
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Behav. Neurosci., 18 August 2022
Sec. Pathological Conditions
Volume 16 - 2022 | https://doi.org/10.3389/fnbeh.2022.995614
This article is part of the Research TopicUsing Novel Technologies and Models to Identify Biomarkers and Explore Therapeutic Strategies for Neurological DisordersView all 11 articles
 Yi Li1†
Yi Li1† Kerong Chen1†Jiapu Wang1†Hanmei Lu1Xiaoyu Li1Lei Yang1Wenlu Zhang1Shujuan Ning1Juan Wang1Yi Sun1Yu Song1Mei Zhang1*Jianhong Hou2*Hongling Shi1*
Kerong Chen1†Jiapu Wang1†Hanmei Lu1Xiaoyu Li1Lei Yang1Wenlu Zhang1Shujuan Ning1Juan Wang1Yi Sun1Yu Song1Mei Zhang1*Jianhong Hou2*Hongling Shi1*Dysphagia is one of the most common manifestations of stroke, which can affect as many as 50–81% of acute stroke patients. Despite the development of diverse treatment approaches, the precise mechanisms underlying therapeutic efficacy remain controversial. Earlier studies have revealed that the onset of dysphagia is associated with neurological damage. Neuroplasticity-based transcranial magnetic stimulation (TMS), a recently introduced technique, is widely used in the treatment of post-stroke dysphagia (PSD) by increasing changes in neurological pathways through synaptogenesis, reorganization, network strengthening, and inhibition. The main objective of this review is to discuss the effectiveness, mechanisms, potential limitations, and prospects of TMS for clinical application in PSD rehabilitation, with a view to provide a reference for future research and clinical practice.
Dysphagia, defined as “difficulty swallowing,” is one of the most important clinical manifestations of stroke and a common consequence of neurological damage caused by a range of diseases (Fung et al., 2004). Studies have confirmed that 50–81% of acute stroke patients may experience swallowing problems (Hamdy, 2010). In most cases, the post-stroke dysphagia (PSD) will improve spontaneously. However, approximately 11–50% of patients may have long-term disability (Kumar et al., 2010; Cohen et al., 2016).
Although dysphagia gradually resolves spontaneously in the early stages of disease in most cases, severe and persistent forms of dysphagia remain prevalent in about 13% of stroke patients (Mann et al., 1999). The presence of dysphagia is linked to increased physical and psychological stress in patients, families, and caregivers, along with reduced quality of life (Eslick and Talley, 2008). In addition, dysphagia may cause various life-threatening complications, such as aspiration pneumonia, asphyxia, dehydration, and malnutrition (Smithard et al., 1996). In particular, aspiration pneumonia can trigger various complications, the most acute being infection and sepsis (Kalita et al., 2015). These complications increase the risk of prolonged hospital stays, high medical expenses and significant mortality, causing a major negative impact at both the individual and society level. Therefore, rehabilitation therapy of PSD remains a significant clinical issue that needs to be urgently addressed.
Studies have demonstrated that central causes of dysphagia in stroke patients include cortical or brain-stem damages, and peripheral causes include damages to the nerves or muscles involved in swallowing. The brain-stem lesions are more commonly associated with dysphagia (Balcerak et al., 2022). Notably, dysphagia is usually caused by infratentorial lesions, while sensory afferent disturbances usually cause dysphagia in supratentorial stroke. However, the exact mechanism of PSD is not well understood.
The treatment options of PSD include behavioral therapy, oral care, pharmacology, neurostimulation, and dietary interventions. Various physical therapies and preventive measures can avoid dysphagia-related complications. However, there is a lack of medical or electrophysiological interventions to facilitate recovery from dysphagia after acute or subacute stroke.
Existing treatments for PSD include postural training (Hägg and Larsson, 2004), dietary modification (Hägg and Anniko, 2008; McCullough et al., 2012), swallowing movements (Hägg and Anniko, 2008), compensation techniques (Lin et al., 2003), drug therapy, oral motor stimulation (Kang et al., 2012), music therapy (Kim, 2010), facial sensory stimulation, pharyngeal electrical stimulation, neuromuscular electrical stimulation, non-invasive brain stimulation, botulinum toxin injection, and acupuncture therapy (Terré et al., 2013; Yang et al., 2015). Nevertheless, these treatment strategies cannot change the physiology of impaired swallowing biomechanics as well as cannot promote the recovery of impaired swallowing neural networks in stroke patients (Speyer et al., 2010).
According to a previous study, the pathogenic cascade of dysphagia is as follows: after peripheral or central (corticobulbar tract) impairment of the cranial nerves innervating the swallowing muscles, tongue movement is limited, with soft palate paralysis. Consequently, intraoral and pharyngeal pressure cannot be fully increased, movement of food from the oral cavity to the pharynx and esophagus is weak, and transit time is significantly prolonged. The retention increases hyperreflexia or spasm of sphincter and cricopharyngeal muscle in the esophageal inlet of patients with supraglomerular damage (pseudobulbar palsy) and movement of the swallowing muscles is uncoordinated, resulting in accidental ingestion of food into the trachea (Ertekin et al., 2000). In recent years, accumulating evidence has shown that transcranial magnetic stimulation (TMS) can induce changes in the excitability of the cerebral cortex, promote plastic alterations in nerves, control the release of neurotransmitters (Lanza et al., 2015), and manage dysphagia through regulating neuroplasticity. The main objective of this review is to synthesize clinical studies and investigate the effectiveness, mechanisms of action, advantages, and disadvantages of TMS in clinical practice.
Transcranial magnetic stimulation is a non-invasive stimulation technique based on the principles of neuroplasticity that induces changes in neurological pathways by altering neurons in target cortical areas through synaptogenesis, reorganization, network strengthening, and inhibition, causing local depolarization of the magnetic field below the skull and activation or inhibition of activity in cortical areas (Hallett, 2000; Koerselman et al., 2004). It was also reported that the feasibility of using external magnetism to stimulate the nerves and brain (Barker et al., 1985). The group described TMS as a non-invasive technique to stimulate the human motor cortex. At present, TMS is widely used as a routine diagnostic tool in neurophysiological studies owing to its safe and technical characteristics (Rossi et al., 2009). This approach is based on speech, language, and swallowing disorders of the nervous system (Naeser et al., 2005; Khedr et al., 2009; Verin and Leroi, 2009; Barwood et al., 2011a,b,c). TMS exerts therapeutic effects by directly modulating specific pathways in the brain, which may ultimately affect longer-term communication and swallowing outcomes. Recent advances in TMS technology facilitate its application in clinical neurorehabilitation programs for patients with brain injury. Earlier reports have also demonstrated positive therapeutic effects on swallowing function after TMS, highlighting its potential as a treatment modality for dysphagia (Ridding and Rothwell, 2007). Multiple systematic reviews and meta-analyses have confirmed the beneficial effects of TMS on PSD (Yang et al., 2015; Pisegna et al., 2016; Liao et al., 2017; Chiang et al., 2019; Marchina et al., 2021) and swallow-related outcomes in patients. Moreover, the most intense effects of peripheral and cortical neurostimulation, including those of TMS, occur during the first 2 weeks after stroke (Yang et al., 2015). The efficacy of TMS for PSD from clinical trials and meta-analyses were illustrated in Table 1.
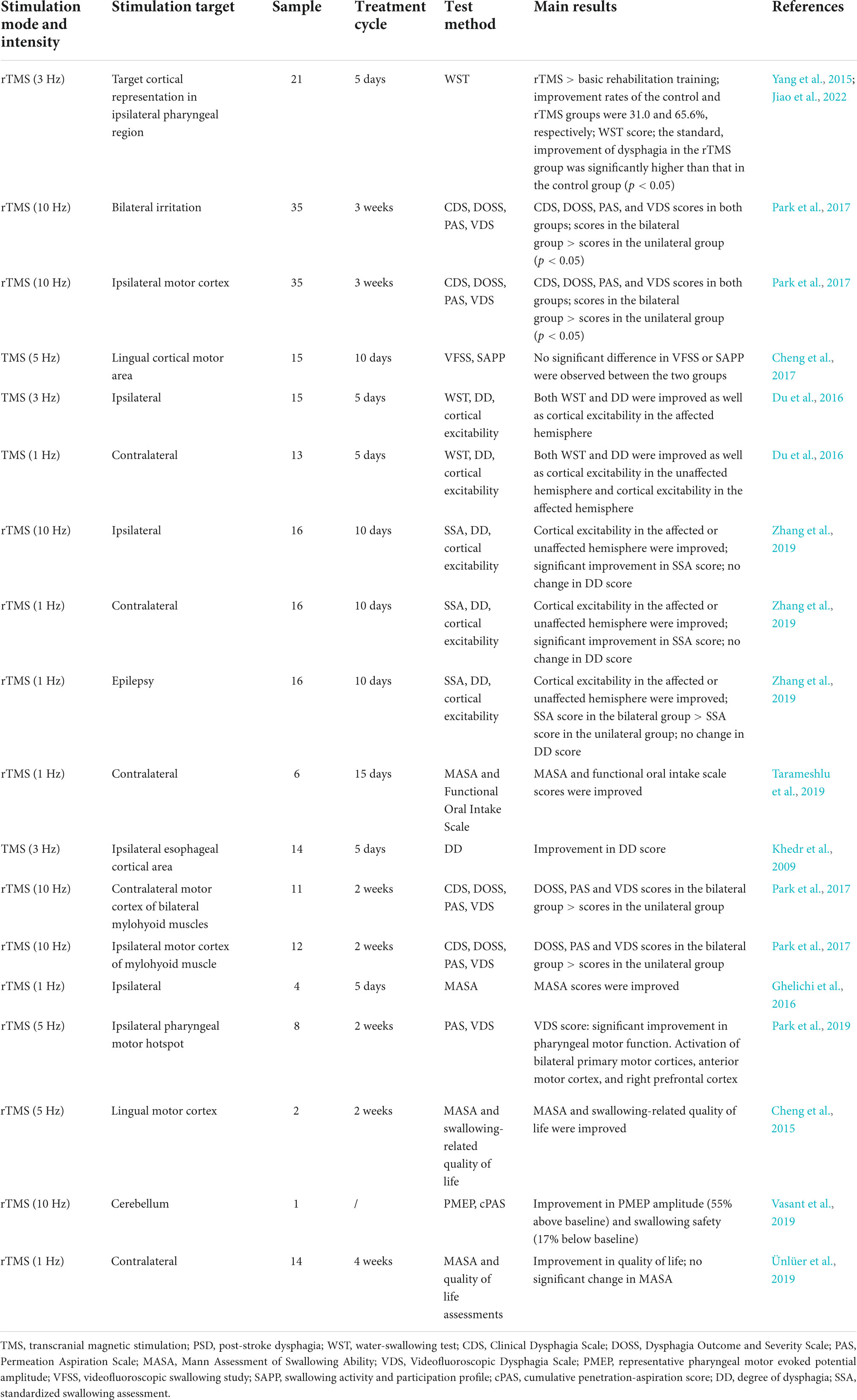
Table 1. Summary of studies on the efficacy of TMS for PSD from clinical trials and meta-analyses.
Transcranial magnetic stimulation, a tool for high-pressure brain stimulation, presents an alternative method for treatment of dysphagia via modulation of neuroplasticity. The procedure is based on the principle of inductance and non-invasively transmits electrical energy to the brain through the scalp and skull (Wassermann, 1998). A large current pulse generator is employed to release high currents thousands of amperes greater than that flowing through the coil, up to several kilowatts in power. These short magnetic pulses cause a sustained increase or decrease in cortical excitability. A brief but intense current is passed through a TMS coil placed on the scalp, creating a magnetic field that penetrates the skull to a depth of about 1.5–2 cm and induces a sufficiently strong electric field to depolarize surface axons and activate cortical neural networks (Lefaucheur et al., 2014). In addition, an electromyographic response to the target musculature is produced, known as motor-evoked potential (MEP) (Fitzgerald et al., 2006). Subsequently, descending motor shooting along the corticospinal tracts from the cortex to peripheral muscles is elicited to adjust the excitability of the cerebral cortex. TMS can be divided into high frequency (≥1 Hz) TMS and low frequency (≤1 Hz) stimulation processes (Wassermann, 1998). High frequency tends to enhance the excitability of the cerebral cortex while low frequency exerts the opposite effect (Hamdy et al., 1998; Fitzgerald et al., 2006). In stroke patients recovering from dysphagia, functional recovery was found to be associated with increased cortical representation of the intact hemisphere, highlighting the importance of reorganization of intact neural networks in PSD recovery (Pascual-Leone et al., 1998). Repetitively applied TMS, also known repetitive TMS (rTMS), can induce changes in synaptic plasticity similar to long-term potentiation (LTP) or long-term depression (LTD), that is, increased or decreased synaptic strength (Stefan et al., 2002; Hoogendam et al., 2010). The precise mechanism remains unknown but is thought to be mediated by the activity of N-methyl-D-aspartate (NMDA) receptors, as revealed by studies using NMDA antagonists (Fitzgerald et al., 2006; Huang et al., 2007). Other known rTMS modalities include intermittent (excitatory) theta burst stimulation (iTBS) and continuous (inhibitory) TBS (cTBS) (Ridding and Rothwell, 2007). However, recent reports suggest that the ability to respond to these protocols varies on an individual basis (Ridding and Rothwell, 2007).
Studies have confirmed that the damages to subcortical white matter (the internal capsule and within the brainstem) caused dysphagia, possibly due to disruption in the sensorimotor pathways of the corticobulbar tract. TMS may exert effects on PSD by regulating sensorimotor pathways in the brain. However, the details of how TMS change the communication and connection of cortical neural networks to achieve the therapeutic effect remain largely unexplored. The advantages and disadvantages of TMS were shown in Table 2.
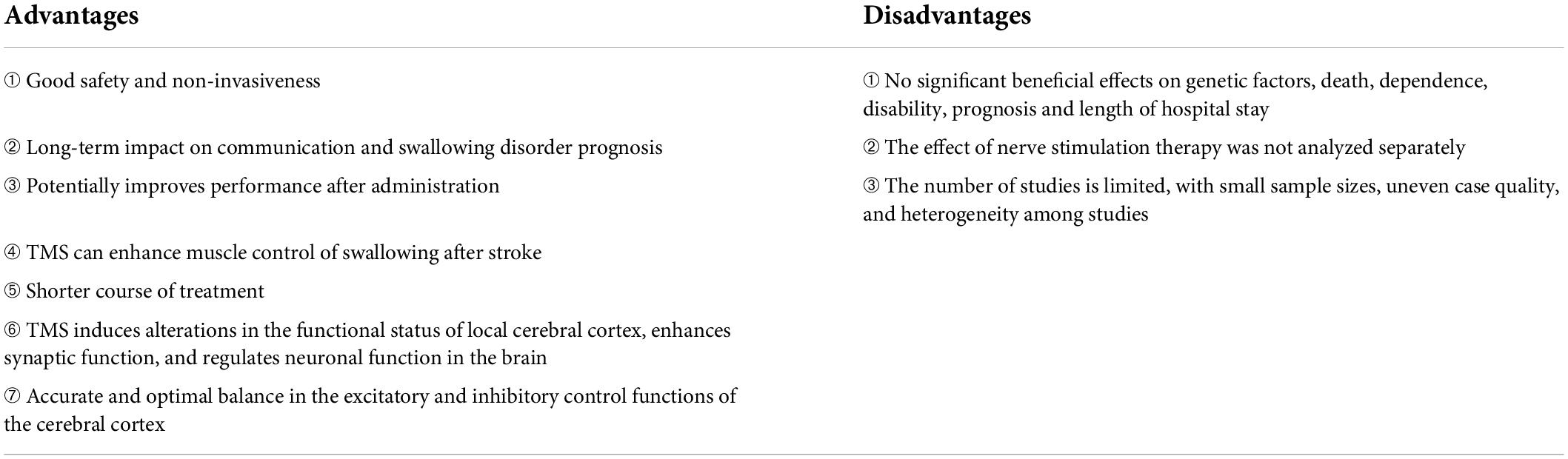
Table 2. Advantages and disadvantages of transcranial magnetic stimulation (TMS).
Transcranial magnetic stimulation is widely regarded as a safe and non-invasive form of nerve stimulation that can be used to directly manipulate cerebral cortex activity. In recent years, this innovative neuromodulation technology has been widely applied in neuroscience and countless cognitive fields (Barwood et al., 2011b) and shown to exert therapeutic effects by directly regulating specific pathways in the brain, which could ultimately affect longer-term communication and swallowing disorder prognosis (Naeser et al., 2005; Cotelli et al., 2008; Khedr et al., 2009; Verin and Leroi, 2009; Barwood et al., 2011a,c; Geeganage et al., 2012; Murdoch et al., 2012). The potential nerve priming effect induced by TMS is reported to effectively improve performance. Recent progress in TMS technology facilitates its application in clinical neurorehabilitation programs for patients with brain injury and the existing evidence shows that high-frequency TMS can enhance the muscle control of swallowing after stroke. For instance, in a study by Verin and Leroi (Geeganage et al., 2012) using TMS to stimulate the musculohyoid cortical area, the swallowing function of the patient improved at 3 days after stimulation. In a review by Cochrane (Zhai et al., 2020) on management of PSD, cortical rTMS reduced the need for physical or cognitive engagement in complex cases and had the potential to shorten the course of treatment. Previous studies have demonstrated that this non-reduced magnetic signal can reach the target area of brain tissue through the skull, thereby changing the functional status of the local cerebral cortex, enhancing synaptic function, and regulating neuronal function in the brain (Bath et al., 2018). Moreover, TMS has different intensities, frequencies and stimulation areas and can modulate the relationships and interactions among neural networks, thus affecting the functions of different regions. TMS promotes accurate and optimal balance of excitatory and inhibitory control functions in the cerebral cortex.
Despite the considerable benefits of TMS, lots of limitations restrict its use in clinical practice in terms of effectiveness, safety, and clinical study design. First, no significant beneficial effects of TMS on genetic factors, death, dependence, disability, prognosis, or length of hospital stay have been reported (Hoshi and Tamura, 1993; Wiethoff et al., 2014; Horvath et al., 2016). Second, patients in a few of earlier trials received traditional rehabilitation training, which made it impossible to separately analyze the effects of nerve stimulation therapy. In treatment of PSD with TMS, the optimal choice of stimulation site (unaffected hemisphere, affected hemisphere, or bilateral hemispheres) has not yet been determined. Based on different viewpoints on the recovery mechanism of PSD, the choice of excitatory stimulation (high frequency) or inhibitory stimulation (low frequency) at the corresponding site (involved, affected, or bilateral side) is controversial. In additions, the number of reported studies is limited, with small sample sizes, uneven case quality and significant heterogeneity among studies. Therefore, the available data are insufficient draw accurate conclusions on the recommended optimal treatment regimen.
This review provides a summary of the efficacy and underlying mechanisms of TMS activity in patients with PSD. A large majority of studies to date has used water-swallowing test (WST), clinical dysphagia scale (CDS), Dysphagia Outcome and Severity Scale (DOSS), Permeation Aspiration Scale (PAS), Mann Assessment of Swallowing Ability (MASA), Videofluoroscopic Dysphagia Scale (VDS), representative pharyngeal motor evoked potential (PMEP) amplitude, cumulative penetration-aspiration score (cPAS), and degree of dysphagia (DD) to evaluate the significance of the results. However, given the evidence for the validity of the results, it may be possible to incorporate more credible tests to draw strong conclusions in future studies. In 1993, Hoshi and Tamura demonstrated the validity of measuring different cortical regions with functional near-infrared spectroscopy (fNIRS). For the first time, the potential of fNIRS imaging brain activation sequences were reported (Ehlis et al., 2009). fNIRS is a neuroimaging technique used to map the function of the human cerebral cortex that utilizes the principle of near-infrared (NIR) spectroscopy (NIRS). Changes in optical properties of the human cerebral cortex are detected simultaneously from multiple measurement sites and the results displayed in the form of maps or images in specific areas. Over the years, fNIRS has emerged as a key neuroimaging technique that has contributed significantly to advances in understanding human brain function. In recent years, the validity of fNIRS measurements has been repeatedly demonstrated by simultaneous functional magnetic resonance imaging (fMRI) measurements, with widely recognized applications in newborn/child and adult language processing in cognitive neuroscience. Although TMS demonstrate great potential to accelerate the improvement of swallowing function in patients with PSD, there is currently a lack of real-time assessment tool for brain function to optimize TMS parameters. As an assessment tool of brain activity, fNIRS can be used to measure the changes in hemoglobin (Hb) concentrations within the brain, which can not only evaluate the effect of TMS treatment, but also can guide the optimization of TMS treatment regimen during the PSD rehabilitation. In the future, we should combine the TMS and fNIRS to serve as a reference for upcoming clinical and laboratory research.
All authors listed have made a substantial, direct, and intellectual contribution to the work, and approved it for publication.
This work was supported by the Yunnan Provincial Academician and Expert Workstation (202005AF150073).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Balcerak, P., Corbiere, S., Zubal, R., and Kägi, G. (2022). Post-stroke Dysphagia: Prognosis and Treatment–A Systematic Review of RCT on Interventional Treatments for Dysphagia Following Subacute Stroke. Front. Neurol. 13:823189. doi: 10.3389/fneur.2022.823189
Barker, A. T., Jalinous, R., and Freeston, I. L. (1985). Non-invasive magnetic stimulation of human motor cortex. Lancet 1, 1106–1107. doi: 10.1016/S0140-6736(85)92413-4
Barwood, C. H., Murdoch, B. E., Whelan, B. M., Lloyd, D., Riek, S., Jd, O. S., et al. (2011a). Improved language performance subsequent to low-frequency rTMS in patients with chronic non-fluent aphasia post-stroke. Eur. J. Neurol. 18, 935–943. doi: 10.1111/j.1468-1331.2010.03284.x
Barwood, C. H., Murdoch, B. E., Whelan, B. M., Lloyd, D., Riek, S., O’Sullivan, J., et al. (2011b). The effects of low frequency Repetitive Transcranial Magnetic Stimulation (rTMS) and sham condition rTMS on behavioural language in chronic non-fluent aphasia: Short term outcomes. NeuroRehabilitation 28, 113–128. doi: 10.3233/NRE-2011-0640
Barwood, C. H., Murdoch, B. E., Whelan, B. M., Lloyd, D., Riek, S., O’Sullivan, J. D., et al. (2011c). Modulation of N400 in chronic non-fluent aphasia using low frequency Repetitive Transcranial Magnetic Stimulation (rTMS). Brain Lang. 116, 125–135. doi: 10.1016/j.bandl.2010.07.004
Bath, P. M., Lee, H. S., and Everton, L. F. (2018). Swallowing therapy for dysphagia in acute and subacute stroke. Cochrane Database Syst. Rev. 10:CD000323. doi: 10.1002/14651858.CD000323.pub3
Cheng, I. K. Y., Chan, K. M. K., Wong, C. S., Li, L. S. W., Chiu, K. M. Y., Cheung, R. T. F., et al. (2017). Neuronavigated high-frequency repetitive transcranial magnetic stimulation for chronic post-stroke dysphagia: A randomized controlled study. J. Rehabil. Med. 49, 475–481. doi: 10.2340/16501977-2235
Cheng, I. K., Chan, K. M., Wong, C. S., and Cheung, R. T. (2015). Preliminary evidence of the effects of high-frequency repetitive transcranial magnetic stimulation (rTMS) on swallowing functions in post-stroke individuals with chronic dysphagia. Int. J. Lang. Commun. Disord. 50, 389–396. doi: 10.1111/1460-6984.12144
Chiang, C. F., Lin, M. T., Hsiao, M. Y., Yeh, Y. C., Liang, Y. C., and Wang, T. G. (2019). Comparative Efficacy of Noninvasive Neurostimulation Therapies for Acute and Subacute Poststroke Dysphagia: A Systematic Review and Network Meta-analysis. Arch. Phys. Med. Rehabil. 100, 739–750.e4. doi: 10.1016/j.apmr.2018.09.117
Cohen, D. L., Roffe, C., Beavan, J., Blackett, B., Fairfield, C. A., Hamdy, S., et al. (2016). Post-stroke dysphagia: A review and design considerations for future trials. Int. J. Stroke 11, 399–411. doi: 10.1177/1747493016639057
Cotelli, M., Manenti, R., Cappa, S. F., Zanetti, O., and Miniussi, C. (2008). Transcranial magnetic stimulation improves naming in Alzheimer disease patients at different stages of cognitive decline. Eur. J. Neurol. 15, 1286–1292. doi: 10.1111/j.1468-1331.2008.02202.x
Du, J., Yang, F., Liu, L., Hu, J., Cai, B., Liu, W., et al. (2016). Repetitive transcranial magnetic stimulation for rehabilitation of poststroke dysphagia: A randomized, double-blind clinical trial. Clin. Neurophysiol. 127, 1907–1913. doi: 10.1016/j.clinph.2015.11.045
Ehlis, A. C., Ringel, T. M., Plichta, M. M., Richter, M. M., Herrmann, M. J., and Fallgatter, A. J. (2009). Cortical correlates of auditory sensory gating: a simultaneous near-infrared spectroscopy event-related potential study. Neuroscience 159, 1032–1043. doi: 10.1016/j.neuroscience.2009.01.015
Ertekin, C., Aydogdu, I., Tarlaci, S., Turman, A. B., and Kiylioglu, N. (2000). Mechanisms of dysphagia in suprabulbar palsy with lacunar infarct. Stroke 31, 1370–1376. doi: 10.1161/01.STR.31.6.1370
Eslick, G. D., and Talley, N. J. (2008). Dysphagia: epidemiology, risk factors and impact on quality of life–a population-based study. Aliment. Pharmacol. Ther. 27, 971–979. doi: 10.1111/j.1365-2036.2008.03664.x
Fitzgerald, P. B., Fountain, S., and Daskalakis, Z. J. (2006). A comprehensive review of the effects of rTMS on motor cortical excitability and inhibition. Clin. Neurophysiol. 117, 2584–2596. doi: 10.1016/j.clinph.2006.06.712
Fung, C. W., Khong, P. L., To, R., Goh, W., and Wong, V. (2004). Video-fluoroscopic study of swallowing in children with neurodevelopmental disorders. Pediatr. Int. 46, 26–30. doi: 10.1111/j.1442-200X.2004.t01-1-.x
Geeganage, C., Beavan, J., Ellender, S., and Bath, P. M. (2012). Interventions for dysphagia and nutritional support in acute and subacute stroke. Cochrane Database Syst. Rev. 10:CD000323. doi: 10.1002/14651858.CD000323.pub2
Ghelichi, L., Joghataei, M. T., Jalaie, S., Nakhostin-Ansari, N., Forogh, B., and Mehrpour, M. (2016). A single-subject study to evaluate the inhibitory repetitive transcranial magnetic stimulation combined with traditional dysphagia therapy in patients with post-stroke dysphagia. Iran. J. Neurol. 15, 140–145.
Hägg, M., and Anniko, M. (2008). Lip muscle training in stroke patients with dysphagia. Acta Otolaryngol. 128, 1027–1033. doi: 10.1080/00016480701813814
Hägg, M., and Larsson, B. (2004). Effects of motor and sensory stimulation in stroke patients with long-lasting dysphagia. Dysphagia 19, 219–230. doi: 10.1007/s00455-004-0016-3
Hallett, M. (2000). Transcranial magnetic stimulation and the human brain. Nature 406, 147–150. doi: 10.1038/35018000
Hamdy, S. (2010). Role of Neurostimulation and Neuroplasticity in the Rehabilitation of Dysphagia After Stroke. Perspect. Swallow. Swallow. Disord. 19, 3–9. doi: 10.1044/sasd19.1.3
Hamdy, S., Aziz, Q., Rothwell, J. C., Power, M., Singh, K. D., Nicholson, D. A., et al. (1998). Recovery of swallowing after dysphagic stroke relates to functional reorganization in the intact motor cortex. Gastroenterology 115, 1104–1112. doi: 10.1016/S0016-5085(98)70081-2
Hoogendam, J. M., Ramakers, G. M., and Di Lazzaro, V. (2010). Physiology of repetitive transcranial magnetic stimulation of the human brain. Brain Stimul. 3, 95–118. doi: 10.1016/j.brs.2009.10.005
Horvath, J. C., Vogrin, S. J., Carter, O., Cook, M. J., and Forte, J. D. (2016). Effects of a common transcranial direct current stimulation (tDCS) protocol on motor evoked potentials found to be highly variable within individuals over 9 testing sessions. Exp. Brain Res. 234, 2629–2642. doi: 10.1007/s00221-016-4667-8
Hoshi, Y., and Tamura, M. (1993). Dynamic multichannel near-infrared optical imaging of human brain activity. J. Appl. Physiol. 75, 1842–1846. doi: 10.1152/jappl.1993.75.4.1842
Huang, Y. Z., Chen, R. S., Rothwell, J. C., and Wen, H. Y. (2007). The after-effect of human theta burst stimulation is NMDA receptor dependent. Clin. Neurophysiol. 118, 1028–1032. doi: 10.1016/j.clinph.2007.01.021
Jiao, Y., Li, G., and Dai, Y. (2022). Clinical effect of repetitive transcranial magnetic stimulation on dysphagia due to stroke. Neurol. Sci. 43, 3139–3144. doi: 10.1007/s10072-021-05799-7
Kalita, M., Majewska, K., Gradowska, A., Karwowska, K., and Ławiński, M. (2015). Food, mechanic and septic complications in patients enterally nutritioned in home conditions. Pol. Przegl. Chir. 86, 466–472. doi: 10.2478/pjs-2014-0083
Kang, J. H., Park, R. Y., Lee, S. J., Kim, J. Y., Yoon, S. R., and Jung, K. I. (2012). The effect of bedside exercise program on stroke patients with Dysphagia. Ann. Rehabil. Med. 36, 512–520. doi: 10.5535/arm.2012.36.4.512
Khedr, E. M., Abo-Elfetoh, N., and Rothwell, J. C. (2009). Treatment of post-stroke dysphagia with repetitive transcranial magnetic stimulation. Acta Neurol. Scand. 119, 155–161. doi: 10.1111/j.1600-0404.2008.01093.x
Kim, S. J. (2010). Music therapy protocol development to enhance swallowing training for stroke patients with dysphagia. J. Music Ther. 47, 102–119. doi: 10.1093/jmt/47.2.102
Koerselman, F., Laman, D. M., van Duijn, H., van Duijn, M. A., and Willems, M. A. (2004). A 3-month, follow-up, randomized, placebo-controlled study of repetitive transcranial magnetic stimulation in depression. J. Clin. Psychiatry 65, 1323–1328. doi: 10.4088/JCP.v65n1005
Kumar, S., Selim, M. H., and Caplan, L. R. (2010). Medical complications after stroke. Lancet. Neurol. 9, 105–118. doi: 10.1016/S1474-4422(09)70266-2
Lanza, G., Cantone, M., Lanuzza, B., Pennisi, M., Bella, R., Pennisi, G., et al. (2015). Distinctive patterns of cortical excitability to transcranial magnetic stimulation in obstructive sleep apnea syndrome, restless legs syndrome, insomnia, and sleep deprivation. Sleep Med. Rev. 19, 39–50. doi: 10.1016/j.smrv.2014.04.001
Lefaucheur, J. P., André-Obadia, N., Antal, A., Ayache, S. S., Baeken, C., Benninger, D. H., et al. (2014). Evidence-based guidelines on the therapeutic use of repetitive transcranial magnetic stimulation (rTMS). Clin. Neurophysiol. 125, 2150–2206. doi: 10.1016/j.clinph.2014.05.021
Liao, X., Xing, G., Guo, Z., Jin, Y., Tang, Q., He, B., et al. (2017). Repetitive transcranial magnetic stimulation as an alternative therapy for dysphagia after stroke: a systematic review and meta-analysis. Clin. Rehabil. 31, 289–298. doi: 10.1177/0269215516644771
Lin, L. C., Wang, S. C., Chen, S. H., Wang, T. G., Chen, M. Y., and Wu, S. C. (2003). Efficacy of swallowing training for residents following stroke. J. Adv. Nurs. 44, 469–478. doi: 10.1046/j.0309-2402.2003.02830.x
Mann, G., Hankey, G. J., and Cameron, D. (1999). Swallowing function after stroke: prognosis and prognostic factors at 6 months. Stroke 30, 744–748. doi: 10.1161/01.STR.30.4.744
Marchina, S., Pisegna, J. M., Massaro, J. M., Langmore, S. E., McVey, C., Wang, J., et al. (2021). Transcranial direct current stimulation for post-stroke dysphagia: a systematic review and meta-analysis of randomized controlled trials. J. Neurol. 268, 293–304. doi: 10.1007/s00415-020-10142-9
McCullough, G. H., Kamarunas, E., Mann, G. C., Schmidley, J. W., Robbins, J. A., and Crary, M. A. (2012). Effects of Mendelsohn maneuver on measures of swallowing duration post stroke. Top. Stroke Rehabil. 19, 234–243. doi: 10.1310/tsr1903-234
Murdoch, B. E., Ng, M. L., and Barwood, C. H. (2012). Treatment of articulatory dysfunction in Parkinson’s disease using repetitive transcranial magnetic stimulation. Eur. J. Neurol. 19, 340–347. doi: 10.1111/j.1468-1331.2011.03524.x
Naeser, M. A., Martin, P. I., Nicholas, M., Baker, E. H., Seekins, H., Kobayashi, M., et al. (2005). Improved picture naming in chronic aphasia after TMS to part of right Broca’s area: an open-protocol study. Brain Lang. 93, 95–105. doi: 10.1016/j.bandl.2004.08.004
Park, E., Kim, M. S., Chang, W. H., Oh, S. M., Kim, Y. K., Lee, A., et al. (2017). Effects of Bilateral Repetitive Transcranial Magnetic Stimulation on Post-Stroke Dysphagia. Brain Stimul. 10, 75–82. doi: 10.1016/j.brs.2016.08.005
Park, J. W., Kim, H., Park, T., Yeo, J. S., Hong, H. J., and Oh, J. Y. (2019). A pilot study of the effects of high-frequency repetitive transcranial magnetic stimulation on dysphagia in the elderly. Neurogastroenterol. Motil. 31:e13561. doi: 10.1111/nmo.13561
Pascual-Leone, A., Tormos, J. M., Keenan, J., Tarazona, F., Cañete, C., and Catalá, M. D. (1998). Study and modulation of human cortical excitability with transcranial magnetic stimulation. J. Clin. Neurophysiol. 15, 333–343. doi: 10.1097/00004691-199807000-00005
Pisegna, J. M., Kaneoka, A., Pearson, W. G. Jr., Kumar, S., and Langmore, S. E. (2016). Effects of non-invasive brain stimulation on post-stroke dysphagia: A systematic review and meta-analysis of randomized controlled trials. Clin. Neurophysiol. 127, 956–968. doi: 10.1016/j.clinph.2015.04.069
Ridding, M. C., and Rothwell, J. C. (2007). Is there a future for therapeutic use of transcranial magnetic stimulation? Nat. Rev. Neurosci. 8, 559–567. doi: 10.1038/nrn2169
Rossi, S., Hallett, M., Rossini, P. M., and Pascual-Leone, A. (2009). Safety, ethical considerations, and application guidelines for the use of transcranial magnetic stimulation in clinical practice and research. Clin. Neurophysiol. 120, 2008–2039. doi: 10.1016/j.clinph.2009.08.016
Smithard, D. G., O’Neill, P. A., Parks, C., and Morris, J. (1996). Complications and outcome after acute stroke. Does dysphagia matter? Stroke 27, 1200–1204. doi: 10.1161/01.STR.27.7.1200
Speyer, R., Baijens, L., Heijnen, M., and Zwijnenberg, I. (2010). Effects of therapy in oropharyngeal dysphagia by speech and language therapists: a systematic review. Dysphagia 25, 40–65. doi: 10.1007/s00455-009-9239-7
Stefan, K., Kunesch, E., Benecke, R., Cohen, L. G., and Classen, J. (2002). Mechanisms of enhancement of human motor cortex excitability induced by interventional paired associative stimulation. J. Physiol. 543, 699–708. doi: 10.1113/jphysiol.2002.023317
Tarameshlu, M., Ansari, N. N., Ghelichi, L., and Jalaei, S. (2019). The effect of repetitive transcranial magnetic stimulation combined with traditional dysphagia therapy on poststroke dysphagia: a pilot double-blinded randomized-controlled trial. Int. J. Rehabil. Res. 42, 133–138. doi: 10.1097/MRR.0000000000000336
Terré, R., Panadés, A., and Mearin, F. (2013). Botulinum toxin treatment for oropharyngeal dysphagia in patients with stroke. Neurogastroenterol. Motil. 25, 896–e702. doi: 10.1111/nmo.12213
Ünlüer, N., Temuçin, ÇM., Demir, N., Serel Arslan, S., and Karaduman, A. A. (2019). Effects of Low-Frequency Repetitive Transcranial Magnetic Stimulation on Swallowing Function and Quality of Life of Post-stroke Patients. Dysphagia 34, 360–371. doi: 10.1007/s00455-018-09965-6
Vasant, D. H., Sasegbon, A., Michou, E., Smith, C., and Hamdy, S. (2019). Rapid improvement in brain and swallowing behavior induced by cerebellar repetitive transcranial magnetic stimulation in poststroke dysphagia: A single patient case-controlled study. Neurogastroenterol. Motility 31:e13609. doi: 10.1111/nmo.13609
Verin, E., and Leroi, A. M. (2009). Poststroke dysphagia rehabilitation by repetitive transcranial magnetic stimulation: a noncontrolled pilot study. Dysphagia 24, 204–210. doi: 10.1007/s00455-008-9195-7
Wassermann, E. M. (1998). Risk and safety of repetitive transcranial magnetic stimulation: report and suggested guidelines from the International Workshop on the Safety of Repetitive Transcranial Magnetic Stimulation. June 5-7, 1996. Electroencephalogr. Clin. Neurophysiol. 108, 1–16. doi: 10.1016/S0168-5597(97)00096-8
Wiethoff, S., Hamada, M., and Rothwell, J. C. (2014). Variability in response to transcranial direct current stimulation of the motor cortex. Brain Stimul. 7, 468–475. doi: 10.1016/j.brs.2014.02.003
Yang, S. N., Pyun, S. B., Kim, H. J., Ahn, H. S., and Rhyu, B. J. (2015). Effectiveness of Non-invasive Brain Stimulation in Dysphagia Subsequent to Stroke: A Systemic Review and Meta-analysis. Dysphagia 30, 383–391. doi: 10.1007/s00455-015-9619-0
Zhai, B., Fu, J., Xiang, S., Shang, Y., Yan, Y., Yin, T., et al. (2020). Repetitive transcranial magnetic stimulation ameliorates recognition memory impairment induced by hindlimb unloading in mice associated with BDNF/TrkB signaling. Neurosci. Res. 153, 40–47. doi: 10.1016/j.neures.2019.04.002
Keywords: post-stroke dysphagia, neuroplasticity, transcranial magnetic stimulation, effectiveness, therapeutic mechanism
Citation: Li Y, Chen K, Wang J, Lu H, Li X, Yang L, Zhang W, Ning S, Wang J, Sun Y, Song Y, Zhang M, Hou J and Shi H (2022) Research progress on transcranial magnetic stimulation for post-stroke dysphagia. Front. Behav. Neurosci. 16:995614. doi: 10.3389/fnbeh.2022.995614
Received: 16 July 2022; Accepted: 29 July 2022;
Published: 18 August 2022.
Edited by:
Dongdong Qin, Yunnan University of Chinese Medicine, ChinaCopyright © 2022 Li, Chen, Wang, Lu, Li, Yang, Zhang, Ning, Wang, Sun, Song, Zhang, Hou and Shi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hongling Shi, a21zaGwxQDEyNi5jb20=; Mei Zhang, MTIxMTkwOTA0N0BxcS5jb20=; Jianhong Hou, aGpoanl5QDEyNi5jb20=
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.