 Chao-yang Guo
Chao-yang Guo Yun-jing Ma
Yun-jing Ma Shu-ting Liu
Shu-ting Liu Ran-ran Zhu
Ran-ran Zhu Xiao-ting Xu
Xiao-ting Xu Zhen-rui Li
Zhen-rui Li Lei Fang
Lei Fang
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Aging Neurosci., 13 May 2022
Sec. Neurocognitive Aging and Behavior
Volume 14 - 2022 | https://doi.org/10.3389/fnagi.2022.872233
This article is part of the Research TopicPhysical Exercise for Age-Related Neuromusculoskeletal DisordersView all 36 articles
Sarcopenia has become a key challenge for healthy aging in older adults. However, it remains unclear whether traditional Chinese medicine can effectively treat sarcopenia. This systematic review analyzes the current evidence for the effect of traditional Chinese medicine (TCM) on sarcopenia. We searched for articles regarding sarcopenia treated by TCM in Cochrane library, PubMed, SinoMed, Web of Science, Embase, and the China National Knowledge Infrastructure (from inception until 10 December 2021). Two researchers independently screened the literature in accordance with the inclusion and exclusion criteria designed by PICOS principles. The risk of bias was assessed by the Cochrane Risk of Bias (ROB) tool. The quality of evidence was assessed by the grading of recommendations, assessment, development, and evaluation (GRADE). Participants’ characteristics, interventions, and the relevant results of the included studies were extracted and synthesized in a narrative way. The total number of participants in the 21 included studies was 1,330. Most of the studies evaluated physical function (n = 20) and muscle strength (n = 18), and a small number of studies (n = 6) assessed muscle mass. Overall, it was found that TCM had a positive impact on muscle strength (grip strength, chair stand test) and physical function (6-m walking speed, timed up and go test, sit and reach) in patients with sarcopenia, inconsistent evidence of effects on muscle mass. However, the small sample size of the included studies led to imprecision in the results, and the presence of blinding of the studies, allocation concealment, and unreasonable problems with the control group design made the results low grade. Among these results, the quality of evidence for grip strength (n = 10) was of medium grade, and the quality of evidence related to the remaining indicators was of low grade. This systematic review showed that traditional Chinese Qigong exercises and Chinese herbal medicine have a positive and important effect on physical performance and muscle strength in older adults with sarcopenia. Future high-quality multicenter randomized controlled trials (RCTs) with large samples are needed to determinate whether acupuncture and other therapies are effective in treating sarcopenia.
Sarcopenia is a progressive and pervasive age-related primary skeletal muscle disorder involving the accelerated loss of muscle strength and mass, which is associated with increased adverse outcomes, including fall fracture, disability, and mortality (Cruz-Jentoft and Sayer, 2019; Chen et al., 2020). Sarcopenia is recognized as an independent condition and was given an International Classification of Diseases-10 code in 2016. The 2019 European Working Group on Sarcopenia in Older People (EWGSOP) updated definition suggests that physical performance should be considered a measure of the severity of sarcopenia (Cruz-Jentoft et al., 2019). More than 50 million people worldwide currently have sarcopenia, and it is expected that more than 200 million people will have sarcopenia by 2050 (Sousa et al., 2016). Physical dysfunction is the primary problem caused by sarcopenia. In Western society, as many as 42% of individuals under 60 years of age have difficulties performing the activities of daily life (e.g., walking speed or standing up from a chair), 15–30% report being unable to lift or carry 10 pounds or more, and more than 30% are confronted with physical disabilities (Louie and Ward, 2010). Sarcopenia has become a key challenge for healthy aging in older adults because the early symptoms are not obvious and are difficult to prevent and manage effectively. The main international treatments for sarcopenia are currently exercise, high-protein nutritional supplementation, and medication (Cruz-Jentoft and Sayer, 2019). However, medications (such as sex hormones, growth hormone, vitamin D, testosterone, and angiotensin-converting enzyme inhibitors) and nutritional supplementation are ineffective (Li et al., 2022). Relevant evidence-based clinical practice guidelines were published in 2018 with strong recommendations for exercise as the primary treatment for sarcopenia (Dent et al., 2018). Exercise has a positive impact on the health of older adults, but aging is usually accompanied by a significant decline in the body’s motor organs and functions, thus emphasizing the importance of appropriate exercise intensity and exercise forms for older adults. Traditional Chinese medicine (TCM), the oldest existing medical model for maintaining health and curing diseases, includes intervention methods such as herbal medicine, acupuncture, moxibustion, Tuina, and Qigong (Chan, 2005). Qigong is a low-load aerobic exercise that is effective in preventing skeletal muscle atrophy with long-term practice (Penn et al., 2019). Chinese herbs, which are pure in nature, have few toxic side effects, and are effective in treating chronic diseases, may become an important treatment to sarcopenia. TCM has gradually been recognized by the public as a supplement to Western medical treatment (Yu et al., 2006). However, no previous study has evaluated the quality of the evidence for TCM for the treatment of sarcopenia.
Moreover, the mechanism by which TCM affects sarcopenia is not yet clear, and it may be related to enhancing neural recruitment, maintaining protein homeostasis, and reducing autophagy and inflammation. Therefore, we performed a systematic review to investigate the clinical evidence of current TCM therapies to treat sarcopenia and analyze their effects.
Six electronic databases—Cochrane library, PubMed, SinoMed, Embase, Web of Science, and the China National Knowledge Infrastructure—(were screened from inception until 10 December 2021. The following Medical Subject Headings (MeSH) terms and their synonyms were used either singularly or in combination: (“Traditional Chinese exercise” OR “Qigong” OR “Tai Chi” OR “Gongfu” OR “Yi Jin Jing” OR “Ba Duan Jin”) AND (“Sarcopenia” OR “Sarcopenias”); (“acupuncture” OR “electric acupuncture”) AND (“Sarcopenia” OR “Sarcopenias”); (“Chinese herbal medicine” OR “herbal medicine” OR “herbs”) AND (“Sarcopenia” OR “Sarcopenias”). Reference lists of related reviews were searched for additional studies.
The PICOS strategy was defined as follows: “P” (patient)—patients with sarcopenia of any age, gender, or race; “I” (intervention)—TCM; “C” (comparison)—comparison with a blank group or a different intervention group; “O” (outcome)—relevant indicators to evaluate muscle and body function; and “S” (study design)—randomized controlled studies, cohort studies, observational studies, or case–control studies.
Articles were included if they met all of the following criteria: 1. participants were diagnosed with sarcopenia based on any established definition (by a working group, a certain article, or clinical experience); 2. patients’ age ≥ 60 years; 3. the study included at least one traditional Chinese medicine treatment method, which could be herbal medicine, traditional Chinese exercise, acupuncture, and their combination. 4. Outcomes included muscle mass, muscle strength, physical function, or related biochemical indicators.
The exclusion criteria were as follows: 1. no original data were included (e.g., review, protocol, and abstract); 2. the participants had other accompanying diseases (e.g., cancer, liver cirrhosis, diabetes, stroke, depressive disorder, and metabolic syndrome).
Two researchers screened the literature independently in accordance with the inclusion and exclusion criteria and used the data extraction table to extract information, such as 1. basic information (e.g., author, year of publication, number of participants and age range); 2. group design measures and measured time points; 3. main outcome results. Any disagreement between the two authors was resolved by a consensus procedure. A third author was further consulted if the disagreement persisted.
Two authors independently assessed the methodological quality of these studies using the Cochrane Risk of Bias (ROB) tool. The tool assessed the following seven characteristics: random sequence generation; allocation concealment; blinding of participants and personnel; blinding of outcome assessment; incomplete outcome data; selective reporting; and other bias. Based on the results of the risk of bias assessment of the included studies, the two authors independently assessed the quality level of the study results using GRADE software. According to the GRADE working group instructions, five factors, namely bias, inconsistency, indirectness, imprecision, and publication bias, lead to lower quality of evidence; and for each study, the quality of evidence was categorized into four levels: high, medium, low, and very low (Guyatt et al., 2008).
There was considerable heterogeneity in the included studies in terms of diagnosis of disease, sample size, outcome indicators, and interventions. We concluded that based on these heterogeneities and differences in study design, meta-analyses would not provide valid results and the risk of meta-analysis providing incorrect results was considerable. Participants’ characteristics, interventions, and the relevant results of the included studies were extracted and synthesized in a narrative way.
The selection process for this systematic review is shown in Figure 1. We used a 2-week period to identify 860 studies from the electronic database by the search strategy described above. After removing duplicate literature, 562 studies remained. After reading the titles and abstracts, 528 studies were excluded. The remaining 34 papers were read in full text. Full-text review removed 13 of these documents, leaving 21 studies that met all of the inclusion and exclusion criteria.
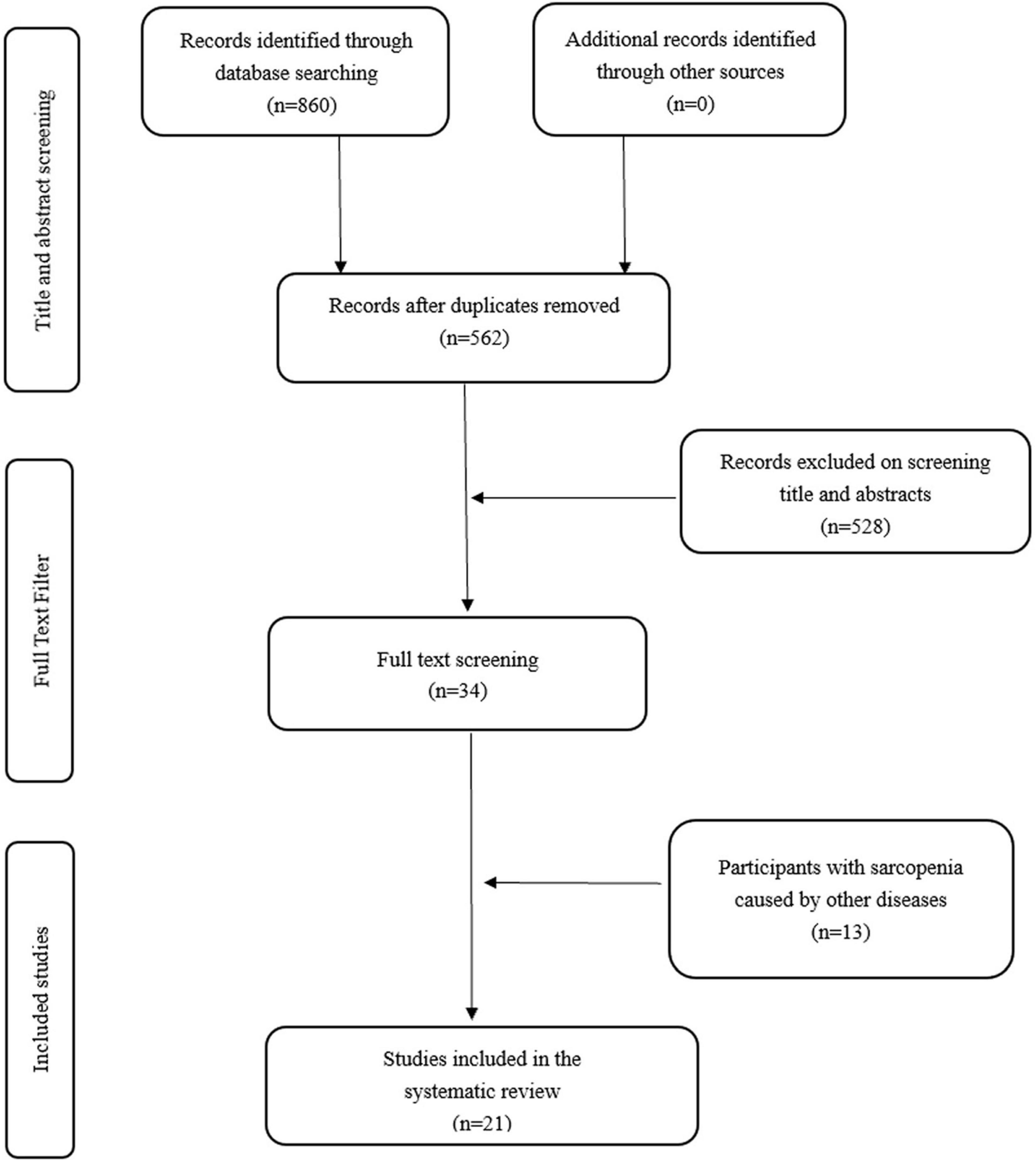
Figure 1. Flow diagram of the selection criteria for the study.
The results of data extraction are shown in Tables 1, 2. A total of 19 trials were from China, one trial was from Brazil, and one trial was from Poland. A total of 21 studies involved a total of 1,330 participants, ranging from 15 to 214 per study. The age range of the included population was between 60 and 101 years. These studies included samples with different diagnostic criteria. Namely, nine studies referred to the Asia working group for sarcopenia (Ren et al., 2016; Zhao et al., 2016; Zhu et al., 2016, 2018; Wen et al., 2018; Liang et al., 2019; Chen, 2020; Zhou et al., 2020; Chen et al., 2021); three studies used European working group for sarcopenia diagnostic criteria (Soares Mendes Damasceno et al., 2019; Fang et al., 2020; Morawin et al., 2021); six studies (Yan et al., 2007; Gong et al., 2011; Jing et al., 2011; Liu et al., 2016; Wang et al., 2016; Zhu et al., 2017) complied with Roubenoff’s view of sarcopenia (Rosenberg, 2011); two studies did not provide diagnostic criteria, but only described subjects as having been diagnosed with sarcopenia in the hospital (Yang and Chen, 2016; Liang et al., 2019); and one study used the 2011 ISCCWG (International Sarcopenia Consensus Conference Working Group) diagnostic criteria (Liu et al., 2020). There was a large difference in outcome indicators in the included studies, and there were many scales and no specific content and scoring criteria. Twenty-one studies were divided into three broad categories by intervention methods: six herbal medicine studies, two acupuncture studies, and 13 Traditional Chinese exercise studies, with interventions ranging in duration from 10 days to 10 months.
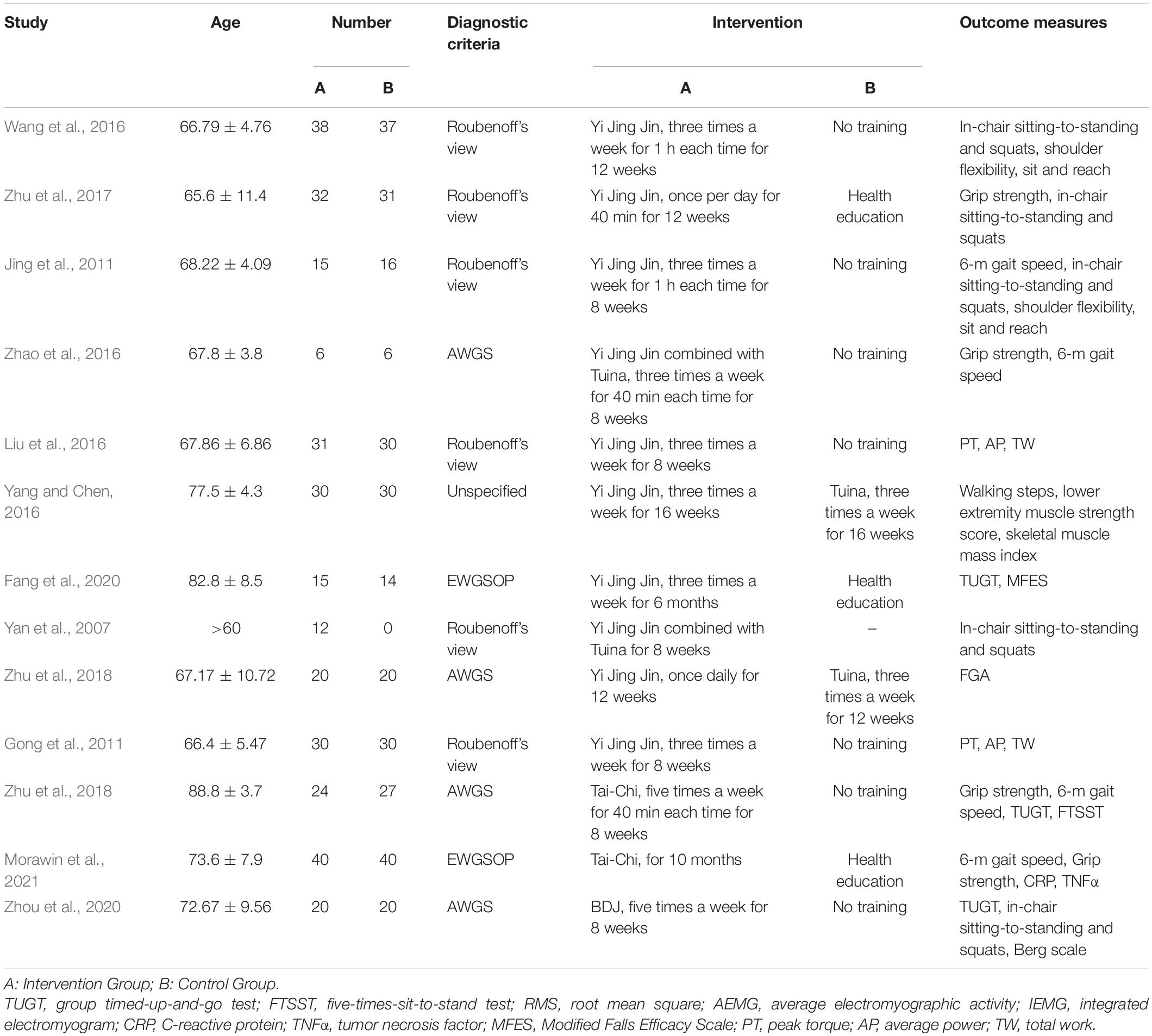
Table 1. Characteristics of the included studies of Traditional Chinese Qigong exercises.
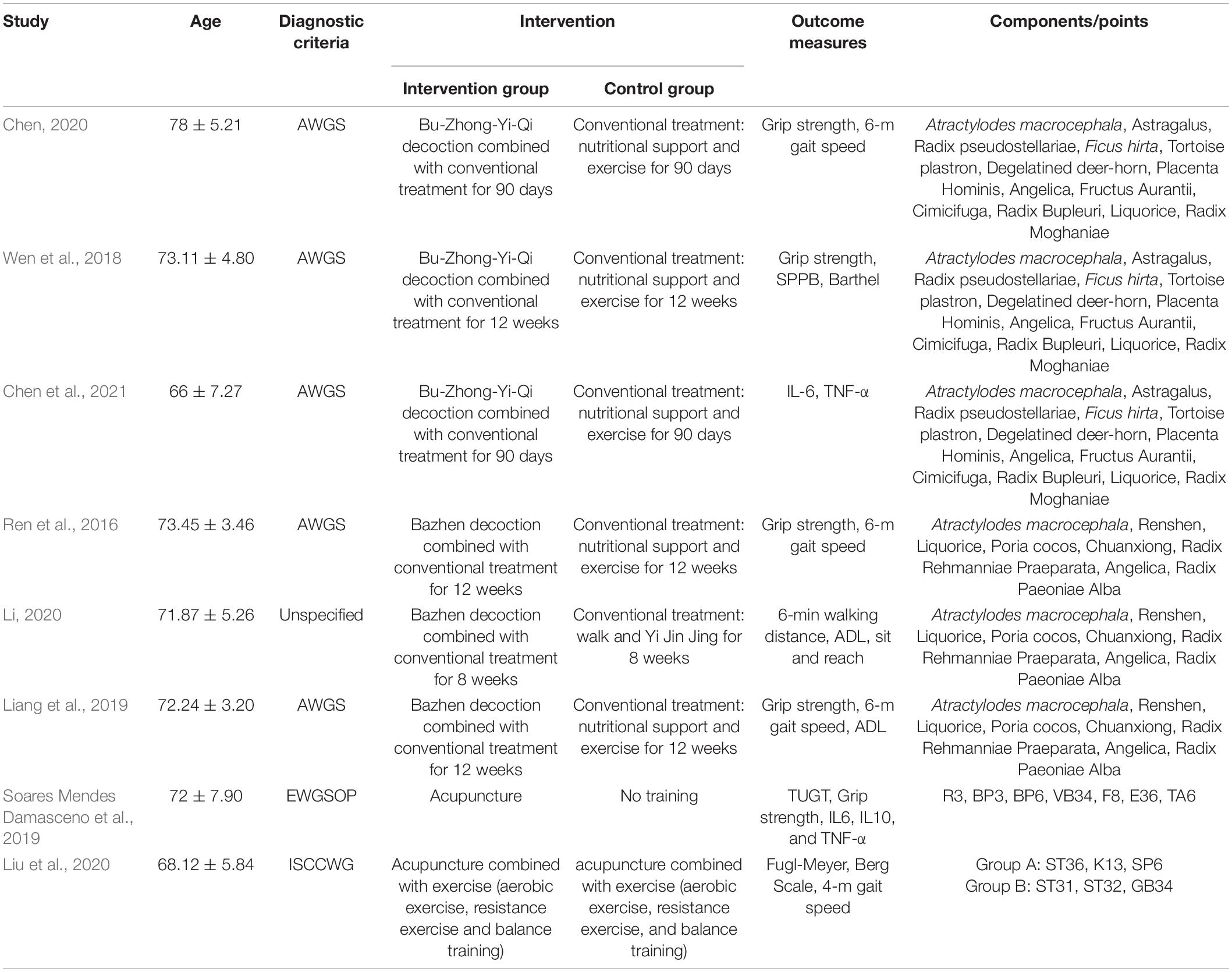
Table 2. Characteristics of the included studies of Chinese herbal medicine and acupuncture.
A total of 20 trials were randomized controlled trials, and one study was a before–after study in the same patient. There were 20 randomized controlled studies mentioned randomization, but four of these studies (Ren et al., 2016; Wang et al., 2016; Zhao et al., 2016; Chen, 2020) did not provide detailed information. Only one study (Fang et al., 2020) provided a specific method of allocation concealment, this was not reported in most of the studies. All of the studies analyzed baseline information, and comparability of the baseline characteristics between the groups was an indicator of whether randomization was actually achieved. Imperfect diagnostic criteria led to uncertain additional risks in seven studies. Only one study (Soares Mendes Damasceno et al., 2019) specifically mentioned that the trial was single-blinded, but the lack of blinding was considered a relatively low risk factor for reducing the quality of the evidence. Overall, the low risk level accounted for about 53% of all risk levels assessed, and the uncertainty was about 46%, as shown in Table 3. All of the studies had small sample sizes, with the largest sample size being 214 and the smallest sample size being 15, and the smaller sample sizes reduced statistical efficacy and limited the reliability of the results. A total of 11 studies used multiple methods of combined treatment; the main confounding factors were not clearly described; and the results were not adjusted for confounding factors. Most of the included studies were conducted in China, so the effect of ethnicity may have added to the limitations of the results. A total of nine studies reported ethical approval (Gong et al., 2011; Zhu et al., 2016; Wen et al., 2018; Liang et al., 2019; Soares Mendes Damasceno et al., 2019; Fang et al., 2020; Liu et al., 2020; Chen et al., 2021; Morawin et al., 2021). According to the GRADE working group guidelines, the favorable factors of a larger sample size, clear and direct data, and high consistency of results improve the quality grade of grip strength results. The evidence for grip strength was of moderate quality among the results generated from these studies, while the evidence for the remaining results was of low quality, as shown in Tables 4–6.
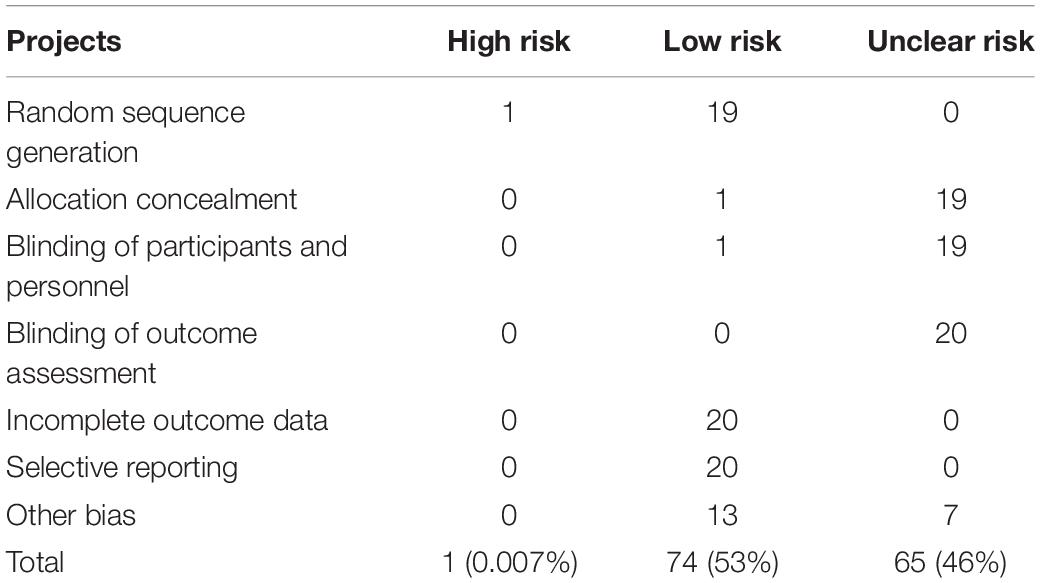
Table 3. Risk of bias evaluation for the included randomized controlled trials (RCTs).

Table 4. Muscle strength for sarcopenia.

Table 5. Physical performance for sarcopenia.
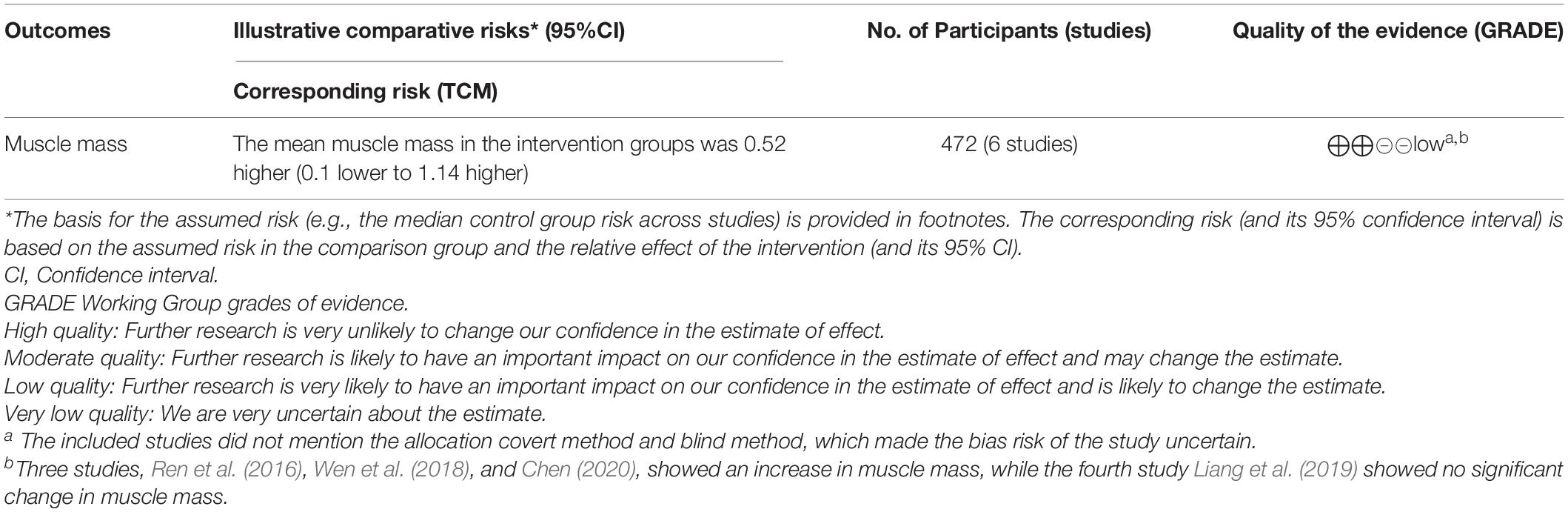
Table 6. Muscle mass for sarcopenia.
There were six studies (Ren et al., 2016; Wen et al., 2018; Liang et al., 2019; Chen, 2020; Li, 2020; Chen et al., 2021) regarding Chinese herbal medicine for treating sarcopenia conducted on the basis of routine rehabilitation (exercise and nutrition), and three studies each used Ba Zhen decoction and Bu Zhong Yi Qi decoction. To investigate the effect of herbs on muscle strength and muscle mass, four studies (Ren et al., 2016; Wen et al., 2018; Liang et al., 2019; Chen, 2020) measured grip strength and the appendicular skeletal muscle mass index (ASMI kg/m2). Physical function was assessed in a variety of ways, with four studies (Ren et al., 2016; Liang et al., 2019; Chen, 2020; Li, 2020) using walking speed, three studies (Wen et al., 2018; Liang et al., 2019; Li, 2020) using activities of daily living (ADL), and one study (Wen et al., 2018) also using the short physical performance battery (SPPB). The results of five studies (Ren et al., 2016; Wen et al., 2018; Liang et al., 2019; Chen, 2020; Li, 2020) showed a significant increase in muscle strength and physical function in the herbal group compared with the control group (p < 0.05). Meanwhile, the results of three studies (Ren et al., 2016; Wen et al., 2018; Chen, 2020) showed a significant increase in muscle mass in the herbal group compared to the control group, while one study showed (Liang et al., 2019) no significant change in muscle mass with herbal medicine. The remaining study (Chen et al., 2021) investigated the effect of Bu Zhong Yi Qi decoction on inflammatory factors in patients with sarcopenia, and after taking it, the patients had lower serum IL-6 and TNF-α levels than the control group (p < 0.05).
There were 13 studies focused on Chinese traditional exercise (TCE). Among them, ten studies (Yan et al., 2007; Gong et al., 2011; Jing et al., 2011; Liu et al., 2016; Wang et al., 2016; Yang and Chen, 2016; Zhao et al., 2016; Zhu et al., 2017, 2018; Fang et al., 2020) involved Yi Jin Jing; two studies (Zhu et al., 2016; Morawin et al., 2021) involved Tai Chi; and one study (Zhou et al., 2020) involved Ba Duan Jing (BDJ). Among the 10 studies on the use of Yi Jin Jing for sarcopenia, eight studies used Yi Jin Jing only; one study (Zhao et al., 2016) involved a combination of Tuina, Yi Jin Jing, and resistance exercise; and another study (Yan et al., 2007) used Yi Jin Jing combined with Tuina. In two of the studies (Yang and Chen, 2016; Zhu et al., 2018), the control group underwent Tuina intervention. To evaluate physical function, four studies (Jing et al., 2011; Zhao et al., 2016; Zhu et al., 2016; Morawin et al., 2021) used a 6-m walking speed test; three studies (Zhu et al., 2016; Fang et al., 2020; Zhou et al., 2020) used the Time Up and Go Test (TUGT); and three studies (Jing et al., 2011; Wang et al., 2016; Li, 2020) used sit and reach. The scales used in these studies included the Berg Balance Scale, Modified Falls Efficacy Scale (MFES), Functional Gait Assessment (FGA), Barthel Index, Five Times Sit-to-Stand Test (FTSST), Tetrax index, and EPESE Physical Assessment Scale. Ten studies showed significant improvements in physical performance after the intervention compared with their respective control groups (p < 0.05). Yang and Chen (Yang and Chen, 2016) used walking steps to assess physical performance, but no time frame was given; lower extremity muscle strength scores were used to assess muscle strength, but no specific measurements or scoring methods were given. To evaluate muscle strength, six studies (Wang et al., 2016; Zhao et al., 2016; Zhu et al., 2016, 2017; Zhou et al., 2020; Morawin et al., 2021) used grip strength; four studies (Yan et al., 2007; Jing et al., 2011; Wang et al., 2016; Zhu et al., 2017) used the number of in-chair sitting-to-standing and squats in 15 s; and two studies (Gong et al., 2011; Liu et al., 2016) used the Biodex isometric muscle strength testing system. There were 10 studies showed that after exercise, patients’ muscle strength increased significantly compared with their respective control groups (p < 0.05). To evaluate muscle mass, two studies (Zhao et al., 2016; Morawin et al., 2021) used the ASMI (kg/m2), but their findings showed no significant change in muscle mass after the intervention compared to the control group. In the Tai Chi study, one of the studies showed no improvement in grip strength in the Tai Chi group compared with the control group after 8 weeks of exercise, but there was a significant improvement in iliopsoas muscle strength (p < 0.0001).
Among the included studies, two studies were on acupuncture. In one study, acupuncture combined with exercise (aerobic exercise, resistance exercise, and balance training) and two groups of acupuncture points were compared. The results showed that patients who received acupuncture at the ST36 showed better 4-m gait speed than those in the other group (Liu et al., 2020). Another clinical study, which did not choose acupuncture at ST36 for treating sarcopenia, showed that acupuncture did not increase muscle strength and physical function (Soares Mendes Damasceno et al., 2019).
TCM may be used to delay sarcopenia by regulating the synthesis and degradation of muscle-related proteins, replenishing nutrients, promoting blood circulation, and eliminating inflammation, as shown in Figure 2.
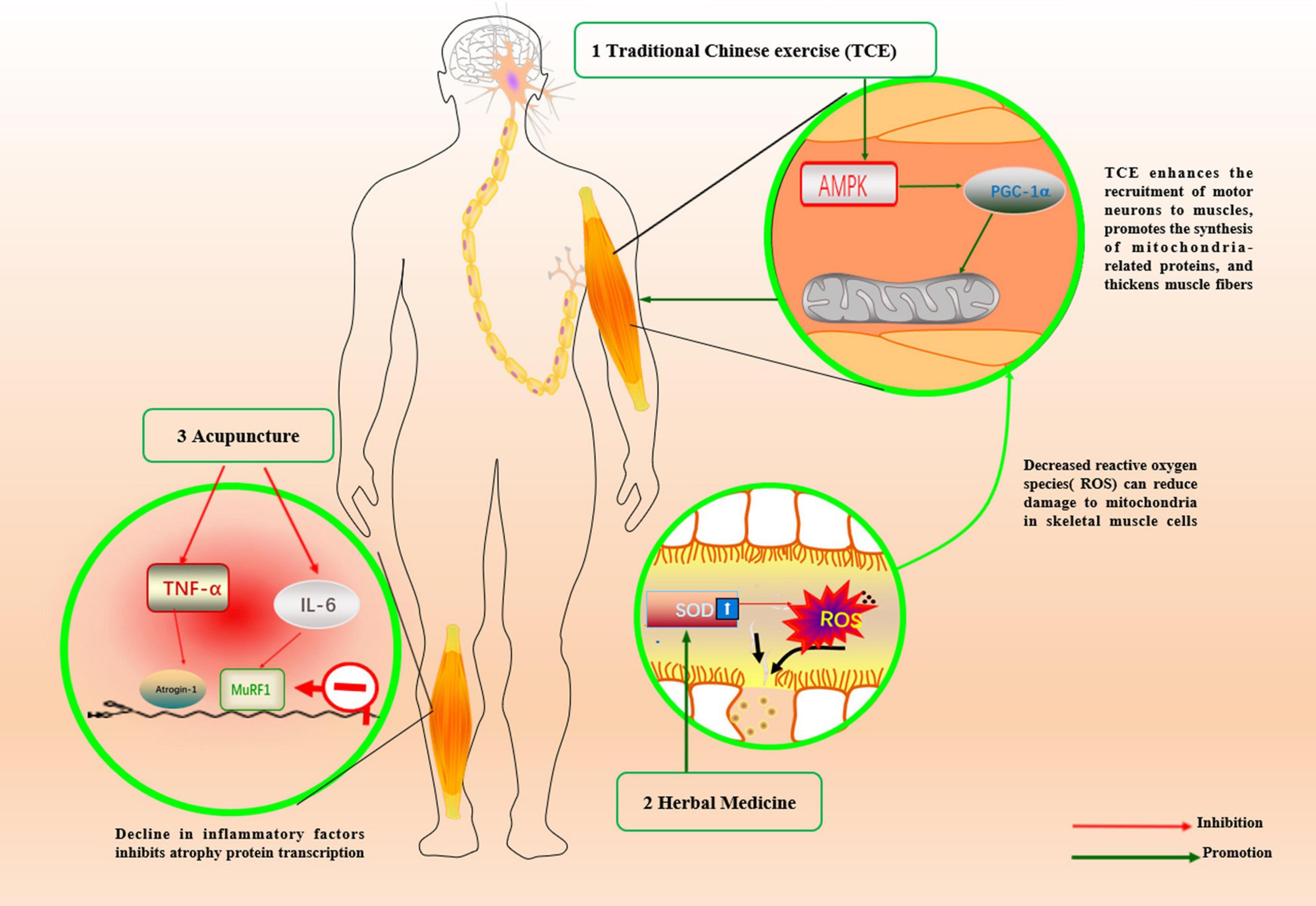
Figure 2. Mechanism of traditional Chinese medicine in the treatment of sarcopenia.
Traditional Chinese exercises have originated from traditional Chinese medicine, and include Wu Qin Xi, Yi Jin Jing, Ba Duan Jin, and Tai Chi. These are gymnastic exercise consisting of various components such as endurance, resistance, balance, flexibility, breathing, and meditation (Nascimento et al., 2019). Exercise has a positive impact on the health of older adults, but the body’s motor organs and functions decline significantly with aging; as a result, it is important to emphasize the appropriate form and intensity of exercise for older adults (Colleluori and Villareal, 2021). Yi Jin Jing is a kind of static exercise. After high-intensity interval static exercise in aging rats, the PGC-1α/FNDC5/UCP1 signaling pathway was activated, PGC-1α was upregulated, mitochondria increased, muscle fiber thickening was observed, and the skeletal muscle atrophy state was improved (Liu et al., 2021). The results of the included studies consistently show that Yi Jin Jing is an effective way to build muscle strength to prevent muscle atrophy, but there are limitations to the findings. Yi Jin Jing may be more helpful in improving lower limb strength and less effective in improving upper limb strength, considering that after practicing Yi Jin Jing, grip strength did not improve significantly, but the number of squats and in-chair sitting-to-standing within 15-s period increased significantly (Jing et al., 2011). Zhao et al. (2016) used a complex intervention that combined Tuina with Yi Jin Jing as one intervention and then combined it with another intervention, resistance exercise. The results showed that the three treatment measures group was more effective than Tuina combined with Yi Jin Jing or resistance exercise in improving muscle strength and physical function (p < 0.05). Whether the beneficial effects of the combination of two or more exercises on the body are caused by the own advantages of the different exercises or simply by the increase in the total amount of exercise cannot be determined. Moreover, the use of multiple treatments simultaneously can easily lead to poor patient compliance and reduce the credibility of the study results. In this study, only walking speed increased, and was statistically significant in the Tuina combined with Yi Jin Jing group compared to the no intervention group; however, there was a significant difference in grip strength compared to pre-intervention. There was an increase in muscle strength after using Tuina combined with Yi Jin Jing intervention, as evidenced by an increase in the number of chair stand tests performed over a 15-s period compared with the pre-treatment period (Yan et al., 2007). However, this evidence does not allow for precise conclusions that Yi Jin Jing combined with Tuina can improve muscle strength, despite significant differences in indicators before and after the intervention. Besides the lack of favorable evidence from the control group, there were other confounding factors such as the difference in the severity of the disease before and after. Yi Jin Jing was more effective than Tuina in FGA scores and total scores (Zhu et al., 2018). However, the degrees of increase in walking times and mean lower limb strength score in the massage group were significantly higher than that in the Yinjjing group (p < 0.05) in another study (Yang and Chen, 2016). Therefore, additional evidence is needed to determine whether Yi Jin Jing or Tuina is more effective.
In studies of Tai Chi for balance problems in the elderly, the diversity of its style may lead to uncertainties in its therapeutic effects. Morawin et al. (2021) used Yang-style 24-form Tai Chi after which patients had increased walking speed and decreased fat mass. Another study (Zhu et al., 2016) used a simple 8-style Taijiquan and showed significant improvements in lower extremity muscle strength and physical performance in the TC group compared to the control group, but the gender of their included population was all male making the results limited. Yang-style 24-form Tai Chi is the form most commonly used to improve balance in the elderly (Liu and Frank, 2010; Sherrington et al., 2019). However, many studies currently use simplified Tai Chi for treatment. A meta-analysis showed that traditional Tai Chi was more effective than simplified Tai Chi in preventing falls in the elderly (Li et al., 2021). However, some studies have also concluded that customized therapeutic Tai Chi is more effective than traditional Tai Chi in reducing the incidence of falls in older adults who are at a higher risk of falling (Li et al., 2018; Penn et al., 2019). During Tai Chi practice, the stability of individual gait is lower than that of normal gait (Yang and Liu, 2020). Although the low stability of gait in Tai Chi increases the risk of falls, it stimulates the body’s postural control system (Jahnke et al., 2010). To maintain balance, the body must autonomously adapt to make postural adjustments and enhance neuromuscular control so as to improve the ability to control body balance. A plantar pressure test system of the elderly after practicing Tai Chi showed that their heel impulse was greater than that of the no-intervention group, suggesting that it promoted better neuromuscular control (Li et al., 2016). This also reflects the yin and yang theory of Tai Chi, which seeks balance in the body between stability and instability. A different study demonstrated that 48 weeks of Taijiquan stability training significantly improved the stability limits of older adults, with 32, 68, and 19% increases in endpoint excursion, movement velocity, and directional control, respectively, compared with the baseline (Li, 2014).
We found only one study (Zhou et al., 2020) on the use of BDJ for sarcopenia. It may be due to the fact that BDJ does not have the same strong influence and wide dissemination as Taijiquan and Yi Jin Jing. The results from a 12-week clinical trial of sitting BDJ showed that it improved balance but not lower limb strength, possibly because sitting BDJ focused more on coordination than on muscle strengthening (Bao et al., 2020). Elderly individuals who have difficulty moving are advised to practice sitting BDJ.
According to Chinese medicine theory, Ba Zhen decoction and Bu Zhong Yi Qi decoction are commonly used Chinese herbal formulas to benefit Qi energy and strengthen the function of spleen and stomach to reduce weakness. The results of the included studies can only indicate that herbal medicine has a beneficial effect on improving muscle strength and physical function in patients based on exercise and nutritional supplementation. Bu Zhong Yi Qi decoction was able to reduce inflammatory factors in patients (Chen et al., 2021), but due to the small sample size, there was a risk of deviation. Animal studies have shown that Astragalus, which is contained in Bu Zhong Yi Qi decoction, has antioxidant and anti-aging effects. Astragalus polysaccharides, the main component of Astragalus, have been shown to significantly increase the activities of catalase (CAT), superoxide dismutase (SOD), and glutathione peroxidase (GPx), as well as anti-hydroxyl radicals in D-gal-induced aging mice (Li et al., 2012). Both Ba Zhen decoction and Bu Zhong Yi Qi decoction contain Atractylodes macrocephala and Chuanxiong. Atractylodes macrocephala can increase SOD activity, scavenge reactive oxygen radicals, and reduce malondialdehyde content in the erythrocytes of mice over 12 months of age (Li et al., 1996). In aging rats, the SOD content in the serum and rectus femoris muscle was increased by gavage of an herbal cuisine containing Atractylodes macrocephala and Astragalus, thus reducing oxidative damage and delaying the aging of skeletal muscles (Li and Liu, 2018). Chuangxiong contains tetramethylpyrazine (TMP), which can improve age-related musculoskeletal disorders in humans and prolong the lifespan (Liu et al., 2019).
The inability of acupuncture to relieve symptoms in patients with sarcopenia may be due to the selection of acupuncture points, but acupuncture may help regulate inflammatory cytokines IL-6 and TNF-α in their bodies (Soares Mendes Damasceno et al., 2019). This is because each point has a clear therapeutic effect, but it is important to combine multiple related points together for systematic acupuncture treatment depending on the condition of the disease. Liu et al. (2020) compared two different groups of acupuncture points and showed that the group with acupuncture containing the Zusanli Point (ST36) outperformed the other group in terms of walking speed. ST36 is the most frequently used acupoint in skeletal muscle-related diseases and is often used to increase muscle function and strength (Ahmedov, 2010). This may be because ST36 is located on the lateral side of the lower leg, the superficial layer is distributed with the lateral sural cutaneous nerve, and the deep layer has branches of the anterior tibial artery and vein. Acupuncture at this point can stimulate the nerve to activate the motor cortex, stimulate muscle contraction, and increase the blood flow of skeletal muscles to improve muscle strength and muscle mass of the lower limb (Noguchi et al., 1999; Ohkubo et al., 2009; Sun et al., 2019). There is a lack of clinical cases of acupuncture for sarcopenia, but there is evidence from relevant animal experiments. These studies are mostly animal models of skeletal muscle atrophy caused by other diseases, which is still different from natural aging-induced skeletal muscle atrophy. Although there are some limitations, the mechanism of sarcopenia treatment by acupuncture can be elucidated to some extent. Muscle-specific E3 ubiquitin ligases, such as atrogin-1 and MuRF1, play a key role in muscle atrophy (Egerman and Glass, 2014). Electroacupuncture in the ST36 and SP9 of rats with diabetes-induced muscular atrophy has been shown to reduce the expression of MURF-1, prevent the degradation of the myosin heavy chain, and delay the process of muscular atrophy (Chen et al., 2019). Autophagy can remove damaged proteins and provide materials for protein self-renewal to inhibit apoptosis of skeletal muscle cells. It has also been reported that electroacupuncture at ST36 and GB30 points can promote autophagy to improve gastrocnemius atrophy in rats with dystrophic muscular atrophy (Zhao et al., 2015).
This is the first systematic review of TCM for the treatment of sarcopenia. This review included clinical and preclinical studies of three major types of TCM approaches for sarcopenia—traditional Chinese Qigong exercises, acupuncture, and Chinese herbal medicine—using a reproducible search method in the available databases. Here, we highlighted the role and problems of TCM in the field of sarcopenia by summarizing and analyzing the current literature. In addition, we used the current evidence to explain the potential mechanisms. However, the available preclinical study models are not fully consistent with the pathogenesis of sarcopenia and there are mechanistic differences. The inclusion criteria for our study were strict, and we excluded studies on TCM for the treatment of secondary sarcopenia (such as metabolic disorders and cancer), thus neglecting the use of TCM for sarcopenia in these diseases. Although global diagnostic criteria for sarcopenia are now available, some earlier studies relied on expert scholarly views of sarcopenia at the time, which has led to an increased risk of uncertain bias. The limited number of eligible studies, the small amount of data, the intervention methods, and the high heterogeneity of the measurement methods prevented a meta-analysis of the existing literature. To improve the quality of evidence for future studies, there is a need for consensus on inclusion criteria for patients with sarcopenia and standardization of muscle strength, muscle function, and muscle mass testing. In the future, a large number of high-quality studies will make it possible to conduct meta-analyses of different methods such as traditional Chinese Qigong exercises, herbal medicine, and acupuncture separately, providing a higher level of evidence to determine whether TCM is effective in treating sarcopenia. Further comparative studies between several methods could be added for superiority analysis.
Traditional Chinese Qigong exercises and Chinese herbal medicine have a positive effect on physical performance and muscle strength in older adults with sarcopenia. Future high-quality multicenter RCTs with large samples are needed to determinate whether acupuncture and other therapies are effective in treating sarcopenia.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
LF conceived the review. SL, ZL, YM, and RZ searched the literature. CG was responsible for data analysis and writing of the first draft. XX, CG, and YM performed the data management and figure modification. LF and YM modified the manuscript. All authors contributed to the article and approved the submitted version.
This work was supported by the 3-year Action Plan for the Development of TCM in Shanghai-Highland construction for International Standardization of TCM [No. ZY(2021-2023)-0212].
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Ahmedov, S. (2010). Ergogenic effect of acupuncture in sport and exercise: a brief review. J. Strength. Cond. Res. 24, 1421–1427. doi: 10.1519/JSC.0b013e3181d156b1
Bao, X., Qiu, Q. X., Shao, Y. J., Quiben, M., and Liu, H. (2020). Effect of sitting ba-duan-jin exercises on balance and quality of life among older adults: a preliminary Study. Rehabil. Nurs. 45, 271–278. doi: 10.1097/rnj.0000000000000219
Chan, K. (2005). Chinese medicinal materials and their interface with Western medical concepts. J. Ethnopharmacol. 96, 1–18. doi: 10.1016/j.jep.2004.09.019
Chen, H., Ma, J., Liu, A., Cui, Y., and Ma, X. (2020). The association between sarcopenia and fracture in middle-aged and elderly people: a systematic review and meta-analysis of cohort studies. Injury 51, 804–811. doi: 10.1016/j.injury.2020.02.072
Chen, X. L., Wu, Z. H., Fan, R., Zou, Z. Q., Long, Z. Y., Yao, L., et al. (2019). [Effect of electroacupuncture on degradation of myosin heavy chain of gastrocnemius muscle in diabetes rats]. Zhen Ci Yan Jiu 44, 653–658. doi: 10.13702/j.1000-0607.180757
Chen, Y. Y. (2020). Clinical effect of Bu ZhongYi Qi Decoction on senile sarcopenia and its effect on C-reactive protein. China Pract. Med. 15, 166–168.
Chen, Y. Y., Wen, C. Y., and Jiao, Q. H. (2021). Effect of Bu Zhong Yi Qi Tang with addition and subtraction on inflammatory factors in elderly patients with sarcopenia. China Med. Pharm. 11, 13–16.
Colleluori, G., and Villareal, D. T. (2021). Aging, obesity, sarcopenia and the effect of diet and exercise intervention. Exp. Gerontol. 155:111561. doi: 10.1016/j.exger.2021.111561
Cruz-Jentoft, A. J., Bahat, G., Bauer, J., Boirie, Y., Bruyère, O., Cederholm, T., et al. (2019). Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing 48, 16–31. doi: 10.1093/ageing/afy169
Dent, E., Morley, J. E., Cruz-Jentoft, A. J., Arai, H., Kritchevsky, S. B., Guralnik, J., et al. (2018). International clinical practice guidelines for sarcopenia (ICFSR): screening, diagnosis and management. J. Nutr. Health Aging 22, 1148–1161. doi: 10.1007/s12603-018-1139-9
Egerman, M. A., and Glass, D. J. (2014). Signaling pathways controlling skeletal muscle mass. Crit. Rev. Biochem. Mol. Biol. 49, 59–68. doi: 10.3109/10409238.2013.857291
Fang, L., Li, Z. R., Tao, C. X., and Luo, J. (2020). A clinical study on the effect of Yi Jin Jing on the risk of fall in elderly patients with sarcopenia balance disorder. Chinese J. Rehabil. Med. 35, 319–323.
Gong, L., Yan, J. T., Yc, L., Fang, L., Zhang, H., Xu, J., et al. (2011). Effect of the Tui Na gongfu method Yi Jin Jing on isometric muscle strength in elderly patients with sarcopenia. Acad. J. Shanghai Univ. Trad. Chinese Med. 25, 55–58.
Guyatt, G. H., Oxman, A. D., Kunz, R., Falck-Ytter, Y., Vist, G. E., Liberati, A., et al. (2008). Going from evidence to recommendations. BMJ 336, 1049–1051. doi: 10.1136/bmj.39493.646875.ae
Jahnke, R., Larkey, L., Rogers, C., Etnier, J., and Lin, F. (2010). A comprehensive review of health benefits of qigong and tai chi. Am. J. Health Promot. 24, e1–e25. doi: 10.4278/ajhp.081013-LIT-248
Jing, D. P., Xu, J., Zhao, J. Z., Hu, Y., and Wang, D. Y. (2011). Effects of the Yi Jin Jing on the daily activity capacity and physical fitness of patients with sarcopenia. Chinese J. Inform. Tradit. Chinese Med. 18, 14–16.
Li, F. (2014). The effects of Tai Ji Quan training on limits of stability in older adults. Clin. Interv. Aging 9, 1261–1268. doi: 10.2147/CIA.S65823
Li, F., Harmer, P., Fitzgerald, K., Eckstrom, E., Akers, L., Chou, L. S., et al. (2018). Effectiveness of a therapeutic tai ji quan intervention vs a multimodal exercise intervention to prevent falls among older adults at high risk of falling: a randomized clinical trial. JAMA Intern. Med. 178, 1301–1310. doi: 10.1001/jamainternmed.2018.3915
Li, H. J., Guo, Z. X., Mao, J. J., Xiong, R. Y., and Tong, M. (1996). Effect of aqueous decoction of Baishu on the anti-aging effect in aged mice. Heilongjiang Med. Pharm. 6, 9–10.
Li, L., Chen, Y. J., Zhai, F. M., Zhang, L. L., and Zhang, Y. (2016). Study on the characteristics of plantar pressure distribution and balance ability of elderly people who have been engaged in Taijiquan exercise for a long time. Chinese J. Rehabil. Med. 31, 984–988.
Li, L., He, Y., Jin, N., Li, H., and Liu, X. (2022). Effects of protein supplementation and exercise on delaying sarcopenia in healthy older individuals in Asian and non-Asian countries: a systematic review and meta-analysis. Food Chem. X 13:100210. doi: 10.1016/j.fochx.2022.100210
Li, Q. (2020). Treatment of 41 cases of sarcopenia in the elderly with the addition of Ba Zhen Tang. Zhejiang J. Tradit. Chinese Med. 55, 33–34.
Li, W., and Liu, X. T. (2018). Effect of medicinal food intervention on the antioxidant capacity of skeletal muscle in aging rats. Chinese J. Gerontol. 38, 3985–3987. doi: 10.3945/jn.114.205583
Li, X. T., Zhang, Y. K., Kuang, H. X., Jin, F. X., Liu, D. W., Gao, M. B., et al. (2012). Mitochondrial protection and anti-aging activity of Astragalus polysaccharides and their potential mechanism. Int. J. Mol. Sci. 13, 1747–1761. doi: 10.3390/ijms13021747
Li, Z. R., Zhan, C., Guo, C. Y., Kong, L. J., Xiao, Z. W., Xue, F., et al. (2021). The optimal amount of taijiquan exercise for fall prevention in the elderly:Meta-analysis. Lishizhen Med. Materia Med. Res. 32, 504–509.
Liang, Q. Y., Wang, Z. L., Liu, R., and Diao, Y. Q. (2019). Observation on curative effect of adding and subtracting Bazhen Decoction combined with nutritional support in the treatment of sarcopenia. Chinese J. Integr. Tradit. Western Med. 39, 821–825.
Liu, B. Y., Wang, J. X., Zhang, Y., Mao, L. X., Fan, H. X., and Zhen, J. M. (2020). Wei San acupuncture combined with rehabilitation training to improve the lower limb motor function and balance and walking ability of sarcopenia. Clin. Res. 28, 136–137.
Liu, H., and Frank, A. (2010). Tai chi as a balance improvement exercise for older adults: a systematic review. J. Geriatr. Phys. Ther. 33, 103–109.
Liu, Y., Guo, C., Liu, S., Zhang, S., Mao, Y., and Fang, L. (2021). Eight weeks of high-intensity interval static strength training improves skeletal muscle atrophy and motor function in aged rats via the PGC-1α/FNDC5/UCP1 pathway. Clin. Interv. Aging 16, 811–821. doi: 10.2147/cia.s308893
Liu, Y., Weng, W., Gao, R., and Liu, Y. (2019). New insights for cellular and molecular mechanisms of aging and aging-related diseases: herbal medicine as potential therapeutic approach. Oxid. Med. Cell Longev. 2019:4598167. doi: 10.1155/2019/4598167
Liu, Y. C., Yan, J. T., Wang, Z. Y., Zhu, Q. G., Fang, M., Zhang, H., et al. (2016). Effect of Yi Jin Jing on skeletal muscle contractile function in elderly sarcopenia. Acad. J. Shanghai Univ. Tradit. Chinese Med. 30, 42–45.
Louie, G. H., and Ward, M. M. (2010). Sex disparities in self-reported physical functioning: true differences, reporting bias, or incomplete adjustment for confounding? J. Am. Geriatr. Soc. 58, 1117–1122. doi: 10.1111/j.1532-5415.2010.02858.x
Morawin, B., Tylutka, A., Chmielowiec, J., and Zembron-Lacny, A. (2021). Circulating mediators of apoptosis and inflammation in aging; physical exercise intervention. Int. J. Environ. Res. Public Health 18:3165. doi: 10.3390/ijerph18063165
Nascimento, C. M., Ingles, M., Salvador-Pascual, A., Cominetti, M. R., Gomez-Cabrera, M. C., and Viña, J. (2019). Sarcopenia, frailty and their prevention by exercise. Free Radic. Biol. Med. 132, 42–49. doi: 10.1016/j.freeradbiomed.2018.08.035
Noguchi, E., Ohsawa, H., Kobayashi, S., Shimura, M., Uchida, S., and Sato, Y. (1999). The effect of electro-acupuncture stimulation on the muscle blood flow of the hindlimb in anesthetized rats. J. Auton. Nerv. Syst. 75, 78–86. doi: 10.1016/s0165-1838(98)00144-1
Ohkubo, M., Hamaoka, T., Niwayama, M., Murase, N., Osada, T., Kime, R., et al. (2009). Local increase in trapezius muscle oxygenation during and after acupuncture. Dyn. Med. 8:2. doi: 10.1186/1476-5918-8-2
Penn, I. W., Sung, W. H., Lin, C. H., Chuang, E., Chuang, T. Y., and Lin, P. H. (2019). Effects of individualized Tai-Chi on balance and lower-limb strength in older adults. BMC Geriatr. 19:235. doi: 10.1186/s12877-019-1250-8
Ren, X. X., Yao, H., and Wang, T. (2016). Clinical observation of Bazhen Decoction combined with basic intervention in the treatment of sarcopenia. China Modern Doctor 54, 127–130.
Rosenberg, I. H. (2011). Sarcopenia: origins and clinical relevance. Clin. Geriatr. Med. 27, 337–339. doi: 10.1016/j.cger.2011.03.003
Sherrington, C., Fairhall, N. J., Wallbank, G. K., Tiedemann, A., Michaleff, Z. A., Howard, K., et al. (2019). Exercise for preventing falls in older people living in the community. Cochrane Database Syst. Rev. 1:Cd012424.
Soares Mendes Damasceno, G., Teixeira, T., de Souza, V. C., Neiva, T. S., Prudente Pereira, K., Teles Landim, M. F., et al. (2019). Acupuncture treatment in elderly people with sarcopenia: effects on the strength and inflammatory mediators. J. Aging Res. 2019:8483576. doi: 10.1155/2019/8483576
Sousa, A. S., Guerra, R. S., Fonseca, I., Pichel, F., Ferreira, S., and Amaral, T. F. (2016). Financial impact of sarcopenia on hospitalization costs. Eur. J. Clin. Nutr. 70, 1046–1051. doi: 10.1038/ejcn.2016.73
Sun, Z. G., Pi, Y. L., Zhang, J., Wang, M., Zou, J., and Wu, W. (2019). Effect of acupuncture at ST36 on motor cortical excitation and inhibition. Brain Behav. 9:e01370. doi: 10.1002/brb3.1370
Wang, B., Ma, S. R., and Hu, Y. (2016). The effect of fitness qigong Yi Jin Jing exercises on the rehabilitation effect of patients with sarcopenia. Chinese J. Gerontol. 36, 898–899.
Wen, C. Y., Chen, Y. Y., Peng, P., and Jiao, Q. H. (2018). Clinical efficacy of Bu ZhongYi Qi Decoction with addition and subtraction as an adjunct to the treatment of senile sarcopenia. Pract. Clin. J. Integr. Tradit. Chinese Western Med. 18, 72–73.
Yan, J. T., Zhang, H., Xue, J., Wu, X. Z., Cheng, J. F., and Yan, Z. (2007). “Effects of Yi Jin Jing training combined with Tuina manipulation on the motor skills of sarcopenia patients,” in Proceedings of the Ninth National Academic Conference of the Professional Committee of Sports Therapy of the Chinese Society of Rehabilitation Medicine, 2007 Xi’an, Shaanxi, 295–299.
Yang, F., and Liu, W. (2020). Biomechanical mechanism of Tai-Chi gait for preventing falls: a pilot study. J. Biomech. 105:109769. doi: 10.1016/j.jbiomech.2020.109769
Yang, J., and Chen, P. (2016). Clinical observation on the improvement of lower limb muscle strength and quality in elderly patients with sarcopenia by Tuina. Zhejiang J. Tradit. Chinese Med. 51:753.
Yu, F., Takahashi, T., Moriya, J., Kawaura, K., Yamakawa, J., Kusaka, K., et al. (2006). Traditional Chinese medicine and Kampo: a review from the distant past for the future. J. Int. Med. Res. 34, 231–239. doi: 10.1177/147323000603400301
Zhao, W., Ming, X., and Liu, J. W. (2015). The role of autophagy in the morphometric effects of electroacupuncture on myocytes in denervated muscle atrophy in rats. Med. J. Chinese Peoples Health 27:171.
Zhao, Y. J., Zhang, Y. M., Guo, Y. H., Dou, Y. L., Zhao, J., and He, Y. X. (2016). Effect of tui na combined with resistance exercise on activities of daily living in patients with sarcopenia. Chinese J. Rehabil. Med. 31, 989–994.
Zhou, S. P., Zou, Y., Sun, X. F., and Xu, Q. L. (2020). A study on the prevention of falls in elderly people with sarcopenia in Baduanjin. Sport Sci. Technol. 41, 27–58.
Zhu, G. F., Luo, K. T., Shen, Z. F., Qian, L. F., Jin, Y. Q., and Fu, Y. X. (2018). The effect of Yi Jin Jing on the balance function of sarcopenia. Zhejiang J. Tradit. Chinese Med. 53, 351–352.
Zhu, G. F., Shen, Z. F., Qing, H. S., Jin, Y. Q., and Lou, Z. Y. (2017). Effect of Yi Jin Jing (Sinew-transforming Qigong Exercises) on skeletal muscle strength in the elderly. J. Acupuncture Tuina Sci. 15, 434–439. doi: 10.1007/s11726-017-1041-8
Keywords: sarcopenia, traditional Chinese medicine, Chinese herb, Qigong exercise, acupuncture, systematic review
Citation: Guo C-y, Ma Y-j, Liu S-t, Zhu R-r, Xu X-t, Li Z-r and Fang L (2022) Traditional Chinese Medicine and Sarcopenia: A Systematic Review. Front. Aging Neurosci. 14:872233. doi: 10.3389/fnagi.2022.872233
Received: 09 February 2022; Accepted: 21 April 2022;
Published: 13 May 2022.
Edited by:
Min Hu, Guangzhou Sport University, ChinaReviewed by:
Luwen Zhu, Heilongjiang University of Chinese Medicine, ChinaCopyright © 2022 Guo, Ma, Liu, Zhu, Xu, Li and Fang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lei Fang, ZmFuZ2xlaTU4NkAxMjYuY29t
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.