 Chunyi Zhou
Chunyi Zhou Chongming Yang
Chongming Yang Yating Ai1
Yating Ai1 Ailin Zhang
Ailin Zhang Yuncui Wang
Yuncui Wang Hui Hu
Hui Hu
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Aging Neurosci. , 13 February 2024
Sec. Alzheimer's Disease and Related Dementias
Volume 16 - 2024 | https://doi.org/10.3389/fnagi.2024.1349196
This article is part of the Research Topic Mild Cognitive Impairment: Influencing Factors and Intervention Effects View all 20 articles
Background: Olfactory testing is emerging as a potentially effective screening method for identifying mild cognitive impairment in the elderly population.
Objective: Olfactory impairment is comorbid with mild cognitive impairment (MCI) in older adults but is not well-documented in subdomains of either olfactory or subtypes of cognitive impairments in older adults. This meta-analysis was aimed at synthesizing the differentiated relationships with updated studies.
Methods: A systematic search was conducted in seven databases from their availability to April 2023. A total of 38 publications were included, including 3,828 MCI patients and 8,160 healthy older adults. Two investigators independently performed the literature review, quality assessment, and data extraction. The meta-analyses were conducted with Stata to estimate the average effects and causes of the heterogeneity.
Results: Compared to normal adults, MCI patients had severe impairments in olfactory function and severe deficits in specific domains of odor identification and discrimination. Olfactory impairment was more severe in patients with amnestic mild cognitive impairment than in patients with non-amnestic MCI. Diverse test instruments of olfactory function caused large heterogeneity in effect sizes.
Conclusion: Valid olfactory tests can be complementary tools for accurate screening of MCI in older adults.
Cumulative evidence showed that olfactory impairment is comorbid with mild cognitive impairment and Alzheimer’s disease, with their common underlying neurodamages in the brain (Rahayel et al., 2012; Roalf et al., 2017; Dong et al., 2022; Pusswald et al., 2023). Olfactory impairment occurs earlier than visual impairment in MCI patients (Hagemeier et al., 2016) and predicts AD onset better than hearing and vision (Olofsson et al., 2020). As MCI usually harbingers AD, screening olfactory impairment has been recommended as a supplemental tool for identifying MCI (Jak et al., 2009); however, its efficacy remained uncertain in subdomains of olfactory and cognitive impairments.
Different aspects of olfactory impairment appeared to predict cognitive functions differentially. Olfactory impairment has been measured by detecting the minimum amount of odor (detection threshold), identifying a specific odor from a given list (identification), differentiating between odors (discrimination), and memorizing an odor and then identifying it (memory; Hedner et al., 2010). Odor detection threshold relies on the peripheral structural functions of the olfactory system and basic perceptual processing (Sohrabi et al., 2012), as opposed to odor identification and discrimination that involve higher brain centers and complex olfactory information processing systems (Stevenson and Boakes, 2003). Odor identification impairment was found to coincide with tau-mediated neuronal damage and occur before memory impairment and clinical symptoms in the course of AD (Bathini et al., 2019).
Subtypes of cognitive impairment include non-amnestic mild cognitive impairment (naMCI) and amnestic MCI (aMCI), which may be associated with olfactory dysfunction differentially. naMCI is more likely to progress to AD-unrelated dementia, such as frontotemporal dementia (FTD) or dementia with Lewy bodies (DLB; Devanand et al., 2015), and some studies suggest that both may be accompanied by severe olfactory dysfunction (Vyhnalek et al., 2015). However, this conclusion is controversial, as there are opposing studies showing that olfactory dysfunction in FTD and DLB patients is minimal or even absent (Luzzi et al., 2007). Most aMCI cases progress to AD dementia, caused by the degeneration of the internal olfactory cortex and hippocampus, which affects the individual’s ability to identify odors (Vyhnalek et al., 2015; Roberts et al., 2016). While aMCI patients usually exhibit more severe olfactory impairment than naMCI patients (Quarmley et al., 2017), others show similar or indistinguishable degrees of olfactory impairment between the aMCI and naMCI subtypes (Roalf et al., 2017) and odor identification deficits (Devanand et al., 2010; Vyhnalek et al., 2015). What complicates the association of olfactory impairments with MCI is that olfactory deficits in odor detection threshold, identification, discrimination, and memory can coexist in MCI patients (Yap et al., 2022). In addition, odor detection thresholds decline in the normal elderly population as well, though faster than discrimination and identification (Hummel et al., 2007). It remained uncertain how reliable it is to use olfactory impairment tests as supplemental tools for identifying MCI.
Earlier meta-analyses investigating olfactory function in MCI and AD patients have not differentiated domains of olfactory impairments and MCI subtypes. For instance, Roalf’s meta-analysis found that olfactory function in MCI patients is slightly worse than that in the normal population (Roalf et al., 2017), but only a few studies included MCI subtypes. In addition, there was no statistically significant impairment of odor memory in MCI patients due to the small number of included studies. Jung’s meta-analysis showed that MCI patients have significant deficits in odor identification compared to AD patients (Jung et al., 2019) but this did not extend to odor discrimination and detection thresholds. Other studies did not consider the heterogeneity of demographics, Mini-Mental State Examination (MMSE) scores, and olfactory test instruments (Wang et al., 2018; Yang et al., 2022). These different approaches to synthesizing previous findings have not rendered differentiated efficacies of olfactory impairment tests for identifying MCI.
This meta-analysis was to synthesize studies that might reveal the differentiated relationships between olfactory impairments and MCI, with a focus mainly on the following issues: (1) domains of olfactory impairment in MCI patients, (2) olfactory function in two subtypes of MCI patients, and (3) differences caused by test instruments of olfactory function, etc. This updated study differs from previous ones in that strict inclusion–exclusion criteria were applied in the literature search, only higher-quality and recent studies were included, and the whole research process adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 statement that can be readily retrieved online (see Supplementary material).
The literature about olfactory function in MCI patients was searched in PubMed, Embase, the Cochrane Library, Web of Science, China Knowledge Network, Wanfang Data, and Vipul.com, within the time frame from their availability to April 2023. Using the Boolean logic for literature retrieval, the search strategy combined subject terms and free words without language restrictions as follows: “Cognitive Dysfunction” OR “Mild Cognitive Impairment” AND (“Smell” OR “Sense of Smell” OR “Olfaction” OR “Olfaction Disorders” OR “Olfaction Dysfunction” OR” Olfaction Impairment”) (see Supplementary material).
The inclusion and exclusion criteria for the studies complied with the requirements of the 2020 PRISMA. The inclusion criteria for this study were as follows: (a) The study subjects were MCI patients aged 50 years and older without co-morbidities or other neurodegenerative diseases. (b) There was a healthy population matched to the age of the MCI group as a control group. (c) The study subjects were MCI patients diagnosed by traditional methods. (d) The subjective olfactory function assessment was judged by the test subjects’ autonomous sniffing of odors. (e) The research design was a cohort or a case–control study.
Studies with the following characteristics were excluded from the meta-analysis: (a) the research reports omitted original effect sizes and the authors could not be contacted or provide them; (b) full reports could not be downloaded and accessed; (c) reports duplicated published data as determined by identical authors, study sites, participating institutions, details of olfactory tests, sample sizes, baseline situations, or study durations; (d) low-quality reports with a score of <7 on the Newcastle-Ottawa Scale (NOS) for assessing the quality of non-randomized studies.
Figure 1 depicts the literature search and selection process for this study. The initial search yielded 2,628 pieces of pertinent reports in total. After meticulous screening, 30 case–control studies and 8 cohort studies were finally selected, including 12 from North America, 17 from Asia, and 9 from Europe. This meta-analysis comprised 3,828 MCI patients and 8,160 healthy controls.
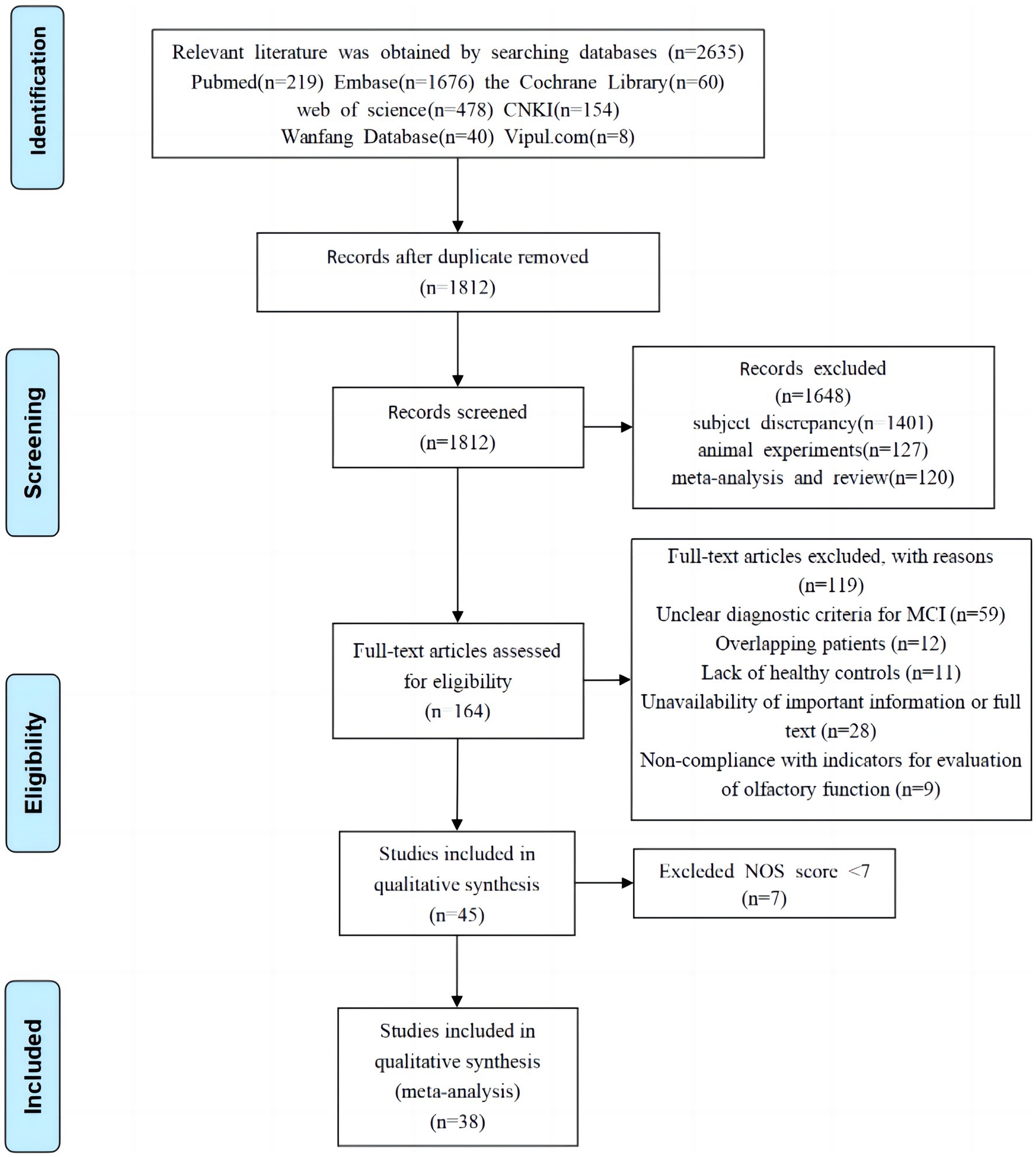
Figure 1. Flowchart of literature screening.
Data extraction and study quality evaluation were performed independently by two investigators of this study trained in evidence-based care according to the inclusion and exclusion criteria and cross-checked. A third investigator was requested to adjudicate any disagreement collaboratively. The extracted data included general information about the literature: title, year of publication, authors, country of study, type of study, sample size, age of participants in the control and MCI groups, olfactory function test instruments, and test scores of neuropsychological scales such as MMSE and MoCA. The quality of the included studies was evaluated using the NOS (Stang, 2010) and rated low (0–4 points), medium (5–6 points), or high (7–10 points). Only high-quality studies (scores ≥ 7) were included in this study. The literature was summarized and organized using Endnote X9 software, and data were extracted using Excel 2019. The fundamental characteristics and quality assessment of these studies are displayed in Table 1.
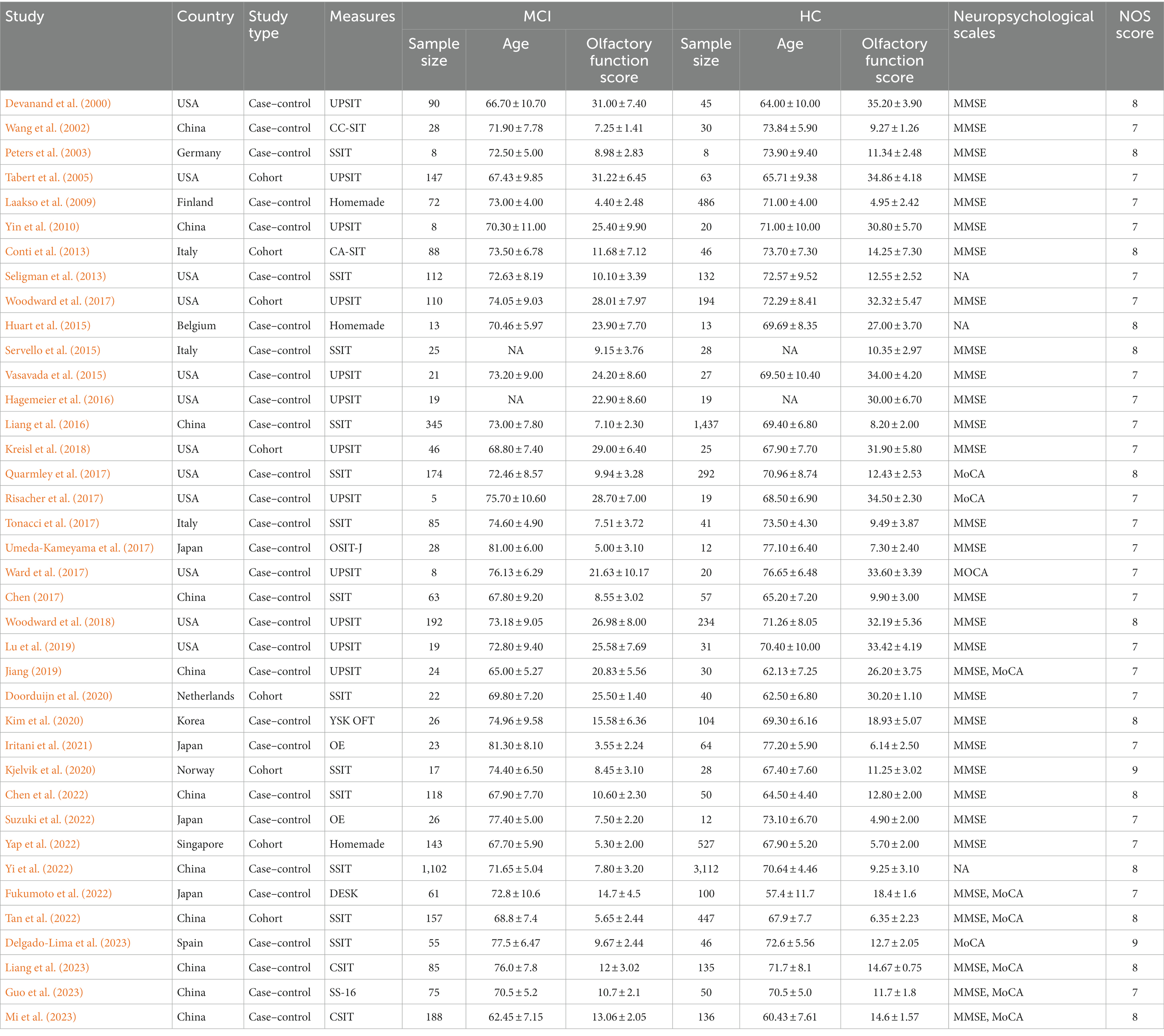
Table 1. Characteristics of the included studies.
The University of Pennsylvania Odor Identification Test (UPSIT) is a forced-choice odor identification assessment in which each subject is sequentially exposed to 40 odors and scores 1 point for each correctly identified odor (Doty et al., 1984).
The Sniffin’ Sticks Identification Test (SSIT) was developed in Germany to measure detection threshold, discrimination, and identification function (Hummel et al., 1997). Subjects were presented with 16 felt-tipped pens containing common household odors, requested to freely identify each with a verbal description, and scored one point for each correct identification.
The Japanese odor stick identification test (OSIT-J) is an identification tool to identify odors familiar to Japanese patients (Shino et al., 2006). Subjects were required to sniff out a target odor from four samples and choose “detectable but unrecognizable” or “no odor detected” (no score). A correct identification was scored 1 point.
The Open-Essence (OE) test is a similar card-based odor identification tool with 12 odors, designed to overcome the inconvenience of odor sample storage (Okutani et al., 2013).
The culturally adapted version of the odor identification test (CA-SIT) is an Italian culture-adapted version of the UPSIT, with six odors removed from the original, which can be easily misidentified by Italians (Doty et al., 1996) and scoring similar to the UPSIT.
The cross-cultural version of the olfactory identification test (CC-SIT) is a cross-cultural version of the UPSIT (Doty et al., 1996) that consists of 12 odors familiar to US, Chinese, French, and Japanese patients. One point was scored for each correct identification, up to a total of 12.
The YSK Olfactory Function Test is a Korean olfactory threshold test used for early screening for dementia in older adults (Kim et al., 2021). The tool consists of a series of kits, such as odorless distilled water as a blank stimulus and 10-step concentrations (0%–16%) of rose-scented 2-phenylethanol. Scores range from 1 to 7, with lower scores indicating higher olfactory thresholds.
The DEmentia Screening Kit (DESK) is an odor identification test tool developed for Japanese patients with dementia or AD (Fukumoto et al., 2022). The kit includes 10 odorants in 2 concentrations (weak/strong), for a total of 20 combinations. Two different concentrations of odors were tested separately with a paper cup each time and a 5-min interval between. Patients were requested to choose an answer from six alternatives to indicate whether they could identify an odor, and they scored 1 point for each correct odor identification.
The Chinese Smell Identification Test (CSIT) is an odor identification test developed by the Institute of Psychology of the Chinese Academy of Sciences in 2019 which contains 40 or 16 odors familiar to Chinese patients (Feng et al., 2019).
In addition, researchers of the three studies created “homemade tests” for participants to identify, discriminate, or detect odors. These could be as simple as small containers (e.g., jars or vials) filled with different scents (e.g., essential oils or spices) for the participants to smell and identify.
Data from the included studies were meta-analyzed using the statistical software Stata (v14). The group mean differences in olfactory function scores were converted to standardized mean differences (SMDs), which are also referred to as Cohen’s d to render differences commensurate across the studies (small ≤ 0.2, medium = 0.05, and large ≥ 0.8; Cohen, 1977). Medians and quartiles were converted to means and standard deviations using the methods of Luo et al. (2018) and Wan et al. (2014). Random effect models (REMs) were employed to estimate the average effect sizes and heterogeneity (I2) between studies (unavailable for a single study), whose sources were further explored through subgroup analyses and meta-regressions. I2 ≥ 50% and p ≤ 0.05 indicate high heterogeneity between studies and the necessity of REM. Sensitivity analysis was also conducted to detect the influence of individual studies on the average effect size. Egger’s test was used to examine the presence of publication bias, with a p-value of ≤0.05 indicating the presence.
The initial research yielded 2,635 pieces of pertinent literature in total. After meticulous screening, 30 case–control studies and 8 cohort studies, including 12 from North America, 17 from Asia, and 9 from Europe, were finally included. The final meta-analysis comprised 3,828 MCI patients and 8,160 healthy controls. Table 2 displays the fundamental characteristics as well as the quality assessment of the selected studies. The overall effect size obtained from a random effect model was SMD = −0.78, 95% CI: −0.89~−0.66, I2 = 81.3%.

Table 2. Meta-regression results.
Figure 2 presents the basic characteristics of the 38 included studies and SMD by certain potential moderators. First, SMD was −0.80 (95% CI: −0.92~−0.67, I2 = 30.1%) for 12 studies in North America, −0.76 (95% CI: −0.92~−0.60, I2 = 84.6%) for 17 studies in Asia, and −0.93 (95% CI, −1.44~−0.43, I2 = 89.8%) for 9 studies in Europe.
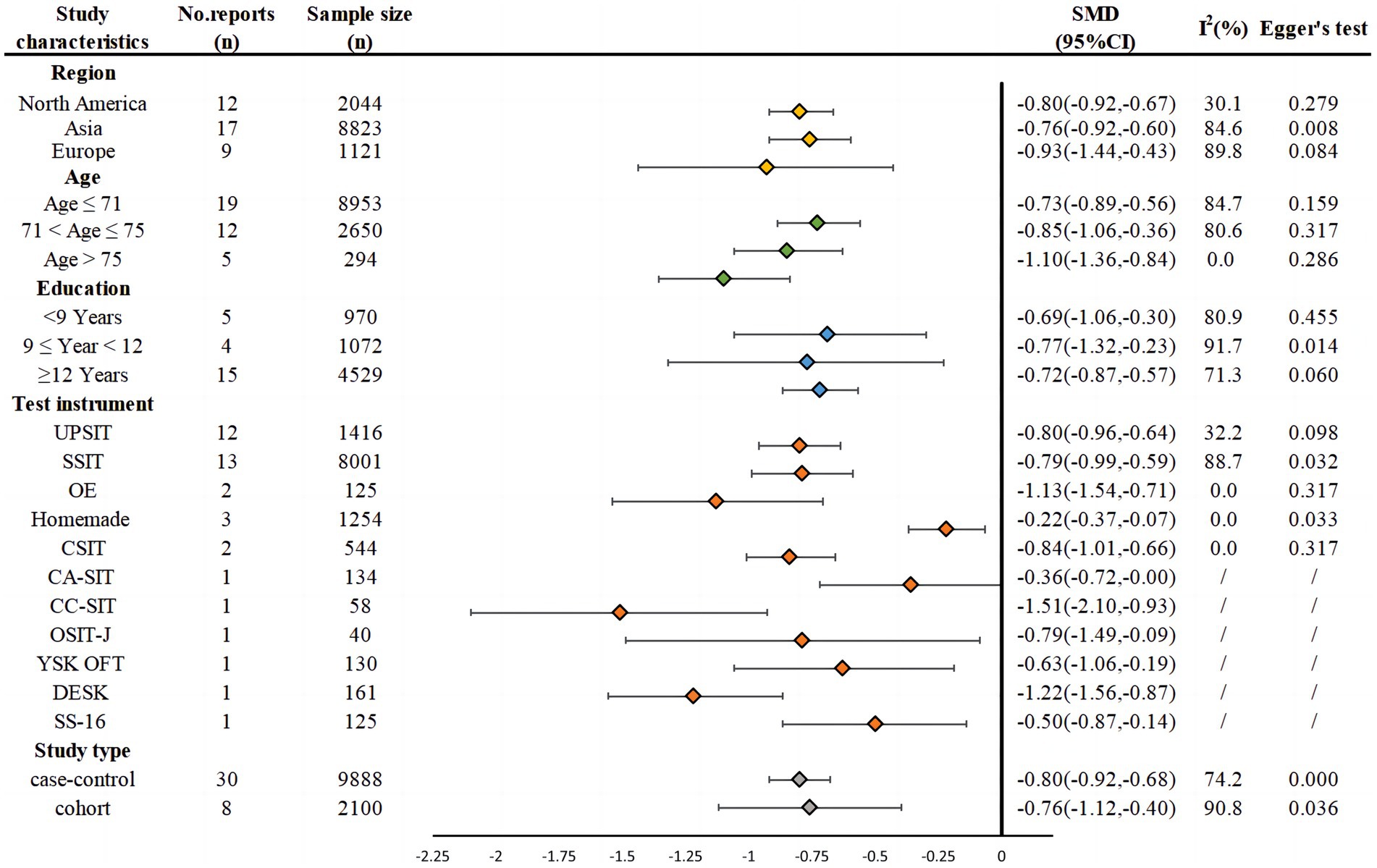
Figure 2. Basic characteristics of the studies and SMD by different moderating variables.
Second, 3 age groups had SMD = −0.74 (95% CI: −0.93~−0.55, I2 = 89.4%) in 15 studies with participants’ mean age ≤ 71 years, SMD = −0.78 (95% CI: −0.98~−0.58, I2 = 75.4%) in 11 studies with participants’ mean age between 71 and 75 years, and SMD = −0.96 (95% CI: −1.29~−0.64, I2 = 0%) in 4 studies with participants’ mean age greater than 75 years.
Third, 3 education groups showed SMD = −0.82 (95% CI: −1.33~−0.31; I2 = 80.0%) in 4 studies whose participants had less than 9 years of education; SMD = −0.57 (95% CI: −1.46~−0.57; I2 = 83.9%) in 3 studies whose participants had between 9 and 12 years of education; and SMD = −0.72 (95% CI: −0.87~−0.57; I2 = 71.3%) in 15 studies whose participants had more than 12 years of education.
The effect sizes also varied by test instruments used in the included studies, with SMD = −0.80 (95% CI: −0.96~−0.64, I2 = 32.2%) by UPSIT; SMD = −0.79 (95% CI: −0.99~−0.59, I2 = 88.7%) by SSIT; SMD = −1.13 (95% CI: −0.96~−0.64, I2 = 32.2%) by OE; SMD = −0.22 (95% CI: −0.37~−0.07) by homemade instruments; SMD = −0.84 (95% CI: −1.01~−0.66) by CSIT; SMD = −0.36 (95% CI: −0.72~−0.00) by CA-SIT, SMD = −1.51 (95% CI: −2.10~−0.93) by CC-SIT, SMD = −0.79 (95% CI: −1.49~−0.09) by OSIT-J, SMD = −0.63 (95% CI: −1.06~−0.19) by YSK OFT, SMD = −1.22 (95%CI: −1.56~−0.87) by DESK, and SMD = −0.50 (95% CI: −0.87~−0.14) by SS-16.
Two types of research design had SMD = −0.80 (95% CI: −0.92~−0.68; I2 = 74.2%) in the 30 case–control studies and SMD = −0.76 (95% CI: −1.12~−0.40; I2 = 90.8%) in the 8 cohort studies.
As shown in Figure 3, MCI patients were lower than the healthy controls in odor detection thresholds (SMD = −0.33, 95% CI: −0.57~0.08, p < 0.001), memory (SMD = −0.48. 95% CI: −0.69~−0.27, p < 0.001), discrimination (SMD = −0.70, 95% CI: −0.59~−0.46, p < 0.001), and identification (SMD = −0.89, 95% CI: −1.05~−0.73, p < 0.001) in ascending order of the effect size.
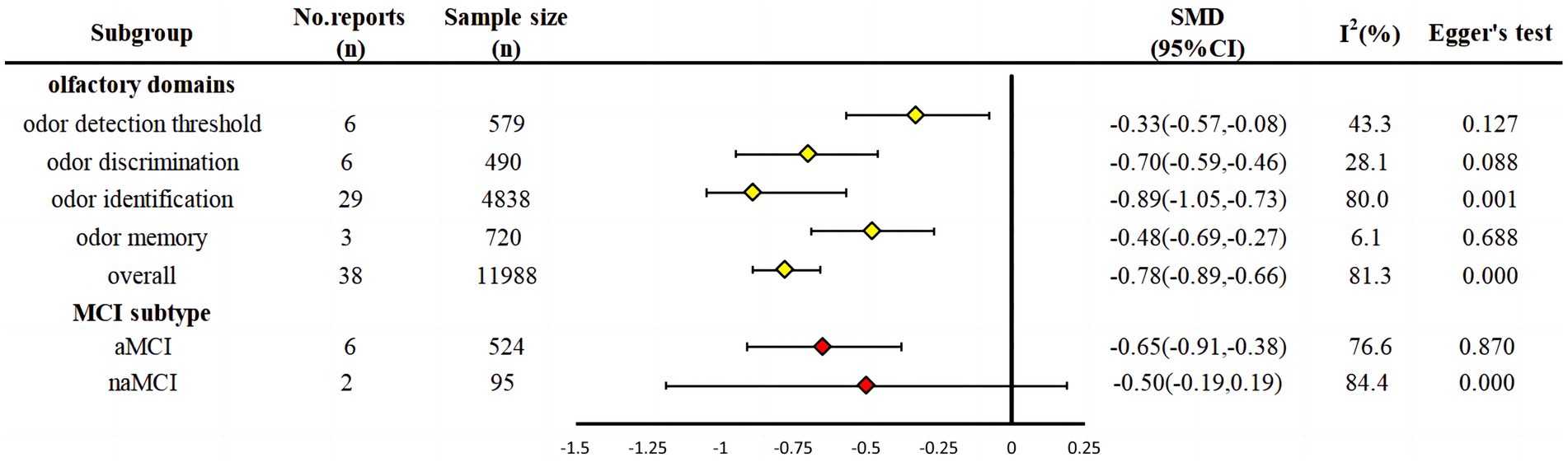
Figure 3. Subgroup analysis.
The degrees of olfactory impairment were more severe in the aMCI group (SMD = −0.65, 95% CI: −0.91~−0.38, p = 0.001) than in the naMCI group (SMD = −0.50, 95% CI: −0.19~0.19, p = 0.155), where the difference in the naMCI group was not statistically significant from zero, as shown in Figure 3. Six studies reported patients with aMCI, with a total sample size of 524 cases (I2 = 76.6%, p = 0.001). Two studies reported patients with naMCI with a total sample size of 95 cases (I2 = 84.4%, p = 0.005). The heterogeneity between the two groups was I2 > 50%, as indicated by a random effect model.
As shown in Table 2, meta-regression was performed on the effect-coded region (Daly et al., 2016), age, education levels, study design, and cognitive test scores (MMSE and MoCA). The results showed that olfactory impairment varied only with MoCA scores when pitted against one another in the model.
Publication bias was evaluated by Egger’s test (p = 0.372), which suggested that there was no significant evidence of publication bias. After excluding studies one by one, the effect size and the 95% CIs showed robustness in all results (see Supplementary material).
The current meta-analysis of 38 high-quality studies revealed that MCI patients had much lower overall olfactory function than the healthy participants in terms of the large effect size. The overall difference also varied across domains of olfactory function, test instruments of olfactory function, subtypes of MCI (naMCI and aMCI), and cognitive tests of MCI.
The effect size in the overall olfactory function was close to the large effect found in the early meta-analysis that compared MCI patients with normal adults (Roalf et al., 2017), but much less than those in studies that compared AD patients (Rahayel et al., 2012; Vyhnalek et al., 2015; Roberts et al., 2016; Kotecha et al., 2018; Jung et al., 2019). This was expected, as the included studies also compared MCI patients with normal adults.
Specific domains of olfactory function in this meta-analysis showed that MCI patients had the most drastic lower function in odor identification and discrimination than normal adults, in terms of the effect size (Cohen, 1977). These large effects imply that these tests may be used exclusively or conjointly with other MoCA to identify MCI in clinical settings. In contrast, the smaller effects in odor detection thresholds and odor memory imply that these tests cannot differentiate MCI patients from normal aging adults (Hummel et al., 2007), and thus may be recommended to the general public to guard against any further deterioration and symptoms of MCI due to neurobiological changes.
Test instruments of olfactory function appeared to contribute largely to the overall olfactory function differences between the MCI and normal individuals, with the effects ranging from the smallest by homemade instruments (SMD = −0.22) to the largest by CC-SIT (SMD = 1.51). Homemade odor samples could have been familiarized and sensitized to the participants in the three studies, so that the odors in these studies could also be detected, identified, or discriminated against easily by MCI patients, resulting in small effect sizes. Small effect sizes suggest that the odor test instruments were not as sensitive and efficacious as those that yielded larger effects. Therefore, certain odor test instruments may be improved for better validity/efficacy.
The aMCI subtype patients exhibited more pronounced deficits in odor identification and discrimination than those with naMCI (SMD = −0.65>0.50), which suggests that olfactory impairment is associated with aMCI (Vyhnalek et al., 2015; Roberts et al., 2016). However, as the effect size of the two studies that involved naMCI patients was non-significant due to small samples and few studies, the differential predictive powers of the two subtypes of MCI need to be ascertained with further studies, especially prospective longitudinal ones.
The meta-regression suggested that the effect sizes were similar across regions and age and education groups when controlled for MCI measures and study designs. This suggests that olfactory function between MCI and normal adults was similar across regions, age groups, and education groups. This might also suggest that the underlying mechanism for the association of olfactory dysfunction with MCI can be universally bio-neurological and that olfactory impairment could be a reliable biomarker and predictor for cognitive decline (Deary et al., 2009; Windon et al., 2020).
MoCA outweighed MMSE in moderating the overall effect size. This may be because the MoCA scale assesses a broader range of cognitive domains, including executive function, visuospatial ability, and language, and is more sensitive in detecting mild cognitive impairment (MCI) and early dementia than the MMSE. MoCA also has fewer ceiling effects than the MMSE by including tasks that are challenging even for high-functioning individuals (Jia et al., 2021). Thus, the MoCA scale appeared to be more sensitive for screening early cognitive decline (Shao et al., 2021).
Despite the rigorous selection of high-quality studies and stringent inclusion criteria applied in this research, it is unfortunate that a considerable degree of heterogeneity persists. This may be due to the inclusion of a wide array of olfactory tests, each assessing different domains of olfactory function. Variability may also arise from the application of identical olfactory tests across diverse populations and countries, leading to potential discrepancies in outcomes. The Sniffin’ Sticks Identification Test (SSIT) in particular demonstrated the greatest heterogeneity, which can be attributed to the multiplicity of testing methodologies employed in various countries, each with its unique approach. Moreover, within the subgroup analysis of olfactory domains, olfactory identification tests revealed the most pronounced heterogeneity. This is likely a consequence of the global emphasis on olfactory identification abilities in the majority of olfactory assessment tools, contributing to a broad spectrum of tools and types and, thus, heightened heterogeneity.
Although this study provides valuable insights into the relationship between olfactory impairment and MCI, several limitations must be considered. First, the high heterogeneity in this study may have been influenced by clinical factors, such as smoking, alcohol consumption, genetic factors, and COVID-19 infection status, which were not controlled for in the included studies. Second, the limited number of original studies on olfactory impairment in different subtypes of MCI patients means that they did not permit explorations of more complicated interactions between olfactory subdomains, subtypes of MCI, and other factors. Future studies may adopt prospective longitudinal designs, improve olfactory function tests, and probe into the neurological causes of the association between olfactory and MCI.
Olfactory impairment accompanies MCI, but the magnitude of the association depends on the measured domains of olfactory function, test instruments to measure both olfactory function and MCI, and subtypes of MCI. Severe deficits in odor identification and discrimination are more associated with MCI in aMCI patients. Valid odor identification and discrimination tests are recommended to complement MoCA and improve screening accuracy.
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding authors.
CZ: Data curation, Writing – original draft. CY: Formal analysis, Methodology, Writing – review & editing. YA: Data curation, Writing – review & editing. XF: Data curation, Formal analysis, Writing – review & editing. AZ: Investigation, Visualization, Writing – review & editing. YW: Funding acquisition, Methodology, Supervision, Writing – review & editing. HH: Funding acquisition, Resources, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This study was supported by the Key project of Science and technology research plan of Education Department of Hubei Province (grant number: D20222004) and the National Natural Science Foundation of China (grant number: 72374068).
This is a short text to acknowledge the contributions of specific colleagues, institutions, or agencies that aided the efforts of the authors.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnagi.2024.1349196/full#supplementary-material
UPSIT, University of Pennsylvania Odor Identification Test; SSIT, Sniffin’ Sticks Identification Test; OSIT-J, Japanese odor stick identification test; CA-SIT, Culturally adapted version of the odor identification test; CC-SIT, Cross-cultural version of the olfactory identification test; YSK OFT, YSK Olfactory Function Test.; DESK, The DEmentia Screening Kit; CSIT, The Chinese Smell Identification Test; OE, Open Essence; SS-16, Sniffin’ sticks test with 16 odors; aMCI, Amnestic mild cognitive impairment; naMCI, Non-amnestic mild cognitive impairment
Bathini, P., Brai, E., and Auber, L. A. (2019). Olfactory dysfunction in the pathophysiological continuum of dementia. Ageing Res. Rev. 55:100956. doi: 10.1016/j.arr.2019.100956
Chen, B. (2017). Cognitive function and multimodal magnetic resonance imaging study of elderly depressed patients with olfactory impairment. [dissertation/master's thesis]. [Guangzhou (Guangdong)]: Southern Medical University.
Chen, B., Wang, Q., Zhong, X., Mai, N., Zhang, M., Zhou, H., et al. (2022). Structural and functional abnormalities of olfactory-related regions in subjective cognitive decline, mild cognitive impairment, and Alzheimer’s disease. Int. J. Neuropsychopharmacol. 25, 361–374. doi: 10.1093/ijnp/pyab091
Cohen, J. (1977). “CHAPTER 2—the t test for means” in Statistical power analysis for the behavioral sciences. ed. J. Cohen (New York: Academic Press), 19–74.
Conti, M. Z., Vicini-Chilovi, B., Riva, M., Zanetti, M., Liberini, P., Padovani, A., et al. (2013). Odor identification deficit predicts clinical conversion from mild cognitive impairment to dementia due to Alzheimer’s disease. Arch. Clin. Neuropsychol. 28, 391–399. doi: 10.1093/arclin/act032
Daly, A., Dekker, T., and Hess, S. (2016). Dummy coding vs effects coding for categorical variables: clarifications and extensions. J. Choice Model. 21, 36–41. doi: 10.1016/j.jocm.2016.09.005
Deary, I. J., Corley, J., Gow, A. J., Harris, S. E., Houlihan, L. M., Marioni, R. E., et al. (2009). Age-associated cognitive decline. Br. Med. Bull. 92, 135–152. doi: 10.1093/bmb/ldp033
Delgado-Lima, A. H., Bouhaben, J., Martínez-Zujeros, S., Pallardo-Rodil, B., Gómez-Pavón, J., and Delgado-Losada, M. L. (2023). Could olfactory identification be a prognostic factor in detecting cognitive impairment risk in the elderly? Geroscience. 45, 2011–2025. doi: 10.1007/s11357-023-00779-5
Devanand, D. P., Lee, S., Manly, J., Andrews, H., Schupf, N., Doty, R. L., et al. (2015). Olfactory deficits predict cognitive decline and Alzheimer dementia in an urban community. Neurology 84, 182–189. doi: 10.1212/WNL.0000000000001132
Devanand, D. P., Michaels-Marston, K. S., Liu, X., Pelton, G. H., Padilla, M., Marder, K., et al. (2000). Olfactory deficits in patients with mild cognitive impairment predict Alzheimer’s disease at follow-up. Am. J. Psychiatry 157, 1399–1405. doi: 10.1176/appi.ajp.157.9.1399
Devanand, D. P., Tabert, M. H., Cuasay, K., Manly, J. J., Schupf, N., Brickman, A. M., et al. (2010). Olfactory identification deficits and MCI in a multi-ethnic elderly community sample. Neurobiol. Aging 31, 1593–1600. doi: 10.1016/j.neurobiolaging.2008.09.008
Dong, Y., Li, Y., Liu, K., Han, X., Liu, R., Ren, Y., et al. (2022). Anosmia, mild cognitive impairment, and biomarkers of brain aging in older adults. Alzheimers Dement. 19, 589–601. doi: 10.1002/alz.12777
Doorduijn, A. S., de van der Schueren, M. A. E., van de Rest, O., de Leeuw, F. A., Fieldhouse, J. L. P., Kester, M. I., et al. (2020). Olfactory and gustatory functioning and food preferences of patients with Alzheimer’s disease and mild cognitive impairment compared to controls: the NUDAD project. J. Neurol. 267, 144–152. doi: 10.1007/s00415-019-09561-0
Doty, R. L., Marcus, A., and William Lee, W. (1996). Development of the 12-item cross-cultural smell identification test(CC-SIT). Laryngoscope 106, 353–356. doi: 10.1097/00005537-199603000-00021
Doty, R. L., Shaman, P., Kimmelman, C. P., and Dann, M. S. (1984). University of Pennsylvania Smell Identification Test: a rapid quantitative olfactory function test for the clinic. Laryngoscope 94, 176–178. doi: 10.1288/00005537-198402000-00004
Feng, G., Zhuang, Y., Yao, F., Ye, Y., Wan, Q., and Zhou, W. (2019). Development of the Chinese smell identification test. Chem. Senses 44, 189–195. doi: 10.1093/chemse/bjz006
Fukumoto, T., Ezaki, T., and Urakami, K. (2022). Verification of the association between cognitive decline and olfactory dysfunction using a DEmentia screening kit in subjects with Alzheimer’s dementia, mild cognitive impairment, and normal cognitive function (DESK study): a multicenter, open-label, interventional study. eNeurologicalSci 29:100439. doi: 10.1016/j.ensci.2022.100439
Guo, W. J., Zhao, A., Yan, Y., Chou, Y. H., and Deng, Y. (2023). Diagnostic value of olfactory testing in Chinese patients with Alzheimer's disease and mild cognitive impairment. Chin Med J 20, 60–64. doi: 10.20047/j.issn1673-7210.2023.02.13
Hagemeier, J., Woodward, M. R., Rafique, U. A., Amrutkar, C. V., Bergsland, N., Dwyer, M. G., et al. (2016). Odor identification deficit in mild cognitive impairment and Alzheimer’s disease is associated with hippocampal and deep gray matter atrophy. Psychiatry Res. Neuroimaging 255, 87–93. doi: 10.1016/j.pscychresns.2016.08.003
Hedner, M., Larsson, M., Arnold, N., Zucco, G. M., and Hummel, T. (2010). Cognitive factors in odor detection, odor discrimination, and odor identification tasks. J. Clin. Exp. Neuropsychol. 32, 1062–1067. doi: 10.1080/13803391003683070
Huart, C., Rombaux, P., Gérard, T., Hanseeuw, B., Lhommel, R., Quenon, L., et al. (2015). Unirhinal olfactory testing for the diagnostic workup of mild cognitive impairment. J. Alzheimers Dis. 47, 253–270. doi: 10.3233/JAD-141494
Hummel, T., Kobal, G., Gudziol, H., and Mackay-Sim, A. (2007). Normative data for the “Sniffin’ sticks” including tests of odor identification, odor discrimination, and olfactory thresholds: an upgrade based on a group of more than 3,000 subjects. Eur. Arch. Otorhinolaryngol. 264, 237–243. doi: 10.1007/s00405-006-0173-0
Hummel, T., Sekinger, B., Wolf, S. R., Pauli, E., and Kobal, G. (1997). “Sniffin” sticks’: olfactory performance assessed by the combined testing of odor identification, odor discrimination and olfactory threshold. Chem. Senses 22, 39–52. doi: 10.1093/chemse/22.1.39
Iritani, O., Okuno, T., Miwa, T., Makizako, H., Okutani, F., Kashibayashi, T., et al. (2021). Olfactory-cognitive index distinguishes involvement of frontal lobe shrinkage, as in sarcopenia from shrinkage of medial temporal areas, and global brain, as in Kihon checklist frailty/dependence, in older adults with progression of normal cognition to Alzheimer’s disease. Geriatr. Gerontol. Int. 21, 291–298. doi: 10.1111/ggi.14128
Jak, A. J., Bangen, K. J., Wierenga, C. E., Delano-Wood, L., Corey-Bloom, J., and Bondi, M. W. (2009). Contributions of neuropsychology and neuroimaging to understanding clinical subtypes of mild cognitive impairment. Int. Rev. Neurobiol. 84, 81–103. doi: 10.1016/S0074-7742(09)00405-X
Jia, X., Wang, Z., Huang, F., Su, C., Du, W., Jiang, H., et al. (2021). A comparison of the Mini-mental state examination (MMSE) with the Montreal cognitive assessment (MoCA) for mild cognitive impairment screening in Chinese middle-aged and older population: a cross-sectional study. BMC Psychiatry 21:485. doi: 10.1186/s12888-021-03495-6
Jiang, Z. (2019). Preliminary exploration of olfactory functional assessment in the clinical application of mild cognitive impairment and Alzheimer's disease. [dissertation/master's thesis]. [Changchun (Jilin)]: University of Jilin.
Jung, H. J., Shin, I.-S., and Lee, J.-E. (2019). Olfactory function in mild cognitive impairment and Alzheimer’s disease: a meta-analysis. Laryngoscope 129, 362–369. doi: 10.1002/lary.27399
Kim, S. M., Kim, H. R., Min, H. J., Kim, K. S., Jin, J.-C., and Han, D. H. (2021). A novel olfactory threshold test for screening cognitive decline among elderly people. PLoS One 16:e0254357. doi: 10.1371/journal.pone.0254357
Kim, H. R., Kim, S. M., Seong, W., Min, H. J., Kim, K. S., Ga, H., et al. (2020). Cut-off scores of an olfactory function test for mild cognitive impairment and dementia. Psychiatry Investig. 17, 1021–1030. doi: 10.30773/pi.2020.0203
Kjelvik, G., Evensmoen, H. R., Hummel, T., Engedal, K., Selbæk, G., Saltvedt, I., et al. (2020). The human brain representation of odor identification in amnestic mild cognitive impairment and Alzheimer’s dementia of mild degree. Front. Neurol. 11:607566. doi: 10.3389/fneur.2020.607566
Kotecha, A. M., Corrêa, A. D. C., Fisher, K. M., and Rushworth, J. V. (2018). Olfactory dysfunction as a global biomarker for sniffing out Alzheimer’s disease: a Meta-analysis. Biosensors 8:E41. doi: 10.3390/bios8020041
Kreisl, W. C., Jin, P., Lee, S., Dayan, E. R., Vallabhajosula, S., Pelton, G., et al. (2018). Odor identification ability predicts PET amyloid status and memory decline in older adults. J. Alzheimers Dis. 62, 1759–1766. doi: 10.3233/JAD-170960
Laakso, M. P., Tervo, S., Hänninen, T., Vanhanen, M., Hallikainen, M., and Soininen, H. (2009). Olfactory identification in non-demented elderly population and in mild cognitive impairment: a comparison of performance in clinical odor identification versus Boston naming test. J. Neural Transm. 116, 891–895. doi: 10.1007/s00702-009-0235-8
Liang, X., Ding, D., Zhao, Q., Guo, Q., Luo, J., Hong, Z., et al. (2016). Association between olfactory identification and cognitive function in community-dwelling elderly: the Shanghai aging study. BMC Neurol. 16:199. doi: 10.1186/s12883-016-0725-x
Liang, W., Wang, L., Geng, H., Jing, X. Y., Wang, X. M., Huo, Y. X., et al. (2023). Application of the Chinese brief olfactory recognition test in early screening for Alzheimer's disease. Chin J Mental Health, 380–387. doi: 10.3969/j.issn.1000-6729.2023.05.004
Lu, J., Yang, Q. X., Zhang, H., Eslinger, P. J., Zhang, X., Wu, S., et al. (2019). Disruptions of the olfactory and default mode networks in Alzheimer’s disease. Brain Behav. 9:e01296. doi: 10.1002/brb3.1296
Luo, D., Wan, X., Liu, J., and Tong, T. (2018). Optimally estimating the sample mean from the sample size, median, mid-range, and/or mid-quartile range. Stat. Methods Med. Res. 27, 1785–1805. doi: 10.1177/0962280216669183
Luzzi, S., Snowden, J. S., Neary, D., Coccia, M., Provinciali, L., and Lambon Ralph, M. A. (2007). Distinct patterns of olfactory impairment in Alzheimer’s disease, semantic dementia, frontotemporal dementia, and corticobasal degeneration. Neuropsychologia 45, 1823–1831. doi: 10.1016/j.neuropsychologia.2006.12.008
Mi, Y., Ma, X., Du, S., Du, C., Li, X., Tan, H., et al. (2023). Olfactory function changes and the predictive performance of the Chinese smell identification test in patients with mild cognitive impairment and Alzheimer’s disease. Front. Aging Neurosci. 15:1068708. doi: 10.3389/fnagi.2023.1068708
Okutani, F., Hirose, K., Kobayashi, T., Kaba, H., and Hyodo, M. (2013). Evaluation of “open essence” odor-identification test card by application to healthy volunteers. Auris Nasus Larynx 40, 76–80. doi: 10.1016/j.anl.2012.02.007
Olofsson, J. K., Larsson, M., Roa, C., Wilson, D. A., and Jonsson Laukka, E. (2020). Interaction between odor identification deficit and APOE4 predicts 6-year cognitive decline in elderly individuals. Behav. Genet. 50, 3–13. doi: 10.1007/s10519-019-09980-9
Peters, J. M., Hummel, T., Kratzsch, T., Lötsch, J., Skarke, C., and Frölich, L. (2003). Olfactory function in mild cognitive impairment and Alzheimer’s disease: an investigation using psychophysical and electrophysiological techniques. Am. J. Psychiatry 160, 1995–2002. doi: 10.1176/appi.ajp.160.11.1995
Pusswald, G., Dapić, B., Bum, C., Schernhammer, E., Stögmann, E., and Lehrner, J. (2023). Olfactory identification, cognition, depressive symptoms, and 5-year mortality in patients with subjective cognitive decline, mild cognitive impairment, and Alzheimer’s disease. Wien. Med. Wochenschr. doi: 10.1007/s10354-023-01008-6
Quarmley, M., Moberg, P. J., Mechanic-Hamilton, D., Kabadi, S., Arnold, S. E., Wolk, D. A., et al. (2017). Odor identification screening improves diagnostic classification in incipient Alzheimer’s disease. J. Alzheimers Dis. 55, 1497–1507. doi: 10.3233/JAD-160842
Rahayel, S., Frasnelli, J., and Joubert, S. (2012). The effect of Alzheimer’s disease and Parkinson’s disease on olfaction: a meta-analysis. Behav. Brain Res. 231, 60–74. doi: 10.1016/j.bbr.2012.02.047
Risacher, S. L., Tallman, E. F., West, J. D., Yoder, K. K., Hutchins, G. D., Fletcher, J. W., et al. (2017). Olfactory identification in subjective cognitive decline and mild cognitive impairment: association with tau but not amyloid positron emission tomography. Alzheimers Dement. 9, 57–66. doi: 10.1016/j.dadm.2017.09.001
Roalf, D. R., Moberg, M. J., Turetsky, B. I., Brennan, L., Kabadi, S., Wolk, D. A., et al. (2017). A quantitative meta-analysis of olfactory dysfunction in mild cognitive impairment. J. Neurol. Neurosurg. Psychiatry 88, 226–232. doi: 10.1136/jnnp-2016-314638
Roberts, R. O., Christianson, T. J. H., Kremers, W. K., Mielke, M. M., Machulda, M. M., Vassilaki, M., et al. (2016). Association between olfactory dysfunction and amnestic mild cognitive impairment and Alzheimer disease dementia. JAMA Neurol. 73, 93–101. doi: 10.1001/jamaneurol.2015.2952
Seligman, S. C., Kamath, V., Giovannetti, T., Arnold, S. E., and Moberg, P. J. (2013). Olfaction and apathy in Alzheimer’s disease, mild cognitive impairment, and healthy older adults. Aging Ment. Health 17, 564–570. doi: 10.1080/13607863.2013.768208
Servello, A., Fioretti, A., Gualdi, G., Di Biasi, C., Pittalis, A., Sollaku, S., et al. (2015). Olfactory dysfunction, olfactory bulb volume and Alzheimer’s disease: is there a correlation? A pilot Study1. J. Alzheimers Dis. 48, 395–402. doi: 10.3233/JAD-150232
Shao, W., Zhao, A., Wu, F., Lu, S., Du, J., Zhao, Q., et al. (2021). Diagnostic value of the Montreal cognitive assessment scale in geriatric neurocognitive disorders. Chin. J. Gerontol. 41, 3551–3554. doi: 10.3969/j.issn.1005-9202.2021.16.044
Shino, M., Furuta, A., Uchida, J., Ooki, S., and Suzaki, H. (2006). Odor stick identification test for Japanese patients with olfactory disturbances. Nippon Jibiinkoka Gakkai Kaiho 109, 689–695. doi: 10.3950/jibiinkoka.109.689
Sohrabi, H. R., Bates, K. A., Weinborn, M. G., Johnston, A. N. B., Bahramian, A., Taddei, K., et al. (2012). Olfactory discrimination predicts cognitive decline among community-dwelling older adults. Transl. Psychiatry 2:e118. doi: 10.1038/tp.2012.43
Stang, A. (2010). Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 25, 603–605. doi: 10.1007/s10654-010-9491-z
Stevenson, R. J., and Boakes, R. A. (2003). A mnemonic theory of odor perception. Psychol. Rev. 110, 340–364. doi: 10.1037/0033-295x.110.2.340
Suzuki, H., Sugiura, S., Nakashima, T., Teranishi, M., Shimono, M., Murotani, K., et al. (2022). Cognitive impairment is correlated with olfactory identification deficits in older Japanese adults: a cross-sectional study using objective and subjective olfactory measures. Geriatr. Gerontol. Int. 22, 924–929. doi: 10.1111/ggi.14483
Tabert, M. H., Liu, X., Doty, R. L., Serby, M., Zamora, D., Pelton, G. H., et al. (2005). A 10-item smell identification scale related to risk for Alzheimer’s disease. Ann. Neurol. 58, 155–160. doi: 10.1002/ana.20533
Tan, Z., Wang, Y., Lu, H., Tian, W., Xu, K., Fan, M., et al. (2022). The effects of brain magnetic resonance imaging indices in the Association of Olfactory Identification and Cognition in Chinese older adults. Front. Aging Neurosci. 14:873032. doi: 10.3389/fnagi.2022.873032
Tonacci, A., Bruno, R. M., Ghiadoni, L., Pratali, L., Berardi, N., Tognoni, G., et al. (2017). Olfactory evaluation in mild cognitive impairment: correlation with neurocognitive performance and endothelial function. Eur. J. Neurosci. 45, 1279–1288. doi: 10.1111/ejn.13565
Umeda-Kameyama, Y., Ishii, S., Kameyama, M., Kondo, K., Ochi, A., Yamasoba, T., et al. (2017). Heterogeneity of odorant identification impairment in patients with Alzheimer’s disease. Sci. Rep. 7:4798. doi: 10.1038/s41598-017-05201-7
Vasavada, M. M., Wang, J., Eslinger, P. J., Gill, D. J., Sun, X., Karunanayaka, P., et al. (2015). Olfactory cortex degeneration in Alzheimer’s disease and mild cognitive impairment. J. Alzheimers Dis. 45, 947–958. doi: 10.3233/JAD-141947
Vyhnalek, M., Magerova, H., Andel, R., Nikolai, T., Kadlecova, A., Laczo, J., et al. (2015). Olfactory identification in amnestic and non-amnestic mild cognitive impairment and its neuropsychological correlates. J. Neurol. Sci. 349, 179–184. doi: 10.1016/j.jns.2015.01.014
Wan, X., Wang, W., Liu, J., and Tong, T. (2014). Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 14:135. doi: 10.1186/1471-2288-14-135
Wang, Y., Du, Y., Tian, Q., and Sun, G. (2018). Meta-analysis of the relationship between olfactory impairment and Alzheimer's disease. Hubei J Tradition Chin Med 40, 3–8.
Wang, Q.-S., Tian, L., Huang, Y.-L., Qin, S., He, L.-Q., and Zhou, J.-N. (2002). Olfactory identification and apolipoprotein E ε4 allele in mild cognitive impairment. Brain Res. 951, 77–81. doi: 10.1016/S0006-8993(02)03137-2
Ward, A. M., Calamia, M., Thiemann, E., Dunlap, J., and Tranel, D. (2017). Association between olfaction and higher cortical functions in Alzheimer’s disease, mild cognitive impairment, and healthy older adults. J. Clin. Exp. Neuropsychol. 39, 646–658. doi: 10.1080/13803395.2016.1253667
Windon, M. J., Kim, S. J., Oh, E. S., and Lin, S. Y. (2020). Predictive value of olfactory impairment for cognitive decline among cognitively normal adults. Laryngoscope 130, 840–847. doi: 10.1002/lary.28166
Woodward, M. R., Amrutkar, C. V., Shah, H. C., Benedict, R. H. B., Rajakrishnan, S., Doody, R. S., et al. (2017). Validation of olfactory deficit as a biomarker of Alzheimer disease. Neurol Clin Pract 7, 5–14. doi: 10.1212/CPJ.0000000000000293
Woodward, M. R., Hafeez, M. U., Qi, Q., Riaz, A., Benedict, R. H. B., Yan, L., et al. (2018). Odorant item specific olfactory identification deficit may differentiate Alzheimer disease from aging. Am. J. Geriatr. Psychiatry 26, 835–846. doi: 10.1016/j.jagp.2018.02.008
Yang, X., Lingfeng, L., Qiumin, H., Zhonghan, S., and Yan, Z. (2022). Alzheimer's disease and olfactory dysfunction: a meta-analysis. Fudan J 49, 32–43. doi: 10.3969/j.issn.1672-8467.2022.01.005
Yap, A. C., Mahendran, R., Kua, E. H., Zhou, W., and Wang, D. Y. (2022). Olfactory dysfunction is associated with mild cognitive impairment in community-dwelling older adults. Front. Aging Neurosci. 14:930686. doi: 10.3389/fnagi.2022.930686
Yi, J. S., Hura, N., Roxbury, C. R., and Lin, S. Y. (2022). Magnetic resonance imaging findings in people with olfactory and cognitive impairments. Laryngoscope 132, 177–187. doi: 10.1002/lary.29812
Keywords: mild cognitive impairment, olfactory function, cognitive function, meta-analysis, smell test
Citation: Zhou C, Yang C, Ai Y, Fang X, Zhang A, Wang Y and Hu H (2024) Valid olfactory impairment tests can help identify mild cognitive impairment: an updated meta-analysis. Front. Aging Neurosci. 16:1349196. doi: 10.3389/fnagi.2024.1349196
Edited by:
Guillermo Felipe López Sánchez, University of Murcia, SpainReviewed by:
Carla Masala, University of Cagliari, ItalyCopyright © 2024 Zhou, Yang, Ai, Fang, Zhang, Wang and Hu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yuncui Wang, eXVuY3VpX3dhbmdAaGJ0Y20uZWR1LmNu; Hui Hu, emhvbmd5aTkwQDE2My5jb20=
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.