
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Mol. Biosci. , 20 October 2022
Sec. Cellular Biochemistry
Volume 9 - 2022 | https://doi.org/10.3389/fmolb.2022.912620
 Shixian Liu1,2,3†Weiwei Liu1,2,3†Zhao Ding1,2,3†Xue Yang1,2,3Yuan Jiang1,2,3Yu Wu1,2,3
Shixian Liu1,2,3†Weiwei Liu1,2,3†Zhao Ding1,2,3†Xue Yang1,2,3Yuan Jiang1,2,3Yu Wu1,2,3 Yehai Liu1*Jing Wu1*
Yehai Liu1*Jing Wu1*Objective: Head and neck squamous cell carcinoma (HNSCC) is a common heterogeneous cancer with complex carcinogenic factors. However, the current TNM staging criteria to judge its severity to formulate treatment plans and evaluate the prognosis are particularly weak. Therefore, a robust diagnostic model capable of accurately diagnosing and predicting HNSCC should be established.
Methods: Gene expression and clinical data were retrieved from The Cancer Genome Atlas and Gene Expression Omnibus databases. Key prognostic genes associated with HNSCC were screened with the weighted gene co-expression network analysis and least absolute shrinkage and selection operator (LASSO) Cox regression model analysis. We used the timeROC and survival R packages to conduct time-dependent receiver operating characteristic curve analyses and calculated the area under the curve at different time points of model prediction. Patients in the training and validation groups were divided into high- and low-risk subgroups, and Kaplan-Meier (K-M) survival curves were plotted for all subgroups. Subsequently, LASSO and support vector machine algorithms were used to screen genes to construct diagnostic model. Furthermore, we used the Wilcoxon signed-rank test to compare the half-maximal inhibitory concentrations of common chemotherapy drugs among patients in different risk groups. Finally, the expression levels of eight genes were measured using quantitative real-time polymerase chain reaction and immunohistochemistry.
Results: Ten genes (SSB, PFKP, NAT10, PCDH9, SHANK2, PAX8, CELSR3, DCLRE1C, MAP2K7, and ODF4) with prognostic potential were identified, and a risk score was derived accordingly. Patients were divided into high- and low-risk groups based on the median risk score. The K-M survival curves confirmed that patients with high scores had significantly worse overall survival. Receiver operating characteristic curves proved that the prognostic signature had good sensitivity and specificity for predicting the prognosis of patients with HNSCC. Univariate and multivariate Cox regression analyses confirmed that the gene signature was an independent prognostic risk factor for HNSCC. Diagnostic model was built by identifying eight genes (SSB, PFKP, NAT10, PCDH9, CELSR3, DCLRE1C, MAP2K7, and ODF4). The high-risk group showed higher sensitivity to various common chemotherapeutic drugs. DCLRE1C expression was higher in normal tissues than in HNSCC tissues.
Conclusion: Our study identified the important role of tumor-driver genes in HNSCC and their potential clinical diagnostic and prognostic values to facilitate individualized management of patients with HNSCC.
Head and neck squamous cell carcinoma (HNSCC) is a heterogeneous group of malignancies that can originate in the tongue, mouth, paranasal sinuses, nasopharynx, oropharynx, hypopharynx, or larynx. Globally, it is the sixth most common cancer type and eighth most common cause of cancer-related deaths (Bray et al., 2018). There are more than 650,000 newly diagnosed cases and 330,000 deaths (Tumban, 2019). The following carcinogenic factors may lead to the occurrence and development of HNSCC: exposure of the upper gastrointestinal mucosa to carcinogens, such as tobacco and alcohol; human papillomavirus infection; and less commonly, Epstein–Barr virus infection (Rickinson, 2014; Diez-Fraile et al., 2020).
The current standard treatment for HNSCC is surgery with or without chemotherapy and/or radiotherapy (Sacconi et al., 2020). Approximately two-thirds of patients with locally or regionally advanced disease adopt a certain combination of these three treatments (Cognetti et al., 2008; Rosenberg and Vokes, 2021). Although surgical methods are constantly being updated and new therapeutic approaches are being developed, the survival rate of patients with HNSCC has not improved significantly. Currently, the standard method for clinicians to judge the severity of HNSCC is TNM staging (Syed et al., 2020). However, the TNM stage considers only the anatomical factors of the tumor; therefore, using it to develop treatment plans for patients and assess the prognosis is particularly inefficient. Coupled with the diverse etiology and high degree of heterogeneity of HNSCC, accurate prediction of patient prognosis poses a great challenge. Therefore, robust prognostic models should be developed.
Some gene mutations induce changes in gene information or abnormal expression of their products, which can transform normal cells to tumor cells with malignant biological behaviors (Ma et al., 2021). These mutant genes are often referred to as tumor-driver genes. They promote the development and progression of tumors and pose a threat to human health (Steeg, 2006; Zhu et al., 2013). Models based on tumor-driver gene sets that can predict the prognosis of patients with HNSCC are lacking.
With the rapid growth and development of next-generation sequencing, bioinformatics analysis has been widely used and adopted for microarray platforms and data to further explore the underlying genetic and molecular mechanisms of diseases and detect specific biomarkers of disease (Morganti et al., 2019). Weighted gene co-expression network analysis (WGCNA) is a popular algorithm that enables highly correlated genes to be grouped into the same module, with the advantage of being able to link, including but not limited to, clinicopathological parameters (Zhang and Horvath, 2005; Emilsson et al., 2008). In this study, we used WGCNA to identify tumor-driver genes that are strongly associated with HNSCC. We then screened the training dataset (The Cancer Genome Atlas [TCGA]) for 28 tumor-driver genes that were significantly related to the prognosis and established a prognostic signature using least absolute shrinkage and selection operator (LASSO) and multivariate Cox regression analysis. In addition, we reevaluated the model’s performance using a different independent dataset, i.e., GSE41613. Accordingly, we constructed a robust diagnostic model capable of accurately diagnosing HNSCC. In addition, our prognostic model can predict the sensitivity of patients with HNSCC to chemotherapeutic drugs.
We obtained expression data from TCGA public database for 546 patients with HNSCC (44 normal and 502 tumor tissues) and follow-up data for each patient (Table 1). The expression and clinical data for patients in the GSE41613 (97 HNSCC tissues), GSE127165 (57 laryngeal squamous cell carcinomas and paired adjacent normal tissues), and GSE37991 (40 paired HNSCC and adjacent carcinomas) datasets were downloaded from the Gene Expression Omnibus (GEO). We downloaded 2,372 tumor-driver genes from an online website (http://ncg.kcl.ac.uk/cancer_genes.php). Data were obtained from databases that were freely available to all and, therefore, did not require ethics committee approval.
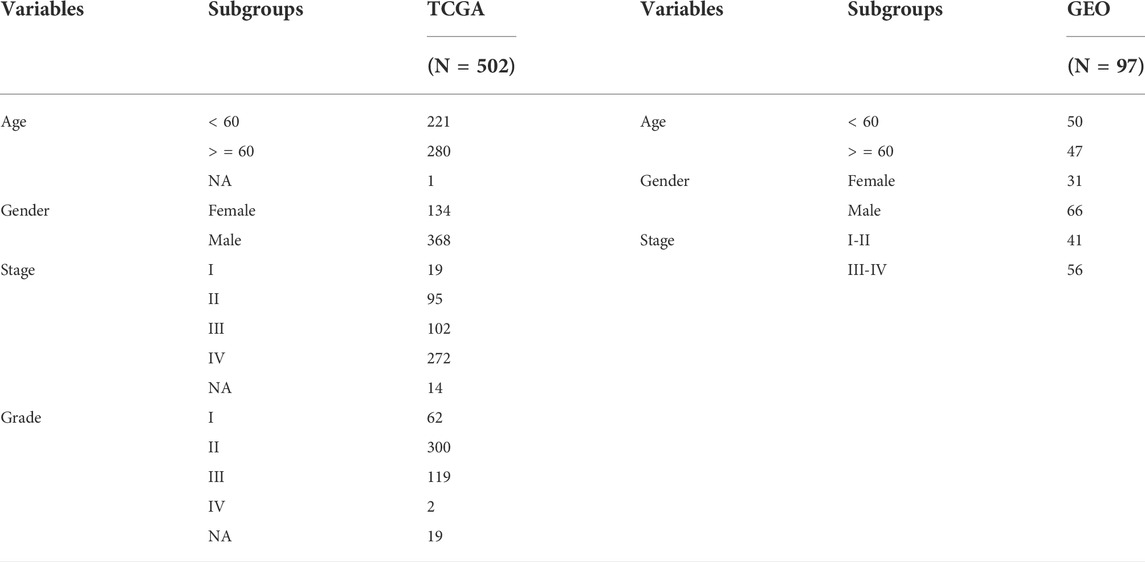
TABLE 1. Clinical data of patients in the TCGA and the GEO validation cohort.
To identify the tumor-driver genes associated with HNSCC, we constructed a co-expression network using the “WGCNA” R package based on the gene expression matrix of the training dataset (Langfelder and Horvath, 2008). First, we filtered genes with a small range of fluctuating expression levels across all samples. We then examined the expression matrix in TCGA dataset and removed the missing values. The cluster analysis was used to identify discrete samples, which were subsequently removed. When the average connectivity was infinitely close to 0 and the scale-free topology fit index (R2) was almost 0.9, the β value was chosen as the soft threshold power. Subsequently, we calculated the topological overlap matrix (TOM) and used matrix 1-TOM to identify hierarchically clustered genes and modules. To ensure reliability of the results, the minimum number of genes in each module was set to 25, and the module branch merge cut height was set to 0.25. The first principal element of each gene module was identified as module eigengenes (MEs). The k-ME value was used as a measure of intra-module connectivity, which represents the correlation between the gene expression level and ME. The modules (|r| ≥ 0.4) that were strongly related to the tumor were selected for the next analysis, and the genes (red, blue, and black) in the eligible modules were extracted.
We first extracted the gene expression matrix from TCGA dataset for the three eligible modules (655 genes in total). A univariate Cox regression analysis was used to screen tumor-driver genes associated with overall survival (OS) in patients with HNSCC in TCGA training dataset (p < 0.005). Immediately afterwards, we used the LASSO regression analysis for 10-fold cross-validation, filtering tumor-driver genes that were more strongly correlated to avoid overfitting. Finally, we used a multivariate Cox regression analysis to develop an optimal prognostic risk model based on the Akaike information criterion (AIC = 2297.34). In the previous process, the genes used to construct the model and their corresponding coefficients were obtained, and a formula for calculating the patient’s risk score was derived, as follows: risk score = ˇgene 1* gene 1 expression + ˇgene 2 * gene 2 expression + ····· + ˇgene N * gene N expression. Samples in each TCGA-HNSCC cohort and validation cohort were categorized into low- and high-risk groups, consistent with the median risk score. We used Kaplan–Meier survival curves with a log-rank test to compare the differences in prognosis between the two groups of patients. To assess the predictive power of the prognostic model, we used the Kaplan–Meier receiver operating characteristic (ROC) and Kaplan–Meier “survival” R packages to conduct time-dependent ROC (tROC) analyses and calculated the area under the curve (AUC) at different time points for model prediction.
To determine the robustness and generalizability of the developed predictive models, an independent external dataset validation is necessary. Therefore, GSE41613, an external dataset, was used to evaluate the model’s performance. Similarly, patients in the validation dataset were divided into high- and low-risk subgroups using the same cutoff values, and Kaplan–Meier survival curves were plotted for both subgroups of patients. A meta-analysis (I2 < 50%, fixed-effects model) was performed using TCGA and GSE41613 datasets to assess the prognostic value of the model in the combined cohort. Furthermore, a stratification analysis was performed to confirm the prognostic importance of the gene signature in all stratified subgroups.
We used cBioPortal, which is a free web server that allows interactive exploration of cancer genomic data (Cerami et al., 2012), to predict the specific mutational profiles of these ten genes in patients with HNSCC (TCGA, PanCancer Atlas). Most of these ten genes were significantly differentially expressed in normal and tumour tissues, but the differences in expression of SHANK2 and DCLRE1C were not significant (Supplementary Figure S1).
To elucidate whether the prognostic model could also serve as a diagnostic model, the genes used to construct the prognostic model were used to screen candidate genes. LASSO is a powerful analysis method that enables both regularization and variable selection to ensure that the model has strong predictive accuracy. In addition, we used another approach (support vector machine recursive feature elimination [SVM-RFE]) to screen the set of diagnostic genes with the highest discriminant ability. Finally, we used the intersecting genes obtained by the two algorithms to construct a diagnostic model. The superior performance of the diagnostic model in a single dataset was not highly convincing; therefore, its performance was re-validated using two other independent datasets (GSE127165 and GSE37991).
Since not all patients with HNSCC are sensitive to chemotherapy owing to individual differences, we used the ‘pRRophetic’ R package to predict the drug sensitivity of patients to reduce the financial burden on patients. Commonly used chemotherapeutic drugs in oncology include cisplatin, lapatinib, methotrexate, and docetaxel. The half-maximal inhibitory concentration (IC50) of multiple chemotherapeutic drugs in each patient with HNSCC was calculated using ridge regression, and the accuracy of prediction was assessed using 10-fold cross-validation. We used the Wilcoxon signed-rank test to compare IC50 of common chemotherapy drugs across risk groups.
Fresh primary HNSCC samples and corresponding non-tumor tissues were collected immediately after surgical resection at the First Affiliated Hospital of Anhui Medical University. The tissues were transported to the laboratory within 2 h. The collected tissue samples were stored at −80°C until use. Clinical samples were approved by the Research Ethics Review Committee of the First Affiliated Hospital of Anhui Medical University. Written informed consent was obtained from all patients.
RNA isolation and purification were performed using TRIzol RNA. The Complementary DNA Synthesis SuperMix Kit (ThermoFisher Scientific) was used to synthesize complementary DNA, which was subjected to qRT-PCR using SYBR® Premix Ex TaqTM II (TaKaRa) and the Real-Time System (Lin et al., 2021) (Roche Life Science). The gene expression levels were normalized to GAPDH messenger RNA (mRNA) expression. Supplementary Table S1 shows the primer sequences used.
Tissues were lysed with the RIPA lysis buffer (Beyotime, Jiangsu, China), separated by polyacrylamide gel electrophoresis using sodium dodecyl sulfate and transferred to polyvinylidene fluoride membranes (Millipore, Billerica, MA, United States ). Closure with 5% skim milk for 1 h was incubated with the primary antibody overnight for primary antibodies (diluted 1:1000) at 4°C overnight. The membranes were then incubated with horseradish peroxidase-conjugated secondary antibody for 1 h at room temperature. Finally, the protein bands were visualized using chemiluminescence (Wan et al., 2021).
Twelve pairs of tissue samples were approved by the First Affiliated Hospital of the Anhui Medical University. All tissue samples were approved by patients. Tumor tissues were paraffin-sectioned. HNSCC tissue sections were deparaffinized in xylene and dehydrated in ethanol. Antigen retrieval was performed using citrate buffer (pH 6), followed by blocking with bovine serum albumin for 1 h to prevent nonspecific binding of antibodies. After tumor tissues were paraffin embedded, they were incubated with specific primary antibodies (DCLRE1C, 1:100, ThermoFisher Scientific) at 4°C overnight. The paraffin sections were then incubated with horseradish peroxidase-conjugated secondary antibodies for 20 min at room temperature. Finally, photographs were acquired using an inverted microscope (Wang et al., 2020). The positive rate was calculated using the immunohistochemistry toolbox plugin in ImageJ software.
To obtain the key modules for HNSCC, we first constructed a co-expression network using 44 normal and 502 HNSCC samples from the training dataset (TCGA cohort; Figure 1A). We then chose β = 4 as the optimal soft threshold, based on which 13 modules were obtained (Figures 1B,C). Furthermore, among these 13 modules, the highest module-trait positive association was found among the red module (r = 0.41; p = 5e-23), blue module (r = 0.44; p = 1e-27), and black module (r = 0.84; p = 2e-32) with HNSCC tissue (Figure 1D). The genes in these modules may play essential biological roles associated with the prognostic signature. Subsequently, 655 genes from the three key modules were selected for further analyses (Supplementary Table S2).
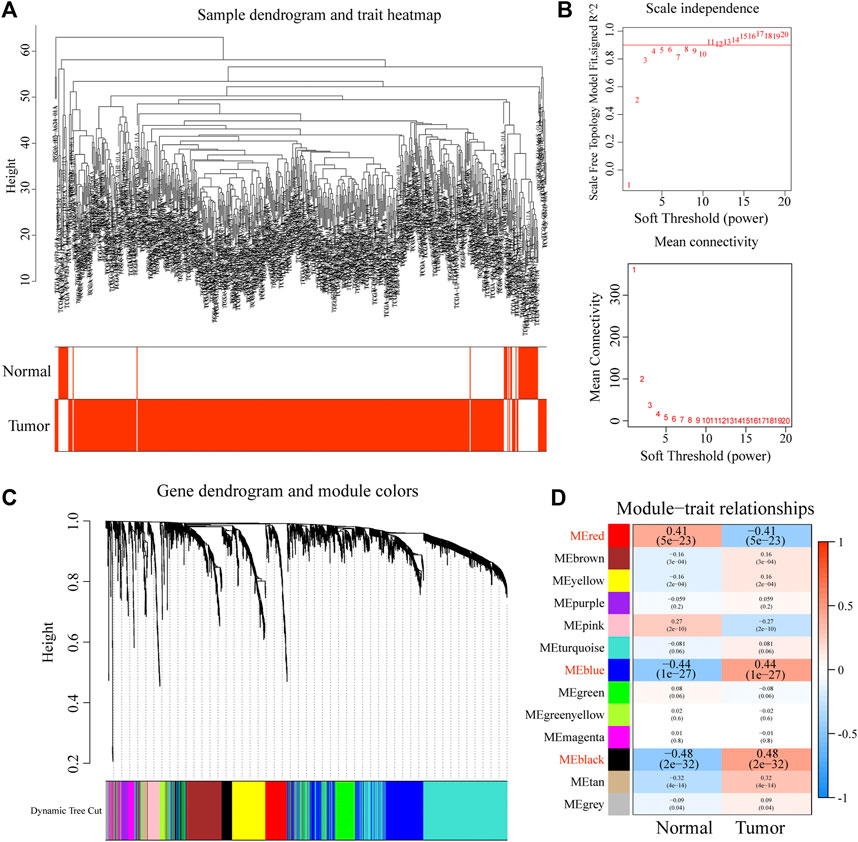
FIGURE 1. Construction of a co-expression network through WGCNA. (A) Clustering dendrogram of HNSCC samples. (B) Network topology for different soft-thresholding powers. (C) The cluster dendrogram of co-expression network modules is ordered by a hierarchical clustering of genes based on the 1-TOM matrix. (D) Module-trait relationships.
A total of 616 overlapping tumor-driver genes were acquired between TCGA and GSE41613 gene expression profiles. The univariate Cox regression analysis conducted between the 616 genes and OS illustrated that 28 genes were significantly correlated with OS (p < 0.005; Figure 2A). To identify the best prognostic genes and build a simplified prognostic model, we applied the LASSO Cox regression algorithm to the 28 prognosis-related genes. Eleven genes were excluded (Figure 2B). The 17 genes that met the screening criteria were subjected to the multivariate Cox regression analysis, at which point an optimal prognostic model was created (Figures 2C,D). The risk score was calculated as follows: risk score = (1.236 * SSB) + (0.628 * PFKP) + (0.567 * NAT10) + (0.498 * PCDH9) + (0.189 * SHANK2) + (−0.443 * PAX8) + (−0.529 * CELSR3) + (−0.806 * DCLRE1C) + (−1.865 * MAP2K7) + (−2.439 * ODF4). The risk score was computed for every case in the two cohorts, and all cases were classified into low- and high-risk groups based on the median threshold.
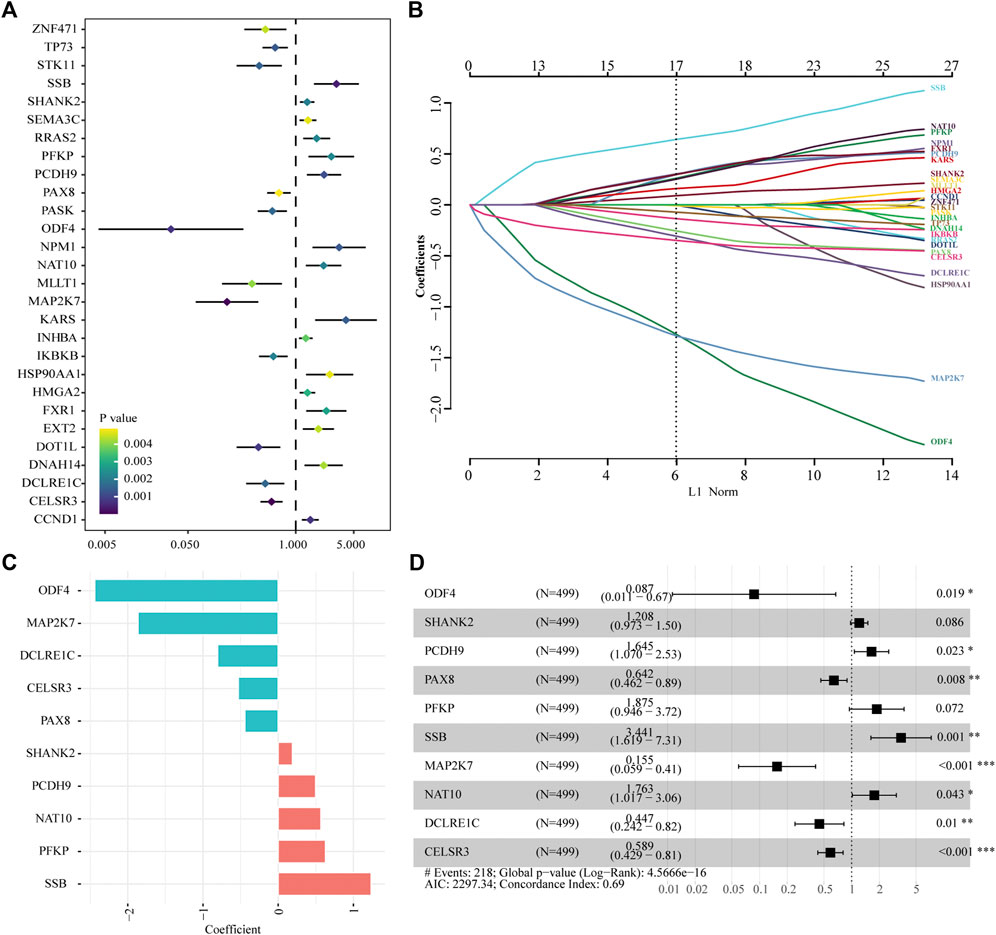
FIGURE 2. Identification of tumor driver genes in TCGA cohort. (A) Univariate Cox regression analysis to identify prognostic genes. (B) LASSO regression analysis to eliminate collinearity. (C) Coefficients of the 10 genes included in the signature. (D) Multivariable Cox proportional-hazards regression analysis of the 10 prognostic genes.
Patients in the two datasets were divided into low- and high-risk groups using the median risk score. Kaplan–Meier curves revealed that patients with HNSCC in the high-risk group had significantly shorter survival times than those in the low-risk group from TCGA cohort (hazard ratio [HR] = 2.29, p < 0.001, Figure 3A). Risk scores were significantly higher in patients who died than in those who were alive (Figure 3B). The multivariate Cox regression analysis showed that the age, stage, and risk score in TCGA dataset were independent predictors of survival outcomes in patients with HNSCC (Figure 3C).In addition, the tROC analysis showed strong performance of our prognostic model, with mean AUC values above 0.7 (Figure 3D).
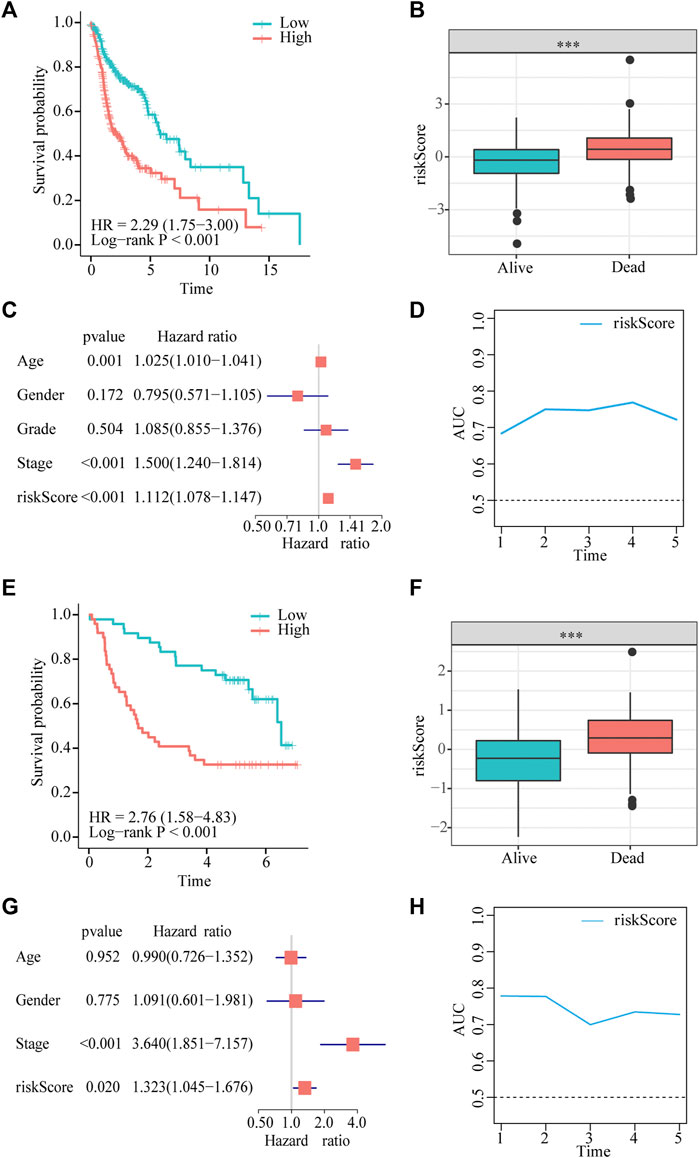
FIGURE 3. Gene signature predicts overall survival (OS) in TCGA and GEO datasets. (A,E) Kaplan-Meier analysis shows that HNSCC patients with higher risk scores have a poor prognosis. (B,F) The risk score is significantly elevated in patients with HNSCC who died during the follow-up. (C,G) Multivariate Cox regression analysis shows that the risk score is an independent prognostic factor for OS. (D,H) tROC analysis shows that the risk score is an accurate variable for survival prediction.
To demonstrate the robustness of the prognostic model, we validated its performance using the GSE41613 dataset. The results of the Kaplan–Meier analysis indicated that OS was lower in the high-risk group than in the low-risk group (HR = 3.11, p < 0.001, Figure 3E). The risk score was significantly higher in patients who died than in those who were alive (Figure 3F). Consistent with the results of multivariate Cox regression in TCGA cohort, the risk score was also an independent prognostic factor for patients with HNSCC with OS (HR = 1.323, p = 0.02, Figure 3G). tROC results in the validation dataset showed very high accuracy of the prognostic model, particularly in predicting 1- and 2-year survival, with AUC values close to 0.8 (Figure 3H).
Furthermore, a meta-analysis was conducted to analyze the prognostic value of the prognostic models developed in the combined cohort. It showed that the prognosis of patients in the high-risk subgroup was worse than that of those in the low-risk subgroup (pooled HR = 2.43; 95% confidence interval: 1.85–3.19; Figure 4A). The association between survival time and the risk score was further investigated in TCGA dataset, and patients who died had higher risk scores. Particularly, those who survived for <1 year had the highest risk scores (Figure 4B). In addition, to explore the prognostic reliability and stability of the signature in different clinical groups, Kaplan–Meier analyses were used to plot survival curves and evaluate survival differences in the pooled cohort to visualize prognostic values. The curves indicated that patients in the high-risk group presented a drastically increased risk of dying among some patients with HNSCC, including age (<60 years, ≥ 60 years; Figures 4C,D), ex (female, male; Figures 4E,F), grade (1–2, 3–4; Figures 4G,H), and stage (I–II, III–IV; Figures 4I,J), demonstrating that the signature was a sturdy prognostic biomarker.
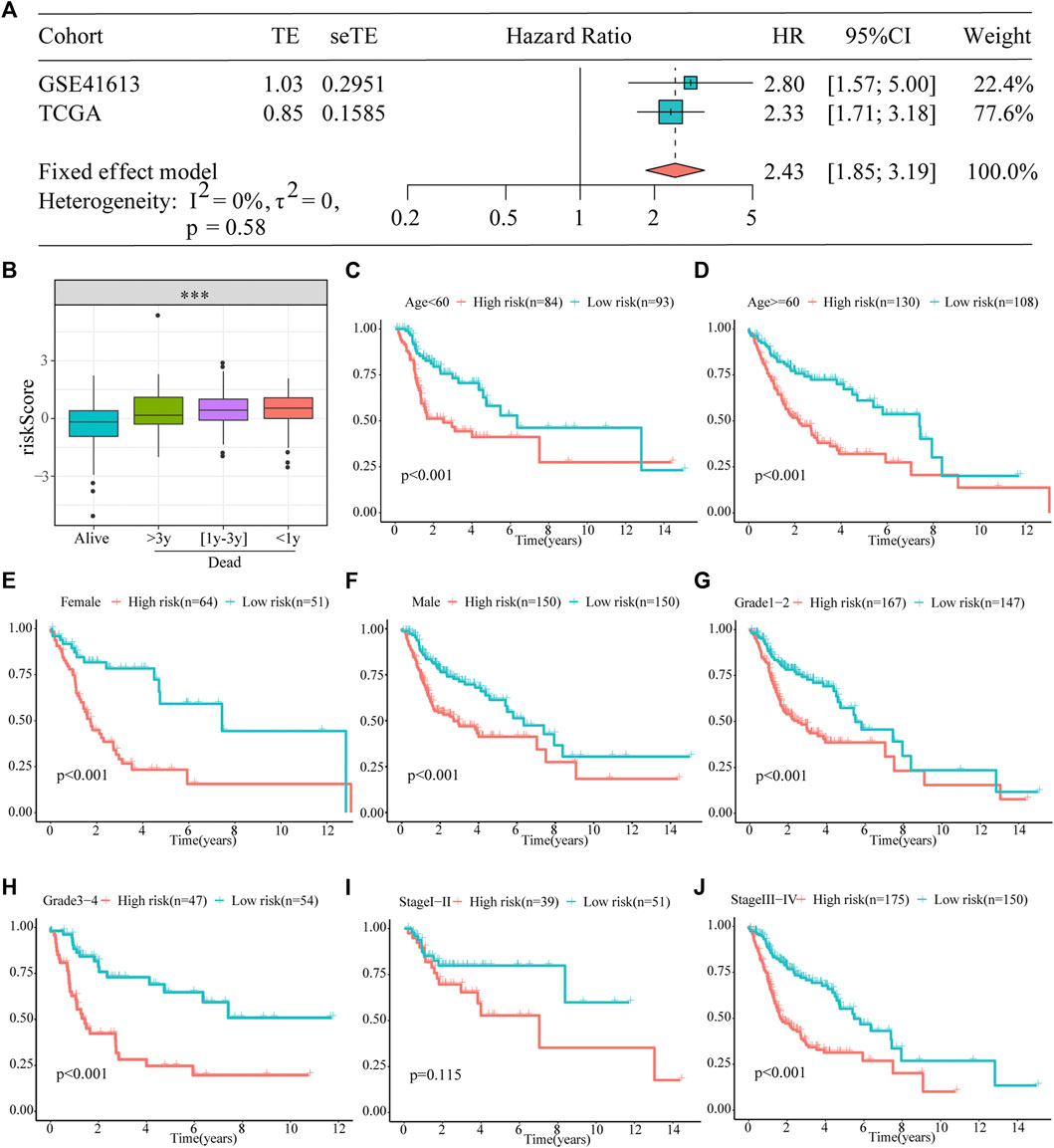
FIGURE 4. Prognostic signature can be used as a marker of survival in pooled cohorts and subgroups. (A) Meta-analysis. (B) The risk score is higher for patients who died than for those who were alive, particularly in the group with shorter survival. (C–J) Kaplan–Meier survival analysis of the signature between the high- and low-risk groups in TCGA cohort stratified by different clinicopathological parameters.
By analyzing HNSCC samples from the cBioPortal database, we assessed alterations in the 10 genes used to create the prognostic signature. The total mutation frequency was 42.2%, and all genes in the prognostic signature had amplified or missense mutations in patients with HNSCC, suggesting that these 10 genes play an important role in HNSCC (Figure 5A). Among the 496 patients with HNSCC, 1.21% had mutations, 21.37% had amplifications, and 2.42% had multiple alterations in SHANK2; 4.84% had mutations, 0.2% had multiple alterations, and 0.4% had deep deletions in PCDH9; 2.82% had mutations, 0.2% had deep deletions in CELSR3, 0.2% had mutations, and 1.81% had amplifications in NAT10; 1.01% had mutations, 0.2% had structural variants, 0.4% had amplifications, and 0.4% had deep deletions in DCLRE1C; 1.01% had mutations, 0.2% had amplifications, and 0.6% had deep deletions in PFKP; 1.01% had amplifications and 0.2% had structural variants in SSB; 0.4% had mutations and 0.2% had deep deletions in MAP2K7; and 0.2% had mutations in ODF4 (Figure 5B).
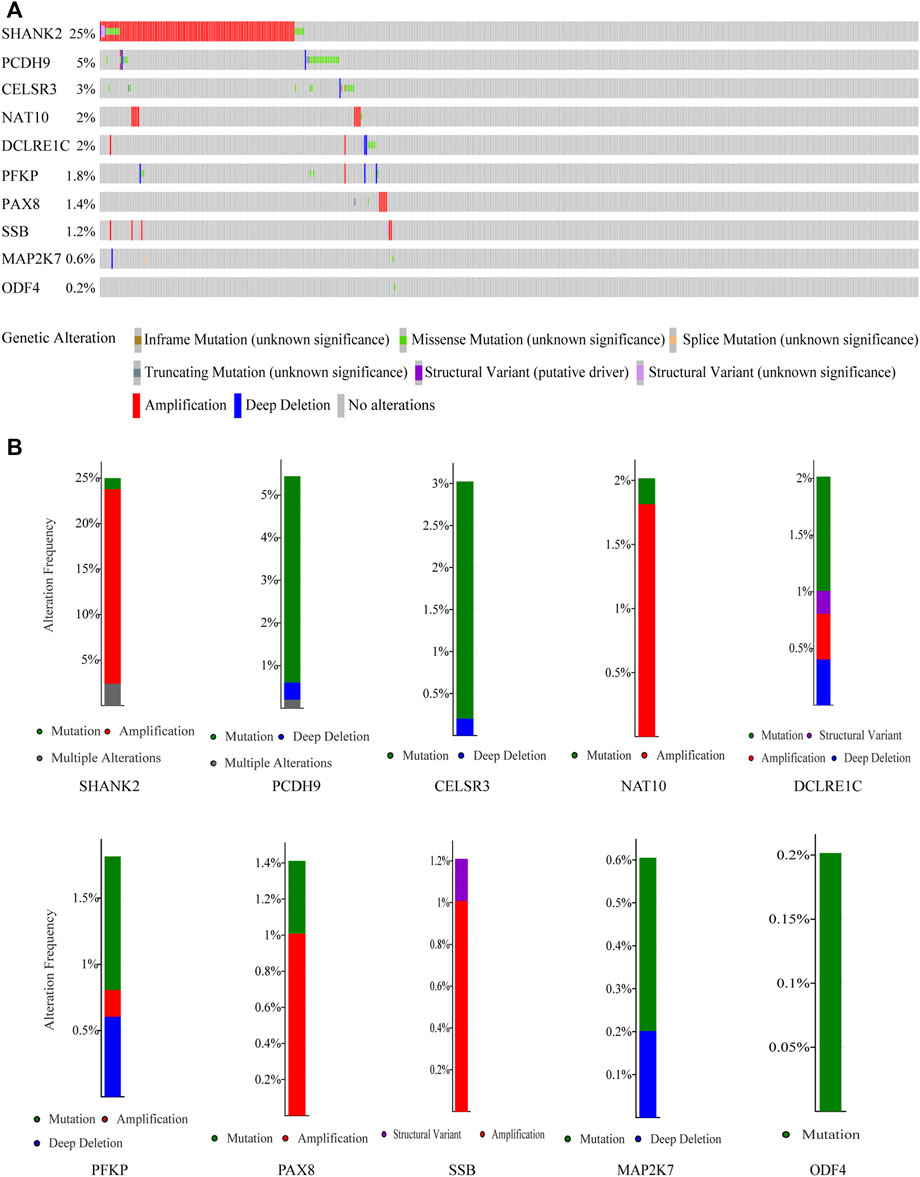
FIGURE 5. Genetic alterations of the 10 genes analyzed utilizing cBioPortal. (A) Genetic alterations in each of the 10 genes in the prognosis signature. (B) Specific alteration frequency of the 10 genes with the study of clinical samples.
We executed two different algorithms, namely SVM and LASSO, on the 10 genes used to construct the prognostic model to improve the accuracy of the diagnostic model. Ten genes were screened using the LASSO algorithm, and nine candidate genes were obtained (Figure 6A). Screening was performed using the SVM-RFE algorithm, and eight genes were identified (Figure 6B). Subsequently, by taking the intersection of the genes obtained using the two algorithms, we obtained eight genes to construct diagnostic markers (Figure 6C). Finally, a multivariate logistic regression analysis was used to construct a diagnostic model based on these eight genes. The model formula is as follows: -8.3049 + (−9.9087*ODF4) + (−2.3662*PCDH9) + (0.8175*PFKP) + (1.2565*SSB) + (0.2716*MAP2K7) + (0.5908*NAT10) + (−1.769*DCLRE1C) + (7.2511*CELSR3). In TCGA dataset, ROC showed that our diagnostic model had a high AUC value (0.953), indicating that the model could accurately differentiate between HNSCC and normal tissues (Figure 6D). In addition, we evaluated the performance of the diagnostic model using two external datasets and found that the model had a high diagnostic value (GSE127165: AUC = 0.914; GSE37991: AUC = 0.950; Figures 6E,F).
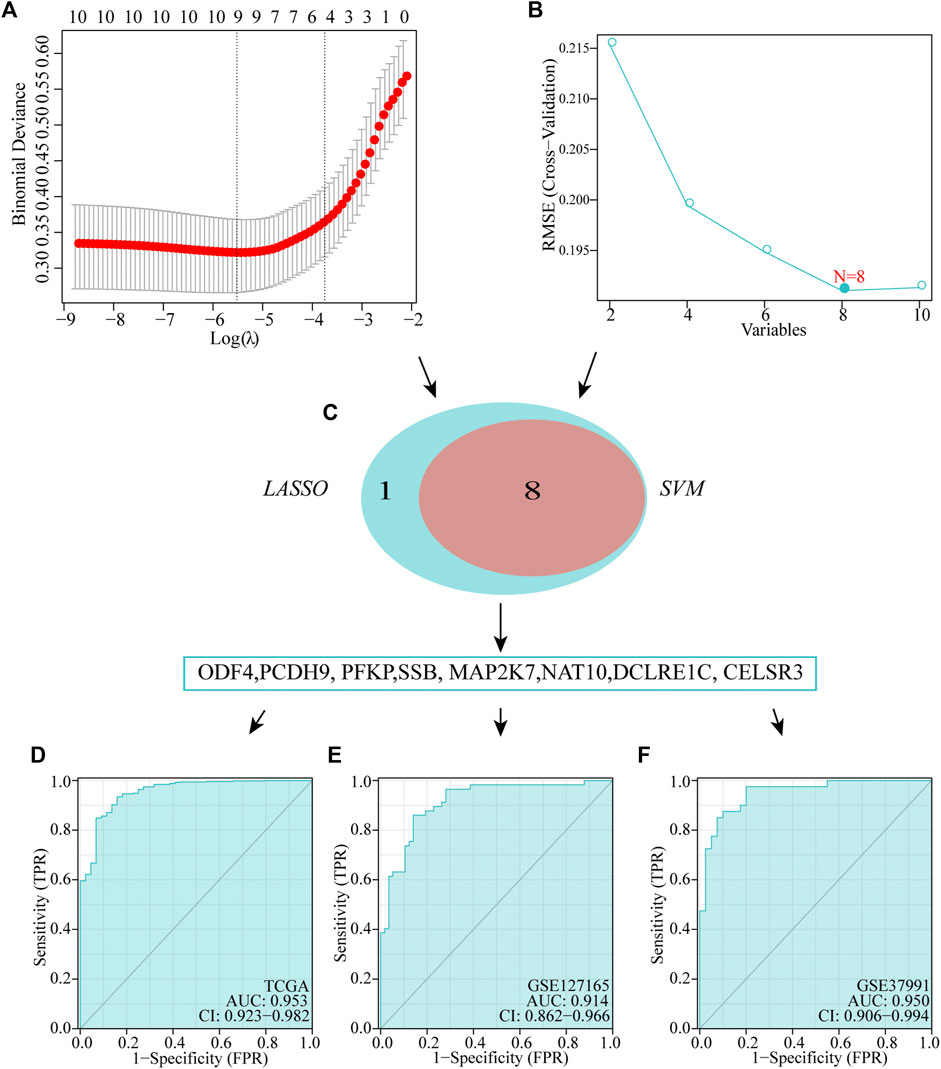
FIGURE 6. Establishment of multigene diagnostic signature. A total of eight genes have been selected through LASSO (A) and SVM (B) analyses, with AUCs of 0.953 (D): TCGA, 0.978 (E): GSE127165, and 0.950 (F): GSE37991.
To investigate whether or not prognostic models can guide the use of chemotherapeutic drugs in clinical practice, we compared IC50 of the high- and low-risk groups with those of various common chemotherapeutic drugs and found higher sensitivity to cisplatin, imatinib, doxorubicin, cytarabine, lapatinib, and docetaxel in the high-risk group (Figure 7A). In addition, IC50 of vinblastine, methotrexate, rapamycin, paclitaxel, vorinostat, and nilotinib was lower in patients with lower risk scores, suggesting that patients with HNSCC in the lower-risk group were sensitive to these drugs (Figure 7B).
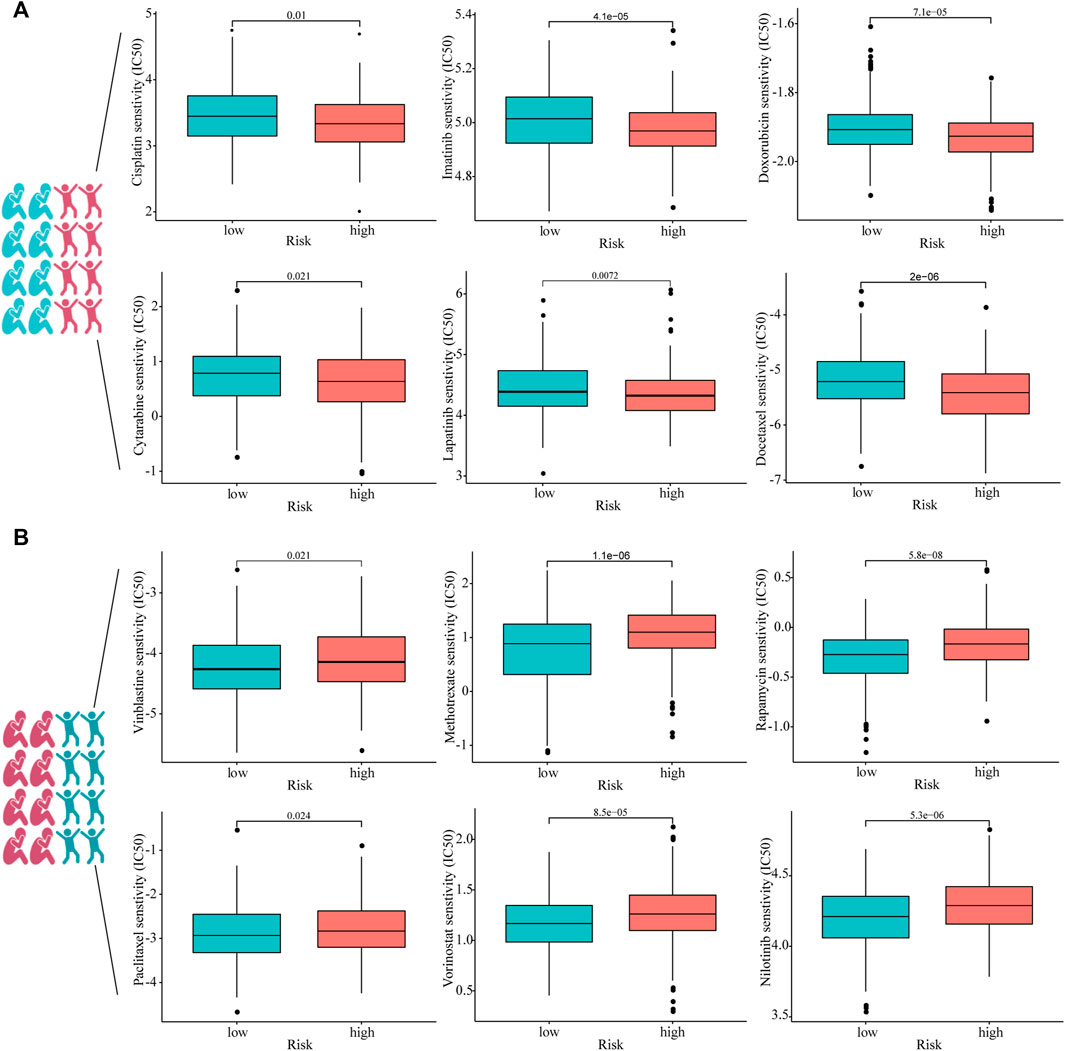
FIGURE 7. Estimated drug sensitivity in patients with HNSCC in high- (n = 249), (A) and low-risk (n = 250), (B) groups.
To detect differences in mRNA expression of the eight signature genes, we conducted reverse transcription qRT-PCR to detect 12 pairs of cancer and normal tissues (Figure 8A). The mRNA expression levels of DCLRE1C, PCDH9, and ODF4 in tumors were significantly lower than those in the normal tissues. In contrast, MAP2K7, CELSR3, and PFKP were overexpressed in tumor tissues. However, mRNA expression levels of SSB and NAT10 did not differ between HNSCC and adjacent normal tissues (Figure 8A). Furthermore, Western blotting and immunohistochemistry analyses revealed that DCLRE1C was expressed at substantially lower levels in HNSCC tissues than in corresponding normal tissues (Figures 8B,C).
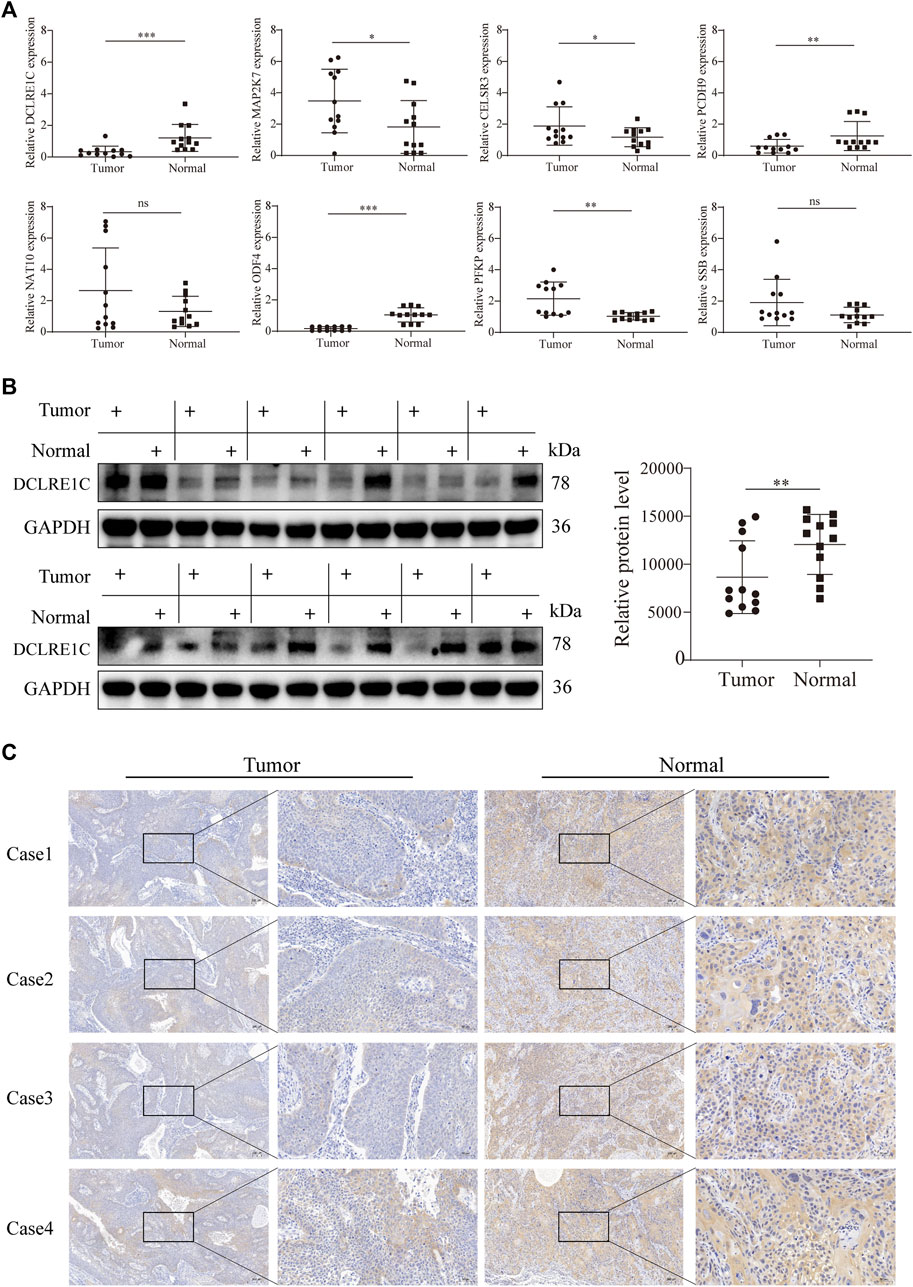
FIGURE 8. Detection of gene expression in tissue samples using qRT-PCR, WB and IHC.(A) qRT-PCR analysis of mRNA levels in tumor and adjacent normal tissues.(B,C) Western blotting, immunohistochemistry analysis of DCLRE1C protein levels in tumor and adjacent normal tissues.
HNSCC is a common cancer worldwide. Even after new therapeutic methods and significant advances in clinical research, the long-term life expectancy and survival rate of patients with HNSCC remain unsatisfactory because of tumor recurrence or metastasis. Although clinical patients have the same medical and pathological levels, because of the complicated etiological elements and high heterogeneity, predicting the survival rate of patients with HNSCC is difficult.
Currently, effective biomarkers with high accuracy for the diagnosis and prognosis of HNSCC are lacking (Zhao et al., 2010). Therefore, establishing accurate prognostic models and diagnostic markers is necessary. However, bioinformatics research has often focused on a single database or only on the prognostic value, which has some limitations (Cui et al., 2020). In recent years, with the rapid development of bioinformatics, numerous novel gene biomarkers have been discovered as critical modulators for the diagnosis and survival prognosis prediction of various diseases (Wang et al., 2009; Zhao and Bai, 2020). Future research should identify clinically significant genes, predict their functions, and explore their prognostic value using bioinformatics.
Altered expression levels of tumor-driver genes may promote malignant biological behavior of tumor cells (Bossi et al., 2016; Zhao et al., 2019). Based on 2,372 tumor-driver genes, new models that can predict the prognosis of patients with HNSCC as well as accurate diagnostic markers may be identified through the combined use of bioinformatics approaches. In this study, we used WGCNA to identify modules associated with HNSCC and successively used univariate, LASSO, and multivariate Cox regression models to filter genes to establish a tumor driver-related gene signature. The performance of this signature was verified using the GSE41613 cohort. In addition, although the meta-analysis and subgroup analysis were based on TCGA cohort, our prognostic model could discriminate between high- and low-risk populations. These results demonstrated the superior predictive performance of the proposed model. In clinical practice, this is conducive to prolonging patient survival if an accurate diagnosis can be made for patients with HNSCC. The diagnostic model that we constructed showed excellent performance in both the training and independent validation sets. However, the constituent genes of the two models are not identical. There may be the following reasons. First, models were built on different people. In more detail, prognostic model were constructed for tumor patients, while diagnostic model were constructed based on normal cohorts and tumor patients. Second, the algorithms used in the construction of the two models were different. The data types in the prognostic model were survival data and in the diagnostic model were dichotomous variables, which were analysed using LASSO “Cox” and “binomial” regressions respectively using the glmnet R package. Third, the diagnostic model use the SVM-RFE algorithm, which is based on the SVM interval maximisation principle and uses the support vector machine weight coefficients as a scoring criterion to rank genes, eliminating one gene at a time with the lowest ranking score, until the final set of ranked features is obtained. After ten genes were screened by this step, SHANK2 and PAX8 genes were filtered out and were not involved in the construction of the diagnostic model. In addition, SHANK2 and DCLRE1C of these ten genes were not differentially expressed in normal and tumor tissues. A number of previous studies have performed differential expression analyses prior to constructing prognostic models (Long et al., 2020; Yan et al., 2022). However, in this study we were concerned that prognosis-related genes would be filtered out during differential analysis, so we included all genes directly in the analysis. This is similar to previous studies (Cai et al., 2021). Regardless, our findings suggest that the performance of these two models is very strong. If the model can be applied to clinical work in the future, this will surely reduce the public health burden.
To date, chemotherapy remains an effective treatment option for patients with HNSCC, and selection of the exact chemotherapeutic drug can reduce patient suffering and prolong life expectancy. Therefore, we maximized the benefit rate for patients by predicting the sensitivity of chemotherapeutic drugs in different subgroups of the population.
In this study, qRT-PCR showed that the expression levels of two genes, DCLRE1C and ODF4, differed significantly between normal and tumor tissues. In addition, ODF4 was expressed at a lower level in the tumor group than in the DCLRE1C group. Therefore, we selected DCLRE1C to continue the subsequent Western blotting and immunohistochemistry analyses, which were consistent with the qRT-PCR results.
Some genes used to build prognostic models have been studied in other cancers. For example, PFKP expression levels are negatively correlated with the prognosis of lung cancer, and the proliferation rate of cells with low PFKP expression is significantly reduced (Shen et al., 2020). In addition, PFKP can be used as a therapeutic target in patients with breast cancer (Yeerken et al., 2020). In oral cancer, regulation of PFKP expression promotes cell proliferation, migration, and invasion (Chen et al., 2018). Recently, Zhang et al. demonstrated through a series of in vivo and in vitro experiments that reduced levels of NAT10 expression could inhibit gastric cancer metastasis (Zhang et al., 2021). In a study on hepatocellular carcinoma, NAT10 expression was significantly upregulated in cancerous tissues, and its expression level was negatively correlated with the OS of patients, suggesting that it is an oncogene (Li et al., 2017). However, in our study, reverse transcription qRT-PCR showed that the difference in expression levels of NAT10 in cancer and normal tissues was not significant. The reason for this result may be the insufficient sample size and the fact that tumor subtypes are not highly representative. Decreased PCDH9 expression is associated with the metastasis of gastric cancer cells (Chen et al., 2015). High levels of miR-200a-3p promote the proliferation of ovarian cancer cells by targeting PCDH9 (Shi et al., 2019). These results indicated that PCDH9 is a tumor-suppressor gene with low expression in tumor tissues, consistent with our reverse transcription qRT-PCR results. PAX8 promotes the proliferation of gastric cancer cells (Bie et al., 2019). Low expression of CELSR3 significantly reduces the migration and invasion of lung adenocarcinoma cells (Li et al., 2021). CELSR3 expression may serve as a prognostic biomarker in patients with prostate cancer and may predict poor outcomes (Chen et al., 2021). In addition, CELSR3 is highly expressed in liver and oral cancers and associated with a poor prognosis (Gu et al., 2019; Zheng et al., 2022). In another study, ODF4 was significantly highly expressed in breast cancer tissue and could be used in combination with other biomarkers to differentiate between cancer and normal tissues (Kazemi-Oula et al., 2015). This is in contrast with the results of our reverse transcription qRT-PCR analyses, and it could play different biological roles in different cancers. Taken together, the potential mechanisms of these genes in HNSCC require further detailed investigations.
The present study has some limitations. First, the sample size from our center was small, and more samples with detailed clinicopathological and prognostic information are necessary to further investigate the performance of the risk signature in predicting HNSCC progression and prognosis. Second, we require a longer follow-up period to further compare HNSCC between low- and high-risk groups because of the relatively limited follow-up period. In addition, functions of the eight genes involved in the malignant progression of HNSCC were not investigated. Further research is required to explore the mechanisms of the eight genes involved in tumor progression.
We developed a new 10-gene model using a combination of bioinformatics approaches, which could accurately predict the prognosis of HNSCC and identify the chemotherapeutic drugs from which patients benefit, thus facilitating personalized management of patients with HNSCC. In addition, we successfully constructed a biomarker capable of accurately diagnosing HNSCC, which can be used in the molecular diagnosis of HNSCC.
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found below: https://www.ncbi.nlm.nih.gov/geo/, GSE41613 https://www.ncbi.nlm.nih.gov/geo/, GSE127165.
YL and JW conceived and designed the study. SL, WL, and ZD developed the methodology. XY, YJ, and YW involved in data acquisition. ZD performed bioinformatic analysis. SL and WL analyzed and interpreted the data. The revision of the manuscript was mainly carried out by SL and ZD. YL and JW supervised the study. All authors approved the final manuscript.
This study was funded by the Key project of Natural Science Foundation of Anhui Provincial Education Department (KJ2018ZD021), the first batch of “Peak Climbing Plan” discipline construction project of the First Affiliated Hospital of Anhui Medical University (Hospital Department [2019] No. 22).
We greatly acknowledge TCGA and GEO database for providing their platforms and contributors for uploading their meaningful datasets. We also thank all members of the laboratory for their kindness and help.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmolb.2022.912620/full#supplementary-material
Bie, L. Y., Li, D., Wei, Y., Li, N., Chen, X. B., and Luo, S. X. (2019). SOX13 dependent PAX8 expression promotes the proliferation of gastric carcinoma cells. Artif. Cells Nanomed. Biotechnol. 47 (1), 3180–3187. doi:10.1080/21691401.2019.1646751
Bossi, D., Cicalese, A., Dellino, G. I., Luzi, L., Riva, L., D'Alesio, C., et al. (2016). In vivo genetic screens of patient-derived tumors revealed unexpected frailty of the transformed phenotype. Cancer Discov. 6 (6), 650–663. doi:10.1158/2159-8290.CD-15-1200
Bray, F., Ferlay, J., Soerjomataram, I., Siegel, R. L., Torre, L. A., and Jemal, A. (2018). Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA. Cancer J. Clin. 68 (6), 394–424. doi:10.3322/caac.21492
Cai, W., Bao, W., Chen, S., Yang, Y., and Li, Y. (2021). Metabolic syndrome related gene signature predicts the prognosis of patients with pancreatic ductal carcinoma. A novel link between metabolic dysregulation and pancreatic ductal carcinoma. Cancer Cell Int. 21 (1), 698. doi:10.1186/s12935-021-02378-w
Cerami, E., Gao, J., Dogrusoz, U., Gross, B. E., Sumer, S. O., Aksoy, B. A., et al. (2012). The cBio cancer genomics portal: An open platform for exploring multidimensional cancer genomics data. Cancer Discov. 2 (5), 401–404. doi:10.1158/2159-8290.CD-12-0095
Chen, G., Liu, H., Zhang, Y., Liang, J., Zhu, Y., Zhang, M., et al. (2018). Silencing PFKP inhibits starvation-induced autophagy, glycolysis, and epithelial mesenchymal transition in oral squamous cell carcinoma. Exp. Cell Res. 370 (1), 46–57. doi:10.1016/j.yexcr.2018.06.007
Chen, X., Ma, Q., Liu, Y., Li, H., Liu, Z., Zhang, Z., et al. (2021). Increased expression of CELSR3 indicates a poor prognostic factor for Prostate Cancer. J. Cancer 12 (4), 1115–1124. doi:10.7150/jca.49567
Chen, Y., Xiang, H., Zhang, Y., Wang, J., and Yu, G. (2015). Loss of PCDH9 is associated with the differentiation of tumor cells and metastasis and predicts poor survival in gastric cancer. Clin. Exp. Metastasis 32 (5), 417–428. doi:10.1007/s10585-015-9712-7
Cognetti, D. M., Weber, R. S., and Lai, S. Y. (2008). Head and neck cancer: An evolving treatment paradigm. Cancer 113 (7), 1911–1932. doi:10.1002/cncr.23654
Cui, K., Liu, C., Li, X., Zhang, Q., and Li, Y. (2020). Comprehensive characterization of the rRNA metabolism-related genes in human cancer. Oncogene 39 (4), 786–800. doi:10.1038/s41388-019-1026-9
Diez-Fraile, A., Ceulaer, J., Derpoorter, C., Spaas, C., Backer, T., Lamoral, P., et al. (2020). Circulating non-coding RNAs in head and neck cancer: Roles in diagnosis, prognosis, and therapy monitoring. Cells 10 (1), E48. doi:10.3390/cells10010048
Emilsson, V., Thorleifsson, G., Zhang, B., Leonardson, A. S., Zink, F., Zhu, J., et al. (2008). Genetics of gene expression and its effect on disease. Nature 452 (7186), 423–428. doi:10.1038/nature06758
Gu, X., Li, H., Sha, L., Mao, Y., Shi, C., and Zhao, W. (2019). CELSR3 mRNA expression is increased in hepatocellular carcinoma and indicates poor prognosis. PeerJ 7, e7816. doi:10.7717/peerj.7816
Kazemi-Oula, G., Ghafouri-Fard, S., Mobasheri, M. B., Geranpayeh, L., and Modarressi, M. H. (2015). Upregulation of RHOXF2 and ODF4 expression in breast cancer tissues. Cell J. 17 (3), 471–477. doi:10.22074/cellj.2015.8
Langfelder, P., and Horvath, S. (2008). WGCNA: an R package for weighted correlation network analysis. BMC Bioinforma. 9, 559. doi:10.1186/1471-2105-9-559
Li, Q., Liu, X., Jin, K., Lu, M., Zhang, C., Du, X., et al. (2017). NAT10 is upregulated in hepatocellular carcinoma and enhances mutant p53 activity. BMC cancer 17 (1), 605. doi:10.1186/s12885-017-3570-4
Li, Y., Zhu, L., Hao, R., Li, Y., Zhao, Q., and Li, S. (2021). Systematic expression analysis of the CELSR family reveals the importance of CELSR3 in human lung adenocarcinoma. J. Cell. Mol. Med. 25 (9), 4349–4362. doi:10.1111/jcmm.16497
Lin, W., Wan, X., Sun, A., Zhou, M., Chen, X., Li, Y., et al. (2021). RUNX1/EGFR pathway contributes to STAT3 activation and tumor growth caused by hyperactivated mTORC1. Mol. Ther. Oncolytics 23, 387–401. doi:10.1016/j.omto.2021.10.009
Long, J., Zhang, S., Zeng, X., Ouyang, Y., Wang, Y., Hu, Z., et al. (2020). Development of an immunogenomic landscape-based prognostic index of head and neck squamous cell carcinoma. Front. Mol. Biosci. 7, 586344. doi:10.3389/fmolb.2020.586344
Ma, Y., Wang, X., Qiu, C., Qin, J., Wang, K., Sun, G., et al. (2021). Using protein microarray to identify and evaluate autoantibodies to tumor-associated antigens in ovarian cancer. Cancer Sci. 112 (2), 537–549. doi:10.1111/cas.14732
Morganti, S., Tarantino, P., Ferraro, E., D'Amico, P., Duso, B. A., and Curigliano, G. (2019). Next generation sequencing (ngs): A revolutionary technology in pharmacogenomics and personalized medicine in cancer. Adv. Exp. Med. Biol. 1168, 9–30. doi:10.1007/978-3-030-24100-1_2
Rickinson, A. B. (2014). Co-Infections, inflammation and oncogenesis: Future directions for EBV research. Semin. Cancer Biol. 26, 99–115. doi:10.1016/j.semcancer.2014.04.004
Rosenberg, A. J., and Vokes, E. E. (2021). Optimizing treatment de-escalation in head and neck cancer: Current and future perspectives. Oncologist 26 (1), 40–48. doi:10.1634/theoncologist.2020-0303
Sacconi, A., Donzelli, S., Pulito, C., Ferrero, S., Spinella, F., Morrone, A., et al. (2020). TMPRSS2, a SARS-CoV-2 internalization protease is downregulated in head and neck cancer patients. J. Exp. Clin. Cancer Res. 39 (1), 200. doi:10.1186/s13046-020-01708-6
Shen, J., Jin, Z., Lv, H., Jin, K., Jonas, K., Zhu, C., et al. (2020). PFKP is highly expressed in lung cancer and regulates glucose metabolism. Cell. Oncol. 43 (4), 617–629. doi:10.1007/s13402-020-00508-6
Shi, C., Yang, Y., Zhang, L., Yu, J., Qin, S., Xu, H., et al. (2019). MiR-200a-3p promoted the malignant behaviors of ovarian cancer cells through regulating PCDH9. Onco. Targets. Ther. 12, 8329–8338. doi:10.2147/OTT.S220339
Steeg, P. S. (2006). Tumor metastasis: Mechanistic insights and clinical challenges. Nat. Med. 12 (8), 895–904. doi:10.1038/nm1469
Syed, M., Flechsig, P., Liermann, J., Windisch, P., Staudinger, F., Akbaba, S., et al. (2020). Fibroblast activation protein inhibitor (FAPI) PET for diagnostics and advanced targeted radiotherapy in head and neck cancers. Eur. J. Nucl. Med. Mol. Imaging 47 (12), 2836–2845. doi:10.1007/s00259-020-04859-y
Tumban, E. (2019). A current update on human papillomavirus-associated head and neck cancers. Viruses 11 (10), E922. doi:10.3390/v11100922
Wan, X., Zhou, M., Huang, F., Zhao, N., Chen, X., Wu, Y., et al. (2021). AKT1-CREB stimulation of PDGFRα expression is pivotal for PTEN deficient tumor development. Cell Death Dis. 12 (2), 172. doi:10.1038/s41419-021-03433-0
Wang, Y., Tang, S., Wu, Y., Wan, X., Zhou, M., Li, H., et al. (2020). Upregulation of 6-phosphofructo-2-kinase (PFKFB3) by hyperactivated mammalian target of rapamycin complex 1 is critical for tumor growth in tuberous sclerosis complex. IUBMB life 72 (5), 965–977. doi:10.1002/iub.2232
Wang, Z., Gerstein, M., and Snyder, M. (2009). RNA-seq: A revolutionary tool for transcriptomics. Nat. Rev. Genet. 10 (1), 57–63. doi:10.1038/nrg2484
Yan, L., Chen, X., Bian, Z., Gu, C., Ji, H., Chen, L., et al. (2022). A ferroptosis associated gene signature for predicting prognosis and immune responses in patients with colorectal carcinoma. Front. Genet. 13, 971364. doi:10.3389/fgene.2022.971364
Yeerken, D., Hong, R., Wang, Y., Gong, Y., Liu, R., Yang, D., et al. (2020). PFKP is transcriptionally repressed by BRCA1/ZBRK1 and predicts prognosis in breast cancer. PloS one 15 (5), e0233750. doi:10.1371/journal.pone.0233750
Zhang, B., and Horvath, S. (2005). A general framework for weighted gene co-expression network analysis. Stat. Appl. Genet. Mol. Biol. 4, Article17. doi:10.2202/1544-6115.1128
Zhang, Y., Jing, Y., Wang, Y., Tang, J., Zhu, X., Jin, W. L., et al. (2021). NAT10 promotes gastric cancer metastasis via N4-acetylated COL5A1. Signal Transduct. Target. Ther. 6 (1), 173. doi:10.1038/s41392-021-00489-4
Zhao, E., and Bai, X. (2020). Nomogram based on microRNA signature contributes to improve survival prediction of clear cell renal cell carcinoma. Biomed. Res. Int. 2020, 7434737. doi:10.1155/2020/7434737
Zhao, S., Liu, J., Nanga, P., Liu, Y., Cicek, A. E., Knoblauch, N., et al. (2019). Detailed modeling of positive selection improves detection of cancer driver genes. Nat. Commun. 10 (1), 3399. doi:10.1038/s41467-019-11284-9
Zhao, W., Langfelder, P., Fuller, T., Dong, J., Li, A., and Hovarth, S. (2010). Weighted gene coexpression network analysis: State of the art. J. Biopharm. Stat. 20 (2), 281–300. doi:10.1080/10543400903572753
Zheng, K., Lan, T., Li, G. P., Huang, L., Chen, Y. P., Su, B. H., et al. (2022). Evaluated expression of CELSR3 in oral squamous cell carcinoma is associated with perineural invasion and poor prognosis. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 133 (5), 564–573. doi:10.1016/j.oooo.2021.10.016
Keywords: signature, HNSCC, WGCNA, prognosis, diagnosis
Citation: Liu S, Liu W, Ding Z, Yang X, Jiang Y, Wu Y, Liu Y and Wu J (2022) Identification and validation of a novel tumor driver gene signature for diagnosis and prognosis of head and neck squamous cell carcinoma. Front. Mol. Biosci. 9:912620. doi: 10.3389/fmolb.2022.912620
Received: 04 April 2022; Accepted: 04 October 2022;
Published: 20 October 2022.
Edited by:
Marco Sciacovelli, University of Cambridge, United KingdomReviewed by:
Zuquan Hu, Guizhou Medical University, ChinaCopyright © 2022 Liu, Liu, Ding, Yang, Jiang, Wu, Liu and Wu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yehai Liu, bGl1eWVoYWlAYWhtdS5lZHUuY24=; Jing Wu, Mjc2Mjg4ODYzQHFxLmNvbQ==
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.