
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Aging Neurosci. , 30 May 2024
Sec. Neurocognitive Aging and Behavior
Volume 16 - 2024 | https://doi.org/10.3389/fnagi.2024.1394460
This article is part of the Research Topic To Know or Not to Know: Causes and Evolution of Lack of Awareness of Cognitive Decline in Neurodegenerative Diseases, Volume II View all 9 articles
 David López-Martos1,2
David López-Martos1,2 Marc Suárez-Calvet1,2,3,4
Marc Suárez-Calvet1,2,3,4 Marta Milà-Alomà1,5,6
Marta Milà-Alomà1,5,6 Juan Domingo Gispert1,2,7
Juan Domingo Gispert1,2,7 Carolina Minguillon1,2,3Clara Quijano-Rubio8Gwendlyn Kollmorgen9
Carolina Minguillon1,2,3Clara Quijano-Rubio8Gwendlyn Kollmorgen9 Henrik Zetterberg10,11,12,13,14,15
Henrik Zetterberg10,11,12,13,14,15 Kaj Blennow10,11,16,17Oriol Grau-Rivera1,2,3,4*
Kaj Blennow10,11,16,17Oriol Grau-Rivera1,2,3,4* Gonzalo Sánchez-Benavides1,2,3* and for the ALFA study
Gonzalo Sánchez-Benavides1,2,3* and for the ALFA studyIntroduction: The lack of cognitive awareness, anosognosia, is a clinical deficit in Alzheimer’s disease (AD) dementia. However, an increased awareness of cognitive function, hypernosognosia, may serve as a marker in the preclinical stage. Subjective cognitive decline (SCD) might correspond to the initial symptom in the dynamic trajectory of awareness, but SCD might be absent along with low awareness of actual cognitive performance in the preclinical stage. We hypothesized that distinct meta-cognitive profiles, both hypernosognosia and anosognosia, might be identified in preclinical-AD. This research evaluated the association between cerebrospinal fluid (CSF) AD biomarkers and the awareness of episodic memory, further exploring dyadic (participant-partner) SCD reports, in the preclinical Alzheimer’s continuum.
Methods: We analyzed 314 cognitively unimpaired (CU) middle-aged individuals (mean age: 60, SD: 4) from the ALFA+ cohort study. Episodic memory was evaluated with the delayed recall from the Memory Binding Test (MBT). Awareness of episodic memory, meta-memory, was defined as the normalized discrepancy between objective and subjective performance. SCD was defined using self-report, and dyadic SCD profiles incorporated the study partner’s report using parallel SCD-Questionnaires. The relationship between CSF Aβ42/40 and CSF p-tau181 with meta-memory was evaluated with multivariable regression models. The role of SCD and the dyadic contingency was explored with the corresponding stratified analysis.
Results: CSF Aβ42/40 was non-linearly associated with meta-memory, showing an increased awareness up to Aβ-positivity and a decreased awareness beyond this threshold. In the non-SCD subset, the non-linear association between CSF Aβ42/40 and meta-memory persisted. In the SCD subset, higher Aβ-pathology was linearly associated with increased awareness. Individuals presenting only study partner’s SCD, defined as unaware decliners, exhibited higher levels of CSF p-tau181 correlated with lower meta-memory performance.
Discussion: These results suggested that distinct meta-cognitive profiles can be identified in preclinical-AD. While most individuals might experience an increased awareness associated with the entrance in the AD continuum, hypernosognosia, some might be already losing insight and stepping into the anosognosic trajectory. This research reinforced that an early anosognosic profile, although at increased risk of AD-related decline, might be currently overlooked considering actual diagnostic criteria, and therefore its medical attention delayed.
Alzheimer’s disease (AD) is a progressive neurodegenerative disorder, causing cognitive, behavioral, and psychiatric symptoms that involve functional impairment in the stage of dementia. The episodic memory system is the central node of disruption in the cognitive architecture of Alzheimer’s (Grober et al., 1987, 2008, 2023). One of the most striking symptoms of Alzheimer’s is anosognosia, a clinical deficit consisting in the patient’s unawareness of the neurological disease, showing lack of appraisal in cognitive, behavioral, and/or functional capacity (Starkstein et al., 2006; Starkstein, 2014). The cognitive neuropsychology of anosognosia in amnestic patients has contributed substantially to delineate the phenomenology of AD dementia, suggesting a selective disconnection between the modules of memory and awareness (McGlynn and Schacter, 1989; Schacter, 1990, 1992). Anosognosia, particularly referring here to the awareness of cognitive deficits in AD patients, might arise from a disruption in the meta-cognitive system. Meta-cognition supports a crucial role in self-referential processing and awareness of cognitive function, considered as a high order cognitive function involving the control and monitoring of thoughts, cognitive processes, and mental states (Sunderaraman and Cosentino, 2017).
Alzheimer’s neuropathology, consistent in abnormal deposition of amyloid-β (Aβ) plaques and tau tangles in the brain, defines the biological presence of the disease. These proteins begin to accumulate decades before the explicit occurrence of the first clinical symptoms (preclinical-AD). Along with the underlying neuropathological progression, the overt manifestation of AD gradually advances from healthy cognition to mild cognitive impairment (MCI), and ultimately, AD dementia. The status of amyloid-β (A), tau (T), and non-specific neurodegeneration ([N]) biomarkers are used to describe in a research framework the AT(N) profiles along the Alzheimer’s continuum (Jack et al., 2018). The current clinical criteria from the National Institute on Aging and the Alzheimer’s association (NIA-AA) characterize the transitional stage between healthy cognition and MCI by considering longitudinal cognitive assessment and/or subjective cognitive complaints (Jack et al., 2018). Currently, a critical point in the field is to uncover the biological, cognitive, and behavioral underpinnings of the disease’s trajectory, allowing early detection and intervention at the preclinical stage of the Alzheimer’s continuum.
Subjective Cognitive Decline (SCD) is defined as the self-perception of having experienced a change from the previous/expected cognitive capacity despite a clinically normal objective performance, directly related to middle aged and older population presenting concerns related to their own cognitive health. SCD is considered a risk factor for MCI, and it may represent one of the initial symptomatic manifestations of AD (Jessen et al., 2014). Nevertheless, subtle cognitive decline may or may not be evident to the individuals themselves or their close family members. Moreover, cognitive complaints can occur independently of AD pathological changes, and many other factors might lead to SCD, ranging from healthy aging to different clinical disorders (Jessen et al., 2014, 2020). Therefore, the assessment of SCD might result non-specific for AD, and it is currently recognized that that most individuals with SCD will not progress to MCI. Importantly, in the context of self-perception of cognitive function, it has been shown that subclinical levels of anxiety and depression are associated with SCD (Hill et al., 2016; Jenkins et al., 2021), but these symptoms might be: i) a plausible cause of SCD, ii) manifestation of underlying Aβ pathology, or iii) consequence of experiencing SCD (Jessen et al., 2020).
Subtle psychiatric symptoms have been linked with AD biomarkers and the risk of progression in CU individuals (Donovan et al., 2018; Krell-Roesch et al., 2018; Hanseeuw et al., 2020a; Lewis et al., 2022). Therefore, SCD and affective symptoms may interact, and their co-occurrence has already been linked with cognitive decline (Liew, 2020). The Subjective Cognitive Decline Initiative (SCD-I) working group suggested that subthreshold symptoms of anxiety and depression should be accounted in models of preclinical-AD, since these affective characteristics might be manifestations of AD-pathology as well (Jessen et al., 2014). Beyond these considerations, SCD criteria provides important and valuable insights into the early detection of AD pathology and the risk of clinical progression (Jessen et al., 2014, 2020). More recently, measurements of the awareness of cognitive function have been suggested to be a more specific marker than self-reported SCD at the preclinical stage of Alzheimer’s (Cacciamani et al., 2021).
In the context of clinical research in AD, cognitive awareness has been mainly measured through clinician evaluation, participant-partner discrepancy in parallel questionnaires of SCD, and/or objective-subjective discrepancy in neuropsychological performance (Starkstein, 2014). Awareness is commonly altered in MCI and AD dementia patients, with anosognosia reaching up to 80% of estimated prevalence in AD patients (Starkstein, 2014). Anosognosia is a notorious symptom that is associated with the severity of AD dementia, it relates with the patient’s involvement in dangerous behaviors, psychiatric and behavioral problems, and with increased caregiver burden (Horning et al., 2014; Starkstein, 2014). An impaired meta-cognition in AD due to anosognosia might come along with a widespread range of clinical implications, for both patients and their families. Improving our understanding of the cognitive, neuronal, and pathological underpinnings of anosognosia would enhance preclinical stage identification, informing about risk of progression and more precise therapeutic interventions. At the present, however, it is unclear how to delineate the spectrum of distinct subclinical alterations in the awareness of cognitive function present in preclinical-AD.
Cacciamani et al. (2017) presented the first study considering the specificity of awareness prior to the onset of clinical symptoms. They defined awareness of cognitive decline (ACD) using the participant-partner discrepancy in SCD questionnaires, characterizing participants as having low (participant complaints < partner complaints) or high ACD (participant complaints > partner complaints). This study showed that low ACD was associated with greater Aβ load and reduced cortical metabolism in comparison to individuals with high ACD. These insights were accompanied with the note that SCD measures, which involved only the participant’s self-reported SCD, without incorporating the study partner’s SCD, failed to show any consistent association with AD biomarkers. Vannini et al. (2017a) provided a chronological model of awareness across the preclinical and prodromal stages of AD. Considering here the discrepancy between objective and subjective memory performance, they showed that AD dynamically impacts awareness of episodic memory function. Their results indicated that in CU individuals, Aβ-pathology was associated with increased awareness of cognitive function, hypernosognosia, while Aβ-pathology in MCI patients was associated with reduced awareness of cognitive function, anosognosia, indicating a switch in the trajectory of meta-cognition in AD.
We have carried on a magnetic resonance imaging (MRI) study in our group, Sánchez-Benavides et al. (2018a), classifying CU individuals with the participant-partner SCD discrepancy as: unaware decliners (presenting only study partner’s SCD), SCD (self-reported SCD regardless of the study partner’s SCD), and controls (non-SCD and study partner’s non-SCD; neither participant nor study partner reported SCD). We found that unaware decliners showed lower memory performance, along with increased grey matter (GM) volume in medial frontal and insular regions in comparison to controls. The presence of SCD reported by the study partner, regardless of whether the participant themselves reported SCD, was as a significant predictor of lower hippocampal GM volume. These results were discussed in the context of non-linear changes preceding loss of GM volume in self-referential processing brain areas prior to clinical onset, and further suggested that observations made by a study partner regarding cognitive changes are a relevant piece of clinical information holding diagnostic value, independently of the individual’s self-awareness of cognitive decline. Following the literature of non-linear changes at the preclinical stage, Gagliardi et al. (2020) conducted research on awareness in the context of SCD, indicating that Aβ-pathology was non-linearly associated with awareness of episodic memory (objective-subjective discrepancy), showing hypernosognosia up to the threshold of Aβ-positivity, and anosognosia beyond the threshold of the Alzheimer’s pathological change. These results were discussed considering that frontal amyloid deposition might interfere with regions/networks of awareness and cognitive control, suggesting that the non-linear impact on awareness thus might relate to the advancement of Aβ-pathology.
Some longitudinal studies have already addressed the trajectory of awareness in the AD continuum. Hanseeuw et al. (2020b) showed that Aβ-pathology was associated with progressive lack of awareness, as defined with the participant-partner discrepancy. This study indicated that, regardless of clinical progression, the overall tendency in CU participants was an increased awareness. Crucially, considering just participants with clinical progression (i.e., CU to MCI, or MCI to dementia) the clinical status was predicted only with low, but not high awareness. The timeline showed that an increase in awareness was observed 1.6 years before MCI diagnosis, with awareness declining until symptom onset. In MCI patients, awareness was initially low and continued to decrease reaching anosognosia 3.2 years before dementia diagnosis. Cacciamani et al. (2020) described 3 longitudinal trends of ACD evolution (heightened, stable, and decline) in relationship to Aβ-pathology in a SCD cohort, showing in consistency, that progressive lack of awareness, but not persistence of cognitive complaints, was associated with greater Aβ-accumulation. A recent longitudinal study explored these distinct subclinical manifestations considering the awareness of cognitive function in relation to risk of progression in CU individuals, showing again that decreased, but not increased awareness, was associated with higher risk of clinical progression (Mimmack et al., 2023).
Therefore, distinct studies have suggested that prior to clinical onset in the AD continuum, CU individuals might experience a heightened awareness of cognitive function associated with underlying AD-progression, while other studies have suggested that lack of awareness is associated with similar characteristics and clinical progression. Although non-linear changes across preclinical AD have been already proposed, the heterogeneous levels of awareness shown by different individuals in relationship with AD neuropathology is a phenomenon not yet fully understood. Particularly, it is still unclear whether increased or decreased awareness of cognitive function characterizes best preclinical-AD. One the one side, SCD might represent the initial symptom of AD dementia, but on the other side, SCD might be not related to AD, or absent in preclinical stage for individuals progressing to MCI, as well as it can be absent in individuals progressing from MCI to AD (Mitchell et al., 2014). Based on the latest research, seems reasonable that distinct meta-cognitive profiles might emerge in preclinical-AD. In the present research, we hypothesized that, at very early stages in the preclinical Alzheimer’s continuum, there may be two distinct types of metacognitive profiles at risk of AD-related impairment:
(I) Hypernosognosia: Individuals with a sub-estimation of actual memory performance, showing an increased awareness in relationship to AD neuropathology.
(II) Anosognosia: Individuals with an over-estimation of actual memory performance, showing a decreased awareness in relationship to AD neuropathology.
The main objective of the present research was to test this hypothesis in the ALFA+ cohort study by evaluating the association of Cerebrospinal Fluid (CSF) Aβ and Tau biomarkers with awareness of episodic memory. Additionally, the role of self-reported and dyadic (participant-partner) SCD was further explored in these associations at the preclinical stage of the Alzheimer’s continuum.
The present research was performed in the ALFA+ cohort study, a longitudinal study nested to the ALFA study (Alzheimer’s and Families) (Molinuevo et al., 2016). The initial ALFA study included 2,743 middle-aged CU individuals with a high proportion of AD patients’ offspring (47.4%) and apolipoprotein E (APOE) ε4 carriers (34.8%). The nested ALFA+ study included 450 participants selected by their specific AD risk profile (AD parental history, and APOE-ε4 status) (Molinuevo et al., 2016). A detailed phenotyping of the participants, aside from a clinical, cognitive, and lifestyle characterization, involved blood and CSF sample collection for biomarker determination, as well as magnetic resonance imaging (MRI) and positron emission tomography (PET) acquisition.
The ALFA+ inclusion criteria were: (1) individuals who had previously participated in the ALFA study; (2) age between 45 and 65 years at the inclusion in ALFA; and (3) long-term commitment to the study: inclusion and follow-up visits and agreement to undergo all tests and study procedures (MRI, PET, and lumbar puncture). ALFA+ exclusion criteria were: (1) cognitive impairment (Clinical Dementia Rating [CDR] > 0, Mini-Mental State Examination (MMSE) < 27 or semantic fluency < 12); (2) any systemic illness or unstable medical condition that could lead to difficulty complying with the protocol; (3) any contraindication to any test or procedure; and (4) a family history of monogenic AD. In the present study, we included 314 individuals with complete CSF biomarker measurements, and cognitive data.
The ALFA+ study (ALFA-FPM-0311) was approved by the independent ethics committee ‘Parc de Salut Mar’, Barcelona, and registered at Clinicaltrials.gov (identifier: NCT02485730). All participants signed the study’s informed consent form also approved by the independent ethics committee ‘Parc de Salut Mar’, Barcelona.
Cerebrospinal fluid sample collection and processing followed standard procedures (Teunissen et al., 2014), which have been previously described (Milà-Alomà et al., 2020). CSF Aβ40 and Aβ42 were measured with the exploratory NeuroToolKit, a panel of robust prototype immunoassays (Roche Diagnostics International Ltd, Rotkreuz, Switzerland), on a cobas® e 601 module. CSF p-tau181 and t-tau (both corresponding to the mid-region domain of tau protein) were measured using the electrochemiluminescence Elecsys® Phospho-Tau (181P) CSF and Elecsys Total-Tau CSF immunoassays, respectively, on a fully automated cobas e 601 module (Roche Diagnostics International Ltd, Rotkreuz, Switzerland). All CSF biomarker measurements were determined at the Clinical Neurochemistry Laboratory at the University of Gothenburg, Sweden.
Following the NIA-AA research criteria (Jack et al., 2018) to define the AD neuropathologic processes, we used the AT system to classify each biomarker status. AT groups were defined using CSF levels with the cut-off of 0.071 of the CSF Aβ42/40 ratio for A status, and the cut-off of 24 pg/mL of CSF p-tau181 for T status (Milà-Alomà et al., 2020). We excluded from the analysis 12 participants classified with suspected non-Alzheimer’s pathology (A-T+) and included only those with normal biomarker levels (A-T-) or already in the Alzheimer’s continuum (A+ T-, A+T+) (Jack et al., 2018).
The Memory Binding Test (MBT) (Buschke, 2013) Spanish version (Gramunt et al., 2016) was used to assess verbal episodic memory through associative learning. The variables used in the present research to assess objective performance considered the two delayed recall measurements (30 min after learning): the total delayed free recall (0–32), and the total delayed paired recall (0–32). Participants were instructed to self-rate their overall performance in a single score ranging from 0 (worst possible performance) to 100 (best possible performance) after completing both delayed recall tasks. Objective episodic memory performance resulted from the arithmetic mean of the delayed recall (considering the total delayed free recall and the total delayed paired recall). Specifically, the total number of words recalled, both at free and cued delayed recall, was divided by the maximum possible score, and next multiplied by 100, thus obtaining a percentage. This way, objective performance was normalized to a scale from 0 to 100, matching post-diction metrics. A multivariable regression model was used to extract objective and subjective residual memory scores adjusted for demographic effects (sex, age, and education). Considering the full sample of participants, objective and subjective residual scores were standardized, dividing the residuals of each regression model by their estimated standard deviation. Meta-memory standardized residuals were computed subtracting subjective from objective standardized residuals, with positive scores indicating sub-estimation and negative scores indicating over-estimation of actual episodic memory performance.
The Subjective Cognitive Decline Questionnaire (SCD-Q) (Rami et al., 2014) was used as criteria to characterize the participant’s and study partner’s perception of SCD with parallel questionnaires, My-Cognition and Their-Cognition, respectively. The SCD-Q is a validated tool devised to detect and quantify the perceived subjective cognitive decline, comprising the same set of questions for the subject and the informant. The SCD-Q contains 3 initial “yes/no” questions followed by 24 items, inquiring about the presence or absence of difficulties in cognitive-related activities (for each participant and informant parallel versions). In line with previous studies, the presence/absence of subjective cognitive decline (SCD/non-SCD), as well as the mirror for the study partner (study partner’s SCD/study partner’s non-SCD), was defined with “yes/no” to this initial general question: “Do you perceive memory or cognitive difficulties?” for the participant, and “Do you perceive he/she has cognitive or memory difficulties?” for the study partner (Sánchez-Benavides et al., 2018a,b, 2021; Akinci et al., 2022).
The Hospital Anxiety and Depression Scale (HADS) (Zigmond and Snaith, 1983) was used to assess affective symptoms. The variables used in the present research were the anxiety (0–21) and depression (0–21) sub-scores from the HADS.
The analyses were divided into three main blocks. First, main analyses in the whole sample evaluating associations between meta-memory and CSF biomarkers. Second, stratified analyses by SCD status, using two models with the same predictors but in distinct subsets of the sample (non-SCD and SCD). Third, stratified analyses once the study partner’s SCD report was incorporated, combining it with the self-reported SCD measurements previously explored. Here, we considered to focus only on the subset characterized with presence of study partner’s SCD: within this subset, the sample was further stratified considering the self-reported SCD. Thus, there were “unaware decliners” (only the study partner presented SCD), and “aware decliners” (self-reported SCD confirmed by the study partner).
All CSF measurements and meta-memory scores were treated as continuous variables and tested for normality using the Kolmogorov-Smirnov normality test and visual inspection of histograms. In line with previous work, extreme values were excluded for CSF biomarkers (outlier threshold of 3 times the Interquartile Range [IQR]) (Milà-Alomà et al., 2020). The CSF Aβ42/40 ratio followed a normal distribution, but the CSF p-tau181 was not normally distributed and was log10-transformed. Meta-memory scores followed a normal distribution. In the main multivariable regression model, we evaluated the relationship between CSF biomarkers and meta-memory standardized residual scores adjusted for demographics. We used CSF Aβ42/40, and CSF p-tau181, incorporating a quadratic term for CSF Aβ42/40, and the interaction between CSF p-tau181 and the quadratic term for CSF Aβ42/40.
The inclusion of the quadratic term for CSF Aβ42/40 has been justified with theoretical and statistical considerations. Previous research suggested a switch in the trajectory of awareness across preclinical-AD (Vannini et al., 2017a). To the best of our knowledge, only one study to date have explicitly described a non-linear relationship between the continuous levels of Aβ pathology and the awareness of cognitive function in preclinical-AD (Gagliardi et al., 2020). The early impact of Aβ has been associated with awareness of memory performance due to disruption in frontal brain regions supporting cognitive control. While tau is more associated than Aβ with clinical symptoms at later disease stages, both pathologies have synergistic effects (Busche and Hyman, 2020). Yet, there is no literature suggesting that tau (presumably impacting medial temporal lobe) might induce non-linear changes in cognitive function prior to clinical onset.
The assumptions of the multivariable regression models were statistically tested for normality, homoscedasticity, and independence of residuals. Standardized β coefficients with 95% confidence interval (CI) and corresponding p values were reported. A descriptive correlation, instead of regression, was used to analyze associations between meta-memory and CSF biomarkers only after incorporating study partner’s SCD data, since the low sample size restricted the use of inferential statistics. For these analyses, Spearman correlation coefficients with corresponding p values were reported. For all statistical models, including regression and correlation, p values < 0.05 were considered statistically significant, and p values < 0.1 were considered as trends. All computational procedure and statistical analyses were performed using R, version 4.2.1, with RStudio, version 2022.07.1.
We analyzed data from three-hundred fourteen CU participants from the ALFA+ prospective cohort study, with complete CSF biomarkers and awareness measurements. Participant demographic characteristics are shown in Table 1. Two-hundred five (65.3%) individuals were classified as A-T-, eighty-six (27.4%) individuals as A+T-, and twenty-three (7.3%) individuals as A+T+. SCD was defined in eighty-seven (27.7%) individuals, and non-SCD in two-hundred twenty-seven (72.3%) individuals. Study partner’s SCD was defined in twelve (3.8%) individuals, and study partner’s non-SCD in three-hundred two (96.2%) individuals. SCD-Q total scores for My-Cognition and Their-Cognition were also provided in Table 1, along with descriptive characteristics about study partners.
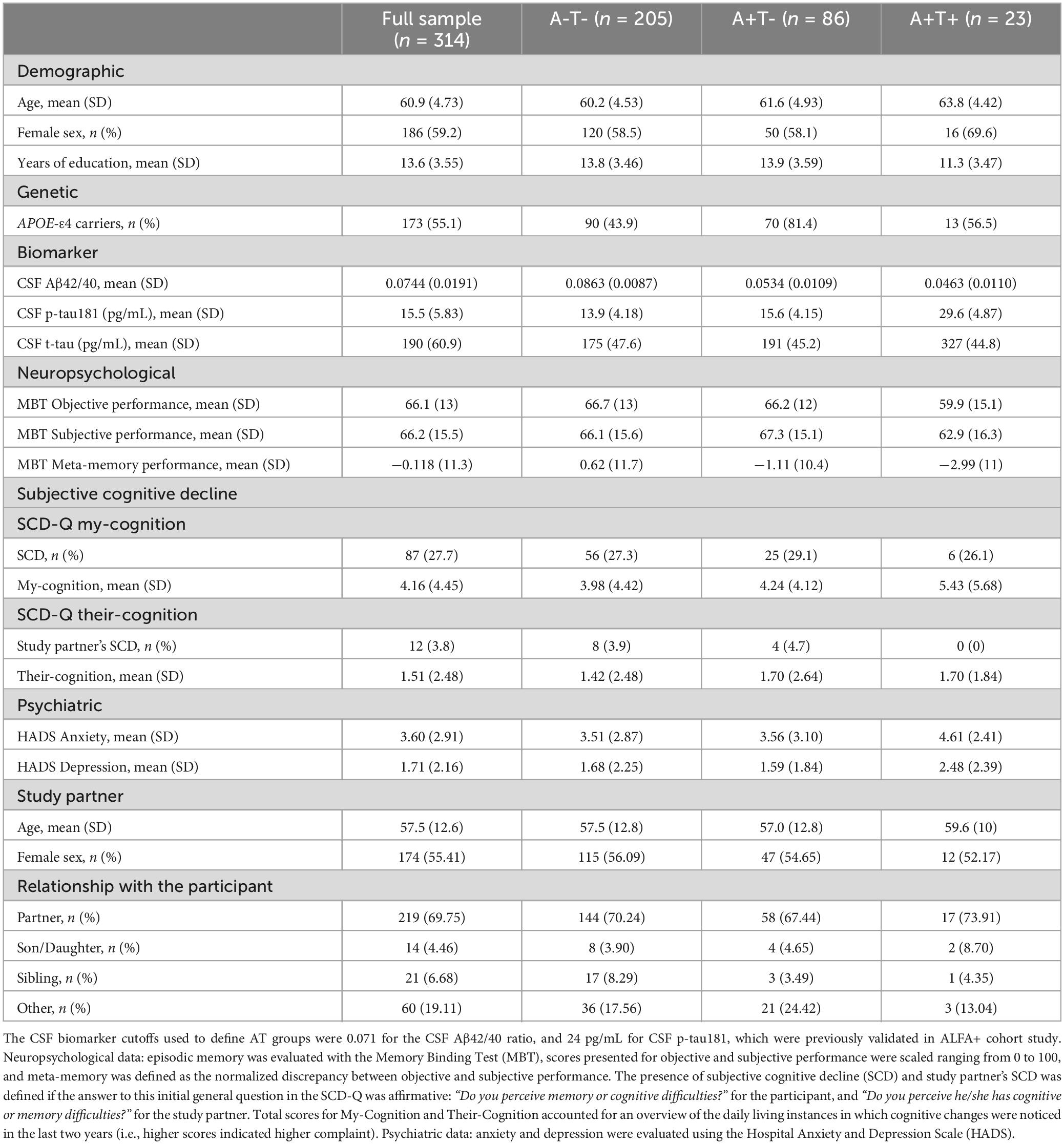
Table 1. Participant characteristics
Participant-partner contingency by SCD status is shown in Table 2. Within non-SCD (n = 227), study partner’s SCD was defined in seven (3.01%) individuals (characterized as unaware decliners; only the study partner presented SCD), and study partner’s non-SCD was defined in two-hundred twenty (96.91%) individuals (characterized as controls; neither participant nor partner reported SCD). Within SCD (n = 87), study partner’s SCD was defined in five (5.75%) individuals (characterized as aware decliners; self-reported SCD confirmed by the study partner), and study partner’s non-SCD was defined in eighty-two (94.25%) individuals (characterized as SCD not confirmed by the study partner).
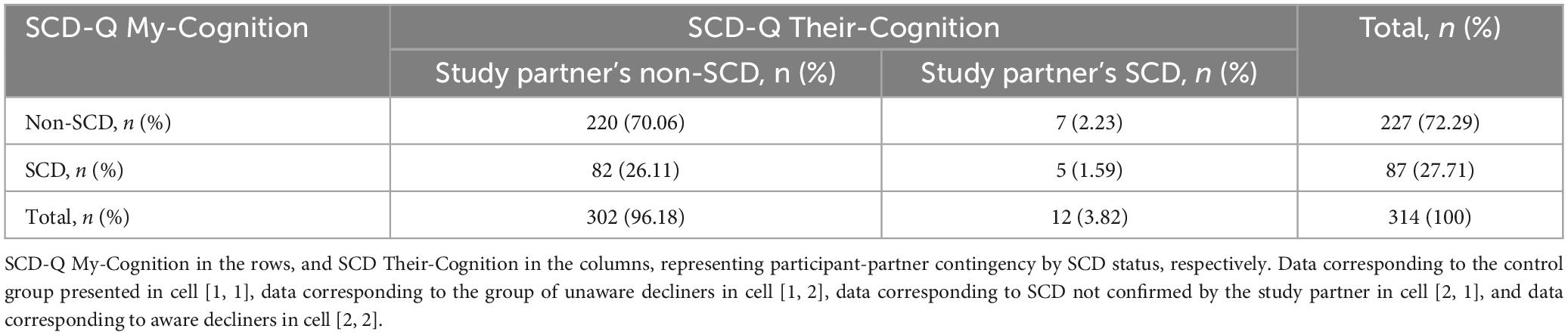
Table 2. Subjective cognitive decline (SCD) status by participant-partner parallel questionnaires.
Meta-memory raw scores were regressed against the demographic data (considering sex, age, and education) to obtain meta-memory standardized residual scores adjusted for these effects. The relationship between meta-memory standardized residuals adjusted for demographics and CSF biomarkers was evaluated. We entered simultaneously in a multivariable regression model the following predictors: CSF p-tau181, CSF Aβ42/40, the quadratic term of CSF Aβ42/40, and the interaction between CSF p-tau181 and the quadratic term of CSF Aβ42/40 (Table 3). Meta-memory was significantly associated with the quadratic term of CSF Aβ42/40 (β = −0.149, p = 0.025), but not with CSF p-tau181. Figure 1 shows the relationship between CSF Aβ42/40 and meta-memory standardized residuals. These results show a non-linear pattern (inverted-U shape) with increased awareness of episodic memory (i.e., hypernosognosia) being associated with lower Aβ42/40 levels up to approximately the threshold of Aβ-positivity (CSF Aβ42/40 < 0.071), followed by lower awareness (i.e., anosognosia) being associated with lower Aβ42/40 levels, after surpassing the threshold of Aβ-positivity.
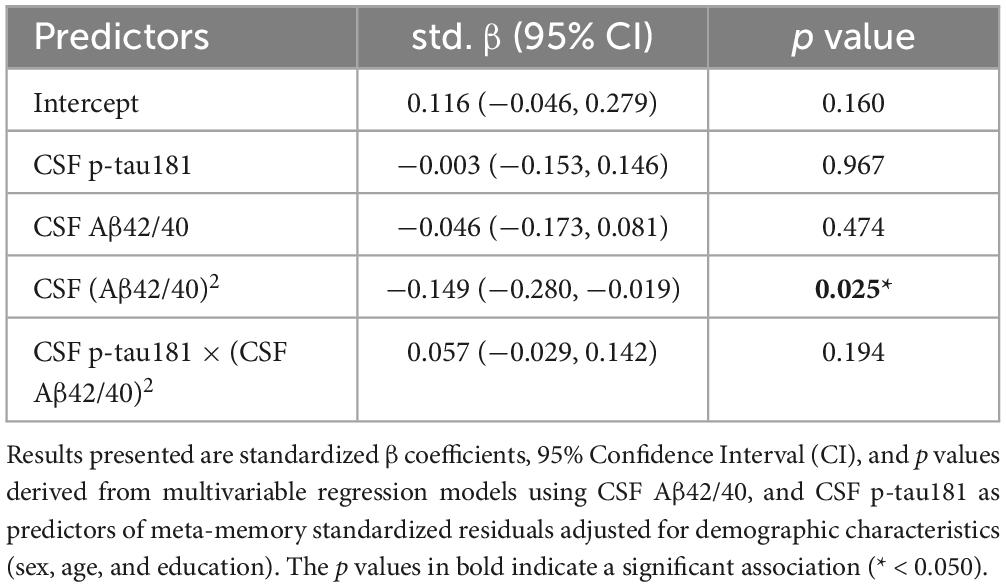
Table 3. Cerebrospinal fluid (CSF) biomarkers associated with meta-memory standardized residuals.
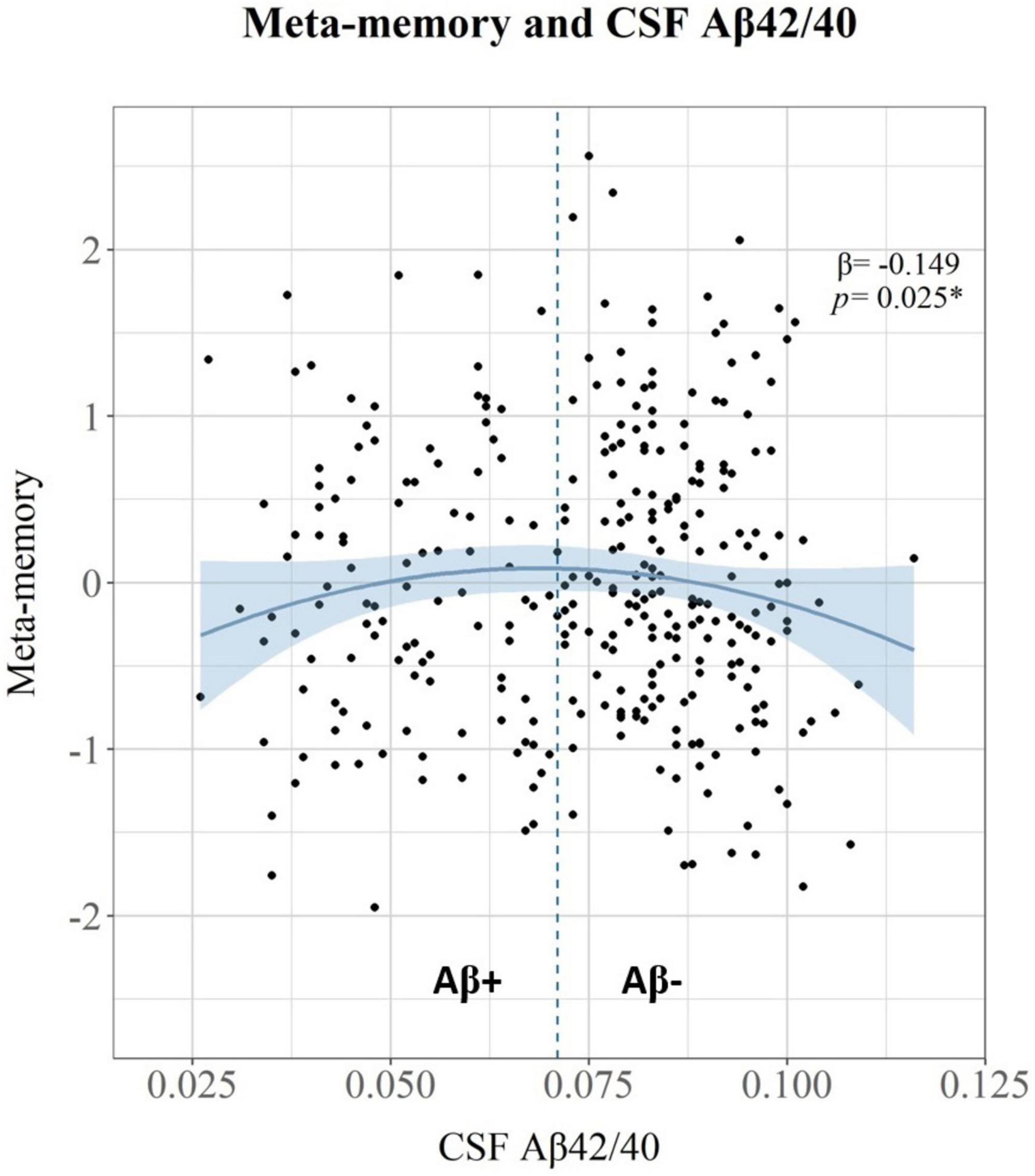
Figure 1. Scatter plot showing the relationship between CSF Aβ42/40 on the X-axis, and meta-memory standardized residual scores adjusted for demographic effects on the Y-axis. The vertical dashed line at x = 0.0071 represents the positivity threshold for CSF Aβ42/40. Standardized β coefficient and p value for the quadratic association between CSF Aβ42/40 and meta-memory standardized residuals are shown in the top-right side.
To further explore the role of SCD, the sample of participants was stratified according to SCD status. The relationship between meta-memory standardized residuals and CSF biomarkers was evaluated in both subsets (non-SCD and SCD). We entered simultaneously in two separate multivariable regression models the following predictors: CSF p-tau181, CSF Aβ42/40, the quadratic term of CSF Aβ42/40, and the interaction between CSF p-tau181 and the quadratic term of CSF Aβ42/40 (Table 4 and Figure 2). In the non-SCD subset, meta-memory was significantly associated with the quadratic term of CSF Aβ42/40 (β = −0.166, p = 0.034), but not with CSF p-tau181. In the subset with SCD, meta-memory was significantly associated with the linear term of CSF Aβ42/40 (β = −0.328, p = 0.008), but not with CSF p-tau181.
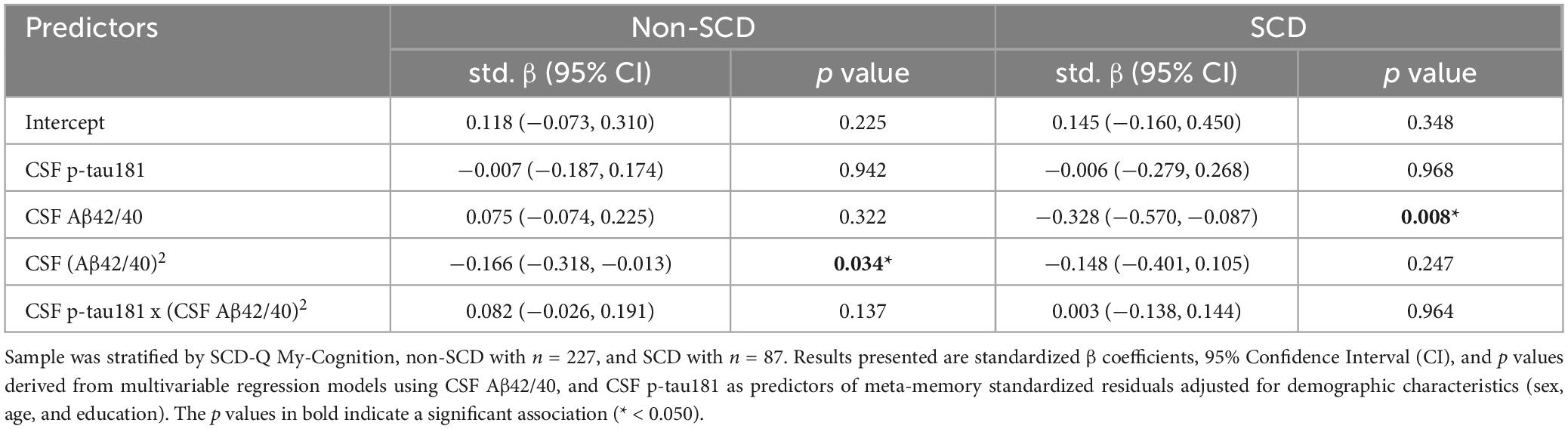
Table 4. Subjective cognitive decline (SCD) stratification: CSF biomarkers associated with meta-memory standardized residuals.
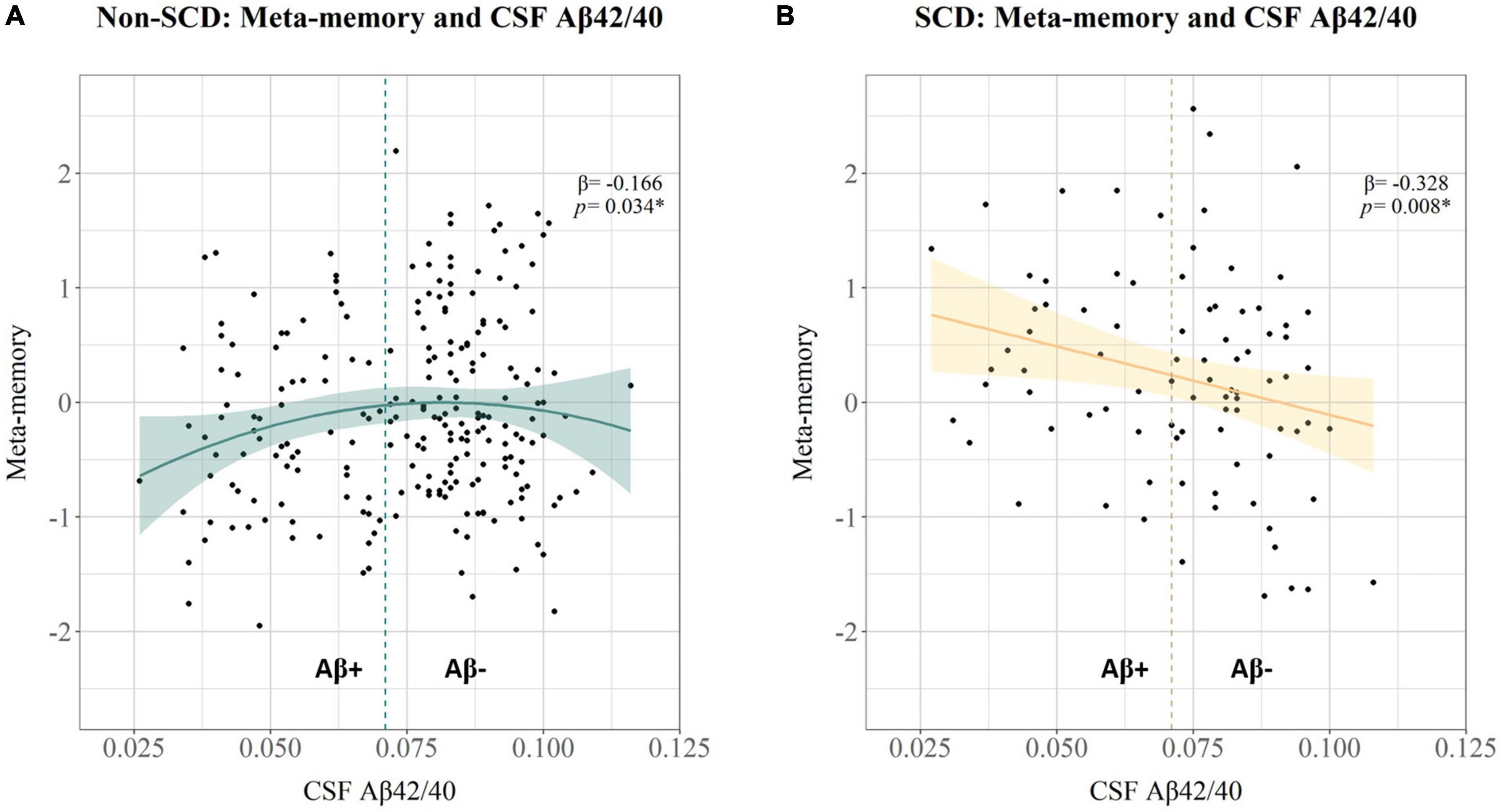
Figure 2. Scatter plots showing the relationship between CSF Aβ42/40 on the X-axis, and meta-memory standardized residual scores adjusted for demographic effects on the Y-axis, for (A) the subset of non-SCD, and (B) the subset of SCD. The vertical dashed lines at x = 0.0071 represent the positivity threshold for CSF Aβ42/40. Standardized β coefficient and p value for the quadratic (A) and linear (B) associations between CSF Aβ42/40 and meta-memory standardized residuals, respectively, are shown in the top-right side of each plot.
To further explore the contribution of dyadic SCD reports, in this section we considered exclusively the subset of participants with study partner’s SCD (3.82%). Within this subset, seven individuals (58 %) were defined as unaware decliners (non-SCD & study partner’s SCD), and five individuals (42 %) were defined as aware decliners (SCD & study partner’s SCD). For each group, meta-memory standardized residuals were evaluated using Spearman correlation matrices with CSF Aβ42/40, and CSF p-tau181. In the group of unaware decliners, meta-memory was significantly correlated with CSF p-tau181 (r = −0.857, p = 0.024), but not with CSF Aβ42/40 (r = 0.571, p = 0.200). Within the group of aware decliners, meta-memory was correlated at the trend level with CSF p-tau181 (r = −0.900, p = 0.083), but not with CSF Aβ42/40 (r = −0.500, p = 0.450).
The sensitivity analysis evaluated the effect of APOE-ε4 status and psychiatric symptoms in these associations. We incorporated APOE-ε4 status in a multivariable regression model (see Supplementary Table 1). While APOE-ε4 status was not associated with meta-memory, the effect of the quadratic term of CSF Aβ42/40 remained significant in the model (β = −0.151, p = 0.025). We incorporated anxiety and depression sub-scores from the HADS in multivariable regression models (see Supplementary Table 2). Although higher levels of anxiety were significantly associated with increased meta-memory (β = 0.131, p = 0.032), the effect of the quadratic term of CSF Aβ42/40 remained significant in the model (β = −0.142, p = 0.033). On the other hand, higher levels of depression were associated, now at the trend level, with increased meta-memory (β = 0.100, p = 0.082) while the effect of the quadratic term of CSF Aβ42/40 remained significant in the model (β = −0.134, p = 0.047).
This cross-sectional observational research evaluated the association between core CSF AD biomarkers and the awareness of episodic memory performance, further exploring the role of SCD in these associations at the preclinical stage of the Alzheimer’s continuum. In the whole sample of participants, main results indicated that CSF Aβ42/40 was associated with meta-memory performance, following a non-linear pattern where higher Aβ burden was associated with both increased awareness (i.e. hypernosognosia) and decreased awareness (i.e. anosognosia) of episodic memory. This relationship showed an inverted U-shaped with the inflexion point approximately aligned with the Aβ-positivity cutoff. Therefore, these results are consistent with prior evidence suggesting that non-linear dynamic changes in meta-memory might be associated with Aβ-deposition in preclinical-AD (Vannini et al., 2017a; Gagliardi et al., 2020).
The present research hypothesized that, at very early stages in the preclinical Alzheimer’s continuum, two distinct types of metacognitive profiles at risk of AD-related decline could be delineated:
(I) Hypernosognosia: Individuals with a sub-estimation of actual memory performance, along with an increased awareness in relationship to AD-neuropathology. This increase in awareness is expected to anticipate gradual meta-cognitive decline with further disease progression.
(II) Anosognosia: Individuals with an over-estimation of actual memory performance, along with decreased awareness in relationship to AD-neuropathology. This decrease in awareness is expected to anticipate substantial meta-cognitive decline with further disease progression, and is, therefore, suggestive of greater risk of Alzheimer’s severity.
Our findings support the existence of these two groups, indicating that distinct meta-cognitive profiles may emerge in preclinical-AD. On the one hand, results in the non-SCD subset showed a non-linear association between Aβ and meta-memory, similar to the relationship found in the whole sample, with increased awareness up to Aβ-positivity, and decreased awareness beyond this threshold. On the other hand, results in the SCD subset showed a linear association between Aβ and meta-memory, with higher Aβ-pathology associated with increased awareness. These results suggested that while some individuals might notice subtle cognitive changes (SCD) associated with the entrance in the AD continuum (defined by the Aβ-positivity threshold), others may not be fully aware of these subtle changes (non-SCD). Although these groups differ in SCD status, both support meta-cognitive profile (I) hypernosognosia, showing sub-estimation of actual memory performance associated linearly and non-linearly, respectively, with Aβ-pathology.
Besides, we explored the contribution of the study partner’s SCD. On the one side, the group of unaware decliners, those individuals presenting only study partner’s SCD, revealed a distinct pathological link with meta-memory performance, showing that increased levels of CSF p-tau181 (i.e., higher pathology) correlated with lower meta-memory performance. On the other side, the group of aware decliners, those individuals presenting study partner’s SCD but now in agreement with self-reported SCD, revealed a similar link with meta-memory performance: showing that increased CSF p-tau181 was correlated, at the trend level, with decreased meta-memory. Despite the small sample size, these results rapidly suggested that the absence of SCD should not be taken as guarantee of cognitive stability. Indeed, both unaware and aware decliners exhibited a similar relationship between CSF p-tau181 and meta-memory performance. Although these groups also differ in SCD status, both support meta-cognitive profile (II) anosognosia, showing over-estimation of actual memory performance in linear relationship to higher tau-pathology.
In the present research, we proposed that both hypernosognosia and anosognosia, as inter-individual meta-cognitive profiles, can be identified, providing relevant information to enhance the characterization of the preclinical stage in the Alzheimer’s continuum. These meta-cognitive profiles were described with distinct methods used to define awareness of cognitive function (objective-subjective discrepancy, participant self-report, participant-partner discrepancy), capturing in turn, distinct features of the actual cognitive state of an individual. We showed that these features can be combined to enhance clinical characterization. To contextualize this observation, we acknowledge that the co-occurrence of SCD with low awareness, or vice versa, might seem contradictory. However, it serves to increase the true dimensionality, as it has already been documented in the literature. Indeed, previous studies have already informed that low awareness can coexist together with SCD in the same individual, in line with our findings showing that some individuals reported cognitive complaints but still over-estimated their actual performance, which in turn reveals under-estimation of deficit severity (Cacciamani et al., 2017, 2020, 2021). Reduced awareness into the degree of deficit severity, even in the presence of reports of cognitive decline, is already indicative of anosognosia, presented here as a negative discrepancy in objective-subjective performance. Following this same reasoning, the participant-partner discrepancy in SCD that defined the group of unaware decliners contributed to disentangle an over-estimation of actual memory performance in relation to higher levels of tau-pathology. These results suggested that some individuals might be overlooked with the use of actual diagnostic criteria simply because they do not report cognitive complaints. The present research is consistent with previous evidence showing that just self-reported SCD alone, might be insufficient information, but incorporating the study partner’s SCD could be necessary to distinguish signs of decline that could go otherwise unnoticed (Miebach et al., 2019; Nosheny et al., 2022).
In consistency with these findings, our group has previously suggested that the presence of the study partner’s SCD, irrespective of self-reported SCD, was associated with lower left posterior hippocampal GM volume. Moreover, we previously found that the group of unaware decliners displayed lower performance in free memory recall and increased GM volume in medial frontal and insular brain areas, suggesting subtle neuronal disruption in cognitive control and self-referential processing (Sánchez-Benavides et al., 2018a). Currently, anosognosia is not fully recognized in MCI diagnosis, and consequently, as a function of the resources available to the clinician and the strategy used to evaluate awareness, individuals with a meaningful deficit of anosognosia might not fit within MCI criteria (Albert et al., 2011). The assessment of SCD is an important part of MCI diagnosis, but the “liberal” use of SCD (e.g., assuming that there is no possible lack of awareness prior to clinical onset) might contribute to misdiagnosis (Mitchell, 2008). Therefore, identifying a group at increased risk of AD-related impairment that might delay seeking for medical care is a matter of equity. In the next years, it is expected that effective treatments for AD will become available, and current research indicates that these treatments could be more effective at early stages in the AD continuum (Boxer and Sperling, 2023). Considering that decreased, but not increased awareness, reflects a greater risk of AD-related decline (Edmonds et al., 2014), improving our understanding of the pathological mechanisms behind anosognosia would provide useful methods and knowledge, from diagnosis to intervention, to close this equity gap.
We considered necessary to provide further explanation for the heterogeneous levels of awareness detected in preclinical-AD. Thus, we explored subthreshold symptoms of anxiety and depression, which are known to be possible manifestations associated with SCD and AD-progression (Jessen et al., 2014). Therefore, we modeled the relationship between CSF biomarkers, affective symptoms, and meta-memory as part of the sensitivity analysis. Higher anxiety was associated with increased awareness, and higher depression showed a trend in the same direction. The quadratic term of CSF Aβ42/40 remained significant in these models, indicating that affective symptoms partially overlapped with the effect of AD neuropathology in awareness, which is consistent with subtle manifestations emerging with underlying AD-progression (Donovan et al., 2018; Krell-Roesch et al., 2018). These results were in line with previous literature showing that subclinical levels of anxiety have been associated to a greater extent than those of depression with Aβ-pathology (Lewis et al., 2022).
Although non-linear changes in awareness across preclinical AD have already been suggested, we proposed that distinct levels of cognitive awareness shown by different individuals might be characterized considering inter-individual meta-cognitive profiles that can help to explain distinct intra-individual dynamics and corresponding trajectories. In the present research, we identified cross-sectionally these distinct profiles: while some individuals experience a heightened awareness of subtle cognitive decline (often leading them to report concerns and/or seek for medical advice), others can demonstrate a lack of insight across distinct dimensions of cognitive awareness (objective-subjective discrepancy in neuropsychological performance, and participant-partner discrepancy in SCD reports). Nevertheless, the rationale behind these distinct pathways to anosognosia is unknown. The literature shows that subtle meta-memory alterations in CU individuals have been associated with Aβ pathology in brain regions overlapping with areas involved in awareness and self-referential processing (Vannini et al., 2017a; Gagliardi et al., 2020). In amnestic MCI patients, greater anosognosia has been associated with reduced functional connectivity in cortical midline structures and reduced metabolism in the hippocampus and precuneus (Vannini et al., 2017b). Considering our results, it remains uncertain whether distinct these meta-cognitive profiles are fundamentally related to the progression of distinct AD neuropathology, as defined by independent contributions of Aβ and Tau pathologies, and/or related to patterns of pathological progression deviating from traditional schemes (Vogel et al., 2021; Collij et al., 2022).
Characterizing subtle meta-cognitive alterations might result challenging considering the underlying pathophysiological heterogeneity present in preclinical-AD cohorts and methodological differences across research settings (demographics, inclusion criteria, biomarker/cognitive measurements, etc.). These factors might contribute, to some extent, to explain the distinct associations between AD biomarkers and levels of awareness in preclinical-AD described in recent review (Cacciamani et al., 2021). The early anosognosic profile, unaware decliners, as defined by the participant-partner discrepancy in SCD, was quite infrequent in our sample (n = 7), but similar in sample size to the group of aware decliners (n = 5). Among participants presenting study partner’s SCD, some participants did not present awareness of cognitive decline, while other participants reported SCD in agreement with their partner (58–42% in our sample, respectively). Further development of methodology for defining this group at risk, might consider applying a cut-off in the objective-subjective discrepancy in neuropsychological performance to capture a larger group of individuals with similar performance characteristics, helping to understand better why some individuals might display a reduced awareness of cognitive function from very early stages. Clearly, longitudinal research needs to account for the characterization of this early anosognosic trajectory and its pathological correlates (in preparation).
A key feature of this research was to account for a sample of relatively young participants, with a mean age of 60 years old, showing a high contrast with most of studies in the field of preclinical-AD, with mean ages around 75. Moreover, the ALFA+ cohort study is mainly composed of early biomarker profiles in the Alzheimer’s continuum (A-T-/A+T-) and further enriched by risk factors (AD parental history, and APOE-ε4 carriers). The ALFA+ study was designed as an observational prospective follow-up of cognitively healthy middle-aged volunteers at increased risk of AD dementia. Therefore, the report of SCD was obtained on request rather than inclusion criteria. The first and only study to date that has directly modeled meta-memory performance as a function of the non-linear effect of Aβ-PET in CU individuals was performed in the context of SCD samples. In the present study we replicated the non-linear association previously described by Gagliardi et al. (2020) between Aβ and meta-memory, but now considering CSF biomarkers and a broader spectrum of population (only the 27% of the present sample in the ALFA+ cohort presented SCD). Since CSF Aβ levels are expected to change slightly before amyloid PET imaging, using fluid biomarkers, the present research was focused at the very early stages of the preclinical Alzheimer’s continuum (Jack et al., 2013).
The present research presented some limitations, as shown by the distribution of AT profiles, the levels of AD pathology were considered from modest to low. We acknowledge that only 23 (7.32%) individuals were classified as A+T+, currently falling within the profile of AD, and this might have obscured some latent relationships between the awareness of cognitive function and the levels of CSF p-tau181, which reflects greater symptom severity than CSF Aβ42/40 does with further disease progression. Other limitations relate to possible confounders, previous research identified that education levels were associated with meta-cognitive performance, but the ALFA+ cohort is mainly composed of highly educated individuals and our results did not yield any significant association with education. A group of interest, namely the unaware decliners, was also very limited in sample size, as previously stated, restricting the use of inferential statistics. Additionally, the report of study partner’s SCD might be influenced by several factors like age, sex, education, and the participant-informant relationship. Similarly, other relevant factors not accounted for in these analyses, such as personality traits related to mental stability (neuroticism, openness, etc.), together with cultural aspects, might contribute to explain distinct levels of awareness of cognitive function. Finally, we have used very sensitive cut-offs in the ALFA+ cohort study for the AT(N) classification system (Milà-Alomà et al., 2020). Therefore, we acknowledge that using more liberal cut-offs for classifying pathological status, or other methods such as PET imaging, might lead to distinct results.
This research suggested that distinct meta-cognitive profiles can be identified at the preclinical stage of the Alzheimer’s continuum. While most individuals might experience an increased awareness associated with the entrance in the AD continuum (i.e., hypernosognosia), some others might be already losing awareness (i.e., anosognosia). Reduced awareness of cognitive function at preclinical stages of AD might currently be overlooked, leading to the omission of some individuals at higher risk of cognitive decline who may not be considered in prevention studies. This research suggested that further characterization of these meta-cognitive profiles might enhance preclinical stage identification, providing insights into the likelihood of clinical progression from the very early stages in the Alzheimer’s continuum.
The data that support the findings of this study are available from the corresponding co-authors, OG-R and GS-B, upon reasonable request.
The studies involving humans were approved in the ALFA+ study (ALFA-FPM-0311) by the independent Ethics Committee “Parc de Salut Mar,” Barcelona, and registered at Clinicaltrials.gov (identifier: NCT02485730). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
DL-M: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Software, Visualization, Writing – original draft, Writing – review and editing. MS-C: Funding acquisition, Resources, Writing – review and editing. MM-A: Writing – review and editing. JG: Funding acquisition, Resources, Writing – review and editing. CM: Project administration, Resources, Writing – review and editing. CQ-R: Resources, Writing – review and editing. GK: Resources, Writing – review and editing. HZ: Resources, Writing – review and editing. KB: Resources, Writing – review and editing. OG-R: Conceptualization, Funding acquisition, Investigation, Project administration, Resources, Supervision, Writing – review and editing, Formal analysis, Methodology, Validation, Visualization. GS-B: Funding acquisition, Investigation, Project administration, Resources, Supervision, Writing – review and editing, Conceptualization, Formal analysis, Methodology, Validation, Visualization.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The design and execution of the study were independent of any influence from funding sources. This includes data collection, analysis, interpretation, manuscript preparation, review, and approval. The research leading to these results has received funding from “la Caixa” Foundation (ID 100010434), under agreement LCF/PR/GN17/50300004, the Alzheimer’s Association, and an international anonymous charity foundation through the TriBEKa Imaging Platform project (TriBEKa-17-519007). Additional support has been received from the Universities and Research Secretariat, Ministry of Business and Knowledge of the Catalan Government under the grant no. 2021 SGR 00913. DL-M was supported by Instituto de Salud Carlos III through the project PI19/00117 (Co-funded by European Regional Development Fund/European Social Fund “A way to make Europe”/”Investing in your future”). MS-C receives funding from the European Research Council (ERC) under the European Union’s Horizon 2020 research and innovation programme (Grant agreement No. 948677); ERA PerMed (ERAPERMED2021-184); Project “PI19/00155” and “PI22/00456, funded by Instituto de Salud Carlos III (ISCIII) and co-funded by the European Union; and from a fellowship from “la Caixa” Foundation (ID 100010434) and from the European Union’s Horizon 2020 research and innovation programme under the Marie Skłodowska-Curie grant agreement No 847648 (LCF/BQ/PR21/11840004). JG receives funding from the European Comission Innovative Health Initiative (Grant Agreement: 101112145), the BrightFocus Foundation (Grant Reference ID: A2022034S), and La Marató de TV3 (Project: 202318 30-31-32). HZ was a Wallenberg Scholar and a Distinguished Professor at the Swedish Research Council supported by grants from the Swedish Research Council (#2023-00356; #2022-01018 and #2019-02397), the European Union’s Horizon Europe research and innovation programme under grant agreement No 101053962, Swedish State Support for Clinical Research (#ALFGBG-71320), the Alzheimer Drug Discovery Foundation (ADDF), USA (#201809-2016862), the AD Strategic Fund and the Alzheimer’s Association (#ADSF-21-831376-C, #ADSF-21-831381-C, #ADSF-21-831377-C, and #ADSF-24-1284328-C), the Bluefield Project, Cure Alzheimer’s Fund, the Olav Thon Foundation, the Erling-Persson Family Foundation, Stiftelsen för Gamla Tjänarinnor, Hjärnfonden, Sweden (#FO2022-0270), the European Union’s Horizon 2020 research and innovation programme under the Marie Skłodowska-Curie grant agreement No 860197 (MIRIADE), the European Union Joint Programme – Neurodegenerative Disease Research (JPND2021-00694), the National Institute for Health and Care Research University College London Hospitals Biomedical Research Centre, and the UK Dementia Research Institute at UCL (UKDRI-1003). KB was supported by the Swedish Research Council (#2017-00915 and #2022-00732), the Swedish Alzheimer Foundation (#AF-930351, #AF-939721 and #AF-968270), Hjärnfonden, Sweden (#FO2017-0243 and #ALZ2022-0006), the Swedish state under the agreement between the Swedish government and the County Councils, the ALF-agreement (#ALFGBG-715986 and #ALFGBG-965240), the European Union Joint Program for Neurodegenerative Disorders (JPND2019-466-236), the Alzheimer’s Association 2021 Zenith Award (ZEN-21-848495), and the Alzheimer’s Association 2022-2025 Grant (SG-23-1038904 QC). OG-R was supported by the Spanish Ministry of Science and Innovation –State Research Agency (IJC2020-043417-I/MCIN/AEI/10.13039/501100011033) and the European Union laquoNextGenerationEUraquo/PRTR. GS-B was supported by the Agencia Estatal de Investigación AEI/10.13039/501100011033 through the project PID2020-119556RA-I00 and Instituto de Salud Carlos III (ISCIII) through the project CP23/00039 (Miguel Servet contract), co-funded by the European Union (FSE+).
This publication is part of the ALFA study (ALzheimer and FAmilies). We would like to express their most sincere gratitude to the ALFA project participants and relatives without whom this research would have not been possible. We thank Roche Diagnostics International Ltd for providing the kits to measure CSF biomarkers, and the laboratory technicians at the Clinical Neurochemistry Lab in Mölndal, Sweden, who performed the analyses.
GS-B worked as a consultant for Roche Farma, S.A. MS-C has given lectures in symposia sponsored by Almirall, Eli Lilly, Novo Nordisk, Roche Diagnostics, and Roche Farma; received consultancy fees (paid to the institution) from Roche Diagnostics; and served on advisory boards of Roche Diagnostics and Grifols. He was granted a project and is a site investigator of a clinical trial (funded to the institution) by Roche Diagnostics. In-kind support for research (to the institution) was received from ADx Neurosciences, Alamar Biosciences, Avid Radiopharmaceuticals, Eli Lilly, Fujirebio, Janssen Research & Development, and Roche Diagnostics. JDG has received research support from GE HealthCare, Roche Diagnostics, Hoffman – La Roche, spearer/consultant fees from Biogen, Philips Nederlands, Roche Diagnostics and Life-Molecular Imaging, and serves in the Molecular Neuroimaging Advisory Board of Prothena Biosciences. HZ has served at scientific advisory boards and/or as a consultant for Abbvie, Acumen, Alector, Alzinova, ALZPath, Amylyx, Annexon, Apellis, Artery Therapeutics, AZTherapies, Cognito Therapeutics, CogRx, Denali, Eisai, Merry Life, Nervgen, Novo Nordisk, Optoceutics, Passage Bio, Pinteon Therapeutics, Prothena, Red Abbey Labs, reMYND, Roche, Samumed, Siemens Healthineers, Triplet Therapeutics, and Wave, has given lectures in symposia sponsored by Alzecure, Biogen, Cellectricon, Fujirebio, Lilly, Novo Nordisk, and Roche, and is a co-founder of Brain Biomarker Solutions in Gothenburg AB (BBS), which is a part of the GU Ventures Incubator Program (outside submitted work). KB has served as a consultant and at advisory boards for Acumen, ALZPath, BioArctic, Biogen, Eisai, Lilly, Moleac Pte. Ltd, Novartis, Ono Pharma, Prothena, Roche Diagnostics, and Siemens Healthineers; has served at data monitoring committees for Julius Clinical and Novartis; has given lectures, produced educational materials and participated in educational programs for AC Immune, Biogen, Celdara Medical, Eisai and Roche Diagnostics; and is a co-founder of Brain Biomarker Solutions in Gothenburg AB (BBS), which is a part of the GU Ventures Incubator Program, outside the work presented in this manuscript. OG-R receives research funding from Roche Pharma. GK was a full-time employee of Roche Diagnostics GmbH, Penzberg, Germany. CQ-R was a full-time employee of Roche Diagnostics International Ltd, Rotkreuz, Switzerland. The rest of coauthors have nothing to disclose. COBAS and ELECSYS are trademarks of Roche. The NeuroToolKit is a panel of exploratory prototype assays designed to robustly evaluate biomarkers associated with key pathologic events characteristic of AD and other neurological disorders, used for research purposes only and not approved for clinical use (Roche Diagnostics International Ltd, Rotkreuz, Switzerland). Elecsys Phospho-Tau (181P) CSF and Elecsys Total-Tau CSF assays are approved for clinical use. All other product names and trademarks are the property of their respective owners.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnagi.2024.1394460/full#supplementary-material
Akinci, M., Sánchez-Benavides, G., Brugulat-Serrat, A., Peña-Gómez, C., Palpatzis, E., Shekari, M., et al. (2022). Subjective cognitive decline and anxious/depressive symptoms during the COVID-19 pandemic: What is the role of stress perception, stress resilience, and β-amyloid? Alzheimers Res. Ther. 14:126. doi: 10.1186/s13195-022-01068-7
Albert, M. S., DeKosky, S. T., Dickson, D., Dubois, B., Feldman, H. H., Fox, N. C., et al. (2011). The diagnosis of mild cognitive impairment due to Alzheimer’s disease: Recommendations from the national institute on aging-Alzheimer’s association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 7, 270–279. doi: 10.1016/j.jalz.2011.03.008
Boxer, A. L., and Sperling, R. (2023). Accelerating Alzheimer’s therapeutic development: The past and future of clinical trials. Cell 186, 4757–4772. doi: 10.1016/j.cell.2023.09.023
Busche, M. A., and Hyman, B. T. (2020). Synergy between amyloid-β and Tau in Alzheimer’s disease. Nat. Neurosci. 23, 1183–1193. doi: 10.1038/s41593-020-0687-6
Buschke, H. (2013). Dementia and memory, eds N. Lars-Göran and N. Ohta (London: Psychology Press), doi: 10.4324/9781315851730
Cacciamani, F., Houot, M., Gagliardi, G., Dubois, B., Sikkes, S., ánchez-Benavides, G. S., et al. (2021). Awareness of cognitive decline in patients with Alzheimer’s disease: A systematic review and meta-analysis. Front. Aging Neurosci. 13:697234. doi: 10.3389/fnagi.2021.697234
Cacciamani, F., Sambati, L., Houot, M., Habert, M. O., Dubois, B., Epelbaum, S., et al. (2020). Awareness of cognitive decline trajectories in asymptomatic individuals at risk for AD. Alzheimers Res. Ther. 12:129. doi: 10.1186/s13195-020-00700-8
Cacciamani, F., Tandetnik, C., Gagliardi, G., Bertin, H., Habert, M. O., Hampel, H., et al. (2017). Low Cognitive awareness, but not complaint, is a good marker of preclinical Alzheimer’s disease. J. Alzheimers Dis. 59, 753–762. doi: 10.3233/JAD-170399
Collij, L. E., Salvadó, G., Wottschel, V., Mastenbroek, S. E., Schoenmakers, P., Heeman, F., et al. (2022). Spatial-temporal patterns of β-amyloid accumulation: A subtype and stage inference model analysis. Neurology 98, E1692–E1703. doi: 10.1212/WNL.0000000000200148
Donovan, N. J., Locascio, J. J., Marshall, G. A., Gatchel, J., Hanseeuw, B. J., Rentz, D. M., et al. (2018). Longitudinal association of amyloid beta and anxious-depressive symptoms in cognitively normal older adults. Am. J. Psychiatry 175, 530–537. doi: 10.1176/appi.ajp.2017.17040442
Edmonds, E. C., Delano-Wood, L., Galasko, D. R., Salmon, D. P., and Bondi, M. W. (2014). Subjective Cognitive complaints contribute to misdiagnosis of mild cognitive impairment. J. Int. Neuropsychol. Soc. 20, 836–847. doi: 10.1017/S135561771400068X
Gagliardi, G., Houot, M., Cacciamani, F., Habert, M. O., Dubois, B., Epelbaum, S., et al. (2020). The meta-memory ratio: A new cohort-independent way to measure cognitive awareness in asymptomatic individuals at risk for Alzheimer’s disease. Alzheimers Res. Ther. 12:57. doi: 10.1186/s13195-020-00626-1
Gramunt, N., Sánchez-Benavides, G., Buschke, H., Diéguez-Vide, F., Peña-Casanova, J., Masramon, X., et al. (2016). The memory binding test: Development of two alternate forms into Spanish and Catalan. J. Alzheimers Dis. 52, 283–293. doi: 10.3233/JAD-151175
Grober, E., Buschke, H., and Korey, S. R. (1987). Genuine memory deficits in dementia. Dev. Neuropsychol. 3, 13–36. doi: 10.1080/87565648709540361
Grober, E., Hall, C. B., Lipton, R. B., Zonderman, A. B., Resnick, S. M., and Kawas, C. (2008). Memory impairment, executive dysfunction, and intellectual decline in preclinical Alzheimer’s disease. J. Int. Neuropsychol. Soc. 14, 266–278. doi: 10.1017/S1355617708080302
Grober, E., Petersen, K. K., Lipton, R. B., Hassenstab, J., Morris, J. C., Gordon, B. A., et al. (2023). Association of stages of objective memory impairment with incident symptomatic cognitive impairment in cognitively normal individuals. Neurology 100, E2279–E2289. doi: 10.1212/WNL.0000000000207276
Hanseeuw, B. J., Jonas, V., Jackson, J., Betensky, R. A., Rentz, D. M., Johnson, K. A., et al. (2020a). Association of anxiety with subcortical amyloidosis in cognitively normal older adults. Mol. Psychiatry 25, 2599–2607. doi: 10.1038/s41380-018-0214-2
Hanseeuw, B. J., Scott, M. R., Sikkes, S. A. M., Properzi, M., Gatchel, J. R., Salmon, E., et al. (2020b). Evolution of anosognosia in Alzheimer’s disease and its relationship to amyloid. Ann. Neurol. 87, 267–280. doi: 10.1002/ana.25649
Hill, N. L., Mogle, J., Wion, R., Munoz, E., DePasquale, N., Yevchak, A. M., et al. (2016). Subjective cognitive impairment and affective symptoms: A systematic review. Gerontologist. Gerontol. Soc. Am. 56, e109–e127. doi: 10.1093/geront/gnw091
Horning, S. M., Melrose, R., and Sultzer, D. (2014). Insight in Alzheimer’s disease and its relation to psychiatric and behavioral disturbances. Int. J. Geriatr. Psychiatry 29, 77–84. doi: 10.1002/gps.3972
Jack, C. R., Bennett, D. A., Blennow, K., Carrillo, M. C., Dunn, B., Haeberlein, S. B., et al. (2018). NIA-AA research framework: Toward a biological definition of Alzheimer’s disease. Alzheimers Dement. 14, 535–562. doi: 10.1016/j.jalz.2018.02.018
Jack, C. R., Knopman, D. S., Jagust, W. J., Petersen, R. C., Weiner, M. W., Aisen, P. S., et al. (2013). Tracking pathophysiological processes in Alzheimer’s disease: An updated hypothetical model of dynamic biomarkers. Lancet Neurol. 12, 207–216. doi: 10.1016/S1474-4422(12)70291-0
Jenkins, A., Tree, J., and Tales, A. (2021). Distinct profile differences in subjective cognitive decline in the general public are associated with metacognition, negative affective symptoms, neuroticism, stress, and poor quality of life. J. Alzheimers Dis. 80, 1231–1242. doi: 10.3233/JAD-200882
Jessen, F., Amariglio, R. E., van Boxtel, M., Breteler, M., Ceccaldi, M., Chételat, G., et al. (2014). A conceptual framework for research on subjective cognitive decline in preclinical Alzheimer’s disease. Alzheimers Dement. 10, 844–852. doi: 10.1016/j.jalz.2014.01.001
Jessen, Frank, Rebecca, E., Amariglio, Rachel, F., and Buckley, et al. (2020). The characterisation of subjective cognitive decline. Lancet Neurol. 19, 271–278. doi: 10.1016/S1474-4422(19)30368-0
Krell-Roesch, J., Lowe, V. J., Neureiter, J., Pink, A., Roberts, R. O., Mielke, M. M., et al. (2018). Depressive and anxiety symptoms and cortical amyloid deposition among cognitively normal elderly persons: The mayo clinic study of aging. Int. Psychogeriatr. 30, 245–251. doi: 10.1017/S1041610217002368
Lewis, C. K., Bernstein, O. M., Grill, J. D., Gillen, D. L., and Sultzer, D. L. (2022). Anxiety and depressive symptoms and cortical amyloid-β burden in cognitively unimpaired older adults. J. Prev. Alzheimers Dis. 9, 286–296. doi: 10.14283/jpad.2022.13
Liew, T. M. (2020). Subjective cognitive decline, anxiety symptoms, and the risk of mild cognitive impairment and dementia. Alzheimers Res. Ther. 12:107. doi: 10.1186/s13195-020-00673-8
McGlynn, S. M., and Schacter, D. L. (1989). Unawareness of deficits in neuropsychological syndromes. J. Clin. Exp. Neuropsychol. 11, 143–205. doi: 10.1080/01688638908400882
Miebach, L., Wolfsgruber, S., Polcher, A., Peters, O., Menne, F., Luther, K., et al. (2019). Which features of subjective cognitive decline are related to amyloid pathology? Findings from the DELCODE study. Alzheimers Res. Ther. 11:66. doi: 10.1186/s13195-019-0515-y
Milà-Alomà, M., Salvadó, G., Gispert, J. D., Vilor-Tejedor, N., Grau-Rivera, O., Sala-Vila, A., et al. (2020). Amyloid beta, tau, synaptic, neurodegeneration, and glial biomarkers in the preclinical stage of the Alzheimer’s continuum. Alzheimers Dement. 16, 1358–1371. doi: 10.1002/alz.12131
Mimmack, K. J., Gagliardi, G. P., Marshall, G. A., and Vannini, P. (2023). Measurement of dimensions of self-awareness of memory function and their association with clinical progression in cognitively normal older adults. JAMA Netw. Open 6:e239964. doi: 10.1001/jamanetworkopen.2023.9964
Mitchell, A. J. (2008). Is it time to separate subjective cognitive complaints from the diagnosis of mild cognitive impairment? Age Ageing 37, 497–499. doi: 10.1093/ageing/afn147
Mitchell, A. J., Beaumont, H., Ferguson, D., Yadegarfar, M., and Stubbs, B. (2014). Risk of dementia and mild cognitive impairment in older people with subjective memory complaints: Meta-analysis. Acta Psychiatr. Scand. 130, 439–451. doi: 10.1111/acps.12336
Molinuevo, J. L., Gramunt, N., Gispert, J. D., Fauria, K., Esteller, M., Minguillon, C., et al. (2016). The ALFA project: A research platform to identify early pathophysiological features of Alzheimer’s disease. Alzheimers Dement. 2, 82–92. doi: 10.1016/j.trci.2016.02.003
Nosheny, R. L., Amariglio, R., Sikkes, S. A. M., Van Hulle, C., Bicalho, M. A. C., Dowling, N. M., et al. (2022). The role of dyadic cognitive report and subjective cognitive decline in early ADRD clinical research and trials: Current knowledge, gaps, and recommendations. Alzheimers Dement. Transl. Res. Clin. Interv. 8:e12357. doi: 10.1002/trc2.12357
Rami, L., Mollica, M. A., Garcfa-Sanchez, C., Saldafia, J., Sanchez, B., Sala, I., et al. (2014). The subjective cognitive decline questionnaire (SCD-Q): A validation study. J. Alzheimers Dis. 41, 453–466. doi: 10.3233/JAD-132027
Sánchez-Benavides, G., Grau-Rivera, O., Cacciaglia, R., Suárez-Calvet, M., Falcon, C., Minguillon, C., et al. (2018a). Distinct cognitive and brain morphological features in healthy subjects unaware of informant-reported cognitive decline. J. Alzheimers Dis. 65, 181–191. doi: 10.3233/JAD-180378
Sánchez-Benavides, G., Grau-Rivera, O., Suárez-Calvet, M., Minguillon, C., Cacciaglia, R., Gramunt, N., et al. (2018b). Brain and cognitive correlates of subjective cognitive decline-plus features in a population-based cohort. Alzheimers Res. Ther. 10:123. doi: 10.1186/s13195-018-0449-9
Sánchez-Benavides, G., Suárez-Calvet, M., Milà-Alomà, M., Arenaza-Urquijo, E. M., Grau-Rivera, O., Operto, G., et al. (2021). Amyloid-β positive individuals with subjective cognitive decline present increased CSF neurofilament light levels that relate to lower hippocampal volume. Neurobiol. Aging 104, 24–31. doi: 10.1016/j.neurobiolaging.2021.02.026
Schacter, D. L. (1990). Toward a cognitive neuropsychology of awareness: Implicit knowledge and anosognosia. J. Clin. Exp. Neuropsychol. 12, 155–178. doi: 10.1080/01688639008400962
Schacter, D. L. (1992). Consciousness and awareness in memory and amnesia: Critical issues. Neuropsychol. Consciousness 45, 179–200. doi: 10.1016/B978-0-12-498045-7.50014-1
Starkstein, S. E. (2014). Anosognosia in Alzheimer’s disease: Diagnosis, frequency, mechanism and clinical correlates. Cortex 61, 64–73. doi: 10.1016/j.cortex.2014.07.019
Starkstein, S. E., Jorge, R., Mizrahi, R., and Robinson, R. G. (2006). A diagnostic formulation for anosognosia in Alzheimer’s disease. J. Neurol. Neurosurg. Psychiatry 77, 719–725. doi: 10.1136/jnnp.2005.085373
Sunderaraman, P., and Cosentino, S. (2017). Integrating the constructs of anosognosia and metacognition: A review of recent findings in dementia. Curr. Neurol. Neurosci. Rep. 17:27. doi: 10.1007/s11910-017-0734-1
Teunissen, C. E., Tumani, H., Engelborghs, S., and Mollenhauer, B. (2014). Biobanking of CSF: International standardization to optimize biomarker development. Clin. Biochem. 47, 288–292. doi: 10.1016/j.clinbiochem.2013.12.024
Vannini, P., Amariglio, R., Hanseeuw, B., Johnson, K. A., McLaren, D. G., Chhatwal, J., et al. (2017a). Memory self-awareness in the preclinical and prodromal stages of Alzheimer’s disease. Neuropsychologia 99, 343–349. doi: 10.1016/j.neuropsychologia.2017.04.002
Vannini, P., Hanseeuw, B., Munro, C. E., Amariglio, R. E., Marshall, G. A., Rentz, D. M., et al. (2017b). Anosognosia for memory deficits in mild cognitive impairment: Insight into the neural mechanism using functional and molecular imaging. Neuroimage Clin. 15, 408–414. doi: 10.1016/j.nicl.2017.05.020
Vogel, J. W., Young, A. L., Oxtoby, N. P., Smith, R., Ossenkoppele, R., Strandberg, O. T., et al. (2021). Four distinct trajectories of tau deposition identified in Alzheimer’s disease. Nat. Med. 27, 871–881. doi: 10.1038/s41591-021-01309-6
Keywords: Alzheimer’s disease, preclinical, awareness, episodic memory, biomarkers
Citation: López-Martos D, Suárez-Calvet M, Milà-Alomà M, Gispert DJ, Minguillon C, Quijano-Rubio C, Kollmorgen G, Zetterberg H, Blennow K, Grau-Rivera O and Sánchez-Benavides G (2024) Awareness of episodic memory and meta-cognitive profiles: associations with cerebrospinal fluid biomarkers at the preclinical stage of the Alzheimer’s continuum. Front. Aging Neurosci. 16:1394460. doi: 10.3389/fnagi.2024.1394460
Received: 01 March 2024; Accepted: 13 May 2024;
Published: 30 May 2024.
Edited by:
Patrizia Vannini, Brigham and Women’s Hospital and Harvard Medical School, United StatesReviewed by:
Valentina Bessi, University of Florence, ItalyCopyright © 2024 López-Martos, Suárez-Calvet, Milà-Alomà, Gispert, Minguillon, Quijano-Rubio, Kollmorgen, Zetterberg, Blennow, Grau-Rivera and Sánchez-Benavides. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Oriol Grau-Rivera, b2dyYXVAYmFyY2Vsb25hYmV0YS5vcmc=; Gonzalo Sánchez-Benavides, Z3NhbmNoZXpiQGJhcmNlbG9uYWJldGEub3Jn
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.