 Yang Song
Yang Song Lei Yao
Lei Yao Junfeng Zhou
Junfeng Zhou
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Microbiol. , 10 November 2023
Sec. Virology
Volume 14 - 2023 | https://doi.org/10.3389/fmicb.2023.1294056
This article is part of the Research Topic Respiratory RNA Viruses: Molecular Mechanisms of Viral Replication and Pathogenicity View all 18 articles
The global COVID-19 pandemic has presented a significant, ongoing challenge since its emergence in late 2019. Today, the Omicron strain, which is less lethal but more contagious than the original outbreak strain, continues to pose substantial health risks. In this background, the management of psoriatic comorbidities has become even more complex, particularly for patients with underlying inflammatory, metabolic, or cardiovascular diseases. This review aims to summarize current research on comorbid COVID-19 and psoriasis, and provide insights into the development of evidence-based management strategies. By providing appropriate patient instruction, implementing protective measures, and re-evaluating medication prescriptions based on each patient’s unique situation, healthcare professionals can effectively address the challenges faced by patients with comorbid psoriasis in the COVID-19 era.
The COVID-19 outbreak caused by Severe Acute Respiratory Syndrome Coronavirus type-2 (SARS-CoV-2) has been spreading worldwide. Because of the frequent genetic mutation and recombination of SARS-CoV-2, many new variants of this coronavirus have emerged. Although less lethal than previous strains, these prevalent, mildly virulent variants (e.g. BQ and XBB subvariants of Omicron) are capable of spreading much more efficiently, and harbor an advantage in antibody evasion (Wang et al., 2023), causing less urgent, but long-lasting health problems. Patients with immunosuppressed and impaired organ functions are the most susceptible to SARS-CoV-2 infection in this post-COVID era.
Psoriasis is a common chronic inflammatory skin problem worldwide. Complete cure of this disease is considered impossible due to the complex underlying pathogenic mechanisms, which include genetic, epigenetic, environmental, and autoimmune factors (mainly induced by IL-17 and TNF-α). Long-lasting or recurrent lesions may cause discomfort that consequently lowers the quality of life of patients. Traditionally, management of psoriasis has been relatively challenging due to the lack of a single effective treatment. Approaches that include both customized combined therapy and patient education are necessary. Recently, biologics (including TNF-α inhibitors, IL-17, and IL-12/23 inhibitors) have become a revolutionary modality in the management of psoriasis based on randomized controlled trial evidence and large sample size real-world research. TNF-α inhibitors have been used to treat autoimmune disease for many years before they are introduced to psoriasis. Major adverse effects are serious infections like tuberculosis and hepatitis, along with increased risk of tumors. IL-17 and IL-23, IL-12/23 inhibitors are new biotics with a better safe profile. Overall, biotics are quick-acting, highly effective, and safe; Other small molecular agents like Janus kinase (JAK) inhibitors also have satisfactory therapeutic effect and safety, however, a maintenance treatment with biotics or JAK inhibitors is still necessary for a long-lasting relief.
Comorbidity management is another challenge for psoriasis patients, especially those with a very long course of disease, high Psoriasis Area and Severity Index (PASI) score, or resistance to treatments. Patients with psoriasis clearly have higher risks of developing cardiovascular, metabolic, and autoimmune diseases. These comorbidities can further damage the patient’s health, and bring complexity to the management of their psoriasis. Today as COVID has become a new global health challenge, it has brought greater difficulties for psoriasis patients with comorbidities. Because underlying diseases, such as inflammatory, metabolic, and cardiovascular diseases are risk factors for COVID infection and more severe disease courses.
This review summarizes the research on the comorbidity of COVID-19 and psoriasis, and aims to shed light on the current thinking around management strategies based on existing evidence.
Patients with psoriasis are more likely to develop systemic disorders, such as eye complications (sclerotitis, uveitis), gastrointestinal diseases (colitis gravis, Crohn’s disease), metabolic syndrome (hypertension, obesity, cardiovascular disease, diabetes, hyperlipidemia, hyperuricemia/gout), psoriatic arthritis (PsA), and other autoimmune diseases (vitiligo, alopecia areata). These comorbidities are collectively known as “psoriatic disease” (Aggarwal et al., 2018). Although the underlying mechanisms of these disorders in psoriasis have not been completely elucidated, they share similar triggers with psoriasis (Gisondi et al., 2020), such as genetic, environmental, and psychological factors. Additionally, the release of inflammatory cytokines, such as tumor necrosis factor TNF- α and interleukin (IL)-17 by psoriasis patients (Brembilla et al., 2018), leads to a systemically high inflammation burden that contributes to the development and exacerbation of psoriatic diseases. Research has shown that inflammation exists in many organs (e.g., aorta, liver, joints) other than skin, even in patients with mild lesions (Youn et al., 2015). In addition to the direct harm to different organs, a chain of events drives the development of psoriasis comorbidities (Figure 1). Chronic inflammation increases risks of obesity and insulin resistance (Boehncke et al., 2007), and injury to the blood vessel endothelium accelerates atherosclerotic plaque formation and lowers blood vessel elasticity. Together with conditions such as diabetes and dyslipidemia, atherosclerosis develops gradually and may eventually lead to severe cardiovascular diseases.
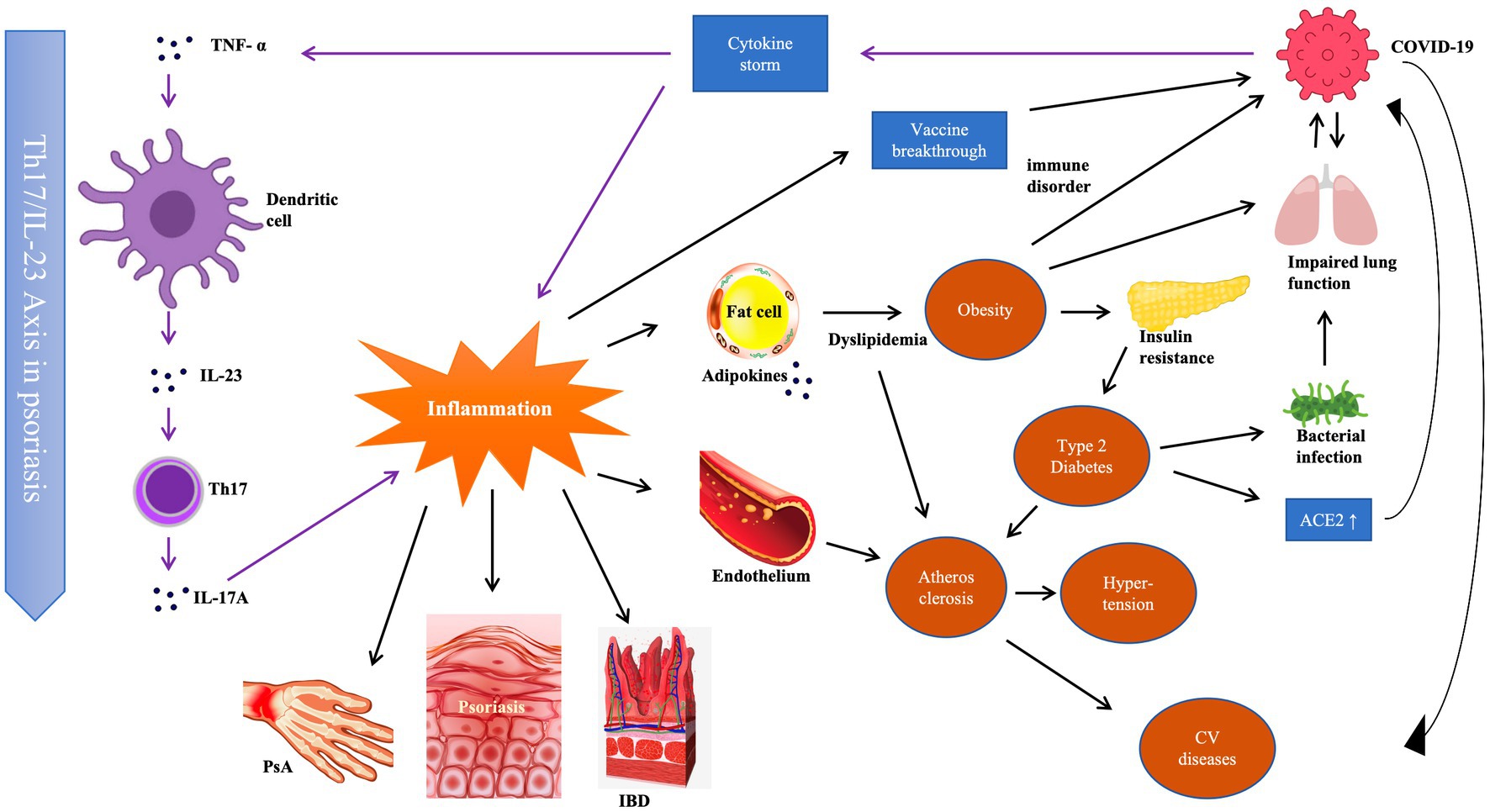
Figure 1. Immunological correlation among psoriasis, its comorbidities and COVID-19.
Conversely, these diseases can also worsen the autoimmune disorder in psoriasis, making it challenging to control lesions and prevent recurrence. Psoriatic diseases also have negative impacts on the treatment options in patients with certain comorbidities as they may be contraindications of some drugs. Considering the significant influence of comorbidity on psoriasis, guidelines, and expert consensuses recommend monitoring of psoriatic disease as an important part of psoriasis management (Elmets et al., 2019).
Today, although the risk to healthy people is greatly reduced, SARS-CoV-2 remains an imposing menace to people with underlying health conditions and older age (Espinosa et al., 2020; Gallo Marin et al., 2021).
There are controversies regarding susceptibility to COVID-19 infection of patients with cutaneous psoriasis. A large amount of research has lifted the veil of the immune response and pathogenic mechanisms of COVID-19 (Hosseini et al., 2020). The T-cell disorders of psoriasis may interfere with the anti-coronavirus immune response, which relies on CD4+ and CD8+ T-cell function (Sette and Crotty, 2021). The inflammatory status can also facilitate invasion of SARS-CoV-2 through an environmental elastase pathway. Comparative analysis of gene expression revealed that ACE2 and FURIN, which are genes significantly associated with SARS-CoV-2 infection, are upregulated in psoriasis patients, and 48 of 161 genes that are upregulated in the lungs of COVID-19 patients are also positively regulated in psoriasis (Singh et al., 2021). Surprisingly, however, some clinical studies reported that in psoriasis patients with skin involvement only, the chances of getting infected or developing a severe case were not higher than those in healthy populations. Although the underlying reasons for these contrary findings have not been well investigated, two hypotheses have been proposed: (1) genetic background may impact the development of the COVID-19-induced cytokine storm; and (2) anti-inflammation therapy to treat psoriasis may help to control the cytokine storm and/or lung fibrosis. Basic research and additional clinical studies of larger samples are needed to elucidate this issue.
Unlike the confusion in determining the role of cutaneous psoriasis in coronavirus infection, comorbidities like obesity, diabetes, and cardiovascular diseases, surely put patients at a higher risk of COVID-19 infection. Obesity, which is common among psoriasis patients suffering from metabolic syndrome, contributes to immune disorders and leads to an inhibited immune response against SARS-CoV-2 (Magdy Beshbishy et al., 2020). Obesity also damages lung function (Dixon and Peters, 2018), increasing the vulnerability to respiratory viral diseases (Green and Beck, 2017; Llamas-Velasco et al., 2021). Indeed, the increased risk of pulmonary fibrosis in patients with obesity raises the likelihood that they will develop a more severe course of COVID-19 (Steenblock et al., 2022).
Diabetes, like cutaneous psoriasis, does not appear to increase the risk of SARS-CoV-2 infection (Albulescu et al., 2020); however, it is a risk factor for severe COVID-19 disease and death. ACE2 is also upregulated in patients with type 2 diabetes (Gutta et al., 2018), which may exacerbate the damage to alveolar epithelial cells (Albulescu et al., 2020) and lead to a rapidly progressing course of COVID-19. Furthermore, the increased risk of acquiring bacterial infections among patients with high blood sugar levels, and the chronic inflammation status and high platelet reactivity of patients with diabetes (Demirtunc et al., 2009; Maiocchi et al., 2018), put these individuals at higher risks of developing severe COVID-19 disease or death.
Pre-existing cardiovascular diseases are associated with higher rates of severity and morbimortality from COVID-19 and, among patients requiring hospitalization, hypertension is the most common concomitant cardiovascular condition (Richardson et al., 2020; Zheng et al., 2020). Acute myocardial infarction and heart failure are also correlated with SARS-CoV-2 infection. The cellular damage to blood vessel epithelium by the chronic inflammatory status in psoriasis patients leads to a higher rate of hypertension and accelerated atherosclerotic plaque formation (Lowes et al., 2014; Boehncke, 2018). The hypercoagulative state of psoriasis patients especially after COVID-19 infection also raises the possibility of thrombogenesis, which may have life-threatening consequences in patients with cytokine storm or impaired lung function.
Another possible explanation for why patients with these comorbidities are at high risk during COVID-19 is that the damaged immune system leads to vaccine breakthrough (Hanckova and Betakova, 2021; Juthani et al., 2021).
After the acute phase of COVID-19, some patients develop long-term health problems, which are also called “long COVID” (Lai et al., 2023), and include fatigue, chest tightness, anxiety, and other specific presentations if other organs are involved (Desai et al., 2022). Psoriasis patients are also vulnerable.
A common feature of the complex relationships encompassing psoriasis, its related comorbidities, and coronavirus infection, is inflammation. As stated above, psoriasis patients with comorbidities usually exhibit a more severe inflammatory status driven by IL-17 and TNF-α. SARS-CoV-2 infection can trigger an adaptive immune response in which fluctuations in immune function may cause onset, worsening, or recurrence of psoriasis (Zahedi Niaki et al., 2020; Silva Andrade et al., 2021). The COVID-19 induced IL-17 immune response (Queiroz et al., 2022) and TNF-α release (Vianello et al., 2022; Davis et al., 2023) can worsen psoriasis and its comorbidities. Therefore, patients with psoriasis comorbidities are more likely to be negatively impacted by post-COVID-19 effects.
Besides COVID-19 infection, dermatologists, and patients alike should be made aware that the COVID-19 vaccination itself may also induce or exacerbate psoriasis (Potestio et al., 2023).
Seasonal reinfection of SARS-CoV-2 variants has become a health problem that seems to be unavoidable. Proper patient education is necessary to help psoriasis patients with comorbidities experience increased quality of life, lower the frequency of recurrence, and control systemic complications. Patients should avoid factors that may further suppress immune function and adopt protective measures, such as mask-wearing. Upon noticing signs of COVID-19 infection, patients should quickly seek a diagnosis and early active treatment because prolonged infection may increase inflammatory damage. Prescriptions for patients with comorbidities should also be re-evaluated during the COVID-19 era. Below, we highlight treatment recommendations in specific patient comorbidity groups in the COVID era (Table 1).
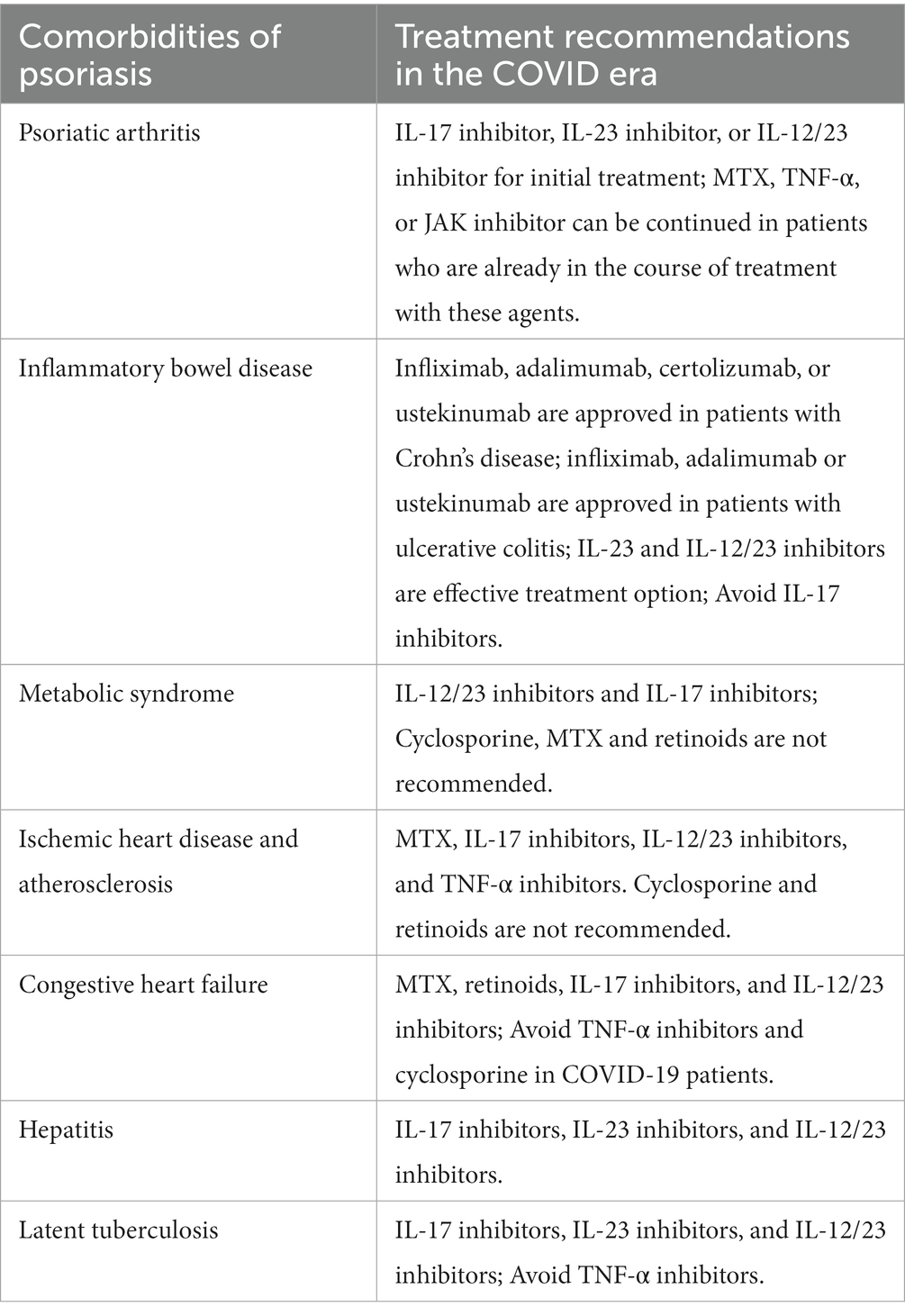
Table 1. Common comorbidities of psoriasis and the recommended treatment options in the COVID era.
For patients with moderate-to-severe PsA, early use of MTX is recommended to prevent disease progression and joint destruction (Michelsen et al., 2023). Despite the suggestion by some studies that MTX administered within 2 weeks after vaccination may affect the vaccine response (Arnold et al., 2021), there is no evidence of an increased risk of COVID-19 in patients receiving MTX therapy. It is recommended to continue this medication during COVID-19 (Sadeghinia and Daneshpazhooh, 2021). For active unilateral or oligo-arthritis and enthesitis, local injection of corticosteroid is an option.
When peripheral joint disease cannot be controlled, or when the axial joints are involved, biologic treatment is recommended. The US Food and Drug Administration has approved five TNF-α inhibitors (etanercept, adalimumab, infliximab, pexelizumab, golimumab), two IL-17A inhibitors (secukinumab, ixekizumab), and one IL-12/23 inhibitor (ustekinumab) for the treatment of PsA. Previous guidelines prioritized TNF-α inhibitors, but recent studies suggest that the adoption of a TNF-α inhibitor should no longer be mandatory because ustekinumab and IL-17A antibodies may be equally effective (Sadeghinia and Daneshpazhooh, 2021). The risk of COVID-19 infection in psoriasis patients receiving TNF-α, IL-17, IL-12, and IL-23 inhibitors was also investigated in different cohort studies, systematic evaluations, and meta-analyses. The effects of TNF-α inhibitors on COVID-19 infection remain controversial. Some studies showed a higher risk of infection with TNF-α inhibitor therapy, whereas others showed no significant differences (Dommasch et al., 2019; Jin et al., 2022; Schneeweiss et al., 2023). For instance, In a study on psoriasis patients, the use of TNF-α inhibitors increased overall infection and upper respiratory tract infection by up to 7% compared with placebo, higher than the rates with IL-17 and IL-12/23 inhibitors (Lebwohl et al., 2020).
In studies of JAK inhibitors, ruxolitinib, and baricitinib were found to contribute to a hyperinflammatory state in critical COVID-19 patients, but simultaneously inhibited the receptor-mediated endocytosis of SARS-CoV-2 viral particles, thereby exhibiting antiviral potential (Zahedi Niaki et al., 2020). Currently, there is insufficient evidence of harm or benefit of JAK inhibition therapy in patients with SARS-CoV-2 infection.
For PsA patients with skin involvement, IL-17A, IL-23, or IL-12/23 inhibitors are recommended. For patients with inflammatory bowel disease (IBD), TNF-α, IL-12/23, IL-23, or JAK inhibitors are recommended (Michelsen et al., 2023). For patients with PsA infected with COVID-19, the initial biologic treatment should be one of the safer agents, such as an IL-17, IL-23, or IL-12/23 inhibitor. Among patients already under TNF-α or JAK inhibitor therapy, the treatment can be continued during COVID-19 infection (Sadeghinia and Daneshpazhooh, 2021).
Approved targeted therapies are preferred for patients with psoriasis and active IBD or history of IBD. Infliximab, adalimumab, pexelizumab, and ustekinumab were approved for the treatment of Crohn’s disease, and infliximab, adalimumab, and upadacitinibi for the treatment of ulcerative colitis. Notably, etanercept failed in clinical trials in patients with Crohn’s disease. There is a warning in the prescribing information for IL-17A antibodies for patients with IBD, and active Crohn’s disease is a contraindication to the use of the IL-17 antibody brodalumab (Whitlock et al., 2018). The IL-23 inhibitors guselkumab and risankizumab and the JAK inhibitor upadacitinib have shown good efficacy in Crohn’s disease and ulcerative colitis, with prolonged efficacy and safety (Barberio et al., 2023; Friedberg et al., 2023). Studies also showed efficacy of guselkumab in controlling intestinal inflammation (Higashiyama and Hokaria, 2023).
One study reported an increase of up to 9% in the overall infection rate and a slight increase in the upper respiratory tract infection rate in users of IL-23 blockers (Lebwohl et al., 2020). However, other research did not detect a difference in infection risk among users of TNF-α, IL-17, or IL-12/23 inhibitors in psoriasis or PsA (Li et al., 2020). Additional randomized controlled trials showed that the risk of upper respiratory tract infection in users of IL-23 inhibitors was similar to that with placebo (Brownstone et al., 2020). Today, in the post-pandemic era, IL-12/23 inhibitors are associated with a lower risk of infection, enabling a favorable outcome after COVID-19; thus, it is recommended to initiate or continue their application in psoriasis patients with IBD (Machado et al., 2023).
MTX should be used with caution in patients with diabetes, obesity, and non-alcoholic fatty liver disease because the risk of liver fibrosis increases when the cumulative dose exceeds 1.5 g (Singh et al., 2019). Cyclosporine can increase insulin resistance, and interfere with fatty acid metabolism, thereby leading to dyslipidemia and elevated serum uric acid (Gisondi et al., 2013). Furthermore, a Danish cohort study found that patients receiving cyclosporin had a significantly increased risk of hospitalization for COVID-19 (Galvez-Romero et al., 2021), suggesting caution when administering cyclosporin in patients with metabolic syndrome.
About obesity and biologics, Studies have shown that weight gain may occur in patients treated with TNF-α inhibitors. In contrast, ustekinumab and IL-17 inhibitors generally do not increase body weight (Onsun et al., 2022).
Regarding diabetes and biotics, studies of patients receiving TNF-α antagonists had a lower risk of new diabetes compared with those receiving other drugs, with an adjusted diabetes risk ratio of 0.62 (95%CI: 0.42–0.91) (Solomon et al., 2011). Other studies have found that patients with underlying diabetes or metabolic syndrome receiving anti-TNF-α therapy exhibit improved insulin resistance (Dal Bello et al., 2020). A phase III randomized controlled trial of secukinumab showed that patients on the drug had a trend of lower fasting glucose level compared with placebo during the first 12 weeks (Gerdes et al., 2020).
For COVID-19 patients with psoriasis, IL-17 inhibitors have demonstrated good efficacy and safety. In psoriasis, the incidences of upper respiratory tract infections were comparable in patients treated with IL-17 inhibitors and placebo (Langley et al., 2019). IL-17 may have a pathogenic role in the acute respiratory distress syndrome and lung inflammation associated with severe COVID-19. COVID-19 patients with pulmonary complications have increased populations and activation of Th17 cells. Th17 pathway blockers can downregulate the abnormal immune response of COVID-19 and reduce mortality (Bashyam and Feldman, 2020; Machado et al., 2023).
Systemic retinoids increase the levels of serum triglycerides and cholesterol by transforming high-density lipoprotein to low-density lipoprotein, which contributes to elevated risk of coronary heart disease (Balak et al., 2020). Similarly, cyclosporin can induce or aggravate arterial hypertension (in a dose-dependent manner), aggravate dyslipidemia, and raise blood glucose levels. Cyclosporine may interfere with drugs used in patients with ischemic heart disease, such as beta-blockers, calcium antagonists, fibrates and most statins (Berth-Jones et al., 2019). By contrast, MTX improved arteriosclerosis and reduced the carotid intima-media thickness in patients with moderate-to-severe psoriasis (Martinez-Lopez et al., 2018). MTX was also found to reduce risks of cardiovascular morbidity and mortality compared with cyclosporine and retinoids (Roubille et al., 2015; Tsai et al., 2021).
Treatment with TNF-α monoclonal antibodies and ustekinumab has been shown to reduce aortic vascular inflammation and systemic inflammatory biomarkers (Eder et al., 2018; Gelfand et al., 2020). Furthermore, TNF-α treatment reduces intima-media thickness and arterial stiffness and consequently lower the risk of myocardial infarction (Terui and Asano, 2023) and myocardial damage (Atzeni et al., 2020). Secukinumab may exert beneficial effects on the cardiovascular system in psoriasis patients by improving endothelial function (von Stebut et al., 2019). Anti IL-23 therapy is also beneficial as IL-23 is a proatherogenic cytokine.
Overall, considering efficacy, safety, and impact on COVID infection, MTX is recommended as the preferred conventional medication for patients with psoriasis and ischemic heart disease. Anti-TNF-α antibodies, ustekinumab, and IL-17 inhibitors are suggested as preferred targeted therapies in these patients (without heart failure) in the COVID-19 era.
Cyclosporine is not recommended in patients with psoriasis and advanced congestive heart failure (CHF) because it may increase blood pressure and decrease renal function (Berth-Jones et al., 2019).
A study of patients with heart failure showed a trend of increased mortality and hospital admission rates among patients who received etanercept compared with those who received placebo (Deswal et al., 1999). Infliximab was evaluated in a randomized, double-blind, placebo-controlled phase II pilot study that showed an association between high-dose infliximab (10 mg/kg) and increased mortality and hospitalization rates in patients with heart failure (Chung et al., 2003). TNF is usually considered as a cardiotoxic factor (Kotyla, 2018), the reason why anti-TNF therapy may increase heart failure risk is still unclear.
In the COVID-19 era, expert opinion on the treatment of patients with psoriasis and heart failure with MTX, retinoids, and ustekinumab, IL-17, and IL-23 inhibitors is neutral, depending on the underlying cause of heart failure. MTX and retinoids can be recommended as treatment options for patients with psoriasis and advanced congestive heart failure. Ustekinumab, IL-17, and IL-23 inhibitors are also considered. TNF-α inhibitors, especially adalimumab and infliximab, are contraindicated in patients with congestive heart failure III/IV and should be cautioned in patients with mild congestive heart failure (New York Heart Association I/II). The use of etanercept in patients with CHF should be closely monitored (Campanati et al., 2020). In patients already infected with SARS-Cov-2, concomitant heart failure may deteriorate rapidly, it is reasonable to avoid anti-TNF therapy in all heart failure level patients who are suffering from COVID-19.
TNF-α has been associated with the risk of hepatitis B virus (HBV) reactivation and drug-induced liver injury. A multicenter study in psoriasis patients with hepatitis B or C reported the occurrence of viral reactivation, showing a higher risk with TNF-α inhibitors than with IL-17 inhibitors (Chiu et al., 2021). Three phase III randomized controlled trials (n = 3,736) confirmed the clinical efficacy of ixekizumab in treating patients with psoriasis, and reported no cases of hepatitis B reactivation as of Week 60 (Gordon et al., 2016). A study of 30 patients with chronic inactive HBV infection who were treated with secukinumab indicated that this drug did not increase the risk of hepatitis during treatment (Qin et al., 2022). In a prospective cohort study of ustekinumab in patients with psoriasis (n = 93), the reactivation rate among HBV carriers was 17.4% without prophylaxis (Ting et al., 2018). IL-17 and IL-23 inhibitors, as well as ustekinumab were recommended as preferred systemic treatments for this patient group (Nast et al., 2021).
There are few data on the risk of TB reactivation with retinoids, cyclosporine, and MTX. To date, most published guidelines do not recommend TB screening for these drugs. However, the World Health Organization has issued black box warnings about the risk of TB and other serious infections with TNF-α inhibitors. Furthermore, a review suggested that patients with latent TB who received TNF-α had an approximately two to four-fold increased risk of active TB (Baddley et al., 2018). The mechanism maybe related to the effects of anti-TNF-α therapy on cellular interactions in a latent TB granuloma (Robert and Miossec, 2021). Patients receiving IL-17 as well as IL23 inhibitors had the lowest risk of activating latent TB than other previously approved drugs including TNF-α inhibitors and IL12/23 inhibitors (Nogueira et al., 2021).
The interplay between comorbid COVID-19 and psoriasis presents a compounding challenge for the management of both conditions. Despite the decreased virulence of the prevalent SARS-CoV-2 strains, small seasonal waves of infection continue to cause severe illness, especially among vulnerable populations. Psoriasis patients with comorbidities are particularly at risk. To effectively manage comorbidities in psoriasis patients during the COVID-19 era, it is essential to provide patients with properly individualized therapeutic modalities that improve their quality of life, reduce recurrence rates, and control systemic complications.
YS: Funding acquisition, Writing – original draft, Writing – review & editing. LY: Validation, Writing – review & editing. SL: Methodology, Resources, Writing – review & editing. JZ: Funding acquisition, Writing-original draft, Writing-review & editing, Project administration.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was funded by the Natural Science Foundation of Jilin Province (Project nos. YDZJ202201ZYTS030 and 20220204095YY); and by the Jilin Provincial Healthcare Talent Special Program of Jilin Province Department of Finance (Project number JLSWSRCZX2021-67).
We thank Michelle Kahmeyer-Gabbe, PhD, from Liwen Bianji (Edanz) (www.liwenbianji.cn) for editing the English text of a draft of this manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Aggarwal, D., Arumalla, N., Jethwa, H., and Abraham, S. (2018). The use of biomarkers as a tool for novel psoriatic disease drug discovery. Exp. Opin. Drug Discov. 13, 875–887. doi: 10.1080/17460441.2018.1508206
Albulescu, R., Dima, S. O., Florea, I. R., Lixandru, D., Serban, A. M., Aspritoiu, V. M., et al. (2020). COVID-19 and diabetes mellitus: unraveling the hypotheses that worsen the prognosis (review). Exp. Ther. Med. 20:194. doi: 10.3892/etm.2020.9324
Arnold, J., Winthrop, K., and Emery, P. (2021). COVID-19 vaccination and antirheumatic therapy. Rheumatology (Oxford) 60, 3496–3502. doi: 10.1093/rheumatology/keab223
Atzeni, F., Nucera, V., Galloway, J., Zoltan, S., and Nurmohamed, M. (2020). Cardiovascular risk in ankylosing spondylitis and the effect of anti-TNF drugs: a narrative review. Expert. Opin. Biol. Ther. 20, 517–524. doi: 10.1080/14712598.2020.1704727
Baddley, J. W., Cantini, F., Goletti, D., Gomez-Reino, J. J., Mylonakis, E., San-Juan, R., et al. (2018). ESCMID study Group for Infections in compromised hosts (ESGICH) consensus document on the safety of targeted and biological therapies: an infectious diseases perspective (soluble immune effector molecules [I]: anti-tumor necrosis factor-alpha agents). Clin. Microbiol. Infect. 24, S10–S20. doi: 10.1016/j.cmi.2017.12.025
Balak, D. M. W., Gerdes, S., Parodi, A., and Salgado-Boquete, L. (2020). Long-term safety of Oral systemic therapies for psoriasis: a comprehensive review of the literature. Dermatol. Ther. (Heidelb) 10, 589–613. doi: 10.1007/s13555-020-00409-4
Barberio, B., Gracie, D. J., Black, C. J., and Ford, A. C. (2023). Efficacy of biological therapies and small molecules in induction and maintenance of remission in luminal Crohn’s disease: systematic review and network meta-analysis. Gut 72, 264–274. doi: 10.1136/gutjnl-2022-328052
Bashyam, A. M., and Feldman, S. R. (2020). Should patients stop their biologic treatment during the COVID-19 pandemic. J. Dermatolog. Treat. 31, 317–318. doi: 10.1080/09546634.2020.1742438
Berth-Jones, J., Exton, L. S., Ladoyanni, E., Mohd Mustapa, M. F., Tebbs, V. M., Yesudian, P. D., et al. (2019). British Association of Dermatologists guidelines for the safe and effective prescribing of oral ciclosporin in dermatology 2018. Br. J. Dermatol. 180, 1312–1338. doi: 10.1111/bjd.17587
Boehncke, W. H. (2018). Systemic inflammation and cardiovascular comorbidity in psoriasis patients: causes and consequences. Front. Immunol. 9:579. doi: 10.3389/fimmu.2018.00579
Boehncke, S., Thaci, D., Beschmann, H., Ludwig, R. J., Ackermann, H., Badenhoop, K., et al. (2007). Psoriasis patients show signs of insulin resistance. Br. J. Dermatol. 157, 1249–1251. doi: 10.1111/j.1365-2133.2007.08190.x
Brembilla, N. C., Senra, L., and Boehncke, W. H. (2018). The IL-17 family of cytokines in psoriasis: IL-17A and beyond. Front. Immunol. 9:1682. doi: 10.3389/fimmu.2018.01682
Brownstone, N. D., Thibodeaux, Q. G., Reddy, V. D., Myers, B. A., Chan, S. Y., Bhutani, T., et al. (2020). Novel coronavirus disease (COVID-19) and biologic therapy in psoriasis: infection risk and patient counseling in uncertain times. Dermatol. Ther. 10, 339–349. doi: 10.1007/s13555-020-00377-9
Campanati, A., Diotallevi, F., Martina, E., Paolinelli, M., Radi, G., and Offidani, A. (2020). Safety update of etanercept treatment for moderate to severe plaque psoriasis. Expert Opin. Drug Saf. 19, 439–448. doi: 10.1080/14740338.2020.1740204
Chiu, H. Y., Chiu, Y. M., Chang Liao, N. F., Chi, C. C., Tsai, T. F., Hsieh, C. Y., et al. (2021). Predictors of hepatitis B and C virus reactivation in patients with psoriasis treated with biologic agents: a 9-year multicenter cohort study. J. Am. Acad. Dermatol. 85, 337–344. doi: 10.1016/j.jaad.2019.12.001
Chung, E. S., Packer, M., Lo, K. H., Fasanmade, A. A., Willerson, J. T., and Anti, T. N. (2003). Randomized, double-blind, placebo-controlled, pilot trial of infliximab, a chimeric monoclonal antibody to tumor necrosis factor-alpha, in patients with moderate-to-severe heart failure: results of the anti-TNF therapy against congestive heart failure (ATTACH) trial. Circulation 107, 3133–3140. doi: 10.1161/01.CIR.0000077913.60364.D2
Dal Bello, G., Gisondi, P., Idolazzi, L., and Girolomoni, G. (2020). Psoriatic arthritis and diabetes mellitus: a narrative review. Rheumatol. Ther. 7, 271–285. doi: 10.1007/s40744-020-00206-7
Davis, H. E., McCorkell, L., Vogel, J. M., and Topol, E. J. (2023). Long COVID: major findings, mechanisms and recommendations. Nat. Rev. Microbiol. 21, 133–146. doi: 10.1038/s41579-022-00846-2
Demirtunc, R., Duman, D., Basar, M., Bilgi, M., Teomete, M., and Garip, T. (2009). The relationship between glycemic control and platelet activity in type 2 diabetes mellitus. J. Diabetes Complicat. 23, 89–94. doi: 10.1016/j.jdiacomp.2008.01.006
Desai, A. D., Lavelle, M., Boursiquot, B. C., and Wan, E. Y. (2022). Long-term complications of COVID-19. Am. J. Physiol. Cell Physiol. 322, C1–C11. doi: 10.1152/ajpcell.00375.2021
Deswal, A., Bozkurt, B., Seta, Y., Parilti-Eiswirth, S., Hayes, F. A., Blosch, C., et al. (1999). Safety and efficacy of a soluble P75 tumor necrosis factor receptor (Enbrel, etanercept) in patients with advanced heart failure. Circulation 99, 3224–3226. doi: 10.1161/01.cir.99.25.3224
Dixon, A. E., and Peters, U. (2018). The effect of obesity on lung function. Expert Rev. Respir. Med. 12, 755–767. doi: 10.1080/17476348.2018.1506331
Dommasch, E. D., Kim, S. C., Lee, M. P., and Gagne, J. J. (2019). Risk of serious infection in patients receiving systemic medications for the treatment of psoriasis. JAMA Dermatol. 155, 1142–1152. doi: 10.1001/jamadermatol.2019.1121
Eder, L., Joshi, A. A., Dey, A. K., Cook, R., Siegel, E. L., Gladman, D. D., et al. (2018). Association of Tumor Necrosis Factor Inhibitor Treatment with Reduced Indices of subclinical atherosclerosis in patients with psoriatic disease. Arthritis Rheumatol. 70, 408–416. doi: 10.1002/art.40366
Elmets, C. A., Leonardi, C. L., Davis, D. M. R., Gelfand, J. M., Lichten, J., Mehta, N. N., et al. (2019). Joint AAD-NPF guidelines of care for the management and treatment of psoriasis with awareness and attention to comorbidities. J. Am. Acad. Dermatol. 80, 1073–1113. doi: 10.1016/j.jaad.2018.11.058
Espinosa, O. A., Zanetti, A. D. S., Antunes, E. F., Longhi, F. G., Matos, T. A., and Battaglini, P. F. (2020). Prevalence of comorbidities in patients and mortality cases affected by SARS-CoV2: a systematic review and meta-analysis. Rev. Inst. Med. Trop. São Paulo 62:e43. doi: 10.1590/S1678-9946202062043
Friedberg, S., Choi, D., Hunold, T., Choi, N. K., Garcia, N. M., Picker, E. A., et al. (2023). Upadacitinib is effective and safe in both ulcerative colitis and Crohn’s disease: prospective Real-world experience. Clin. Gastroenterol. Hepatol. 21, 1913–1923.e2. doi: 10.1016/j.cgh.2023.03.001
Gallo Marin, B., Aghagoli, G., Lavine, K., Yang, L., Siff, E. J., Chiang, S. S., et al. (2021). Predictors of COVID-19 severity: a literature review. Rev. Med. Virol. 31, 1–10. doi: 10.1002/rmv.2146
Galvez-Romero, J. L., Palmeros-Rojas, O., Real-Ramirez, F. A., Sanchez-Romero, S., Tome-Maxil, R., Ramirez-Sandoval, M. P., et al. (2021). Cyclosporine a plus low-dose steroid treatment in COVID-19 improves clinical outcomes in patients with moderate to severe disease: a pilot study. J. Intern. Med. 289, 906–920. doi: 10.1111/joim.13223
Gelfand, J. M., Shin, D. B., Alavi, A., Torigian, D. A., Werner, T., Papadopoulos, M., et al. (2020). A phase IV, randomized, double-blind, placebo-controlled crossover study of the effects of Ustekinumab on vascular inflammation in psoriasis (the VIP-U trial). J. Invest. Dermatol. 140, 85–93.e2. doi: 10.1016/j.jid.2019.07.679
Gerdes, S., Pinter, A., Papavassilis, C., and Reinhardt, M. (2020). Effects of secukinumab on metabolic and liver parameters in plaque psoriasis patients. J. Eur. Acad. Dermatol. Venereol. 34, 533–541. doi: 10.1111/jdv.16004
Gisondi, P., Bellinato, F., Girolomoni, G., and Albanesi, C. (2020). Pathogenesis of chronic plaque psoriasis and its intersection with cardio-metabolic comorbidities. Front. Pharmacol. 11:117. doi: 10.3389/fphar.2020.00117
Gisondi, P., Cazzaniga, S., Chimenti, S., Giannetti, A., Maccarone, M., Picardo, M., et al. (2013). Metabolic abnormalities associated with initiation of systemic treatment for psoriasis: evidence from the Italian Psocare registry. J. Eur. Acad. Dermatol. Venereol. 27, e30–e41. doi: 10.1111/j.1468-3083.2012.04450.x
Gordon, K. B., Blauvelt, A., Papp, K. A., Langley, R. G., Luger, T., Ohtsuki, M., et al. (2016). Phase 3 trials of Ixekizumab in moderate-to-severe plaque psoriasis. N. Engl. J. Med. 375, 345–356. doi: 10.1056/NEJMoa1512711
Green, W. D., and Beck, M. A. (2017). Obesity impairs the adaptive immune response to influenza virus. Ann. Am. Thorac. Soc. 14, S406–S409. doi: 10.1513/AnnalsATS.201706-447AW
Gutta, S., Grobe, N., Kumbaji, M., Osman, H., Saklayen, M., Li, G., et al. (2018). Increased urinary angiotensin converting enzyme 2 and neprilysin in patients with type 2 diabetes. Am. J. Physiol. Renal Physiol. 315, F263–F274. doi: 10.1152/ajprenal.00565.2017
Hanckova, M., and Betakova, T. (2021). Pandemics of the 21st century: the risk factor for obese people. Viruses 14:25. doi: 10.3390/v14010025
Higashiyama, M., and Hokaria, R. (2023). New and emerging treatments for inflammatory bowel disease. Digestion 104, 74–81. doi: 10.1159/000527422
Hosseini, A., Hashemi, V., Shomali, N., Asghari, F., Gharibi, T., Akbari, M., et al. (2020). Innate and adaptive immune responses against coronavirus. Biomed. Pharmacother. 132:110859. doi: 10.1016/j.biopha.2020.110859
Jin, Y., Lee, H., Lee, M. P., Landon, J. E., Merola, J. F., Desai, R. J., et al. (2022). Risk of hospitalization for serious infection after initiation of Ustekinumab or other biologics in patients with psoriasis or psoriatic arthritis. Arthritis Care Res. (Hoboken) 74, 1792–1805. doi: 10.1002/acr.24630
Juthani, P. V., Gupta, A., Borges, K. A., Price, C. C., Lee, A. I., Won, C. H., et al. (2021). Hospitalisation among vaccine breakthrough COVID-19 infections. Lancet Infect. Dis. 21, 1485–1486. doi: 10.1016/S1473-3099(21)00558-2
Kotyla, P. J. (2018). Bimodal function of Anti-TNF treatment: shall we be concerned about Anti-TNF treatment in patients with rheumatoid arthritis and heart failure? Int. J. Mol. Sci. 19:1739. doi: 10.3390/ijms19061739
Lai, C. C., Hsu, C. K., Yen, M. Y., Lee, P. I., Ko, W. C., and Hsueh, P. R. (2023). Long COVID: an inevitable sequela of SARS-CoV-2 infection. J. Microbiol. Immunol. Infect. 56, 1–9. doi: 10.1016/j.jmii.2022.10.003
Langley, R. G., Kimball, A. B., Nak, H., Xu, W., Pangallo, B., Osuntokun, O. O., et al. (2019). Long-term safety profile of ixekizumab in patients with moderate-to-severe plaque psoriasis: an integrated analysis from 11 clinical trials. J. Eur. Acad. Dermatol. Venereol. 33, 333–339. doi: 10.1111/jdv.15242
Lebwohl, M., Rivera-Oyola, R., and Murrell, D. F. (2020). Should biologics for psoriasis be interrupted in the era of COVID-19? J. Am. Acad. Dermatol. 82, 1217–1218. doi: 10.1016/j.jaad.2020.03.031
Li, X., Andersen, K. M., Chang, H. Y., Curtis, J. R., and Alexander, G. C. (2020). Comparative risk of serious infections among real-world users of biologics for psoriasis or psoriatic arthritis. Ann. Rheum. Dis. 79, 285–291. doi: 10.1136/annrheumdis-2019-216102
Llamas-Velasco, M., Ovejero-Merino, E., and Salgado-Boquete, L. (2021). Obesity - a risk factor for psoriasis and COVID-19. Actas Dermosifiliogr. 112, 489–494. doi: 10.1016/j.ad.2020.12.001
Lowes, M. A., Suarez-Farinas, M., and Krueger, J. G. (2014). Immunology of psoriasis. Annu. Rev. Immunol. 32, 227–255. doi: 10.1146/annurev-immunol-032713-120225
Machado, P. M., Schafer, M., Mahil, S. K., Liew, J., Gossec, L., Dand, N., et al. (2023). Characteristics associated with poor COVID-19 outcomes in people with psoriasis, psoriatic arthritis and axial spondyloarthritis: data from the COVID-19 PsoProtect and global rheumatology Alliance physician-reported registries. Ann. Rheum. Dis. 82, 698–709. doi: 10.1136/ard-2022-223499
Magdy Beshbishy, A., Hetta, H. F., Hussein, D. E., Saati, A. A., C Uba, C., Rivero-Perez, N., et al. (2020). Factors associated with increased morbidity and mortality of obese and overweight COVID-19 patients. Biology (Basel) 9:280. doi: 10.3390/biology9090280
Maiocchi, S., Alwis, I., Wu, M. C. L., Yuan, Y., and Jackson, S. P. (2018). Thromboinflammatory functions of platelets in ischemia-reperfusion injury and its dysregulation in diabetes. Semin. Thromb. Hemost. 44, 102–113. doi: 10.1055/s-0037-1613694
Martinez-Lopez, A., Blasco-Morente, G., Perez-Lopez, I., Tercedor-Sanchez, J., and Arias-Santiago, S. (2018). Studying the effect of systemic and biological drugs on intima-media thickness in patients suffering from moderate and severe psoriasis. J. Eur. Acad. Dermatol. Venereol. 32, 1492–1498. doi: 10.1111/jdv.14841
Michelsen, B., Ostergaard, M., Nissen, M. J., Ciurea, A., Moller, B., Ornbjerg, L. M., et al. (2023). Differences and similarities between the EULAR/ASAS-EULAR and national recommendations for treatment of patients with psoriatic arthritis and axial spondyloarthritis across Europe. Lancet Reg. Health Eur. 33:100706. doi: 10.1016/j.lanepe.2023.100706
Nast, A., Smith, C., Spuls, P. I., Avila Valle, G., Bata-Csorgo, Z., Boonen, H., et al. (2021). EuroGuiDerm guideline on the systemic treatment of psoriasis vulgaris - part 2: specific clinical and comorbid situations. J. Eur. Acad. Dermatol. Venereol. 35, 281–317. doi: 10.1111/jdv.16926
Nogueira, M., Warren, R. B., and Torres, T. (2021). Risk of tuberculosis reactivation with interleukin (IL)-17 and IL-23 inhibitors in psoriasis - time for a paradigm change. J. Eur. Acad. Dermatol. Venereol. 35, 824–834. doi: 10.1111/jdv.16866
Onsun, N., Akaslan, T. C., Sallahoglu, K., Gulcan, A. S., Bulut, H., and Yabaci, A. (2022). Effects of TNF inhibitors and an IL12/23 inhibitor on changes in body weight and adipokine levels in psoriasis patients: a 48-week comparative study. J. Dermatolog. Treat. 33, 1727–1732. doi: 10.1080/09546634.2021.1901845
Potestio, L., Battista, T., Cacciapuoti, S., Ruggiero, A., Martora, F., Fornaro, L., et al. (2023). New onset and exacerbation of psoriasis following COVID-19 vaccination: a review of the current knowledge. Biomedicine 11:2191. doi: 10.3390/biomedicines11082191
Qin, H., Liu, N., Hu, Y., Yu, N., Yi, X., Gao, Y., et al. (2022). Safety and efficacy of secukinumab in psoriasis patients infected with hepatitis B virus: a retrospective study. Eur. J. Dermatol. 32, 394–400. doi: 10.1684/ejd.2022.4263
Queiroz, M. A. F., Neves, P., Lima, S. S., Lopes, J. D. C., Torres, M., Vallinoto, I., et al. (2022). Cytokine profiles associated with acute COVID-19 and long COVID-19 syndrome. Front. Cell. Infect. Microbiol. 12:922422. doi: 10.3389/fcimb.2022.922422
Richardson, S., Hirsch, J. S., Narasimhan, M., Crawford, J. M., McGinn, T., Davidson, K. W., et al. (2020). Presenting characteristics, comorbidities, and outcomes among 5700 patients hospitalized with COVID-19 in the new York City area. JAMA 323, 2052–2059. doi: 10.1001/jama.2020.6775
Robert, M., and Miossec, P. (2021). Reactivation of latent tuberculosis with TNF inhibitors: critical role of the beta 2 chain of the IL-12 receptor. Cell. Mol. Immunol. 18, 1644–1651. doi: 10.1038/s41423-021-00694-9
Roubille, C., Richer, V., Starnino, T., McCourt, C., McFarlane, A., Fleming, P., et al. (2015). The effects of tumour necrosis factor inhibitors, methotrexate, non-steroidal anti-inflammatory drugs and corticosteroids on cardiovascular events in rheumatoid arthritis, psoriasis and psoriatic arthritis: a systematic review and meta-analysis. Ann. Rheum. Dis. 74, 480–489. doi: 10.1136/annrheumdis-2014-206624
Sadeghinia, A., and Daneshpazhooh, M. (2021). Immunosuppressive drugs for patients with psoriasis during the COVID-19 pandemic era a review. Dermatol. Ther. 34:e14498. doi: 10.1111/dth.14498
Schneeweiss, M. C., Savage, T. J., Wyss, R., Jin, Y., Schoder, K., Merola, J. F., et al. (2023). Risk of infection in children with psoriasis receiving treatment with Ustekinumab, Etanercept, or methotrexate before and after labeling expansion. JAMA Dermatol. 159, 289–298. doi: 10.1001/jamadermatol.2022.6325
Sette, A., and Crotty, S. (2021). Adaptive immunity to SARS-CoV-2 and COVID-19. Cells 184, 861–880. doi: 10.1016/j.cell.2021.01.007
Silva Andrade, B., Siqueira, S., de Assis Soares, W. R., de Souza Rangel, F., Santos, N. O., Dos Santos Freitas, A., et al. (2021). Long-COVID and post-COVID health complications: an up-to-date review on clinical conditions and their possible molecular mechanisms. Viruses 13:700. doi: 10.3390/v13040700
Singh, J. A., Guyatt, G., Ogdie, A., Gladman, D. D., Deal, C., Deodhar, A., et al. (2019). Special article: 2018 American College of Rheumatology/National Psoriasis Foundation guideline for the treatment of psoriatic arthritis. Arthritis Rheumatol. 71, 5–32. doi: 10.1002/art.40726
Singh, M. K., Mobeen, A., Chandra, A., Joshi, S., and Ramachandran, S. (2021). A meta-analysis of comorbidities in COVID-19: which diseases increase the susceptibility of SARS-CoV-2 infection? Comput. Biol. Med. 130:104219. doi: 10.1016/j.compbiomed.2021.104219
Solomon, D. H., Massarotti, E., Garg, R., Liu, J., Canning, C., and Schneeweiss, S. (2011). Association between disease-modifying antirheumatic drugs and diabetes risk in patients with rheumatoid arthritis and psoriasis. JAMA 305, 2525–2531. doi: 10.1001/jama.2011.878
Steenblock, C., Hassanein, M., Khan, E. G., Yaman, M., Kamel, M., Barbir, M., et al. (2022). Obesity and COVID-19: what are the consequences? Horm. Metab. Res. 54, 496–502. doi: 10.1055/a-1878-9757
Terui, H., and Asano, Y. (2023). Biologics for reducing cardiovascular risk in psoriasis patients. J. Clin. Med. 12:1162. doi: 10.3390/jcm12031162
Ting, S. W., Chen, Y. C., and Huang, Y. H. (2018). Risk of hepatitis B reactivation in patients with psoriasis on Ustekinumab. Clin. Drug Investig. 38, 873–880. doi: 10.1007/s40261-018-0671-z
Tsai, M. H., Chan, T. C., Lee, M. S., and Lai, M. S. (2021). Cardiovascular risk associated with methotrexate versus Retinoids in patients with psoriasis: a Nationwide Taiwanese cohort study. Clin. Epidemiol. 13, 693–705. doi: 10.2147/CLEP.S305126
Vianello, A., Guarnieri, G., Braccioni, F., Lococo, S., Molena, B., Cecchetto, A., et al. (2022). The pathogenesis, epidemiology and biomarkers of susceptibility of pulmonary fibrosis in COVID-19 survivors. Clin. Chem. Lab. Med. 60, 307–316. doi: 10.1515/cclm-2021-1021
von Stebut, E., Reich, K., Thaci, D., Koenig, W., Pinter, A., Korber, A., et al. (2019). Impact of Secukinumab on endothelial dysfunction and other cardiovascular disease parameters in psoriasis patients over 52 weeks. J. Invest. Dermatol. 139, 1054–1062. doi: 10.1016/j.jid.2018.10.042
Wang, Q., Iketani, S., Li, Z., Liu, L., Guo, Y., Huang, Y., et al. (2023). Alarming antibody evasion properties of rising SARS-CoV-2 BQ and XBB subvariants. Cells 186, 279–286.e8. doi: 10.1016/j.cell.2022.12.018
Whitlock, S. M., Enos, C. W., Armstrong, A. W., Gottlieb, A., Langley, R. G., Lebwohl, M., et al. (2018). Management of psoriasis in patients with inflammatory bowel disease: from the medical Board of the National Psoriasis Foundation. J. Am. Acad. Dermatol. 78, 383–394. doi: 10.1016/j.jaad.2017.06.043
Youn, S. W., Kang, S. Y., Kim, S. A., Park, G. Y., and Lee, W. W. (2015). Subclinical systemic and vascular inflammation detected by (18) F-fluorodeoxyglucose positron emission tomography/computed tomography in patients with mild psoriasis. J. Dermatol. 42, 559–566. doi: 10.1111/1346-8138.12859
Zahedi Niaki, O., Anadkat, M. J., Chen, S. T., Fox, L. P., Harp, J., Micheletti, R. G., et al. (2020). Navigating immunosuppression in a pandemic: a guide for the dermatologist from the COVID task force of the medical dermatology society and Society of Dermatology Hospitalists. J. Am. Acad. Dermatol. 83, 1150–1159. doi: 10.1016/j.jaad.2020.06.051
Keywords: COVID-19, SARS-CoV-2, psoriasis, comorbidity, management, biologics
Citation: Song Y, Yao L, Li SS and Zhou JF (2023) Psoriasis comorbidity management in the COVID era: a pressing challenge. Front. Microbiol. 14:1294056. doi: 10.3389/fmicb.2023.1294056
Edited by:
Qiang Ding, Tsinghua University, ChinaReviewed by:
Leiliang Zhang, Shandong First Medical University and Shandong Academy of Medical Sciences, ChinaCopyright © 2023 Song, Yao, Li and Zhou. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Junfeng Zhou, dHR4czIxY3RAamx1LmVkdS5jbg==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.