
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Neurorobot. , 26 August 2021
Volume 15 - 2021 | https://doi.org/10.3389/fnbot.2021.723206
This article is part of the Research Topic How Can Wearable Robotic and Sensor Technology Advance Neurorehabilitation? View all 11 articles
 Alexis Brinkemper1*
Alexis Brinkemper1* Mirko Aach2Dennis Grasmücke2Birger Jettkant1Thomas Rosteius1Marcel Dudda3Emre Yilmaz1Thomas Armin Schildhauer1
Mirko Aach2Dennis Grasmücke2Birger Jettkant1Thomas Rosteius1Marcel Dudda3Emre Yilmaz1Thomas Armin Schildhauer1In recent years robotic devices became part of rehabilitation offers for patients suffering from Spinal Cord Injury (SCI) and other diseases. Most scientific publications about such devices focus on functional outcome. The aim of this study was to verify whether an improvement in physiological gait can be demonstrated in addition to the functional parameters after treatment with neurological controlled HAL® Robot Suit. Fifteen subjects with acute (<12 months since injury, n = 5) or chronic (>12 months since injury, n = 10) incomplete paraplegia (AIS B, n = 0/AIS C, n = 2/AIS D, n = 8) or complete paraplegia (AIS A, n = 5) with zones of partial preservation participated. Subjects underwent a body weight supported treadmill training for five times a week over 12 weeks using HAL®. At baseline and at the end of the study a gait analysis was performed and additional functional parameters such as 10-Meter-Walk-Test, Timed-Up-and-Go-Test, 6-Minutes-Walk-Test, and WISCI II score were collected. Results were evaluated for whole group and individually for acute and chronic subgroups. All functional parameters improved. Differences were also found in physiological parameters such as phases of gait cycle and accompanied by significant improvement in all spatiotemporal and gait phase parameters. The presented study shows signs that an improvement in physiological gait can be achieved in addition to improved functional parameters in patients with SCI after completing 12-week training with HAL®.
Trial Registration: DRKS, DRKS00020805. Registered 12 February 2020—Retrospectively registered, https://www.drks.de/DRKS00020805.
In times of increasingly extensive rehabilitation offers and spreading medical technology, robotic therapy approaches, and the use of exoskeletal systems play a progressively important role. For several years, exoskeletons of various manufacturers have been used worldwide for rehabilitation purposes (Aach et al., 2015). Different mechanisms of action enable patients with reduced mobility to regain or improve their walking skills. In terms of their objective, the available models differ in aid, intended for domestic use, and remedies, for example in form of therapy.
In this context, effects of training with HAL® (Hybrid Assistive Limb) Robot Suit (Cyberdyne Inc., Ibaraki, Japan) have been investigated in patients with gait disorders of different etiology for several years. Ueba et al. (2013) and Nilsson et al. (2014) were able to demonstrate the feasibility and safety of training in 22 and 8 patients, respectively, in the acute phase of rehabilitation after stroke. An investigation by Kawamoto et al. (2013) also confirms those findings for chronic stroke patients. Extended by further diagnoses Kubota et al. (2013) concludes in 38 patients [12 strokes, 8 spinal cord injuries (SCI), 4 musculoskeletal diseases, and 14 other diseases] that HAL® training can be performed without occurrence of undesirable events. In Germany, the HAL® Robot Suit was first used in a study by Aach et al. (2015), in which 8 chronic paraplegic patients showed not only a safe usage but also improved in functional testing such like 10-Meter-Walk-Test (10MWT), Timed-Up-and-Go-Test (TUG) and 6-Minutes-Walk-Test (6MWT). Cruciger et al. (2014a) were able to confirm these results also for acute incomplete paraplegic patients. In addition, a positive effect of HAL® training on bladder and bowel function for SCI patients was recently described (Brinkemper et al., 2021).
To date, most investigations have largely focused on functional parameters and treadmill-related data such as distance, walking time or walking speed (Aach et al., 2014; Cruciger et al., 2014a,b; Grasmücke et al., 2017; Jansen et al., 2017, 2018; Sczesny-Kaiser et al., 2017, 2019). To the knowledge of the author it has never been investigated if the improved functional outcome in groups of SCI patients is accompanied by an improvement in gait quality or for example a pathological gait leads to higher velocity. The purpose of this study was to verify for the first time whether an improvement in physiological gait can be demonstrated in addition to the functional parameters in a group of SCI patients.
To investigate intra-individual changes in gait quality of the subjects during the training period, a prospective pre-post research design with repeated measurements of the same subjects was chosen.
The study involved 15 subjects (five females, 10 males) with an average age of 43.33 ± 12.47 years at the time of enrolment, an average height of 172.93 ± 8.46 cm and a mean body weight of 72.2 ± 14.5 kg (Table 1). The inclusion criteria were an acute (<12 months) or chronic (>12 months) incomplete paraplegia (American spinal injury association impairment scale (AIS) B/C/D) or complete paraplegia (AIS A) with zones of partial preservation (ZPP). Further details are given in Table 1. Five acute patients (average time since injury 27 weeks) and 10 chronic patients (average time since injury 752 weeks) participated. Chronic patients underwent conventional training before trial began and were at a stable baseline. The subjects had to have motor functions of flexor and extensor muscles of the hips and knees to be able to control the exoskeleton [Frankel and Janda Grade 1/5 or 2/5 (Janda, 1983)]. Sample size was limited as subjects had to be able to walk at least 12 m to complete gait analysis at beginning of their training period.
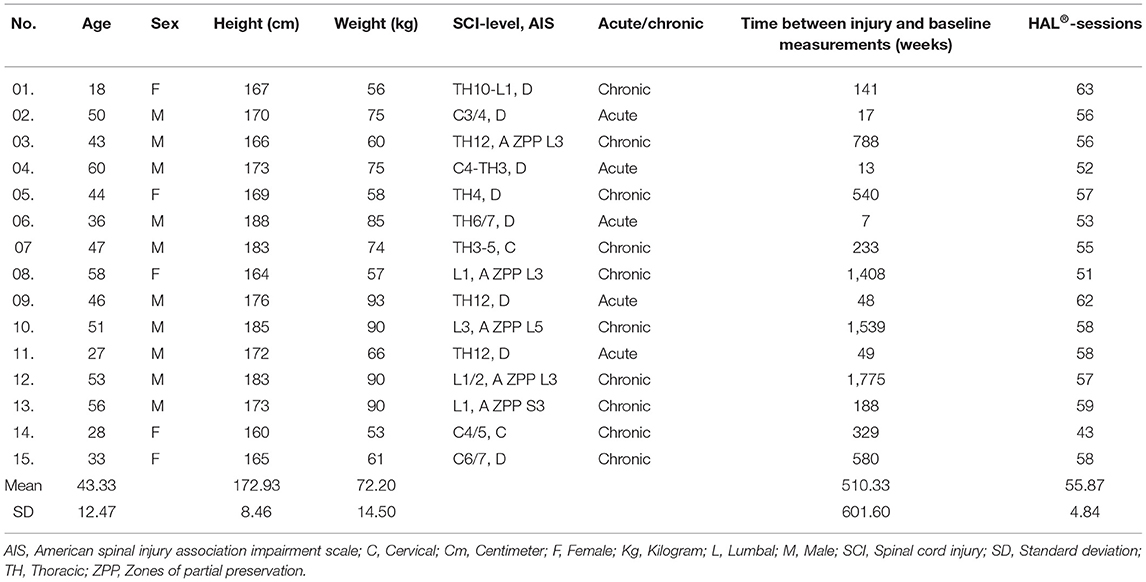
Table 1. Participants characteristics.
Exclusion criteria included cardiopulmonary comorbidities, lower extremity decubitus, infections, osteoporosis, past thrombosis/embolism, contractures or severe spasticity of the lower limb, epilepsy, the presence of electronic medical devices that cannot be removed (e.g., pacemakers), and a body weight over 100 kg. The study was approved by the University of Duisburg-Essen ethical board and strictly follows the Declaration of Helsinki. The subjects were instructed about the objectives and the course of the study and provided written consent.
All patients underwent a body-weight-supported treadmill (PPS 70 Plus, WOODWAY USA Inc.) training of 30 min for five times a week over 12 weeks using HAL® Robot Suit as described previously (Aach et al., 2014) in addition to regular physiotherapy. At the outset the harness system supported roughly 50% of each patient's body weight and was reduced as tolerated within the process of training. The speed could be aligned from 0 km/h up to 4.5 km/h. The velocity of the treadmill was settled individually among comfortable and maximum speed tolerated by the patients. Rest periods were taken as needed. Pulse and blood pressure were observed to prevent overexertion. Training was performed in the “Zentrum für Neurorobotales Bewegungstraining” in Bochum, Germany. All training sessions were observed by qualified and HAL®-trained physiotherapists. The mean number of training sessions was 55.78 ± 4.84.
HAL® Robot Suit is a wearable cyborg that is controlled using remaining muscle impulses of the lower extremities (Sankai, 2007). The system consists of a back module, a hip frame, an upper and lower leg frame on the right and left side as well as own sensor shoes. All components can be individually sized to suit the individual user. Servo motors at the hip and knee joints provide the necessary torque support. Bioelectric signals (BES) are detected via electrodes applied to the skin surface directly above the flexion and extension muscles of the hips and knees, and a connection between patients and the exoskeleton is established via cable. Using these BES HAL® generates torque support which allows a voluntary robotic-supported movement. Settings of torque support at each joint are adjusted by a HAL® therapist using multiple information provided from HAL® such as BES, joint angle and plantar pressure, visualized on a controller. Over the course of the training these settings are optimized and adapted as needed. During training with HAL® no assistive devices are used. Patient can use treadmill handrails to support balance.
To measure physiological parameters (spatiotemporal and kinematic), patients underwent a gait analysis walking on a walkway with a length of 12 m. Ten meters in the middle were recorded to exclude acceleration phase at the beginning and slow-down phase at the end. Due to the fact that a walking impairment was present, walking speed was not predetermined. Subjects were merely asked to walk in a comfortable speed. In order to avoid fatigue-induced deviations in walking pattern, measurements took place in the morning without previously performed training session. One trial was collected for each patient.
Gait analysis was performed on the first (T0) and last day (T1) of the respective training period during free walking without HAL® but with individually needed aids (for instance walking frame, crutches, walking stick). Gait was recorded three-dimensionally by an inertial sensor system with a sampling frequency of 100 Hertz (MyoMotion® Research Pro-7-sensor system, Noraxon U.S.A., Inc.). The validity and reliability of wearable inertial measurement units are particularly accepted for the analysis of spatiotemporal characteristics and gait parameters (Washabaugh et al., 2017; Kobsar et al., 2020). Seven sensors were placed at defined anatomical points (Sacrum, left and right thigh, left and right shank, left and right foot) of the lower extremities. To attach the wireless sensors straps were used, which could be adapted to individual body constitutions. Each two sensors define the intermediate joint and enable to monitor joint angles as well as temporal and spatial parameters during gait. Via Bluetooth, the recorded position data was transferred in real time to a measuring computer and allowed, after calibration in neutral zero position, an observation and recording of the joint movement during walking.
Primary physiological outcome parameters were stance phase (%), loading response phase (%), midstance phase (%), pre-swing phase (%), swing phase (%), double stance phase (%), step length (cm), length of double stride (cm), velocity (km/h), cadence (steps/min), step time (s), time for double stride (s), maximum and minimum angles (°) of hip-, knee-, and ankle joint in the sagittal plane at defined points of gait cycle and range of motion (ROM) of hip-, knee-, and ankle joint (°).
For the evaluation of functional improvements, established test methods such as 10MWT (s), TUG (s), 6MWT (m), and WISCI II Score have been implemented as secondary outcomes. Data for 10MWT and WISCI II Score represents mean of the first five training days (pre) and last five training days (post). TUG and 6MWT were performed on T0 and T1.
Results were evaluated after completion of the study using the statistical analysis program Statistica 13.3 (Palo Alto, USA). Wilcoxon signed-rank test has been used to identify significant changes between data at baseline and endpoint for whole group and for subgroups of acute and chronic patients. Mean values, standard deviations (SD), median and interquartile range (IQR) were calculated. To compare extent of change between both groups, Mann-Whitney U-test was performed. Statistical significance was set at p ≤ 0.05. As we aimed to answer several questions using the data obtained, we used the Bonferroni correction for multiple comparisons and the global α level, divided equally among the individual tests resulting in α1 ≤ 0.025 (Hochberg, 1988).
Comparisons were made for whole group (n = 15) and the group was divided into subgroups of acute (n = 5) and chronic patients (n = 10). 53.33% of the participants represent AIS D, 13.33% AIS C and 33.33% AIS A. No AIS B patient participated. Data from gait analysis was time-normalized to 100% gait cycle for 27.6 steps (pre) and 21.2 steps (post) on average. No adverse events occurred during the intervention. Basis for the statistical comparison of pre- to post-measurement of the kinematic parameters were the maximum and minimum joint angle values averaged over subjects of respective group. Since those maximum and minimum values occur differently in subjects over time of a gait cycle, there are differences to the visualization of the averaged angular curves.
Hip and knee joint angles were calculated in relation to the vertical line calibrated in an upright position as 0°. Positive deviations represent flexion and negative deviations represent extension. Ankle angles were computed divergent from the neutral position (leg axis vertical to the foot) and are given positive for dorsal extension and negative for the plantar flexion.
Norm angular curves are based on data from MyoMotion, Noraxon Inc., USA for normal walking at moderate speed. Data from gait analysis was defined as physiological parameters, giving information about quality of gait while functional parameters only consider information about needed time or achieved distance disregarding quality. Results are shown in Table 2.
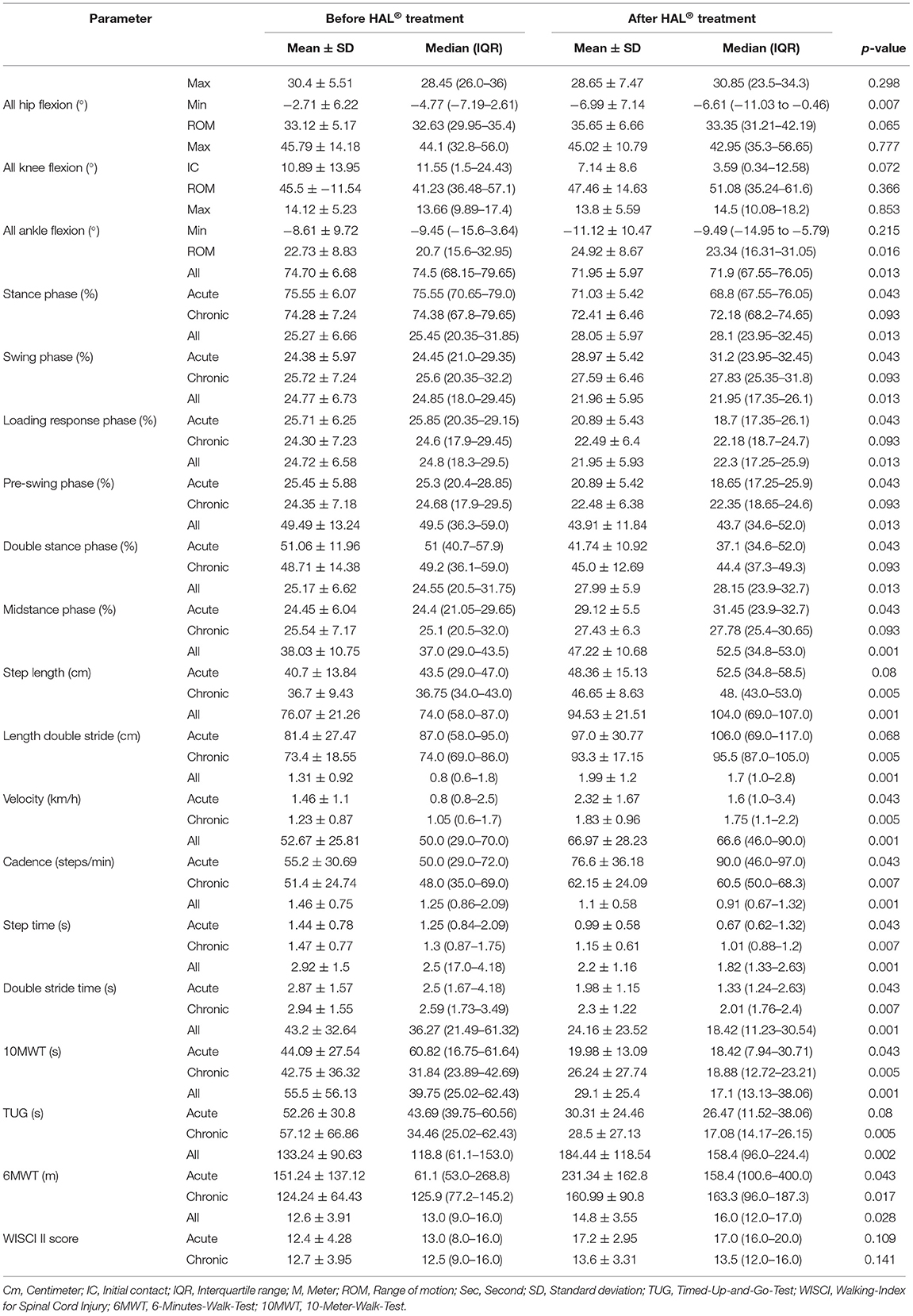
Table 2. Measurement descriptives and statistical outcome.
Stance phase were decreased over all patients from 74.70 ± 6.68% at baseline to 71.95 ± 5.97% (p ≤ 0.013) after intervention while swing phase was increased from 25.27 ± 6.66% to 28.05 ± 5.97% (p ≤ 0.013). Phase of loading response decreased from 24.77 ± 6.73% to 21.96 ± 5.95% (p ≤ 0.013) as well as pre-swing phase from 24.72 ± 6.58% to 21.95 ± 5.93% (p ≤ 0.013) and double stance phase from 49.49 ± 13.24% to 43.91 ± 11.84% (p ≤ 0.013). Mid stance phase was increased from 25.17 ± 6.62% at baseline to 27.99 ± 5.9% (p ≤ 0.013) at the end. Individual subgroup analysis showed no significant changes for acute or chronic patients. Gait phase parameters are shown in Figure 1.
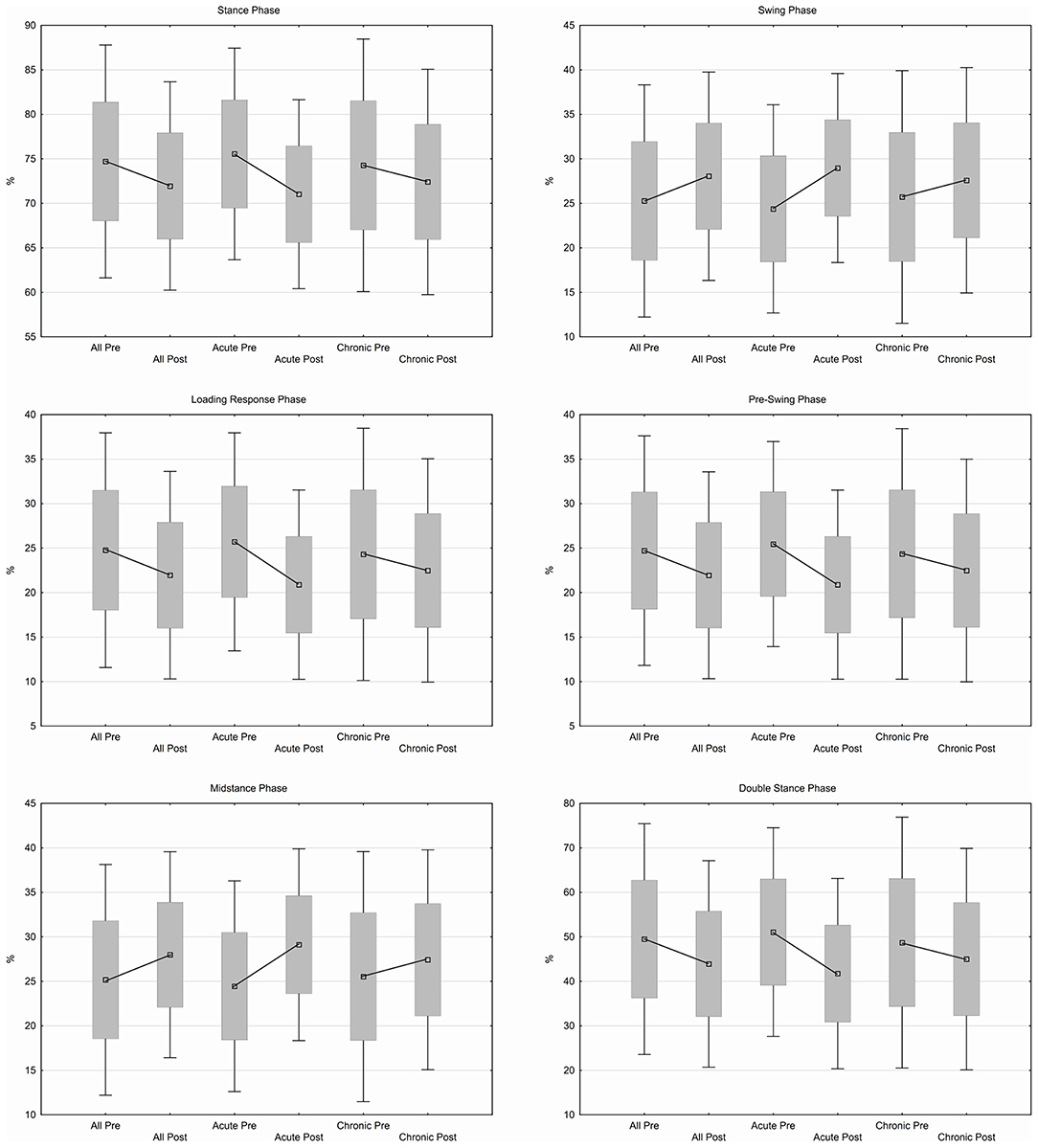
Figure 1. Gait phase parameters.
Step length increased from 38.03 ± 10.75 cm to 47.22 ± 10.68 cm (p ≤ 0.001) as well as length of double stride from 76.07 ± 21.26 cm to 94.53 ± 21.51 cm (p ≤ 0.001). Velocity and cadence were increased from 1.31 ± 0.92 km/h to 1.99 ± 1.2 km/h (p ≤ 0.001) respective 52.67 ± 25.81 steps/min to 66.97 ± 28.23 steps/min (p ≤ 0.001) while step time and time for double stride were decreased from 1.46 ± 0.75 s to 1.1 ± 0.58 s (p ≤ 0.001) and from 2.92 ± 1.5 s to 2.2 ± 1.16 s (p ≤ 0.001). Individually chronic patients significantly improved for all spatiotemporal parameters (step length, p ≤ 0.005; length of double stride, p ≤ 0.005; velocity, p ≤ 0.005; cadence, p ≤ 0.007; step time, p ≤ 0.007; time for double stride, p ≤ 0.007) while acute patients did not. Spatiotemporal parameters are shown in Figure 2.
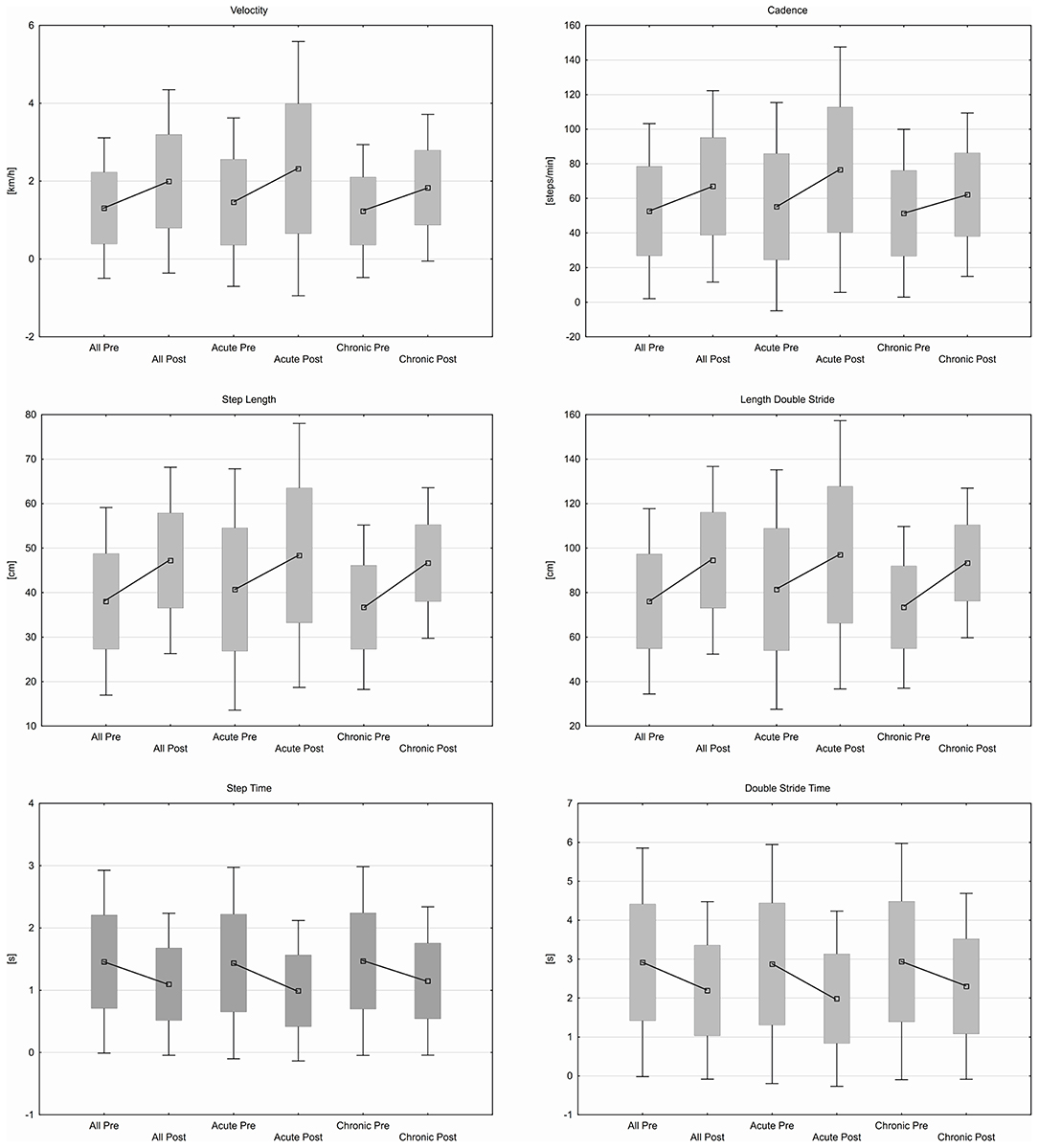
Figure 2. Spatiotemporal parameter.
Over all participants showed a greater amount of hip extension prior to swing phase (−2.71 ± 6.22° −6.99 ± 7.14°, p ≤ 0.007). The basic characteristic pattern of hip flexion/extension did not change. Hip ROM increased over all (33.12 ± 5.17°-35.65 ± 6.66°) but remained insignificant (p ≤ 0.065). No significant change was found when observing acute and chronic group individually.
Knee flexion at the phase of initial contact was reduced from 10.89 ± 13.95° to 7.14 ± 8.6° (p ≤ 0.072) over all patients. Maximum knee flexion in swing phase occurred earlier during gait cycle. Knee ROM increased from 45.5 ± 11.54° to 47.46 ± 14.63° (p ≤ 0.366). For chronic patients no noteworthy changes where found while acute patients showed a significantly greater extension (or less flexion) (18.23 ± 8.89°-8.59 ± 4.87°, p ≤ 0.014) at point of initial contact.
Local maximum plantar flexion in stance phase was increased over all patients from −6.56 ± 8.79° to −9.5 ± 8.81° (p ≤ 0.089). Maximum dorsal extension in stance phase occurred earlier during gait cycle. Ankle joint showed a larger amount in ROM after treatment (22.73 ± 8.83°-24.92 ± 8.67°, p ≤ 0.016). No changes were found regarding subgroups. Joint angles are shown in Figure 3.
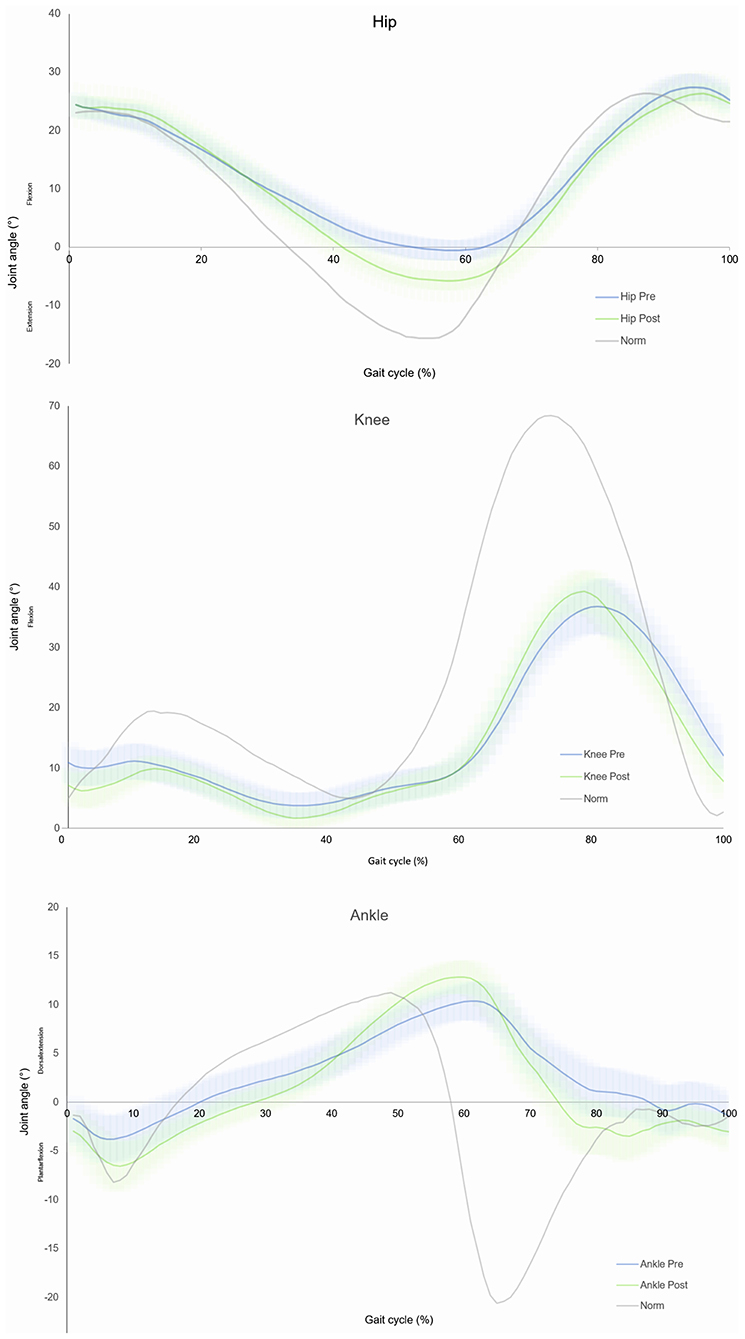
Figure 3. Sagittal plane joint angles over all individuals of hip, knee and ankle.
Patients improved over all participants in 10MWT from 43.2 ± 32.64 s at baseline to 24.16 ± 23.52 s (p ≤ 0.001) after 12 weeks training. Time needed for TUG decreased from 55.5 ± 56.13 s to 29.1 ± 25.4 s (p ≤ 0.001) and patients improved in 6MWT from 133.24 ± 90.63 m at the beginning to 184.44 ± 118.54 m (p ≤ 0.002) at the end of training period. WISCI II Score changed from 12.6 ± 3.91 to 14.8 ± 3.55 (p ≤ 0.028). Changes in group of acute patients remain insignificant while chronic patients showed significant results in 10MWT (p ≤ 0.005), 6MWT (p ≤ 0.017), and TUG (p ≤ 0.005). Functional parameters are shown in Figure 4.
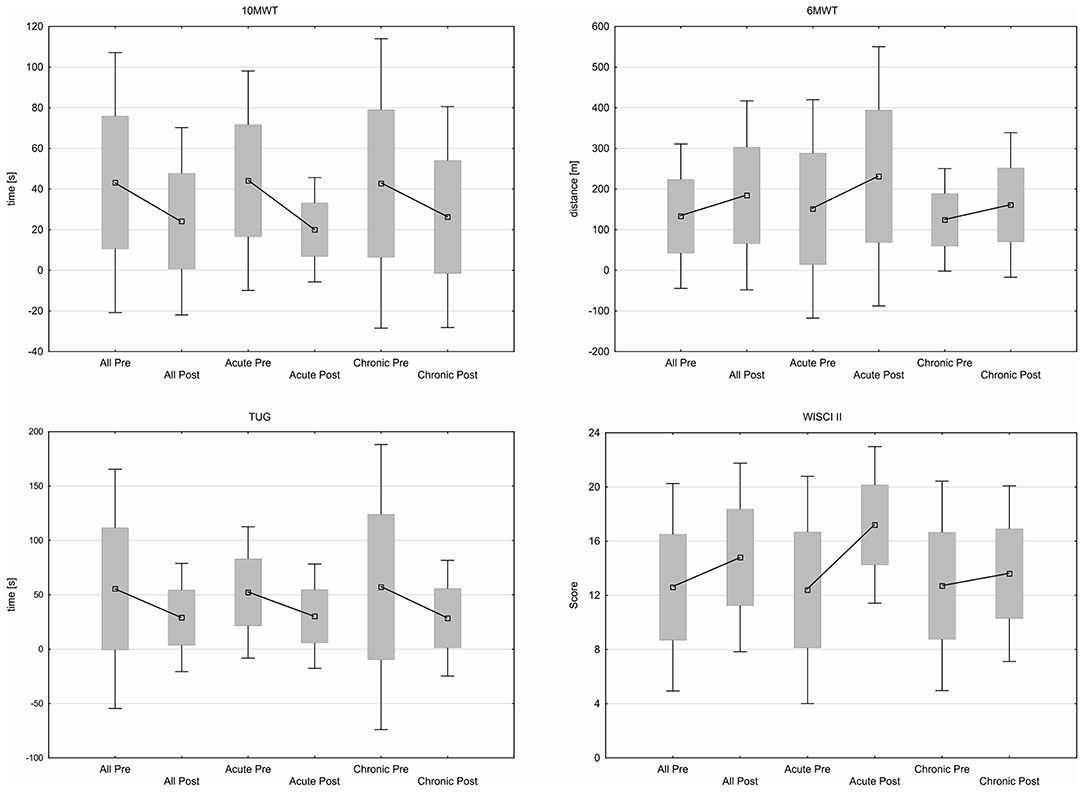
Figure 4. Functional outcome in 10MWT, 6MWT, TUG, WISCI II score.
Enhanced gait velocity is often equated with improved walking ability. In contrast, Van Hedel et al. (2006) postulates that an increased gait speed e.g., in 10MWT should not be an exclusive criterion to adjudicate on gait ability. In addition to the functional assessment of walking it is important to consider the physiology of walking for example to avoid excessive stress on the lower extremities. Bones and ligamentous structures can be injured caused by long-term stress as a consequence of an inadequate gait pattern or lead to serious diseases that have a negative impact on the patient. Inflammation and pain as a result can arise and thwart the patient in his further course of rehabilitation. Consequently studies should not only focus on functional outcomes but also on physiology when assessing the rehabilitation progress. Hence, several studies evaluated gait parameter changes after HAL® treatment and found improvements, for example in patients after Stroke (Tanaka et al., 2019), in groups of patients with cerebral palsy (Matsuda et al., 2018; Mataki et al., 2020) and in case reports of patients with SCI (Kanazawa et al., 2019; Watanabe et al., 2019). Investigations in larger groups of people living with SCI are missing.
Therefore, the objective of this study was to verify for the first time whether an improvement in physiological gait can be demonstrated in addition to the functional parameters in a group of patients with SCI after completing an exoskeleton treatment.
As expected, due to prior studies (Aach et al., 2014; Cruciger et al., 2014a,b; Grasmücke et al., 2017; Jansen et al., 2017, 2018; Sczesny-Kaiser et al., 2019) all functional parameters improved during the 12-week training period showing reduced time needed for the 10MWT and TUG as well as an increased walk capacity in the 6MWT and WISCI II Score. Representing newly observed physiological parameters, differences were also found in some phases of gait cycle showing improved knee extension during initial contact and increased maximum hip extension prior to swing phase. All joint angles showed a larger ROM. Those findings were accompanied by significant improvement in all spatiotemporal and gait phase parameters. The obtained results show for the first time that patients present changes after training with HAL® Robot Suit in both functional and physiological gait parameters.
Overall, the data for joint angles shown at the beginning of the training phase reflects those deficits described by Perry and Burnfield (2010) and Van der Salm et al. (2015) as typical in SCI patients. At the initial contact, patients had a nearly normal hip flexion that was kept up over phase of loading response. In the further course an insufficient hip extension was shown before changeover from stand to swing phase, possibly due to reduced muscle strength of the hip extensors because of diminished innervation. Too low hip extension in the stance phase has a direct impact on stability of gait because center of gravity falls too far forward and as a reaction people tend to decrease contralateral stride length to prevent falling (Perry, 2003; Van der Salm et al., 2015). Furthermore, required forces for adequate propulsion are difficult to apply when hip extension is limited. Abel et al. (2002) described that kind of gait abnormality as inefficient but do not value as dangerous mechanism. Following HAL® treatment, patients showed significant growth of average 4.28° more hip extension potentially providing better gait stability and possibly reflecting improved control of hip extensor muscles. These findings are in accordance with those described by Watanabe et al. (2019).
Knee joint angles showed an immoderate flexion at initial contact, too low flexion during phase of loading response and a small value of flexion during swing phase. Lack of knee extension at initial contact results presumably from reduced extension velocity at the end of previous swing phase which otherwise leads to passive extension of knee joint. After treatment a slightly reduced flexion at initial contact could be observed. During phase of loading response, the knee normally flexes cushioning impact forces. However, this flexion is found very little in measured subjects presenting a protective posture. Due to lack of force in rectus femoris muscle, subjects cannot stabilize this slightly bent position and tend to buckle conditioned by gravity. Moreover, there is a strong connection between the low flexion and slow pace of patients (Perry, 2003). Also, after intervention flexion values in loading response remain low but characteristic waveform can now be observed due to already mentioned improved knee extension at initial contact. In swing phase where maximum knee flexion within one gait cycle is reached, angle values were nearly unchanged. However, the maximum flexion occurred earlier suggesting that subjects were able to respond faster to muscular requirements of a movement.
Having a look at ankle angles, patients showed an accordant plantar flexion at initial contact before and after treatment. Subsequently, in phase of loading response, patients had insufficient plantar flexion prior to treatment which could be improved during exercise resulting in a more appropriate foot drop. Reason for reduced plantar flexion in the beginning could be weakness of soleus muscle, which was then strengthened along treatment. In the following, patients showed a slight dorsal extension movement potentially due to lack of muscle forces as well. Prior to swing phase maximum dorsal extension is reached both before and after treatment. In pre-swing normally a quick plantar flexion can be observed up to its maximum. Before treatment, this movement was executed to a lesser extent and over a longer period of time. After intervention, patients were able to perform faster and to a larger degree but a deficiency still remains. In regard to muscles it reflects what was already seen in phase of loading response, soleus muscle seems to work intensified. In the end of gait cycle both before and after treatment patients showed only a slight dorsal extension in preparation of the following initial contact. Summarizing ankle angle data indicates that those phases of gait cycle where plantar flexor muscles are active could improve whereas phases in which dorsal extensor muscles are active could do less.
It should be taken into account that muscle groups that have a slight innervation and marginal muscle strength levels from the beginning naturally have a lower potential for improvement than those muscle groups that are better innervated and already have moderate strength.
Beside joint angles, which have shown a certain adaption, spatiotemporal and gait phase parameters were evaluated providing information on harmonization of gait. Percentage distribution of stance phase and swing phase respective all sub phases within gait cycle were improved significantly. Subjects were able to perform steps faster while at the same time gaining more space, which is an indication of an enhanced coordination of lower extremities. Improved step length is also advantaged by already discussed improved hip extension prior to swing phase. In contrast to the effects shown here, Shin et al. (2011) with reference to Pepin and Barbeau (1992) postulates that SCI patients after conventional training tend to increase velocity only by prolonged step length but not by step frequency. Sczesny-Kaiser et al. (2015) reported about cortical reorganization after HAL® treatment, which could be an explanation for optimized coordination of movement. They found a changed representation of partially paralyzed lower extremities in somatosensory cortex which could be caused by recruitment and more effective use of existing afferent nerve pathways.
Last but not least data showed significant improvement in cadence and velocity, which represents, beside importance of other discussed factors, a central goal of rehabilitation for affected patients giving them the opportunity to participate more in everyday life. Subgroup analysis of acute and chronic patients showed that both could benefit from this treatment even though individual results often remain insignificant.
Our data supports findings of previous studies reporting of improvements in terms of spatiotemporal gait parameters and joint angles during the gait cycle after HAL® treatment (Kanazawa et al., 2019; Watanabe et al., 2019). However, presented data only shows statistical significance and not necessarily clinical significance as no comparison was made with minimal clinically important difference values for this population.
The present study has several further limitations. One is the small number of patients as well as the highly individual gait behavior of patients with SCI and the fact that only one trial for each patient was collected because patients were not able to perform several trials one after another. Further studies with a larger group of patients are necessary to confirm the presented results. Moreover, in acute injured subjects it is difficult to value spontaneous remission as one part of the healing process. For better subgroup analysis, number of patients within each group has to be larger. In the present study we were able to show changes in gait in the course of treatment. However, the muscular background is subject to assumptions. In further studies, measurement of electromyography before and after treatment could be reasonable to get more detailed information. Capture of ground reaction forces during walking would also allow more specific interpretation, giving valuable data about appearing forces in each phase of a gait cycle.
In conclusion, the presented study shows signs that an improvement in physiological gait can be achieved in addition to functional improvements in patients with SCI completing a 12-week training with HAL® Robot Suit.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
The studies involving human participants were reviewed and approved by University of Duisburg-Essen Ethical Board. The patients/participants provided their written informed consent to participate in this study.
AB: conceptualization, methodology, investigation, writing—original draft, visualization, and project administration. MA: conceptualization, methodology, and writing—reviewing and editing. DG, TR, and EY: methodology, investigation, and writing—reviewing and editing. BJ: formal analysis, data curation, writing—reviewing and editing, and visualization. MD: conceptualization, writing—reviewing and editing, and supervision. TS: conceptualization, methodology, writing—reviewing and editing, and supervision. All authors read and approved the final manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We acknowledge support by the Open Acces Publication Funds of the Ruhr-Universität Bochum.
AIS, American Spinal Injury Association Impairment Scale; BES, Bioelectrical signals; HAL, Hybrid Assistive Limb; IC, Initial contact; ROM, Range of motion; SCI, Spinal cord injury; SD, Standard deviation; TUG, Timed-Up-and-Go-Test; WISCI, Walking-Index for Spinal Cord Injury; ZPP, Zones of partial preservation; 6MWT, 6-Minutes-Walk-Test 10MWT, 10-Meter-Walk-Test.
Aach, M., Cruciger, O., Sczesny-Kaiser, M., Höffken, O., Meindl, R. C., Tegenthoff, M., et al. (2014). Voluntary driven exoskeleton as a new tool for rehabilitation in chronic spinal cord injury - a pilot study. Spine J. 14, 2847–2853. doi: 10.1016/j.spinee.2014.03.042
Aach, M., Meindl, R. C., Geßmann, J., Schildhauer, T. A., Citak, M., and Cruciger, O. (2015). Exoskeletons for rehabilitation of patients with spinal cord injuries. Options and limitations. Unfallchirurg 118, 130–137. doi: 10.1007/s00113-014-2616-1
Abel, R., Schablowski, M., Rupp, R., and Gerner, H. (2002). Gait analysis on the treadmill - monitoring exercise in the treatment of paraplegia. Spinal Cord. 40, 17–22. doi: 10.1038/sj.sc.3101239. [Epub ahead of print].
Brinkemper, A., Grasmücke, D., Yilmaz, E., Reinecke, F., Schildhauer, T. A., and Aach, M. (2021). Influence of locomotion therapy with the wearable cyborg HAL on bladder and bowel function in acute and chronic SCI patients. Global Spine J. doi: 10.1177/21925682211003851. [Epub ahead of print].
Cruciger, O., Schildhauer, T. A., Meindl, R. C., Tegenthoff, M., Schwenkreis, P., Citak, M., et al. (2014b). Impact of locomotion training with a neurologic controlled hybrid assistive limb (HAL) exoskeleton on neuropathic pain and health related quality of life (HRQoL) in chronic SCI: a case study. Disabil. Rehabil. Assist. Technol. 11, 529–534. doi: 10.3109/17483107.2014.981875
Cruciger, O., Tegenthoff, M., Schwenkreis, P., Schildhauer, T. A., and Aach, M. (2014a). Locomotion training using voluntary driven exoskeleton (HAL) in acute incomplete SCI. Neurology 83:474. doi: 10.1212/WNL.0000000000000645
Grasmücke, D., Zieriacks, A., Jansen, O., Fisahn, C., Sczesny-Kaiser, M., Wessling, M., et al. (2017). Against the odds: what to expect in rehabilitation of chronic spinal cord injury with a neurologically controlled Hybrid Assistive Limb exoskeleton. A subgroup analysis of 55 patients according to age and lesion level. Neurosurg. Focus 42:E15. doi: 10.3171/2017.2.FOCUS171
Hochberg, Y. (1988). A sharper Bonferroni procedure for multiple tests of significance. Biometrika. 75, 800–802. doi: 10.1093/biomet/75.4.800
Jansen, O., Grasmücke, D., Meindl, R. C., Tegenthoff, M., Schwenkreis, P., Sczesny-Kaiser, M., et al. (2018). Hybrid assistive limb exoskeleton HAL in the rehabilitation of chronic spinal cord injury: proof of concept; the results in 21 patients. World Neurosurg. 110, e73–e78. doi: 10.1016/j.wneu.2017.10.080
Jansen, O., Schildhauer, T. A., Meindl, R. C., Tegenthoff, M., Schwenkreis, P., Sczesny-Kaiser, M., et al. (2017). Functional outcome of neurologic-controlled hal-exoskeletal neurorehabilitation in chronic spinal cord injury: a pilot with one year treatment and variable treatment frequency. Global Spine J. 7, 735–743. doi: 10.1177/2192568217713754
Kanazawa, A., Yoshikawa, K., Koseki, K., Takeuchi, R., and Mutsuzaki, H. (2019). A consecutive 25-week program of gait training, using the alternating hybrid assistive limb (HAL®) robot and conventional training, and its effects on the walking ability of a patient with chronic thoracic spinal cord injury: a single case reversal design. Medicina 55:746. doi: 10.3390/medicina55110746
Kawamoto, H., Kamibayashi, K., Nakata, Y., Yamawaki, K., Ari-yasu, R., Sankai, Y., et al. (2013). Pilot study of locomotion improvement using hybrid assistive limb in chronic stroke patients. BMC Neurol. 13:141. doi: 10.1186/1471-2377-13-141
Kobsar, D., Charlton, J. M., Tse, C. T. F., Esculier, J. F., Graffos, A., Krowchuk, N. M., et al. (2020). Validity and reliability of wearable inertial sensors in healthy adult walking: a systematic review and meta-analysis. J. Neuroeng. Rehabil. 17:62. doi: 10.1186/s12984-020-00685-3
Kubota, S., Nakata, Y., Eguchi, K., Kawamoto, H., Kamibayashi, K., Sakane, M., et al. (2013). feasibility of rehabilitation training with a newly developed wearable robot for patients with limited mobility. Arch. Phys. Med. Rehabil. 94, 1080–1087. doi: 10.1016/j.apmr.2012.12.020
Mataki, Y., Mutsuzaki, H., Kamada, H., Takeuchi, R., Nakagawa, S., Yoshikawa, K., et al. (2020). Effect of the hybrid assistive limb on the gait pattern for cerebral palsy. Medicina 56:673. doi: 10.3390/medicina56120673
Matsuda, M., Mataki, Y., Mutsuzaki, H., Yoshikawa, K., Takahashi, K., Enomoto, K., et al. (2018). Immediate effects of a single session of robot-assisted gait training using Hybrid Assistive Limb (HAL) for cerebral palsy. J. Phys. Ther. Sci. 30, 207–212. doi: 10.1589/jpts.30.207
Nilsson, A., Skough Vreede, K., Häglund, V., Kawamoto, H., Sankai, Y., and Borg, J. (2014). Gait training early after stroke with a new exoskeleton - the hybrid assistive limb: a study of safety and feasibility. J. Neuroeng. Rehabil. 11:92. doi: 10.1186/1743-0003-11-92
Pepin, A., and Barbeau, H. (1992). Effects of treadmill speed and incline on the walking pattern of normal and spastic paretic subjects. Soc. Neurosci. Abstr. 18:860.
Perry, J., and Burnfield, J. (2010). Gait Analysis. Normal and Pathological Function, 2nd Edn. West Deptford, NJ: Slack Incorporated.
Sankai, Y. (2007). HAL: hybrid assistive limb based on cybernics. Robot. Res. 66, 25–34. doi: 10.1007/978-3-642-14743-2_3
Sczesny-Kaiser, M., Höffken, O., Aach, M., Cruciger, O., Grasmücke, D., Meindl, R., et al. (2015). HAL® exoskeleton training improves walking parameters and normalizes cortical excitability in primary somatosensory cortex in spinal cord injury patients. J. Neuroeng. Rehabil. 12:68. doi: 10.1186/s12984-015-0058-9
Sczesny-Kaiser, M., Kowalewski, R., Schildhauer, T. A., Aach, M., Jansen, O., Grasmücke, D., et al. (2017). Treadmill training with HAL exoskeleton-a novel approach for symptomatic therapy in patients with limb-girdle muscular dystrophy-preliminary study. Front. Neurosci. 11:449. doi: 10.3389/fnins.2017.00449
Sczesny-Kaiser, M., Trost, R., Aach, M., Schildhauer, T. A., Schwenkreis, P., and Tegenthoff, M. (2019). A randomized and controlled crossover study investigating the improvement of walking and posture functions in chronic stroke patients using HAL exoskeleton - the HALESTRO study (HAL-Exoskeleton STROke Study). Front. Neurosci. 13:259. doi: 10.3389/fnins.2019.00259
Shin, J., Yoo, J., Jung, T. H., and Goo, H. R. (2011). Comparison of lower extremity motor score parameters for patients with incomplete spinal cord injury using gait parameters. Spinal Cord. 49, 529–533. doi: 10.1038/sc.2010.158
Tanaka, H., Nankaku, M., Nishikawa, T., Hosoe, T., Yonezawa, H., Mori, H., et al. (2019). Spatiotemporal gait characteristic changes with gait training using the hybrid assistive limb for chronic stroke patients. Gait Posture 71, 205–210. doi: 10.1016/j.gaitpost.2019.05.003
Ueba, T., Hamada, O., Ogata, T., Inoue, T., Shiota, E., and Sankai, Y. (2013). Feasibility and safety of acute phase rehabilitation after stroke using the hybrid assistive limb robot suit. Neurol. Med. Chir. 53, 287–290. doi: 10.2176/nmc.53.287
Van der Salm, A., Nene, A. V., Maxwell, D. J., Veltink, P. H., Hermens, H. J., and IJzerman, M. J. (2015). Gait impairments in a group of patients with incomplete spinal cord injury and their relevance regarding therapeutic approaches using functional electrical stimulation. Artificial Organs. 29, 8–14. doi: 10.1111/j.1525-1594.2004.29004.x
Van Hedel, H. J., Wirz, M., and Curt, A. (2006). Improving walking assessment in subjects with an incomplete spinal cord injury: responsiveness. Spinal Cord 44, 352–356. doi: 10.1038/sj.sc.3101853
Washabaugh, E. P., Kalyanaraman, T., Adamczyk, P. G., Claflin, E. S., and Krishnan, C. (2017). Validity and repeatability of inertial measurement units for measuring gait parameters. Gait Posture 55, 87–93. doi: 10.1016/j.gaitpost.2017.04.013
Keywords: spinal cord injury, gait analysis, exoskeleton, hybrid assistive limb, rehabilitation
Citation: Brinkemper A, Aach M, Grasmücke D, Jettkant B, Rosteius T, Dudda M, Yilmaz E and Schildhauer TA (2021) Improved Physiological Gait in Acute and Chronic SCI Patients After Training With Wearable Cyborg Hybrid Assistive Limb. Front. Neurorobot. 15:723206. doi: 10.3389/fnbot.2021.723206
Received: 10 June 2021; Accepted: 27 July 2021;
Published: 26 August 2021.
Edited by:
Hao Su, City College of New York (CUNY), United StatesReviewed by:
Yu Cao, Huazhong University of Science and Technology, ChinaCopyright © 2021 Brinkemper, Aach, Grasmücke, Jettkant, Rosteius, Dudda, Yilmaz and Schildhauer. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Alexis Brinkemper, YWxleGlzLmJyaW5rZW1wZXJAYmVyZ21hbm5zaGVpbC5kZQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.