 Philip V. Peplow
Philip V. Peplow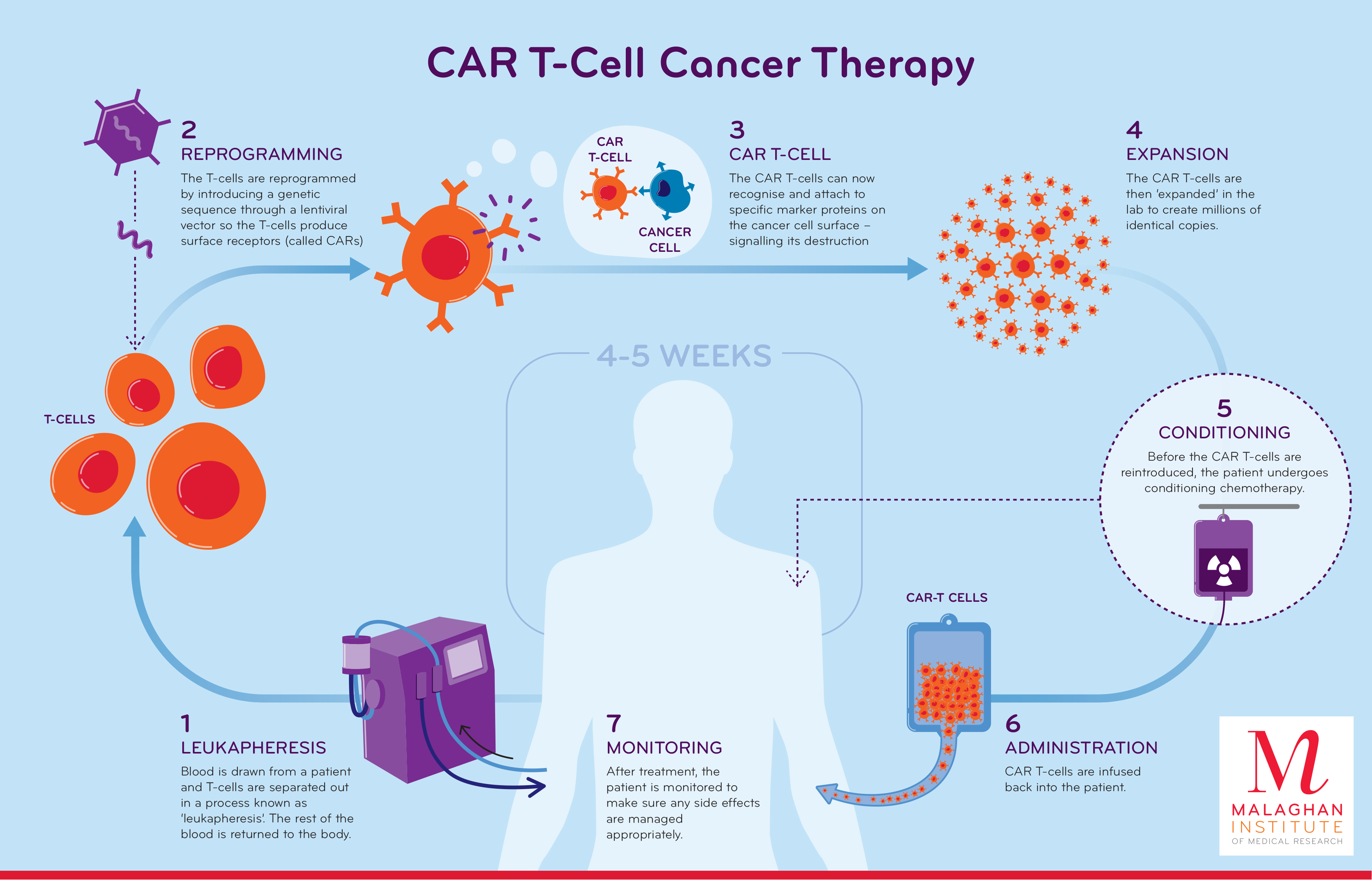{kind=link}

94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
OPINION article
Front. Med. Technol. , 11 April 2024
Sec. Animal Models in Medical Translation
Volume 6 - 2024 | https://doi.org/10.3389/fmedt.2024.1384648
Human subjects are living longer due to improvements in personal and medical care. However, this is associated with an increase in age-related diseases and disorders (e.g., neurodegenerative diseases such as Alzheimer's disease, Parkinson's disease; musculoskeletal disorders such as osteoarthritis, osteoporosis, rheumatoid arthritis; metabolic disorders such as obesity, diabetes; cardiovascular disorders such as heart failure, hypertension) with increased personal and hospital costs, and many patients having to be cared for in nursing homes. A major problem in countries such as China with a very large population is that there will not be sufficient specialized facilities to care for their aging population who develop dementia and other age-related disorders. The burden of disease due to cancer in China is significant with lifestyle-related cancers including lung cancer, colorectal cancer, and breast cancer increasing and being the most prevalent cancer types in China (1). Up till now, exercise and diet have been the main interventions used to slow down the aging process, and a recent study has demonstrated that caloric restriction may slow aging in humans (2).
Senescent cells, which increase in number over time, play a role in age-related tissue decline. Genetic removal of senescent cells can reduce various age-related pathologies, including metabolic dysfunction and decreased physical fitness. Drugs have been used to remove senescent cells but require continuous administration. Reprogramming patients' disease-fighting T cells to target diseased and senescent cells may be a way for human subjects to live a healthier, better quality of life, with fewer major illnesses. Low doses of genetically modified T cells could be administered to adults to destroy senescent cells, and this would avoid undesirable side effects possibly caused by large doses.
Like all white blood cells (which includes granulocytes, monocytes and lymphocytes, the latter comprising T and B cells), T cells are created in the bone marrow and mature in the thymus acquiring special markers that determine whether they will become a helper or killer T cell. A unique receptor on the surface of each cell can recognize one type of antigen on antigen-presenting cells. Helper T cells play the main role in coordinating an immune response once, for example, a virus or bacteria has been identified. Helper T cells in the thymus acquire a protein marker known as CD4, whereas T cells in the thymus that acquire a protein marker known as CD8 become cytotoxic, or killer, T cells. These T cells can recognize and destroy tumor cells.
A recent study in young mice found that genetically modified (reprogrammed) T cells erased age-related deterioration by targeting senescent cells and the mice regained their youthful characteristics while also avoiding inflammation. Giving reprogrammed T cells to aged mice caused them to rejuvenate (3). There are several reports of successfully using genetically engineered T cells to treat human cancer patients (4). Also, it has been shown that CD8 T cells can infiltrate the brain in mice and was dependent on luminal expression of major histocompatibility complex class 1 by cerebral endothelium (5). This suggests that genetically modified T cells can cross the blood brain barrier and could be used in the neuro-oncology setting (6) and possibly to treat other brain diseases.
Leukapheresis is used to obtain healthy white blood cells to treat patients by chimeric antigen receptor (CAR)-T cells. Most CAR-T cells are produced from autologous peripheral blood mononuclear cells (PBMCs), followed by T cell selection, activation, gene modification, and expansion (7). The T cells are reprogrammed by genetic modification that may involve introducing a genetic sequence through a lentiviral vector so that the T cells produce surface receptors called CARs. The CAR-T cells can now attach to specific marker proteins on the surface of targeted cells leading to their destruction. The CAR-T cells are increased in number ex vivo and, after the cancer patients have received chemotherapy, are administered back to the patient, with monitoring to ensure any side effects are managed appropriately (8). This technique has the potential to treat cancers, diabetes, autoimmune and inflammatory diseases.
Clinical studies with first generation CAR-T cells had poor results due to the low number of these cells existing in vivo. By incorporating co-stimulatory signal domains from CD28, 4-1BB, CD134 or an inducible co-stimulator into the CAR intracellular structure, the number of the CAR-T cells was significantly improved and they had promising results in cancer patients. Third-generation CARs have been developed to include not only CD3ζ (CD247) and one co-stimulatory domain but also an additional co-stimulatory signal (9). Fourth-generation CAR-T cells co-express some key cytokines or co-stimulatory ligands, such as IL-12, IL-15, and IL-7, or suicide genes, which significantly enhance the expansion activity of T cells. To avoid host immune rejection or graft-vs.-host disease against transplanted CAR-T cells, it has been proposed for fifth generation CAR-T cells to knock out the human leukocyte antigen (HLA) and T-cell receptor (TCR) genes of T cells obtained from healthy donors (10–12). This strategy can be used for the treatment of multiple patients as it would not require being modified depending on the patient (11).
CAR-T cells co-expressing ligand proteins of immune activating receptors, such as 4-1BB ligand (4-1BB-L) or ICOS ligand ICOS-L), to produce co-stimulatory signaling (13, 14) have been developed. CD38 CAR-T cells with CD28 signaling and 4-1BB-L co-stimulatory signaling had a potent anti-tumor effect (13).
The commercial production of CAR-T cells has several limitations including the rather long time between their production and administration, with the need for bridging therapy, the requirement to cryopreserve the product, and issues with accessibility and affectability (15). Some of these limitations could be overcome by point of care CAR-T cells with shorter time from production to administration and thus not requiring cryopreservation or bridging therapy. Several technologies are being developed to increase and optimize the production of next generation CAR-T cells. Apheresis is the most widely used method in commercial CAR-T cell production protocols. Apheresis collects the mononuclear cell layer from anticoagulated whole blood, with patients being connected to a device that moves peripheral blood through a single-use disposable tubing set. The blood is separated by centrifugal force into appropriate density bands for isolation and collection of the desired cell layer. The use of automated manufacturing stations may enhance capacity and throughput without introducing significant product handling (16).
In the USA, the FDA approved CAR-T cell therapies in 2017, and the one-time treatments has led to unprecedented response rates in patients with diffuse large B cell lymphoma and B-cell acute lymphocytic leukemia. In the UK, it was approved in 2018 for treating children and adults with lymphoma and leukaemia. In the USA, an infusion of CAR-T cell therapy costs approximately $400,000, while in the UK the tisagenlecleucel form of CAR-T, also known as Kymriah, costs around £282,000 per patient at its full list price. In Canada, the total cost of CD 19-targeted CAR-T cell therapy was estimated to be $62,500 per patient in the first year, and of patient monitoring and follow-up for five years following CAR-T cell administration estimated to be $17,160 (17). In the USA the cost of treating cancer patients with several lines of chemotherapy vs. CAR-T cell therapies is considered not to be very different. In India, CAR-T cell therapy with actalycabtagene autoleucel has been undertaken in 38 patients with lymphoma and 15 with leukemia: 26 of 38 patients with lymphoma (68%) and 11 of 15 patients with leukemia (72%) responded to the treatment. All of the patients in the leukemia group had no signs of cancer. None of the 53 patients developed the neurologic side effects that are often seen in patients treated with CAR-T cell therapies approved in the USA, and only a small proportion (5%) had a severe form of an immune-related side effect known as cytokine release syndrome. Only five patients required hospitalization because of side effects. The cost of NexCAR 19 treatment is expected to be approximately $50,000 (18). As more pharma companies and laboratories become involved with this new technology, the costs are likely to become lower as further advances and innovations take place. Some hospitals have introduced a scoring system to aid selection of patients for CAR-T cell therapy (19, 20) and maximize benefit for patients (21). By using CAR-T cell therapy to slow age-related decline in health, the number of patients requiring hospital treatment (e.g., for cancer) would be reduced leading to a substantial saving in healthcare costs. Some medical insurance companies cover the cost of CAR-T cell therapy.
At present, CAR-T cell therapy has been used for treating lymphoma and leukaemia cancer patients. Recently, it has been shown that glioblastoma, a very aggressive brain cancer, shrinks after CAR-T cell therapy (22). A team in Australia is investigating the use of CAR-T Reg cells to suppress the immune response that attacks the pancreas, causing type 1 diabetes (23). In laboratory models, CAR-T Reg cells have shown great potential for treating asthma (24), hemophilia (25) and autoimmune diseases (26).
Firstly, it would be important to replicate the findings of CAR-T cell therapy in young and aged mice as reported by Amor et al. (3). Normal healthy mice could be used, and then possibly to treat some mouse models of neurodegenerative disease (e.g., Alzheimer's disease, Parkinson's disease) and perform behavioral testing to see if there is an improvement in memory/learning/movement. Clinical trials could be started with healthy human subjects to examine safety and tolerability of low dose CAR-T cell therapy.
This is a personal opinion of an emerging treatment modality that could have significant impact on slowing age-related decline in human health and wellbeing, as well as reducing personal and hospital costs. Further information can be found in the cited references.
PP: Writing – original draft.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. He S, Xia C, Li H, Cao M, Yang F, Yan X, et al. Cancer profiles in China and comparisons with the USA: a comprehensive analysis in the incidence, mortality, survival, staging, and attribution to risk factors. Sci China Life Sci. (2024) 67:122–31. doi: 10.1007/s11427-023-2423-1
2. Waziry R, Ryan CP, Corcoran DL, Huffman KM, Kobor MS, Kothari M, et al. Effect of long-term caloric restriction on DNA methylation measures of biological aging in healthy adults from the CALERIE trial. Nat Aging. (2023) 3:248–57. doi: 10.1038/s43587-022-00357-y
3. Amor C, Fernández-Maestre I, Chowdhury S, Ho YJ, Nadella S, Graham C, et al. Prophylactic and long-lasting efficacy of senolytic CAR T cells against age-related metabolic dysfunction. Nat Aging. (2024) 4:336–49. doi: 10.1038/s43587-023-00560-5
4. Zhao L, Cao YJ. Engineered T cell therapy for cancer in the clinic. Front Immunol. (2019) 10:2250. doi: 10.3389/fimmu.2019.02250
5. Galea I, Bernardes-Silva M, Forse PA, van Rooijen N, Liblau RS, Perry VH. An antigen-specific pathway for CD8 T cells across the blood-brain barrier. J Exp Med. (2007) 204:2023–30. doi: 10.1084/jem.20070064
6. Patterson JD, Henson JC, Breese RO, Bielamowicz KJ, Rodriguez A. CAR T cell therapy for pediatric brain tumors. Front Oncol. (2020) 10:1582. doi: 10.3389/fonc.2020.01582
7. Pessach I, Nagler A. Leukapheresis for CAR-T cell production and therapy. Transfus Apher Sci. (2023) 62:103828. doi: 10.1016/j.transci.2023.103828
8. Malaghan Institute of Medical Research. CAR-T cell cancer therapy. Available online at: https://www.malaghan.org.nz/assets/Uploads/MMR-CAR-T-Infographic-V4-High-Res4-5-WEEKS2.jpg (accessed March 24, 2024).
9. Tang XY, Sun Y, Zhang A, Hu GL, Cao W, Wang DH, et al. Third-generation CD28/4-1BB chimeric antigen receptor T cells for chemotherapy relapsed or refractory acute lymphoblastic leukaemia: a non-randomised, open-label phase I trial protocol. BMJ Open. (2016) 6:e013904. doi: 10.1136/bmjopen-2016-013904
10. Ren J, Liu X, Fang C, Jiang S, June CH, Zhao Y. Multiplex genome editing to generate universal CAR T cells resistant to PD1 inhibition. Clin Cancer Res. (2017) 23:2255–66. doi: 10.1158/1078-0432.CCR-16-1300
11. Soria JC, Ohe Y, Vansteenkiste J, Reungwetwattana T, Chewaskulyong B, Lee KH, et al. Osimertinib in untreated EGFR-mutated advanced non-small-cell lung cancer. N Eng J Med. (2018) 378:113–25. doi: 10.1056/NEJMoa1713137
12. Zhao J, Lin Q, Song Y, Liu D. Universal CARs, universal T cells, and universal CAR T cells. J Hematol Oncol. (2018) 11:132. doi: 10.1186/s13045-018-0677-2
13. Drent E, Poels R, Ruiter R, van de Donk NWCJ, Zweegman S, Yuan H, et al. Combined CD28 and 4-1BB costimulation potentiates affinity-tuned chimeric antigen receptor-engineered T cells. Clin Cancer Res. (2019) 25:4014–25. doi: 10.1158/1078-0432.CCR-18-2559
14. Hu W, Huang X, Huang X, Chen W, Hao L, Chen Z. Chimeric antigen receptor modified T cell (CAR-T) co-expressed with ICOSL-41BB promote CAR-T proliferation and tumor rejection. Biomed Pharmacother. (2019) 118:109333. doi: 10.1016/j.biopha.2019.109333
15. Fried S, Shkury E, Itzhaki O, Sdayoor I, Yerushalmi R, Shem-Tov N, et al. Point-of-care anti-CD19 chimeric antigen receptor T-cell therapy for relapsed/refractory follicular lymphoma. Leuk Lymphoma. (2023) 64:1956–63. doi: 10.1080/10428194.2023.2246611
16. Abou-El-Enein M, Elsallab M, Feldman SA, Fesnak AD, Heslop HE, Marks P, et al. Scalable manufacturing of CAR T cells for cancer immunotherapy. Blood Cancer Discov. (2021) 2:408–22. doi: 10.1158/2643-3230.BCD-21-0084
17. Lachaine J, Jain MD, Bibeau J, Marino JP. PCN191 Cost associated with implementation of CAR T-cell therapy for the management of hematologic cancers in Canada. Value Health. (2021) 24(Suppl1):S55. doi: 10.1016/j.jval.2021.04.282
18. NIH. India’s first homegrown CAR T-Cell therapy has roots in NCI collaboration. Available online at: https://www.cancer.gov/news-events/cancer-currents-blog/2024/nexcar19-car-t-cell-therapy-india-nci-collaboration (accessed March 24, 2024).
19. Faiman B, Khouri J, Williams LS, Anwer F. Ethical challenges in CAR-T slot allocation. Transplant Cell Ther. (2023) 29:215–6. doi: 10.1016/j.jtct.2023.03.003
20. Faiman B, Valent J, Khouri J, Williams L, Samaras CJ, Mazzoni S, et al. P-007: proposed clinical factor scoring system for chimeric antigen receptor T-cell (CAR T) patient selection in relapsed and refractory multiple myeloma (RRMM). Clin Lymphoma Myeloma Leuk. (2022) 22:S39–40. doi: 10.1016/S2152-2650(22)00337-8
21. Kourelis T, Bansal R, Berdeja J, Siegel D, Patel K, Mailankody S, et al. Ethical challenges with multiple myeloma BCMA chimeric antigen receptor T cell slot allocation: a multi-institution experience. Transplant Cell Ther. (2023) 29:255–8. doi: 10.1016/j.jtct.2023.01.012
22. Bagley SJ, Logun M, Fraietta JA, Wang X, Desai AS, Bagley LJ, et al. Intrathecal bivalent CAR T cells targeting EGFR and IL13Rα2 in recurrent glioblastoma: phase 1 trial interim results. Nat Med. (2024). doi: 10.1038/s41591-024-02893-z
23. Diabetes Australia. New cell therapy to”switch off” the effects of type 1diabetes. Available online at: https://www.diabetesaustralia.com.au/mediarelease/new-cell-therapy-type-1-diabetes/ (accessed March 24, 2024).
24. Skuljec J, Chmielewski M, Happle C, Habener A, Busse M, Abken H, et al. Chimeric antigen receptor-redirected regulatory T cells suppress experimental allergic airway inflammation, a model of asthma. Front Immunol. (2017) 8:1125. doi: 10.3389/fimmu.2017.01125
25. Yoon J, Schmidt A, Zhang AH, Königs C, Kim YC, Scott DW. FVIII-specific human chimeric antigen receptor T-regulatory cells suppress T- and B-cell responses to FVIII. Blood. (2017) 129:238–45. doi: 10.1182/blood-2016-07-727834
Keywords: reprogramming T cells, treatment, age-related decline, human, health
Citation: Peplow PV (2024) Reprogramming T cells as an emerging treatment to slow human age-related decline in health. Front. Med. Technol. 6:1384648. doi: 10.3389/fmedt.2024.1384648
Received: 10 February 2024; Accepted: 1 April 2024;
Published: 11 April 2024.
Edited by:
Michael Liebman, IPQ Analytics, United StatesReviewed by:
Hui Xie, Antengene Corporation, China© 2024 Peplow. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Philip V. Peplow cHZwZXBsb3dAZ21haWwuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.