
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Aging Neurosci. , 03 January 2024
Sec. Parkinson’s Disease and Aging-related Movement Disorders
Volume 15 - 2023 | https://doi.org/10.3389/fnagi.2023.1292524
This article is part of the Research Topic Translational Advances in Lewy Body Diseases and Other Related Movement Disorders: Mechanisms, Biomarkers, Diagnosis, and Therapies View all 7 articles
 Sung Hoon Kang1
Sung Hoon Kang1 Yunjin Choi2
Yunjin Choi2 Su Jin Chung3Seok-Joo Moon4
Su Jin Chung3Seok-Joo Moon4 Chi Kyung Kim1Ji Hyun Kim1Kyungmi Oh1
Chi Kyung Kim1Ji Hyun Kim1Kyungmi Oh1 Joon Shik Yoon5Sang Won Seo6,7Geum Joon Cho8Seong-Beom Koh1*
Joon Shik Yoon5Sang Won Seo6,7Geum Joon Cho8Seong-Beom Koh1*Background: Diabetes is associated with an increased risk of Parkinson’s disease dementia (PDD); however, it is unknown whether this association is dependent on continuous hyperglycemia, hypoglycemic events, or glycemic variability. We aimed to investigate the relationship between visit-to-visit fasting glucose variability and PDD development in patients with Parkinson’s disease (PD).
Methods: Using data from the Korean National Health Insurance Service, we examined 9,264 patients aged ≥40 years with de novo Parkinson’s disease (PD) who underwent ≥3 health examinations and were followed up until December 2019. Glucose variability was measured using the coefficient of variation, variability independent of the mean, and average real variability. Fine and Gray competing regression analysis was performed to determine the effect of glucose variability on incident PDD.
Results: During the 9.5-year follow-up period, 1,757 of 9,264 (19.0%) patients developed PDD. Patients with a higher visit-to-visit glucose variability had a higher risk of future PDD. In the multivariable adjusted model, patients with PD in the highest quartile (subdistribution hazard ratio [SHR] = 1.50, 95% CI 1.19 to 1.88), quartile 3 (SHR = 1.29, 95% CI 1.02 to 1.62), and quartile 2 (SHR = 1.30, 95% CI 1.04 to 1.63) were independently associated with a higher risk of PDD than those in the lowest quartile.
Conclusion: We highlighted the effect of long-term glucose variability on the development of PDD in patients with PD. Furthermore, our findings suggest that preventive measures for constant glucose control may be necessary to prevent PDD.
Parkinson’s disease (PD) is a common neurodegenerative disease characterized by the deterioration of motor function (Ko et al., 2022). Patients with PD may also exhibit non-motor symptoms, including cognitive dysfunction. The incidence of Parkinson’s disease dementia (PDD) has been increasing because of longer survival resulting from advanced treatment methods (Kang et al., 2023). PDD leads to a reduced quality of life and poor prognosis; therefore, identifying modifiable risk factors for PDD is important for designing strategies to prevent the development of PDD in patients with PD.
Growing evidence has shown that patients with diabetes have a higher incidence of PD and dementia, including Alzheimer’s disease dementia and vascular dementia (Curb et al., 1999; Chornenkyy et al., 2019; Cheong et al., 2020). Several studies have proposed that PD patients with diabetes may have an increased risk of cognitive dysfunction and PDD. Cross-sectional studies have shown diabetes to be independently associated with more severe cognitive dysfunction in PD (Bohnen et al., 2014; Giuntini et al., 2014). In one longitudinal study, PD patients with diabetes had a greater progression of cortical atrophy, leading to cognitive decline (Ong et al., 2017). One meta-analysis found that diabetes increased the risk of PDD (Guo et al., 2019). However, it remains unknown whether this association is dependent on continuous hyperglycemia, hypoglycemic events, or glycemic variability.
Recently, several studies have suggested an association between higher glucose variability and oxidative stress, inflammatory processes, and insulin resistance (Monnier et al., 2006; Ceriello et al., 2008), leading to cardiovascular disease and mortality regardless of baseline glucose levels (Gorst et al., 2015; Wang et al., 2017). Previous studies have also reported that patients with higher glucose variability have an increased risk of incident dementia and PD, irrespective of the presence of diabetes (Lee et al., 2018; Chung et al., 2021). Given these findings, higher glucose variability may be an independent predictor of PDD in patients with PD.
Using the Korean National Health Insurance Service (KNHIS) data, our study aimed to investigate the association between visit-to-visit fasting glucose variability and the risk of incident PDD in patients with PD. We hypothesized that higher glucose variability might be an independent risk factor for PDD due to its shared pathogenesis with vascular dementia and primary degeneration in the subcortical regions (Pillon et al., 1993).
This study was approved by the Institutional Review Board of the Korea University Guro Hospital and adhered to the principles of the Declaration of Helsinki. Anonymous and de-identified information was used for analysis; therefore, informed consent was not obtained.
We used a customized dataset from the KNHIS, which includes more than 99% of the Korean population (approximately 50 million individuals).1 The KNHIS database includes personal information, health insurance claim codes (procedures and prescriptions), diagnostic codes from the Korean Standard Classification of Diseases, 7th Revision, based on the International Classification of Diseases, 10th Revision (ICD-10), death records from the Korean National Statistical Office, and general medical examination data for each participant from 2002 to 2019. Data on body mass index (BMI), smoking status, and alcohol consumption were obtained from the general health examinations in the KNHIS database.
Patients with de novo PD aged ≥40 years between January 2002 and December 2010 were enrolled based on the ICD-10 code G20 for PD and PD medication prescriptions. A total of 114,848 eligible candidates were identified. We excluded 1,132 patients with a previous history of dementia diagnosis, 3,379 with a diagnosis of dementia within the first year of follow-up to rule out dementia with Lewy bodies, 30,712 with a diagnosis of Parkinson’s syndrome (ICD-10 codes G21, G22, or G23), 68,589 without at least three fasting glucose levels in health examinations between January 2002 and one year after the date of PD diagnosis, and 1,769 with an interval > 1 year between the date of PD diagnosis and the index health examination, which is the nearest examination from the date of PD diagnosis. As a result, 9,264 patients were included in this study.
The health examination included blood pressure (BP) and BMI measurements, and blood sampling, including fasting glucose and total cholesterol levels at the nearest examination from the date of PD diagnosis (index health examination). Hypertension was defined according to the ICD-10 codes (I10-15) and a prescription of antihypertensive medication or a systolic/diastolic BP ≥ 140/90 mmHg. Diabetes was defined according to the corresponding ICD-10 codes (E8-14) and a prescription of glucose-lowering medication or fasting glucose ≥126 mg/dL. Hyperlipidemia was defined according to ICD-10 code (E78) and a prescription of lipid-lowering medication or total cholesterol level ≥ 240 mg/dL. Smoking status was categorized into three groups: those who had never smoked, ex-smokers, and current smokers. Heavy alcohol consumption was defined as alcohol consumption ≥ three times per week. Regular exercise was defined as performing physical activity ≥ three times per week.
Glucose variability was calculated form three or more fasting glucose levels measured at the patients’ health examination between January 2002 and one year after the PD diagnosis date. Three measures of variability were considered (Kang et al., 2022), variability independent of mean (VIM), coefficient of variation (CV), and average real variability (ARV). VIM was calculated by dividing the standard deviation (SD) by the mean raised to the power β (SD/meanβ), in which β was the regression coefficient based on the PROC NLIN procedure of the SAS package. CV was calculated as the SD divided by the mean. ARV was the average of the absolute differences between consecutive values and was calculated using the following formula, in which N was the number of glucose measurements:
The outcome of the study was the development of PDD (newly diagnosed dementia in patients with PD), which was defined according to the relevant ICD-10 codes (F00, F02, F03, F05, or G30) and prescriptions of dementia medication, including donepezil, rivastigmine, galantamine, and memantine. To exclude Lewy body dementia, we excluded patients diagnosed with dementia within one year after the diagnosis of PD. The competing risk was death, obtained from death records from the Korean National Statistical Office. Patients without PDD during follow-up were considered to have completed the study on the date of death or at the end of follow-up. All patients were followed up from the date of PD diagnosis (baseline) to the date of PDD diagnosis, date of death, or until December 2019.
Baseline characteristics are presented as the mean ± SD or median (interquartile range [IQR]) and frequency (%). The patients were divided into four groups based on the glucose CV quartiles. PDD incidence was examined according to glucose variability. The association between glucose variability and the development of PDD was investigated using a Fine and Gray competing regression model with glucose variability as a separate predictor and death as a competing risk, controlling for age, sex, the presence of hypertension, diabetes and hyperlipidemia, heavy alcohol consumption, smoking, and regular exercise (Model 1). To account for the possible effects of systolic and diastolic BP, fasting glucose, total cholesterol, and BMI at the index health examination, further analyses were performed after controlling for the covariates in Model 1 plus systolic BP, diastolic BP, fasting glucose, total cholesterol, and BMI at the index health examination (Model 2). Sensitivity analyses were used to exclude patients with diabetes to eliminate the effects of diabetes, including continuous hyperglycemia and hypoglycemic events. Furthermore, analyses using other measures of glucose variability, including VIM and ARV, were performed.
All reported p-values were two-sided and statistical significance was set at 0.05. All analyses were performed using SAS (version 9.4; SAS Institute, Inc.).
Patients with PD were classified into four groups based on the glucose CV. CV was normally distributed, and the CV quartiles were defined based on the cut-off points 0.072, 0.112, and 0.168. Table 1 shows the baseline demographics of the PD cohort, presented as the mean ± SD or n (%). Mean age, systolic BP, fasting glucose and total cholesterol, female ratio, frequency of hypertension, diabetes, dyslipidemia, smoking, heavy alcohol consumption, and regular exercise were different across all groups. Of note, patients in the higher quartiles were older and had higher systolic BP, fasting glucose levels, and prevalence of hypertension, diabetes, and hyperlipidemia. However, no significant difference was found in diastolic BP (p = 0.491) or BMI (p = 0.673). The median follow-up duration was 9.5 (5.7–10.9) years.
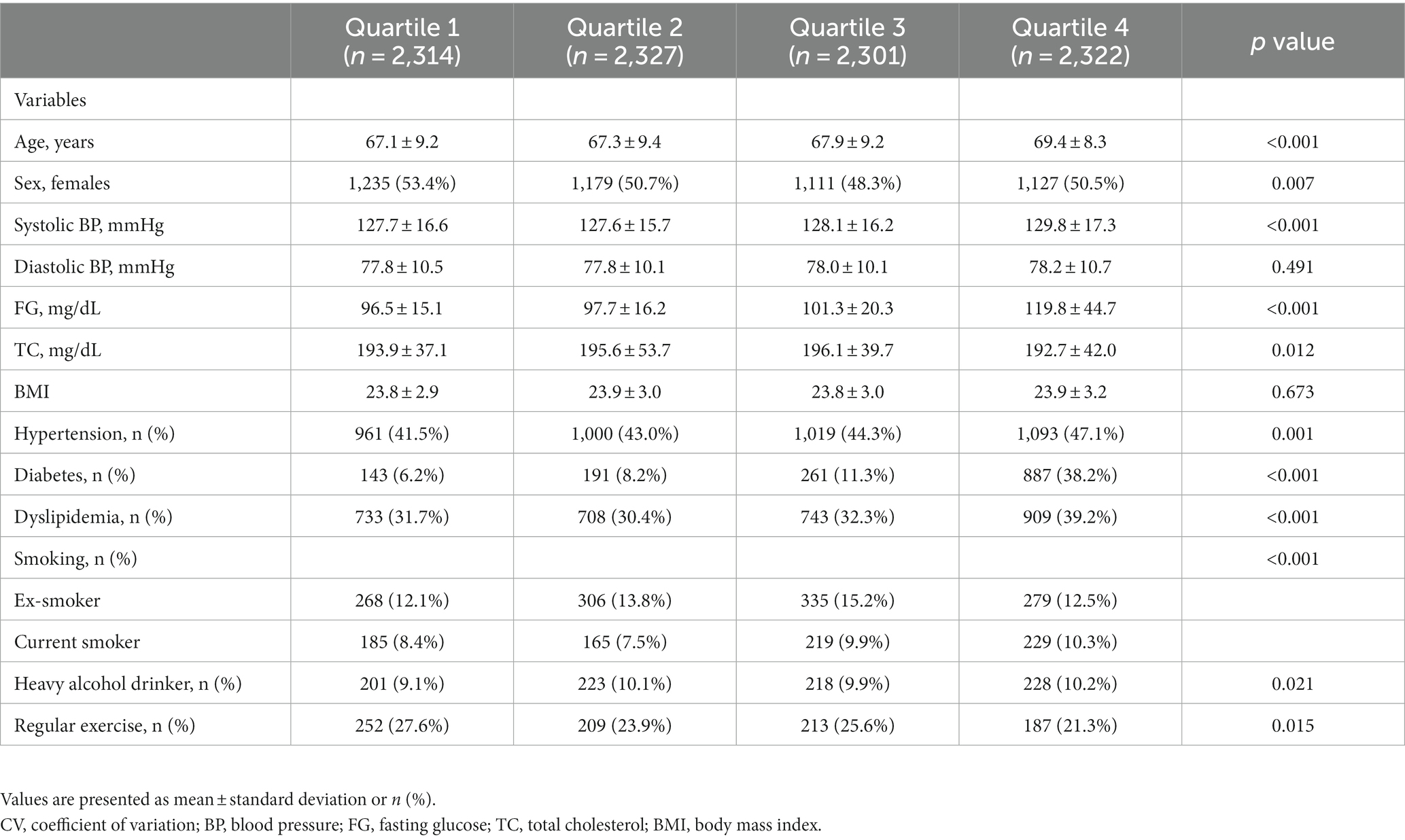
Table 1. Baseline characteristics of study participants according to CV quartile.
During the median 9.5-year follow-up period, 1,757 of 9,264 (19.0%) patients developed PDD. The incidence of PDD increased with increasing glucose variability, from 18.28 per 1,000 person-years in quartile 1 to 20.80 in quartile 2, 22.91 in quartile 3, and 29.14 in quartile 4 (Table 2). In Model 1, higher glucose variability was associated with a higher risk of PDD development after controlling for age, sex, presence of hypertension, diabetes, and hyperlipidemia, heavy alcohol consumption, smoking, and regular exercise. Patients with PD in quartiles 2 (subdistribution hazard ratio [SHR] = 1.30, 95% CI 1.03 to 1.63), 3 (SHR = 1.30, 95% Cl 1.03 to 1.63), and 4 (SHR = 1.50, 95% CI 1.20 to 1.87) had a higher risk of PDD than those in quartile 1 (Table 2). In Model 2, patients with PD in quartiles 2 (SHR = 1.30, 95% CI 1.04 to 1.63), 3 (SHR = 1.29, 95% CI 1.02 to 1.62), and 4 (SHR = 1.50, 95% CI 1.19 to 1.88) independently remained at a higher risk of PDD than those in quartile 1 after additionally controlling for systolic BP, fasting glucose, total cholesterol, and BMI at the index health examination (Table 2).
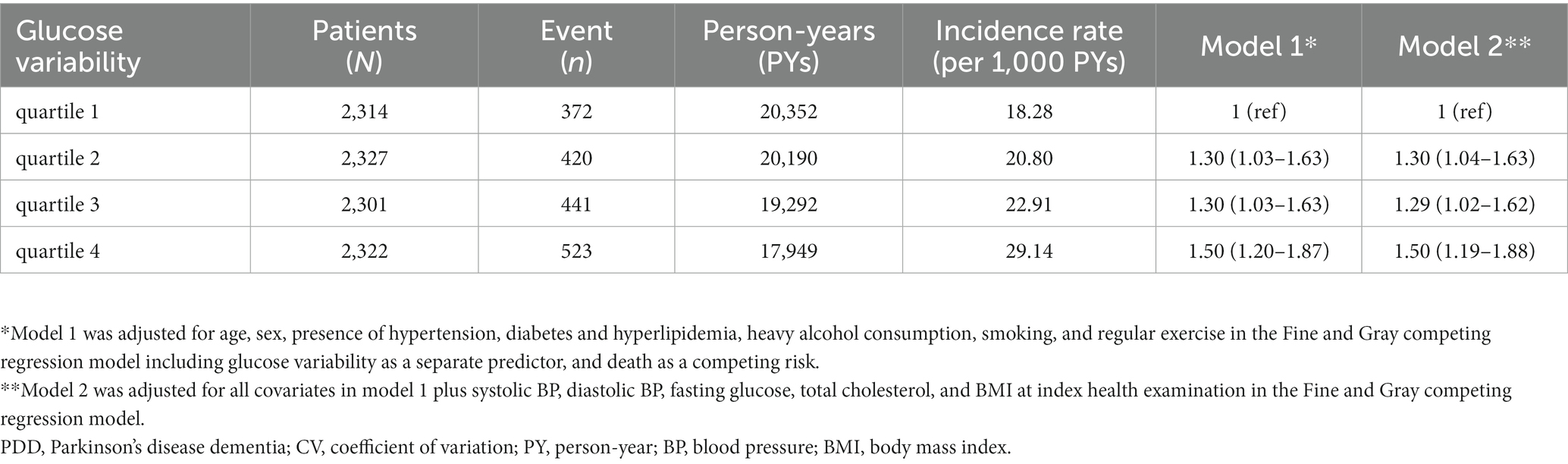
Table 2. Incidence of PDD according to quartiles of glucose variability (CV).
Among the PD patients without diabetes, those in quartile 4 (SHR = 1.47, 95% CI 1.19 to 1.82) were at a higher risk of developing PDD than those in quartile 1 after controlling for age, sex, presence of hypertension and hyperlipidemia, heavy alcohol consumption, smoking, and regular exercise in Model 1 (Table 3). In Model 2, patients in quartile 4 (SHR = 1.46, 95% CI 1.17 to 1.8) remained independently at a higher risk of PDD than those in quartile 1 after additionally controlling for systolic BP, fasting glucose, total cholesterol, and BMI at index health examination (Table 3).
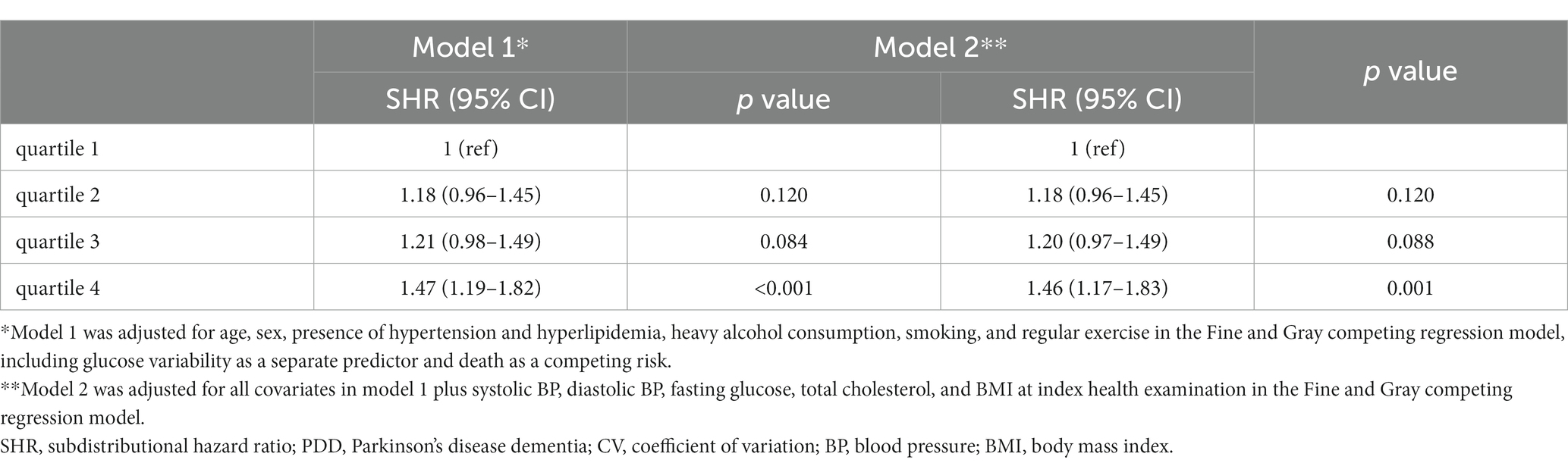
Table 3. SHR for PDD in the patients without diabetes according to glucose variability (CV).
In terms of other measures of variability (VIM and ARV), the results showed similar trends. Specifically, using VIM, patients with PD in quartile 4 (SHR = 1.49, 95% CI 1.18 to 1.87) had a higher risk of PDD than those in quartile 1 after controlling for age, sex, presence of hypertension, diabetes and hyperlipidemia, heavy alcohol consumption, smoking, regular exercise, and the index health examination measurements, including systolic BP, baseline fasting glucose, total cholesterol, and BMI (Table 4). For ARV, PD patients in quartiles 3 (SHR = 1.28, 95% CI 1.02 to 1.61) and 4 (SHR = 1.39, 95% CI 1.10 to 1.77) had a higher risk of PDD than those in quartile 1 after controlling for the potential confounders mentioned above (Table 4).
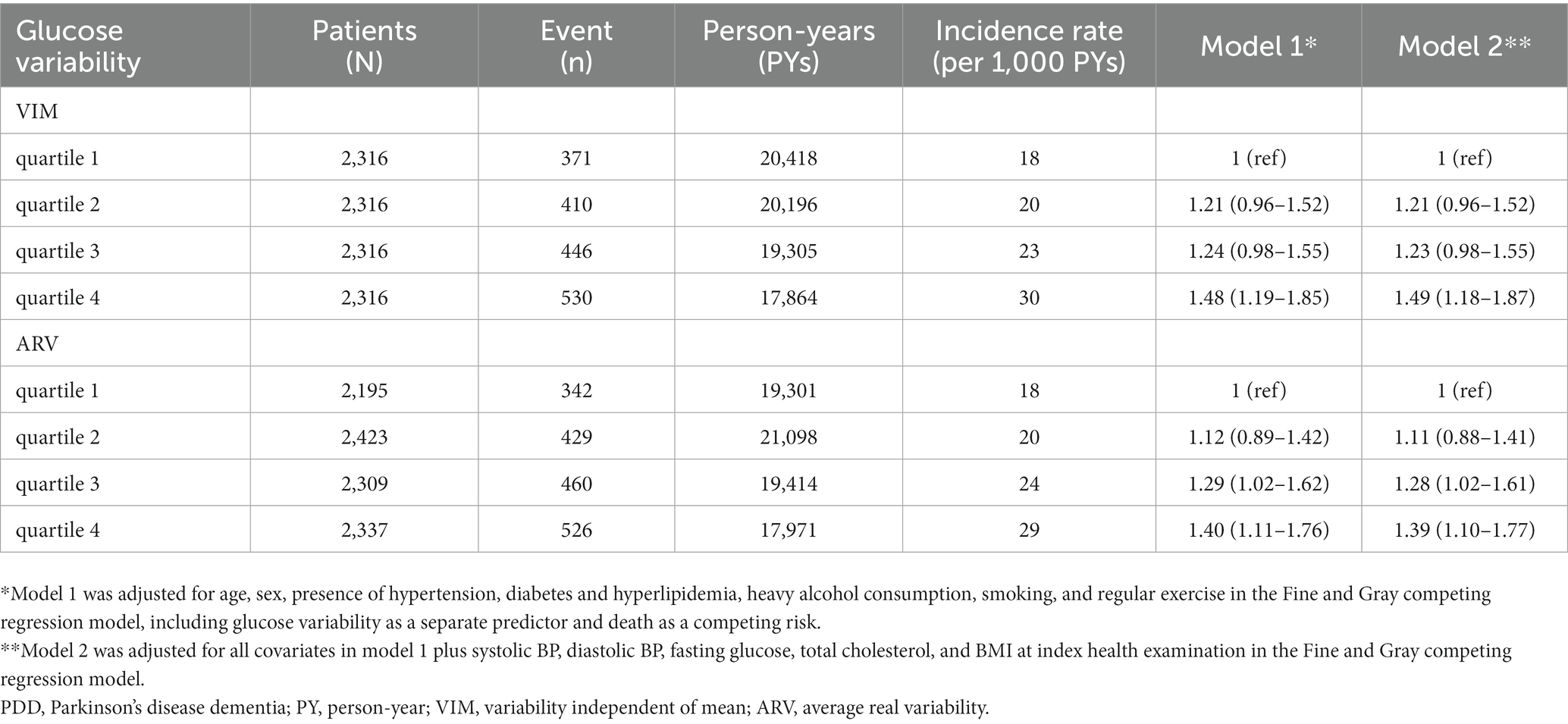
Table 4. Incidence rate of PDD according to quartiles of glucose variability (other measures).
This large-scale nationwide cohort study investigated the association between glucose variability and PDD incidence. Our results found that a higher visit-to-visit glucose variability was associated with a greater incidence of PDD in patients with PD, regardless of baseline fasting glucose levels. In particular, the effects of higher glucose variability remained valid in patients without diabetes. These findings present higher glucose variability as a modifiable risk factor for incident PDD. Therefore, prevention strategies that include controlling glucose levels are needed to protect against PDD development in patients with PD.
Recent studies on the identification of prognostic factors related to various complications in patients with diabetes have focused on glucose variability, as well as continuous hyperglycemia or hypoglycemic events, and found it to be associated with cognitive impairment (Takao et al., 2014), Alzheimer’s disease (Li et al., 2017; Zheng et al., 2021; Lee et al., 2022), and vascular dementia (Lee et al., 2022). Additionally, among individuals without diabetes, glucose variability has been reported to increase the risk of both cognitive impairment (Bancks et al., 2018) and Alzheimer’s disease (Lee et al., 2018). However, there is a paucity of information on the effects of glucose variability on poor clinical outcomes, including the development of dementia in patients with PD.
Our novel finding was that long-term glucose variability, a reflection of residual insulin secretion and the stability of medication effect and adherence, is a risk factor for PDD, regardless of other cardiovascular risk factors and baseline glucose levels. In particular, the increased risk of PDD remained in the highest quartile of glucose variability among patients without diabetes, indicating that glucose variability might affect the development of PDD independently of continuous hyperglycemia and hypoglycemic events. Furthermore, patients in the highest quartile of glucose variability consistently had a higher risk of PDD than those in the lowest quartile using all three variability indices (CV, ARV, and VIM). While further studies are needed to elucidate these findings, several mechanisms might explain the impact of glucose variability on the development of dementia in patients with PD. Previous studies have shown that, compared with consistent hyperglycemia, glucose variability exerts more deleterious effects on inflammatory reactions, oxidative stress, and endothelial dysfunction, which are closely related to neurodegeneration (Quagliaro et al., 2005; Ceriello et al., 2008). Glucose variability has also been found to cause insulin resistance and cerebral small vessel damage, thus hindering the clearance of pathogenic proteins in the brain (Keating and El-Osta, 2013; Takao et al., 2014). Shared mitochondrial dysfunction may offer an alternative explanation. Striatal neurons and pancreatic β-cells have low mitochondrial capacity and are vulnerable to dysfunctions in mitochondrial respiratory chain enzyme (Schernhammer et al., 2011). Furthermore, growing evidence has shown that insulin signaling pathway disruptions may play a major role in the pathogenesis of PD, including inflammation, oxidative stress, and increased α-synuclein deposition in the brain, which are associated with poor prognosis (Kim et al., 2011; Athauda and Foltynie, 2016). In fact, insulin receptor mRNA expression in the striatum was lower in the brain tissues of patients with PD than in those without PD.
The strengths of this study lie in the large number of patients with PD and the long follow-up duration in a nationwide cohort. However, this study also had several limitations that must be addressed. First, discrepancies in the diagnosis of PD and PDD between clinical practice and the KNHIS claim data may have produced inaccurate results. PDD was defined according to ICD-10 codes (F00, F02, F03, F05 or G30) in PD patients, although F00 and G30 refers to dementia of the Alzheimer type. As the KNHIS covers the dementia medication (donepezil, rivastigmine, galantamine, and/or memantine) for only patients with dementia of the Alzheimer type, most Korean doctors put F00 or G30 codes for patients with PDD to prescribe the dementia medication covered under health insurance. However, this issue might be mitigated by the inclusion of the diagnostic code of PD in the registration code in the program for rare intractable diseases to increase diagnostic accuracy. Second, due to the limitation of claims data, we were unable to assess the potential confounders including glycosylated hemoglobin, exact cognitive performance at baseline, neuroimaging finding, concomitant cerebrovascular disease, education years, PD motor subtype, and compliance with PD medication of each patient. This was partially overcome by the exclusion of subjects with a prior diagnosis of dementia and diagnosis of dementia within the first year of follow-up. Third, although fasting glucose level may be affected by the meal consumed the night before blood sampling, we could not evaluation this information. Finally, we did not account for the effects of glucose-lowering medications and compliance with glucose-lowering medications. However, we defined diabetes according to the diagnostic code and prescriptions of glucose-lowering medication and adjusted our analyses for the presence of diabetes, which may have mitigated this issue to a certain extent. Despite these limitations, our study successfully identified the effect of long-term glucose variability on cognitive decline in patients with PD. Our findings suggest that preventive measures for constant glucose control may be necessary to prevent PDD.
Publicly available datasets were analyzed in this study. This data can be found at NCBI, accession numbers: ERP110230 and PRJNA517480.
This study was approved by the Institutional Review Board of the Korea University Guro Hospital and adhered to the principles of the Declaration of Helsinki. The studies were conducted in accordance with the local legislation and institutional requirements. The ethics committee/institutional review board waived the requirement of written informed consent for participation from the participants or the participants' legal guardians/next of kin because Anonymous and de-identified information was used for analysis; therefore, informed consent was not obtained.
SK: Conceptualization, Data curation, Investigation, Methodology, Writing – original draft, Writing – review & editing, Funding acquisition, Validation. YC: Data curation, Formal analysis, Writing – review & editing. SC: Data curation, Writing – review & editing. S-JM: Formal analysis, Writing – review & editing. CK: Data curation, Writing – review & editing. JK: Data curation, Writing – review & editing. KO: Data curation, Writing – review & editing. JY: Data curation, Writing – review & editing. SS: Data curation, Writing – review & editing. GC: Data curation, Writing – review & editing. S-BK: Data curation, Methodology, Project administration, Supervision, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This study was supported by the “Korea National Institute of Health” research project (2022-ER1005-01) and Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education (grant number: 2022R1I1A1A01056956).
This study was performed using the database from the National Health Insurance System, and the results do not necessarily represent the opinions of the National Health Insurance Corporation.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Athauda, D., and Foltynie, T. (2016). Insulin resistance and Parkinson's disease: a new target for disease modification? Prog. Neurobiol. 145-146, 98–120. doi: 10.1016/j.pneurobio.2016.10.001
Bancks, M. P., Carnethon, M. R., Jacobs, D. R., Launer, L. J., Reis, J. P., Schreiner, P. J., et al. (2018). Fasting glucose variability in young adulthood and cognitive function in middle age: the coronary artery risk development in young adults (CARDIA) study. Diabetes Care 41, 2579–2585. doi: 10.2337/dc18-1287
Bohnen, N. I., Kotagal, V., Müller, M. L., Koeppe, R. A., Scott, P. J., Albin, R. L., et al. (2014). Diabetes mellitus is independently associated with more severe cognitive impairment in Parkinson disease. Parkinsonism Relat. Disord. 20, 1394–1398. doi: 10.1016/j.parkreldis.2014.10.008
Ceriello, A., Esposito, K., Piconi, L., Ihnat, M. A., Thorpe, J. E., Testa, R., et al. (2008). Oscillating glucose is more deleterious to endothelial function and oxidative stress than mean glucose in normal and type 2 diabetic patients. Diabetes 57, 1349–1354. doi: 10.2337/db08-0063
Cheong, J. L. Y., de Pablo-Fernandez, E., Foltynie, T., and Noyce, A. J. (2020). The association between type 2 diabetes mellitus and Parkinson's disease. J. Parkinsons Dis. 10, 775–789. doi: 10.3233/jpd-191900
Chornenkyy, Y., Wang, W. X., Wei, A., and Nelson, P. T. (2019). Alzheimer's disease and type 2 diabetes mellitus are distinct diseases with potential overlapping metabolic dysfunction upstream of observed cognitive decline. Brain pathol 29, 3–17. doi: 10.1111/bpa.12655
Chung, H. S., Lee, J. S., Kim, J. A., Roh, E., Lee, Y. B., Hong, S. H., et al. (2021). Fasting plasma glucose variability in midlife and risk of Parkinson's disease: a nationwide population-based study. Diabetes Metab. 47:101195. doi: 10.1016/j.diabet.2020.08.006
Curb, J. D., Rodriguez, B. L., Abbott, R. D., Petrovitch, H., Ross, G. W., Masaki, K. H., et al. (1999). Longitudinal association of vascular and Alzheimer's dementias, diabetes, and glucose tolerance. Neurology 52, 971–975. doi: 10.1212/wnl.52.5.971
Giuntini, M., Baldacci, F., Del Prete, E., Bonuccelli, U., and Ceravolo, R. (2014). Diabetes is associated with postural and cognitive domains in Parkinson's disease. Results from a single-center study. Parkinsonism Relat. Disord. 20, 671–672. doi: 10.1016/j.parkreldis.2014.02.016
Gorst, C., Kwok, C. S., Aslam, S., Buchan, I., Kontopantelis, E., Myint, P. K., et al. (2015). Long-term glycemic variability and risk of adverse outcomes: a systematic review and Meta-analysis. Diabetes Care 38, 2354–2369. doi: 10.2337/dc15-1188
Guo, Y., Xu, W., Liu, F. T., Li, J. Q., Cao, X. P., Tan, L., et al. (2019). Modifiable risk factors for cognitive impairment in Parkinson's disease: a systematic review and meta-analysis of prospective cohort studies. Mov Disord 34, 876–883. doi: 10.1002/mds.27665
Kang, S. H., Choi, Y., Chung, S. J., Kim, C. K., Kim, J. H., Oh, K., et al. (2023). Independent effect of cardiometabolic syndromes and depression on dementia in Parkinson's disease: a 12-year longitudinal follow-up study of a nationwide cohort. Eur. J. Neurol. 30, 911–919. doi: 10.1111/ene.15689
Kang, S. H., Kim, J. H., Chang, Y., Cheon, B. K., Choe, Y. S., Jang, H., et al. (2022). Independent effect of body mass index variation on amyloid-β positivity. Front. Aging Neurosci. 14:924550. doi: 10.3389/fnagi.2022.924550
Keating, S. T., and El-Osta, A. (2013). Glycemic memories and the epigenetic component of diabetic nephropathy. Curr. Diab. Rep. 13, 574–581. doi: 10.1007/s11892-013-0383-y
Kim, S. R., Ries, V., Cheng, H. C., Kareva, T., Oo, T. F., Yu, W. H., et al. (2011). Age and α-synuclein expression interact to reveal a dependence of dopaminergic axons on endogenous Akt/PKB signaling. Neurobiol. Dis. 44, 215–222. doi: 10.1016/j.nbd.2011.07.003
Ko, J., Ha, J., Lee, J. J., Jin, S., Lee, J., Baek, M. S., et al. (2022). Reliability and validity of the subjective cognitive complaints questionnaire for Parkinson's disease (SCCQ-PD). J Clin Neuro 18, 171–178. doi: 10.3988/jcn.2022.18.2.171
Lee, S. H., Han, K., Cho, H., Park, Y. M., Kwon, H. S., Kang, G., et al. (2018). Variability in metabolic parameters and risk of dementia: a nationwide population-based study. Alzheimers Res. Ther. 10:110. doi: 10.1186/s13195-018-0442-3
Lee, D. Y., Kim, J., Park, S., Park, S. Y., Yu, J. H., Seo, J. A., et al. (2022). Fasting glucose variability and the risk of dementia in individuals with diabetes: a Nationwide cohort study. Diabetes Metab. J. 46, 923–935. doi: 10.4093/dmj.2021.0346
Li, T. C., Yang, C. P., Tseng, S. T., Li, C. I., Liu, C. S., Lin, W. Y., et al. (2017). Visit-to-visit variations in fasting plasma glucose and HbA(1c) associated with an increased risk of Alzheimer disease: Taiwan diabetes study. Diabetes Care 40, 1210–1217. doi: 10.2337/dc16-2238
Monnier, L., Mas, E., Ginet, C., Michel, F., Villon, L., Cristol, J. P., et al. (2006). Activation of oxidative stress by acute glucose fluctuations compared with sustained chronic hyperglycemia in patients with type 2 diabetes. JAMA 295, 1681–1687. doi: 10.1001/jama.295.14.1681
Ong, M., Foo, H., Chander, R. J., Wen, M. C., Au, W. L., Sitoh, Y. Y., et al. (2017). Influence of diabetes mellitus on longitudinal atrophy and cognition in Parkinson's disease. J. Neurol. Sci. 377, 122–126. doi: 10.1016/j.jns.2017.04.010
Pillon, B., Deweer, B., Agid, Y., and Dubois, B. (1993). Explicit memory in Alzheimer's, Huntington's, and Parkinson's diseases. Arch. Neurol. 50, 374–379. doi: 10.1001/archneur.1993.00540040036010
Quagliaro, L., Piconi, L., Assaloni, R., Da Ros, R., Maier, A., Zuodar, G., et al. (2005). Intermittent high glucose enhances ICAM-1, VCAM-1 and E-selectin expression in human umbilical vein endothelial cells in culture: the distinct role of protein kinase C and mitochondrial superoxide production. Atherosclerosis 183, 259–267. doi: 10.1016/j.atherosclerosis.2005.03.015
Schernhammer, E., Hansen, J., Rugbjerg, K., Wermuth, L., and Ritz, B. (2011). Diabetes and the risk of developing Parkinson's disease in Denmark. Diabetes Care 34, 1102–1108. doi: 10.2337/dc10-1333
Takao, T., Matsuyama, Y., Yanagisawa, H., Kikuchi, M., and Kawazu, S. (2014). Association between HbA1c variability and mortality in patients with type 2 diabetes. J. Diabetes Complicat. 28, 494–499. doi: 10.1016/j.jdiacomp.2014.02.006
Wang, A., Liu, X., Xu, J., Han, X., Su, Z., Chen, S., et al. (2017). Visit-to-visit variability of fasting plasma glucose and the risk of cardiovascular disease and all-cause mortality in the general population. J. Am. Heart Assoc. 6:e006757. doi: 10.1161/jaha.117.006757
Keywords: Parkinson’ s disease, Parkinson’s disease dementia, glucose variability, fasting glucose, risk factors
Citation: Kang SH, Choi Y, Chung SJ, Moon S-J, Kim CK, Kim JH, Oh K, Yoon JS, Seo SW, Cho GJ and Koh S-B (2024) Fasting glucose variability and risk of dementia in Parkinson’s disease: a 9-year longitudinal follow-up study of a nationwide cohort. Front. Aging Neurosci. 15:1292524. doi: 10.3389/fnagi.2023.1292524
Edited by:
Omar M. El-Agnaf, Hamad bin Khalifa University, QatarReviewed by:
Sharad Purohit, Augusta University, United StatesCopyright © 2024 Kang, Choi, Chung, Moon, Kim, Kim, Oh, Yoon, Seo, Cho and Koh. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Seong-Beom Koh, cGFya2luc29uQGtvcmVhLmFjLmty
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.