 Arnaud Chalin1†
Arnaud Chalin1† Antoine Arvor2†
Antoine Arvor2† Anne-Sophie Hervault1Marc Plaisance2Léa Niol1Stéphanie Simon2
Anne-Sophie Hervault1Marc Plaisance2Léa Niol1Stéphanie Simon2 Hervé Volland2*
Hervé Volland2*- 1NG Biotech – Research and Development Department, Guipry-Messac, France
- 2Université Paris-Saclay, Commissariat à l'Energie Atomique et aux Energies Alternatives (CEA), Institut National de Recherche pour l'Agriculture, l'Alimentation et l'Environnement (INRAE), Médicaments et Technologies pour la Santé (MTS), Service de Pharmacologie et d'Immunoanalyse (SPI), Laboratoire d'Etudes et de Recherches en Immunoanalyse (LERI), Gif-sur-Yvette, France
Introduction: Candida auris is a recently discovered yeast with a multi-drug resistant profile associated with high mortality rates. The rapid identification of Candida auris in hospital settings is crucial to allow appropriate therapeutic and rapid implementation of infection management measures. The aim of this study was to develop a lateral flow immunoassay (LFIA) for the rapid identification of Candida auris.
Methods: Highly specific monoclonal antibodies were obtained by immunizing mice with membrane proteins from Candida auris which were then used to develop a LFIA whose performance was assessed by testing 12 strains of Candida auris and 37 strains of other Candida species. Isolates were grown on either Sabouraud dextrose, CHROMagarTM Candida Plus or HardyCHROMTM Candida + auris agar plates. The strains were also cultured on salt sabouraud-dextrose with chloramphenicol or a commercially available Salt-Sabouraud Dulcitol Broth with chloramphenicol and gentamicin, and processed using a simple centrifugation protocol to recover a pellet. Finally, the colonies or yeast extract were transferred to the LFIA to determine the specificity and sensitivity of the assay.
Results: The LFIA reached 100% specificity and sensitivity from solid agar plates. For both enrichment broths, some Candida non-auris species were able to grow, but the LFIA remained 100% specific. The use of a dextrose-based sabouraud broth resulted in earlier identification with the LFIA, with most of the Candida auris strains detected at 24 h.
Conclusion: The developed LFIA prototype represents a powerful tool to fight the emerging threat of Candida auris. Clinical validation represents the next step.
1 Introduction
Nosocomial candidiasis represents a major threat to immunocompromised and critically-ill patients, and is the most important fungal infection in hospitalized patients worldwide (Brown et al., 2012; Pfaller and Castanheira, 2016). The mortality rate of candidemia, a life-threatening condition, has not decreased over the past two decades despite the introduction of new antifungal agents (Pfaller and Castanheira, 2016). This is a result of the complexity of Candida infection diagnosis, leading to challenges in rapid administration of adequate antifungal therapy, and inappropriate use of empiric therapies (Garey et al., 2006; Azoulay et al., 2012; Drgona et al., 2014).
Among the Candida species, Candida auris is a recently discovered ascomycetous yeast first identified in 2009 from the external ear canal of an inpatient in a Japanese hospital (Satoh et al., 2009). Candida auris simultaneously emerged on different continents around the world (Lockhart et al., 2017) and is currently divided into four major clades plus 1 minor clade (Lockhart et al., 2017; Chow et al., 2019). The rapid spread of Candida auris, associated high mortality rates (30–72%) (Chakrabarti et al., 2015; Lockhart et al., 2017; Jeffery-Smith et al., 2018; Ruiz-Gaitan et al., 2018; Osei Sekyere, 2019) and its multi-drug resistant profile justify the attention being paid to this worldwide emerging threat (Chowdhary et al., 2017; WHO, 2022). Indeed, Candida auris is usually resistant to the azole antifungal class, including fluconazole and voriconazole, and can also show resistance to echinocandins, amphotericin B and flucytosine (Ruiz Gaitan et al., 2017; Jacobs et al., 2022; Kilburn et al., 2022). Moreover, it is very worrying to note the emergence of pan-resistance to four major classes of antifungals in some Candida auris clinical isolates (Jacobs et al., 2022).
Risk factors are identical to those of candidiasis caused by other species and typical of opportunistic and nosocomial organisms, namely: prolonged hospitalization especially in an intensive care unit (ICU) (Rudramurthy et al., 2017), and immunosuppression or prior exposure to broad-spectrum antibiotics and antifungal therapy (Calvo et al., 2016; Lockhart et al., 2017; Rudramurthy et al., 2017). Candida auris is a notable nosocomial agent due to its opportunistic behavior, but also because of its persistence on surfaces (Welsh et al., 2017; Short et al., 2019) and ability to colonize patient skin (Horton et al., 2020; Uppuluri, 2020). Consequently, Candida auris can easily spread in the hospital environment if infection control measures are insufficient, including disinfection, isolation and testing protocols (Eckbo et al., 2021; Prestel et al., 2021; Villanueva-Lozano et al., 2021; Thoma et al., 2022).
The rapid identification of Candida auris in hospital settings is therefore crucial to avoid therapeutic failure, fatal outcomes, to limit selective pressure caused by antifungal misuse and to allow infection management measures to be implemented as soon as possible.
Candida auris colonization can be determined by taking axilla or groin swabs, followed by an enrichment step using Sabouraud-based broth containing 10% sodium chloride and incubation for several days (Welsh et al., 2017). This method can be used to selectively look for Candida auris colonization, but still requires the yeast to be isolated on a solid media (Sabouraud or specific chromogenic media) for further examination, which requires a further 48 h or more until final identification. In the past, Candida auris has been misidentified as other Candida or yeast species (Lone and Ahmad, 2019) illustrating the need for new and updated identification methods. In recent years, substantial work has been performed in this direction with the development of selective and differential chromogenic culture media, several Deoxyribonucleic Acid (DNA)-based diagnostics, biochemical assimilations and protein profiles (Dennis et al., 2021). However, these are expensive, require trained technicians as well as complex equipment, thus limiting their broad availability. Affordable and easy-to-use tools are still required to fight effectively the spread of Candida auris in hospital settings (Dennis et al., 2021). Lateral flow immunoassay (LFIA) technology is fast, affordable, easy-to-use and highly suitable for use in hospital laboratories, but also in frontline and low-resource laboratories. In the last decade, LFIA tests have become key tools in the fight against antimicrobial resistance (AMR) (Boutal et al., 2022) among others. The aim of this work was to select, characterize and produce monoclonal antibodies (Mabs) specific for Candida auris and develop a LFIA prototype for the rapid identification of Candida auris on agar plates or directly from cloudy enrichment broths.
2 Materials and methods
2.1 Ethics statements
All experiments were performed in compliance with French and European regulations on the care of laboratory animals (European Community Directive 86/609, French Law 2001-486, 6 June 2001) and with the agreements of the Ethics Committee of the Commissariat à l'Energie Atomique (CEtEA “Comité d'Ethique en Experimentation Animale” n°44) nos. 12-026 and 15-055 delivered to Stéphanie Simon by the French Veterinary Services and CEA agreement D-91-272-106 from the Veterinary Inspection Department of Essonne (France).
2.2 Reagents
Phosphate-buffered saline (PBS) (ref. 524650), β-mercaptoethanol (ref. 63689, CAS: 60-24-2), sodium chloride (NaCl) (ref. 31434, CAS: 7646-14-5), chloramphenicol (ref. C0857, CAS: 56-75-7) and NHS-biotin (ref. B2643, CAS: 72040-63-2) were provided by Sigma Aldrich (Saint Quentin Fallavier, France). Sabouraud dextrose medium (2% dextrose and 1% peptone digest) was either provided by Sigma Aldrich (ref. S3306) or Beckton Dickinson (ref. 215193). All the Candida strains used are listed in Table 1. Biozzi mice were bred at the animal care unit of CEA (Gif sur Yvette, France). Sabouraud dextrose agar plates were purchased from Liofilchem (ref. 10035), CHROMagarTM Candida Plus manufactured by CHROMagarTM, and HardyCHROMTM Candida + auris manufactured by HardyCHROMTM. Sabouraud-Salt Dulcitol Broth (SSDB) supplemented with chloramphenicol and gentamicin was manufactured by S2MediaTM (ref. 5137) and was made according to the Centre for Disease Control (CDC) formula recommendation for isolation and enrichment of Candida auris. Enzyme immunoassays (EIAs) were performed with Maxisorp 96-well microtiter plates (Nunc) (Paris, France), and all reagents were diluted in EIA buffer [0.1 M phosphate buffer pH 7.4 containing 0.15 M NaCl, 0.1% bovine serum albumin (BSA) and 0.01% sodium azide]. Plates coated with proteins were saturated in EIA buffer (18 h at 4°C) and washed with washing buffer (0.1 M potassium phosphate pH 7.4 containing 0.05% Tween 20). Plates coated with yeasts were saturated in EIA buffer (18 h at 4°C) and washed with washing buffer without Tween® 20 (0.1 M potassium phosphate pH 7.4). Nitrocellulose strips with polystyrene backing were from GE Healthcare (Prima 40). Ellman's medium [7.5 × 10−4 M acetylthiocholine iodide (enzyme substrate) and 2.5 × 10−4 M 5,5′-dithiobis 2 nitrobenzoic acid (DTNB)], streptavidin-acetylcholinesterase (G4), Goat anti-mouse antibody-acétylcholinesterase and phosphate buffered saline pH 7.4 (10 mM sodium phosphate pH 7.4 containing 150 mM NaCl) were prepared at CEA (Gif-sur-Yvette, France). BCA protein assay kit (ref. 23235) was provided by Thermo Scientific™ (Waltham, Massachusetts, USA). Goat anti-mouse IgG/IgM polyclonal antibodies were provided by Jackson ImmunoResearch (ref. 115-005-044, Ely, United Kingdom). The colloidal gold solution was provided by NG Biotech (Guipry, France).
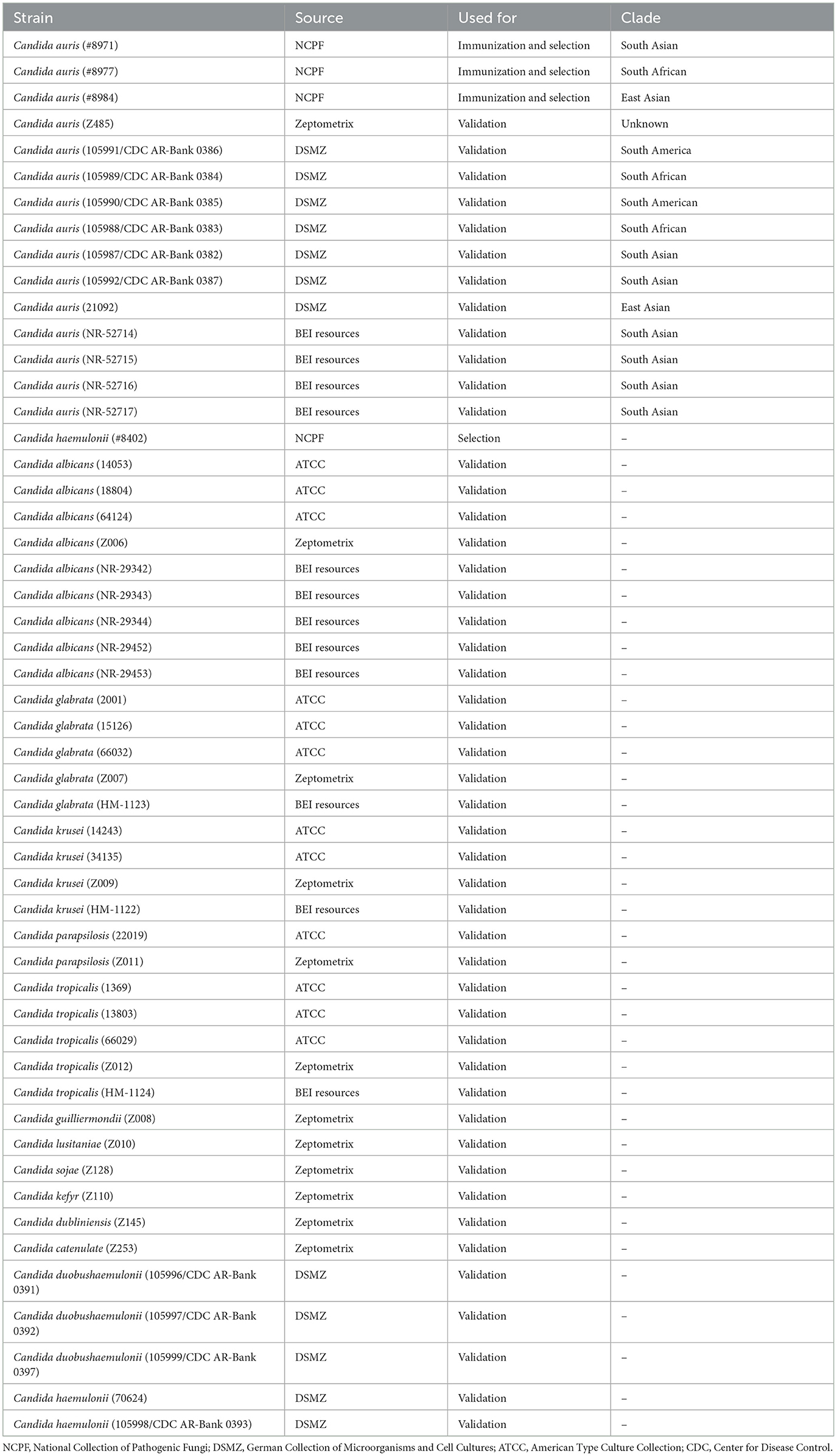
Table 1. List of Candida auris and non-auris strains used for immunization of mice, selection of the best monoclonal antibodies and/or validation of the lateral flow immunoassay prototype.
2.3 Preparation of immunogen and biotinylated surface proteins
Three Candida auris strains (#8971, #8977, #8984) (Table 1) were used for mice immunization and antibody selection. One Candida haemulonii strain (#8402) was used for antibody selection. Candida species were routinely maintained either in liquid Sabouraud dextrose medium, or on Sabouraud dextrose agar plates. For long-term storage, Candida cultures were kept frozen at −80°C with 20% glycerol. Using a 1 μL inoculation loop, yeasts in glycerol stock solution were transferred to a small volume of Sabouraud dextrose medium. Overnight grown yeasts (37, 35, or 30°C for Candida auris, Candida haemulonii and Candida albicans, respectively) were then used to inoculate a larger volume of Sabouraud dextrose medium. Yeast cells were pelleted twice by centrifugation at 3,000 g for 10 min and resuspended in the same volume of phosphate buffered saline pH 7.4 for washing. After the last wash, yeasts were resuspended in one tenth of the initial culture volume in ammonium carbonate buffer (1.89 g/L) containing 1% β-mercaptoethanol and incubated at 37°C for 30 min as described by Casanova and Chaffin (1991) for surface protein shaving. Supernatant was then collected by centrifugation at 3,000 g for 10 min and filtered at 0.22 μm to remove remaining yeast cells and before being dialysed thoroughly at 4°C in a capped Becher against phosphate buffered saline pH 7.4 to remove β-mercaptoethanol. Protein concentration was assessed with a BCA protein assay. Surface proteins were aliquoted and stored at −20°C until further use.
The immunogen preparation was made by mixing equivalent proportions of the surface proteins from the 3 Candida auris strains at 500 μg/mL in 50 mM potassium phosphate buffer pH 7.4. The surface protein solution was then mixed equally with Alum adjuvant to obtain the immunogen preparation.
Finally, the biotinylated surface proteins were prepared as follows. The medium protein size in the mix was approximately estimated by running surface proteins on SDS-PAGE. Biotin was conjugated to surface proteins by mixing NHS-biotin with surface proteins in 0.1 M borate buffer pH 9.0 (ratio NHS-biotin/protein = 20) and incubated for 30 min at room temperature. Unreacted ester functions were inactivated with 1 M Tris buffer pH 8.0 for 15 min at room temperature. Biotinylated surface proteins were then diluted in EIA buffer.
2.4 Production and screening of mouse monoclonal antibodies
Ten-week old Biozzi mice were immunized every 3 weeks with 50 μg of immunogen by intraperitoneal injection. Mice were bled to recover sera, before the first immunization and 2 weeks after each immunization. The polyclonal response was evaluated by testing sera with an immunoenzymatic test. Briefly, in microtiter plates coated with goat anti-mouse IgG/IgM polyclonal antibodies, 50 μl of biotinylated surface proteins were added to 50 μl of each serum diluted in EIA buffer. After overnight incubation at 4°C, the plates were washed with washing buffer, and 100 μl of streptavidin linked to acetylcholinesterase (G4) was deposited in the wells. After 1 h at room temperature, the plates were washed again and 200 μl of Ellman's medium was added to the wells. After a 30-min incubation, the absorbance was measured at 414 nm. The two mice showing the best immune response were selected for Mab production and given a daily intravenous booster injection of 50 μg immunogen for 3 days. Two days after the last boost, hybridoma were produced by fusing spleen cells with NS1 myeloma cells. Hybridoma culture supernatants were screened for antibody production by immunoenzymatic assay. Briefly, hybridoma were distributed on 20 microplates and culture supernatants were tested following Format 1 immunoenzymatic assay (Figure 1). Biotinylated surface proteins of Candida auris (#8971) were used for this immunoenzymatic assay. Hybridoma contained in wells giving the highest signals were selected. For the second selection step, hybridoma were tested by immunoenzymatic tests Format 1 and 2 (Figure 1). Biotinylated surface proteins of 3 Candida auris strains (#8971, #8977, #8984) and 1 Candida haemulonii strain (#8402) were tested separately following Format 1. Four different microplate coatings at 5 × 108 CFU/ml with 3 Candida auris strains (#8971, #8977, #8984) and 1 Candida haemulonii strain (#8402) were tested following Format 2. Hybridoma contained in wells giving the highest signals for Candida auris in any conditions and no signal for Candida haemulonii were selected for the next steps. The hybridoma were subsequently cloned by limiting dilutions. Mabs were produced in vitro and were purified using protein G affinity chromatography. The purity of the Mabs was then assessed by SDS-PAGE in reducing and non-reducing conditions.
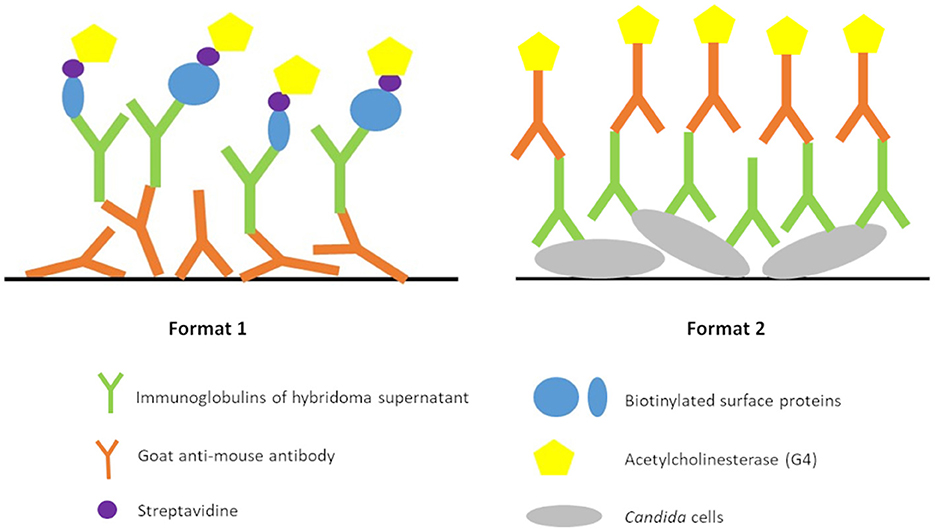
Figure 1. Immunoenzymatic test formats used for hybridoma screening.
To evaluate the best Mab pairs for use in the LFIA, a combinatorial analysis was carried out with each Mab either as capture or detection antibody, using shaved Candida surface proteins or whole Candida yeast as target. The colloidal-gold-labeled Mabs were prepared according to NG-Biotech instructions and the strips (0.5 cm width and 4.5 cm length) were prepared as follows. The test strip comprised a sample pad, a nitrocellulose membrane, and an absorption pad, all attached to a backing card. The detection zone comprised immobilized anti-mouse antibodies as a control line and anti-Candida auris antibodies as a test line (0.5 and 1 mg/ml in 50 mM potassium phosphate buffer pH 7.4, respectively) dispensed at 1 μl/cm using an automatic dispenser (BioDot Airjet XYZ 3050; BioDot, Irvine, CA, USA). After drying for 30 min at 37°C in an air oven, the absorption pad and the sample pad were stuck to the top and the bottom edges of the membrane, respectively. The membranes were cut into strips of 5 mm width using an automatic programmable cutter (Guillotine Cutting CM4000; BioDot). Shaved Candida surface proteins were mixed in migration buffer to a final concentration of 5 μg/ml supplemented with 0.01% N-ethylmaleimide. Whole yeasts were mixed in migration buffer to a final absorbance of OD600 = 1. After 5 min incubation, 100 μl of shaved Candida surface proteins or whole yeast suspensions were mixed with 10 μl of colloidal-gold-labeled Mabs in a 96-well microtiter plate and incubated for an additional 5 min. The LFIA strips were then inserted into the wells with the sample pad in contact with the liquid. After a 15 min migration the results were determined visually.
2.5 Candida auris LFIA prototype validation on solid media
The selected antibodies were produced on a large scale by CEA and provided to NG biotech (Guipry, France) for the development of the Candida auris LFIA prototype (Figure 2). Mouse anti-Candida auris capture antibody was immobilized on a test line and anti-mouse antibody was immobilized on a control line. The Candida strains (Table 1) used for validation of the LFIA prototype were grown for 48 h at 37°C on Sabouraud dextrose, CHROMagarTM Candida +, and HardyCHROMTM Candida + auris agar plates, with the exception of Candida dubliniensis, Candida catenulata and Candida duobushaemulonii which required 3, 4, and 5 days of growth, respectively. Using a 1 μL inoculation loop, three colonies were taken and resuspended in 150 μL of the lysis buffer and vortexed. A volume of 150 μL of migration buffer was added and the tube was vortexed again. Finally, 100 μL of the yeast extract was transferred onto the LFIA prototype and allowed to migrate for 15 min. The results were determined visually by monitoring the appearance of a red band on the test line, along with a band corresponding to the internal control.
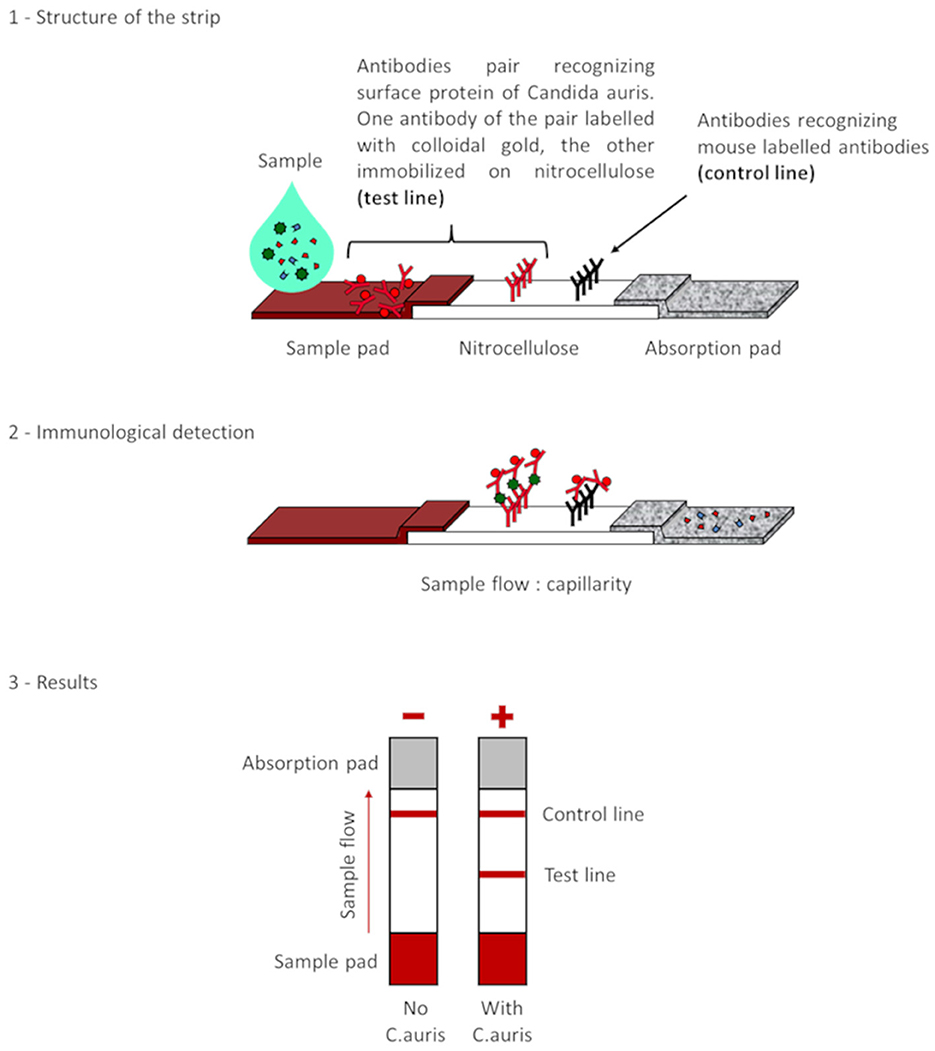
Figure 2. Principle of the lateral flow immunoassay Candida auris prototype.
2.6 Candida auris LFIA prototype validation on enrichment broth
The LFIA prototype was also evaluated on two different enrichment broths: SSDB manufactured by S2MediaTM (0.5% casein digest, 0.5% peptic digest of animal tissue, 2% dulcitol, 10% NaCl, 50 mg/L gentamicin and chloramphenicol) and a second prepared by adding 30 g of Sabouraud-dextrose (Beckton Dickinson), 100 g NaCl (10%) and 50 mg of chloramphenicol into 1 L of demineralized water. The solution was mixed under agitation until complete dissolution and then sterile-filtered using a 0.45 μ filter. Some of the Candida strains listed in Table 1 were then inoculated as follows. Each strain was cultured on a Sabouraud dextrose agar plate for 48–120 h at 37°C and colonies were added to sterile physiological water to reach 0.5 McFarland (equivalent to approximately ≈1–5 106 cells/mL). Then, 70 μL of this suspension was spiked into 7 mL of each of the enrichment broths. The inoculated broths were incubated at 40°C under agitation at 250 rpm for a maximum of 72 h with a visual monitoring of turbidity every 24 h. The enrichment broths were then processed as follows on the rapid test every 24 h even if no turbidity was noticed. First, 1 mL of broth was added to a microtube and centrifuged for 1 min at 10,000 g. The supernatant was discarded and the pellet was resuspended into 1 mL of PBS and centrifuged again for 1 min at 10,000 g. The supernatant was discarded and the pellet was processed by adding 150 μL of Lysis bufferTM, vortexed, with the addition of 150 μL of migration buffer after a final vortex. Finally, 100 μL of the yeast extract was transferred onto the LFIA prototype, and allowed to migrate for 15 min. The results were visually determined by monitoring the appearance of a red band on the test line, along with a band corresponding to the internal control.
3 Results
3.1 Selection of Candida auris antibodies
After fusion of NS1 and lymphocyte B cells, 104 hybridoma presenting the highest signals were selected with Format 1 (Figure 1) immunoenzymatic assay. Twenty hybridoma presenting the highest signals for Candida auris and no signal for Candida haemulonii were then selected with Format 1 and 2 (Figure 1) immunoenzymatic assays. After cloning of hybridoma cell lines by limiting dilution, 18 monoclonal antibodies were obtained and successfully purified. Of 37 pairs of antibodies performing on the LFIA format, five pairs with the best LFIA performance were selected for preliminary specificity and sensitivity testing. A final selection based on these two parameters allowed us to integrate the best pair into the LFIA prototype.
3.2 Candida auris LFIA prototype evaluation on Sabouraud dextrose, CHROMagarTM Candida +, and HardyCHROMTM Candida + auris agar plates
The specificity and sensitivity results obtained on the LFIA prototype using the selected Mabs are shown in Tables 2, 3, respectively. All the 37 Candida non-auris strains tested were found to be negative demonstrating a specificity of 100%, and all 12 Candida auris strains, covering the four main clades, were detected with a clear unambiguous signal demonstrating a sensitivity of 100%. Results between Sabouraud dextrose, CHROMagarTM Candida +, and HardyCHROMTM Candida + auris agar plates were concordant in terms of sensitivity and specificity. However, a slightly decreased signal was noted on the rapid test for both chromogenic medias, compared to the standard Sabouraud dextrose agar plate.

Table 2. Specificity results with various Candida non-auris isolates grown on Sabouraud, CHROMagarTM Candida + and HardyCHROMTM Candida + auris agar plates with the lateral flow immunoassay prototype using the best selected antibody pair.
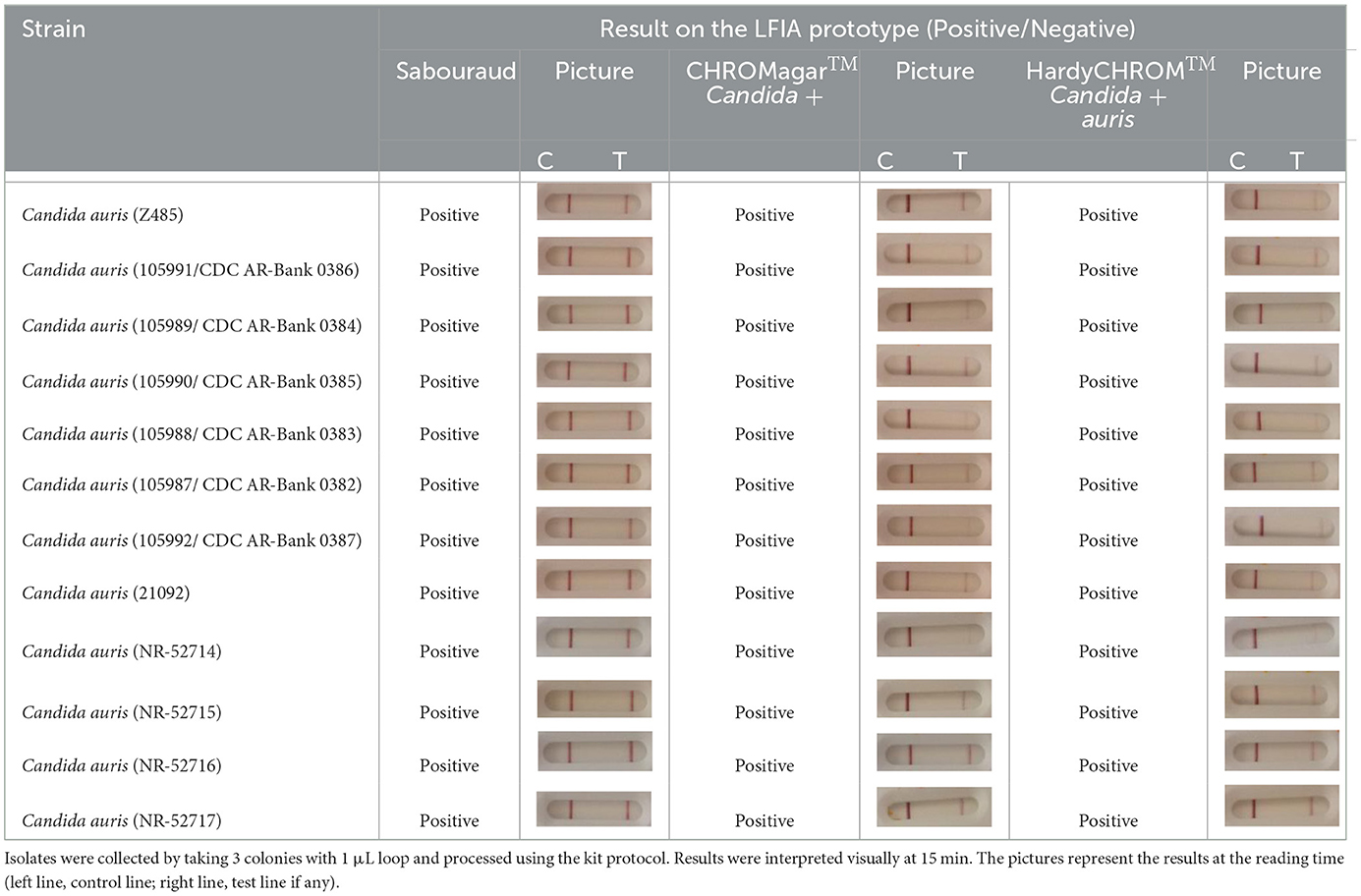
Table 3. Sensitivity results with various Candida auris isolates grown on Sabouraud, CHROMagarTM Candida + or HardyCHROMTM Candida + auris agar plates with the lateral flow immunoassay prototype using the best selected antibody pair.
3.3 Candida auris LFIA prototype evaluation on enrichment broth
Most of the Candida non-auris strains did not grow in the broths used, with the exception of Candida guilliermondii, Candida glabrata, Candida duobushaemulonii and/or Candida parapsilosis. In contrast, all Candida auris strains grew in both media. However, significant differences were seen between the two broths. The Candida auris strains grew more quickly on the dextrose-based broth with 83.3% (Table 4) culture positive compared to 41.7% (Table 5) culture positive with SSDB after 24 h incubation. With both broths, 100% culture positive was reached after 48 h incubation. When cultured on dextrose-based media, all Candida auris species found positive at 48 h were also found positive on the rapid test at 24 h. However, with SSDB, none of the Candida auris species found positive from culture at 48 h were positive on the rapid test, which may be explained by the weak turbidity obtained at 24 h.
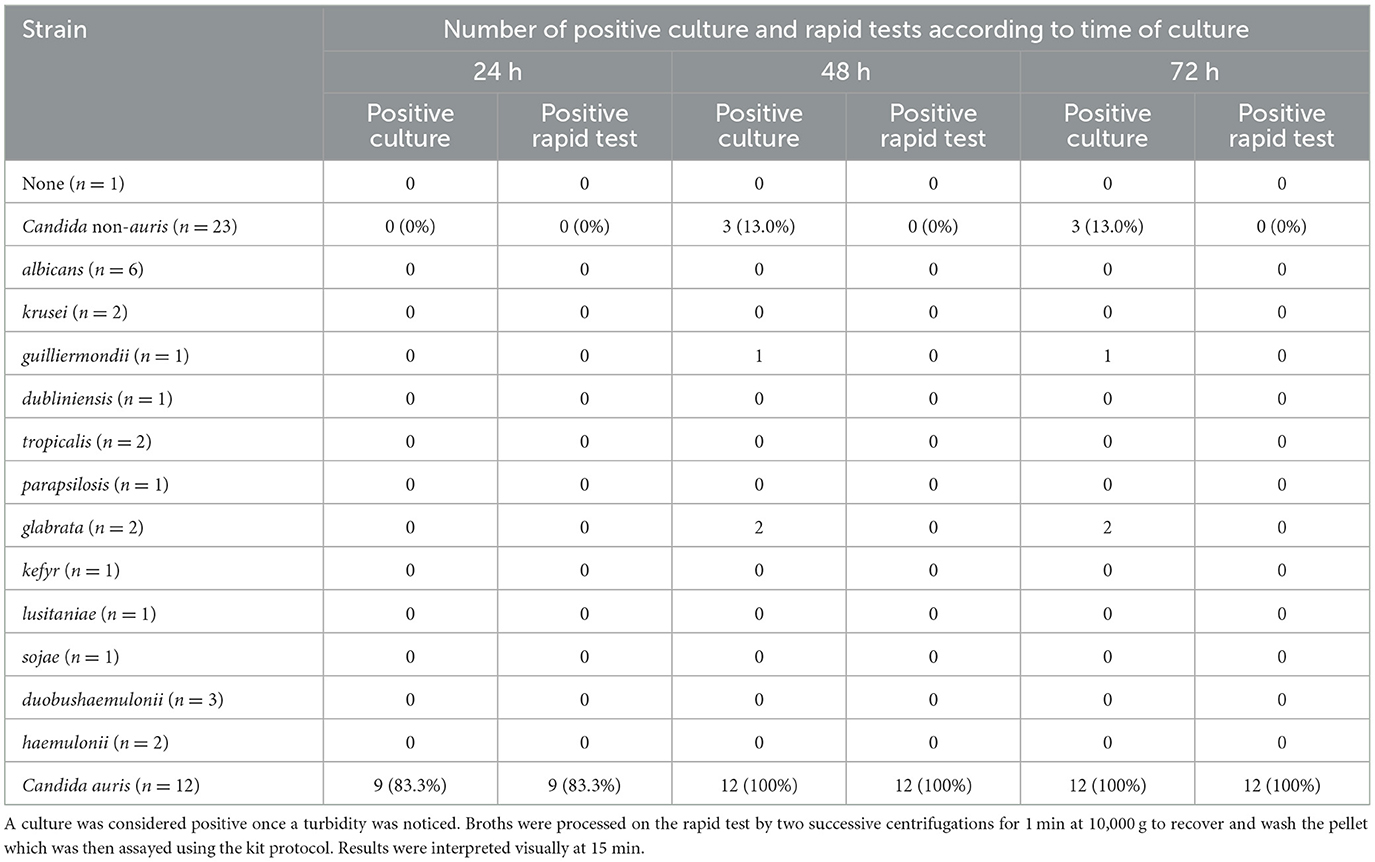
Table 4. Number of positive culture and rapid tests from various Candida auris and non-auris isolates grown on dextrose-sabouraud enrichment broth containing 10% NaCl and 50 mg/L chloramphenicol at 40°C for up to 72 h.
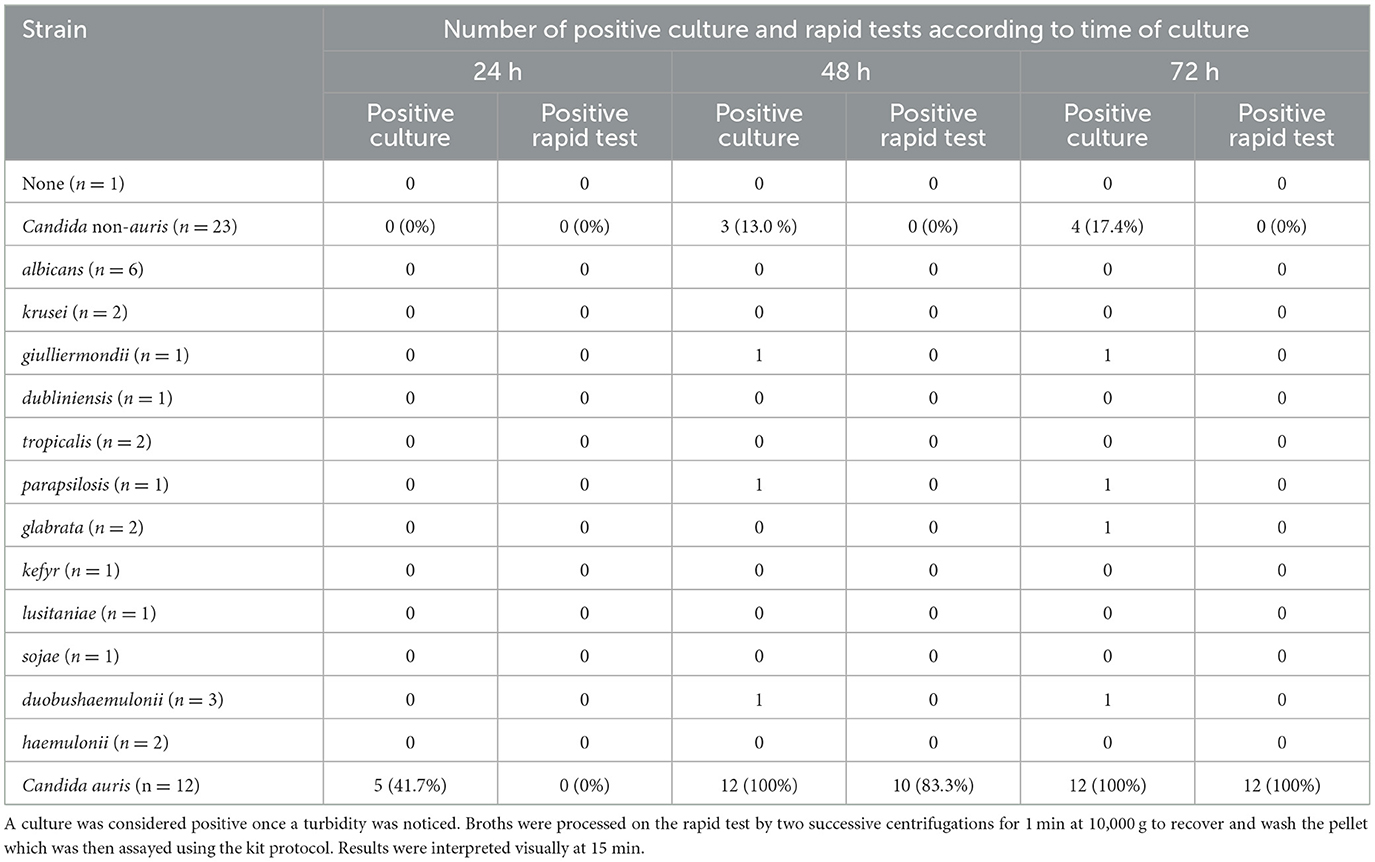
Table 5. Number of positive culture and rapid tests from various Candida auris and non-auris isolates grown on Salt Sabouraud Dulcitol Broth (SSDB) containing 50 mg/L chloramphenicol and gentamicin at 40°C for up to 72 h.
4 Discussion
The aims of this study were 2-fold: (i) to obtain highly specific Mabs for Candida auris surface proteins; and (ii) to design and validate the performance of a LFIA prototype for rapid identification of Candida auris from colonies grown on agar plates or directly from enrichment broth. Among 104 pre-selected hybridoma, selection of the best antibody pair for use in the LFIA prototype achieved high identification accuracy. Indeed, this rapid test was able to detect 100% of the 12 Candida auris strains tested, covering the four mains clades, as well as being 100% specific for 37 other Candida species, including those most encountered in clinical settings (Yapar, 2014). All results were concordant when the strains were grown on a regular sabouraud-dextrose agar plate or on CHROMagarTM Candida Plus and HardyCHROMTM Candida + auris media, although a slightly reduced signal was noted with the rapid test on the chromogenic media. Furthermore, the LFIA prototype was able to detect all the Candida auris strains directly from turbid enrichment broths using a simple protocol for yeast concentration by centrifugation with excellent accuracy. In our study, the use of SSDB did not provide any advantages over a dextrose-based broth with chloramphenicol and salt. In both cases, some Candida non-auris species were still able to grow (Candida glabrata, Candida guilliermondii, Candida duobushaemulonii, and/or Candida parapsilosis) indicating that the SSDB was not more selective. On the contrary, the use of SSDB resulted in a growth decrease for some Candida auris strains, lengthening the time to result.
Although this LFIA prototype shows very promising results, further data are required such as determining its ability to detect the fifth clade of Candida auris that has recently emerged (Chow et al., 2019), as well as the specificity of the antibodies against other rare Candida species or microorganisms such as Candida famata, which can be misidentified with other methods (Keighley et al., 2021).
Mycological culture remains central to the diagnostic approach with Candida auris. However, most of the commercially available agar plates are unable to differentiate Candida auris from other species (Keighley et al., 2021). Nonetheless, a recent study showed that CHROMagarTM Candida Plus could accurately distinguish Candida auris from other species, but the ambiguous colors sometimes found with chromogenic media can lead to uncertainty regarding the identification (Borman et al., 2021; Mulet Bayona et al., 2022). Furthermore, false positive results have been seen with Candida pseudohaemulonii and Candida vulturna (de Jong et al., 2021). Consequently, a confirmatory test is always required.
Non-culture-based methods, such as phenotypic and biochemical identification, show many limitations when differentiating Candida auris from other species (Keighley et al., 2021). However, matrix-assisted laser desorption ionization time-of-flight (MALDI-TOF) mass spectrometry has proven to be accurate and reliable at identifying Candida auris species as well as characterizing the antifungal susceptibility profile (Keighley et al., 2021; Abdolrasouli and Fraser, 2022). Although the time to results is short and the cost of analysis is affordable (Dhiman et al., 2011), this assay still requires an expensive analyzer and trained technicians thus limiting broad availability of the method. Molecular amplification-based methods, such as Polymerase Chain Reaction (PCR) or Loop-Mediated Amplification Method (LAMP), are also powerful tools and accurate for Candida auris identification (Yamamoto et al., 2018; Alvarado et al., 2021; Mulet Bayona et al., 2021; Zhang et al., 2023). However, commercially available kits are mainly used in positive blood cultures or other direct samples considering their high cost (Lockhart et al., 2022). Finally, DNA sequencing is also a powerful tool for Candida auris identification, but is complex and expensive and consequently not available in most clinical microbiology laboratories (Lockhart et al., 2022). In the past decade, LFIA rapid tests have emerged as important and reliable tools in the field of clinical microbiology, particularly in the detection of AMR (Boutal et al., 2022). The newly-developed LFIA prototype overcomes many limitations of currently available methods for Candida auris identification and is affordable, does not require expensive equipment, is easy to use, can be stored long term at room temperature, and provides an unambiguous interpretation. This will allow its broad use in clinical laboratories in low as well as high income countries. In addition, the ability to provide an identification directly from a turbid enrichment broth reduces the time to final identification by around 48 h compared with surveillance samples enrichment followed by isolation on solid media. This allow to save precious time when it comes to patient isolation to limit the spread of Candida auris in hospital settings.
5 Conclusion
In conclusion, we have developed a new LFIA prototype for the rapid identification of Candida auris on isolates grown on agar plates or directly from positive enrichment broths used in surveillance. We anticipate that this powerful new tool will help fight the dissemination of the emerging threat of Candida auris in clinical settings. The strength of our study is that the LFIA prototype reached 100% specificity and sensitivity on a highly diverse and clinically relevant Candida auris and Candida non-auris panel, including species often falsely mixed-up with Candida auris. The weakness of our study is that the LFIA prototype was evaluated on a relatively low number of strains and the detection from enrichment broth performed on contrived specimens only. Therefore, validation of the LFIA prototype in clinical setting represents the next step.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Author contributions
AC: Writing – original draft, Validation, Investigation, Funding acquisition, Conceptualization. AA: Writing – original draft, Validation, Investigation, Conceptualization. A-SH: Writing – original draft, Methodology, Investigation. MP: Writing – original draft, Methodology, Investigation. LN: Writing – original draft, Methodology, Investigation. SS: Writing – original draft, Supervision, Funding acquisition. HV: Funding acquisition, Writing – review & editing, Supervision, Project administration.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This study was founded by the French government through France 2030 program.
Acknowledgments
We would like to thank Hardy Diagnostics for donating HardyCHROMTM Candida + auris agar plate.
Conflict of interest
AC, A-SH, and LN are employees of NG Biotech company which plans to market the test described in this manuscript.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
AMR, Antimicrobial resistance; CDC, Center for disease control; DNA, Deoxyribonucleic acid; EIA, Enzyme immunoassay; G4, Acetylcholinesterase; ICU, Intensive care unit; LAMP, Loop-mediated amplification method; LFIA, Lateral flow immunoassay; Mabs, Monoclonal antibodies; MALDI TOF, Matrix-assisted laser desorption ionization time-of-flight; PCR, Polymerase chain reaction; SSDB, Salt-sabouraud dulcitol broth.
References
Abdolrasouli, A., and Fraser, M. A. (2022). Candida auris identification and profiling by MALDI-ToF mass spectrometry. Methods Mol. Biol. 2517, 21–32. doi: 10.1007/978-1-0716-2417-3_2
Alvarado, M., Bartolome Alvarez, J., Lockhart, S. R., Valentin, E., Ruiz-Gaitan, A. C., Eraso, E., et al. (2021). Identification of Candida auris and related species by multiplex PCR based on unique GPI protein-encoding genes. Mycoses 64, 194–202. doi: 10.1111/myc.13204
Azoulay, E., Dupont, H., Tabah, A., Lortholary, O., Stahl, J. P., Francais, A., et al. (2012). Systemic antifungal therapy in critically ill patients without invasive fungal infection*. Crit. Care Med. 40, 813–822. doi: 10.1097/CCM.0b013e318236f297
Borman, A. M., Fraser, M., and Johnson, E. M. (2021). CHROMagarTM Candida Plus: a novel chromogenic agar that permits the rapid identification of Candida auris. Med. Mycol. 59, 253–258. doi: 10.1093/mmy/myaa049
Boutal, H., Moguet, C., Pommies, L., Simon, S., Naas, T., Volland, H., et al. (2022). The revolution of lateral flow assay in the field of AMR detection. Diagnostics 12:1744. doi: 10.3390/diagnostics12071744
Brown, G. D., Denning, D. W., Gow, N. A., Levitz, S. M., Netea, M. G., White, T. C., et al. (2012). Hidden killers: human fungal infections. Sci. Transl. Med. 4:165rv.13. doi: 10.1126/scitranslmed.3004404
Calvo, B., Melo, A. S., Perozo-Mena, A., Hernandez, M., Francisco, E. C., Hagen, F., et al. (2016). First report of Candida auris in America: clinical and microbiological aspects of 18 episodes of candidemia. J. Infect. 73, 369–374. doi: 10.1016/j.jinf.2016.07.008
Casanova, M., and Chaffin, W. L. (1991). Cell wall glycoproteins of Candida albicans as released by different methods. J. Gen. Microbiol. 137, 1045–1051. doi: 10.1099/00221287-137-5-1045
Chakrabarti, A., Sood, P., Rudramurthy, S. M., Chen, S., Kaur, H., Capoor, M., et al. (2015). Incidence, characteristics and outcome of ICU-acquired candidemia in India. Intens. Care Med. 41, 285–295. doi: 10.1007/s00134-014-3603-2
Chow, N. A., de Groot, T., Badali, H., Abastabar, M., Chiller, T. M., Meis, J. F., et al. (2019). Potential fifth clade of Candida auris, Iran, 2018. Emerging Infect. Dis. 25, 1780–1781. doi: 10.3201/eid2509.190686
Chowdhary, A., Sharma, C., and Meis, J. F. (2017). Candida auris: a rapidly emerging cause of hospital-acquired multidrug-resistant fungal infections globally. PLoS Pathog. 13:e1006290. doi: 10.1371/journal.ppat.1006290
de Jong, A. W., Dieleman, C., Carbia, M., Mohd Tap, R., and Hagen, F. (2021). Performance of two novel chromogenic media for the identification of multidrug-resistant Candida auris compared with other commercially available formulations. J. Clin. Microbiol. 59:e03220-20. doi: 10.1128/JCM.03220-20
Dennis, E. K., Chaturvedi, S., and Chaturvedi, V. (2021). So many diagnostic tests, so little time: review and preview of Candida auris testing in clinical and public health laboratories. Front. Microbiol. 12:757835. doi: 10.3389/fmicb.2021.757835
Dhiman, N., Hall, L., Wohlfiel, S. L., Buckwalter, S. P., and Wengenack, N. L. (2011). Performance and cost analysis of matrix-assisted laser desorption ionization-time of flight mass spectrometry for routine identification of yeast. J. Clin. Microbiol. 49, 1614–1616. doi: 10.1128/JCM.02381-10
Drgona, L., Khachatryan, A., Stephens, J., Charbonneau, C., Kantecki, M., Haider, S., et al. (2014). Clinical and economic burden of invasive fungal diseases in Europe: focus on pre-emptive and empirical treatment of Aspergillus and Candida species. Eur. J. Clin. Microbiol. Infect. Dis. 33, 7–21. doi: 10.1007/s10096-013-1944-3
Eckbo, E. J., Wong, T., Bharat, A., Cameron-Lane, M., Hoang, L., Dawar, M., et al. (2021). First reported outbreak of the emerging pathogen Candida auris in Canada. Am. J. Infect. Control. 49, 804–807. doi: 10.1016/j.ajic.2021.01.013
Garey, K. W., Rege, M., Pai, M. P., Mingo, D. E., Suda, K. J., Turpin, R. S., et al. (2006). Time to initiation of fluconazole therapy impacts mortality in patients with candidemia: a multi-institutional study. Clin. Infect. Dis. 43, 25–31. doi: 10.1086/504810
Horton, M. V., Johnson, C. J., Kernien, J. F., Patel, T. D., Lam, B. C., Cheong, J. Z. A., et al. (2020). Candida auris forms high-burden biofilms in skin niche conditions and on porcine skin. mSphere 5:e00910-19. doi: 10.1128/mSphere.00910-19
Jacobs, S. E., Jacobs, J. L., Dennis, E. K., Taimur, S., Rana, M., Patel, D., et al. (2022). Candida auris pan-drug-resistant to four classes of antifungal agents. Antimicrob. Agents Chemother. 66:e0005322. doi: 10.1128/aac.00053-22
Jeffery-Smith, A., Taori, S. K., Schelenz, S., Jeffery, K., Johnson, E. M., Borman, A., et al. (2018). Candida auris: a review of the literature. Clin. Microbiol. Rev. 31. doi: 10.1128/CMR.00029-17
Keighley, C., Garnham, K., Harch, S. A. J., Robertson, M., Chaw, K., Teng, J. C., et al. (2021). Candida auris: diagnostic challenges and emerging opportunities for the clinical microbiology laboratory. Curr. Fungal Infect. Rep. 15, 116–126. doi: 10.1007/s12281-021-00420-y
Kilburn, S., Innes, G., Quinn, M., Southwick, K., Ostrowsky, B., Greenko, J. A., et al. (2022). Antifungal resistance trends of candida auris clinical isolates in New York and New Jersey from 2016 to 2020. Antimicrob. Agents Chemother. 66:e0224221. doi: 10.1128/aac.02242-21
Lockhart, S. R., Etienne, K. A., Vallabhaneni, S., Farooqi, J., Chowdhary, A., Govender, N. P., et al. (2017). Simultaneous emergence of multidrug-resistant Candida auris on 3 continents confirmed by whole-genome sequencing and epidemiological analyses. Clin. Infect. Dis. 64, 134–140. doi: 10.1093/cid/ciw691
Lockhart, S. R., Lyman, M. M., and Sexton, D. J. (2022). Tools for detecting a “superbug”: updates on Candida auris testing. J. Clin. Microbiol. 60:e0080821. doi: 10.1128/jcm.00808-21
Lone, S. A., and Ahmad, A. (2019). Candida auris-the growing menace to global health. Mycoses 62, 620–637. doi: 10.1111/myc.12904
Mulet Bayona, J. V., Salvador Garcia, C., Tormo Palop, N., and Gimeno Cardona, C. (2021). Validation and implementation of a commercial real-time PCR assay for direct detection of Candida auris from surveillance samples. Mycoses 64, 612–615. doi: 10.1111/myc.13250
Mulet Bayona, J. V., Salvador Garcia, C., Tormo Palop, N., Valentin Martin, A., Gonzalez Padron, C., Colomina Rodriguez, J., et al. (2022). Novel chromogenic medium CHROMagar(TM) Candida Plus for detection of candida auris and other Candida species from surveillance and environmental samples: a multicenter study. J. Fungi 8:281. doi: 10.3390/jof8030281
Osei Sekyere, J. (2019). Candida auris: a systematic review and meta-analysis of current updates on an emerging multidrug-resistant pathogen. Microbiologyopen 8:e00901. doi: 10.1002/mbo3.901
Pfaller, M. A., and Castanheira, M. (2016). Nosocomial candidiasis: antifungal stewardship and the importance of rapid diagnosis. Med. Mycol. 54, 1–22. doi: 10.1093/mmy/myv076
Prestel, C., Anderson, E., Forsberg, K., Lyman, M., de Perio, M. A., Kuhar, D., et al. (2021). Candida auris outbreak in a COVID-19 specialty care unit - Florida, July-August 2020. MMWR Morb. Mortal. Wkly. Rep. 70, 56–57. doi: 10.15585/mmwr.mm7002e3
Rudramurthy, S. M., Chakrabarti, A., Paul, R. A., Sood, P., Kaur, H., Capoor, M. R., et al. (2017). Candida auris candidaemia in Indian ICUs: analysis of risk factors. J. Antimicrob. Chemother. 72, 1794–1801. doi: 10.1093/jac/dkx034
Ruiz Gaitan, A. C., Moret, A., Lopez Hontangas, J. L., Molina, J. M., Aleixandre Lopez, A. I., Cabezas, A. H., et al. (2017). Nosocomial fungemia by Candida auris: first four reported cases in continental Europe. Rev. Iberoam. Micol. 34, 23–27. doi: 10.1016/j.riam.2016.11.002
Ruiz-Gaitan, A., Moret, A. M., Tasias-Pitarch, M., Aleixandre-Lopez, A. I., Martinez-Morel, H., Calabuig, E., et al. (2018). An outbreak due to Candida auris with prolonged colonisation and candidaemia in a tertiary care European hospital. Mycoses 61, 498–505. doi: 10.1111/myc.12781
Satoh, K., Makimura, K., Hasumi, Y., Nishiyama, Y., Uchida, K., Yamaguchi, H., et al. (2009). Candida auris sp. nov., a novel ascomycetous yeast isolated from the external ear canal of an inpatient in a Japanese hospital. Microbiol. Immunol. 53, 41–44. doi: 10.1111/j.1348-0421.2008.00083.x
Short, B., Brown, J., Delaney, C., Sherry, L., Williams, C., Ramage, G., et al. (2019). Candida auris exhibits resilient biofilm characteristics in vitro: implications for environmental persistence. J. Hosp. Infect. 103, 92–96. doi: 10.1016/j.jhin.2019.06.006
Thoma, R., Seneghini, M., Seiffert, S. N., Vuichard Gysin, D., Scanferla, G., Haller, S., et al. (2022). The challenge of preventing and containing outbreaks of multidrug-resistant organisms and Candida auris during the coronavirus disease 2019 pandemic: report of a carbapenem-resistant Acinetobacter baumannii outbreak and a systematic review of the literature. Antimicrob. Resist. Infect. Control. 11:12. doi: 10.1186/s13756-022-01052-8
Uppuluri, P. (2020). Candida auris biofilm colonization on skin niche conditions. mSphere 5:00972-19. doi: 10.1128/mSphere.00972-19
Villanueva-Lozano, H., Trevino-Rangel, R. J., Gonzalez, G. M., Ramirez-Elizondo, M. T., Lara-Medrano, R., Aleman-Bocanegra, M. C., et al. (2021). Outbreak of Candida auris infection in a COVID-19 hospital in Mexico. Clin Microbiol Infect. 27, 813–816. doi: 10.1016/j.cmi.2020.12.030
Welsh, R. M., Bentz, M. L., Shams, A., Houston, H., Lyons, A., Rose, L. J., et al. (2017). Survival, persistence, and isolation of the emerging multidrug-resistant pathogenic yeast Candida auris on a plastic health care surface. J. Clin. Microbiol. 55, 2996–3005. doi: 10.1128/JCM.00921-17
WHO (2022). WHO Fungal Priority Pathogens List to Guide Research, Development and Public Health Action. Geneva.
Yamamoto, M., Alshahni, M. M., Tamura, T., Satoh, K., Iguchi, S., Kikuchi, K., et al. (2018). Rapid detection of Candida auris based on loop-mediated isothermal amplification (LAMP). J. Clin. Microbiol. 56:e00591-18. doi: 10.1128/JCM.00591-18
Yapar, N. (2014). Epidemiology and risk factors for invasive candidiasis. Ther. Clin. Risk Manag. 10, 95–105. doi: 10.2147/TCRM.S40160
Keywords: Candida auris, lateral flow immunoassay, surveillance sample, identification, validation
Citation: Chalin A, Arvor A, Hervault A-S, Plaisance M, Niol L, Simon S and Volland H (2024) A lateral flow immunoassay for the rapid identification of Candida auris from isolates or directly from surveillance enrichment broths. Front. Microbiol. 15:1439273. doi: 10.3389/fmicb.2024.1439273
Received: 27 May 2024; Accepted: 17 June 2024;
Published: 03 July 2024.
Edited by:
Piet W. J. De Groot, Universidad de Castilla-La Mancha, SpainReviewed by:
Oliver Bader, University Medical Center Göttingen, GermanyMaría Alvarado, Carlos III Health Institute (ISCIII), Spain
Copyright © 2024 Chalin, Arvor, Hervault, Plaisance, Niol, Simon and Volland. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hervé Volland, aGVydmUudm9sbGFuZCYjeDAwMDQwO2NlYS5mcg==
†These authors have contributed equally to this work and share first authorship