
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Microbiol., 14 December 2021
Sec. Antimicrobials, Resistance and Chemotherapy
Volume 12 - 2021 | https://doi.org/10.3389/fmicb.2021.777054
This article is part of the Research TopicCarbapenemases in Gram-negative Bacteria: A Global Health Threat and Therapeutic ChallengeView all 19 articles
 Daniela Gonçalves1,2,3,4†
Daniela Gonçalves1,2,3,4† Pedro Cecílio1†Alberta Faustino5Carmen Iglesias5Fernando Branca5Alexandra Estrada5
Pedro Cecílio1†Alberta Faustino5Carmen Iglesias5Fernando Branca5Alexandra Estrada5 Helena Ferreira1,2*
Helena Ferreira1,2*The emergence of infections (and colonization) with Enterobacteriaceae-producing carbapenemases is a threatening public health problem. In the last decades, we watched an isolated case becoming a brutal outbreak, a sporadic description becoming an endemic problem. The present study aims to highlight the dissemination of IMP-22-producing Klebsiella pneumoniae in the North of Portugal, through the phenotypic and genotypic characterization of isolates collected from hospitalized patients (n=5) and out-patients of the emergency ward of the same acute care hospital (n=2), and isolates responsible for the intestinal colonization of residents in a Long-Term Care Facility (n=4). Pulsed-field gel electrophoresis (PFGE) results, associated with conjugation experiments pointed to a pattern of both vertical and horizontal dissemination. Overall, and complementing other studies that give relevance to IMP-22-producing K. pneumoniae in the clinical settings, here we show for the first time the public health threatening breach of the hospital frontier of this resistance threat, toward the community.
Antimicrobial resistance is among the major public health problems of the 21st century. In 2015 the World Health Organization launched the “Global Action Plan on Antimicrobial Resistance” (giving great relevance to antibiotics) to respond to this global issue on five fronts (WHO, 2015). Still, each year, only in the United States and the European Union, 50,000 individuals die due to antibiotic therapy failure (CDC, 2019). Even considering the “last-line” treatment options for infections caused by resistant Enterobacteriaceae, carbapenems, we know today several enzymes that can effectively hydrolyze their β-lactam ring, and consequently, compromise their activity (Queenan and Bush, 2007).
Carbapenemases can be divided into two different groups according to their dependency on cations for enzyme activity: serine/non-metallo- (zinc-independent; classes A, C, and D) and metallo-carbapenemases (MBLs; zinc-dependent; class B; Queenan and Bush, 2007). Within the latter, a versatile family of beta-lactamases often associated with Enterobacteriaceae, the VIM, IMP, and NDM types are the most relevant carbapenemases globally (Poirel et al., 2011; Nordmann, 2014). Interestingly VIM and IMP are so well settled, that they are considered an endemic problem in the Mediterranean basin (Poirel et al., 2011; Pitout et al., 2015). However, in Portugal, the occurrence of MBL-producing Enterobacteriaceae in the clinical settings is apparently not common; only a few sporadic cases were reported, including a VIM-34-producing Klebsiella pneumoniae (Rodrigues et al., 2014) and a VIM-2-producing Klebsiella oxytoca (Conceicao et al., 2005). In fact, recent studies confirmed that among carbapenemase-producing Enterobacteriaceae (CPE), MBL-producing bacteria only represent 5% in Portugal (Manageiro et al., 2018; Gorgulho et al., 2020).
IMP-22 was first described in Italy in two non-related environmental strains of Pseudomonas fluorescens as well as in one clinical isolate of Pseudomonas aeruginosa (Pellegrini et al., 2009). Since the first description, the same enzyme was then described also in a Pseudomonas spp. single clinical isolate from Austria (Duljasz et al., 2009) and recently emerged in Spain, always in the clinics, associated first with P. aeruginosa (Viedma et al., 2012) and then mainly with K. pneumoniae (Miro et al., 2013; Pena et al., 2014) but also with E. coli (Ortega et al., 2016).
Here, we report and describe the successful installation of IMP-22-producing K. pneumoniae in a Portuguese acute care hospital (in the North of Portugal), due to both vertical and horizontal dissemination. Furthermore, we describe for the first time the breach of the hospital frontier, with the detection and characterization of an IMP-22-producing K. pneumoniae isolate, via the screening of intestinal colonizers of residents of a long-term care facility (LTCF). These results ultimately highlight the circulation of patients between hospital and extra-hospital care settings as the most probable justification for the “dissemination of multiresistant bacteria toward the community.”
This study was performed in the context of one of the largest acute care hospitals in the North of Portugal (705 beds), covering a population of 1.2 million people (hereafter called Hospital A). During a one-year study period (from March 2011 to May 2012) K. pneumoniae clinical isolates showing reduced susceptibility to carbapenems (imipenem or ertapenem or meropenem) were identified as part of routine diagnostics in the hospital Clinical Pathology Service. Isolates were collected from both inpatients admitted to the internal medicine service and from patients admitted to the hospital emergency ward.
An extra-hospital healthcare institution for dependent and old people in the North of Portugal was studied. The LTCF with 54 beds has three different typologies of care: long-term maintenance (LTM, 22 beds), medium-term and rehabilitation (MTR, 22 beds), and palliative care (PC, 10 beds). The institution is located in the same geographic area as Hospital A (distance of 4 Km), and consequently, the circulation of patients between these two healthcare institutions occurs frequently.
Thirty-eight fecal samples from LTCF residents were collected between January and February 2012, suspended in Brain Heart Infusion (BHI; Oxoid, Hampshire, United Kingdom), and incubated overnight at 37°C. The enriched suspensions were then plated onto MacConkey agar plates (Oxoid, Hampshire, United Kingdom) supplemented with meropenem (1mg/l). Isolates that grew in the selective media were re-inoculated in a new plate to exclude any satellite growers (maximum of four random colonies per plate).
The clinical isolates were identified using the Vitek® 2 automated system (bioMérieux, Marcy l’Étoile, France). Bacteria isolated as part of the intestinal colonization screening were identified using the bacterial identification biochemical galleries API® 20E and ID®32GN (bioMérieux).
The antimicrobial susceptibility of clinical isolates was assessed through the determination of the minimum inhibitory concentration (MIC) of different antimicrobial agents, performed using the Vitek® 2 (bioMérieux) and/or WalkAway (Beckman Coulter, Brea, CA, United States) automated systems. The MICs detected for ampicillin, piperacillin, ticarcillin, amoxicillin + clavulanic acid, piperacillin + tazobactam, ticarcillin + clavulanic acid, cephalothin, cefuroxime, ceftazidime, cefotaxime, cefepime, aztreonam, imipenem, ertapenem, meropenem (β-lactams), gentamicin, tobramycin, amikacin, minocycline, ciprofloxacin, levofloxacin, pefloxacin, nitrofurantoin, trimethoprim + sulfamethoxazole, and rifampicin (non-β-lactams) were interpreted into susceptible, intermediate susceptible or resistant according to the clinical and laboratory standards institute (CLSI) guidelines (Queenan and Bush, 2007; Supplementary Table S1). For isolates collected in the LTCF intestinal colonization screening, antimicrobial susceptibility was determined by disk-diffusion methods; susceptibility to both β-lactams [ampicillin (10μg), amoxicillin + clavulanic acid (20+10μg), ceftazidime (30μg), cefotaxime (30μg), cefepime (30μg), cefoxitin (30μg), aztreonam (30μg), imipenem (10μg), ertapenem (10μg), and meropenem (10μg)] and non-β-lactam antibiotics [streptomycin (10μg), gentamicin (10μg), netilmicin (30μg), tobramycin (10μg), amikacin (30μg), tetracycline (30μg), nalidixic acid (30μg), ciprofloxacin (5μg), nitrofurantoin (300μg), chloramphenicol (30μg), tigecycline (15μg), and trimethoprim + sulfamethoxazole (1.25/23.75μg)] was defined according to the CLSI guidelines (CLSI, 2013) or the EUCAST criteria in the case of tigecycline1 (Supplementary Table S2).
An initial carbapenemase production screening (MBLs) was performed using the double disk synergism method (DDSM) - IMP (10μg) versus IMP (10μg)+EDTA (0,5M), followed by the confirmatory MBL E-test IP/IPI [(MIC determination; IMP (4-256μg/ml) versus IMP (1-364μg/ml)+EDTA (constant level)] (bioMérieux, Marcy l’Étoile, France). The E-test was considered MBL suggestive when the MIC ratio of imipenem/imipenem plus EDTA was ≥8 and/or when the presence of a phantom zone or deformation of the inhibitory ellipse was observed. The modified hodge test (MHT) was performed in parallel, to screen for non-MBL carbapenemase production. Briefly, an imipenem disk (10μg) was placed at the center of a Müeller-Hinton agar plate (Oxoid, Hampshire, United Kingdom), previously inoculated with E. coli ATCC 25922, and the clinical isolates were streaked heavily from the edge of the disk toward the edge of the plate. The MHT was considered positive when E. coli growth was observed within the usual inhibition zone of the imipenem disk (CLSI, 2013). As a final confirmatory step the biochemical Blue-Carba test was performed as described elsewhere (Pires et al., 2013).
Total DNA was extracted from all isolates via the boiling of single bacterial colony suspensions for 10min, followed by a 5min centrifugation step at 15,000rpm. The supernatant was then collected and stored at 4°C until further use. Relevant beta-lactamase [blaTEM, blaOXA, blaSHV (Dallenne et al., 2010), and blaCTX-M group 1 (Machado et al., 2005)] and carbapenemase [blaVIM, blaIMP, blaKPC, blaOXA-48, and blaNDM (Poirel et al., 2011)] genes were screened using the primers and amplification conditions described in the literature (Machado et al., 2005; Dallenne et al., 2010; Poirel et al., 2011; Goncalves et al., 2016; Teixeira et al., 2016). Whenever relevant, amplicons were sequenced using the ABI-PRISM 3100 automatic genetic analyzer (Thermo Fischer Scientific, Waltham, MA, United States). Sequence analysis and alignment were performed using the National Center for Biotechnology Information tool.2 As a final confirmation step, IMP-22 specific primers were used (Pellegrini et al., 2009). A compilation of all primer sequences used in this study can be found in (Goncalves et al., 2016).
The clonal relationships of the K. pneumoniae clinical isolates were studied via pulsed-field gel electrophoresis (PFGE), after total genomic DNA digestion with XbaI (Gautom, 1997). Briefly, carbapenem-resistant clinical isolates were cultured in brain heart infusion (BHI) for 24h at 37°C, then “trapped” into 1.6% agarose plugs. A lysis step was performed at 54°C for 2h (50mm Tris, 50mm EDTA, 1% N-lauryl-sarcosine, 0.1 mg/ml proteinase K, pH 8.0), followed by 2–3 washing cycles, and afterward, the digestion overnight with 30U of XbaI at 37°C. Total DNA digests were separated on 1.0% agarose gels (SeaKem Gold Agarose, Lonza, Basel, Switzerland) via PFGE using the CHEFF DR III system (Bio-Rad Laboratories, Hercules, CA, United States) and the following conditions: electric field strength of 6V/cm2 (200V), 14°C, and pulse time of 15s–25s for 16h. After electrophoresis, the gels were stained with ethidium bromide (10μg/ml) for 30min and watched under a UV light (Bio-Rad Laboratories). Data analysis was performed using the BIONUMERICS software, version 8.0 (bioMérieux, Marcy l’Étoile, France); the UPGMA algorithm based on the Dice coefficient (1.0% band tolerance; 1.0% optimization) was applied. The PFGE profiles were defined on the basis of DNA banding patterns in accordance with the criteria defined by Tenover et al. (1995). Isolates with a pattern similarity profile above ≥80% were considered identical.
Conjugation experiments were performed to investigate the transfer of carbapenem resistance determinants. E. coli HB101 (azide resistant, lactose-negative) was used as the recipient strain. Donor and recipient bacterial strains were individually grown overnight in Trypticase Soy Broth (TSB; Oxoid, Hampshire, United Kingdom) and drops of donor and recipient bacterial suspensions were then mixed on the surface of a Müeller-Hinton Agar plate (Oxoid) and re-incubated at 37°C for 24h. The resulting bacterial growth was re-inoculated on Müeller-Hinton medium supplemented with meropenem or ceftazidime (10mg/l) and azide (100μg/ml) and incubated for a maximum of 72h at 37°C. Growing colonies on the selective medium were randomly chosen and inoculated in MacConkey agar (Oxoid) to assess lactose fermentation. Lactose non-fermenters were subjected to antimicrobial susceptibility determination and to genotypic characterization as above stated.
This research was conducted in accordance with the Declaration of Helsinki Ethical Principles. This study was approved by the Ethics Committee of Hospital de Braga, Braga, Portugal. Additionally, human fecal sample collection was performed in accordance with the Good Clinical Practice guidelines; the LTCF direction provided the necessary authorization to conduct this study. Of note, all of the study participants provided written informed consent.
Eight carbapenem-resistant K. pneumoniae showing reduced susceptibility to at least one of the carbapenems tested were isolated from different biological samples of seven distinct hospitalized patients: five inpatients of the internal medicine service of Hospital A and two patients admitted to the emergency ward of the same hospital. The most common type of biological sample from which these bacteria were isolated was sputum (n=5), followed by urine (n=2) and blood (n=1; Table 1). Two of the carbapenem-resistant K. pneumoniae (isolates H13 and H50) were isolated from the same patient (patient 3) in different periods (December 2011 and April 2012, respectively; Table 1). The patients were mostly elderly (median age 74years; range 36–92years) with distinct underlying illnesses, namely urinary tract infection (n=1), endocarditis (n=1), renal insufficiency (n=2), brain tumor (n=1), nosocomial pneumonia (n=1), acute pancreatitis (n=1), respiratory insufficiency (n=2), and bladder tumor (n=1; Table 1). All of the patients had previous hospitalization history in Hospital A, with many of them spending prolonged periods at the internal medicine ward. Of note, patients 3, 6, and 7 received meropenem therapy during their hospitalization period (Table 1).
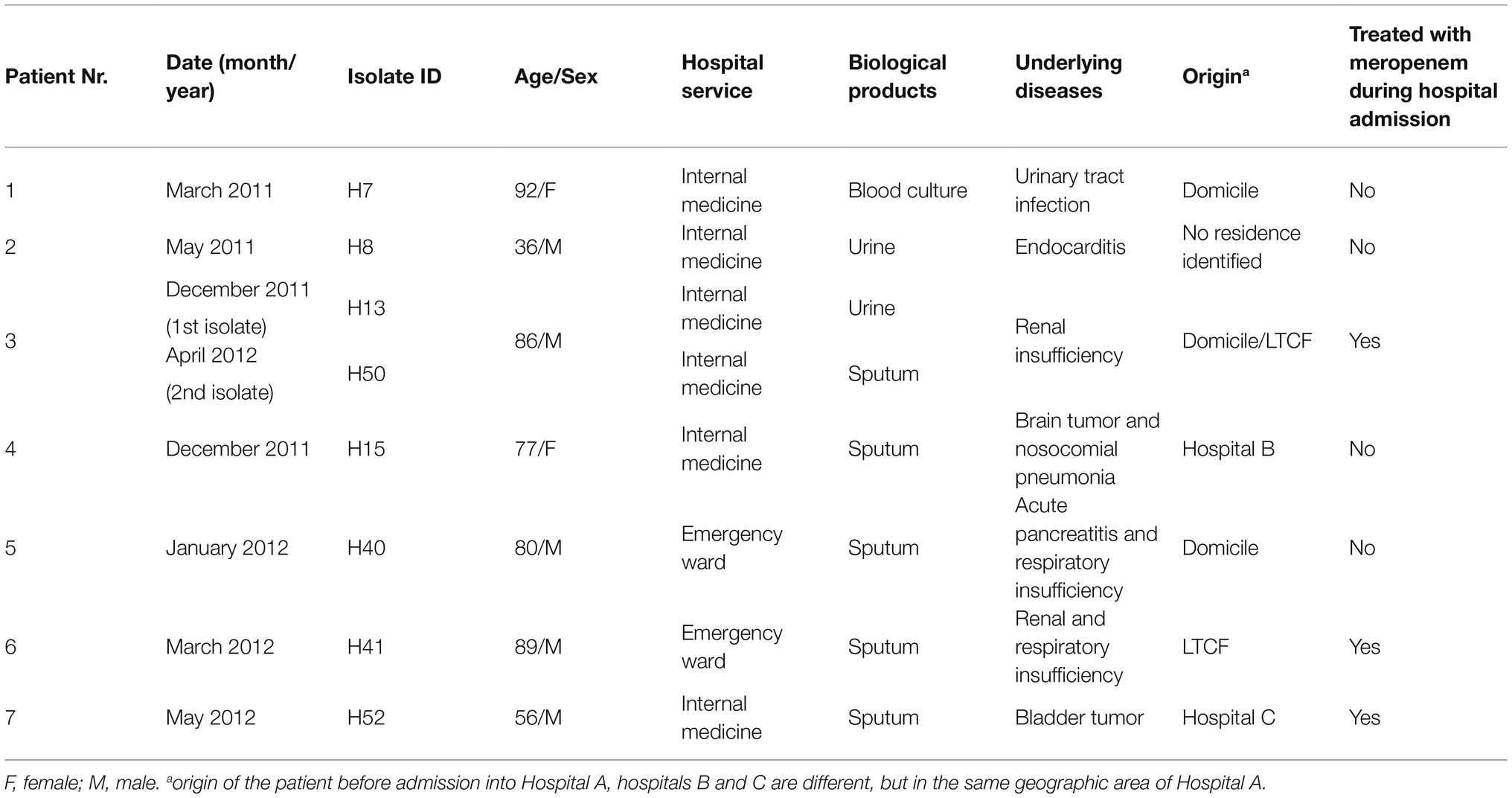
Table 1. Hospital K. pneumoniae isolates: clinical context.
Four carbapenem-resistant K. pneumoniae isolates (10.53%, 4/38) with reduced susceptibility to imipenem were detected in fecal samples of residents of a LTCF (two different typologies of care; LTM, n=3; MTR, n=1; Table 2). The four residents colonized with carbapenem-resistant bacteria were mostly elderly (median age 72.5years; range 63–82years), with previous history of stroke (n=2), stroke associated with other pathologies (endocarditis and pneumonia; n=1), and chronic renal insufficiency (n=1; Table 2). Three of them had recent hospitalization history in Hospital A: two spent prolonged periods in the internal medicine ward (residents A and D) while the third one was admitted to the orthopedics service (resident B). The fourth resident (C) had hospitalization history in three different hospitals in the same geographic area of Hospital A (one hospital in Braga district and two hospitals in Porto district; Table 2).
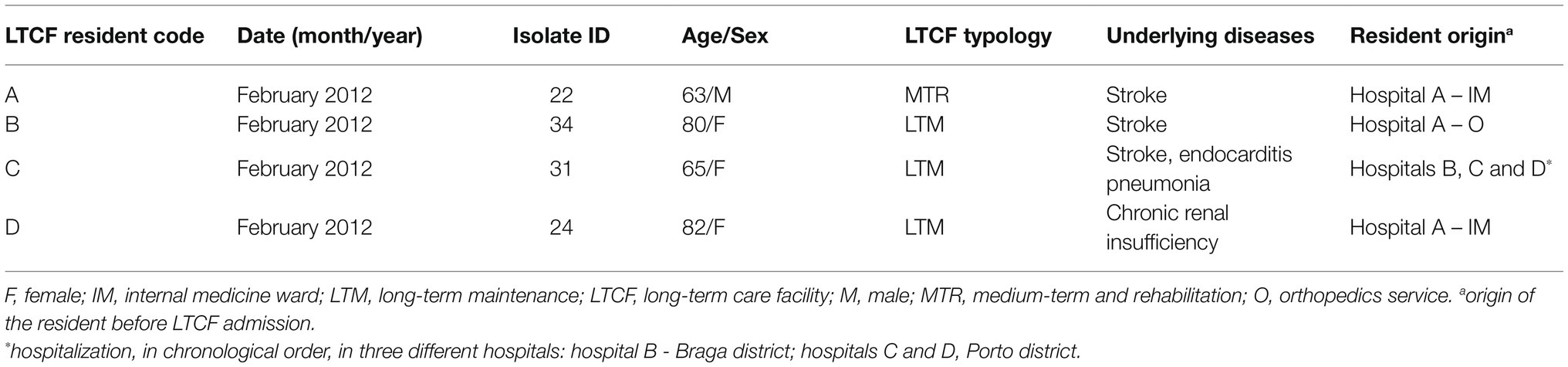
Table 2. Extra-hospital carbapenem-resistant K. pneumoniae isolates: epidemiological contextualization.
All clinical isolates showed reduced susceptibility to meropenem (MIC ≥16; R). Additionally, of the set of clinical isolates analyzed, six presented resistance to Ertapenem, and two to imipenem (three others showed an intermediate phenotype; Table 3). Importantly, most of the clinical isolates also showed resistance to expanded-spectrum cephalosporins, other β-lactams and β-lactam/β-lactamase inhibitor combinations; additionally resistance to gentamycin (n=2), tobramycin (n=5), ciprofloxacin (n=6), norfloxacin (n=1), pefloxacin (n=1), trimethoprim/sulfamethoxazole (n=7), and tetracycline (n=6) was also detected (Table 3).
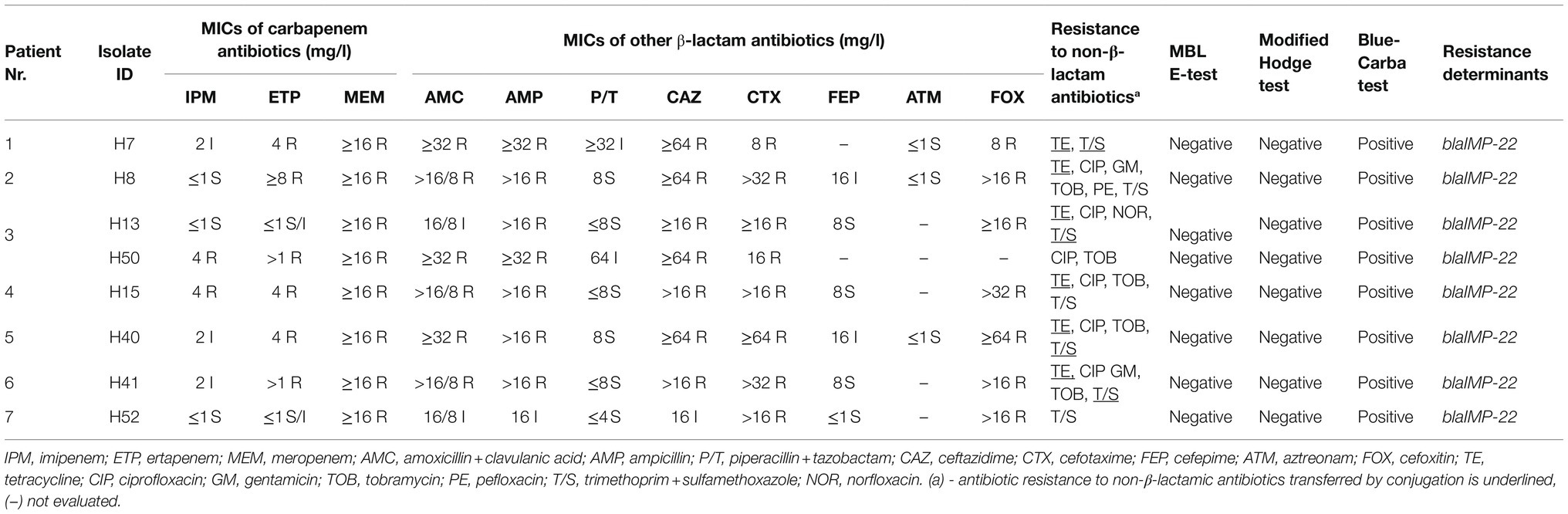
Table 3. IMP-22-producing K. pneumoniae clinical isolates: phenotypic and genotypic antimicrobial susceptibility patterns.
The four intestinal colonization K. pneumoniae isolates also showed reduced susceptibility to imipenem (Table 4). Two of them also showed reduced susceptibility to ertapenem (isolates 22 and 24), with only one (isolate 22) showing resistance to the three carbapenems tested (imipenem, ertapenem, and meropenem). The majority of the intestinal isolates also showed resistance to expanded-spectrum cephalosporins (n=3), other β-lactams (n=4), β-lactam/β-lactamase inhibitor combinations (n=4) as well as to non-β-lactam antibiotics, including tetracycline (n=3), trimethoprim/sulfamethoxazole (n=3), nalidixic acid (n=4), ciprofloxacin (n=4), chloramphenicol (n=2), and streptomycin (n=1; Table 4).

Table 4. Carbapenem-resistant intestinal colonization K. pneumoniae isolates: phenotypic and genotypic antimicrobial susceptibility features.
Of note, all clinical and intestinal colonization K. pneumoniae isolates were defined as multidrug-resistant (MDR) in accordance with the definition proposed by Magiorakos and colleagues (non-susceptible to ≥1 agent in ≥3 antimicrobial categories; Magiorakos et al., 2012).
Interestingly, the production of MBL in the context of all of the K. pneumoniae clinical isolates was initially defined as negative, as per the MBL E-test IP/IPI. Additionally, the results of the MHT were also negative for all of the clinical isolates. However, contrary to these findings, the results of the Blue-Carba test (all positive), suggested the expression of carbapenemases in all clinical isolates. Similarly, one of the intestinal colonization K. pneumoniae isolates was also determined as a carbapenemase producer, as per the results of the Blue-Carba test. Of note, according to the CLSI guidelines, extended-spectrum β-lactamase production was not detected, both in the clinical and intestinal colonization carbapenem-resistant isolates.
Finally, the blaIMP-22 gene was detected via PCR followed by sequencing in all of the eight K. pneumoniae clinical isolates and in one of the carbapenem-resistant intestinal isolates, part of the commensal intestinal microbiota of one LTCF resident (isolate 22). PCR amplification was further confirmed using IMP-22 specific primers, supporting our sequencing results. No other carbapenemase genes were detected in the set of K. pneumoniae isolates.
For epidemiological purposes, since many different carbapenem-resistant isolates were isolated in a short period of time in Hospital A, next, we investigated the genetic relationships of the eight IMP-22-producing K. pneumoniae clinical isolates using PFGE. Three distinct PFGE profiles (I to III) were revealed. Importantly, six of the clinical isolates (namely H7, H8, H13, H15, H40, and H41) shared the same profile (profile I), indicating that these isolates are genetically identical and have the same origin (Figure 1). The two remaining isolates, H52 and H50 showed two different profiles (profiles II and III, respectively; Figure 1). Of note, the isolates belonging to the single major clone (clone I) were isolated from four patients admitted to the medicine ward (isolates H7, H8, H13, and H15), and two patients admitted to the emergency ward (isolates H40 and H41); however, these two patients had previously been admitted to the same hospital. Interestingly, the two isolates collected from the same patient showed different PFGE patterns: H13, with the predominant profile I, was isolated during a first prolonged stay in Hospital A, while H50, with a unique typing pattern unrelated to profile I, was isolated during a second hospitalization, after a period spent in an LTCF in the same geographic region of Hospital A (the same LTCF from which the IMP-22-producing K. pneumoniae intestinal colonizer was isolated).
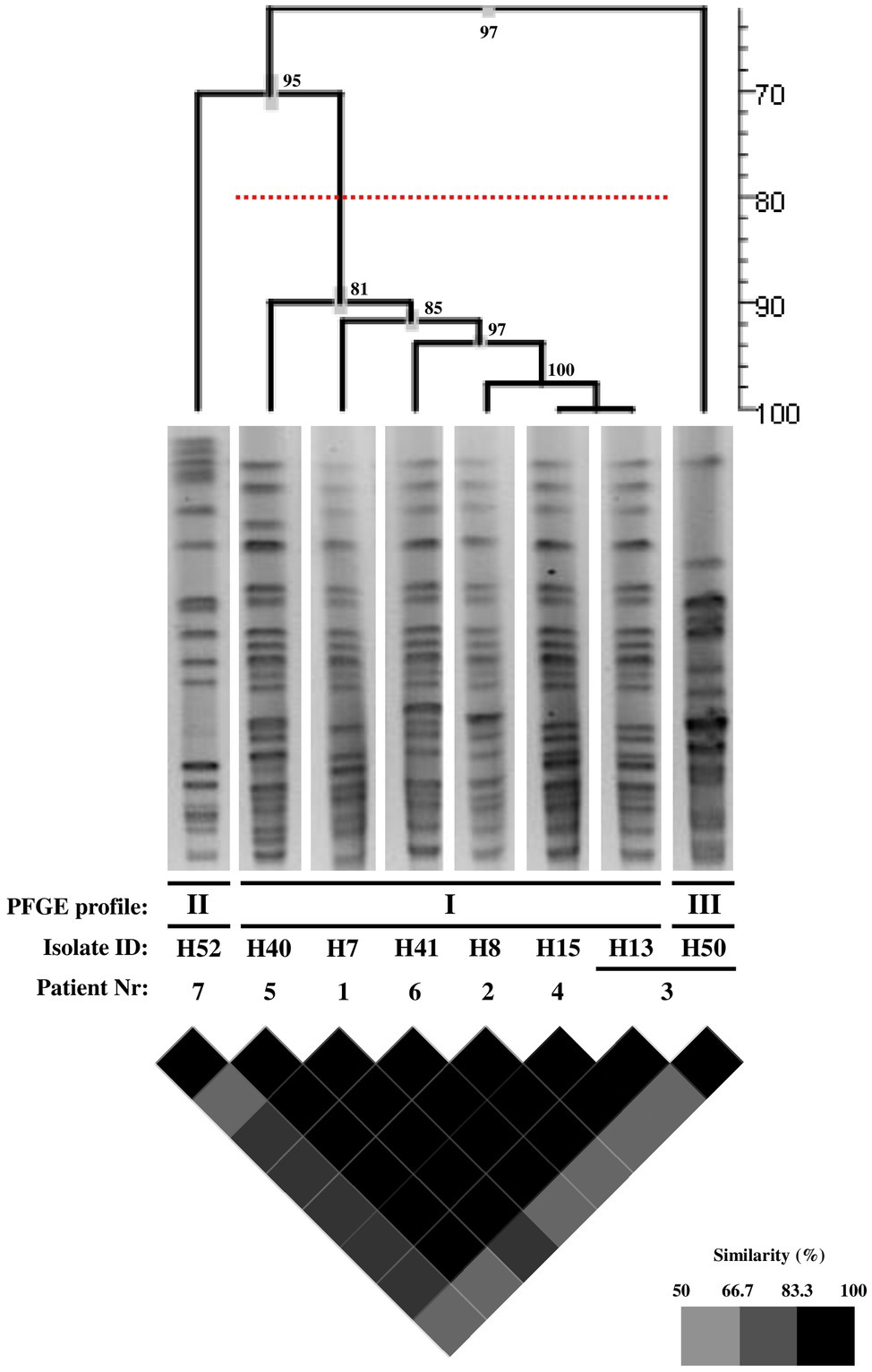
Figure 1. PFGE analysis of the IMP-22-producing K. pneumoniae clinical isolates. The clonal relationships between the eight K. pneumoniae clinical isolates were studied via pulsed-field gel electrophoresis (PFGE), after total genomic DNA digestion with XbaI. Cluster analysis was performed using the UPGMA algorithm based on the Dice coefficient (1.0% band tolerance; 1.0% optimization). The dendrogram obtained is shown, as are the isolated band patterns’ used in the cluster analysis. Additionally, a similarity matrix is also provided. Together with both the dendrogram and the similarity matrix, a similarity scale (in percentage) is provided (distance or color code, respectively). Additionally, in the dendrogram, the cophenetic correlation values are given in each node, as is the standard deviation (in grey). The PFGE profiles were defined on the basis of DNA banding patterns in accordance with the criteria defined by Tenover et al. (1995); isolates with a pattern similarity profile above ≥80% (represented by the dashed red line in the dendrogram) were considered identical.
Since the findings in the context of the patient from which two isolates were collected suggest the horizontal transfer of blaIMP-22 (two different PFGE types), we further performed conjugation experiments. Importantly, our results confirmed the above hypothesis; we observed the transference not only of the carbapenem resistance determinant but also of resistance determinants to non-β-lactam antibiotics (Table 3; underlined), in the context of six clinical isolates (H7, H8, H13, H15, H40, and H41), all belonging to the single major clone. On the other hand, no conjugation was achieved in the context of the two remaining clones isolated from clinical samples, as well as of the carbapenem-resistant K. pneumoniae intestinal isolates. Importantly, the presence of the blaIMP-22 gene in all of the trans-conjugants obtained was confirmed via PCR and sequencing.
Since the widespread use of carbapenems in the clinical settings, carbapenem-resistant Enterobacteriaceae have been increasingly detected worldwide (including in Portugal), not only in hospitals, but also in extra-hospital healthcare institutions, as well as in the environment (Logan and Weinstein, 2017). Among these bacteria, K. pneumoniae are formidable nosocomial pathogens with the potential to acquire resistance to multiple antimicrobial agents and consequently associated with high mortality and morbidity; of note, the emergence of MDR K. pneumoniae in extra-hospital healthcare institutions in the community, including LTCF, has been more and more reported (Navon-Venezia et al., 2017). Here, we describe for the first time not only the emergence of IMP-22-producing K. pneumoniae in an acute care hospital in the North of Portugal, but also, and more importantly, the breach of the hospital frontier toward the community, with the detection of one IMP-22-producing K. pneumoniae isolate as a component of the fecal microbiota of a resident of an extra-hospital health care setting (LTCF) in the same geographic area.
IMP-22 MBLs, first described associated with Pseudomonas spp. in different European countries are now emerging in K. pneumoniae in the Iberian Peninsula. In fact, the finding of the blaIMP-22 gene in P. fluorescens environmental strains (Pellegrini et al., 2009) as well as in P. aeruginosa, K. pneumoniae, and E. coli (Duljasz et al., 2009; Pellegrini et al., 2009; Viedma et al., 2012; Miro et al., 2013; Pena et al., 2014; Ortega et al., 2016) clinical isolates in different European countries suggest the ongoing spread of this blaMBL gene among Gram-negative bacteria. Importantly, our results support this notion and highlight the spread of this particular resistance determinant via both vertical and horizontal transmission, not only in the clinics but also in the community. Indeed, our results show a clonal spread of IMP-22-producing K. pneumoniae in the clinical settings, but also the possible plasmid-mediated spread of the blaIMP-22 gene in both the clinics and the community. These data reflect the complexity of the spread of CPE alerting for the need for adequate infection control practices in all healthcare institutions.
Different clonal outbreaks caused by carbapenem-resistant K. pneumoniae have been reported in particular hospitals in Portugal; however, most if not all of the reported outbreaks were associated with non-metallo-carbapenemases (including KPC-3 and OXA-48; (Conceicao et al., 2005; Rodrigues et al., 2014; Vubil et al., 2017; Manageiro et al., 2018; Mendes et al., 2018; Aires-de-Sousa et al., 2019; Perdigao et al., 2019; Gorgulho et al., 2020; Guerra et al., 2020; Lopes et al., 2020). In fact, only around 5% of the reported CPE in Portugal are associated with metallo-carbapenemases (Manageiro et al., 2018; Gorgulho et al., 2020). Therefore, our report of an outbreak caused by IMP-22-producing K. pneumoniae has epidemiological relevance, complementing the landscape of carbapenemase-producing bacteria in Portugal. Of note, the first IMP-22-producing K. pneumoniae clinical isolate was detected in March 2011, and since then, during one-year period (till May 2012) seven more isolates were found in the same hospital (and one more in the community). These data may suggest the successful installation of such resistant bacteria in the North of Portugal, with public health implications.
The original source and potential route of transmission of these IMP-22-producing K. pneumoniae isolates (clinical and intestinal commensal) is not known. However, our results suggest a common source, at least considering the IMP-22-producing K. pneumoniae clinical isolates of the predominant clone. The link between most patients admitted to Hospital A was their stay in the medicine ward; therefore, it is not unreasonable to speculate that transmission occurred during the hospital stay. Of note, although the K. pneumoniae isolates from patients 5 and 6 were detected in the emergency ward, both patients were previously admitted for a long period to the medicine ward of Hospital A; after hospital discharge, patient 5 went home, and patient 6 went to an LTCF in the same geographic region (the facility where the IMP-22 positive intestinal colonizer strain was isolated), but then returned to Hospital A due to health status complications. Therefore, intestinal colonization of these patients with IMP-22-producing K. pneumoniae is a serious hypothesis to be considered, after hospital discharge. Importantly, our results are in line with the more and more recognized notion that extra-hospital care institutions are a highway for the escape of MDR bacteria from the hospitals to the community, as well as for the (re)-introduction of MDR bacteria into hospitals (Masgala et al., 2015; Mody et al., 2018).
Interestingly, our results also suggest that, although most transmission events were clonal, some of them were horizontal in nature. This was particularly clear in the context of patient number 3, with two different isolates (detected during two distinct hospitalizations) showing non-related PFGE profiles. This, together with the fact that we were able to obtain trans-conjugants with all of the clinical isolates from the predominant clone suggest that these K. pneumoniae isolates are able to disseminate this particular carbapenem resistance determinant. Our results are, therefore, worrisome, thinking on the possibility of the emergence of more fit IMP-22-producing Enterobacteriaceae and their installation in the clinics and the community, in Portugal and even abroad (depending on the dissemination success of the bacteria).
Remarkably, MBL detection, as per the E-test IP/IPI, was negative in the context of all IMP-22-producing isolates, highlighting the need for the use of adequate phenotypic approaches to detect these particular carbapenem-resistant strains. Although according to some reports there is still “no gold standard CPE detection method” (Berry et al., 2019), many recognize the genotypic approach (detection of carbapenemase-encoding genes) as the most suitable (Nordmann and Poirel, 2013). However, the diagnosis capacity is not homogeneous around the world; the COVID-19 pandemic exposed the clear inequality-derived differences among countries (Giri and Rana, 2020; Millar, 2020). Therefore, phenotypic methods are still widely used as a primary approach to detect CPE. Importantly, our results highlight the need to use complementary (phenotypic) methods, to prevent the potential disregard of carbapenemase-producing strains, such as the IMP-22-producing K. pneumoniae isolates we report here; metallo-carbapenemase producers not detected using the standard E-test IP/IPI method (thus inadequate for the detection of IMP-22-producing K. pneumoniae), but detected using the Blue-Carba test. Of note, if possible, the genotypic determination of MBL is recommended in situations of reduced susceptibility to carbapenems, excluding imipenem. Altogether, our results alert for the need for the correct detection of CPE in routine clinical microbiology testing, to avoid outbreak installation.
The early identification of CPE in hospitalized patients and the implementation of adequate infection control measures are, thus, extremely important to prevent the persistence and spread of carbapenem-resistant bacteria (Magiorakos et al., 2017), such as the IMP-22-producing K. pneumoniae strains we report in this study, not only in the hospital settings but also in the community. In fact, after hospital discharge, patients can remain colonized and contribute for the dissemination of these MDR K. pneumoniae within extra-hospital care settings, namely, LTCF, and nursing homes (Chen et al., 2021). Therefore, the early identification of carriers and the implementation of adequate control strategies are essential to prevent nosocomial outbreaks. This is precisely what we show in this study. The individual colonized with the IMP-22-producing K. pneumoniae had previous hospitalization history in the medicine ward of the same acute care hospital where the clinical isolates were detected; therefore, our results suggest that this individual was colonized during hospitalization and served as a silent vehicle transporting the IMP-22-producing K. pneumoniae toward the community after discharge.
This study is not without limitations. First, antibiotic susceptibility of clinical and community isolates was assessed using two different methods, MIC determination, and disc-diffusion assays, respectively. However, for both methods, the CLSI/EUCAST guidelines were strictly followed. Second, the community isolate was not included in the analysis of clonal relationships. Therefore, we do not know whether this isolate belongs to the major clone, to one of the two single clones, or if it is a different clone; all of these options are possible. Third, although our results clearly suggest that the single clones were derived from horizontal dissemination events, this must yet be clearly shown. To address these limitations, we plan, in a follow-up study, to perform whole-genome sequencing of the isolates that will allow us to determine their MLST (and the clonal relationships of all of the isolates) and their resistome, as well as to perform detailed plasmid analyses and undoubtedly prove the horizontal transfer of the IMP-22 resistance determinant.
Altogether, our results align with the dogma that the presence of patients colonized with MDR Enterobacteriaceae in LTCF can represent a serious risk of dissemination and potential infection of elderly patients in the community, requiring, therefore strict epidemiological attention. In the future, as a preventive measure of the dissemination of multidrug-resistant bacteria, we suggest the active screening of intestinal colonization, both at hospital admission and hospital discharge, as well as, sporadically, in extra-hospital healthcare settings including LTCF and nursing homes; the detection of carbapenem-resistant bacteria at these stages will allow the implementation of rational infection control measures, with the potential to prevent outbreaks both in the clinics and the community.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
This research was conducted in accordance with the Declaration of Helsinki Ethical Principles. This study was approved by the Ethics Committee of Hospital de Braga, Braga, Portugal. Additionally, human fecal sample collection was performed in accordance with the Good Clinical Practice guidelines; the LTCF direction provided the necessary authorization to conduct this study. Of note, all of the study participants provided written informed consent.
DG and HF conceived and designed the experiments. DG and PC performed the experiments and wrote the original draft. DG, PC, and HF analyzed the data. DG, PC, AF, CI, FB, AE, and HF critically discussed the results and critically revised and edited the paper. HF assured the funding and contributed with the reagents, materials, and analysis tools. AF, CI, FB, and AE provided the clinical strains. All authors approved the current version of this manuscript.
This study was supported by internal funding.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The authors are grateful to Professor Laurent Poirel for generously providing the NDM and OXA-48 producing control strains and to Professor Luísa Peixe for access to the InfoQuest FP software.
The Supplementary Material for this article can be found online at:
https://www.frontiersin.org/articles/10.3389/fmicb.2021.777054/full#supplementary-material
Aires-de-Sousa, M., Ortiz de la Rosa, J. M., Goncalves, M. L., Pereira, A. L., Nordmann, P., and Poirel, L. (2019). Epidemiology of Carbapenemase-producing Klebsiella pneumoniae in a hospital, Portugal. Emerg. Infect. Dis. 25:1632. doi: 10.3201/eid2509.190656
Berry, C., Davies, K., Woodford, N., Wilcox, M., and Chilton, C. (2019). Survey of screening methods, rates and policies for the detection of carbapenemase-producing Enterobacteriaceae in English hospitals. J. Hosp. Infect. 101, 158–162. doi: 10.1016/j.jhin.2018.08.005
CDC (2019) Infographic: Antibiotic Resistance The Global Threat Available at: https://www.cdc.gov/globalhealth/infographics/antibiotic-resistance/antibiotic_resistance_global_threat.htm. (Accessed May 27, 2021).
Chen, H. Y., Jean, S. S., Lee, Y. L., Lu, M. C., Ko, W. C., Liu, P. Y., et al. (2021). Carbapenem-resistant Enterobacterales in long-term care facilities: A global and narrative review. Front. Cell. Infect. Microbiol. 11:601968. doi: 10.3389/fcimb.2021.601968
CLSI (2013). Performance standards for antimicrobial susceptibility testing. Wayne, PA: Clinical and Laboratory Standards Institute. Supplement M100–S23 p.
Conceicao, T., Brizio, A., Duarte, A., and Barros, R. (2005). First isolation of Bla(VIM-2) in Klebsiella oxytoca clinical isolates from Portugal. Antimicrob. Agents Chemother. 49:476. doi: 10.1128/AAC.49.1.476.2005
Dallenne, C., Da Costa, A., Decre, D., Favier, C., and Arlet, G. (2010). Development of a set of multiplex PCR assays for the detection of genes encoding important beta-lactamases in Enterobacteriaceae. J. Antimicrob. Chemother. 65, 490–495. doi: 10.1093/jac/dkp498
Duljasz, W., Gniadkowski, M., Sitter, S., Wojna, A., and Jebelean, C. (2009). First organisms with acquired metallo-beta-lactamases (IMP-13, IMP-22, and VIM-2) reported in Austria. Antimicrob. Agents Chemother. 53, 2221–2222. doi: 10.1128/AAC.01573-08
Gautom, R. K. (1997). Rapid pulsed-field gel electrophoresis protocol for typing of Escherichia coli O157:H7 and other gram-negative organisms in 1 day. J. Clin. Microbiol. 35, 2977–2980. doi: 10.1128/jcm.35.11.2977-2980.1997
Giri, A. K., and Rana, D. R. S. J. B. (2020). Charting the challenges behind the testing of COVID-19 in developing countries: Nepal as a case study. Biosafety Health 2:53. doi: 10.1016/j.bsheal.2020.05.002
Goncalves, D., Cecilio, P., and Ferreira, H. (2016). Nursing homes and long-term care facilities: reservoirs of CTX-M-15-producing Escherichia coli O25b-ST131 in Portugal. J. Glob. Antimicrob. Resist. 7, 69–71. doi: 10.1016/j.jgar.2016.08.001
Gorgulho, A., Grilo, A. M., de Figueiredo, M., and Selada, J. (2020). Carbapenemase-producing Enterobacteriaceae in a Portuguese hospital - a five-year retrospective study. Germs 10, 95–103. doi: 10.18683/germs.2020.1190
Guerra, A. M., Lira, A., Lameirao, A., Selaru, A., Abreu, G., Lopes, P., et al. (2020). Multiplicity of Carbapenemase-Producers Three Years after a KPC-3-Producing K. pneumoniae ST147-K64 Hospital Outbreak. Antibiotics 9:806. doi: 10.3390/antibiotics9110806
Logan, L. K., and Weinstein, R. A. (2017). The epidemiology of Carbapenem-resistant Enterobacteriaceae: The impact and evolution of a global menace. J. Infect. Dis. 215(suppl. 1), S28–S36. doi: 10.1093/infdis/jiw282
Lopes, E., Saavedra, M. J., Costa, E., de Lencastre, H., Poirel, L., and Aires-de-Sousa, M. (2020). Epidemiology of carbapenemase-producing Klebsiella pneumoniae in northern Portugal: predominance of KPC-2 and OXA-48. J. Glob. Antimicrob. Resist. 22, 349–353. doi: 10.1016/j.jgar.2020.04.007
Machado, E., Canton, R., Baquero, F., Galan, J. C., Rollan, A., Peixe, L., et al. (2005). Integron content of extended-spectrum-beta-lactamase-producing Escherichia coli strains over 12 years in a single hospital in Madrid, Spain. Antimicrob Agents Chemother 49, 1823–1829. doi: 10.1128/AAC.49.5.1823-1829.2005
Magiorakos, A. P., Burns, K., Rodriguez Bano, J., Borg, M., Daikos, G., Dumpis, U., et al. (2017). Infection prevention and control measures and tools for the prevention of entry of carbapenem-resistant Enterobacteriaceae into healthcare settings: guidance from the European Centre for Disease Prevention and Control. Antimicrob. Resist. Infect. Control 6:113. doi: 10.1186/s13756-017-0259-z
Magiorakos, A. P., Srinivasan, A., Carey, R. B., Carmeli, Y., Falagas, M. E., Giske, C. G., et al. (2012). Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: an international expert proposal for interim standard definitions for acquired resistance. Clin. Microbiol. Infect. 18, 268–281. doi: 10.1111/j.1469-0691.2011.03570.x
Manageiro, V., Romao, R., Moura, I. B., Sampaio, D. A., Vieira, L., Ferreira, E., et al. (2018). Molecular epidemiology and risk factors of Carbapenemase-producing Enterobacteriaceae isolates in Portuguese hospitals: results From European survey on Carbapenemase-producing Enterobacteriaceae (EuSCAPE). Front. Microbiol. 9:2834. doi: 10.3389/fmicb.2018.02834
Masgala, A., Kostaki, K., and Ioannnidis, I. (2015). Multi drug resistant gram negative pathogens in long term care facilities: ASteadily arising problem. J. Infect. Dis. Diagno. 1:101. doi: 10.4172/2576-389X.1000124
Mendes, A. C., Novais, A., Campos, J., Rodrigues, C., Santos, C., Antunes, P., et al. (2018). Mcr-1 in Carbapenemase-producing Klebsiella pneumoniae with hospitalized patients, Portugal, 2016-2017. Emerg. Infect. Dis. 24, 762–766. doi: 10.3201/eid2404.171787
Millar, M. (2020). “A capability perspective on antibiotic resistance, inequality, and child development,” in Ethics and Drug Resistance: Collective Responsibility for Global Public Health Public Health Ethics Analysis. eds. E. Jamrozik and M. Selgelid (Cham, Switzerland: Springer).
Miro, E., Aguero, J., Larrosa, M. N., Fernandez, A., Conejo, M. C., Bou, G., et al. (2013). Prevalence and molecular epidemiology of acquired AmpC beta-lactamases and carbapenemases in Enterobacteriaceae isolates from 35 hospitals in Spain. Eur. J. Clin. Microbiol. Infect. Dis. 32, 253–259. doi: 10.1007/s10096-012-1737-0
Mody, L., Foxman, B., Bradley, S., McNamara, S., Lansing, B., Gibson, K., et al. (2018). Longitudinal assessment of multidrug-resistant organisms in newly admitted nursing facility patients: implications for an evolving population. Clin. Infect. Dis. 67, 837–844. doi: 10.1093/cid/ciy194
Navon-Venezia, S., Kondratyeva, K., and Carattoli, A. (2017). Klebsiella pneumoniae: a major worldwide source and shuttle for antibiotic resistance. FEMS Microbiol. Rev. 41, 252–275. doi: 10.1093/femsre/fux013
Nordmann, P. (2014). Carbapenemase-producing Enterobacteriaceae: overview of a major public health challenge. Med. Mal. Infect. 44, 51–56. doi: 10.1016/j.medmal.2013.11.007
Nordmann, P., and Poirel, L. (2013). Strategies for identification of carbapenemase-producing Enterobacteriaceae. J. Antimicrob. Chemother. 68, 487–489. doi: 10.1093/jac/dks426
Ortega, A., Saez, D., Bautista, V., Fernandez-Romero, S., Lara, N., Aracil, B., et al. (2016). Carbapenemase-producing Escherichia coli is becoming more prevalent in Spain mainly because of the polyclonal dissemination of OXA-48. J. Antimicrob. Chemother. 71, 2131–2138. doi: 10.1093/jac/dkw148
Pellegrini, C., Mercuri, P. S., Celenza, G., Galleni, M., Segatore, B., Sacchetti, E., et al. (2009). Identification of Bla(IMP-22) in pseudomonas spp. in urban wastewater and nosocomial environments: biochemical characterization of a new IMP metallo-enzyme variant and its genetic location. J. Antimicrob. Chemother. 63:901. doi: 10.1093/jac/dkp061
Pena, I., Picazo, J. J., Rodriguez-Avial, C., and Rodriguez-Avial, I. (2014). Carbapenemase-producing Enterobacteriaceae in a tertiary hospital in Madrid, Spain: high percentage of colistin resistance among VIM-1-producing Klebsiella pneumoniae ST11 isolates. Int. J. Antimicrob. Agents 43, 460–464. doi: 10.1016/j.ijantimicag.2014.01.021
Perdigao, J., Modesto, A., Pereira, A. L., Neto, O., Matos, V., Godinho, A., et al. (2019). Whole-genome sequencing resolves a polyclonal outbreak by extended-spectrum beta-lactam and carbapenem-resistant Klebsiella pneumoniae in a Portuguese tertiary-care hospital. Microb. Genom 7:349. doi: 10.1099/mgen.0.000349
Pires, J., Novais, A., and Peixe, L. (2013). Blue-carba, an easy biochemical test for detection of diverse carbapenemase producers directly from bacterial cultures. J. Clin. Microbiol. 51, 4281–4283. doi: 10.1128/JCM.01634-13
Pitout, J. D., Nordmann, P., and Poirel, L. (2015). Carbapenemase-producing Klebsiella pneumoniae, a key pathogen set for global nosocomial dominance. Antimicrob. Agents Chemother. 59, 5873–5884. doi: 10.1128/AAC.01019-15
Poirel, L., Walsh, T. R., Cuvillier, V., and Nordmann, P. (2011). Multiplex PCR for detection of acquired carbapenemase genes. Diagn. Microbiol. Infect. Dis. 70, 119–123. doi: 10.1016/j.diagmicrobio.2010.12.002
Queenan, A. M., and Bush, K. (2007). Carbapenemases: the versatile beta-lactamases. Clin Microbiol Rev 20, 440–458. doi: 10.1128/CMR.00001-07
Rodrigues, C., Novais, A., Machado, E., and Peixe, L. (2014). Detection of VIM-34, a novel VIM-1 variant identified in the intercontinental ST15 Klebsiella pneumoniae clone. J. Antimicrob. Chemother. 69, 274–275. doi: 10.1093/jac/dkt314
Teixeira, J. V., Cecilio, P., Goncalves, D., Vilar, V. J., Pinto, E., and Ferreira, H. N. (2016). Multidrug-resistant Enterobacteriaceae from indoor air of an urban wastewater treatment plant. Environ. Monit. Assess. 188:388. doi: 10.1007/s10661-016-5382-4
Tenover, F. C., Arbeit, R. D., Goering, R. V., Mickelsen, P. A., Murray, B. E., Persing, D. H., et al. (1995). Interpreting chromosomal DNA restriction patterns produced by pulsed-field gel electrophoresis: criteria for bacterial strain typing. J. Clin. Microbiol. 33, 2233–2239. doi: 10.1128/jcm.33.9.2233-2239.1995
Viedma, E., Juan, C., Villa, J., Barrado, L., Orellana, M. A., Sanz, F., et al. (2012). VIM-2-producing multidrug-resistant Pseudomonas aeruginosa ST175 clone, Spain. Emerg. Infect. Dis 18, 1235–1241. doi: 10.3201/eid1808.111234
Vubil, D., Figueiredo, R., Reis, T., Canha, C., Boaventura, L., and Das, G. J. (2017). Outbreak of KPC-3-producing ST15 and ST348 Klebsiella pneumoniae in a Portuguese hospital. Epidemiol. Infect. 145, 595–599. doi: 10.1017/S0950268816002442
WHO (2015). Global Action Plan on Antimicrobial Resistance. Available at: http://www.who.int/antimicrobial-resistance/publications/global-action-plan/en/ (Accessed April 27, 2021).
Keywords: Klebsiella pneumoniae, antimicrobial resistance, carbapenemases, metallo-β-lactamases, nosocomial infections, intestinal colonization, long-term care facilities
Citation: Gonçalves D, Cecílio P, Faustino A, Iglesias C, Branca F, Estrada A and Ferreira H (2021) Intra- and Extra-Hospital Dissemination of IMP-22-Producing Klebsiella pneumoniae in Northern Portugal: The Breach of the Hospital Frontier Toward the Community. Front. Microbiol. 12:777054. doi: 10.3389/fmicb.2021.777054
Edited by:
Mullika Traidej Chomnawang, Mahidol University, ThailandReviewed by:
Carlos Henrique Camargo, Adolfo Lutz Institute, BrazilCopyright © 2021 Gonçalves, Cecílio, Faustino, Iglesias, Branca, Estrada and Ferreira. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Helena Ferreira, aGZlcnJAZmYudXAucHQ=
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.