 Mar Ariza1,2,3
Mar Ariza1,2,3 Neus Cano1,3
Neus Cano1,3 Bàrbara Segura1,2,4,5
Bàrbara Segura1,2,4,5 Ana Adan2,6
Ana Adan2,6 Núria Bargalló4,7,8
Núria Bargalló4,7,8 Xavier Caldú2,6,9
Xavier Caldú2,6,9 Anna Campabadal1,2,4
Anna Campabadal1,2,4 Maria Angeles Jurado2,6,9
Maria Angeles Jurado2,6,9 Maria Mataró2,6,9
Maria Mataró2,6,9 Roser Pueyo2,6,9
Roser Pueyo2,6,9 Roser Sala-Llonch2,4,10,11
Roser Sala-Llonch2,4,10,11 Cristian Barrué12
Cristian Barrué12 Javier Bejar12
Javier Bejar12 Claudio Ulises Cortés12 NAUTILUS-Project Collaborative Group
Claudio Ulises Cortés12 NAUTILUS-Project Collaborative Group Carme Junqué1,2,4,5
Carme Junqué1,2,4,5 Maite Garolera3,13*
Maite Garolera3,13*- 1Medical Psychology Unit, Department of Medicine, University of Barcelona, Barcelona, Spain
- 2Institute of Neurosciences, University of Barcelona, Barcelona, Spain
- 3Clinical Research Group for Brain, Cognition and Behavior, Consorci Sanitari de Terrassa (CST), Terrassa, Spain
- 4Institut d’Investigacions Biomèdiques August Pi i Sunyer (IDIBAPS), Barcelona, Spain
- 5Centro de Investigación Biomédica en Red sobre Enfermedades Neurodegenerativas (CIBERNED), Barcelona, Spain
- 6Department of Clinical Psychology and Psychobiology, University of Barcelona, Barcelona, Spain
- 7Diagnostic Imaging Centre, Hospital Clínic de Barcelona, University of Barcelona, Barcelona, Spain
- 8Centro de Investigación Biomédica en Red de Salud Mental (CIBERSAM), Instituto de Salud Carlos III, Barcelona, Spain
- 9Institut de Recerca Sant Joan de Déu (IRSJD), Barcelona, Spain
- 10Department of Biomedicine, University of Barcelona, Barcelona, Spain
- 11Centro de Investigación Biomédica en Red en Bioingeniería, Biomateriales y Nanomedicina (CIBER-BBN), Barcelona, Spain
- 12Department of Computer Science, Universitat Politècnica de Catalunya – BarcelonaTech, Barcelona, Spain
- 13Neuropsychology Unit, Consorci Sanitari de Terrassa (CST), Terrassa, Spain
One of the most prevalent symptoms of post-COVID condition is cognitive impairment, which results in a significant degree of disability and low quality of life. In studies with large sample sizes, attention, memory, and executive function were reported as long-term cognitive symptoms. This study aims to describe cognitive dysfunction in large post-COVID condition individuals, compare objective neuropsychological performance in those post-COVID condition individuals with and without cognitive complaints, and identify short cognitive exams that can differentiate individuals with post-COVID symptoms from controls. To address these aims, the Nautilus project was started in June 2021. During the first year, we collected 428 participants’ data, including 319 post-COVID and 109 healthy controls (18–65 years old) from those who underwent a comprehensive neuropsychological battery for cognitive assessment. Scores on tests assessing global cognition, learning and long-term memory, processing speed, language and executive functions were significantly worse in the post-COVID condition group than in healthy controls. Montreal Cognitive Assessment, digit symbol test, and phonetic verbal fluency were significant in the binomial logistic regression model and could effectively distinguish patients from controls with good overall sensitivity and accuracy. Neuropsychological test results did not differ between those with and without cognitive complaints. Our research suggests that patients with post-COVID conditions experience significant cognitive impairment and that routine tests like the Montreal Cognitive Assessment, digit symbol, and phonetic verbal fluency test might identify cognitive impairment. Thus, the administration of these tests would be helpful for all patients with post-COVID-19 symptoms, regardless of whether cognitive complaints are present or absent.
Study registration: www.ClinicalTrials.gov, identifiers NCT05307549 and NCT05307575.
Introduction
Since the World Health Organization (WHO) declared COVID-19 a pandemic in March 2020, it has been an ongoing challenge for healthcare systems worldwide. Until the development and implementation of vaccines, most efforts focused on the disease’s acute phase. With a large part of the population now vaccinated and more defined treatment strategies being made available, concerns about mortality have somewhat decreased. However, a significant number of people who have been infected have persistent symptoms, causing disability or decreased quality of life. The post-COVID-19 condition (PCC) occurs approximately 3 months from the onset, with symptoms lasting for at least 2 months, cannot be attributed to alternative diagnoses, and impact everyday functioning (Soriano et al., 2022). PCC is more common in the more severe COVID-19 forms, but it still affects patients who are not hospitalized (Chen et al., 2022). Regarding age, PCC affects both young and old persons, even though it occurs more frequently in the elderly (Daugherty et al., 2021; Cohen et al., 2022). Moreover, women are more likely than men to have PCC (Davis et al., 2021).
PCC is characterized by a wide variety of symptoms, either fixed or fluctuating. They may arise for the first time or continue from the acute phase in a milder or more severe form (Soriano et al., 2022). The most prevalent symptoms include fatigue, pain, headaches, dyspnea, changed smell and taste, cognitive impairment, and mental health issues. These symptoms most likely belong to numerous syndromes, resulting from various pathophysiological processes across the disease spectrum. Proposed mechanisms to explain the pathogenesis of PCC include organ damage in the acute infection phase, a persistent hyperinflammatory state, viral activity associated with a host viral reservoir, or an incompetent antibody response (Proal and VanElzakker, 2021). In addition to acute disease, other factors such as previous comorbidities (Cellai and O’Keefe, 2020), psychological disorders (Mazza et al., 2020), or lifestyle changes due to the pandemic (Galea et al., 2020) may explain this chronicity.
Cognitive dysfunction is one of the most reported symptoms of PCC and generates more significant disability or a decrease in quality of life. In long-COVID studies, brain fog and cognitive dysfunction are self-reported in around 70–80% of patients (Davis et al., 2021; Guo et al., 2022; Ziauddeen et al., 2022). Patients with critical forms of the disease, severe neurological manifestations, or older individuals are more likely to have long-term cognitive dysfunction, according to previous investigations involving patients who experienced acute respiratory distress syndrome from causes other than the SARS-CoV-2 virus (Hopkins et al., 2005; Denke et al., 2018). However, for unknown reasons, cognitive dysfunction also occur frequently in young people with non-severe forms of COVID-19 (Davis et al., 2021).
Initial neuropsychological evaluations supported people’s self-reported data. Attention, memory, and executive function were impaired in participants discharged from the hospital or who recently recovered from a moderate or mild case of COVID-19 (Almeria et al., 2020; Woo et al., 2020; Zhou et al., 2020; Silva et al., 2021). From an online assessment platform, nine computerized cognitive tests were employed in a prospective evaluation with a sample size of more than 84,000 participants. In tests of reasoning, problem-solving, spatial planning, and target detection, 12,689 people who suspected they had COVID-19 performed worse than those who did not report the disease. Depending on the severity of COVID-19, these cognitive deficiencies had varying degrees of impact on several tests (Hampshire et al., 2021).
Studies that focused on long-term cognitive symptoms have confirmed the initial findings with case studies or small samples. A study on 740 people conducted 7 months after the COVID-19 diagnosis using cut-off scores [defined as a Z-score ≤ 1.5 standard deviation (SD) below measure-specific age-, educational level-, and sex-adjusted norm of classical standardized tests] found impairments in all domains assessed, ranging from 10% in attention and working memory to 24% in verbal encoding (Becker et al., 2021). Another study on 66 PCC subjects selected according to cognitive complaints also found low scores across domains ranging from 15 to 52% in attention and 12 to 32% in executive functions (García-Sánchez et al., 2022). However, both these studies lacked a control group. Delgado-Alonso et al. (2022) compared the results of a paper and pencil and computerized testing of a sample of 50 people with post-COVID cognitive complaints with 50 healthy controls (HCs). They found impaired attention-concentration, episodic memory, visuospatial processing, and executive functions (Delgado-Alonso et al., 2022). Guo et al. (2022) compared 181 people with PCC and 185 HCs by using several online experimental tasks, and only found impairments in memory but not executive functions or language.
Despite existing research, more data is needed to comprehend COVID-19’s impacts on cognition. This study aims first to describe the cognitive dysfunctions in a large PCC and compare them with a HC group. Our second aim is comparing the objective performance in individuals with and without subjective cognitive complaints. We expect to find more affectation in PCC individual with cognitive complaints. Finally, we aim to detect the neuropsychological tests that better discriminate patients from controls, to be proposed as short cognitive screenings. We selected a neuropsychological battery using instruments typically utilized in clinical settings, but we also included the recognition of emotions because of its sensitivity to the orbital cortex (Adolphs, 2002). To date, no study has been published that evaluates social cognition in PCC individuals. We expect to find more affectations in emotion recognition in PCC group.
Materials and methods
Participants
The sample comprised 428 participants from the Nautilus Project (ClinicalTrials.gov IDs: NCT05307549 and NCT05307575). Three hundred and nineteen participants with PCC and 109 HCs were evaluated at the Neuropsychology and COVID-19 Units across 16 hospitals in Catalonia, Madrid, and Andorra, coordinated by the Consorci Sanitari de Terrassa (Terrassa, Barcelona, Spain). The inclusion criteria for the PCC group were as follows: (a) confirmed diagnosis of COVID-19 according to WHO criteria with signs and symptoms of the disease during the acute phase; (b) at least 12 weeks after infection; and (c) age between 18 and 65 years. The exclusion criteria were: (a) established diagnosis before COVID-19 disease of psychiatric, neurological, neurodevelopmental disorder, or systemic pathologies known to cause cognitive deficits, and (b) motor or sensory alterations that impede the neuropsychological examination. The HCs did not have COVID-19 (no positive test or compatible symptoms), and the same exclusion criteria were applicable to the PCC group. All participants were native Spanish speakers.
Procedure
The overall procedure consisted of two sessions. In the first session, various questionnaires were administered to collect information about demographic factors, previous comorbidities, and data on COVID-19. Participants provided information on their age, sex, formal education, citizenship, ethnicity, profession, and income. They were questioned about their medical history and behavior related to their health. Moreover, they were also asked about their COVID-19 experience, including their symptoms, treatment, hospitalization, and time since diagnosis. We also collected information on their post-COVID symptoms, including cognitive ones.
Each participant underwent a cognitive assessment with a comprehensive neuropsychological battery in the second session. We used the Montreal Cognitive Assessment (MoCA) as a general cognitive screening tool (Nasreddine et al., 2005; Ojeda et al., 2016). The Matrix subtest from the Wechsler Adult Intelligent Scale (WAIS) III was used to assess abstract reasoning (Wechsler, 1999). To assess verbal memory, we used the Spanish version of Rey’s Auditory Verbal Learning Test (RAVLT) (Schmidt, 1996; Alviarez-Schulze et al., 2022). Visual memory was evaluated with the 30-min delayed recall test from the Rey–Osterrieth Complex Figure Test (ROCF) (Meyers and Meyers, 1996). The copy trial of the ROCF evaluated the visuo-constructive abilities. The WAIS-III Digit Span subtest was used to measure verbal attention (digit span forward) and working memory (digit span backward) (Wechsler, 1999). Visual scanning, tracking, and motor speed were assessed by the digit symbol test from the WAIS-III (Wechsler, 1999). Parts A and B of the Trail Making Test (TMT) were administered to measure visual scanning, motor speed and attention, and mental flexibility (Reitan, 1958). The Controlled Oral Word Association Test (COWAT) (Benton and Hamsher, 1989; Peña-Casanova et al., 2009) was used to evaluate verbal fluency and language. The number of words beginning with the letters P, M, and R recalled in 1 min was recorded. Semantic fluency was evaluated using the category “animals” (Ardila et al., 2006). The number of correct animals recalled in 1 min was considered. The Stroop test consists of three subtests: words, colors, and color words that conflict with the color in which they are presented. Here, the interference score was calculated as a measure of cognitive inhibitory control (Golden, 2005). The Boston Naming Test (BNT) was used to evaluate language (Allegri et al., 1997). Emotion recognition was assessed with the Reading the Mind in the Eye Test (Fernández-Abascal et al., 2013). The Word Accentuation Test (TAP) was included as an estimate of premorbid IQ (Gomar et al., 2011). In addition to cognitive measures, we used the Chalder Fatigue Scale (CFQ) (Jackson, 2014) to assess fatigue, the Generalized Anxiety Disorder 7-item scale (GAD-7) (Spitzer et al., 2006; García-Campayo et al., 2010) to assess anxiety, and the Patient Health Questionnaire-9 (PHQ-9) (Diez-Quevedo et al., 2001; Kroenke et al., 2001) to assess depression. All evaluations were performed by trained neuropsychologists.
The recruitment was carried out between June 2021 and June 2022. The study was conducted with the approval of the Drug Research Ethics Committee (CEIm) of Consorci Sanitari de Terrassa (CEIm code: 02-20-107-070) and the Ethics Committee of the University of Barcelona (IRB00003099). All participants provided written informed consent.
Statistical analyses
Descriptive statistics were conducted for all the variables of the study. Group differences in demographics were examined by conducting two-tailed Student’s t-tests. The Fisher’s exact test assessed a comparison of binarized measures between the two groups. One-way analysis of covariance (ANCOVA) was performed to determine differences in cognitive functioning among groups, including age, sex, education, and estimated IQ as nuisance variables. Graphical representations and descriptive statistics were used to study the assumptions. The effect size was calculated using the value partial eta squared (). We used logistic regression to assess the additive contribution of neuropsychological variables in classifying the PCC and HC. We used age, years of education, and sex as covariables. Results were presented as odds ratios with 95% confidence intervals (CIs). We reported the accuracy, sensitivity, and specificity, and positive and negative predictive values. The area under the ROC curve (AUROC) was also calculated. Analyses were performed using IBM SPSS Statistics 27.0 (IBM Corporation, Armonk, NY, USA) and R Statistical Software (version 4.2.0; The R Foundation for Statistical Computing Platform). The critical level for statistical significance was set at α = 0.05. A Bonferroni adjustment was made for ANCOVA analyses such that statistical significance was accepted when p < 0.0025.
Results
Table 1 shows the socio-demographic characteristics and comorbidities of the PCC and HC groups. The PCC group had a higher proportion of women (77 vs. 62%), were older, had less formal education, and had a lower estimated IQ than the control group. Therefore, age, sex, educational level, and estimated IQ were covariates in comparing cognitive results between the two groups. Compared to the HC group, respiratory disease, high blood pressure, and obesity were more prevalent among PCC participants. On average, patients had a positive test 320 days before their neuropsychological evaluation (SD = 156.66 days, range: 84–795 days).

Table 1. Socio-demographic characteristics and comorbidities for the PCC and HC groups.
Regarding the severity of the disease, 150 (47%) PCC patients were hospitalized, of which 77 (51.3%) were admitted to the intensive care unit (ICU). The remaining 169 (53%) individuals with PCC were outpatients and had a mild illness at home. Of those, 139 (82.2%) had disturbance of activities of daily living, and 30 (17.8%) continued to carry out their activities as usual. Table 2 shows symptoms reported by participants with PCC at the time of assessment. Fatigue, pain, and headache were the most reported post-COVID general symptoms, whereas cognitive complaints, depressive, and anxiety manifestations were the most frequently reported among the neuropsychiatric symptoms.
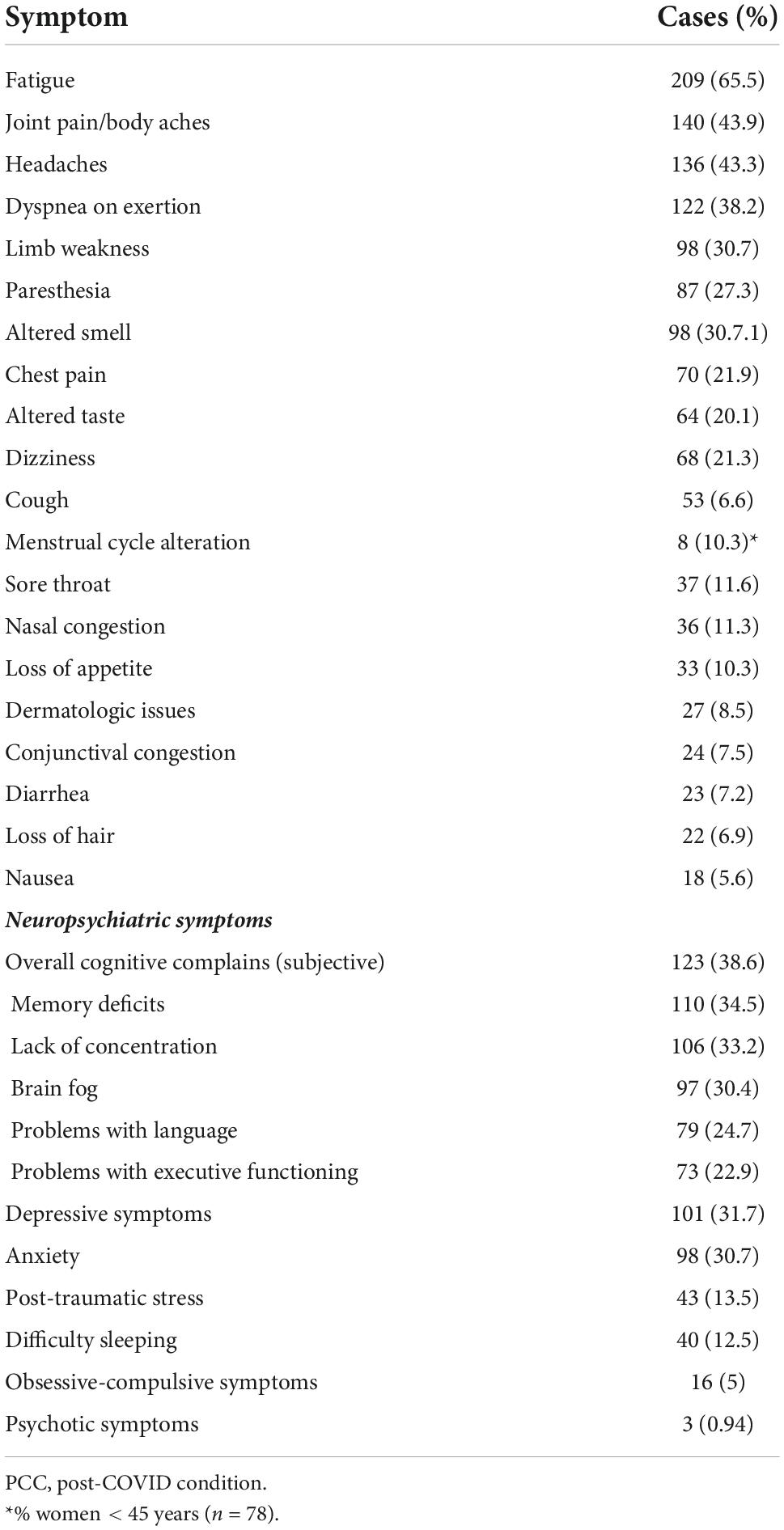
Table 2. Post-COVID-19 condition reported symptoms at the time for neuropsychological assessment (N = 319).
After adjusting for covariates and considering the Bonferroni correction for the number of comparisons (which leaves us with a significance level of p = 0.0025), there was a statistically significant poor performance of PPC group in MoCA, matrix reasoning, RAVLT sum, RAVLT delayed recall, digit symbol, Stroop words, Stroop colors, Stroop interference, phonetic fluency, and semantic fluency than in HC group (Table 3 and Figures 1, 2).
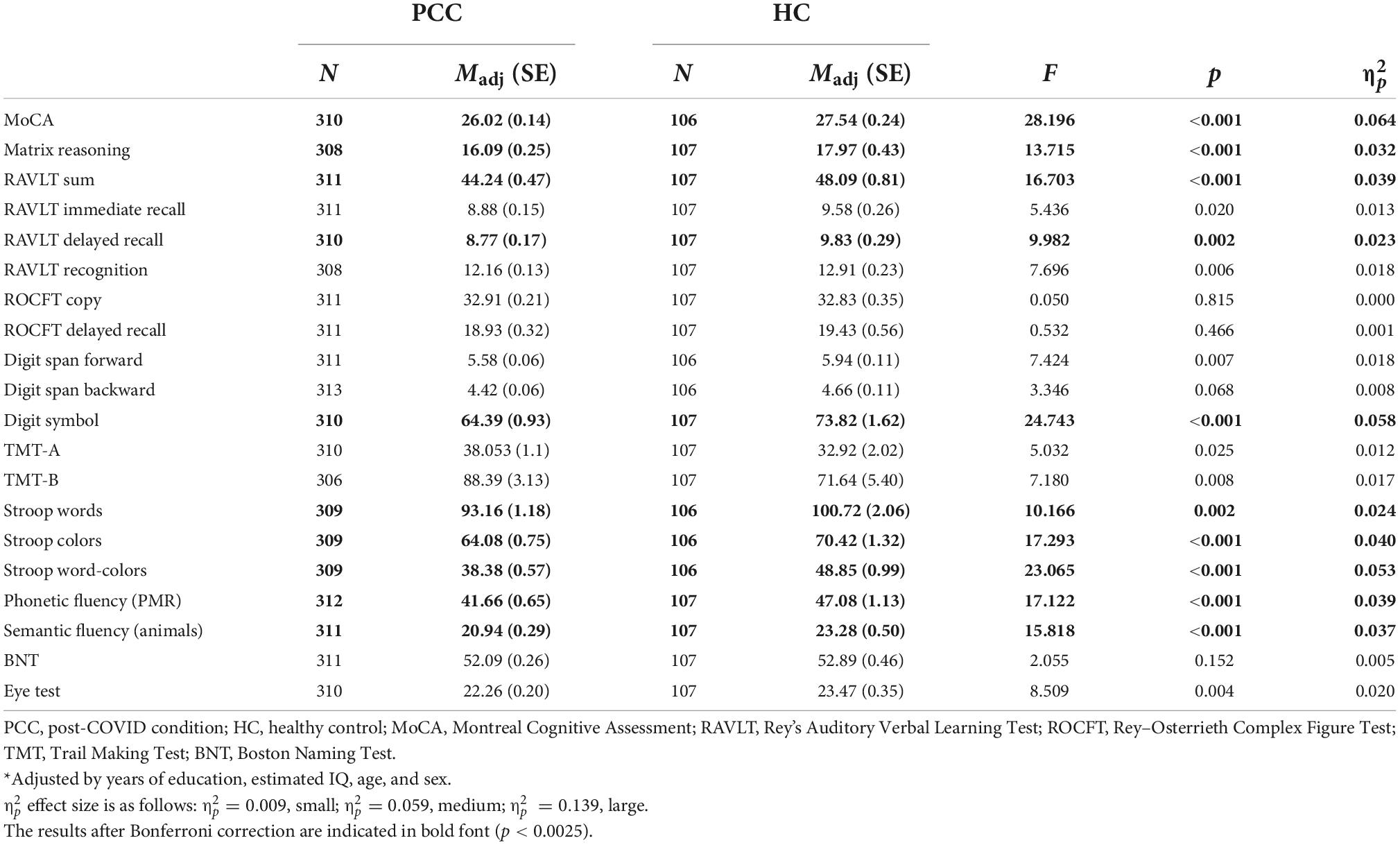
Table 3. Adjusted* means for the neuropsychological variables for PCC and HC groups.
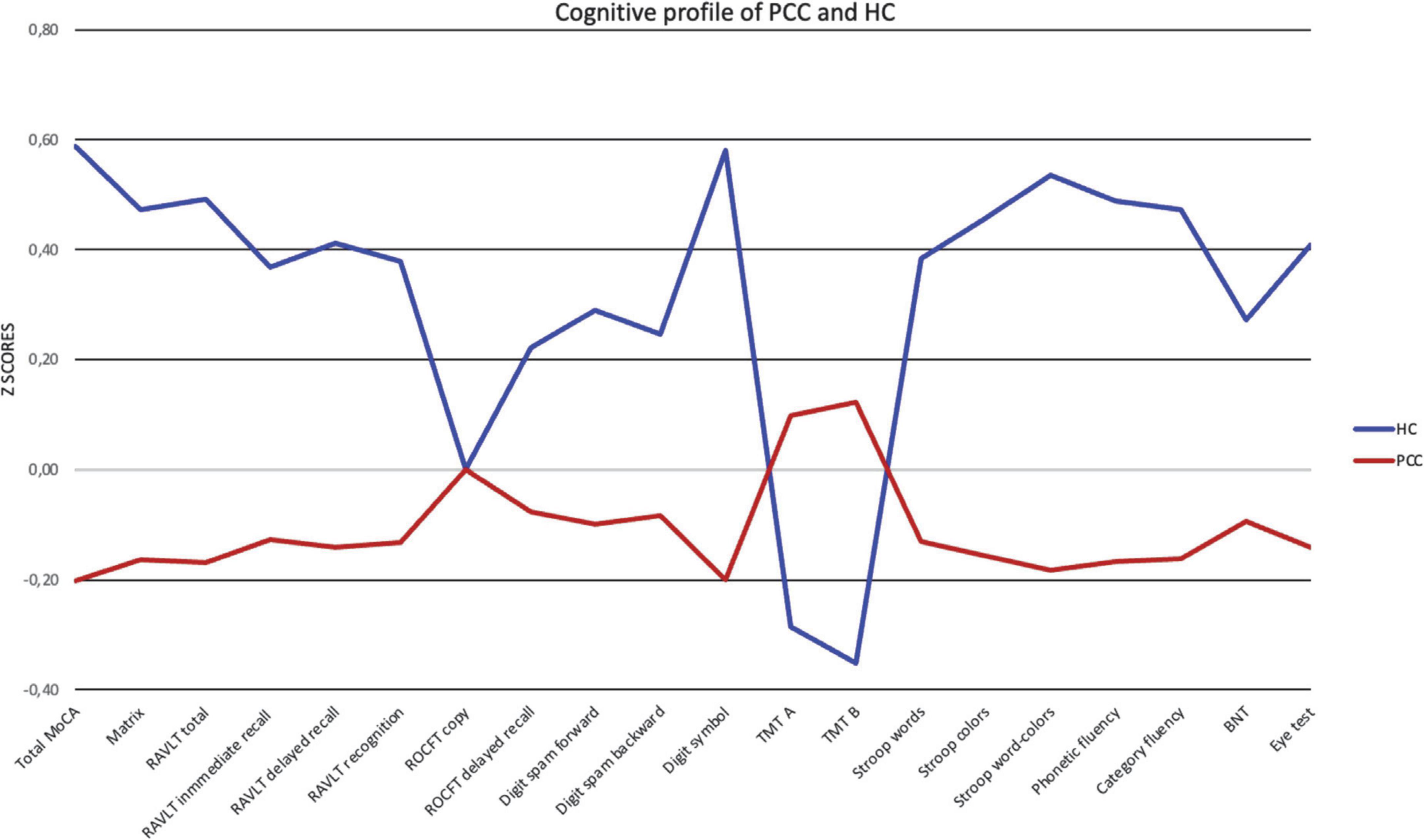
Figure 1. Cognitive profile for PCC and HC. Healthy controls (HC) in blue, PCC in red. Data are presented as Z-scores. Lower Z-scores indicate poorer performance, except for TMT (time), where lower Z-scores mean better performance.
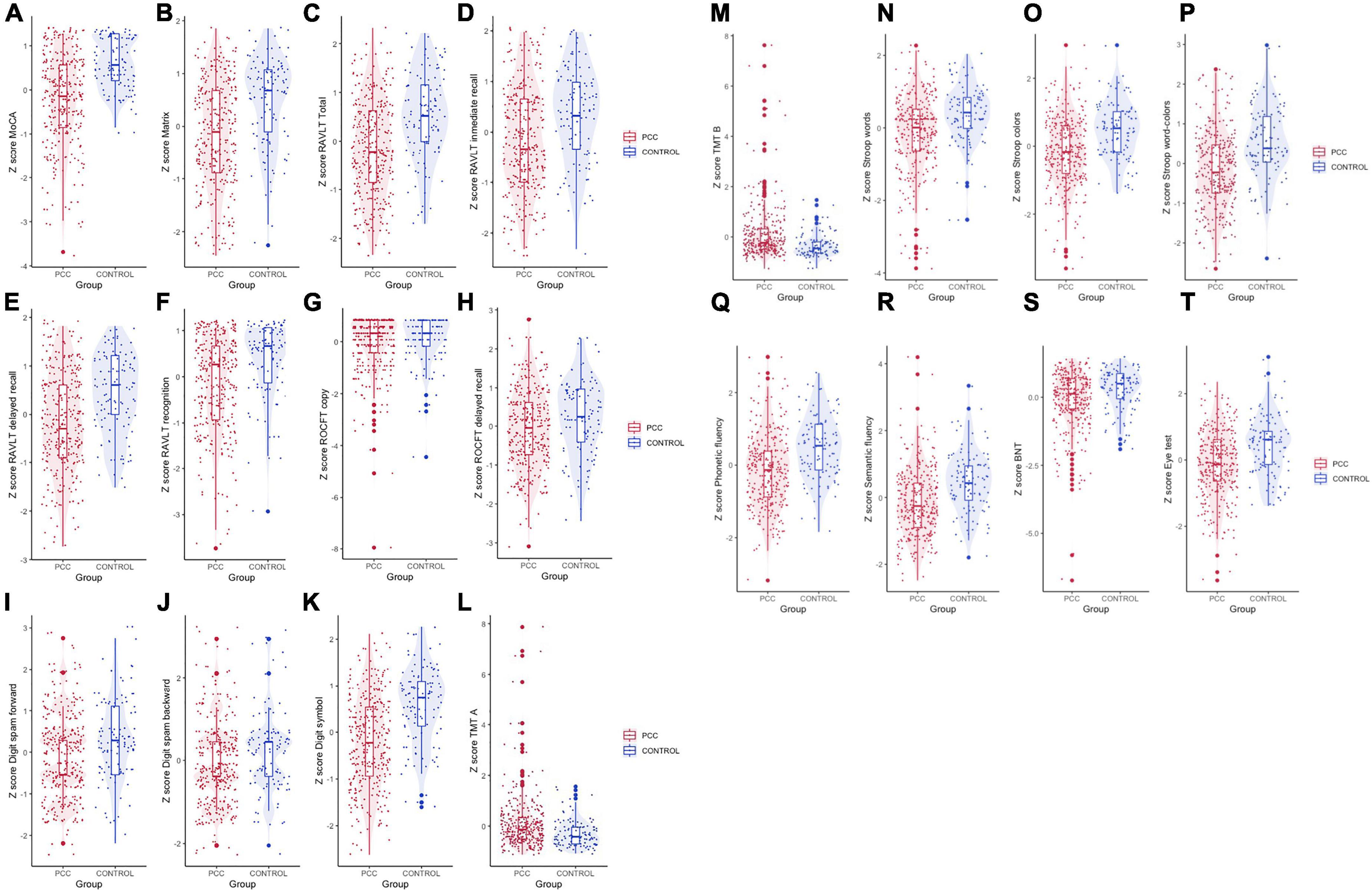
Figure 2. Violin plot for cognitive variables of PCC and HC groups. Data are presented as Z-scores. (A) MoCA, (B) matrix reasoning, (C) Rey’s Auditory Verbal Learning test (RAVLT) total (sum of 5 trials), (D) RAVLT immediate recall, (E) RAVLT delayed recall, (F) RAVLT recognition, (G) Rey–Osterrieth Complex Figure Test (ROCFT) copy, (H) ROCFT delayed recall, (I) digit spam forward, (J) digit spam backward, (K) digit symbol test (coding), (L) Trail Making Test (TMT) A, (M) TMT B; (N) Stroop test words, (O) Stroop test colors, (P) Stroop test word-colors (interference), (Q) phonetic fluency (PMR), (R) semantic fluency (animals), (S) Boston Naming Test (BNT), and (T) Reading the Mind in the Eyes test (Eye test).
The PCC group showed statistically significant higher scores of CFQ (PCC: mean = 6.21, SD = 4.33 vs. HC: mean = 1.73, SD = 3.07; t = −9.730, p < 0.001, d = 1.104), GAD-7 (PCC: mean = 6.73, SD = 5.55 vs. HC: mean = 3.18, SD = 3.12; t = −6.178, p < 0.001, d = 0.702), and PHQ-9 (PCC: mean = 9.13, SD = 6.64 vs. HC: mean = 3.08, SD = 2.79; t = 9.004, p < 0.001, d = 1.023) than those of the HC group. We reanalyzed the data by taking fatigue, anxiety, and depression scale scores as covariates. After adjusting for these variables, there was a statistically significant poor performance of the PPC group in MoCA (F = 10.120; p = 0.002; partial η2 = 0.025), RAVLT sum (F = 4.843; p = 0.028; partial η2 = 0.012), digit symbol (F = 7.448; p = 0.007; partial η2 = 0.019), Stroop word-colors (F = 5.757; p = 0.017; partial η2 = 0.015), phonetic fluency (F = 5.802; p = 0.016; partial η2 = 0.015), semantic fluency (F = 6.055; p = 0.014; partial η2 = 0.015), and Reading the Mind in the Eyes test (F = 7.576; p = 0.006; partial η2 = 0.019). However, no result remained statistically significant after Bonferroni correction (see Supplementary Table).
We focused on the neuropsychological variables that better distinguished patients and controls. We performed binomial logistic regression using the group as the outcome and the significant variables after the Bonferroni correction in the comparison between the two groups as predictors. We added demographic variables (age, years of formal education, and sex) as covariables. Linearity of the continuous variables for the logit of the dependent variable was assessed using the Box–Tidwell procedure (Box and Tidwell, 1962). A Bonferroni correction was applied using all 19 terms in the model, resulting in statistical significance being accepted when p < 0.00263 (Tabachnick and Fidell, 2014). Based on this assessment, all continuous independent variables were found to be linearly related to the logit of the dependent variable. The logistic regression model was statistically significant (χ2(3) = 87.862, p < 0.001). The link test was nonsignificant, indicating good model specification. The Hosmer–Lemeshow goodness-of-fit test was non-significant, indicating good model fit (χ2(8) = 12.639, p = 0.125). The model explained 28.0% (Nagelkerke R2) of the variance. Of the nine predictor variables, three made significant contributions to the model: total MoCA [odds ratio (OR) = 0.731], digit symbol test (OR = 0.973), and phonetic fluency (OR = 0.977) (Table 4). The model demonstrated overall classification accuracy of 74.5%, with a sensitivity of 89.9% and a specificity of 30.6%. The positive predictive value was 78.63%, and the negative predictive value was 51.56%. The AUROC 0.788 (95% CI: 0.744–0.832), which is an acceptable level of discrimination (Hosmer et al., 2013; Figure 3).

Table 4. Logistic regression classifying participants in PCC and HC groups based on significant neuropsychological results.
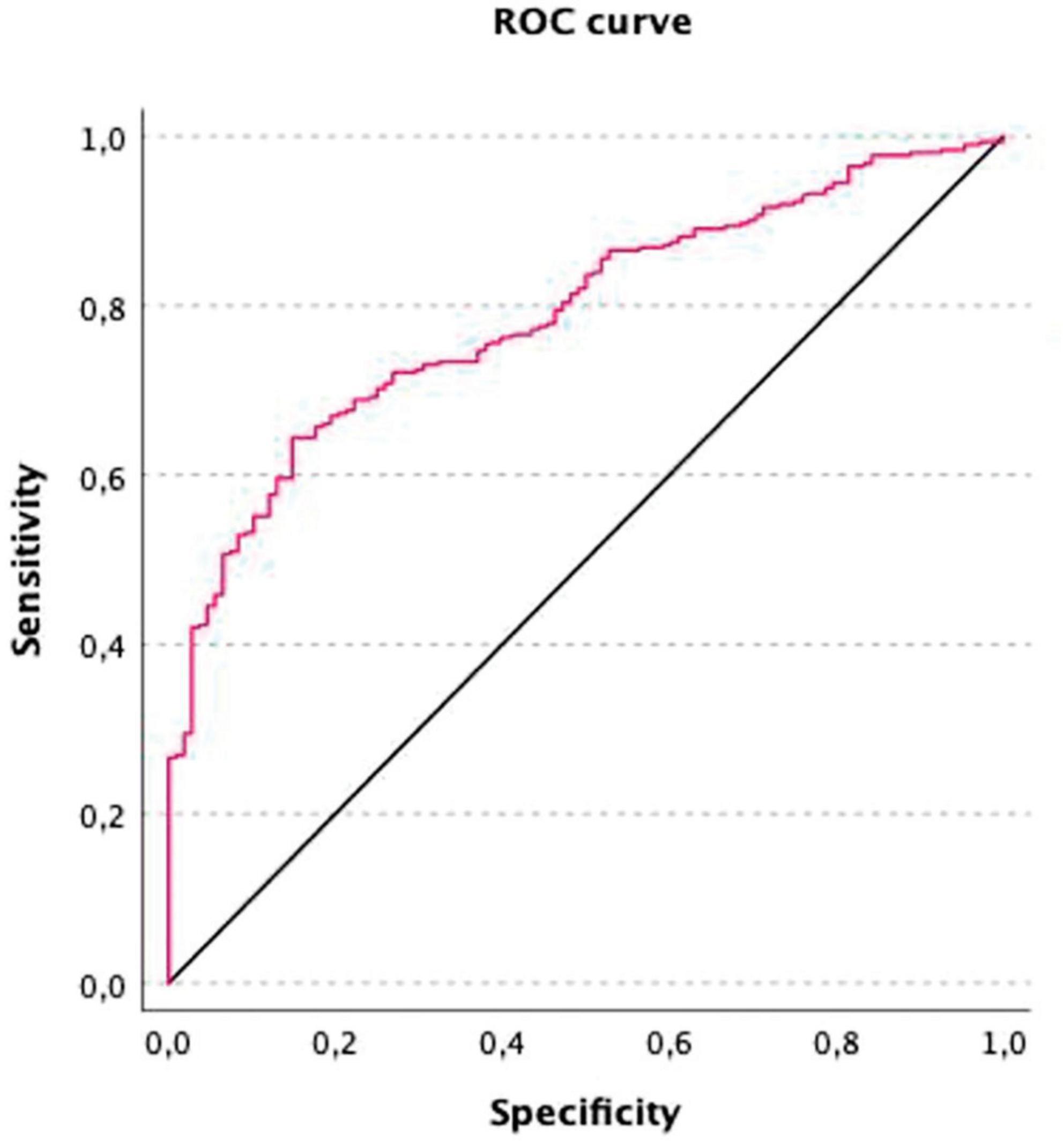
Figure 3. Receiver operating characteristic (ROC) curve for discrimination between PCC and controls based on MoCA, digit symbol, and phonetic fluency. The model’s total diagnostic accuracy is summarized by the AUROC. A value of 0 represents a completely inaccurate test, and a value of 1 represents a completely accurate test. AUC = 0.788 (95% CI: 0.744–0.832).
To evaluate whether the cognitive complaint is a determining factor in worse neuropsychological performance, we formed two groups: subjects who reported cognitive complaints (CC) (n = 123, 38.6%) and those who did not notice cognitive changes (NCC) (n = 196). The groups were similar in age (NCC: mean = 49.11, SD = 9.829 vs. CC: mean = 48.97, SD = 7.941); education (NCC: mean = 13.68, SD = 3.266 vs. CC: mean = 13.93, SD = 3.461), and estimated IQ (NCC: mean = 101.86, SD = 8.162 vs. CC: mean = 100.95, SD = 7.382), but the CC group had significantly more days since the positive test than the NCC group (CC: mean = 370, SD = 199.329, NCC: mean = 288, SD = 111.748; t = −4.193, p < 0.001, d = 0.546). Additionally, the CC group had 87 (70.7%) women compared to the 112 (57%) in the NCC group (χ2(1) = 5.947, p = 0.015). There were no differences in GAD-7 scores (NCC: mean = 6.44, SD = 5.67 vs. CC: mean = 7.20, SD = 5.35) between groups. However, the scores of the CFQ (NCC: mean = 7.94, SD = 6.39 vs. CC: mean = 11.06, SD = 6.62) and the PHQ-9 (NCC: mean = 5.37, SD = 4.37 vs. CC: mean = 7.60, SD = 9.91) were significantly higher in the CC group than in the NCC group (CFQ: t = −4.488, p < 0.001, d = 0.530; PHQ-9: t = −4.065, p < 0.001, d = 0.481). Thus, we compared the neuropsychological performance of both groups controlling for sex, days of evolution, fatigue, and depression. We did not find significant differences at the Bonferroni level in the neuropsychological variables between participants with cognitive complaints and those without.
Discussion
The present study aimed to characterize the cognitive impairment of a large sample of participants with PCC. Previous studies have shown that people who had COVID-19 performed worse than comparable healthy subjects in all cognitive domains, namely attention, executive functions, memory, and language (Becker et al., 2021; Delgado-Alonso et al., 2022; García-Sánchez et al., 2022; Guo et al., 2022; Zhao et al., 2022). Compared to the HCs, we found lower functioning of the PCC sample in tests of all domains other than attention and visuoconstructive functions.
Contrary to other authors (Becker et al., 2021; Delgado-Alonso et al., 2022; García-Sánchez et al., 2022), we did not find differences in attention between groups. Performance in TMT-A, a test in the attention domain, was not significant, although it was before the Bonferroni correction. García-Sánchez et al. (2022) highlighted the attentional deficits linked to COVID-19, but they used the CPT, a specific attention test that allow to separate between attentional accuracy and responsiveness speed, to detect a slight decrease in attentional abilities. Processing speed is a key component of attention as most attention tests are speed sensitive. Delgado-Alonso et al. (2022) found impaired attention. However, they collapsed several tests, such as Stroop, Symbol Digits Modalities Test, and reaction time tests, in addition to TMT-A and digit span forward, in the domain named attention and processing speed (Delgado-Alonso et al., 2022). Processing speed was affected also in our PCC group. Similar to us, Becker et al. (2021) measured attention with routine tests in clinical settings. They reported a 10% affectation when taking one standard deviation of the Z-score in reference to the HCs. However, this impairment was more prevalent in hospitalized patients, and therefore probably in more severe cases. A total of 24% of our PCC participants underwent critical care, which is risk factor for impairment in attention and processing speed (Hopkins et al., 1999). Neuroinflammatory reactions occur with severe systemic infection, as well as mild COVID-19 infections. A pattern of activated white matter microglia similar to that associated with the chemo-brain has been identified in individuals with SARS-CoV-2 infection (Fernández-Castañeda et al., 2022). PPC patients’ mental processing speed likely stems from impairments in complex brain networks rather than specific dysfunctions. The evidence points to an attentional deficit in PCC patients, but the poor results in several tests potentially reflect processing speed issues.
Regarding the memory domain, we found an obvious impairment of verbal learning similar to other authors (Becker et al., 2021; Delgado-Alonso et al., 2022), but we did not find impaired visuoconstructive functions and visual memory. Chronic inflammation has been linked to neuronal impairment, especially in the hippocampus (Belarbi and Rosi, 2013). It has been suggested that patients with PCC could suffer from a chronic inflammatory condition (Maamar et al., 2022). This could explain these memory problems, especially in those who have had milder forms of COVID-19. In addition, affectations in the hippocampus have been related to memory loss at 3 months post-COVID (Lu et al., 2020).
We found that the performance of the Reading the Mind in the Eyes test also differed between PCCs and controls. However, Bonferroni’s corrections were applied, and the differences did not reach the criteria for significance. To date, no studies have been published that evaluate social cognition in PCC individuals even though impaired social cognition can result in difficulties with social communication (Henry et al., 2006). Surprisingly, the Eye test did not correlate with depression and anxiety scores in our PCC participants. Social cognition is affected in depressed individuals (Nejati et al., 2012; Weightman et al., 2014). It has been proposed that the association between decreased social cognition and psychosocial issues in depressed individuals may be mediated by executive functions (Knight and Baune, 2019). The affectation of emotion recognition found in our sample could be explained by the reduction in gray matter in the orbito-frontal cortex seen in a large-sample of the COVID-19 re-imaging study (Douaud et al., 2022).
The neuropsychological profile observed in our data, which is consistent with the mild executive dysfunction syndrome reported by Bertuccelli et al. (2022) in a recent meta-analysis, indicates that individuals infected with COVID-19 are likely to develop neurodegeneration and dementia in the future. Periodical neuropsychological follow-up of PCC individuals is recommended to control the progression of cognitive deficits. We are unsure whether they will continue, resolve, or worsen. This monitoring will also enable us to ensure that the tests used to identify these deficiencies are the best ones available. In any case, the focus of clinical and research professionals should always be on creating interventions for cognitive stimulation.
Interestingly, our results are significant after removing the effect of many variables and performing the Bonferroni correction for multiple comparisons. Group differences were small-to-medium, as indicated by effect size calculations. Low effect size has also been reported by other authors (Delgado-Alonso et al., 2022; García-Sánchez et al., 2022). However, our results might have clinical relevance despite the small or medium effect size. It is a relatively young sample (<65 years of age) with cognitive impairments, which may affect the functionality. In our sample, we do not use objective measures to evaluate the functionality. However, 39.5% of PCC subjects had employment status changes, compared to 8.3% of HCs. Further investigation that additionally examines the mental health, quality of life, and functionality of PCC patients is needed.
Several studies have revealed that subjects with PCC present high levels of fatigue, depression, and anxiety (Fernández-de-Las-Peñas et al., 2021; Mattioli et al., 2021), which are correlated with cognitive deficits (Mattioli et al., 2021; Delgado-Alonso et al., 2022; García-Sánchez et al., 2022; Whiteside et al., 2022). Our results are consistent with those of previous reports. Fatigue, depression, and anxiety explain part of our sample’s variance in cognitive performance, as evidenced by the reduction of cognitive differences between the PCC and HC groups after controlling for these factors. In PCC patients, depression, anxiety, and executive dysfunction have been found to predict fatigue (Calabria et al., 2022). However, it is unknown how depression and cognitive impairment are related causally. Depression plays a role in poor cognitive function. However, it cannot be ruled out that post-COVID symptoms such as cognitive deficits may cause depression. It is also possible that the same illness process causes cognitive impairment and depression, but more research is required to draw exact conclusions about the connection between depression and cognitive deficits.
We found that the neuropsychological tests that best discriminate between PCC and HCs are the MoCA, digit symbol test, and phonetic fluency. The model obtained differentiates acceptably well, has good sensitivity, and correctly identifies PCCs. Two of the tests showing discrimination power are usual screening tools for mild cognitive impairment (MCI) (Nasreddine et al., 2005; González-Blanch et al., 2011). According to a recent meta-analysis, MoCA has already demonstrated its efficacy in detecting cognitive impairments associated with COVID-19 in the first 6 months (Crivelli et al., 2022). Our results reveal that the sensitivity of MoCA to detect cognitive impairment extends well beyond the first 6 months. Digit symbols are a susceptible test for brain damage. This task has not been related to brain structure or function, rather its deficient performance has been linked to various biological or functional pathologies (Lezak et al., 2012). On the other hand, verbal fluency, both phonetic and semantic, has also been shown to discriminate between people with MCI and healthy people, particularly semantic fluency (McDonnell et al., 2020). Semantic fluency does not appear in our model, but phonetic fluency does. It seems that performance in phonetic fluency tests is more sensitive in discriminating between people with PCC and healthy people. Distinct brain structures are involved in these language processing components: word retrieval in semantic fluency depends on semantic associations and each association’s meaning, whereas phonetic fluency involves uncommonly used procedures requiring more effort (Bayles et al., 1989).
Contrary to what we expected, we found no differences in the neuropsychological performance between participants who presented a cognitive complaint and those who did not. According to Calabria et al. (2022), our scores on depression and fatigue were higher in the cognitive-complaint subjects than in those without it. However, patients with cognitive complaints were not cognitively poorer than patients without them, and their increased complaining may have been due to their high levels of depression and fatigue. Our data suggest that anyone with PCC may have cognitive impairment influencing their functionality and quality of life, even if they do not complain. In fact, Zhao et al. (2022) found poor performance on sustained attention tasks up to 9 months after infection in a sample of people who did not seek post-COVID care. Cognitive function screening should be protocolized in the evaluation of people with PPC, even without cognitive complaints.
When interpreting the results, it is essential to consider the limitations and strengths of the current study. Our control group is not optimal, because we had to control some variables statistically. We aimed to match the PCC sample by age, sex, and education. Enrolling people who have not had the disease proved increasingly difficult. Although we could have used old samples from other studies, we wanted to control for the “pandemic” effect (i.e., lockdowns and stress) so that the control group experienced the same environmental circumstances, with the only difference being that they did not experience the infection. Another limitation refers to the choice of instrument to assess visuoconstructive skills and verbal memory. We used the ROCF test, which was normal for both the copying and memory parts. However, tests used by other authors are better suited to measure visual memory and it is possible that our test has not been adequate enough to assess visual memory impairment in COVID-19 patients. We did not investigate associations between cognitive status and biomarkers of clinical severity (i.e., ferritin or CRP). To understand the pathogenesis of cognitive dysfunction in COVID-19 patients, future studies with bigger samples are required to assess these characteristics.
However, our sample size is reasonably large, representing the full spectrum of severity of COVID-19. Moreover, the sample includes both individuals with and without cognitive complaints. This allows the results to be extrapolated to the entire PCC population. In addition, the selection of the sample has been made by ruling out comorbidities that could cause cognitive impairment, which means that we have a clean sample.
Conclusion
To conclude, despite the methodological limitations, the results of our study, with a large, representative sample of individuals with PCC and a large HC group, show that people with PCC present significant impairments in global cognition, learning and long-term memory, processing speed, language, and executive functions. Even though it has been almost a year since the COVID positive test, these impairments are still observed. We also provide evidence that cognitive deficits can affect anyone with PCC, regardless of whether they experience cognitive complaints. Further, we believe that all patients with post-COVID-19 symptoms would benefit from the routine use of three assessing tools such as MoCA, digit symbol, and verbal fluency test to rule out cognitive impairment. These tests are currently utilized in research and clinical settings. They are simple to conduct and accurate, making them popular among healthcare professionals and patients alike. Healthcare professionals will find our results to be clinically helpful when evaluating cognition in PCC.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by the Drug Research Ethics Committee (CEIm) of Consorci Sanitari de Terrassa, Terrassa, Barcelona, Spain (CEIm code: 02-20-107-070) Ethics Committee of the University of Barcelona (IRB00003099). The patients/participants provided their written informed consent to participate in this study.
Members of the NAUTILUS-Project Collaborative Group
Vanesa Arauzo and Jose A. Bernia, Consorci Sanitari de Terrassa (CST), Terrassa, Spain.
Marta Balague-Marmaña and Berta Valles-Pauls, Hospital Sant Joan Despí Moisès Broggi, Consorci Sanitari Integral.
Jesús Caballero, Hospital Universitari Arnau de Vilanova, Lleida, Spain.
Anna Carnes-Vendrell and Gerard Piñol-Ripoll, Hospital Universitari de Santa Maria, Lleida, Spain.
Ester Gonzalez-Aguado and Carme Tayó-Juli, Consorci Sanitari Alt Penedès-Garraf, Vilafranca de Penedés, Barcelona, Spain.
Eva Forcadell-Ferreres and Silvia Reverte-Vilarroya, Hospital Verge de la Cinta, Tortosa, Tarragona, Spain.
Susanna Forné, Fundació Sant Hospital de la Seu d’Urgell, La Seu d’Urgell, Lleida, Spain.
Anna Bartes-Plan and Jordina Muñoz-Padros, Consorci Hospitalari de Vic, Vic, Barcelona, Spain.
Jose A. Muñoz-Moreno and Anna Prats-Paris, Servei de Malalties Infeccioses, Fundació Lluita contra les Infeccions – Hospital Universitari Germans Trias i Pujol, Badalona, Barcelona, Spain.
Inmaculada Rico and Nuria Sabé, Hospital Universitari de Bellvitge, L’Hospitalet de Llobregat, Barcelona, Spain.
Marta Almeria and Laura Casas, Hospital Universitari Mútua Terrassa, Terrassa, Barcelona, Spain.
Maria José Ciudad and Anna Ferré, Badalona Serveis Assistencials, Badalona, Barcelona, Spain.
Tamar Garzon and Manuela Lozano, Institut d’Assistència Sanitària, Girona, Spain.
Marta Cullell and Sonia Vega, Fundació Salut Empordà, Figueres, Girona, Spain.
Sílvia Alsina, Fundació Hospital de Puigcerdà, Puigcerdà, Girona, Spain.
Maria J. Maldonado-Belmonte and Susana Vazquez-Rivera, Hospital Universitario Central de la Cruz Roja San José y Santa Adela, Madrid, Spain.
Eva Baillès and Sandra Navarro, Servei Andorrà d’Atenció Sanitària (SAAS), Andorra.
Author contributions
MA, MG, CJ, and BS designed the study. NC and NAUTILUS-Project Collaborative Group collected the data. MA performed the statistical analyses and wrote the first version of the manuscript. CJ revised the manuscript critically for important intellectual content. All authors revised the manuscript drafts and approved the final manuscript.
Funding
This research was supported by the Agency for Management of University and Research Grants (AGAUR) from the Generalitat de Catalunya (Pandemies, 202PANDE00053) and La Marató de TV3 Foundation (202111-30-31-32).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnagi.2022.1029842/full#supplementary-material
References
Adolphs, R. (2002). Neural systems for recognizing emotion. Curr. Opin. Neurobiol. 12, 169–177. doi: 10.1016/S0959-4388(02)00301-X
Allegri, R. F., Mangone, C. A., Villavicencio, A. F., Rymberg, S., Taragano, F. E., and Baumann, D. (1997). Spanish boston naming test norms. Clin. Neuropsychol. 11, 416–420. doi: 10.1080/13854049708400471
Almeria, M., Cejudo, J. C., Sotoca, J., Deus, J., and Krupinski, J. (2020). Cognitive profile following COVID-19 infection: clinical predictors leading to neuropsychological impairment. Brain Behav. Immun. Health 9:100163. doi: 10.1016/J.BBIH.2020.100163
Alviarez-Schulze, V., Cattaneo, G., Pachón-García, C., Solana-Sánchez, J., Tormos, J. M., Pascual-Leone, A., et al. (2022). Validation and normative data of the spanish version of the rey auditory verbal learning test and associated long-term forgetting measures in middle-aged adults. Front. Aging Neurosci. 14:809019. doi: 10.3389/fnagi.2022.809019
Ardila, A., Ostrosky-Solís, F., and Bernal, B. (2006). Cognitive testing toward the future: the example of semantic verbal fluency (ANIMALS). Int. J. Psychol. 41, 324–332. doi: 10.1080/00207590500345542
Bayles, K. A., Tomoeda, C. K., Caffrey, J. T., Kaszniak, A. W., Salmon, D. P., Jacobs, D., et al. (1989). Semantic and letter category naming in Alzheimer’s patients: a predictable difference. Dev. Neuropsychol. 5, 335–347. doi: 10.1080/87565648909540443
Becker, J. H., Lin, J. J., Doernberg, M., Stone, K., Navis, A., Festa, J. R., et al. (2021). Assessment of cognitive function in patients after COVID-19 infection. JAMA Netw. Open 4:e2130645. doi: 10.1001/JAMANETWORKOPEN.2021.30645
Belarbi, K., and Rosi, S. (2013). Modulation of adult-born neurons in the inflamed hippocampus. Front. Cell Neurosci. 7:145. doi: 10.3389/FNCEL.2013.00145
Bertuccelli, M., Ciringione, L., Rubega, M., Bisiacchi, P., Masiero, S., and Del Felice, A. (2022). Cognitive impairment in people with previous COVID-19 infection: A scoping review. Cortex 154, 212–230. doi: 10.1016/j.cortex.2022.06.002
Box, G. E. P., and Tidwell, P. W. (1962). Transformation of the independent variables. Technometrics 4, 531–550. doi: 10.1080/00401706.1962.10490038
Calabria, M., García-Sánchez, C., Grunden, N., Pons, C., Arroyo, J. A., Gómez-Anson, B., et al. (2022). Post-COVID-19 fatigue: the contribution of cognitive and neuropsychiatric symptoms. J. Neurol. 269, 3990–3999. doi: 10.1007/s00415-022-11141-11148
Cellai, M., and O’Keefe, J. B. (2020). Characterization of prolonged COVID-19 symptoms in an outpatient telemedicine clinic. Open Forum Infect. Dis. 7, 1–4. doi: 10.1093/ofid/ofaa420
Chen, C., Haupert, S. R., Zimmermann, L., Shi, X., Fritsche, L. G., and Mukherjee, B. (2022). Global prevalence of post COVID-19 condition or long COVID: a meta-analysis and systematic review. J. Infect. Dis. Online ahead of print. doi: 10.1093/INFDIS/JIAC136
Cohen, K., Ren, S., Heath, K., Dasmariñas, M. C., Jubilo, K. G., Guo, Y., et al. (2022). Risk of persistent and new clinical sequelae among adults aged 65 years and older during the post-acute phase of SARS-CoV-2 infection: retrospective cohort study. BMJ 376:e068414. doi: 10.1136/BMJ-2021-068414
Crivelli, L., Palmer, K., Calandri, I., Guekht, A., Beghi, E., Carroll, W., et al. (2022). Changes in cognitive functioning after COVID-19: a systematic review and meta-analysis. Alzheimers Dement. 18:1047. doi: 10.1002/ALZ.12644
Daugherty, S. E., Guo, Y., Heath, K., Dasmariñas, M. C., Jubilo, K. G., Samranvedhya, J., et al. (2021). Risk of clinical sequelae after the acute phase of SARS-CoV-2 infection: retrospective cohort study. BMJ 373:n1098. doi: 10.1136/BMJ.N1098
Davis, H. E., Assaf, G. S., McCorkell, L., Wei, H., Low, R. J., Re’em, Y., et al. (2021). Characterizing long COVID in an international cohort: 7 months of symptoms and their impact. EClinicalMedicine 38:101019. doi: 10.1016/j.eclinm.2021.101019
Delgado-Alonso, C., Valles-Salgado, M., Delgado-Álvarez, A., Yus, M., Gómez-Ruiz, N., Jorquera, M., et al. (2022). Cognitive dysfunction associated with COVID-19: a comprehensive neuropsychological study. J. Psych. Res. 150, 40–46. doi: 10.1016/j.jpsychires.2022.03.033
Denke, C., Balzer, F., Menk, M., Szur, S., Brosinsky, G., Tafelski, S., et al. (2018). Long-term sequelae of acute respiratory distress syndrome caused by severe community-acquired pneumonia: delirium-associated cognitive impairment and post-traumatic stress disorder. J. Int. Med. Res. 46, 2265–2283. doi: 10.1177/0300060518762040
Diez-Quevedo, C., Rangil, T., Sanchez-Planell, L., Kroenke, K., and Spitzer, R. L. (2001). Validation and utility of the patient health questionnaire in diagnosing mental disorders in 1003 general hospital Spanish inpatients. Psychosom. Med. 63, 679–686. doi: 10.1097/00006842-200107000-00021
Douaud, G., Lee, S., Alfaro-Almagro, F., Arthofer, C., Wang, C., Lange, F., et al. (2022). Brain imaging before and after COVID-19 in UK Biobank. Nature 604, 697–707. doi: 10.1038/s41586-022-04569-4565
Fernández-Abascal, E. G., Cabello, R., Fernández-Berrocal, P., and Baron-Cohen, S. (2013). Test-retest reliability of the “Reading the Mind in the Eyes” test: a one-year follow-up study. Mol. Autism 4:33. doi: 10.1186/2040-2392-4-33/TABLES/2
Fernández-Castañeda, A., Lu, P., Geraghty, A. C., Song, E., Lee, M.-H., Wood, J., et al. (2022). Mild respiratory COVID can cause multi-lineage neural cell and myelin dysregulation. Cell 185, 2452–2468.e16. doi: 10.1016/j.cell.2022.06.008
Fernández-de-Las-Peñas, C., Gómez-Mayordomo, V., de-la-Llave-Rincón, A. I., Palacios-Ceña, M., Rodríguez-Jiménez, J., Florencio, L. L., et al. (2021). Anxiety, depression and poor sleep quality as long-term post-COVID sequelae in previously hospitalized patients: a multicenter study. J. Infect. 83, 496–522. doi: 10.1016/j.jinf.2021.06.022
Galea, S., Merchant, M. R., and Lurie, N. (2020). The mental health consequences of COVID-19 and physical distancing the need for prevention and early intervention. JAMA 180, 817–818. doi: 10.1001/jamainternmed.2020.1562
García-Campayo, J., Zamorano, E., Ruiz, M. A., Pardo, A., Pérez-Páramo, M., López-Gómez, V., et al. (2010). Cultural adaptation into Spanish of the generalized anxiety disorder-7 (GAD-7) scale as a screening tool. Health Qual Life Outcomes 20:8. doi: 10.1186/1477-7525-8-8
García-Sánchez, C., Calabria, M., Grunden, N., Pons, C., Arroyo, J. A., Gómez-Anson, B., et al. (2022). Neuropsychological deficits in patients with cognitive complaints after COVID-19. Brain Behav. 12:e2508. doi: 10.1002/brb3.2508
Gomar, J. J., Ortiz-Gil, J., McKenna, P. J., Salvador, R., Sans-Sansa, B., Sarró, S., et al. (2011). Validation of the word accentuation Test (TAP) as a means of estimating premorbid IQ in Spanish speakers. Schizophr. Res. 128, 175–176. doi: 10.1016/j.schres.2010.11.016
González-Blanch, C., Pérez-Iglesias, R., Rodríguez-Sánchez, J. M., Pardo-García, G., Martínez-García, O., Vázquez-Barquero, J. L., et al. (2011). A digit symbol coding task as a screening instrument for cognitive impairment in first-episode psychosis. Arch. Clin. Neuropsychol. 26, 48–58. doi: 10.1093/ARCLIN/ACQ086
Guo, P., Benito Ballesteros, A., Yeung, S. P., Liu, R., Saha, A., Curtis, L., et al. (2022). COVCOG 1: factors predicting physical, neurological and cognitive symptoms in long COVID in a community sample. a first publication from the covid and cognition study. Front. Aging Neurosci. 14:804922. doi: 10.3389/FNAGI.2022.804922
Hampshire, A., Trender, W., Chamberlain, S. R., Jolly, A. E., Grant, J. E., Patrick, F., et al. (2021). Cognitive deficits in people who have recovered from COVID-19. EClinicalMedicine 39:101044. doi: 10.1016/J.ECLINM.2021.101044
Henry, J. D., Phillips, L. H., Crawford, J. R., Ietswaart, M., and Summers, F. (2006). Theory of mind following traumatic brain injury: the role of emotion recognition and executive dysfunction. Neuropsychologia 44, 1623–1628. doi: 10.1016/j.neuropsychologia.2006.03.020
Hopkins, R. O., Weaver, L. K., Collingridge, D., Parkinson, R. B., Chan, K. J., and Orme, J. F. (2005). Two-year cognitive, emotional, and quality-of-life outcomes in acute respiratory distress syndrome. Am. J. Respir. Crit. Care Med. 171, 340–347. doi: 10.1164/rccm.200406-763OC
Hopkins, R. O., Weaver, L. K., Pope, D., Orme, J. F., Bigler, E. D., and Larson-Lohr, V. (1999). Neuropsychological sequelae and impaired health status in survivors of severe acute respiratory distress syndrome. Am. J. Respir. Crit. Care Med. 160, 50–56. doi: 10.1164/ajrccm.160.1.9708059
Hosmer, D. W. Jr., Lemeshow, S., and Sturdivant, R. X. (2013). Applied Logistic Regression, 3rd Edn. Hoboken, NJ: Wiley.
Jackson, C. (2014). The chalder fatigue scale (CFQ 11). Occup. Med. 65:86. doi: 10.1093/occmed/kqu168
Knight, M. J., and Baune, B. T. (2019). The direct and indirect relationship between social cognition and psychosocial dysfunction in major depressive disorder. Front. Psychiatry 10:347. doi: 10.3389/FPSYT.2019.00347/BIBTEX
Kroenke, K., Spitzer, R. L., and Williams, J. B. (2001). The PHQ-9: validity of a brief depression severity measure. J. Gen. Intern. Med. 16, 606–613. doi: 10.1046/j.1525-1497.2001.016009606.x
Lezak, M. D., Howieson, D. B., Bigler, E. D., and Tranel, D. (2012). Neuropsychological Assessment, 5th Edn. Oxford: Oxford University Press.
Lu, Y., Li, X., Geng, D., Mei, N., Wu, P. Y., Huang, C. C., et al. (2020). Cerebral micro-structural changes in COVID-19 patients - an MRI-based 3-month follow-up study: a brief title: cerebral changes in COVID-19. EClinicalMedicine 25:100484. doi: 10.1016/j.eclinm.2020.100484
Maamar, M., Artime, A., Pariente, E., Fierro, P., Ruiz, Y., Gutiérrez, S., et al. (2022). Post-COVID-19 syndrome, low-grade inflammation and inflammatory markers: a cross-sectional study. Curr. Med. Res. Opin 38:1. doi: 10.1080/03007995.2022.2042991
Mattioli, F., Stampatori, C., Righetti, F., Sala, E., Tomasi, C., and De Palma, G. (2021). Neurological and cognitive sequelae of Covid-19: a four month follow-up. J. Neurol. 268, 4422–4428. doi: 10.1007/s00415-021-10579-10576
Mazza, M. G., de Lorenzo, R., Conte, C., Poletti, S., Vai, B., Bollettini, I., et al. (2020). Anxiety and depression in COVID-19 survivors: role of inflammatory and clinical predictors. Brain Behav. Immun. 89, 594–600. doi: 10.1016/j.bbi.2020.07.037
McDonnell, M., Dill, L., Panos, S., Amano, S., Brown, W., Giurgius, S., et al. (2020). Verbal fluency as a screening tool for mild cognitive impairment. Int. Psychogeriatr. 32:1055. doi: 10.1017/S1041610219000644
Meyers, J. E., and Meyers, K. R. (1996). Rey Complex Figure Test and Recognition Trial - Professional Manual. Odessa, FL: Psychological Assessment Resources.
Nasreddine, Z. S., Phillips, N. A., Bédirian, V., Charbonneau, S., Whitehead, V., Collin, I., et al. (2005). The montreal cognitive assessment, MoCA: a brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 53, 695–699. doi: 10.1111/j.1532-5415.2005.53221.x
Nejati, V., Zabihzadeh, A., Maleki, G., and Tehranchi, A. (2012). Mind reading and mindfulness deficits in patients with major depression disorder. Proc. Soc. Behav. Sci. 32, 431–437. doi: 10.1016/j.sbspro.2012.01.065
Ojeda, N., del Pino, R., Ibarretxe-Bilbao, N., Schretlen, D. J., and Peña, J. (2016). [Montreal cognitive assessment test: normalization and standardization for Spanish population]. Rev. Neurol. 63, 488–496. doi: 10.33588/rn.6311.2016241
Peña-Casanova, J., Quiñones-Úbeda, S., Gramunt-Fombuena, N., Quintana-Aparicio, M., Aguilar, M., Badenes, D., et al. (2009). Spanish multicenter normative studies (NEURONORMA Project): norms for verbal fluency tests. Arch. Clin. Neuropsychol. 24, 395–411. doi: 10.1093/ARCLIN/ACP042
Proal, A. D., and VanElzakker, M. B. (2021). Long COVID or Post-acute Sequelae of COVID-19 (PASC): an overview of biological factors that may contribute to persistent symptoms. Front. Microbiol. 12:698169. doi: 10.3389/FMICB.2021.698169
Reitan, R. M. M. (1958). Validity of the trail making test as an indicator of organic brain damage. Percep. Mot. Skills 8, 271–276. doi: 10.2466/PMS.8.7.271-276
Schmidt, M. (1996). Rey Auditory and Verbal Learning Test: A handbook. Los Angeles, CA: Western Psychological Services.
Silva, L. S., Joao, R. B., Nogueira, M. H., Aventurato, I. K., de Campos, B. M., de Brito, M. R., et al. (2021). Functional and microstructural brain abnormalities, fatigue, and cognitive dysfunction after mild COVID-19. medRxiv [preprint] doi: 10.1101/2021.03.20.21253414
Soriano, J. B., Murthy, S., Marshall, J. C., Relan, P., and Diaz, J. V. (2022). A clinical case definition of post-COVID-19 condition by a Delphi consensus. Lancet Infect. Dis. 22, e102–e107.
Spitzer, R. L., Kroenke, K., Williams, J. B., and Löwe, B. (2006). A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch. Intern. Med. 166, 1092–1097. doi: 10.1001/archinte.166.10.1092
Tabachnick, B. G., and Fidell, L. S. (2014). Using Multivariate Statistics, 6th Edn. England: Pearson Harlow.
Wechsler, D. (1999). WAIS III escala de inteligencia de Wechsler para adultos-III. Madrid: TEA Ediciones.
Weightman, M. J., Air, T. M., and Baune, B. T. (2014). A review of the role of social cognition in major depressive disorder. Front. Psychiatry 5:179. doi: 10.3389/fpsyt.2014.00179
Whiteside, D. M., Basso, M. R., Naini, S. M., Porter, J., Holker, E., Waldron, E. J., et al. (2022). Outcomes in post-acute sequelae of COVID-19 (PASC) at 6 months post-infection Part 1: cognitive functioning. Clin. Neuropsychol. 36, 806–828. doi: 10.1080/13854046.2022.2030412
Woo, M. S., Malsy, J., Pöttgen, J., Zai, S. S., Ufer, F., Hadjilaou, A., et al. (2020). Frequent neurocognitive deficits after recovery from mild COVID-19. Brain Comm. 2:fcaa205. doi: 10.1093/braincomms/fcaa205
Zhao, S., Shibata, K., Hellyer, P. J., Trender, W., Manohar, S., Hampshire, A., et al. (2022). Rapid vigilance and episodic memory decrements in COVID-19 survivors. Brain Comm. 4, 1–19. doi: 10.1093/braincomms/fcab295
Zhou, H., Lu, S., Chen, J., Wei, N., Wang, D., Lyu, H., et al. (2020). The landscape of cognitive function in recovered COVID-19 patients. J. Psych. Res. 129, 98–102. doi: 10.1016/j.jpsychires.2020.06.022
Keywords: COVID-19, post-COVID-19 condition, NeuroCOVID, neuropsychological test, cognitive function
Citation: Ariza M, Cano N, Segura B, Adan A, Bargalló N, Caldú X, Campabadal A, Jurado MA, Mataró M, Pueyo R, Sala-Llonch R, Barrué C, Bejar J, Cortés CU, NAUTILUS-Project Collaborative Group, Junqué C and Garolera M (2022) Neuropsychological impairment in post-COVID condition individuals with and without cognitive complaints. Front. Aging Neurosci. 14:1029842. doi: 10.3389/fnagi.2022.1029842
Received: 27 August 2022; Accepted: 03 October 2022;
Published: 20 October 2022.
Edited by:
Patricia C. Heyn, Marymount University, United StatesReviewed by:
Lambros Messinis, Aristotle University of Thessaloniki, GreeceIoana Miclutia, Iuliu Haţieganu University of Medicine and Pharmacy, Romania
Copyright © 2022 Ariza, Cano, Segura, Adan, Bargalló, Caldú, Campabadal, Jurado, Mataró, Pueyo, Sala-Llonch, Barrué, Bejar, Cortés, NAUTILUS-Project Collaborative Group, Junqué and Garolera. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Maite Garolera, bWdhcm9sZXJhQGNzdC5jYXQ=