeneity in self-reported recovery time [median (Q1-Q3): 2 (0, 24) hours].
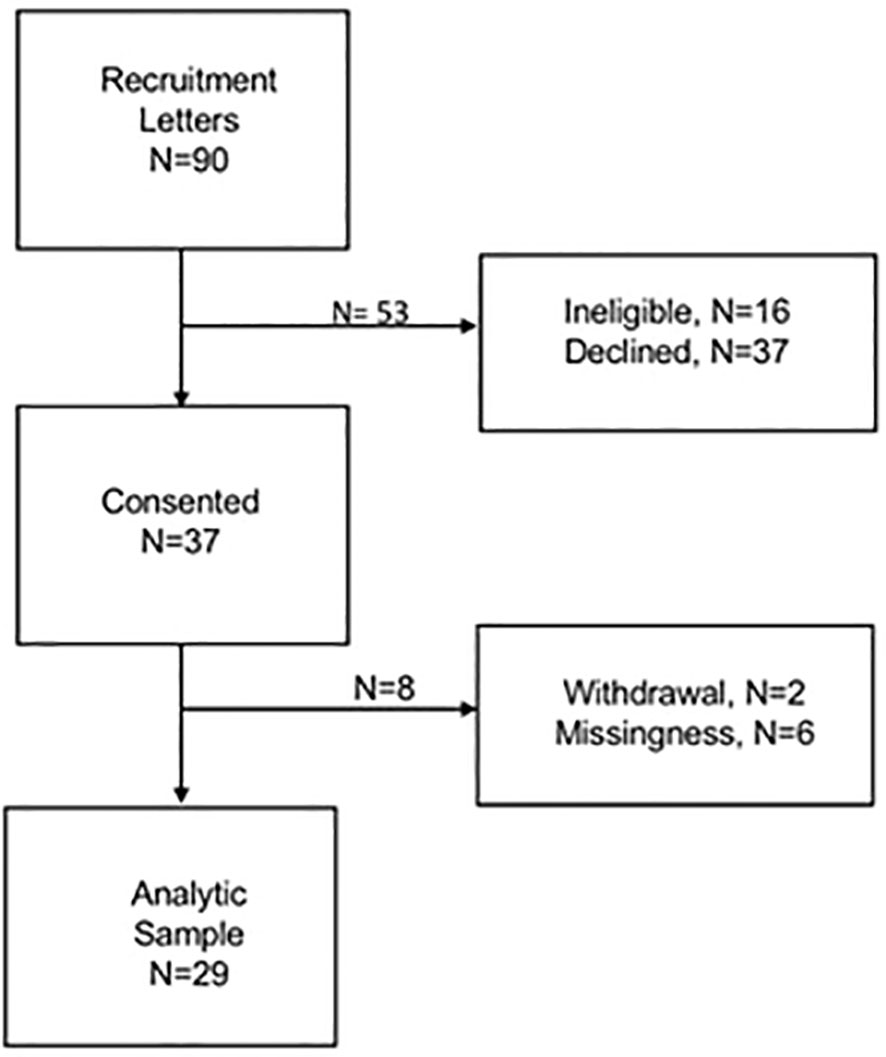
Figure 2 Flowchart of study participants .
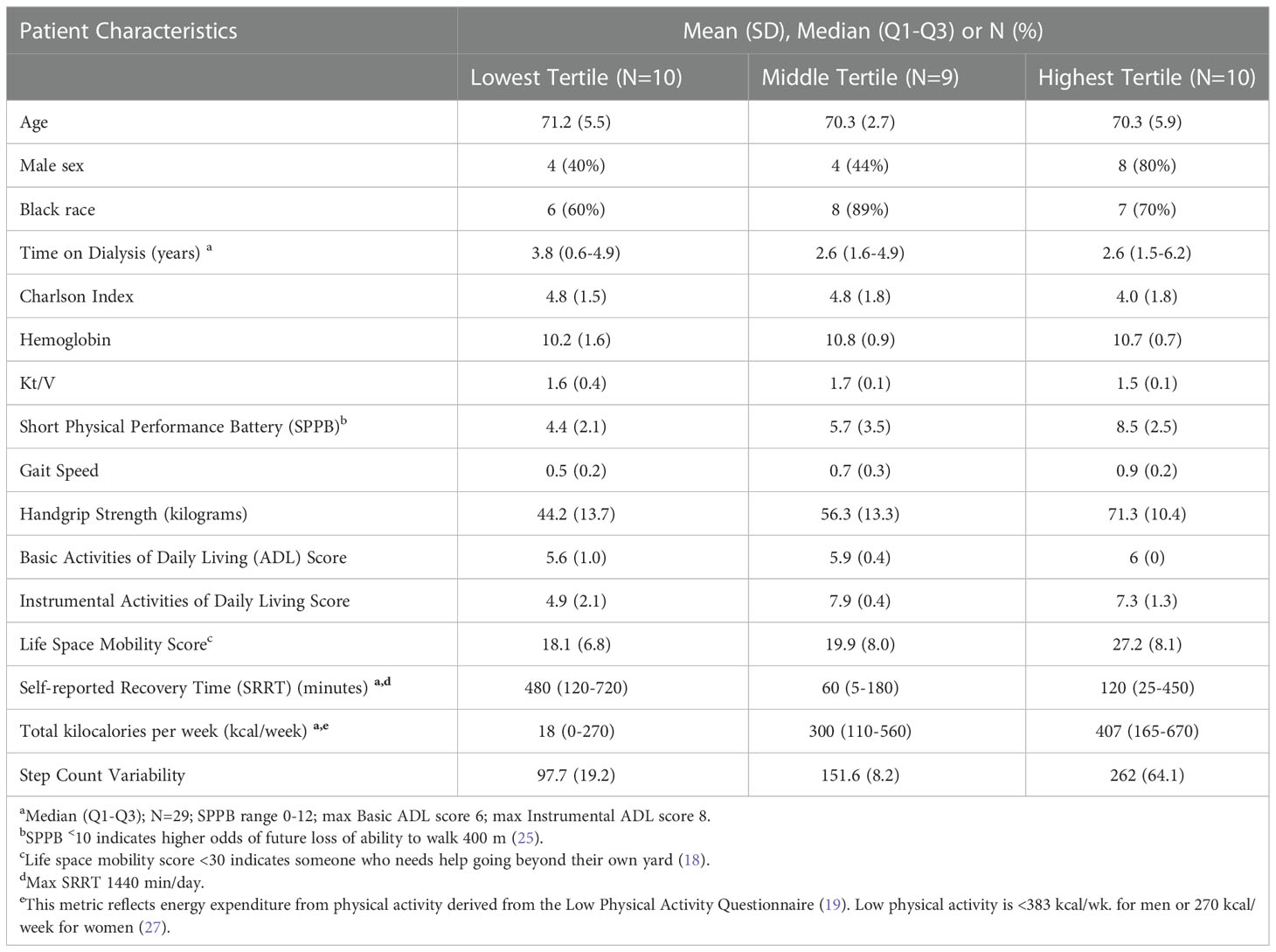
Table 1 Baseline characteristics of participants.
Feasibility
On average, participants wore accelerometer on their wrist 14.9 (1.1) hours a day over 12.9 (1.9) days. Although one of the participants excluded from analyses noted the device “bothered” them, none of the participants included in our analyses reported side effects. The majority of participants (25 of 29) had some missing interval fatigue data.
Step counts and their correlation with step count variability
Figure 3 shows example patterns of step counts at 4-hr blocks:1) a participant with similar step counts during dialysis 4-hr blocks and other 4-hour blocks (Figure 3A) and 2) a participant with higher step counts at 4-hr blocks outside of dialysis in most blocks (Figure 3B). There was a strong, positive correlation between step count and step count variability (Pearson’s r=0.89, p<0.0001). The mean step count variability was 140.0 ± 67.3 steps, and participants within highest tertile of step count variability had higher step counts in post-dialysis 4-hr blocks compared to those in lower tertiles (Figure 4).
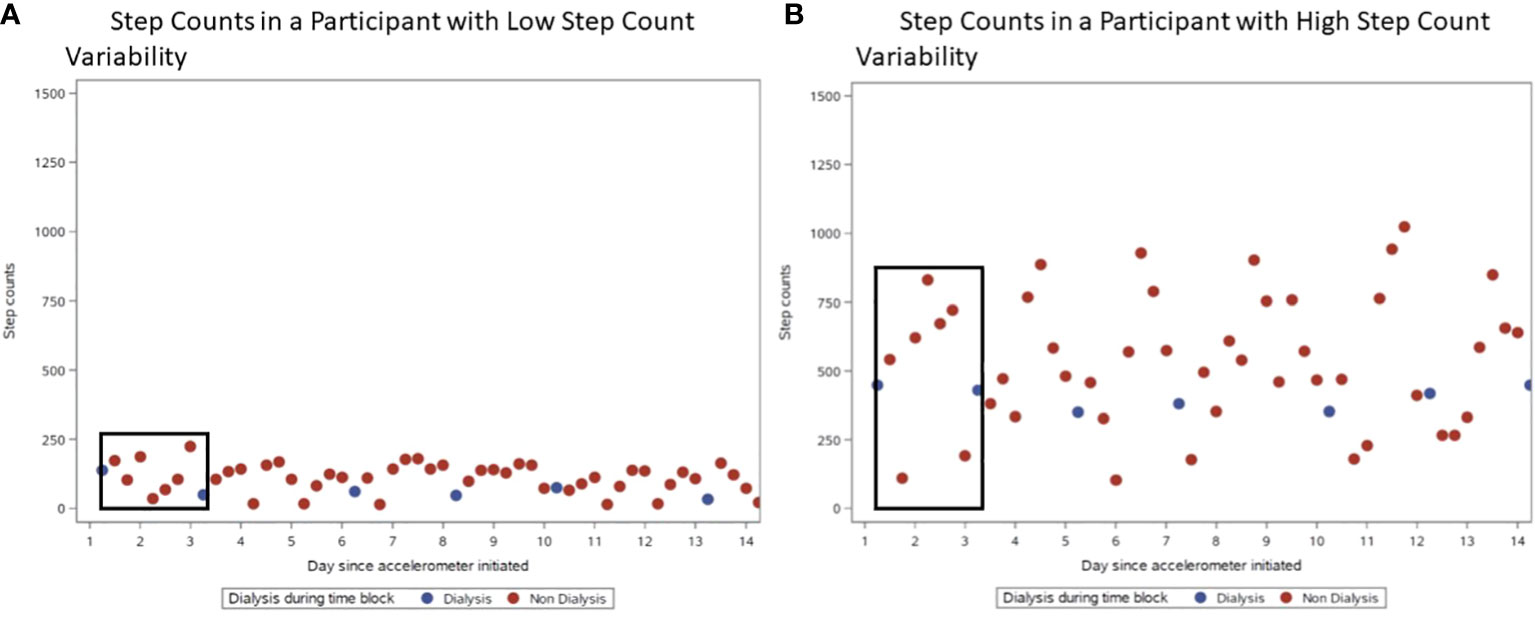
Figure 3 Examples of Physical Activity Data at 4-hour blocks. For both plots from actual study participants, the blue dots indicate dialysis 4-hour blocks, and the red dots indicate non-dialysis 4-hour blocks. Black boxes demonstrate a set of 4-hour blocks between two consecutive dialysis sessions. (A) Step Counts in a Participant with Low Step Count Variability. (B) Step Counts in a Participant with High Step Count Variability.
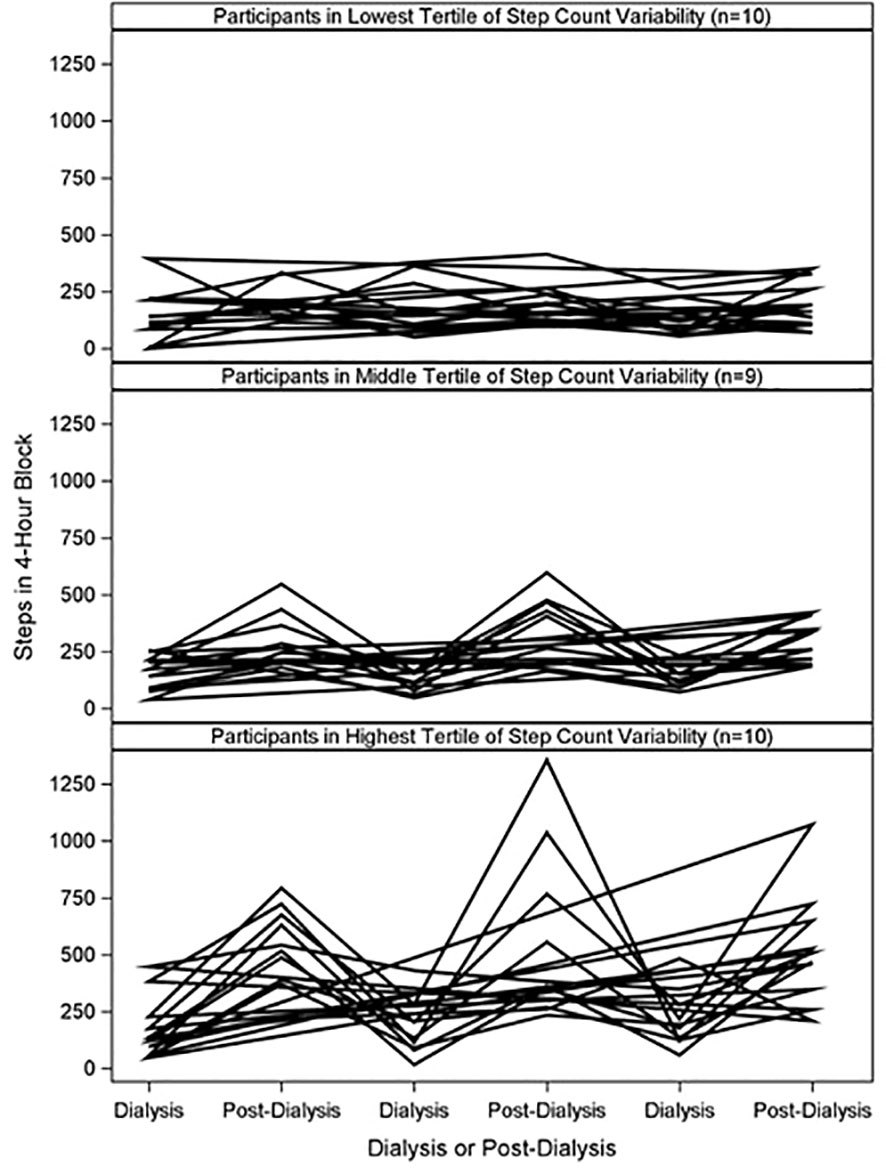
Figure 4 Individual Step Counts at Dialysis and Post-Dialysis Blocks by Tertile of Step Count Variability. Participants were grouped into tertiles of step count variability. Plot shows step counts at dialysis and post-dialysis 4-hour blocks from three distinct dialysis days.
Step count variability and its correlation with measures of physical function
Step count variability had a positive Pearson correlation with physical function measures: SPPB, gait speed, handgrip strength, ADLs and life space mobility (Table 2). Highest correlations were with objective measures of physical function: gait speed (Pearson’s r=0.59, p-value=0.001) and handgrip strength (Pearson’s r=0.71, p-value<0.0001).
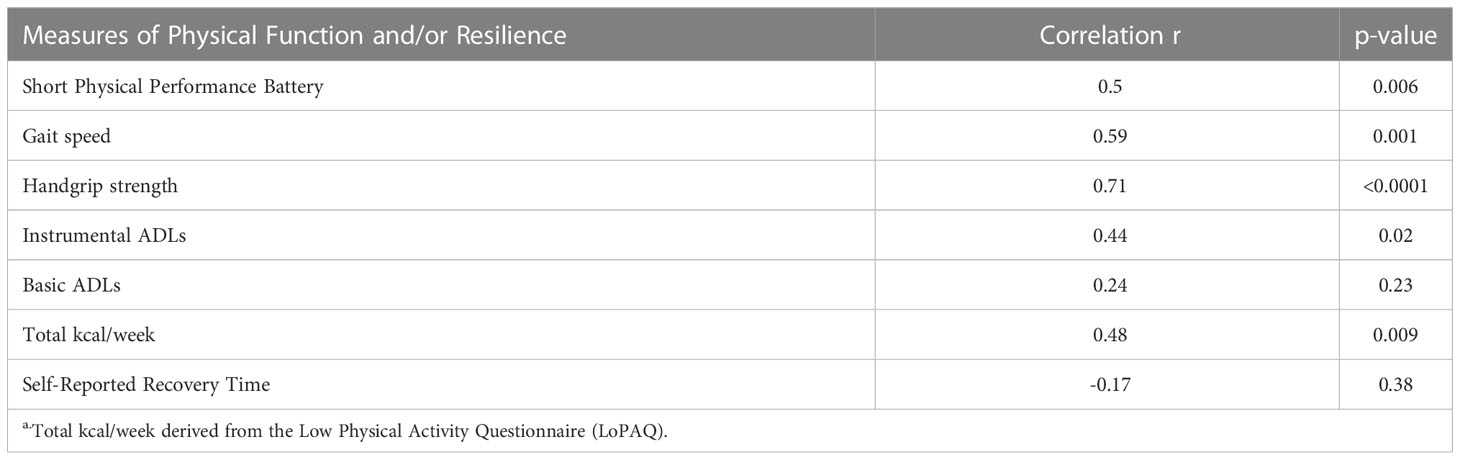
Table 2 Pearson Correlations between Step Count Variability and Measures of Physical Function and/or Resilience a.
Step count/step count variability and correlation with alternative measures of physical resilience
Median (Q1-Q3) interval fatigue after hemodialysis was slightly higher than fatigue reported on non-dialysis days [4(2-6) vs. 3(1-5)]. There was a weak, inverse Spearman correlation between step counts and interval fatigue in the 4-hr block after hemodialysis [r=-0.19 (n=102, p=0.06)], and, for step counts and interval fatigue at all other 4-hr blocks [r=-0.17 (n=210, p=0.01)].
Step count variability had a positive, moderate Pearson correlation with total kcal/week (from Low Physical activity Questionnaire) but weak, inverse Pearson correlation with self-reported recovery time (Table 2).
Discussion
In this study, we found it is feasible to measure physical activity via accelerometer in an older dialysis cohort. Step count variability, a measure that reflects how activity patterns return to baseline after hemodialysis, had moderate to high correlations with physical function measures: hand grip strength, gait speed, life space mobility, SPPB, and ADLs. These findings suggest that step count variability could be a measure of physical resilience in older adults receiving dialysis. Additional work is needed to confirm that step count variability is sensitive to change with resilience-promoting interventions and therefore reasonable target for efforts to maintain or improve physical resilience in this population.
This study uniquely identifies step count variability as a potential measure of physical resilience based on the correlations between step count variability and physical function measures in older adults receiving dialysis. Prior studies in both a general older adult cohort and a dialysis exercise intervention cohort also demonstrate a positive correlation between physical activity (either exercise intensity or accelerometer) and physical function measured by physical performance measures or questionnaire (27, 29). In a similar study design, Majchrzak et al. found physical activity and physical function to be positively correlated, however they found physical activity to be similar on both dialysis and non-dialysis days (6). Our study provides novel information by exploring recovery of physical activity after dialysis through step count variability, instead of step counts alone. Using step count variability, we found that the extent of physical activity within 4-hr blocks does vary among older adults when they are not receiving hemodialysis and can indicate better physical function even in older participants who on average had low physical function based on SPPB and life-space mobility scores (22, 30).
Prior evidence suggests self-reported fatigue and recovery time would be inversely related to physical activity (19) (15, 31). However, our study showed self-reported fatigue and recovery time instruments, while less resource-intensive than accelerometer use, had only weak inverse correlations with physical activity. These findings could be partially explained by the fact that interval fatigue assessment could not be reliably obtained in this population and the small sample size. The weak correlations may also partially be explained by their inherent subjectivity. Some patients receiving dialysis may rate fatigue or recovery time that does not correspond with their activity level for a myriad of reasons to stay active despite fatigue (e.g., caregiving responsibilities, employment) (32). Also, fatigue and recovery time may be interpreted differently from person to person due to culture or other individual attributes (33). Despite the findings from this pilot study, fatigue and post-dialysis recovery are important patient-centered outcomes identified by the hemodialysis population (34, 35). Future work is needed to evaluate interval fatigue and recovery time as potential measures of physical resilience. For now, clinicians and researchers should consider fatigue and low physical activity as separate, although related issues, in clinical evaluation and outcome measures.
While most physical activity studies in the dialysis population have been conducted in patients 1-2 decades younger than those in this cohort (31, 32), our study diminishes concern about the feasibility of accelerometer use in older adults receiving dialysis. There may be concern that older adults may not be able to follow instructions and adhere to the study protocol; however, the majority (>80%) followed instructions, wearing the device for nearly 15 hours a day, and had eligible data for analyses. Another concern would be that older adults receiving dialysis are less active (demonstrated by the low self-reported total kcal/week by participants (36)) than younger patients, so the data may not be robust enough to identify differences within a sedentary group. However, we found clear correlations with physical function measures. Given these early findings, additional studies are needed to validate this measure against other clinical outcomes thought to reflect physical resilience (e.g., recovery after elective surgery).
Then, subsequent applications of step count variability could involve use as an outcome measure in studies designed to improve physical resilience. Such work would be useful as often physical activity improvement may precede other measurable improvements (e.g., physical function or quality of life). Additionally, step count variability could be applied in identification of high risk patients as low physical resilience phenotypes have been associated with adverse outcomes in older adults receiving hemodialysis (37).
This study’s strength lies in its unique cohort of older Black adults receiving hemodialysis (average age 71) who are not routinely included in research studies. Our study had several limitations. First, our measure of interval fatigue on a scale ranging from 0 to 10, is not validated, subject to measurement error, and interval fatigue data was missing in most participants. As a result, we were not able to explore additional analyses of fatigue as a measure of physical resilience or evaluate correlation with physical function. Additional studies for measuring interval fatigue should explore formal psychometric evaluation to create a more valid measure and approach for data collection. The existing Standardized Outcomes in Nephrology-Hemodialysis fatigue instrument could be an alternative measure for interval fatigue after additional studies confirm the instrument’s responsiveness to change and its validation in diverse populations (38). Then, further research could more adequately evaluate the relationships of fatigue with physical function and physical resilience. Second, some participants were excluded for not wearing accelerometer as directed. Future use of accelerometers, especially in an older study population, should require additional reminders and/or staff support to improve study protocol adherence. Third, physical activity may have been influenced by seasonal differences, however we still observed that step count variability was correlated with physical function. Last, the small sample size makes our findings susceptible to Type 1 and Type 2 error, such that these findings should be evaluated in a larger sample to confirm validity.
In conclusion, we identified step count variability as a potential measure of physical resilience for older adults receiving dialysis. This study provides a significant contribution for measure selection in future studies of physical resilience in the dialysis population. Such studies are needed to establish evidence for maintenance or improvement of physical resilience in older adults receiving hemodialysis.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by Duke University IRB. The patients/participants provided their written informed consent to participate in this study.
Author contributions
RH, KH, RS, CP, CC-E contributed to conception and study design. JR and RH collected data. CG, KH, RH organized the data. RS performed statistical analyses. AL and RH wrote the first draft of the manuscript. All authors contributed to manuscript revision, read, and approved the submitted version.
Funding
AL was a part of the American Kidney Fund Clinical Scientist in Nephrology Program. KH was supported by VA Merit Award (RRD RX003120) National Institute on Aging under Award Numbers P30AG028716, K76AG059930, and National Center for Advancing Translational Sciences under Award Number KL2TR001115 of the National Institutes of Health. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. This research is also supported by the American Society of Nephrology. The findings and interpretation do not necessarily represent the official views of this foundation.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Hall RK, Luciano A, Pendergast JF, Colon-Emeric CS. Self-reported physical function decline and mortality in older adults receiving hemodialysis. Kidney Med (2019) 1(5):288–95. doi: 10.1016/j.xkme.2019.08.001
2. Whitson HE, Duan-Porter W, Schmader KE, Morey MC, Cohen HJ, Colón-Emeric CS. Physical resilience in older adults: Systematic review and development of an emerging construct. J Gerontol A Biol Sci Med Sci (2016) 71(4):489–95. doi: 10.1093/gerona/glv202
3. Colón-Emeric C, Whitson HE, Pieper CF, Sloane R, Orwig D, Huffman KM, et al. Resiliency groups following hip fracture in older adults. J Am Geriatr Soc (2019) 67(12):2519–27. doi: 10.1111/jgs.16152
4. Duan-Porter W, Cohen HJ, Demark-Wahnefried W, Sloane R, Pendergast JF, Snyder DC, et al. Physical resilience of older cancer survivors: An emerging concept. J Geriatr Oncol (2016) 7(6):471–8. doi: 10.1016/j.jgo.2016.07.009
5. Jofre R, Rodriguez-Benitez P, Lopez-Gomez JM, Perez-Garcia R. Inflammatory syndrome in patients on hemodialysis. J Am Soc Nephrol (2006) 17(12 Suppl 3):S274–80. doi: 10.1681/ASN.2006080926
6. Majchrzak KM, Pupim LB, Chen K, Martin CJ, Gaffney S, Greene JH, et al. Physical activity patterns in chronic hemodialysis patients: comparison of dialysis and nondialysis days. J Ren Nutr (2005) 15(2):217–24. doi: 10.1053/j.jrn.2004.08.002
7. Gomes EP, Reboredo MM, Carvalho EV, Teixeira DR, Carvalho LF, Filho GF, et al. Physical activity in hemodialysis patients measured by triaxial accelerometer. BioMed Res Int (2015) 2015:645645. doi: 10.1155/2015/645645
8. Shiota K, Hashimoto T. Promotion and support of physical activity in elderly patients on hemodialysis: a case study. J Phys Ther Sci (2016) 28(4):1378–83. doi: 10.1589/jpts.28.1378
9. Chaves PH, Varadhan R, Lipsitz LA, Stein PK, Windham BG, Tian J, et al. Physiological complexity underlying heart rate dynamics and frailty status in community-dwelling older women. J Am Geriatr Soc (2008) 56(9):1698–703. doi: 10.1111/j.1532-5415.2008.01858.x
10. Whitson HE, Crabtree D, Pieper CF, Ha C, Au S, Berger M, et al. A template for physical resilience research in older adults: Methods of the PRIME-KNEE study. J Am Geriatr Soc (2021) 69(11):3232–41. doi: 10.1111/jgs.17384
11. Merchant RA, Aprahamian I, Woo J, Vellas B, Morley JE. Editorial: Resilience and successful aging. J Nutr Health Aging (2022) 26(7):652–6. doi: 10.1007/s12603-022-1818-4
12. Varadhan R, Walston JD, Bandeen-Roche K. Can a link be found between physical resilience and frailty in older adults by studying dynamical systems? J Am Geriatr Soc (2018) 66(8):1455–8. doi: 10.1111/jgs.15409
13. Whitson HE, Cohen HJ, Schmader KE, Morey MC, Kuchel G, Colon-Emeric CS. Physical resilience: Not simply the opposite of frailty. J Am Geriatr Soc (2018) 66(8):1459–61. doi: 10.1111/jgs.15233
14. Jarrett H, Fitzgerald L, Routen AC. Interinstrument reliability of the ActiGraph GT3X+ ambulatory activity monitor during free-living conditions in adults. J Phys Act Health (2015) 12(3):382–7. doi: 10.1123/jpah.2013-0070
15. Jhamb M, Weisbord SD, Steel JL, Unruh M. Fatigue in patients receiving maintenance dialysis: a review of definitions, measures, and contributing factors. Am J Kidney Dis (2008) 52(2):353–65. doi: 10.1053/j.ajkd.2008.05.005
16. Brys ADH, Lenaert B, Van Heugten CM, Gambaro G, Bossola M. Exploring the diurnal course of fatigue in patients on hemodialysis treatment and its relation with depressive symptoms and classical conditioning. J Pain Symp Manage (2019) 57(5):890–8.e4. doi: 10.1016/j.jpainsymman.2019.02.010
17. Abdel-Kader K, Jhamb M, Mandich LA, Yabes J, Keene RM, Beach S, et al. Ecological momentary assessment of fatigue, sleepiness, and exhaustion in ESKD. BMC Nephrol (2014) 15:29. doi: 10.1186/1471-2369-15-29
18. Murphy SL, Alexander NB, Levoska M, Smith DM. Relationship between fatigue and subsequent physical activity among older adults with symptomatic osteoarthritis. Arthritis Care Res (2013) 65(10):1617–24. doi: 10.1002/acr.22030
19. Lindsay RM, Heidenheim PA, Nesrallah G, Garg AX, Suri R. Daily hemodialysis study group London health sciences c. minutes to recovery after a hemodialysis session: a simple health-related quality of life question that is reliable, valid, and sensitive to change. Clin J Am Soc Nephrol (2006) 1(5):952–9. doi: 10.2215/CJN.00040106
20. Lawton MP, Brody EM. Assessment of older people: self-maintaining and instrumental activities of daily living. Gerontologist (1969) 9(3):179–86. doi: 10.1093/geront/9.3_Part_1.179
21. Katz S, Ford AB, Moskowitz RW, Jackson BA, Jaffe MW. Studies of illness in the aged. the index of adl: a standardized measure of biological and psychosocial function. Jama (1963) 185:914–9. doi: 10.1001/jama.1963.03060120024016
22. Peel C, Baker PS, Roth DL, Brown CJ, Bodner EV, Allman RM. Assessing mobility in older adults: The UAB study of aging life-space assessment. Phys Ther (2005) 85(10):1008–19. doi: 10.1093/ptj/85.10.1008
23. Johansen KL, Painter P, Delgado C, Doyle J. Characterization of physical activity and sitting time among patients on hemodialysis using a new physical activity instrument. J Ren Nutr (2015) 25(1):25–30. doi: 10.1053/j.jrn.2014.06.012
24. Sasaki JE, John D, Freedson PS. Validation and comparison of ActiGraph activity monitors. J Sci Med Sport (2011) 14(5):411–6. doi: 10.1016/j.jsams.2011.04.003
25. Troiano RP, Berrigan D, Dodd KW, Masse LC, Tilert T, McDowell M. Physical activity in the united states measured by accelerometer. Med Sci Sports Exerc (2008) 40(1):181–8. doi: 10.1249/mss.0b013e31815a51b3
26. Task Force of the European Society of Cardiology the North American Society of Pacing Electrophysiology. Heart rate variability. Circulation (1996) 93(5):1043–65. doi: 10.1161/01.CIR.93.5.1043
27. Hrubeniuk TJ, Sénéchal M, Mayo A, Bouchard DR. Association between physical function and various patterns of physical activity in older adults: a cross-sectional analysis. Aging Clin Exp Res (2020) 32(6):1017–24. doi: 10.1007/s40520-019-01288-2
28. Desrosiers J, Bravo G, Hébert R, Dutil E. Normative data for grip strength of elderly men and women. Am J Occup Ther (1995) 49(7):637–44. doi: 10.5014/ajot.49.7.637
29. Manfredini F, Mallamaci F, D'Arrigo G, Baggetta R, Bolignano D, Torino C, et al. Exercise in patients on dialysis: A multicenter, randomized clinical trial. J Am Soc Nephrol (2017) 28(4):1259–68. doi: 10.1681/ASN.2016030378
30. Vasunilashorn S, Coppin AK, Patel KV, Lauretani F, Ferrucci L, Bandinelli S, et al. Use of the short physical performance battery score to predict loss of ability to walk 400 meters: Analysis from the InCHIANTI study. Journals Gerontol: Ser A (2009) 64A(2):223–9. doi: 10.1093/gerona/gln022
31. Sheshadri A, Kittiskulnam P, Johansen KL. Higher physical activity is associated with less fatigue and insomnia among patients on hemodialysis. Kidney Int Rep (2019) 4(2):285–92. doi: 10.1016/j.ekir.2018.10.014
32. Delgado C, Johansen KL. Barriers to exercise participation among dialysis patients. Nephrol Dial Transplant (2012) 27(3):1152–7. doi: 10.1093/ndt/gfr404
33. McLlvenny S. Fatigue as a transcultural issue. Eur J Gen Pract (2000) 6(1):20–2. doi: 10.3109/13814780009074502
34. Tong A, Manns B, Hemmelgarn B, Wheeler DC, Evangelidis N, Tugwell P, et al. Establishing core outcome domains in hemodialysis: Report of the standardized outcomes in nephrology-hemodialysis (SONG-HD) consensus workshop. Am J Kidney Dis (2017) 69(1):97–107. doi: 10.1053/j.ajkd.2016.05.022
35. Urquhart-Secord R, Craig JC, Hemmelgarn B, Tam-Tham H, Manns B, Howell M, et al. Patient and caregiver priorities for outcomes in hemodialysis: An international nominal group technique study. Am J Kidney Dis (2016) 68(3):444–54. doi: 10.1053/j.ajkd.2016.02.037
36. Fried LP, Tangen CM, Walston J, Newman AB, Hirsch C, Gottdiener J, et al. Frailty in older adults: Evidence for a phenotype. Journals Gerontol: Ser A (2001) 56(3):M146–M57. doi: 10.1093/gerona/56.3.M146
37. Hladek MD, Zhu J, Crews DC, McAdams-DeMarco MA, Buta B, Varadhan R, et al. Physical resilience phenotype trajectories in incident hemodialysis: Characterization and mortality risk assessment. Kidney Int Rep (2022) 7(9):2006–15. doi: 10.1016/j.ekir.2022.06.009
Keywords: physical activity, physical function, older adults, hemodialysis, resilience
Citation: Lucas A, Rutledge J, Sloane R, Hall K, Green C, Pieper C, Colón-Emeric C and Hall R (2023) Physical activity is a potential measure of physical resilience in older adults receiving hemodialysis. Front. Nephrol. 2:1032468. doi: 10.3389/fneph.2022.1032468
Received: 30 August 2022; Accepted: 19 December 2022;
Published: 06 January 2023.
Edited by:
Laura Plantinga, Emory University, United StatesReviewed by:
Murilo Guedes, Pontifical Catholic University of Parana, BrazilLuca Neri, Fresenius Medical Care - Applied Advanced Analytics, EMEA region, Italy
Copyright © 2023 Lucas, Rutledge, Sloane, Hall, Green, Pieper, Colón-Emeric and Hall. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Rasheeda Hall, cmFzaGVlZGEuc3RlcGhlbnNAZG0uZHVrZS5lZHU=; @Rasheeda_HallMD