 Monica E. Nelson1*
Monica E. Nelson1* Britney M. Veal1
Britney M. Veal1 Ross Andel2,3
Ross Andel2,3 Julie Martinkova3
Julie Martinkova3 Katerina Veverova3
Katerina Veverova3 Hana Horakova3
Hana Horakova3 Zuzana Nedelska3
Zuzana Nedelska3 Jan Laczó3
Jan Laczó3 Martin Vyhnalek3
Martin Vyhnalek3 Jakub Hort3
Jakub Hort3- 1School of Aging Studies, University of South Florida, Tampa, FL, United States
- 2Edson College of Nursing and Health Innovation, Arizona State University, Phoenix, AZ, United States
- 3Department of Neurology, Second Faculty of Medicine, Charles University and Motol University Hospital, Prague, Czechia
Background: Dementia syndrome is one of the most devastating conditions in older adults. As treatments to stop neurodegeneration become available, accurate and timely diagnosis will increase in importance. One issue is that cognitive performance sometimes does not match the corresponding level of neuropathology, affecting diagnostic accuracy. Cognitive reserve (CR), which can preserve cognitive function despite underlying neuropathology, explains at least some variability in cognitive performance. We examined the influence of CR proxies (education and occupational position) on the relationship between hippocampal or total gray matter volume and cognition.
Methods: We used data from the Czech Brain Aging Study. Participants were clinically confirmed to be without dementia (n = 457, including subjective cognitive decline and amnestic mild cognitive impairment) or with dementia syndrome (n = 113).
Results: For participants without dementia, higher education magnified the associations between (a) hippocampal volume and executive control (b = 0.09, p = 0.033), (b) total gray matter volume and language (b = 0.12, p < 0.001), and (c) total gray matter volume and memory (b = 0.08, p = 0.018). Similarly, higher occupational position magnified the association between total gray matter volume and (a) attention/working memory (b = 0.09, p = 0.009), (b) language (b = 0.13, p = 0.002), and (c) memory (b = 0.10, p = 0.013). For participants with dementia, the associations between hippocampal (b = –0.26, p = 0.024) and total gray matter (b = –0.28, p = 0.024) volume and visuospatial skills decreased in magnitude with higher education.
Conclusion: We found that the association between brain volume and cognitive performance varies based on CR, with greater CR related to a stronger link between brain volume and cognition before, and a weaker link after, dementia diagnosis.
Introduction
Alzheimer’s disease (AD) is the most prevalent cause of dementia syndrome in older adults (Alzheimer’s Association, 2022). The pathophysiological mechanisms thought to cause AD include impaired amyloid-beta and tau protein metabolism and neurodegeneration leading to regional and whole brain atrophy (according to the amyloid cascade hypothesis; Hardy and Higgins, 1992; Karran et al., 2011; Jack and Holtzman, 2013; Jack et al., 2013); however, it is known that clinical progression of the disease does not always align with levels of neuropathology load. Therefore, there can be a dichotomy between expected and observed cognitive performance based on level of neuropathology which raises the question of what additional factors may be contributing to the preservation of cognitive functions in older adults. Stern et al. (2020) discuss the concept of resilience, which is related to brain reserve, brain maintenance, and cognitive reserve, as an explanation for this dichotomy.
Cognitive reserve is an active mechanism thought to be influenced by lifetime experiences and achievements and explains better cognitive performance in the presence of neuropathology (Stern et al., 2020). Cognitive reserve is typically measured through sociobehavioral proxies (e.g., education or occupation) which are thought to contribute to reserve (Stern, 2002, 2009). Stern et al. (2020) suggest that an effective way to test the cognitive reserve hypothesis is through examining whether measures of reserve moderate the association between brain health and cognition.
Some studies have assessed how markers of cognitive reserve, such as education or occupation, moderate the relationship between AD-related neuropathology and cognitive outcomes but with discrepant findings. For example, in healthy older adults, higher educational attainment was associated with a weaker negative relationship between positron emission tomography (PET)-assessed amyloid-beta load and episodic memory performance (Joannette et al., 2020). However, higher education was also associated with a stronger positive relationship between hippocampal volume and delayed recall in healthy older adults (O’Shea et al., 2018). Similar divergent results have emerged in samples that included participants with cognitive impairment. For example, in a Dutch sample of older adults from a memory clinic that included participants with subjective cognitive impairment (SCI), mild cognitive impairment (MCI), and AD dementia, there was a weaker positive relationship between medial temporal lobe volume and global cognitive abilities (i.e., greater volume/less atrophy related to better cognition) in more educated participants (Staekenborg et al., 2020). However, a study using data from a memory clinic in South Korea, which included participants with normal cognitive function, MCI, and dementia, reported that less right temporoparietal tau pathology and greater cortical thickness of the left inferior temporal gyrus were related to better memory performance—these relationships were stronger for individuals with higher cognitive reserve (a combination of education and work complexity) (Lee et al., 2019). Clearly, more research is needed to disentangle discrepancies between studies investigating cognitive reserve, brain health, and cognitive outcomes, especially within (rather than across) subgroups with the same cognitive status.
It is possible that these discrepant findings may result from the presence of a non-linear relationship between cognitive reserve, brain health markers, and cognitive outcomes. Evidence suggests that cognitive reserve interacts with cognitive performance and brain health differentially depending on the cognitive status of the sample being studied (e.g., healthy versus pathological aging; Menardi et al., 2018). Specifically, the interaction between brain health and cognition transitions from protective in healthy aging (i.e., higher cognitive reserve associated with better brain health) to compensatory in pathological aging (i.e., higher cognitive reserve associated with greater pathology; Menardi et al., 2018), but in both situations, higher cognitive reserve is associated with better cognitive performance. However, this explanation may be too simple since divergent findings regarding the moderating effect of cognitive reserve on brain health-cognition relationships have been found in both healthy and pathological aging.
Building on past research (O’Shea et al., 2018; Lee et al., 2019; Joannette et al., 2020; Staekenborg et al., 2020), we investigated how two common proxies of cognitive reserve (education and occupational position) moderated the relationship between brain health, represented by hippocampal and total gray matter volume, and cognition in participants without dementia (i.e., subjective cognitive decline [SCD] and amnestic MCI [aMCI]) and with dementia syndrome. We modeled our approach after Joannette et al. (2020) who identified regions of significant moderations utilizing the Johnson–Neyman technique (Johnson and Fay, 1950), but with significant moderations probed via pre-defined groupings of cognitive reserve (Joannette et al., 2020). Since we used a sample from a memory clinic with variation in levels of clinical impairment, we may be able to detect at what point the relationship between brain volume and cognition becomes affected by markers of cognitive reserve. To extend past research that used only memory (O’Shea et al., 2018; Joannette et al., 2020) or general cognitive abilities (Staekenborg et al., 2020) as the cognitive outcome, we assessed a full range of cognitive domains in analyses.
Materials and methods
Participants
The Czech Brain Aging Study (CBAS) is a longitudinal cohort study of patients in the Memory Clinic in Motol University Hospital and Charles University, Prague, Czech Republic (Sheardova et al., 2019). The participants were referred to the Memory Clinic by general practitioners, neurologists, or psychiatrists for self- and/or informant-reported cognitive complaints. The presented cross-sectional study utilized the cognitive testing and neuroimaging data from these participants, though other studies on laboratory and genetic results and spatial navigation exist. All participants provided informed consent. The Institutional Review Board of Motol University Hospital continually approves this research project.
A total of 873 individuals had at least one magnetic resonance imaging (MRI) scan, forming the initial sample. Participants with greater than 6 months between their MRI scan and neuropsychological tests (n = 33), missing information on education (n = 9), occupational position (n = 77), or diagnosis (n = 22), who had a main lifetime occupation in the armed forces (n = 5), who had non-amnestic MCI (n = 84), or completed less than 50% of neuropsychological tests used to create each of the cognitive domains (n = 19) were dropped. To limit the sample to participants with mild dementia, participants diagnosed with dementia who did not have information about their Mini Mental State Exam (MMSE) or who had a score less than 18 were dropped (n = 54). Therefore, the final analytic sample included 570 participants who were diagnosed without dementia (n = 457; including SCD [n = 149] and aMCI [n = 308]) or with dementia syndrome (n = 113). We included aMCI specifically since (a) it has been shown to relate more strongly to dementia progression than non-amnestic MCI (Peltz et al., 2011; Michaud et al., 2017), (b) it is the most common type of MCI, and (c) it is more likely associated with a neurodegenerative cause compared to non-amnestic MCI (Petersen et al., 2009).
Participants without dementia included individuals with clinical diagnoses of SCD or aMCI. SCD was defined as having normal objective cognitive performance, self-reported persistent cognitive complaints within the last 5 years in comparison with a previously normal status and being unrelated to an acute event, and having a Clinical Dementia Rating (CDR) global score of ≤ 0.5 (Jessen et al., 2014). aMCI was defined as scoring ≥ 1.5 standard deviations below age- and education-adjusted neuropsychological test means in at least one of the memory tests, a CDR score ≤ 0.5, and cognitive complaints reported by the patient or a reliable informant (Petersen, 2004). Although aMCI was based mainly on neuropsychological tests, agreement within a multidisciplinary clinical team was required for the formal diagnosis, including a cognitive neurologist, clinical neuropsychologist, and psychometricians, taking into account the nature of the cognitive complaints and the patient’s medical history. To maintain parsimonious presentation of the results, we combined the two groups indicative of cognitive impairment (but without dementia)—SCD and aMCI. The decision to group SCD and aMCI is supported by the fact that individuals with SCD and aMCI are presumed to be on a cognitive continuum with at least some overlap whereby the two diagnoses have a tendency to fluctuate over time.
Dementia syndrome was diagnosed based on a consensus panel (Sheardova et al., 2019) using the Diagnostic and Statistical Manual of Mental Disorders: Text Revision (DSM-IV-TR) guidelines (American Psychiatric Association, 2000). The progression to dementia and the etiology of dementia syndrome was established during the regular consensus meetings of neurologists and neuropsychologists. The diagnosis was mainly based on clinical history reported by the patient and the caregiver, neurological examination, and neuropsychological assessment. Brain MRI and PET scans were also considered when available. Most participants diagnosed with dementia syndrome had either AD (42%) or mixed dementia (40%) as their etiology, with other etiologies (e.g., vascular dementia, frontotemporal dementia, dementia with Lewy bodies; 15%) or unavailable etiologies (4%) present in the remainder of the sample. The etiology of dementia syndrome was based on the current clinical criteria for probable AD (McKhann et al., 2011), probable vascular dementia (Román et al., 1993), probable dementia with Lewy bodies (McKeith et al., 2017), or probable behavioral variant of frontotemporal dementia (Rascovsky et al., 2011).
Measures
Cognitive domains
Neuropsychological tests were used to create cognitive domains by standardizing scores on each test then averaging the individual tests into a composite variable. Standardization was completed separately for participants with and without dementia; thus, participants’ performance on these tests would be compared against other participants in the same diagnostic group.
Attention/working memory
This domain (α = 0.78) was assessed with four tests. We used Trail Making Test – Part A (TMT-A) with a maximum time of 180 s (Bezdicek et al., 2012). Participants who were unable to complete it within the given time frame were scored as 181 s. For analyses the score was reversed. The other tests included: Digit Symbol Coding Test, Digit Span – Forward (Digits-F), and Digit Span – Backward (Digits-B) from the Wechsler Adult Intelligence Scale – Revised (Wechsler, 1997), assessed with sub-scores (i.e., number of correct items).
Executive control
This domain (α = 0.62) was assessed with two tests: Controlled Oral Word Association Test (COWAT) with letters N, K, and P (Czech Republic Version) (Nikolai et al., 2015), and Trail Making Test – Part B (TMT-B) (Bezdicek et al., 2012). The maximum time for completion of the TMT-B was 300 s. However, those who were unable to complete it within the given time frame were scored as 301 s. For analyses the score was reversed.
Language
This domain (α = 0.84) was assessed with four tests: Boston Naming Test (BNT) (Goodglass et al., 1983), Verbal Fluency Test – Vegetables (VFT-V), Verbal Fluency Test – Animals (VFT-A) (Nikolai et al., 2015), and the Similarities subtest from the Wechsler Adult Intelligence Scale – III (Wechsler, 1997).
Memory
This domain (α = 0.93) was assessed with four tests. Specifically, the Rey Auditory Verbal Learning Test – Immediate Recall (AVLT-I; Sum of Trials 1-5) and Delayed Recall (AVLT-D) (Bezdicek et al., 2014), Brief Visuospatial Memory Test – Revised Immediate Recall (BVMTR-I; Sum of Trials 1–3) and Delayed Recall (BVMTR-D) (Benedict et al., 1996), and the Uniform Data Set Logical Memory Immediate Recall Test (Log-I) and Delayed Recall Test (Log-D) (Nikolai et al., 2018). The Rey–Osterrieth Complex Figure Test Recall was a test of non-verbal memory (Osterrieth, 1944). The AVLT, BVMTR, and Log included both immediate and delayed components in one exam.
Visuospatial skills
This domain (α = 0.77) was assessed with two tests: Clock Drawing Test (Mazancova et al., 2017) (Cohen scoring system) and the Rey-Osterrieth Complex Figure Test Copy (Meyers and Meyers, 1995).
Magnetic resonance imaging
MRI scans were acquired on a 1.5T scanner (Avanto; Siemens, Erlangen, Germany) using T1-weighted three-dimensional high-resolution magnetization-prepared rapid acquisition with gradient echo (MPRAGE) sequence with the following parameters: TR/TE/TI = 2000/3.08/1100 ms, flip angle 15°, 192 continuous partitions, slice thickness 1.0 mm, and in-plane resolution 1 mm. Scans were visually examined by a neuroradiologist, blinded to the diagnosis, for sufficient technical quality and the absence of structural findings contradicting eligibility (Nedelska et al., 2012; Kerbler et al., 2015). MRI volumetry was processed using Freesurfer automated package (v5.3.01; Fischl et al., 2002). The current analyses focused on total hippocampal volume, which was calculated as the sum of the right and left hippocampal volumes, and total gray matter volume, both measured in cubic millimeters. Hippocampal volume and total gray matter volume were adjusted for estimated total intracranial volume (eTIV) to adjust for differences in head size (Voevodskaya et al., 2014). For analyses, eTIV-adjusted volumes were converted to z-scores based on diagnostic groups (i.e., participants without and with dementia).
Cognitive reserve proxies
Two cognitive reserve proxies were used in the current study. Education was measured as years of formal education (range: 8–27 years). Occupational position was coded by two independent raters according to the 2008 International Standard Classification of Occupations (ISCO-08; International Labour Office, 2012). The raters (JM, KV) were familiar with the data and native speakers of Czech language. The initial agreement was 87.5%. Coding for the remaining 12.5% of occupations was finalized during a consensus meeting between the two raters. Occupational position was coded based on main lifetime occupation; where unavailable (34.6%), last occupation was used. Participants were classified into one of the 10 categories represented by ISCO-08. Lower scores corresponded to higher occupational positions (1: managers, 2: professionals, 3: technicians and associate professionals, 4: clerical support workers, 5: services and sales workers, 6: skilled agricultural, forestry, and fishery workers, 7: craft and related trades workers, 8: plant and machine operators and assemblers, 9: elementary occupations, 0: armed forces workers). Due to the varied occupational positions that armed forces workers could align with, participants whose main lifetime occupation corresponded to armed forces workers were dropped from analyses. For analytic purposes, the ISCO-08 score was recoded such that higher scores were associated with higher occupational positions. We assessed the relative strength of education and occupation as cognitive reserve proxies by conducting analyses using standardized variables (z-scores). For interpretation of interactions, we graphed the associations between brain volume and cognition for individuals with high (+1 SD from mean) and low (–1 SD from mean) cognitive reserve.
Covariates
Age (years), sex (male or female), and depressive symptoms as measured by the Geriatric Depression Scale 15-item version (Yesavage et al., 1982) (GDS-15; cutoff ≥ 5) served as covariates.
Statistical analyses
Descriptive statistics were used to describe the two groups. Independent sample t-tests or chi-square tests were used to assess differences between groups on the study variables. Separate regression analyses were conducted by diagnosis to examine the interrelation between brain volume (i.e., hippocampal or total gray matter volume), cognitive reserve proxies (education or occupational position), and cognition (five cognitive domains). Covariates included age, sex, and depressive symptoms. Since the relationship between depressive symptoms and cognitive performance is complex (Butters et al., 2008) (e.g., depression could be a risk factor for, consequence of, or reaction to cognitive impairment), we also conducted analyses not controlling for depressive symptoms to determine the stability of effects. Additionally, as sex has been shown to influence reserve or resilience effects (Sundermann et al., 2016; Ewers, 2020; Subramaniapillai et al., 2021; Pa et al., 2022), we also conducted analyses stratified by sex.
We examined whether the cognitive reserve proxy variables moderated the relationship between brain volume and cognition. Significant interactions were probed with the Johnson-Neyman technique (Johnson and Fay, 1950) to identify “regions of significance,” that is, points at which there were significant moderated relationships between brain volume and cognition (Joannette et al., 2020). Significant interactions between brain volume and cognitive reserve proxies were graphed with high and low reserve corresponding to ±1 SD from the mean, respectively. Since main lifetime occupation represents the longest exposure to work environment and is therefore more likely to contribute to cognitive reserve than last occupation, we conducted sensitivity analyses restricting our sample to only participants who had data available on main lifetime occupation. All analyses were conducted using SAS software, Version 9.4 of the SAS System for Windows (SAS Institute, Cary, NC, USA). Moderation analyses were conducted with the PROCESS Macro Version 3.4.1 in SAS (Hayes and Little, 2018). Significance was assessed with a two-tailed test at p < 0.05. In order to account for multiple comparisons, we used the Holm–Bonferroni Sequential Correction method (Holm, 1979) in a model-wise fashion such that the lowest p-value within a model was compared to the most stringent level of significance (p < 0.005) which was reduced iteratively for subsequent effects. Effects were considered significant if they fell below the level prespecified by the correction method.
Results
Table 1 contains descriptive statistics for all study variables. Participants without dementia (i.e., SCD or aMCI) were significantly younger than participants with dementia. There was a greater frequency of women than men in the full sample, with no significant difference between groups. Participants without dementia had higher educational attainment and occupational position than participants with dementia. Depressive symptoms did not differ between groups. The diagnostic groups differed in terms of hippocampal volume, total gray matter volume, MMSE score, and each of the raw scores for the neuropsychological tests, as expected, such that brain volume was greater and cognition was better in participants without dementia compared to participants with dementia.
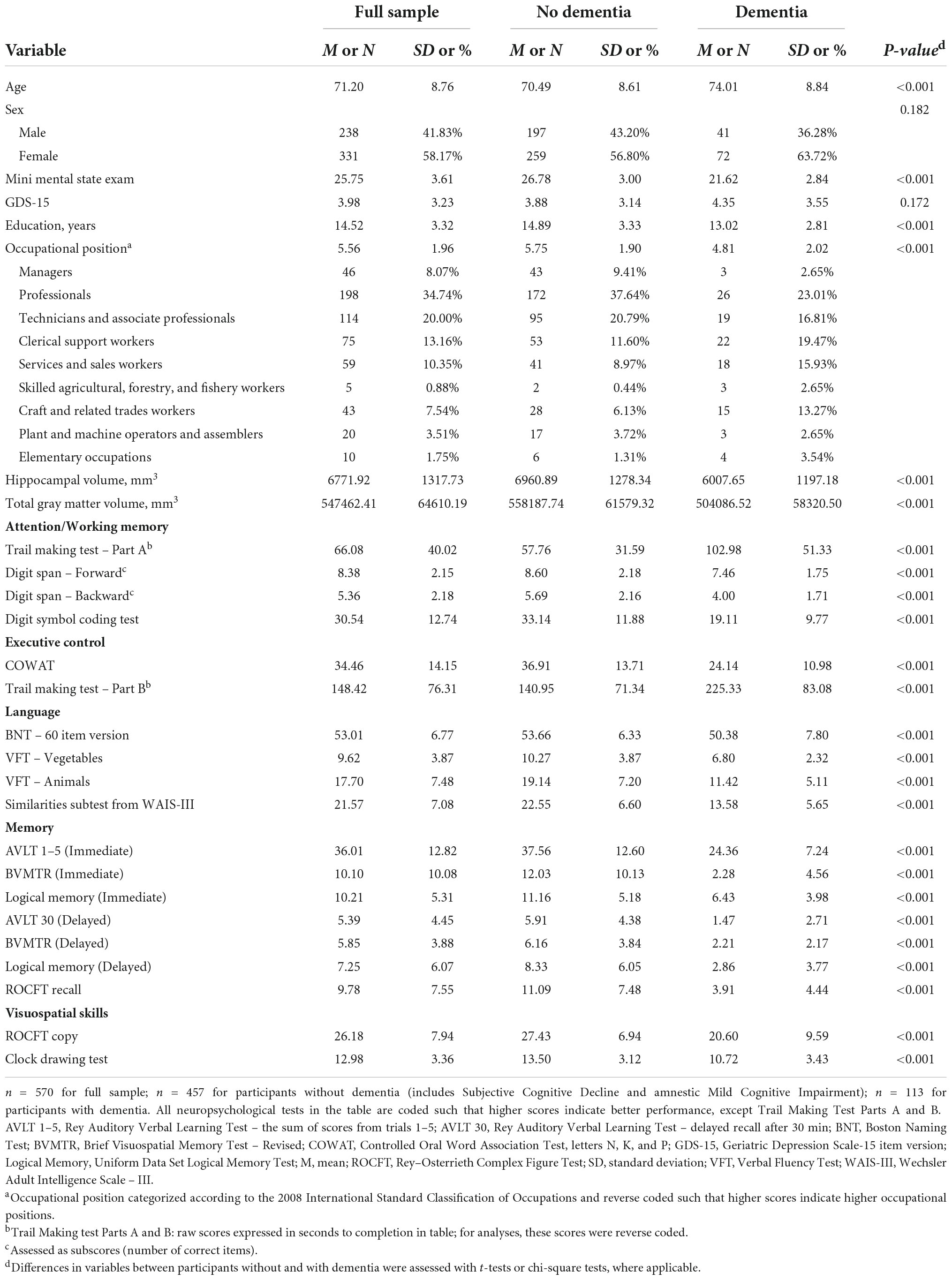
Table 1. Descriptive statistics of study variables for the full sample and by diagnosis.
Participants without dementia
Table 2 contains results from the regression analyses for participants without dementia (i.e., SCD or aMCI), controlling for age, sex, and depressive symptoms. Results remained the same after dropping depressive symptoms as a covariate (results not shown). Hippocampal volume was positively related to executive control, language, memory, and visuospatial skills (ps < 0.001 to p = 0.006), whereas total gray matter volume was positively related to all five cognitive domains (all ps < 0.001). Education moderated the association between hippocampal volume and executive control (b = 0.09, SE = 0.04, p = 0.033), total gray matter volume and language (b = 0.12, SE = 0.04, p < 0.001), and total gray matter volume and memory (b = 0.08, SE = 0.03, p = 0.018). Application of the Johnson–Neyman technique revealed overall similar patterns of moderation by education for the hippocampal volume-executive control relationship and the relationships between total gray matter volume and language and memory. Specifically, there was a significant positive association between brain volume and these cognitive domains that corresponded to about 10–13 years of education, with the brain volume-cognition link getting stronger as education increased. Examination of Figures 1A–C illustrates a generally strong positive association between brain volume and cognition for high education, and either a weaker or non-significant positive association between brain volume and cognition for low education. Only the interaction between total gray matter volume and education in association with language remained significant after correction for multiple comparisons.
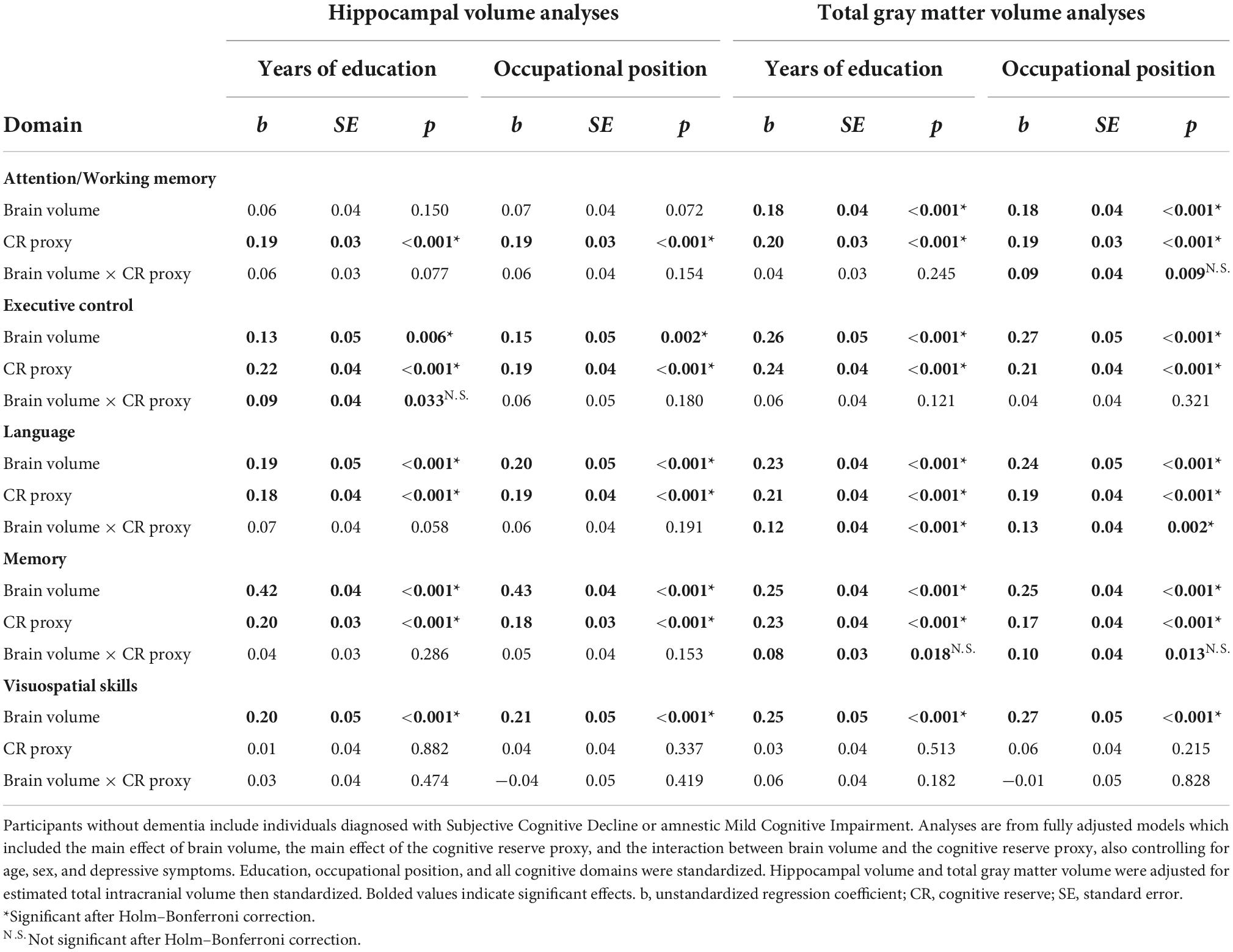
Table 2. Moderation analyses for participants without dementia.
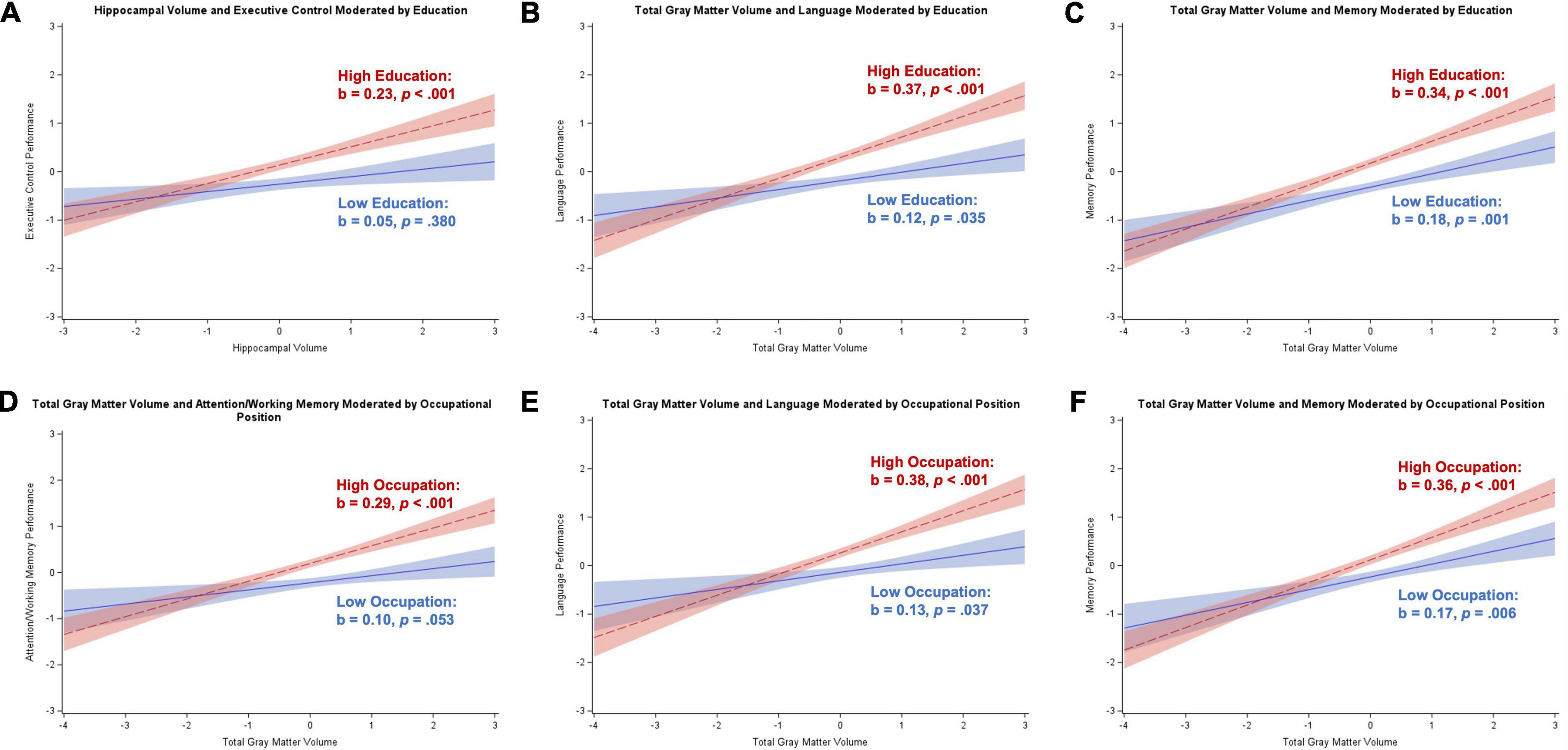
Figure 1. Plots of significant moderations by education and occupational position of the associations between cognition and brain volume in participants without dementia. High education or occupational position corresponds to 1 SD above the mean and low education or occupational position corresponds to 1 SD below the mean. The red dotted line represents high cognitive reserve, and the blue solid line represents low cognitive reserve. Shaded areas represent 95% confidence intervals. Cognition and brain volume were standardized. (A) Significant positive association between hippocampal volume and executive control for individuals with high education; non-significant for low education. (B) Significant positive association between total gray matter volume and language for individuals with low and high education; stronger relationship for high education. (C) Significant positive association between total gray matter volume and memory for individuals with low and high education; stronger relationship for high education. (D) Significant positive association between total gray matter volume and attention/working memory for individuals with high occupational position; non-significant for low occupational position. (E) Significant positive association between total gray matter volume and language for individuals with low and high occupational position; stronger relationship for high occupational position. (F) Significant positive association between total gray matter volume and memory for individuals with low and high occupational position; stronger relationship for high occupational position.
Occupational position moderated the association between total gray matter volume and attention/working memory (b = 0.09, SE = 0.04, p = 0.009), language (b = 0.13, SE = 0.04, p = 0.002), and memory (b = 0.10, SE = 0.04, p = 0.013). The Johnson–Neyman technique revealed similar moderating effects of occupational position in each cognitive domain. Specifically, there were significant positive associations between brain volume and cognition for individuals with over level 3 occupational positions (starting with skilled workers/service or sales workers), with the brain volume-cognition relationships strengthening as occupational position increased. Figures 1D–F illustrates a strong positive association between total gray matter volume and cognition for participants with high occupational positions and either a weaker or non-significant positive association for participants with low occupational positions. Similar to the education analyses, only the total gray matter volume-occupational position interaction relating to language remained significant after correcting for multiple comparisons.
Covariate effects for participants without dementia
Table 3 contains the effects of age, sex, and depressive symptoms from the moderation analyses conducted for participants without dementia. Across the two cognitive reserve proxies and two brain areas of interest, age was negatively related to all five cognitive outcomes for all but two models. Women performed better on executive control and worse on language and visuospatial skills compared to men. Having more depressive symptoms was related to worse attention/working memory, executive control, and visuospatial skills.
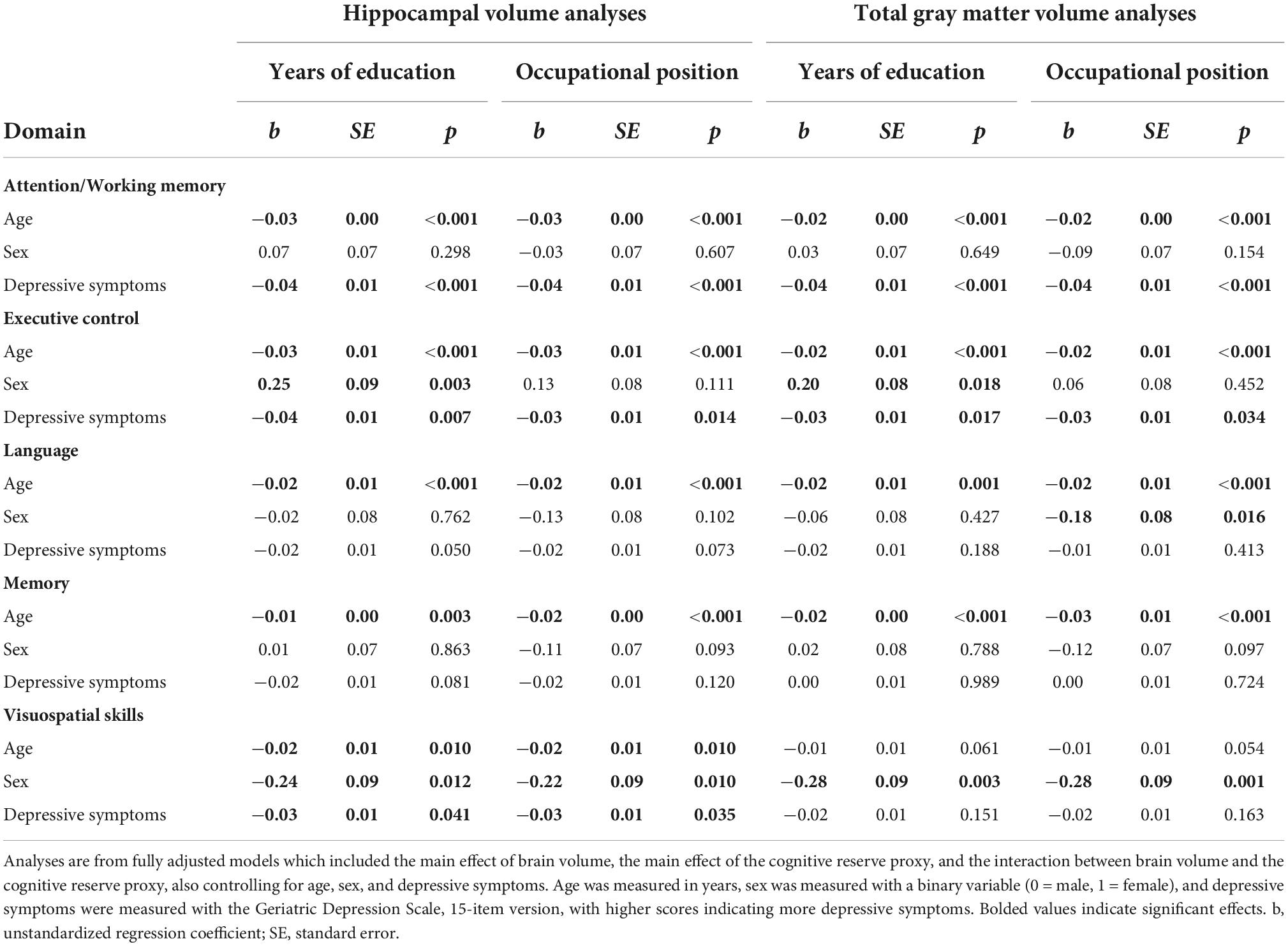
Table 3. Covariate effects from moderation analyses for participants without dementia.
Participants with dementia
Table 4 contains results from the regression analyses for participants with dementia syndrome, controlling for age, sex, and depressive symptoms. Results after excluding depressive symptoms as a covariate were consistent with main analyses (results not shown). Hippocampal volume was negatively associated with attention/working memory and visuospatial skills, and positively related to memory (ps = 0.003–0.045). Total gray matter volume was positively related to executive control (p = 0.044). Education moderated the association between hippocampal volume and visuospatial skills (b = –0.26, SE = 0.11, p = 0.024), with the Johnson–Neyman technique identifying 12+ years of education associated with a significant negative effect. Figure 2A illustrates a strong negative relationship for participants with high education and a non-significant negative relationship for participants with low education. Education also moderated the association between total gray matter volume and visuospatial skills (b = –0.28, SE = 0.12, p = 0.024), but in this case, there was a significant positive relationship for participants with low-to-middle educational attainment (i.e., 8–13 years). Figure 2B illustrates a significant positive association between total gray matter volume and visuospatial skills for individuals with low education, and a non-significant negative relationship between these variables for individuals with high education. Correction for multiple comparisons reduced these two interaction effects to null.
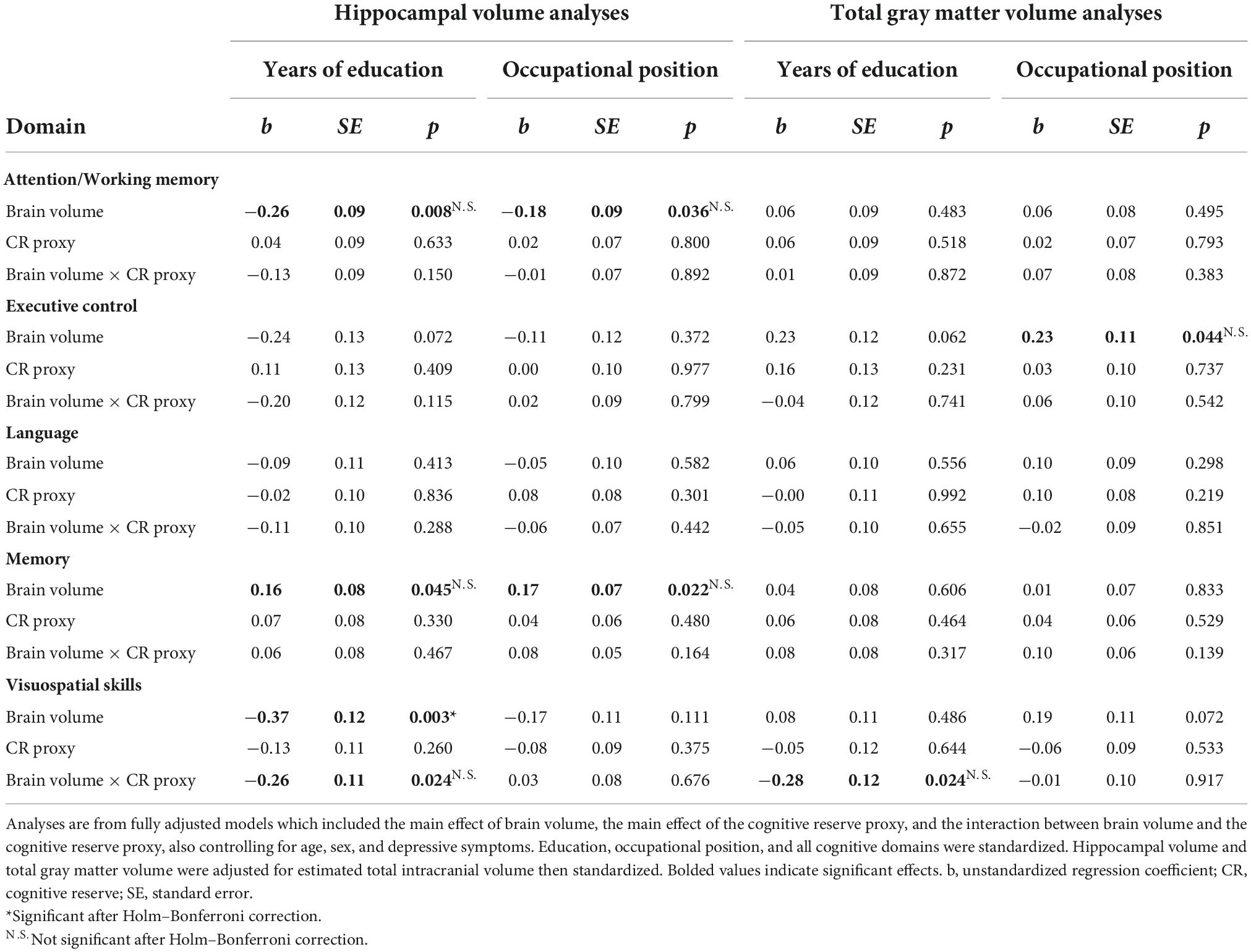
Table 4. Moderation analyses for participants with dementia.
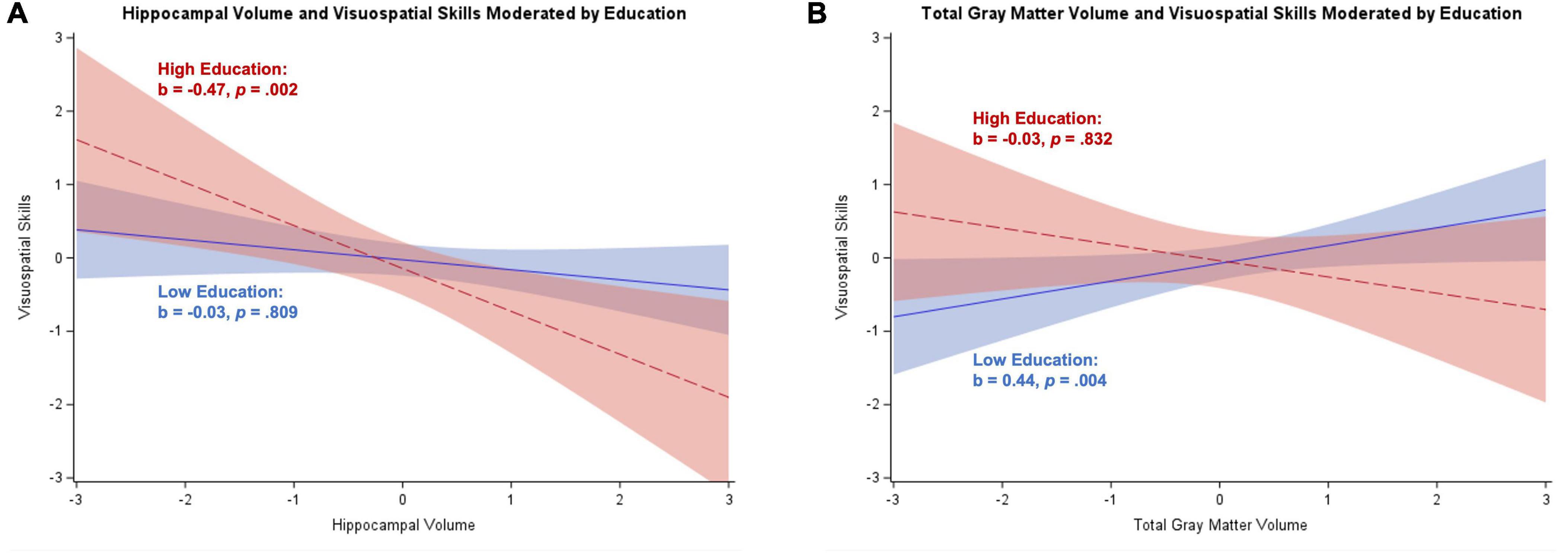
Figure 2. Plots of significant moderations by education of the associations between brain volume and visuospatial skills for participants with dementia. High education corresponds to 1 SD above the mean and low education corresponds to 1 SD below the mean. The red dotted line represents high education, and the blue solid line represents low education. Shaded areas represent 95% confidence intervals. Visuospatial skills and brain volume were standardized. (A) Significant negative relationship between hippocampal volume and visuospatial skills for individuals with high education; non-significant for low education. (B) Significant positive association between total gray matter volume and visuospatial skills for participants with low education; non-significant negative association for individuals with high education.
In sensitivity analyses, we assessed whether effects were similar when the sample was restricted to the 84 participants who had an AD etiology (pure or mixed). Hippocampal volume was negatively related to visuospatial skills (b = –0.29, SE = 0.15, p = 0.049), total gray matter volume was positively associated with executive control performance (analyses with education as moderator: b = 0.30, SE = 0.13, p = 0.027; analyses with occupational position as moderator: b = 0.29, SE = 0.12, p = 0.022), and education was positively related to executive control performance (total gray matter volume analyses: b = 0.29, SE = 0.15, p = 0.049). No other main effects were significant and there was no evidence that education or occupational position moderated the association between brain volume and cognition.
Covariate effects for participants with dementia
Table 5 contains the effects of age, sex, and depressive symptoms from the moderation analyses conducted for participants with dementia. Age was negatively related to memory performance. There were no main effects of sex in any of the models conducted. Having more depressive symptoms was related to better memory performance but worse executive control and visuospatial skills.
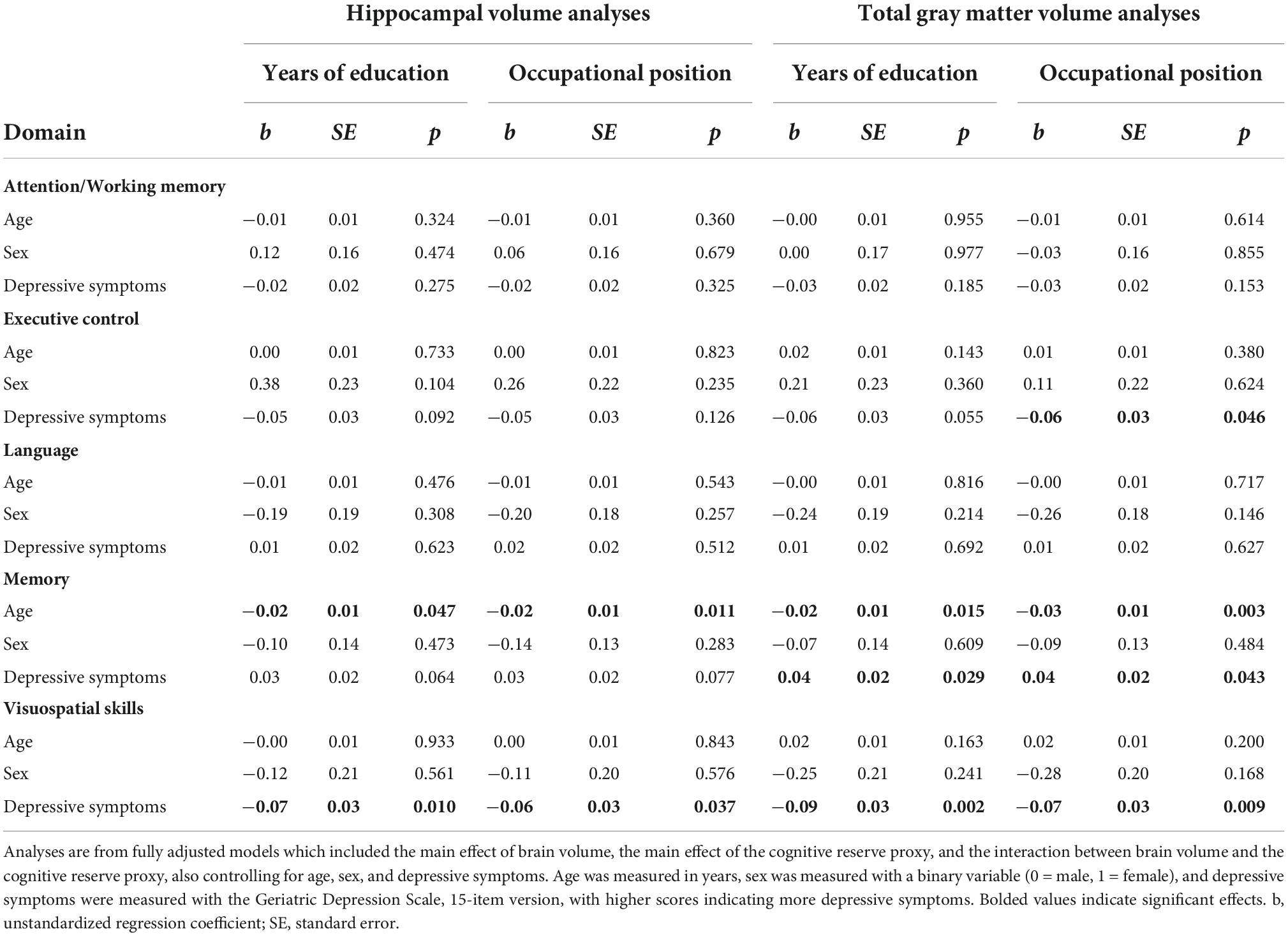
Table 5. Covariate effects from moderation analyses for participants with dementia.
Supplemental analyses
Moderation analyses separating participants without dementia
In order to provide a more refined tracking of how cognitive reserve may modify the relationship between brain volume and cognitive outcomes across the cognitive status continuum, we ran supplemental analyses for participants without dementia separately for those with SCD and aMCI.
Participants with subjective cognitive decline
Moderation analyses for participants with SCD revealed a positive relationship between hippocampal volume and executive control, memory, and visuospatial skills (ps < 0.001 to p = 0.045), and a positive relationship between total gray matter volume and visuospatial skills (p < 0.001). Education moderated the relationship between hippocampal volume and attention/working memory (b = 0.12, SE = 0.05, p = 0.020) and executive control (b = 0.17, SE = 0.06, p = 0.009), and total gray matter volume and attention/working memory (b = 0.16, SE = 0.06, p = 0.010), executive control (b = 0.20, SE = 0.08, p = 0.012), and language (b = 0.15, SE = 0.07, p = 0.037). The Johnson–Neyman technique revealed a significant positive relationship between brain volume and cognition starting between 14 and 21 years of education that strengthened as education increased. There was also a significant negative relationship between total gray matter volume and attention/working memory for participants with less than 9 years of education that strengthened with decreasing education. These results are illustrated in Figure 3.

Figure 3. Plots of significant moderations by education of the associations between brain volume and cognition for participants with subjective cognitive decline. High education corresponds to 1 SD above the mean and low education corresponds to 1 SD below the mean. The red dotted line represents high education, and the blue solid line represents low education. Shaded areas represent 95% confidence intervals. Cognition and brain volume were standardized. (A) Non-significant positive association between hippocampal volume and attention/working memory for participants with high education; non-significant negative association for low education. (B) Significant positive association between total gray matter volume and attention/working memory for participants with high education; non-significant negative association for low education. (C) Significant positive association between total gray matter volume and language for participants with high education; non-significant negative association for low education. (D) Significant positive association between hippocampal volume and executive control for participants with high education; non-significant positive association for low education. (E) Significant positive association between total gray matter volume and executive control for participants with high education; non-significant positive association for low education.
Occupational position moderated the relationship between hippocampal volume and attention/working memory (b = 0.11, SE = 0.06, p = 0.046) and language (b = 0.18, SE = 0.07, p = 0.007), and total gray matter volume and attention/working memory (b = 0.13, SE = 0.06, p = 0.038), language (b = 0.19, SE = 0.07, p = 0.012), and visuospatial skills (b = –0.27, SE = 0.09, p = 0.004). The Johnson–Neyman technique revealed no regions of significance for the relationships between brain volume and attention/working memory, implying a more general trend as opposed to a specific region of significance. For language, there were significant negative relationships with brain volume for participants with either “plant and machine operators and assemblers” occupations or “elementary” occupations (≤1 on scale), but also significant positive relationships with brain volume for participants with managerial or professional occupations (≥7 on scale). For visuospatial skills, participants with less than professional occupations (<7 on scale) had a significant positive association with total gray matter volume that strengthened with decreasing occupational position. These results are illustrated in Figure 4.
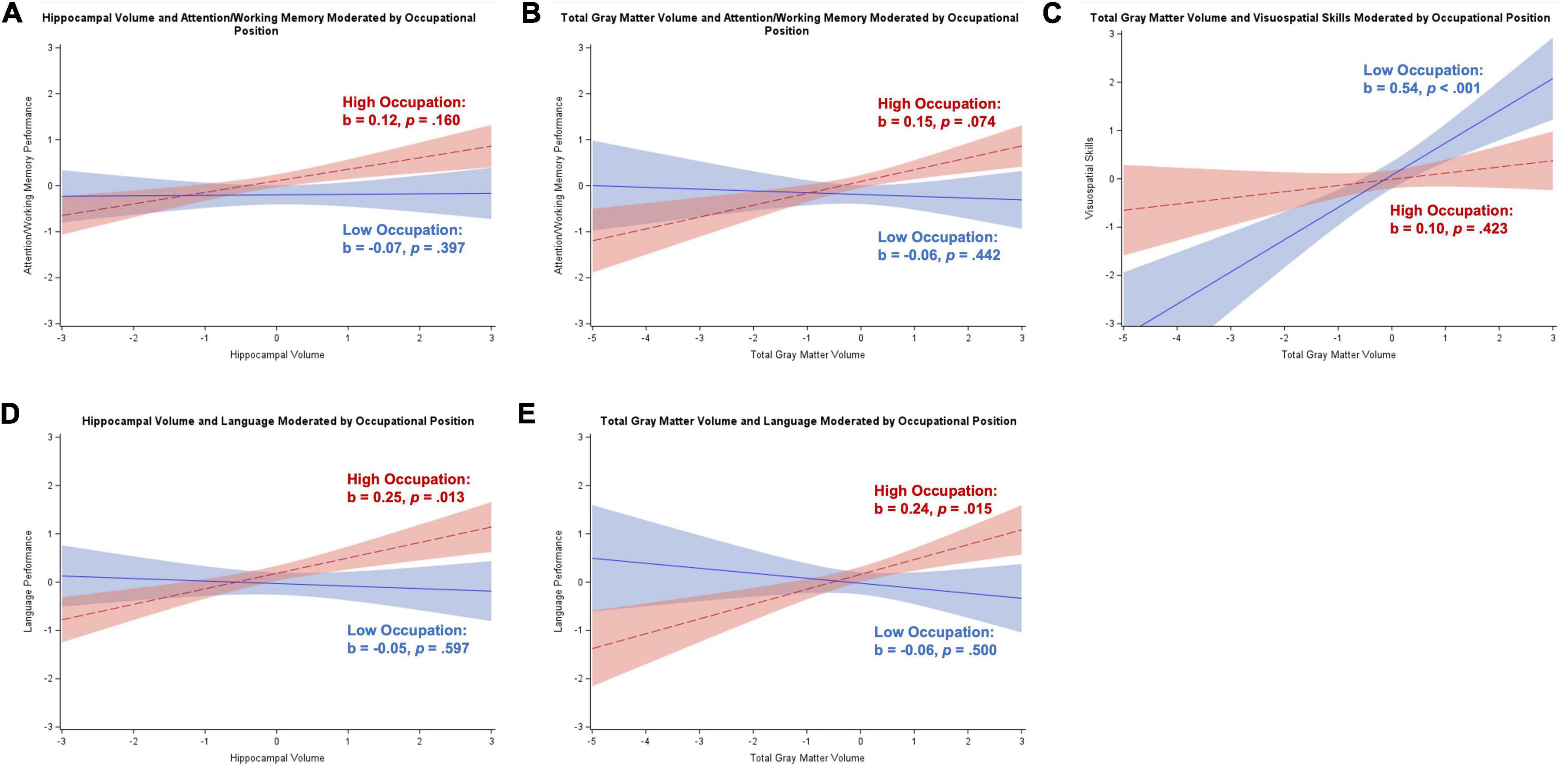
Figure 4. Plots of significant moderations by occupational position of the associations between brain volume and cognition for participants with subjective cognitive decline. High occupational position corresponds to 1 SD above the mean and low occupational position corresponds to 1 SD below the mean. The red dotted line represents high occupational position, and the blue solid line represents low occupational position. Shaded areas represent 95% confidence intervals. Cognition and brain volume were standardized. (A) Non-significant positive association between hippocampal volume and attention/working memory for participants with high occupational position; non-significant negative association for low occupational position. (B) Non-significant positive association between total gray matter volume and attention/working memory for participants with high occupational position; non-significant negative association for low occupational position. (C) Non-significant positive association between total gray matter volume and visuospatial skills for participants with high occupational position; significant positive association for low occupational position. (D) Significant positive association between hippocampal volume and language for participants with high occupational position; non-significant negative association for low occupational position. (E) Significant positive association between total gray matter volume and language for participants with high occupational position; non-significant negative association for low occupational position.
Participants with amnestic mild cognitive impairment
Moderation analyses for participants with aMCI revealed a significant positive association between hippocampal volume and memory (p < 0.001) and significant positive associations between total gray matter volume and each of the five cognitive domains (ps < 0.001 to p = 0.018). Education moderated the association between total gray matter volume and language (b = 0.13, SE = 0.04, p = 0.003) and memory (b = 0.10, SE = 0.04, p = 0.011). The Johnson–Neyman technique revealed that for both language and memory, there was a significant positive association with total gray matter volume for participants with over 12 years of education that strengthened with increasing education (see Figures 5A,B).
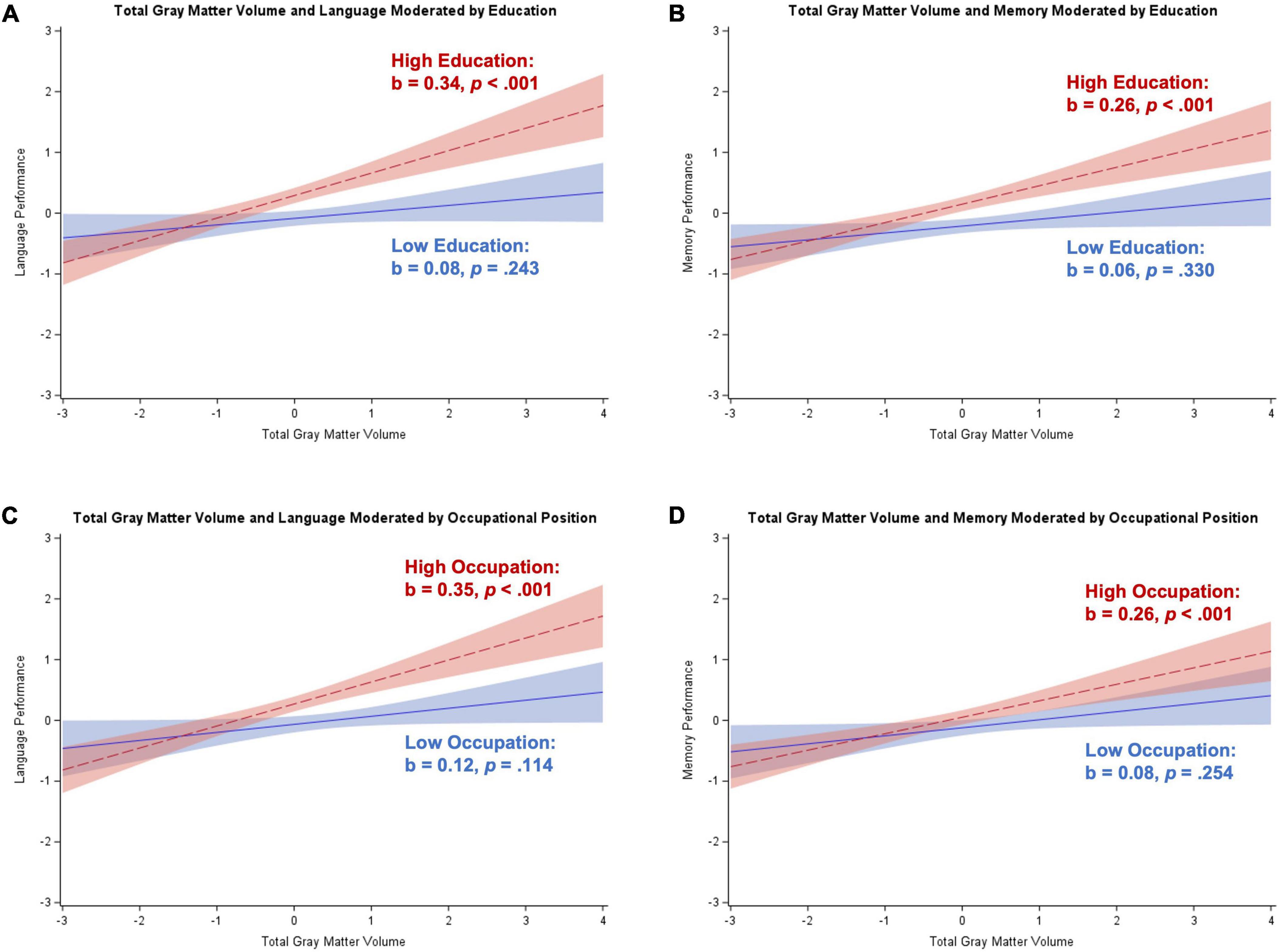
Figure 5. Plots of significant moderations by education and occupational position of the associations between total gray matter volume and cognition for participants with amnestic mild cognitive impairment. High education or occupational position corresponds to 1 SD above the mean and low education or occupational position corresponds to 1 SD below the mean. The red dotted line represents high education or occupational position, and the blue solid line represents low education or occupational position. Shaded areas represent 95% confidence intervals. Cognition and total gray matter volume were standardized. (A) Significant positive association between total gray matter volume and language for participants with high education; non-significant positive association for low education. (B) Significant positive association between total gray matter volume and memory for participants with high education; non-significant positive association for low education. (C) Significant positive association between total gray matter volume and language for participants with high occupational position; non-significant positive association for low occupational position. (D) Significant positive association between total gray matter volume and memory for participants with high occupational position; non-significant positive association for low occupational position.
Occupational position also moderated the association between total gray matter volume and language (b = 0.12, SE = 0.05, p = 0.014) and memory (b = 0.09, SE = 0.04, p = 0.039). The Johnson–Neyman technique revealed that there was a significant positive association between total gray matter volume and both language and memory for participants with at least “services and sales workers” occupations (>4 on scale) that strengthened with increasing occupational position (see Figures 5C,D).
Restricting to participants with data on main lifetime occupation
Restricting our occupational position analyses to participants with data available for main lifetime occupation reduced our sample to 373 participants (311 without dementia; 62 with dementia). For participants without dementia, similar to main analyses, occupational position was positively related to attention/working memory, executive control, language, and memory performance (all ps < 0.001). However, whereas in main analyses occupational position moderated the relationship between total gray matter volume and attention/working memory, language, and memory, analyses restricted to participants with data on main lifetime occupation revealed occupational position moderated the association between hippocampal volume and attention/working memory (b = 0.10, SE = 0.05, p = 0.031) and memory (b = 0.11, SE = 0.05, p = 0.018). Similar to main analyses, higher occupational position magnified the association between brain volume and cognition, such that having a higher occupational position was related to a stronger positive relationship between hippocampal volume and attention/working memory and memory. Thus, in sum, the moderating effect was still present in two of the three original cognitive domains, although it was present for a different brain region.
For participants with dementia, using main lifetime occupation as the proxy (rather than information about main lifetime occupation supplemented with last occupation when main occupation was not available) revealed an interaction between hippocampal volume and occupational position on language performance (b = –0.28, SE = 0.11, p = 0.016). The Johnson–Neyman technique indicated that higher occupational position was related to a stronger negative association between hippocampal volume and language performance. This is similar to effects found in main analyses although for a different cognitive domain.
Assessing the influence of sex on reserve/resilience effects
The main analyses were also conducted separated for men and women in order to observe whether sex influenced the moderating effect of cognitive reserve proxies on the association between brain volume and cognition. Like main analyses, these models were conducted separately for participants without and with dementia. Fully adjusted models controlled for age and depressive symptoms. Analyses for men included 197 participants without dementia and 41 participants with dementia. Analyses for women included 259 participants without dementia and 72 participants with dementia. Table 6 presents results for men and women without dementia and Table 7 presents results for men and women with dementia.
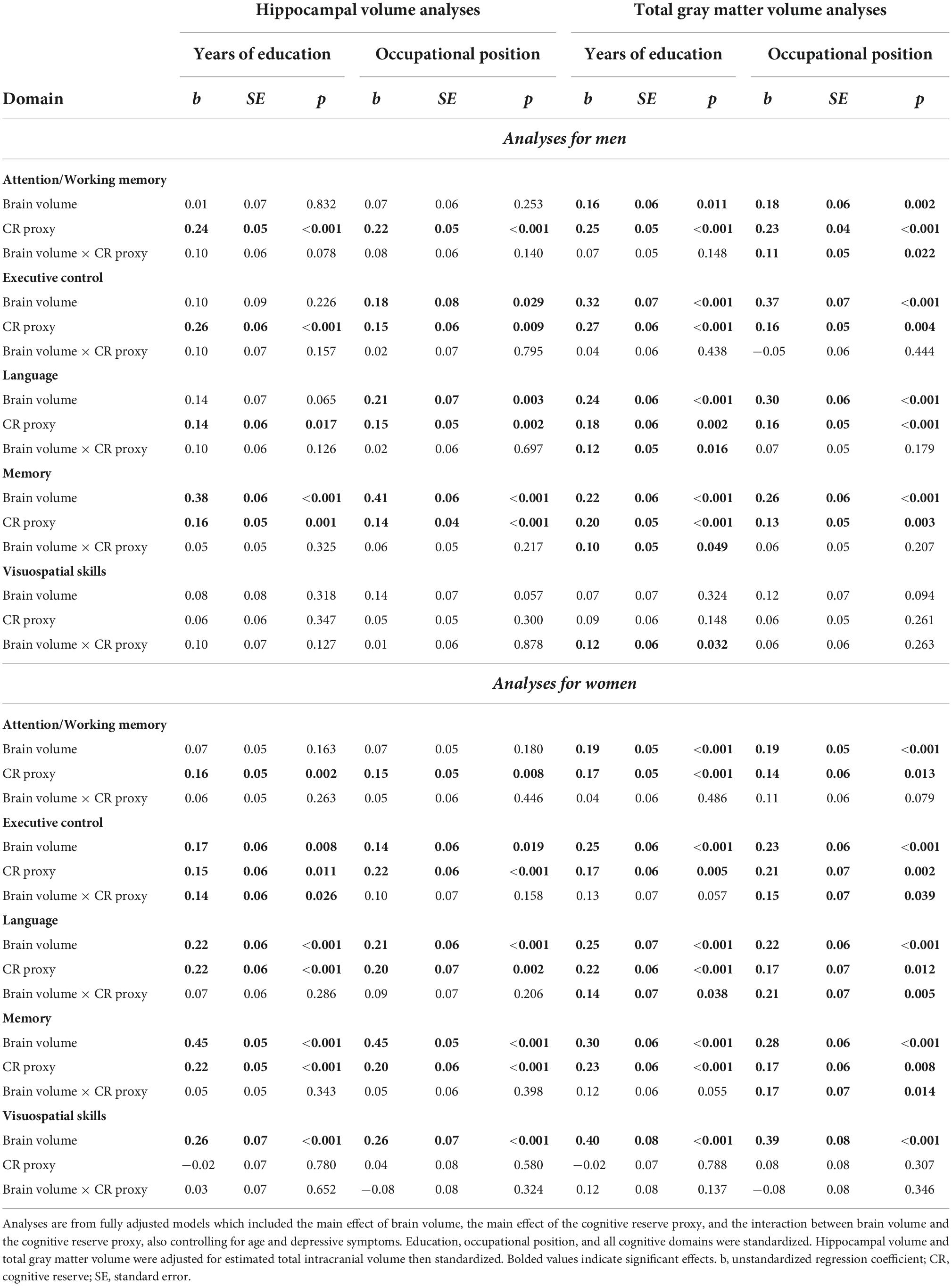
Table 6. Sensitivity moderation analyses for participants without dementia stratified by sex.
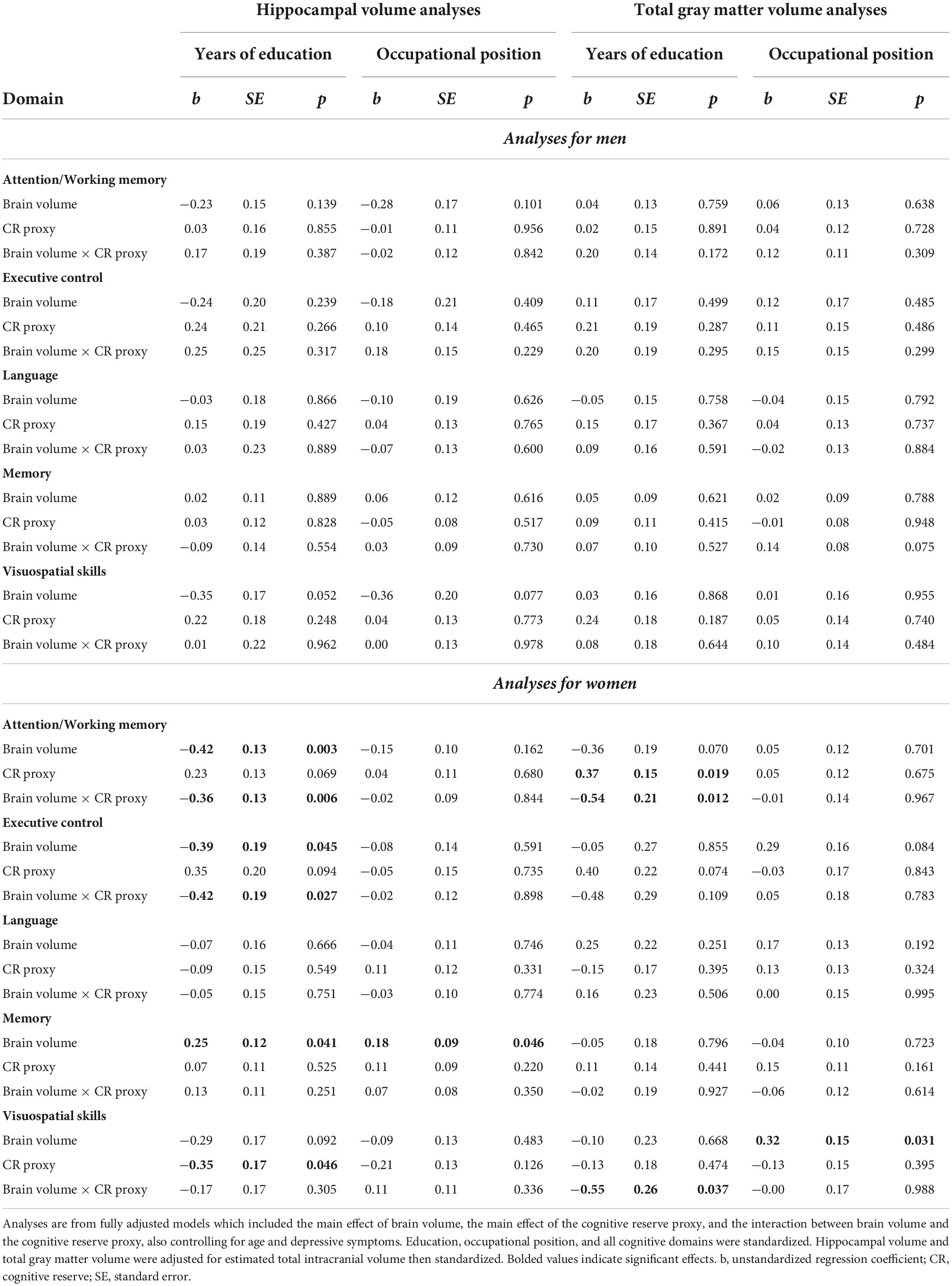
Table 7. Sensitivity moderation analyses for participants with dementia stratified by sex.
Moderation analyses for men
For men without dementia, hippocampal volume was positively related to executive control, language, and memory performance (ps < 0.001 to p = 0.029). Total gray matter volume was positively related to attention/working memory, executive control, language, and memory performance (ps < 0.001 to p = 0.011). Education moderated the association between total gray matter volume and language (b = 0.12, SE = 0.05, p = 0.016), memory (b = 0.10, SE = 0.05, p = 0.049), and visuospatial skills (b = 0.12, SE = 0.06, p = 0.032). The Johnson–Neyman technique revealed that there was a significant positive association between total gray matter volume and cognition starting between 12 and 16 years of education, with the association strengthening with increasing education. These results are illustrated in Figures 6A–C.
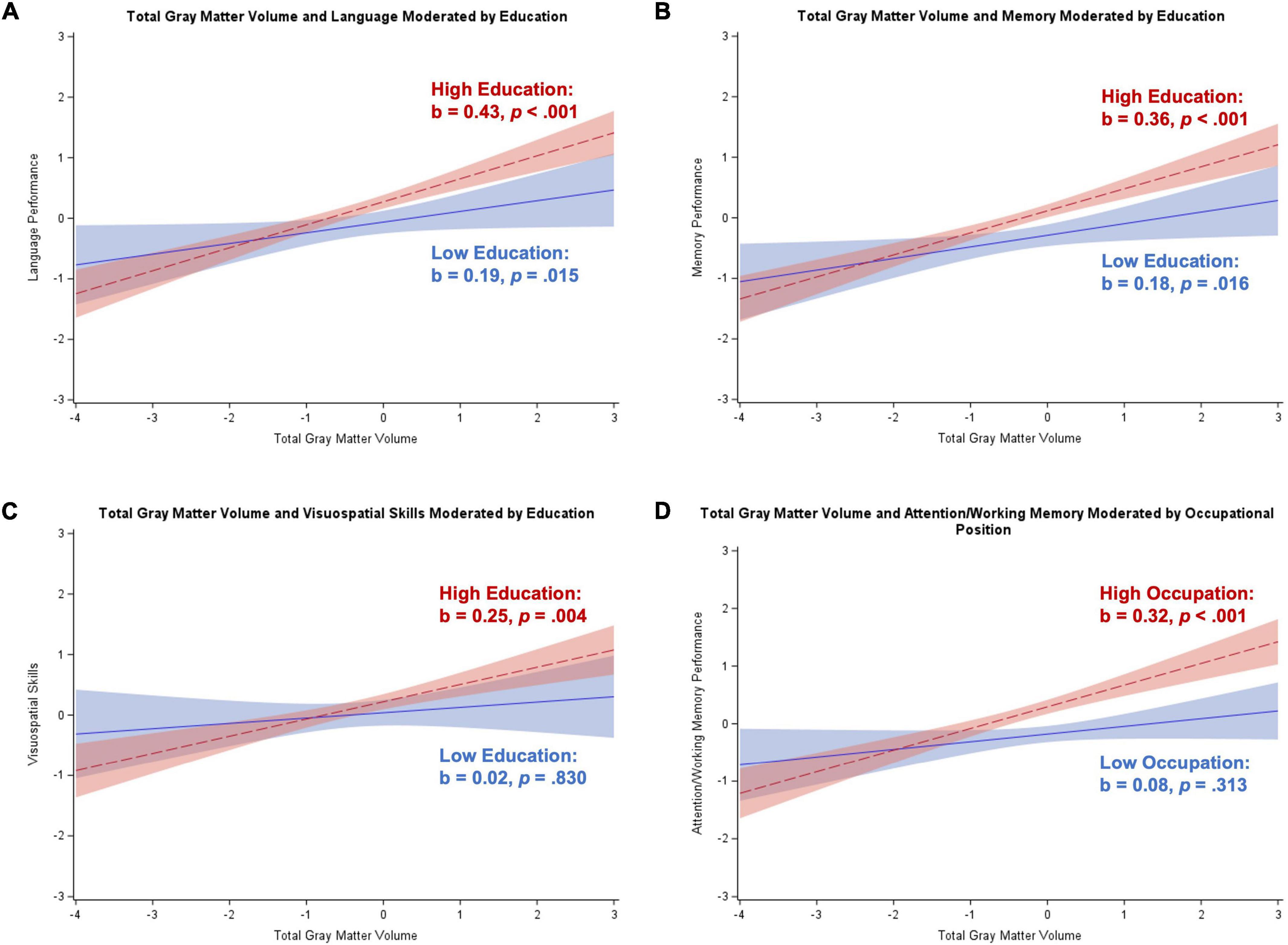
Figure 6. Plots of significant moderations by education and occupational position of the associations between total gray matter volume and cognition for men without dementia. High education or occupational position corresponds to 1 SD above the mean and low education or occupational position corresponds to 1 SD below the mean. The red dotted line represents high education or occupational position, and the blue solid line represents low education or occupational position. Shaded areas represent 95% confidence intervals. Cognition and total gray matter volume were standardized. (A) Significant positive association between total gray matter volume and language for participants with high education; significant positive association for low education. (B) Significant positive association between total gray matter volume and memory for participants with high education; significant positive association for low education. (C) Significant positive association between total gray matter volume and visuospatial skills for participants with high education; non-significant positive association for low education. (D) Significant positive association between total gray matter volume and attention/working memory for participants with high occupational position; non-significant positive association for low occupational position.
Occupational position moderated the association between total gray matter volume and attention/working memory in men without dementia (b = 0.11, SE = 0.05, p = 0.022). The Johnson–Neyman technique revealed that participants with around “clerical support workers” occupations (>4.7 on scale) had a significant positive association between total gray matter volume and attention/working memory that strengthened with increasing occupational position (see Figure 6D). There were no significant main effects or interactions for analyses in men with dementia.
Moderation analyses for women
For women without dementia, hippocampal volume was positively related to executive control, language, memory, and visuospatial skills (ps < 0.001 to p = 0.019). Total gray matter volume was positively related to all five cognitive domains (all ps < 0.001). Education moderated the associations between hippocampal volume and executive control (b = 0.14, SE = 0.06, p = 0.026) and total gray matter volume and language (b = 0.14, SE = 0.07, p = 0.038). The Johnson–Neyman technique revealed that women with greater than 12–13 years of education had a positive association between brain volume and cognition that strengthened with increasing education (see Figures 7A,B).
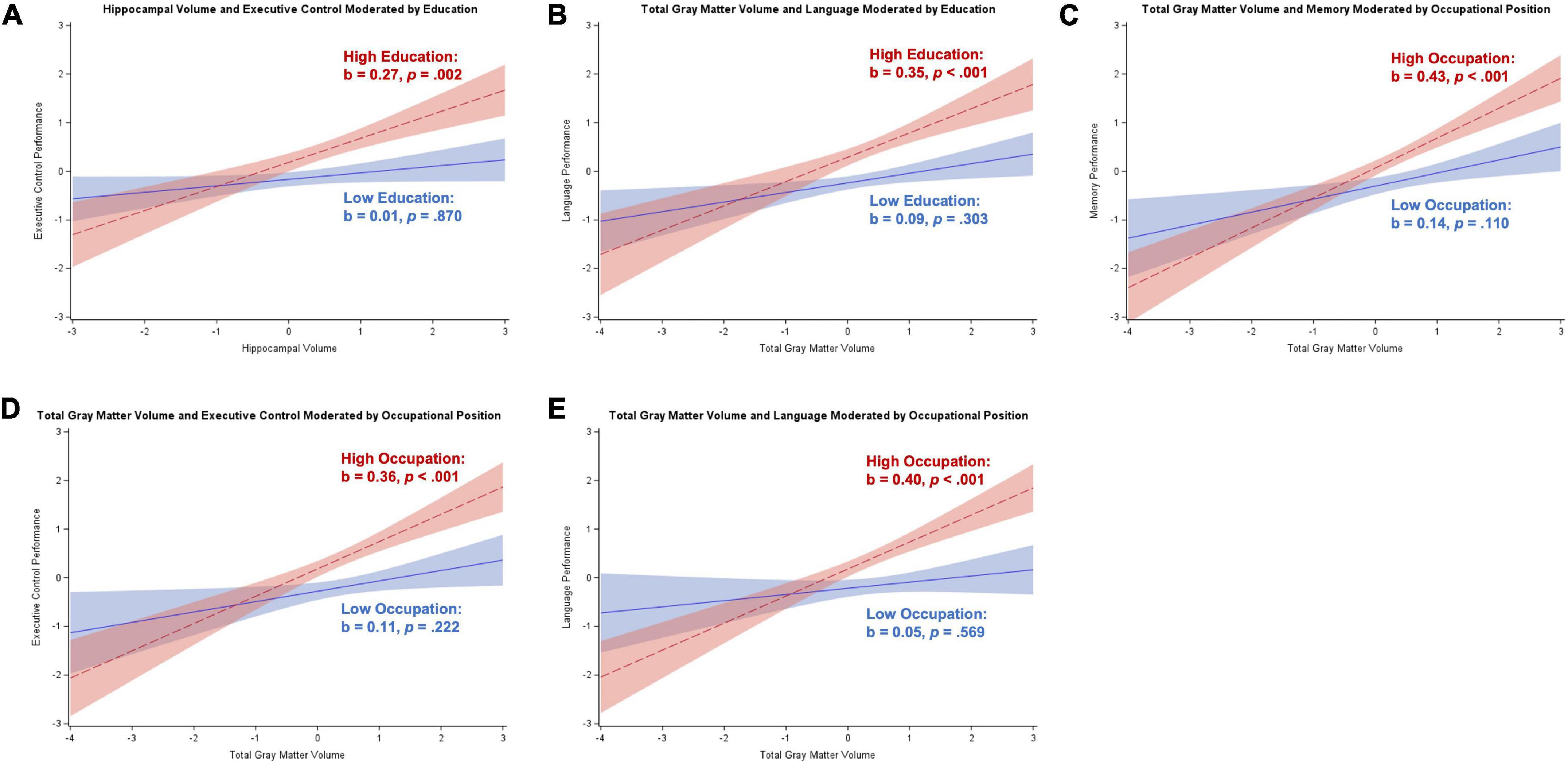
Figure 7. Plots of significant moderations by education and occupational position of the associations between brain volume and cognition for women without dementia. High education or occupational position corresponds to 1 SD above the mean and low education or occupational position corresponds to 1 SD below the mean. The red dotted line represents high education or occupational position, and the blue solid line represents low education or occupational position. Shaded areas represent 95% confidence intervals. Cognition and brain volume were standardized. (A) Significant positive association between hippocampal volume and executive control for participants with high education; non-significant positive association for low education. (B) Significant positive association between total gray matter volume and language for participants with high education; non-significant positive association for low education. (C) Significant positive association between total gray matter volume and memory for participants with high occupational position; non-significant positive association for low occupational position. (D) Significant positive association between total gray matter volume and executive control for participants with high occupational position; non-significant positive association for low occupational position. (E) Significant positive association between total gray matter volume and language for participants with high occupational position; non-significant positive association for low occupational position.
Occupational position moderated the associations between total gray matter volume and executive control (b = 0.15, SE = 0.07, p = 0.039), language (b = 0.21, SE = 0.07, p = 0.005), and memory (b = 0.17, SE = 0.07, p = 0.014). The Johnson–Neyman technique revealed that women with between “services and sales workers” and “clerical support workers” occupations (4–5 on scale) had a significant positive association between total gray matter volume and cognition that strengthened with increasing occupational position (see Figures 7C–E).
For women with dementia, hippocampal volume was negatively related to attention/working memory and executive control and positively related to memory (p = 0.003 to p = 0.046). Total gray matter volume was positively related to visuospatial skills (p = 0.031). Education moderated the associations between hippocampal volume and attention/working memory (b = –0.36, SE = 0.13, p = 0.006) and executive control (b = –0.42, SE = 0.19, p = 0.027), and total gray matter volume and attention/working memory (b = –0.54, SE = 0.21, p = 0.012) and visuospatial skills (b = –0.55, SE = 0.26, p = 0.037). The Johnson–Neyman technique revealed that the relationship between total gray matter volume and attention/working memory and visuospatial skills was positive for women with less than 10–12 years of education that strengthened as education decreased. Additionally, for the brain volume and attention/working memory and executive control relationships, there was a significant negative association for women with between 12 and 15 years of education that strengthened with increasing education. These results are illustrated in Figure 8.
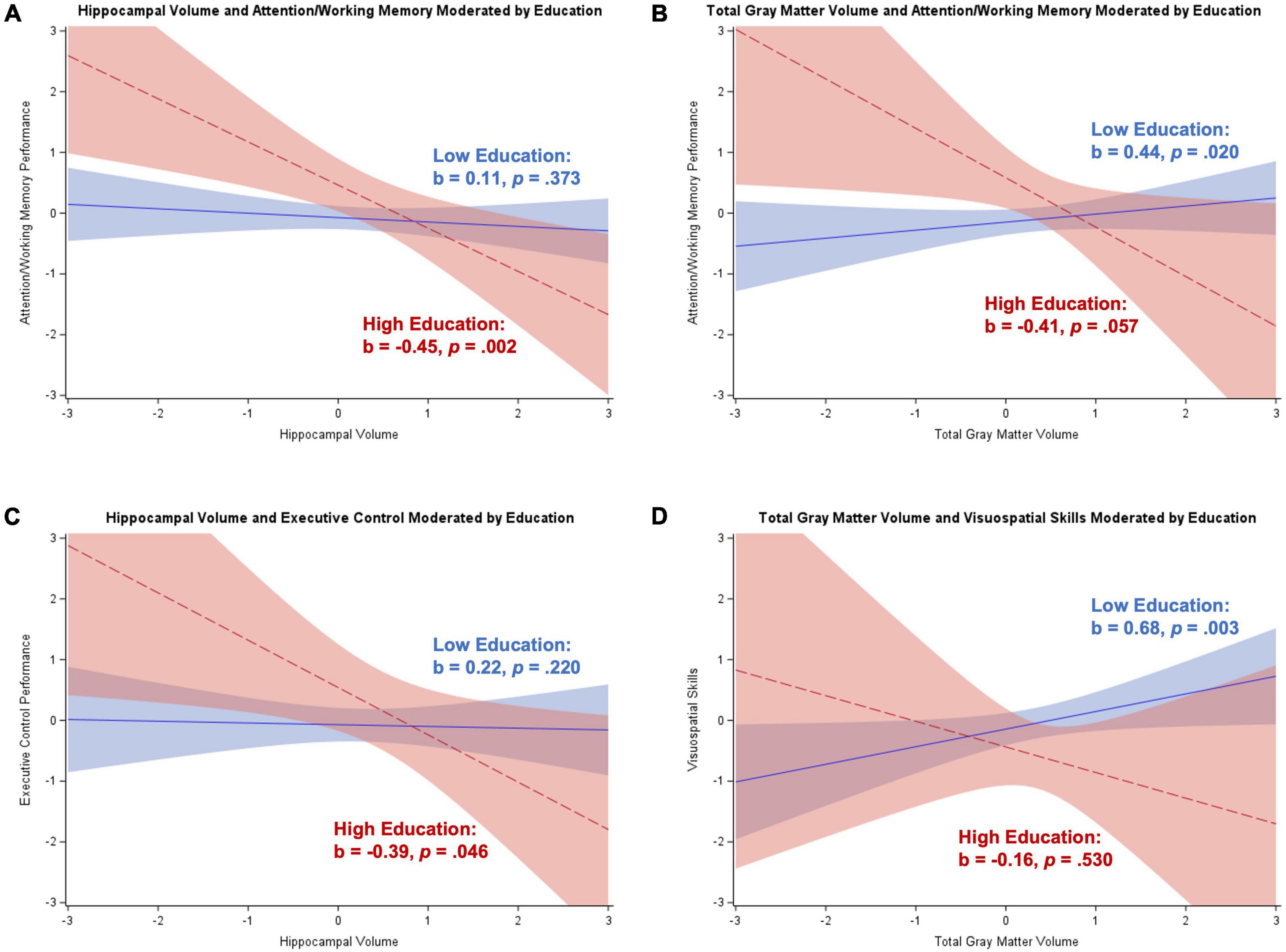
Figure 8. Plots of significant moderations by education of the associations between brain volume and cognition for women with dementia. High education corresponds to 1 SD above the mean and low education corresponds to 1 SD below the mean. The red dotted line represents high education, and the blue solid line represents low education. Shaded areas represent 95% confidence intervals. Cognition and brain volume were standardized. (A) Significant negative association between hippocampal volume and attention/working memory for participants with high education; non-significant positive association for low education. (B) Non-significant negative association between total gray matter volume and attention/working memory for participants with high education; significant positive association for low education. (C) Significant negative association between hippocampal volume and executive control for participants with high education; non-significant positive association for low education. (D) Non-significant negative association between total gray matter volume and visuospatial skills for participants with high education; significant positive association for low education.
Discussion
We examined the moderating effect of cognitive reserve on the association between brain volume and common cognitive domains in participants without dementia (i.e., SCD and aMCI) and with dementia syndrome. Our results indicate that the effect of cognitive reserve on the relationship between brain volume and cognition depends on (a) what diagnostic group is under investigation, (b) what cognitive domain is included, and (c) what is used as the proxy for cognitive reserve. For participants already experiencing cognitive difficulties but who are still free of dementia (i.e., SCD and aMCI), we found some evidence of a protective effect of both education and occupational position, whereby among those with higher cognitive reserve, brain volume and cognitive performance (i.e., attention/working memory, executive control, language, and memory) were more closely related than among those with low cognitive reserve. Therefore, those with high cognitive reserve appeared to be able to utilize available neural resources, when still available despite existing cognitive problems, more efficiently than those with low reserve. Caution is warranted in interpreting these interactions as only the association between total gray matter volume and language was significantly moderated by education after correction for multiple comparisons was applied.
In participants with dementia, typically, high cognitive reserve (in those with high education and/or occupational position) is depleted to a great extent, as often reflected in greater neural loss and accelerated decline compared to patients with dementia with low reserve (Stern, 2002, 2009; Stern et al., 2020). This is described as a compensatory effect, where individuals with high reserve can compensate for neurodegeneration by using cognitive reserve related resources until these are no longer available due to overwhelming neuropathology, when dementia becomes clinically apparent. We found some evidence for this pre-dementia compensatory effect of cognitive reserve, whereby hippocampal volume and total gray matter volume were more beneficial to visuospatial skills among those with less education (Table 4). This may suggest that, after dementia diagnosis, individuals with low (but not high) education can still compensate for advancing neuropathology and perform relatively well when neural resources are available and poorly when they are not. In fact, illustration of the effects estimated separately for low and high education (Figure 2A) suggested that there was a negative association between greater hippocampal volume and poorer visuospatial skills for those with higher education specifically. This effect may be spurious as we would more likely expect a null effect and, in fact, these effects were reduced to null after correction for multiple comparisons. Alternatively, it may be that other biological factors besides hippocampal volume explain this effect. That is, visuospatial performance may be particularly impaired in those with high cognitive reserve (because of more extensive underlying neuropathology at/after dementia onset), but it may not be fully reflected in the measurement of volume alone. Only participants with dementia in the mild to moderate stage of the syndrome were included, where memory impairment dominates. It may be that structures outside of the hippocampus drive differences in visuospatial performance. This explanation is also supported by the fact that the pattern of results seemed to be driven by low education in the total gray matter volume analyses. Age- and disease-related heterogeneity in gray matter atrophy exists (Fjell et al., 2014; Kang et al., 2019), so this global measure of brain integrity may reflect distinct atrophy patterns that could differentially influence visuospatial ability. Previously observed interactions between lifestyle factors, early life exposures, and biological mechanisms (Arenaza-Urquijo and Vemuri, 2018; de Rooij, 2022; Hoenig and Drzezga, 2022) indicate that complex interrelations between cognitive reserve and brain volume may result in different groups of reserve driving patterns found in different brain areas.
According to the cognitive reserve hypothesis (Stern, 2009), the relationship between brain integrity and cognitive performance differs depending on the clinical impairment under investigation. Specifically, individuals without cognitive impairment who have higher reserve can rely on preserved resources. Once clinical impairment sets in, there is a transition from still performing well with extensive neuropathology to the same individuals often exhibiting poorer cognitive performance due to greater underlying neuropathology which progressed to the point where cognitive functions are no longer protected. This relationship maps onto the mechanisms through which cognitive reserve is thought to operate—specifically, neural reserve and neural compensation (Stern, 2009).
Our results indicate that for participants without dementia (i.e., SCD and aMCI), (a) greater brain volume, whether hippocampal or total gray matter volume, was relatively consistently associated with better cognitive scores; (b) in terms of cognitive reserve proxies, both higher educational attainment and higher occupational position were related to better attention/working memory, executive control, language, and memory; and (c) the association between greater neural resources (i.e., hippocampal or total gray matter volume) and better cognitive scores was generally stronger among participants with greater cognitive reserve. Results from supplemental analyses restricted to participants with data available on main lifetime occupation were generally consistent with main analyses.
The significant moderations indicating a stronger relationship between brain volume and cognitive abilities for participants without dementia who had higher cognitive reserve suggest that individuals with higher education or occupational position are better capable of utilizing remaining neural resources to preserve cognitive performance. Particularly the moderation by education of the relationship between hippocampal volume and executive control is intriguing and may have important clinical and practical implications. Measures of executive control are reflective of daily functioning (including instrumental and basic activities of daily living; Vaughan and Giovanello, 2010; Martyr and Clare, 2012) and executive dysfunction has been reported in early AD, where hippocampal volume is particularly relevant (Albert, 1996). Therefore, paying attention to markers of cognitive reserve in determining underlying neurodegeneration in relation to the actual clinical diagnosis of dementia may be particularly important, as those with higher reserve may be more likely to be diagnosed later in their progression through the typical AD-related neuropathological spectrum. However, given the cross-sectional nature of this study, we cannot rule out that the patterns of results could be explained by developmental or other pre-existing differences.
Supplemental analyses separating participants without dementia into SCD and aMCI groups revealed similar results to the analyses in which the two groups were combined, although the moderating effects of cognitive reserve on the brain volume-cognition associations appeared to be more apparent in participants with SCD compared to aMCI. This pattern may suggest that cognitive reserve begins to lose some of the protective effects on cognitive performance as individuals progress through stages of cognitive impairment. Additionally, results for SCD were found for both the hippocampal volume analyses and total gray matter volume analyses whereas for aMCI they were found for total gray matter volume analyses only. Since the hippocampus is affected early along the AD continuum, the lack of effects for aMCI may indicate impairment that has started in the hippocampus but has yet to influence other brain areas.
For participants with dementia, the relationship between greater total gray matter volume and better visuospatial skills was magnified in those with less education, providing evidence for the compensatory aspect of cognitive reserve. There are several plausible explanations for this result. First, individuals with high reserve who may have experienced significant atrophy (leading to less objective brain volume) can compensate for this loss and still perform well cognitively. Second, individuals with high reserve who have objectively greater brain volume, but poorer cognitive performance compared to individuals with low reserve, may have already experienced relatively extensive atrophy compared to their pre-dementia volume. Therefore, even though they appear to have greater absolute volume than the sample average, this presumed volume loss may have contributed to their poor performance on cognitive tests relative to participants with low cognitive reserve. These assumptions should be tested with longitudinal data.
Given that visuospatial skills was the only domain that evidenced a significant moderation, it is possible that the neuropathology experienced in dementia may have been too extensive for participants with high reserve to compensate performance in the other cognitive domains. Still, higher education has also been found to strengthen the effect of total gray matter atrophy on cognitive decline (Mungas et al., 2018), so this pattern may reflect the rapid decline participants with high reserve experience after dementia onset. Sensitivity analyses limited to participants with an AD dementia diagnosis (pure or mixed) did not reveal any significant moderating effects of cognitive reserve on the brain volume-cognition relationship. This may be the result of an underpowered analysis, since the magnitude of effects were similar for the interactions found in main analyses, but these effects did not meet the significance criterion.
The supplemental analyses restricting the sample to participants with data on main lifetime occupation revealed relatively consistent results, except that a significant interaction between hippocampal volume and language appeared. This pattern may suggest that language ability is particularly affected by prolonged exposure to a particular work environment.
We also conducted analyses in participants without and with dementia stratified by sex. Overall, regardless of what domain or proxy was of focus, in men and women without dementia, higher cognitive reserve strengthened the brain volume-cognition relationship. There was one overlapping effect between men and women without dementia (i.e., interaction between total gray matter volume and education on language performance). In men, education moderated the total gray matter volume associations with memory and visuospatial skills, and occupational position moderated the total gray matter volume-attention/working memory relationship. In women, education moderated the association between hippocampal volume and executive control, and occupational position moderated the associations between total gray matter volume and executive control, language, and memory. The magnitude of the interaction effects was slightly stronger in women. In participants with dementia, there were no significant effects found for men, but inverse relationships found between brain volume and cognition for women with high education. Future work should assess sex in relation to cognitive reserve to determine whether these effects replicate.
Interpretation of findings
Our results contribute to the growing field assessing relationships between cognitive reserve, brain health, and cognitive/clinical outcomes by suggesting that both the protective and compensatory components of cognitive reserve seem to be present at different points in clinical impairment. For individuals with higher reserve, there seems to be an inflection point such that before the onset of clinically ascertained dementia, higher reserve is associated with better brain health; cognitive reserve becomes compensatory once neuropathology begins to accumulate allowing individuals to maintain cognitive performance and avoid clinical impairment; and finally individuals with high reserve exhibit accelerated cognitive decline due to the expansive accumulation of neuropathology over time. Our results provide additional evidence for the notion that the transition from cognitive reserve being protective to compensatory may occur at the clinical onset of dementia (Stern et al., 2020). Although our study does not include measures of neuropathology, neurodegeneration is thought to be a downstream process that results from the accumulation of beta-amyloid and tau in the brain, followed by loss of volume. The role of cognitive reserve as protective vs. compensatory against neuropathology may reflect the same underlying process which should be assessed more thoroughly in future work.
A non-linear relationship between brain health and cognitive outcomes among individuals with high reserve may help explain our results and help disentangle the discrepant findings of past research investigating the moderating effect of cognitive reserve on the brain health-cognition relationship. Staekenborg et al. (2020) recently hypothesized this U-shaped relationship between cognitive reserve and neuropathology which also aligns with the model of compensation Gregory et al. (2017) present to understand relationships between cognitive performance and brain volume in neurodegenerative disease. A U-shaped relationship between cognitive reserve, brain volume, and neuropathology supports both (a) the stronger positive relationship between brain volume and cognition for individuals with high reserve prior to the probable appearance of extensive neuropathology and clinical impairment and (b) the attenuated relationship between brain volume and cognitive outcomes for individuals with high reserve after extensive neuropathology has likely accumulated and the compensatory mechanism of reserve is no longer available. Conversely, regarding (a), given the cross-sectional nature of this study, the positive relationship between brain volume and cognition found in participants without dementia could be due to developmental or other pre-existing differences between groups. Regarding (b), we also found evidence of an inverse relationship between brain volume and cognition for participants with high reserve in the dementia group. This may reflect two complementary phenomena: first, individuals with high reserve who have experienced neurodegeneration may still be able to compensate their performance despite the relatively extensive neurodegeneration. This pattern is reflected in Figure 2 where participants with less brain volume than the sample average, but high cognitive reserve, perform better than participants at the same level of brain volume but who have low cognitive reserve. Second, individuals with greater brain volume relative to the sample average and high cognitive reserve may reflect individuals who have experienced extensive neurodegeneration but still have objectively greater brain volume than the sample, impeding on their ability to perform cognitively at the expected level. Finally, our study includes brain volume rather than neuropathology. Since brain atrophy would be farther down the cascade than neuropathological changes including the spread of beta-amyloid and tau in the brain, it is possible that a different pattern results in this downstream measure compared to more immediate neuropathology effects.
Another explanation of divergent findings could revolve around the inclusion of different types of AD neuropathology or brain integrity in studies. Specifically, what is chosen as the marker of AD neuropathology or brain integrity may impact how cognitive reserve influences the pathology-cognition relationship depending on the level of cognitive impairment of the sample. According to the amyloid-cascade hypothesis (Hardy and Higgins, 1992; Karran et al., 2011; Jack and Holtzman, 2013; Jack et al., 2013), the temporal ordering of AD pathophysiology begins with amyloid-beta, followed by tau, and leading to eventual neurodegeneration. Cognitive reserve’s attenuating effect on neuropathology may be better detected by markers of amyloid-beta accumulation in healthy older adults who exhibit no clinical symptoms of dementia or individuals early in the disease progression before significant cognitive decline occurs (Menardi et al., 2018). Subsequently, later pathophysiological markers of AD (i.e., volumetric measures reflecting neurodegeneration) may have a detectable attenuating effect of cognitive reserve on the brain health-cognition relationship once more advanced clinical impairment has occurred. Prior to the appearance of the compensatory mechanism of reserve, associations between brain health and cognitive outcomes may be stronger for individuals with higher levels of reserve compared to lower levels of reserve, representing the neural reserve component of cognitive reserve (Stern, 2009).
Other reasons for the discrepant findings among studies in this area may reflect differences among samples. Sociocultural differences between samples may reflect inconsistent associations between neuropathology and cognition depending on contextual aspects of cognitive reserve proxies. For example, the qualitative aspects of education present in the United States compared to European nations in the 1900s, differences in mandatory or standard educational requirements, and differences in years of education across samples may all contribute to these mixed findings. Similarly, differences in occupational characteristics across culturally distinct geographic regions or occupational opportunities available in certain historical timepoints may also result in disparate findings. Additionally, differences in risk for cognitive decline and dementia are known to exist, yet little is known about how cognitive reserve may relate to these demographic differences. For example, some research suggests that cognitive reserve may operate differently in men and women due to biological or sociocultural differences between the sexes (Rocca, 2017; Ewers, 2020; Subramaniapillai et al., 2021). Investigating these potentially interacting causes of mixed findings is important for future work to better understand what influences individuals’ risk for future impairment.
Strengths, limitations, and future directions
Strengths of the current study include (a) examination of the cognitive reserve hypothesis among different diagnostic groups to assess how cognitive reserve may differentially moderate the association between brain volume and cognition, (b) the use of an extensive neuropsychological battery that allowed for investigation of several cognitive domains, and (c) the inclusion of two commonly used proxies of cognitive reserve. One main weakness is the cross-sectional design which prevented (a) investigation of longitudinal change in cognition or brain volume, (b) causal/directional interpretation of the results, and (c) the disentanglement of the role of cognitive reserve as protective and/or compensatory. Other weaknesses include: low reliability in one of the cognitive domains (i.e., executive control) as indicated by Cronbach’s alpha values, absence of the use of biomarkers in diagnosis, and the use of a sample from one memory clinic in the Czech Republic which could limit generalizability of results. Future research should include participants who exhibit transitions to dementia from normal cognition to assess how moderating effects of cognitive reserve proxies on brain integrity-cognition relationships may weaken as clinical progression, and the associated neurodegeneration, occurs. For example, testing moderating effects of cognitive reserve at different clinical thresholds (i.e., assessing these relationships in the same participants who transition from SCD to aMCI to dementia) would more clearly reveal the extent to which cognitive reserve operates as protective and/or compensatory and how effects differ in each diagnosis. Additionally, further examination of how development versus brain atrophy may influence associations is warranted. Future work should also consider how inclusion of different AD biomarkers and markers of neuropathology may affect how cognitive reserve moderates associations between brain structure and cognitive outcomes. Finally, since our study presents exploratory findings regarding the moderating effect of cognitive reserve in participants with dementia of different etiologies, future research should isolate AD dementia more specifically to verify the robustness of findings.
Implications
By recognizing that cognitive reserve moderates the brain volume-cognition relationship, clinical decisions should incorporate markers of cognitive reserve, which in turn may help clinicians identify the link between the level of brain health and actual cognitive performance. If individuals are known to have low markers for reserve (e.g., low education or occupational position), other proxies of reserve could be offered to these individuals (e.g., increased cognitive or physical leisure activity) to promote brain health. At a population-level, more support could be provided for educational attainment and occupational advancement to promote healthy cognitive aging throughout society.
Conclusion
We provided evidence for cognitive reserve as a moderator of the relationship between brain volume and cognition. This study contributes to the growing evidence that life-course cognitive reserve proxies such as educational attainment and occupational position may play an important role in understanding the association between neural resources, represented by brain volume, and cognition in older adults. The findings also provide unique and new information about the distinct influences of cognitive reserve proxies on the specific associations between brain volume and cognition in participants without and with dementia syndrome.
Data availability statement
The data analyzed in this study is subject to the following licenses/restrictions: Data available to researchers upon request after completing data use agreement. Requests to access these datasets should be directed to JH, amFrdWIuaG9ydEBmbm1vdG9sLmN6.
Ethics statement
The studies involving human participants were reviewed and approved by the Institutional Review Board of Motol University Hospital. The patients/participants provided their written informed consent to participate in this study.
Author contributions
MN: conceptualization, formal analysis, visualization, writing (original draft), and writing (reviewing and editing). BV: conceptualization, formal analysis, and writing (reviewing and editing). RA: conceptualization, formal analysis, supervision, and writing (reviewing and editing). JM and KV: conceptualization, data curation, methodology, and writing (reviewing and editing). HH, ZN, JL, and MV: conceptualization, data curation, funding acquisition, methodology, and writing (reviewing and editing). JH: conceptualization, data curation, funding acquisition, methodology, project administration, and writing (reviewing and editing). All authors contributed to the article and approved the submitted version.
Funding
This work was supported by the project of National Institute for Neurological Research (Programme EXCELES, ID Project No. LX22NPO5107) – Funded by the European Union – Next Generation EU, the Institutional Support of Excellence 2 2. LF UK (Grant No. 6980382), the Czech Science Foundation (GACR) (registration number 22-33968S) to HH, MV, JL, and JH, the Ministry of Health of the Czech Republic (grant number NV 18-04-00346) to ZN, and Charles University, Second Faculty of Medicine (grant PRIMUS 22/MED/011/) to ZN.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Footnotes
References
Albert, M. S. (1996). Cognitive and neurobiologic markers of early Alzheimer disease. Proc. Natl. Acad. Sci. U.S.A. 93, 13547–13551. doi: 10.1073/pnas.93.24.13547
Alzheimer’s Association (2022). What is Alzheimer’s Disease [Online]. Available online at: https://www.alz.org/alzheimers-dementia/what-is-alzheimers (accessed August 1, 2022).
American Psychiatric Association (2000). Diagnostic and statistical manual of mental disorders: DSM-IV-TR. Washington, DC: American Psychiatric Association.
Arenaza-Urquijo, E. M., and Vemuri, P. (2018). Resistance vs resilience to Alzheimer disease: Clarifying terminology for preclinical studies. Neurology 90, 695–703. doi: 10.1212/wnl.0000000000005303
Benedict, R. H. B., Schretlen, D., Groninger, L., Dobraski, M., and Shpritz, B. (1996). Revision of the brief visuospatial memory test: Studies of normal performance, reliability, and validity. Psychol. Assess. 8, 145–153. doi: 10.1037/1040-3590.8.2.145
Bezdicek, O., Motak, L., Axelrod, B. N., Preiss, M., Nikolai, T., Vyhnalek, M., et al. (2012). Czech version of the trail making test: Normative data and clinical utility. Arch. Clin. Neuropsychol. 27, 906–914. doi: 10.1093/arclin/acs084
Bezdicek, O., Stepankova, H., Motak, L., Axelrod, B. N., Woodard, J. L., Preiss, M., et al. (2014). Czech version of rey auditory verbal learning test: Normative data. Aging Neuropsychol. Cogn. 21, 693–721. doi: 10.1080/13825585.2013.865699
Butters, M. A., Young, J. B., Lopez, O., Aizenstein, H. J., Mulsant, B. H., Reynolds, C. F. III, et al. (2008). Pathways linking late-life depression to persistent cognitive impairment and dementia. Dialogues Clin. Neurosci. 10, 345–357. doi: 10.31887/DCNS.2008.10.3/mabutters
de Rooij, S. R. (2022). Are brain and cognitive reserve shaped by early life circumstances? Front. Neurosci. 16:825811. doi: 10.3389/fnins.2022.825811
Ewers, M. (2020). Reserve in Alzheimer’s disease: Update on the concept, functional mechanisms and sex differences. Curr. Opin. Psychiatry 33, 178–184. doi: 10.1097/yco.0000000000000574
Fischl, B., Salat, D. H., Busa, E., Albert, M., Dieterich, M., Haselgrove, C., et al. (2002). Whole brain segmentation: Automated labeling of neuroanatomical structures in the human brain. Neuron 33, 341–355. doi: 10.1016/s0896-6273(02)00569-x
Fjell, A. M., McEvoy, L., Holland, D., Dale, A. M., and Walhovd, K. B. (2014). What is normal in normal aging? Effects of aging, amyloid and Alzheimer’s disease on the cerebral cortex and the hippocampus. Prog. Neurobiol. 117, 20–40. doi: 10.1016/j.pneurobio.2014.02.004
Goodglass, H., Kaplan, E., and Weintraub, S. (1983). Boston naming test. Washington, D.C: Lea & Febiger.
Gregory, S., Long, J. D., Klöppel, S., Razi, A., Scheller, E., Minkova, L., et al. (2017). Operationalizing compensation over time in neurodegenerative disease. Brain 140, 1158–1165. doi: 10.1093/brain/awx022
Hardy, J. A., and Higgins, G. A. (1992). Alzheimer’s disease: The amyloid cascade hypothesis. Science 256, 184–185. doi: 10.1126/science.1566067
Hayes, A. F., and Little, T. D. (2018). Introduction to mediation, moderation, and conditional process analysis: A regression-based approach. New York, NY: Guilford Publications.
Hoenig, M. C., and Drzezga, A. (2022). Clear-headed into old age: Resilience and resistance against brain aging-A PET imaging perspective. J. Neurochem. 1–21. doi: 10.1111/jnc.15598
International Labour Office (2012). International standard classification of occupations 2008 (ISCO-08): Structure, group definitions and correspondence tables. Geneva: International Labour Office.
Jack, C. R. Jr., and Holtzman, D. M. (2013). Biomarker modeling of Alzheimer’s disease. Neuron 80, 1347–1358. doi: 10.1016/j.neuron.2013.12.003
Jack, C. R. Jr., Knopman, D. S., Jagust, W. J., Petersen, R. C., Weiner, M. W., Aisen, P. S., et al. (2013). Tracking pathophysiological processes in Alzheimer’s disease: An updated hypothetical model of dynamic biomarkers. Lancet Neurol. 12, 207–216. doi: 10.1016/s1474-4422(12)70291-0
Jessen, F., Amariglio, R. E., van Boxtel, M., Breteler, M., Ceccaldi, M., Chetelat, G., et al. (2014). A conceptual framework for research on subjective cognitive decline in preclinical Alzheimer’s disease. Alzheimers Dement 10, 844–852. doi: 10.1016/j.jalz.2014.01.001
Joannette, M., Bocti, C., Dupont, P. S., Lavallée, M. M., Nikelski, J., Vallet, G. T., et al. (2020). Education as a moderator of the relationship between episodic memory and amyloid load in normal aging. J Gerontol. A Biol. Sci. Med. Sci. 75, 1820–1826. doi: 10.1093/gerona/glz235
Johnson, P. O., and Fay, L. C. (1950). The Johnson-Neyman technique, its theory and application. Psychometrika 15, 349–367. doi: 10.1007/bf02288864
Kang, D. W., Lim, H. K., Joo, S. H., Lee, N. R., and Lee, C. U. (2019). Differential associations between volumes of atrophic cortical brain regions and memory performances in early and late mild cognitive impairment. Front. Aging Neurosci. 11:245. doi: 10.3389/fnagi.2019.00245
Karran, E., Mercken, M., and De Strooper, B. (2011). The amyloid cascade hypothesis for Alzheimer’s disease: An appraisal for the development of therapeutics. Nat .Rev. Drug. Discov. 10, 698–712. doi: 10.1038/nrd3505
Kerbler, G. M., Nedelska, Z., Fripp, J., Laczó, J., Vyhnalek, M., Lisý, J., et al. (2015). Basal forebrain atrophy contributes to allocentric navigation impairment in Alzheimer’s Disease patients. Front. Aging Neurosci. 7:185. doi: 10.3389/fnagi.2015.00185
Lee, D. H., Lee, P., Seo, S. W., Roh, J. H., Oh, M., Oh, J. S., et al. (2019). Neural substrates of cognitive reserve in Alzheimer’s disease spectrum and normal aging. Neuroimage 186, 690–702. doi: 10.1016/j.neuroimage.2018.11.053
Martyr, A., and Clare, L. (2012). Executive function and activities of daily living in Alzheimer’s disease: A correlational meta-analysis. Dement Geriatr. Cogn. Disord. 33, 189–203. doi: 10.1159/000338233
Mazancova, A. F., Nikolai, T., Stepankova, H., Kopecek, M., and Bezdicek, O. (2017). The reliability of clock drawing test scoring systems modeled on the normative data in healthy aging and nonamnestic mild cognitive impairment. Assessment 24, 945–957. doi: 10.1177/1073191116632586
McKeith, I. G., Boeve, B. F., Dickson, D. W., Halliday, G., Taylor, J. P., Weintraub, D., et al. (2017). Diagnosis and management of dementia with Lewy bodies: Fourth consensus report of the DLB Consortium. Neurology 89, 88–100. doi: 10.1212/wnl.0000000000004058
McKhann, G. M., Knopman, D. S., Chertkow, H., Hyman, B. T., Jack, C. R. Jr., Kawas, C. H., et al. (2011). The diagnosis of dementia due to Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement 7, 263–269. doi: 10.1016/j.jalz.2011.03.005
Menardi, A., Pascual-Leone, A., Fried, P. J., and Santarnecchi, E. (2018). The role of cognitive reserve in alzheimer’s disease and aging: A Multi-modal imaging review. J. Alzheimers Dis. 66, 1341–1362. doi: 10.3233/jad-180549
Meyers, J. E., and Meyers, K. R. (1995). Rey complex figure test and recognition trial (RCFT). Odessa, FL: Psychological Assessment Resources.
Michaud, T. L., Su, D., Siahpush, M., and Murman, D. L. (2017). The risk of incident mild cognitive impairment and progression to dementia considering mild cognitive impairment subtypes. Dement Geriatr. Cogn. Dis. Extra. 7, 15–29. doi: 10.1159/000452486
Mungas, D., Gavett, B., Fletcher, E., Farias, S. T., DeCarli, C., and Reed, B. (2018). Education amplifies brain atrophy effect on cognitive decline: Implications for cognitive reserve. Neurobiol. Aging 68, 142–150. doi: 10.1016/j.neurobiolaging.2018.04.002
Nedelska, Z., Andel, R., Laczo, J., Vlcek, K., Horinek, D., Lisy, J., et al. (2012). Spatial navigation impairment is proportional to right hippocampal volume. Proc. Natl. Acad. Sci. U.S.A. 109, 2590–2594. doi: 10.1073/pnas.1121588109
Nikolai, T., Stepankova, H., Kopecek, M., Sulc, Z., Vyhnalek, M., and Bezdicek, O. (2018). The uniform data set, czech version: Normative data in older adults from an international perspective. J. Alzheimers Dis. 61, 1233–1240. doi: 10.3233/JAD-170595
Nikolai, T., Štěpánková, H., Michalec, J., Bezdíček, O., Horáková, K., Marková, H., et al. (2015). Testy verbální fluence, èeská normativní studie pro osoby vyššího věku. Česká a slovenská neurologie a neurochirurgie 111, 292–299.
O’Shea, D. M., Langer, K., Woods, A. J., Porges, E. C., Williamson, J. B., O’Shea, A., et al. (2018). Educational attainment moderates the association between hippocampal volumes and memory performances in healthy older adults. Front. Aging Neurosci. 10:361. doi: 10.3389/fnagi.2018.00361
Osterrieth, P. (1944). Le test de copie d’une figure complexe [The test of copying a complex figure]. Arch. Psychol. 30, 206–356. doi: 10.1016/j.psychres.2005.10.012
Pa, J., Aslanyan, V., Casaletto, K. B., Rentería, M. A., Harrati, A., Tom, S. E., et al. (2022). Effects of sex, APOE4, and lifestyle activities on cognitive reserve in older adults. Neurology 99:e789. doi: 10.1212/WNL.0000000000200675
Peltz, C. B., Corrada, M. M., Berlau, D. J., and Kawas, C. H. (2011). Incidence of dementia in oldest-old with amnestic MCI and other cognitive impairments. Neurology 77, 1906–1912. doi: 10.1212/WNL.0b013e318238ee89
Petersen, R. C. (2004). Mild cognitive impairment as a diagnostic entity. J. Intern. Med. 256, 183–194. doi: 10.1111/j.1365-2796.2004.01388.x
Petersen, R. C., Roberts, R. O., Knopman, D. S., Boeve, B. F., Geda, Y. E., Ivnik, R. J., et al. (2009). Mild cognitive impairment: Ten years later. Arch. Neurol. 66, 1447–1455. doi: 10.1001/archneurol.2009.266
Rascovsky, K., Hodges, J. R., Knopman, D., Mendez, M. F., Kramer, J. H., Neuhaus, J., et al. (2011). Sensitivity of revised diagnostic criteria for the behavioural variant of frontotemporal dementia. Brain 134(Pt 9), 2456–2477. doi: 10.1093/brain/awr179
Rocca, W. A. (2017). Time, sex, gender, history, and dementia. Alzheimer Dis. Assoc. Disord. 31, 76–79. doi: 10.1097/wad.0000000000000187
Román, G. C., Tatemichi, T. K., Erkinjuntti, T., Cummings, J. L., Masdeu, J. C., Garcia, J. H., et al. (1993). Vascular dementia: Diagnostic criteria for research studies. Report of the NINDS-AIREN International Workshop. Neurology 43, 250–260. doi: 10.1212/wnl.43.2.250
Sheardova, K., Vyhnalek, M., Nedelska, Z., Laczo, J., Andel, R., Marciniak, R., et al. (2019). Czech Brain Aging Study (CBAS): Prospective multicentre cohort study on risk and protective factors for dementia in the Czech Republic. BMJ Open 9:e030379. doi: 10.1136/bmjopen-2019-030379
Staekenborg, S. S., Kelly, N., Schuur, J., Koster, P., Scherder, E., Tielkes, C. E. M., et al. (2020). Education as proxy for cognitive reserve in a large elderly memory clinic: ‘Window of Benefit’. J. Alzheimers Dis. 76, 671–679. doi: 10.3233/jad-191332
Stern, Y. (2002). What is cognitive reserve? Theory and research application of the reserve concept. J. Intl. Neuropsychol. Soc. 8, 448–460.
Stern, Y., Arenaza-Urquijo, E. M., Bartrés-Faz, D., Belleville, S., Cantilon, M., Chetelat, G., et al. (2020). Whitepaper: Defining and investigating cognitive reserve, brain reserve, and brain maintenance. Alzheimers Dement 16, 1305–1311. doi: 10.1016/j.jalz.2018.07.219
Subramaniapillai, S., Almey, A., Natasha Rajah, M., and Einstein, G. (2021). Sex and gender differences in cognitive and brain reserve: Implications for Alzheimer’s disease in women. Front. Neuroendocrinol. 60:100879. doi: 10.1016/j.yfrne.2020.100879
Sundermann, E. E., Maki, P. M., Rubin, L. H., Lipton, R. B., Landau, S., and Biegon, A. (2016). Female advantage in verbal memory: Evidence of sex-specific cognitive reserve. Neurology 87, 1916–1924. doi: 10.1212/wnl.0000000000003288
Vaughan, L., and Giovanello, K. (2010). Executive function in daily life: Age-related influences of executive processes on instrumental activities of daily living. Psychol. Aging 25, 343–355. doi: 10.1037/a0017729
Voevodskaya, O., Simmons, A., Nordenskjöld, R., Kullberg, J., Ahlström, H., Lind, L., et al. (2014). The effects of intracranial volume adjustment approaches on multiple regional MRI volumes in healthy aging and Alzheimer’s disease. Front. Aging Neurosci. 6:264. doi: 10.3389/fnagi.2014.00264
Keywords: executive control, attention/working memory, language, MRI, visuospatial skills
Citation: Nelson ME, Veal BM, Andel R, Martinkova J, Veverova K, Horakova H, Nedelska Z, Laczó J, Vyhnalek M and Hort J (2022) Moderating effect of cognitive reserve on brain integrity and cognitive performance. Front. Aging Neurosci. 14:1018071. doi: 10.3389/fnagi.2022.1018071
Received: 12 August 2022; Accepted: 14 October 2022;
Published: 03 November 2022.
Edited by:
Anja Soldan, Johns Hopkins University, United StatesReviewed by:
Jeremy Andrew Elman, Department of Psychiatry, School of Medicine, University of California, San Diego, United StatesColin Groot, Lund University, Sweden
Copyright © 2022 Nelson, Veal, Andel, Martinkova, Veverova, Horakova, Nedelska, Laczó, Vyhnalek and Hort. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Monica E. Nelson, bW5lbHNvbjEwQHVzZi5lZHU=