 Neel I. Nissen1*
Neel I. Nissen1* Astrid Z. Johansen2
Astrid Z. Johansen2 Inna M. Chen2Christina Jensen1Emilie A. Madsen1Carsten P. Hansen3Jeppe Thorlacius-Ussing1Morten Karsdal1Julia S. Johansen2,4,5Hadi M. H. Diab6
Inna M. Chen2Christina Jensen1Emilie A. Madsen1Carsten P. Hansen3Jeppe Thorlacius-Ussing1Morten Karsdal1Julia S. Johansen2,4,5Hadi M. H. Diab6 Lars N. Jørgensen4,6Nicholas Willumsen1
Lars N. Jørgensen4,6Nicholas Willumsen1- 1Nordic Bioscience A/S, Herlev, Denmark
- 2Department of Oncology, Copenhagen University Hospital, Gentofte, Denmark
- 3Department of Surgery, Copenhagen University Hospital – Rigshospitalet, Copenhagen, Denmark
- 4Institute of Clinical Medicine, Faculty of Health and Medical Sciences, University of Copenhagen, Copenhagen, Denmark
- 5Department of Medicine, Copenhagen University Hospital, Gentofte, Denmark
- 6Digestive Disease Center, Bispebjerg and Frederiksberg Hospital, University of Copenhagen, Copenhagen, Denmark
Introduction: Pancreatic ductal adenocarcinoma (PDAC) is characterized by a pronounced fibrotic tumor microenvironment, which impairs treatment response. Type I and V collagens are responsible for the densely packed fibrils in the tumor fibrosis environment. While the role of the major type I collagen in cancer is well described, less is known about the minor type V collagen. Quantifying collagen propeptides in serum has been shown to have prognostic and predictive value. In this study, we evaluated the clinical utility of measuring the propeptide of type V collagen (PRO-C5) in serum from a discovery cohort and a validation cohort of patients with PDAC as well as in non-pancreatic solid tumor types to explore the relevance of the PRO-C5 biomarker in cancer.
Methods: Serum PRO-C5 was measured in three cohorts: a discovery cohort (19 healthy controls, 12 patients with chronic pancreatitis and 33 patients with PDAC (stage I-IV)), a validation cohort (800 patients with PDAC (stage I-IV)), and a non-pancreatic solid tumor type cohort of 33 healthy controls and 200 patients with 10 different non-pancreatic solid tumor types. The levels of serum PRO-C5 in patients with cancer were compared to levels in healthy controls. The association between PRO-C5 levels and overall survival (OS) was evaluated in patients with PDAC after adjusting for established prognostic factors.
Results: PRO-C5 was significantly increased in serum from patients with PDAC compared to healthy controls (p < 0.001). High PRO-C5 levels were significantly associated with short OS in both the discovery- and the validation cohort, especially in early stages of PDAC (validation cohort stage II, HR = 2.0, 95%CI1.2-3.4). The association was independent of other prognostic parameters including stage, performance status and CA19-9. Furthermore, serum levels of PRO-C5 were significantly increased in serum from patients with other non-pancreatic solid tumor types compared to healthy controls.
Conclusion: High levels of serum PRO-C5 is prognostic for short OS in patients with PDAC and may provide clinical value in many other tumor types beyond PDAC. This underlines the importance of type V collagen in tumor fibrosis. PRO-C5 could have the potential to be used in several aspects within drug discovery, patient stratification and drug efficacy.
1 Introduction
Pancreatic ductal adenocarcinoma (PDAC) is a devastating disease as only 20% of the patients have resectable disease (McGuigan et al., 2018; Klein, 2019; Khalaf et al., 2021; Siegel et al., 2021). The remaining patients can only be offered palliative oncologic treatment or best supportive care (McGuigan et al., 2018). However, there is a high degree of treatment resistance to oncologic treatment. One explanation is an extremely fibrotic PDAC tumor microenvironment. Tumor fibrosis cause increased interstitial pressure, which in turn reduces drug delivery (Heldin et al., 2004; Thomas and Radhakrishnan, 2019). In addition, tumor fibrosis inhibits T-cell activity and migration, which results in diminished efficacy of immunotherapy (Mariathasan et al., 2018; Chen et al., 2021; Ogawa et al., 2021; Grout et al., 2022; Lander et al., 2022). Therefore, there is a high need for novel strategies to overcome tumor fibrosis in the treatment of patients with PDAC and consequently to identify tumors with high fibrotic activity.
Tumor fibrosis is characterized by an augmented activity of cancer-associated fibroblasts (CAFs), responsible for an abnormal extracellular matrix (ECM) remodeling (Nissen et al., 2019). The CAF-mediated ECM remodeling results in degradation of existing collagen fibers that are replaced by new and more densely packed collagen fibers, creating a stromal barrier surrounding the tumor cells (Nissen et al., 2019) (Winkler et al., 2020). Type I collagen is the most abundant CAF-derived fibrillar collagen and a major component of the collagen fibers that play important roles during tumor progression (Menke et al., 2001; Armstrong et al., 2004; Cheng and Leung, 2011; Gao et al., 2016; Barcus et al., 2017; Chen et al., 2022). The pathogenic phenotype of CAFs was originally thought to derive from the ability to produce large quantities of collagen, but recent studies focusing on type I collagen have emphasized the importance of the collagen quality and fiber architecture, as a central component in its tumorigenic capacity (Chen et al., 2022; Su et al., 2022). Interestingly, the minor fibrillar type V collagen has been suggested to be a key regulator of type I collagen architecture.
Type V collagen has many roles in the healthy ECM, as it binds to different ECM proteins such as other collagens, TGF-β, elastin and metalloproteinases, thereby modulating cellular behavior (Symoens et al., 2010). The most abundant isoform of type V collagen consist of two α1 chains and one α2 chain that forms a heterotrimer. In healthy tissue, type I and V collagen have a very close relationship, as the two collagens copolymerize into heterotypic fibrils (Wenstrup et al., 2004; Aszódi et al., 2006; Sun et al., 2011) (Figure 1). The binding of type V collagen to type I collagen is important for structural integrity and deficiency of type V collagen results in disorders like Ehlers-Danlos syndrome and corneal disease, which are characterized by abnormal collagen fibrils (Mak et al., 2016). Type V collagen deficient mice (COL5a1−/−) embryos die already at day 10.5 as they also lack type I collagen fibrils. Moreover, heterozygous type V collagen mice (COL5a1−/+) survive, but show 50% decrease in collagen content and fibrillar density (Wenstrup et al., 2004). Thus, the binding between type V and I collagen results in a homeostatic fibril structure and tissue architecture. However, a complete understanding of its role in tumor progression remains (Mak et al., 2016). In comparison to type I collagen, type V collagen is expressed in relatively low levels in healthy tissues. In cancer, type V collagen, especially the α2 chain, has been shown to be upregulated in colorectal, gastric and breast cancer and is associated with PDAC cell proliferation, invasion, metastasis, and angiogenesis (Barsky et al., 1982; Imamura et al., 1995; Sun et al., 2011; Berchtold et al., 2015; Mak et al., 2016; Huang et al., 2017; Ren et al., 2018; Tan and Chen, 2018; Balancin et al., 2020; Wang et al., 2021a; Tan et al., 2021). Altogether, this indicates, that type V collagen may be a key factor in determining fibrillar density and hence tumor fibrosis.
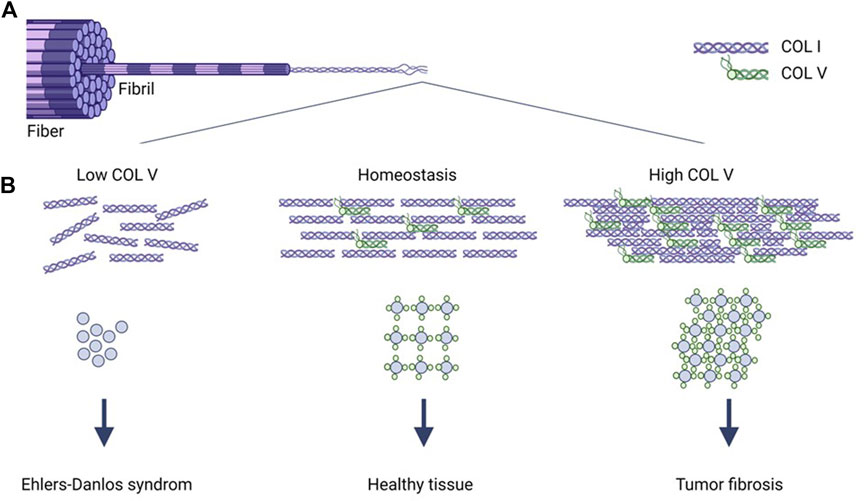
FIGURE 1. Type V collagen regulates type I collagen architecture. Collagen fibers consist of collagen fibrils, which are made up by self-assembled collagen microfibrils (A). Type V collagen is incorporated into the type I collagen microfibril structure, where it during homeostasis regulates structural integrity of type I collagen (B). Type V collagen (low COLV) deficiency results in abnormal type I collagen fibrils and the well-known Ehlers-Danlos syndrome (B). Augmented type V collagen expression (high COLV) results in more condensed and linearized type I collagen fibrils and dense fibers characteristic of tumor fibrosis (B). COLI, type I collagen; COLV, type V collagen.
The present study explored the biomarker potential of measuring the C-propeptide of the α2 chain of type V collagen (PRO-C5) in serum from a discovery cohort and a validation cohort of patients with PDAC as well as in 10 non-pancreatic solid tumor types to explore if the PRO-C5 biomarker had relevance in PDAC and other tumor types.
2 Materials and methods
2.1 Patients
The PDAC discovery cohort (Cohort 1), consisted of 19 age- and sex-matched healthy controls, 12 patients with chronic pancreatitis and 33 patients with PDAC (stage I-IV). The PDAC validation cohort (Cohort 2), consisted of 800 patients with PDAC (stage I-IV). Serum samples from patients with chronic pancreatitis and PDAC in cohort 1 and 2 were from the Danish BIOPAC study “Biomarkers in patients with pancreatic cancer (BIOPAC) – can they provide new information of the disease and improve diagnosis and prognosis of the patients” (ClinicalTrials.gov ID: NCT03311776). The study has been described elsewhere (Chen et al., 2019; Bagni et al., 2020; Nissen et al., 2021a; Nissen et al., 2022). The study was carried out in accordance with the Danish Regional Committee on Health Research Ethics. The BIOPAC protocol was approved by the Danish Regional Committee on Health Research Ethics (VEK ref. KA-20060113; and the retrospective protocol VEK H-17039022) and the Data Protection Agency (j.nr. 2006-41-6848, 2012-58-0004, HGH-2015-027; I-Suite j. nr. 03960; and PACTIUS P-2020-834). All subjects gave written informed consent in accordance with the Declaration of Helsinki, version 8. Serum samples were collected before operation or before start of palliative chemotherapy. Clinical data were collected prospectively. The patients were followed until September 2022 or death, whichever came first. Serum samples were measured blinded without information of the clinical characteristics. Clinical data included age, sex, stage (American Joint Commission on Cancer, eighth edition), number of metastatic sites, liver metastasis, body mass index (BMI), diabetes, tobacco use, alcohol use, carbohydrate antigen 19-9 (CA19-9), performance status (PS), Charlson age comorbidity index (CACI) and overall survival (OS). Cohort 3 consisted of 33 age and sex matched healthy controls and 200 patients with different types of non-pancreatic cancers: bladder (n = 20), breast (n = 20), colorectal (n = 20), head and neck (n = 20), kidney (n = 20), lung (n = 20), malignant melanoma (n = 20), ovarian (n = 20), prostate (n = 20), and stomach (n = 20). Serum from patients with cancer in cohort 3 were obtained from the commercial vendor Proteogenex (CA, United States). Healthy controls in cohort 1 and 3 were obtained from Valley BioMedical (VA, United States) and BioIVT (Westbury, NY, United States), respectively. Appropriate Institutional Review Board/Independent Ethical Committee approved sample collection and all subjects filed for informed consent. Patient demographics for cohort 1, 2 and 3 are shown in Tables 1, 2, respectively.
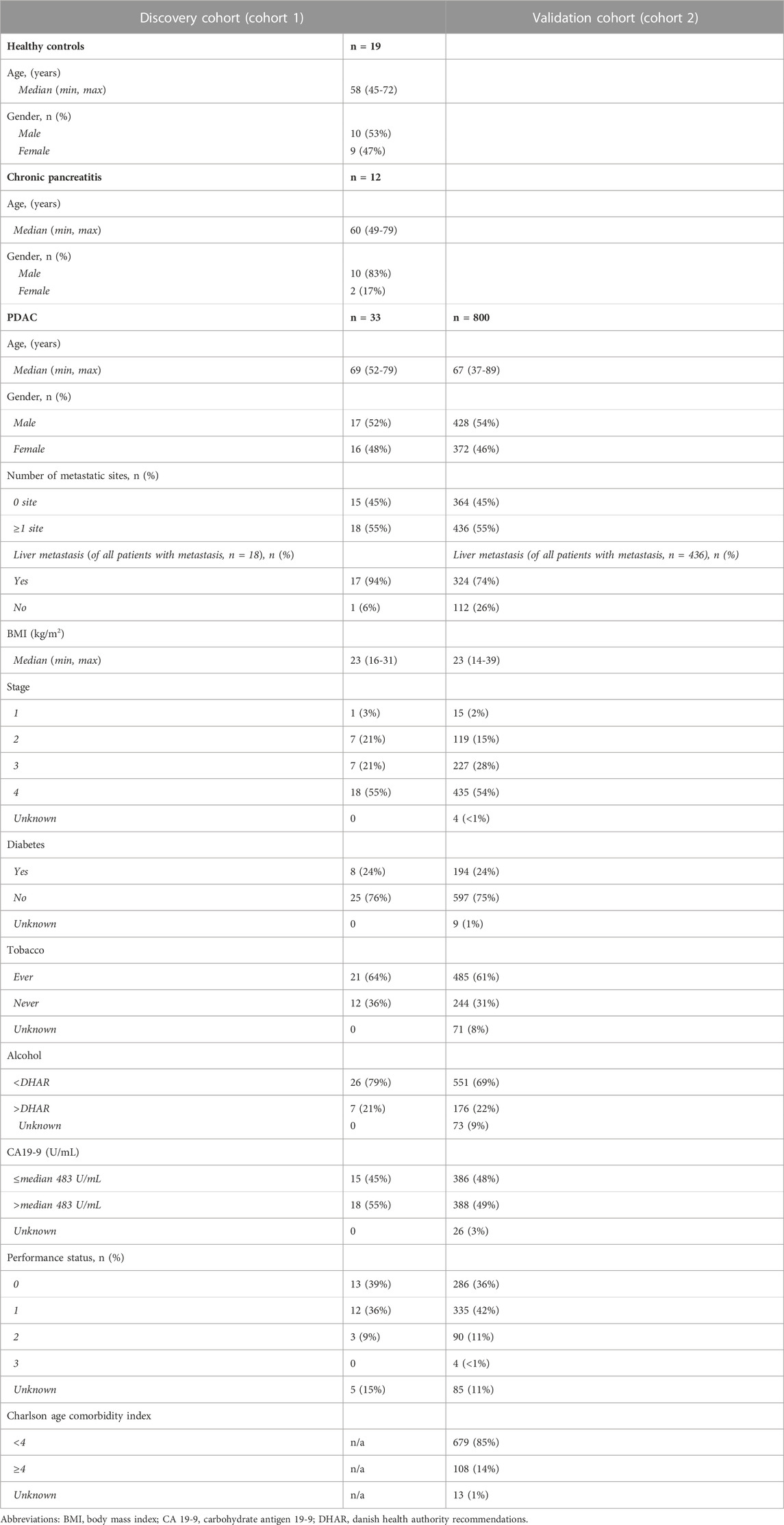
TABLE 1. Patient demographics for Cohort 1 and Cohort 2.
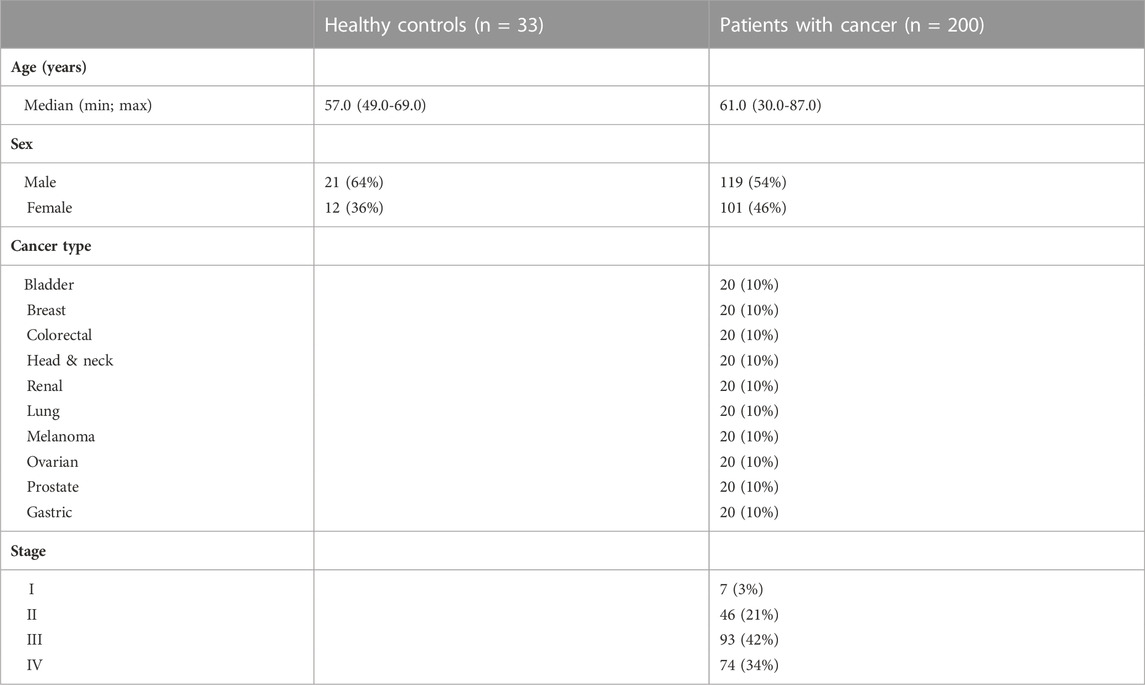
TABLE 2. Patient demographics for Cohort 3.
2.2 Assessment of the C-propeptide of type V collagen fragments (PRO-C5) in human serum
Serum levels of the C-propeptide of type V collagen were measured using the ELISA based assay PRO-C5 according to manufacturer´s instruction (Nordic Bioscience A/S, Denmark). The technical details of the assays have previously been described (Vassiliadis et al., 2011; Vassiliadis et al., 2012).
2.3 Statistics
Biomarker results were reported in accordance with the REMARK (reporting recommendations for tumor marker prognostic study) guidelines (Altman et al., 2012). A Kruskal–Wallis multiple comparison test was used to test the difference between PRO-C5 serum levels in healthy controls, and patients with either chronic pancreatitis or PDAC (cohort 1) as well as for PRO-C5 serum levels in healthy controls and in 10 different cancer indications (cohort 3). Non-parametric Mann Whitney tests were used to assess associations with PRO-C5 serum levels in early (stage I-II) and late (stage III-IV) stages of PDAC in cohort 1 and cohort 2. Kaplan-Meier curves were used to assess the association between high and low serum levels of PRO-C5 and OS. To provide granularity on the association between PRO-C5 and overall survival, and to explore a potential cut off proximity to be tested in the validation cohort, the patients in the discovery cohort, cohort 1, were stratified into four groups based on quartiles (Q1, Q2, Q3 and Q4). In cohort 2, patients were stratified based on the 75th percentile, meaning Q1-Q3 vs. Q4 (cut-off: 832 ng/ml). When exploring the association between PRO-C5 serum levels and OS in specific stages of PDAC, patients were stratified based on the 75th percentile, meaning Q1-Q3 vs. Q4 (Stage II cut-off 725 ng/ml; stage III cut-off 792 ng/ml; stage IV cut-off 841 ng/ml). In cohort 1, a univariate Cox proportional-hazard regression model was used to calculate the hazard ratios (HR) with 95% confidence interval (Cl) for short OS per PRO-C5 biomarker levels (Q4, or Q3 or Q2 vs. Q1). In cohort 2, a univariate Cox proportional-hazard regression model was used to calculate the hazard ratios (HR) with 95% confidence interval (Cl) for short OS per PRO-C5 biomarker levels (continuous and Q1-Q3 vs. Q4) and clinical covariates: age (continuous), gender (female vs. male), number of metastatic sites (≥1 vs. 0), liver metastasis (yes vs. no), BMI (continuous), stage (I-II vs. III-IV), diabetes (yes vs. no), tobacco use (ever vs. never), alcohol use (below and above the Danish Health Authority recommendations [DHAR]), CA19-9 (>median vs. ≤ median [median = 483 U/mL]), PS (1 + 2 + 3 vs. 0) and CACI (≥4 vs. < 4). In addition, in cohort 2, a multivariate Cox proportional-hazard regression models including PRO-C5 (continuous and Q1-Q3 vs. Q4), age, metastatic sites (≥1 vs. 0), liver metastasis (yes vs. no), stage (I-II vs. III-IV), CA19-9 (>median vs. ≤ median [median = 483 U/mL]), PS (1 + 2 + 3 vs. 0) and CACI (≥4 vs. < 4) was used to evaluate potential independent prognostic value of the PRO-C5 biomarker for predicting OS. When the model was used for patients in individual stages only age, CA19-9 (>median vs. ≤ median [median = 483 U/mL]), PS (1 + 2 + 3 vs. 0) and CACI (≥4 vs. < 4) were included for stage II and III. For stage IV, age, CA19-9 (>median vs. ≤ median [median = 483 U/mL]), PS (1 + 2 + 3 vs. 0), CACI (≥4 vs. < 4), number of metastatic sites (≥1 vs. 0) and liver metastasis (yes vs. no) were included. Patients in disease stage I were not analyzed due to the low number of patients in this group (n = 15). A p-value of p < 0.05 was considered statistically significant. Graph design and statistical analyses were performed using GraphPad Prism Version 9 (GraphPad Software, Inc.) and MedCalc version 19.3 (Medcalc Software).
3 Results
3.1 PRO-C5 is elevated in patients with PDAC and associates with poor OS–Discovery cohort
In the discovery cohort, cohort 1, PRO-C5 was significantly elevated in serum from patients with PDAC compared to healthy controls (median PRO-C5 values: PDAC 1071 ng/ml vs. healthy controls 550 ng/ml, p < 0.001). PRO-C5 was not significantly increased in patients with chronic pancreatitis (median PRO-C5 value 786 ng/ml) compared to healthy controls nor in patients with PDAC compared to chronic pancreatitis (Figure 2A). When stratifying patients with PDAC into early and late stage (stage I-II vs. III-IV), patients in late stage PDAC had significantly increased PRO-C5 (median PRO-C5 values: 635 ng/ml vs. 1360 ng/ml, respectively, p = 0.0018) (Figure 2B).
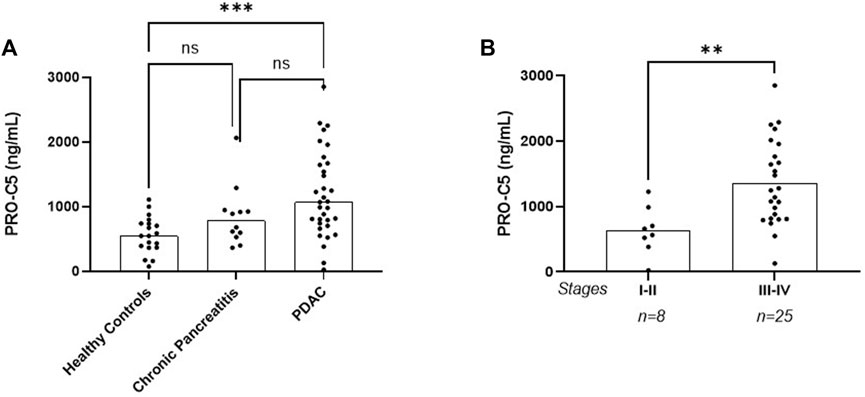
FIGURE 2. PRO-C5 is elevated in serum from patients with pancreatic ductal adenocarcinoma (PDAC) in the discovery cohort. (A) Individual serum PRO-C5 levels in patients with PDAC (n = 33), chronic pancreatitis (n = 12) and healthy controls (19). Differences in PRO-C5 levels between disease indication were analyzed with a Kruskal–Wallis multiple comparison test non-parametric test. (B) Individual serum PRO-C5 levels in patients with early (stage I-II) and late (stage III-IV) stage PDAC. Differences in PRO-C5 levels between early and late stage PDAC were analyzed with a non-parametric Mann Whitney test. Ns, p > 0.05; **p < 0.01; ***p < 0.001.
To investigate the association between PRO-C5 serum levels and OS, we assessed the prognostic potential of PRO-C5 by Kaplan-Meier curves and a univariate Cox proportional-hazard model. Patients were stratified into quartiles i.e., Q1 containing patient with the lowest levels of PRO-C5 and Q4 containing patients with the highest levels of PRO-C5. Patients in Q1, Q2, Q3 and Q4 had median OS of 28.0 months, 7.1 months, 15.5 months, and 3.8 months, respectively (log-rank, p = 0.0005). Thus, the difference in median OS between Q4 and Q1 were more than 2 years (24.2 months) (Figure 3). In support, univariate Cox proportional-hazard model showed that patients in Q4 had a 940% increased risk of mortality compared with patients in Q1 (Q4 vs. Q1: HR = 10.4, 95% CI 2.9-37.2, p = 0.0003) (Figure 3). There was no significant difference in risk of mortality and PRO-C5 levels between Q4 vs. Q2 and Q4 vs. Q3 (Figure 3).
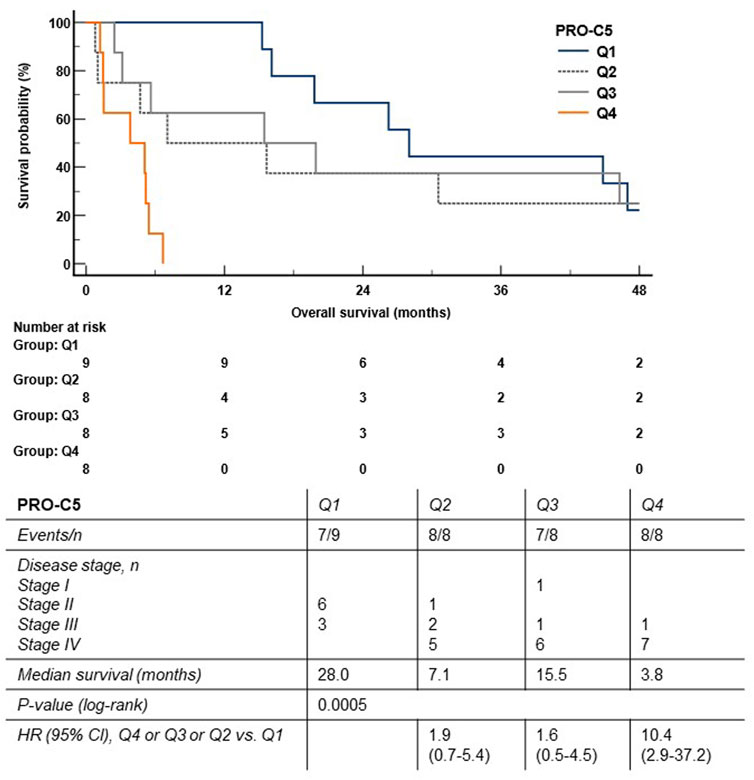
FIGURE 3. High levels of serum PRO-C5 were associated with short overall survival in the discovery cohort. The Kaplan-Meier survival plot shows the association between overall survival and serum PRO-C5. Patients were stratified into quartiles (Q1 (blue) patient with the lowest PRO-C5; and Q4 (orange) patients with the highest levels of PRO-C5). Hazard ratios (HR), 95% confidence intervals (CI) and log-rank test are shown.
3.2 PRO-C5 is elevated in patients with PDAC and associates with poor OS–Validation cohort
In the validation cohort, cohort 2, we were overall able to confirm the findings from the discovery cohort including a PRO-C5 increase in late stage PDAC compared to early stage PDAC (p = 0.004) (Figure 4A). To evaluate the association between PRO-C5 serum levels and OS in the PDAC validation cohort, patients were stratified into two groups based on the quartiles similar to the approach used in cohort 1 above: one containing patients with low levels of serum PRO-C5 (below the Q4 percentile), and another containing patients with high levels of serum PRO-C5 (above the Q4 percentile). Patients with low and high PRO-C5 had a median OS of 10.1 and 6.4 months, respectively (log-rank p < 0.0001) (Figure 4B). In addition, univariate Cox proportional-hazard modelling showed that patients with high levels of PRO-C5 had a 50% higher risk of mortality as compared to patients with low levels of PRO-C5 (High PRO-C5 vs. low PRO-C5: HR = 1.5, 95% CI 1.3-1.8, p < 0.0001) (Figure 4B and Table 3). To evaluate if the association of OS and PRO-C5 was independent of clinical covariates, a multivariate Cox proportional-hazard model including age, number of metastatic sites, liver metastasis, stage, CA19-9, PS and CACI was performed. The model showed that the prognostic value of PRO-C5 remained statistically significant when adjusting for these clinical covariates (HR = 1.4, 95% CI 1.2-1.7, p = 0.0001) (Table 3), which indicated that PRO-C5 is a risk factor independent of other common risk factors.
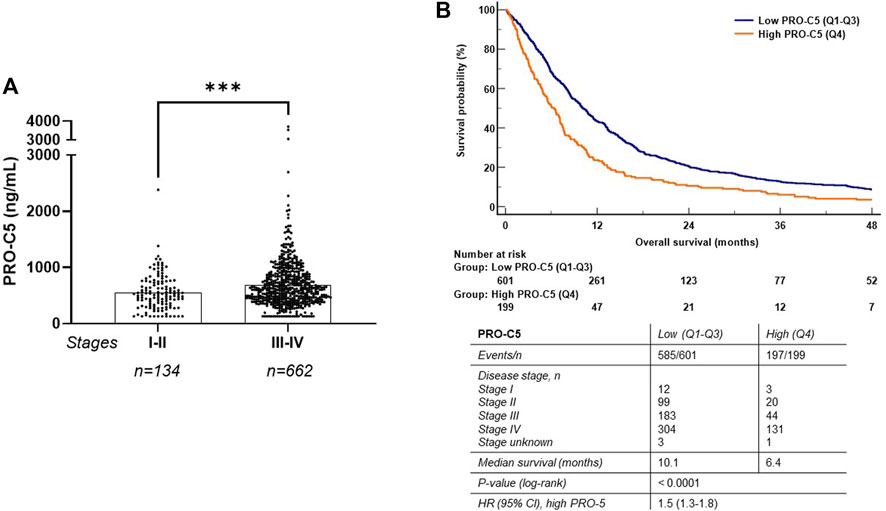
FIGURE 4. High levels of serum PRO-C5 were associated with short overall survival in the validation cohort. (A) Individual serum PRO-C5 levels in patients with early (stage I-II) and late (stage III-IV) PDAC. Differences in PRO-C5 levels between early and late stage PDAC were analyzed with a non-parametric Mann Whitney test. (B) A Kaplan-Meier survival plot shows the association between overall survival and levels of PRO-C5. Patients were stratified into low (Q1-Q3, blue) and high (Q4, orange) PRO-C5 (cutoff, 832 ng/ml). Hazard ratios (HR), 95% confidence intervals (CI) and log-rank test are shown. ***p < 0.001.
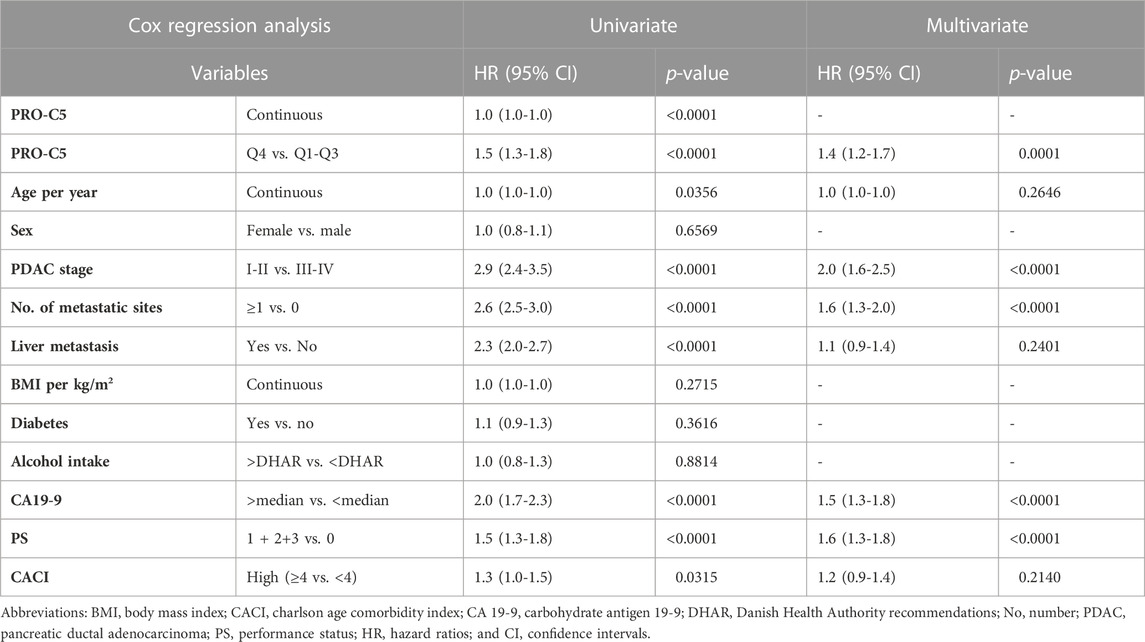
TABLE 3. Uni- and multivariate cox regression analysis in 800 patients with pancreatic ductal adenocarcinoma stage I-IV.
Next, we wanted to gain more granularity on the association between high serum PRO-C5 and OS in patients stratified into specific stages of PDAC. Patients in disease stage I were not analyzed due to the low number of patients in this group (n = 15). For each cancer stage, patients were stratified into high and low PRO-C5 using the 75th percentile as a cutoff.
Patients with stage II disease (n = 117) and low levels of PRO-C5 had a medium OS at 24.3 months compared to 8.5 months in patients with low PRO-C5 (log rank test, p = 0.0041) (Figure 5A). Thus, the difference in median OS between the two groups was more than 1 year (15.8 months). Univariate Cox proportional-hazard model showed that patients with stage II PDAC and high levels of PRO-C5 had a 100% increased risk of death compared to patients with low PRO-C5 (HR = 2.0, 95% CI 1.2-3.3, p = 0.0049) (Figure 5A). A multivariate Cox proportional-hazard model including age, CA19-9, PS and CACI showed that the association between high PRO-C5 and short OS was independent of the clinical variables in patients with stage II disease (HR = 2.0, 95% CI 1.2-3.4, p = 0.010) (Table 4).
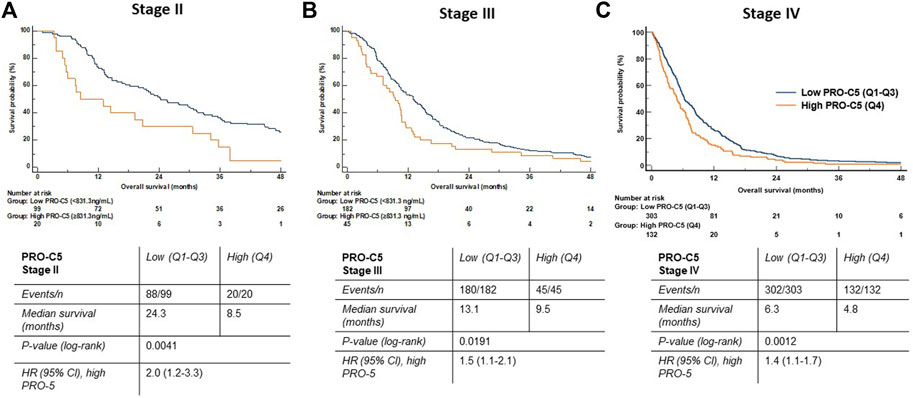
FIGURE 5. High levels of serum PRO-C5 were associated with short overall survival in patients with PDAC according to stage II, III and IV in the validation cohort. Kaplan-Meier survival plots show the association between overall survival and levels of PRO-C5 in stage II (A), stage III (B) and stage IV patients (C). In all plots, patients were stratified into low (Q1-Q3, blue) and high (Q4, orange) PRO-C5 (Stage II: cut-off 725 ng/ml, stage III: cut-off 792 ng/ml, stage IV: cut-off 841 ng/ml). Hazard ratios (HR), 95% confidence intervals (CI) and log-rank test are shown.
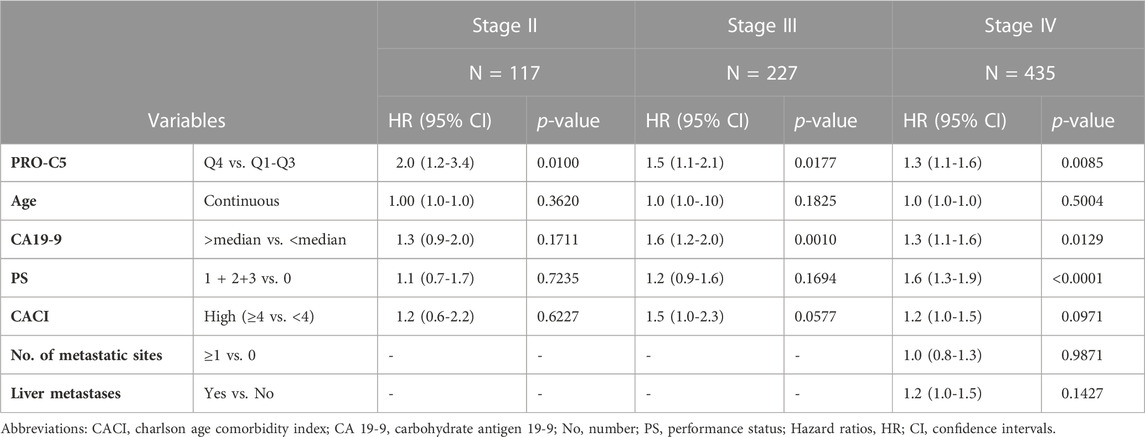
TABLE 4. Multivariate Cox proportional-hazard regression model in patients with pancreatic ductal adenocarcinoma divided into stage II, III and IV.
Patients with stage III disease (n = 227) and low levels of PRO-C5 had a median OS of 13.1 months compared to 9.5 months in patients with high PRO-C5 (log rank test, p = 0.0191) (Figure 5B). Univariate Cox proportional-hazard model showed that patients with stage III disease and high PRO-C5 had a 50% increased risk of death compared to patients with low PRO-C5 (HR = 1.5, 95% CI 1.1-2.1, p = 0.0191) (Figure 5B). A multivariate Cox proportional-hazard model including age, CA19-9, PS and CACI showed that the association between high PRO-C5 and short OS was independent of the clinical variables in patients with stage III disease (HR = 1.5, 95% 1.1-2.1, p = 0.0177) (Table 4).
Patients with stage IV disease (n = 435) and low levels of PRO-C5 had a median OS of 6.3 months compared to 4.8 months in patients with high PRO-C5 (log rank test, p = 0.0012) (Figure 5C). Univariate Cox proportional-hazard model showed that patients with stage IV disease and high PRO-C5 had a 40% increased risk of death compared to patients with low PRO-C5 (HR = 1.4, 95% CI 1.1-1.7, p = 0.0012) (Figure 5C). A multivariate Cox proportional-hazard model including age, CA19-9, PS, CACI, number of metastatic sites and liver metastasis showed that the association between high PRO-C5 and short OS was independent of the clinical variables in patients with stage IV disease (HR = 1.3, 95% CI 1.1-1.6, p = 0.0085) (Table 4).
3.3 PRO-C5 is increased in serum from patients with different non-pancreatic types of cancer
Next, we wanted to explore the PRO-C5 biomarker potential in other non-pancreatic cancer types (cohort 3). Bladder-, breast-, colorectal-, head and neck-, kidney-, lung-, ovarian cancer and melanoma had significantly elevated PRO-C5 levels compared to healthy controls (p < 0.05 to 0.0001), whereas this was not found for patients with prostate- and stomach cancer Figure 6. PRO-C5 levels for individual stages in each cancer disease can be seen in S1.
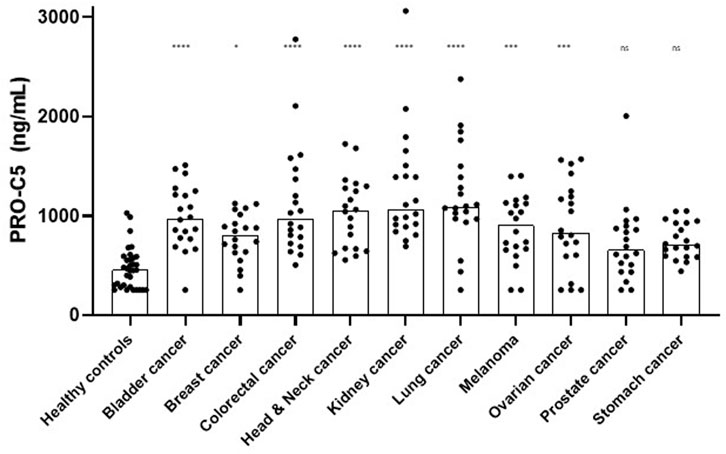
FIGURE 6. PRO-C5 was elevated in serum from patients with different types of cancer. PRO-C5 individual measurements in patients with different non-pancreatic types of cancer: bladder cancer (n = 20), breast cancer (n = 20), colorectal cancer (n = 20), head and neck cancer (n = 20), kidney cancer (n = 20), lung cancer (n = 20), malignant melanoma (n = 20), ovarian cancer (n = 20), prostate cancer (n = 20) or stomach cancer (n = 20); and compared to healthy controls (n = 33). Bar plots showing the median PRO-C5 value. A Kruskall-Wallis test was used to analyze the difference in PRO-C5 between cancer types. Ns, non-significant; *p < 0.05; ***p < 0.001; ****p < 0.0001.
4 Discussion
In this study we evaluated the biomarker potential of measuring the α2 chain of the type V collagen C-propeptide (PRO-C5) in serum from patients with cancer. In a discovery cohort we found that serum PRO-C5 was increased in patients with PDAC compared to healthy controls. Furthermore, high levels of PRO-C5 were associated with locally advanced or metastatic PDAC and patients with PDAC with high serum PRO-C5 had increased risk of dying compared to patients with low levels. The results were validated in a large group of 800 patients with PDAC where high PRO-C5 was associated with poor OS in stage II, III and IV independent of other risk factors including PS and CA19-9. Interestingly, the largest relative difference in OS was seen for patients in stage II where the median OS was more than 1 year longer in patients with low PRO-C5 compared to patients with high PRO-C5. In comparison, CA19-9 was also independently associated with OS in patients with stage III and IV disease, but not for patients in stage II. We also showed a relevance of PRO-C5 in other solid tumor types as supported by the gene-expression of the α2 chain that has been shown to be upregulated in many different types of cancer indications (Barsky et al., 1982; Imamura et al., 1995; Sun et al., 2011; Berchtold et al., 2015; Mak et al., 2016; Huang et al., 2017; Ren et al., 2018; Tan and Chen, 2018; Balancin et al., 2020; Wang et al., 2021a; Tan et al., 2021).
Similar to PRO-C5, other biomarkers originating from the tumor fibrotic compartment have shown potential as prognostic and predictive biomarkers in various types of cancers including PDAC (SN et al., 2018; Willumsen et al., 2018; Jensen et al., 2020a; Jensen et al., 2020b; Nissen et al., 2021a; Nissen et al., 2021b; Wang et al., 2021b; Jensen et al., 2021; Nissen et al., 2022; Willumsen et al., 2022). PRO-C3, measuring the formation of type III collagen, has been reported to be prognostic for OS in patients with PDAC (Willumsen et al., 2019; Chen et al., 2020; Nissen et al., 2022). Moreover, the turnover of type III collagen is predictive of response to PEGPH20, an experimental anti-fibrotic drug (Wang et al., 2021b). Like type I collagen, type III collagen is a major fibrillar collagen present in both healthy and diseased tissue (Ricard-Blum, 2011). In contrast to type I and type III collagen which make up the bulk of a fiber, type V collagen is regarded as a minor collagen assisting the major fibrillar collagens in the assembly of a fiber. Lately, other minor collagens, such as the fibrillar type XI and the FACIT collagens (type XIX, XX and XXII) have gained interest as more disease specific biomarkers and/or targets. Similar to what we show for type V collagen here, our group have earlier shown that biomarkers that measure type XI, XIX, XX and XXII collagens are also upregulated in different types of cancers (Thorlacius-Ussing et al., 2020; Nissen et al., 2021a; Madsen et al., 2022; Thorlacius-Ussing et al., 2022). In addition, high serum levels of type XI, XX and XXII collagens were all prognostic for short OS in patients with PDAC (Nissen et al., 2021a; Madsen et al., 2022; Thorlacius-Ussing et al., 2022). These minor collagens are mainly expressed in high levels during embryogenesis and in cancer progression, compared to the relative upregulation of major collagens, which are already present in high amount. Despite the fact that the major type I collagen is important for tumor progression and interacts closely with type V collagen, a biomarker measuring serum type I collagen formation was not increased in the same cohort of different tumor types compared to controls as measured here for PRO-C5 (cohort 3) (Madsen et al., 2022). This supports, that alterations in tumor fibrosis goes beyond type I collagen. Part of this explanation may be that type I collagen is the most abundant protein in the body, and therefore may have less sensitivity as a serological biomarker than the less abundant minor type V collagen, which also underlines the important role of type V collagen in tumor fibrosis. PRO-C5 may have the potential to be used as a treatment guide already in stage II PDAC, and to monitor drug efficacy and detect responders to different treatments. Interestingly, the present study suggests that PRO-C5 may be applicable in many other solid cancer types.
Tumor fibrosis results in stiff tissue, and we and others have earlier shown that CAFs produce more linearized and aligned collagen fibers (Drifka et al., 2015; Drifka et al., 2016a; Bolm et al., 2020; Nissen et al., 2022). Cancer cells are believed to use these linearized collagen fibers to metastasize (Drifka et al., 2016b). When the type V collagen/type I collagen ratio increases, the fibrils become smaller in vitro (Adachi and Hayashi, 1986; Birk et al., 1990). What this exactly means for biological function is still unknown. Recently, Chen et al., showed that pancreatic cancer cells produce unique type I collagen homotrimers (α1/α1/α1) in comparison to the type I collagen heterotrimers (α1/α2/α1) produced by fibroblasts (Chen et al., 2022). Moreover, they showed that deletion of type I collagen homotrimers increased survival in a PDAC mouse model and increased T-cell infiltration and efficacy toward anti-PD-1 immunotherapy (Chen et al., 2022). Studies have also shown that type V collagen can exist in both homo- and heterotrimers, e.g., as α1(V)2α2(V), α1(V)3 or α1(V)α2(V)α3(V) (Chanut-Delalande et al., 2001; Chanut-Delalande et al., 2004; Mak et al., 2016), but the impact of this is yet to be determined. It could be discussed if the homotrimer structure of type I collagen could actually be affected by type V collagen. In line with this, Chen et al., showed that pancreatic cancer cells expressing Col1α1, but not Col1α2, had an elevation of Col5α2 expression (Chen et al., 2022). Altogether these data could lead to the hypothesis, that increased type V collagen expression leads to more linearized type I collagen fibers promoting tumor progression and metastasis.
Some confounders in this study should be mentioned. Selection bias in the BIOPAC cohort may occur, as only patients in good performance for operation or palliative chemotherapy were included. Moreover, several publications have shown that PRO-C5 is associated with liver fibrosis, and it could be speculated if the high PRO-C5 levels are an indirect measure of liver metastases (Vassiliadis et al., 2011; Vassiliadis et al., 2012; Leeming et al., 2015). However, we found that the prognostic value of PRO-C5 was independent of liver metastases which support that the measured PRO-C5 originates from the tumor fibrosis compartment.
In conclusion, the C-propeptide of the minor fibrillar type V collagen is elevated in serum from patients with cancer. In addition, high levels are independently associated with short OS in patients with PDAC, especially patients with stage II disease. This emphasizes the importance and complexity of tumor fibrosis. PRO-C5 may have the potential of guidance in many aspects within drug discovery, patient stratification and drug efficacy.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by Danish Regional Committee on Health Research Ethics. The patients/participants provided their written informed consent to participate in this study.
Author contributions
Conception of the work: all authors. Drafting of the article: NN and NW. Biomarker measurements: NN. Preparing figures: NN. Patient inclusion and sample collection: AJ, IC, CH, JJ, HD, and LJ. Collection of clinical data: AJ, IC, CH, and JJ. Critical revision of the article: All authors. Final approval: all authors.
Conflict of interest
NN, CJ, EM, JT-U, MK, and NW are all employed by Nordic Bioscience A/S.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmolb.2023.1158058/full#supplementary-material
Supplementary Figure S1 | PRO-C5 levels in independent stages of varies cancer diseases. I: stage I, II: stage II, III: stage III, IV: stage IV.
References
Adachi, E., and Hayashi, T. (1986). In vitro formation of hybrid fibrils of type V collagen and type I collagen. Limited growth of type I collagen into thick fibrils by type V collagen. Connect. Tissue Res. 14, 257–266. doi:10.3109/03008208609017469
Altman, D. G., McShane, L. M., Sauerbrei, W., and Taube, S. E. (2012). Reporting recommendations for tumor marker prognostic studies (REMARK): Explanation and elaboration. PLoS Med. 9, e1001216. doi:10.1371/journal.pmed.1001216
Armstrong, T., Packham, G., Murphy, L. B., Bateman, A. C., Conti, J. A., Fine, D. R., et al. (2004). Type I collagen promotes the malignant phenotype of pancreatic ductal adenocarcinoma. Clin.Cancer Res. 10, 7427–7437. doi:10.1158/1078-0432.CCR-03-0825
Aszódi, A., Legate, K. R., Nakchbandi, I., Fässler, R., and Aszodi, A. (2006). What mouse mutants teach us about extracellular matrix function. Annu. Rev. Cell Dev. Biol. 22, 591–621. doi:10.1146/annurev.cellbio.22.010305.104258
Bagni, K., Chen, I. M., Johansen, A. Z., Dehlendorff, C., Jensen, B. V., Hansen, C. P., et al. (2020). Prognostic impact of charlson’s age-comorbidity index and other risk factors in patients with pancreatic cancer. Eur. J. Cancer Care (Engl). 29, e13219. doi:10.1111/ecc.13219
Balancin, M. L., Teodoro, W. R., Baldavira, C. M., Prieto, T. G., Farhat, C., Velosa, A. P., et al. (2020). Different histological patterns of type-V collagen levels confer a matrices-privileged tissue microenvironment for invasion in malignant tumors with prognostic value. Pathol. Res. Pract. 216, 153277. doi:10.1016/j.prp.2020.153277
Barcus, C. E., O’Leary, K. A., Brockman, J. L., Rugowski, D. E., Liu, Y., Garcia, N., et al. (2017). Elevated collagen-I augments tumor progressive signals, intravasation and metastasis of prolactin-induced estrogen receptor alpha positive mammary tumor cells. Breast Cancer Res. 19, 9–13. doi:10.1186/s13058-017-0801-1
Barsky, S. H., Rao, C. N., Grotendorst, G. R., and Liotta, L. A. (1982). Increased content of type V collagen in desmoplasia of human breast carcinoma. Am. J. Pathol. 108, 276–283.
Berchtold, S., Grünwald, B., Krüger, A., Reithmeier, A., Hähl, T., Cheng, T., et al. (2015). Collagen type V promotes the malignant phenotype of pancreatic ductal adenocarcinoma. Cancer Lett. 356, 721–732. doi:10.1016/j.canlet.2014.10.020
Birk, D. E., Fitch, J. M., Babiarz, J. P., Doane, K. J., and Linsenmayer, T. F. (1990). Collagen fibrillogenesis in vitro: Interaction of types I and V collagen regulates fibril diameter. J. Cell Sci. 95, 649–657. doi:10.1242/jcs.95.4.649
Bolm, L., Zghurskyi, P., Lapshyn, H., Petrova, E., Zemskov, S., Vashist, Y. K., et al. (2020). Alignment of stroma fibers, microvessel density and immune cell populations determine overall survival in pancreatic cancer-an analysis of stromal morphology. PLoS One 15, e0234568. doi:10.1371/journal.pone.0234568
Chanut-Delalande, H., Bonod-Bidaud, C., Cogne, S., Malbouyres, M., Ramirez, F., Fichard, A., et al. (2004). Development of a functional skin matrix requires deposition of collagen V heterotrimers. Mol. Cell. Biol. 24, 6049–6057. doi:10.1128/MCB.24.13.6049-6057.2004
Chanut-Delalande, H., Fichard, A., Bernocco, S., Garrone, R., Hulmes, D. J. S., and Ruggiero, F. (2001). Control of heterotypic fibril formation by collagen V is determined by chain stoichiometry. J. Biol. Chem. 276, 24352–24359. doi:10.1074/jbc.M101182200
Chen, I., Jensen, B. V., Bojesen, S. E., Johansen, A. Z., Schultz, N. A., Hansen, C. P., et al. (2019). Identification of new biomarkers in patients with pancreatic cancer (BIOPAC): A study protocol of an open cohort study. J. Cancer Sci. Ther. 11, 232.
Chen, I. M., Willumsen, N., Dehlendorff, C., Johansen, A. Z., Jensen, B. V., Hansen, C. P., et al. (2020). Clinical value of serum hyaluronan and propeptide of type III collagen in patients with pancreatic cancer. Int. J. Cancer 146, 2913–2922. doi:10.1002/ijc.32751
Chen, Y., Kim, J., Yang, S., Wang, H., Wu, C.-J., Sugimoto, H., et al. (2021). Type I collagen deletion in ΑSMA(+) myofibroblasts augments immune suppression and accelerates progression of pancreatic cancer. Cancer Cell 39, 548–565.e6. doi:10.1016/j.ccell.2021.02.007
Chen, Y., Yang, S., Tavormina, J., Tampe, D., Zeisberg, M., Wang, H., et al. (2022). Oncogenic collagen I homotrimers from cancer cells bind to Α3β1 integrin and impact tumor microbiome and immunity to promote pancreatic cancer. Cancer Cell 40, 818–834.e9. doi:10.1016/j.ccell.2022.06.011
Cheng, J. C., and Leung, P. C. K. (2011). Type I collagen down-regulates E-cadherin expression by increasing PI3KCA in cancer cells. Cancer Lett. 304, 107–116. doi:10.1016/j.canlet.2011.02.008
Drifka, C. R., Loeffler, A. G., Esquibel, C. R., Weber, S. M., Eliceiri, K. W., and Kao, W. J. (2016). Human pancreatic stellate cells modulate 3D collagen alignment to promote the migration of pancreatic ductal adenocarcinoma cells. Biomed. Microdevices 18, 105. doi:10.1007/s10544-016-0128-1
Drifka, C. R., Loeffler, A. G., Mathewson, K., Keikhosravi, A., Eickhoff, J. C., Liu, Y., et al. (2016). Highly aligned stromal collagen is a negative prognostic factor following pancreatic ductal adenocarcinoma resection. Oncotarget 7, 76197–76213. doi:10.18632/oncotarget.12772
Drifka, C. R., Tod, J., Loeffler, A. G., Liu, Y., Thomas, G. J., Eliceiri, K. W., et al. (2015). Periductal stromal collagen topology of pancreatic ductal adenocarcinoma differs from that of normal and chronic pancreatitis. Mod. Pathol. 28, 1470–1480. doi:10.1038/modpathol.2015.97
Gao, H., Chakraborty, G., Zhang, Z., Akalay, I., Gadiya, M., Gao, Y., et al. (2016). Multi-organ site metastatic reactivation mediated by non-canonical discoidin domain receptor 1 signaling. Cell 166, 47–62. doi:10.1016/j.cell.2016.06.009
Grout, J. A., Sirven, P., Leader, A. M., Maskey, S., Hector, E., Puisieux, I., et al. (2022). Spatial positioning and matrix programs of cancer-associated fibroblasts promote t cell exclusion in human lung tumors. Cancer Discov. 12. CD-21-1714. doi:10.1158/2159-8290.CD-21-1714
Heldin, C. H., Rubin, K., Pietras, K., and Östman, A. (2004). High interstitial fluid pressure - an obstacle in cancer therapy. Nat. Rev. Cancer 4, 806–813. doi:10.1038/nrc1456
Huang, G., Ge, G., Izzi, V., and Greenspan, D. S. (2017). α3 Chains of type V collagen regulate breast tumour growth via glypican-1. Nat. Commun. 8, 14351. doi:10.1038/ncomms14351
Imamura, T., Iguchi, H., Manabe, T., Ohshio, G., Yoshimura, T., Wang, Z. H., et al. (1995). Quantitative analysis of collagen and collagen subtypes I, III, and V in human pancreatic cancer, tumor-associated chronic pancreatitis, and alcoholic chronic pancreatitis. Pancreas 11, 357–364. doi:10.1097/00006676-199511000-00007
Jensen, C., Nissen, N. I., Von Arenstorff, C. S., Karsdal, M. A., and Willumsen, N. (2021). Serological assessment of collagen fragments and tumor fibrosis may guide immune checkpoint inhibitor therapy. J. Exp. Clin. Cancer Res. 40 (1), 326. doi:10.1186/s13046-021-02133-z
Jensen, C., Holm Nielsen, S., Eslam, M., Genovese, F., Nielsen, M. J., Vongsuvanh, R., et al. (2020). Cross-linked multimeric pro-peptides of type III collagen (PC3X) in hepatocellular carcinoma - a biomarker that provides additional prognostic value in afp positive patients. J. Hepatocell. Carcinoma 7, 301–313. doi:10.2147/jhc.s275008<
Jensen, C., Sinkeviciute, D., Madsen, D. H., Önnerfjord, P., Hansen, M., Schmidt, H., et al. (2020). Granzyme B degraded type IV collagen products in serum identify melanoma patients responding to immune checkpoint blockade. Cancers (Basel). 12, E2786. doi:10.3390/cancers12102786
Khalaf, N., El-Serag, H. B., Abrams, H. R., and Thrift, A. P. (2021). Burden of pancreatic cancer: From epidemiology to practice. Clin. Gastroenterol. Hepatol. 19, 876–884. doi:10.1016/j.cgh.2020.02.054
Klein, A. P. (2019). Pancreatic cancer: A growing burden. Lancet Gastroenterol. Hepatol. 4, 895–896. doi:10.1016/S2468-1253(19)30323-1
Lander, V. E., Belle, J. I., Kingston, N. L., Herndon, J. M., Hogg, G. D., Liu, X., et al. (2022). Stromal reprogramming by FAK inhibition overcomes radiation resistance to allow for immune priming and response to checkpoint blockade. Cancer Discov. 12, 2774–2799. doi:10.1158/2159-8290.CD-22-0192
Leeming, D. J., Veidal, S. S., Karsdal, M. A., Nielsen, M. J., Trebicka, J., Busk, T., et al. (2015). Pro-C5, a marker of true type V collagen formation and fibrillation, correlates with portal hypertension in patients with alcoholic cirrhosis. Scand. J. Gastroenterol. 50, 584–592. doi:10.3109/00365521.2014.996590
Madsen, E. A., Thorlacius-Ussing, J., Nissen, N. I., Jensen, C., Chen, I. M., Johansen, J. S., et al. (2022). Type XXII collagen complements fibrillar collagens in the serological assessment of tumor fibrosis and the outcome in pancreatic cancer. Cells 11, 3763. doi:10.3390/cells11233763
Mak, K. M., Png, C. Y. M., and Lee, D. J. (2016). Type V collagen in Health, disease, and fibrosis. Anat. Rec. 299, 613–629. doi:10.1002/ar.23330
Mariathasan, S., Turley, S., Nickles, D., Castiglioni, A., Yuen, K., Wang, Y., et al. (2018). TGFβ attenuates tumour response to PD-L1 blockade by contributing to exclusion of T cells. Nature 22, 544–548. doi:10.1038/nature25501
McGuigan, A., Kelly, P., Turkington, R. C., Jones, C., Coleman, H. G., and McCain, R. S. (2018). Pancreatic cancer: A Review of clinical diagnosis, epidemiology, treatment and outcomes. World J. Gastroenterol. 21, 4846–4861. doi:10.3748/wjg.v24.i43.4846
Menke, A., Philippi, C., Vogelmann, R., Seidel, B., Lutz, M. P., Adler, G., et al. (2001). Down-regulation of E-cadherin gene expression by collagen type I and type III in pancreatic cancer cell lines. Biochemistry 61, 3508–3517.
Nissen, N. I., Johansen, A. Z., Chen, I. M., Johansen, J. S., Pedersen, R. S., Hansen, C. P., et al. (2022). Collagen biomarkers quantify fibroblast activity in vitro and predict survival in patients with pancreatic ductal adenocarcinoma. Cancers (Basel) 14, 819–821. doi:10.3390/cancers14030819
Nissen, N. I., Karsdal, M., and Willumsen, N. (2019). Collagens and cancer associated fibroblasts in the reactive stroma and its relation to cancer biology. J. Exp. Clin. Cancer Res. 38, 115. doi:10.1186/s13046-019-1110-6
Nissen, N. I., Kehlet, S., Boisen, M. K., Liljefors, M., Jensen, C., Johansen, A. Z., et al. (2021). Prognostic value of blood-based fibrosis biomarkers in patients with metastatic colorectal cancer receiving chemotherapy and bevacizumab. Sci. Rep. 11, 1–12. doi:10.1038/s41598-020-79608-0
Nissen, N. I., Kehlet, S., Johansen, A. Z., Chen, I. M., Karsdal, M., Johansen, J. S., et al. (2021). Noninvasive prognostic biomarker potential of quantifying the propeptides of type XI collagen alpha-1 chain (PRO-C11) in patients with pancreatic ductal adenocarcinoma. Int. J. Cancer 149, 228–238. doi:10.1002/ijc.33551
Ogawa, Y., Masugi, Y., Abe, T., Yamazaki, K., Ueno, A., Fujii-Nishimura, Y., et al. (2021). Three distinct stroma types in human pancreatic cancer identified by image analysis of fibroblast subpopulations and collagen. Clin. Cancer Res. 27, 107–119. doi:10.1158/1078-0432.CCR-20-2298
Ren, W., Zhang, Y., Zhang, L., Lin, Q., Zhang, J., and Xu, G. (2018). Overexpression of collagen type V Α1 chain in human breast invasive ductal carcinoma is mediated by TGF-β1. Int. J. Oncol. 52, 1694–1704. doi:10.3892/ijo.2018.4317
Ricard-Blum, S. (2011). The collagen family. Cold Spring Harb. Perspect. Biol. 3, a004978. doi:10.1101/cshperspect.a004978
Siegel, R. L., Miller, K. D., Fuchs, H. E., and Jemal, A. (2021). Cancer statistics, 2021. Ca. Cancer J. Clin. 71, 7–33. doi:10.3322/caac.21654
Kehlet, S. N., Boisen, A, H., Mk, B., Johansen, J.S., Karsdal, M. A., Nicholas, W., et al. (2018). Prognostic evaluation of a new class of liquid biopsy biomakrers in patients with metastatic colorectal cancer: Using the tumor microenvironment as a source of protein biomarkers. J. Clin. Oncol. 15, 3588. doi:10.1200/JCO.2018.36.15_suppl.3588
Su, H., Yang, F., Fu, R., Trinh, B., Sun, N., Liu, J., et al. (2022). Collagenolysis-dependent DDR1 signalling dictates pancreatic cancer outcome. Nature 610, 366–372. doi:10.1038/s41586-022-05169-z
Sun, M., Chen, S., Adams, S. M., Florer, J. B., Liu, H., Kao, W. W. Y., et al. (2011). Collagen V is a dominant regulator of collagen fibrillogenesis: Dysfunctional regulation of structure and function in a corneal-stroma-specific col5a1-null mouse model. J. Cell Sci. 124, 4096–4105. doi:10.1242/jcs.091363
Symoens, S., Renard, M., Bonod-Bidaud, C., Syx, D., Vaganay, E., Malfait, F., et al. (2010). Identification of binding partners interacting with the Α1-N-propeptide of type V collagen. Biochem. J. 433, 371–381. doi:10.1042/BJ20101061
Tan, Y., and Chen, Q. (2018). The TCGA and GEO databases identify COL5A2 as a poorly prognostic gene in patients with advanced gastric cancer. Res. Sq. 1–19.
Tan, Y., Chen, Q., Xing, Y., Zhang, C., Pan, S., An, W., et al. (2021). High expression of COL5A2, a member of COL5 family, indicates the poor survival and facilitates cell migration in gastric cancer. Biosci. Rep. 41, BSR20204293–15. doi:10.1042/BSR20204293
Thomas, D., and Radhakrishnan, P. (2019). Tumor-stromal crosstalk in pancreatic cancer and tissue fibrosis. Mol. Cancer 18, 14–15. doi:10.1186/s12943-018-0927-5
Thorlacius-Ussing, J., Jensen, C., Madsen, E. A., Nissen, N. I., Manon-Jensen, T., Chen, I. M., et al. (2022). Type XX collagen is elevated in circulation of patients with solid tumors. Int. J. Mol. Sci. 23, 4144. doi:10.3390/IJMS23084144
Thorlacius-Ussing, J., Manon-Jensen, T., Sun, S., Leeming, D. J., Sand, J. M., Karsdal, M., et al. (2020). Serum type xix collagen is significantly elevated in non-small cell lung cancer: A preliminary study on biomarker potential. Cancers (Basel). 12, 1510–1514. doi:10.3390/cancers12061510
Vassiliadis, E., Veidal, S. S., Hansen, C., Karsdal, M. A., and Leeming, D. J. (2012). Circulating levels of a collagen type V propeptide fragment in a carbon tetrachloride reversible model of liver fibrosis. Biomark. Insights 7, 159–166. doi:10.4137/BMI.S10975
Vassiliadis, E., Veidal, S. S., Simonsen, H., Larsen, D. V., Vainer, B., Chen, X., et al. (2011). Immunological detection of the type v collagen propeptide fragment, PVCP-1230 connective tissue remodeling associated with liver fibrosis. Biomarkers. doi:10.3109/1354750X.2011.584131
Wang, J., Jiang, Y. H., Yang, P. Y., and Liu, F. (2021). Increased collagen type v Α2 (Col5a2) in colorectal cancer is associated with poor prognosis and tumor progression. Onco. Targets. Ther. 14, 2991–3002. doi:10.2147/OTT.S288422
Wang, S., Bager, C. L., Karsdal, M. A., Chondros, D., Taverna, D., and Willumsen, N. (2021). Blood-based extracellular matrix biomarkers as predictors of survival in patients with metastatic pancreatic ductal adenocarcinoma receiving pegvorhyaluronidase alfa. J. Transl. Med. 19, 39–12. doi:10.1186/s12967-021-02701-z
Wenstrup, R. J., Florer, J. B., Brunskill, E. W., Bell, S. M., Chervoneva, I., and Birk, D. E. (2004). Type V collagen controls the initiation of collagen fibril assembly. J. Biol. Chem. 279, 53331–53337. doi:10.1074/jbc.M409622200
Willumsen, N., Ali, S. M., Leitzel, K., Drabick, J. J., Yee, N., Polimera, H. V., et al. (2019). Collagen fragments quantified in serum as measures of desmoplasia associate with survival outcome in patients with advanced pancreatic cancer. Sci. Rep. 9, 19761. doi:10.1038/s41598-019-56268-3
Willumsen, N., Jensen, C., Green, G., Nissen, N. I., Neely, J., Nelson, D. M., et al. (2022). Fibrotic activity quantified in serum by measurements of type III collagen pro-peptides can Be used for prognosis across different solid tumor types. Cell. Mol. Life Sci. 794, 204–211. doi:10.1007/S00018-022-04226-0
Willumsen, N., Thomsen, L. B., Bager, C. L., Jensen, C., and Karsdal, M. A. (2018). Quantification of altered tissue turnover in a liquid biopsy: A proposed precision medicine tool to assess chronic inflammation and desmoplasia associated with a pro-cancerous niche and response to immuno-therapeutic anti-tumor modalities. Cancer Immunol. Immunother. 67, 1–12. doi:10.1007/s00262-017-2074-z
Keywords: cancer, collagen, PDAC, prediction, prognosis, tumor fibrosis, type V collagen
Citation: Nissen NI, Johansen AZ, Chen IM, Jensen C, Madsen EA, Hansen CP, Thorlacius-Ussing J, Karsdal M, Johansen JS, Diab HMH, Jørgensen LN and Willumsen N (2023) High serum levels of the C-propetide of type V collagen (PRO-C5) are prognostic for short overall survival in patients with pancreatic ductal adenocarcinoma. Front. Mol. Biosci. 10:1158058. doi: 10.3389/fmolb.2023.1158058
Received: 03 February 2023; Accepted: 23 February 2023;
Published: 10 March 2023.
Edited by:
William C. Cho, QEH, Hong Kong SAR, ChinaReviewed by:
Juan R. De Los Toyos, University of Oviedo, SpainJoan Chang, The University of Manchester, United Kingdom
Copyright © 2023 Nissen, Johansen, Chen, Jensen, Madsen, Hansen, Thorlacius-Ussing, Karsdal, Johansen, Diab, Jørgensen and Willumsen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Neel I. Nissen, bmluQG5vcmRpY2Jpby5jb20=