 Andreas Petersen1*
Andreas Petersen1* Kjersti W. Larssen2
Kjersti W. Larssen2 Frode W. Gran2
Frode W. Gran2 Hege Enger2
Hege Enger2 Sara Hæggman3Barbro Mäkitalo3Gunnsteinn Haraldsson4
Sara Hæggman3Barbro Mäkitalo3Gunnsteinn Haraldsson4 Laura Lindholm5
Laura Lindholm5 Jaana Vuopio5,6,7Anna Emilie Henius1Jens Nielsen8
Jaana Vuopio5,6,7Anna Emilie Henius1Jens Nielsen8 Anders R. Larsen1
Anders R. Larsen1- 1Bacteria, Parasites and Fungi, Statens Serum Institut, Copenhagen, Denmark
- 2Department of Medical Microbiology, St. Olav Hospital, Trondheim, Norway
- 3Public Health Agency of Sweden, Solna, Sweden
- 4Department of Clinical Microbiology, Landspitali University Hospital and University of Iceland, Reykjavik, Iceland
- 5Finnish Institute for Health and Welfare, Helsinki, Finland
- 6Institute of Biomedicine, University of Turku, Turku, Finland
- 7Clinical Microbiology Laboratory, Turku University Hospital, Turku, Finland
- 8Infectious Disease Epidemiology & Prevention, Statens Serum Institut, Copenhagen, Denmark
Methicillin-resistant Staphylococcus aureus (MRSA) is notifiable in Denmark, Finland, Iceland, Norway and Sweden. The prevalence of MRSA in this region has been low for many years, but all five countries experience increasing numbers of new cases. The aim of the study was to describe the molecular epidemiology in the Nordic countries 2009-2016. Numbers of new cases of MRSA from 1997 to 2016 were compared, and a database containing information on spa-type and place of residence or acquisition, for all new MRSA isolates from 2009 to 2016 was established. A website was developed to visualize the geographic distribution of the spa-types. The incidence of new MRSA cases increased in all Nordic countries with Denmark having 61.8 new cases per 100,000 inhabitants in 2016 as the highest. The number of new cases 2009 to 2016 was 60,984. spa-typing revealed a high genetic diversity, with a total of 2,344 different spa-types identified. The majority of these spa-types (N = 2,017) were found in 1-10 cases. The most common spa-types t127/CC1, t223/CC22, and t304/CC6:8 increased significantly in all Nordic countries during the study period, except for Iceland, while spa-type t002/CC5 decreased in the same four countries. The trends of other common spa-types were different in each of the Nordic countries. The Nordic countries were shown to share similar trends but also to have country-specific characteristics in their MRSA populations. A continued increasing numbers of MRSA will challenge the surveillance economically. A more selected molecular surveillance will probably have to be employed in the future.
Introduction
The Nordic countries (Denmark, Finland, Iceland, Norway and Sweden) have had a very low prevalence of methicillin resistant Staphylococcus aureus (MRSA) for many years, with <2.5% of S. aureus bacteraemia isolates being MRSA (Surveillance Atlas of Infectious Diseases)1. This is probably due to several factors such as a prudent use of antibiotics and a longstanding extensive MRSA screening, surveillance and infection control programs, outlined in regional and national guidelines with the main points summarized in Table 1. Public funding of costs related to screening, follow up and treatment and/or decolonization may also be important factors in keeping MRSA transmission rates at a low level.
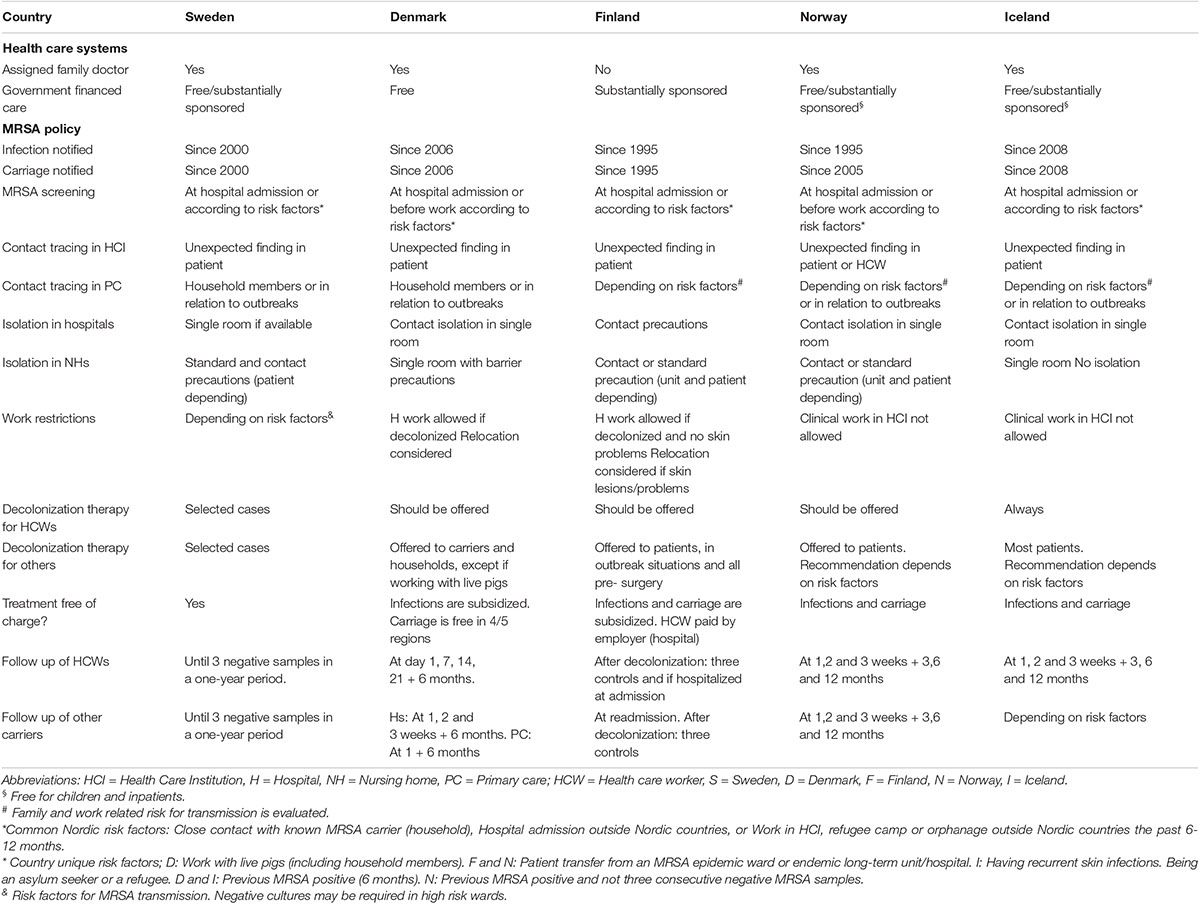
Table 1. Health care systems and MRSA policy in the Nordic countries.
MRSA is listed as a notifiable finding in the Nordic countries, and the countries have well established national surveillance systems for MRSA. The reference laboratories contribute with genotyping of the isolates. Since 2006-2009, the surveillance in the Nordic countries has included spa-typing, detection of Panton-Valentine leukocidin (PVL) genes as well as registration of clinical and/or demographic data. The Nordic Staphylococci Reference Laboratories (NSRL) share information on the MRSA surveillance data and methodology and quality control programs, with an overall aim to provide the best laboratory methods in place for the surveillance to support the control of MRSA especially in hospitals, and keeping the prevalence of invasive MRSA low (Skov and SSAC MRSA Working Party, 2005; Skov et al., 2008).
An increase in the numbers of new MRSA cases and a shift toward more cases of community acquired MRSA have been observed in the Nordic countries (Stenhem et al., 2006; Larsen et al., 2009, Holzknecht et al., 2010; Elstrom et al., 2012; Larsson et al., 2014; Swedres-Svarm, 2016; Junnila et al., 2020). This challenges the infection control practices and actions to prevent further transmission, and although the majority of cases are asymptomatic carriers, found through screening and contact tracing, or uncomplicated skin or soft tissue infections, an increase in MRSA blood stream infections or other severe infections may be expected in the years to come (Datta and Huang, 2008).
The aim of this study was to compare the emergence and dissemination of MRSA clones in the Nordic countries. This was done by assembling spa-typing results and associated demographic data in one database. Data are visualized by the use of a web based Geographic Information System (GIS-mapping) tool. The tool was developed to ensure a freely accessible and searchable database, which can easily visualize differences and trends in emerging MRSA clones within or between countries. The increasing dataset provides insight into clones of particular interest that may help guide national surveillance systems and policy makers in directing measures to control further spread of MRSA.
Materials and Methods
The number of MRSA cases reported to the NSRLs between 1997 and 2016 were compared with population data to obtain MRSA incidence in the respective countries. Demographic data were retrieved from the following sources: Statistics Denmark2, Statistics Finland3, Statistics Iceland4, Statistics Norway5, and Statistics Sweden6.
Since 2009, the Nordic countries use the same typing methods for national surveillance of MRSA. Relevant genetic information such as spa-type, clonal complex (CC), presence of PVL-gene, and date (of MRSA sample taken or received) were uploaded to a central Nordic database and linked to geolocation representing where and when the isolate was found.
Frequency of the most common spa-types and PVL-positive isolates seen in relation to the total number of isolates was calculated for each year. Negative binomial regression analysis was used to analyze for trends for spa-types and prevalence of PVL-positive MRSA for each country. Trends were described by incidence rate ratios (IRR).
Simpson’s index of diversity of spa-types was calculated for all isolates and for each country (Hunter and Gaston, 1988).
A website was developed to illustrate the geographical distribution of the MRSA isolates7. Nordicmrsa.org provides a graphical user interface utilizing Leaflet (Cheng et al., 2019) to create a dynamic map that takes latitude and longitude to display the geolocation of selected spa-types or CC with customized markers on the map. The app has been implemented in R using the shiny package (Chang et al., 2020; R Core Team, 2020).
Ethical Considerations
This publication only made use of bacterial isolates and typing results submitted to the reference laboratories as part of national MRSA surveillance programs. Cases were anonymized by each NSRL. No patient information was used or shared between the research group members. Geolocation are shown on an aggregated level in order to ensure anonymity represented by either hospital district-level (Finland and Iceland), county-level (Sweden), hospital or city hall, depending on whether the isolates were found within a hospital or in the community (Denmark) or at a municipality-level (Norway).
Results
Before year 2000, the Nordic countries had very low numbers of MRSA cases, which increased steadily throughout the study period. From 2000 to 2016 the annual incidence rates of MRSA increased 6-35 fold, except in Finland where it remained relatively stable after 2004, between 23.7 and 33.5 cases per 100.000 inhabitants (Figure 1). Denmark experienced a particular high incidence increase from 2012, reaching the highest incidence of 61.8 in 2016. This was largely due to the epidemic of livestock associated (LA-) MRSA CC398 comprising 35% of all new Danish MRSA cases in 2016 (Figure 1). LA-MRSA CC398 mostly consists of spa-types t034 and t011. LA-MRSA CC398 were only encountered in a limited number of cases in the other Nordic countries during the study period (N = 2, 97, 81 and 113 for Iceland, Sweden, Finland and Norway, respectively). When excluding LA-MRSA CC398, the increase in Denmark was similar to the ones in Sweden and Norway, reaching incidences of 40.1, 44.0, and 50.1 cases per 100,000 inhabitants, respectively.
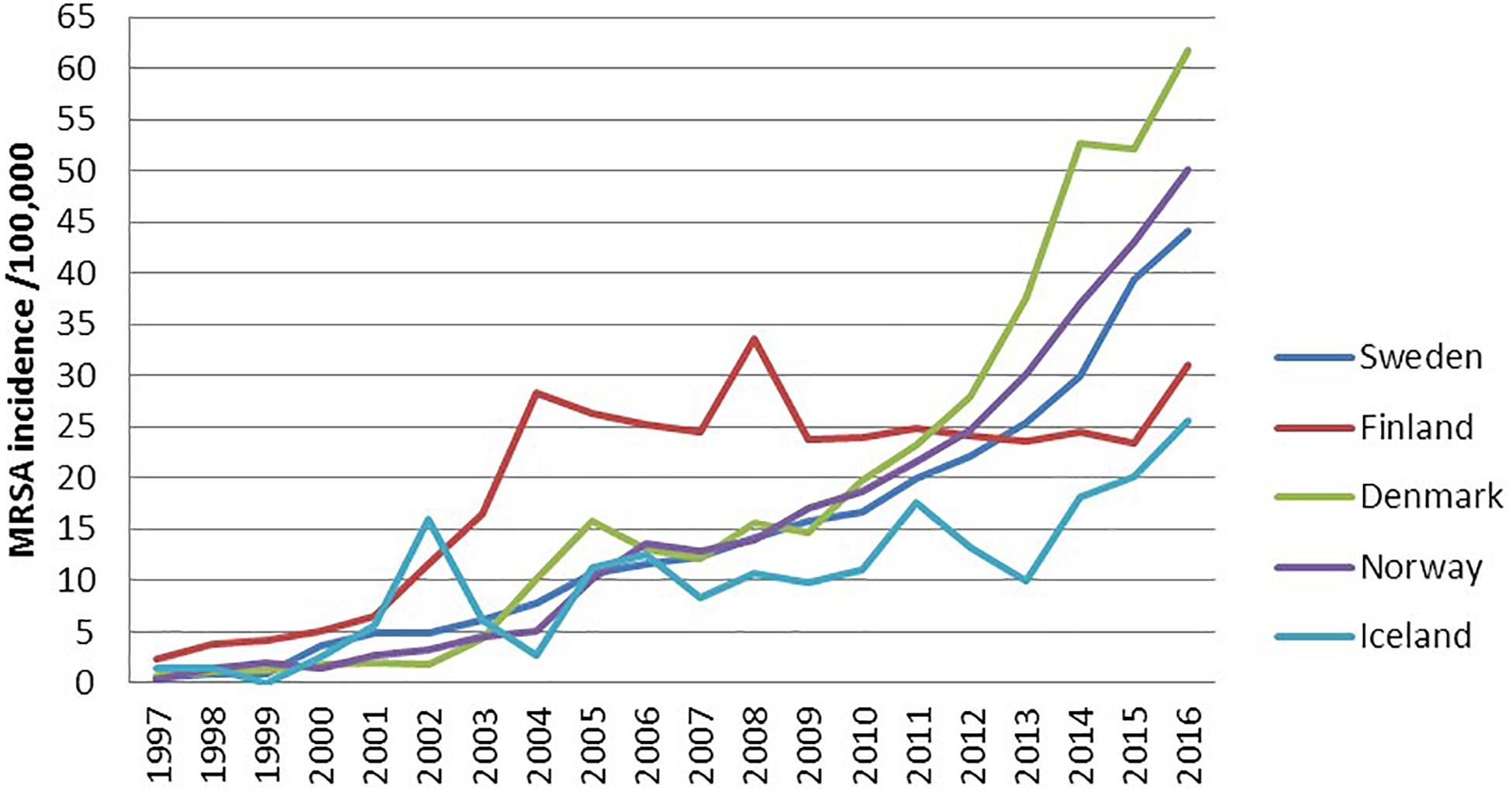
Figure 1. Incidence of notified MRSA cases in the Nordic countries, 1997–2016.
The population in the Nordic countries ranged from 332,526 in Iceland to 9,851,017 in Sweden in 2016. All Nordic countries experienced a population increase of 3.0-8.6% between 2009 and 2016. A total of 60,984 new MRSA cases were reported in the Nordic countries in 2009-16. The total numbers for each country were: 20,683; 16,234; 11,320; 12,339 and 408 for Sweden, Denmark, Finland, Norway and Iceland, respectively.
spa-typing revealed a very high genetic diversity, with a total of 2,344 different types identified. Of these 2,017 were observed in ≤10 cases across the period, hereafter referred to as sporadic clones. A total of 646 (1.1%) isolates were non-typeable with spa-typing. The diversity increased from 485 different spa- types in 2009 to 910 in 2016 (excluding CC398 isolates from Denmark). Sweden and Norway had the highest diversity, but a pattern with a high number of spa-types identified only in one year, and a low number of spa-types identified in all years, was observed in all Nordic countries (Table 2). Of the many different spa-types found in each of the countries, between 54-65% were found in only one of the years in the study period (Table 2). In contrast, only 2-6% of the spa-types in each country were found throughout the period. In Norway, Denmark, Finland and Sweden between 37-46% of all spa-types were only found in the respective country (Table 2). For Iceland 13% of the spa-types were not found in any of the other Nordic countries.

Table 2. Diversity of spa-types among MRSA in the Nordic countries 2009-2016.
Table 3 shows trends during the study period for the ten most prevalent spa-types in the Nordic countries. The few number of MRSA isolates in Iceland prevented any statistical analysis of trends. For the remaining countries, similarities and dissimilarities were seen. The proportion of spa-types t127/CC1, t223/CC22 and t304/CC6:8 increased significantly, with an incidence rate ratio (IRR) between 1.10 – 1.19 for t127, 1.17 – 1.21 for t223, and 1.25 – 1.51 for t304. In contrast, spa-type t002 decreased in prevalence in the four Nordic countries. For other spa-types the trends were different in each of the four Nordic countries; as illustrated by t044/CC80 which decreased in prevalence in Denmark and Norway, was stable in Sweden, and increased in Finland (Table 3). Figure 2 shows the geographic distribution of spa-type t223/CC22 in the Nordic countries in the years 2010, 2012, 2014, and 2016, respectively. From 149 cases in 2010, the numbers increased and was 1,024 in 2016.
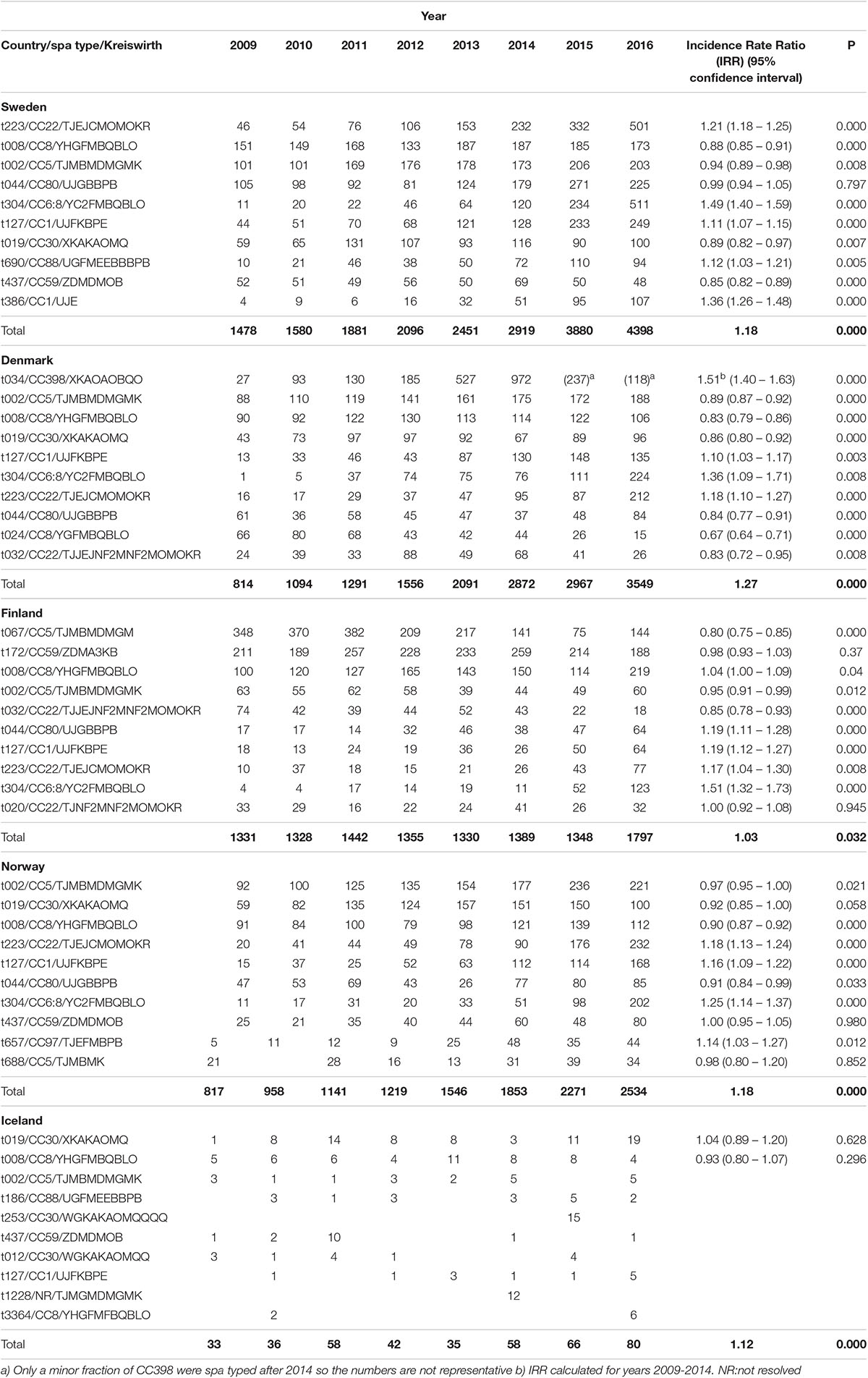
Table 3. Numbers and trends of the ten most prevalent spa types among MRSA cases in the Nordic countries in 2009–2016. Total denotes total number of MRSA per year and trend of total numbers.
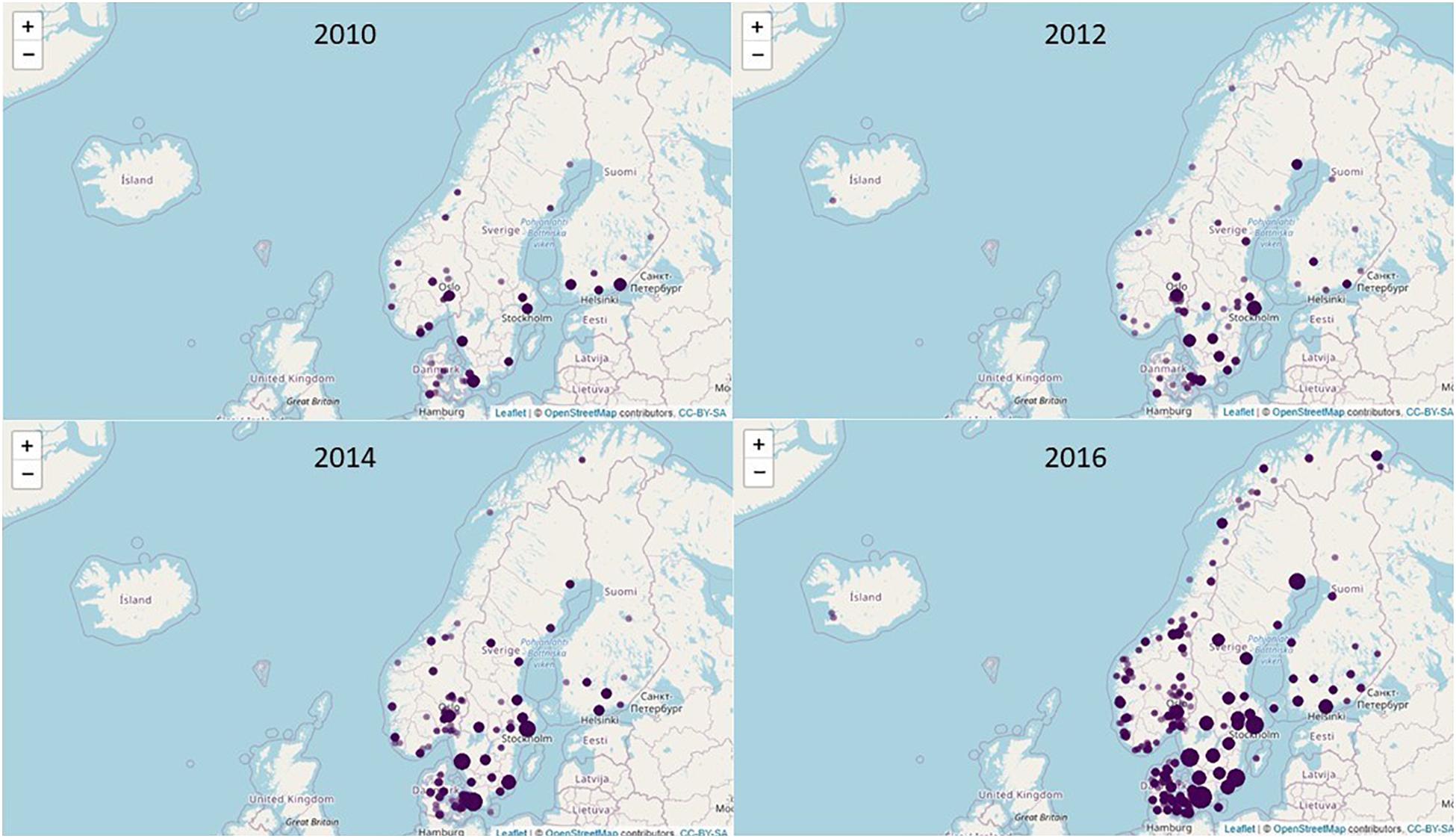
Figure 2. Geographic distribution of MRSA spa-type t223 in the Nordic countries in the years.2010, 2012, 2014, and 2016.
Country-specific clones included the livestock-associated t034/CC398, t011/CC398 and the mecC -MRSA t843/CC130 in Denmark, and t067/CC5 and t172/CC59 in Finland. Seventy percent of the spa-types t790/CC22 and t991/CC913 were found in Sweden.
Information on PVL was available for 50,313 isolates (83%). The information was almost complete for Denmark, Iceland, Norway and Sweden (96-100%) while Finland only had information for 1,489 isolates (13%). A total of 16,175 isolates were PVL-positive (32%) with a decreasing trend during the study period (36% in 2009, 28% in 2016; IRR = 0.95 (0.94-0.97)). Table 4 shows the ten most prevalent PVL-positive spa-types. The three most prevalent were t008/CC8, which corresponds to the USA 300 clone, t019/CC30, (South-West Pacific clone) and t044/CC80, the European community-acquired (CA)-MRSA clone.
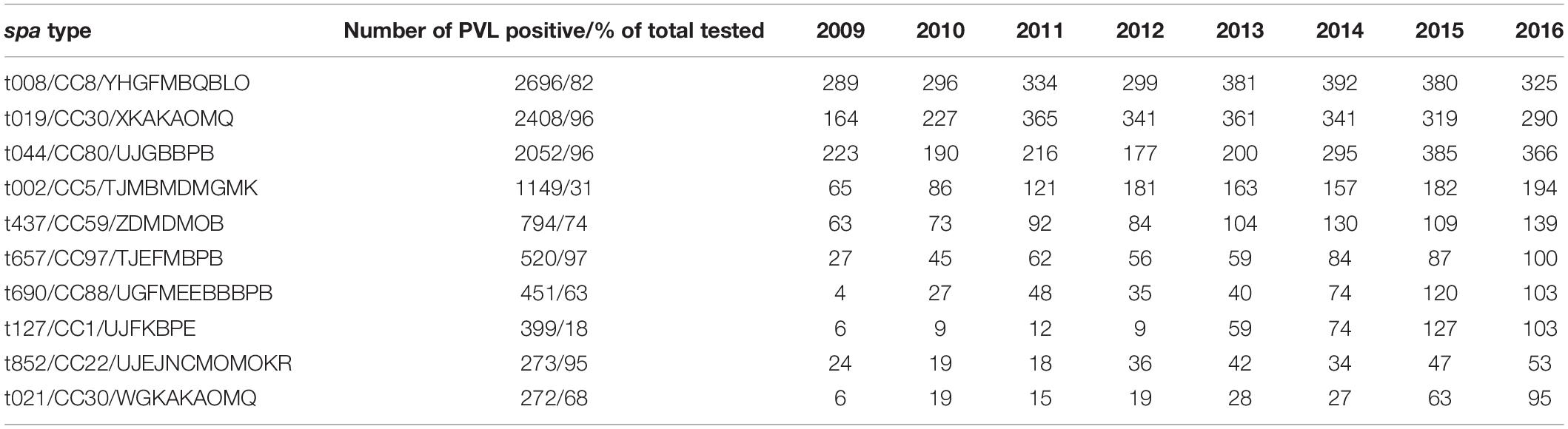
Table 4. The ten most prevalent PVL positive MRSA spa types in the Nordic countries 2009-2016 in total and by year.
Discussion
In our comparison of MRSA surveillance results across the Nordic Countries, we have observed several uniform patterns, including an overall low prevalence of MRSA, but also a rapidly increasing incidence in the last decade.
The low prevalence of MRSA in the Nordic countries likely results from the use of preventive guidelines established more than a decade ago with the main aim of protecting in-patients. A European comparison of guidelines for MRSA prevention and control pointed out that having longstanding MRSA prevention guidelines that also included nursing homes, general practice and home care, as well as notification of MRSA and isolation of MRSA cases in single rooms, were among the features that separated low prevalent MRSA countries from countries with higher MRSA prevalence (Kalenic et al., 2010).
The increase of MRSA in the Nordic countries was driven by increases outside hospital settings by both LA- and CA-MRSA (Di Ruscio et al., 2018; Junnila et al., 2020). The typical PVL-positive CA-MRSA clones (e.g., CC8, CC30, and CC80) are established in the community and are most likely supplemented with new imported cases due to travel and immigration. Several reports have highlighted increasing travel to and migration from high- prevalence countries and subsequent spread in the communities as a major route for the increasing number of MRSA in the Nordic countries. This assumption has been supported by results obtained by routine typing, and detection of the PVL genes of all MRSA (Fossum and Bukholm, 2006; Stenhem et al., 2006; Böcher et al., 2008; Kanerva et al., 2009; Larsen et al., 2009; Holzknecht et al., 2010; Vainio et al., 2011; Larsson et al., 2014; Nurjadi et al., 2015). However, in contrast to this assumption the overall prevalence of PVL-positive MRSA was decreasing in the Nordic countries during the study period.
The total number of MRSA reported here comprises both infections and screening samples. Screening practices have varied through the study period and, to some extent, between the Nordic countries. However, when looking only at the blood stream infections, an increase has also been observed (see Text Footnote 1), suggesting that an increased burden of MRSA may lead to more serious infections.
The genetic diversity of MRSA in the Nordic countries was very high with the vast majority of spa-types being just sporadic, causing very limited spread. Only a few MRSA clones seem to prevail, and these are in general international successful MRSA clones.
We observed a recent increase in the number of t223/CC22 and t304/CC6:8 isolates, which are prevalent in the Middle East countries, indicating that this may be due to immigration related to the civil war in Syria (Aro and Kantele, 2018). spa-type t223/CC22 (mainly PVL negative) has been observed in both community and health care settings in Norway, primarily as colonization, and largely associated with immigration from Syria, Russia and Afghanistan in recent years (Di Ruscio et al., 2018). In Sweden, this spa-type emerged rapidly around 2010, and was associated with young age and increased immigration from the Middle East (Larsson et al., 2014).
Norway experienced several hospital acquired MRSA (HA-MRSA) outbreaks of PVL negative t304/CC8 in South Western Norway between 2004 and 2011. Since then this specific clone has become extinct, and replaced by other t304 clones more associated with the community setting (Blomfeldt et al., 2016; Di Ruscio et al., 2018). In Denmark, t304/CC6 has been associated with hospital outbreaks in recent years (Bartels et al., 2015).
In addition to clones demonstrated among several of the Nordic countries, some country-specific differences were noted. Since 2009, dissemination of LA-MRSA CC398 in Danish pigs has been a main driver of the increase in new MRSA cases. Denmark differs from the other Nordic countries by having intensive pig farming, with more than 30 million pigs produced annually and approximately 10,000 people working in the farms. An investigation in 2016 found 88% of the pig farms to be MRSA positive (DANMAP, 2016). The annual number of new human LA-MRSA CC398 cases in 2014-2016 was between 1,173-1,277 with 85% having direct contact to pigs (DANMAP, 2016). In contrast, Norway has a less intensive pig production with approximately 1.6 million pigs slaughtered annually. After several separate introductions of LA-MRSA in 2013-2014, a strict policy including a yearly surveillance program, eradication of MRSA in stables by slaughter of pigs and decontamination of personnel has been applied (Grøntvedt et al., 2016). This strategy has so far proven successful, with no cases identified in 872 screened pig herds in Norway in 2016. In the other Nordic countries, spread in pigs and humans has so far been sporadic.
spa-type t067/ST125/CC5/SCCmec IA, PVL negative was involved in a large HA-associated outbreak mainly in one of the hospital districts from Finland. It affected both long-term care facilities and acute hospitals during 2001-2011 (Kanerva et al., 2009; Laine et al., 2013; Jokinen et al., 2015), but decreased from 350-400 cases in the beginning to 75 cases in 2015. An increase was again recorded in 2016 (N = 144). spa-type t172/ST375, CC59, SCCmec IV, PVL negative was almost exclusively found in Finland (1,779/1,882, 94%). It is the most common CA-MRSA in Finland, but it is not known why it is almost absent in the other Nordic countries. spa-type t991/CC913 was primarily found in Sweden (236/337, 70%). It was involved in outbreaks in hospital settings involving 25 cases, but no major explanation for the country-specificity of this clone in Sweden could be established. One third of the patients originated from the Middle East.
In Norway, the PVL-positive, multi-resistant Bengal Bay clone t657/ST772/CC97/SCCmec V, PVL positive has increased rapidly and caused several small-scale outbreaks in South Eastern Norway, particularly since 2013-2014. Cases have been linked mainly to the Indian subcontinent, through family history, home country visit, tourism and immigration (Blomfeldt et al., 2017).
spa typing is the typing method of choice in all Nordic countries. It is rapid, unambiguous and the spa types are easily communicated. It can be used in routine infection control in hospitals as well as describing national and international trends. spa types of MRSA isolated from individual patients are also surprisingly stable over time, given that single mutations or genetic alterations change the spa type. For the most prevalent types, additional typing such as MLST and SCCmec may be useful to characterize the isolates in more depth. Whole genome sequencing has been implemented in most of the NSRLs to be used for expanded typing and characterization of strains of interest, either for outbreak investigations, epidemiological studies and/or primary research.
The MRSA policies in the Nordic countries seems rather effective in preventing MRSA in hospitals, but have only limited effect on CA-MRSA and import of MRSA. MRSA imported by travel and migration spread in the community and can explain part of the increase observed both in total numbers of registered cases, and in the increasing diversity of clones. In line with this, a recent study reported import of travel-associated CA-MRSA to Europe from intercontinental travelers with skin and soft-tissue infections and found that the condition was transmissible (Nurjadi et al., 2019).
The increasing numbers of MRSA and other antimicrobial resistant microorganisms will continue to challenge the Nordic health care systems and call for revisions of the established policies. The NSRLs play an important role in providing high quality surveillance data for infection control and decision making, in a timely and easy-to-reach manner. In this study we have developed and combined our data in a publicly available database and used it to describe common traits and new emerging threats in the Nordic countries. This has only been possible due to the political and methodological similarities in our countries and can therefore not easily encompass other countries. The NSRLs are now challenged economically by the increase in number of MRSA cases. In the future, a more selective genotyping based on risk factors and/or selected epidemiological settings, such as association to outbreaks, livestock, invasive infections or health-care institutions will probably have to be employed. spa-typing is, due to the large genetic diversity still an inexpensive and effective screening method for epidemiological surveillance but whole genome sequencing is needed to investigate outbreaks and new transmission patterns. Studies like the current will therefore be difficult to repeat in the future, as the NRLs in the Nordic countries will have different priorities.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Author Contributions
AP conceived the study, collected and analyzed the data, and wrote and revised the manuscript. KL conceived the study, collected the data, and wrote the manuscript. FG collected the data, set up the home page, and revised the manuscript. HE, BM, and JV collected the data and revised the manuscript. SH, LL, and GH conceived the study, collected the data, and revised the manuscript. AH wrote the app for displaying MRSA cases and revised the manuscript. JN performed the statistical analysis and revised the manuscript. AL conceived the study and wrote and revised the manuscript. All authors contributed to the article and approved the submitted version.
Funding
This study was funded by Svenska Läkarsällskapet (SLS-412231).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We thank all referring laboratories for sending isolates and results to the national reference laboratories. We thank all personnel involved in the typing of MRSA during the study period.
Footnotes
- ^ https://atlas.ecdc.europa.eu/public/index.aspx
- ^ www.dst.dk
- ^ www.stat.fi
- ^ www.statice.is
- ^ www.ssb.no
- ^ www.scb.se
- ^ www.nordicmrsa.org
References
Aro, T., and Kantele, A. (2018). High rates of MRSA among asylum seekers and refugees admitted to Helsinki university hospital, 2010 to 2017. Euro Surveill. 23:45. doi: 10.2807/1560-7917.ES.2018.23.45.1700797
Bartels, M. D., Boye, K., Larsen, A. R., Skov, R., and Westh, H. (2007). Rapid increase of genetically diverse methicillin-resistant Staphylococcus aureus, Copenhagen, Denmark. Emerg. Infect. Dis. 13, 1533–1540. doi: 10.3201/eid1310.070503
Bartels, M. D., Larner-Svensson, H., Meiniche, H., Kristoffersen, K., Schonning, K., Nielsen, J. B., et al. (2015). Monitoring meticillin resistant Staphylococcus aureus and its spread in Copenhagen, Denmark, 2013, through routine whole genome sequencing. Euro Surveill. 20:21112.
Blomfeldt, A., Hasan, A. A., and Aamot, H. V. (2016). Can MLVA differentiate among endemic-like MRSA isolates with identical spa-type in a low-prevalence region? PLoS One 11:e0148772. doi: 10.1371/journal.pone.0148772
Blomfeldt, A., Larssen, K. W., Moghen, A., Gabrielsen, C., Elstrom, P., Aamot, H. V., et al. (2017). Emerging multidrug-resistant Bengal Bay clone ST772-MRSA-V in Norway: molecular epidemiology 2004-2014. Eur. J. Clin. Microbiol. Infect. Dis. 36, 1911–1921. doi: 10.1007/s10096-017-3014-8
Böcher, S., Gervelmeyer, A., Monnet, D. L., Mølbak, K., Skov, R. L., and Danish CA-MRSA Study Group (2008). Methicillin-resistant Staphylococcus aureus: risk factors associated with community-onset infections in Denmark. Clin. Microbiol. Infect. 14, 942–948. doi: 10.1111/j.1469-0691.2008.02055.x
Chang, W., Cheng, J., Allair, J. J., Xie, Y., and McPherson, J. (2020). Shiny: Web Application Framework for R. R Package Version 1.4.0.2. Available online at: https://CRAN.R-project.org/package=shiny (accessed April 19, 2021).
Cheng, J., Karambelkar, B., and Xie, Y. (2019). Leaflet: Create Interactive Web Maps with the JavaScript ‘Leaflet’ Library. R Package Version 2.0.3. Available online at: https://CRAN.R-project.org/package=leaflet (accessed April 19, 2021).
DANMAP (2016). Use of Antimicrobial Agents and Occurrence of Antimicrobial Resistance in Bacteria from Food, Animals, Food and Humans in Denmark. Available online at: https://www.danmap.org (accessed April 19, 2021).
Datta, R., and Huang, S. S. (2008). Risk of infection and death due to methicillin-resistant Staphylococcus aureus in long-term carriers. Clin. Infect. Dis. 47, 176–181.
Di Ruscio, F., Bjornholt, J. V., Larssen, K. W., Leegaard, T. M., Moen, A. E., and de Blasio, B. F. (2018). Epidemiology and spa-type diversity of meticillin-resistant Staphylococcus aureus in community and healthcare settings in Norway. J. Hosp. Infect. 100, 316–321. doi: 10.1016/j.jhin.2017.12.019
Elstrom, P., Kacelnik, O., Bruun, T., Iversen, B., Hauge, S. H., and Aavitsland, P. (2012). Meticillin-resistant Staphylococcus aureus in Norway, a low-incidence country, 2006-2010. J. Hosp. Infect. 80, 36–40. doi: 10.1016/j.jhin.2011.10.004
Fossum, A. E., and Bukholm, G. (2006). Increased incidence of methicillin-resistant Staphylococcus aureus ST80, novel ST125 and SCCmecIV in the south-eastern part of Norway during a 12-year period. Clin. Microbiol. Infect. 12, 627–633. doi: 10.1111/j.1469-0691.2006.01467.x
Grøntvedt, C. A., Elstrøm, P., Stegger, M., Skov, R. L., Andersen, P. S., Larssen, K. W., et al. (2016). Methicillin-resistant Staphylococcus aureus CC398 in humans and pigs in Norway: a “One Health” perspective on introduction and transmission. Clin. Infect. Dis. 63, 1431–1438.
Holzknecht, B. J., Hardardottir, H., Haraldsson, G., Westh, H., Valsdottir, F., Boye, K., et al. (2010). Changing epidemiology of methicillin-resistant Staphylococcus aureus in Iceland from 2000 to 2008: a challenge to current guidelines. J. Clin. Microbiol. 48, 4221–4227. doi: 10.1128/jcm.01382-10
Hunter, P. R., and Gaston, M. A. (1988). Numerical index of the discriminatory ability of typing systems: an application of Simpson’s index of diversity. J. Clin. Microbiol. 26, 2465–2466. doi: 10.1128/jcm.26.11.2465-2466.1988
Jokinen, E., Laine, J., Huttunen, R., Arvola, P., Vuopio, J., Lindholm, L., et al. (2015). Combined interventions are effective in MRSA control. Infect. Dis. 47, 801–807. doi: 10.3109/23744235.2015.1063158
Junnila, J., Hirvioja, T., Rintala, E., Auranen, K., Rantakokko-Jalava, K., Silvola, J., et al. (2020). Changing epidemiology of methicillin-resistant Staphylococcus aureus in a low endemicity area- new challenges for MRSA control. Eur. J. Clin. Microbiol. Infect. Dis. 39, 2299–2307. doi: 10.1007/s10096-020-03824-9
Kalenic, S., Pal, M. P., Palcevski, V. V., Horvatic, J., Mestrovic, T., Barsic, B., et al. (2010). Guidelines for prevention, control and treatment of infections caused by methicillin-resistant Staphylococcus aureus (MRSA): changes and updates of chapter 7.0: treatment of patients with MRSA infection. Lijec Vjesn 132, 340–344.
Kanerva, M., Salmenlinna, S., Vuopio-Varkila, J., Lehtinen, P., Mottonen, T., Virtanen, M. J., et al. (2009). Community-associated methicillin-resistant Staphylococcus aureus isolated in Finland in 2004 to 2006. J. Clin. Microbiol. 47, 2655–2657. doi: 10.1128/jcm.00771-09
Laine, J., Huttunen, R., Vuento, R., Arvola, P., Levola, R., Vuorihuhta, M., et al. (2013). Methicillin-resistant Staphylococcus aureus epidemic restricted to one health district in Finland: a population-based descriptive study in Pirkanmaa, Finland, years 2001–2011. Scand. J. Infect. Dis. 45, 45–53. doi: 10.3109/00365548.2012.710853
Larsen, A. R., Stegger, M., Bocher, S., Sorum, M., Monnet, D. L., and Skov, R. L. (2009). Emergence and characterization of community-associated methicillin-resistant Staphylococcus aureus infections in Denmark, 1999 to 2006. J. Clin. Microbiol. 47, 73–78.
Larsson, A. K., Gustafsson, E., Johansson, P. J., Odenholt, I., Petersson, A. C., and Melander, E. (2014). Epidemiology of MRSA in southern Sweden: strong relation to foreign country of origin, health care abroad and foreign travel. Eur. J. Clin. Microbiol. Infect. Dis. 33, 61–68. doi: 10.1007/s10096-013-1929-2
Nurjadi, D., Fleck, R., Lindner, A., Schäfer, J., Gertler, M., Mueller, A., et al. (2019). Import of community-associated, methicillin-resistant Staphylococcus aureus to Europe through skin and soft-tissue infection in intercontinental travellers, 2011-2016. Clin. Microbiol. Infect. 25, 739–746. doi: 10.1016/j.cmi.2018.09.023
Nurjadi, D., Friedrich-Janicke, B., Schafer, J., Van Genderen, P. J., Goorhuis, A., Perignon, A., et al. (2015). Skin and soft tissue infections in intercontinental travellers and the import of multi-resistant Staphylococcus aureus to Europe. Clin. Microbiol. Infect. 21:567. doi: 10.1016/j.cmi.2015.01.016
R Core Team (2020). R: A Language and Environment for Statistical Computing. Vienna: R Foundation for Statistical Computing.
Skov, R., Gudlaugsson, O., Hardardottir, H., Harthug, S., Jakobsen, T., Kolmos, H. J., et al. (2008). Proposal for common Nordic epidemiological terms and definitions for methicillin-resistant Staphylococcus aureus (MRSA). Scand. J. Inf. Dis. 40, 495–502. doi: 10.1080/00365540701864658
Skov, R., and SSAC MRSA Working Party (2005). MRSA infections increasing in the Nordic countries. Euro Surveill. 10:E050804.2.
Stenhem, M., Ortqvist, A., Ringberg, H., Larsson, L., Olsson-Liljequist, B., Haeggman, S., et al. (2006). Epidemiology of methicillin-resistant Staphylococcus aureus (MRSA) in Sweden 2000-2003, increasing incidence and regional differences. BMC Infect. Dis. 6:30. doi: 10.1186/1471-2334-6-30
Swedres-Svarm (2016). Consumption of Antibiotics and Occurrence Of Resistance in Sweden. Solna/Uppsala. Available online at: https://www.folkhalsomyndigheten.se/contentassets/d118ac95c12d4c11b3e61d34ee6d2332/swedres-svarm-2016-16124.pdf (accessed April 19, 2021).
Keywords: MRSA, surveillance, Staphylococcus aureus, spa-typing, epidemiology
Citation: Petersen A, Larssen KW, Gran FW, Enger H, Hæggman S, Mäkitalo B, Haraldsson G, Lindholm L, Vuopio J, Henius AE, Nielsen J and Larsen AR (2021) Increasing Incidences and Clonal Diversity of Methicillin-Resistant Staphylococcus aureus in the Nordic Countries - Results From the Nordic MRSA Surveillance. Front. Microbiol. 12:668900. doi: 10.3389/fmicb.2021.668900
Received: 17 February 2021; Accepted: 09 April 2021;
Published: 30 April 2021.
Edited by:
David Christopher Coleman, Dublin Dental University Hospital, IrelandReviewed by:
Kunyan Zhang, University of Calgary, CanadaStefan Monecke, Leibniz Institute of Photonic Technology (IPHT), Germany
Copyright © 2021 Petersen, Larssen, Gran, Enger, Hæggman, Mäkitalo, Haraldsson, Lindholm, Vuopio, Henius, Nielsen and Larsen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Andreas Petersen, YWFwQHNzaS5kaw==