
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Neuroanat. , 10 June 2022
Volume 16 - 2022 | https://doi.org/10.3389/fnana.2022.863900
This article is part of the Research Topic What does Human Pathology Bring to the Understanding of the Fundamental Mechanisms of Development? View all 9 articles
 Kinga A. Sándor-Bajusz1,2*
Kinga A. Sándor-Bajusz1,2* Asaad Sadi3
Asaad Sadi3 Eszter Varga1
Eszter Varga1 Györgyi Csábi1
Györgyi Csábi1 Georgios N. Antonoglou4
Georgios N. Antonoglou4 Szimonetta Lohner5,6
Szimonetta Lohner5,6Background: Neuroimaging of individuals with non-syndromic oral clefts have revealed subtle brain structural differences compared to matched controls. Previous studies strongly suggest a unified primary dysfunction of normal brain and face development which could explain these neuroanatomical differences and the neuropsychiatric issues frequently observed in these individuals. Currently there are no studies that have assessed the overall empirical evidence of the association between oral clefts and brain structure. Our aim was to summarize the available evidence on potential brain structural differences in individuals with non-syndromic oral clefts and their matched controls.
Methods: MEDLINE, Scopus, Cochrane Central Register of Controlled Trials, Web of Science and Embase were systematically searched in September 2020 for case-control studies that reported structural brain MRI in individuals with non-syndromic oral clefts and healthy controls. Studies of syndromic oral clefts were excluded. Two review authors independently screened studies for eligibility, extracted data and assessed risk of bias with the Newcastle-Ottawa Scale. Random effects meta-analyses of mean differences (MDs) and their 95% confidence intervals (95% CI) were performed in order to compare global and regional brain MRI volumes.
Results: Ten studies from 18 records were included in the review. A total of 741 participants were analyzed. A moderate to high risk of bias was determined for the included studies. The cerebellum (MD: −12.46 cm3, 95% CI: −18.26, −6.67, n = 3 studies, 354 participants), occipital lobes (MD: −7.39, 95% CI: −12.80, −1.99, n = 2 studies, 120 participants), temporal lobes (MD: −10.53 cm3, 95% CI: −18.23, −2.82, n = 2 studies, 120 participants) and total gray matter (MD: −41.14 cm3; 95% CI: −57.36 to −24.92, n = 2 studies, 172 participants) were significantly smaller in the cleft group compared to controls.
Discussion: There may be structural brain differences between individuals with non-syndromic oral clefts and controls based on the available evidence. Improvement in study design, size, methodology and participant selection could allow a more thorough analysis and decrease study heterogeneity.
Oral clefts are one of the most common birth defects with a worldwide incidence of 1:700 births (Mossey and Modell, 2012). Oral clefts can be syndromic or non-syndromic, the latter occurring as a single anomaly in the absence of other physical and developmental disorders (Mossey and Modell, 2012; Bjørnland et al., 2021). The etiology of oral clefts is multifactorial, including gene-environmental interactions, hereditary causes, antenatal nutrition, and drug exposure (Lithovius et al., 2014; Bjørnland et al., 2021). Oral clefts can be anatomically classified as cleft lip (CL), cleft palate (CP), and combined cleft lip and palate (CLP) (Lithovius et al., 2014; Bjørnland et al., 2021).
Syndromic oral clefts are predisposed to more complex treatment due to the underlying genetic disorder and other associated health complications (Sándor-Bajusz et al., 2021). Syndromic individuals often have mental comorbidities including intellectual disability and learning disorders (Hardin-Jones and Chapman, 2011; Diaz-Stransky and Tierney, 2012; Feragen et al., 2014; McDonald-McGinn et al., 2015; Zinkstok et al., 2019). Decades of research revealed the presence of neuropsychiatric and neurodevelopmental disorders in individuals with non-syndromic oral clefts (Broder et al., 1998; Richman and Ryan, 2003; Conrad et al., 2008; Pedersen et al., 2016; Ansen-Wilson et al., 2018; Tillman et al., 2018). Children with oral clefts are associated with a significant agglomeration of psychiatry disorders including intellectual disability, autism spectrum disorder, ADHD and learning disorders (Pedersen et al., 2016; Ansen-Wilson et al., 2018; Tillman et al., 2018). Neurodevelopmental delays have been documented in younger children including fine motor, gross motor and both expressive and receptive language development (Conrad et al., 2008; Hardin-Jones and Chapman, 2011; Gallagher and Collett, 2019). These observations were suggested to be the consequence of multiple stressors including social stigma, frequent anesthesia exposure and/or cleft-related airway obstruction impairing proper neurodevelopment (Gallagher and Collett, 2019).
New advances in oral cleft research have strongly suggested a unified primary dysfunction of normal brain and face development, that could explain the neurodevelopmental-related deficits observed in these children (Conrad et al., 2021). This primary dysfunction seems to affect a crucial developmental stage of a physiological migration of cells that will later form the face and parts of the brain and the central nervous system (Ansen-Wilson et al., 2018; Ornoy, 2020). Neuroimaging studies have additionally revealed significant differences in the brain structure of individuals with non-syndromic oral clefts compared to matched controls. However, a definitive statement cannot be made due to the heterogeneity among the studies including quality, sample size, methodology and outcomes (Yang et al., 2012; Gallagher and Collett, 2019).
The aim of the present systematic review was to assess the overall empirical evidence of the association between of non-syndromic oral clefts and the brain.
The current meta-analysis was registered in PROSPERO (International Prospective Register of Systematic Reviews1; RRID:SCR_019061, identifier CRD42020167773), and is reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses 2020 (PRISMA 2020, RRID:SCR_018721) guideline (Page et al., 2021).
Searches of the following databases were conducted until 7 September 2020: MEDLINE (Ovid; RRID:SCR_002185), Scopus, Cochrane Central Register of Controlled Trials (CENTRAL; RRID:SCR_006576), Web of Science and Embase (RRID:SCR_001650). Clinicaltrials.gov (RRID:SCR_002309) was searched to identify ongoing/completed studies and unpublished SRs (see Supplementary Table 1 for the full search strategy used in each of the databases).
The following criteria had to be met for inclusion into the study: (1) Case-control studies with humans; (2) Individuals with non-syndromic (isolated) oral clefts, without restriction to age; (3) Healthy controls; (4) Structural brain differences of individuals with non-syndromic oral clefts vs. their controls as a relevant outcome: structural differences had to be explored with brain MRI. No restrictions were applied for language.
The publication was excluded if it had any of the following: (1) Animal studies (2) Individuals with syndromes (syndromic forms of oral clefts, such as Pierre-Robin sequence or Velocardiofacial syndrome).
The selection process was performed with the Covidence systematic review software (RRID:SCR_016484) (Veritas Health Innovation, 2017).
Two review authors (KSB and EV) screened the titles and/or abstracts of studies retrieved from the searches. Additional sources were also screened (hand searching, reference/citation lists) to identify articles that may potentially meet the inclusion criteria. Full texts of these potentially eligible records were retrieved and assessed by one review author (KSB), while a second checked the decisions (EV). Any differences between the two reviewers were settled by consensus after consulting a third author (GA or SL).
Data was extracted independently by three authors (KSB, AS, and EV). Discrepancies were resolved the same way as stated above.
Study setting (design, institution, country), patient demographics (number, age, sex, ethnicity, gender, type of oral cleft, brain imaging details, data processing) and outcome measurement details (general and regional brain MRI measurements) were collected. Any data that were not described in the article were calculated from existing data, or were obtained by contacting the authors.
The primary outcome measures were structural differences of the brain of individuals with oral clefts vs. individuals without oral clefts (controls) investigated via MRI. Other sought outcomes included the correlation between observed structural differences in the brain of individuals with oral clefts and alterations in neurological and/or mental functioning compared to controls.
The Newcastle-Ottawa Scale (NOS) (Wells et al., 2000) was used for all outcomes to assess the quality of non-randomized case-control studies included in the systematic review. Assessment was completed by two authors (KSB, AS) and independently checked by a third (SL) the same way to resolve discrepancies.
Review Manager Software Version 5.4 was used for data synthesis (RRID:SCR_003581) (Cochrane, 2020). The random-effects model was chosen a priori as the primary method to estimate all pooled estimates for studies that were comparable in design, exposure and outcomes. This model was used to account for the differences within study populations such as age, sex, and type of oral clefts. Mean Differences (MDs) and their corresponding 95% confidence intervals (CI 95%) were used for continuous outcomes.
The extent and impact of between-study heterogeneity was assessed by inspecting the forest plots and by calculating the tau-squared and the I-squared statistics, respectively. The I-squared thresholds represented heterogeneity that may not be important (0–40%), moderate (30–60%), substantial (50–90%), or considerable (75–100%). Possible sources of heterogeneity in meta-analyses were sought through pre-specified mixed-effects subgroup analyses if at least two studies were included for a comparison (same intervention/outcome). Pre-defined subgroup analyses included: (i) age; (ii) sex; (iii) ethnicity; (iv) cleft form (non-syndromic vs. syndromic).
Assessment of reporting biases (small-study effects or publication bias) was planned through the inspection of a contour-enhanced funnel plot and with the Egger’s weighted regression test if a sufficient number of trials were identified (n > 10).
A total of 257 records were identified following the database searches. Overall, 245 records underwent title and abstract screening following duplicate removal. Thirty-two records were retrieved and assessed for eligibility. Two records were additionally identified by handsearching, and only one met the inclusion criteria (Yang et al., 2012). A total of 10 studies from 18 records met the inclusion criteria. Three records included individuals diagnosed with Van der Woude syndrome, a syndromic form of oral clefts (Nopoulos et al., 2000, 2002, 2005). These records were included in the current systematic review as none of the syndromic individuals exceeded 15% of total cleft participants.
The study selection process is shown in the flow diagram of Figure 1.
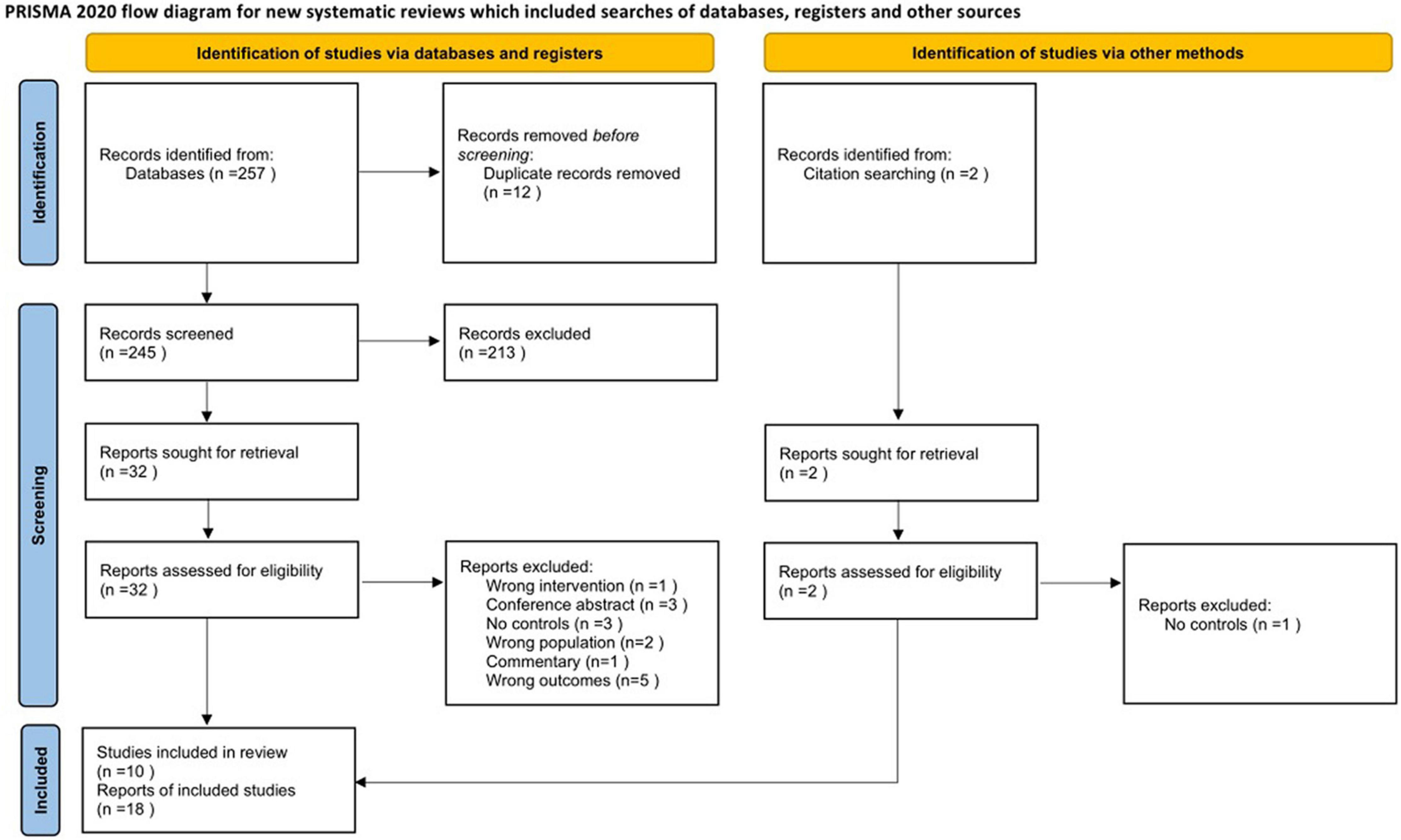
Figure 1. Flow diagram of the study selection process.
Fifteen records seemed to meet the inclusion criteria, however, they were excluded during the full-text screening process. The reasons for exclusion were as follows: absence of a control group (n = 3 Shen and Huang, 1996; Mueller et al., 2007; Zheng et al., 2019), conference abstracts or commentaries (n = 4 Chollet et al., 2010; Tollefson and Sykes, 2010; DeVolder et al., 2014, 2015), wrong study population that only included syndromic cases of oral clefts (n = 2 Nopoulos et al., 2007a,b), absence of neuroimaging (n = 5 Čeponiene et al., 1999; Scott et al., 2005; Kummer et al., 2007; Conrad et al., 2008; Watkins et al., 2018), or neuroimaging other than brain MRI (n = 1 Becker et al., 2008).
The study characteristics are presented in Tables 1A,B. The majority were conducted in the US. Other countries included Australia (Adamson et al., 2014), Brazil (Bodoni et al., 2021), and China (Yang et al., 2012; Li et al., 2020). Study size ranged between 24 and 234 participants. The majority of the participants were males of Caucasian ethnicity. Most of the participants were children.
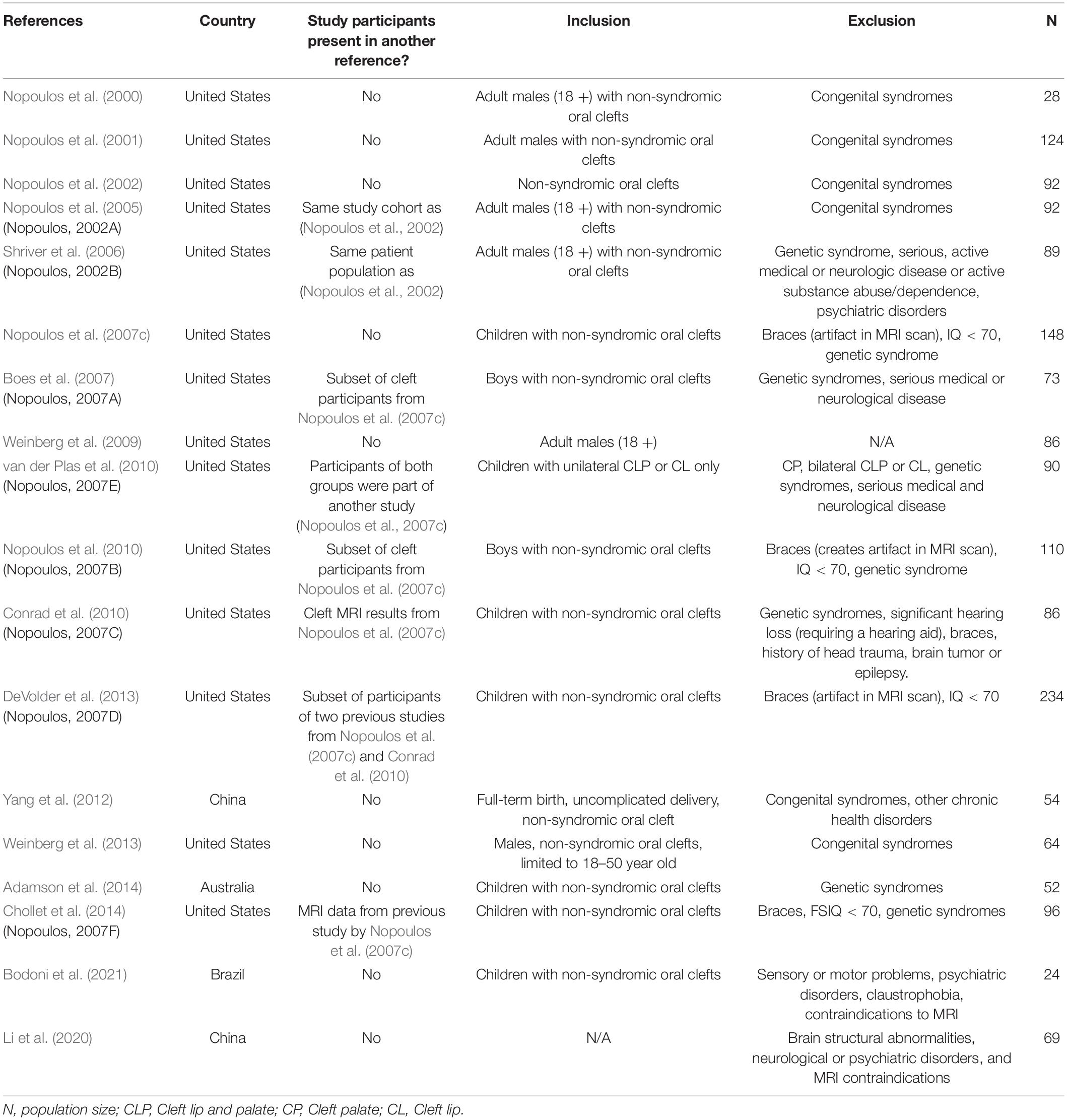
Table 1A. Characteristics of included studies.
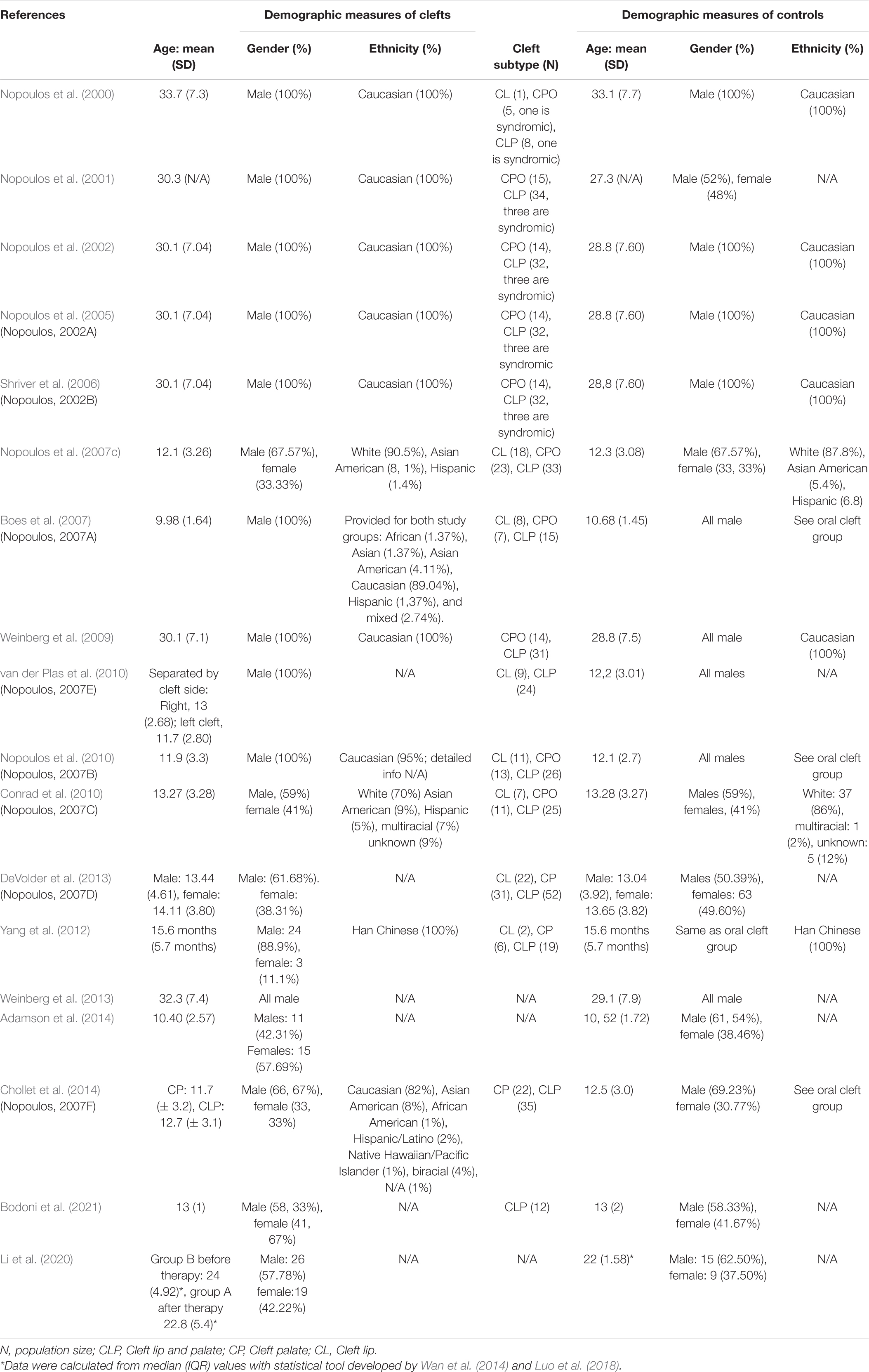
Table 1B. Demographic data of included studies.
The risk of bias assessment of included studies are shown in Table 2. The overall risk of bias ranged from medium to high. Selection of cleft participants, their comparators and the assessment of exposure were described in half of the studies. Information on recruitment and reasons for dropout were not available in most studies. Only one study reported blinding personnel of group status during MRI scanning (Nopoulos et al., 2007c).
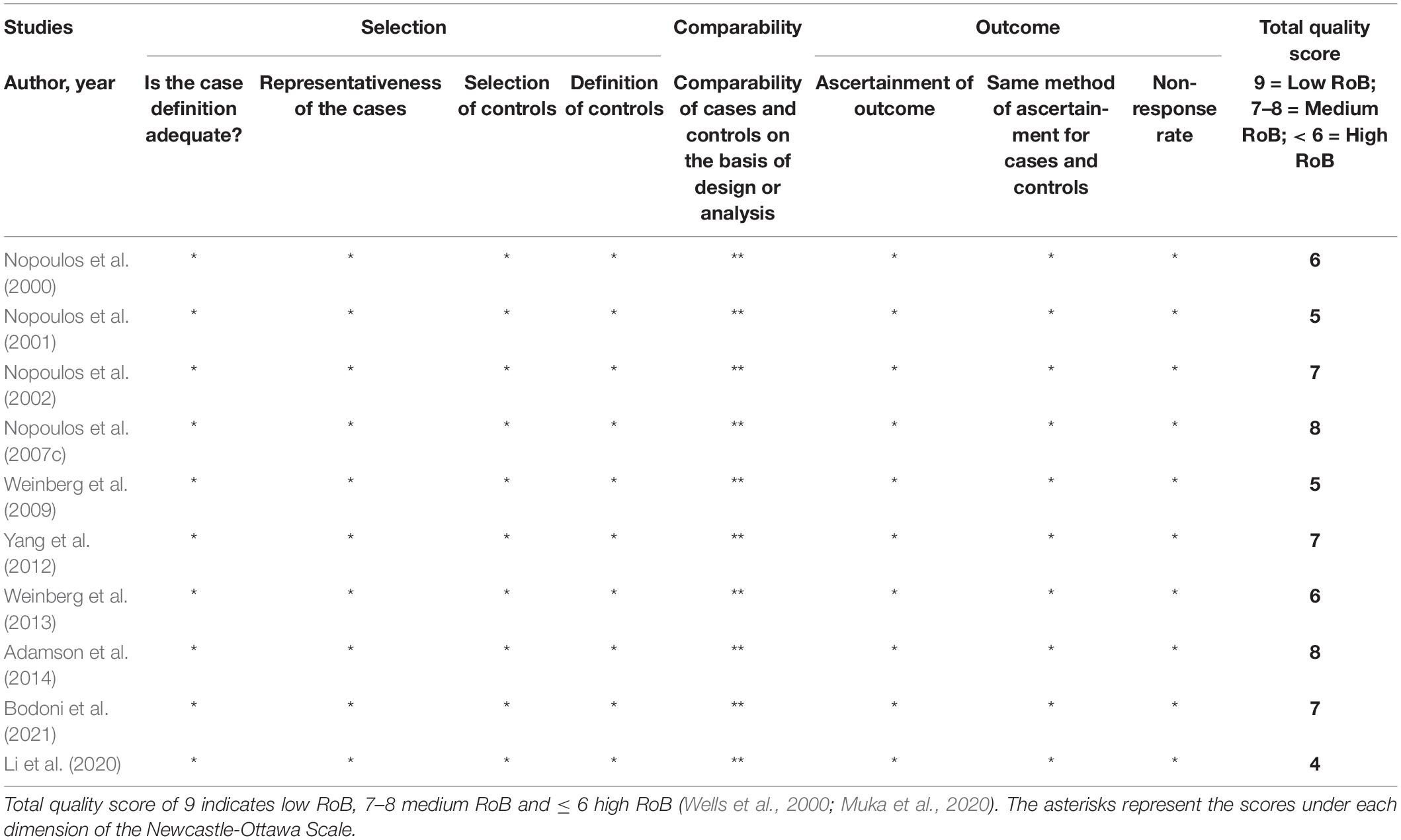
Table 2. Risk of bias (RoB) assessment using the Newcastle-Ottawa Scale.
Five studies were comparable in terms of study design, exposure and outcome. Studies were pooled using a random-effect meta-analysis.
All five studies segmented the brain according to all or one of the following: intracranial volume was divided into total brain tissue and cerebrospinal fluid; the brain tissue was divided into the cerebrum and cerebellum; the cerebrum was subdivided into the frontal, parietal, temporal, and occipital lobes. The majority of the studies used the Talairach Atlas-based method for measures of general and regional brain tissue. Most studies used three different sequences (T1-weighted, T2-weighted, and/or proton density images) with comparable parameters to classify tissue into gray matter, white matter, and cerebrospinal fluid. Additional details of MRI analysis are presented in Supplementary Table 2.
Global measurements were anatomically grouped into three groups: total brain volumes (including MRI volumes of the cerebrum and cerebellum), cerebral volumes (only MRI volumes of the cerebrum), and cerebellar volumes (only MRI volumes of the cerebellum).
The cleft group had lower total gray matter volume compared to controls (MD: −41.14 cm3; 95% CI: −57.36 to −24.92; n = 2; 172 participants; I2: 0%) (Figure 2). There were no differences in brain size of oral cleft subjects compared to controls (MD: −38.86 cm3; 95% CI: −83.88 to 6.16; n = 4;322 participants; I2: 48%) (Figure 3). No differences were found in white matter volume of oral cleft subjects and their controls (MD: −21.93 cm3; 95% CI: −64.20 to 20.33; n = 2; 172 participants; I2: 69%) (see Supplementary Figure 1).

Figure 2. Forest plot for total brain gray matter volume (cm3).
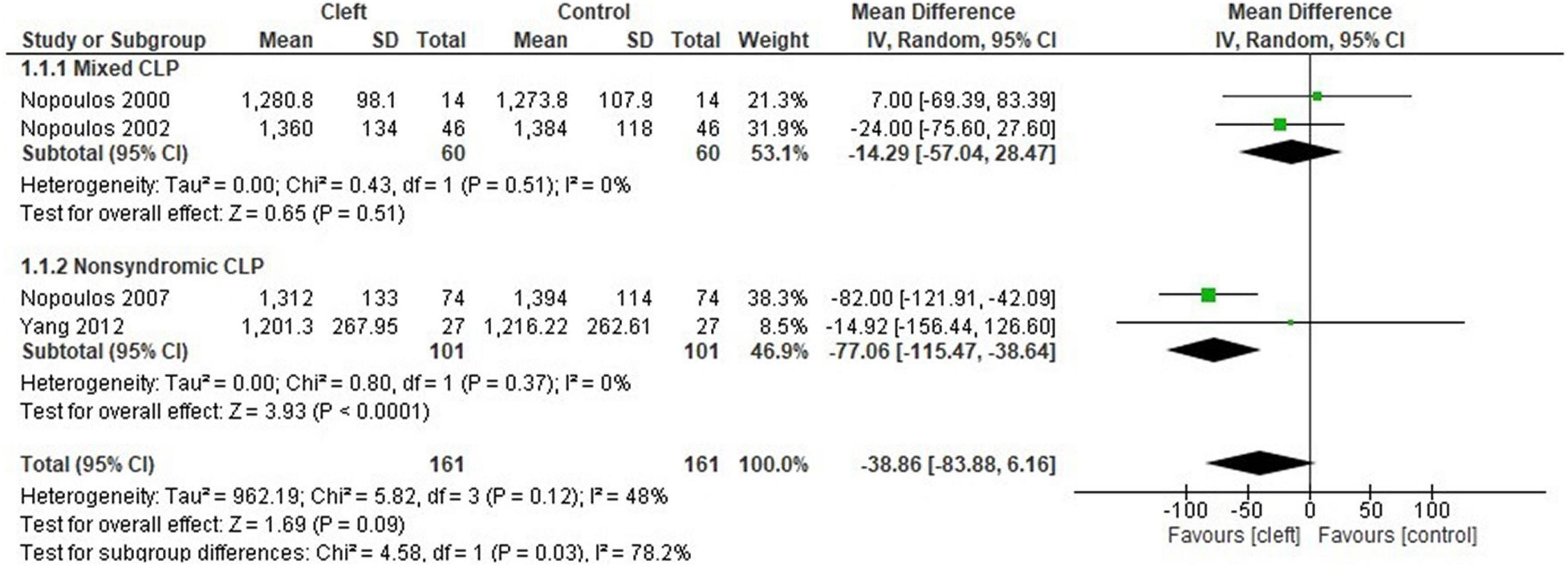
Figure 3. Forest plot for total brain volume (cm3) with subgroup analysis (non-syndromic vs. mixed).
Total volume of the cerebrum in the oral cleft group did not differ from the control group (MD: −22.42 cm3; 95% CI: −66.40 to 21.56; n = 3; 268 participants; I2: 58%) (Figure 4). There were no differences in gray matter volume of the cerebrum between oral clefts and controls (MD: −6.45 cm3; 95% CI: −25.17 to 12.27; n = 2; 202 participants; I2: 0%) (see Supplementary Figure 2). An included study found a significantly lower gray matter volume on the left side of the cerebrum in individuals with oral cleft (Yang et al., 2012, P = 0.033). However, the study could not be included in the meta-analysis due to incomplete data (missing SD values). No differences were observed in cerebral white matter volume between oral clefts and controls (MD: −5.08 cm3; 95% CI: −20.19 to 10.03; n = 2; 146 participants; I2:0%) (Supplementary Figure 3).
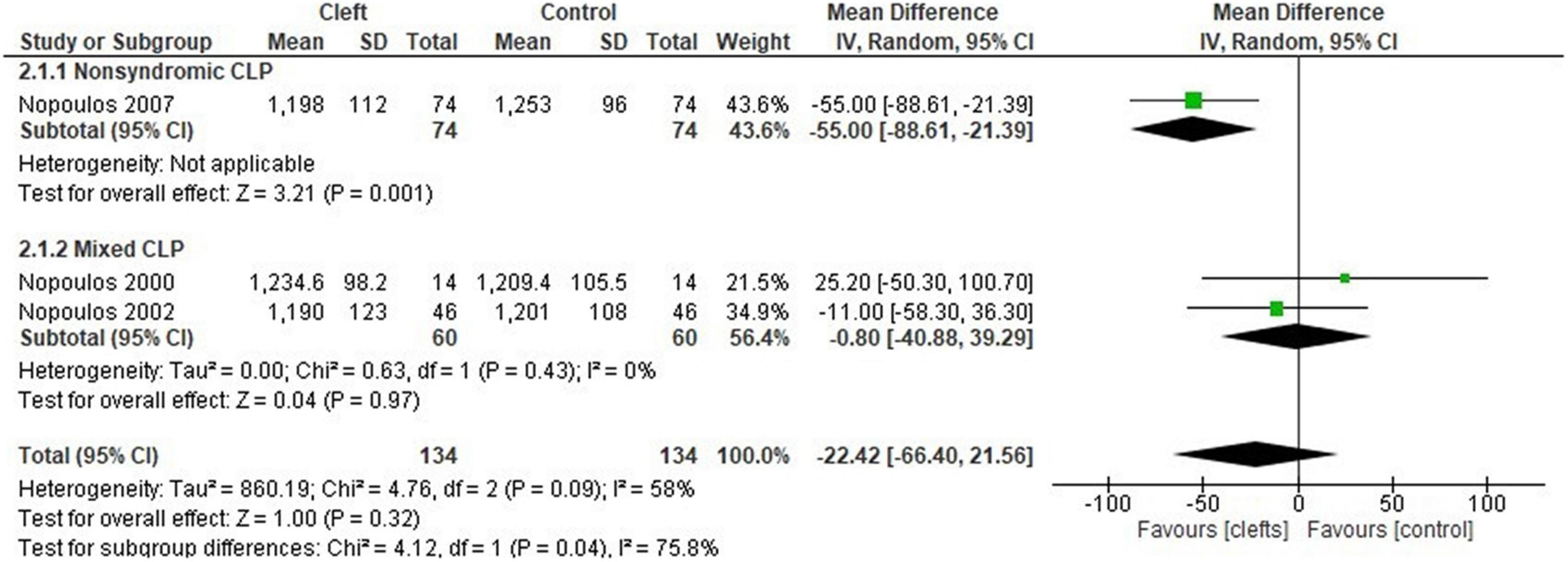
Figure 4. Forest plot for total volume of the cerebrum (cm3) with subgroup analysis (non-syndromic vs. mixed).
The cerebellum was significantly smaller in oral clefts compared to controls (MD: −12.46 cm3; 95% CI: −18.26, −6.67; n = 3; 354 participants; I2: 0%, n = 3) (Figure 5).

Figure 5. Forest plot for total volume of the cerebellum (cm3).
The size of the frontal lobe did not differ between the cleft group and controls (MD: 18.27 cm3; 95% CI: −12.62 to 49.16; n = 2; 120 participants I2: 0%) (Supplementary Figure 4). There were no differences in frontal gray matter volume between oral clefts and controls (MD: 4.77 cm3; 95% CI: −7.84 to 17.38; n = 2; 165 participants; I2: 0%) (Supplementary Figure 5). There were no differences in the two components of the ventrofrontal cortex; the straight gyrus (MD: −0.17 cm3; 95% CI: −1.35 to 1.00; n = 2; 165 participants; I2: 90%) and orbitofrontal cortex (MD: −0.99 cm3; 95% CI: −2.69 to 0.71; n = 2; 165 participants; I2: 0%) (see Supplementary Figures 6, 7).
There were no differences in the size of the parietal lobe between the cleft group and controls (MD: 4.91 cm3; 95% CI: −4.29 to 14.10; n = 2; 120 participants; I2: 0%) (see Supplementary Figure 8).
Smaller temporal lobes were found for the cleft group compared to controls (MD: −10.53 cm3; 95% CI: −18.23 to −2.82; n = 2; 120 participants; I2: 0%) (Figure 6). No differences were found on any side of the Superior temporal plane (STP) (left side MD: −0.37 cm3; −1.78 to 1.04; n = 2; 143 participants; I2: 66%. Right side MD: 0.20 cm3; 95% CI: −0.21 to 0.60; n = 2; 143 participants; I2: 0%) (Supplementary Figures 9, 10).

Figure 6. Forest plot for temporal lobe volume (cm3).
The cleft group had significantly smaller occipital lobes compared to controls (MD: −7.39 cm3; 95% CI: −12.80 to −1.99; n = 2; 120 participants; I2: 0%) (Figure 7).

Figure 7. Forest plot for occipital lobe volume (cm3).
Tables 3, 4 summarize studies that were not included in the meta-analyses due to the variability in either methods or outcome.
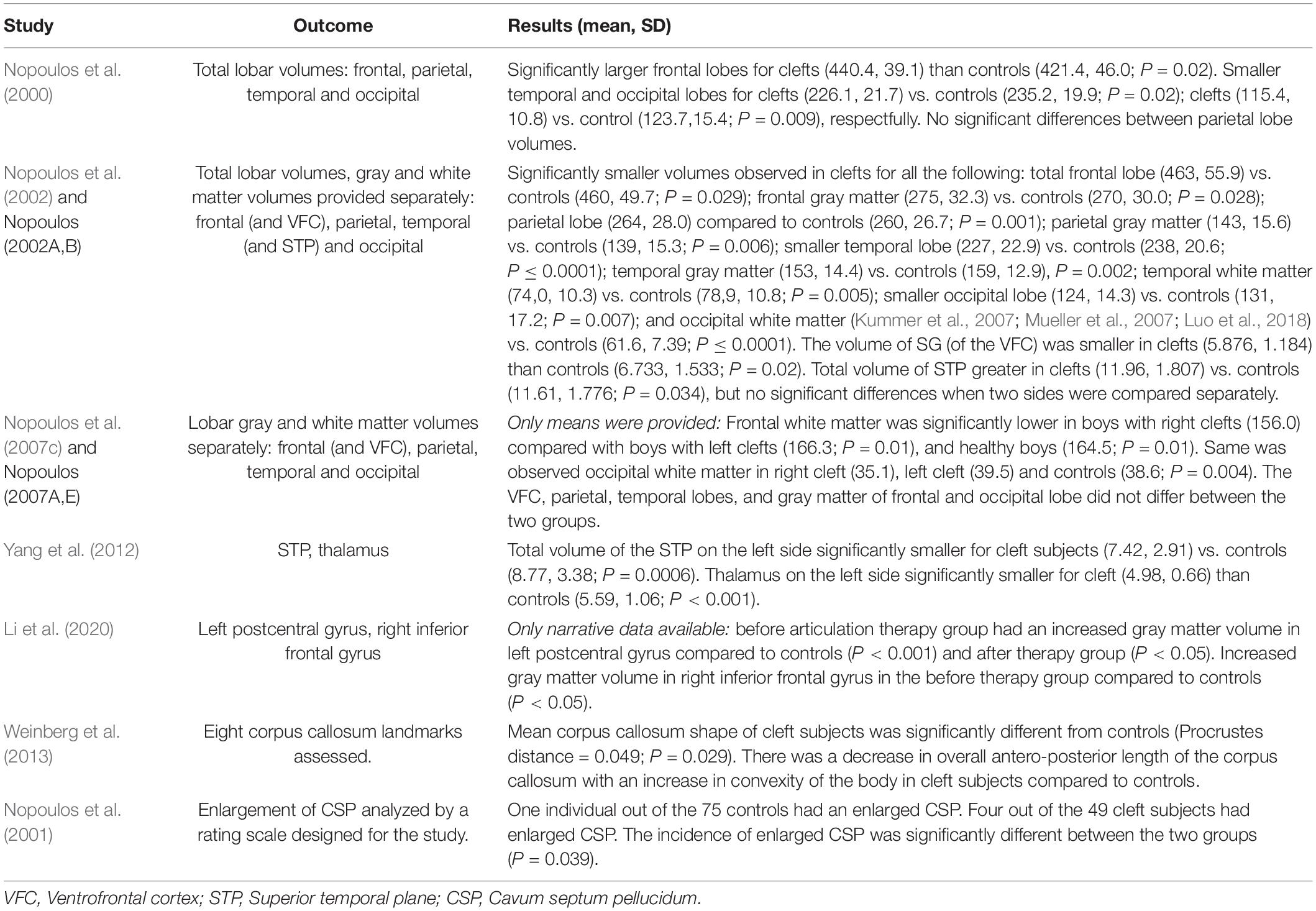
Table 3. Regional measurements.
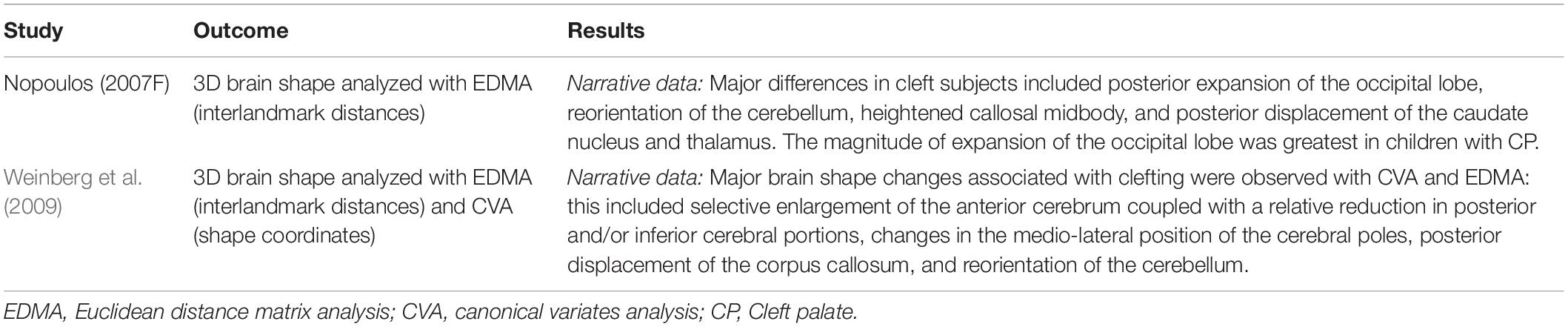
Table 4. 3D morphometric analysis of brain shape.
Heterogeneity of methods and outcomes prevented statistical pooling for meta-analyses for most secondary outcomes, with the exception of IQ scores. These secondary outcomes are illustrated in Table 5.
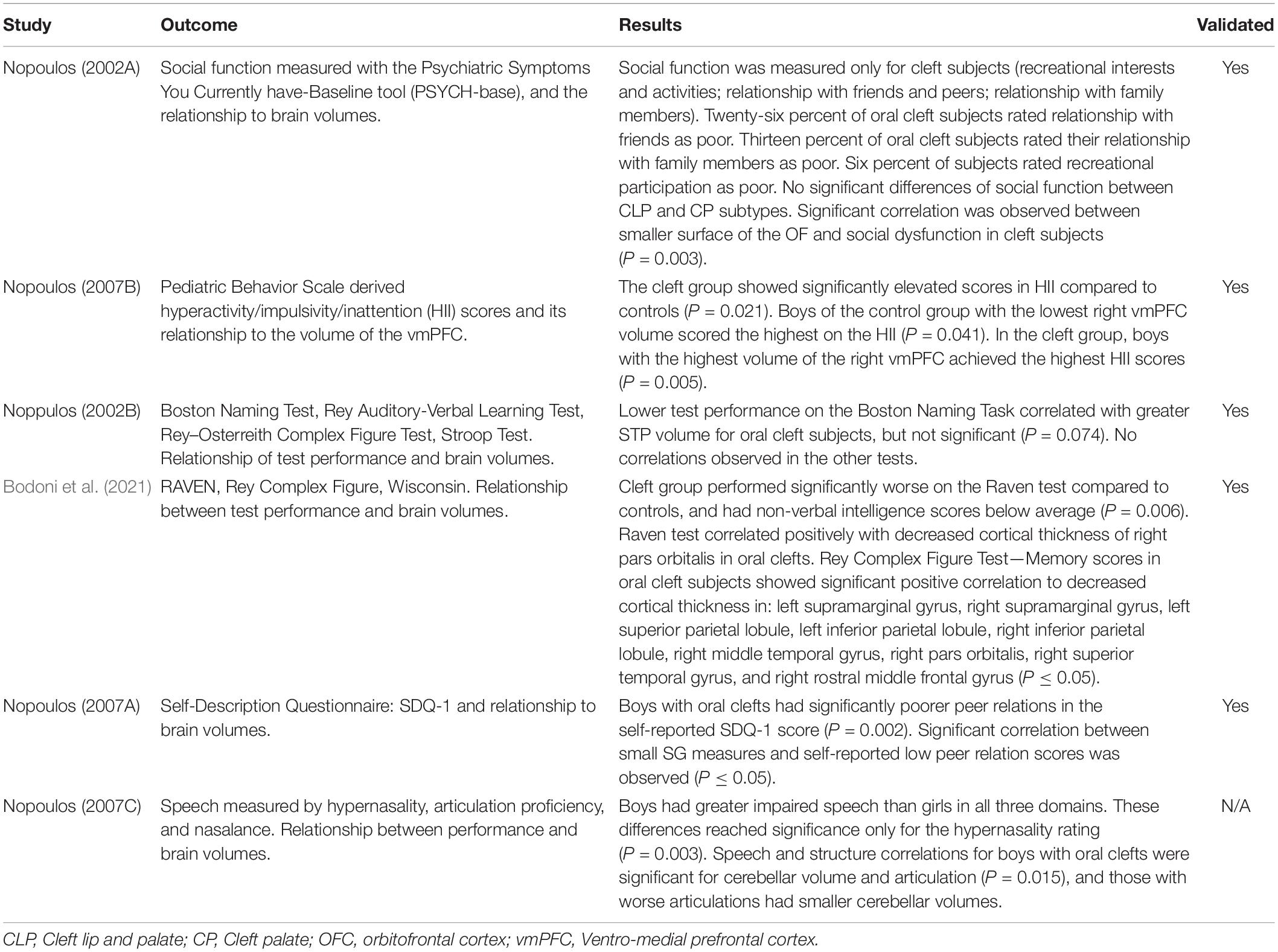
Table 5. Psychometric tools used to measure psychosocial functioning.
Significantly lower FSIQ scores were as observed in individuals with oral clefts compared to controls (MD: −12.58; FSIQ; 95% CI: −21.98 to -3.17; n = 2; 234 participants; I2 = 84%) (Figure 8). All of the studies used the Wechsler Intelligence Scale of different editions.

Figure 8. Forest plot for full-scale IQ scores.
Four meta-analyses demonstrated moderate to considerable levels of heterogeneity. Subgroup analysis was feasible for only two of the four meta-analyses (Figures 3, 4). Subgroup analyses were performed for age, sex, ethnicity, non-syndromic, and mixed (syndromic and non-syndromic) oral clefts.
The non-syndromic subgroup had significantly smaller total brain volume compared to controls. However, this significant difference was not seen in the mixed subgroup (syndromic and non-syndromic cases) (MD: −77.06 cm3; 95% CI: −115.47 to −38.64; n = 2; 202 participants; I2 = 0%; Figure 3). The same phenomenon was observed for age (children vs. adults), sex (male only vs. mixed) and ethnicity (Caucasian vs. mixed) (Supplementary Figures 11A–C). These factors may be possible sources of the heterogeneity seen in the main analysis.
A decrease in heterogeneity was found in the subgroup analysis of mixed oral clefts (MD: −0.80 cm3; 95%CI: −40.88 to 39.29; n = 2; 120 participants; I2 = 0%; Figure 4). The same phenomenon was observed for age (children vs. adults) and sex (male vs. male and female) (Supplementary Figures 12A,B).
Tests for funnel plot asymmetry could not be used to detect reporting bias due to the few studies included in the meta-analysis (n ≤ 10) (Higgins et al., 2019).
The aim of this review was to analyze the empirical evidence of the association between non-syndromic oral clefts and the brain. Overall, oral cleft subjects had smaller cerebral gray matter, cerebellum, temporal lobes, and occipital lobes compared to controls. Individuals with oral clefts had lower FSIQ scores compared to matched controls. Most of the studies controlled for confounders such as age and/or sex to control for brain growth and development; however, only half of the studies for subjects and/or parent’s sociodemographic level (Nopoulos et al., 2000, 2002, 2007c; Li et al., 2020; Bodoni et al., 2021). The risk of bias for the included studies was moderate to high. Most included studies did not analyze cleft subtypes separately which was likely due to the small sample size across subgroups.
Some effects of oral clefts may have remained hidden as a consequence to the small number of studies for most outcomes. A few studies have included syndromic cases of oral cleft, notably Van der Woude syndrome. Van der Woude is a dominantly inherited syndrome caused by the deletion of a gene encoding the interferon regulatory factor-6 (IRF6) on chromosome 1q32 (Johns Hopkins University, 2022). The authors state that the oral cleft occurs in an isolated matter without any other significant developmental issues and allow these individuals to be a part of the non-syndromic group. However, there have been documented cases of cognitive deficits and brain structural abnormalities of Van der Woude syndrome (Nopoulos et al., 2007a; Rincic et al., 2016). Including individuals with Van der Woude syndrome may have an impact on the results of the non-syndromic cleft population.
The total gray matter volume was significantly smaller in the cleft group, an interesting outcome as the total brain and cerebral volume did not significantly differ between the two groups. We hypothesize the following to explain this observation: (1) Shifts in brain tissue distribution in individuals with non-syndromic oral clefts have been shown previously (Nopoulos et al., 2007c). This phenomenon was suggested to occur due to a “compensatory overgrowth” of either brain tissue component unaffecting total brain size (Nopoulos et al., 2002). The cerebellum was significantly smaller in the cleft group; however, the gray or white matter volumes of the cerebellum could not be analyzed separately due to the lack of data in studies. This may indicate the presence of a smaller cerebellar cortex in the oral cleft group (i.e., gray matter), a difference which may not affect the overall tissue size of the “compensated” brain. (2) Subgroup analysis revealed a significantly smaller brain and cerebrum in studies with exclusively non-syndromic oral cleft participants. These differences were not observed in studies with mixed syndromic participants (Figures 3, 4). Total brain gray matter volume was analyzed in studies with non-syndromic individuals exclusively (Figure 2). Non-syndromic oral clefts may have smaller total brain and cerebrum, but the presence of syndromic individuals might have influenced this outcome.
There is supportive evidence regarding a primary unified maldevelopment of the brain during clefting; this might be an underlying etiology for the high risk of neuropsychiatric and neurodevelopmental issues seen in this patient population (Ansen-Wilson et al., 2018). Previous systematic reviews have shown an increased risk of neurodevelopmental and academic difficulties in individuals with non-syndromic oral clefts (Hunt et al., 2005; Al-Namankany and Alhubaishi, 2018; Gallagher and Collett, 2019). These studies, however, highlight the difficulty of summarizing the available evidence due to the lack of uniformity and consistency across studies. It has been proposed that syndromes and additional conditions related to the cleft should be analyzed in a separate group in order to observe if the additional condition is of any way a confounding variable affecting cognitive functioning (Feragen et al., 2014). Future studies should consider the assessment of brain structural data in reference to the subtype of oral clefts, the side affected, additional congenital malformations or comorbidities, anamnestic data on neurodevelopment, age and gender.
Our study has several important limitations. The majority of participants were Caucasian and originated from one register (University of Iowa Cleft Lip and Palate Registry). The clinic-based recruitment and the absence of blinding during the MRI procedures may have introduced bias. Most studies did not report participation rate or investigate the differences between participants and dropouts. We could not analyze structural brain differences across the subtypes of oral cleft and gender due to the small sample sizes. It was not possible to isolate data of the syndromic cases from the overall data of respective studies. Furthermore, the impact of surgical interventions on the developing brain could not be analyzed due to lack of data regarding the timing of the surgery, age of the patient, type of cleft repair surgery and anesthesia exposure. Only one study included the cleft repair status of its participants (Yang et al., 2012). Demographic factors, such as age and/or sex of the participants were provided by most of the included studies; however, there was a lack of detailed information of parental socio-economic factors including education and financial backgrounds. Parental socio-economic factors are known to strongly relate to the child’s neurodevelopment (Noble et al., 2015; Rakesh and Whittle, 2021) and may be a crucial factor in the developing brain of children with oral clefts. It is unclear how brain structural differences affect psychosocial functioning due to the variable assessment tools used in the included studies.
The meta-analyses combined data across studies in order to estimate the effect of oral clefts on brain structure. The main limitations of these meta-analyses are the incomplete reporting of study designs and the variable definition of the patient population across the studies. The interpretation and synthesis of the included studies may have been influenced by these factors. Applicability of our results may be affected due to the limited data for certain subgroups, such as cleft type and gender.
The current review has a number of strengths. To the best of our knowledge, this is the first study to have assessed the overall empirical evidence of brain imaging studies in oral clefts carried out for over two decades. We were able to highlight possible sources of heterogeneity including sex, ethnicity, age and syndromic cases of oral clefts.
There may be structural brain differences between individuals with non-syndromic oral clefts and controls based on the available evidence. Structural brain MRI studies may provide evidence on how the type and degree of clefting plays a role with later cognitive development and functioning. Improvement in study design, size, methodology, and participant selection may allow a more thorough analysis and decrease study heterogeneity. Future studies may greatly benefit the clinical field in establishing timely therapeutic interventions for the necessary cognitive domains as a part of the complex therapy applied to these patients.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
KS-B: review design, protocol drafting, search strategy, screening against eligibility criteria, data extraction, data analysis and interpretation, risk of bias assessment, and manuscript drafting. AS: data extraction, data analysis, risk of bias assessment, and manuscript drafting. EV: screening against eligibility criteria, data extraction, and data analysis. GC: search strategy, protocol drafting, data interpretation, and manuscript drafting. GA: review design, protocol drafting, screening against eligibility criteria, data extraction, data analysis, and interpretation. SL: review design, protocol drafting, search strategy, duplicate removals, data analysis and interpretation, risk of bias assessment, and manuscript drafting. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnana.2022.863900/full#supplementary-material
Adamson, C. L., Anderson, V. A., Nopoulos, P., Seal, M. L., and Da Costa, A. C. (2014). Regional brain morphometric characteristics of nonsyndromic cleft lip and palate. Dev. Neurosci. 36, 490–498. doi: 10.1159/000365389
Al-Namankany, A., and Alhubaishi, A. (2018). Effects of cleft lip and palate on children’s psychological health: a systematic review. J. Taibah. Univ. Med. Sci. 13, 311–318. doi: 10.1016/j.jtumed.2018.04.007
Ansen-Wilson, L. J., Everson, J. L., Fink, D. M., Kietzman, H. W., Sullivan, R., and Lipinski, R. J. (2018). Common basis for orofacial clefting and cortical interneuronopathy. Transl. Psychiatry 8:8. doi: 10.1038/s41398-017-0057-7
Becker, D. B., Coalson, R. S., Sachanandani, N. S., Fair, D., Lugar, H. M., Kirchner, L. E., et al. (2008). Functional neuroanatomy of lexical processing in children with cleft lip and palate. Plast. Reconstr. Surg. 122, 1371–1382. doi: 10.1097/PRS.0b013e3181881f54
Bjørnland, T., Nørholt, S. E., Rasmusson, L., and Sándor, G. K. (2021). Nordic Textbook of Oral and Maxillofacial Surgery Munksgaard. Available online at: https://books.google.hu/books?id=aR1rzgEACAAJ (accessed January 26, 2022).
Boes, A. D., Murko, V., Wood, J. L., Langbehn, D. R., Canady, J., Richman, L., et al. (2007). Social function in boys with cleft lip and palate: relationship to ventral frontal cortex morphology. Behav. Brain Res. 181, 224–231. doi: 10.1016/j.bbr.2007.04.009
Bodoni, P. S. B., Leoni, R. F., do Vale, A. B., da Silva, P. H. R., Meira Junior, S. G., Richieri Costa, A., et al. (2021). Neuropsychological functioning and its relationship with brain anatomical measures of children and adolescents with non-syndromic cleft lip and palate. Child Neuropsychol. 27, 2–16. doi: 10.1080/09297049.2020.1776240
Broder, H. L., Richman, L. C., and Matheson, P. B. (1998). Learning disability, school achievement, and grade retention among children with cleft: a two-center study. Cleft Palate Craniofac. J. 35, 127–131. doi: 10.1597/1545-15691998035<0127:LDSAAG<2.3.CO;2
Čeponiene, R., Hukki, J., Cheour, M., Haapanen, M. L., Ranta, R., and Näätänen, R. (1999). Cortical auditory dysfunction in children with oral clefts: relation with cleft type. Clin. Neurophysiol. 110, 1921–1926.
Chollet, M. B., Nopoulos, P., Conrad, A., and DeLeon, V. (2010). Brain morphology of children with cleft lip and/or palate. FASEB J. 24, 1369–1370.
Chollet, M. B., DeLeon, V. B., Conrad, A. L., and Nopoulos, P. (2014). Morphometric analysis of brain shape in children with nonsyndromic cleft lip and/or palate. J. Child Neurol. 29, 1616–1625. doi: 10.1177/0883073813510603
Cochrane (2020). Review Manager (RevMan) [Computer program]. Version 5.4. London: The Cochrane Collaboration.
Conrad, A. L., Canady, J., Richman, L., and Nopoulos, P. (2008). Incidence of neurological soft signs in children with isolated cleft of the lip or palate. Percept. Mot. Skills 106, 197–206. doi: 10.2466/pms.106.1.197-206
Conrad, A. L., Dailey, S., Richman, L., Canady, J., Karnell, M. P., Axelson, E., et al. (2010). Cerebellum structure differences and relationship to speech in boys and girls with nonsyndromic cleft of the lip and/or palate. Cleft Palate Craniofac. J. 47, 469–475. doi: 10.1597/08-228
Conrad, A. L., Wermke, K., Eisenmann, M., Kuhlmann, E., Benavides, A., Koscik, T., et al. (2021). Preliminary evaluation of pre-speech and neurodevelopmental measures in 7–11-week-old infants with isolated oral clefts. Pediatr. Res. 89, 85–90. doi: 10.1038/s41390-020-0887-5
DeVolder, I., Conrad, A., Magnotta, V., and Nopoulos, P. (2015). Difficulties in timing perception related to abnormal brain structure in children and adolescents with nonsyndromic cleft lip and/or cleft palate. Cleft Palate Craniofac. J. 52:e110.
DeVolder, I., Conrad, A., Richman, L., Magnotta, V., and Nopoulos, P. C. (2014). White matter structure in individuals with isolated cleft lip and/or palate: a diffusion tensor imaging study. Cleft Palate Craniofac. J. 51.
DeVolder, I., Richman, L., Conrad, A. L., Magnotta, V., and Nopoulos, P. (2013). Abnormal cerebellar structure is dependent on phenotype of isolated cleft of the lip and/or palate. Cerebellum 12, 236–244. doi: 10.1007/s12311-012-0418-y
Diaz-Stransky, A., and Tierney, E. (2012). Cognitive and behavioral aspects of Smith-Lemli-Opitz syndrome. Am. J. Med. Genet. Part C Semin. Med. Genet. 160C, 295–300. doi: 10.1002/ajmg.c.31342
Feragen, K. B., Stock, N. M., and Rumsey, N. (2014). Toward a reconsideration of inclusion and exclusion criteria in cleft lip and palate: implications for psychological research. Cleft Palate Craniofac. J. 51, 569–578. doi: 10.1597/12-326
Gallagher, E. R., and Collett, B. R. (2019). Neurodevelopmental and academic outcomes in children with orofacial clefts: a systematic review. Pediatrics 144:e20184027. doi: 10.1542/peds.2018-4027
Hardin-Jones, M., and Chapman, K. (2011). Cognitive and language issues associated with cleft lip and palate. Semin. Speech Lang. 32, 127–140. doi: 10.1055/s-0031-1277715
Higgins, J. P. T., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M. J., et al. (2019). “Cochrane handbook for systematic reviews of interventions,” in Cochrane Handbook for Systematic Reviews of Interventions, eds J. P. T. Higgins, J. Thomas, J. Chandler, M. Cumpston, T. Li, M. J. Page, et al. (Hoboken, NJ: Wiley).
Hunt, O., Burden, D., Hepper, P., and Johnston, C. (2005). The psychosocial effects of cleft lip and palate: a systematic review. Eur. J. Orthod. 27, 274–285. doi: 10.1093/ejo/cji004
Johns Hopkins University (2022). Online Mendelian Inheritance in Man, OMIM. Baltimore, MD: Johns Hopkins University.
Kummer, A. W., Lee, L., Stutz, L. S., Maroney, A., and Brandt, J. W. (2007). The prevalence of apraxia characteristics in patients with velocardiofacial syndrome as compared with other cleft populations. Cleft Palate Craniofac. J. 44, 175–181. doi: 10.1597/05-170.1
Li, Z., Zhang, W., Li, C., Wang, M., Wang, S., Chen, R., et al. (2020). Articulation rehabilitation induces cortical plasticity in adults with non-syndromic cleft lip and palate. Aging (Albany NY) 12, 13147–13159. doi: 10.18632/aging.103402
Lithovius, R. H., Ylikontiola, L. P., Harila, V., and Sándor, G. K. (2014). A descriptive epidemiology study of cleft lip and palate in Northern Finland. Acta Odontol. Scand. 72, 372–375. doi: 10.3109/00016357.2013.840737
Luo, D., Wan, X., Liu, J., and Tong, T. (2018). Optimally estimating the sample mean from the sample size, median, mid-range, and/or mid-quartile range. Stat. Methods Med. Res. 27, 1785–1805. doi: 10.1177/0962280216669183
McDonald-McGinn, D. M., Sullivan, K. E., Marino, B., Philip, N., Swillen, A., Vorstman, J. A. S., et al. (2015). 22q11.2 deletion syndrome. Nat. Rev. Dis. Prim. 1:15071.
Mossey, P. A., and Modell, B. (2012). “Epidemiology of oral clefts 2012: an international perspective,” in Cleft Lip and Palate: Epidemiology, Aetiology and Treatment, ed. M. T. Cobourne (Basel: S. Karger AG), 1–18. doi: 10.1159/000337464
Mueller, A. A., Sader, R., Honigmann, K., Zeilhofer, H. F., and Schwenzer-Zimmerer, K. (2007). Central nervous malformations in presence of clefts reflect developmental interplay. Int. J. Oral Maxillofac. Surg. 36, 289–295. doi: 10.1016/j.ijom.2006.10.018
Muka, T., Glisic, M., Milic, J., Verhoog, S., Bohlius, J., Bramer, W., et al. (2020). A 24-step guide on how to design, conduct, and successfully publish a systematic review and meta-analysis in medical research. Eur. J. Epidemiol. 35, 49–60. doi: 10.1007/s10654-019-00576-5
Noble, K. G., Houston, S. M., Brito, N. H., Bartsch, H., Kan, E., Kuperman, J. M., et al. (2015). Family income, parental education and brain structure in children and adolescents. Nat. Neurosci. 18, 773–778. doi: 10.1038/nn.3983
Nopoulos, P., Berg, S., Canady, J., Richman, L., Van Demark, D., and Andreasen, N. C. (2000). Abnormal brain morphology in patients with isolated cleft lip, cleft palate, or both: a preliminary analysis. Cleft Palate Craniofac. J. 37, 441–446. doi: 10.1597/1545-15692000037<0441:ABMIPW<2.0.CO;2
Nopoulos, P., Berg, S., Canady, J., Richman, L., Van Demark, D., and Andreasen, N. C. (2002). Structural brain abnormalities in adult males with clefts of the lip and/or palate. Genet. Med. 4, 1–9. doi: 10.1097/00125817-200201000-00001
Nopoulos, P., Boes, A. D., Jabines, A., Conrad, A. L., Canady, J., Richman, L., et al. (2010). Hyperactivity, impulsivity, and inattention in boys with cleft lip and palate: relationship to ventromedial prefrontal cortex morphology. J. Neurodev. Disord. 2, 235–242. doi: 10.1007/s11689-010-9060-5
Nopoulos, P., Choe, I., Berg, S., Van Demark, D., Canady, J., and Richman, L. (2005). Ventral frontal cortex morphology in adult males with isolated orofacial clefts: relationship to abnormalities in social function. Cleft Palate Craniofac. J. 42, 138–144. doi: 10.1597/03-112.1
Nopoulos, P., Richman, L., Andreasen, N., Murray, J., and Schutte, B. (2007a). Abnormal brain structure in adults with Van der Woude syndrome. Clin. Genet. 71, 511–517. doi: 10.1111/j.1399-0004.2007.00799.x
Nopoulos, P., Richman, L., Andreasen, N., Murray, J. C., and Schutte, B. (2007b). Cognitive dysfunction in adults with Van der Woude syndrome. Genet. Med. 9, 213–218. doi: 10.1097/GIM.0b013e3180335abd
Nopoulos, P., Langbehn, D. R., Canady, J., Magnotta, V., and Richman, L. (2007c). Abnormal brain structure in children with isolated clefts of the lip or palate. Arch. Pediatr. Adolesc. Med. 161, 753. doi: 10.1001/archpedi.161.8.753
Nopoulos, P., Berg, S., VanDemark, D., Richman, L., Canady, J., and Andreasen, N. C. (2001). Increased incidence of a midline brain anomaly in patients with nonsyndromic clefts of the lip and/or palate. J. Neuroimaging 11, 418–424. doi: 10.1111/j.1552-6569.2001.tb00072.x
Ornoy, A. (2020). Craniofacial malformations and their association with brain development: the importance of a multidisciplinary approach for treatment. Odontology 108, 1–15. doi: 10.1007/s10266-019-00433-7
Page, M. J., McKenzie, J. E., Bossuyt, P. M., Boutron, I., Hoffmann, T. C., Mulrow, C. D., et al. (2021). The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 372:n71. doi: 10.1136/bmj.n71
Pedersen, D. A., Wehby, G. L., Murray, J. C., and Christensen, K. (2016). Psychiatric diagnoses in individuals with non-syndromic oral clefts: a danish population-based cohort study Maher B, editor. PLoS One 11:e0156261. doi: 10.1371/journal.pone.0156261
Rakesh, D., and Whittle, S. (2021). Socioeconomic status and the developing brain – a systematic review of neuroimaging findings in youth. Neurosci. Biobehav. Rev. 130, 379–407. doi: 10.1016/j.neubiorev.2021.08.027
Richman, L. C., and Ryan, S. M. (2003). Do the reading disabilities of children with cleft fit into current models of developmental dyslexia? Cleft Palate Craniofac. J. 40, 154–157. doi: 10.1597/1545-1569_2003_040_0154_dtrdoc_2.0.co_2
Rincic, M., Rados, M., Krsnik, Z., Gotovac, K., Borovecki, F., Liehr, T., et al. (2016). Complex intrachromosomal rearrangement in 1q leading to 1q32.2 microdeletion: a potential role of SRGAP2 in the gyrification of cerebral cortex. Mol. Cytogenet. 9:19. doi: 10.1186/s13039-016-0221-4
Sándor-Bajusz, K., Maros, T., Olasz, L., Sándor, G., Hadzsiev, K., and Vástyán, A. (2021). The influence of genetic syndromes on the algorithm of cleft lip and palate repair – a retrospective study. Ann. Maxillofac. Surg. 11, 270–273. doi: 10.4103/ams.ams_77_21
Scott, N. M., Weinberg, S. M., Neiswanger, K., Brandon, C. A., and Marazita, M. L. (2005). Hair whorls and handedness: informative phenotypic markers in nonsyndromic cleft lip with or without cleft palate (NS CL/P) cases and their unaffected relatives. Am. J. Med. Genet. 136, 158–161. doi: 10.1002/ajmg.a.30806
Shen, E. Y., and Huang, F. Y. (1996). Cleft lip and palate associated with malformation of the central nervous system: a prospective neurosonographic study. Zhonghua Min. Guo Xiao Er Ke Yi Xue Hui Za Zhi 37, 39–44.
Shriver, A. S., Canady, J., Richman, L., Andreasen, N. C., and Nopoulos, P. (2006). Structure and function of the superior temporal plane in adult males with cleft lip and palate: pathologic enlargement with no relationship to childhood hearing deficits. J. Child Psychol. Psychiatry 47, 994–1002. doi: 10.1111/j.1469-7610.2006.01679.x
Tillman, K. K., Hakelius, M., Höijer, J., Ramklint, M., Ekselius, L., Nowinski, D., et al. (2018). Increased risk for neurodevelopmental disorders in children with orofacial clefts. J. Am. Acad. Child Adolesc. Psychiatry 57, 876–883. doi: 10.1016/j.jaac.2018.06.024
Tollefson, T. T., and Sykes, J. M. (2010). Differences in brain structure related to laterality of cleft lip. Arch. Fac. Plast. Surg. 12, 431–432. doi: 10.1001/archfacial.2010.83
van der Plas, E., Conrad, A., Canady, J., Richman, L., and Nopoulos, P. (2010). Effects of unilateral clefts on brain structure. Arch. Pediatr. Adolesc. Med. 164, 763–768. doi: 10.1001/archpediatrics.2010.123
Wan, X., Wang, W., Liu, J., and Tong, T. (2014). Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med Res Methodol. 14:135. doi: 10.1186/1471-2288-14-135
Watkins, S. E., Meyer, R. E., Aylsworth, A. S., Marcus, J. R., Allori, A. C., Pimenta, L., et al. (2018). Academic achievement among children with nonsyndromic orofacial clefts: a population-based study. Cleft Palate Craniofac. J. 55, 12–20. doi: 10.1177/1055665617718823
Wells, G., Shea, B., O’Connell, D., Peterson, J., Welch, V., Losos, M., et al. (2000). The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Ottawa, ON: Ottawa Hospital Research Institute.
Weinberg, S. M., Andreasen, N. C., and Nopoulos, P. (2009). Three-dimensional morphometric analysis of brain shape in nonsyndromic orofacial clefting. J. Anat. 214, 926–936. doi: 10.1111/j.1469-7580.2009.01084.x
Weinberg, S. M., Parsons, T. E., Fogel, M. R., Walter, C. P., Conrad, A. L., and Nopoulos, P. (2013). Corpus callosum shape is altered in individuals with nonsyndromic cleft lip and palate. Am. J. Med. Genet. A 161A, 1002–1007. doi: 10.1002/ajmg.a.35835
Yang, F. F., McPherson, B., Shu, H., Xie, N., and Xiang, K. (2012). Structural abnormalities of the central auditory pathway in infants with nonsyndromic cleft lip and/or palate. Cleft Palate Craniofac. J. 49, 137–145. doi: 10.1597/11-014
Zheng, W., Li, B., Zou, Y., and Lou, F. (2019). The prenatal diagnosis and classification of cleft palate: the role and value of magnetic resonance imaging. Eur. Radiol. 29, 5600–5606. doi: 10.1007/s00330-019-06089-9
Keywords: cleft lip, cleft palate, neurodevelopment, brain, neuroimaging
Citation: Sándor-Bajusz KA, Sadi A, Varga E, Csábi G, Antonoglou GN and Lohner S (2022) The Brain in Oral Clefting: A Systematic Review With Meta-Analyses. Front. Neuroanat. 16:863900. doi: 10.3389/fnana.2022.863900
Received: 14 February 2022; Accepted: 11 April 2022;
Published: 10 June 2022.
Edited by:
Salvador Martinez, Miguel Hernández University of Elche, SpainReviewed by:
Lana Vasung, Harvard Medical School, United StatesCopyright © 2022 Sándor-Bajusz, Sadi, Varga, Csábi, Antonoglou and Lohner. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Kinga A. Sándor-Bajusz, c2FuZG9yLmtpbmdhQHB0ZS5odQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.