
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Aging Neurosci. , 07 February 2024
Sec. Neurocognitive Aging and Behavior
Volume 16 - 2024 | https://doi.org/10.3389/fnagi.2024.1253028
 Emma Segura1,2
Emma Segura1,2 Adrià Vilà-Balló1,2,3
Adrià Vilà-Balló1,2,3 Aida Mallorquí4
Aida Mallorquí4 María F. Porto1,2
María F. Porto1,2 Esther Duarte5,6
Esther Duarte5,6 Jennifer Grau-Sánchez1,7
Jennifer Grau-Sánchez1,7 Antoni Rodríguez-Fornells1,2,3,8*
Antoni Rodríguez-Fornells1,2,3,8*Background: Anhedonia refers to the diminished capacity to experience pleasure. It has been described both as a symptom of depression and an enduring behavioral trait that contributes its development. Specifically, in stroke patients, anhedonia has been closely linked to depression, resulting in reduced sensitivity to everyday pleasures and intrinsic motivation to engage in rehabilitation programs and maintain a healthy active lifestyle. This condition may hinder patients’ recovery, diminishing their autonomy, functioning, and quality of life.
Objective: We aimed to explore the prevalence and level of anhedonia and those variables that might be associated in patients with both ischemic and hemorrhagic stroke at subacute and chronic phases of the disease.
Methods: We conducted an exploratory cohort study with a sample of 125 patients with subacute and chronic stroke presenting upper-limb motor deficits. We measured participants’ level of anhedonia with four items from the Beck Depression Inventory-II that describe the symptoms of this condition: loss of pleasure, loss of interest, loss of energy, and loss of interest in sex. We also collected demographic and clinical information and evaluated motor and cognitive functions as well as levels of depression, apathy, and various mood states. The results were compared to a sample of 71 healthy participants of similar age, sex, and level of education.
Results: Stroke patients demonstrated a significantly higher prevalence (18.5–19.7%) and level of anhedonia compared to the healthy controls (4.3%), regardless of stroke phase, level of motor impairment, and other clinical variables. Furthermore, post-stroke anhedonia was associated with lower levels of motivation and higher levels of negative mood states such as fatigue and anger in the long term. Importantly, anhedonia level was superior in stroke patients than in healthy controls while controlling for confounding effects of related emotional conditions.
Conclusion: This study provides novel evidence on the prevalence, level and factors related to anhedonia post-stroke. We emphasize the importance of assessing and treating anhedonia in this population, as well as conducting large-scale cohort and longitudinal studies to test its influence on long-term functional and emotional recovery.
Anhedonia is defined as the diminished capacity to experience pleasure. The concept was rarely used before the 1980s and was officialized in the DSM-III, becoming a necessary symptom for depression diagnosis (Der-Avakian and Markou, 2012). In 2008, the American Psychiatric Association developed the Research Domain Criteria framework to integrate transdiagnostic neurobehavioral evidence in the study of mental disorders, where anhedonia was considered a behavioral correlate of the negative valence human systems domain (Cuthbert, 2021). Anhedonia has also been addressed as a residual symptom of schizophrenia (Der-Avakian and Markou, 2012), but most recently, it was included in the DSM-V as a crucial symptom for diagnosing the major depression melancholic subtype and differentiating it from other mental disorders (American Psychiatric Association, 2013).
Besides the medical symptom approach, anhedonia has been described as an enduring and stable behavioral trait that characterizes an individual’s personality (Der-Avakian and Markou, 2012). The manifestation of anhedonia has been associated with deficits in the reward processing system, specifically in the dopaminergic projections between the midbrain dopaminergic nucleus, striatum, amygdala, hippocampus, and prefrontal cortex, requested for modulating behavioral responses to rewards (Camara et al., 2009; Der-Avakian and Markou, 2012). Previous studies have suggested the genetic influence of developing anhedonia by demonstrating genetic polymorphisms of dopamine synthesis, metabolism, and regulator proteins that impair functional activity of brain regions belonging to the reward system (Ren et al., 2018). Accordingly, it has been proposed the potential endophenotype role of anhedonia as a vulnerability marker present before the onset of depression that might increase the severity and prolong the course of this mood disorder (Gong et al., 2017). Furthermore, suffering depression with severe symptoms of anhedonia has also been associated with an elevated risk of suicide (Bonanni et al., 2019). Individuals with high anhedonia-trait levels could thus be more likely to develop depression in a particular context (Pizzagalli et al., 2005; Auerbach et al., 2019). For example, anhedonia has been associated with increased levels of depression at hospital discharge in stroke patients (Sibon et al., 2012). In this regard, the disruption of dopaminergic networks after a stroke could trigger the onset of mood disorders and cognitive deficits including memory dysfunction, leading to the development of anhedonia (Piamarta et al., 2004; Terroni et al., 2015).
In addition to mental health disorders, anhedonia has been found in other health conditions involving chronic pain and inflammatory processes (Carpinelli et al., 2019; Lucido et al., 2021). For instance, a control–case study reported higher anhedonia levels in chronic pain sufferers when compared to healthy controls, with 25% of patients obtaining scores over the standard cutoff point (Garland et al., 2020). Interestingly, this result was not entirely motivated by a comorbid depression diagnosis, pointing out a more nuanced perspective of the psychological consequences of some health conditions. Furthermore, a recent review on endometriosis, a gynecological chronic systemic inflammatory disease characterized by the presence of chronic pelvic pain, presented anhedonia as a severe symptom which is not assessed in the usual clinical treatment despite the deleterious consequences in patients’ mental health and quality of life (QoL) (Mallorqui et al., 2022).
Stroke is the most prevalent neurological disease and a leading cause of acquired long-term disability worldwide (Katan and Luft, 2018; Feigin et al., 2019). Motor, cognitive, and language deficits are common post-stroke consequences that limit the accomplishment of daily activities and restrict participation in familiar, social, work, and community life (Hartman-Maeir et al., 2007; Tang et al., 2020). The reduction of the functional autonomy of stroke survivors has negative effects on their emotional well-being and QoL, leading to mood disorders such as depression and anxiety (Patel et al., 2002; Marcheschi et al., 2018; Diamond et al., 2023). Importantly, most patients still present or even increase motor deficits in the chronic phase of the disease (Kwakkel et al., 2003). Once patients complete formal rehabilitation programs, a decrease in physical activity mostly attributed to a lack of a rehabilitation routine and/or therapist presence can provoke a decline in motor functions (Ashe et al., 2009). This underscores the importance of intrinsic motivation in sustaining a healthy and active lifestyle (Chan et al., 2009).
Stroke survivors pass through challenging periods in which they need to adapt their lives to their new condition. Between 25 and 79% of stroke patients suffer post-stroke depression (PSD), whose cause is associated with the physical and psychological adversities they must cope with (Whyte and Mulsant, 2002). Previous research have demonstrated the negative impact of PSD on motor and cognitive recovery, becoming an additional disabling factor responsible for 15% of increased disability (Paolucci et al., 2019). This detrimental consequence has been associated with deficits in regulating motivation-related behaviors (Gainotti et al., 2001). Many studies have focused on exploring the negative impact of apathy on stroke rehabilitation (Marin, 1991; Sibon et al., 2012), but motivational mechanisms and goal-directed behaviors are also disrupted by anhedonia, an understudied condition in the stroke population. Despite the substantial overlap between apathy and anhedonia, the former is associated with an impairment in selecting future behaviors based on emotional signals, while anhedonia is characterized by diminishing sensitivity to everyday pleasures and positive mood, crucial aspects for goal-directed engagement in rewarding activities (Verrienti et al., 2023). Considering the role of anhedonia in motivational aspects crucial for stroke survivors’ recovery, a recent study by Ashaie et al. (2023) explored the association between three dimensions of PSD somatic symptoms, negative affect, and anhedonia. They found that anhedonia predicted subsequent increases in somatic symptoms during the first year after rehabilitation discharge, indicating its impact on physical distress rather than stroke itself. In this regard, the authors emphasized the importance of examining specific dimensions of PSD, such as anhedonia, to understand their development and etiology and thus be able to guide clinicians in implementing targeted treatments and improving therapeutic outcomes (Ashaie et al., 2023). Currently, no previous study has examined the presence of anhedonia in patients with both ischemic and hemorrhagic stroke and over a wide range of time post-stroke.
In the present exploratory cohort study, we aimed to determine the prevalence and levels of anhedonia in subacute and chronic stroke survivors with upper-limb motor deficits, and to explore the factors associated with this condition in the stroke population. We hypothesized that two groups of subacute and chronic stroke patients would show a higher prevalence and level of anhedonia than a group of healthy individuals, and that anhedonia would be related to negative mood states. A better understanding of the onset of anhedonia post-stroke and its related factors would help design more effective and evidence-based interventions aimed to improve patients’ emotional well-being and promote adherence to rehabilitation and healthy active lifestyles.
Two groups of patients, one with subacute stroke (SS) (n = 54; females = 24; age = 61.44 ± 8.72 years; time since stroke = 2 ± 1.5 months) and another with chronic stroke (CS) (n = 71; females = 17; age = 62.27 ± 11.40; time since stroke = 20.75 ± 48.63 months), were included in the present study. All patients were recruited from the Physical Medicine and Rehabilitation Department of Hospital del Mar, Centre l’Esperança (Barcelona, Spain) to participate in experimental studies or randomized controlled trials that aimed to test the effectiveness of music-based interventions in the improvement of upper-limb motor functions. As part of these studies, patients underwent a basal evaluation that included motor, cognitive, emotional well-being and QoL assessment (Ripollés et al., 2016; Grau-Sánchez et al., 2018, 2021).
The studies were conducted by a group of research assistants that included psychologists and occupational therapists with training in clinical research. The inclusion criteria for both samples of stroke patients were: (1) mild-to-moderate paresis of the upper extremity after a first-ever stroke; (2) no major cognitive deficits affecting comprehension; (3) no neurological or psychiatric co-morbidity, except for PSD; (4) no other musculoskeletal condition affecting upper extremity motor function (e.g., fracture or arthritis); (5) ability to speak Spanish and/or Catalan. The specific inclusion criteria for the subacute sample were (1) less than 6 months after the stroke and (2) being involved in a program of outpatient rehabilitation at the Department of Physical Medicine and Rehabilitation at the Hospital del Mar, Centre l’Esperança. The specific inclusion criteria for the chronic stroke sample (1) more than 6 months post-stroke, and (2) have previously completed a 6-month formal rehabilitation program.
A group of healthy participants (HC) (n = 70; females = 31; age = 59.31 ± 13.81 years) who never suffered a stroke was recruited as a control group. The inclusion criteria were: (1) no presence of paresis or any musculoskeletal condition affecting upper-limb motor function; (2) no major cognitive deficits affecting comprehension; (3) no neurological or psychiatric co-morbidity; (4) ability to speak Spanish and/or Catalan. When recruiting the control sample, we considered their age, sex, and level of education to obtain similar groups in terms of demographic characteristics. They were recruited through the dissemination of the study in social networks, among relatives of research assistants, and from a residential service of temporary stays for elderly people called Respir in Barcelona.
Demographic and clinical variables such as age, sex, stroke etiology, affected hemisphere, lesion location, and time since stroke were collected from medical records. A structured interview was conducted at the hospital to assess patients’ upper-limb paresis and global cognitive function and check if they fulfilled the inclusion criteria. Paresis level was measured using the Medical Research Council Scale at the distal muscles of the upper extremity. Global cognitive function was measured using the Spanish version of the Mini-Mental State Examination (MMSE, Folstein and Folstein, 1975; Lobo, 1999) in subacute stroke patients, chronic stroke patients recruited by Ripollés et al. (2016), and healthy control participants; and the Spanish version of Montreal Cognitive Assessment (MoCA, Nasreddine et al., 2005; Gallego et al., 2009) in chronic stroke patients recruited by Grau-Sánchez et al. (2021). The presence of mild cognitive impairment (MCI) was defined following the cutoffs used in Pendlebury et al. (2012), indicating MCI when scoring lower than 27 in MMSE; and the cutoffs established by Pereiro et al. (2017), indicating the presence of MCI when scoring lower than 26 in MoCA.
Those patients who fulfilled the inclusion criteria were invited to attend another day at the hospital to complete the baseline evaluation. It consisted of a one-hour session of motor and cognitive functions assessments and was conducted by research members blinded to the intervention group. Furthermore, self-report emotional and QoL questionnaires were given to patients to complete at home (Ripollés et al., 2016; Grau-Sánchez et al., 2018, 2021). The motor, cognitive and emotional evaluation of healthy controls participants was performed entirely in person at their home or remotely via the Zoom platform depending on their preference.
Upper-limb functional movements were evaluated using the Action Research Arm Test (ARAT) (Lyle, 1981). The ARAT has excellent test–retest and inter/intra-rater reliability (Van Der Lee et al., 2001; Platz et al., 2005) and it is recommended for use in chronic stroke and outpatient rehabilitation by the StrokeEDGE Task Force Group (Sullivan et al., 2013). The test consists of 19 items divided into four subtests: grasp, grip, pinch, and gross movement. For each item, the patient is asked to perform a simple task involving a functional movement of the affected upper-limb. Each task is rated with a 4-point ordinal scale (from 0: “not possible to perform the task” to 3: “performing the task normally”). The minimum score is 0 and the maximum is 57, with higher scores indicating a higher level of upper-limb functionality.
Working memory and attention were assessed using the Digit Span (forward and backward) subtest from the Wechsler Adult Intelligence Scale III (WAIS-IV, Wechsler, 2013). It consists of two parts: Digit Span Forward, in which participants are asked to repeat aloud a series of digits in the same order that gradually increases until the individual is unable to repeat the sequence; and Digit Span Backward, with the same procedure but the digits must be repeated in the reverse order. Scores are based on the longest length of sequence repeated correctly for each part. The minimum score is 0 and the maximum scores are 16 and 14 in the Forward and Backward parts, respectively. Raw scores were transformed into normative data considering individuals’ age according to Wechsler (2013), with higher scores indicating a higher capacity of attention and working memory.
Verbal learning and memory abilities were measured using the Spanish Version of the Rey Auditory Verbal Learning Test (RAVLT) (Marqués et al., 2013). In this test, participants are asked to listen and memorize a list of 15 unrelated words and immediately recall them for a total of five trials. Then, an interference list of 15 different unrelated words is presented and participants are asked to recall as many words as possible. After a 20-min delay, participants are asked to recall as many words as possible from the first list, and to complete a recognition task on both lists with distractors. For each task, the minimum score is 0 and the maximum is 15. The total sum words of the first five trials (0–75 score) were transformed into normative data considering individuals’ age according to Stricker et al. (2021), with higher scores indicating a higher capacity of verbal memory.
Depression was assessed using the Spanish version of the Beck Depression Inventory-II (BDI-II) (Beck et al., 1996; Sanz et al., 2003), a self-report measure comprised of 21 multiple-choice questions scored from 0 to 3 about patients’ feelings, thoughts, and behaviors over the past week. The minimum score is 0 and the maximum is 63, with higher scores indicating depression severity. The level of depression was defined following the cutoffs established by Beck and Beamesderfer (1974) for the stroke population: no depression (0–9 scores), mild depression (10–18 scores), moderate depression (19–29 scores), and severe depression (30–63 scores).
Anhedonia was assessed by calculating the total sum score of four items from the BDI-II that describe the symptoms of this behavioral trait according to Pizzagalli et al. (2005): loss of pleasure (item 4), loss of interest (item 12), loss of energy (item 15), and loss of interest in sex (item 21). The minimum score is 0 and the maximum is 12, with higher scores indicating higher anhedonia. Participants were classified into higher or lower levels of anhedonia following the cutoff obtained from calculating the 95% distribution value of the anhedonia BDI-II subscale score in HC, which was 4. Participants who obtained an anhedonia score greater than 4 were classified as higher anhedonic (HAnh), while those who obtained a score equal to or lower than 4 were classified as lower anhedonic (LAnh).
A non-anhedonic component of depression was calculated by subtracting the anhedonia BDI-II subscale score from the BDI-II total score, in order to explore the relationship between anhedonia and the non-anhedonic component of depression. The minimum score is 0 and the maximum 51, with higher scores indicating higher non-anhedonic depression. Individuals were classified into higher and lower levels of non-anhedonic depression following the cutoff obtained from calculating the 95% distribution value of the non-anhedonic depression BDI-II subscale score in HC, which was 16.65. Participants who obtained a non-anhedonic depression score greater than 16.65 were classified as higher non-anhedonic depressed (HDep), while those who obtained a score equal to or lower than 16.65 were classified as lower non-anhedonic depressed (LDep).
Apathy was evaluated using the Self-Rated Version of the Apathy Evaluation Scale (AES-S) and the Informant Version of the Apathy Evaluation Scale (AES-I), both translated into Spanish (Marin, 1991). The AES-S and AES-I consist of 18 items scored on a 4-point Likert scale (from 1: “a lot” to 4: “nothing”) about behavioral, cognitive, and emotional aspects of patients’ apathy over the past 4 weeks. The minimum score is 18 and the maximum 72, with higher scores indicating more apathy. The presence of apathy was defined following the cutoffs established by Andersson et al. (1999), indicating the presence of apathy in the stroke population when scoring equal or higher than 34 in both self- and informant-versions of the apathy scale (AES-S and AES-I).
Different dimensions of mood such as anger, vigor, fatigue, confusion, tension and depression levels were assessed with the Profile of Mood States (POMS) by asking the participant to rate feelings or emotions felt over the past week (McNair et al., 1971). This measure includes 65 items scored on a 5-point Likert scale (from 0: “not at all” to 4: “extremely”) and classified into the six subscales. The minimum score is 0 in all subscales, and the maximum scores are 48 in Anger-Hostility, 32 in Vigor-Activity and Tension-Anxiety, 28 in Fatigue-Inertia, 24 in Confusion-Bewilderment, and 60 in Depression-Dejection. Higher scores indicate higher levels of each mood dimension.
Absolute frequencies and percentages were calculated for the categorical variables: sex, stroke etiology, affected hemisphere, lesion location, global cognitive function level (MCI < 27 in MMSE; MCI < 26 in MoCA), depression level (none: 0–9 scores; mild: 10–18 scores; moderate: 19–29 scores; severe: 30–63 scores), anhedonia level (HAnh >4; LAnh ≤4), non-anhedonic depression level (HDep >16.65; LDep ≤16.65), and presence of apathy (scoring ≥34 in AES-S and AES-I). The mean and standard deviation (SD) were calculated for the quantitative variables with a parametric distribution: age, Digit Span, RAVLT, and Vigor-POMS score. The median and the interquartile range (IQR) were calculated for the quantitative variables with a nonparametric distribution: years of education, months post-stroke, and the scores on ARAT, MMSE, MoCA, anhedonia BDI-II subscale, AES-S, AES-I, BDI-II, non-anhedonic depression BDI-II subscale, and all POMS subscales. Regarding the level of global cognitive function, we combined MMSE and MoCA scores due to their strong correlation (r = 0.79) in subacute stroke patients (Toglia et al., 2011).
The differences between the three groups (SS, CS, and HC) were evaluated with two-way ANOVA test and Kruskal–Wallis test for independent samples for quantitative variables with parametric and nonparametric distribution, respectively, and Fisher’s exact test for categorical variables. Post-hoc analysis was conducted using Tukey’s and Dunn’s tests for continuous variables with parametric and nonparametric distribution, respectively, applying Bonferroni correction for multiple comparisons. We used Fisher’s exact test for pairwise comparisons of categorical variables between groups.
Considering that anhedonia level did not differ between subacute and chronic samples (see Descriptive analysis in Results), a secondary analysis was performed to explore the contribution of anhedonia to different factors in the stroke population. Thus, demographic, clinical, and emotional outcomes were compared between stroke patients classified as HAnh (scoring >4 in anhedonia BDI-II subscale) and LAnh (scoring ≤4 in anhedonia BDI-II subscale).
The anhedonia score was correlated with continuous demographic, clinical, and emotional variables to further explore which factors were related to anhedonia levels in both groups of patients (SS and CS). We used Spearman’s test to check correlations since anhedonia scores showed a nonparametric distribution.
Due to the strong correlation between anhedonia and non-anhedonic depression, partial correlation analyses were applied to explore the relationship between the anhedonia and the continuous demographic, clinical and emotional variables while controlling the influence of the non-anhedonic depression BDI-II subscale in subacute and chronic stroke patients, as well as in the whole sample of patients. Based on the strong correlation between anhedonia and the other emotional variables in both SS and CS groups (see Correlation analysis in Results), an additional analysis was performed comparing anhedonia level between stroke patients and the HC group while controlling for the confounding effects of total BDI-II score, non-anhedonic BDI-II subscale score, AES-S and AES-I scores, and all POMS subscales scores.
The descriptive and correlation statistical analyses were conducted using the R (version 4.2.2) and RStudio (version 2022.12.0 + 353), and the level of significance was set at 0.05.
There were no significant differences in age, years of education, stroke etiology, and affected hemisphere between groups (see Table 1). The SS showed a major distribution of stroke lesions in cortico-subcortical regions compared to the CS, which showed a major distribution in subcortical areas. Post-hoc analysis (see
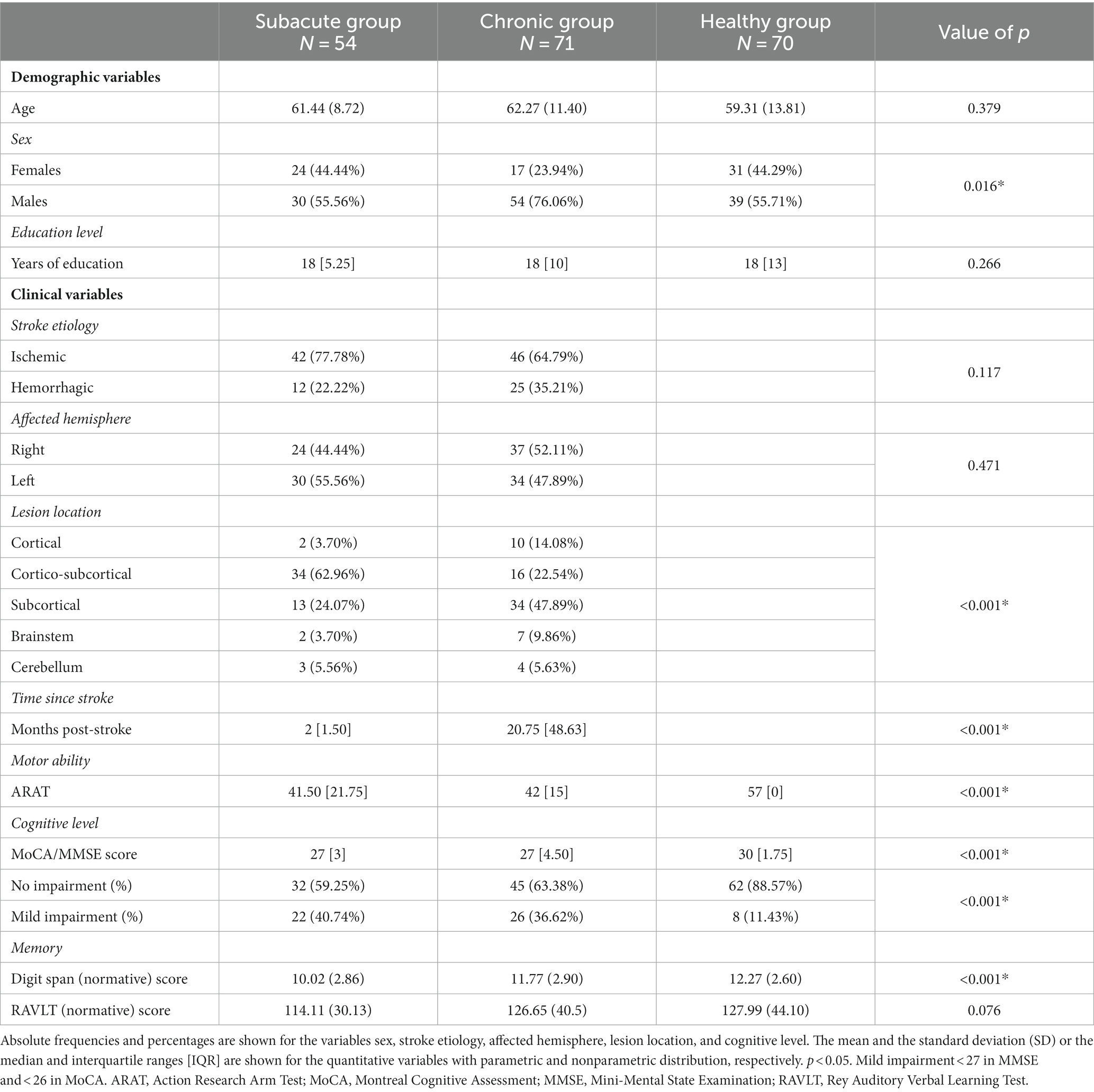
Table 1. Descriptive analysis of demographic and clinical variables.
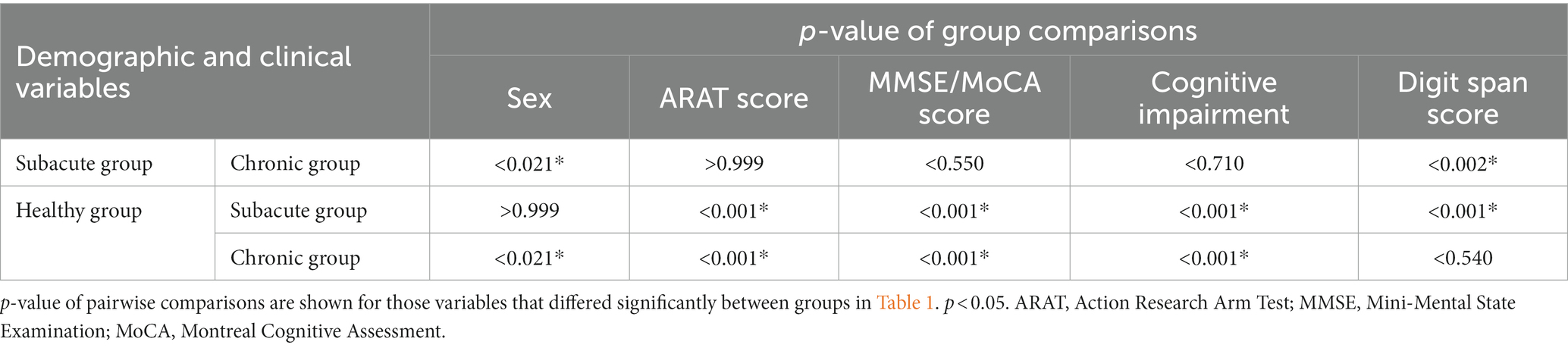
Table 2. Post-hoc analysis of demographic and clinical variables.
There were significant differences between groups in all emotional variables, except for the classification of non-anhedonic depression level (HDep >16.65 in non-anhedonic depression BDI-II subscale) and for the POMS, where groups only differed in Vigor-Activity subscale (see Table 3). Post-hoc analysis revealed that all significant differences were between HC and both groups of patients, who did not differ between them (see
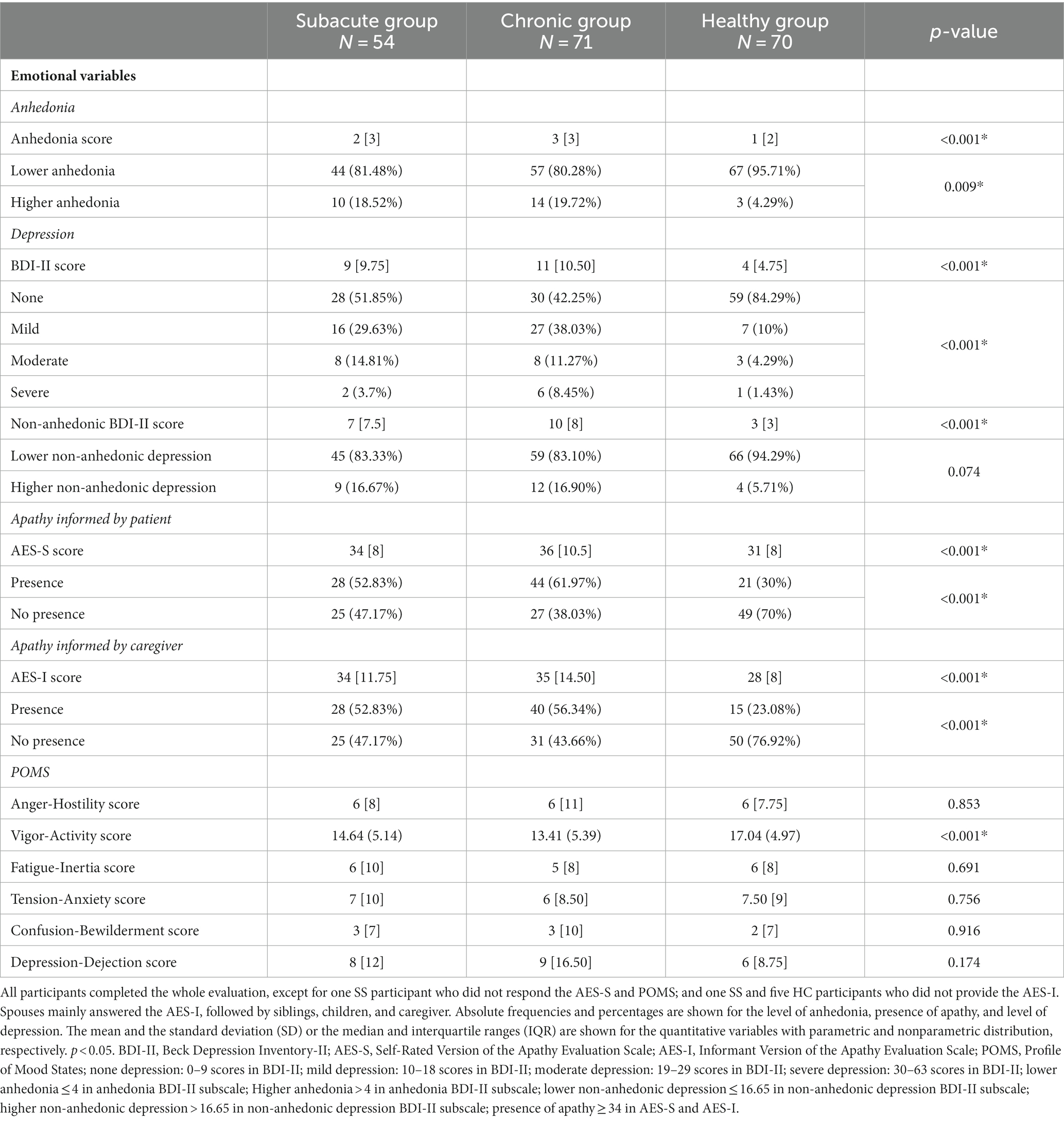
Table 3. Descriptive analysis of emotional variables.
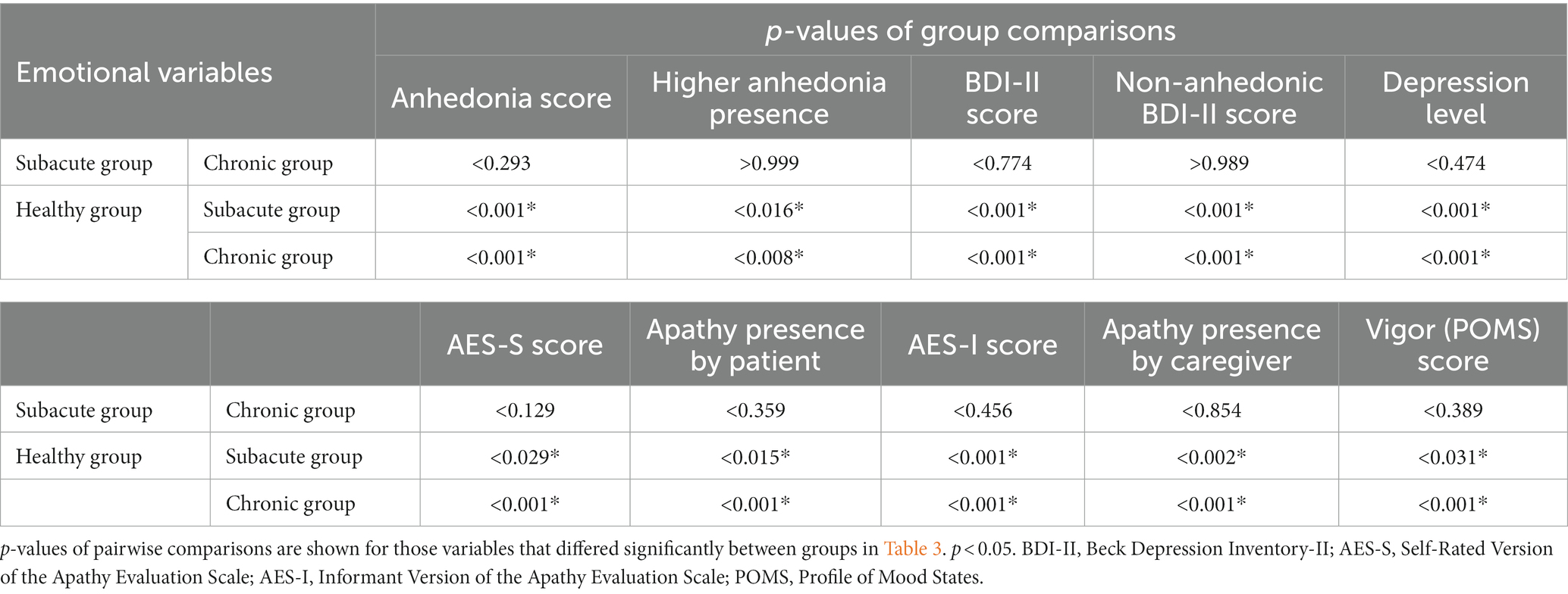
Table 4. Post-hoc analysis of emotional variables.
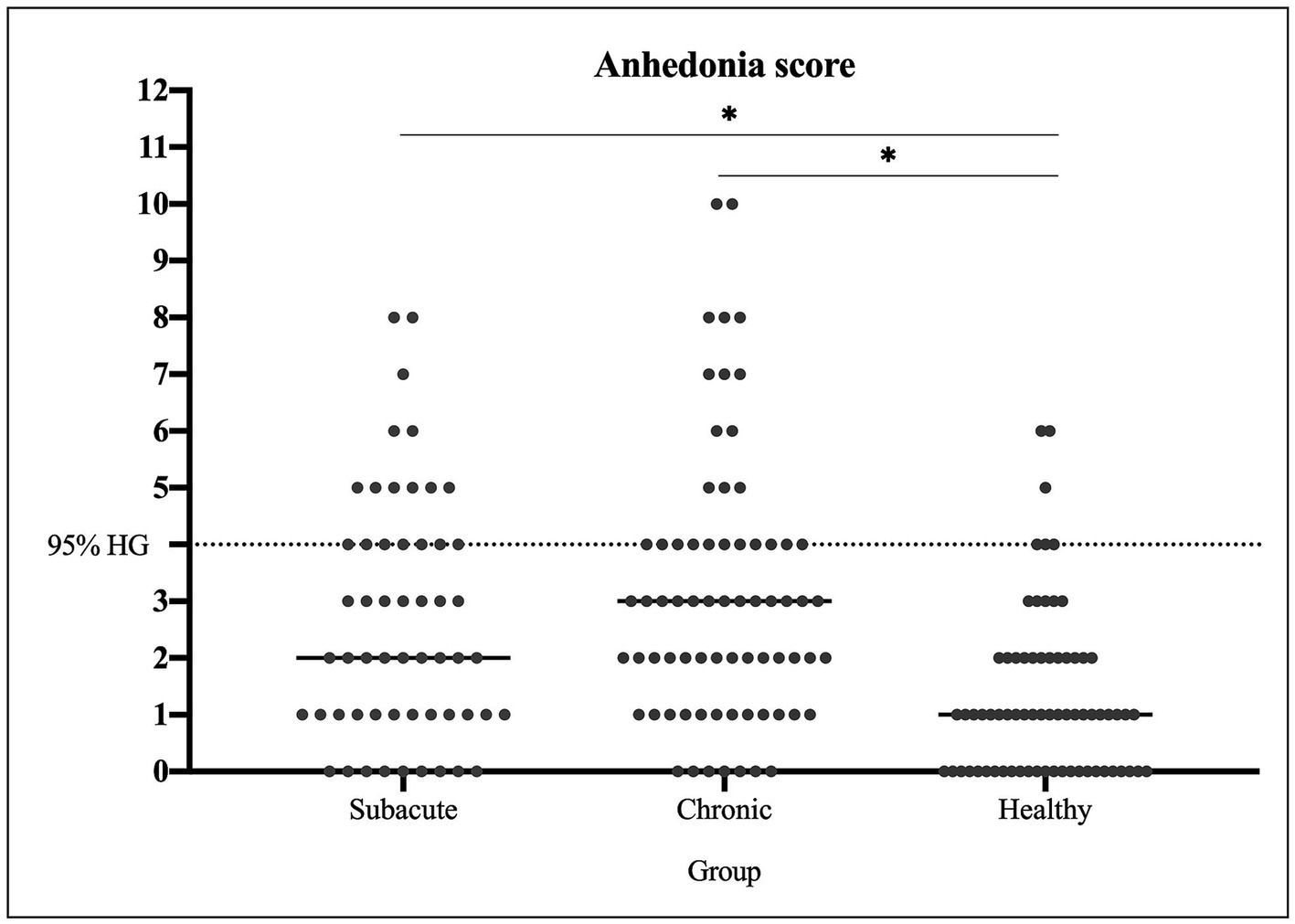
Figure 1. Anhedonia distribution between groups. Anhedonia score is shown for all individuals of each group: subacute stroke, chronic stroke, and healthy controls.
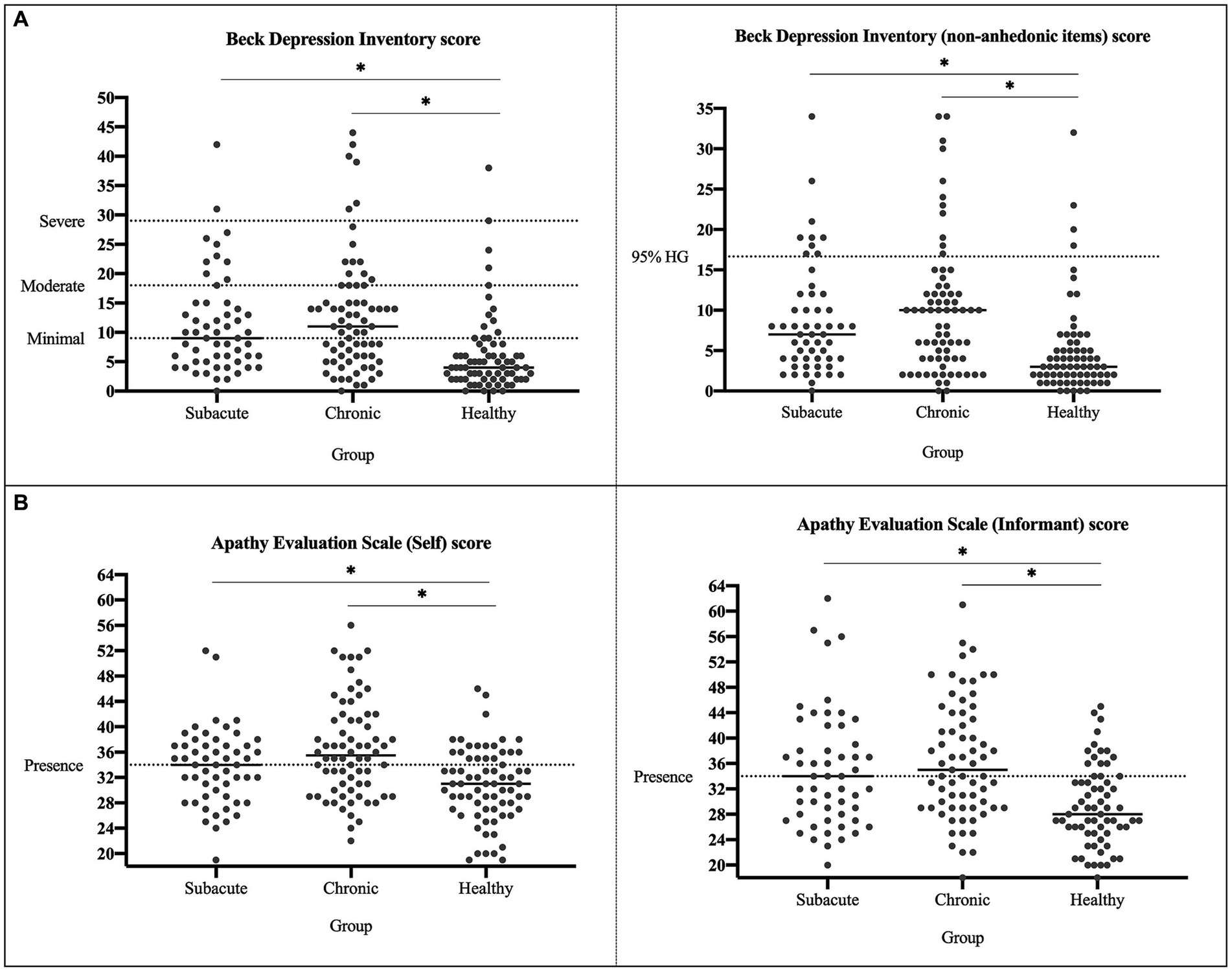
Figure 2. Apathy and depression distribution between groups. (A) Apathy scores of both self- and informant-versions are shown for all individuals from each group. (B) Depression scores with all the items and without the anhedonia items are shown for all individuals from each group.
When comparing demographic variables between stroke patients with different anhedonia level, HAnh patients (scoring >4 in anhedonia BDI-II subscale) showed significantly lower years of education than LAnh patients, while no differences were found on any clinical variable. At the emotional level, HAnh patients reported significantly higher levels of depression, apathy (AES-S and AES-I), Anger-Hostility, Fatigue-Inertia, Tension-Anxiety, and Confusion-Bewilderment, and significantly lower levels of Vigor-Activity compared to LAnh patients. While 70.83% of HAnh patients showed moderate and severe levels of depression (19–63 scores in BDI-II), with, 93.07% of LAnh patients demonstrated no or mild depression (0–18 scores in BDI-II), with none of them reaching the severe level. A significantly larger percentage of relatives reported presence of apathy (scoring ≥34 in AES-I) in HAnh patients (79.17%) compared to LAnh patients (49.50%). Interestingly, no differences were found in the proportion of patients classified as HDep (scoring >16.65 in non-anhedonic depression BDI-II subscale) and LDep between groups (see Supplementary Table S1).
Correlation analyses were applied to explore the association between anhedonia and the continuous demographic, clinical and emotional variables in SS and CS patients (see Figure 3; Supplementary Table S2). In both groups, anhedonia correlated positively with non-anhedonic depression BDI-II subscale and apathy scales (AES-S and AES-I), being AES-S more strongly correlated in CS than in SS patients (see Supplementary Figure S1). Moreover, anhedonia correlated with most POMS subscales, except for Vigor-Activity, which correlated negatively only in CS patients (see Figure 3; Supplementary Figure S2). The variable that correlated most strongly with the anhedonia in both groups was the non-anhedonic depression BDI-II subscale, followed by Fatigue-Inertia, Depression-Dejection, and Anger-Hostility of POMS. In CS patients, anhedonia correlated positively higher with AES-S compared to SS patients.
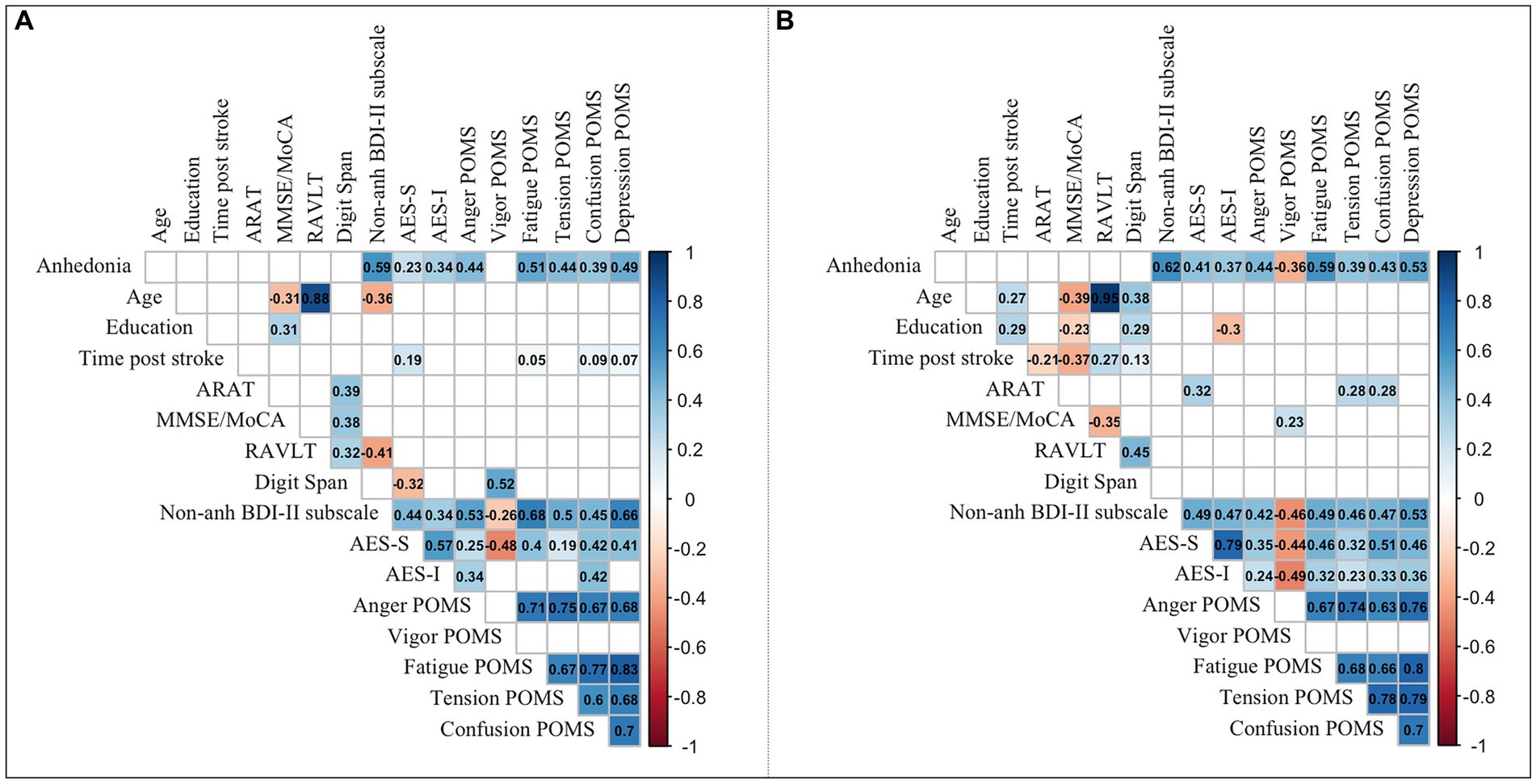
Figure 3. Correlations between demographic, clinical, and emotional variables. Significant correlation coefficients are shown for (A) subacute stroke patients, and (B) chronic stroke patients. p < 0.05. ARAT, Action Research Arm Test; MoCA, Montreal Cognitive Assessment; MMSE, Mini-Mental State Examination; RAVLT, Rey Auditory Verbal Learning Test; BDI-II, Beck Depression Inventory-II; AES-S, Self-Rated Version of the Apathy Evaluation Scale; AES-I, Informant Version of the Apathy Evaluation Scale; POMS, Profile of Mood States; POMS subscales: Anger-Hostility, Vigor-Activity, Fatigue-Inertia, Tension-Anxiety, Confusion-Bewilderment, Depression-Dejection.
Partial correlation analyses were applied to explore the relationship between the anhedonia and the continuous demographic, clinical and emotional variables while controlling for the influence of the non-anhedonic depression BDI-II subscale in subacute and chronic stroke patients, and in the whole sample of patients (see Figure 4; Supplementary Table S3). In SS patients, the anhedonia score correlated positively with time post-stroke (measured in days). By contrast, in CS patients, anhedonia positively correlated with patients’ age and three subscales of POMS: Anger-Hostility, Fatigue-Inertia, and Depression-Dejection. When looking at the whole sample of stroke patients, anhedonia correlated positively with age and four subscales of POMS: Anger-Hostility, Fatigue-Inertia, Confusion-Bewilderment, and Depression-Dejection.
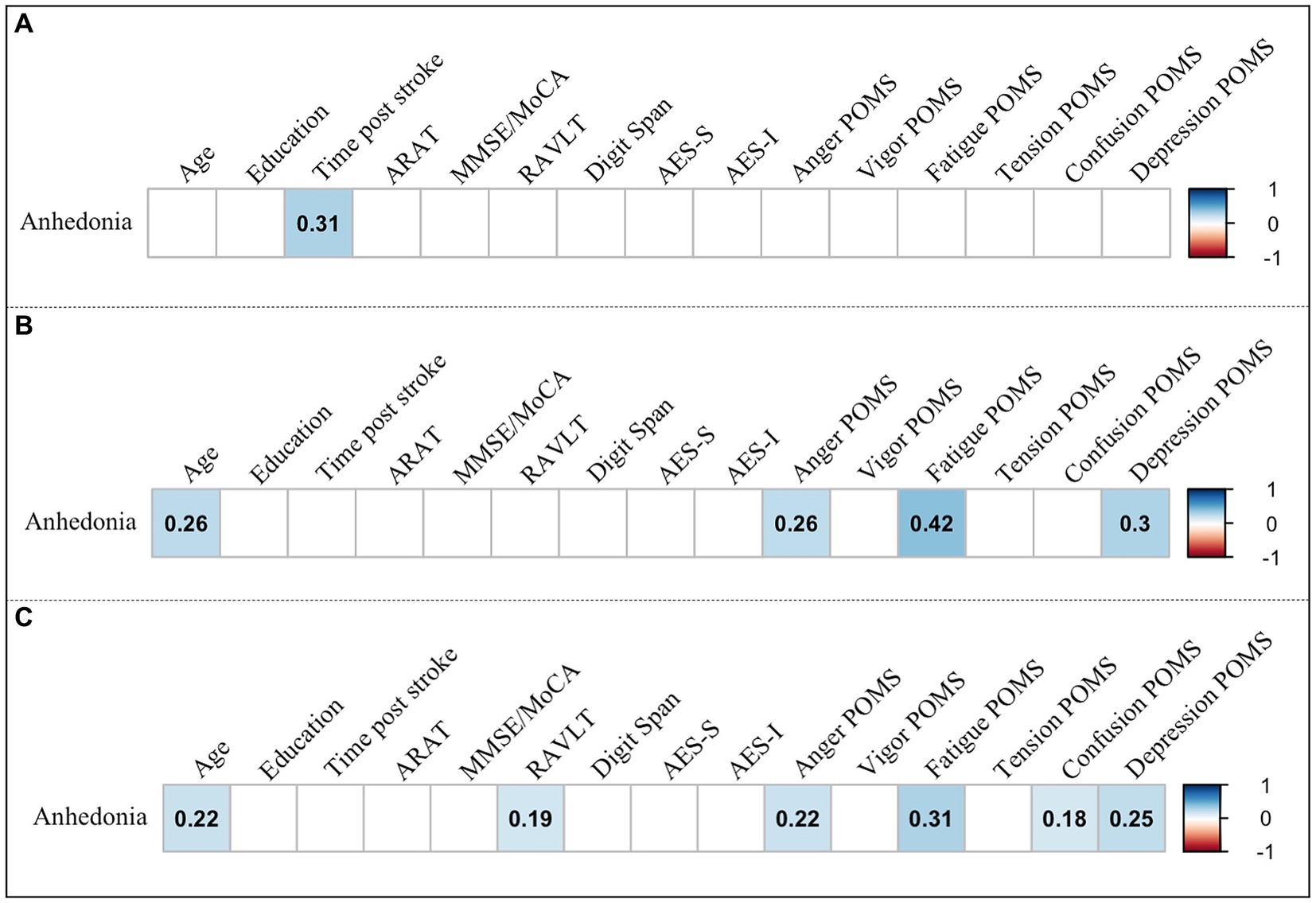
Figure 4. Partial correlations of anhedonia with demographic, clinical, and emotional variables. Significant correlation coefficients are shown for (A) subacute stroke, (B) chronic stroke, and (C) all stroke patients. p < 0.05. ARAT, Action Research Arm Test; MoCA, Montreal Cognitive Assessment; MMSE, Mini-Mental State Examination; RAVLT, Rey Auditory Verbal Learning Test; AES-S, Self-Rated Version of the Apathy Evaluation Scale; AES-I, Informant Version of the Apathy Evaluation Scale; POMS, Profile of Mood States; POMS subscales: Anger-Hostility, Vigor-Activity, Fatigue-Inertia, Tension-Anxiety, Confusion-Bewilderment, Depression-Dejection.
After comparing anhedonia level between stroke patients and HC while controlling for the confounding effects of the other emotional outcomes, we observed significant differences between stroke and healthy samples (t(189.72) = 5.95; p < 0.001; anhedonia mean score in stroke patients = 2.9 ± 2.3; anhedonia mean score in healthy controls = 1.3 ± 1.4).
Anhedonia is an enduring behavioral trait characterized by a lack of reactivity to pleasurable stimuli (Der-Avakian and Markou, 2012). Although anhedonia has been associated with high levels of depression at hospital discharge post-stroke, no previous studies have explored its prevalence in subacute and chronic stroke patients with both ischemic and hemorrhagic etiologies (Sibon et al., 2012). We conducted an exploratory cohort study to investigate the prevalence and level of anhedonia in stroke survivors with upper-limb motor deficits in the subacute and chronic phases of the disease covering a wide range of time since stroke, from 1 month to 17 years post-stroke. We examined demographic, clinical, cognitive, motor, and emotional factors that could be related to post-stroke anhedonia. The exploratory nature of the study aimed to check the usefulness and importance of assessing anhedonia and related factors in the stroke population at both early and late stages of the disease (Hallingberg et al., 2018).
Our results clearly showed that people who had suffered a stroke were significantly more anhedonic than people who never suffered a stroke with similar age and years of education. In both subacute and chronic stroke patients, nearly 18–20% of individuals showed a higher level of anhedonia, whereas only 4.3% of healthy controls. Importantly, studies on chronic pain and other inflammatory conditions have observed similar results (Lucido et al., 2021). For example, Garland et al. (2020) reported that nearly 25% of chronic pain patients exhibited higher anhedonia levels, which is in line with previous research demonstrating higher anhedonia levels in women suffering endometric chronic pelvic pain (Mallorqui et al., 2022). Additionally, a recent review revealed the relationship of acute and chronic stress with increased peripheral and central inflammation and consequent dysregulation of the reward system, leading to the onset or development of anhedonia (Boyle et al., 2023).
Patients with both subacute and chronic stroke showed similar levels of anhedonia regardless of stroke etiology, time since stroke, affected hemisphere, lesion location, and levels of motor and cognitive functions. In contrast to previous studies that found a correlation between stroke in the left frontal cortex or left basal ganglia and the risk for PSD (Starkstein and Robinson, 1989), the present results are in line with other studies that did not support the influence of the affected hemisphere and the exact lesion location on the development of emotional and mood disorders (Carson et al., 2000; Colita et al., 2023). Our findings align with a neurophysiological explanation based on the inflammatory effect on brain functioning, which has been increasingly recognized as a key factor in the onset or development of several psychiatric disorders, including depression (Hassamal, 2023). When an ischemic or hemorrhagic stroke occurs, it results in neuronal cell death and the release of cytokines that elicit localized inflammation in the damaged brain region, among other neurochemical events (Brouns and De Deyn, 2009; Fann et al., 2013). At 6 months post-stroke, in the chronic phase of the disease, inflammatory cytokines levels have been found to decrease in the infarct zone and increase in more distal ipsilateral and contralateral brain areas (Pascotini et al., 2015; Hou et al., 2021; Stuckey et al., 2021). Notably, neuroinflammatory cytokines provoke a decrease in dopamine and an increase in glutamate concentrations, reducing the functional connectivity between the ventral striatum and prefrontal cortex (Felger et al., 2016). The altered neurotransmission in the reward system would result in abnormal reward valuation, abnormal calculation of required effort, and deficits in decision-making for optimal reward-based actions, thus affecting hedonic capacity (Der-Avakian and Markou, 2012; Treadway et al., 2012; Cooper et al., 2018).
Although the state of neuroinflammation after several years post-stroke remains unknown, previous studies on ischemic stroke demonstrated that inflammatory cytokines released in the acute phase can lead to tissue damage and continued cell death in the injury site and penumbra (Tobin et al., 2014; Pascotini et al., 2015). This process has been associated with a more severe, prolonged, and treatment-resistant course of mood disorders (Hassamal, 2023). Hence, the chronic low-grade endogenous inflammation could continuously shape the pathology following stroke, promoting the ongoing impairment of the mesolimbic pathway in the long term regardless of lesion location, stroke etiology, and time since stroke (Shi et al., 2019; Stuckey et al., 2021). Additionally, these impairments in top-down cognitive-behavioral processes could alienate patients from natural and previously acquired resources of pleasure and positive experiences, potentially contributing to anhedonia development even years after stroke (Mallorqui et al., 2022).
Individuals with anhedonia are characterized by enjoying less of things in life by themselves and with others, which triggers a lack of interest in engaging in rewarding activities and participating in community life in the long term (Kusec et al., 2019). In the stroke population, this could affect the desire and motivation to initiate and complete interventions at various steps of the neurorehabilitation process, thus decreasing the likelihood of potential recovery. Engaging in rehabilitation programs has been strongly associated with improving motor, neurocognitive, psychological, biological, and socio-environmental outcomes (Maclean and Pound, 2000; Siegert and Taylor, 2004). In this vein, a negative loop could be installed in which high levels of anhedonia impede recovery, leading to a decrease in patients’ autonomy and emotional well-being, which in turn could increase anhedonia levels. In our results, stroke patients demonstrated significantly lower motor and cognitive functions than healthy controls, while no differences were found between subacute and chronic groups. Based on prior evidence suggesting a correlation between moderate or severe depression and poor functional outcomes in both subacute and chronic stroke phases (Pohjasvaara et al., 2001), we expected to find a correlation between anhedonia and functional impairments. However, no associations were observed between any functional outcome and the level of anhedonia and non-anhedonic depression in both groups of patients (see Supplementary Tables S1–S3). While improved mood has been correlated with a greater cognitive enhancement in depressed patients (Murata et al., 2000), the influence of PSD on motor recovery is not clear. Some studies found no difference in motor improvement between depressed and non-depressed patients (Nannetti et al., 2005), while others suggested a poor motor recovery in non-treated depressed stroke patients (Gainotti et al., 1997). In this vein, larger-scale longitudinal studies testing the score change in functional outcomes would be needed to explore the influence of post-stroke anhedonia on functional outcomes recovery.
Most stroke survivors must cope with a sudden reduction of their autonomy and QoL, a context that can trigger the onset or development of mood disorders such as depression, often manifesting with symptoms such as anhedonia (Der-Avakian and Markou, 2012; Feigin et al., 2017; Marcheschi et al., 2018). As expected, anhedonia post-stroke was associated with a lack of motivation and negative mood states. Both groups of patients were significantly more apathetic than healthy controls. Moreover, apathy was more strongly correlated with anhedonia in chronic patients. Importantly, the decrease in affection, enthusiasm, and interest caused by apathy has been associated with delayed rehabilitation, reduced social interaction, and increased caregiver burden, affecting the QoL of patients and their relatives (Åström et al., 1992; Hama et al., 2007). Anhedonia was also strongly related to negative mood states such as fatigue-inertia, and to a lesser extent, anger-hostility, depression-dejection, tension-anxiety, and confusion-bewilderment in both groups of patients. Only the chronic group showed a decreased sense of vigor-activity related to anhedonia, suggesting the long-term negative impact of anhedonia on engaging in a healthy active lifestyle. These results are in line with a recent previous study suggesting the role of anhedonia as a predictor of somatic symptoms of depression, such as fatigue, over the first year after discharge from rehabilitation (Ashaie et al., 2023). Our findings also underlines the likely role of anhedonia in generating a deteriorating looping effect at a behavioral level (Mallorqui et al., 2022). Additionally, older patients in the chronic group exhibited higher levels of anhedonia, consistent with previous research suggesting that the ageing brain is more sensitive to neurodegeneration mechanisms (Yan et al., 2010; Li et al., 2020; Stuckey et al., 2021). Consequently, older patients with stroke would be at a higher risk of suffering from anhedonia in the long term, not only due to the greater likelihood of social isolation (Yeh and Lo, 2004), but also because of the detrimental neurophysiological effects provoked by the brain injury. Crucially, anhedonia was significantly higher in stroke patients compared to healthy controls when controlling for the confounding effects of depression, apathy, fatigue, anger, vigor, tension, and confusion despite its strong correlation with them. This suggests the individual role of anhedonia as an emotional condition that can appear or increase in individuals after suffering a stroke.
The present study has some limitations. First, the results cannot be extrapolated to all stroke patients, as the sample was selected for its recovery potential to participate in intensive post-stroke rehabilitation programs. Therefore, the data we explored belong to a group of patients with a higher motivation and activity level than the entire stroke population. Moreover, due to the exploratory nature of this study, our sample of stroke patients was small and limited to those with upper-limb motor deficits. Considering that stroke patients also experience other neurological and cognitive impairments such as aphasia, execution dysfunction or memory disorders (Grönberg et al., 2022; Cramer et al., 2023), our inclusion criteria made the results not representative of the entire stroke population. However, motor impairment remains one of the most prevalent consequences after stroke, with approximately half of survivors experiencing impaired upper-limb movements in the chronic phase of the disease (Lee et al., 2015; Ingram et al., 2021). Additionally, the clinical characterization of lesion location was overly broad, constraining the extent to which meaningful conclusions can be drawn regarding the impact of this variable on the development of anhedonia. Lastly, due to the difficulty of recruiting patients with identical demographic and clinical characteristics, the stroke groups were unbalanced in terms of sex and lesion location, which could affect the association of these factors with anhedonia.
This exploratory cohort study provides valuable insights about the prevalence, level, and factors related to anhedonia in the stroke population. The results reveal an important increase in anhedonia among individuals with ischemic and hemorrhagic stroke and at both subacute and chronic stages compared to a sample of healthy individuals. Crucially, patients exhibited similar levels of anhedonia regardless of stroke etiology, time since stroke, affected hemisphere, lesion location, and levels of motor and cognitive functions. Furthermore, anhedonia was associated with a lack of motivation and higher levels of negative mood states such as fatigue and anger, thereby reducing emotional well-being and QoL, and presumably leading to a potential decrease in engagement with rehabilitation programs. Importantly, anhedonia levels were significantly superior in stroke patients compared to healthy controls when controlling for the confounding effects of depression, non-anhedonic depression, apathy, fatigue, anger, vigor, confusion, and tension, suggesting its individual role in the stroke population. Anhedonia has been identified as a stable trait over time with poor remission despite pharmacological, psychological or neurostimulation treatments (Shankman et al., 2010; Pizzagalli, 2022). For this reason, more research is needed to explore the presence of anhedonia in large-scale cohort and longitudinal studies, including stroke patients with other functional consequences, to test its influence on long-term functional and emotional recovery. Lastly, studying the prevalence of anhedonia in patients with other neurological and inflammatory diseases would contribute to a better understanding of the etiology of this condition and help develop more effective behavioral interventions to incorporate its treatment into stroke rehabilitation programs.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by ethics committees of Bellvitge University Hospital and Hospital del Mar. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
AR-F and JG-S conceived the study. AR-F, JG-S, and ES designed the study. ED, JG-S, and ES recruited the participants. ES, JG-S, and MP conducted and corrected the evaluations. ES and AV-B analyzed the data. ES, AM, and AR-F wrote the manuscript. All authors contributed to the article and approved the submitted version.
This work was supported by the Fundació La Marató de TV3 (2016, stroke and traumatic spinal cord and brain injury program) under grant number 201729.30, and by Ministerio de Ciencia e Innovación, which is part of Agencia Estatal de Investigación (AEI), through the Generación de Conocimiento, under grant number PID2021-127130NB-I00 / DOI: 10.13039/501100011033.
We gratefully acknowledge all the persons who participated in the study for their cooperation, as well as CERCA Programme / Generalitat de Catalunya for institutional support.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnagi.2024.1253028/full#supplementary-material
American Psychiatric Association (2013) Diagnostic and Statistical Manual of Mental Disorders. 5th, Washington, DC: APA Publishing.
Andersson, S., Krogstad, J. M., and Finset, A. (1999). Apathy and depressed mood in acquired brain damage: relationship to lesion localization and psychophysiological reactivity. Psychol. Med. 29, 447–456. doi: 10.1017/S0033291798008046
Ashaie, S. A., Funkhouser, C. J., Jabbarinejad, R., Cherney, L. R., and Shankman, S. A. (2023). Longitudinal trajectories of post-stroke depression symptom subgroups. Neurorehabil. Neural Repair 37, 46–52. doi: 10.1177/15459683221143464
Ashe, M. C., Miller, W. C., Eng, J. J., and Noreau, L.Physical Activity and Chronic Conditions Research Team (2009). Physical activity and chronic conditions research team: older adults, chronic disease and leisure-time physical activity. Gerontology 55, 64–72. doi: 10.1159/000141518.Older
Åström, M., Asplund, K., and Åström, T. (1992). Psychosocial function and life satisfaction after stroke. Stroke 23, 527–531. doi: 10.1161/01.STR.23.4.527
Auerbach, R. P., Pagliaccio, D., and Pizzagalli, D. A. (2019). Toward an improved understanding of anhedonia. JAMA Psychiatry 76, 571–573. doi: 10.1001/jamapsychiatry.2018.4600
Beck, A. T., and Beamesderfer, A. (1974). Assessment of depression: the depression inventory. Mod. Probl. Pharmacopsychiatry 7, 151–169. doi: 10.1159/000395074
Beck, A. T., Steer, R. A., and Brown, G. K. (1996) ‘Beck Depression Inventory-II’, TX: Psychological Corporation.
Bonanni, L., Gualtieri, F., Lester, D., Falcone, G., Nardella, A., Fiorillo, A., et al. (2019). Can anhedonia be considered a suicide risk factor? A review of the literature. Lietuvis̆koji Med. 55:458. doi: 10.3390/medicina55080458
Boyle, C. C., Bower, J. E., Eisenberger, N. I., and Irwin, M. R. (2023). Stress to inflammation and anhedonia: mechanistic insights from preclinical and clinical models. Neurosci. Biobehav. Rev. 152:105307. doi: 10.1016/j.neubiorev.2023.105307
Brouns, R., and De Deyn, P. P. (2009). The complexity of neurobiological processes in acute ischemic stroke. Clin. Neurol. Neurosurg. 111, 483–495. doi: 10.1016/j.clineuro.2009.04.001
Camara, E., Rodriguez-Fornells, A., and Münte, T. F. (2009). Functional connectivity of reward processing in the brain. Front. Hum. Neurosci. 2, 19–14. doi: 10.3389/neuro.09.019.2008
Carpinelli, L., Bucci, C., Santonicola, A., Zingone, F., Ciacci, C., and Iovino, P. (2019). Anhedonia in irritable bowel syndrome and in inflammatory bowel diseases and its relationship with abdominal pain. Neurogastroenterol. Motil. 31, e13531–e13537. doi: 10.1111/nmo.13531
Carson, A. J., MacHale, S., Allen, K., Lawrie, S. M., Dennis, M., House, A., et al. (2000). Depression after stroke and lesion location: a systematic review. Lancet 356, 122–126. doi: 10.1016/S0140-6736(00)02448-X
Chan, D. K., Lonsdale, C., Ho, P. Y., Yung, P. S., and Chan, K. M. (2009). Patient motivation and adherence to Postsurgery rehabilitation exercise recommendations: the influence of physiotherapists’ autonomy-supportive behaviors. Arch. Phys. Med. Rehabil. 90, 1977–1982. doi: 10.1016/j.apmr.2009.05.024
Colita, D., Burdusel, D., Glavan, D., Hermann, D. M., Colită, C. I., Colita, E., et al. (2023). Molecular mechanisms underlying major depressive disorder and post-stroke affective disorders. J. Affect. Disord. 344, 149–158. doi: 10.1016/j.jad.2023.10.037
Cooper, J. A., Arulpragasam, A. R., and Treadway, M. T. (2018). Anhedonia in depression: biological mechanisms and computational models. Curr. Opin. Behav. Sci. 22, 128–135. doi: 10.1016/j.cobeha.2018.01.024
Cramer, S. C., Richards, L. G., Bernhardt, J., and Duncan, P. (2023). Cognitive deficits after stroke. Stroke 54, 5–9. doi: 10.1161/STROKEAHA.122.041775
Cuthbert, B. N. (2021). The RDoC framework: facilitating transition from ICD/DSM to dimensional approaches that integrate neuroscience and psychopathology. Ann. Medico Psychol. 179, 75–85. doi: 10.1016/j.amp.2020.11.013
Der-Avakian, A., and Markou, A. (2012). The neurobiology of anhedonia and other reward-related deficits. Trends Neurosci. 35, 68–77. doi: 10.1016/j.tins.2011.11.005
Diamond, P. R., Dysch, L., and Daniels, J. (2023). Health anxiety in stroke survivors: a cross-sectional study on the prevalence of health anxiety in stroke survivors and its impact on quality of life. Disabil. Rehabil. 45, 27–33. doi: 10.1080/09638288.2021.2022778
Fann, D. Y. W., Lee, S. Y., Manzanero, S., Chunduri, P., Sobey, C. G., and Arumugam, T. V. (2013). Pathogenesis of acute stroke and the role of inflammasomes. Ageing Res. Rev. 12, 941–966. doi: 10.1016/j.arr.2013.09.004
Feigin, V. L., Nichols, E., Alam, T., Bannick, M. S., Beghi, E., Blake, N., et al. (2019). Global, regional, and national burden of neurological disorders, 1990–2016: a systematic analysis for the global burden of disease study 2016. Lancet Neurol. 18, 459–480. doi: 10.1016/S1474-4422(18)30499-X
Feigin, V. L., Norrving, B., and Mensah, G. A. (2017). Global burden of stroke. Circ. Res. 120, 439–448. doi: 10.1161/CIRCRESAHA.116.308413
Felger, J. C., Li, Z., Haroon, E., Woolwine, B. J., Jung, M. Y., Hu, X., et al. (2016). Inflammation is associated with decreased functional connectivity within corticostriatal reward circuitry in depression. Mol. Psychiatry 21, 1358–1365. doi: 10.1038/mp.2015.168
Folstein, M. F., and Folstein, S. E. (1975). “Mini-mental state”: a practical method for grading the cognitive state of patients for the clinician. J. Psychiatry 12, 189–198. doi: 10.3744/snak.2003.40.2.021
Gainotti, G., Antonucci, G., Marra, C., and Paolucci, S. (2001). Relation between depression after stroke, antidepressant therapy, and functional recovery. J. Neurol. Neurosurg. Psychiatry 71, 258–261. doi: 10.1136/jnnp.71.2.258
Gainotti, G., Azzoni, A., Razzano, C., Lanzillotta, M., Marra, C., and Gasparini, F. (1997). The post-stroke depression rating scale: a test specifically devised to investigate affective disorders of stroke patients. J. Clin. Exp. Neuropsychol. 19, 340–356. doi: 10.1080/01688639708403863
Gallego, M. L., Ferrándiz, M. H., Garriga, O. T., Nierga, I. P., López-Pausa, S., and Franch, J. V. (2009). Validación del Montreal Cognitive Assessment (MoCA): test de cribado para el deterioro cognitivo leve. Datos preliminares. Alzheimer. Real Invest Demenc. 43, 4–11.
Garland, E. L., Trøstheim, M., Eikemo, M., Ernst, G., and Leknes, S. (2020). Anhedonia in chronic pain and prescription opioid misuse. Psychol. Med. 50, 1977–1988. doi: 10.1017/S0033291719002010
Gong, L., Yin, Y., He, C., Ye, Q., Bai, F., Yuan, Y., et al. (2017). Disrupted reward circuits is associated with cognitive deficits and depression severity in major depressive disorder. J. Psychiatr. Res. 84, 9–17. doi: 10.1016/j.jpsychires.2016.09.016
Grau-Sánchez, J., Duarte, E., Ramos-Escobar, N., Sierpowska, J., Rueda, N., Redón, S., et al. (2018). Music-supported therapy in the rehabilitation of subacute stroke patients: a randomized controlled trial. Ann. N. Y. Acad. Sci. 1423, 318–328. doi: 10.1111/nyas.13590
Grau-Sánchez, J., Segura, E., Sanchez-Pinsach, D., Raghavan, P., Münte, T. F., Palumbo, A. M., et al. (2021). Enriched music-supported therapy for chronic stroke patients: a study protocol of a randomised controlled trial. BMC Neurol. 21, 19–16. doi: 10.1186/s12883-020-02019-1
Grönberg, A., Henriksson, I., Stenman, M., and Lindgren, A. G. (2022). Incidence of aphasia in ischemic stroke. Neuroepidemiology 56, 174–182. doi: 10.1159/000524206
Hallingberg, B., Turley, R., Segrott, J., Wight, D., Craig, P., Moore, L., et al. (2018). Exploratory studies to decide whether and how to proceed with full-scale evaluations of public health interventions: a systematic review of guidance. Pilot Feasibil. Stud. 4, 104–112. doi: 10.1186/s40814-018-0290-8
Hama, S., Yamashita, H., Shigenobu, M., Watanabe, A., Hiramoto, K., Kurisu, K., et al. (2007). Depression or apathy and functional recovery after stroke. Int. J. Geriatr. Psychiatry 22, 1046–1051. doi: 10.1002/gps.1866
Hartman-Maeir, A., Soroker, N., Ring, H., Avni, N., and Katz, N. (2007). Activities, participation and satisfaction one-year post stroke. Disabil. Rehabil. 29, 559–566. doi: 10.1080/09638280600924996
Hassamal, S. (2023). Chronic stress, neuroinflammation, and depression: an overview of pathophysiological mechanisms and emerging anti-inflammatories. Front. Psych. 14:1130989. doi: 10.3389/fpsyt.2023.1130989
Hou, D., Wang, C., Ye, X., Zhong, P., and Wu, D. (2021). Persistent inflammation worsens short-term outcomes in massive stroke patients. BMC Neurol. 21, 62–68. doi: 10.1186/s12883-021-02097-9
Ingram, L. A., Butler, A. A., Brodie, M. A., Lord, S. R., and Gandevia, S. C. (2021). Quantifying upper limb motor impairment in chronic stroke: a physiological profiling approach. J. Appl. Physiol. 131, 949–965. doi: 10.1152/japplphysiol.00078.2021
Katan, M., and Luft, A. (2018). Global burden of stroke. Semin. Neurol. 38, 208–211. doi: 10.1055/s-0038-1649503
Kusec, A., Velikonja, D., DeMatteo, C., and Harris, J. E. (2019). Motivation in rehabilitation and acquired brain injury: can theory help us understand it? Disabil. Rehabil. 41, 2343–2349. doi: 10.1080/09638288.2018.1467504
Kwakkel, G., Kollen, B. J., van der Grond, J., and Prevo, A. J. H. (2003). Probability of regaining dexterity in the flaccid upper limb: impact of severity of paresis and time since onset in acute stroke. Stroke 34, 2181–2186. doi: 10.1161/01.STR.0000087172.16305.CD
Lee, K. B., Lim, S. H., Kim, K. H., Kim, K. J., Kim, Y. R., Chang, W. N., et al. (2015). Six-month functional recovery of stroke patients: a multi-time-point study. Int. J. Rehabil. Res. 38, 173–180. doi: 10.1097/MRR.0000000000000108
Li, T., Huang, Y., Cai, W., Chen, X., Men, X., Lu, T., et al. (2020). Age-related cerebral small vessel disease and inflammaging. Cell Death Dis. 11:932. doi: 10.1038/s41419-020-03137-x
Lobo, A. (1999). Erratum: Revalidacion y normalizacion del mini-examen cognoscitivo (primera version en castellano del mini-mental status examination) en la poblacion general geriatrica (Medicina Clinica (1999) 112 (767-774)). Med. Clinica 113:197.
Lucido, M. J., Bekhbat, M., Goldsmith, D. R., Treadway, M. T., Haroon, E., Felger, J. C., et al. (2021). Aiding and abetting anhedonia: impact of inflammation on the brain and pharmacological implications. Pharmacol. Rev. 73, 1084–1117. doi: 10.1124/pharmrev.120.000043
Lyle, R. C. (1981). A performance test for assessment of upper limb function in physical rehabilitation treatment and research. Int. J. Rehabil. Res. 4, 483–492. doi: 10.1097/00004356-198112000-00001
Maclean, N., and Pound, P. (2000). A critical review of the concept of patient motivation in the literature on physical rehabilitation. Soc. Sci. Med. 50, 495–506. doi: 10.1016/S0277-9536(99)00334-2
Mallorqui, A., Martinez-Zamora, M.-A., and Carmona, F. (2022). Anhedonia in endometriosis: an unexplored symptom. Front. Psychol. 13:935349. doi: 10.3389/fpsyg.2022.935349
Marcheschi, E., von Koch, L., Pessah-Rasmussen, H., and Elf, M. (2018). Home setting after stroke, facilitators and barriers: a systematic literature review. Health Soc. Care Community 26, e451–e459. doi: 10.1111/hsc.12518
Marin, R. S. (1991). Apathy: a neuropsychiatric syndrome. J. Neuropsychiatry Clin. Neurosci. 3, 243–254. doi: 10.1176/jnp.3.3.243
Marqués, N. O., Caro, I. A., Uterga Valiente, J. M., and Rodríguez, S. M. (2013). Normative data for a Spanish version of the Rey auditory-verbal learning test in older people. Span. J. Psychol. 16, E60–E12. doi: 10.1017/sjp.2013.63
McNair, D. M., Lorr, M., and Droppleman, L. F. (1971) ‘Manual for the Profile of Mood States ’, CA: Educational and Industrial Testing Services.
Murata, Y., Kimura, M., and Robinson, R. G. (2000). Does cognitive impairment cause poststroke depression? Am. J. Geriatr. Psychiatr. 8, 310–317. doi: 10.1097/00019442-200011000-00007
Nannetti, L., Paci, M., Pasquini, J., Lombardi, B., and Taiti, P. G. (2005). Motor and functional recovery in patients with post-stroke depression. Disabil. Rehabil. 27, 170–175. doi: 10.1080/09638280400009378
Nasreddine, Z. S., Phillips, N. A., Bédirian, V., Charbonneau, S., Whitehead, V., Collin, I., et al. (2005). The Montreal cognitive assessment, MoCA: a brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 53, 695–699. doi: 10.1111/j.1532-5415.2005.53221.x
Paolucci, S., Iosa, M., Coiro, P., Venturiero, V., Savo, A., de Angelis, D., et al. (2019). Post-stroke depression increases disability more than 15% in ischemic stroke survivors: a case-control study. Front. Neurol. 10, 1–9. doi: 10.3389/fneur.2019.00926
Pascotini, E. T., Flores, A. E., Kegler, A., Gabbi, P., Bochi, G. V., Algarve, T. D., et al. (2015). Apoptotic markers and DNA damage are related to late phase of stroke: involvement of dyslipidemia and inflammation. Physiol. Behav. 151, 369–378. doi: 10.1016/j.physbeh.2015.08.005
Patel, M. D., Coshall, C., Rudd, A. G., and Wolfe, C. D. A. (2002). Cognitive impairment after stroke: clinical determinants and its associations with long-term stroke outcomes. J. Am. Geriatr. Soc. 50, 700–706. doi: 10.1046/j.1532-5415.2002.50165.x
Pendlebury, S. T., Markwick, A., de Jager, C. A., Zamboni, G., Wilcock, G. K., and Rothwell, P. M. (2012). Differences in cognitive profile between TIA, stroke and elderly memory research subjects: a comparison of the MMSE and MoCA. Cerebrovasc. Dis. 34, 48–54. doi: 10.1159/000338905
Pereiro, A. X., Ramos-Lema, S., Lojo-Seoane, C., Guàrdia-Olmos, J., Facal-Mayo, D., and Juncos-Rabadán, O. (2017). Normative data for the Montreal cognitive assessment (MOCA) in a Spanish sample of community-dweller adults. Eur. Geriatr. Med. 8, 240–244. doi: 10.1016/j.eurger.2017.04.003
Piamarta, F., Iurlaro, S., Isella, V., Atzeni, L., Grimaldi, M., Russo, A., et al. (2004). Unconventional affective symptoms and executive functions after stroke in the elderly. Arch. Gerontol. Geriatr. Suppl. 9, 315–323. doi: 10.1016/j.archger.2004.04.042
Pizzagalli, D. A. (2022). Toward a better understanding of the mechanisms and pathophysiology of anhedonia: are we ready for translation? Am. J. Psychiatry 179, 458–469. doi: 10.1176/appi.ajp.20220423
Pizzagalli, D. A., Jahn, A. L., and O’Shea, J. P. (2005). Toward an objective characterization of an anhedonic phenotype: a signal-detection approach. Biol. Psychiatry 57, 319–327. doi: 10.1016/j.biopsych.2004.11.026
Platz, T., Pinkowski, C., van Wijck, F., Kim, I. H., di Bella, P., and Johnson, G. (2005). Reliability and validity of arm function assessment with standardized guidelines for the Fugl-Meyer test, action research arm test and box and block test: a multicentre study. Clin. Rehabil. 19, 404–411. doi: 10.1191/0269215505cr832oa
Pohjasvaara, T., Vataja, R., Leppävuori, A., Kaste, M., and Erkinjuntti, T. (2001). Depression is an independent predictor of poor long-term functional outcome post-stroke. Eur. J. Neurol. 8, 315–319. doi: 10.1046/j.1468-1331.2001.00182.x
Ren, H., Fabbri, C., Uher, R., Rietschel, M., Mors, O., Henigsberg, N., et al. (2018). Genes associated with anhedonia: a new analysis in a large clinical trial (GENDEP). Transl. Psychiatry 8:150. doi: 10.1038/s41398-018-0198-3
Ripollés, P., Rojo, N., Grau-Sánchez, J., Amengual, J. L., Càmara, E., Marco-Pallarés, J., et al. (2016). Music supported therapy promotes motor plasticity in individuals with chronic stroke. Brain Imaging Behav. 10, 1289–1307. doi: 10.1007/s11682-015-9498-x
Sanz, J., Perdigón, A. L., and Vázquez, C. (2003). The spanish adaptation of Beck’s Depression Inventory-II (BDI-II): 2. Psychometric properties in the general population’. Clinica y Salud 14, 249–280.
Shankman, S. A., Nelson, B. D., Harrow, M., and Faull, R. (2010). Does physical anhedonia play a role in depression? A 20-year longitudinal study. J. Affect. Disord. 120, 170–176. doi: 10.4324/9781315609607-7
Shi, K., Tian, D. C., Li, Z. G., Ducruet, A. F., Lawton, M. T., and Shi, F. D. (2019). Global brain inflammation in stroke. Lancet Neurol. 18, 1058–1066. doi: 10.1016/S1474-4422(19)30078-X
Sibon, I., Lassalle-Lagadec, S., Renou, P., and Swendsen, J. (2012). Evolution of depression symptoms following stroke: a prospective study using computerized ambulatory monitoring. Cerebrovasc. Dis. 33, 280–285. doi: 10.1159/000334663
Siegert, R. J., and Taylor, W. J. (2004). Theoretical aspects of goal-setting and motivation in rehabilitation. Disabil. Rehabil. 26, 1–8. doi: 10.1080/09638280410001644932
Starkstein, S. E., and Robinson, R. G. (1989). Affective disorders and cerebral vascular disease. Br. J. Psychiatry 154, 170–182. doi: 10.1192/bjp.154.2.170
Stricker, N. H., Christianson, T. J., Lundt, E. S., Alden, E. C., Machulda, M. M., Fields, J. A., et al. (2021). Mayo normative studies: regression-based normative data for the auditory verbal learning test for ages 30-91 years and the importance of adjusting for sex. J. Int. Neuropsychol. Soc. 27, 211–226. doi: 10.1017/S1355617720000752
Stuckey, S. M., Ong, L. K., Collins-Praino, L. E., and Turner, R. J. (2021). Neuroinflammation as a key driver of secondary neurodegeneration following stroke? Int. J. Mol. Sci. 22:13101. doi: 10.3390/ijms222313101
Sullivan, J. E., Crowner, B. E., Kluding, P. M., Nichols, D., Rose, D. K., Yoshida, R., et al. (2013). Outcome measures for individuals with stroke: process and recommendations from the American physical therapy association neurology section task force. Phys. Ther. 93, 1383–1396. doi: 10.2522/ptj.20120492
Tang, E. Y. H., Price, C., Stephan, B. C. M., Robinson, L., and Exley, C. (2020). Impact of memory problems post-stroke on patients and their family Carers: a qualitative study. Front. Med. 7:267. doi: 10.3389/fmed.2020.00267
Terroni, L., Amaro, E. Jr., Iosifescu, D. V., Mattos, P., Yamamoto, F. I., Tinone, G., et al. (2015). The association of post-stroke anhedonia with salivary cortisol levels and stroke lesion in hippocampal/parahippocampal region. Neuropsychiatr. Dis. Treat. 11, 233–242. doi: 10.2147/NDT.S73722
Tobin, M. K., Bonds, J. A., Minshall, R. D., Pelligrino, D. A., Testai, F. D., and Lazarov, O. (2014). Neurogenesis and inflammation after ischemic stroke: what is known and where we go from here. J. Cereb. Blood Flow Metab. 34, 1573–1584. doi: 10.1038/jcbfm.2014.130
Toglia, J., Fitzgerald, K. A., O'Dell, M. W., Mastrogiovanni, A. R., and Lin, C. D. (2011). The mini-mental state examination and Montreal cognitive assessment in persons with mild subacute stroke: relationship to functional outcome. Arch. Phys. Med. Rehabil. 92, 792–798. doi: 10.1016/j.apmr.2010.12.034
Treadway, M. T., Bossaller, N. A., Shelton, R. C., and Zald, D. H. (2012). Effort-based decision-making in major depressive disorder: a translational model of motivational anhedonia. J. Abnorm. Psychol. 121, 553–558. doi: 10.1037/a0028813
Van Der Lee, J. H., Beckerman, H., Lankhorst, G. J., and Bouter, L. M. (2001). The responsiveness of the Action Research Arm test and the Fugl-Meyer Assessment scale in chronic stroke patients. J Rehabil Med 33, 110–113. doi: 10.1080/165019701750165916
Verrienti, G., Raccagni, C., Lombardozzi, G., de Bartolo, D., and Iosa, M. (2023). Motivation as a measurable outcome in stroke rehabilitation: a systematic review of the literature. Int. J. Environ. Res. Public Health 20:4187. doi: 10.3390/ijerph20054187
Wechsler, D. (2013) ‘Escala de Memoria de Wechsler-IV Manual Técnico y de Interpretación ’, Madric: NCS Pearson, Inc.
Whyte, E. M., and Mulsant, B. H. (2002). Post stroke depression: epidemiology, pathophysiology, and biological treatment. Biol. Psychiatry 52, 253–264. doi: 10.1016/S0006-3223(02)01424-5
Yan, T., Feng, Y., and Zhai, Q. (2010). Axon degeneration: mechanisms and implications of a distinct program from cell death. Neurochem. Int. 56, 529–534. doi: 10.1016/j.neuint.2010.01.013
Keywords: subacute and chronic stroke, anhedonia, depression, motivation, rehabilitation
Citation: Segura E, Vilà-Balló A, Mallorquí A, Porto MF, Duarte E, Grau-Sánchez J and Rodríguez-Fornells A (2024) The presence of anhedonia in individuals with subacute and chronic stroke: an exploratory cohort study. Front. Aging Neurosci. 16:1253028. doi: 10.3389/fnagi.2024.1253028
Edited by:
Michelle Dow Keawphalouk Narangajavana, Massachusetts Institute of Technology, United StatesReviewed by:
Faisal Alotaibi, King Faisal Specialist Hospital and Research Centre, Saudi ArabiaCopyright © 2024 Segura, Vilà-Balló, Mallorquí, Porto, Duarte, Grau-Sánchez and Rodríguez-Fornells. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Antoni Rodríguez-Fornells, YW50b25pLnJvZHJpZ3VlekBpY3JlYS5jYXQ=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.