
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Aging Neurosci., 20 June 2022
Sec. Alzheimer's Disease and Related Dementias
Volume 14 - 2022 | https://doi.org/10.3389/fnagi.2022.899158
This article is part of the Research TopicPreclinical Biomarkers and Functional Compensation in Brain Aging, Volume IIView all 5 articles
 Inès Moulinet1†
Inès Moulinet1† Edelweiss Touron1†Florence Mézenge1
Edelweiss Touron1†Florence Mézenge1 Sophie Dautricourt1,2
Sophie Dautricourt1,2 Vincent De La Sayette2
Vincent De La Sayette2 Denis Vivien1,3Natalie L. Marchant4Géraldine Poisnel1
Denis Vivien1,3Natalie L. Marchant4Géraldine Poisnel1 Gaël Chételat1*
Gaël Chételat1*Background: Depressive and anxiety symptoms are frequent in Alzheimer’s disease and associated with increased risk of developing Alzheimer’s disease in older adults. We sought to examine their relationships to Alzheimer’s disease biomarkers across the preclinical and clinical stages of the disease.
Method: Fifty-six healthy controls, 35 patients with subjective cognitive decline and 56 amyloid-positive cognitively impaired patients on the Alzheimer’s continuum completed depression and anxiety questionnaires, neuropsychological tests and neuroimaging assessments. We performed multiple regressions in each group separately to assess within group associations of depressive and anxiety symptoms with either cognition (global cognition and episodic memory) or neuroimaging data (gray matter volume, glucose metabolism and amyloid load).
Results: Depressive symptoms, but not anxiety, were higher in patients with subjective cognitive decline and cognitively impaired patients on the Alzheimer’s continuum compared to healthy controls. Greater depressive symptoms were associated with higher amyloid load in subjective cognitive decline patients, while they were related to higher cognition and glucose metabolism, and to better awareness of cognitive difficulties, in cognitively impaired patients on the Alzheimer’s continuum. In contrast, anxiety symptoms were not associated with brain integrity in any group.
Conclusion: These data show that more depressive symptoms are associated with greater Alzheimer’s disease biomarkers in subjective cognitive decline patients, while they reflect better cognitive deficit awareness in cognitively impaired patients on the Alzheimer’s continuum. Our findings highlight the relevance of assessing and treating depressive symptoms in the preclinical stages of Alzheimer’s disease.
Neuropsychiatric symptoms (NPS) are present in 90% of patients with Alzheimer’s disease (AD) dementia (Finkel et al., 1996), with depressive and anxiety symptoms being two of the most common NPS (Banning et al., 2019). They are associated with decrease in quality of life, caregiver’s burden, and increased institutionalization (Gilley et al., 2004; Hoe et al., 2006, 2007). In cognitively unimpaired individuals, it has been shown that depressive and anxiety symptoms, even at a subclinical level, increase the risk of cognitive decline (Geda et al., 2014; Zhang et al., 2020) and of developing AD (Harrington et al., 2015; Petkus et al., 2016). With regards to the cognitive and brain substrates of depressive and anxiety symptoms, studies are sparse and findings are mixed. In patients with AD dementia, one previous study found that patients with persistent neuropsychiatric symptoms had worse cognitive outcomes (Poulin et al., 2017). Regarding neuroimaging biomarkers, some studies found that depressive and anxiety symptoms were associated with more AD neuroimaging hallmarks in either Mild Cognitive Impairment (MCI) or AD patients (Chen et al., 2021; Mendez, 2021), such as lower gray matter volume (GM) (Son et al., 2013; Dhikav et al., 2014; Fujishima et al., 2014; Lebedeva et al., 2014; Tagai et al., 2014; Hayata et al., 2015; Wu et al., 2020), lower glucose metabolism and/or perfusion (Hashimoto et al., 2006; Levy-Cooperman et al., 2008), and higher amyloid deposition (Brendel et al., 2015; Bensamoun et al., 2016; Krell-Roesch et al., 2019). However, conflicting results have been reported in other studies showing a link between depressive symptoms and higher gray matter volume (Auning et al., 2015; Enache et al., 2015), glucose metabolism and/or perfusion (Tagai et al., 2014; Auning et al., 2015; Brendel et al., 2015; Tommaso et al., 2016) or no association between psychoaffective factors and neuroimaging markers (Horínek et al., 2006; Starkstein et al., 2009; Serra et al., 2010; Poulin et al., 2011; Mori et al., 2014; Chung et al., 2015; Bensamoun et al., 2016; Huey et al., 2017; Banning et al., 2019). Moreover, studies that assessed these relationships in patients with subjective cognitive decline (SCD), i.e., cognitively unimpaired individuals, who are concerned that they have reduced cognitive function (Jessen et al., 2020), are sparse and reported mixed findings. Thus, higher depressive symptoms were associated with both lower (Enache et al., 2015) or higher (Auning et al., 2015) hippocampal gray matter volume in SCD patients.
Given the impact of depressive and anxiety symptoms on quality of life and even prognosis, improving our knowledge on their cognitive and brain substrates across the clinical continuum from normal cognition to Alzheimer’s dementia is particularly relevant for clinical management and AD risk reduction. To date, the existing literature on this research field showed inconsistencies between studies especially regarding the direction of the neuroimaging findings. Furthermore, to our knowledge, no study included cognitive measures and complementary multimodal neuroimaging data throughout the Alzheimer’s clinical continuum at the same time. Therefore, this study aims at providing a comprehensive assessment of the links between depressive and anxiety symptoms, and cognition as well as multiple measures of brain integrity, throughout the clinical continuum from normal cognition to Alzheimer’s dementia, to further our understanding of the relevance and mechanisms of psychoaffective factors in preclinical and clinical AD. We hypothesized that depressive and anxiety symptoms would be associated with AD-related cognitive and brain alterations in both preclinical and later stages.
All participants were recruited as part of the Imagerie Multimodale de la Maladie d’Alzheimer à un Stade Précoce (IMAP +) Study in Caen, France. Ninety-one patients and 56 controls above 50 years old were included, all living at home, and with no history or clinical evidence of neurologic or psychiatric disorder, alcohol use disorder or drug abuse. Notably, none of the participants met diagnostic criteria for major depression or anxiety disorder, as defined in the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition. The inclusion and group classification of the participants were based on a clinical interview and a standardized neuropsychological assessment (including tests of episodic memory, working memory, language skills, executive functions, and visuospatial abilities), according to internationally agreed criteria [see details in (La Joie et al., 2012, 2016; Perrotin et al., 2017)]. Patients were either patients with SCD (n = 35) or patients on the Alzheimer’s continuum (ADC patients; n = 56) and were all recruited from local memory clinics. SCD patients reported memory complaints and showed normal performance in all tests of the standardized neuropsychological assessment. During the interview, the clinician ensured that the complaint was not related to current medication or medical condition, and did not fulfill NINCDS-ADRDA criteria for probable AD (McKhann et al., 1984).
ADC patients were all selected to be positive for amyloid (see Section “Neuroimaging data and processing” for details). They included patients with MCI selected based on Petersen’s criteria (n = 28) (Petersen and Morris, 2005) and patients with dementia fulfilling NINCDS-ADRDA clinical criteria for probable AD (n = 28) (McKhann et al., 1984). Clinical diagnosis was assigned by consensus under the supervision of a senior neurologist and neuropsychologists. The SCD group consisted of both amyloid positive and amyloid negative participants (amyloid negative n = 23; amyloid positive n = 4; florbetapir-Positron Emission Tomography (PET) images not available n = 8). Finally, the 56 healthy elderly control subjects were recruited from the community, performed in the normal range on all tests from the standardized neuropsychological assessment, and were all selected to be amyloid negative (see below).
IMAP + was approved by the regional ethics committee (Comité de Protection des Personnes Nord-Ouest III) and is registered with ClinicalTrials.gov (number NCT01638949). All participants gave written informed consent before the examinations.
The Montgomery-Åsberg Depression Rating Scale (MADRS) (Montgomery and Asberg, 1979), a clinician-administered 10-item questionnaire with scores ranging from 0 to 60, was used to assess depressive symptoms at the time of the evaluation. The Spielberger State-Trait Anxiety Inventory form Y-A (STAI-A) (Spielberger et al., 1970), a 20-item self-rated questionnaire with scores ranging from 20 to 80, assessed state anxiety symptoms at the time of the evaluation. For both scales, higher scores indicated higher levels of symptoms of depression and anxiety. All participants were screened so as not to meet diagnostic criteria for major depression or anxiety disorders (see exclusion criteria above), but our goal was to assess depressive and anxiety symptoms on a continuum below this threshold for disorder (Altman and Royston, 2006; Laborde-Lahoz et al., 2015). Therefore, these scores were used as continuous variables in all analyses (see Section “Statistical analysis”) instead of classifying patients as presenting or not depressive/anxiety symptoms or disorders.
Global cognition was measured using the Mini Mental State Examination (Folstein et al., 1975) (MMSE, scores from 0 to 30). Verbal episodic memory was assessed using the Encoding, Storage and Recuperation (ESR) word list free recall sub-score (Eustache et al., 2015), consisting on the recall of two distinct 16-word lists after either a superficial or a deep encoding phase. The final score resulted from the sum of the superficial and deep encoding sub-scores (scores from 0 to 32).
All participants underwent neuroimaging scans on the same Magnetic Resonance Imaging (MRI) and PET scanners at the Cyceron Centre (Caen, France), as previously described in detail (La Joie et al., 2012; Besson et al., 2015), within 3-month interval from the psychoaffective and cognitive assessments. We measured GM volume with MRI, brain glucose metabolism with 18F-fluorodeoxyglucose (FDG)-PET and amyloid deposition with florbetapir-PET. The detailed acquisition procedure is available in the Supplementary Material 1. Global GM volumes from the MRI and neocortical standardized uptake value ratio (SUVr) from the PET scans were extracted as described below and used in the following analyses as continuous variables.
All neuroimaging pre-processing steps were performed with the Statistical Parametric Mapping version 12 (SPM12) software (Wellcome Trust Centre for Neuroimaging, London, United Kingdom). Briefly, T1-weighted MRI images were segmented and spatially normalized to the Montreal Neurological Institute (MNI) space and non-linear warping effects on volumes were corrected by modulating the resulting normalized GM segments (Chételat et al., 2008; Villain et al., 2008; La Joie et al., 2012).
PET images were corrected for partial volume effects using the Müller-Gärtner method (Müller-Gärtner et al., 2016). Resulting images were coregistered onto their corresponding MRI, normalized with the deformation parameters used for the MRI procedure, and then quantitatively normalized using the cerebellar GM as the reference region (Chételat et al., 2008; Villain et al., 2008; La Joie et al., 2012; Bejanin et al., 2019).
For each participant, a total GM volume and global FDG-PET value was calculated by applying a binary mask of GM (including voxels with a GM probability > 30% excluding the cerebellum) on the corresponding preprocessed images. The global neocortical SUVr was obtained from the florbetapir-PET images using a neocortex mask (including all regions but the cerebellum, hippocampus, amygdala and subcortical gray nuclei), as described in detail elsewhere (La Joie et al., 2012). This global neocortical SUVr was used as a continuous variable for further analyses (see below) and also to classify subjects as positive or negative for amyloid. This classification was used to select amyloid-negative HC and amyloid-positive MCI/AD patients. The threshold was calculated from a group of 45 young participants from the IMAP project (between 20 and 40 years old) using the mean + 2SD, corresponding to a SUVr of 1.02 under which participants were considered amyloid negative and above which patients were considered amyloid-positive (Besson et al., 2015; Perrotin et al., 2017).
To assess the differences in psychoaffective factors across clinical groups, we conducted analyses of covariance (ANCOVA) with education, age and sex as covariates and then performed post hoc tests to assess group-differences when a main effect of the clinical group was found. We also performed multiple regressions to assess within group associations between psychoaffective measures (i.e., depressive and anxiety symptoms) on the one hand, and cognition (global cognition and episodic memory) and neuroimaging data (GM volume, glucose metabolism and amyloid load) on the other hand. Results are presented with correction for level of education, age and sex. When a significant association was found with either depressive or anxiety symptoms, then the same analysis was repeated adding the other psychoaffective score (anxiety or depressive symptoms, respectively) as an additional covariate to further test whether the association was specific to the one and independent from the other. Indeed, these two symptoms are known to be related and found to be correlated in the present study in the ADC patient group (Spearman’s correlation p = 0.01, r = 0.356). Pairwise deletion was used in case of missing data and all statistical analyses were performed using the STATISTICA software (v13.0, StatSoft Inc., Tulsa, OK, United States).
Scores of depressive and anxiety symptoms were not normally distributed; thus, correlation analyses were repeated with non-parametric Spearman’s correlation tests. The score for depressive symptoms also showed an important floor effect with a large number of participants having a score of zero. To check that the results were consistent and not driven by the floor effect, we repeated all analyses regarding depressive symptoms excluding these participants, i.e., within subgroups of participants with at least one depressive symptom (n = 21 HC, n = 23 SCD, n = 42 ADC patients).
Group characteristics are listed in Table 1.
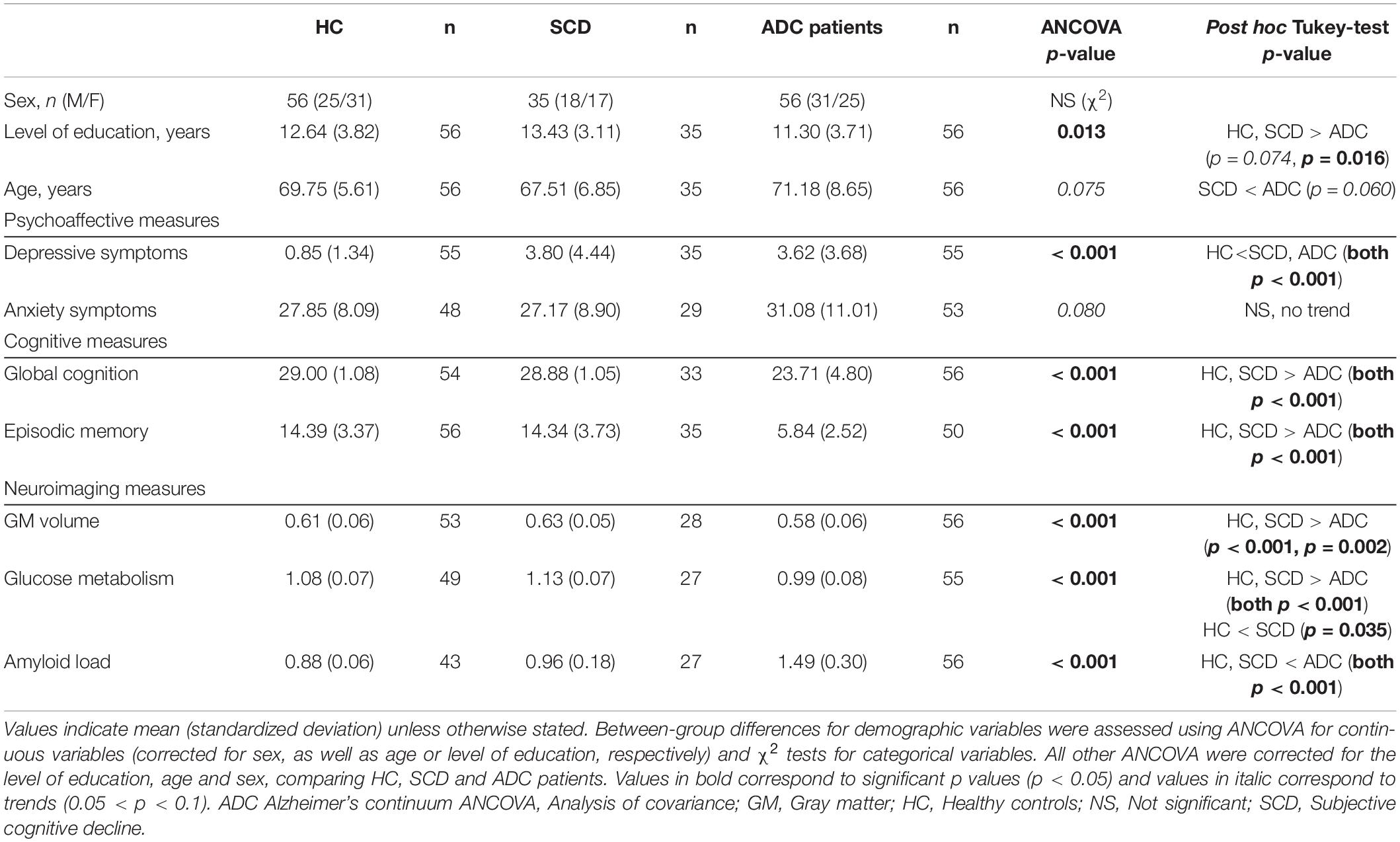
Table 1. Study sample characteristics.
With regard to psychoaffective factors, depressive symptoms significantly differed across groups (Table 1 and Figure 1A) even after accounting for anxiety symptoms (p < 0.001). Post hoc analyses showed that patients, either SCD or ADC patients, had more depressive symptoms than HC, but did not differ from each other (HC-SCD p < 0.001; HC-ADC patients p < 0.001; SCD-ADC patients p = 0.9). Regarding anxiety symptoms, we found a trend of group difference (Table 1 and Figure 1B) that did not remain when also correcting for depressive symptoms (p = 0.1). However, post hoc analyses revealed no significant between-group differences (HC-SCD p = 0.922; HC-ADC patients p = 0.144; SCD-ADC patients p = 0.129).
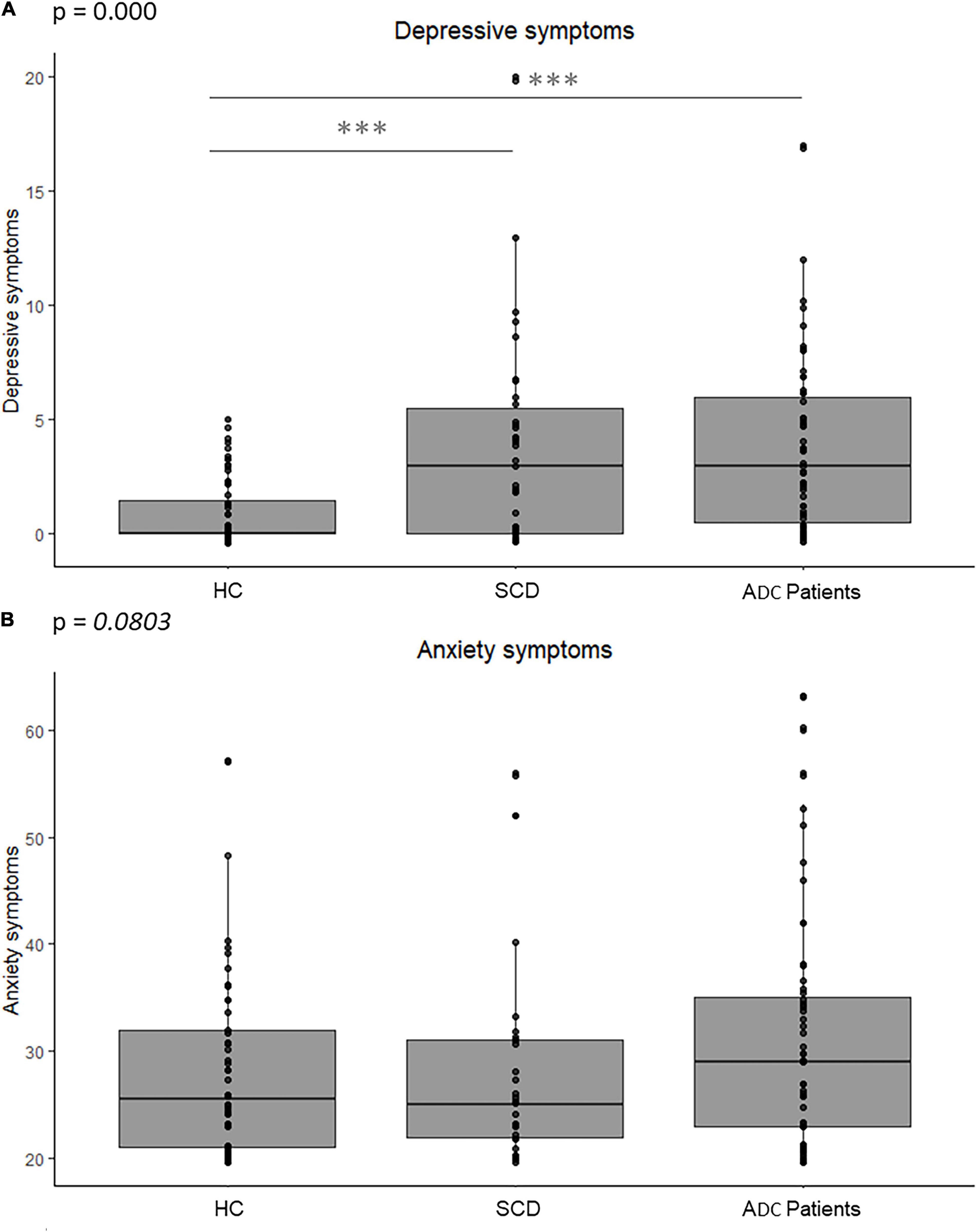
Figure 1. Difference in psychoaffective factors between groups of healthy controls, SCD and ADC patients. Graphs indicate boxplots of depressive and anxiety symptoms in each group. The p value of the main effect of group, measured with ANCOVAs corrected for the level of education, age and sex, is indicated on the graph. Significant post hoc results between each group are indicated with stars, ***corresponding to p values (p < 0.001). (A) ANCOVA on depressive symptoms. (B) ANCOVA on anxiety symptoms. ADC, Alzheimer’s continuum; ANCOVA, Analysis of covariance; HC, Healthy controls; p, p value; SCD, Subjective cognitive decline.
The results of the analyses assessing the links between depressive or anxiety symptoms on the one hand, and cognitive or neuroimaging measures on the other hand, are reported in Table 2. Higher depressive symptoms were associated with higher amyloid load in the SCD group (Figure 2A1). In contrast, in the group of ADC patients, higher depressive symptoms were associated with better episodic memory performance and higher glucose metabolism (Figure 2A2) and tended to be related to a better global cognition. We found the same results when also correcting for anxiety symptoms, but the association with global cognition was no longer a trend (p = 0.1; see Supplementary Table 1). Non-parametric analyses showed a similar pattern of results, though less strong (see Supplementary Table 2). We also found the same results as in our main analyses in the subgroup with at least one depressive symptom, except for the association between depressive symptoms and episodic memory performance in the ADC patient group, which was no longer significant (see Supplementary Table 3). Finally, to test whether the link between depressive symptoms and amyloid load was specific to the SCD stage, or reflected the greater variability of the amyloid measure in the SCD group as it included both amyloid-positive and amyloid-negative patients, we repeated this analysis in a group of MCI + AD that included both amyloid-positive and amyloid-negative patients (see Supplementary Table 4 for further details). We found no correlation (p = 0.9, r = 0.01) between depressive symptoms and amyloid load in this group.
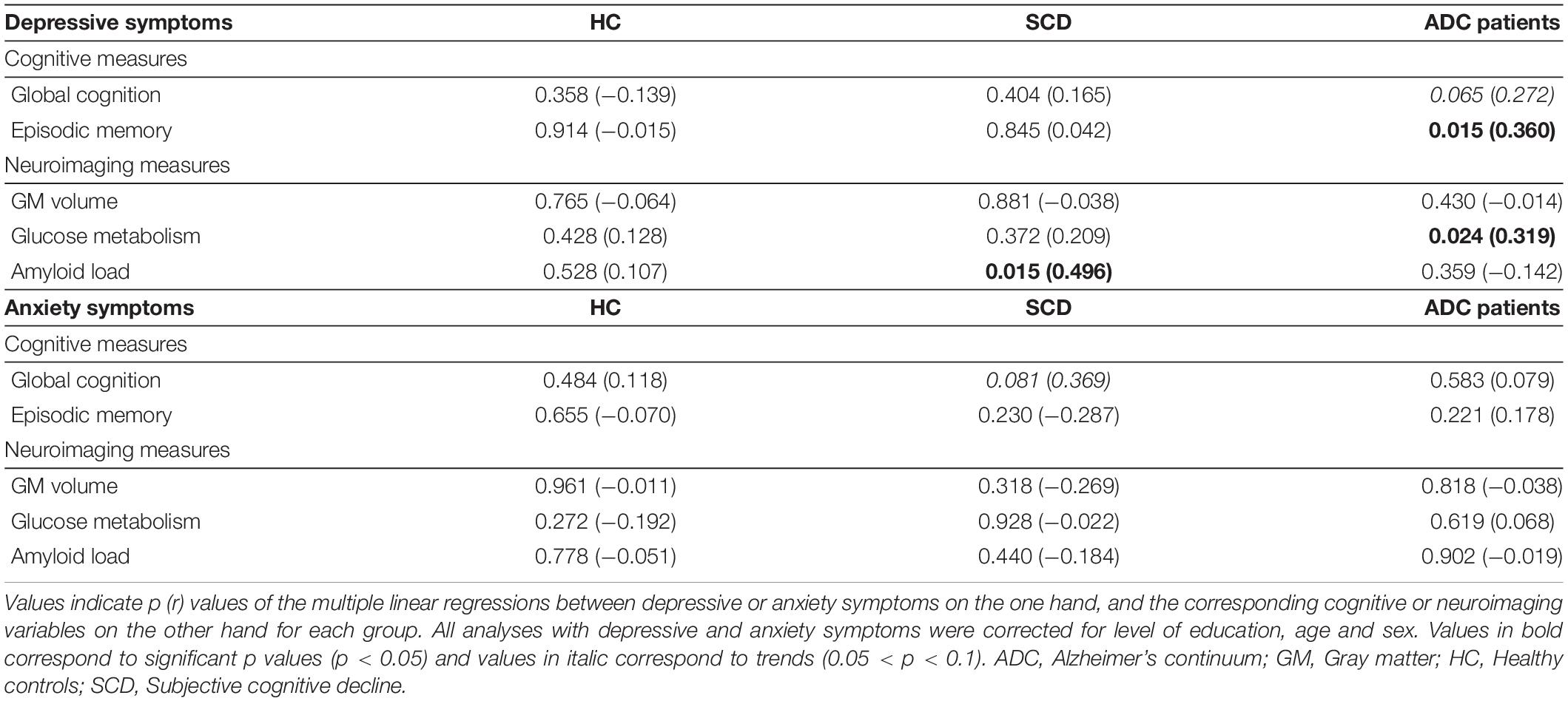
Table 2. Relationships of psychoaffective factors to cognition and neuroimaging measures.
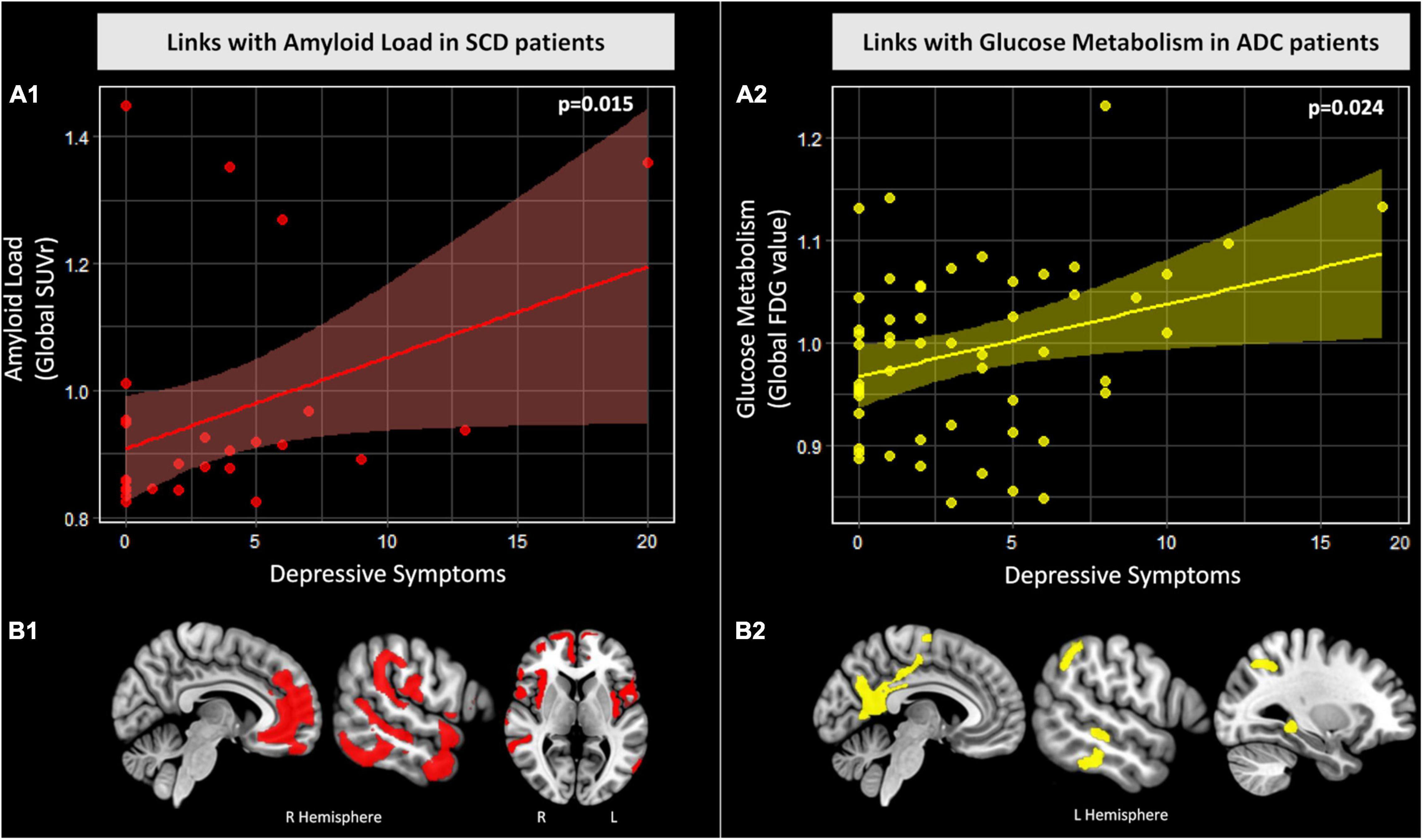
Figure 2. Relationships between depressive symptoms and amyloid load in SCD patients and glucose metabolism in ADC patients. (A) Graphs of the associations between depressive symptoms and global measures of amyloid load in SCD patients (A1) and glucose metabolism in ADC patients (A2). Reported statistics were obtained from the multiple linear regressions corrected for level of education, age and sex. Raw values are plotted and linear trends and confidence intervals (95%) are represented for SCD patients (red) and ADC patients (yellow). (B) Results of the voxelwise multiple regressions between depressive symptoms and amyloid deposition in SCD patients [(B1) red] and glucose metabolism in ADC patients [(B2) yellow]. Analyses were corrected for level of education, age and sex. All results are presented at a puncorrected < 0.005 threshold combined with a minimum cluster size determined by Monte-Carlo simulations to achieve a corrected statistical significance of p < 0.05 (i.e., kcorrected ≥ 1476 voxels for amyloid deposition and kcorrected ≥ 1757 voxels for glucose metabolism). Abbreviations ADC, Alzheimer’s continuum; FDG, 18F-fluorodeoxyglucose; L, Left; p, p value; R, Right; SCD, Subjective cognitive decline; SUVr, Standardized uptake value ratio.
As for anxiety symptoms, a trend for a positive association was found with global cognition within the SCD group (Table 2), as well as when also correcting for depressive symptoms (p = 0.06; see Supplementary Table 1). This association became significant with non-parametric analyses (p = 0.03; see Supplementary Table 2).
No association was found in the group of healthy controls with either depressive or anxiety symptoms (Table 2 and Supplementary Tables 1–3).
The positive relationship between episodic memory performance and depressive symptoms in ADC patients was not expected. Interestingly, a study showing similar results suggested that awareness of one’s cognitive deficits could be associated with worsened mood (Cerbone et al., 2020).
Along this line, we hypothesized that our finding with episodic memory might reflect anosognosia, such that ADC patients at a more advanced cognitive stage (i.e., with lower episodic memory performance) would be more anosognosic, either about their depressive symptoms (so that they have a lower depression score because they are less aware of their depressive symptoms); or about their cognitive deficits (so that they are less depressed about those). We thus ran additional analyses within the ADC patient group to test this hypothesis. We computed two composite delta scores of anosognosia for each ADC patient (Perrotin et al., 2015), one for global cognition and one for episodic memory performance, corresponding to the difference between the z-score of objective performance and the reversed z-score of subjective assessment [using the Cognitive Difficulties Scale (CDS) (McNair and Kahn, 1983; Kuhn et al., 2019)] for either global cognition (MMSE) or episodic memory (ESR) (see Supplementary Material 2 for further details). To test our hypothesis, we assessed the link between these two delta scores and depressive symptoms with multiple regressions corrected for level of education, age and sex, within the ADC patients. We found a positive association between the delta scores (awareness of cognitive and memory difficulties) and depressive symptoms (p = 0.01 and p < 0.001, respectively), as well as objective performance in global cognition (p < 0.001) and episodic memory (p < 0.001). This suggests that ADC patients with better cognitive and/or memory performance, are more aware of their cognitive difficulties and show more depressive symptoms; or reversely, that those with greater cognitive/memory deficits are more anosognosic and report fewer depressive symptoms.
We aimed to further investigate the brain substrates specifically involved in the positive associations found in the main analyses (Section “Psychoaffective factors and their links with cognition and neuroimaging biomarkers”) between depressive symptoms and both amyloid load in SCD patients and glucose metabolism in ADC patients. For this purpose, we performed voxelwise multiple regression analyses in SPM12 between depressive symptoms and amyloid deposition in SCD patients on the one hand, and glucose metabolism in ADC patients on the other hand. All analyses were corrected for education, age and sex. Results were evaluated for significance at puncorrected < 0.005 combined with a minimum cluster size determined by Monte-Carlo simulations using the AFNI’s 3dClustSim program to achieve a corrected statistical significance of p < 0.05.
In the SCD group, we found that higher depressive symptoms were associated with higher amyloid deposition mainly in the bilateral medial prefrontal, temporo-parietal, temporal, insular cortices and the right hippocampus (Figure 2B1).
In the ADC group, we found that higher depressive symptoms were associated with higher glucose metabolism in the bilateral precuneus, posterior cingulate—retrosplenial area, left temporal, superior parietal and temporal regions and the left hippocampus (Figure 2B2).
This study is, to our knowledge, the first to assess the links of anxiety and depressive symptoms with multiple AD-relevant indices, including cognitive and neuroimaging measures (i.e., global cognition, episodic memory, GM atrophy, glucose metabolism and amyloid deposition), in SCD and Alzheimer’s continuum. Altogether, we showed that SCD and ADC patients had higher depressive symptoms compared to healthy elders, which were associated with higher amyloid pathology in SCD, and with higher episodic memory performance and glucose metabolism in ADC patients.
In this study, we found no difference between groups regarding anxiety symptoms, but higher depressive symptoms in SCD and ADC patients compared to controls. This is in line with a previous study showing a higher frequency of depressive symptoms in clinical MCI and AD patients compared to controls, while anxiety symptoms were only different between mild and severe AD (Fernández-Martínez et al., 2010). Additionally, we found no association of anxiety symptoms with cognition and neuroimaging data, which is at odds with previous studies showing significant relationships with GM atrophy (Tagai et al., 2014; Hayata et al., 2015) and glucose hypometabolism (Hashimoto et al., 2006) in AD. This might be due to the fact that, in the present study, we focused on state measures of either anxiety or depressive symptoms, while these previous studies assessed trait anxiety. In addition, in these previous studies the level of anxiety symptoms of the patients was measured through an interview with their caregiver, while in our study it was self-rated by the patient. Thus, the differences in results could reflect discrepancies between self-rated and informant-rated anxiety.
In the SCD group, we found that depressive symptoms were not related to objective cognitive/memory performance but were associated with higher amyloid load mainly in medial prefrontal and temporo-parietal regions, which are among the earliest regions affected by amyloid deposition in AD (Grothe et al., 2016, Grothe et al., 2017). While some previous studies found higher depressive symptoms (Balash et al., 2013; Buckley et al., 2013), and higher amyloid load (Amariglio et al., 2012, 2015; Perrotin et al., 2012, 2017; Snitz et al., 2015) associated with subjective cognitive decline, no study to date formally assessed the links between depressive symptoms and amyloid deposition, in this specific population. Our finding of an association between depressive symptoms with amyloid load in SCD could indicate that depressive symptoms represent a manifestation of the ongoing pathology and/or are a risk factor promoting amyloid accumulation, or that both depressive symptoms and amyloid plaques are caused by a common, yet unknown, factor.
Furthermore, we found that this association between depressive symptoms and amyloid was specific to this SCD stage, where there is subjective but no objective cognitive deficit, as it was neither found in the HC group nor in the MCI/AD patients, even when not selected for being amyloid-positive. Previous findings were conflicting as, in cognitively unimpaired elders (corresponding to our HC), some (Krell-Roesch et al., 2018) but not all (Donovan et al., 2015) studies found a relationship between depressive symptoms and amyloid load. Similarly, while some studies reported a link between depressive symptoms and amyloid load in MCI (Brendel et al., 2015; Krell-Roesch et al., 2019), a recent systematic review showed that most studies in fact did not find this association (Banning et al., 2019).
Recent criteria for SCD and updates about this concept have highlighted that SCD with biomarker evidence for AD have increased risk for future cognitive decline (Jessen et al., 2014, 2020). As we found depressive symptoms to be associated with amyloid deposition in SCD patients in our study, this suggests that SCD patients with depressive symptoms may be at even greater risk for cognitive decline. Altogether, this suggests that depressive symptoms in SCD is not a mere psychological consequence of their memory concern, but might be considered as an additional risk factor, and thus treated, in this population.
In the ADC patient group, we found depressive symptoms to be associated with better episodic memory performance and higher glucose metabolism, i.e., with a less advanced clinical and neurodegenerative stage of the disease. Previous studies showed conflicting findings; thus, one study found worse cognitive performance to be associated with depressive symptoms, but they assessed a mixed group of cognitively healthy elders and MCI patients (Zhang et al., 2020). Another study found no association between depressive symptoms and global cognition in either MCI or AD patients (Fernández-Martínez et al., 2010). However, our findings are in line with recent studies showing higher glucose metabolism in frontal regions and the fusiform gyrus in MCI patients with depressive symptoms (Auning et al., 2015; Brendel et al., 2015). In contrast to the preclinical stage (SCD), the emergence of anosognosia (i.e., progressive decrease in awareness of cognitive deficits) is known to occur as the disease progresses from MCI to AD stages (Hanseeuw et al., 2020; Vannini et al., 2020; Bastin et al., 2021; Cacciamani et al., 2021a,b). In these patients, the presence of anosognosia might impact their neuropsychiatric symptoms or ability to report those. Indeed, a recent study found that MCI patients with lower depression scores showed steeper decline in dementia severity measures compared to those with higher depression scores (Cerbone et al., 2020). The authors suggested that being aware of one’s cognitive deficits could be associated with worsened mood (more depressive symptoms), while, conversely, MCI patients who are less or not aware of their cognitive deficits may be less affected and show less to no depressive symptoms. Alternatively, it is also possible that patients at a more advanced stage of the disease (i.e., with more cognitive deficits) tend to report fewer depressive symptoms as they are less aware of their symptoms (more anosognosic). In line with these interpretations, depressive symptoms were found to be associated with less anosognosia in a group of patients with AD dementia (Kashiwa et al., 2005). In addition, the functional neural substrates of depressive symptoms in ADC patients were localized in regions which are known to be related to anosognosia in MCI and AD patients. Indeed, previous works highlighted that greater anosognosia in these patients was associated with reduced glucose metabolism in the posterior cingulate cortex, hippocampus, superior temporal and parietal gyri (Salmon et al., 2006; Nobili et al., 2010; Perrotin et al., 2015; Vannini et al., 2017; Hallam et al., 2020). The fact that we found higher depressive symptoms to be associated with better awareness of cognitive difficulties in our ADC patient group is also in line with those hypotheses.
In contrast to cognition and glucose metabolism, we found no link between depressive symptoms and GM volume nor amyloid deposition in ADC patients. Previous findings are conflicting, with studies also reporting no links (Bruen et al., 2008; Starkstein et al., 2009; Berlow et al., 2010; Mori et al., 2014; Huey et al., 2017) while others found a positive association (Auning et al., 2015; Enache et al., 2015), or a negative (Lebedeva et al., 2014; Wu et al., 2020) with depressive symptoms in MCI or AD populations. Our findings suggest that glucose metabolism appears to be more strongly associated with depressive symptoms in amyloid-positive MCI-AD patients than GM volume or amyloid deposition.
Even though the MADRS has been shown to be a good measure of depression relatively independent from dementia severity (Müller-Thomsen et al., 2005), as our participants were selected for the lack of clinically significant anxiety or depression, one of the limitations of our study refers to the skewed distribution of MADRS, with 42% of the total participants reporting depressive symptoms. To limit the bias associated with the low variability and thus low power of analyses, we repeated all analyses with non-parametric tests, as well as in subgroups including only individuals with at least one depressive symptom.
Our study, assessing multiple hallmarks of AD (i.e., global cognition, episodic memory, gray matter volume, glucose metabolism and amyloid load), was cross-sectional in design and thus couldn’t assess the causality and direction of these links. Future longitudinal analyses would allow to investigate this question by examining the links between baseline levels and changes over time in depressive and anxiety symptoms and neuroimaging biomarkers. Similarly, as discussed above, we investigated state measures of depressive and anxiety symptoms as they represent states at a given time that we expect to easily change over time and be modifiable through treatment/interventions. Moreover, anxiety symptoms were assessed using a self-report questionnaire; as it is subjective, the measure could be biased by the subject’s honesty, awareness and introspective ability.
This study showed that depressive symptoms were associated with higher amyloid load in SCD, and with better episodic memory and higher glucose metabolism in ADC patients. Overall, our findings suggest that depressive symptoms reflect distinct processes along the course of AD, with higher symptoms reflecting greater likelihood of AD biomarker at the SCD stage, while, conversely, they would reflect greater awareness of cognitive deficits associated with less severe cognitive stage of the disease in ADC patients. Thus, this study shows the relevance of assessing and following depressive symptoms in SCD, and to manage them in cognitively impaired patients, to improve the prevention as well as the prognosis and quality of life of both patients and caregivers.
The datasets presented in this article are not readily available because IMAP data are made available upon request to the sponsor (Caen University Hospital) and the principal investigator. Requests to access the datasets should be directed to GC, Y2hldGVsYXRAY3ljZXJvbi5mcg==.
The studies involving human participants were reviewed and approved by Comité de Protection des Personnes Nord-Ouest III. The patients/participants provided their written informed consent to participate in this study.
IM and GC contributed to the conception and design of the study. IM, ET, and GC contributed to the acquisition, analysis, or interpretation of the data and wrote the draft manuscript. IM, ET, FM, SD, VD, DV, NM, GP, and GC contributed to the critical revision of the manuscript for important intellectual content. IM performed the statistical analysis. GC obtained the funding. FM, DV, and GP contributed to the administrative, technical, or material support. GC and VD were the principal investigators of the IMAP + research protocol. All authors took public responsibility for the whole or part of the content, contributed to the acquisition, analysis and interpretation of data, manuscript revision, and read and approved the submitted version.
This project was supported by Agence Nationale de la Recherche (LONGVIE, 2007) Association France Alzheimer et maladies apparentées AAP 2013, Fondation Plan Alzheimer (Alzheimer Plan 2008–2012), Institut National de la Santé et de la Recherche Médicale (INSERM), European Union’s Horizon2020 Research and Innovation Program (grant667696), Programme Hospitalier de Recherche Clinique (PHRCN 2011-A01493-38 and PHRCN 2012 12-006-0347), Région Basse-Normandie, University of Caen Normandy. Funding sources had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and the decision to submit the manuscript for publication. ET received a thesis grant from the French Ministère de l’Enseignement Supérieur et de la Recherche (paid to ET). SD received French ministerial scholarship and University grant for traveling and attending a scientific meeting in Berlin (paid to SD). DV received fundings from Inserm and from European Union Horizon 2020 (all payments made to DV’s institution). NM received grants from the Alzheimer’s Society, European Union Horizon 2020 and Medical Research Council (all payments made to NM’s institution) and European Union’s Horizon 2020 research and innovation programme for travel (payment made to NM). GC received research support from the EU’s Horizon 2020 research and innovation programme (grant agreement number 667696), Fondation d’entreprise MMA des Entrepreneurs du Futur, Fondation Alzheimer, Programme Hospitalier de Recherche Clinique, Région Normandie, Association France Alzheimer et maladies apparentées and Fondation Vaincre Alzheimer (all to Inserm), and personal fees from Inserm, Fondation Alzheimer and Fondation d’entreprise MMA des Entrepreneurs du Futur.
GP was a member of the DSMB of the Age-well trial for the Inserm Partner (not paid). GC was Member of the External Advisory Board (EAB) of the Lifebrain H2020 European project and of the Operational Committee of the Foundation Plan Alzheimer (personal fees) and of the Imaging Scientific Advisory Groups of European Prediction of Alzheimer’s Disease (EPAD) Consortium, EU (not paid).
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We would like to thank all the persons who contributed to this research: Brigitte Landeau, Elizabeth Kuhn, Renaud La Joie, Julie Gonneaud, Audrey Perrotin, Eider Arenaza-Urquijo, Alexandre Bejanin, Siya Sherif, Robin de Flores, Clémence Tomadesso, Justine Mutlu, Nicolas Villain, Marine Fouquet, Katell Mevel, Francis Eustache, Stéphanie Egret, Jean-Claude Baron, Fausto Viader, Alice Pélerin, Malo Gaubert, Géraldine Rauchs, Anne Quillard, Anne Chocat, Ahmed Abbas, Louisa Barré, Alain Manrique, Denis Guilloteau, Florence Pasquier, Serge Belliard, Christopher Rowe, Victor Villemagne, Antoine Lutz, the Cyceron staff members and the volunteers who were included in these studies.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnagi.2022.899158/full#supplementary-material
Altman, D. G., and Royston, P. (2006). The cost of dichotomising continuous variables. BMJ 332:1080. doi: 10.1136/bmj.332.7549.1080
Amariglio, R. E., Becker, J. A., Carmasin, J., Wadsworth, L. P., Lorius, N., Sullivan, C., et al. (2012). Subjective cognitive complaints and amyloid burden in cognitively normal older individuals. Neuropsychologia 50, 2880–2886. doi: 10.1016/j.neuropsychologia.2012.08.011
Amariglio, R. E., Mormino, E. C., Pietras, A. C., Marshall, G. A., Vannini, P., Johnson, K. A., et al. (2015). Subjective cognitive concerns, amyloid-β, and neurodegeneration in clinically normal elderly. Neurology 85, 56–62. doi: 10.1212/WNL.0000000000001712
Auning, E., Selnes, P., Grambaite, R., Šaltytė Benth, J., Haram, A., Løvli Stav, A., et al. (2015). Neurobiological correlates of depressive symptoms in people with subjective and mild cognitive impairment. Acta Psychiatr. Scand 131, 139–147. doi: 10.1111/acps.12352
Balash, Y., Mordechovich, M., Shabtai, H., Giladi, N., Gurevich, T., and Korczyn, A. D. (2013). Subjective memory complaints in elders: depression, anxiety, or cognitive decline? Acta Neurol. Scand. 127, 344–350. doi: 10.1111/ane.12038
Banning, L. C. P., Ramakers, I. H. G. B., Deckers, K., Verhey, F. R. J., and Aalten, P. (2019). Affective symptoms and AT(N) biomarkers in mild cognitive impairment and Alzheimer’s disease: a systematic literature review. Neurosci. Biobehav. Rev. 107, 346–359. doi: 10.1016/j.neubiorev.2019.09.014
Bastin, C., Giacomelli, F., Miévis, F., Lemaire, C., Guillaume, B., and Salmon, E. (2021). Anosognosia in mild cognitive impairment: lack of awareness of memory difficulties characterizes prodromal alzheimer’s disease. Front. Psychiatry 12:631518. doi: 10.3389/fpsyt.2021.631518
Bejanin, A., La Joie, R., Landeau, B., Belliard, S., de La Sayette, V., Eustache, F., et al. (2019). Distinct interplay between atrophy and hypometabolism in alzheimer’s versus semantic dementia. Cereb. Cortex 29, 1889–1899. doi: 10.1093/cercor/bhy069
Bensamoun, D., Guignard, R., Furst, A. J., Derreumaux, A., Manera, V., Darcourt, J., et al. (2016). Associations between neuropsychiatric symptoms and cerebral amyloid deposition in cognitively impaired elderly people. J. Alzheimer’s Dis. 49, 387–398. doi: 10.3233/JAD-150181
Berlow, Y. A., Wells, W. M., Ellison, J. M., Sung, Y. H., Renshaw, P. F., and Harper, D. G. (2010). Neuropsychiatric correlates of white matter hyperintensities in Alzheimer’s disease. Int. J. Geriatric Psychiatry 25, 780–788. doi: 10.1002/gps.2418
Besson, F. L., Joie, R. L., Doeuvre, L., Gaubert, M., Mézenge, F., Egret, S., et al. (2015). Cognitive and brain profiles associated with current neuroimaging biomarkers of preclinical alzheimer’s disease. J. Neurosci. 35, 10402–10411. doi: 10.1523/JNEUROSCI.0150-15.2015
Brendel, M., Pogarell, O., Xiong, G., Delker, A., Bartenstein, P., Rominger, A., et al. (2015). Depressive symptoms accelerate cognitive decline in amyloid-positive MCI patients. Eur. J. Nucl. Med. Mol. Imaging 42, 716–724. doi: 10.1007/s00259-014-2975-4
Bruen, P. D., McGeown, W. J., Shanks, M. F., and Venneri, A. (2008). Neuroanatomical correlates of neuropsychiatric symptoms in Alzheimer’s disease. Brain 131, 2455–2463. doi: 10.1093/brain/awn151
Buckley, R., Saling, M. M., Ames, D., Rowe, C. C., Lautenschlager, N. T., Macaulay, S. L., et al. (2013). Factors affecting subjective memory complaints in the AIBL aging study: biomarkers, memory, affect, and age. Int. Psychogeriatr. 25, 1307–1315. doi: 10.1017/S1041610213000665
Cacciamani, F., Houot, M., Gagliardi, G., Dubois, B., Sikkes, S., Sánchez-Benavides, G., et al. (2021a). Awareness of cognitive decline in patients with alzheimer’s disease: a systematic review and meta-analysis. Front. Aging Neurosci. 13:697234. doi: 10.3389/fnagi.2021.697234
Cacciamani, F., Valladier, A., Maheux, E., Koval, I., Durrleman, S., and Epelbaum, S. (2021b). Changes in the awareness of cognitive decline across the course of Alzheimer’s disease: Comparison of two assessment methods. Alzheimer’s Dement. 17, e053074. doi: 10.1002/alz.053074
Cerbone, B., Massman, P. J., Kulesz, P. A., Woods, S. P., and York, M. K. (2020). Predictors of rate of cognitive decline in patients with amnestic mild cognitive impairment. Clin. Neuropsychol. 36, 138–164. doi: 10.1080/13854046.2020.1773933
Chen, Y., Dang, M., and Zhang, Z. (2021). Brain mechanisms underlying neuropsychiatric symptoms in Alzheimer’s disease: a systematic review of symptom-general and –specific lesion patterns. Mol. Neurodegener. 16:38. doi: 10.1186/s13024-021-00456-1
Chételat, C., Desgranges, B., Landeau, B., Mézenge, F., Poline, J. B., de la Sayette, V., et al. (2008). Direct voxel-based comparison between grey matter hypometabolism and atrophy in Alzheimer’s disease. Brain 131, 60–71. doi: 10.1093/brain/awm288
Chung, J. K., Plitman, E., Nakajima, S., Chakravarty, M. M., Caravaggio, F., Gerretsen, P., et al. (2015). Cortical Amyloid β Deposition and Current Depressive Symptoms in Alzheimer Disease and Mild Cognitive Impairment. J. Geriatric Psychiatry Neurol. 29, 149–159. doi: 10.1177/0891988715606230
Dhikav, V., Sethi, M., and Anand, K. S. (2014). Medial temporal lobe atrophy in Alzheimer’s disease/mild cognitive impairment with depression. Br. J Radiol 87:20140150. doi: 10.1259/bjr.20140150
Donovan, N. J., Hsu, D. C., Dagley, A. S., Schultz, A. P., Amariglio, R. E., Mormino, E. C., et al. (2015). Depressive Symptoms and Biomarkers of Alzheimer’s Disease in Cognitively Normal Older Adults. J. Alzheimers Dis. 46, 63–73. doi: 10.3233/JAD-142940
Enache, D., Cavallin, L., Lindberg, O., Farahmand, B., Kramberger, M., Westman, E., et al. (2015). Medial temporal lobe atrophy and depressive symptoms in elderly patients with and without alzheimer disease. J. Geriatric Psychiatry Neurol. 28, 40–48. doi: 10.1177/0891988714541873
Eustache, F., Laisney, M., Lalevée, C., Pèlerin, A., Perrotin, A., Egret, S., et al. (2015). Une nouvelle épreuve de mémoire épisodique: l’épreuve ESR-forme réduite (ESR-r), adaptée du paradigme ESR (encodage, stockage, récupération). Rev. Neuropsychol. 7, 217–225. doi: 10.1684/nrp.2015.0351
Fernández-Martínez, M., Molano, A., Castro, J., and Zarranz, J. J. (2010). Prevalence of neuropsychiatric symptoms in mild cognitive impairment and Alzheimer’s disease, and its relationship with cognitive impairment. Curr. Alzheimer Res. 7, 517–526. doi: 10.2174/156720510792231748
Finkel, S. I., Costa e Silva, J., Cohen, G., Miller, S., and Sartorius, N. (1996). Behavioral and psychological signs and symptoms of dementia: a consensus statement on current knowledge and implications for research and treatment. Int. Psychogeriatr. 8(Suppl. 3), 497–500. doi: 10.1017/s1041610297003943
Folstein, M. F., Folstein, S. E., and McHugh, P. R. (1975). Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 12, 189–198. doi: 10.1016/0022-3956(75)90026-6
Fujishima, M., Maikusa, N., Nakamura, K., Nakatsuka, M., Matsuda, H., and Meguro, K. (2014). Mild cognitive impairment, poor episodic memory, and late-life depression are associated with cerebral cortical thinning and increased white matter hyperintensities. Front. Aging Neurosci. 6:306. doi: 10.3389/fnagi.2014.00306
Geda, Y. E., Roberts, R. O., Mielke, M. M., Knopman, D. S., Christianson, T. J. H., Pankratz, V. S., et al. (2014). Baseline neuropsychiatric symptoms and the risk of incident mild cognitive impairment: a population-based study. Am. J. Psychiatry 171, 572–581. doi: 10.1176/appi.ajp.2014.13060821
Gilley, D. W., Bienias, J. L., Wilson, R. S., Bennett, D. A., Beck, T. L., and Evans, D. A. (2004). Influence of behavioral symptoms on rates of institutionalization for persons with Alzheimer’s disease. Psychol. Med. 34, 1129–1135. doi: 10.1017/S0033291703001831
Grothe, M. J., Barthel, H., Sepulcre, J., Dyrba, M., Sabri, O., Teipel, S. J., et al. (2017). In vivo staging of regional amyloid deposition. Neurology 89, 2031–2038. doi: 10.1212/WNL.0000000000004643
Grothe, M. J., Teipel, S. J., Alzheimer’s Disease Neuroimaging Initiative (2016). Spatial patterns of atrophy, hypometabolism, and amyloid deposition in Alzheimer’s disease correspond to dissociable functional brain networks. Hum. Brain Mapp. 37, 35–53. doi: 10.1002/hbm.23018
Hallam, B., Chan, J., Gonzalez Costafreda, S., Bhome, R., and Huntley, J. (2020). What are the neural correlates of meta-cognition and anosognosia in Alzheimer’s disease? A systematic review. Neurobiol. Aging 94, 250–264. doi: 10.1016/j.neurobiolaging.2020.06.011
Hanseeuw, B. J., Scott, M. R., Sikkes, S. A. M., Properzi, M., Gatchel, J. R., Salmon, E., et al. (2020). Evolution of anosognosia in alzheimer’s disease and its relationship to amyloid. Ann. Neurol. 87, 267–280. doi: 10.1002/ana.25649
Harrington, K. D., Lim, Y. Y., Gould, E., and Maruff, P. (2015). Amyloid-beta and depression in healthy older adults: a systematic review. Aust N Z J Psychiatry 49, 36–46. doi: 10.1177/0004867414557161
Hashimoto, H., Monserratt, L., Nguyen, P., Feil, D., Harwood, D., Mandelkern, M. A., et al. (2006). Anxiety and regional cortical glucose metabolism in patients with Alzheimer’s disease. J. Neuropsychiatry Clin. Neurosci. 18, 521–528. doi: 10.1176/jnp.2006.18.4.521
Hayata, T. T., Bergo, F. P. G., Rezende, T. J., Damasceno, A., Damasceno, B. P., Cendes, F., et al. (2015). Cortical correlates of affective syndrome in dementia due to Alzheimer’s disease. Arq. Neuro-Psiquiatr. 73, 553–560. doi: 10.1590/0004-282X20150068
Hoe, J., Hancock, G., Livingston, G., and Orrell, M. (2006). Quality of life of people with dementia in residential care homes. Br. J. Psychiatry 188, 460–464. doi: 10.1192/bjp.bp.104.007658
Hoe, J., Katona, C., Orrell, M., and Livingston, G. (2007). Quality of life in dementia: care recipient and caregiver perceptions of quality of life in dementia: the LASER-AD study. Int. J. Geriatr. Psychiatry 22, 1031–1036. doi: 10.1002/gps.1786
Horínek, D., Petrovický, P., Hort, J., Krásenský, J., Brabec, J., Bojar, M., et al. (2006). Amygdalar volume and psychiatric symptoms in Alzheimer’s disease: an MRI analysis. Acta Neurol. Scand 113, 40–45. doi: 10.1111/j.1600-0404.2006.00540.x
Huey, E. D., Lee, S., Cheran, G., Grafman, J., and Devanand, D. P. (2017). Brain Regions Involved in Arousal and Reward Processing are Associated with Apathy in Alzheimer’s Disease and Frontotemporal Dementia. J. Alzheimer’s Dis. 55, 551–558. doi: 10.3233/JAD-160107
Jessen, F., Amariglio, R. E., Buckley, R. F., van der Flier, W. M., Han, Y., Molinuevo, J. L., et al. (2020). The characterisation of subjective cognitive decline. Lancet. Neurol. 19, 271–278. doi: 10.1016/S1474-4422(19)30368-0
Jessen, F., Amariglio, R. E., van Boxtel, M., Breteler, M., Ceccaldi, M., Chételat, G., et al. (2014). A conceptual framework for research on subjective cognitive decline in preclinical Alzheimer’s disease. Alzheimers Dement 10, 844–852. doi: 10.1016/j.jalz.2014.01.001
Kashiwa, Y., Kitabayashi, Y., Narumoto, J., Nakamura, K., Ueda, H., and Fukui, K. (2005). Anosognosia in Alzheimer’s disease: Association with patient characteristics, psychiatric symptoms and cognitive deficits. Psychiatry Clin. Neurosci. 59, 697–704. doi: 10.1111/j.1440-1819.2005.01439.x
Krell-Roesch, J., Lowe, V. J., Neureiter, J., Pink, A., Roberts, R. O., Mielke, M. M., et al. (2018). DEPRESSIVE and anxiety symptoms and cortical amyloid deposition among cognitively normal elderly persons: the mayo clinic study of aging. Int. Psychogeriatr. 30, 245–251. doi: 10.1017/S1041610217002368
Krell-Roesch, J., Vassilaki, M., Mielke, M. M., Kremers, W. K., Lowe, V. J., Vemuri, P., et al. (2019). Cortical β-amyloid burden, neuropsychiatric symptoms, and cognitive status: the Mayo Clinic Study of Aging. Trans. Psychiatry 9, 1–8. doi: 10.1038/s41398-019-0456-z
Kuhn, E., Moulinet, I., Perrotin, A., La Joie, R., Landeau, B., Tomadesso, C., et al. (2019). Cross-sectional and longitudinal characterization of SCD patients recruited from the community versus from a memory clinic: subjective cognitive decline, psychoaffective factors, cognitive performances, and atrophy progression over time. Alzheimers Res. Ther. 11:61. doi: 10.1186/s13195-019-0514-z
La Joie, R., Perrotin, A., Barré, L., Hommet, C., Mézenge, F., Ibazizene, M., et al. (2012). Region-specific hierarchy between atrophy, hypometabolism, and β-amyloid (Aβ) load in Alzheimer’s disease dementia. J. Neurosci. 32, 16265–16273. doi: 10.1523/JNEUROSCI.2170-12.2012
La Joie, R., Perrotin, A., Egret, S., Pasquier, F., Tomadesso, C., Mézenge, F., et al. (2016). Qualitative and quantitative assessment of self-reported cognitive difficulties in nondemented elders: association with medical help seeking, cognitive deficits, and β-amyloid imaging. Alzheimers Dement. (Amst) 5, 23–34. doi: 10.1016/j.dadm.2016.12.005
Laborde-Lahoz, P., El-Gabalawy, R., Kinley, J., Kirwin, P. D., Sareen, J., and Pietrzak, R. H. (2015). Subsyndromal depression among older adults in the USA: prevalence, comorbidity, and risk for new-onset psychiatric disorders in late life. Int. J. Geriatr. Psychiatry 30, 677–685. doi: 10.1002/gps.4204
Lebedeva, A., Westman, E., Lebedev, A. V., Li, X., Winblad, B., Simmons, A., et al. (2014). Structural brain changes associated with depressive symptoms in the elderly with Alzheimer’s disease. J. Neurol. Neurosurg. Psychiatry 85, 930–935. doi: 10.1136/jnnp-2013-307110
Levy-Cooperman, N., Burhan, A. M., Rafi-Tari, S., Kusano, M., Ramirez, J., Caldwell, C., et al. (2008). Frontal lobe hypoperfusion and depressive symptoms in Alzheimer disease. J. Psychiatry Neurosci. 33, 218–226.
McKhann, G., Drachman, D., Folstein, M., Katzman, R., Price, D., and Stadlan, E. M. (1984). Clinical diagnosis of alzheimer’s disease: report of the nincds-adrda work group under the auspices of department of health and human services task force on alzheimer’s disease. Neurology 34, 939–944. doi: 10.1212/wnl.34.7.939
McNair, D., and Kahn, R. (1983). Self-assessment of cognitive deficits. Assessment in Geriatric Psychopharmacology. Assess. Geriatric Psychopharmacol. 119–136.
Mendez, M. F. (2021). The relationship between anxiety and alzheimer’s disease. J. Alzheimers Dis. Rep. 5, 171–177. doi: 10.3233/ADR-210294
Montgomery, S. A., and Asberg, M. (1979). A new depression scale designed to be sensitive to change. Br. J. Psychiatry 134, 382–389. doi: 10.1192/bjp.134.4.382
Mori, T., Shimada, H., Shinotoh, H., Hirano, S., Eguchi, Y., Yamada, M., et al. (2014). Apathy correlates with prefrontal amyloid β deposition in Alzheimer’s disease. J. Neurol. Neurosurg. Psychiatry 85, 449–455. doi: 10.1136/jnnp-2013-306110
Müller-Gärtner, H. W., Links, J. M., Prince, J. L., Bryan, R. N., McVeigh, E., Leal, J. P., et al. (2016). Measurement of radiotracer concentration in brain gray matter using positron emission tomography: MRI-Based correction for partial volume effects. J. Cereb. Blood Flow Metab. 12, 571–583. doi: 10.1038/jcbfm.1992.81
Müller-Thomsen, T., Arlt, S., Mann, U., Maß, R., and Ganzer, S. (2005). Detecting depression in Alzheimer’s disease: evaluation of four different scales. Arch. Clin. Neuropsychol. 20, 271–276. doi: 10.1016/j.acn.2004.03.010
Nobili, F., Mazzei, D., Dessi, B., Morbelli, S., Brugnolo, A., Barbieri, P., et al. (2010). Unawareness of memory deficit in amnestic MCI: FDG-PET findings. J. Alzheimers Dis. 22, 993–1003. doi: 10.3233/JAD-2010-100423
Perrotin, A., Desgranges, B., Landeau, B., Mézenge, F., Joie, R. L., Egret, S., et al. (2015). Anosognosia in Alzheimer disease: disconnection between memory and self-related brain networks. Ann. Neurol. 78, 477–486. doi: 10.1002/ana.24462
Perrotin, A., La Joie, R., de La Sayette, V., Barré, L., Mézenge, F., Mutlu, J., et al. (2017). Subjective cognitive decline in cognitively normal elders from the community or from a memory clinic: differential affective and imaging correlates. Alzheimers Dement. 13, 550–560. doi: 10.1016/j.jalz.2016.08.011
Perrotin, A., Mormino, E. C., Madison, C. M., Hayenga, A. O., and Jagust, W. J. (2012). Subjective cognition and amyloid deposition imaging: a Pittsburgh Compound B positron emission tomography study in normal elderly individuals. Arch. Neurol. 69, 223–229. doi: 10.1001/archneurol.2011.666
Petersen, R. C., and Morris, J. C. (2005). Mild cognitive impairment as a clinical entity and treatment target. Arch. Neurol. 62, 1160–1163. doi: 10.1001/archneur.62.7.1160
Petkus, A. J., Reynolds, C. A., Wetherell, J. L., Kremen, W. S., Pedersen, N. L., and Gatz, M. (2016). Anxiety is associated with increased risk of dementia in older Swedish twins. Alzheimers Dement. 12, 399–406. doi: 10.1016/j.jalz.2015.09.008
Poulin, S. P., Bergeron, D., and Dickerson, B. C., Alzheimer’s Disease, and Neuroimaging Initiative. (2017). Risk factors, neuroanatomical correlates, and outcome of neuropsychiatric symptoms in alzheimer’s disease. J. Alzheimers Dis. 60, 483–493. doi: 10.3233/JAD-160767
Poulin, S. P., Dautoff, R., Morris, J. C., Barrett, L. F., and Dickerson, B. C. (2011). Amygdala atrophy is prominent in early Alzheimer’s disease and relates to symptom severity. Psychiatry Res. Neuroimaging 194, 7–13. doi: 10.1016/j.pscychresns.2011.06.014
Salmon, E., Perani, D., Herholz, K., Marique, P., Kalbe, E., Holthoff, V., et al. (2006). Neural correlates of anosognosia for cognitive impairment in Alzheimer’s disease. Hum. Brain Mapp. 27, 588–597. doi: 10.1002/hbm.20203
Serra, L., Perri, R., Cercignani, M., Spanò, B., Fadda, L., Marra, C., et al. (2010). Are the Behavioral Symptoms of Alzheimer’s Disease Directly Associated with Neurodegeneration? J. Alzheimer’s Dis. 21, 627–639. doi: 10.3233/JAD-2010-100048
Snitz, B. E., Lopez, O. L., McDade, E., Becker, J. T., Cohen, A. D., Price, J. C., et al. (2015). Amyloid-beta imaging in older adults presenting to a memory clinic with subjective cognitive decline. J. Alzheimers Dis. 48, S151–S159. doi: 10.3233/JAD-150113
Son, J. H., Han, D. H., Min, K. J., and Kee, B. S. (2013). Correlation between gray matter volume in the temporal lobe and depressive symptoms in patients with Alzheimer’s disease. Neurosci. Lett. 548, 15–20. doi: 10.1016/j.neulet.2013.05.021
Spielberger, C. D., Gorsuch, R. L., and Lushene, R. E. (1970). Manual for the State-Trait Anxiety Inventory. Polo Alto, CA: Consulting Psychologists Press.
Starkstein, S. E., Mizrahi, R., Capizzano, A. A., Acion, L., Brockman, S., and Power, B. D. (2009). Neuroimaging correlates of apathy and depression in alzheimer’s disease. JNP 21, 259–265. doi: 10.1176/jnp.2009.21.3.259
Tagai, K., Nagata, T., Shinagawa, S., Nemoto, K., Inamura, K., Tsuno, N., et al. (2014). Correlation between both morphologic and functional changes and anxiety in Alzheimer’s disease. Dement. Geriatr. Cogn. Disord 38, 153–160. doi: 10.1159/000358822
Tommaso, B., Leonardo, I., Giuseppe, M., Nagehan, A., Bruce, L. M., William, J. J., et al. (2016). Neuropsychiatric subsyndromes and brain metabolic network dysfunctions in early onset alzheimer’s disease. Hum. Brain Mapp. 37, 4234–4247. doi: 10.1002/hbm.23305
Vannini, P., Hanseeuw, B. J., Gatchel, J. R., Sikkes, S. A. M., Alzate, D., Zuluaga, Y., et al. (2020). Trajectory of unawareness of memory decline in individuals with autosomal dominant alzheimer disease. JAMA. Netw. Open 3:e2027472. doi: 10.1001/jamanetworkopen.2020.27472
Vannini, P., Hanseeuw, B., Munro, C. E., Amariglio, R. E., Marshall, G. A., Rentz, D. M., et al. (2017). Anosognosia for memory deficits in mild cognitive impairment: Insight into the neural mechanism using functional and molecular imaging. Neuroimage Clin. 15, 408–414. doi: 10.1016/j.nicl.2017.05.020
Villain, N., Desgranges, B., Viader, F., de la Sayette, V., Mézenge, F., Landeau, B., et al. (2008). Relationships between hippocampal atrophy, white matter disruption, and gray matter hypometabolism in Alzheimer’s disease. J. Neurosci. 28, 6174–6181. doi: 10.1523/JNEUROSCI.1392-08.2008
Wu, Y., Wu, X., Wei, Q., Wang, K., and Tian, Y. (2020). Differences in cerebral structure associated with depressive symptoms in the elderly with alzheimer’s disease. Front. Aging Neurosci. 12:107. doi: 10.3389/fnagi.2020.00107
Zhang, Z., Wei, F., Shen, X.-N., Ma, Y.-H., Chen, K.-L., Dong, Q., et al. (2020). Associations of subsyndromal symptomatic depression with cognitive decline and brain atrophy in elderly individuals without dementia: a longitudinal study. J. Affect. Disord. 274, 262–268. doi: 10.1016/j.jad.2020.05.097
Keywords: Alzheimer’s disease, amyloid deposition, cognition, depressive symptoms, anxiety, glucose metabolism, subjective cognitive decline, gray matter
Citation: Moulinet I, Touron E, Mézenge F, Dautricourt S, De La Sayette V, Vivien D, Marchant NL, Poisnel G and Chételat G (2022) Depressive Symptoms Have Distinct Relationships With Neuroimaging Biomarkers Across the Alzheimer’s Clinical Continuum. Front. Aging Neurosci. 14:899158. doi: 10.3389/fnagi.2022.899158
Received: 18 March 2022; Accepted: 30 May 2022;
Published: 20 June 2022.
Edited by:
Panteleimon Giannakopoulos, Université de Genève, SwitzerlandReviewed by:
Elodie Bertrand, Université de Paris, FranceCopyright © 2022 Moulinet, Touron, Mézenge, Dautricourt, De La Sayette, Vivien, Marchant, Poisnel and Chételat. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Gaël Chételat, Y2hldGVsYXRAY3ljZXJvbi5mcg==
†These authors share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.