
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
OPINION article
Front. Microbiol. , 17 April 2023
Sec. Virology
Volume 14 - 2023 | https://doi.org/10.3389/fmicb.2023.1154296
 Md. Aminul Islam1,2*
Md. Aminul Islam1,2* Fatema Hasan Kaifa2
Fatema Hasan Kaifa2 Deepak Chandran3
Deepak Chandran3 Manojit Bhattacharya4
Manojit Bhattacharya4 Chiranjib Chakraborty5
Chiranjib Chakraborty5 Prosun Bhattacharya6*
Prosun Bhattacharya6* Kuldeep Dhama7
Kuldeep Dhama7COVID-19 pandemic has caused over 6.71 million deaths out of 660 million confirmed cases as of January 12, 2023 (Rakib et al., 2021, 2022; WHO, 2022). SARS-CoV-2, the virus responsible for this worldwide pandemic is a member of the broad family of viruses known as coronaviruses (CoVs) (Islam et al., 2021, 2022a,b). It seems difficult to terminate the present pandemic despite continued vaccination programs and booster shots since new SARS-CoV-2 variants and subvariants are constantly emerging with different potentials of transmissibility, infectivity, and fatality (Jakariya et al., 2021; Sakib et al., 2021; Wong, 2022). Evaluating novel variants based on epidemic intelligence along with screening for genomic variants is regularly done on behalf of (ECDC, 2023). Omicron (B.1.1.529) and its subvariants BA.1, BA.2, BA.3, BA.4, BA.5, and its descendant lineages are the only variants of concerns (VOCs) currently circulating, while Alpha (B.1.1.7), Beta (B.1.351), Gamma (P.1), and Delta (B.1.617.2) are now categorized as previously circulating VOCs (Dhama et al., 2022). Unexpectedly, the Delta variant caused a sharp rise in COVID-19 cases and more fatalities in 2021, while Omicron variant then caused a gigantic and absolutely massive rise in 2022. The Omicron variant (Pango lineage B.1.1.529) has spawned numerous offshoots, including the BA.2, BA.3, BA.1, and BA.1.1, BA.2.12.1, BA.2.75, BA.2.75.2, BA.4, BA.4.6, and BA.5, BQ.1, BQ.1.1 (BA.4/5), BF.7, and XBB.1.5 (Fernandes et al., 2022). The BA.2, BA.4, and BA.5 have been discovered in 2022; almost all of the variants have South African origin except for BA.2.75 which was discovered in India (Dhama et al., 2023). BQ.1.1 now makes up 34% of cases nationwide, whereas XBB.1.5 makes up 28% of instances. In Nebraska, BA.5 and BQ.1 accounted for 23% of cases each as of December 31, 2022. Other Omicron variations may include XBB and XBB.1.1, yet, they are not specifically included in the most recent study, following the recent upheaval of BQ.1.1, accounting 23% of cases based in Nebraska (Nebraska Medicine, 2023). The most recent information also suggests the appearance of the variant XBB.1.5, which is a recombinant of the subvariants BA.2.10.1 and BA.2.75. Omicron XBB1.5 sub-lineage has been listed by ECDC as a variant of interest (VOI) as of January 12, 2023 (ECDC, 2023). According to ECDC arithmetical model in the EU/EEA, the XBB1.5 sub lineage of XBB, SARS-CoV-2 Omicron variant could turn into dominant after 1 to 2 months where it is identified 2.5% last 2 weeks of 2022 and spreading quickly (12% detected) in the United States (ECDC, 2023a).
Like other variants, the Omicron variant is composed of a variety of lineages and sublineages. Although these lineages are extremely analogous to one another, variations across lineages may influence how the virus behaves. The XBB strain is a hybrid of BA.2.10.1 and BA.2.75 varieties. Initial research suggests that XBB has a greater risk of reinfection than the other circulating Omicron sublineages (Uraki et al., 2023). Only those who contracted XBB prior to the emergence of Omicron type were at risk of reinfection. The hypothesis that other Omicron lineages could be able to evade the immune responses they have already caused is, as of now, unproven (WHO, 2023a). The rapid spread of the XBB.1.5 Omicron subvariant in the northeastern United States has prompted concern from the World Health Organization (WHO). Until now, the transmission rate of this variant has been the highest of any subtype (WHO, 2023b). XBB.1.5 shares the same resistance to vaccination and disease-induced immune reactivity as its close siblings XBB and XBB.1. XBB.1.5, however, contains a mutation that increases its ability to adhere to cells, providing it a competitive advantage. When a virus is able to infect people who have been previously exposed to it, either by infection or immunization, it is said to exhibit immune evasiveness. The XBB.1.5 strain achieved this property by creating a novel mutation in its receptor-binding domain (RBD) termed F486P. The extent to which it causes or contributes to more severe disorders is unclear. According to the experts, this is an extremely remote possibility (Kurhade et al., 2022).
The SARS-CoV-2 subvariants BQ.1.1 and XBB.1 have spread widely because they are more successful at growing than the vast majority of Omicron mutants. However, recent studies have shown that the recombinant mutant XBB subvariant XBB.1.5 has a substantial growth advantage over BQ.1.1 and XBB.1 (Tamura et al., 2022). Because of its greater transmissibility, XBB.1.5 has swiftly become the predominant strain in the United States and is almost certainly may be the cause of rising cases in the forthcoming time amid the ongoing COVID-19 pandemic. XBB/XBB.1 has been demonstrated to be even more resistant to neutralization by plasma/serum from vaccinated or recovering healthy individuals than BQ.1.1. Ser486Pro is an unusual 2-nucleotide change on the spike (S) protein that is only seen in XBB.1.5 and not in XBB.1. Urgent research into the causes of XBB.1.5's rapid propagation, especially the part played by Ser486Pro, is required (Cao et al., 2022; Yue et al., 2023).
This winter, most respiratory viruses have been circulating at higher rates than usual. To date, XBB.1.5 has been found to be the Omicron sub-variant that spreads the most rapidly. Its rapid proliferation can be attributed to the additional mutations it carries. The cause is a mutation in a region of the spike protein required for binding to its receptor, ACE2 (Angiotensin Converting Enzyme 2). Because of its superior ability to invade human cells, this variety has emerged possibility as the most dangerous. In many simulations, XBB.1.5 was found to have a higher transmission R value and infection rate than earlier versions. The Centers for Disease Control and Prevention (CDC) reports that only 15% of Americans age 5 and older have received a bivalent booster, suggesting that many people are currently less protected than they may be against the new strain (CDC, 2023). Certain data suggest that the probability of acquiring a chronic case of COVID-19 is lower for people who contracted an earlier form of the Omicron variations as compared to those who got the Delta strain. But if XBB.1.5 spreads, even a small number of people with chronic issues could substantially increase chronic COVID cases. Regardless of its current status, the CDC predicts an increase in reported infections over the next few weeks. The fact that this variant has recently caused an uptick in hospitalization rates in New York City suggests that it has a propensity to do so in other areas where it is prevalent. Breathing problems, headaches, sore throats, blocked noses, achy bodies, and fevers are all symptoms frequently reported by those with the Omicron XBB sub-variant lineage. At least 74 nations and 43 US states have confirmed cases of XBB, according to the https://outbreak.info/. Taking into account sample collection dates up to and including October 22, 2022, the novel variant XBB.1.5 was first identified in the United States at that time (ECDC, 2023). The CDC claims that the origin of the novel XBB.1.5 variant is unknown, but that outbreaks have been predominantly connected to North-Eastern nations, as is evident from Table 1.
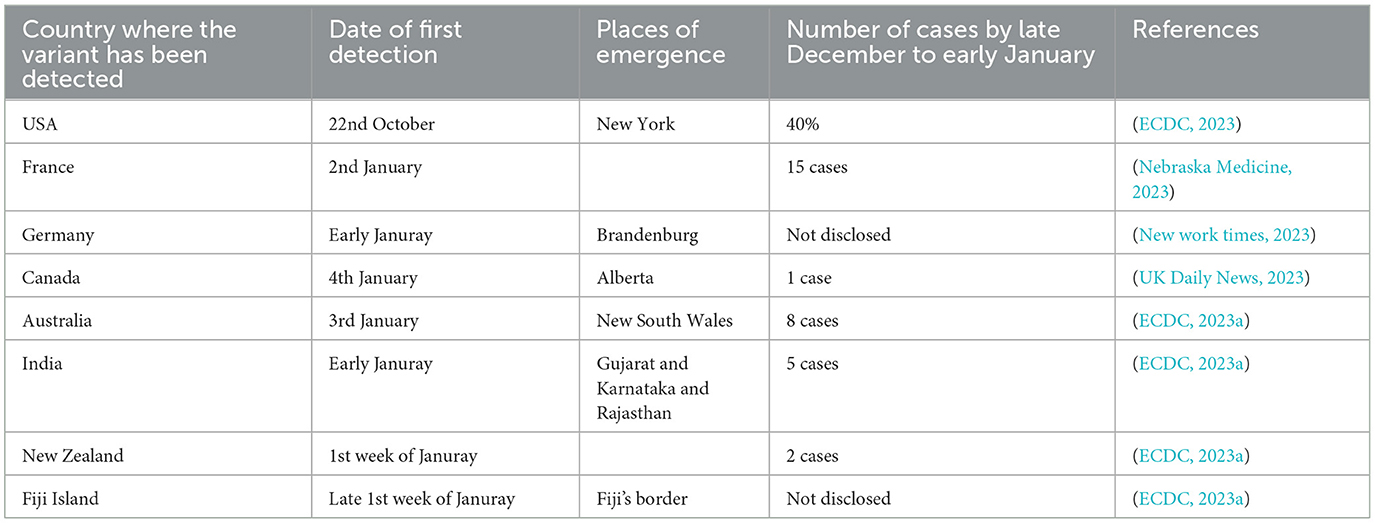
Table 1. The outbreaks of novel XBB1.5 variant since October 2022.
According to the CDC, the younger version, known as XBB.1.5, accounted for 27.6% of cases nationwide and 72.0% of new cases in the Northeast, indicated precisely in the above table (CDC, COVID-19).
According to Dr. Lynora Saxinger, an expert in infectious diseases at the University of Alberta (NB News, 2023), the new subvariant appears to be “an antibody-escaper,” because of its enhanced proliferation and mutational powers. Recent laboratory investigations reveal that XBB can hide from antibodies associated with prior COVID-19 infections or vaccines (ECDC, 2023b), suggesting that an exposed person is more likely to become unwell, become reinfected, and develop symptoms. Scientist and assistant professor at Peking University Yunlong Cao claims that XBB.1.5 is superior to the XBB.1 form at attaching to cells via a critical receptor and at evading protective antibodies. Its rapid spread, especially in the United States, is very concerning, despite the lack of evidence that it causes more severe illness than other Omicron variants.
Due to their ability to evade the immune system, causing vaccine breakthrough infections and reinfection, the emerging newer Omicron strains indicate that masks are still necessary and it is not yet safe to relax. Vaccines and booster doses can reduce hospitalizations, disease severity, deaths, and long-term effects of SARS-CoV-2 variants including Omicron and its subvariants (Ahmed et al., 2021). The best way to protect yourself from SARS-CoV-2 and its variations is to vaccinate (Zhou et al., 2022). Omicron can be treated, deaths avoided, and major issues get resolved with the use of booster doses and immunizations. Against the Omicron form, even three doses of the COVID-19 vaccine only offer limited protection, therefore additional boosters are required to confer better immunity. There is a pressing need for improved vaccination methods and technologies as well as universal access to immunizations. When Omicron subvariants increase in number, newer and better vaccines with higher efficacy and mAbs with high potential are required in the clinics for treating COVID-19 patients (Fernandes et al., 2022). Vaccines that can be administered by the nose (intranasal, mucosal vaccines), nanoparticle-based vaccines, universal vaccines aimed at pan-beta-coronaviruses, and mutation proof vaccines are urgently required at this time (Akkiz, 2022; Ke et al., 2022) An increase in surveillance and monitoring, strict vigilance, the adoption of suggested COVID-19 protection and control strategies, and increased immunization programs and booster doses are all urgently needed to combat emerging SARS-CoV-2 variants and subvariants (Ahemd et al., 2021). Limiting the transmission and spread of COVID-19 and its associated mortality and the emergence of new Omicron subvariants can be achieved through the use of face masks, frequent hand washing, social/physical distancing, adequate cleaning and disinfection measures, and the avoidance of crowded settings and mass gatherings (Aleem et al., 2022).
Patients frequently take natural drugs that inhibit the S protein (iguesterin, baicalin), 3CLpro (iguesterin, cryptotanshinone), helicase (silvestrol), and RdRp. Among these are Allium sativum, Camellia sinensis, Zingiber officinale, Nigella sativa, and several Echinacea species (Sharun et al., 2022). Although terpenoids have been shown to be useful in suppressing viral replication, there are also alkaloids with strong anti-coronavirus activities. Patients with severe cases of COVID-19 typically have severely weakened innate immunity. Several antiviral medications, such as Monalizumab, interferon, and chloroquine, can restore the function of CD8+ T and NK cells (generally decreased in severe cases). However, the best way to ensure your health, both now and in the future, is to avoid getting sick in the first place. In an effort to keep everyone healthy, additional measures need to follow boost immunity, such as getting enough sleep, regulating stress, reducing inflammation, improving diet, taking healthy nutritious foods, probiotics, staying hydrated, and exercising. Rapid, accurate, timely diagnosis of COVID-19, SARS-CoV-2 whole genome sequencing, booster doses vaccines, mask, proper hygiene rules, one health guidelines, and wastewater based surveillance to monitor hotspots might follow to tackle this new XBB.1.5.
MI: conceptualized, wrote the first draft, and edited. FK, DC, CC, KD, and PB: updated the manuscript, edited, and reviewed. All authors have critically reviewed and approved the final draft.
Authors acknowledge Advanced Molecular Lab, President Abdul Hamid Medical College, Kishoreganj, Bangladesh-2310, and all of the institutions in this manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Ahmed, F., Islam, M. A., Kumar, M., Hossain, M., Bhattacharya, P., Islam, M. T., et al. (2021). First detection of SARS-CoV-2 genetic material in the vicinity of COVID-19 isolation Centre in Bangladesh: variation along the sewer network. Sci. Total Environ. 776, 145724. doi: 10.1016/j.scitotenv.2021.145724
Akkiz, H. (2022). The biological functions and clinical significance of SARS-CoV-2 variants of corcern. Front. Med. 9, 849217. doi: 10.3389/fmed.2022.849217
Aleem, A., Akbar Samad, A. B., and Slenker, A. K. (2022). “Emerging variants of SARS-CoV-2 and novel therapeutics against coronavirus (COVID-19),” in StatPearls (Treasure Island, FL: StatPearls Publishing).
Cao, Y., Jian, F., Wang, J., Yu, Y., Song, W., Yisimayi, A., et al. (2022). Imprinted SARS-CoV-2 humoral immunity induces convergent Omicron RBD evolution. Nature 614, 521–529. doi: 10.1038/s41586-022-05644-7
CDC (2023). COVID-19. Available online at: https://www.cdc.gov/coronavirus/2019-ncov/variants/index.html (accessed January 10, 2023).
Dhama, K., Chandran, D., Chopra, H., Islam, M. A., Bin, E. U., Rehman, M. E. U., et al. (2022). SARS-CoV-2 emerging Omicron subvariants with a special focus on BF.7 and XBB.1.5 recently posing fears of rising cases amid ongoing COVID-19 pandemic. J. Exp. Biol. Agric. Sci. 10, 1215–1221. doi: 10.18006/2022.10(6)0.1215.1221
Dhama, K., Nainu, F., Frediansyah, A., Yatoo, M. I., Mohapatra, R. K., Chakraborty, S., et al. (2023). Global emerging Omicron variant of SARS-CoV-2: impacts, challenges and strategies. J. Infect. Public Health 16, 4–14. doi: 10.1016/j.jiph.2022.11.024
ECDC (2023). Update on SARS-CoV-2 Variants: ECDC Assessment of the XBB.1.5 Sub-Lineage, n.d. (accesed January 10, 2023).
ECDC (2023a). Available online at: https://www.ecdc.europa.eu/en/covid-19/variants-concern (accessed January 10, 2023).
ECDC (2023b). Available from: https://www.ecdc.europa.eu/en/news-events/covid-19-implications-spread-omicron-xbb15 (accessed January 15, 2022).
Fernandes, Q., Inchakalody, V. P., Merhi, M., Mestiri, S., Taib, N., Moustafa Abo El-Ella, D., et al. (2022). Emerging COVID-19 variants and their impact on SARS-CoV-2 diagnosis, therapeutics and vaccines. Ann. Med. 54, 524–540. doi: 10.1080/07853890.2022.2031274
Islam, A., Rahman, A., Jakariya, Bahadur, N. M., Hossen, F., Mukharjee, S. K., et al. (2022a). A 30-day follow-up study on the prevalence of SARS-CoV-2 genetic markers in wastewater from the residence of COVID-19 patient and comparison with clinical positivity. Sci. Total Environ. 159350. doi: 10.1016/j.scitotenv.2022.159350
Islam, M. A., Haque, M. A., Rahman, M. A., Hossen, F., Reza, M., Barua, A., et al. (2022b). A review on measures to rejuvenate immune system: natural mode of protection against coronavirus infection. Front. Immunol. 13, 837290. doi: 10.3389/fimmu.2022.837290
Islam, M. A., Marzan, A. L., Sydul, M. I., Sultana, S., Parvej, M. I., Hossaine, M. S., et al. (2021). Sex-specific epidemiological and clinical characteristics of COVID-19 patients in the southeast region of Bangladesh, MedRxiv doi: 10.1101/2021.07.05.21259933
Jakariya, M., Ahmed, F., Islam, M. A., Ahmed, T., Marzan, A., Al Hossain, M., et al. (2021). Wastewater based surveillance system to detect SARS-CoV-2 genetic material for countries with on-site sanitation facilities: an experience from Bangladesh. medRxiv doi: 10.1101/2021.07.30.21261347
Ke, H., Chang, M. R., and Marasco, W. A. (2022). Immune evasion of SARS-CoV-2 omicron subvariants. Vaccines 10, 1545. doi: 10.3390/vaccines10091545
Kurhade, C., Zou, J., Xia, H., Liu, M., Chang, H. C., Ren, P., et al. (2022). Low neutralization of SARS-CoV-2 Omicron BA.2.75.2, BQ.1.1 and XBB.1 by parental mRNA vaccine or a BA.5 bivalent booster. Nat. Med. doi: 10.1101/2022.10.31.514580
NB News (2023). Available online at: https://www.nbcnews.com/health/health-news/xbb15-subvariant-cdc-reports-new-omicron-strain-taking-rcna63512 (accessed January 10, 2023).
Nebraska Medicine (2023). Available online at: https://www.nebraskamed.com/COVID/what-covid-19-variants-are-going-around (accessed January 10, 2023).
New work times (2023). Available online at: https://www.nytimes.com/2023/01/07/science/covid-omicron-variants-xbb.html (accessed January 10, 2023).
Rakib, S. H., Masum, S., Farhana, R. A., Islam, M. A., Islam, M. F., and Reza, M. T. (2022). “Design of a cost-effective ultraviolet disinfection unit to minimize the cross-contamination of COVID-19 in Transport,” in International Conference on Advancement in Electrical and Electronic Engineering (ICAEEE) (Gazipur: IEEE). doi: 10.1109/ICAEEE54957.2022.9836348
Rakib, S. H., Masum, S., Patwari, M. R. I., Fahima, R. A., Farhana, A., and Islam, M. A. (2021). “Design and development of a low cost ultraviolet disinfection system to reduce the cross infection of SARS-CoV-2 in ambulances,” in International Conference on Electronics, Communications and Information Technology (ICECIT) (Khulna: IEEE). doi: 10.1109/ICECIT54077.2021.9641131
Sakib, M. M. H., Nishat, A. A., Islam, M. T., Raihan Uddin, M. A., Iqbal, M. S., Bin Hossen, F. F., et al. (2021). Computational screening of 645 antiviral peptides against the receptor-binding domain of the spike protein in SARS-CoV-2. Comput. Biol. Med. 136, 104759. doi: 10.1016/j.compbiomed.2021.104759
Sharun, K., Tiwari, R., Yatoo, M. I., Natesan, S., Megawati, D., Singh, K. P., et al. (2022). A comprehensive review on pharmacologic agents, immunotherapies and supportive therapeutics for COVID-19. Narra J. 2, e92. doi: 10.52225/narra.v2i3.92
Tamura, T., Ito, J., Uriu, K., Zahradnik, J., Kida, I., Nasser, H., et al. (2022). Virological characteristics of the SARS-CoV-2 XBB variant derived from recombination of two Omicron subvariants. bioRxiv. 2022.2012.2027.521986. doi: 10.1101/2022.12.27.521986
UK Daily News (2023). Available online at: https://ukdaily.news/covid-xbb-1-5-bf-7-what-is-the-situation-in-france-of-the-sub-variants-that-are-wreaking-havoc-abroad-282658.html (accessed January 10, 2023).
Uraki, R., Ito, M., Furusawa, Y., Yamayoshi, S., Iwatsuki-Horimoto, K., Adachi, E., et al. (2023). Humoral immune evasion of the omicron subvariants BQ.1.1 and XBB. Lancet Infect. Dis. 23, 30–32. doi: 10.1016/S1473-3099(22)00816-7
WHO (2022). Available online at: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19-−11-march-2020 (accesed January 08, 2022).
WHO (2023a). WHO Coronavirus (COVID-19) Dashboard. https://covid19.who.int/ (accessed January 10, 2023).
WHO (2023b). World Health Organization. Tracking SARS-CoV-2 Variants. Available online at: https://www.who.int/en/activities/tracking-SARS-CoV-2-variants (accessed January 02, 2023).
Wong, C. (2022). Subvariant “soup” may drive wave. New Sci. 256, 11. doi: 10.1016/S0262-4079(22)01970-4
Yue, C., Song, W., Wang, L., Jian, F., Chen, X., Gao, F., et al. (2023). Enhanced transmissibility of XBB.1.5 is contributed by both strong ACE2 binding and antibody evasion. bioRxiv 2023.01.03.522427 doi: 10.1101/2023.01.03.522427
Keywords: COVID-19, Omicron, XBB.1.5 sub-lineage, SARS-CoV-2, new variants, transmission
Citation: Islam MA, Kaifa FH, Chandran D, Bhattacharya M, Chakraborty C, Bhattacharya P and Dhama K (2023) XBB.1.5: A new threatening SARS-CoV-2 Omicron subvariant. Front. Microbiol. 14:1154296. doi: 10.3389/fmicb.2023.1154296
Received: 30 January 2023; Accepted: 28 March 2023;
Published: 17 April 2023.
Edited by:
Pragya Dhruv Yadav, ICMR-National Institute of Virology, IndiaReviewed by:
Kazuhiko Kanou, National Institute of Infectious Diseases (NIID), JapanCopyright © 2023 Islam, Kaifa, Chandran, Bhattacharya, Chakraborty, Bhattacharya and Dhama. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Md. Aminul Islam, YW1pbnVsQHBhaG1jLmVkdS5iZA==; YW1pbnVsbWJnQGdtYWlsLmNvbQ==; Prosun Bhattacharya, cHJvc3VuQGt0aC5zZQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.