 Javier Moreno-Morales1†
Javier Moreno-Morales1† Andrea Vergara2†
Andrea Vergara2† Tomislav Kostyanev3
Tomislav Kostyanev3 Jesús Rodriguez-Baño4
Jesús Rodriguez-Baño4 Herman Goossens3,5
Herman Goossens3,5 Jordi Vila1,2*
Jordi Vila1,2*- 1Institute for Global Health (ISGlobal), Hospital Clínic – Universitat de Barcelona, Barcelona, Spain
- 2Department of Clinical Microbiology – CDB, Hospital Clínic, University of Barcelona, Barcelona, Spain
- 3Department of Medical Microbiology, Vaccine and Infectious Disease Institute, University of Antwerp, Antwerp, Belgium
- 4Unidad Clínica de Enfermedades Infecciosas, Microbiología y Medicina Preventiva, Hospital Universitario Virgen Macarena/Departamento de Medicina, Universidad de Sevilla/Instituto de Biomedicina de Sevilla (IBiS), Seville, Spain
- 5Laboratory of Medical Microbiology, University Hospital Antwerp, Antwerp, Belgium
Carbapenem-resistant Acinetobacter spp. mainly Acinetobacter baumannii are frequently causing nosocomial infections with high mortality. In this study, the efficacy of the Eazyplex® SuperBug Complete A system, based on loop-mediated isothermal amplification (LAMP), to detect the presence of carbapenemases in Acinetobacter spp. directly from bronchoalveolar lavage (BAL) samples was assessed. A total of 22 Acinetobacter spp. strains producing OXA-23, OXA-40, OXA-58, NDM, and IMP were selected. Eazyplex SuperBug Complete A kit, used with the Genie II device, is a molecular diagnostics kit that detects a selection of genes that express carbapenemases (blaKPC, blaNDM, blaVIM, blaOXA–48, blaOXA–23, blaOXA–40, and blaOXA–58). Negative BAL samples were identified, McFarland solutions were prepared from each of the 22 Acinetobacter strains and serial dilutions in saline solution were made to finally spike BAL samples to a concentration of 102 and 103 CFU/ml. Fifteen concentrations out of the 44 tested out did not provide detection of the carbapenemase-producing gene, all but one being at the lowest concentration tested at 102 CFU/ml; therefore, the limit of sensitivity is 103 CFU/ml. This assay represents the kind of advantages that investing in molecular diagnostics brings to the clinical practice, allowing the identification of carbapenemases in less than 30 min with a sensitivity of 103 CFU/ml.
Introduction
Carbapenems are potent β-lactam antibiotics with broad-spectrum and bactericidal mode of action (Codjoe and Donkor, 2017). Their use was increased due to the spread of extended spectrum β-lactamase-producing Enterobacteriales toward whom they are active (Hawkey and Livermore, 2012; Bush and Bradford, 2020). Carbapenems are considered one of the most efficacious antimicrobials to treat bacterial infections (Codjoe and Donkor, 2017). However, resistance by carbapenemases did not take long to appear, and it poses a major threat to public health (Hawkey and Livermore, 2012).
Acinetobacter spp. members and specially carbapenem-resistant Acinetobacter baumannii (CRAB) are among the world’s most dangerous pathogen threats. CRAB has been classified as a critical priority pathogen by the WHO’s priority pathogens to guide research and development (R&D) of new antibiotics (Tacconelli et al., 2018; World Health Organization, 2019) and as an urgent threat that requires aggressive action by Centers for Disease Control and Prevention (CDC) (Centers for Disease Control, 2019).
Even though community-acquired Acinetobacter infections can occur, the most common and acute infections happen in the nosocomial setting. Acinetobacter lurks around intensive care units and surgical wards causing a number of infections (e.g., on burns and soft tissue, urinary tract, and bloodstream) and specially ventilator-associated pneumonia (VAP) in patients under mechanical ventilation (Evans et al., 2012; Bush and Bradford, 2020).
Ventilator-associated pneumonia develops in intensive care units in patients under ventilation for at least 48 h. Rapid diagnostic of VAP-causing pathogens is of utmost importance: VAP patients not only have longer hospital stays and need more antibiotics, therefore their treatment is more expensive, but also have higher mortality (Torres et al., 2017; Bonell et al., 2019).
This study aims to evaluate Eazyplex® SuperBug Complete A based on loop-mediated isothermal amplification (LAMP) for detecting carbapenemase produced by Acinetobacter directly from inoculated bronchoalveolar lavage (BAL) samples.
Materials and Methods
Eazyplex® SuperBug Complete A kit (AmplexDiagnostics GmbH, Germany), used with the Genie II device (OptiGene, Horsham, United Kingdom), is a molecular diagnostics kit that detects a selection of genes that express carbapenemases (including metallo-β-lactamases and oxacillinases). Results after detection of bacterial DNA are presented within 30 min.
The kit is composed of eight tube strips each with a mix of lyophilized agents for the amplification of one of the following seven genes: blaKPC, blaNDM, blaVIM, blaOXA–48, blaOXA–23, blaOXA–40, and blaOXA–58. The eighth tube is an internal inhibitory control.
Once the samples are prepared and the strip is inside the Genie II device, a LAMP is performed. The reaction is incubated at 66°C for 30 min, and detection is performed via fluorescence excitation, for up to two strips at a time.
A total of 22 Acinetobacter spp. strains producing OXA-23, OXA-40, OXA-58, NDM, and IMP were selected (Table 1). Isolate identification was performed via MALDI-TOF/MS (Bruker Daltonics, Bremen, Germany). Carbapenemase gene detection was checked via conventional PCR for each of the strains (Woodford et al., 2006; Kulah et al., 2010; Solé et al., 2011). The strains selected basically were epidemiologically unrelated due to its different sequence types (ST) or geographical origins.
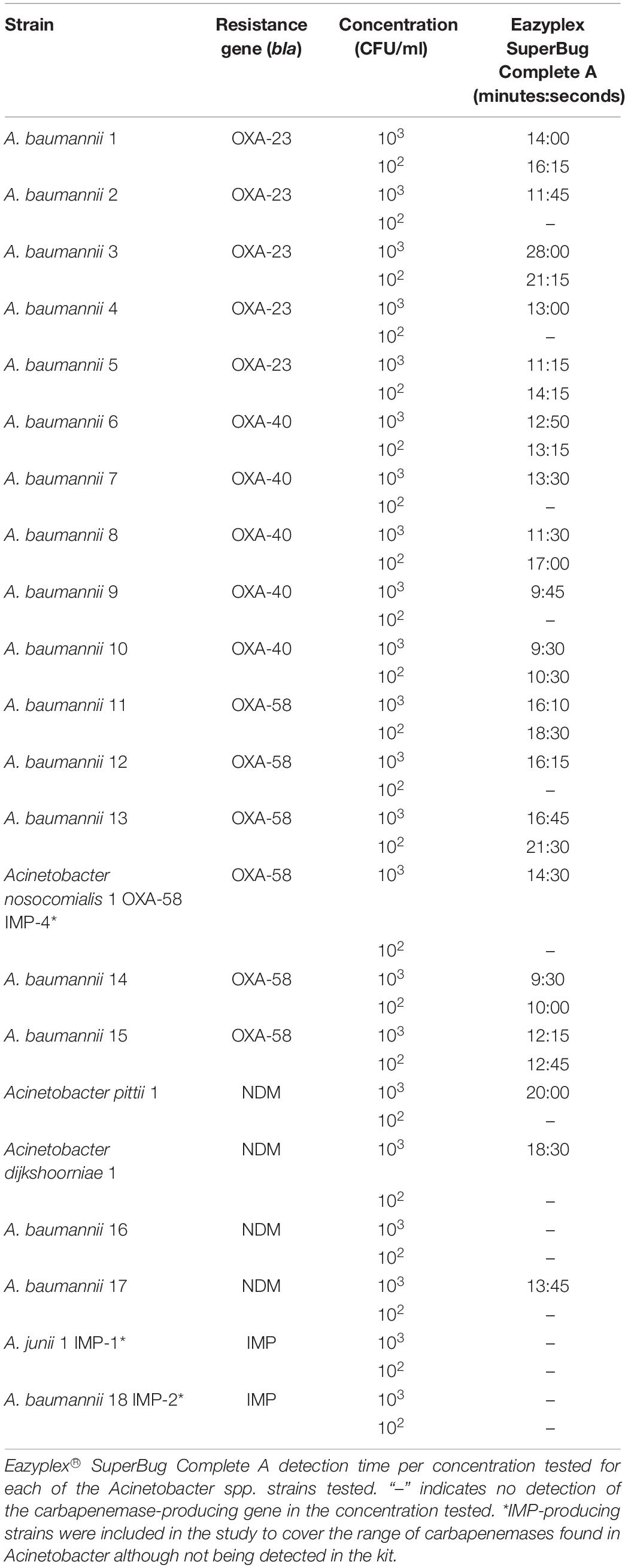
Table 1. Eazyplex SuperBug Complete A kit was used to detect carbapenemases of Acinetobacter spp. from spiked BAL.
Negative BAL samples were identified and collected at the Clinical Microbiology Laboratory from Hospital Clinic of Barcelona; samples were stored at −80°C. McFarland solutions were prepared from each of the 22 Acinetobacter strains, and serial dilutions in saline solution were made to finally spike BAL samples to a concentration of 102 and 103 CFU/ml.
The protocol consisted in: centrifugation of 850 μl of the 102 and 103 spiked BAL samples (at 14,000 g for 5 min), addition of 500 μl of resuspension and lysis fluid (RALF, provided with the kit) to the pellet obtained, incubation at 99°C for 2 min and a final centrifugation step (4,000 rpm for 2 min). Finally, 25 μl of the supernatant was added to each tube of the assay strip. The hands-on time took a maximum of 15 min per strain.
Results and Discussion
Increasing resistance to antimicrobials and specifically carbapenems is reported in A. baumannii in the past years. In Spain, there has been an increase of up to 40% in A. baumannii clinical isolates presenting resistance to carbapenems from 2000 to 2010; 86% of the 446 A. baumannii clinical isolates presented resistance to carbapenems in 2010’s study (Fernández-Cuenca et al., 2013).
This situation is rather common. Recently, European Centre for Disease Prevention and Control (ECDC) has reported ≥50% of Acinetobacter spp. invasive isolates present resistance to carbapenems in Hungary, Poland, Bulgaria, Latvia, Italy, Spain, Cyprus, Romania, Lithuania, Greece, and Croatia in 2018’s Annual Report of the European Antimicrobial Resistance Surveillance Network (European Centre for Disease Prevention and Control, 2018).
Current effective antibiotics for the treatment of CRAB are scarce and are not the most suitable therapeutic agents due to poor pharmacokinetics, toxicity (as in the case of polymyxins), and emergence of resistance (Garnacho-Montero et al., 2015). Chromosome and/or plasmid encoded carbapenemases are the main mechanism of resistance to carbapenems in CRAB (Roca et al., 2012; Bush and Bradford, 2020); thus, rapid detection of carbapenemases is key to guide effective antibiotic therapies (Garnacho-Montero et al., 2015).
Although the Complete A kit is not specific for Acinetobacter, carbapenemase coverage is enough to check for the main carbapenemases present in Acinetobacter. Of all the carbapenemases described in A. baumannii, oxacillinases are by far the most frequently found among the most prevalent clones, being the international clone 2 OXA-23 producing A. baumannii worldwide spread.
Detection of carbapenemase-producing genes in the tested strains using Eazyplex SuperBug Complete A assay is shown in Table 1, and the results agree with conventional PCR results. Detection time values vary per strain and gene. Only 15 concentrations tested out of 44 did not provide detection of the carbapenemase-producing gene, all being at the lowest concentration tested at 102 CFU/ml; therefore, with the limit of sensitivity being 103 CFU/ml, we consider that this kit has enough sensitivity for the detection of carbapenemase-producing Acinetobacter in clinical BAL samples, taking into consideration that the cut-off for BAL is 104 CFU/ml.
With a maximum hands-on time of 15 min per sample and 30 min run time (approximately 45 min total), this assay proves to be a great advantage compared to routine methods in the clinical microbiology laboratory that need 16–24 h for results to be obtained. Naturally, further antimicrobial susceptibility testing should be considered in all samples. The only rapid test (4 h) that allows the detection of the most frequent pathogens causing HAP is the Unyvero Hospitalized Pneumonia (HPN; Curetis GmbH, Germany). This multiplex panel also includes some resistant markers (18 in total); among them, it can detect the genes encoding VIM, IMP, NDM, KPC, OXA-23, OXA-24, OXA-48, and OXA-58. However, as far as we know, it has not been validated for detection of carbapenemases in A. baumannii.
We visualize the following workflow for diagnosis of hospital-acquired pneumonia (HAP): when the sample arrives to the clinical microbiology laboratory, rapid identification of the bacteria causing HAP is performed also using an in-house LAMP reaction approach (Vergara et al., 2020a); if A. baumannii is identified as the pathogen causing the infection, the method to detect specific carbapenemases in Acinetobacter described in this study is performed. However, if Enterobacterales is detected, the same approach can be applied (Vergara et al., 2020b).
Using Eazyplex® SuperBug Complete A assay will allow to guide and optimize antibiotic therapies earlier than with usual techniques used in the laboratory, which likely means a decrease in mortality. This assay represents the kind of advantages that investing in molecular diagnostics brings to the clinical practice: allows the identification of specific resistance mechanisms in approximately 45 min and if sample identification using LAMP was included as a first step (1 h), both pathogen and resistance mechanism could be identified in less than 2 h.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
Author Contributions
JV, JR-B, and HG: conceptualization, design, and writing–review and editing. JM-M and TK: methodology. AV: supervision and validation. JV: writing–original draft preparation and funding acquisition. All authors contributed to the article and approved the submitted version.
Funding
We acknowledge support from the Spanish Ministry of Science and Innovation through the “Centro de Excelencia Severo Ochoa 2019–2023” Program (CEX2018-000806-S) and support from the Generalitat de Catalunya through the CERCA Program. We were supported by the Plan Nacional de I + D + i 2013-2016 and Instituto de Salud Carlos III, Subdirección General de Redes y Centros de Investigación Cooperativa, Ministerio de Economía, Industria y Competitividad, and Spanish Network for Research in Infectious Diseases (REIPI RD16/0016/0010) and co-financed by the European Development Regional Fund “A way to achieve Europe,” Operative program Intelligent Growth 2014–2020. The research leading to these results was conducted as part of the COMBACTE-CARE project (Grant Number 115620). This work was also supported by award 2017 SGR 0809 from the Agència de Gestió d’Ajuts Universitaris i de Recerca of the Generalitat de Catalunya.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We would like to thank Ignasi Roca for kindly providing strains in this study and Thierry Naas for providing some of the strains harboring IMP. This manuscript has been released as a pre-print at https://www.biorxiv.org/content/10.1101/2020.05.11.089904v1 (Moreno-Morales et al., 2020).
References
Bonell, A., Azarrafiy, R., Huong, V. T. L., Viet, T., Phu, V. D., Dat, V. Q., et al. (2019). A systematic review and meta-analysis of ventilator-associated pneumonia in adults in Asia: an analysis of national income level on incidence and etiology. Clin. Infect. Dis. 68, 511–518. doi: 10.1093/cid/ciy543
Bush, K., and Bradford, P. A. (2020). Epidemiology of β-lactamase-producing pathogens. Clin. Microbiol. Rev. 33:e00047-19.
Centers for Disease Control (2019). Antibiotic Resistance Threats in the United States, 2019. Atlanta: CDC.
Codjoe, F., and Donkor, E. (2017). Carbapenem resistance: a review. Med. Sci. 6:1. doi: 10.3390/medsci6010001
European Centre for Disease Prevention and Control (2018). Surveillance Report. Surveillance of Antimicrobial Resistance in Europe 2018. Available online at: https://www.ecdc.europa.eu/sites/default/files/documents/surveillance-antimicrobial-resistance-Europe-2018.pdf (accessed July 1, 2020).
Evans, A., Hamouda, B., and Amyes, G. B. (2012). The rise of carbapenem-resistant Acinetobacter baumannii. Curr. Pharm. Des. 19, 223–238. doi: 10.2174/1381612811306020223
Fernández-Cuenca, F., Tomás-Carmona, M., Caballero-Moyano, F., Bou, G., Martínez-Martínez, L., Vila, J., et al. (2013). Actividad de 18 agentes antimicrobianos frente a aislados clínicos de Acinetobacter baumannii: segundo estudio nacional multicéntrico (proyecto GEIH-REIPI-Ab 2010). Enferm. Infecc. Microbiol. Clin. 31:353. doi: 10.1016/j.eimc.2013.03.001
Garnacho-Montero, J., Dimopoulos, G., Poulakou, G., Akova, M., Cisneros, J. M., De Waele, J., et al. (2015). Task force on management and prevention of Acinetobacter baumannii infections in the ICU. Intensive Care Med. 41, 2057–2075. doi: 10.1007/s00134-015-4079-4
Hawkey, P. M., and Livermore, D. M. (2012). Carbapenem antibiotics for serious infections. BMJ 344:e3236. doi: 10.1136/bmj.e3236
Kulah, C., Mooij, M. J., Comert, F., Aktas, E., Celebi, G., Ozlu, N., et al. (2010). Characterisation of carbapenem-resistant Acinetobacter baumannii outbreak strains producing OXA-58 in Turkey. Int. J. Antimicrob. Agents 36, 114–118. doi: 10.1016/j.ijantimicag.2010.03.017
Moreno-Morales, J., Vergara, A., Kostyanev, T., Rodriguez-Baño, J., Goossens, H., and Vila, J. (2020). Evaluation of a loop-mediated isothermal amplification assay to detect carbapenemases from Acinetobacter spp. directly from bronchoalveolar lavage fluid. bioRxiv [Preprint]. doi: 10.1101/2020.05.11.089904
Roca, I., Espinal, P., Vila-Farrés, X., and Vila, J. (2012). The Acinetobacter baumannii oxymoron: commensal hospital dweller turned pan-drug-resistant menace. Front. Microbiol. 3:148. doi: 10.3389/fmicb.2012.00148
Solé, M., Pitart, C., Roca, I., Fàbrega, A., Salvador, P., Muñoz, L., et al. (2011). First description of an Escherichia coli strain producing NDM-1 carbapenemase in Spain. Antimicrob. Agents Chemother. 55, 4402–4404. doi: 10.1128/aac.00642-11
Tacconelli, E., Carrara, E., Savoldi, A., Harbarth, S., Mendelson, M., Monnet, D. L., et al. (2018). Discovery, research, and development of new antibiotics: the WHO priority list of antibiotic-resistant bacteria and tuberculosis. Lancet Infect. Dis. 18, 318–327.
Torres, A., Niederman, M. S., Chastre, J., Ewig, S., Fernandez-Vandellos, P., Hanberger, H., et al. (2017). International ERS/ESICM/ESCMID/ALAT guidelines for the management of hospital-acquired pneumonia and ventilator-associated pneumonia. Eur. Respir. J. 50:1700582. doi: 10.1183/13993003.00582-2017
Vergara, A., Boutal, H., Ceccato, A., López, M., Cruells, A., Bueno-Freire, L., et al. (2020a). Assessment of a loop-mediated isothermal amplification (LAMP) assay for the rapid detection of pathogenic bacteria from respiratory samples in patients with hospital-acquired pneumonia. Microorganisms 8:103. doi: 10.3390/microorganisms8010103
Vergara, A., Moreno-Morales, J., Roca, I., Pitart, C., Kostyanev, T., Rodriguez-Baño, J., et al. (2020b). A comparative study between real-time PCR and loop-mediated isothermal amplification to detect carbapenemase and/or ESBL genes in Enterobacteriaceae directly from bronchoalveolar lavage fluid samples. J. Antimicrob. Chemother. 75, 1453–1457. doi: 10.1093/jac/dkaa031/5740616
Woodford, N., Ellington, M., Coelho, J., Turton, J., Ward, M., Brown, S., et al. (2006). Multiplex PCR for genes encoding prevalent OXA carbapenemases in Acinetobacter spp. Int. J. Antimicrob. Agents 27, 351–353. doi: 10.1016/j.ijantimicag.2006.01.004
Keywords: carbapenemases, Acinetobacter spp., bronchoalveolar lavage, detection, oxacillinases
Citation: Moreno-Morales J, Vergara A, Kostyanev T, Rodriguez-Baño J, Goossens H and Vila J (2021) Evaluation of a Loop-Mediated Isothermal Amplification Assay to Detect Carbapenemases Directly From Bronchoalveolar Lavage Fluid Spiked With Acinetobacter spp. Front. Microbiol. 11:597684. doi: 10.3389/fmicb.2020.597684
Received: 21 August 2020; Accepted: 07 December 2020;
Published: 13 January 2021.
Edited by:
Raffaele Zarrilli, University of Naples Federico II, ItalyReviewed by:
Katie Hopkins, Public Health England, United KingdomLaurent Dortet, Bicêtre Hospital, France
Copyright © 2021 Moreno-Morales, Vergara, Kostyanev, Rodriguez-Baño, Goossens and Vila. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jordi Vila, anZpbGFAY2xpbmljLmNhdA==
†These authors have contributed equally to this work