 Xiaohan Wang
Xiaohan Wang Yanan Yan
Yanan Yan Yurong Liu
Yurong Liu Chun Xu
Chun Xu Jingwen Zhuang
Jingwen Zhuang Zhiping Wang
Zhiping Wang
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Aging Neurosci. , 17 March 2025
Sec. Neurocognitive Aging and Behavior
Volume 17 - 2025 | https://doi.org/10.3389/fnagi.2025.1542628
This article is part of the Research Topic Repurposing Medications: Bridging Chronic Disease Management and Dementia Prevention View all 4 articles
Objectives: To evaluate the effect of preoperative continuation vs. discontinuation of angiotensin-converting enzyme inhibitors (ACEIs) and angiotensin II receptor blockers (ARBs) on early cognitive function in elderly patients undergoing noncardiac surgery.
Methods: This prospective randomized controlled study was performed at the Affiliated Hospital of Xuzhou Medical University. Elderly patients aged 65 years or older, scheduled for elective noncardiac surgery under general anesthesia, and receiving long-term ACEI/ARBs therapy were randomly assigned to either continue or discontinue ACEI/ARBs therapy on the morning of surgery. The primary outcome was postoperative early cognitive function, assessed via neuropsychological tests including Auditory Verbal Learning Test-Huashan (AVLT-H), Clock Drawing Test (CDT), Number Connection Test (NCT), and Digit Span Test (DST) preoperatively and on postoperative day 1 (POD1). Secondary outcomes included intraoperative hypotension, use of phenylephrine, intraoperative fluid administration, incidence of hypertension, and length of hospital stay.
Results: The NCT scores in the discontinued use of ACEI/ARBs group showed a significant decline on POD1 compared to baseline (p = 0.038). Both groups exhibited an increase in immediate recall scores from preoperative to POD1 (p = 0.003 and p = 0.002, respectively). The continued use of ACEI/ARBs group showed an increase in short-delayed recall (p = 0.007). However, there were no significant differences between the two groups (p > 0.05). The discontinued ACEI/ARB group had fewer episodes of intraoperative hypotension (p = 0.037) and lower requirements for phenylephrine (p = 0.016), despite a higher incidence of preoperative hypertension (p = 0.012). The continued use group received a larger volume of crystalloid fluids during surgery (p = 0.020). No significant differences were observed between the groups in the volume of colloid fluids administered (p > 0.05). There were no significant differences in postoperative hypertension or length of hospital stay between the groups (p > 0.05).
Conclusion: Preoperative continuation or discontinuation of ACEI/ARBs did not significantly affect early postoperative cognitive function in elderly patients.
Angiotensin-converting enzyme inhibitors (ACEIs) and angiotensin II receptor blockers (ARBs) are frequently used in the treatment of hypertension and heart failure (Halvorsen et al., 2022), especially in elderly patients. These medications regulate blood pressure and fluid balance by inhibiting the renin-angiotensin-aldosterone system (RAAS) (Ksiazek et al., 2024). However, their use in elderly patients undergoing surgery has raised concerns about their potential impact on cognitive function (Halvorsen et al., 2024; Legrand, 2024). Postoperative cognitive dysfunction (POCD) is a common complication observed in older adults, associated with increased morbidity, longer hospital stays, and a higher risk of mortality (Bedford, 1955; Steinmetz and Rasmussen, 2016). POCD is typically diagnosed through neuropsychological testing (Moller et al., 1998), but its underlying mechanisms remain unclear. Possible contributing factors include neuroinflammation (Hovens et al., 2014), cerebral microembolism (Liu et al., 2009), and undetected perioperative stroke (Mrkobrada et al., 2019). As the number of elderly patients undergoing noncardiac surgery continues to rise, understanding the effects of ACEIs and ARBs on cognitive outcomes is crucial for optimizing perioperative care.
Several studies have examined the relationship between ACEIs/ARBs and cognitive function, yielding inconsistent results. Some suggest that inhibiting the RAAS may protect against cognitive decline by enhancing the memory-protective effects of the angiotensin type 4 receptor (AT4R) (Cosarderelioglu et al., 2023), improving cerebral perfusion, and reducing oxidative stress. However, other research indicates that continuing these medications before surgery may increase the risk of intraoperative hypotension (IOH) (Hollmann et al., 2018), which can impair cerebral perfusion (Krenk et al., 2010; Pappa et al., 2017). Cerebral autoregulation, a mechanism that stabilizes blood flow to the brain (Armstead, 2016), is disrupted during IOH, leading to hypoperfusion and potential ischemic injury. This can disturb brain homeostasis and contribute to postoperative cognitive dysfunction (POCD) (Wang, 2014). The conflicting findings highlight the need for further investigation into how ACEIs and ARBs affect postoperative cognitive outcomes, particularly in elderly patients who are particularly vulnerable to both surgical stress and polypharmacy.
The objective of this study is to investigate the impact of continuing vs. discontinuing ACEIs/ARBs on cognitive function in elderly patients undergoing elective noncardiac surgery. We hypothesize that continued use of these medications may impair cognitive outcomes, potentially due to their impact on blood pressure regulation. Conversely, discontinuing ACEIs/ARBs prior to surgery may reduce the risk of hypotension and its negative effects on cerebral blood flow, thereby improving cognitive outcomes. This randomized controlled trial seeks to provide clearer evidence on the role of these medications in postoperative early cognitive recovery, ultimately guiding clinical decision-making in perioperative care.
This prospective, randomized controlled trial was carried out at the Affiliated Hospital of Xuzhou Medical University, a 4150-bed tertiary university-affiliated teaching hospital in Jiangsu, China. The trial protocol received approval from the hospital's medical ethics committee (Approval Number: XYFY2024-KL529-01) and was registered with the Chinese Clinical Trials Registry (Registration Number: ChiCTR2400091763). The study adhered to the Consolidated Standards of Reporting Trials (CONSORT) guidelines. Written informed consent was obtained from all participants before their enrollment in the study.
Patients aged 65 years or older were eligible for inclusion if they were scheduled for elective noncardiac surgery under general anesthesia and had been on long-term treatment with ACEIs or ARBs for a minimum of three months prior to the surgery. These medications were taken once daily in the morning.
The exclusion criteria included pre-existing cognitive impairment assessed by Montreal Cognitive Assessment (MoCA) (scores ≤ 17 for illiterate, ≤ 20 for primary, ≤ 22 for junior high, and ≤ 24 for university), inadequate blood pressure control with antihypertensive medications, preoperative hypotension (blood pressure < 90/60 mmHg), mental or neurological disorders or history of stroke, use of neuroprotective drugs, surgeries requiring controlled hypotension (e.g., hepatectomy, rotator cuff repair), and impairments in speech, vision, or hearing.
The rejection criteria included patients diagnosed with delirium using the Confusion Assessment Method (CAM) scale one day after surgery.
Eligible patients were randomly assigned to either continue or discontinue ACEI/ARBs in a 1:1 ratio, using a computer-generated randomization system. An investigator, who was not involved in data collection, informed patients of their group assignment. A second investigator, blinded to the group assignments, recorded and assessed the data. In the continuation group, ACEI/ARBs therapy was maintained on the morning of surgery. In the discontinuation group, ACEI/ARBs therapy was stopped on the morning of surgery, with the last dose taken 1 day prior. The night before surgery, a ward nurse informed patients whether to continue or discontinue their medication. Before entering the operating room, the nurse confirmed that patients had taken their antihypertensive medications as instructed. Patients who did not adhere to the medication instructions were excluded from the trial.
Anesthetic management was standardized based on current best practices by experienced anesthesiologists, who were blinded to the patients' preoperative ACEI/ARBs continuation/discontinuation status. After the patient entered the operating room, the venous access to the elbow of the right upper limb was opened. Non-invasive blood pressure, electrocardiogram (ECG), saturation of pulse oximetry (SpO2), and bispect ral index (BIS) were routinely monitored. After local anesthesia with lidocaine, invasive blood pressure was monitored by puncture and catheterization of the radial artery under ultrasound guidance.
All patients received intravenous induction with the same drugs. General anesthesia was induced by intravenous injection of midazolam 0.05 mg/kg, sufentanil 0.5 μg/kg, etomidate 0.3 mg/kg and rocuronium 0.6 mg/kg. When BIS dropped below 60, endotracheal intubation was performed. The intubation depth was 23 cm. The endotracheal tube was connected to the breathing circuit and the volume control mode was used for mechanical ventilation. Low tidal volume was 6–8 mL/kg, respiratory rate was 12–20 times/min, inspiratory/expiratory ratio was 1:1.5, oxygen flow rate was 2 L/min, and end-tidal carbon dioxide partial pressure was maintained at 35–45 mmHg. Anesthesia was maintained with combined intravenous and inhalant anesthesia, 1–2% sevoflurane was inhaled, 0.2–0.5 μg/kg/min remifentanil and 2–6 mg/kg/h propofol were pumped intravenously, and BIS value was maintained at 40–60. If the heart rate was < 50 beats per min, atropine 0.25–0.50 mg was administered intravenously, and the dose could be repeated if necessary. Multi-mode temperature protection measures and nasopharyngeal temperature monitoring were adopted during the whole operation. Postoperative pain was controlled with an intravenous injection of 50 mg flurbiprofen axetil at the time the surgeon started the skin suture.
After the operation, the patient was transferred to the postanesthesia care unit (PACU) for close monitoring. The patient's degree of wakefulness, the smoothness of spontaneous breathing, the presence of swallowing reflexes, and the recovery of muscle strength were carefully assessed. The tube was extubated when the tidal volume was >6 mL/kg. After extubation, the patient still needs to continue to be observed in the PACU for a period of time to ensure that vital signs are stable and there are no adverse effects.
Baseline patient characteristics collected included age, sex, BMI, education level, current smoking status, comorbidities (diabetes mellitus, coronary artery disease, cancer, and history of general anesthesia), preoperative laboratory values (hemoglobin and creatinine), preoperative hemodynamic parameters (blood pressure and pulse), and preoperative cognitive assessment. Intraoperative data extracted included the type and duration of surgery, as well as the need for transfusion.
The primary outcome was postoperative early cognitive function, assessed using neuropsychological tests on postoperative day 1 (POD1). Secondary outcomes included the incidence of hypotension within 15 min of anesthesia induction (defined as a 30% decrease in systolic blood pressure from baseline or a mean arterial pressure < 55 mmHg), intraoperative phenylephrine dosage (μg/h), infusion volume (crystalloid and colloid fluids), incidence of hypertension upon admission to the operating room and within 24 h post-surgery, and length of hospital stay.
To maintain standardization and consistency in data collection, widely recognized neuropsychological tests were employed (Jannati et al., 2024; Stefanidis et al., 2025).
The Auditory Verbal Learning Test-Huashan (AVLT-H) involves the researcher reading 12 words aloud, and the patient is asked to recall as many words as possible immediately afterward. The total number of words recalled across three trials is recorded as the immediate recall score, which assesses the patient's capacity to learn new information. A short-delayed recall test is administered after a 5-min interval, and a long-delayed recall test is performed after 20 min. The short-delayed and long-delayed recall scores reflect the patient's ability to retain new information over time. Higher scores on the AVLT-H indicate better memory function.
The Clock Drawing Test (CDT) requires the patient to draw a clock on a blank piece of paper, ensuring all numbers are included. The hour and minute hands should indicate 11:10. Scoring is based on the Rouleau scale, which evaluates three components: completeness of the clock face (maximum 2 scores), correct display and order of numbers (maximum 4 scores), and proper positioning of the hands (maximum 4 scores). The CDT is a screening tool used to assess cognitive function and detect early signs of dementia. A lower total CDT score indicates worse cognitive function.
The Number Connection Test (NCT) requires the patient to connect 25 randomly arranged circles, numbered from 1 to 25, in order from smallest to largest. The time taken to complete the task is recorded. The total score reflects executive function, with a lower score indicating better executive function.
The Digit Span Test (DST) requires the patient to recite a series of numbers in either sequential or reverse order. The total score is based on the longest sequence of digits the patient can accurately recall. The DST measures memory span, with a higher score indicating a greater memory span.
Data analysis was conducted using SPSS version 25.0. Normally distributed measurement data are presented as mean ± standard deviation, while non-normally distributed data are presented as median (M) and interquartile range (IQR). Independent sample t-tests were employed to compare normally distributed data between the two groups, and the Mann-Whitney U test was used for non-normally distributed data. Categorical data are presented as counts (percentages), and group comparisons were made using the chi-square test or Fisher's exact test, as appropriate. A p-value of < 0.05 was considered statistically significant.
The immediate recall score of the AVLT-H was used as the primary endpoint for sample size calculation. Drawing from the results of a pilot study, the immediate recall score in the continued use of ACEI/ARBs group was 13.93 ± 4.01, and in the discontinued use of ACEI/ARBs group, it was 15.80 ± 3.49. With an alpha level set at 0.05 and a power of 0.80, the calculated sample size required for each group was 51. To account for a 10% dropout rate, 57 patients per group were needed, resulting in a total sample size of 114.
Between September 2024 and November 2024, a total of 120 patients were screened for eligibility. Nine patients were excluded due to the exclusion criteria, and three patients opted not to participate in the study. As a result, 108 patients were recruited and randomly assigned to either the continued use of ACEI/ARBs group (n = 54) or the discontinued use of ACEI/ARBs group (n = 54). Four patients were lost to follow-up due to surgery cancellation or unexpected ICU admission. Ultimately, 104 patients completed the neuropsychological test on POD1 and were included in the analysis of the primary outcome (Figure 1). No significant differences were observed in baseline characteristics, surgical details or preoperative cognitive assessment between the two groups (Table 1).
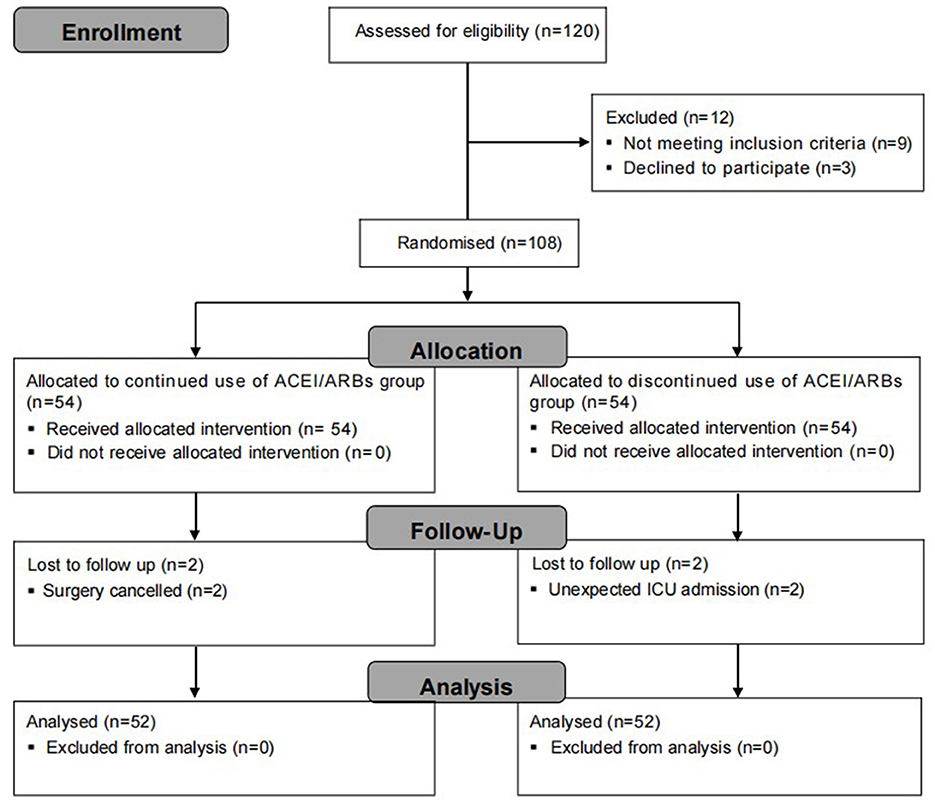
Figure 1. Flow chart of patient enrollment in this study.
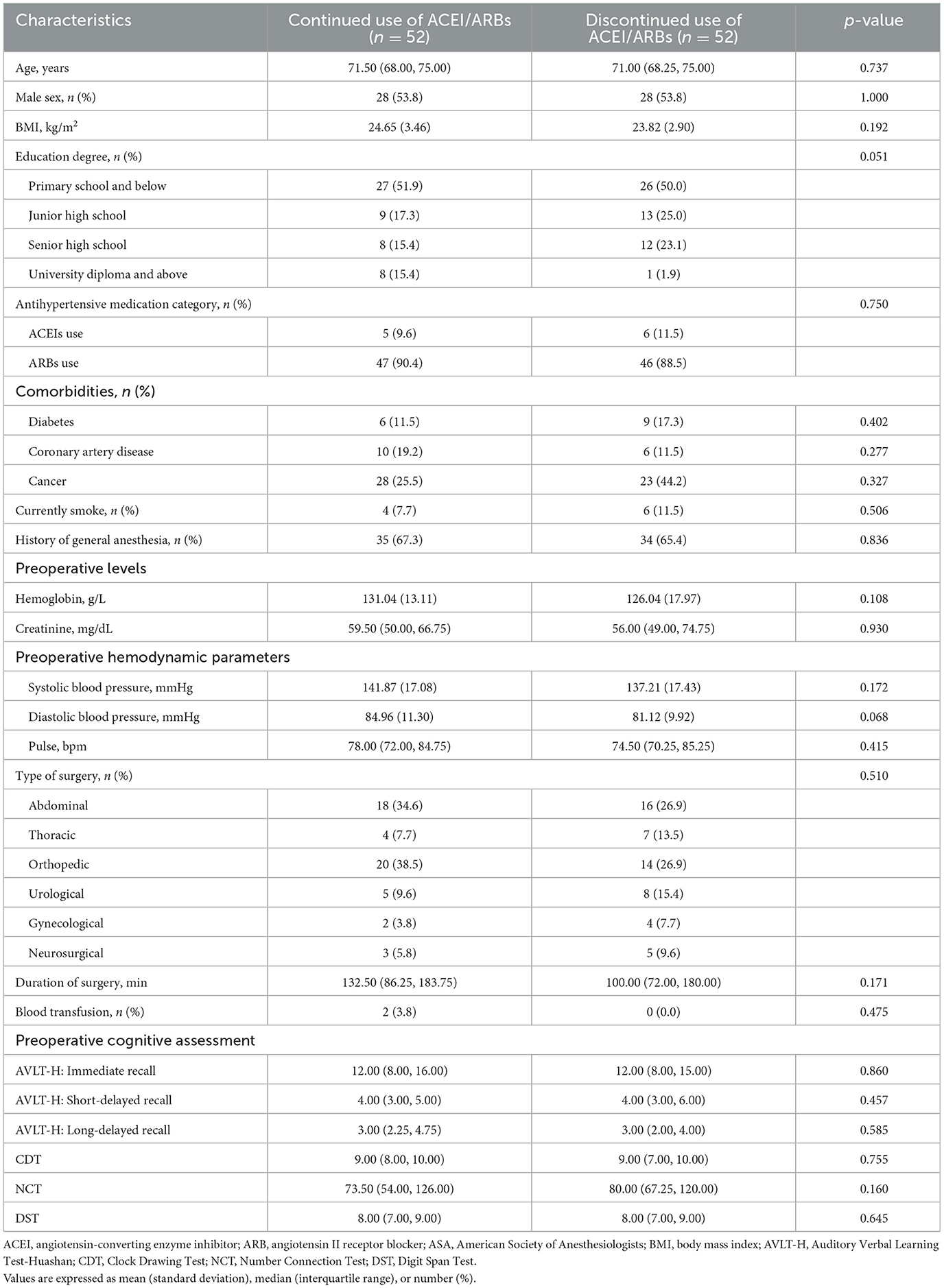
Table 1. Baseline characteristics of the patients and details of surgery.
Cognitive function, as assessed by neuropsychological tests, is summarized in Table 2. The NCT scores in the discontinued use of ACEI/ARBs group showed a significant decline on POD1 compared to baseline (p = 0.038). In contrast, both groups exhibited an increase in immediate recall scores from preoperative to POD1 (p = 0.003 and p = 0.002, respectively). The continued use of ACEI/ARBs group also showed an improvement in short-delayed recall (p = 0.007). However, no significant changes were observed in other cognitive measures, including long-delayed recall, CDT, and DST, within either group (p > 0.05).
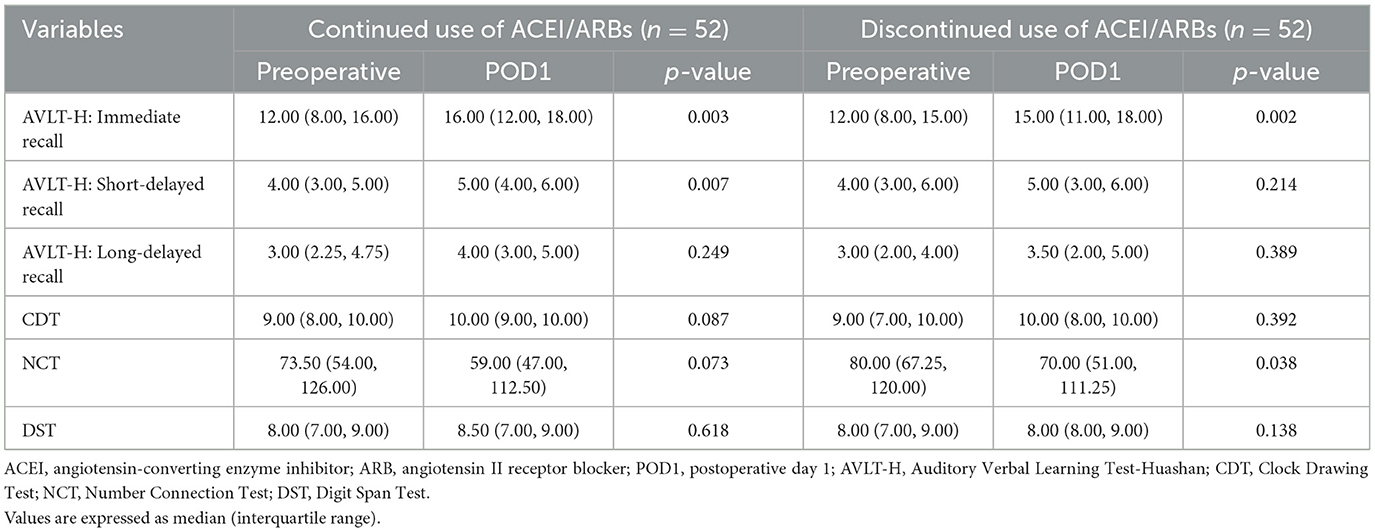
Table 2. Cognitive function assessed by neuropsychological tests.
The two groups showed no significant differences in the magnitude of decline in cognitive function, as assessed by immediate recall, short-delayed recall, long-delayed recall, CDT, NCT, and DST (Table 3).
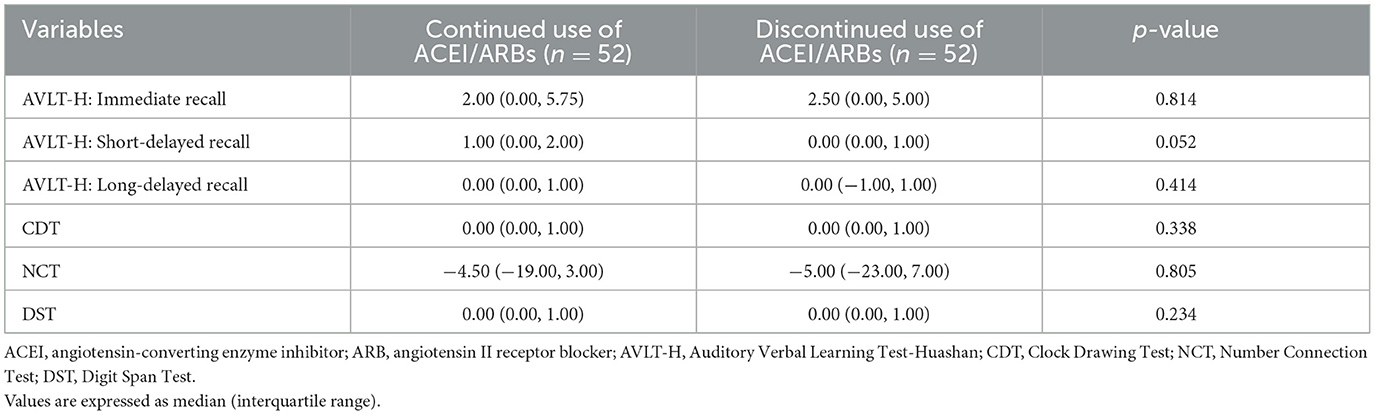
Table 3. Change in cognitive function from baseline.
The continued use of ACEI/ARBs group had a higher incidence of hypotension (42.3 vs. 23.1%, p = 0.037) and required a greater dose of phenylephrine per hour (3.73 μg/h vs. 1.29 μg/h, p = 0.016). Additionally, the continued use group received a larger volume of crystalloid fluids during surgery (1,450 vs. 1,200 mL, p = 0.020). However, no significant differences were observed between the groups in the volume of colloid fluids administered (p > 0.05). Regarding preoperative hypertension, the continued use group had a lower incidence (13.5 vs. 34.6%, p = 0.012). There were no significant differences in postoperative hypertension or length of hospital stay between the groups (Table 4).
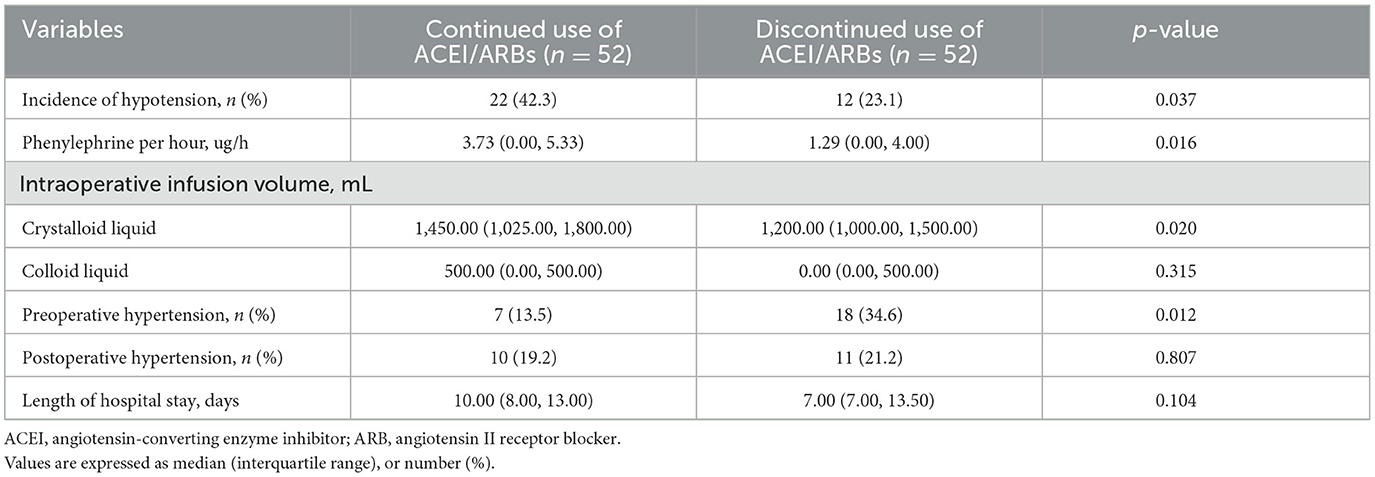
Table 4. Secondary outcomes.
The primary findings of this study suggested that both the continuation and discontinuation of ACEI/ARBs before noncardiac surgery resulted in similar cognitive outcomes, as assessed by neuropsychological tests. Both groups showed some improvements or impairments in cognitive performance, but these changes were comparable between the groups. Patients in the ACEI/ARBs discontinuation group experienced fewer episodes of intraoperative hypotension and required less phenylephrine, despite a higher incidence of preoperative hypertension. These results indicated that while discontinuing ACEI/ARBs may offer advantages in blood pressure management during surgery, it did not have a significant impact on early cognitive function compared to continuing the medications.
Our findings are consistent with some previous studies but differ in certain respects. For example, a study by Erlandson et al. (2017) found modest declines in neurocognitive performance in specific domains associated with ACEI/ARB therapy, but no consistent evidence that these medications affected global neurocognitive function. Both studies suggested that while cognitive impairments may be observed postoperatively in certain areas—such as executive function, processing speed, or verbal learning and memory—no significant differences in cognitive outcomes were observed between patients who continued or discontinued ACEI/ARB therapy.
However, in contrast to our study, a systematic review (Stuhec et al., 2017) of 15 RCTs found that ARBs may improve cognitive function in elderly patients without prior cerebrovascular disease, particularly with regard to episodic memory. ACEIs, while similarly effective in lowering blood pressure, did not appear to improve cognitive function in the elderly. These findings align with a previous network meta-analysis (Levi Marpillat et al., 2013). On the other hand, a combined meta-analysis of RCTs and observational studies (Zhuang et al., 2016) suggested that centrally acting ACEIs (CACEIs) may help prevent cognitive decline, whereas ARBs showed no such benefit. The discrepancies between studies could be due to differences in antihypertensive drug classes, the specific cognitive tests used, or perioperative factors such as intraoperative blood pressure management, which appeared to influence outcomes in our cohort. Additional research is required to better understand the effects of CACEIs, peripheral ACEIs (PACEIs), and ARBs on cognitive function.
The mechanisms through which ACEIs and ARBs may affect cognitive function are complex and multifactorial. Emerging evidence suggests that both the peripheral and central nervous systems' renin-angiotensin system (RAS) (de Miranda et al., 2024), particularly the ACE/Ang II/angiotensin II type 1 receptor (AT1R) pathway (Leong et al., 2002), play crucial roles in regulating immune responses (Bauer and Teixeira, 2021), oxidative stress, and the activation of the hypothalamic-pituitary-adrenal (HPA) axis (Belvederi Murri et al., 2016). This pathway is implicated in neuroinflammation and cognitive decline, contributing to behavioral disorders and amyloid deposition, which further exacerbate cognitive impairment (Tiwari et al., 2023). Furthermore, the difference in protective effectiveness between ARBs and ACEIs, as mentioned before, may be attributed to their diverse mechanisms of antagonism toward independent receptor pathways or their disparate impacts on amyloid metabolism.
A deeper understanding of the cellular and molecular mechanisms underlying cognitive decline could lead to the identification of novel biological targets for therapeutic intervention. These insights might also pave the way for repurposing existing medications, such as RAS modulators, for cognitive-related disorders. Scotti et al.'s (2021) meta-analysis demonstrated that the employment of AT1R blockers contributed to a significant relieve of the risk of any dementia. Therefore, inhibiting the AT1R function (Vasconcelos et al., 2021) in the brain could present a promising therapeutic strategy for treating neuropsychiatric conditions linked to altered brain immune responses and cognitive dysfunction. However, clinical trials are essential to evaluate the efficacy of these potential treatments.
Our study found that patients in the continued ACEI/ARBs group experienced a higher incidence of intraoperative hypotension and greater use of vasoactive drugs, which aligns with findings from the broader literature. For example, a multicenter randomized clinical trial (Legrand et al., 2024) involving 2,222 patients undergoing major noncardiac surgery showed that those who continued renin-angiotensin system inhibitors (RASI) preoperatively had more frequent and prolonged episodes of intraoperative hypotension. Similar results were observed in ambulatory surgery patients (Gurunathan et al., 2024), where antihypertensive use was linked to a higher frequency of early and overall hypotension compared to those not on antihypertensive medications. This finding is further supported by a meta-analysis (Ahmed et al., 2024), which concluded that withholding RAAS inhibitors before noncardiac surgery significantly reduced intraoperative hypotension and the incidence of acute kidney injury (AKI) without impacting mortality or major adverse cardiovascular events (MACE). Intraoperative hypotension (IOH) is a common complication during noncardiac surgery (Ackland and Abbott, 2022), and it is associated with severe postoperative outcomes, such as 30-day mortality, AKI, and stroke (Cai et al., 2023). Our finding of increased preoperative hypertension with ACEI/ARB discontinuation before surgery also mirrors results from the SPACE trial by Ackland et al. (2024), which reported that discontinuing RAS inhibitors in noncardiac surgery patients raised the risk of clinically significant hypertensive events. Differences across studies may arise due to variations in patient demographics, surgical types, and institutional protocols. Future studies are needed to determine the optimal medication strategy that balances the prevention of both hypotension and hypertensive events.
Several limitations in our study must be acknowledged. Firstly, our study's conclusions are limited by the relatively small sample size, which may not fully capture the variability in patient responses to ACEI/ARB discontinuation or continuation. The study also involved a single center with a predominantly homogeneous population, potentially limiting the generalizability of the findings. Secondly, although we employed standardized neuropsychological tests to assess cognitive function, these measures might not capture all aspects of cognitive change post-surgery. Thirdly, our evaluation of cognitive function was limited to the first postoperative day. Future studies should consider including longer follow-up periods, such as at 1 week, one month, or even longer, to more comprehensively assess the long-term effects of ACEI/ARBs on postoperative cognitive function. Fourthly, the study could not be blinded to the patients, as it was not feasible to conceal whether ACEI/ARBs were continued or discontinued preoperatively. Moreover, our study did not include an evaluation of preoperative sleep quality using tools like the Pittsburgh Sleep Quality Index (PSQI), which is a confounding variable for postoperative cognitive assessments. Lastly, the study did not compare the separate effects of ACEIs and ARBs, nor did it include a control group of patients not taking any antihypertensive medication.
In conclusion, preoperative continuation or discontinuation of ACEI/ARBs did not significantly impact postoperative early cognitive function in elderly patients undergoing noncardiac surgery. Patients in the ACEI/ARBs discontinuation group experienced fewer episodes of intraoperative hypotension and less need for vasoactive drugs, despite a higher incidence of preoperative hypertension. Future research should aim to explore the broader implications of ACEI/ARB management on various postoperative outcomes and delve deeper into patient-specific factors that may dictate the optimal perioperative medication strategy.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
The studies involving humans were approved by Ethics Committee of the Affiliated Hospital of Xuzhou Medical University. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
XW: Conceptualization, Investigation, Methodology, Visualization, Writing – original draft. YY: Formal analysis, Investigation, Software, Writing – original draft. YL: Data curation, Investigation, Writing – review & editing. CX: Data curation, Investigation, Writing – review & editing. JZ: Data curation, Investigation, Writing – review & editing. ZW: Conceptualization, Project administration, Supervision, Writing – review & editing.
The author(s) declare financial support was received for the research and/or publication of this article. This work was supported by Jiangsu Natural Science Foundation (Grant Number BK20221222); and Jiangsu Provincial Medical Innovation Center (Grant Number CXZX202211). The funders played no role in the study design, data collection, data analysis, data interpretation, or writing of the paper and the decision to submit it for publication.
The authors thank all of the patients for their participation in this study and also all of our colleagues at our institution for their contribution to the medical care of the patients.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The reviewer YZ declared a shared parent affiliation with the author(s) to the handling editor at the time of review.
The author(s) declare that no Gen AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Ackland, G. L., and Abbott, T. E. F. (2022). Hypotension as a marker or mediator of perioperative organ injury: a narrative review. Br. J. Anaesth. 128, 915–930. doi: 10.1016/j.bja.2022.01.012
Ackland, G. L., Patel, A., Abbott, T. E. F., Begum, S., Dias, P., Crane, D. R., et al. (2024). Discontinuation vs. continuation of renin–angiotensin system inhibition before non-cardiac surgery: the SPACE trial. Eur. Heart J. 45, 1146–1155. doi: 10.1093/eurheartj/ehad716
Ahmed, M., Fatima, E., Shafiq, A., Ahsan, A., Zulfiqar, E., Masood, F., et al. (2024). Continuation versus discontinuation of renin-angiotensin aldosterone system inhibitors before non-cardiac surgery: a systematic review and meta-analysis. J. Clin. Anesth. 99:111679. doi: 10.1016/j.jclinane.2024.111679
Armstead, W. M. (2016). Cerebral blood flow autoregulation and dysautoregulation. Anesthesiol. Clin. 34, 465–477. doi: 10.1016/j.anclin.2016.04.002
Bauer, M. E., and Teixeira, A. L. (2021). Neuroinflammation in mood disorders: role of regulatory immune cells. Neuroimmunomodulation 28, 99–107. doi: 10.1159/000515594
Bedford, P. D. (1955). Adverse cerebral effects of anæsthesia on old people. Lancet 266, 259–264. doi: 10.1016/S0140-6736(55)92689-1
Belvederi Murri, M., Prestia, D., Mondelli, V., Pariante, C., Patti, S., Olivieri, B., et al. (2016). The HPA axis in bipolar disorder: systematic review and meta-analysis. Psychoneuroendocrinology 63, 327–342. doi: 10.1016/j.psyneuen.2015.10.014
Cai, J., Tang, M., Wu, H., Yuan, J., Liang, H., Wu, X., et al. (2023). Association of intraoperative hypotension and severe postoperative complications during non-cardiac surgery in adult patients: a systematic review and meta-analysis. Heliyon 9:e15997. doi: 10.1016/j.heliyon.2023.e15997
Cosarderelioglu, C., Nidadavolu, L. S., George, C. J., Marx-Rattner, R., Powell, L., Xue, Q.-L., et al. (2023). Angiotensin receptor blocker use is associated with upregulation of the memory-protective angiotensin type 4 receptor (AT4R) in the postmortem brains of individuals without cognitive impairment. Geroscience 45, 371–384. doi: 10.1007/s11357-022-00639-8
de Miranda, A. S., Macedo, D. S., Rocha, N. P., and Teixeira, A. L. (2024). Targeting the renin-angiotensin system (RAS) for neuropsychiatric disorders. Curr. Neuropharmacol. 22, 107–122. doi: 10.2174/1570159X20666220927093815
Erlandson, K. M., Kitch, D., Wester, C. W., Kalayjian, R. C., Overton, E. T., Castillo-Mancilla, J., et al. (2017). The impact of statin and angiotensin-converting enzyme inhibitor/angiotensin receptor blocker therapy on cognitive function in adults with human immunodeficiency virus infection. Clin. Infect. Dis. 65, 2042–2049. doi: 10.1093/cid/cix645
Gurunathan, U., Roe, A., Milligan, C., Hay, K., Ravichandran, G., and Chawla, G. (2024). Preoperative renin-angiotensin system antagonists intake and blood pressure responses during ambulatory surgical procedures: a prospective cohort study. Anesth. Analg. 138, 763–774. doi: 10.1213/ANE.0000000000006728
Halvorsen, S., Mehilli, J., Cassese, S., Hall, T. S., Abdelhamid, M., Barbato, E., et al. (2022). 2022 ESC Guidelines on cardiovascular assessment and management of patients undergoing non-cardiac surgery. Eur. Heart J. 43, 3826–3924. doi: 10.1093/eurheartj/ehac270
Halvorsen, S., Vranckx, P., and van Diepen, S. (2024). Should renin–angiotensin system inhibitors be stopped or not before non-cardiac surgery? Eur. Heart J. Acute Cardiovasc. Care 13, 670–671. doi: 10.1093/ehjacc/zuae101
Hollmann, C., Fernandes, N. L., and Biccard, B. M. (2018). A systematic review of outcomes associated with withholding or continuing angiotensin-converting enzyme inhibitors and angiotensin receptor blockers before noncardiac surgery. Anesth. Analg. 127, 678–687. doi: 10.1213/ANE.0000000000002837
Hovens, I. B., Schoemaker, R. G., van der Zee, E. A., Absalom, A. R., Heineman, E., and van Leeuwen, B. L. (2014). Postoperative cognitive dysfunction: Involvement of neuroinflammation and neuronal functioning. Brain Behav. Immun. 38, 202–210. doi: 10.1016/j.bbi.2014.02.002
Jannati, A., Toro-Serey, C., Gomes-Osman, J., Banks, R., Ciesla, M., Showalter, J., et al. (2024). Digital clock and recall is superior to the mini-mental state examination for the detection of mild cognitive impairment and mild dementia. Alzheimers Res. Ther. 16:2. doi: 10.1186/s13195-023-01367-7
Krenk, L., Rasmussen, L. S., and Kehlet, H. (2010). New insights into the pathophysiology of postoperative cognitive dysfunction. Acta Anaesthesiol. Scand. 54, 951–956. doi: 10.1111/j.1399-6576.2010.02268.x
Ksiazek, S. H., Hu, L., Andò, S., Pirklbauer, M., Säemann, M. D., Ruotolo, C., et al. (2024). Renin–angiotensin–aldosterone system: from history to practice of a secular topic. Int. J. Mol. Sci. 25:4035. doi: 10.3390/ijms25074035
Legrand, M. (2024). Should renin–angiotensin system inhibitors be held prior to major surgery? Br. J. Anaesth. 132, 831–834. doi: 10.1016/j.bja.2024.03.003
Legrand, M., Falcone, J., Cholley, B., Charbonneau, H., Delaporte, A., Lemoine, A., et al. (2024). Continuation vs discontinuation of renin-angiotensin system inhibitors before major noncardiac surgery. JAMA 332:970. doi: 10.1001/jama.2024.17123
Leong, D. S., Terrón, J. A., Falcón-Neri, A., Armando, I., Ito, T., Jöhren, O., et al. (2002). Restraint stress modulates brain, pituitary and adrenal expression of angiotensin II AT(1A), AT(1B) and AT(2) receptors. Neuroendocrinology 75, 227–240. doi: 10.1159/000054714
Levi Marpillat, N., Macquin-Mavier, I., Tropeano, A.-I., Bachoud-Levi, A.-C., and Maison, P. (2013). Antihypertensive classes, cognitive decline and incidence of dementia. J. Hypertens. 31, 1073–1082. doi: 10.1097/HJH.0b013e3283603f53
Liu, Y.-H., Wang, D.-X., Li, L.-H., Wu, X.-M., Shan, G.-J., Su, Y., et al. (2009). The effects of cardiopulmonary bypass on the number of cerebral microemboli and the incidence of cognitive dysfunction after coronary artery bypass graft surgery. Anesth. Analg. 109, 1013–1022. doi: 10.1213/ane.0b013e3181aed2bb
Moller, J., Cluitmans, P., Rasmussen, L., Houx, P., Rasmussen, H., Canet, J., et al. (1998). Long-term postoperative cognitive dysfunction in the elderly: ISPOCD1 study. Lancet 351, 857–861. doi: 10.1016/S0140-6736(97)07382-0
Mrkobrada, M., Chan, M. T. V., Cowan, D., Campbell, D., Wang, C. Y., Torres, D., et al. (2019). Perioperative covert stroke in patients undergoing non-cardiac surgery (NeuroVISION): a prospective cohort study. Lancet 394, 1022–1029. doi: 10.1016/S0140-6736(19)31795-7
Pappa, M., Theodosiadis, N., Tsounis, A., and Sarafis, P. (2017). Pathogenesis and treatment of post-operative cognitive dysfunction. Electron Phys. 9, 3768–3775. doi: 10.19082/3768
Scotti, L., Bassi, L., Soranna, D., Verde, F., Silani, V., Torsello, A., et al. (2021). Association between renin-angiotensin-aldosterone system inhibitors and risk of dementia: a meta-analysis. Pharmacol. Res. 166:105515. doi: 10.1016/j.phrs.2021.105515
Stefanidis, K. B., Schiemer, C., Mieran, T., and Summers, M. J. (2025). Identifying standardised neuropsychological test measures sensitive to cannabis consumption: a systematic review. J. Affect Disord. 369, 772–781. doi: 10.1016/j.jad.2024.10.051
Steinmetz, J., and Rasmussen, L. S. (2016). Peri-operative cognitive dysfunction and protection. Anaesthesia 71, 58–63. doi: 10.1111/anae.13308
Stuhec, M., Keuschler, J., Serra-Mestres, J., and Isetta, M. (2017). Effects of different antihypertensive medication groups on cognitive function in older patients: a systematic review. Eur. Psychiatry 46, 1–15. doi: 10.1016/j.eurpsy.2017.07.015
Tiwari, V., Singh, J., Tiwari, P., Chaturvedi, S., Gupta, S., Mishra, A., et al. (2023). ACE2/ANG-(1-7)/Mas receptor axis activation prevents inflammation and improves cognitive functions in streptozotocin induced rat model of Alzheimer's disease-like phenotypes. Eur. J. Pharmacol. 946:175623. doi: 10.1016/j.ejphar.2023.175623
Vasconcelos, G. S., dos Santos Júnior, M. A., Monte, A. S., da Silva, F. E. R., de Carvalho Lima, C. N., Neto, A. B., et al. (2021). Low-dose candesartan prevents schizophrenia-like behavioral alterations in a neurodevelopmental two-hit model of schizophrenia. Prog. Neuropsychopharmacol. Biol. Psychiatry 111:110348. doi: 10.1016/j.pnpbp.2021.110348
Wang, F. (2014). Postoperative cognitive dysfunction: current developments in mechanism and prevention. Med. Sci. Monit. 20, 1908–1912. doi: 10.12659/MSM.892485
Keywords: angiotensin-converting enzyme inhibitors, angiotensin II receptor blockers, cognitive function, elderly, hypotension
Citation: Wang X, Yan Y, Liu Y, Xu C, Zhuang J and Wang Z (2025) Preoperative continuation vs. discontinuation of angiotensin-converting enzyme inhibitors/angiotensin II receptor blockers on early cognitive function in elderly patients undergoing noncardiac surgery: a randomized controlled trial. Front. Aging Neurosci. 17:1542628. doi: 10.3389/fnagi.2025.1542628
Received: 10 December 2024; Accepted: 03 March 2025;
Published: 17 March 2025.
Edited by:
Zhen Zhou, University of Tasmania, AustraliaReviewed by:
Nevena Divac, University of Belgrade, SerbiaCopyright © 2025 Wang, Yan, Liu, Xu, Zhuang and Wang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Zhiping Wang, emhwc3F4dEAxMjYuY29t
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.