
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Aging Neurosci. , 05 December 2024
Sec. Alzheimer's Disease and Related Dementias
Volume 16 - 2024 | https://doi.org/10.3389/fnagi.2024.1479926
 Eddy Roccati1*
Eddy Roccati1* Alex Kitsos1
Alex Kitsos1 Aidan David Bindoff1
Aidan David Bindoff1 Jane Elizabeth Alty1,2
Jane Elizabeth Alty1,2 Larissa Bartlett1
Larissa Bartlett1 Jessica Marie Collins1
Jessica Marie Collins1 Anna Elizabeth King1
Anna Elizabeth King1 Hannah Fair1
Hannah Fair1 Kathleen Doherty1
Kathleen Doherty1 James Clement Vickers1
James Clement Vickers1Introduction: Previous research has tended to focus on early-life education for dementia risk reduction, yet there are great gains for building cognitive reserve in mid- to later-life through educational interventions. ISLAND (Island Study Linking Ageing and Neurodegenerative Disease) Campus offered free university study to all ISLAND participants, with flexible in-person/online learning models to remove educational, socioeconomic and geographical barriers. Here the core hypothesis of ISLAND Campus was investigated: that engagement in later life education leads to improvements in modifiable risk factors for dementia, cognition and blood-based biomarkers.
Methods: ISLAND Campus participants were matched on age and gender to non-Campus participants via propensity score method, with optimal matching based on logistic regression. Participants completed online surveys on health, demographics, modifiable dementia risk factors via a customized Dementia Risk Profile (DRP) tool and provided blood samples for APOE genotyping and plasma phosphorylated-tau (p-tau). Cognition was measured online via the validated Cambridge Neuropsychological Test Automated Battery Paired Associates Learning (PAL) and Spatial Working Memory (SWM) tasks. Impact of the opt-in formal educational intervention was tested in R via ANCOVA.
Results: Total participants were 986 (intervention = 492, control = 492), mean age of 61.2 years, 73.2% female, 11.7 mean years of education and 25.0% APOE e4+. Over 4 years of follow-up, intervention participants significantly improved working memory (SWM) and their risk factor profiles as measured via the DRP (p < 0.001), indicating a significant change towards lower dementia risk. Intervention and control participants were similar on socioeconomic status, location of residence, p-tau and APOE e4 presence, however Campus participants displayed a significantly higher proportion of prior university study completion (76.0%) than controls (60.0%). Intervention participants enrolled in a variety of university degrees, the most common were Diploma of Family History (n = 103, 20.9%), Diploma of Arts (n = 74, 15.0%) and Diploma of Fine Arts (n = 52, 10.5%).
Discussion: ISLAND Campus has shown how free later-life university education was associated with improvements in modifiable dementia risk factors over time and cognition. Given opt-in intervention participants were significantly more likely to have a prior university education, later life formal educational interventions should be targeted at individuals with lower prior education.
Fewer years of education in early-life is a substantial contributor to dementia risk (Livingston et al., 2020, 2024), yet there is limited evidence for targeting mid- to later-life education in primary prevention policies (Collins et al., 2019). Single-domain interventions targeting cognitively stimulating interventions have demonstrated inconsistent results (Wolinsky et al., 2013; Ball et al., 2002), likely due to a shorter duration of intervention (weeks to months), explaining initial post-intervention benefits that were unsustainable at follow-up (Wolinsky et al., 2013; Ball et al., 2002; Kivipelto et al., 2020). Multidomain trials are typically longer in duration (up to 2 years) (Ngandu et al., 2015), however, they tend to use older cohorts (Bäckman et al., 2004) and potentially confound informal cognitive training with concomitant interventions targeting hypertension, cardiovascular health, physical activity and diet (Ngandu et al., 2015). Further, research to date has focussed mainly on formal education in childhood and early adulthood, neglecting the potential for older adults to gain neuroprotection and build cognitive reserve at a critical period in their lives, as well as the added benefit from formal education as a contributor to motivation to change lifestyle behaviors toward better brain health (Siette et al., 2023).
Educational attainment is recognized as a fundamental determinant of health (Phelan et al., 2010), and we now know that formal education is a promising autonomous and sustainable strategy to improve health in mid- to later-life (Yamashita et al., 2019). Despite the preponderance of studies investigating education in early-life, there is growing evidence that education later in life can reduce dementia risk, even for people with low educational attainment in their earlier years (Najar et al., 2019). This benefit is hypothesized to be attributable to an increase in cognitive activity that subsequently boosts an individual’s cognitive reserve, or their resistance to neuropathological insult throughout the course of ageing (Alty et al., 2023; Hill et al., 2021). Education is multifaceted, and previous research has demonstrated how lower education is linked to reduced brain volume (Gonzalez-Gomez et al., 2024), reduced connectivity (Montemurro et al., 2023) and ultimately an increased risk for dementia (Livingston et al., 2024). Given this, existing socioeconomic inequities and life course inequality are likely contributing to disparities in educational attainment (Hilal and Brayne, 2022; Walhovd et al., 2022), and subsequent brain health outcomes (Hatzenbuehler et al., 2024).
In the Australian island state of Tasmania, research has demonstrated the feasibility and efficacy of mid- to later-life formal educational interventions, both to improve cognition (Bindoff et al., 2021) and improve modifiable risk factor adherence (Bartlett et al., 2023). The Tasmanian Healthy Brain Project (THBP) was a prospective, longitudinal investigation into the impact of mid- to later-life tertiary education on cognitive decline in adults aged 50–79 years of age at baseline in 2010–2011 (Summers et al., 2013). Participants were offered subsidized educational enrolment fees, and were invited for biennial neuropsychological evaluation (Summers et al., 2013). Over 10 years, participation in the THBP’s formal tertiary educational intervention was significantly associated with improved cognitive trajectories, particularly in domains of language and verbal/episodic memory (Bindoff et al., 2021).
To build on these results, we designed a prospective longitudinal follow-up study: ‘ISLAND Campus’. ISLAND (Island Study Linking Ageing and Neurodegenerative Disease) is a longitudinal study of over 14,000 participants (Bartlett et al., 2021) that has a public health focus with the ultimate goal of reducing dementia incidence in Tasmania. Based around the model of the THBP, ISLAND Campus provided the opportunity for participants to engage in further study in a select group of courses at no cost. ISLAND Campus expanded on THBP’s foundation by removing several barriers to participation, such as being completely fee-free for participants, open to any Tasmanian over 50 years of age and offering flexible in-person/online learning models that endeavored to remove geographical and socioeconomic barriers to participation. ISLAND Campus participants also completed a battery of surveys relating to dementia risk, such as the Dementia Risk Profile (DRP), a traffic-light personalized report on individual modifiable risk factors based on WHO (2019) dementia guidelines.
Our ultimate aims with ISLAND Campus are to determine the impact of mid- to later-life university education on modifiable dementia risk behaviors, cognitive function and plasma biomarkers. ISLAND Campus will delve deeper than the THBP, by understanding the unique intentions, expectations and barriers to participation in later life education, as well as incorporating an array of covariates that may mediate this relationship, such as perceived stress, general self-efficacy and health literacy. Here we present pilot results from the ISLAND Campus sub-study. We hypothesized that those who have taken up the university level education as part of ISLAND Campus will demonstrate improvements in key measures of dementia risk compared with their non-intervention counterparts in the general ISLAND cohort; higher cognitive scores, lower plasma concentrations of p-tau 181 and lower DRP profile scores.
This longitudinal observational study included 984 participants recruited from ISLAND which began recruitment in October 2019 and was open to all people living in Tasmania over the age of 50 years (Bartlett et al., 2022). No other inclusion or exclusion criteria was set. ISLAND Campus was initially offered to all ISLAND participants in the second semester of 2020. Between June and September 2020, full fee-waiver scholarships were made available by University of Tasmania (UTAS) to study participants to undertake a full university course of their choosing. ISLAND Campus participants were recruited via email and the ISLAND Home Portal, where their status as an ISLAND participant was confirmed with UTAS’ Division of Future Students to apply the fee-free waiver. Campus was available to all ISLAND participants, regardless of geographical location, socioeconomic status or previous educational attainment. To be eligible for Campus, ISLAND participants needed to provide additional mandatory survey data in addition to the general ISLAND protocol (Bartlett et al., 2022). As of October 1, 2022, a total of 13,822 had registered interest in the main ISLAND study, of whom 1,487 participants consented to Campus and 783 were deemed eligible to receive a fee-free UTAS course. Of the 783 ISLAND participants eligible to receive a full fee waiver for their UTAS course, 596 enrolled in a course/unit from Semester 2, 2020 onwards and 492 completed a course/unit as part of the ISLAND Campus initiative. These 492 participants who completed a course/unit as part of Campus were matched with 492 who did not consent to Campus. Group differences between all ISLAND participants with available data (n = 3,249) and ISLAND Campus (n = 492) are displayed in Supplementary Table 1. Participant flow diagram in CONSORT (Moher et al., 2010) format is displayed in Supplementary Figure 1.
ISLAND surveys used in this analysis were Background Health Survey and DRP (Bartlett et al., 2022). Using pre-defined cut-offs for body mass index (BMI), physical activity, cognitive activity, alcohol consumption, diet, smoking and cardiometabolic health; the DRP calculates an individual’s risk as low (green), medium (orange) or high (red) for each domain (Roccati et al., 2023). ISLAND Campus student enrolment and completion data was provided by UTAS’ Division of Future Students. In addition to the general ISLAND surveys, participants completed several further validated psychometric surveys such as the Perceived Stress Scale (PSS) (Cohen et al., 1983), New General Self-Efficacy Scale (NGSS) (Chen et al., 2001), All Aspects of Health Literacy Scale (AAHL) (Chinn and McCarthy, 2013).
Cognitive function was longitudinally measured in 2021 and 2023 using validated tests from the Cambridge Neuropsychological Test Automated Battery (Robbins et al., 2004) (CANTAB). Two cognitive domains were assessed remotely via the online ISLAND Home Portal: Paired Associates Learning (PAL) assessed episodic memory through the learning and recall of visual information over successive trials and has been shown to be sensitive to cognitive decline in early AD (Swainson et al., 2001); Spatial Working Memory (SWM) assessed executive function, via the retention and manipulation of visuospatial information. PAL Total Errors (Adjusted) indicates the number of times a participant chose the incorrect box for a stimulus on assessment problems (PALTE), plus an adjustment for the estimated number of errors they would have made on any problems, attempts and recalls they did not reach. This measure allows performance comparisons on errors made across all participants regardless of those who terminated early versus those completing the final stage of the task. SWM Strategy indicates the number of times a participants begun a new search pattern from the same box they started with previously. If they always begun a search from the same starting point, we inferred that the participant is employing a planned strategy for finding the tokens. Therefore, a low score indicates high strategy use (1 = they always begin the search from the same box), and a high score indicates that they are beginning their searches from many different boxes. This score is calculated across assessed trials with 6 tokens or more.
All ISLAND participants were invited to provide a blood sample at in-person clinics geographically dispersed across Tasmania held throughout 2021. Participants booked in for collection via the ISLAND Home Portal and were asked to avoid exercise in the 24 h prior to their collection to prevent acute increases in circulating proteins. After providing in-person consent, blood samples were collected by trained phlebotomists via venepuncture into 2 × 8.5 mL tubes: 1 × gold serum separator tube vacutainer for serum; 1 × purple ethylenediaminetetraacetic acid vacutainer for plasma. The plasma tubes were centrifuged at 2000’g for 10 min at 4°C, and the resulting plasma aliquoted into screw-top polypropylene tubes and stored in −80°C freezers within 2 h of collection. Prior to cross-sectional p-tau 181 analysis, plasma sample aliquots were removed from −80°C storage and kept at room temperature for 1 h to thaw. Samples were then mixed by vortexing for approximately 10 s and then centrifuged at 10,000’g for 5 min at room temperature to remove particulate matter. Plasma p- tau 181 was measured using the commercially available Quanterix pTau181 Advantage V2 Single Molecule Array (Simoa) Kit (Cat no. 103714) on the Quanterix SR-X biomarker system. Briefly, the kits were removed from 4°C and allowed to warm to room temperature for 30–60 min. The resorufin-β-D-galactopyranoside (RGP) reagent was prepared by placing it on the Quanterix Plate Shaker at 800 rpm for 25 min at 35°C. The assay was performed as per manufacturer’s instructions, with the supplied calibrators and high and low control samples run in duplicate and participant plasma samples run in single. Fitted concentrations are provided, as interpolated from the calibration curve fitted by the Quanterix SR-X biomarker system software. The intraassay coefficient of variation CV for the high and low control samples were 2.65 and 4.18%, respectively.
Statistical analyses were completed in R (version 4.3.1) (R Core Team, 2023), where 2-sided p values <0.05 were considered statistically significant. Due to the potential imbalances between intervention (ISLAND Campus) and control (ISLAND non-Campus) participants, we conducted propensity score matching using the ‘matchit’ package for R (Stuart et al., 2011), a commonly used method to account for non-random group assignment in observational studies (Olmos and Govindasamy, 2015). Propensity scores are the conditional probability of assignment to a treatment condition given a set of observed covariates: e = p (z = i|χ2) (Olmos and Govindasamy, 2015). They provide a powerful method of matching an intervention group (n = 492 Campus) with a control group drawn from a pool of potential control group subjects (n = 3,249 ISLAND). ISLAND Campus participants (n = 492) were matched on age and gender to non-Campus participants (n = 492) via propensity score matching method, with optimal matching based on logistic regression. A propensity score model using age and gender was selected due to showing the best model fit (lowest Akaike Information Criterion) between control and intervention covariate distribution. Group balance hypothesis testing was conducted using χ (Collins et al., 2019) test for categorical variables and 1-way analysis of variance (ANOVA) test for continuous variables. Multiple generalized additive regression models were conducted to analyze the impact of the intervention (post-exposure ~ intervention + pre-exposure + covariates + error) on modifiable risk factors for dementia as measured by the DRP, cognition measured via CANTAB and plasma concentrations of p-tau 181. For a robust assessment of the impact of the ISLAND Campus intervention (post-exposure), models adjusted for propensity score weight (PSW) as well as baseline data (pre-exposure) and covariates for longitudinal analysis. Model assumptions were tested via ‘performance’ (Lüdecke et al., 2021), summary results prepared using ‘stargazer’ (Hlavac, 2018) packages for R. Trajectories were projected using generalized additive models with thin plate regression splines. Model 1 was unadjusted. Model 2 adjusted for age, gender and education. Model 3 adjusted for age, gender, education, baseline values and PSW. Multiple comparisons were corrected for using the Bonferroni method. To ensure our study was sufficiently powered to detect the observed effect size of the ISLAND Campus intervention, a post-hoc power analysis was conducted using the ‘pwr’ package for R (Champely et al., 2017).
All ISLAND Campus participants completed informed consent prior any data collection activity. ISLAND Campus is a core sub-study of ISLAND and has been approved by UTAS’ Health and Medical Human Research Ethics Committee (HREC H001864). All procedures were carried out in accordance with the National Health and Medical Research Council’s National Statement on Ethical Conduct in Human Research and the Declaration of Helsinki.
Out of 3,249 ISLAND participants, a total of 984 (intervention = 492, control = 492) matched via propensity score method were included in the current study (mean age of 61.1 years, 73.2% female, 11.6 mean years of education, 23.9% APOE e4+). Intervention and control participants were similar on socioeconomic status, location of residence and APOE e4 presence; however intervention participants had significantly higher prevalence of prior university study completion (76.0%) than controls (60.0%). Demographics of these participants compared with the non-Campus ISLAND participants are presented in Table 1. Intervention participants enrolled in a variety of university degrees, the most common were Diploma of Family History (n = 103, 20.8%), Diploma of Arts (n = 74, 15.0%) and Diploma of Fine Arts (n = 52, 10.6%). These diplomas are equivalent to 1 year of full-time study. A full course enrolment list is provided in Table 2.
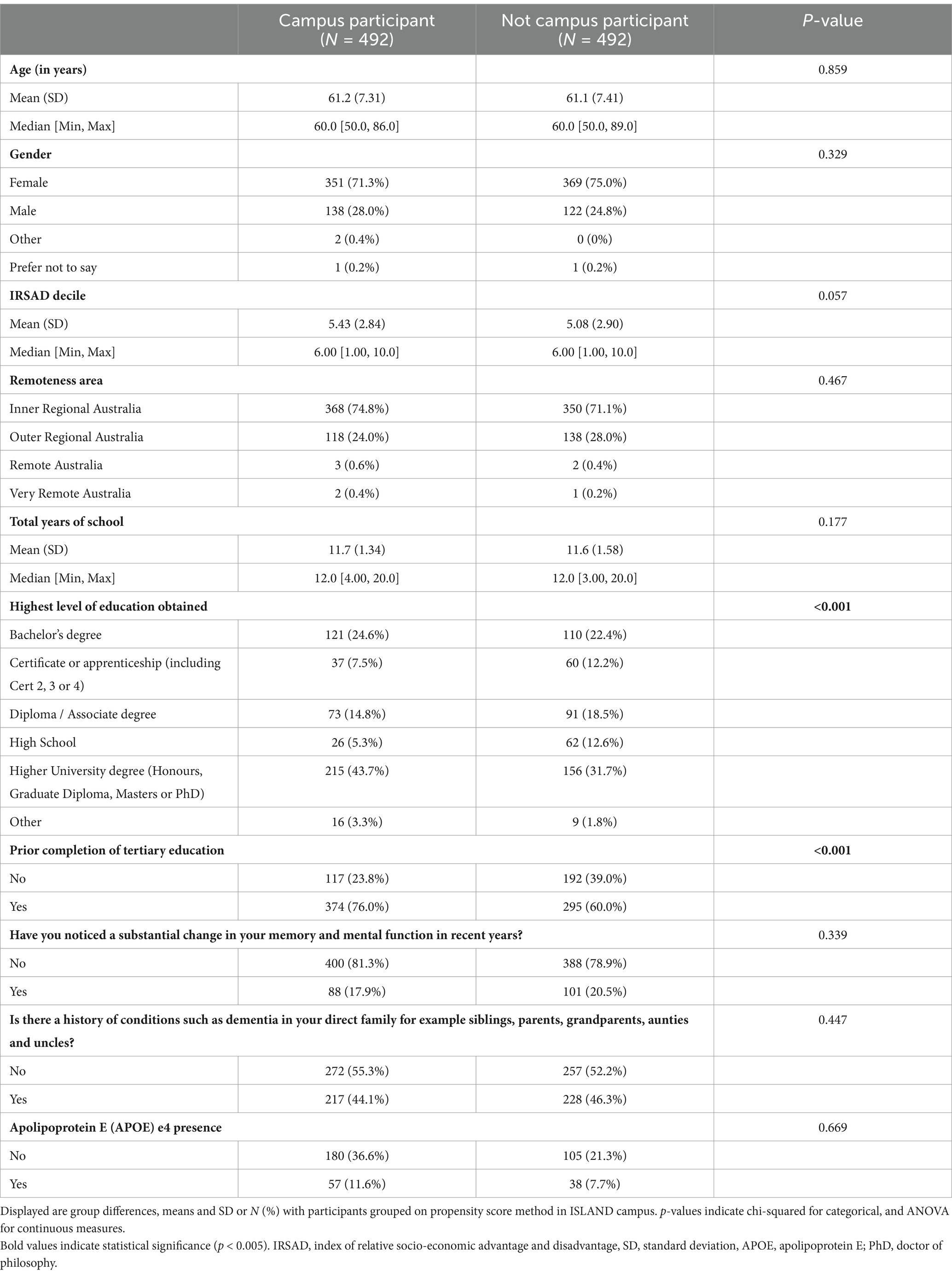
Table 1. Demographics of the cohort.

Table 2. ISLAND Campus course enrolment.
Participation in ISLAND Campus had a significantly positive impact on total DRP change, with those in the intervention group displaying greater improvements on total DRP over time (Table 3; Figure 1). This observation remained after controlling for covariates of age, gender, prior tertiary education, baseline DRP and PSW. At baseline, participants were comparable in terms of modifiable risk factors as measured by the DRP (Supplementary Table 2). At follow-up, ISLAND Campus participants displayed significantly lower BMI risk and lower cognitive activity risk compared with their non-Campus counterparts (Supplementary Table 2). Graphed longitudinally, ISLAND Campus participants showed movement toward lower total scores on total DRP (Figure 2), as well as when split into low, medium and high score categories on the DRP (Figure 3).
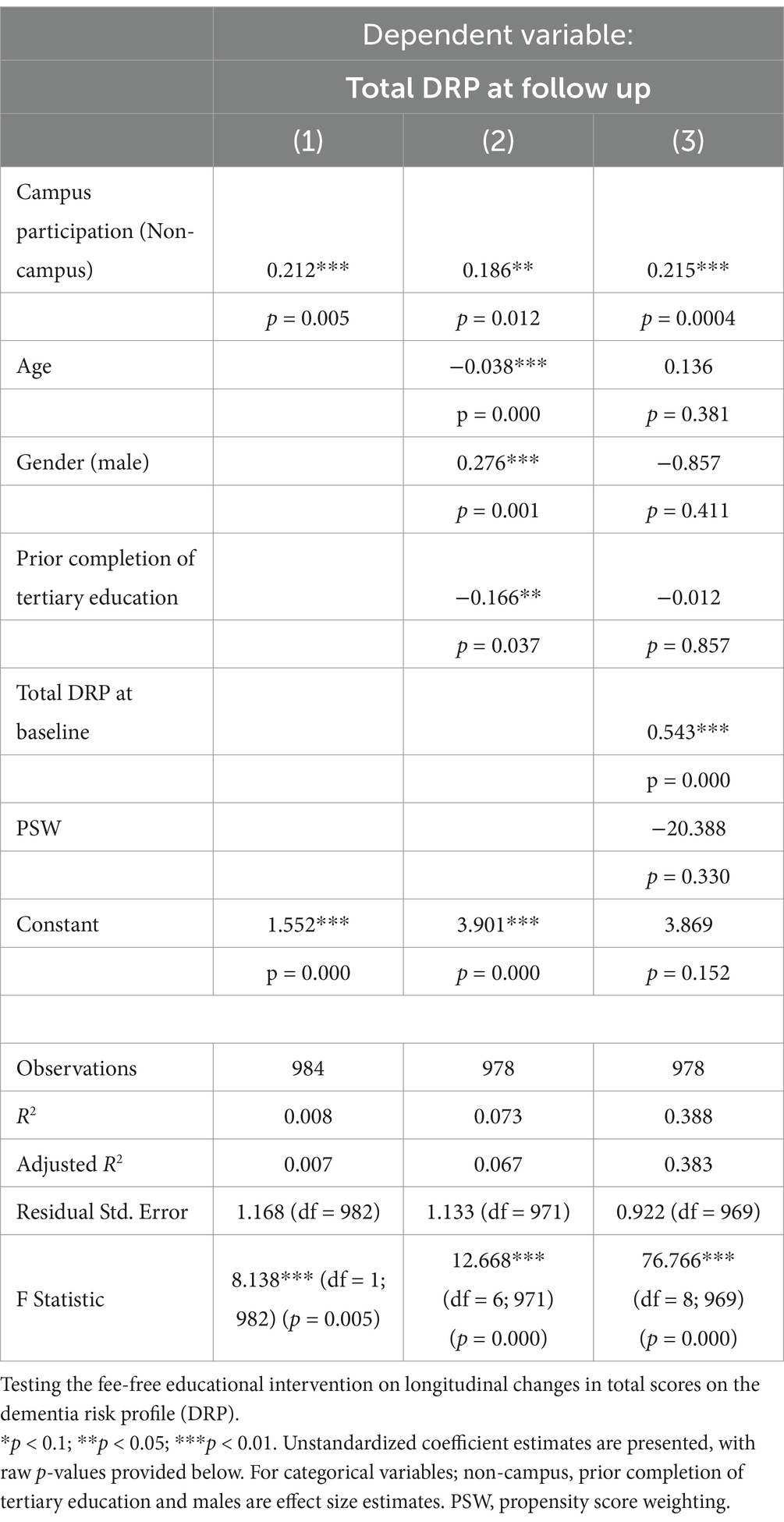
Table 3. Impact of ISLAND campus intervention on DRP.
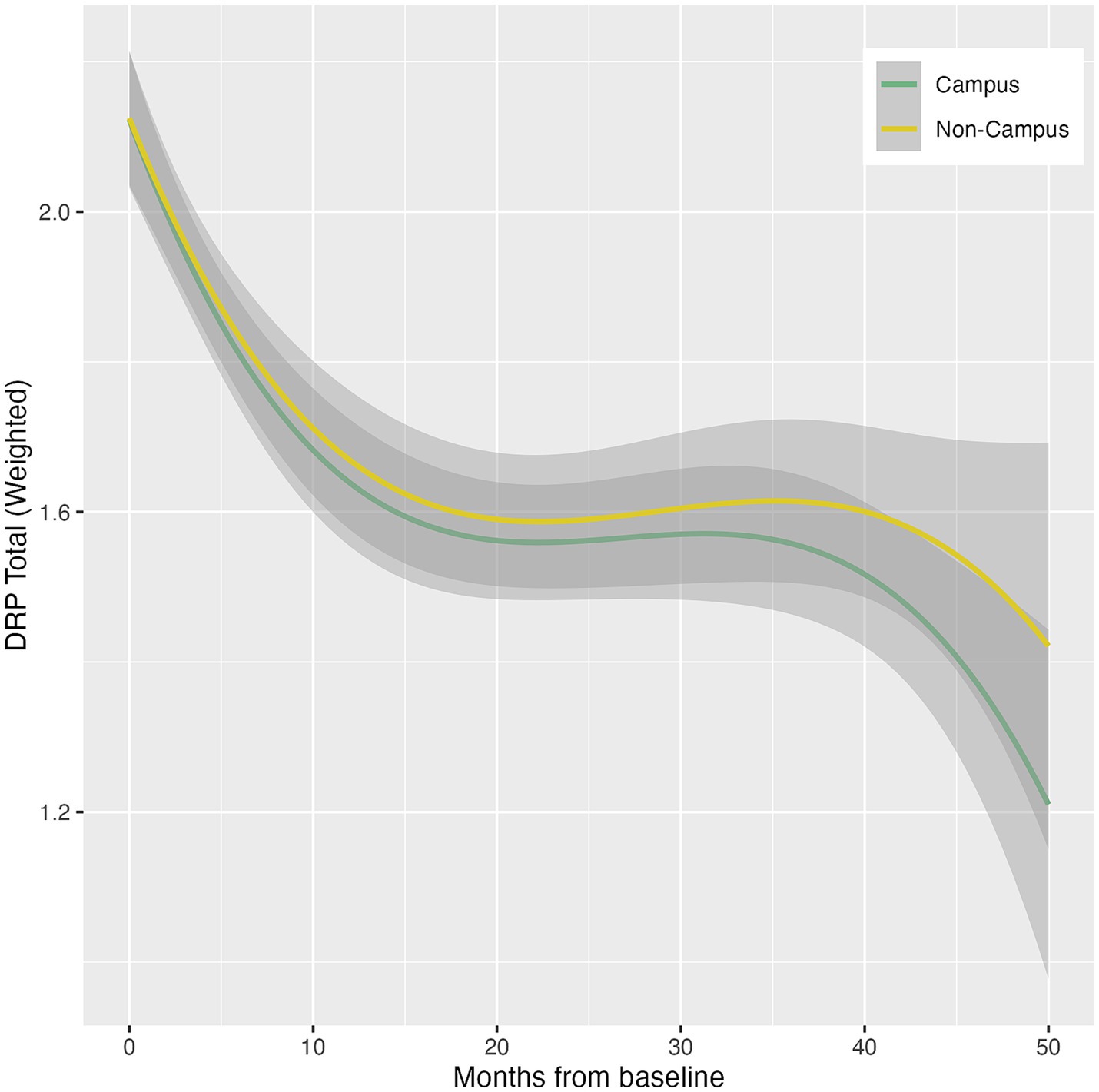
Figure 1. Total change in DRP between intervention (Campus) and control (Non-campus) participants in the ISLAND Campus study. For each DRP category (low, medium and high) delta scores indicate longitudinal change (Follow up – Baseline) with a negative result indicating movement toward a lower DRP total score.
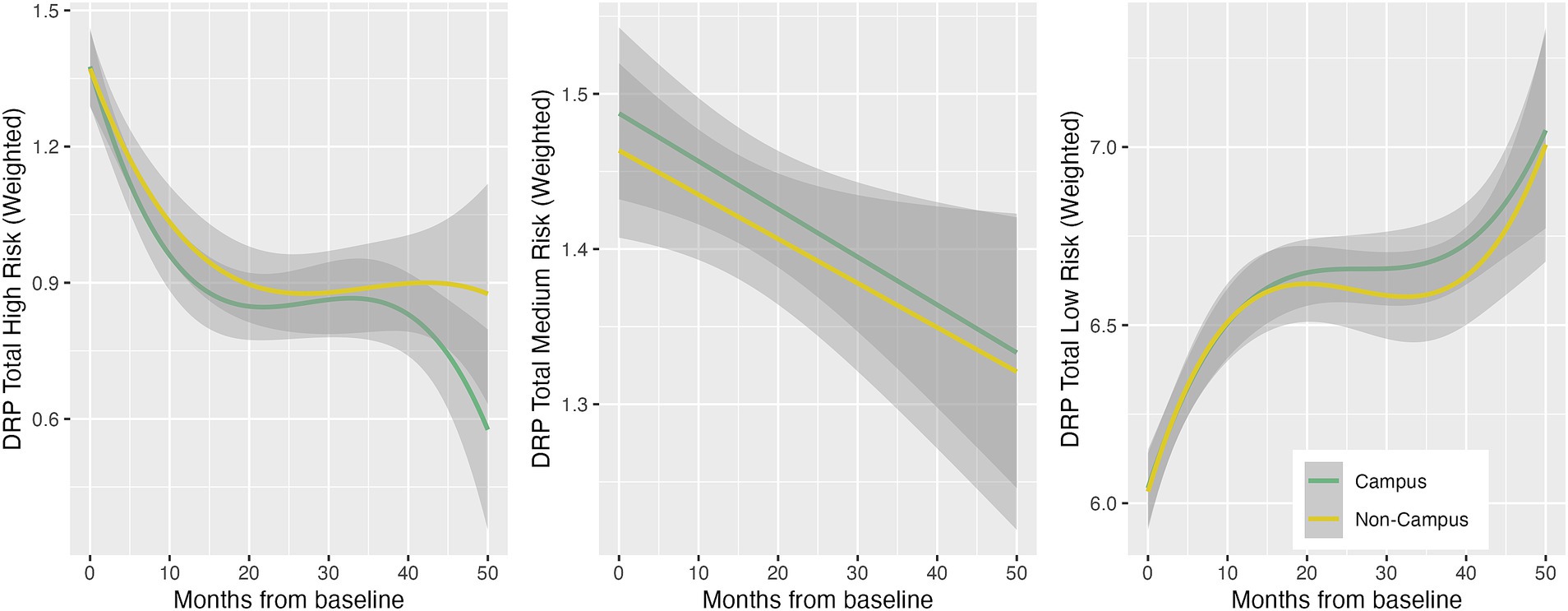
Figure 2. Longitudinal total DRP score trajectories between intervention (Campus) and control (Non-campus) participants in the ISLAND Campus study. Trajectories are generalized additive models with penalty-based smoothing regression splines.
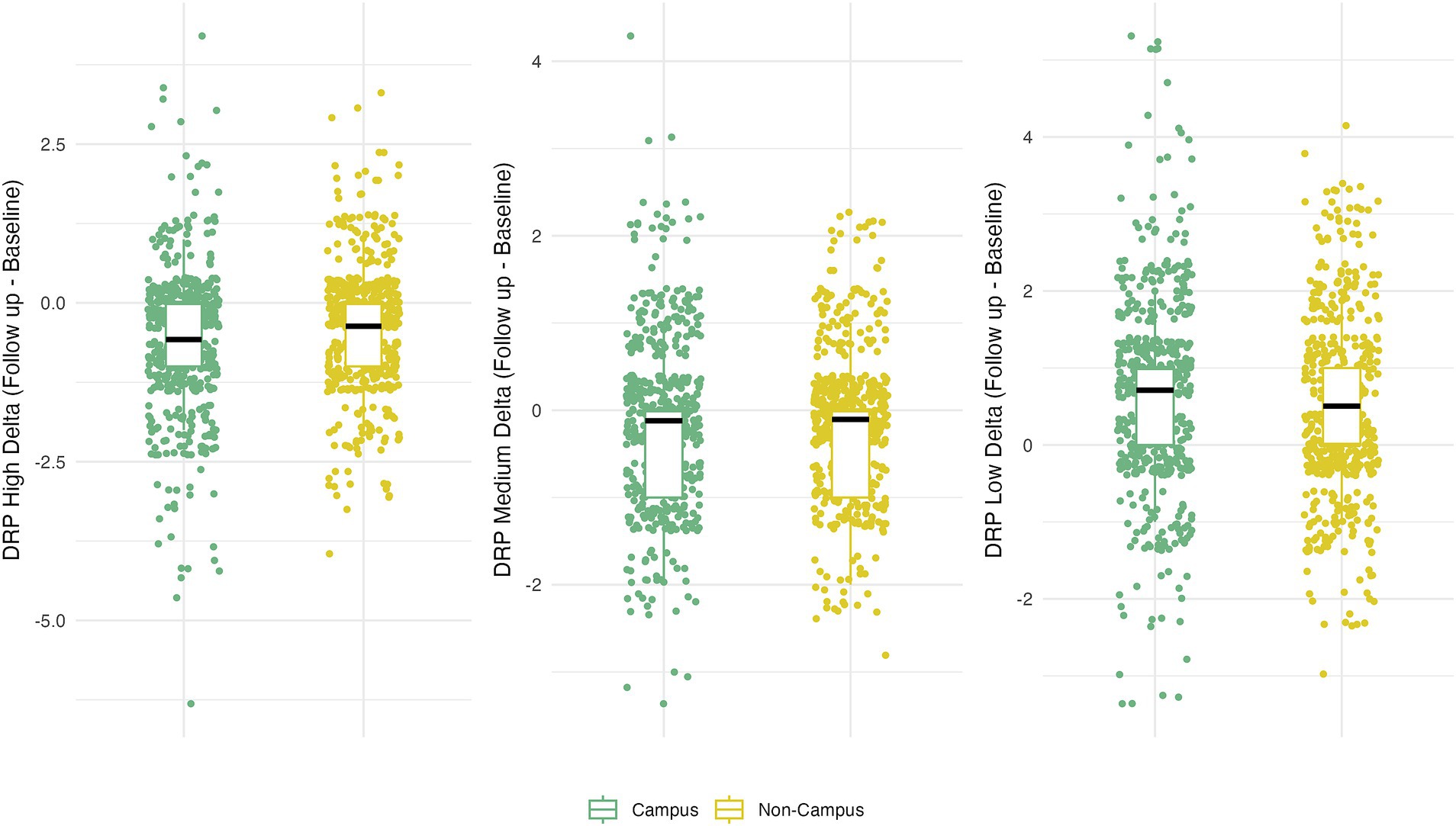
Figure 3. Longitudinal low, medium and high DRP score trajectories between intervention (Campus) and control (Non-campus) participants in the ISLAND Campus study. Trajectories are generalized additive models with thin plate regression splines, accounting for PSW.
ISLAND Campus participation was not significantly associated with longitudinal change in CANTAB PAL (Table 4), and this association remained non-significant after adjusting for covariates. Between baseline and follow up, ISLAND Campus participants significantly improved their spatial working memory (SWM). This effect remained after controlling for covariates such as age, gender, prior tertiary education, baseline CANTAB SWM and PWS (Table 5).
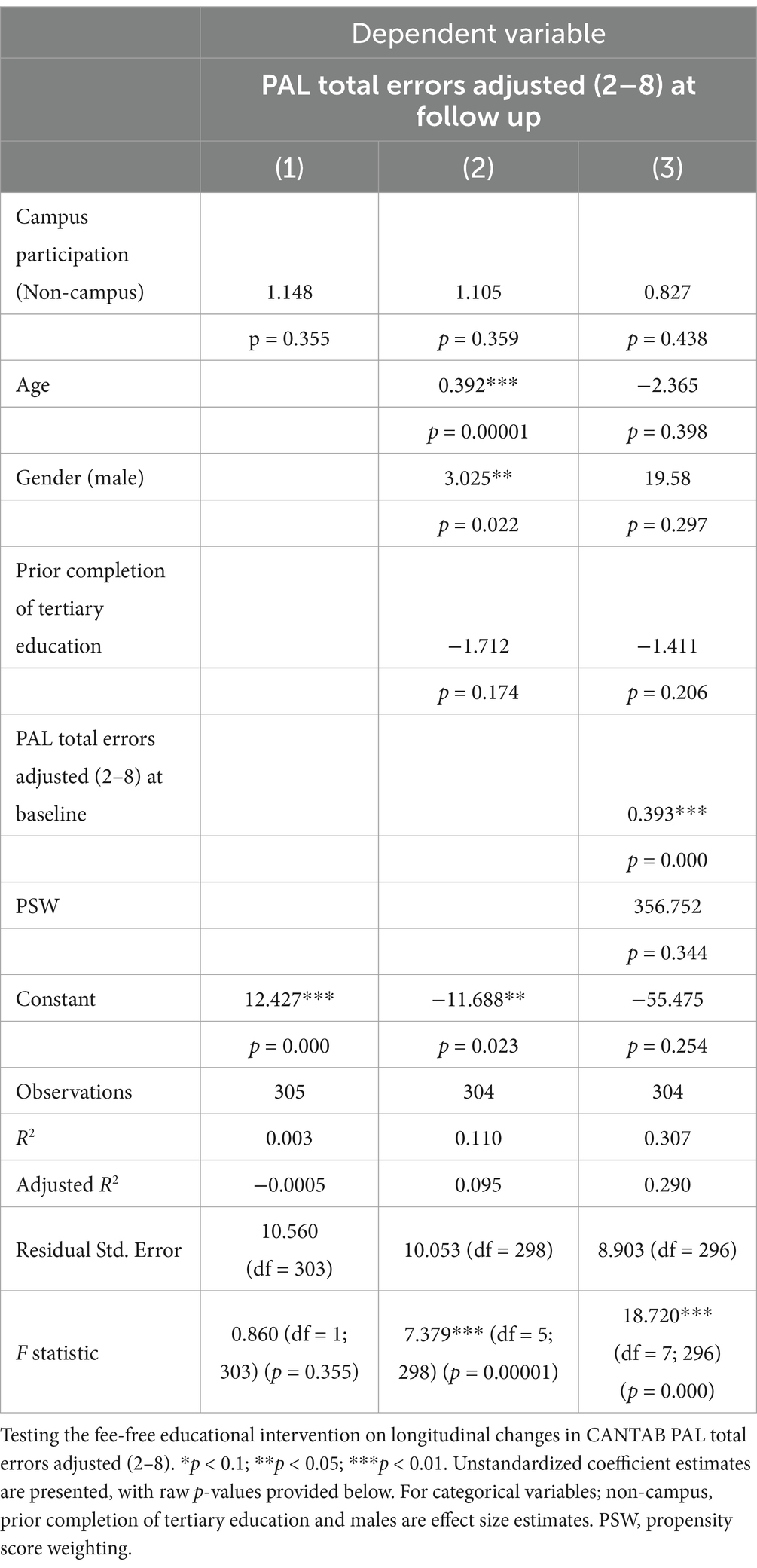
Table 4. Impact of ISLAND campus intervention on cognition via CANTAB paired associates learning (PAL).
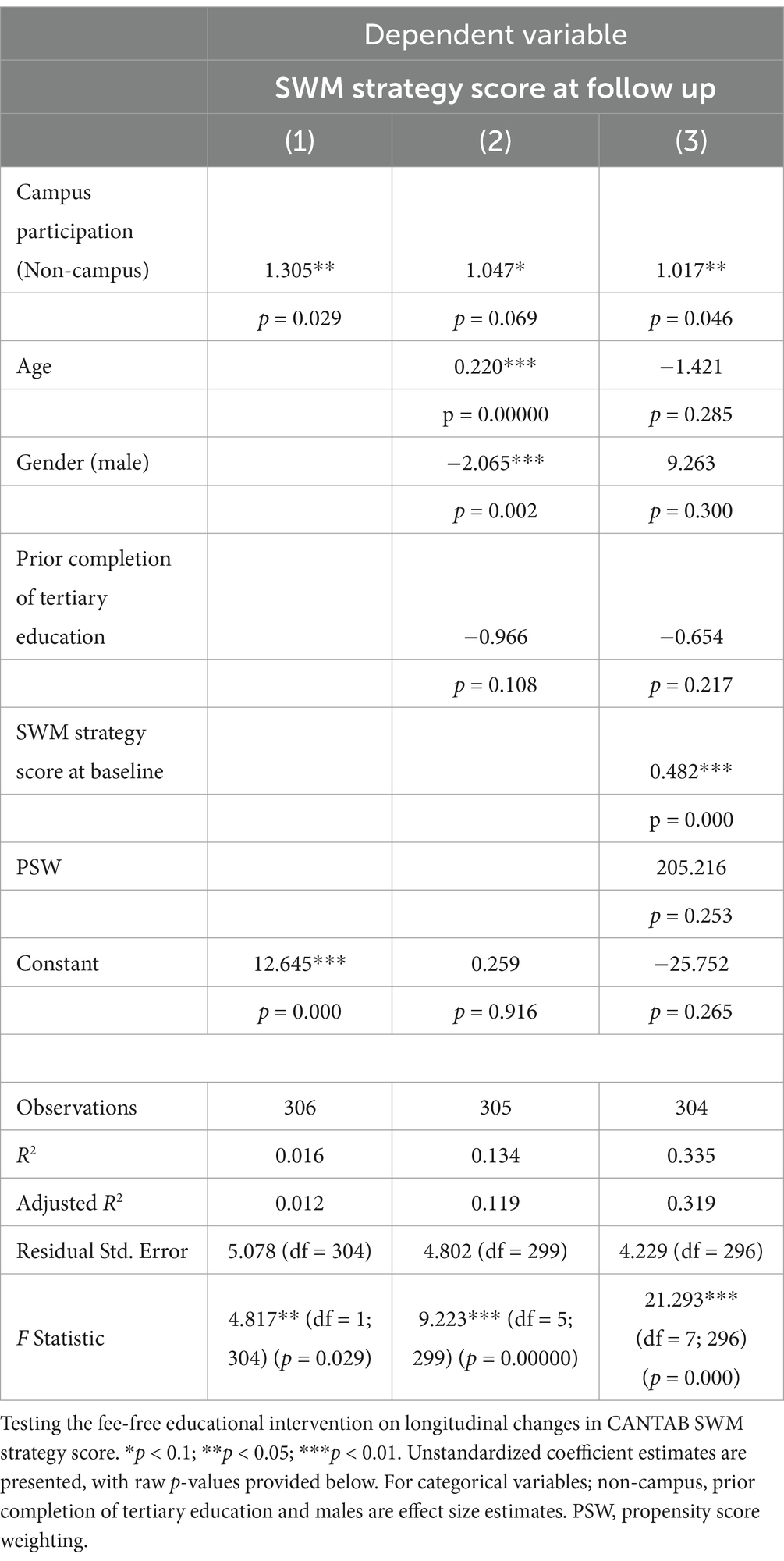
Table 5. Impact of ISLAND campus intervention on cognition via CANTAB spatial working memory (SWM).
A subset of participants (n = 231) were analyzed for plasma concentrations of phosphorylated tau 181 (p-tau 181). There was no significant association between ISLAND Campus participation and plasma concentrations of phosphorylated tau 181 (pg/mL; Supplementary Table 3; Supplementary Figure 2). This cross-sectional observation of p-tau 181 concentrations remained after adjusting for covariates.
All participants completed the Perceived Stress Scale (PSS, Supplementary Table 4). When compared with control (non-Campus) participants, ISLAND Campus intervention participants displayed similar PSS total scores, as well as similar responses for the 10-item instrument. There were significant differences among several domains of the New General Self-Efficacy Scale (NGSS) between intervention (ISLAND Campus) and control (non-Campus) participants (Supplementary Table 5). ISLAND Campus participants displayed significantly higher NGSS total scores, as well as higher agreement with self-efficacy sentiments on goal-attainment, overcoming barriers and overcoming challenges. There were no differences observed between intervention and control participants in health literacy, as measured by the All Aspects of Health Literacy Scale (AAHL, Supplementary Table 6).
Our post-hoc power analyses were conducted using the R (Collins et al., 2019) from the fully adjusted models, with a significance value of 0.05, giving the study a statistical power of above 0.85 for all fully adjusted GAMs, indicating this study was adequately powered to detect a medium-sized effect (coefficient estimate) of ISLAND Campus on DRP and cognitive outcomes.
In this large-scale prospective cohort of healthy Australian adults, we found that engaging with a formal tertiary educational intervention had a positive impact on dementia risk reduction and working memory. ISLAND Campus offered completely free formal educational degrees to any Tasmanian over 50 years of age, then measured the impact of this intervention on a variety of dementia risk measurement tools. This was a unique investigation conducted at UTAS, the only university located in Australia’s island state of Tasmania. To the best of our knowledge, this is the only longitudinal investigation of the impact of a fee-free formal tertiary educational intervention on modifiable risk factors for dementia, cognition and plasma concentrations of p-tau 181. We used a robust method of propensity score matching to show how a fee-free tertiary educational intervention for adults can have a positive impact on dementia risk factor reduction and cognition, and offers an ideal educational intervention for dementia prevention strategies in mid- to later-life.
We found ISLAND Campus participants significantly improved their scores on the DRP. Both intervention and control participants were similar at baseline, so the observed differences reported in DRP may be indicating the educational intervention had a sustained positive impact on participants adherence to modifiable risk factors for dementia. When we investigated the specific risk factors that were amenable to change, the DRP categories of BMI risk and Cognitive Activity risk displayed significant differences over time. ISLAND Campus participants showed a significant reduction in risk under these categories of the DRP, suggesting the fee-free educational intervention not only had a positive impact on engagement with cognitively stimulating activities, but also on other modifiable risk factors for dementia, potentially due to the increased engagement in participants’ own health management and literacy. Improvements in Cognitive Activity remained after adjusting for covariates such as education, suggesting Campus had an impact on Cognitive Activity beyond the bounds of tertiary education.
Compared to controls, ISLAND Campus participants significantly improved their SWM over 2 years yet we observed no changes in PAL. Engagement with formal tertiary education is multifaceted, involving planning, problem solving and mental organization, all skills that are linked to SWM and the prefrontal cortex (Yue et al., 2024). ISLAND Campus participants also may have been challenged by the navigation of digital platforms, academic schedule management and multitasking which may have selectively recruited SWM abilities. We did not observe changes in PAL over time, likely due to this task’s reliance on hippocampal function (Van Dijk et al., 2010). Previous research shows general age-related decline of hippocampal function and PAL (Lee et al., 2013), therefore the ISLAND Campus intervention may not have been running long enough to see improvements in these trajectories. Our results were also similar to previous studies such as those in the THBP (Bindoff et al., 2021), where we also found cognitive improvements over time regardless of age, with the domains most amenable to change being language, verbal learning and episodic memory. Amid a global movement of mid- to later- life individuals continuing with education throughout the lifecourse (Isopahkala-Bouret et al., 2018), age is unlikely to be a barrier to engagement in mid- to later- life education as a public health intervention.
We observed strong uptake of the intervention which was available to all ISLAND participants, thus greatly reducing socioeconomic and geographical barriers to participation. When comparing ISLAND Campus (intervention) and non-Campus (control) participants, there were no significant differences in age, gender, IRSAD decile, remoteness area, total education in years, memory complaints, family history of dementia or APOE presence. Intervention participants were aged between 50 and 86 years, showing age was no barrier to participation in this tertiary educational intervention. The only significant baseline difference observed between intervention and control participants was prior completion of tertiary education, with ISLAND Campus participants displaying significantly higher education than their non-Campus counterparts. We believe this difference is likely due to previous tertiary education removing the stigma and barriers of subsequent tertiary educational engagement, and in future will target ISLAND participants with no prior tertiary education in Campus invitations, where the greatest gains are likely to be seen.
ISLAND Campus participants enrolled in a variety of courses offered at UTAS, such as Diplomas, Bachelors, Associate Degrees, Graduate Certificates and Masters. There was substantial diversity among courses chosen, for example with uptake of Family History (n = 103, 20.9%), Sustainable Living (n = 37, 7.5%), Dementia Care (n = 17, 3.4%) and Music (n = 7, 1.4%). Given growing evidence for digital literacy, online access and device ownership increasing in older adults (Morrison et al., 2023), Campus offered a unique and accessible intervention to an engaged group of participants. With less pressure to select tertiary courses that offer subsequent employment opportunities, we may be observing the impact of education at a stage of life where improving and maintaining quality of life is more of a priority than employment opportunity. We did not observe any significant baseline differences in p-tau181, although given the cross-sectional nature of our biological analysis method, we may expect to see changes in subsequent biennial rounds of biomarker sampling. Previous research has shown even in cognitively heterogenous cohorts, plasma p-tau 181 shows relative stability over 2 years (Karikari et al., 2021), therefore to observe an impact of a cognitively stimulating intervention in mid- to later- life, longitudinal analysis is necessary.
ISLAND Campus participants were similar to non-Campus participants in terms of stress perception and health literacy, however we did observe significantly higher scores for self-efficacy in intervention participants, indicating stronger sentiment for goal attainment, overcoming barriers and overcoming challenges. It may be the fee-free tertiary education was easier to engage with for individuals who had clear goals and motivations for achieving those goals. ISLAND is a public health campaign, with nested interventions designed to bring about positive dementia risk reduction activities in the community. One of the main aims of the 10-year ISLAND Project is to build participants’ self-efficacy to tackle dementia risk management (Bartlett et al., 2023; Bartlett et al., 2022). Through ISLAND Campus, we may be observing how educational interventions have capacity to build knowledge and an ability to appraise evidence and experience in tackling new opportunities for self-development and growth. For the remainder of the ISLAND Project, we hope to investigate the sustained impact of Campus on building self-efficacy, resilience and health literacy in the existing cohort, as well as offer an additional enrolment window for participants who may have missed out on the original opportunity. This will also provide opportunity to recruit a more diverse cross-section of Tasmania, with intervention efforts primarily targeted toward those without prior history of tertiary level education.
There are numerous strengths to this unique study. ISLAND Campus was a longitudinal initiative offered to all ISLAND participants, with minimal exclusion criteria; any Tasmanian over 50 was eligible to enrol. ISLAND Campus was designed to reduce socioeconomic and geographical barriers to participation in education, we saw no impact of geographic location or socioeconomic status on participation. Building on our previous results from the THBP (Bindoff et al., 2021), ISLAND Campus was offered via flexible in-person/online learning models, that were more readily available as a result of the COVID-19 pandemic (Bartlett et al., 2021). This study addressed gaps in equity, where traditional hierarchical models of family archetypes and career trajectories may have prevented participants from exploring tertiary education earlier in life (Machů et al., 2022). Further, by offering fee-free tertiary degrees to anyone over 50, ISLAND Campus removed the socioeconomic incentive to undertake formal tertiary education, instead advocating for education as a tool for cognitive stimulation and enjoyment. Future endeavors to replicate our findings should strive for equity in educational offerings, to ensure the benefits to brain health equity are available to diverse populations. Our analytic technique of propensity score matching provided a robust effect of the intervention on observational longitudinal data, without requiring random assignment of intervention (Olmos and Govindasamy, 2015) Further, given the breadth and scope of ISLAND survey tools and data collection (Bartlett et al., 2022), we were able to statistically account for a multitude of covariates that may have impacted our results, including the propensity weightings calculated to compare intervention and control participants.
There are several limitations to note. We observed ISLAND Campus intervention participants had significantly higher prior history of tertiary education than their control counterparts. However, this was accounted for in all subsequent analyses, and did not impact our main results. Given Campus participants were anonymous from general university students, we were unable to account for the standardization of the educational experience. However, identifying Campus participants from general university studentship may have imparted implicit bias that may have impacted our results. Further, as this was an opt-in, non-random intervention, we are unable to claim causation, yet our method of propensity score matching and weighting based on age and gender provides a robust estimate of the effect of the intervention, without requiring random allocation. We acknowledge several of our measures were self-reported in nature and may have imparted a bias to our findings, particularly with respect to the annual DRP. Further, several measures were cross-sectional, including our psychosocial surveys (PSS, NGSS, AAHL), however longitudinal data collection is underway.
Previous research has classified education as an early life modifiable risk factor for dementia (Livingston et al., 2020), limiting the modeling of educational interventions in mid- to later-life (Mukadam et al., 2020). ISLAND Campus demonstrates how education is an endeavor throughout the lifecourse, and that educational interventions can have efficacy in mid- to later-life as well as the traditional model of education in early life. Here we have shown how a longitudinal formal tertiary educational intervention open to anyone in the community over 50 years of age can have an equitable, sustained and positive impact on dementia risk reduction through modifiable risk factors and cognition. With biennial biomarker collection planned, we are interested to see whether fee-free formal tertiary education can potentially reduce the hallmark biomarkers of dementia, or mitigate the neuropathological effects of biomarkers on cognitive capacity.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
The studies involving humans were approved by the University of Tasmania Health and Medical Human Research Ethics Committee (HREC H0018264). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
ER: Conceptualization, Data curation, Formal analysis, Methodology, Visualization, Writing – original draft, Writing – review & editing. AlK: Conceptualization, Data curation, Formal analysis, Writing – review & editing. AB: Formal analysis, Investigation, Writing – review & editing. JA: Conceptualization, Writing – review & editing. LB: Conceptualization, Writing – review & editing. JC: Writing – review & editing. AnK: Conceptualization, Funding acquisition, Supervision, Writing – review & editing. HF: Writing – review & editing. KD: Writing – review & editing. JV: Conceptualization, Funding acquisition, Supervision, Writing – review & editing.
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This was a sub-study of the ISLAND Project, which is supported by the Medical Research Future Fund Keeping Tasmanians out of Hospital, the Hopkins Foundation, the University of Tasmania (UTAS), St Luke’s Health, and the Masonic Centenary Medical Research Foundation.
We would like to extend great acknowledgement to the ISLAND participants for their ongoing contributions to this world first study. We would also like to thank the UTAS staff members that have assisted in the data collection and curation of this innovative investigation: Jared McClure, Senior Student Insights Analyst, Division of Future Students; Graeme McCormack, Lab Technician, Wicking Dementia Research and Education Centre; Joshua Eastgate, Senior Technical Developer, Wicking Dementia Research and Education Centre. Further, for the ongoing contributions of the ISLAND Project Team (Adam Kane, Florence Sward) and ISLAND’s Data Managers (Alex Kitsos, Timothy Saunder).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnagi.2024.1479926/full#supplementary-material
Alty, J. E., Bindoff, A. D., Stuart, K. E., Roccati, E., Collins, J. M., King, A. E., et al. (2023). Sex-specific protective effects of cognitive reserve on age-related cognitive decline: a 5-year prospective cohort study. Neurology 100, e211–e219. doi: 10.1212/WNL.0000000000201369
Bäckman, L., Wahlin, Å., Small, B. J., Herlitz, A., Winblad, B., and Fratiglioni, L. (2004). Cognitive functioning in aging and dementia: the Kungsholmen project. Aging Neuropsychol. Cogn. 11, 212–244. doi: 10.1080/13825580490511099
Ball, K., Berch, D. B., Helmers, K. F., Jobe, J. B., Leveck, M. D., Marsiske, M., et al. (2002). Effects of cognitive training interventions with older adults: a randomized controlled trial. JAMA 288, 2271–2281. doi: 10.1001/jama.288.18.2271
Bartlett, L., Bindoff, A., Doherty, K., Kim, S., Eccleston, C., Kitsos, A., et al. (2023). An online, public health framework supporting behaviour change to reduce dementia risk: Interim results from the island study linking ageing and neurodegenerative disease. BMC Public Health 23:1886. doi: 10.1186/s12889-023-16805-2
Bartlett, L., Brady, J. J., Farrow, M., Kim, S., Bindoff, A., Fair, H., et al. (2021). Change in modifiable dementia risk factors during COVID-19 lockdown: the experience of over 50s in Tasmania, Australia. Alzheimer's Dement. 7:e12169. doi: 10.1002/trc2.12169
Bartlett, L., Doherty, K., Farrow, M., Kim, S., Hill, E., King, A., et al. (2021). The island study linking ageing and neurodegenerative disease: protocol and progress. Alzheimer's Dement. 2021, 1–15.
Bartlett, L., Doherty, K., Farrow, M., et al. (2022). Island study linking aging and neurodegenerative disease (ISLAND) targeting dementia risk reduction: protocol for a prospective web-based cohort study. JMIR Research Protocols 11:e34688. doi: 10.2196/34688
Bindoff, A. D., Summers, M. J., Hill, E., Alty, J., and Vickers, J. C. (2021). Studying at university in later life slows cognitive decline: a long‐term prospective study. Alzheimers Dement. 7, 1–10. doi: 10.1002/trc2.12207
Champely, S, Ekstrom, C, Dalgaard, P, Gill, J., Weibelzahl, S., Anandkumar, A., et al. Pwr: basic functions for power analysis. (2017).
Chen, G., Gully, S. M., and Eden, D. (2001). Validation of a new general self-efficacy scale. Organ. Res. Methods 4, 62–83. doi: 10.1177/109442810141004
Chinn, D., and McCarthy, C. (2013). All aspects of health literacy scale (AAHLS): developing a tool to measure functional, communicative and critical health literacy in primary healthcare settings. Patient Educ. Couns. 90, 247–253. doi: 10.1016/j.pec.2012.10.019
Cohen, S., Kamarck, T., and Mermelstein, R. (1983). A global measure of perceived stress. J. Health Soc. Behav. 24:385. doi: 10.2307/2136404
Collins, R., Silarova, B., and Clare, L. (2019). Dementia primary prevention policies and strategies and their local implementation: a scoping review using England as a case study. J. Alzheimers Dis. 70, S303–S318. doi: 10.3233/JAD-180608
Gonzalez-Gomez, R., Legaz, A., Moguilner, S., Cruzat, J., Hernández, H., Baez, S., et al. (2024). Educational disparities in brain health and dementia across Latin America and the United States. Alzheimers Dement. 20, 5912–5925. doi: 10.1002/alz.14085
Hatzenbuehler, M. L., McLaughlin, K. A., Weissman, D. G., and Cikara, M. (2024). A research agenda for understanding how social inequality is linked to brain structure and function. Nat. Hum. Behav. 8, 20–31. doi: 10.1038/s41562-023-01774-8
Hilal, S., and Brayne, C. (2022). Epidemiologic trends, social determinants, and brain health: the role of life course inequalities. Stroke 53, 437–443. doi: 10.1161/STROKEAHA.121.032609
Hill, E., Collins, J. M., Bindoff, A., King, A. E., Alty, J., Summers, M. J., et al. (2021). Association between components of cognitive reserve and serum BDNF in healthy older adults. Neuroscience 13, 1–9. doi: 10.3389/fnagi.2021.725914
Hlavac, M. (2018). Stargazer: well-formatted regression and summary statistics tables. R Pack. Vers. 5:2.
Isopahkala-Bouret, U., Börjesson, M., Beach, D., Haltia, N., Jónasson, J. T., Jauhiainen, A., et al. (2018). Access and stratification in Nordic higher education. A review of cross-cutting research themes and issues*. Inquiry 9, 142–154. doi: 10.1080/20004508.2018.1429769
Karikari, T. K., Benedet, A. L., Ashton, N. J., Lantero Rodriguez, J., Snellman, A., Suárez-Calvet, M., et al. (2021). Diagnostic performance and prediction of clinical progression of plasma phospho-tau181 in the Alzheimer’s Disease Neuroimaging Initiative. Mol. Psychiatry 26, 429–442. doi: 10.1038/s41380-020-00923-z
Kivipelto, M., Mangialasche, F., Snyder, H. M., Allegri, R., Andrieu, S., Arai, H., et al. (2020). World-wide FINGERS network: a global approach to risk reduction and prevention of dementia. Alzheimers Dement. 16, 1078–1094. doi: 10.1002/alz.12123
Lee, A., Archer, J., Wong, C. K. Y., Chen, S.-H. A., and Qiu, A. (2013). Age-related decline in associative learning in healthy Chinese adults. PLoS One 8:e80648. doi: 10.1371/journal.pone.0080648
Livingston, G., Huntley, J., Liu, K. Y., Costafreda, S. G., Selbæk, G., Alladi, S., et al. (2024). Dementia prevention, intervention, and care: 2024 report of the lancet standing commission. Lancet 404, 572–628. doi: 10.1016/S0140-6736(24)01296-0
Livingston, G., Huntley, J., Sommerlad, A., Ames, D., Ballard, C., Banerjee, S., et al. (2020). Dementia prevention, intervention, and care: 2020 report of the lancet commission. Lancet 396, 413–446. doi: 10.1016/s0140-6736(20)30367-6
Lüdecke, D., Ben-Shachar, M. S., Patil, I., Waggoner, P., and Makowski, D. (2021). Performance: an R package for assessment, comparison and testing of statistical models. J. Open Source Software 6, 1–8. doi: 10.21105/joss.03139
Machů, V., Arends, I., Veldman, K., and Bültmann, U. (2022). Work-family trajectories and health: a systematic review. Adv. Life Course Res. 52:100466. doi: 10.1016/j.alcr.2022.100466
Moher, D., Hopewell, S., Schulz, K. F., Montori, V., Gøtzsche, P. C., Devereaux, P. J., et al. (2010). CONSORT 2010 explanation and elaboration: updated guidelines for reporting parallel group randomised trials. BMJ 2010, 701–741. doi: 10.3736/jcim20100801
Montemurro, S., Filippini, N., Ferrazzi, G., Mantini, D., Arcara, G., and Marino, M. (2023). Education differentiates cognitive performance and resting state fMRI connectivity in healthy aging. Front. Aging Neurosci. 15, 1–10. doi: 10.3389/fnagi.2023.1168576
Morrison, B. A., Nicholson, J., Wood, B., and Briggs, P. (2023). Life after lockdown: the experiences of older adults in a contactless digital world. Front. Psychol. 13:1100521. doi: 10.3389/fpsyg.2022.1100521
Mukadam, N., Anderson, R., Knapp, M., Wittenberg, R., Karagiannidou, M., Costafreda, S. G., et al. (2020). Effective interventions for potentially modifiable risk factors for late-onset dementia: a costs and cost-effectiveness modelling study. Lancet Healthy Longevity 1, e13–e20. doi: 10.1016/S2666-7568(20)30004-0
Najar, J., Östling, S., Gudmundsson, P., Sundh, V., Johansson, L., Kern, S., et al. (2019). Cognitive and physical activity and dementia: a 44-year longitudinal population study of women. Neurology 92, e1322–e1330. doi: 10.1212/WNL.0000000000007021
Ngandu, T., Lehtisalo, J., Solomon, A., Levälahti, E., Ahtiluoto, S., Antikainen, R., et al. (2015). A 2 year multidomain intervention of diet, exercise, cognitive training, and vascular risk monitoring versus control to prevent cognitive decline in at-risk elderly people (FINGER): a randomised controlled trial. Lancet 385, 2255–2263. doi: 10.1016/S0140-6736(15)60461-5
Olmos, A., and Govindasamy, P. (2015). A practical guide for using propensity score weighting in R. Pract. Assess. Res. Eval. 20:13. doi: 10.7275/jjtm-r398
Phelan, J. C., Link, B. G., and Tehranifar, P. (2010). Social conditions as fundamental causes of health inequalities: theory, evidence, and policy implications. J. Health Soc. Behav. 51, S28–S40. doi: 10.1177/0022146510383498
R Core Team (2023). R: A language and environment for statistical computing. Vienna, Austria: R Foundation for Statistical Computing Available at: https://www.R-project.org/.
Robbins, T. W., James, M., Owen, A. M., Sahakian, B. J., McInnes, L., and Rabbitt, P. (2004). Cambridge neuropsychological test automated battery (CANTAB): a factor analytic study of a large sample of normal elderly volunteers. Dement. Geriatr. Cogn. Disord. 5, 266–281. doi: 10.1159/000106735
Roccati, E., Collins, J. M., Bindoff, A. D., Alty, J. E., Bartlett, L., King, A. E., et al. (2023). Modifiable risk factors for dementia, cognition, and plasma phosphorylated tau 181 in a large-scale cohort of Australian older adults. Neurobiol. Aging 131, 106–114. doi: 10.1016/j.neurobiolaging.2023.06.018
Siette, J., Dodds, L., Deckers, K., Köhler, S., and Armitage, C. J. (2023). Cross-sectional survey of attitudes and beliefs towards dementia risk reduction among Australian older adults. BMC Public Health 23:1021. doi: 10.1186/s12889-023-15843-0
Stuart, E. A., King, G., Imai, K., and Ho, D. (2011). MatchIt: nonparametric preprocessing for parametric causal inference. J. Stat. Softw. 42, 1–28. doi: 10.18637/jss.v042.i08
Summers, M. J., Saunders, N. L. J., Valenzuela, M. J., Summers, J. J., Ritchie, K., Robinson, A., et al. (2013). The Tasmanian healthy brain project (THBP): a prospective longitudinal examination of the effect of university-level education in older adults in preventing age-related cognitive decline and reducing the risk of dementia. Int. Psychogeriatr. 25, 1145–1155. doi: 10.1017/S1041610213000380
Swainson, R., Hodges, J., Galton, C., Semple, J., Michael, A., Dunn, B., et al. (2001). Early detection and differential diagnosis of Alzheimer’s disease and depression with neuropsychological tasks. Dement. Geriatr. Cogn. Disord. 12, 265–280. doi: 10.1159/000051269
Van Dijk, K. R., Hedden, T., Venkataraman, A., Evans, K. C., Lazar, S. W., and Buckner, R. L. (2010). Intrinsic functional connectivity as a tool for human connectomics: theory, properties, and optimization. J. Neurophysiol. 103, 297–321. doi: 10.1152/jn.00783.2009
Walhovd, K. B., Fjell, A. M., Wang, Y., Amlien, I. K., Mowinckel, A. M., Lindenberger, U., et al. (2022). Education and income show heterogeneous relationships to lifespan brain and cognitive differences across European and US cohorts. Cereb. Cortex 32, 839–854. doi: 10.1093/cercor/bhab248
Wolinsky, F. D., Vander Weg, M. W., Howren, M. B., Jones, M. P., and Dotson, M. M. (2013). A randomized controlled trial of cognitive training using a visual speed of processing intervention in middle aged and older adults. PLoS One 8:e61624. doi: 10.1371/journal.pone.0061624
Yamashita, T., Bardo, A. R., Liu, D., and Yoo, J. W. (2019). Education, lifelong learning and self-rated health in later life in the USA. Health Educ. J. 78, 328–339. doi: 10.1177/0017896918809500
Keywords: education, modifiable risk factors, cognition, biomarkers, intervention, longitudinal, epidemiology, public health
Citation: Roccati E, Kitsos A, Bindoff AD, Alty JE, Bartlett L, Collins JM, King AE, Fair H, Doherty K and Vickers JC (2024) ISLAND Campus: a fee-free formal university educational intervention in mid- to later-life to reduce modifiable risk factors for dementia and improve cognition. Front. Aging Neurosci. 16:1479926. doi: 10.3389/fnagi.2024.1479926
Edited by:
Francesco Panza, University of Bari Aldo Moro, ItalyReviewed by:
Juan F. Cardona, University of the Valley, ColombiaCopyright © 2024 Roccati, Kitsos, Bindoff, Alty, Bartlett, Collins, King, Fair, Doherty and Vickers. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Eddy Roccati, ZWRkeS5yb2NjYXRpQHV0YXMuZWR1LmF1
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.