
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Microbiol., 25 April 2022
Sec. Virology
Volume 13 - 2022 | https://doi.org/10.3389/fmicb.2022.802292
This article is part of the Research TopicHuman coronavirus research: 20 Years since the SARS-CoV outbreakView all 11 articles
 Monica Irungbam1†Anubhuti Chitkara1†
Monica Irungbam1†Anubhuti Chitkara1† Vijay Kumar Singh2
Vijay Kumar Singh2 Subash Chandra Sonkar2*Abhisek Dubey1Aastha Bansal1Ritika Shrivastava1Binita Goswami1,2Vikas Manchanda3Sonal Saxena3Ritu Saxena4Sandeep Garg5Farah Husain6Tanmay Talukdar7
Subash Chandra Sonkar2*Abhisek Dubey1Aastha Bansal1Ritika Shrivastava1Binita Goswami1,2Vikas Manchanda3Sonal Saxena3Ritu Saxena4Sandeep Garg5Farah Husain6Tanmay Talukdar7 Dinesh Kumar8
Dinesh Kumar8 Bidhan Chandra Koner1,2*
Bidhan Chandra Koner1,2*
Background: Antibody testing is often used for serosurveillance of coronavirus disease 2019 (COVID-19). Enzyme-linked immunosorbent assay and chemiluminescence-based antibody tests are quite sensitive and specific for such serological testing. Rapid antibody tests against different antigens are developed and effectively used for this purpose. However, their diagnostic efficiency, especially in real-life hospital setting, needs to be evaluated. Thus, the present study was conducted in a dedicated COVID-19 hospital in New Delhi, India, to evaluate the diagnostic efficacy of a rapid antibody kit against the receptor-binding domain (RBD) of the spike protein of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2).
Methods: Sixty COVID-19 confirmed cases by reverse transcriptase–polymerase chain reaction (RT-PCR) were recruited and categorized as early, intermediate, and late cases based on the days passed after their first RT-PCR–positive test report, with 20 subjects in each category. Twenty samples from pre-COVID era and 20 RT-PCR–negative collected during the study period were taken as controls. immunoglobulin M (IgM) and immunoglobulin G (IgG) antibodies against the RBD of the spike (S) protein of SARS-CoV-2 virus were detected by rapid antibody test and compared with the total antibody against the nucleocapsid (N) antigen of SARS-CoV-2 by electrochemiluminescence-based immunoassay (ECLIA).
Results: The detection of IgM against the RBD of the spike protein by rapid kit was less sensitive and less specific for the diagnosis of SARS-CoV-2 infection. However, diagnostic efficacy of IgG by rapid kit was highly sensitive and specific when compared with the total antibody against N antigen measured by ECLIA.
Conclusion: It can be concluded that detection of IgM against the RBD of S protein by rapid kit is less effective, but IgG detection can be used as an effective diagnostic tool for SARS-CoV-2 infection in real-life hospital setting.
The world is facing the outbreak of coronavirus disease 2019 (COVID-19), which has become a public health event of international concern (Afzal, 2020; Dubey et al., 2020, 2021; Feng et al., 2020; He et al., 2020; Nilsson et al., 2021). Accurate and rapid diagnosis of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection is needed for prompt and effective patient care. Quantitative reverse transcriptase–polymerase chain reaction (RT-PCR) is the clinically accepted standard method for molecular diagnosis of SARS-CoV-2 detection. Alternatively, rapid antigen test (RAT) kit is also used for COVID-19 diagnosis. However, RT-PCR test has 70% sensitivity and 95% specificity and poses risks related to specimen collection and sample handling (Long et al., 2020a; Pray et al., 2021). A recent meta-analysis revealed that the average sensitivity and specificity of RAT for SARS-CoV-2 were 56.2 and 99.5%, respectively (Long et al., 2020b). These tests may also be falsely negative due to quality of sample or timing of carrying the test as the viral load in upper respiratory tract secretions peaks in the first week of symptoms, but may decline below the limit of detection in those presenting later. In individuals who have recovered, RT-PCR provides no information about prior exposure or immunity. Addressing this concern, various researchers developed a solution to minimize these risks by assaying immunoglobulin G (IgG) and immunoglobulin M (IgM) against the virus. Serological testing with good detection performance can be used as supplementary diagnosis of COVID-19 suspect cases with negative nucleic acid test result (Young et al., 2020). Also, to diagnose patients after the acute phase of the infection or with atypical clinical presentation with no nasopharyngeal shedding of the virus, serology testing is very useful (Noh et al., 2020; Young et al., 2020; Alsaud et al., 2021). In addition, serological testing provides a useful surveillance tool to track seroprevalence and assess the immune status in a community and may also be useful for decisions on lockdown entry–exit strategies (Parai et al., 2021).
The human body produces specific antibodies after the virus invades. The specific IgM antibody appears first, and then the titer of IgG antibody rises. Thus, the detection of IgM and IgG is believed to be another important diagnostic tool along with RT-PCR and RAT. The tests available detects anti–SARS-CoV-2 immunoglobulins, which are usually formed in the patient’s body at the earliest by 1 week and on average within 2–3 weeks from the onset of infection (Jacofsky et al., 2020; Long et al., 2020a).
Various SARS-CoV-2 serological tests using different targeted antigenic proteins have been available now. Some of them use whole virus lysate, recombinant full S (spike) or N (nucleocapsid) proteins, peptides of the N, or specific domains S1, S2, or RBD (receptor-binding domain) of the S protein. Studies have shown that S and N proteins of the virus are the most immunogenic, and these serological tests can be performed with various techniques (Saif, 1993; Duan et al., 2020). Enzyme-linked immunosorbent assay (ELISA) and chemiluminescence are considered standard methods for the same. Rapid antibody kits are also available as a point-of-care testing tool. This rapid serological test is a simple procedure, needs no special equipment, is relatively cheap, and gives fast results. However, utility of this type of rapid antibody detection kit in the diagnosis of COVID-19 in real-life hospital settings is warranted. This study is conducted to evaluate the sensitivity and specificity of a rapid antibody kit in real-life hospital setting that detects IgM and IgG separately by comparing with the total antibody detection by chemiluminescence method.
The observational study was conducted in the Department of Biochemistry in collaboration with the Multidisciplinary Research Unit, Maulana Azad Medical College and Department of Medicine Lok Nayak Hospital, New Delhi, India, after ethical approval. Ethical approval number of the study is F.1/IEC/MAMC/(81/09/2020/No: 278) dated 24 November 2020. The study was carried out between December 2020 and June 2021.
All the cases included in this study were COVID-19 cases confirmed by RT-PCR. Blood samples sent in red-capped blood collection vials for other biochemical tests were used, and no separate sample from them was collected for the study. Patients were categorized as “early cases” (group I) if they were recruited within the first week of positive RT-PCR test, as “intermediate cases” (group II) if taken between 8 and 14 days, and “late cases” (group III) if recruited after 14 days of their first RT-PCR–positive test. Recruitment continued until 20 samples were collected in each group. Blood sample was collected from 20 RT-PCR–negative subjects who were treated as controls. Twenty serum samples collected during January 2019 to June 2019 and preserved at −80°C were used as pre–COVID-19 era controls. Pre–COVID-19 samples (archived serum sample of pre–COVID-19) was used as negative controls for additional confirmation of test results.
Total antibody against the nucleocapsid (N) antigen of SARS-CoV-2 was assayed from the serum of these samples using electrochemiluminescence (ECL)–based Elecsys® Anti–SARS-CoV-2 immunoassay kit manufactured by Roche Diagnostics adapted to fully automated Cobas e411 immunoassay system. The cut-off indices for positive immunoassay was greater than 1.0 (arbitrary unit) by this method.
The ImmunoQuick COVID-19 kit evaluated in this study was produced by ImmunoScience India Private Limited, Pune, Maharashtra, India. ImmunoQuick COVID-19 was developed using the principle of immunochromatography for the rapid and qualitative detection of IgM and IgG antibodies against the RBD of spike (S) protein of COVID-19 virus in human serum, plasma, or whole blood. In an internal evaluation of the performance characteristics of the rapid kit carried out by the manufacturer, serum, plasma, and whole blood samples of total 125 RT-PCR–negative and 160 RT-PCR COVID-19–positive were used. Sensitivity and specificity were found to be 97.5% (156/160) and 98.4% (123/125), respectively. Cross-reactivity studied with dengue-, HIV-, hepatitis C virus-, and HBsAg-positive serum samples showed no cross-reactivity. Endpoint titer was found satisfactory. External evaluation of the ImmunoQuick COVID-19 IgM/IgG test kit was performed by the National Institute of Virology–Indian Council of Medical Research, Department of Health Research, Government of India at Pune and was found satisfactory as per the Centers for Disease Control and Prevention and World Health Organization guidelines. The manufacturer obtained the regulatory approval for manufacturing the kit from the Central Drugs Standard Control Organization under Directorate General of Health Services, Ministry of Health & Family Welfare, Government of India. The manufacturing of the kit followed the ISO 13485:2016 QMS guidelines. The tests were performed at the Immunoassay Laboratory of Department of Biochemistry, Maulana Azad Medical College, New Delhi, by laboratory technicians/resident doctors immediately after receiving the blood samples by the method described below:
Test cassette, specimens, buffer, and/or controls were allowed to equilibrate to the temperature of an air-conditioned room (20–22°C) prior to testing. The test cassette was removed from the sealed foil pouch and was used as earliest possible. At the time of executing the test, it was made sure that the test device was placed on a clean and level surface. Sample was taken with mini plastic dropper provided in the kit, and one drop of it was transferred to the specimen well (marked as S on the cassette) of the test device. Then two drops of sample buffer were added to the buffer well (B) immediately, and air bubbles were avoided while dispensing it. As the fluid migrates through the membrane on which antigens are impregnated, the color line(s) develop. The results were read within 10 min. The results were visible as soon as 2 min. The result was read as negative when the colored line in the control line region (C) changed from blue to red and no line appeared in the test line regions M or G. The test result indicated the presence of IgM anti–SARS-CoV-2 antibodies when the colored line in the control line region (C) changed from blue to red and a colored line appeared in the test line region M. The test result indicated the presence of IgG anti–SARS-CoV-2 antibodies when the colored line in the control line region (C) changed from blue to red and a colored line appeared in the test line region G. The test results indicated the presence of IgM and IgG anti–SARS-CoV-2 antibodies when the colored line in the control line region (C) changed from blue to red and two colored lines appear in the test line regions M and G. The result was considered as invalid when the control line was partially red and failed to completely change from blue to red. Insufficient specimen volume or incorrect procedural techniques were the most likely reasons for control line failure. During the study, we never encountered any invalid test result.
Data of the test results were arranged in the table as follows:
Specificity, sensitivity, negative predictive value (NPV), and positive predictive value (PPV) of anti-RBD IgM and IgG were calculated from a 2 × 2 table using formulas as follows:
The strength of the agreement of the two methods was calculated by using the Cohen κ index. Results were interpreted according to the following κ values: (i) 0.01–0.20, slight agreement; (ii) 0.21–0.40, fair agreement; (iii) 0.41–0.60, moderate agreement; (iv) 0.61–0.80, substantial agreement; and (v) 0.81–1.00, perfect agreement. p < 0.05 was considered statistically significant for all statistical tests.
Of the 60 patients enrolled in the study, patients were having mild, moderate, or severe COVID-19 and were divided into three groups as early, intermediate, and late cases as previously mentioned. Male-to-female ratio was 14:6 in group I, 16:4 in group II, and 15:5 in group III. Gender difference in these groups was statistically insignificant. The ages of the participants in the study groups ranged from 21 to 68 years, with no statistically significant difference among the groups. Of 100 participants, 16% were smokers, and 10% were smokers and alcoholic as well. The distribution of comorbid conditions in different groups is shown in Table 1.
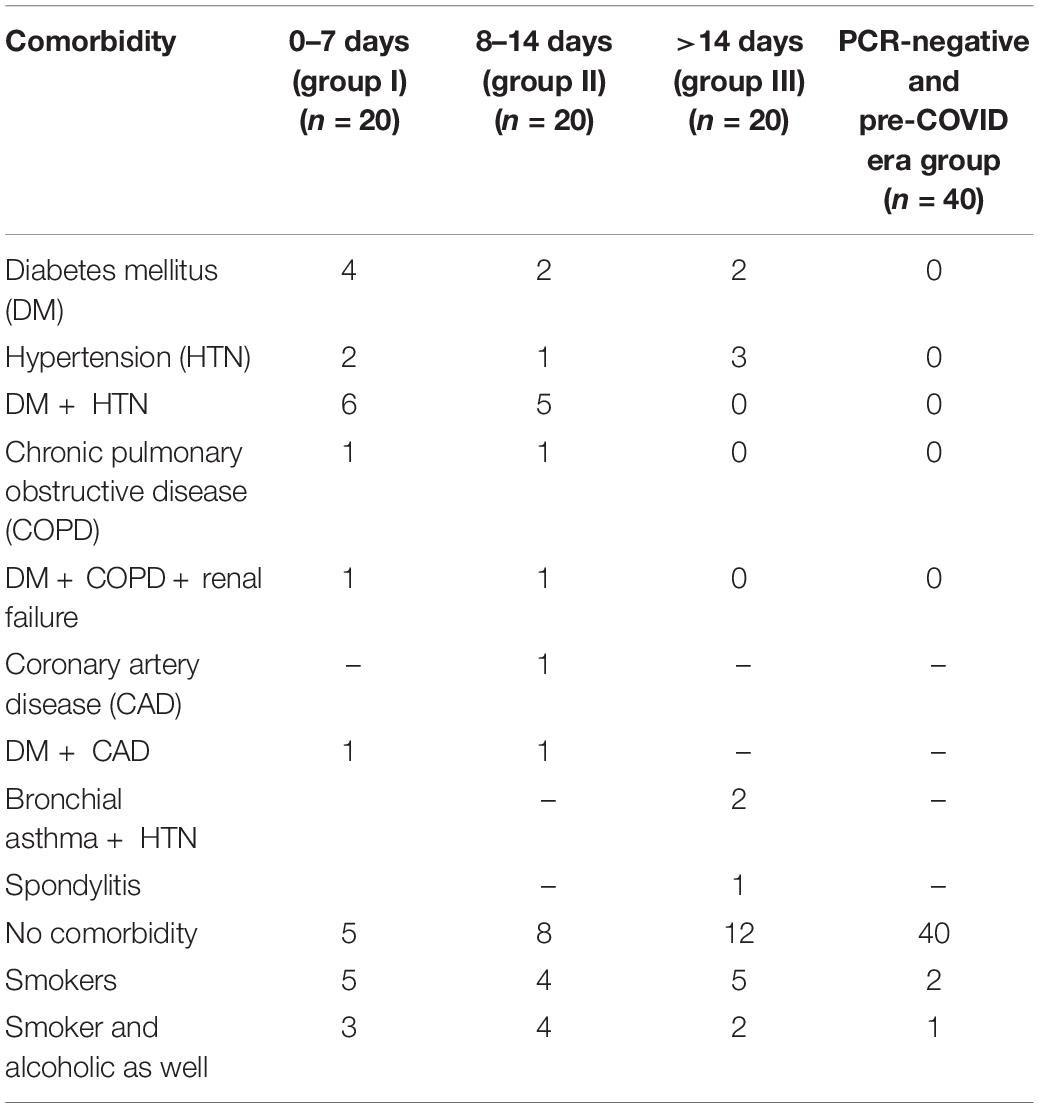
Table 1. Distribution of various comorbidities among different study groups.
The results of total antibody positive (level >1.0) and negative (level <1.0) against N protein of SARS-CoV-2 virus and achieved pre-COVID era non-COVID samples by ECL-based immunoassay (ECLIA) are presented in Table 2.

Table 2. Distribution of total antibody against nucleocapsid protein of SARS-CoV-2 test results at 0–7, 8–14, and >14 days of RT-PCR–positive confirmed COVID-19 cases, PCR-negative subjects, and pre–COVID-19 controls.
The present study was designed to evaluate the diagnostic efficacy of a rapid antibody kit against the RBD of the S protein of COVID-19 in a real-life hospital setting. Among the diagnostic immunoassay methods, chemiluminescence-based immunoassay (CLIA) is considered to be very sensitive and effective. In the present study, diagnostic efficacy of total antibody assay against nucleocapsid protein by ECL method in the early, intermediate, and late cases was performed. Tables 2, 3 show that during first 7 days after PCR positivity, the sensitivity, specificity, PPV, and NPV of ECLIA-based antibody assay were 80, 100, 100, and 83.3%, respectively; between 8 and 14 days after PCR positivity, those were 95, 100, 95, and 95.2%, respectively, and for late cases, those were 100% for all indices. This indicates that ECLIA is a very effective diagnostic tool for COVID-19, and its efficacy after 7 days is very close to that of RT-PCR. Even within 7 days, it was found to be very effective. Thus, for comparison of any other antibody testing method for COVID-19, ECLIA-based immunoassay of total antibody against nucleocapsid protein can be considered as a standard method.
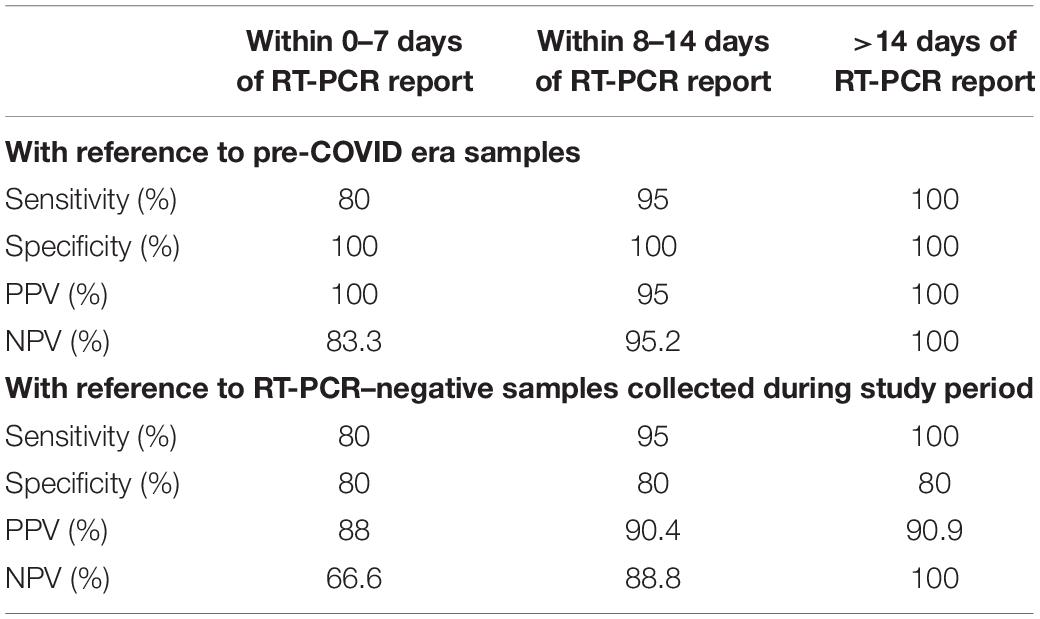
Table 3. Accuracy indices of total antibody assay against nucleocapsid protein by ECLIA at 0–7, 8–14, and >14 days of COVID diagnosis by RT-PCR with reference to pre-COVID era samples and RT-PCR–negative samples collected during the study period.
For the assessment of seroprevalence, most of the authorities recommend antibody assay either by ELISA or CLIA-based methods. The manufacturers of rapid antibody assays claim that rapid test is also effective in serosurveillance particularly in remote areas where there are no laboratory facilities. However, the diagnostic efficacy of these rapid antibody kit has also been evaluated in standard laboratory conditions (Li et al., 2020; Zhang et al., 2020), but not in real-life hospital settings treating COVID-19 patients. Performance evaluation in real-life situation is an important component of postmarket surveillance. There are limited data to prove their efficacy in the hospital setting. Thus, in this study, we tried that in a dedicated COVID hospital.
Tables 4, 5 show that the assay of IgM by rapid kit has sensitivity of 37.5% for early cases and 31.6% for intermediate cases, although specificity and PPV were 100%. NPV was found to be 28 and 7.14%, and Cohen κ was 0.1935 and 0.044, respectively. After 14 days, as expected, IgM antibody by rapid kit was undetectable because of class switching of the antibody. Hence, we conclude that IgM detection by rapid kit has very limited effectiveness as a diagnostic tool for COVID-19 in real-life hospital setting.
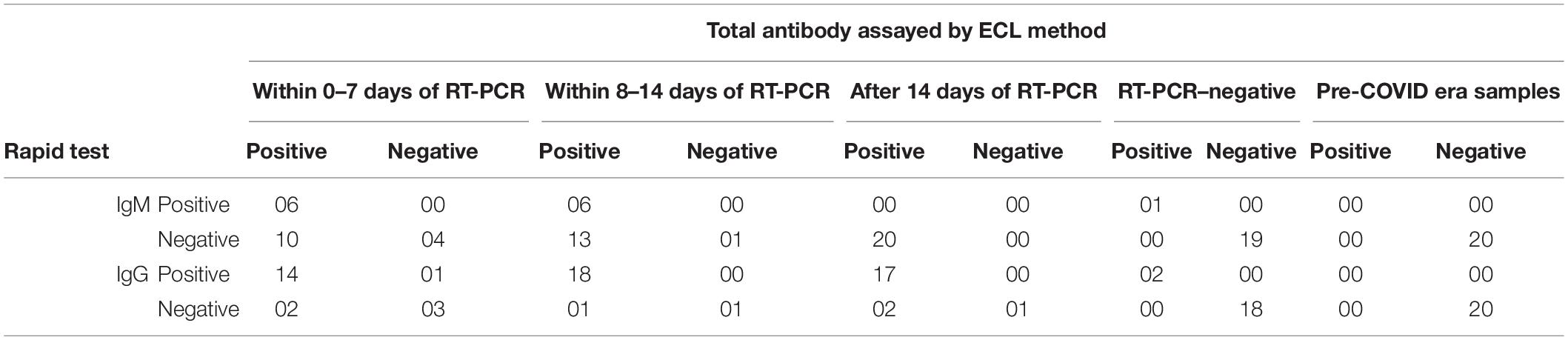
Table 4. Table showing distribution of positive and negative antibody test results by rapid test kit and ECLIA method on samples collected from COVID patients at 0–7, 8–14, and after 14 days of RT-PCR–positive and RT-PCR–negative subjects and pre-COVID samples.
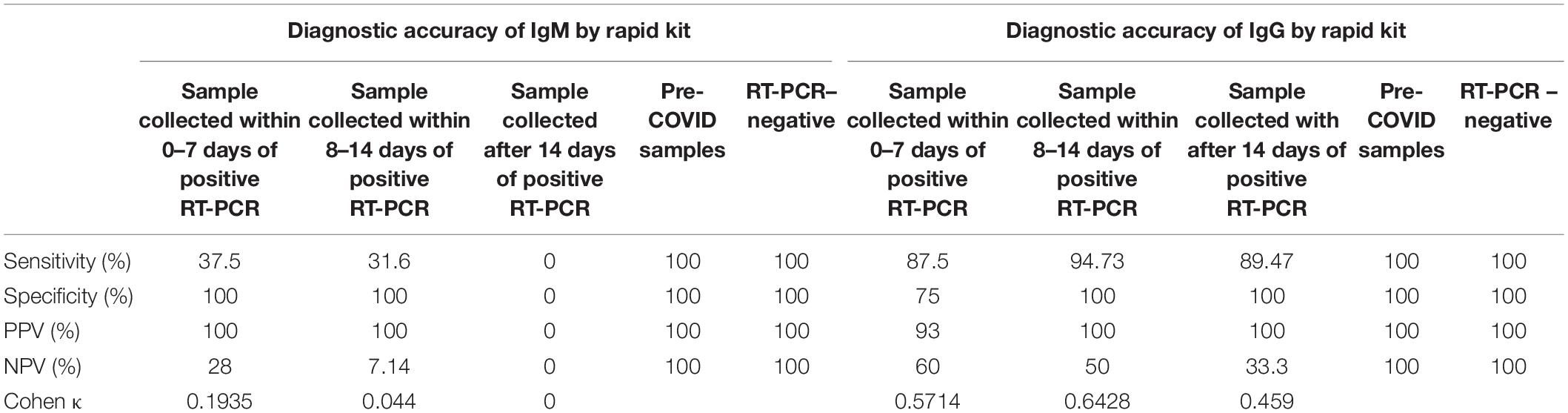
Table 5. Accuracy indices of IgM and IgG antibody (against the RBD of the spike protein of SARS-CoV-2 virus) by rapid test for the diagnosis of COVID-19 (calculated by taking total antibody levels by ECL as standard methods.
As shown in Tables 4, 5, detection of IgG by rapid kit for early intermediate and late cases was 87.5, 94.7, and 89.5%, respectively, and specificity was 75, 100, and 100%, respectively. Similarly, PPV was 93, 100, and 100%, respectively; NPV was 60, 50, and 33.3%, respectively; and Cohen κ was 0.5714, 0.6428, and 0.459, respectively. This indicates that IgG detection is effective enough in the diagnosis of COVID-19 in the hospital setting. Even within 0–7 days, its sensitivity and specificity were high, indicating a possible early class switching of antibody against the RBD of the spike protein. These observations go against the contention that antibody detection or assay best suits the serosurveillance and not the diagnosis. From this, we conclude that the efficacy of IgG against the RBD of the spike protein is as effective as that by CLIA and can be utilized in the hospital setting. However, combining IgM detection with IgG does not improve the diagnostic efficacy and hence is a mere wastage of resources. Thus, we recommend IgG (against the RBD of S protein) assay by rapid kit in the diagnosis of COVID-19 for the screening of suspected patients where RT-PCR or CLIA-based antibody assay facility is not available. Even a variation in performances of assays is likely to exist when diagnosing different populations such as individuals with different diet habits, mental well-being, and so on (Soni et al., 2020a,b, c; Mehta et al., 2021).
However, the limitation of the present study is that while evaluating rapid test, we evaluated the detection of antibody against the RBD of the spike protein of SARS-CoV-2 virus but took assay of total antibody against a different one, that is, nucleocapsid (N) protein, as our standard reference method. Another limitation is that the study was conducted in only one hospital of New Delhi involving a limited number of samples from the local population. Immune response being variable in different populations, its applicability in other populations is worth evaluating.
The original contributions presented in the study are included in the article. Further inquiries can be directed to the corresponding author/s.
BK, BG, AC, SCS, SG, FH, SS, and VM conceived and designed the experiments. MI, VS, AB, AD, SCS, and RSh carried out the experiments. MI, VS, AB, and AD contributed to collection of clinical samples. AC, SCS, BG, and BK performed the analysis and analyzed the data. MI, AC, SCS, BG, and BK wrote and finalized the manuscript. BK, DK, and TT contributed to resources. All authors read and approved the final manuscript.
The infrastructure of multidisciplinary research unit (MRU) at Maulana Azad Medical College, New Delhi which is funded by the Department of Health Research, Ministry of Health and Family Welfare, Government of India was used for carrying out the experiments for the study.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Afzal, A. (2020). Molecular diagnostic technologies for COVID-19: limitations and challenges. J. Adv. Res. 26, 149–159. doi: 10.1016/j.jare.2020.08.002
Alsaud, A. E., Nair, A. P., Matarneh, A. S., Sasi, S., El Hassan, R., Khan, F., et al. (2021). Case report: prolonged viral shedding in six COVID-19 patients. Am. J. Trop. Med. Hyg. 104, 1472–1475. doi: 10.4269/ajtmh.20-0933
Duan, L., Zheng, Q., Zhang, H., Niu, Y., Lou, Y., and Wang, H. (2020). The SARS-CoV-2 spike glycoprotein biosynthesis, structure, function, and antigenicity: implications for the design of spike–based vaccine immunogens. Front. Immunol. 11:576622. doi: 10.3389/fimmu.2020.576622
Dubey, A., Bansal, A., Sonkar, S. C., Goswami, B., Makwane, N., Manchanda, V., et al. (2020). In–house assembled protective devices in laboratory safety against SARS-nCoV-2 in clinical biochemistry laboratory of a COVID dedicated hospital. medRxiv [Preprint] medRxiv 2020 08.24.20155713, doi: 10.1101/2020.08.24.20155713
Dubey, A., Kotnala, G., Mandal, T. K., Sonkar, S. C., Singh, V. K., Guru, S. A., et al. (2021). Evidence of the presence of SARS-CoV-2 virus in atmospheric air and surfaces of a dedicated COVID hospital. J. Med. Virol. 93, 5339–5349. doi: 10.1002/jmv.27029
Feng, W., Newbigging, A. M., Le, C., Pang, B., Peng, H., Cao, Y., et al. (2020). Molecular diagnosis of COVID-19: challenges and research needs. Anal. Chem. 92, 10196–10209.
He, J., Hu, P., Gao, Y., Zheng, S., Xu, C., Liu, R., et al. (2020). Comparison and application of different immunoassay methods for the detection of SARS-CoV-2. J. Med. Virol. 92, 2777–2784. doi: 10.1002/jmv.26187
Jacofsky, D., Jacofsky, E. M., and Jacofsky, M. (2020). Understanding antibody testing for COVID-19. J Arthroplasty. 35, S74–S81.
Li, Z., Yi, Y., Luo, X., Xiong, N., Liu, Y., Li, S., et al. (2020). Development and clinical application of a rapid IgM–IgG combined antibody test for SARS-CoV-2 infection diagnosis. J. Med. Virol. 92, 1518–1524. doi: 10.1002/jmv.25727
Long, Q.-X., Liu, B.-Z., Deng, H.-J., Wu, G.-C., Deng, K., Chen, Y.-K., et al. (2020a). Antibody responses to SARS-CoV-2 in patients with COVID-19. Nat. Med. 26, 845–848.
Long, Q.-X., Tang, X.-J., Shi, Q.-L., Li, Q., Deng, H.-J., Yuan, J., et al. (2020b). Clinical and immunological assessment of asymptomatic SARS-CoV-2 infections. Nat. Med. 26, 1200–1204. doi: 10.1038/s41591-020-0965-6
Mehta, A., Soni, V. K., Sharma, K., Ratre, Y. K., Shukla, D., Singh, A. K., et al. (2021). Finding horcrux of psychiatric symptoms in COVID-19: deficiencies of amino acids and vitamin D. Asian J. Psychiatr. 55:102523. doi: 10.1016/j.ajp.2020.102523
Nilsson, A. C., Holm, D. K., Justesen, U. S., Gorm-Jensen, T., Andersen, N. S., Øvrehus, A., et al. (2021). Comparison of six commercially available SARS-CoV-2 antibody assays–choice of assay depends on intended use. Int. J. Infect. Dis. 103, 381–388. doi: 10.1016/j.ijid.2020.12.017
Noh, J. Y., Yoon, J. G., Seong, H., Choi, W. S., Sohn, J. W., Cheong, H. J., et al. (2020). Asymptomatic infection and atypical manifestations of COVID-19: comparison of viral shedding duration. J. Infect. 81, 816–846. doi: 10.1016/j.jinf.2020.05.035
Parai, D., Dash, G. C., Choudhary, H. R., Peter, A., Rout, U. K., Nanda, R. R., et al. (2021). Diagnostic accuracy comparison of three fully automated chemiluminescent immunoassay platforms for the detection of SARS-CoV-2 antibodies. J. Virol Methods 292:114121. doi: 10.1016/j.jviromet.2021.114121
Pray, I. W., Ford, L., Cole, D., Lee, C., Bigouette, J. P., Abedi, G. R., et al. (2021). Performance of an antigen–based test for asymptomatic and symptomatic SARS-CoV-2 testing at two university campuses – wisconsin, September–October 2020. MMWR Morb. Mortal. Wkly. Rep. 69, 1642–1647. doi: 10.15585/mmwr.mm695152a3
Soni, V. K., Mehta, A., Ratre, Y. K., Tiwari, A. K., Amit, A., Singh, R. P., et al. (2020a). Curcumin, a traditional spice component, can hold the promise against COVID-19? Eur. J. Pharmacol. 886:173551. doi: 10.1016/j.ejphar.2020.173551
Soni, V. K., Mehta, A., Shukla, D., Kumar, S., and Vishvakarma, N. K. (2020b). Fight COVID-19 depression with immunity booster: curcumin for psychoneuroimmunomodulation. Asian J. Psychiatr. 53:102378. doi: 10.1016/j.ajp.2020.102378
Soni, V. K., Shukla, D., Kumar, A., and Vishvakarma, N. K. (2020c). Curcumin circumvent lactate–induced chemoresistance in hepatic cancer cells through modulation of hydroxycarboxylic acid receptor-1. Int. J. Biochem. Cell Biol. 123:105752. doi: 10.1016/j.biocel.2020.105752
Young, B. E., Ong, S. W. X., Kalimuddin, S., Low, J. G., Tan, S. Y., Loh, J., et al. (2020). Epidemiologic features and clinical course of patients infected with SARS-CoV-2 in Singapore. JAMA 323, 1488–1494. doi: 10.1001/jama.2020.3204
Keywords: SARS-CoV-2, COVID-19, receptor-binding domain (RBD), spike surface glycoprotein, chemiluminescence analysis, rapid antibody tests for COVID-19
Citation: Irungbam M, Chitkara A, Singh VK, Sonkar SC, Dubey A, Bansal A, Shrivastava R, Goswami B, Manchanda V, Saxena S, Saxena R, Garg S, Husain F, Talukdar T, Kumar D and Koner BC (2022) Evaluation of Performance of Detection of Immunoglobulin G and Immunoglobulin M Antibody Against Spike Protein of SARS-CoV-2 by a Rapid Kit in a Real-Life Hospital Setting. Front. Microbiol. 13:802292. doi: 10.3389/fmicb.2022.802292
Received: 26 October 2021; Accepted: 26 January 2022;
Published: 25 April 2022.
Edited by:
Sunil Kumar Lal, Monash University Malaysia, MalaysiaReviewed by:
Ajay Kumar, Banaras Hindu University, IndiaCopyright © 2022 Irungbam, Chitkara, Singh, Sonkar, Dubey, Bansal, Shrivastava, Goswami, Manchanda, Saxena, Saxena, Garg, Husain, Talukdar, Kumar and Koner. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Subash Chandra Sonkar, ZHJzY3NvbmthckBnbWFpbC5jb20=; Bidhan Chandra Koner, YmNrb25lckBob3RtYWlsLmNvbQ==
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.