
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Aging Neurosci. , 14 April 2015
Sec. Alzheimer's Disease and Related Dementias
Volume 7 - 2015 | https://doi.org/10.3389/fnagi.2015.00048
 Liang Zhan1,2*†
Liang Zhan1,2*† Jiayu Zhou3,4†
Jiayu Zhou3,4† Yalin Wang3
Yalin Wang3 Yan Jin1
Yan Jin1 Neda Jahanshad1
Neda Jahanshad1 Gautam Prasad1
Gautam Prasad1 Talia M. Nir1
Talia M. Nir1 Cassandra D. Leonardo1
Cassandra D. Leonardo1 Jieping Ye3,4
Jieping Ye3,4 Paul M. Thompson1,2* for the Alzheimer’s Disease Neuroimaging Initiative‡
Paul M. Thompson1,2* for the Alzheimer’s Disease Neuroimaging Initiative‡Alzheimer’s disease (AD) involves a gradual breakdown of brain connectivity, and network analyses offer a promising new approach to track and understand disease progression. Even so, our ability to detect degenerative changes in brain networks depends on the methods used. Here we compared several tractography and feature extraction methods to see which ones gave best diagnostic classification for 202 people with AD, mild cognitive impairment or normal cognition, scanned with 41-gradient diffusion-weighted magnetic resonance imaging as part of the Alzheimer’s Disease Neuroimaging Initiative (ADNI) project. We computed brain networks based on whole brain tractography with nine different methods – four of them tensor-based deterministic (FACT, RK2, SL, and TL), two orientation distribution function (ODF)-based deterministic (FACT, RK2), two ODF-based probabilistic approaches (Hough and PICo), and one “ball-and-stick” approach (Probtrackx). Brain networks derived from different tractography algorithms did not differ in terms of classification performance on ADNI, but performing principal components analysis on networks helped classification in some cases. Small differences may still be detectable in a truly vast cohort, but these experiments help assess the relative advantages of different tractography algorithms, and different post-processing choices, when used for classification.
Alzheimer’s disease (AD) – the commonest form of dementia – is characterized by memory loss in its early stages, typically followed by a progressive decline in other cognitive domains (Braak and Braak, 1996; Bartzokis, 2011; Braskie et al., 2011; Hua et al., 2013). Recent models of AD suggest that cognitive deficits arise from the progressive disconnection of cortical and subcortical regions, involving neuronal loss and white matter (WM) injury (Delbeuck et al., 2003). Several magnetic resonance imaging (MRI) analysis methods can track structural atrophy. Diffusion-weighted MRI (DWI), a variant of standard anatomical MRI, is sensitive to microscopic WM injury not always detectable with standard anatomical MRI. DWI tracks anisotropic water diffusion along axons, revealing microstructural WM fiber bundles connecting cortical and subcortical regions. With whole-brain tractography, one can reconstruct major fiber bundles in the brain’s anatomical network (LeBihan, 1990). In both AD and mild cognitive impairment (MCI), diffusion MRI studies have associated cognitive impairment with progressive deterioration in the corpus callosum, cingulum, superior longitudinal fasciculus, and fornix (Medina et al., 2006; Stebbins and Murphy, 2009; Liu et al., 2011; Daianu et al., 2013; Nir et al., 2013; Jin et al., 2015).
Many studies of brain disease – not just AD – use whole-brain tractography to assess large-scale connections in the brain. Tractography is a method used to reconstruct the pathways of major WM fiber bundles, by fitting a curved path through the directional diffusion data at each voxel. Tractography can reveal brain abnormalities in multiple sclerosis (Mesaros et al., 2012), a variety of cognitive disorders (Catani, 2006), Parkinson’s disease (García-Gomar et al., 2013), brain trauma (Dennis et al., 2015b), psychiatric conditions such as body dysmorphic disorder (Arienzo et al., 2013), and even in genetics (Jin et al., 2011, 2013). To assess these differences, dozens of tractography algorithms have been developed (Behrens et al., 2007; Kreher et al., 2008; Fillard et al., 2009) but there is little consensus on which method is the best to use, and this may also depend on the goal of the study. To the best of our knowledge, no empirical studies have compared tractography methods for studies of brain disease.
There are two main steps in the tractography: the first is to fit a diffusion model at each voxel of the image, and the second is fiber tracking across voxels. The most straightforward way is to use the standard tensor model, which requires at least six diffusion-weighted images (DWIs) and one baseline (non-diffusion-weighted) image to estimate the six unknown parameters of the tensor. The local dominant fiber direction at each voxel is then estimated as the eigenvector associated with the largest eigenvalue of the tensor. Fibers can be followed across voxels using greedy algorithms such as “fiber assignment by continuous tracking” (FACT), which builds streamlines1 across the image by following the diffusion tensors’ principal eigenvectors in the current direction of propagation (Mori et al., 1999). More complex models, based on multiple tensors, orientation distribution functions (ODFs), or “ball-and-stick” models, can extract multiple fiber directions per voxel.
The two main classes of fiber tracking methods are deterministic and probabilistic approach. Deterministic methods tend to be simple and fast. One of the first deterministic tractography approaches, FACT, can be run on a 3D brain image in several minutes. Probabilistic algorithms may require longer computation times. On a single processor, it typically takes several hours to run the Hough method (Aganj et al., 2011), one of the probabilistic algorithms, which fits vast numbers of polynomial curves through an ODF and tends to find the most dominant tracts of the brain using global optimization. Clearly, different algorithms recover different sets of fibers (Zhan et al., 2013b; Dennis et al., 2015a), and the fiber bundles that best differentiate patients from controls may be extracted by some algorithms but not others. When applied to detect brain differences in disease, it is not clear how tractography algorithms differ or if some are more sensitive to differences than others. This depends on which fibers are extracted and how accurately, the level of extraneous fibers and noise, and whether the fiber bundles affected most by the disease are extracted or missed.
Some prior studies compared different tractography algorithms for accuracy and robustness to image noise (Lazar and Alexander, 2003; Huang et al., 2004; Moldrich et al., 2010; Fillard et al., 2011). In Lazar and Alexander (2003), a Monte Carlo simulation was used to study the influence of principal direction estimation and streamline integration methods on the robustness to noise of DTI tractography. Fillard et al. (2011) used a hardware phantom to compare 10 fiber reconstruction methods at different signal-to-noise (SNR) levels. Phantom-based evaluations use simple tract shapes, which tend to be more regular than tracts in the living brain. Huang et al. (2004) created several noisy versions of a high-SNR mouse brain dataset to compare fiber bundle selection strategies. Moldrich et al. (2010) tested several tractography algorithms for studying WM pathways in the ex vivo mouse brain. Using deterministic and probabilistic algorithms across a range of regions of interest, they found that probabilistic tractography was more robust than deterministic tractography for visualizing both white and gray matter (GM) pathways. Moreover, as far as we know, no empirical studies have compared tractography methods for studies of brain disease.
Based on tractography, there at least two common ways that the integrity and connectivity of WM can be studied, i.e., the analysis of individual anatomically meaningful tracts (Jin et al., 2012, 2014) and the connectivity strength between parcellated GM regions (Zhan et al., 2012a,b, 2015). In the latter, brain connectivity maps (structural networks) are often computed by combining the tracts with an anatomical parcellation scheme (Jahanshad et al., 2011; Zhan et al., 2013b). Before further analysis, the brain networks can be thresholded, to keep only those connections with a weight or value, for example nodal degree (number of connections), higher than a given threshold. Network analysis of these brain connectivity matrices can reveal organizational properties of brain networks. Clearly, the tractography and feature extraction method choices affect how well we can identify disease-related differences. To understand how these choices affect how well we can detect effects of AD, we applied nine tractography methods to the Alzheimer’s Disease Neuroimaging Initiative (ADNI) dataset, and investigated five feature extraction approaches on the computed networks. Our goal was to evaluate the performance of different tractography and feature extraction methods. Rather than test their anatomical accuracy, we focused on their ability to detect disease-related effects.
Data used in preparing this article were obtained from ADNI2, the second stage of the Northern American ADNI2. ADNI’s primary goal is to test whether serial MRI, positron emission tomography (PET), other biological markers, and clinical and neuropsychological assessments can be combined to measure the progression of MCI and early AD. For up-to-date information, please see http://www.adni-info.org.
In our experiments, we analyzed 202 subjects’ diffusion MRI and structural MRI data collected from 16 sites across the United States and Canada for the ADNI2 project. Note that only around one third of the ADNI2 participants have diffusion MRI scans, and the other two-thirds are scanned with resting state functional MRI or arterial spin labeling (ASL). Detailed inclusion and exclusion criteria are found in the ADNI2 protocol3. Subjects are divided into three broad diagnostic categories: normal elderly controls (NCs), people with MCI and patients with AD. Subject demographics are summarized in Table 1.
TABLE 1. Summary of ADNI data used in this study.
Each subject underwent whole-brain MRI scanning on 3-Tesla GE Medical Systems scanners. T1-weighted SPGR (spoiled gradient echo) sequences (256 x 256 matrix; voxel size = 1.2 × 1.0 × 1.0 mm3; TI = 400 ms; TR = 6.98 ms; TE = 2.85 ms; flip angle = 11°), were collected as well as DWI (128 × 128 matrix; voxel size: 2.7 × 2.7 × 2.7 mm3; scan time = 9 min; more imaging details may be found at http://adni.loni.usc.edu/wp-content/uploads/2010/05/ADNI2_GE_3T_22.0_T2.pdf). 46 separate images were acquired for each DWI scan: five T2-weighted images with no diffusion sensitization (b0 images) and 41 DWIs (b = 1000 s/mm2). The DWI protocol for ADNI was chosen after a detailed evaluation of different protocols that could be performed in a reasonable amount of time; we reported these comparisons previously (Jahanshad et al., 2010; Zhan et al., 2013a). All T1-weighted MR and DWI images were checked visually for quality assurance to exclude scans with excessive motion and/or artifacts; all scans were included.
We evaluated several tractography and feature extraction choices, and how well they detect disease effects in ADNI2. Figure 1 illustrates the overall study design, which is detailed in Section “Preprocessing to Statistical Analysis.”

FIGURE 1. Flow chart describing the steps taken in this study to create, analyze, and compare structural networks.
For each subject, extra-cerebral tissue was removed from the T1-weighted anatomical scans using ROBEX, a robust automated brain extraction program trained on manually “skull-stripped” MRI data (Iglesias et al., 2011). Skull-stripped volumes were visually inspected, and manually edited if needed. Anatomical scans then underwent intensity inhomogeneity normalization using the MNI nu_correct tool4. To align data from different subjects into the same 3D coordinate space, each anatomical image was linearly aligned to a standard brain template (the Colin27; Holmes et al., 1998) using FSL flirt (Jenkinson et al., 2002).
Then each subject’s raw DWI volumes were aligned to the b0 image using the FSL eddy-correct tool5 to correct for head motion and eddy current distortions. The gradient table was also corrected accordingly. Non-brain tissue was removed from the DWIs using the Brain Extraction Tool (BET) from FSL (Smith, 2002). To correct for echo-planar induced (EPI) susceptibility artifacts, which can cause distortions at tissue-fluid interfaces, skull-stripped b0 images were linearly aligned and then elastically registered to their respective preprocessed T1-weighted structural scans using an inverse consistent registration algorithm with a mutual information cost function (Leow et al., 2007). The resulting 3D deformation fields were then applied to the remaining 41 DWI volumes to generate full preprocessed DWI dataset for the downstream computation.
Nine different tractography methods were evaluated, including deterministic and probabilistic approaches. Among the deterministic methods were four tensor-based deterministic algorithms: FACT (Mori et al., 1999), the second-order Runge–Kutta (RK2) method (Basser et al., 2000), the tensorline (TL; Lazar et al., 2003) and interpolated streamline (SL) methods (Conturo et al., 1999) and two deterministic tractography algorithms based on fourth order spherical harmonic derived ODFs – FACT and RK2. We also tested three probabilistic approaches: one was “ball-and-stick model based probabilistic tracking” (Probtrackx) from the FSL toolbox (Behrens et al., 2007) and the other two were based on ODFs represented by fourth order spherical harmonic series: the Hough voting method (Aganj et al., 2011) and the probabilistic index of connectivity (PICo) method (Parker et al., 2003).
Developed in the 1990s, FACT was one of the first deterministic tractography methods for DTI. It is still perhaps the most popular fiber tracking approach for both scientific and clinical applications. The main idea is to trace out the path of the diffusion tensor’s principal eigenvector (the unit eigenvector associated with the maximum eigenvalue) in the image, while testing for sudden transitions in the local fiber orientation. The RK2 algorithm uses the second order Runge–Kutta method to solve a differential equation to more reliably estimate the fiber trajectory. The key idea behind RK2 is to equate the tangent vector with the principal eigenvector. The TL method tracks fibers using diffusion tensor “deflection,” and uses the entire tensor to determine the direction of tract propagation, instead of just the principal eigenvector. The SL method reconstructs fiber trajectories throughout the brain by tracking the direction of greatest diffusion in interpolated steps (typically 0.5 mm). All six deterministic tracking approaches (tensor-FACT, RK2, SL, TL, and ODF-FACT, RK2) were applied using their implementations in the Diffusion Toolkit6. Fiber tracking was restricted to regions where fractional anisotropy (FA) ≥ 0.2 to avoid GM and cerebrospinal fluid; fiber paths were stopped if the fiber direction encountered a sharp turn (with a critical angle threshold ≥ 30°). Sharp “right-angle” turns may be biologically possible in some cases (Wedeen et al., 2012), but allowing right-angle turns in tractography would create large numbers of false positive pathways at fiber crossings. Usually deterministic approaches generate around 30,000–50,000 non-duplicated fibers (3D curves) per brain.
Probtrackx was performed after Bedpostx has been applied. Bedpostx stands for Bayesian Estimation of Diffusion Parameters Obtained using Sampling Techniques (Behrens et al., 2007). The X stands for modeling crossing fibers. Bedpostx runs Markov Chain Monte Carlo sampling to build up distributions on diffusion parameters at each voxel. It creates all the files necessary for running probabilistic tractography. In our study, up to three fibers were modeled per voxel. Once Bedpostx had been run, we chose all voxels with FA ≥ 0.2 as the seeds. Following Bedpostx, Probtrackx was run on each individual seed voxel. Probtrackx repeatedly samples from the voxel-wise principal diffusion direction calculated in Bedpostx, creating a new streamline at each iteration. This builds a distribution on the likely tract location and path, given the data. 1000 iterations were run to ensure convergence of the Markov chains, from which the posterior distributions of the local estimate of the fiber orientation distribution were sampled.
Hough probabilistic tractography was performed with code provided by the authors (Aganj et al., 2011). In short, ODFs at each voxel were computed using the normalized and dimensionless constant solid angle ODF estimator, derived for Q-ball imaging (QBI) as in (Aganj et al., 2010). Tractography was performed by probabilistically seeding voxels with a prior probability based on the FA value (FA ≥ 0.2). All possible curves passing through a seed point were estimated and each received a score estimating the probability of the existence of the fiber, computed from the ODFs. Then the Hough transform voting process was adopted to determine the best fitting curves through each point. Each subject’s dataset contained approximately 10,000 non-duplicated fibers per brain. Hough probabilistic tractography aims to optimize the fiber pathway globally, so there is no explicit upper limit on the number of detectable crossing fibers although the data angular resolution will limit this in practice.
Probabilistic index of connectivity probabilistic tractography was conducted with Camino7. Seed points were chosen at those voxels with FA ≥ 0.2. ODFs were estimated using fourth order Spherical Harmonics and a maximum of three local ODF maxima (where fibers mix or cross) were set to be detected at each voxel. Then, a probability density function (PDF) profile can be produced from the derived local ODF maxima. Monte-Carlo simulation was used to generate fibers emanating from seed points inside the entire brain. Streamline fiber tracking followed the voxel-wise PDF profile with the Euler interpolation method, for 10 iterations per each seed point. The maximum fiber turning angle was set to 30°/voxel. Tracing stopped at any voxel whose FA was less than 0.2. This approach generates many more fibers than other methods used in this study.
The parameter settings for each of these tractography algorithms can also be varied, leading to a huge number of comparisons. To avoid that, we used parameter settings for each method that had been previously optimized by our group or others; in most cases, they were the default parameter settings of the methods. To avoid undue complexity, we concede that changing these parameters could conceivably affect how the methods are ranked. Moreover, all fibers shorter than 10 mm were filtered out, as these were much more likely to be false positive fibers.
One hundred thirteen cortical and subcortical ROIs (listed in the Supplement) were defined using the Harvard Oxford Cortical and Subcortical probabilistic atlas (Desikan et al., 2006). Midline cortical masks were bisected into left and right components, to define separate hemispheric ROIs for each cortical region. Since this is a probabilistic atlas, masks were thresholded at 10% to ensure inclusion of tissue along the gray-WM interface, where fiber orientation mapping and tractography are most reliable. To register these ROIs to each subject’s DWI space, we used FSL’s flirt function to determine the optimal affine transformation between the MNI152 T1 average brain (on which the Harvard Oxford probabilistic atlases are based) and each subject’s skull-stripped T1-weighted image (see Preprocessing), as well as the optimal affine transformation between each subject’s skull-stripped T1 and unique FA images. We used a 12 degree-of-freedom registration with a mutual information cost function. After combining the above two steps’ transformation matrices, we transformed the 113 ROIs to each subject’s DWI space using nearest-neighbor interpolation. To ensure that ROI masks did not overlap with each other after registration, each voxel was uniquely assigned to the mask for which it had the highest probability of membership. We admit there are other ways to define ROIs, such as FreeSurfer parcellation or using non-linear registration method with other atlases. However, testing all possible paracellations was beyond the scope of this paper, here we used the same brain parcellation scheme to compare different tractography methods.
For each ROI pair, the number of detected fibers connecting them was determined from the tractography results in Section “Whole Brain Tractography.” A fiber was considered to connect two ROIs if it intersected both of them. This process was repeated for all ROI pairs, to compute a whole brain fiber connectivity matrix. This matrix is symmetric, by definition, and has a zero diagonal (no self-connections; Zhan et al., 2013b). To avoid computation bias in the later feature extraction and evaluation sections, we normalized each brain matrix by the maximum value in the matrix, as matrices derived from different tractography methods have different scales and ranges.
Up to this step, each subject has nine matrices. Now we need to select feature extraction methods for the classification. Typically the training of a classifier requires the subjects to be described by feature vectors. Therefore the brain networks, represented by matrices – equivalent to very high-dimensional vectors – cannot easily be used to train classifiers, without some dimension reduction or feature selection. As such a feature extraction process is needed to extract useful information from brain networks and represent it in a simpler vector form. One simple approach is to directly use all of the numerical values from the matrix representing the brain network. We call this approach the “raw features” approach, where we just use all the numerical information in the network. One apparent advantage is that this approach requires no extra computation. Even so, the approach generates a huge feature space. Also, the network matrix elements are always corrupted by a certain level of noise. With the huge feature space and limited sample sizes, classifiers may be especially susceptible to such noise. To make the learning process more robust, we chose some commonly used feature selection techniques by thresholding the matrices globally or at individual level, to reduce the number of features. We also chose to use one of the mostly used dimension reduction methods, principal components analysis (PCA) to reduce the number of features. We also tested another closely related approach for dimension reduction on the 2D matrices, based on generalized low-rank approximation of matrices (GLRAM). Thus, for each matrix belonging to the 202 subjects, five different feature extraction methods were selected and described as follows:
Raw features. In our study, the matrices are always symmetric, so we used all the values in the upper triangle of the matrices as features for classification. This feature space is a 6328 × N vector: 6328 = (113 × 112/2) and N is the number of subjects.
Global threshold. In this method, we first compute the mean matrix by averaging the matrices across all subjects. We then rank the elements of the upper triangle of the mean matrix, and record the locations of the largest 5–40% elements, respectively. (We experimented with a wider range from 5 to 100% but obtained best results with the largest 5–40% of the elements, so we report experimental performance in this range.) We then used this subset of elements from the subject matrices as features for classification. In other words, if the threshold = 0.25, we first computed a mean network by averaging all subjects’ networks, then masked the top 25% elements’ positions in the upper triangle of the mean network. Based on this “global” mask, all values except in these masked positions were set to zero for each subject’s network. Then the upper triangle of the thresholded network was defined as features for classification. The feature space is a 6328xN vector with all values in unmasked positions set to zero and N is the number of subjects.
Individual binary threshold. In this method, we convert the values in the matrices into binary variables. If a value exceeds a given threshold, it is set to 1, and 0 otherwise. This individual threshold is obtained by ranking the elements within each subject, and a value is set to 0/1 depending on its relative ranking among all entries within that same matrix. We vary the threshold from the top 5% to top 40% (to be consistent with global threshold method), and perform classification at each thresholding level. The feature space is a 6328xN vector, but with all values less than threshold set to zero. Again, N is the number of subjects.
PCA. The raw feature space is large (113 ∗ 112 /2 = 6328 matrix elements or features), and in the training phase we have fewer than 100 samples. To tackle the ‘large dimension, small sample size’ problem, we employed PCA to reduce the data dimensionality. We first take the upper diagonal as features, and form a sample-by-feature input matrix. We then perform PCA on the input matrix to perform dimension reduction by keeping the first k principal components, where we vary k from 10 to 150. The reduced input matrix is then used to perform classification. The feature space is a k × N vector, where k is the parameter we investigated in Section “Comparing Classification Performance after Using GLRAM,” which is 10–150. Again, N is the number of subjects.
GLRAM (Ye, 2005). One way to reduce the matrix dimension is to use a generalized low-rank approximation, in which we collectively factorize all the subject matrices into three components. That is, for the matrix of each subject Mi, we factorize it as Mi = L × Xi × R, where L ∈ Rd×k and R ∈ Rk×d are shared orthonormal transformations for all matrices, and Xi ∈ Rk×k is a reduced matrix. We use Xi as the new feature representation for classification. One important parameter in GLRAM is the reduced row/column dimensionality. Again, a range of parameter values was investigated to seek the “best” option for the classification. The feature space is am m2 × N vector, N is the number of subjects, and m is the reduced matrix dimension.
After feature extraction from the matrices, we evaluated these feature vectors for three between-group comparisons including AD vs. NC, AD vs. MCI, NC vs. MCI. One could define some metric of group separation to summarize the results, but in practice algorithms may have different strengths and weaknesses depending on the groups compared, as different sets of fibers may differ across diagnostic groups. In these comparisons, AD, MCI, and NC are groups listed in Table 1. We performed the classification as follows:
We selected all the subjects relevant to the classification task.
We performed z-score normalization for each feature, i.e., for each feature, we subtract the mean value of the feature across the selected subjects and divide by the standard deviation.
The class labels are typically unbalanced in our study. To avoid bias, we constructed 20 balanced training/testing sample splits, as follows:
(a) Randomly draw 85% of the data from the smaller class for training, and the remaining 15% for testing.
(b) In the larger class, we match the same number of training samples by a random subsampling, and the rest are put in the test set.
For example, in the AD/NC task, we have 39 AD samples and 51 NC samples. We first use 33 AD samples (85%) for training and six AD samples (15%) for testing. Then we randomly select 33 NC samples and include them in the training set and include the remaining 18 samples in the test set.
In each training/testing split, we use the training set to train a sparse logistic regression classifier (the classifier parameters are estimated from the training data via fivefold cross validation), and we test the classifier’s effectiveness on the test set. The AUC (area under ROC curve) is computed by averaging the trapezoidal approximations for the curve created by true positive rate (TPR) and false positive rate (FPR). TPR is the proportion of positive samples correctly identified as positive and FPR is the proportion of negative samples correctly identified as negative. Multiple classification models were generated for every cross fold. Each provides a prediction, positive or negative, for the given class instance. In the machine learning field, AUC is a common measure of classification performance. For tractography, other measures may also be useful, such as ground truth accuracy and completeness of fiber recovery. So admittedly we are only studying one metric, although it is probably as important as the others.
However, it may be inaccurate to characterize the tractography algorithm performance using the averaged AUC based on only 20 splits. Thus, the 95% confidence interval (CI) for the AUC was computed and one-way analysis of variance (ANOVA) was performed on the AUCs. Our null hypothesis (H0) was: there is no significant difference in the AUCs from different tractography algorithms. If H0 was rejected, post hoc multiple group comparisons were planned to investigate where these differences are. All statistical analysis steps were performed using IBM SPSS Statistics V22. The experiment-wise alpha threshold was set to p < 0.05. In our study, a Bonferroni correction was adopted for multiple hypothesis correction. However, all the p-values reported here have been adjusted by SPSS with the appropriate correction for the effective number of multiple comparisons used. For instance, for a three-group experiment, a pairwise comparison (i.e., a t-test) that yields a p-value of 0.016 would be considered significant at the 0.05 level, because 0.016 < (0.05/3). Instead of giving the nominal two-tailed p-value, SPSS adjusts the p-value by multiplying it by 3, in this case giving a Bonferroni p of 0.048 (0.016 times 3). (SPSS adjusts the actual p-value by applying the Bonferroni correction backward.)
Table 2 compares fiber lengths and numbers for different tractography algorithms. We did not report them for Probtrackx, which does not output these parameters. In Table 2, ODF-based deterministic tractography (ODF-FACT, RK2) tended to generate more false positive fibers (such as shorter fibers) than tensor-based deterministic tractography (tensor-FACT, RK2, SL, and TL). Moreover, the “noisy fiber ratio” (see last column in Table 2) suggests that deterministic approaches (tensor-FACT, RK2, SL, TL, and ODF-FACT, RK2) and PICo may generate more false positive fibers than Hough. Hough fits fibers by global optimization, but greedy algorithms process small neighborhoods at each step, much like FACT or PICo. Clearly, the differences in fiber numbers and lengths may affect downstream analysis, as described below.
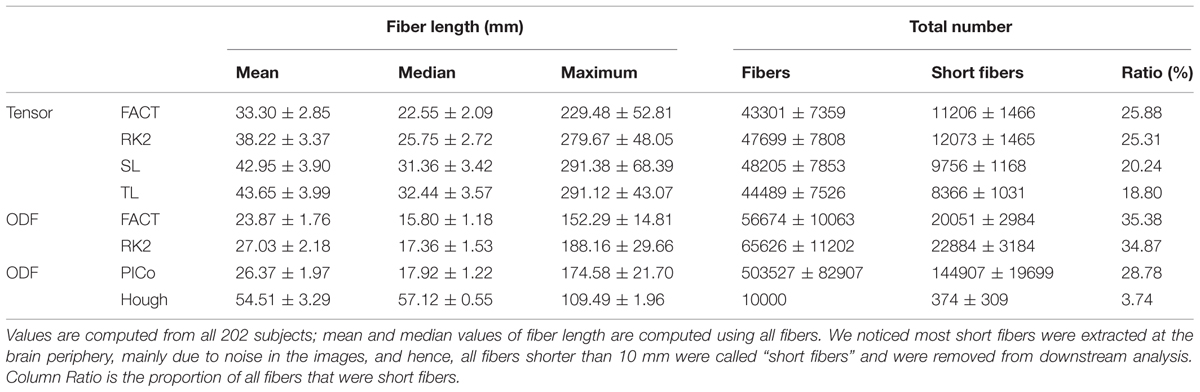
TABLE 2. Compares the fiber length and number for different tractography algorithms except Probtrackx.
Figure 2 compares the mean normalized brain networks for nine tractography algorithms. This mean normalized network is computed from all 202 subjects. Visually, the deterministic approaches – including tensor-FACT, RK2, SL, TL, and ODF-FACT, RK2 – have very similar connection patterns and the probabilistic approaches (PICo, Hough, and Probtrackx) have very different patterns. The apparent connectivity values are also different. If we randomly consider one connection between the 11th ROI and the 107th ROI (see Supplement for the numbering of ROIs), the apparent connectivity varies from a minimum of 0.021 (Hough) and maximum of 0.148 (tensor-TL).
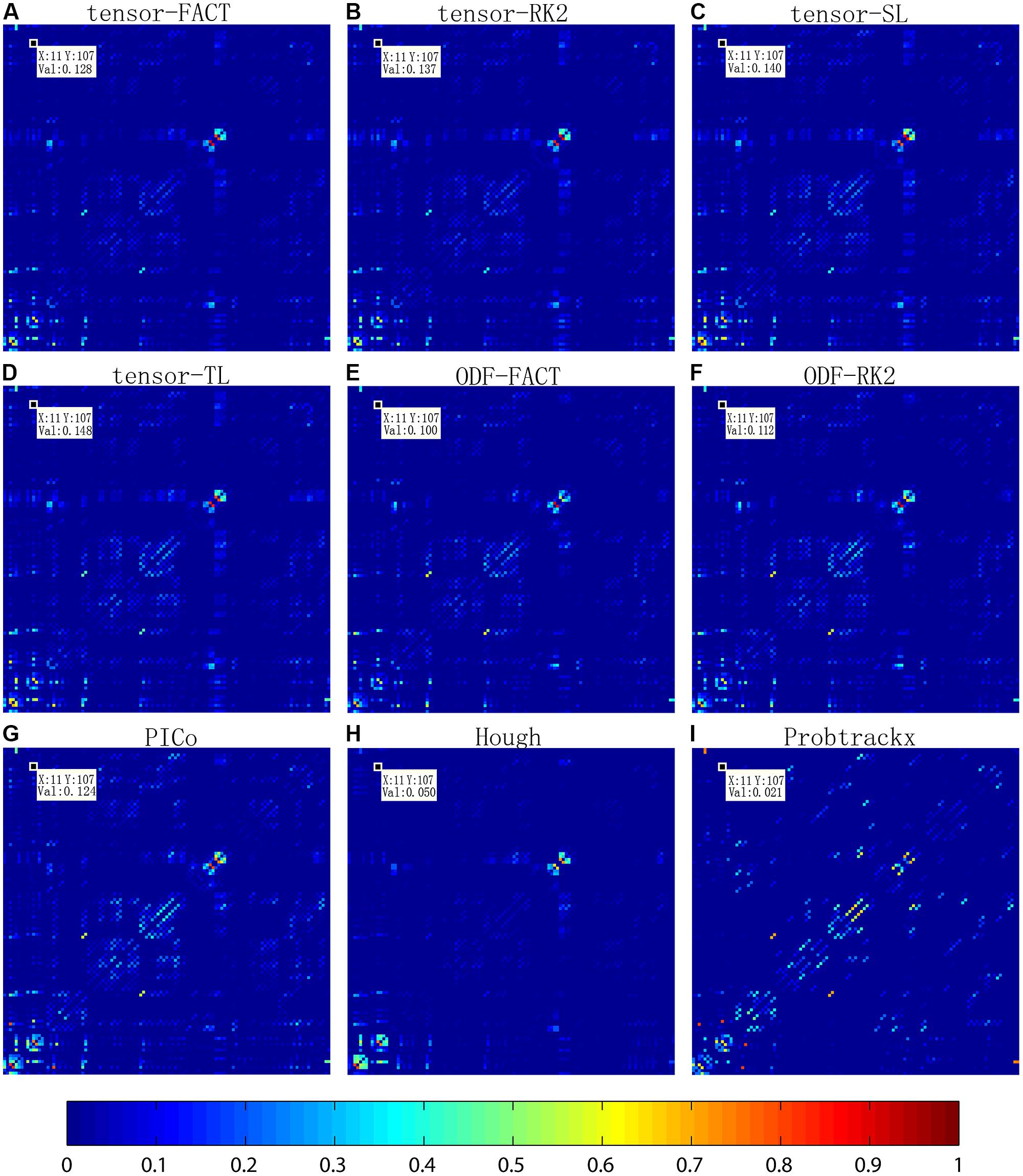
FIGURE 2. Comparison of averaged normalized brain networks from nine different tractography algorithms, including (A) tensor-based FACT; (B) tensor-based RK2; (C) tensor-based SL; (D) tensor-based TL; (E) ODF-based FACT; (F) ODF-based RK2; (G) ODF-based PICo; (H) ODF-based Hough, and (I) Ball-and-stick model based Probtrackx, from all 202 subjects. In each network, each cell represents the connectivity between each pair of ROIs; the ROI index runs from 1 to 113 from left to right and from bottom to top. ROI names are detailed in the Supplement. Visually, brain networks from different tractography algorithms may have similar patterns but in reality, the recovered brain network varies, as shown by the value in the randomly selected cell (11,107).
Figure 3 shows the CI for the AUC of nine tractography algorithms for the three diagnostic group discrimination tasks on raw matrices. Three different colors represent three diagnostic tasks. As we can see from Figure 3, all AUCs in the same diagnostic task have some level of overlap. This means there is no significant difference among the AUCs of nine tractography algorithm for each diagnostic task. Our results from one-way ANOVA (Table 3) are also confirmed this. All three computed values of the F statistic in Table 3 (1.111, 1.348, and 1.945) are less than the critical F-value (1.9929) for (8,171) degrees of freedom at α = 0.05, thus we have to accept the null hypothesis. This suggests that there are no significant group differences in the mean AUCs computed from nine tractography algorithms for each diagnostic task using raw matrices as the features.
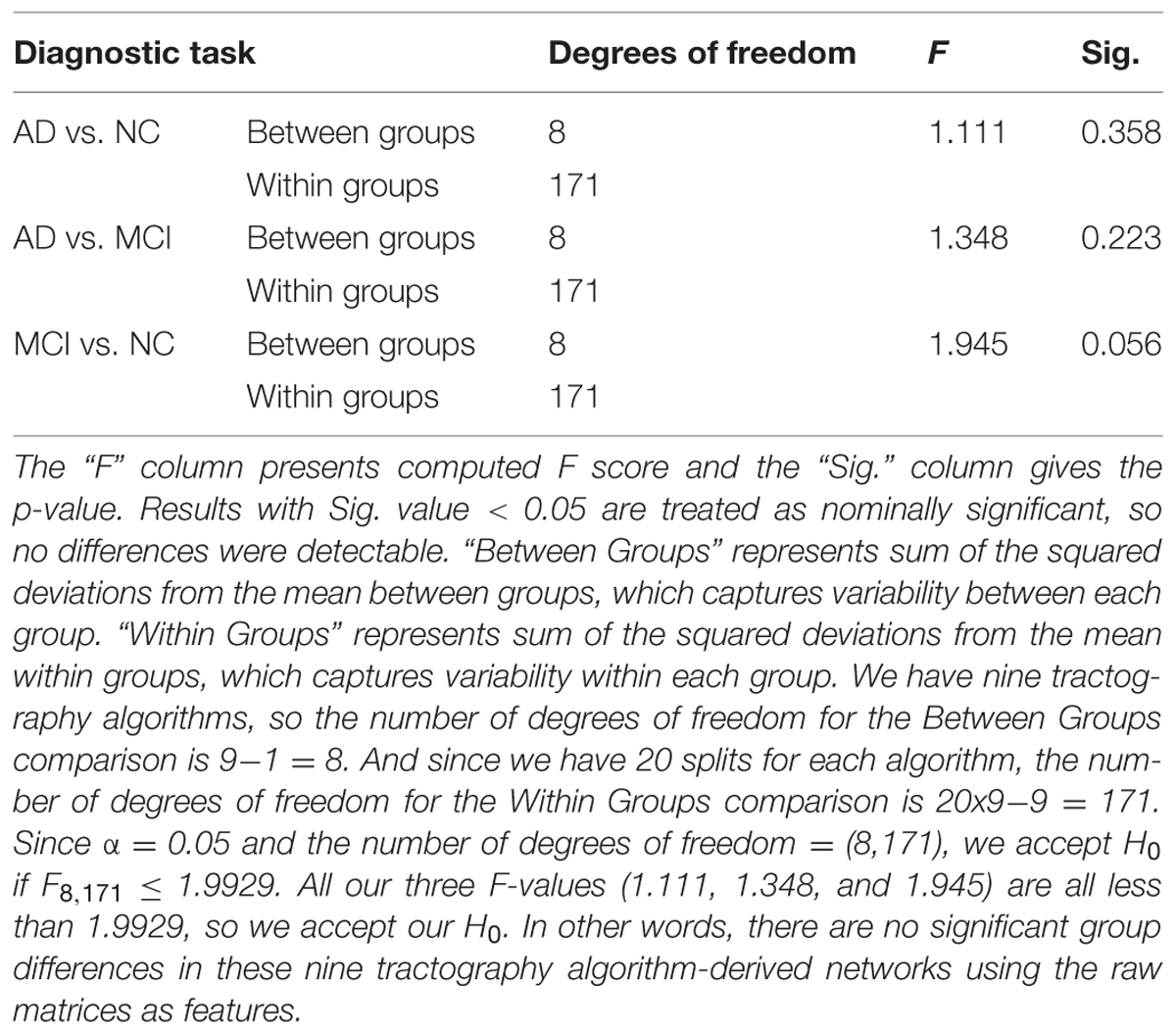
TABLE 3. One-way ANOVA test on the classification performance of nine tractography algorithms for three diagnostic tasks when using the raw matrices as features.
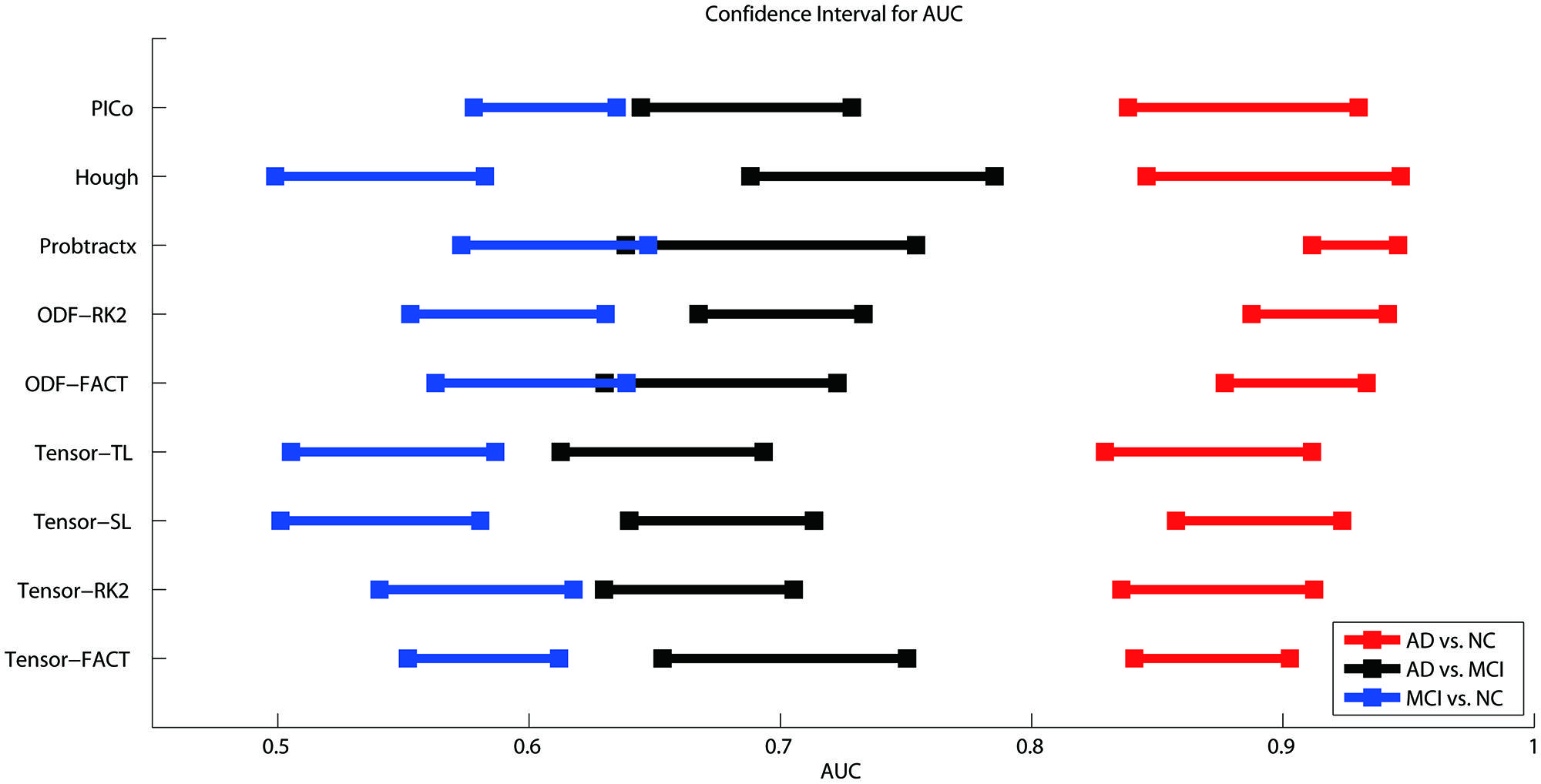
FIGURE 3. Ninety five percent confidence intervals (CI) for the AUC (classification accuracy) for three diagnostic tasks represented by the three color bars (blue, black, and red) for nine tractography algorithms. The red color means the AD vs. NC classification task, black colors denote AD vs. MCI, and blue colors indicate MCI vs. NC. The y-axis indicates the tractography algorithms and x-axis shows the AUC value. In theory, the higher the AUC value, the better the classification performance. However, if the CI of AUCs has some overlap, we cannot conclude that one algorithm is better than the others, even if the mean AUCs are numerically different. As is evident from the three color bars’ horizontal positions, some classifications are more difficult: AD v. NC is the easiest, and MCI v. NC is the most difficult, perhaps in line with expectation.
When using the raw matrix data as features, there is no universally superior method that performs best for all tasks. However, the classification problems do differ in difficulty. As expected, it is easier to distinguish healthy controls from the AD group than from the MCI group. In general, classification accuracy depends on the problem but not strongly on the tractography algorithm.
As described in Section “Feature Extractions” on the “Global Threshold” and “Individual Binary Threshold,” we tried a range of different threshold values from 0.05 to 0.4, at intervals of 0.05. Although the meaning of the threshold value is slightly different between “Global Threshold” and “Individual Binary Threshold,” they have same threshold value range so we presented both results together to check whether the “threshold value” affects classification performance and whether there are any significant differences among these nine tractography algorithms in terms of classification performance using these thresholded matrices as the features.
Table 4A summarizes one-way ANOVA F-test results on the AUCs using thresholded matrix features. Our critical F-value in the degrees of freedom = (7,152) at α = 0.05 is 2.0703. In Table 4A, all computed F-values larger than 2.0703 have been marked in red, which means in these seven situations the threshold values do affect the AUCs. To further investigate how threshold values affect AUCs on these seven situations, we did post hoc multiple group comparisons and Bonferroni correction was adopted to correct for multiple comparison. After applying Bonferroni correction, the three nominally significant situations (ODF-RK2 using the Global Threshold feature method for AD vs. NC, tensor-TL using the Individual Binary Threshold feature method for AD vs. MCI, and the Hough method using Individual Binary Threshold feature method for MCI vs. NC) no longer showed significant differences for different threshold values. Thus, when using the Global Threshold method to extract features, the classification performance of all tractography algorithms in each of three diagnostic tasks are not affected by the threshold values. This is also true for the task AD vs. NC when using the Individual Binary Threshold feature extraction method. Table 4B summarizes post hoc multiple comparison results for tensor-RK2 and Hough in task AD vs. MCI as well as Tensor-TL and PICo for task MCI vs. NC using the Individual Binary Threshold as the feature extraction method. Only comparisons with statistical significance between different threshold values are shown in Table 4B. Using Individual Binary Threshold feature extraction method, the classification performances in the tasks AD vs. MCI and MCI vs. NC are statistically affected by the threshold values for some tractography algorithms: Tensor-RK2, Hough or Tensor-TL and PICo.
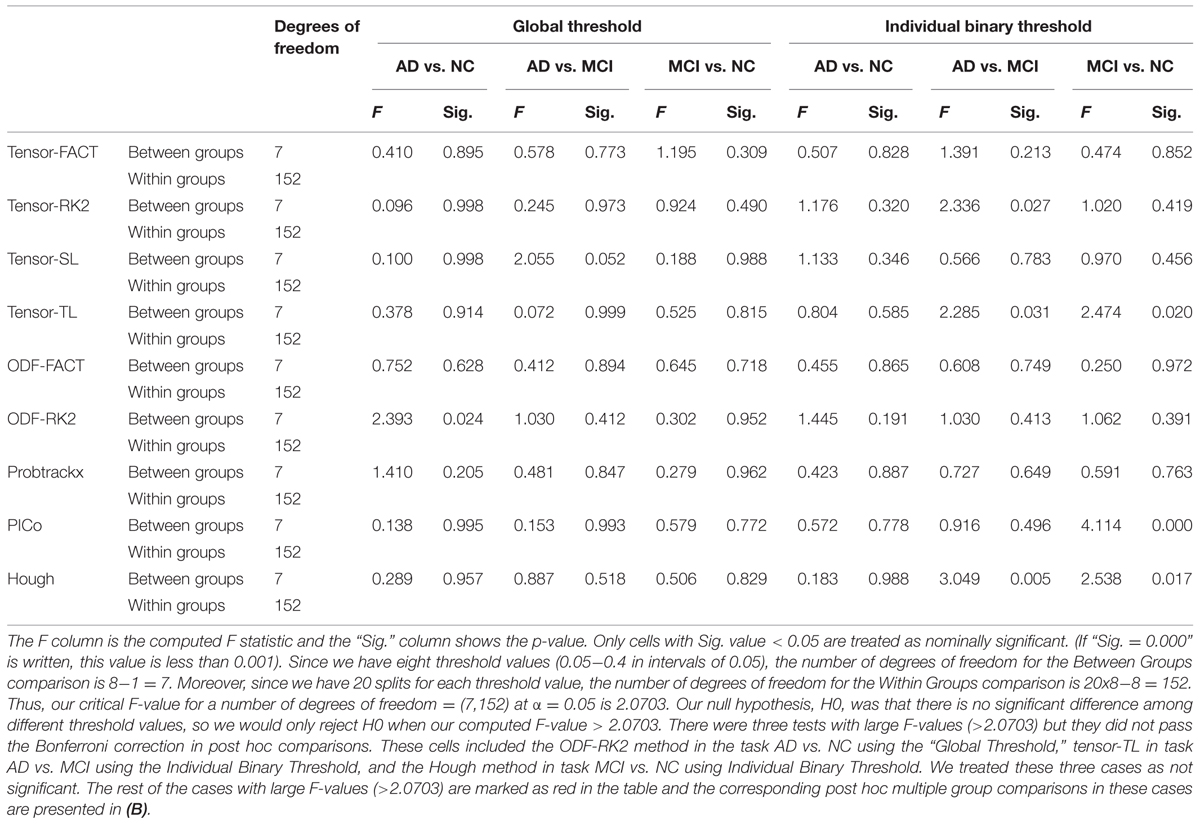
TABLE 4A. One-way ANOVA test on the classification performance across different threshold values for nine tractography algorithms in three diagnostic tasks.
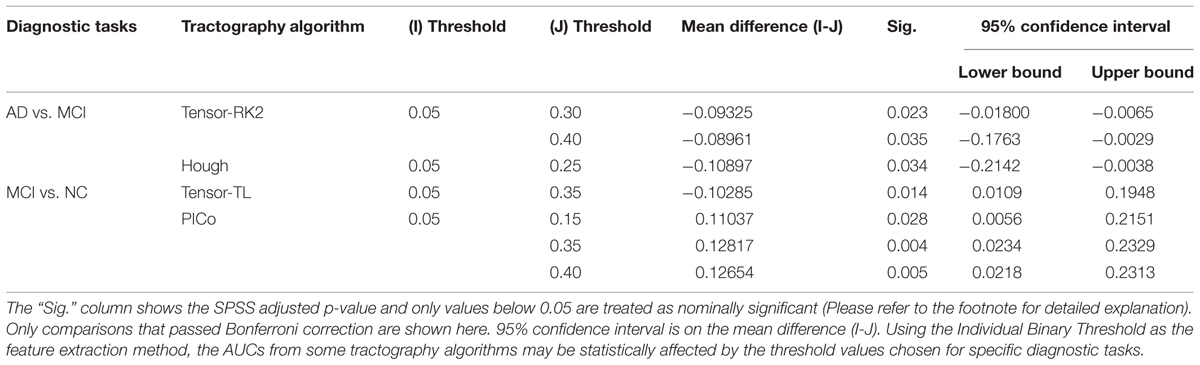
TABLE 4B. Post hoc comparison results for the Individual Binary Threshold method.
Now we come to our second hypothesis test in this section, to see whether our classification performances vary among different tractography algorithms, when using thresholded matrices as the feature. However, this is a complex question as there are nine tractography algorithms with eight different threshold values; for each threshold value we conduct 20 different splits of the data, which means there are 20 AUCs for each threshold point for each tractography. To simplify the analysis, we picked the threshold value with the largest average AUC for each tractography algorithm and then conducted a one-way ANOVA on AUCs computed from different tractography algorithm-derived thresholded matrices. Our results (Supplementary Table S2) show that all computed F Raw Feature-values are less than the critical F-value (1.9929) at the α = 0.05 level with degrees of freedom = (8,171). This does not allow us to reject the null hypothesis (H0) that there are no statistical differences among the AUCs computed from these nine tractography algorithm-derived thresholded matrices in each diagnostic task, no matter what the Global Threshold or Individual Binary Threshold.
As described in Section “Feature Extractions” (on PCA), we evaluated a range of choices: from the first 10 principal components (PCs) to the first 150 PCs, computed from all the data. Our first hypothesis test is whether the choice of number of PCs affects how each tractography algorithm performs. The second hypothesis test is whether the choice of tractography algorithm affects the classification performance when using certain number of PCs.
For the first hypothesis test, our null hypothesis (H0) is that the choice of the number of PCs will not affect the classification performance. We performed one-way ANOVA on the AUCs from 12 different numbers of PCs and our results (Table 5A) show that some tractography algorithms in some diagnostic tasks are statistically affected by the number of PCs when using PCA for feature extraction. Interestingly, for the classification task AD vs. NC, only the tensor-RK2 method was affected while for task AD vs. MCI, most tractography algorithms except ODF-RK2 and PICo were affected by the number of PCs used. Post hoc comparisons (Table 5B) confirmed this. Moreover, from Table 5B we can see that in those tractography algorithms affected by the number of PCs, the AUCs for smaller numbers of PCs are higher than the AUCs in larger number of PCs. For example: for the task AD vs. MCI, the AUC of tensor-FACT using 10 PCs is statistically (by 0.14 units) “higher” than same algorithm using 150 PCs. This trend is consistent for all tractography algorithms listed in Table 5B, which suggests that these top PCs have recovered enough information for the classification and more PCs may impair the classification accuracy for these tractography algorithms. Comparisons that did not pass Bonferroni correction are not listed in Table 5B, so are no significant differences in classification performance among different choice of PCs. In other words, only tests that passed Bonferroni correction are shown in Table 5B.
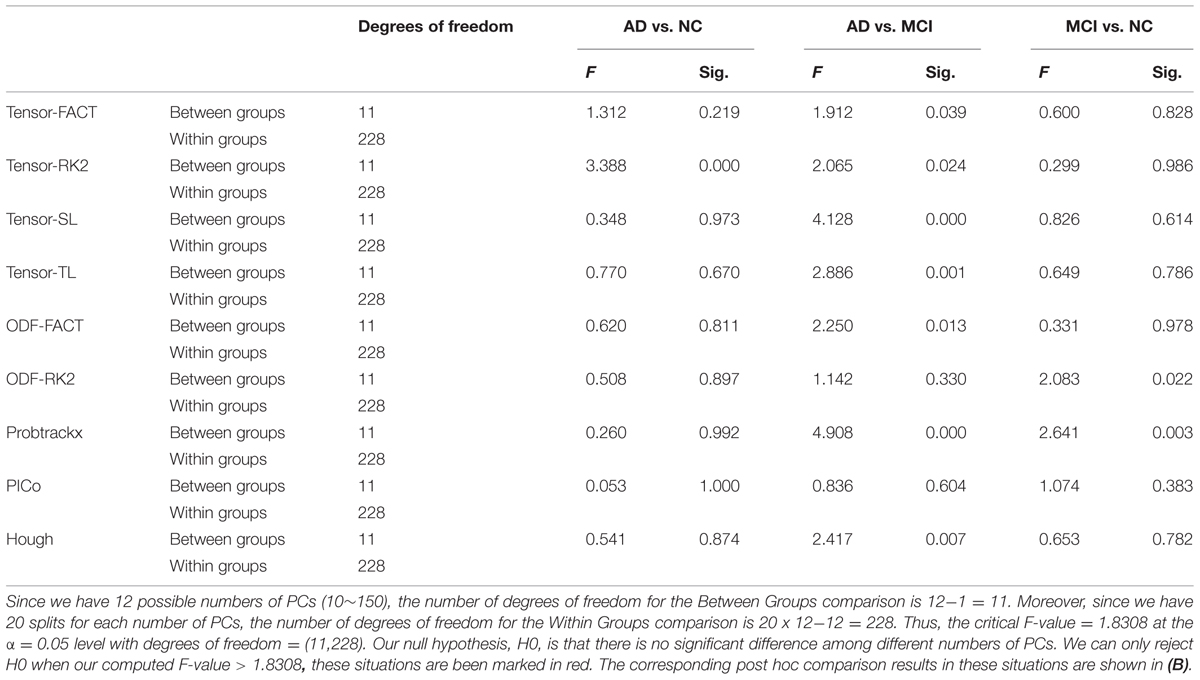
TABLE 5A. One-way ANOVA test on the classification performances across different numbers of PCs for nine tractography algorithms in three diagnostic tasks.
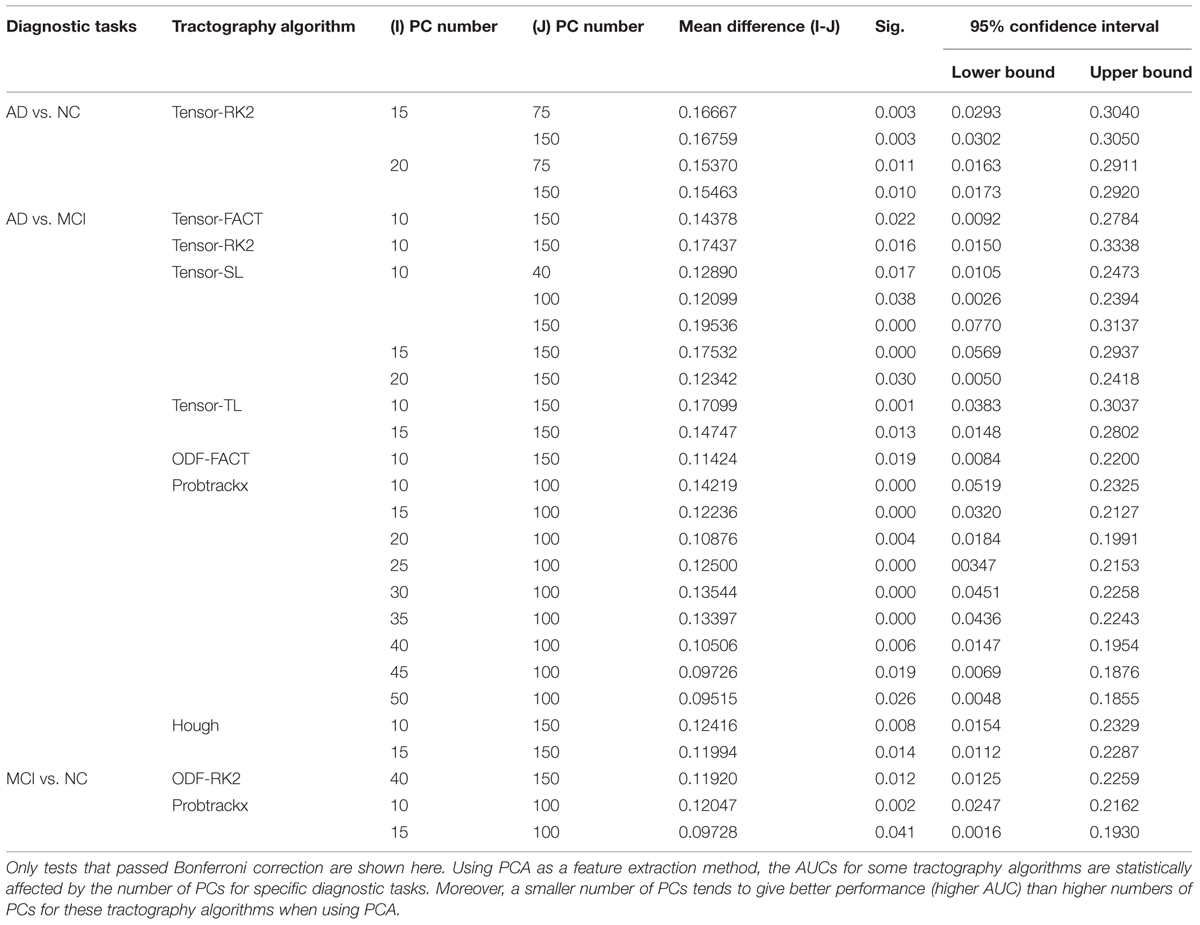
TABLE 5B. Post hoc comparisons results.
Based on this reasoning, we use 10 PCs for each tractography algorithm and conducted one-way ANOVA across the nine tractography algorithms to check this section’s second null hypothesis (H0): the classification performances when using PCA from different tractography algorithm show no significant difference for each diagnostic task. Our result (Tables 6A,B) shows that for tasks AD vs. NC and MCI vs. NC, we have to reject H0, but for AD vs. MCI, we cannot reject H0. In both task AD vs. NC and task MCI vs. NC, there exist some comparisons between some tractography algorithms which do pass Bonferroni correction (Table 6B) while for task AD vs. MCI, although the F-value in one-way ANOVA (Table 6A) are larger than the critical F-value (= 1.9929 at the α = 0.05 level with the degrees of freedom (8,171)), this does not pass Bonferroni correction, so we can conclude that the classification performances when using PCA from different tractography algorithm have no detectable difference for the task AD vs. MCI. Moreover, for the task MCI vs. NC, Probtrackx performs significantly better than most deterministic tractography approaches (tensor-FACT, RK2, TL and ODF-RK2; Table 6B).
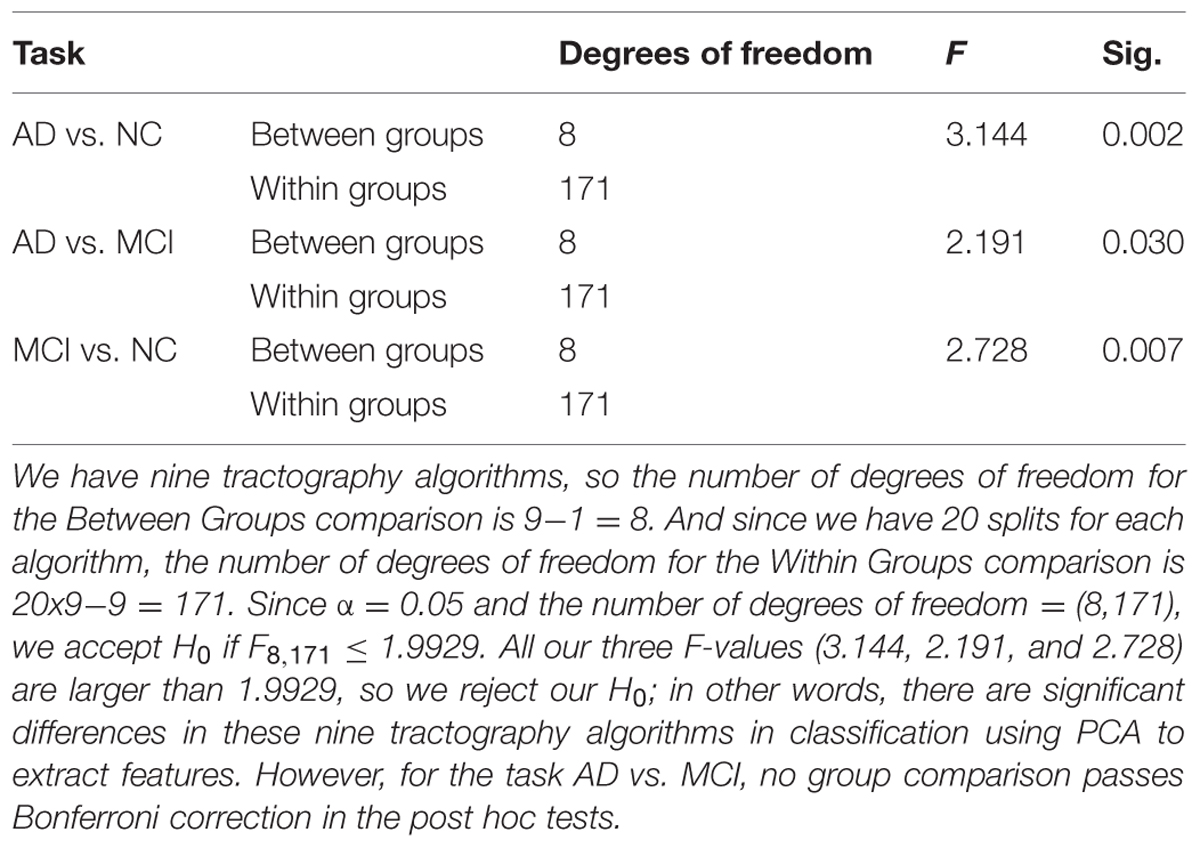
TABLE 6A. Statistical analysis results for classification performances from nine tractography algorithms using PCA. (A) One-way ANOVA.
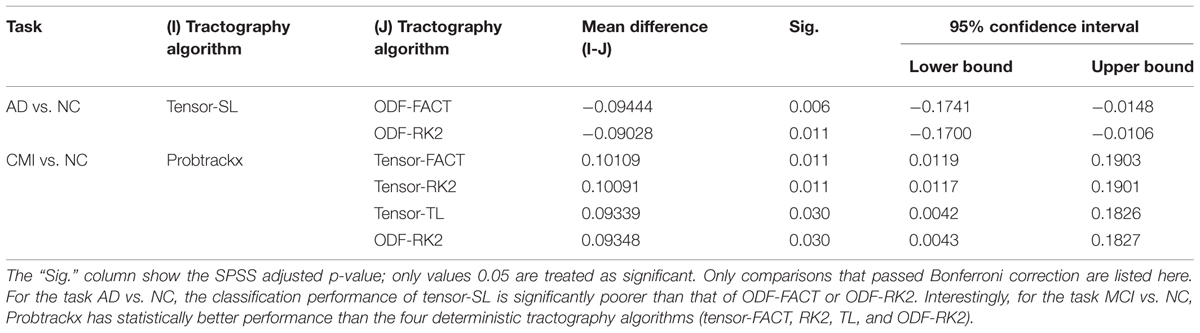
TABLE 6B. Post hoc group comparisons.
In this section, we tested another feature extraction (dimension reduction) method, “GLRAM.” Our first hypothesis test is whether the classification performance of each tractography algorithm shows any differences when using GLRAM with different levels of dimension reduction. Our second hypothesis test is whether the classification performance of different tractography algorithms shows any differences when using GLRAM as a feature extraction method.
In GLRAM, an important parameter is to determine the dimension of the reduced matrix; different dimensions for the reduced matrix may lead to different results. For example, a higher dimension for the reduced matrix means less information loss, although it is not clear whether this helps for classification. Thus, we tested a range of reduced dimension parameters, from 5 to 35, at intervals of 5 (in total, seven different dimensions).
Tables 7A,B illustrate the influence of the dimension parameter on the classification performance of each tractography algorithm using GLRAM. For one task (AD vs. NC), the tractography algorithms’ performance was not affected by the dimension parameter of GLRAM. In other tasks, only one tractography algorithm’s performance in each task was affected by the choice of the dimension parameter in GLRAM (Table 7B). For example, by using Probtrackx in task AD vs. MCI, the lower dimension dataset (5) gave better performance than higher dimension sets (10, 25, 30, and 35). This is evident because the mean differences are all significant and positive; even so, the trend appears to be opposite when using the Tensor-SL approach for the task MCI vs. NC.
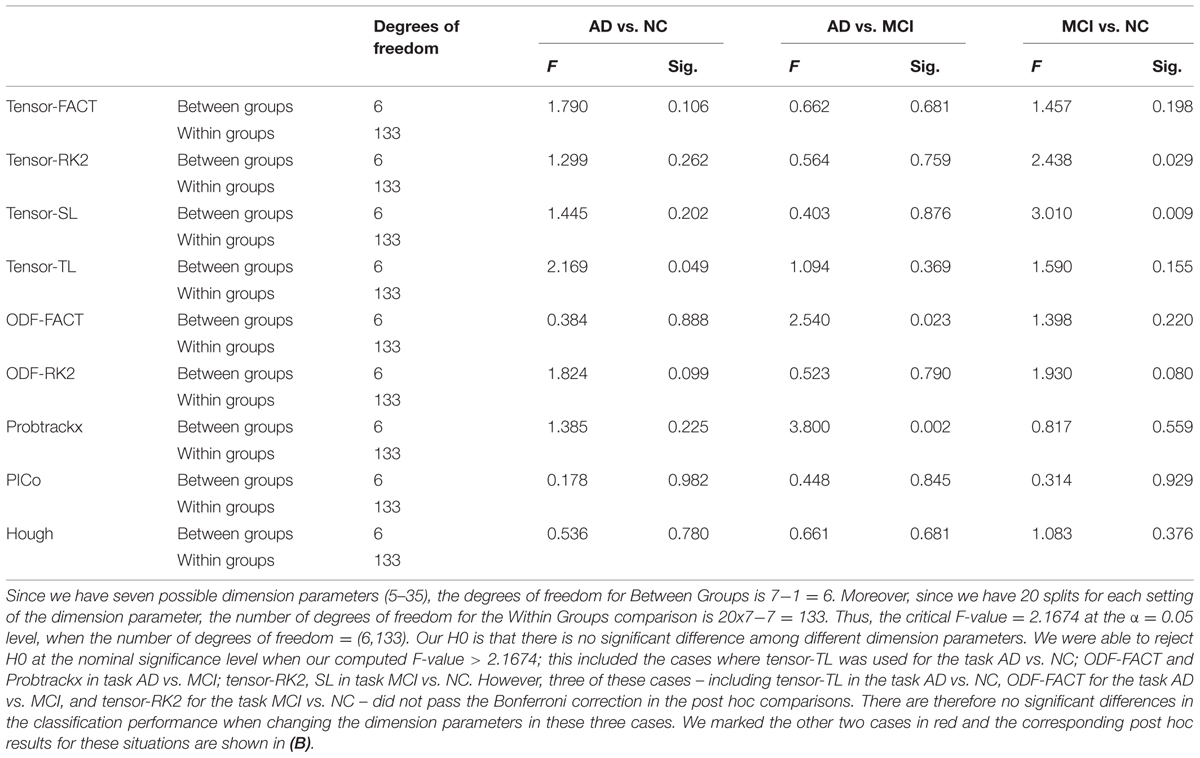
TABLE 7A. One-way ANOVA testing for differences in the classification performances across different GLRAM dimension parameters for nine tractography algorithms in three diagnostic tasks.
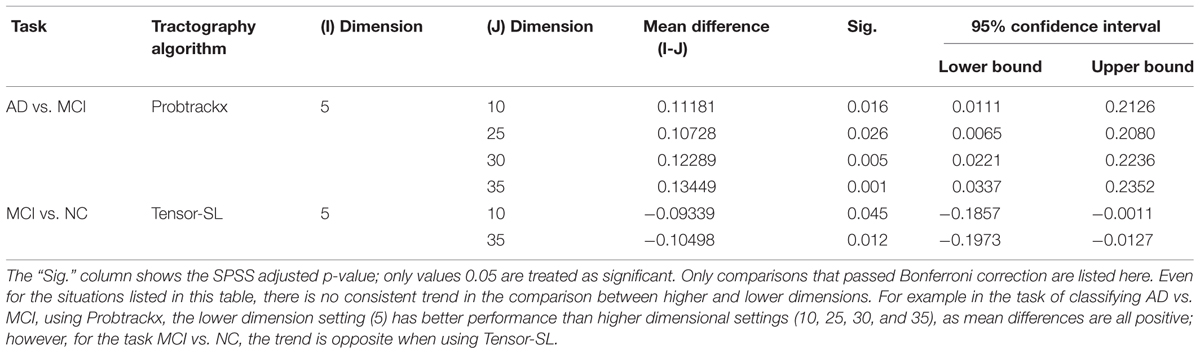
TABLE 7B. Post hoc comparisons.
After we studied the effects of GLRAM dimension parameters on each tractography algorithm in terms of its classification performance, we picked up the dimension parameter with the largest average AUC for each tractography algorithm and then conducted one-way ANOVA across nine tractography algorithms to test our null hypothesis (H0) that the choice of tractography algorithms does not affect the classification performance. Our result (Supplementary Table S3) is favor of accepting H0, in other words, there is no evidence that the choice of tractography algorithms affects the classification performance when using GLRAM as the feature extraction method.
Finally, we tested whether the classification performance is affected by the choice of the feature extraction methods. For each tractography algorithm, there are five feature extraction choices, which include “Raw feature,” “Global Threshold” using the threshold value with the highest average AUC, “Individual Binary Threshold” using the threshold value with the highest average AUC, “PCA” using 10 PCs, “GLRAM” using the dimension parameter with the highest average AUC. Here our null hypothesis (H0) was that there are no significant differences among these five feature extraction methods for any tractography algorithm. So we performed one-way ANOVA on each of nine tractography algorithm among the five feature extraction methods, for each diagnostic task. Our results (Table 8A) show that this depends on the diagnostic task as well as the choice of tractography algorithm. For example, the performance of tensor-SL (Table 8A) was significantly affected by the choice of feature extraction methods for the task AD vs. NC but not in the other tasks. Some tractography algorithms’ performance was statistically consistent across different feature extraction methods, such as tensor-FACT in all three tasks (Table 8A). We also performed post hoc tests on the “significant” cases in Table 8A and our results (Table 8B) showed that after Bonferroni correction, some feature extraction methods perform significantly better than other extraction methods for some tasks, but not in other tasks, so the trend is not consistent. The diagnostic task and the choice of tractography algorithm both affect the results, so there is no universally optimal method.
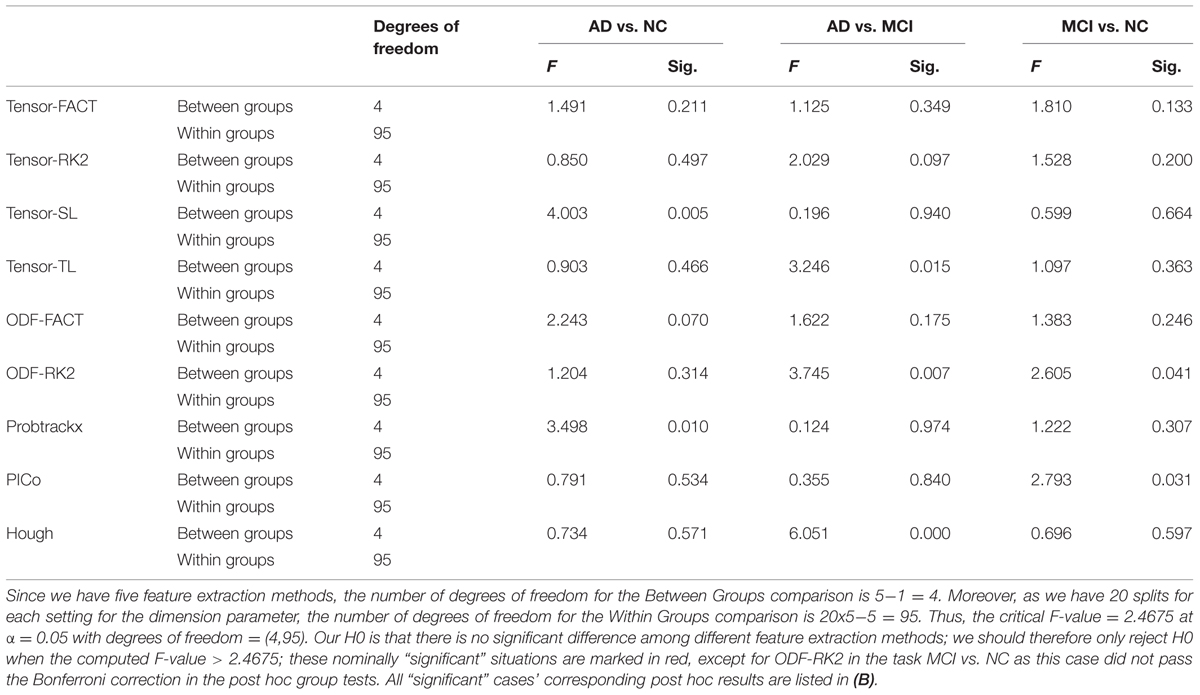
TABLE 8A. One-way ANOVA on the classification performances across five feature methods for nine tractography algorithms in three diagnostic tasks.
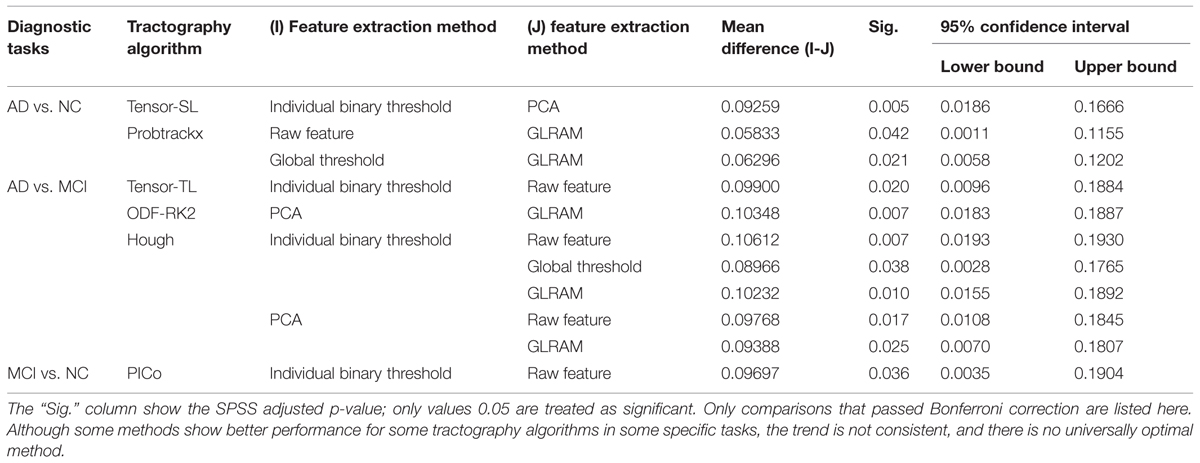
TABLE 8B. Post hoc comparisons.
In this study, we have adopted five feature extraction methods on nine whole brain tractography derived brain networks for three diagnostic classification tasks. There are three possible factors affecting the ultimate classification accuracy: the difficulty of the diagnostic task, the feature extraction method and the tractography algorithm.
Our result (Figure 3) shows the classification accuracy is strongly correlated with the difficulty of the diagnostic task. The AD vs. NC is the easiest task since there are clear evidences to show that the AD patients have detectable pathological changes (such as short term memory loss, problems with language, disorientation, mood swings, loss of motivation, not managing self care, and behavioral issues) in the brain structures and functions (Burns, 2009; Burns and Iliffe, 2009; Querfurth and LaFerla, 2010; Ballard et al., 2011; Fritze et al., 2011; Todd et al., 2013). While MCI is found to be a transitional stage between normal aging and dementia (Schroeter et al., 2009), the detectable pathological changes of MCI is smaller than AD. Also, there are several subtypes of MCI (e.g., early-MCI and late-MCI; Jessen et al., 2014). So it may increase the complexity to define a simple trend in MCI patient group. Based on our result in Figure 3, the difficulty of the diagnostic task has the order: NC vs. MCI > AD vs. MCI > AD vs. NC.
The five feature extraction methods have been widely used in machine learning area (Mocks and Verleger, 1986; Ye, 2005; Yuan and Zou, 2013). Although the “raw features” approach suffers from the “curse of dimensionality” problem, one apparent advantage of this approach is that the method does not require additional computation. For “global threshold,” we need to compute the mean matrix and apply the matrix to each sample, which costs O(NxM) where M = 6328. In “individual binary threshold,” we also need to scan through the matrices, the costs of which is still O(NxM). For principle components analysis approach, we need to solve a singular value decomposition problem, which is O(N M2) in our case. Given N is very small, the complexity can be thought as O(M2). GLRAM uses an iterative algorithm, and in each iteration the major computation costs are to solve two top-k eigen-decomposition problems, where k is the dimension of the reduced matrix. Since the size of the reduce k is typically much smaller than D, the operation can be considered as order O(D2). Although different algorithms have different computational complexities, and all of them can be efficiently computed in modern computers given the scale of our data. In our experiments, the difference in time costs among these algorithms cannot be noticed. In terms of ultimate classification accuracy, there is no feature extraction method is significantly better than others. However for each feature extraction method, the parameter setting may or may not affect the later result. For example, global threshold or GLRAM is less affected by the parameter selection while the performance of PCA and Individual Binary Threshold indeed change with the parameters.
In this study, nine tractography algorithms were selected from two categories: the deterministic approach and the probabilistic approach. Deterministic tractography recovers fibers emanating from a seed voxel by following the principal direction of the diffusion tensor or the dominant direction of the diffusion ODF. Although the deterministic tractography approach is very efficient, it depends on the choice of initial seed points and can be sensitive to the estimated principal directions. Probabilistic tractography approaches can be computationally more intensive but they are in some cases more robust to partial volume averaging effects and uncertainties in the underlying fiber direction, which are inevitable due to imaging noise. This work is part of a body of work that has examined relative merits of different tractography methods for different tasks and goals. One annual conference, MICCAI, has held annual competitions in recent years. The most recent, in 2014, brought together 15 international tractography teams from leading academic centers. Fillard et al. (2011) evaluated 10 fiber reconstruction methods were evaluated on a specially constructed phantom dataset, with known ground truth on the geometry of the fibers. For medium to low SNR datasets, the authors recommended the use of a prior on the spatial smoothness of either the diffusion model to improve tractography results. Later work on real datasets compared how well different methods could recover the corticospinal tract (CST) from two diffusion imaging data from neurosurgical cases (Neher et al., 2012). Girard et al. (2014) also compared settings in tractography methods (e.g., stopping criteria and seeding techniques) to avoid biases in over-selecting shorter fibers (Girard et al., 2014).
Before we ran this study, we carefully examined the parameter setting for each tractography to make sure the tracked fibers are reasonable. And these parameter settings have been used in lots of other studies in our group. We admitted there are many factors that can affect the performance of each tractography algorithm. All these nine whole brain tractography were computed using LONI Pipeline8, which is a 306-node, dual-processor SUN Microsystems V20z cluster. As for the computing time, tensor-based deterministic approaches (tensor-FACT, RK2, SL, and TL) only take less than 5 min and ODF-based deterministic approaches (ODF-FACT, RK2) take about 6∼7 min per brain per CPU. PICo takes about 6∼8 h and Hough takes about 22∼24 h per brain per CPU. And for FSL PROBTRACTX, the prerequisite step BEDPOSTX requires ∼6 h using 110 CPUs per brain and PROBTRACTX requires another 2∼3 h per brain per CPU. So the computation cost for these nine tractography algorithms are Probtrackx > Hough > PICo > ODF-FACT, RK2 > tensor-FACT, RK2, SL, TL. However, our results indicated that although there may have some differences in terms of fiber length or fiber tracking directions for each specific tractography (Figure 2), the classification accuracy has no relationship with the computation cost. There were no detectable differences in classification performance among different tractography algorithms when using the raw matrices (Table 3), a global or individual binary threshold (Supplementary Table S2) or the GLRAM method (Supplementary Table S3) as feature extraction methods for each of the three diagnostic tasks. However, when using PCA (Table 6), for task the AD vs. NC, ODF-based deterministic approaches are better than tensor-based deterministic approach; for the task MCI vs. NC, Probtrackx performed better than deterministic approaches, while for the task AD vs. MCI, there is no significant difference among these nine tractography algorithms. As a general principle, we could expect the probabilistic methods to do better than deterministic methods, and high-order ODF methods should perform better than tensor models, but only in tasks where the additional information is useful. MCI vs. NC is a relatively hard classification task and perhaps best suited to pick up the advantages of more accurate modeling of diffusion and connectivity. In general, the simpler methods already give good performance on the easier classification tasks (e.g., AD vs. NC), while more challenging task tended to benefit from more sophisticated modeling. Moreover, the number of PCs chosen did affect the classification, with a small number of PCs (such as 10) being best in some cases, when adopting PCA as feature extraction method in all three diagnostic tasks (Tables 5A,B).
The choice of feature extraction method depends on the problem and the level of sophistication needed for modeling the networks. For tasks that were easier (i.e., when groups differed more), we often failed to detect any practical difference across methods or processing choices. But differences were evident in performance on some of the trickier classification problems. The optimal feature extraction method and tractography algorithm may depend on the diagnostic task. For example, for the somewhat easy classification task of separating AD from NC, individual binary thresholding performed better than PCA for tensor-SL and GLRAM performed worse than using the raw matrices or a global threshold for Probtrackx. This is probably because the AD vs. NC differences are so severe that they can even be picked up by simply binary thresholding on the matrix elements, without requiring more sophisticated data reduction. There were no detectable differences for the rest of seven tractography algorithms in terms of these five feature extraction methods. Similar situations for the tasks AD vs. MCI and MCI vs. NC can be found in Table 8B.
Finally, in this study we selected sparse logistic regression classification for performance evaluation and we admitted that the choice of classification algorithm also affects the result. In fact, we have tried different classification algorithms, such as linear support vector machine (SVM), Gaussian SVM or Random Forest, in a separate study. We didn’t include this part here since it will make the content too complex.
Here, we studied how the choice of tractography method affects our ability to classify different diagnostic groups in aging populations, including AD, based on structural brain networks. Clearly, the diffusion MRI-derived networks would not be the only feature used for diagnostic classification in any realistic setting, but it is important to know which methods perform best (or worst), and with what parameter choices. Most practically, we wanted to know if any methods are best avoided when trying to sensitively detect disease effects on structural brain networks.
Our study had three main findings. First, and as expected, some diagnostic groups were easier to distinguish than others (Figure 3). Diagnostic accuracy was higher for AD vs. NC comparisons than for NC vs. MCI comparisons. Differences among algorithms within a task were relatively small compared to the differences in accuracy for different tasks. Secondly, the best tractography algorithm for each diagnostic task differs, but there were no universally optimal methods, or feature extraction methods. Lastly, we tested if any choice of dimensionality reduction method was helpful for classification. With some exceptions, there did not seem to be a universally helpful method (Tables 8A,B). The optimal feature extraction method may also depend on the diagnostic task and the choice of the tractography algorithms.
Our study has some limitations. First, it could be argued that the method that best classified patients from controls need not be the most accurate method in the sense of extracting “true” fibers. For instance, a tractography method that fails to extract fibers in certain parts of the brain would not normally be considered the best, even if it gave good classification performance. So an important ancillary study might compare the accuracy of these methods relative to ground truth. A second limitation is that DWI would not normally be the method of choice to classify AD stages; structural atrophy, or amyloid and tau proteins measured in the blood or CSF tends to be favored, because of the known pathology of the disease. Even so, our goal was not to achieve optimal classification, but evaluate tractography features and methods likely to contribute to classification. In the meantime, having a workflow to classify brain networks might offer an additional diagnostic tool for AD and might help other studies unrelated to AD. Also, the following caveats apply. We cannot rule out that the algorithm performance depends on the quality of the data used for testing. The ADNI data is somewhat standard and makes sense to use for evaluation, as it is typical of that collected in DWI studies of clinical cohorts.
Finally, we concede that network analysis is an evolving field. In this study, we chose brain parcellation based on 113 regions. Other atlas and partitions are possible, and it is even possible to adapt the cortical parcellation to achieve better classification. Moreover, slightly changing the parameter setting (such as critical angle) for each tractography method could also affect the performance. To avoid adding too many free parameters to the study, we did not explore these issues here, but such tuning tactics are plausible to improve the discriminatory power of network analysis for any particular tractography or feature set.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Algorithm development and image analysis for this study was funded, in part, by grants to PT from the NIBIB (R01 EB008281, R01 EB008432), by the NIA, NIBIB, NIMH, the National Library of Medicine, and the National Center for Research Resources (AG016570, AG040060, EB01651, MH097268, LM05639, RR019771 to PT. PT is also supported, in part, by U54 EB020403 (the “Big Data to Knowledge” Program), supported by the National Cancer Institute (NCI), the NIBIB and a cross-NIH Consortium. This work is also supported by R21 AG043760 to YW, R01 LM010730 to JY, and by the National Science Foundation (IIS-0812551, IIS-0953662 to JY). Data collection and sharing for this project was funded by ADNI (NIH Grant U01 AG024904). ADNI is funded by the National Institute on Aging, the National Institute of Biomedical Imaging and Bioengineering, and through contributions from the following: Abbott; Alzheimer’s Association; Alzheimer’s Drug Discovery Foundation; Amorfix Life Sciences Ltd.; AstraZeneca; Bayer HealthCare; BioClinica, Inc.; Biogen Idec Inc.; Bristol-Myers Squibb Company; Eisai Inc.; Elan Pharmaceuticals Inc.; Eli Lilly and Company; F. Hoffmann-La Roche Ltd. and its affiliated company Genentech, Inc.; GE Healthcare; Innogenetics, N.V.; IXICO Ltd.; Janssen Alzheimer Immunotherapy Research & Development, LLC.; Johnson & Johnson Pharmaceutical Research & Development LLC.; Medpace, Inc.; Merck & Co., Inc.; Meso Scale Diagnostics, LLC.; Novartis Pharmaceuticals Corporation; Pfizer Inc.; Servier; Synarc Inc.; and Takeda Pharmaceutical Company. The Canadian Institutes of Health Research is providing funds to support ADNI clinical sites in Canada. Private sector contributions are facilitated by the Foundation for the National Institutes of Health. The grantee organization is the Northern California Institute for Research and Education, and the study is coordinated by the Alzheimer’s Disease Cooperative Study at the University of California, San Diego. ADNI data are disseminated by the Laboratory for Neuro Imaging at the University of Southern California. This research was also supported by NIH grants P30 AG010129 and K01 AG030514 from the National Institute of General Medical Sciences.
The Supplementary Material for this article can be found online at: http://www.frontiersin.org/journal/10.3389/fnagi.2015.00048/abstract
Aganj, I., Lenglet, C., Jahanshad, N., Yacoub, E., Harel, N., Thompson, P. M.,et al. (2011). A Hough transform global probabilistic approach to multiple-subject diffusion MRI tractography. Med. Image Anal. 15, 414–425. doi: 10.1016/j.media.2011.01.003
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
Aganj, I., Lenglet, C., Sapiro, G., Yacoub, E., Ugurbil, K., and Harel, N. (2010). Reconstruction of the Orientation Distribution Function in Single- and Multiple-Shell Q-Ball imaging within constant solid angle. Magn. Reson. Med. 64, 554–566. doi: 10.1002/mrm.22365
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
Arienzo, D., Leow, A., Brown, J. A., Zhan, L., Gadelkarim, J., Hovav, S.,et al. (2013). Abnormal brain network organization in body dysmorphic disorder. Neuropsychopharmacology 38, 1130–1139. doi: 10.1038/npp.2013.18
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
Ballard, C., Gauthier, S., Corbett, A., Brayne, C., Aarsland, D., and Jones, E. (2011). Alzheimer’s disease. Lancet 377, 1019–1031. doi: 10.1016/S0140-6736(10)61349-9
Bartzokis, G. (2011). Alzheimer’s disease as homeostatic responses to age-related myelin breakdown. Neurobiol. Aging 32, 1341–1371. doi: 10.1016/j.neurobiolaging.2009.08.007
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
Basser, P. J., Pajevic, S., Pierpaoli, C., Duda, J., and Aldroubi, A. (2000). In vivo fiber tractography using DT-MRI data. Magn. Reson. Med. 44, 625–632. doi: 10.1002/1522-2594(200010)44:4<625::AID-MRM17>3.0.CO;2-O
Behrens, T. E., Berg, H. J., Jbabdi, S., Rushworth, M. F., and Woolrich, M. W. (2007). Probabilistic diffusion tractography with multiple fibre orientations: what can we gain? Neuroimage 34, 144–155. doi: 10.1016/j.neuroimage.2006.09.018
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
Braak, H., and Braak, E. (1996). Development of Alzheimer-related neurofibrillary changes in the neocortex inversely recapitulates cortical myelogenesis. Acta Neuropathol. 92, 197–201. doi: 10.1007/s004010050508
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
Braskie, M. N., Jahanshad, N., Stein, J. L., Barysheva, M., McMahon, K. L., de Zubicaray, G. I.,et al. (2011). Common Alzheimer’s disease risk variant within the CLU gene affects white matter microstructure in young adults. J. Neurosci. 31, 6764–6770. doi: 10.1523/JNEUROSCI.5794-10.2011
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
Burns, A. (2009). Alzheimer’s disease: on the verges of treatment and prevention. Lancet Neurol. 8, 4–5. doi: 10.1016/S1474-4422(08)70271-0
Burns, A., and Iliffe, S. (2009). Alzheimer’s disease. BMJ 338, b158. doi: 10.1136/bmj.b158
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
Catani, M. (2006). Diffusion tensor magnetic resonance imaging tractography in cognitive disorders. Curr. Opin. Neurol. 19, 599–606. doi: 10.1097/01.wco.0000247610.44106.3f
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
Conturo, T. E., Lori, N. F., Cull, T. S., Akbudak, E., Snyder, A. Z., Shimony, J. S.,et al. (1999). Tracking neuronal fiber pathways in the living human brain. Proc. Natl. Acad. Sci. U.S.A. 96, 10422–10427. doi: 10.1073/pnas.96.18.10422
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
Daianu, M., Jahanshad, N., Nir, T. M., Toga, A. W., Jack, C. R. Jr., Weiner, M. W.,et al. (2013). Breakdown of brain connectivity between normal aging and Alzheimer’s disease: a structural k-core network analysis. Brain Connect. 3, 407–422. doi: 10.1089/brain.2012.0137
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
Delbeuck, X., Van der Linden, M., and Collette, F. (2003). Alzheimer’s disease as a disconnection syndrome? Neuropsychol. Rev. 13, 79–92. doi: 10.1023/A:1023832305702
Dennis, E., Jin, Y., Kernan, C., Babikian, T., Mink, R., Babikian, T.,et al. (2015a). “White matter integrity in traumatic brain injury: effects of permissible fiber turning angle,” in Proceedings of the IEEE International Symposium on Biomedical Imaging, New York, NY.
Dennis, E. L., Jin, Y., Villalon-Reina, J. E., Zhan, L., Kernan, C. L., Babikian, T.,et al. (2015b). White matter disruption in moderate/severe pediatric traumatic brain injury: advanced tract-based analyses. Neuroimage Clin. 7, 493–505. doi: 10.1016/j.nicl.2015.02.002
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
Desikan, R. S., Segonne, F., Fischl, B., Quinn, B. T., Dickerson, B. C., Blacker, D.,et al. (2006). An automated labeling system for subdividing the human cerebral cortex on MRI scans into gyral based regions of interest. Neuroimage 31, 968–980. doi: 10.1016/j.neuroimage.2006.01.021
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
Fillard, P., Descoteaux, M., Goh, A., Gouttard, S., Jeurissen, B., Malcolm, J.,et al. (2011). Quantitative evaluation of 10 tractography algorithms on a realistic diffusion MR phantom. Neuroimage 56, 220–234. doi: 10.1016/j.neuroimage.2011.01.032
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
Fillard, P., Poupon, C., and Mangin, J. F. (2009). A novel global tractography algorithm based on an adaptive spin glass model. Med. Image. Comput. Comput. Assist. Interv. 12, 927–934. doi: 10.1007/978-3-642-04268-3_114
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
Fritze, F., Ehrt, U., Hortobagyi, T., Ballard, C., and Aarsland, D. (2011). Depressive symptoms in Alzheimer’s disease and lewy body dementia: a one-year follow-up study. Dement. Geriatr. Cogn. Disord. 32, 143–149. doi: 10.1159/000332016
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
García-Gomar, M., Concha, L., Alcauter, S., Abraham, J., Carrillo-Ruiz, J., Farfan, G.,et al. (2013). Probabilistic tractography of the posterior subthalamic area in Parkinson’s disease patients. J. Biomed. Sci. Eng. 6, 381–390. doi: 10.4236/jbise.2013.63A048
Girard, G., Whittingstall, K., Deriche, R., and Descoteaux, M. (2014). Towards quantitative connectivity analysis: reducing tractography biases. Neuroimage 98, 266–278. doi: 10.1016/j.neuroimage.2014.04.074
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
Holmes, C. J., Hoge, R., Collins, L., Woods, R., Toga, A. W., and Evans, A. C. (1998). Enhancement of MR images using registration for signal averaging. J. Comput. Assist. Tomogr. 22, 324–333. doi: 10.1097/00004728-199803000-00032
Hua, X., Hibar, D. P., Ching, C. R., Boyle, C. P., Rajagopalan, P., Gutman, B. A.,et al. (2013). Unbiased tensor-based morphometry: improved robustness and sample size estimates for Alzheimer’s disease clinical trials. Neuroimage 66, 648–661. doi: 10.1016/j.neuroimage.2012.10.086
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
Huang, H., Zhang, J., van Zijl, P. C., and Mori, S. (2004). Analysis of noise effects on DTI-based tractography using the brute-force and multi-ROI approach. Magn. Reson. Med. 52, 559–565. doi: 10.1002/mrm.20147
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
Iglesias, J. E., Liu, C. Y., Thompson, P. M., and Tu, Z. (2011). Robust brain extraction across datasets and comparison with publicly available methods. IEEE Trans. Med. Imaging 30, 1617–1634. doi: 10.1109/TMI.2011.2138152
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
Jahanshad, N., Aganj, I., Lenglet, C., Joshi, A., Jin, Y., Barysheva, M.,et al. (2011). “Sex differences in the human connectome: 4-Tesla high angular resolution diffusion imaging (HARDI) tractography in 234 young adult twins,” in Proceedings of the Eighth IEEE International Symposium on Biomedical Imaging (ISBI), Chicago, IL, 939–943. doi: 10.1109/ISBI.2011.5872558
Jahanshad, N., Zhan, L., Bernstein, M. A., Borowski, B. J., Jack, C. R., Toga, A. W.,et al. (2010). “Diffusion tensor imaging in seven minutes: determining trade-offs between spatial and directional resolution,” in Proceedings of the IEEE International Symposium on Biomedical Imaging (ISBI), Rotterdam, 1161–1164.
Jenkinson, M., Bannister, P., Brady, M., and Smith, S. (2002). Improved optimization for the robust and accurate linear registration and motion correction of brain images. Neuroimage 17, 825–841. doi: 10.1006/nimg.2002.1132
Jessen, F., Wolfsgruber, S., Wiese, B., Bickel, H., Mosch, E., Kaduszkiewicz, H.,et al. (2014). AD dementia risk in late MCI, in early MCI, and in subjective memory impairment. Alzheimers Dement. 10, 76–83. doi: 10.1016/j.jalz.2012.09.017
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
Jin, Y., Shi, Y., Joshi, S., Jahanshad, N., Zhan, L., de Zubicaray, G.,et al. (2011). Heritability of white matter fiber tract shapes: a HARDI study of 198 twins. Multimodal Brain Image Anal. 7012, 35–43. doi: 10.1007/978-3-642-24446-9_5
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
Jin, Y., Shi, Y., Zhan, L., de Zubicaray, G. I., McMahon, K. L., Martin, N. G.,et al. (2013). Labeling white matter tracts in HARDI by fusing multiple tract atlases with applications to genetics. Proc. IEEE Int. Symp. Biomed. Imaging 2013, 512–515.
Jin, Y., Shi, Y., Zhan, L., Gutman, B. A., de Zubicaray, G. I., McMahon, K. L.,et al. (2014). Automatic clustering of white matter fibers in brain diffusion MRI with an application to genetics. Neuroimage 100, 75–90. doi: 10.1016/j.neuroimage.2014.04.048
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
Jin, Y., Shi, Y., Zhan, L., Li, J., de Zubicaray, G., McMahon, K.,et al. (2012). Automatic population HARDI white matter tract clustering by label fusion of multiple tract atlases. Multimodal Brain Image Anal. 7509, 147–156. doi: 10.1007/978-3-642-33530-3_12
Jin, Y., Shi, Y., Zhan, L., and Thompson, P. (2015). “Automated multi-atlas labeling of the fornix and its integrity in Alzheimer’s disease,” in Proceedings of the IEEE International Symposium on Biomedical Imaging, New York, NY.
Kreher, B. W., Mader, I., and Kiselev, V. G. (2008). Gibbs tracking: a novel approach for the reconstruction of neuronal pathways. Magn. Reson. Med. 60, 953–963. doi: 10.1002/mrm.21749
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
Lazar, M., and Alexander, A. L. (2003). An error analysis of white matter tractography methods: synthetic diffusion tensor field simulations. Neuroimage 20, 1140–1153. doi: 10.1016/S1053-8119(03)00277-5
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
Lazar, M., Weinstein, D. M., Tsuruda, J. S., Hasan, K. M., Arfanakis, K., Meyerand, M. E.,et al. (2003). White matter tractography using diffusion tensor deflection. Hum. Brain Mapp. 18, 306–321. doi: 10.1002/hbm.10102
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
LeBihan, D. (1990). IVIM method measures diffusion and perfusion. Diagn. Imaging (San Franc.) 12, 133–136.
Leow, A. D., Yanovsky, I., Chiang, M. C., Lee, A. D., Klunder, A. D., Lu, A.,et al. (2007). Statistical properties of Jacobian maps and the realization of unbiased large-deformation nonlinear image registration. IEEE Trans. Med. Imaging 26, 822–832. doi: 10.1109/TMI.2007.892646
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
Liu, Y., Spulber, G., Lehtimaki, K. K., Kononen, M., Hallikainen, I., Grohn, H.,et al. (2011). Diffusion tensor imaging and tract-based spatial statistics in Alzheimer’s disease and mild cognitive impairment. Neurobiol. Aging 32, 1558–1571. doi: 10.1016/j.neurobiolaging.2009.10.006
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
Medina, D., DeToledo-Morrell, L., Urresta, F., Gabrieli, J. D., Moseley, M., Fleischman, D.,et al. (2006). White matter changes in mild cognitive impairment and AD: a diffusion tensor imaging study. Neurobiol. Aging 27, 663–672. doi: 10.1016/j.neurobiolaging.2005.03.026
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
Mesaros, S., Rocca, M. A., Kacar, K., Kostic, J., Copetti, M., Stosic-Opincal, T.,et al. (2012). Diffusion tensor MRI tractography and cognitive impairment in multiple sclerosis. Neurology 78, 969–975. doi: 10.1212/WNL.0b013e31824d5859
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
Mocks, J., and Verleger, R. (1986). Principal component analysis of event-related potentials: a note on misallocation of variance. Electroencephalogr. Clin. Neurophysiol. 65, 393–398. doi: 10.1016/0168-5597(86)90018-3
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
Moldrich, R. X., Pannek, K., Hoch, R., Rubenstein, J. L., Kurniawan, N. D., and Richards, L. J. (2010). Comparative mouse brain tractography of diffusion magnetic resonance imaging. Neuroimage 51, 1027–1036. doi: 10.1016/j.neuroimage.2010.03.035
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
Mori, S., Crain, B. J., Chacko, V. P., and van Zijl, P. C. (1999). Three-dimensional tracking of axonal projections in the brain by magnetic resonance imaging. Ann. Neurol. 45, 265–269. doi: 10.1002/1531-8249(199902)45:2<265::AID-ANA21>3.0.CO;2-3
Neher, P., Stieltjes, B., Reisert, M., Meinzer, H., and Fritzsche, K. (2012). “MITK global tractography,” in Proceedings of the DTI Tractography Challenge (MICCAI), Nice. doi: 10.1117/12.911215
Nir, T. M., Jahanshad, N., Villalon-Reina, J. E., Toga, A. W., Jack, C. R., Weiner, M. W.,et al. (2013). Effectiveness of regional DTI measures in distinguishing Alzheimer’s disease, MCI, and normal aging. Neuroimage Clin. 3, 180–195. doi: 10.1016/j.nicl.2013.07.006
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
Parker, G. J., Haroon, H. A., and Wheeler-Kingshott, C. A. (2003). A framework for a streamline-based probabilistic index of connectivity (PICo) using a structural interpretation of MRI diffusion measurements. J. Magn. Reson. Imaging 18, 242–254. doi: 10.1002/jmri.10350
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
Querfurth, H. W., and LaFerla, F. M. (2010). Alzheimer’s disease. N. Engl. J. Med. 362, 329–344. doi: 10.1056/NEJMra0909142
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
Schroeter, M. L., Stein, T., Maslowski, N., and Neumann, J. (2009). Neural correlates of Alzheimer’s disease and mild cognitive impairment: a systematic and quantitative meta-analysis involving 1351 patients. Neuroimage 47, 1196–1206. doi: 10.1016/j.neuroimage.2009.05.037
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
Smith, S. M. (2002). Fast robust automated brain extraction. Hum. Brain Mapp. 17, 143–155. doi: 10.1002/hbm.10062
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
Stebbins, G. T., and Murphy, C. M. (2009). Diffusion tensor imaging in Alzheimer’s disease and mild cognitive impairment. Behav. Neurol. 21, 39–49. doi: 10.1155/2009/915041
Todd, S., Barr, S., Roberts, M., and Passmore, A. P. (2013). Survival in dementia and predictors of mortality: a review. Int. J. Geriatr. Psychiatry 28, 1109–1124. doi: 10.1002/gps.3946
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
Wedeen, V. J., Rosene, D. L., Wang, R., Dai, G., Mortazavi, F., Hagmann, P.,et al. (2012). The geometric structure of the brain fiber pathways. Science 335, 1628–1634. doi: 10.1126/science.1215280
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
Ye, J. (2005). Generalized Low Rank Approximations of Matrices. Mach. Learn. 61, 167–191. doi: 10.1007/s10994-005-3561-6
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
Yuan, Z., and Zou, X. (2013). Global threshold dynamics in an HIV virus model with nonlinear infection rate and distributed invasion and production delays. Math. Biosci. Eng. 10, 483–498. doi: 10.3934/mbe.2013.10.483
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
Zhan, L., Franc, D., Patel, V., Jahanshad, N., Jin, Y., Mueller, B. A.,et al. (2012a). “How do spatial and angular resolution affect brain connectivity maps from diffusion MRI?” in Proceedings of the 9th IEEE International Symposium on Biomedical Imaging, Barcelona, 1–6.
Zhan, L., Mueller, B. A., Jahanshad, N., Jin, Y., Lenglet, C., Yacoub, E.,et al. (2012b). Magnetic resonance field strength effects on diffusion measures and brain connectivity networks. Brain Connect. 3, 72–86. doi: 10.1089/brain.2012.0114
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
Zhan, L., Jahanshad, N., Ennis, D. B., Jin, Y., Bernstein, M. A., Borowski, B. J.,et al. (2013a). Angular versus spatial resolution trade-offs for diffusion imaging under time constraints. Hum. Brain Mapp. 34, 2688–2706. doi: 10.1002/hbm.22094
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
Zhan, L., Jahanshad, N., Jin, Y., Toga, A. W., McMahon, K. L., de Zubicaray, G. I.,et al. (2013b) “Brain network efficiency and topology depend on the fiber tracking method: 11 tractography algorithms compared in 536 subjects,” in Proceedings of the 10th IEEE International Symposium on Biomedical Imaging, San Francisco, CA, 1134–1137.
Keywords: Alzheimer’s disease, brain network, tractography, classification, PCA, GLRAM, diffusion MRI
Citation: Zhan L, Zhou J, Wang Y, Jin Y, Jahanshad N, Prasad G, Nir TM, Leonardo CD, Ye J, Thompson PM and Alzheimer’s Disease Neuroimaging Initiative (2015) Comparison of nine tractography algorithms for detecting abnormal structural brain networks in Alzheimer’s disease. Front. Aging Neurosci. 7:48. doi: 10.3389/fnagi.2015.00048
Received: 20 January 2015; Paper pending published: 07 March 2015;
Accepted: 25 March 2015; Published online: 14 April 2015
Edited by:
Fernanda Laezza, University of Texas Medical Branch, USACopyright © 2015 Zhan, Zhou, Wang, Jin, Jahanshad, Prasad, Nir, Leonardo, Ye, Thompson and Alzheimer’s Disease Neuroimaging Initiative. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Paul M. Thompson and Liang Zhan, Imaging Genetics Center, University of Southern California, 4676 Admiralty Way, Suite 400, Marina del Rey, Los Angeles, CA 90292, USAcHRob21wQHVzYy5lZHU=;emhhbi5saWFuZ0BnbWFpbC5jb20=
†These authors have contributed equally to this work.
‡Data used in preparing this article were obtained from the Alzheimer’s Disease Neuroimaging Initiative (ADNI) database (adni.loni.usc.edu). As such, the investigators within the ADNI contributed to the design and implementation of ADNI and/or provided data but most of them did not participate in this analysis or writing this report. A complete list of ADNI investigators can be found at: http://adni.loni.usc.edu/wp-content/uploads/how_to_apply/ADNI_Acknowledgement_List.pdf
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.