
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Microbiol. , 25 March 2022
Sec. Antimicrobials, Resistance and Chemotherapy
Volume 13 - 2022 | https://doi.org/10.3389/fmicb.2022.857569
This article is part of the Research Topic Helicobacter pylori infection: pathogenesis, antibiotic resistance, advances and therapy, new treatment strategies View all 12 articles
 Younghee Choe1†
Younghee Choe1† Joon Sung Kim1*†Hyun Ho Choi2Dae Bum Kim3Jae Myung Park4†Jung Hwan Oh5†
Joon Sung Kim1*†Hyun Ho Choi2Dae Bum Kim3Jae Myung Park4†Jung Hwan Oh5† Tae Ho Kim6†Dae Young Cheung7†Woo Chul Chung3†Byung-Wook Kim1†Sung Soo Kim2†
Tae Ho Kim6†Dae Young Cheung7†Woo Chul Chung3†Byung-Wook Kim1†Sung Soo Kim2†Background: Bismuth quadruple therapy (BQT) is recommended as empirical first-line therapy because it is not affected by antibiotic resistance. We examined whether past exposure to metronidazole affected BQT outcomes.
Methods: The records of seven hospitals were searched for patients who received BQT for Helicobacter pylori eradication between 2009 and 2020. The association between past metronidazole exposure and the eradication rate was evaluated.
Results: This study was a multicenter retrospective study. Around 37,602 people tested for H. pylori infection were identified, and 7,233 received BQT. About 2,802 (38.7%) underwent a 13C-urea breath test to confirm eradication. The BQT efficacy was 86.4% among patients without metronidazole exposure and 72.8% among patients with exposure (p < 0.001). The eradication rate of BQT 14 days in patients with past exposure was higher than that of BQT <14 days (85.5 vs. 66.0%, p = 0.009). Multivariate analysis revealed that past metronidazole exposure [odds ratio (OR) 2.6, 95% CI 1.8–3.7; p < 0.001] and BQT <14 days (OR 1.5, 95% CI 1.2–2.0; p = 0.002) were independent risk factors for eradication failure.
Conclusion: Past metronidazole exposure significantly lowered the BQT eradication rate. BQT 14 days should be recommended for patients with suspected metronidazole exposure.
Helicobacter pylori is the primary etiologic cause of gastric adenocarcinoma (Lee et al., 2016; Hooi et al., 2017; Chiang et al., 2021). A recent systematic review reported that eradication resulted in a 46% reduced incidence of and 39% reduced mortality from gastric cancer (de Martel et al., 2020; Ford et al., 2020). The Kyoto global consensus and Houston consensus conferences recommend treating all individuals with proven H. pylori infection (Sugano et al., 2015; El-Serag et al., 2018). Traditionally, eradication for H. pylori was based on a standard triple regimen consisting of a proton pump inhibitor (PPI), amoxicillin, and clarithromycin. However, this regimen is no longer recommended without susceptibility testing due to the high rates of clarithromycin resistance in many countries (Malfertheiner et al., 2011; Yeo et al., 2018).
Many current guidelines recommend bismuth quadruple therapy (BQT) as first-line therapy in areas with high clarithromycin resistance because BQT is less affected by antibiotic resistance (Fallone et al., 2016; Chey et al., 2017; Malfertheiner et al., 2017; Chen et al., 2019; Jung et al., 2020; Shah et al., 2021). However, BQT is difficult to use due to its frequent dosing, side effects, and availability (Howden and Graham, 2021). According to the recent European Registry, BQT users reported higher rates of side effects than those on other regimens (Nyssen et al., 2021a). BQT is generally recommended for 14 days rather than 7 or 10 days (Fallone et al., 2019; Kim et al., 2020; Shah et al., 2021). This is because prolonging the duration of metronidazole use to 14 days is expected to overcome resistance. However, few studies have confirmed this in clinical trials.
Several studies reported that clarithromycin-based triple therapy was affected by past macrolides exposure (Boltin et al., 2019; Kwon et al., 2019). There have been studies examining the relationship between past metronidazole exposure and BQT eradication rates. However, no meaningful additional analysis was performed other than the eradication rate due to the small number of patients (McNulty et al., 2012; Boltin et al., 2020; Lee et al., 2020). Our purpose was to investigate whether past metronidazole exposure influenced the eradication rates of the BQT regimen. We also examined the eradication rates according to the BQT duration in patients with or without metronidazole exposure.
This was a multicenter retrospective study of patients from seven university hospitals from 2009 to 2020. We identified patients aged 20–79 years who underwent an endoscopy and were diagnosed with H. pylori by histology or a rapid urease test. Patients who were prescribed BQT for eradication were included. Age, sex, body mass index, smoking history, endoscopic findings, and pathologic results were identified. We also investigated the BQT duration and the type of PPI used for the BQT regimen. Medical records were reviewed to identify patients who had been prescribed metronidazole before their BQT prescription.
This study protocol was approved by the Institutional Review Board (IRB) of Catholic Medical Center (IRB approval number, XC20WIDI0119). The requirement for written informed consent was waived because anonymous data were used. This study followed the ethical principles of the Declaration of Helsinki.
Patients’ medical records were examined to determine whether they had received metronidazole before the prescription of BQT. All inpatient or outpatient antibiotic prescription records were searched, and metronidazole prescription records were extracted. The patient’s diagnosis, drug administration method, dosage, the number of doses per day, and total administration duration were examined together with all metronidazole prescription records. However, only the intravenous or oral administration cases were extracted, and topical preparations were excluded. We also investigated past metronidazole exposure intervals up to the BQT therapy regimen.
Helicobacter pylori infection was confirmed by rapid urease test, histopathology, or urea breath test. Dual priming oligonucleotide (DPO)-based multiplex PCR (Seeplex® ClaR-H. pylori ACE detection kit, Seegene Inc., Seoul, Korea) was performed in some patients confirmed with H. pylori infection to examine the presence of clarithromycin resistance. The precise methods of DPO-PCR have been described elsewhere (Posteraro et al., 2006; Woo et al., 2009; Lehours et al., 2011). BQT was prescribed as second-line therapy after the failure of the first-line triple therapy or first-line therapy in patients confirmed with clarithromycin resistance by DPO-PCR methods.
Bismuth quadruple therapy consisted of a PPI (standard dose) twice daily, bismuthate tripotassium dicitrate (300 mg) and tetracycline (500 mg) four times daily, and metronidazole (500 mg) three times daily. The PPIs used were lansoprazole (30 mg/T), pantoprazole (40 mg/T), rabeprazole (20 mg/T), esomeprazole (40 mg/C), and ilaprazole (10 mg/T). The BQT duration was 7, 10, or 14 days at the physician’s discretion. All patients underwent a urea breath test after 4–12 weeks to confirm the success of eradication. For the urea breath test, 13C-urea 100 mg tablets (UBiTkit™, Otsuka Electronics, Co., Ltd., Osaka, Japan) were orally taken with water after fasting for at least 4 h. Exhaled breath samples obtained after that were analyzed using the 13C-urea breath test (UBiT-IR300®), and the cut-off value for judging H. pylori-positive and negative was set to 2.5‰ (Graham et al., 1987; Graham and Klein, 1991; Atherton and Spiller, 1994).
The primary endpoint was to compare the BQT eradication rates according to patients’ past metronidazole exposure. The secondary endpoint was to identify risk factors associated with eradication failure. We examined whether past metronidazole exposure influenced the BQT eradication rate and whether prolonging the BQT duration was associated with treatment outcomes. We also examined whether the duration of past metronidazole exposure affected the BQT outcome and whether the interval between the past exposure and the prescription of BQT affected H. pylori eradication rates.
The baseline patient characteristics are summarized using descriptive statistics. Continuous data are presented as the mean (SD) or median (interquartile range), and categorical data are given quantities and proportions. The student’s t-test was used to compare continuous variables. Categorical variables were compared using the χ2 test or Fisher’s exact test. The duration of the past treatment was analyzed by linear-by-linear association because the independent variables were classified to be three or more. Logistic regression analysis was used to identify independent risk factors for eradication failure, and multiple regression analysis was used to analyze the correlation between these factors and eradication failure (i.e., factors that showed significant differences in univariate analysis).
The SPSS statistical program, version 22 (SPSS, Chicago, Illinois), was used for all analyses, and the significance level was set at a value of p < 0.05.
Around 37,602 patients were tested for H. pylori infection in the seven participating hospitals, and 7,238 of them received metronidazole containing eradication therapy. In total, 7,233 patients were prescribed BQT. Of the 7,233 patients prescribed BQT, 2,802 were followed up after eradication and included in this study (Figure 1). The mean age was 57.8 ± 11.4 years, and 53.2% of patients were male. About 158 (5.6%) patients had previously received metronidazole intravenously or orally. The baseline characteristics of the groups with and without past metronidazole exposure are shown in Table 1.
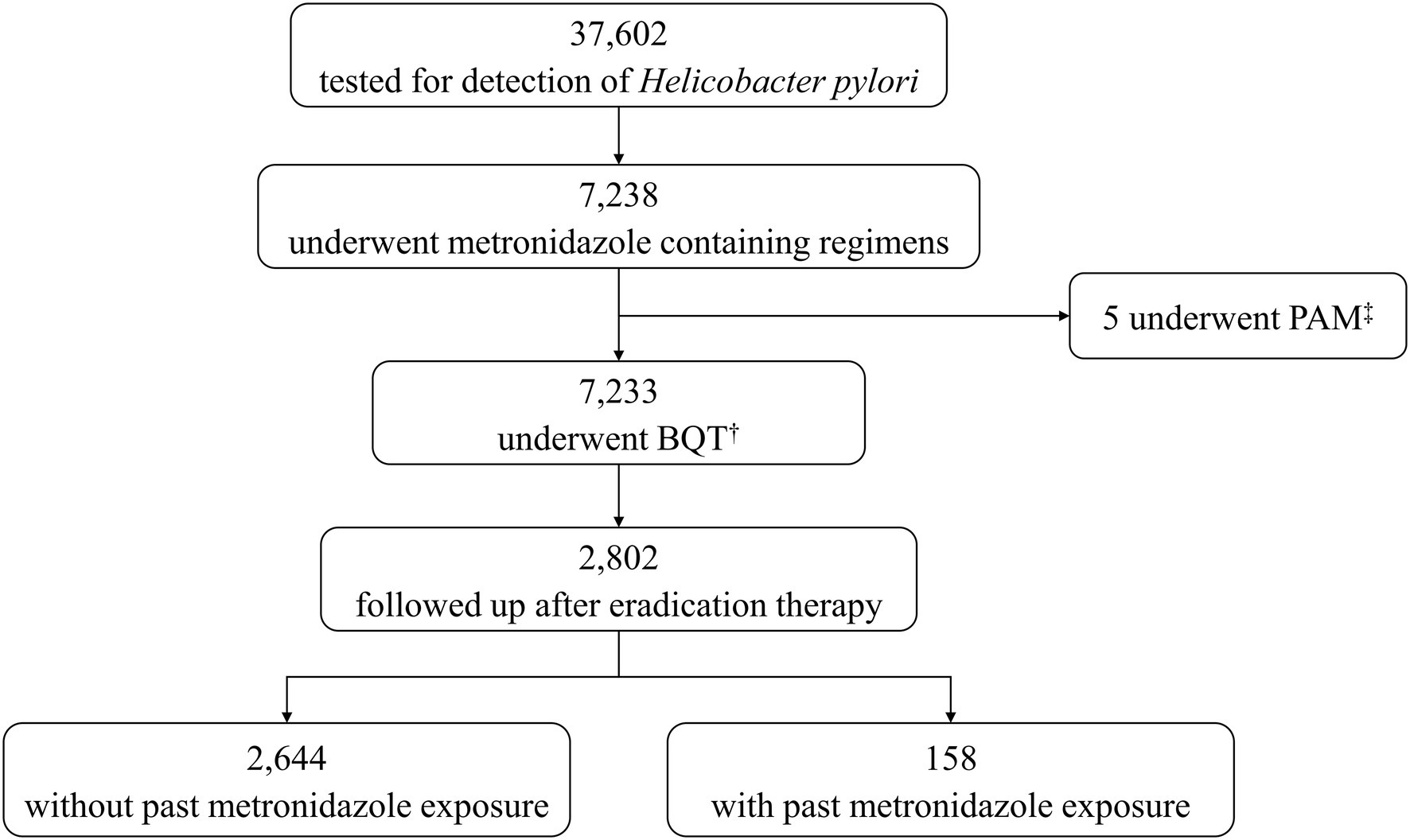
Figure 1. Flow chart. †BQT, bismuth quadruple therapy, ‡PAM, proton pump inhibitor, amoxicillin, and metronidazole.
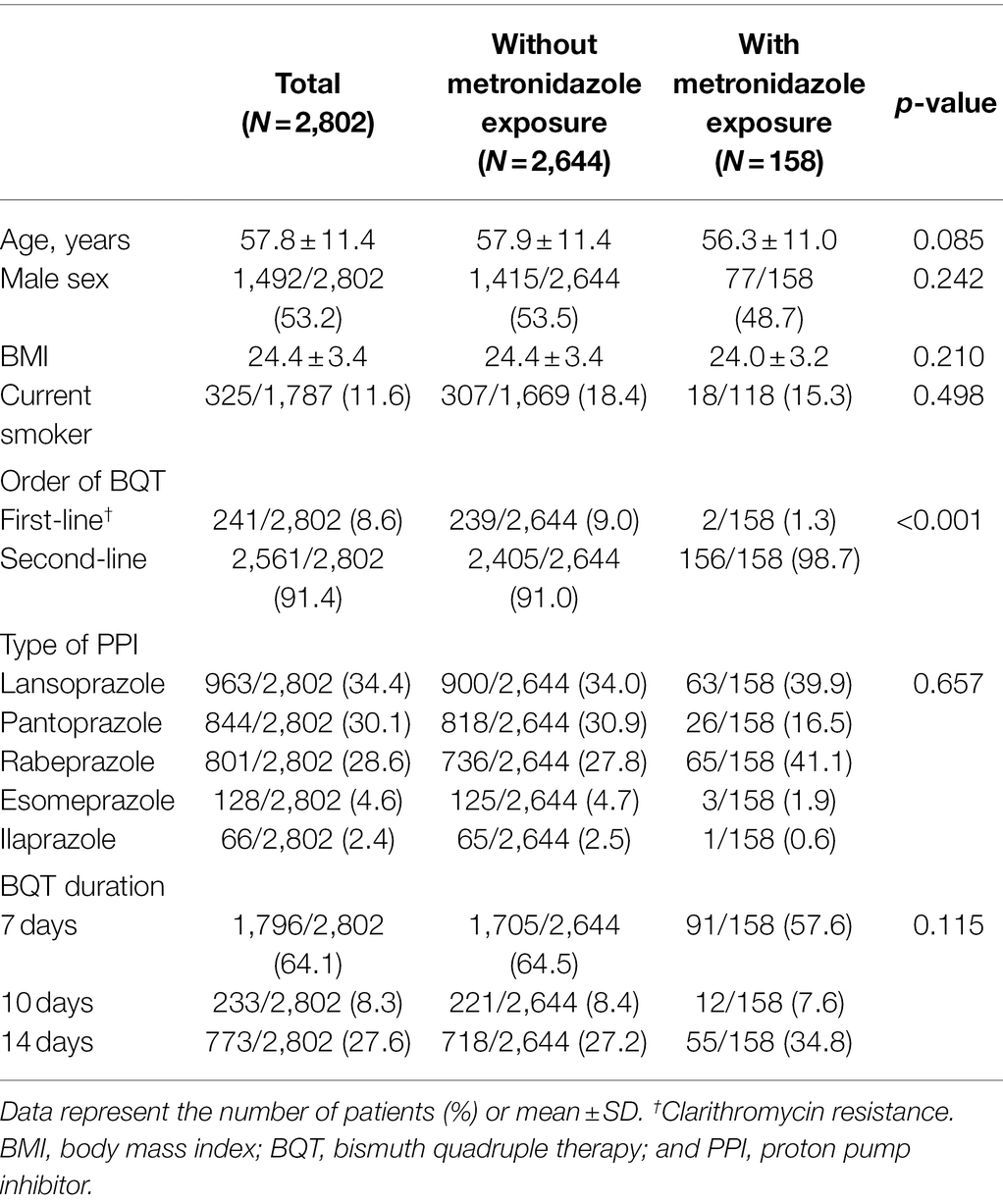
Table 1. Baseline characteristics.
Bismuth quadruple therapy regimen was prescribed as second-line therapy in 2,561 (91.4%) patients and as first-line therapy in 241 (8.6%) patients. BQT was prescribed more frequently as a first-line regimen in patients without metronidazole exposure (p < 0.001). The BQT duration was 7 days in 64.1%, 10 days in 8.3%, and 14 days in 27.6%. There was no significant difference in the duration of BQT in patients with or without metronidazole exposure (p = 0.115).
The BQT eradication rates for H. pylori were 86.4% in patients without metronidazole exposure and 72.8% in patients with exposure (p < 0.001; Table 2). There was no significant difference in the eradication rates of BQT <14 days and 14 days in patients without metronidazole exposure (87.5 vs. 89.1%, p = 0.289). The eradication rates of BQT 14 days were higher than BQT <14 days in patients with exposure (85.5 vs. 67.0%, p = 0.014).
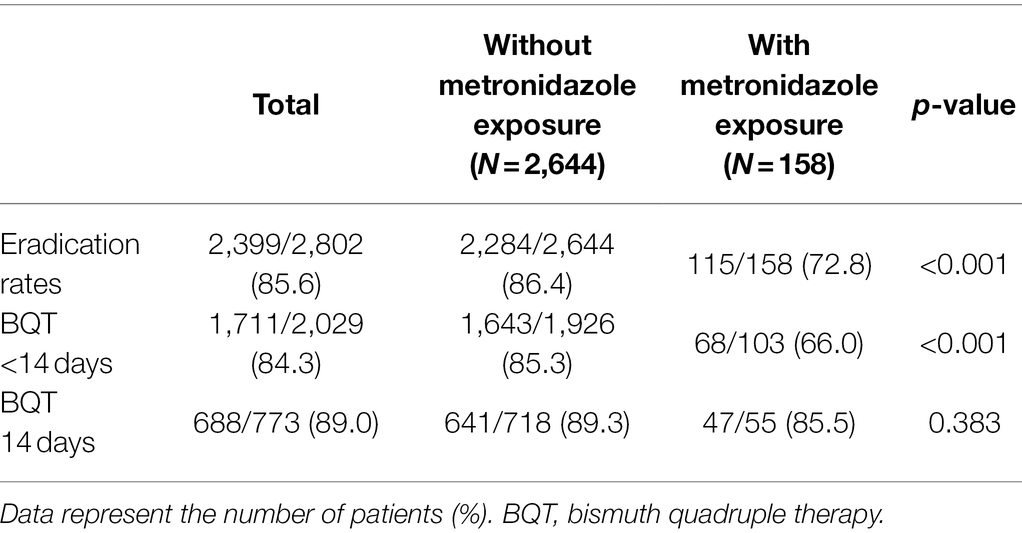
Table 2. Eradication rates of bismuth quadruple therapy for Helicobacter pylori with and without past metronidazole exposure.
We examined whether the duration of past metronidazole exposure and interval to BQT affected eradication. The eradication rates for less than 5 days, 5–9 days, and more than 10 days of past exposure were 81.8, 72.0, and 61.1% (Table 3). Figure 2A showed a tendency for the eradication rate to increase as the metronidazole exposure duration in the past increases (p < 0.001 by linear-by-linear association).
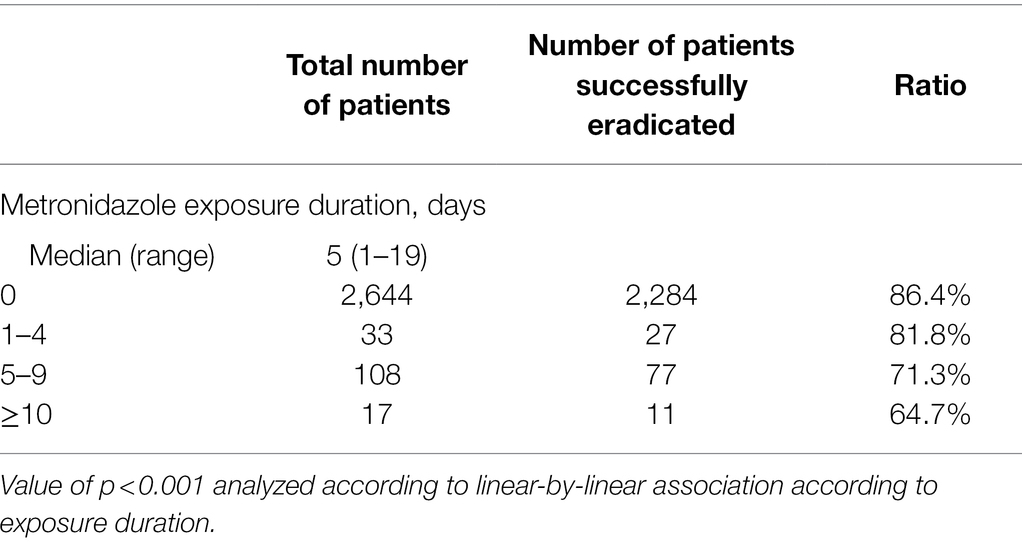
Table 3. Past metronidazole exposure duration in people receiving bismuth quadruple therapy.
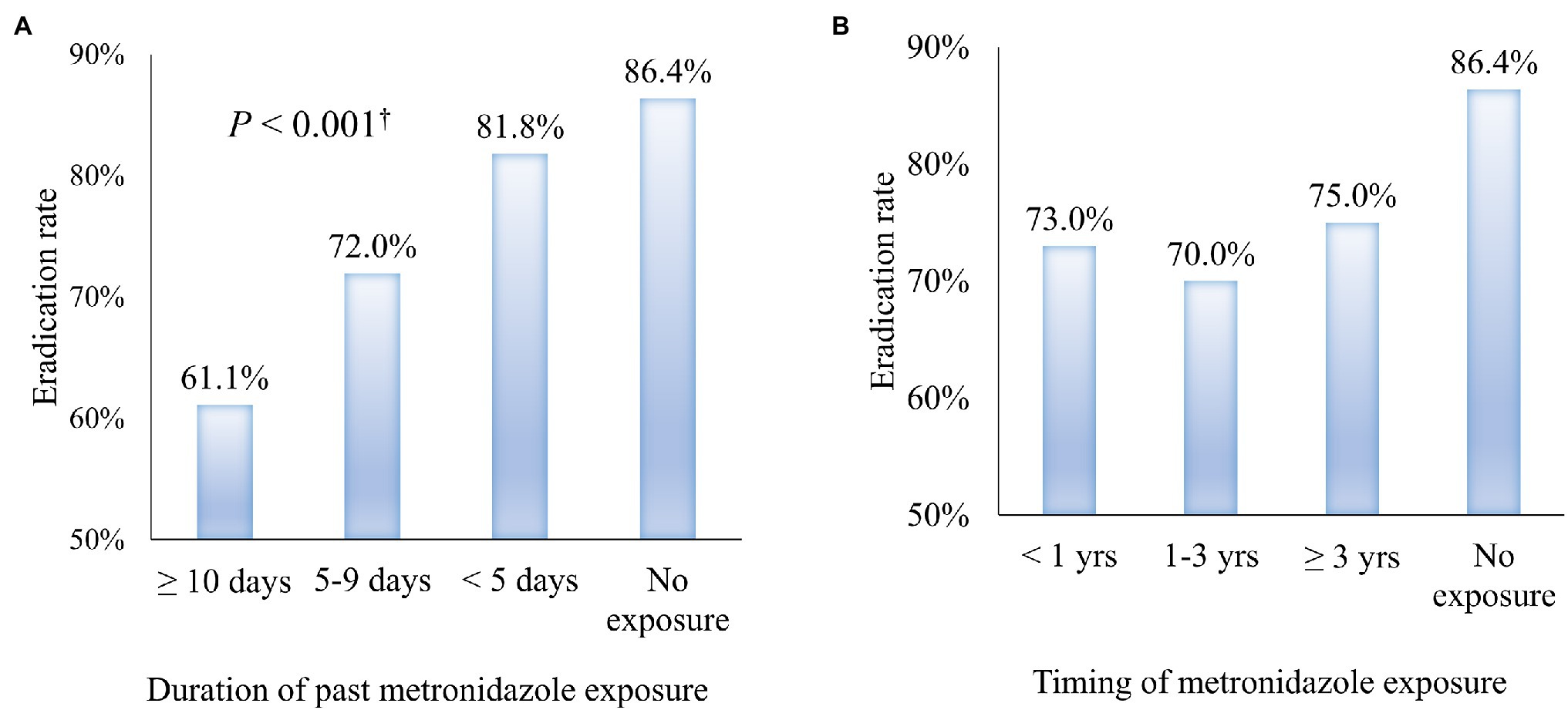
Figure 2. The trend of Helicobacter pylori eradication rate according to past metronidazole exposure. (A) Eradication rate of H. pylori by the duration of previous metronidazole exposure (B) Eradication rate of H. pylori by the interval from past metronidazole exposure to the prescription of bismuth quadruple therapy.
We also examined if the interval from past exposure to BQT prescription affected its outcomes. The intervals between past metronidazole exposure were 73, 70, and 75% for patients less than 12 months, 12–36 months, and ≥36 months, respectively. There was no significant difference between the exposure interval and the current BQT eradication rate (Figure 2B).
We performed a logistic regression analysis to identify H. pylori eradication failure (Table 4). Univariate analysis revealed BQT prescribed as first-line, past metronidazole exposure and BQT <14 days to be significantly associated with eradication failure. Multivariate analysis confirmed that BQT prescribed as first-line (odds ratio 1.79; 95% CI, 1.28–2.50; p = 0.001), past metronidazole exposure (odds ratio 2.57; 95% CI, 1.77–3.73; p < 0.001), and BQT <14 days (odds ratio 1.51; 95% CI, 1.16–1.96; p = 0.002) were independent risk factors for H. pylori eradication failure.
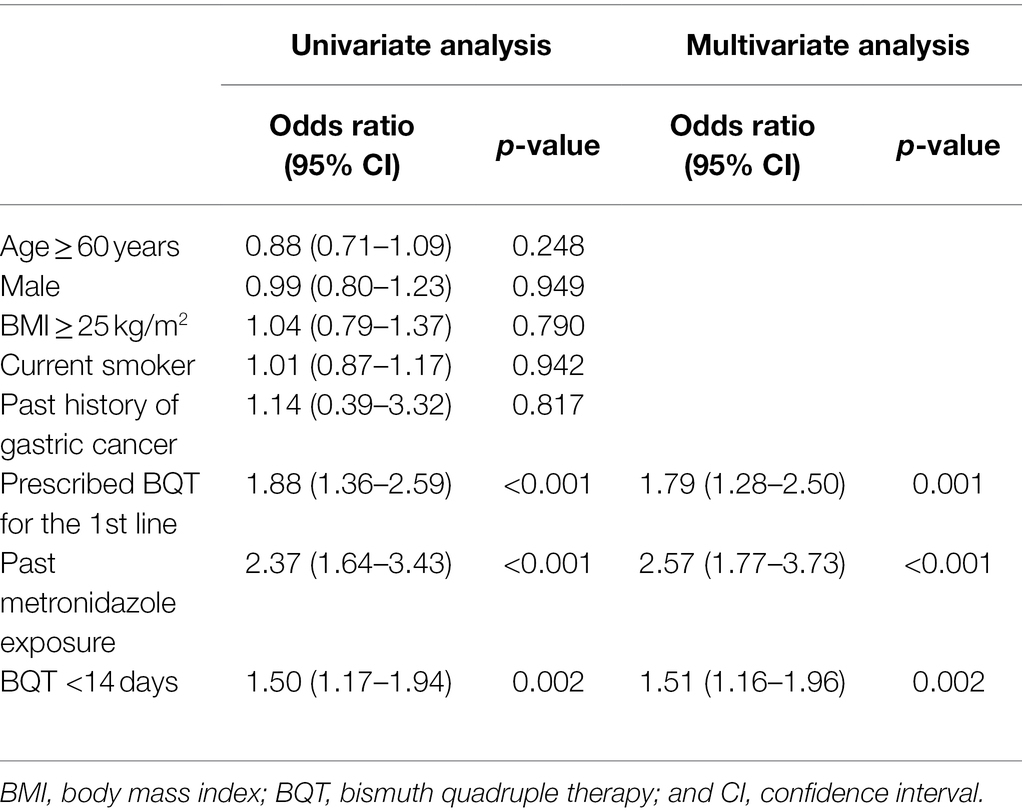
Table 4. Univariate and multivariate analysis of factors related to Helicobacter pylori eradication failure.
Current guidelines recommend BQT as empirical therapy because it has proven to be effective in areas with high antibiotic resistance (Fallone et al., 2016; Chey et al., 2017; Malfertheiner et al., 2017; Chen et al., 2019; Shah et al., 2021). Metronidazole resistance is high in many countries, and a recent study reported global resistance rates to be 40–70% (Savoldi et al., 2018; Schubert et al., 2020; Megraud et al., 2021). BQT 14 days is generally recommended in areas with high metronidazole resistance as extending the duration to 14 days is expected to overcome resistance. In our clinical practice, patients often complain of difficulty taking BQT for 14 days due to the complexity of the regimen and adverse events. According to a European Registry survey from 2013 to 2018, patients prescribed BQT had the highest risk of adverse events compared with other eradication regimens (Nyssen et al., 2021b). A systematic review reported that adverse events increased as the BQT duration prolonged from 7 to 14 days (Yuan et al., 2013). These studies suggest that the dosage frequency and adverse events of BQT can affect patient compliance. There is also little evidence that increasing BQT duration to 14 days is more effective than 7 or 10 days in patients with metronidazole resistance.
Metronidazole resistance is not easy to demonstrate. Culture tests can confirm antibiotic resistance. However, H. pylori are intricate to incubate, and the long time deters its use in clinical practice. The E-test, widely used to measure antibiotic resistance, is known to overestimate metronidazole resistance (Osato et al., 2001). An in vitro test for metronidazole resistance is not an absolute preclusion criterion for use because in vitro resistance does not reliably correlate with H. pylori eradication failure. A recent study reported no association between metronidazole resistance determined by molecular-based experiments and eradication success (Argueta et al., 2021). Phenotypic methods for metronidazole resistance testing are not well standardized, and results can vary depending on the method used, which can result in lower predictive value.
In our study, we found that past metronidazole exposure lowered the BQT eradication rate. Prolonging the BQT duration to 14 days significantly increased eradication rates in patients with past exposure. The eradication rates of BQT <14 days in patients without exposure were similar to BQT 14 days. This suggest that BQT regimens of shorter duration may be effective in patients without metronidazole exposure history or metronidazole resistance. For patients suspected with a past metronidazole exposure, BQT should be prescribed for 14 days or levofloxacin-based regimens may be considered in areas with low quinolone resistance.
A previous study investigated the relationship between the dose of past macrolides exposure and the eradication rate of standard triple therapy (Boltin et al., 2019). They reported that increased macrolides exposure was associated with lower eradication rates. To our knowledge, no study examined if the duration of past metronidazole exposure and the interval from exposure to eradication affected the eradication rate. In our study, the eradication rate decreased as the duration of past metronidazole exposure increased. However, the interval from metronidazole exposure to BQT prescription was not related to the eradication rate. Based on our results, BQT 14 days may be recommended for patients with suspected past metronidazole exposure, regardless of the interval from exposure. BQT 7 days can achieve high eradication rates with fewer side effects in areas with low metronidazole resistance or in patients without metronidazole exposure.
A three-in-one formulation (Pylera®) of three drugs, bismuth subcitrate, metronidazole, and tetracycline, is frequently prescribed in the United States and Europe. This formulation is preferred to BQT because of its small number of capsules but consists of 10 days. Few studies have compared the BQT eradication rates for 10 and 14 days (Dore et al., 2011). According to our study, 10-day BQT may not be sufficient in patients with past metronidazole exposure, suggesting that 10-day regimens should be avoided in areas with high metronidazole resistance.
Our study has several limitations. First, our study is a retrospective study which inevitably includes inherent limitations due to its study design. Most importantly, the baseline characteristics of patients with and without exposure were different. Specifically, BQT was prescribed as first-line regimens more often in patients without past metronidazole exposure. Second, patients classified as unexposed in this study might have been prescribed metronidazole at other hospitals. However, it is essential to note that metronidazole is not commonly prescribed in primary clinics in Korea (Park et al., 2017; Health Insurance Review and Assessment Service, 2021). Also, reclassification of these patients into the exposed group is expected to strengthen our findings further. Third, the follow-up loss rate was high in patients who were prescribed BQT. However, our study was retrospective, and the high follow-up loss rate reflects the reality of actual clinics. Another study reported that only 34.9% of those prescribed H. pylori eradication regimens visited the hospital to check their eradication results (Kumar et al., 2021). Finally, this study was conducted in a region with high metronidazole resistance. Our results may not be applicable in areas with different metronidazole.
In conclusion, past metronidazole exposure lowered the H. pylori eradication rate of BQT regimens, and longer exposure duration was associated with lower eradication rates. Prolonging the BQT duration to 14 days should be considered in patients with past metronidazole exposure.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
The studies involving human participants were reviewed and approved by Institutional Review Board (IRB) of Catholic Medical Center (IRB approval number, XC20WIDI0119). Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
YC designed the study, reviewed the literature, acquired and analyzed data, administrated the project, performed statistical analyses, wrote the original draft, and reviewed and edited the manuscript. JK supervised the study and was responsible for paper conception and manuscript review, and editing. JP acquired data and reviewed and edited the manuscript. HC, DK, JO, TK, and DC acquired data and edited the manuscript. WC, B-WK, and SK analyzed data and edited the manuscript. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
BQT, Bismuth quadruple therapy; DPO, Dual-priming oligonucleotide; H. pylori, Helicobacter pylori; PCR, Polymerase chain reaction; PPI, Proton pump inhibitor.
Argueta, E. A., Alsamman, M. A., Moss, S. F., and D’Agata, E. M. C. (2021). Impact of antimicrobial resistance rates on eradication of Helicobacter pylori in a US population. Gastroenterology 160, 2181.e1–2183.e1. doi: 10.1053/j.gastro.2021.02.014
Atherton, J. C., and Spiller, R. C. (1994). The urea breath test for Helicobacter pylori. Gut 35, 723–725. doi: 10.1136/gut.35.6.723
Boltin, D., Levi, Z., Gingold-Belfer, R., Gabay, H., Shochat, T., Niv, Y., et al. (2019). Impact of previous exposure to macrolide antibiotics on Helicobacter pylori infection treatment outcomes. Am. J. Gastroenterol. 114, 900–906. doi: 10.14309/ajg.0000000000000223
Boltin, D., Levi, Z., Gingold-Belfer, R., Gabay, H., Shochat, T., Schmilovitz-Weiss, H., et al. (2020). Effect of previous nitroimidazole treatment on Helicobacter pylori eradication success. J. Clin. Gastroenterol. 54, 333–337. doi: 10.1097/mcg.0000000000001237
Chen, Q., Long, X., Ji, Y., Liang, X., Li, D., Gao, H., et al. (2019). Randomised controlled trial: susceptibility-guided therapy versus empiric bismuth quadruple therapy for first-line Helicobacter pylori treatment. Aliment. Pharmacol. Ther. 49, 1385–1394. doi: 10.1111/apt.15273
Chey, W. D., Leontiadis, G. I., Howden, C. W., and Moss, S. F. (2017). ACG clinical guideline: treatment of Helicobacter pylori infection. Am. J. Gastroenterol. 112, 212–239. doi: 10.1038/ajg.2016.563
Chiang, T. H. C., Tseng, C. C., Liou, P. H., Wu, J. M., Shun, M. S., Lee, C. T., et al. (2021). Bismuth salts with versus without acid suppression for Helicobacter pylori infection: a transmission electron microscope study. Helicobacter 26:e12801. doi: 10.1111/hel.12801
de Martel, C., Georges, D., Bray, F., Ferlay, J., and Clifford, G. M. (2020). Global burden of cancer attributable to infections in 2018: a worldwide incidence analysis. Lancet Glob. Health 8, e180–e190. doi: 10.1016/s2214-109x(19)30488-7
Dore, M. P., Farina, V., Cuccu, M., Mameli, L., Massarelli, G., and Graham, D. Y. (2011). Twice-a-day bismuth-containing quadruple therapy for Helicobacter pylori eradication: a randomized trial of 10 and 14 days. Helicobacter 16, 295–300. doi: 10.1111/j.1523-5378.2011.00857.x
El-Serag, H. B., Kao, J. Y., Kanwal, F., Gilger, M., LoVecchio, F., Moss, S. F., et al. (2018). Houston consensus conference on testing for Helicobacter pylori infection in the United States. Clin. Gastroenterol. Hepatol. 16, 992.e6–1002.e6. doi: 10.1016/j.cgh.2018.03.013
Fallone, C. A., Chiba, N., van Zanten, S. V., Fischbach, L., Gisbert, J. P., Hunt, R. H., et al. (2016). The Toronto consensus for the treatment of Helicobacter pylori infection in adults. Gastroenterology 151, 51.e14–69.e14. doi: 10.1053/j.gastro.2016.04.006
Fallone, C. A., Moss, S. F., and Malfertheiner, P. (2019). Reconciliation of recent Helicobacter pylori treatment guidelines in a time of increasing resistance to antibiotics. Gastroenterology 157, 44–53. doi: 10.1053/j.gastro.2019.04.011
Ford, A. C., Yuan, Y., and Moayyedi, P. (2020). Helicobacter pylori eradication therapy to prevent gastric cancer: systematic review and meta-analysis. Gut 69, 2113–2121. doi: 10.1136/gutjnl-2020-320839
Graham, D. Y., and Klein, P. D. (1991). What you should know about the methods, problems, interpretations, and uses of urea breath tests. Am. J. Gastroenterol. 86, 1118–1122.
Graham, D. Y., Klein, P. D., Evans, D. J. Jr., Evans, D. G., Alpert, L. C., Opekun, A. R., et al. (1987). Campylobacter pylori detected noninvasively by the 13C-urea breath test. Lancet 1, 1174–1177. doi: 10.1016/s0140-6736(87)92145-3
Health Insurance Review and Assessment Service (2021). “[Assessment Report of the Adequacy of Drug Use, 2020].” July 2021 edition. Available at: http://www.hira.or.kr/bbsDummy.do?pgmid=HIRAA020002000100 (Accessed January 29, 2022).
Hooi, J. K. Y., Lai, W. Y., Ng, W. K., Suen, M. M. Y., Underwood, F. E., Tanyingoh, D., et al. (2017). Global prevalence of Helicobacter pylori infection: systematic review and meta-analysis. Gastroenterology 153, 420–429. doi: 10.1053/j.gastro.2017.04.022
Howden, C. W., and Graham, D. Y. (2021). Recent developments pertaining to H. pylori infection. Am. J. Gastroenterol. 116, 1–3. doi: 10.14309/ajg.0000000000001031
Jung, H. K., Kang, S. J., Lee, Y. C., Yang, H.-J., Park, S.-Y., Shin, C. M., et al. (2020). Evidence-based guidelines for the treatment of Helicobacter pylori infection in Korea: 2020 revised edition. Korean J. Helicobacter Up. Gastrointest. Res. 20, 261–287. doi: 10.7704/kjhugr.2020.0045
Kim, T. H., Park, J. M., Cheung, D. Y., and Oh, J. H. (2020). Comparison of 7- and 14-day eradication therapy for Helicobacter pylori with first- and second-line regimen: randomized clinical trial. J. Korean Med. Sci. 35:e33. doi: 10.3346/jkms.2020.35.e33
Kumar, S., Metz, D. C., Kaplan, D. E., and Goldberg, D. S. (2021). Low rates of retesting for eradication of Helicobacter pylori infection after treatment in the veterans health administration. Clin. Gastroenterol. Hepatol. 19, 305.e1–313.e1. doi: 10.1016/j.cgh.2020.03.059
Kwon, Y. H., Jeon, S. W., Nam, S. Y., Lee, H. S., and Park, J. H. (2019). Efficacy of tailored therapy for Helicobacter pylori eradication based on clarithromycin resistance and survey of previous antibiotic exposure: A single-center prospective pilot study. Helicobacter 24:e12585. doi: 10.1111/hel.12585
Lee, Y. C., Chiang, T. H., Chou, C. K., Tu, Y. K., Liao, W. C., Wu, M. S., et al. (2016). Association between Helicobacter pylori eradication and gastric cancer incidence: a systematic review and meta-analysis. Gastroenterology 150, 1113.e5–1124.e5. doi: 10.1053/j.gastro.2016.01.028
Lee, G. H., Lee, K. M., Shin, S. J., Kang, J. K., Noh, C. K., Kim, J. H., et al. (2020). Impact of previous metronidazole exposure on metronidazole-based second-line quadruple therapy for Helicobacter pylori infection. Korean J. Intern. Med. 35, 1094–1103. doi: 10.3904/kjim.2020.174
Lehours, P., Siffré, E., and Mégraud, F. (2011). DPO multiplex PCR as an alternative to culture and susceptibility testing to detect Helicobacter pylori and its resistance to clarithromycin. BMC Gastroenterol. 11:112. doi: 10.1186/1471-230x-11-112
Malfertheiner, P., Bazzoli, F., Delchier, J. C., Celiñski, K., Giguère, M., Rivière, M., et al. (2011). Helicobacter pylori eradication with a capsule containing bismuth subcitrate potassium, metronidazole, and tetracycline given with omeprazole versus clarithromycin-based triple therapy: a randomised, open-label, non-inferiority, phase 3 trial. Lancet 377, 905–913. doi: 10.1016/s0140-6736(11)60020-2
Malfertheiner, P., Megraud, F., O’Morain, C. A., Gisbert, J. P., Kuipers, E. J., Axon, A. T., et al. (2017). Management of Helicobacter pylori infection-the Maastricht V/florence consensus report. Gut 66, 6–30. doi: 10.1136/gutjnl-2016-312288
McNulty, C. A., Lasseter, G., Shaw, I., Nichols, T., D’Arcy, S., Lawson, A. J., et al. (2012). Is Helicobacter pylori antibiotic resistance surveillance needed and how can it be delivered? Aliment. Pharmacol. Ther. 35, 1221–1230. doi: 10.1111/j.1365-2036.2012.05083.x
Megraud, F., Bruyndonckx, R., Coenen, S., Wittkop, L., Huang, T. D., Hoebeke, M., et al. (2021). Helicobacter pylori resistance to antibiotics in Europe in 2018 and its relationship to antibiotic consumption in the community. Gut 70, 1815–1822. doi: 10.1136/gutjnl-2021-324032
Nyssen, O. P., Bordin, D., Tepes, B., Perez-Aisa, A., Vaira, D., Caldas, M., et al. (2021a). European registry on Helicobacter pylori management (Hp-EuReg): patterns and trends in first-line empirical eradication prescription and outcomes of 5 years and 21 533 patients. Gut 70, 40–54. doi: 10.1136/gutjnl-2020-321372
Nyssen, O. P., Perez-Aisa, A., Tepes, B., Castro-Fernandez, M., Kupcinskas, J., Jonaitis, L., et al. (2021b). Adverse event profile during the treatment of Helicobacter pylori: a real-world experience of 22,000 patients from the European Registry on H. pylori management (Hp-EuReg). Am. J. Gastroenterol. 116, 1220–1229. doi: 10.14309/ajg.0000000000001246
Osato, M. S., Reddy, R., Reddy, S. G., Penland, R. L., and Graham, D. Y. (2001). Comparison of the Etest and the NCCLS-approved agar dilution method to detect metronidazole and clarithromycin resistant Helicobacter pylori. Int. J. Antimicrob. Agents 17, 39–44. doi: 10.1016/s0924-8579(00)00320-4
Park, J., Han, E., Lee, S. O., and Kim, D. S. (2017). Antibiotic use in South Korea from 2007 to 2014: a health insurance database-generated time series analysis. PLoS One 12:e0177435. doi: 10.1371/journal.pone.0177435
Posteraro, P., Branca, G., Sanguinetti, M., Ranno, S., Cammarota, G., Rahimi, S., et al. (2006). Rapid detection of clarithromycin resistance in Helicobacter pylori using a PCR-based denaturing HPLC assay. J. Antimicrob. Chemother. 57, 71–78. doi: 10.1093/jac/dki406
Savoldi, A., Carrara, E., Graham, D. Y., Conti, M., and Tacconelli, E. (2018). Prevalence of antibiotic resistance in Helicobacter pylori: a systematic review and meta-analysis in World Health Organization regions. Gastroenterology 155, 1372.e17–1382.e17. doi: 10.1053/j.gastro.2018.07.007
Schubert, J. P., Gehlert, J., Rayner, C. K., Roberts-Thomson, I. C., Costello, S., Mangoni, A. A., et al. (2020). Antibiotic resistance of Helicobacter pylori in Australia and New Zealand: a systematic review and meta-analysis. J. Gastroenterol. Hepatol. 36, 1450–1456. doi: 10.1111/jgh.15352
Shah, S. C., Iyer, P. G., and Moss, S. F. (2021). AGA clinical practice update on the management of refractory Helicobacter pylori infection: expert review. Gastroenterology 160, 1831–1841. doi: 10.1053/j.gastro.2020.11.059
Sugano, K., Tack, J., Kuipers, E. J., Graham, D. Y., El-Omar, E. M., Miura, S., et al. (2015). Kyoto global consensus report on Helicobacter pylori gastritis. Gut 64, 1353–1367. doi: 10.1136/gutjnl-2015-309252
Woo, H. Y., Park, D. I., Park, H., Kim, M. K., Kim, D. H., Kim, I. S., et al. (2009). Dual-priming oligonucleotide-based multiplex PCR for the detection of Helicobacter pylori and determination of clarithromycin resistance with gastric biopsy specimens. Helicobacter 14, 22–28. doi: 10.1111/j.1523-5378.2009.00654.x
Yeo, Y. H., Shiu, S. I., Ho, H. J., Zou, B., Lin, J. T., Wu, M. S., et al. (2018). First-line Helicobacter pylori eradication therapies in countries with high and low clarithromycin resistance: a systematic review and network meta-analysis. Gut 67, 20–27. doi: 10.1136/gutjnl-2016-311868
Keywords: anti-bacterial agents, bismuth quadruple therapy, microbial drug resistance, duration of therapy, eradication rate, Helicobacter infections, metronidazole
Citation: Choe Y, Kim JS, Choi HH, Kim DB, Park JM, Oh JH, Kim TH, Cheung DY, Chung WC, Kim B-W and Kim SS (2022) The Influence of Past Metronidazole Exposure on the Outcome of Helicobacter pylori Eradication. Front. Microbiol. 13:857569. doi: 10.3389/fmicb.2022.857569
Edited by:
Peter Malfertheiner, University Hospital Magdeburg, GermanyReviewed by:
Yi-Chia Lee, National Taiwan University, TaiwanCopyright © 2022 Choe, Kim, Choi, Kim, Park, Oh, Kim, Cheung, Chung, Kim and Kim. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Joon Sung Kim, a2lqb29uc0BjYXRob2xpYy5hYy5rcg==
†ORCID: Younghee Choe, orcid.org/0000-0002-9443-2108
Joon Sung Kim, orcid.org/0000-0001-9158-1012
Jae Myung Park, orcid.org/0000-0002-1534-7467
Jung Hwan Oh, orcid.org/0000-0002-9274-882X
Tae Ho Kim, orcid.org/0000-0003-2015-5176
Dae Young Cheung, orcid.org/0000-0003-4150-3555
Woo Chul Chung, orcid.org/0000-0003-1044-0440
Byung-Wook Kim, orcid.org/0000-0002-2290-4954
Sung Soo Kim, orcid.org/0000-0002-9831-0597
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.