
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Med. , 10 March 2025
Sec. Gastroenterology
Volume 12 - 2025 | https://doi.org/10.3389/fmed.2025.1433849
This article is part of the Research Topic Foods, Dietary Supplements, and Herbal Products Treating the Diseases of the 21st Century: Moving from Traditional to Scientific Research: Volume II View all 16 articles
 Hui Yu1Ling Li1Jing Gu2Jing Wang3Hui Su4Hui Lu5Yuqing Zhou6Jingfang Xia7Yongping Xu8Danhua Liang9Yuling Yang10
Hui Yu1Ling Li1Jing Gu2Jing Wang3Hui Su4Hui Lu5Yuqing Zhou6Jingfang Xia7Yongping Xu8Danhua Liang9Yuling Yang10 Ying Chen10*
Ying Chen10*Background: To investigate the knowledge, attitude, and practice (KAP) of patients with gastric cancer (GC) toward nutritional therapy.
Methods: This cross-sectional study was conducted from January to March 2024 at the Affiliated Hospital of Jiangnan University (Wuxi, China) and enrolled patients with GC. Questionnaires (Cronbach’s α = 0.923) were used to collect data on demographics and KAP dimensions. Scores >75% were considered good. Multivariable analyses were performed to examine the factors associated with KAP. A structural equation modeling (SEM) analysis was performed to examine the relationships among KAP dimensions.
Results: The analysis included 486 valid questionnaires. The median knowledge, attitude, and practice scores were 6.0 (0–16; 37.5%), 26.0 (7–35; 74.3%), and 28.7 (8–40; 71.7%) indicating poor KAP. Only agricultural, forestry, animal husbandry, fishery, and water conservancy production personnel (OR = 0.09, 95%CI: 0.02–0.49, p = 0.006) were independently associated with knowledge. Knowledge (OR = 1.11, 95%CI: 1.05–1.18, p < 0.001) and a monthly income of 10,000–20,000 (OR = 3.85, 95%CI: 1.23–12.06, p = 0.021) were independently associated with attitude. Knowledge (OR = 1.22, 95%CI: 1.15–1.30, p < 0.001), attitude (OR = 1.21, 95%CI: 1.11–1.32, p < 0.001), personnel other than leading cadres of state organs and enterprises (all OR < 1 and all p < 0.05), and a monthly income of 10,000–20,000 yuan (OR = 3.02, 95%CI: 1.15–7.96, p = 0.025) were independently associated with practice. Knowledge had a direct positive influence on attitude (β = 0.350, p < 0.001) and practice (β = 0.460, p < 0.001) and an indirect positive influence on practice (β = 0.146, p < 0.001). Attitude had a direct positive influence on practice (β = 0.417, p < 0.001).
Conclusion: Patients with GC in Wuxi partly had poor KAP toward nutritional support.
In recent years, the overall incidence of gastric cancer has been gradually declining worldwide, passing from the fifth most common cancer to the sixth position (1), but it remains a high-incidence cancer in China, with 43.9% of the global cases (2). Being a major player in the digestive system, removing the stomach (in part or totally) will compromise the digestive and nutritional functions of the patient (3, 4). Patients with advanced gastric cancer can also experience malnutrition preoperatively, compromising the perioperative period due to the decline in skeletal muscle mass and function, leading to increased rates of postoperative complications, nosocomial infections, mortality, prolonged hospitalization, decreased quality of life, and increased medical expenses (5, 6). In advanced stages, malnutrition in patients with gastric cancer can also lead to increased rates of adverse reactions during chemotherapy, decreased treatment tolerance, and reduced treatment completion rates, impacting treatment efficacy and quality of life and ultimately resulting in poorer survival (7). Factors such as inadequate nutrient intake, weight loss, and undergoing anti-tumor treatments (including surgery, radiotherapy, and systemic therapies) are considerations for selecting indications for nutritional intervention (7, 8). Currently, nutritional support for patients with gastric cancer aims primarily to preserve lean body tissue, reduce the occurrence of complications during the perioperative and peri-chemotherapy periods, ensure the safe completion of radical gastrectomy, ensure completion of adequate doses and courses of radiotherapy and chemotherapy, ultimately improving efficacy and prognosis, and realizing benefits from a health economics perspective (6, 9, 10).
In patients still able to feed by themselves, selecting healthy foods that will optimize energy and nutrient intake is paramount. For patients who will need nutritional support, having some knowledge about nutritional support and nutrition in the context of cancer could help the discussion with healthcare providers and translate into better choices and practice. Knowledge, attitude, and practice (KAP) surveys are research tools that provide quantitative and qualitative data about the gaps, misconceptions, and misunderstandings that can impair the optimal performance of a specific subject in a specific population (11, 12). KAP studies are particularly useful to design interventional and motivational interventions in a specific population. One study investigated the beliefs and experiences of patients with esophageal cancer toward nutritional support, but only in the peri-radiotherapy period (13). A recent study identified “caregiver self-efficacy and preparedness,” “caregiver needs are neglected,” and “nutrition as a source of conflict” as barriers to optimal nutrition in patients with gastric cancer (14). A systematic review highlighted that Chinese cancer patients have a poor KAP toward healthy eating (15). Nevertheless, the KAP of patients with gastric cancer regarding nutritional therapy remains unclear.
Hence, this study aimed to investigate the KAP of patients with gastric cancer toward nutritional therapy. The results could help design interventions to improve the KAP of patients toward nutritional status, which could translate into better patient outcomes.
The study was reported according to the Checklist for Reporting Results of Internet E-Surveys (CHERRIES) (Supplementary material) (16).
This cross-sectional study was conducted from January to March 2024 at the Affiliated Hospital of Jiangnan University (Wuxi, China) and enrolled patients with gastric cancer through convenience sampling. This study was approved by the Medical Ethics Committee of the Affiliated Hospital of Jiangnan University (Ethic No. LS2023102). All participants provided written or online informed consent before completing the survey.
The inclusion criteria were (1) patients with gastric cancer who have undergone surgery and (2) agreed to participate in the study. The exclusion criteria were (1) severe cognitive impairment, (2) mental abnormalities, or (3) any conditions that prevent normal communication or ability to complete a questionnaire.
The design of the questionnaire was based on guidelines on nutritional support in cancer patients (17–20) and relevant literature (21). After the initial design, feedback was sought from five senior oncology nursing experts, six experts in oncology nursing and nursing management, and three associate chief oncologists. The questionnaire was subsequently revised based on their suggestions and underwent a pilot study with a small sample size (23 respondents), resulting in a reliability coefficient (Cronbach’s α) of 0.923.
The final questionnaire was in Chinese and consisted of four sections: demographic information (age, gender, residence, education level, occupation type, average monthly household income, marital status, medical insurance type, cancer classification, etc.), knowledge dimension, attitude dimension, and practice dimension. The knowledge dimension comprised two aspects with a total of eight questions, with 2 points for “very knowledgeable,” 1 point for “heard about it,” and 0 points for “not sure,” with a score range of 0–16 points. The attitude dimension consisted of seven questions scored using a 5-point Likert scale ranging from “strongly agree” (5 points) to “strongly disagree” (1 point), with a score range of 7–35 points. The practice dimension includes eight questions, which are also scored using a 5-point Likert scale ranging from “always” (5 points) to “never” (1 point), with a score range of 8–40 points. Adequate knowledge, positive attitude, and proactive practice were defined as a total score of each dimension >75% (22).
This study combined online questionnaire filling and paper questionnaires. Participation in the study was voluntary, and no incentives were offered. Except for the modes of administration and responding, the two questionnaires were exactly the same, differing only in the mode of administration and response collection. All items were listed one after the other online and on the paper-based questionnaire. Paper questionnaires were distributed to the participants during inpatient and outpatient visits. The online questionnaire was distributed via Questionnaire Star1 to the participants. The participants could scan the QR code using WeChat or follow the provided link to access and complete the questionnaire. The survey was closed and limited to those receiving the QR code or obtaining a paper copy. The participants were assured of anonymity during the survey process. All data are stored on the secure servers at the corresponding author’s center. The research team was comprised of three nurses trained as research assistants. They were responsible for questionnaire promotion and distribution and the meticulous review of all submissions for completeness, internal consistency, and logical coherence. The investigators were trained to grasp the problem’s meaning and the investigation process, enhancing data accuracy and consistency. Responses to all items were mandatory for submission of the online questionnaire. The questionnaires containing incomplete answers (paper questionnaires missing one or more responses), questionnaires with uniform responses across all items, and questionnaires with all the knowledge items responded with “not sure” (which could raise doubt the questionnaire was read or answered carefully) were considered invalid.
The sample size should ideally be at least 10 times the number of predictors (23). With 23 independent variables in this questionnaire, the minimum sample size required would be 230. Accounting for a 20% non-response rate, the final necessary sample size would be 288.
The variables were tested for normal distribution using the Kolmogorov–Smirnov test. Normally distributed continuous data were presented as means ± standard deviations and analyzed using Student’s t-test (two-level comparisons) or ANOVA (comparison of more than two levels). Continuous data with a skewed distribution were presented as medians (interquartile ranges) and analyzed using the Mann-Whiney U-test (two-level comparisons) of the Kruskall-Wallis H-test (comparisons of more than two levels). Categorical data were presented as n (%). The correlations between KAP dimension scores were assessed using the Pearson correlation coefficient for data that meet the assumptions of normal distribution and the Spearman correlation coefficient for data that do not. Variables with a univariable p-value <0.1 were included in the multivariable analyses. Incorporating the KAP theoretical framework, a structural equation model (SEM) was used to verify whether attitudes mediate the relationship between knowledge and behavioral practices. The indirect and direct effects were calculated and compared. The threshold criteria for goodness-of-fit indices of the SEM model were RMSEA < 0.08, SRMR < 0.08, TLI > 0.8, and CFI > 0.8. If the goodness-of-fit thresholds cannot be met, path analysis was conducted to test the mediation effects. Statistical analysis was performed using Stata 18.0 (StataCorp LLC, College Station, TX, USA). p-values were reported to three decimals, and two-sided p-values <0.05 were considered statistically significant.
In this study, 503 questionnaires were distributed (301 online and 202 paper), but 17 were considered invalid (all knowledge items answered with “not sure”). Hence, this analysis included 486 valid questionnaires. There were 291 (59.9%) males; 23.5, 31.9, and 29.4% of the participants were 50–59, 60–69, and ≥70 years old, respectively. The highest frequencies were observed for urban residents (59.5%), junior high school and below education (64.2%), ordinary staff and related personnel (33.3%), family monthly income of 5,000–10,000 CNY (37.4%), married (92.0%), and with medical insurance (98.8%) (Table 1).
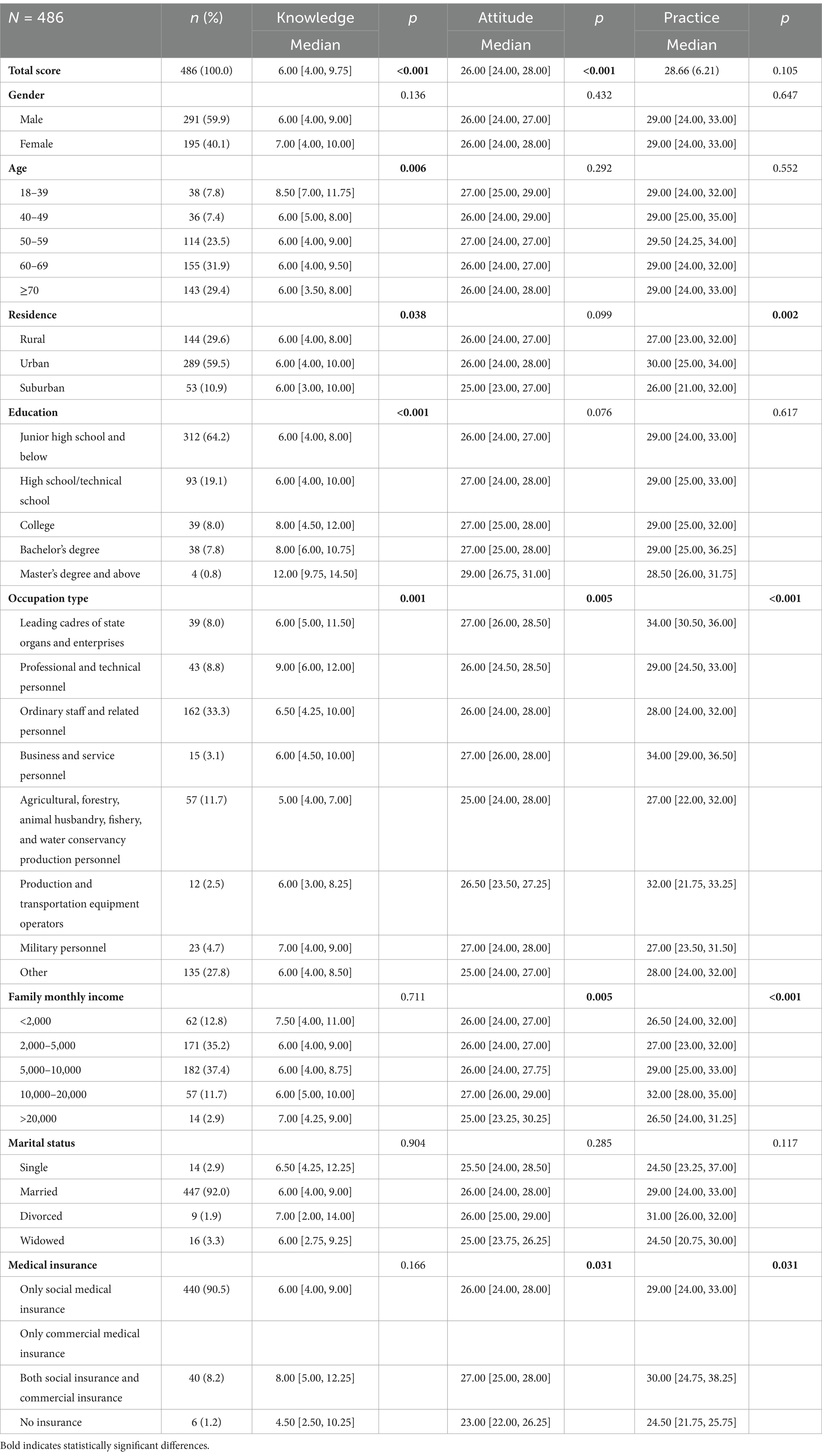
Table 1. Characteristics of the participants.
The median knowledge score was 6.0 (0–16; 37.5%), indicating poor knowledge. Differences in knowledge were observed according to age (p = 0.006), residence (p = 0.038), education (p < 0.001), and occupation (p = 0.001) (Table 1). The knowledge item with the highest score was K1 (25.9% very familiar; 61.5% heard of; “Malnutrition is common among gastric cancer patients, and compared to other tumors, gastric cancer is more prone to causing severe and prolonged malnutrition.”). The item with the lowest score was K4 (11.9% very familiar; 33.3% heard of; “During surgery, the energy intake goal for patients is measured based on actual measurements or calculated at 104.65 to 125.58 kilojoules per kilogram of body weight, and the protein intake goal is 1.2 to 1.5 grams per kilogram of body weight.”) (Table 2).
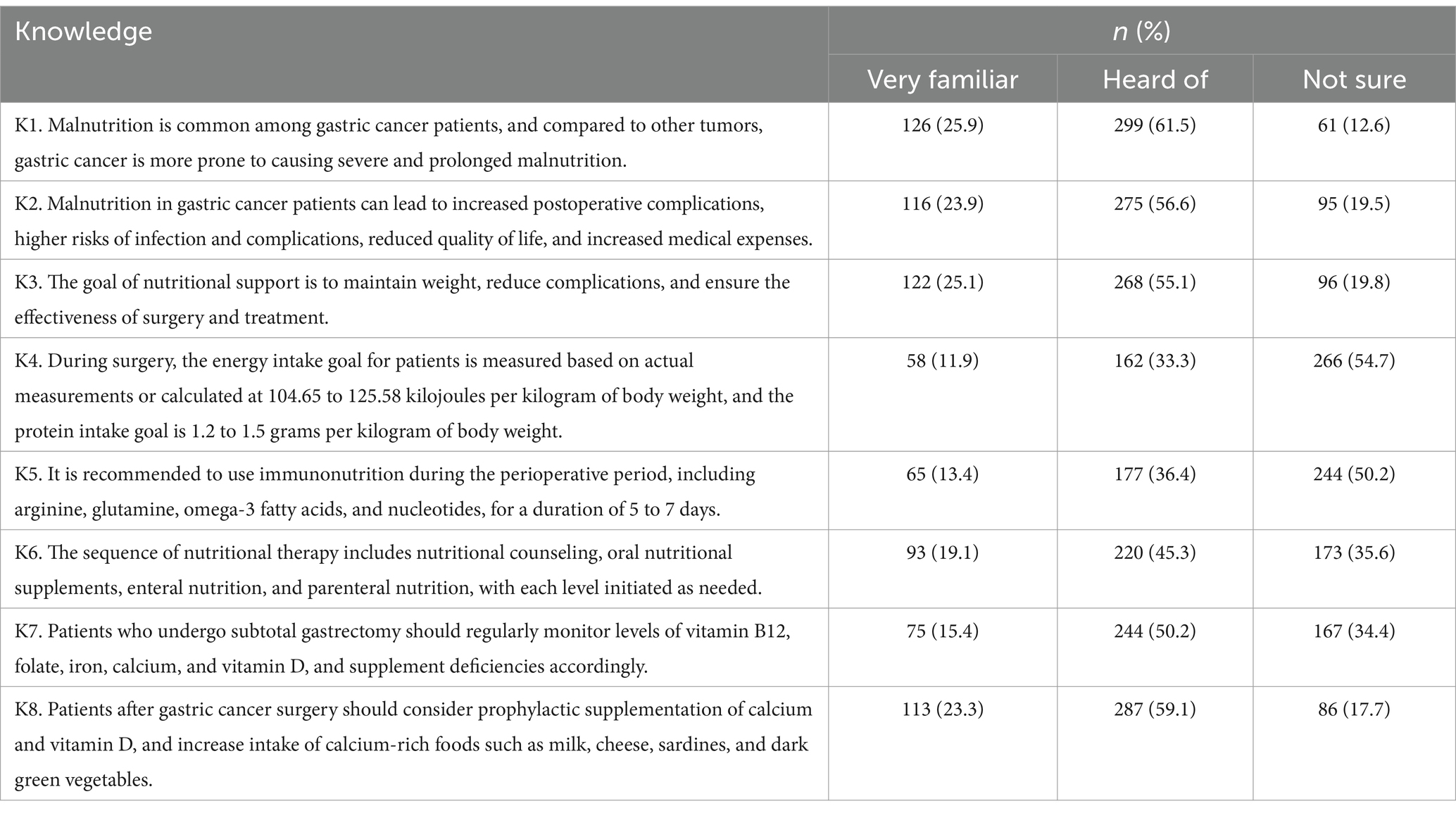
Table 2. Knowledge.
The median attitude score was 26.0 (7–35; 74.3%), indicating a negative attitude. Differences in attitude were observed according to occupation (p = 0.005), income (p = 0.005), and insurance (p = 0.031) (Table 1). The attitude item with the highest score was A2 (93.9% agree; “During the perioperative and peri-chemotherapy periods, I need to pay special attention to my nutritional intake to reduce complications and improve treatment outcomes.”). The item with the lowest score was A7 (60.5% agree; “I am worried that nutritional therapy will increase my financial burden, and I am unsure if I can afford the associated costs.”) (Table 3).
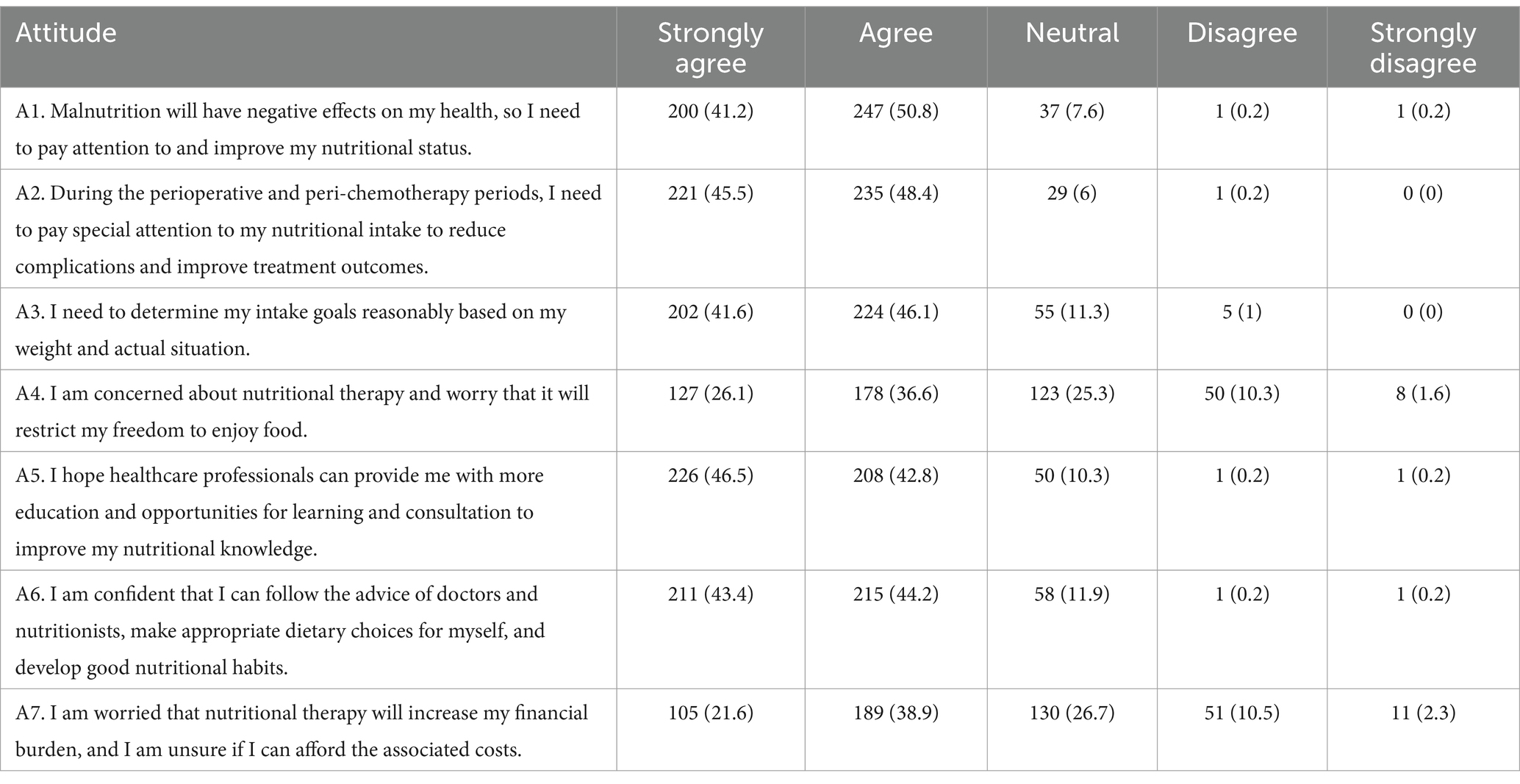
Table 3. Attitude.
The median practice score was 28.7 (8–40; 71.7%), indicating poor practice. Differences in practice were observed according to residence (p = 0.002), occupation (p < 0.001), income (p < 0.001), and insurance (p = 0.031) (Table 1). The practice item with the highest score was P3 (74.3% consistent; “I will choose foods rich in vitamins and minerals, such as fresh fruits, vegetables, whole grains, and low-fat dairy products, to support immune system function and overall health.”). The item with the lowest score was P7 (39.9% consistent; “I will actively participate in nutritional education activities to enhance my knowledge of nutritional therapy.”) (Table 4).
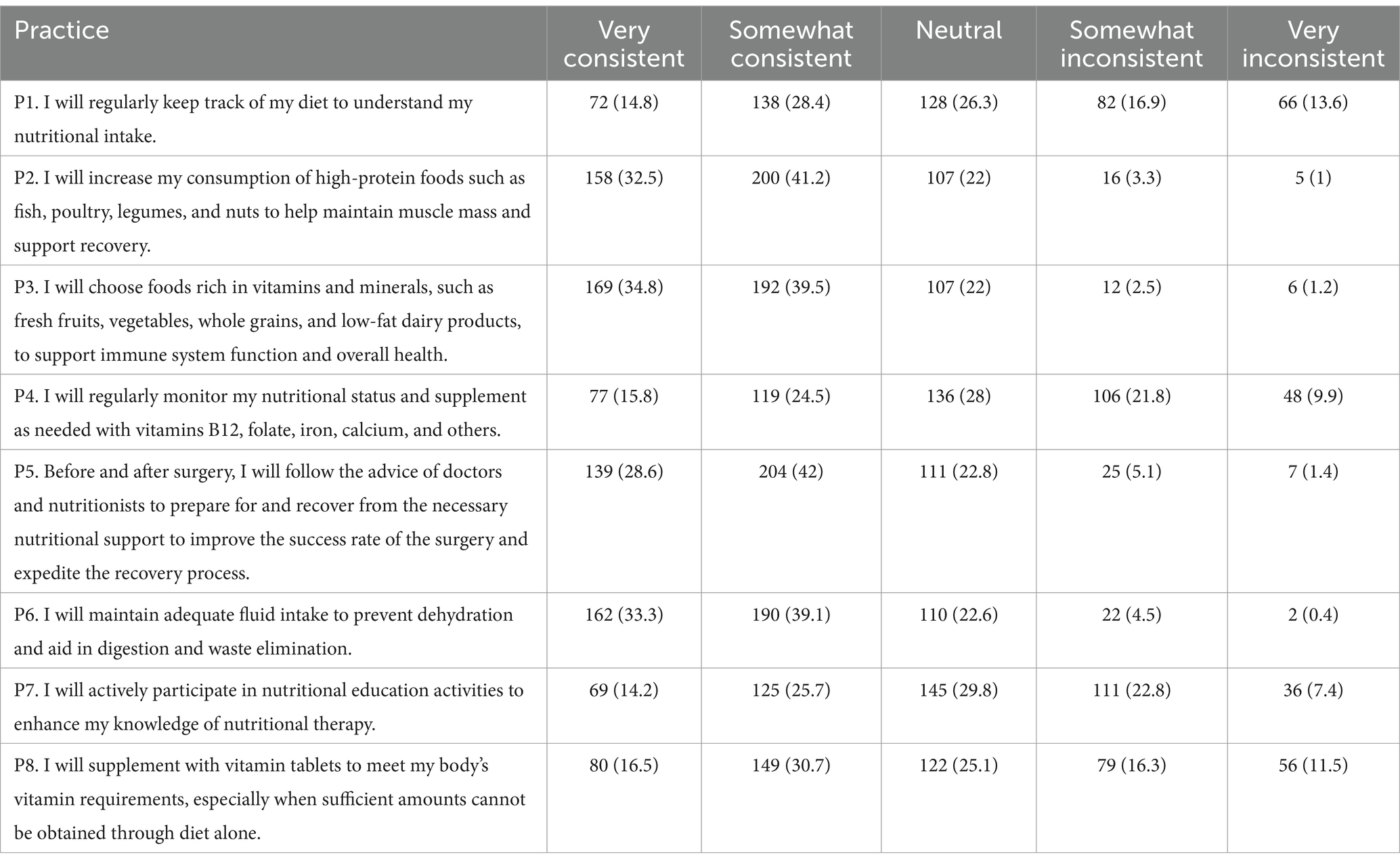
Table 4. Practice.
As shown in Table 5, the knowledge scores correlated to the attitude (r = 0.174, p < 0.001) and practice (r = 0.387, p < 0.001) scores, while the attitude scores correlated to the practice scores (r = 0.374, p < 0.001).
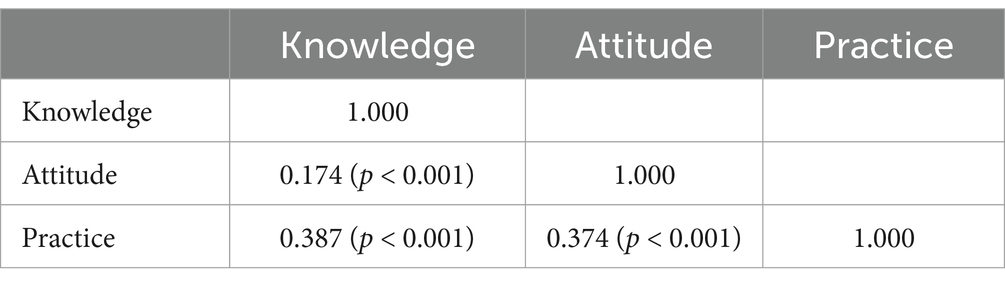
Table 5. Correlation analysis.
Only agricultural, forestry, animal husbandry, fishery, and water conservancy production personnel (OR = 0.09, 95%CI: 0.02–0.49, p = 0.006) were independently associated with knowledge (Table 6). The knowledge scores (OR = 1.11, 95%CI: 1.05–1.18, p < 0.001) and a monthly income of 10,000–20,000 yuan (OR = 3.85, 95%CI: 1.23–12.06, p = 0.021) were independently associated with the attitude scores (Table 7). The knowledge scores (OR = 1.22, 95%CI: 1.15–1.30, p < 0.001), the attitude scores (OR = 1.21, 95%CI: 1.11–1.32, p < 0.001), professional and technical personnel (OR = 0.21, 95%CI: 0.06–0.73, p = 0.014), ordinary staff and related personnel (OR = 0.25, 95%CI: 0.08–0.75, p = 0.013), military personnel (OR = 0.22, 95%CI: 0.06–0.88, p = 0.032), other personnel (OR = 0.31, 95%CI: 0.10–0.95, p = 0.040), and a monthly income of 10,000–20,000 (OR = 3.02, 95%CI: 1.15–7.96, p = 0.025) were independently associated with the practice scores (Table 8).
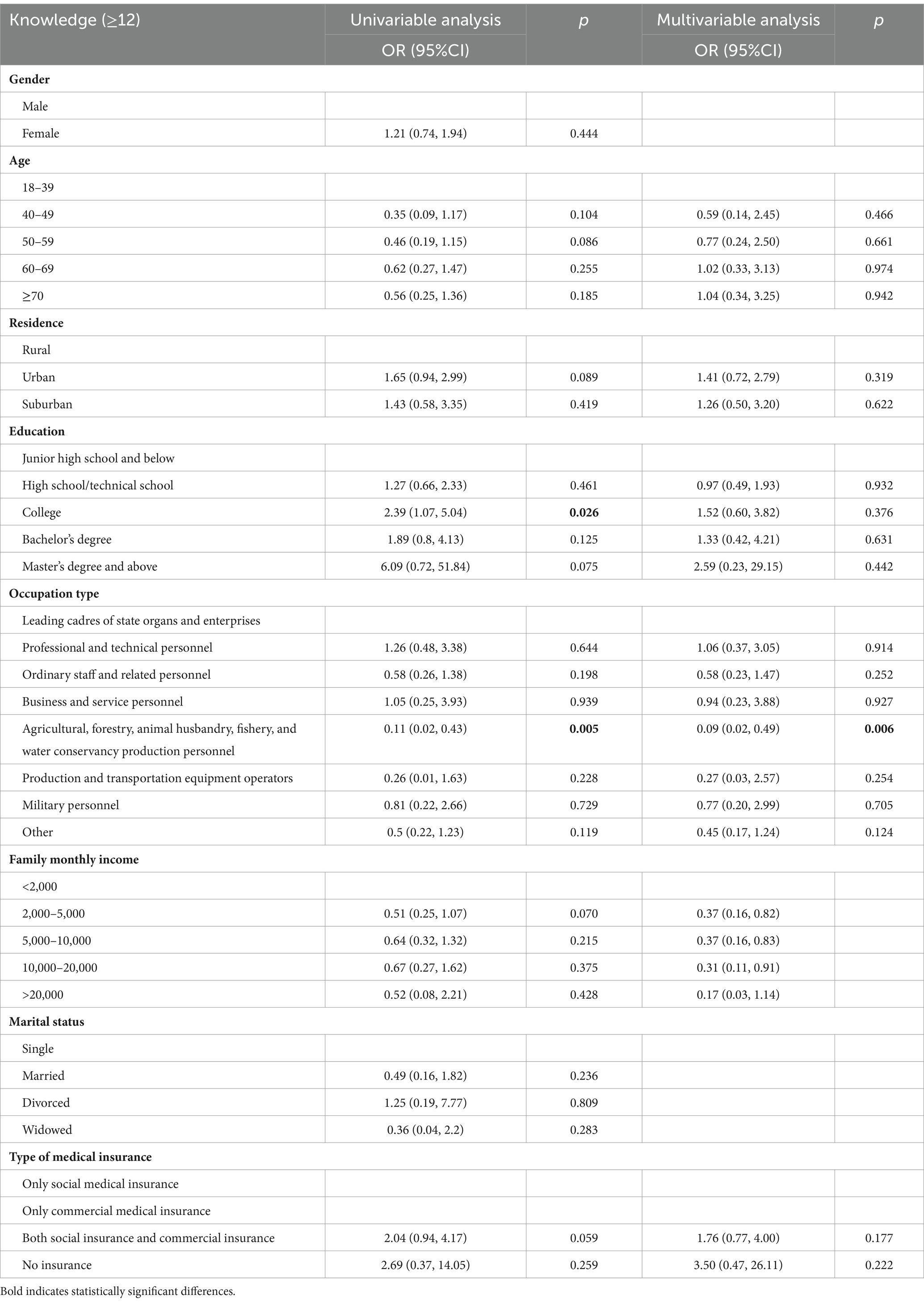
Table 6. Univariable and multivariable analyses of knowledge.
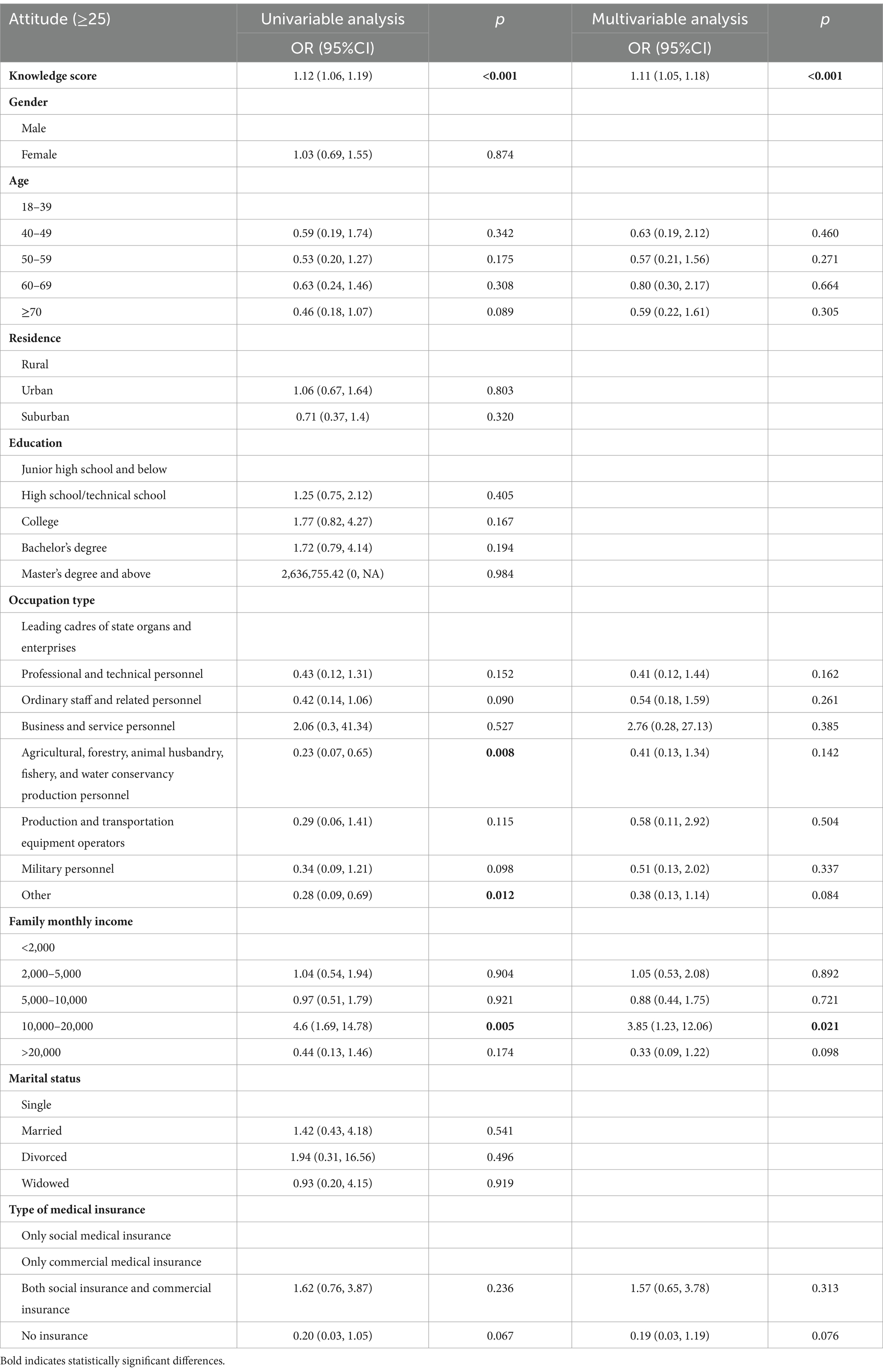
Table 7. Univariable and multivariable analyses of attitude.
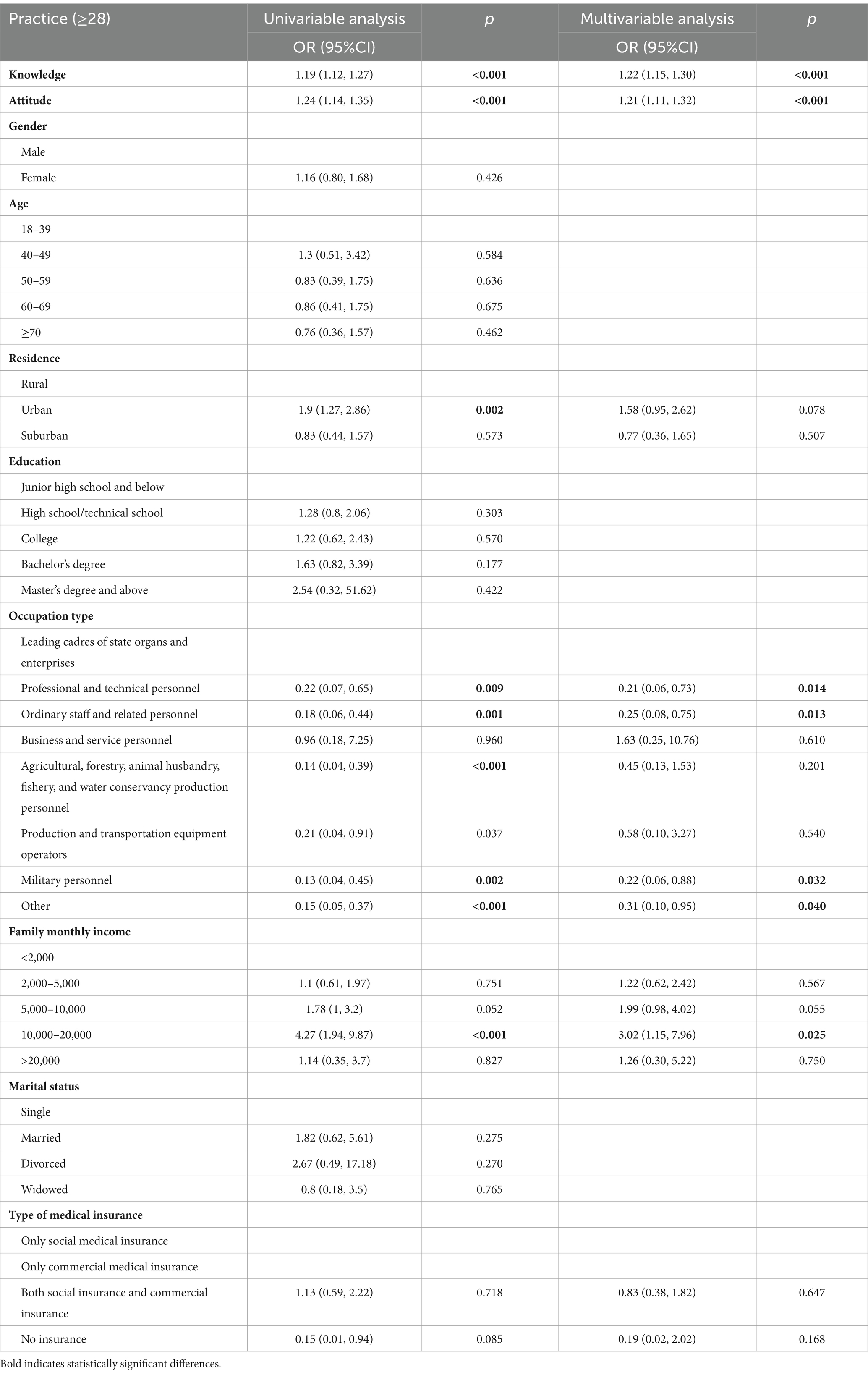
Table 8. Univariable and multivariable analyses of practice.
The SEM is depicted in Figure 1. All four SEM fit indices showed good fit (Table 9). Knowledge had a direct positive influence on attitude (β = 0.350, p < 0.001) and practice (β = 0.460, p < 0.001) and an indirect positive influence on practice (β = 0.146, p < 0.001). Attitude had a direct positive influence on practice (β = 0.417, p < 0.001) (Table 10).
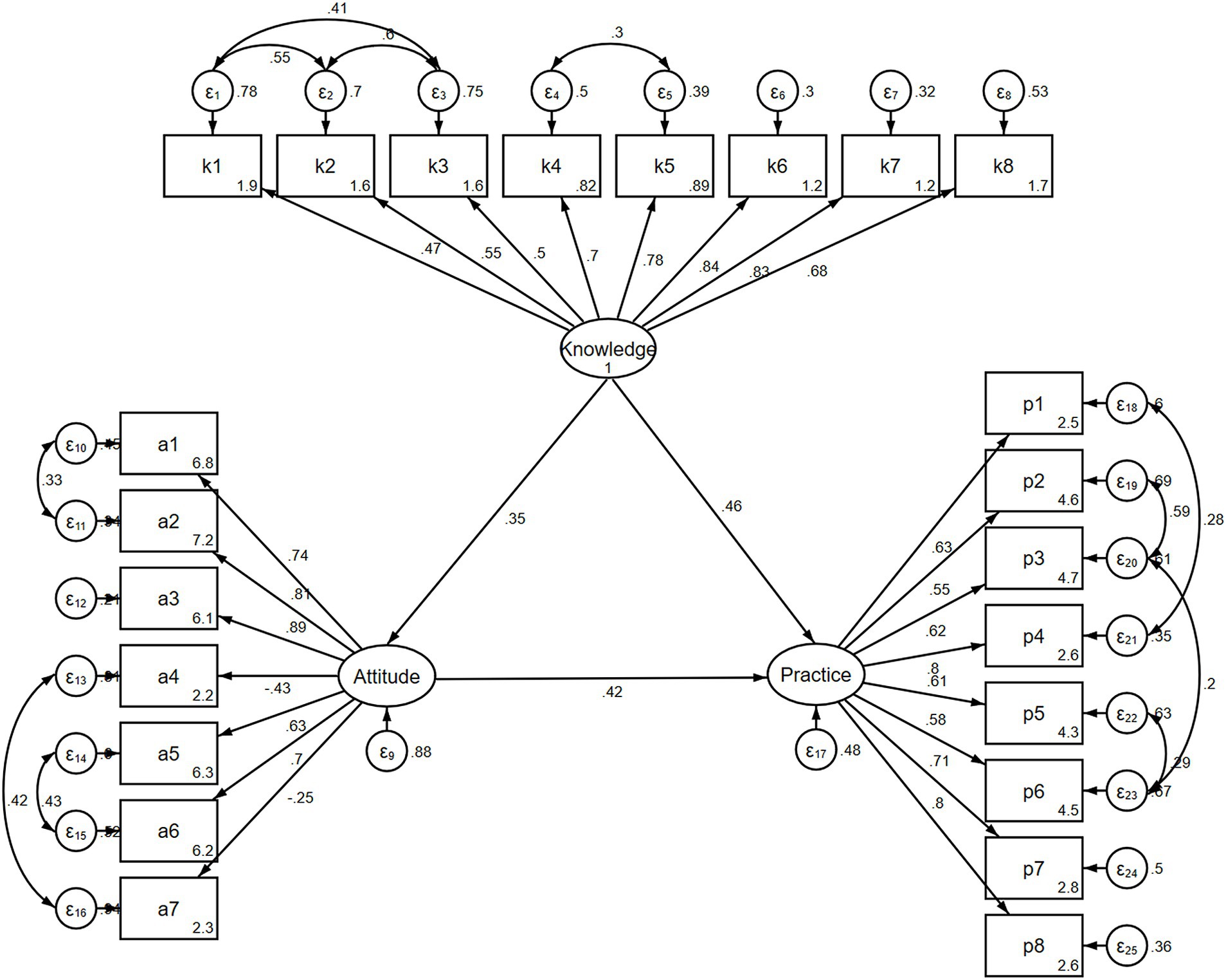
Figure 1. Structural equation modeling.
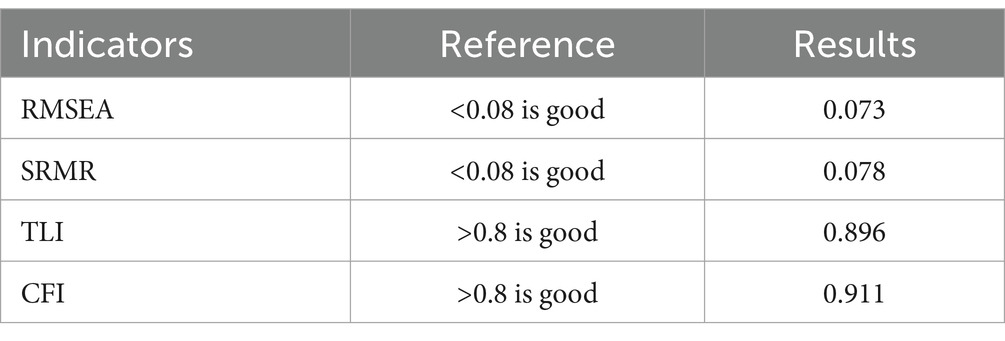
Table 9. SEM fit indicators.

Table 10. SEM analysis.
Proper nutritional support is crucial in cancer patients due to the physiological stresses of the cancer, surgery, radiotherapy, and chemotherapy (19). Nutritional support in patients with GC is particularly important due to the impact of the cancer and then gastrectomy on digestion and nutrition (3, 4). A proper nutritional status is conducive to a better prognosis (6, 9, 10). Still, maintaining a proper nutritional status requires knowledge and attitude to make adequate lifestyle choices and be able to make informed choices about medical nutritional support. The present study of patients with gastric cancer in Wuxi indicates that the KAP toward nutritional support is poor. No previous studies examined the question in patients with GC, but a previous study of patients with esophageal cancer in the peri-radiotherapy period showed that the lack of nutrition-related knowledge, a lack of motivation, and factors related to nutrition were the main barriers to maintaining a proper nutritional status, supporting the present study. Tang et al. (15) also reported that Chinese cancer patients had a poor KAP toward healthy eating. Although nutritional support might be perceived as secondary to cancer therapies by the patients, healthcare providers should provide adequate information about nutrition to the patients. Still, a study showed that digestive surgeons had poor KAP toward nutritional support to cancer patients (24). Although the KAP of physicians was not assessed in the present study, it should be investigated in the future to design continuing education activities to improve the KAP of physicians. Indeed, healthcare providers are widely regarded as crucial sources of reliable health-related knowledge by patients (25, 26). Poor knowledge in the physicians could lead to inaccurate information being transferred to the patients.
The correlation, multivariable, and SEM analyses showed that knowledge influenced attitude and practice, and attitude influenced practice. Hence, improving knowledge through education activities should translate into better practice, as supported by the KAP theory (11, 12, 27). The KAP conceptual framework considers knowledge to be the basis for practice and that attitudes are the force driving practice (11, 12, 27). Hence, improving knowledge should lead to more positive attitudes and more proactive practices.
The multivariable analyses revealed a positive association between superior job positions and higher income levels with better KAP. It is widely acknowledged that individuals with higher socioeconomic status tend to possess greater healthcare literacy (28). Therefore, it is imperative to meticulously screen patients and implement tailored educational interventions to enhance healthcare outcomes. The present study suggests that patients with GC with a lower income and lower job position could be the ones most in need of proper education about nutrition in GC.
Translating KAP findings into actionable recommendations is an important step in maximizing the impact of such studies. The KAP conceptual framework assumes that improving knowledge can lead to more positive attitudes and proactive practices (11, 12, 27). Based on its findings, the present study identified specific knowledge gaps and demographic groups that could benefit from targeted interventions. All eight knowledge items showed poor scores, highlighting the need for education of patients with GC regarding nutritional support, including the risk of malnutrition in GC, the goal of nutritional support, the content and administration of nutritional support in patients with GC, and the need for the supplementation of specific micronutrients and vitamins. In addition, knowledge scores were lower in individuals not having desk occupations, which are often associated with a lower socioeconomic status. The results could inform the design of a nutritional information and education campaign tailored to the specific needs of the population in Wuxi City, focusing on agricultural, forestry, animal husbandry, fishery, and water conservancy production personnel and individuals with a lower income to highlight knowledge about the risk of malnutrition in GC, the health hazards associated with malnutrition in the oncological context, the goal of malnutrition, the proper energy intake, proper nutrients after surgery, the types of nutrition after surgery, and the prophylactic use of specific vitamins and micronutrients. On a policy level, guidelines and consensuses for nutritional support in patients with gastric cancer are available (6, 9, 10, 29), and policymakers and stakeholders should be aware of such guidelines and provide support and resources to the physicians and patients to help them implement optimal nutritional support after gastric cancer. Teaching patients what and how to eat after gastric cancer is important, but some patients could require more support to achieve optimal outcomes. Various support programs are available in different provinces and countries. Nutritional support programs for patients with gastric cancer can help with eating difficulties, weight loss, and side effects. Programs may include nutrition counseling, adapted recipes, and cooking demonstrations (6, 9, 10, 30, 31).
This study had limitations. It was a single-center study that enrolled participants from a single geographical area, limiting generalizability. The study was cross-sectional, preventing the analysis of causality. The participants were selected through convenience sampling, which could introduce bias, and future studies should consider probability sampling. A SEM analysis was performed to examine causality, but causality is statistically inferred instead of being observed, and the results must be taken cautiously (32–34). In addition, the data represent a single point in time, but they could serve as a historical control to examine the effects of future interventions on KAP. All KAP studies are at risk of social desirability bias, according to which the participants can be tempted to answer what they know they should think and do instead of what they actually do (35, 36). Considering that all KAP scores were poor, that bias is less likely. All data were self-reported. Since the accuracy of self-reported clinical data relies directly on the degree of understanding of the patient regarding his/her condition, precise clinical data were not collected from the patients because of the high risks of various biases. In addition, linking the questionnaire to the patient’s chart was not possible because the questionnaires were completed anonymously. Therefore, including the exact condition of the patients in the analysis was not possible. In order to accommodate as many participants as possible and to avoid the bias introduced by having access to the internet, the questionnaire was administered online and on paper. Although all questionnaires were filled out by the participants themselves, the setting where the participant completed it (e.g., at home vs. at the hospital) could have influenced the results. Finally, a health education session was not provided after participation, which could be considered in future studies.
In conclusion, patients with GC in Wuxi demonstrated poor KAP regarding nutritional support. Socioeconomic status was a significant factor affecting KAP, with lower KAP observed in patients with a lower socioeconomic status. Knowledge was found to influence attitudes and practices, while attitudes influenced practices. These findings suggest that improving patient education could enhance the KAP toward nutritional support in the population of patients with GC.
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
This study was approved by the Medical Ethic Committee of Affiliated Hospital of Jiangnan University (LS2023102). The participants provided their written or online informed consent to participate in this study.
HY: Conceptualization, Methodology, Project administration, Resources, Writing – original draft, Writing – review & editing. LL: Investigation, Project administration, Visualization, Writing – original draft, Writing – review & editing. JG: Investigation, Methodology, Writing – original draft, Writing – review & editing. JW: Formal analysis, Investigation, Writing – original draft, Writing – review & editing. HS: Formal analysis, Methodology, Writing – original draft, Writing – review & editing. HL: Conceptualization, Methodology, Writing – original draft, Writing – review & editing. YZ: Data curation, Project administration, Writing – original draft, Writing – review & editing. JX: Project administration, Resources, Writing – original draft, Writing – review & editing. YX: Data curation, Formal analysis, Writing – original draft, Writing – review & editing. DL: Investigation, Methodology, Writing – original draft, Writing – review & editing. YY: Conceptualization, Formal analysis, Writing – original draft, Writing – review & editing. YC: Data curation, Formal analysis, Writing – original draft, Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2025.1433849/full#supplementary-material
1. Sung, H, Ferlay, J, Siegel, RL, Laversanne, M, Soerjomataram, I, Jemal, A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. (2021) 71:209–49. doi: 10.3322/caac.21660
2. Yan, X, Lei, L, Li, H, Cao, M, Yang, F, He, S, et al. Stomach cancer burden in China: epidemiology and prevention. Chin J Cancer Res. (2023) 35:81–91. doi: 10.21147/j.issn.1000-9604.2023.02.01
3. Gharagozlian, S, Mala, T, Brekke, HK, Kolbjornsen, LC, Ullerud, AA, and Johnson, E. Nutritional status, sarcopenia, gastrointestinal symptoms and quality of life after gastrectomy for cancer - a cross-sectional pilot study. Clin Nutr ESPEN. (2020) 37:195–201. doi: 10.1016/j.clnesp.2020.03.001
4. Wang, HM, Wang, TJ, Huang, CS, Liang, SY, Yu, CH, Lin, TR, et al. Nutritional status and related factors in patients with gastric Cancer after gastrectomy: a cross-sectional study. Nutrients. (2022) 14:2634. doi: 10.3390/nu14132634
5. Kim, KW, Lee, K, Lee, JB, Park, T, Khang, S, Jeong, H, et al. Preoperative nutritional risk index and postoperative one-year skeletal muscle loss can predict the prognosis of patients with gastric adenocarcinoma: a registry-based study. BMC Cancer. (2021) 21:157. doi: 10.1186/s12885-021-07885-7
6. Serra, F, Pedrazzoli, P, Brugnatelli, S, Pagani, A, Corallo, S, Rosti, G, et al. Nutritional support management in resectable gastric cancer. Drugs Context. (2022) 11:1–11. doi: 10.7573/dic.2022-5-1
7. Arends, J. Malnutrition in cancer patients: causes, consequences and treatment options. Eur J Surg Oncol. (2023) 50:107074. doi: 10.1016/j.ejso.2023.107074
8. Santarpia, L, Contaldo, F, and Pasanisi, F. Nutritional screening and early treatment of malnutrition in cancer patients. J Cachexia Sarcopenia Muscle. (2011) 2:27–35. doi: 10.1007/s13539-011-0022-x
9. Rosania, R, Chiapponi, C, Malfertheiner, P, and Venerito, M. Nutrition in patients with gastric cancer: an update. Gastrointest Tumors. (2016) 2:178–87. doi: 10.1159/000445188
10. Carrillo Lozano, E, Oses Zarate, V, and Campos Del Portillo, R. Nutritional management of gastric cancer. Endocrinol Diabetes Nutr Engl Ed. (2021) 68:428–38. doi: 10.1016/j.endien.2020.09.005
11. Andrade, C, Menon, V, Ameen, S, and Kumar Praharaj, S. Designing and conducting knowledge, attitude, and practice surveys in psychiatry: practical guidance. Indian J Psychol Med. (2020) 42:478–81. doi: 10.1177/0253717620946111
12. World Health Organization. Advocacy, communication and social mobilization for TB control: a guide to developing knowledge, attitude and practice surveys. (2008). Available online at: http://whqlibdoc.who.int/publications/2008/9789241596176_eng.pdf (Accessed November 22, 2022).
13. Wang, P, Zheng, X, Luo, Z, Wang, Y, Guo, Z, and Zhou, Y. Perceptions and experiences of nutritional management needs for patients with esophageal cancer during the peri-radiotherapy period: a qualitative study. Asia Pac J Oncol Nurs. (2022) 9:202–9. doi: 10.1016/j.apjon.2022.01.002
14. Milliron, BJ, Klobodu, C, Deutsch, J, Martyn, K, Dychtwald, D, Riahi, E, et al. “Keep your chin up, and keep eating”: perceptions of barriers and facilitators to healthful dietary behaviors among individuals with gastrointestinal cancer and caregivers. Cancer Control. (2023) 30:10732748231208316. doi: 10.1177/10732748231208316
15. Tang, H, Zhang, Y, Cao, B, Liang, Y, Na, R, Yang, Z, et al. Knowledge, attitudes and behaviors toward healthy eating among Chinese cancer patients treated with chemotherapy: a systematic review. Asia Pac J Oncol Nurs. (2023) 10:100163. doi: 10.1016/j.apjon.2022.100163
16. Eysenbach, G. Improving the quality of web surveys: the checklist for reporting results of internet E-surveys (CHERRIES). J Med Internet Res. (2004) 6:e34. doi: 10.2196/jmir.6.3.e34
17. Caccialanza, R, Pedrazzoli, P, Cereda, E, Gavazzi, C, Pinto, C, Paccagnella, A, et al. Nutritional support in cancer patients: a position paper from the Italian Society of Medical Oncology (AIOM) and the Italian Society of Artificial Nutrition and Metabolism (SINPE). J Cancer. (2016) 7:131–5. doi: 10.7150/jca.13818
18. de Las Penas, R, Majem, M, Perez-Altozano, J, Virizuela, JA, Cancer, E, Diz, P, et al. SEOM clinical guidelines on nutrition in cancer patients (2018). Clin Transl Oncol. (2019) 21:87–93. doi: 10.1007/s12094-018-02009-3
19. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines). Survivorship. Version 1.2023. Fort Washington: National Comprehensive Cancer Network (2023).
20. Muscaritoli, M, Arends, J, Bachmann, P, Baracos, V, Barthelemy, N, Bertz, H, et al. ESPEN practical guideline: Clinical Nutrition in cancer. Clin Nutr. (2021) 40:2898–913. doi: 10.1016/j.clnu.2021.02.005
21. Kim, H, Suh, EE, Lee, HJ, and Yang, HK. The effects of patient participation-based dietary intervention on nutritional and functional status for patients with gastrectomy: a randomized controlled trial. Cancer Nurs. (2014) 37:E10–20. doi: 10.1097/NCC.0b013e31829193c8
22. Obagha, EC, Ajayi, I, Abdullahi, GA, and Umeokonkwo, CD. Clients’ satisfaction with preventive services for malaria during pregnancy in Anambra state, Nigeria. BMC Public Health. (2020) 20:1660. doi: 10.1186/s12889-020-09767-2
23. Naqvi, AA, Hassali, MA, Rizvi, M, Zehra, A, Nisa, ZU, Islam, MA, et al. Validation of the general medication adherence scale in Pakistani patients with rheumatoid arthritis. Front Pharmacol. (2020) 11:1039. doi: 10.3389/fphar.2020.01039
24. Duran-Poveda, M, Suarez-de-la-Rica, A, Cancer Minchot, E, Ocon-Breton, J, Sanchez-Pernaute, A, and Rodriguez-Caravaca, G. Knowledge and practices of digestive surgeons concerning specialized nutritional support in cancer patients: a survey study. Nutrients. (2022) 14:4764. doi: 10.3390/nu14224764
25. Alduraywish, SA, Altamimi, LA, Aldhuwayhi, RA, AlZamil, LR, Alzeghayer, LY, Alsaleh, FS, et al. Sources of health information and their impacts on medical knowledge perception among the Saudi Arabian population: cross-sectional study. J Med Internet Res. (2020) 22:e14414. doi: 10.2196/14414
26. Swoboda, CM, Van Hulle, JM, McAlearney, AS, and Huerta, TR. Odds of talking to healthcare providers as the initial source of healthcare information: updated cross-sectional results from the health information National Trends Survey (HINTS). BMC Fam Pract. (2018) 19:146. doi: 10.1186/s12875-018-0805-7
27. Kaliyaperumal, K. Guideline for conducting a knowledge, attitude and practice. AECS Illumination. (2004) 4:7–9.
28. Svendsen, MT, Bak, CK, Sorensen, K, Pelikan, J, Riddersholm, SJ, Skals, RK, et al. Associations of health literacy with socioeconomic position, health risk behavior, and health status: a large national population-based survey among Danish adults. BMC Public Health. (2020) 20:565. doi: 10.1186/s12889-020-08498-8
29. Mizukami, T, and Piao, Y. Role of nutritional care and general guidance for patients with advanced or metastatic gastric cancer. Future Oncol. (2021) 17:3101–9. doi: 10.2217/fon-2021-0186
30. Zhang, Y, Zhang, J, Zhu, L, Hao, J, He, F, Xu, T, et al. A narrative review of nutritional therapy for gastrointestinal cancer patients underwent surgery. J Investig Surg. (2023) 36:2150337. doi: 10.1080/08941939.2022.2150337
31. Johnston, EA, Ayre, SK, Au-Yeung, YT, and Goodwin, BC. A scoping review of group nutrition education and cooking programs for people affected by cancer. J Acad Nutr Diet. (2024) 124:1302–1327.e1. doi: 10.1016/j.jand.2024.02.011
32. Beran, TN, and Violato, C. Structural equation modeling in medical research: a primer. BMC Res Notes. (2010) 3:267. doi: 10.1186/1756-0500-3-267
33. Fan, Y, Chen, J, and Shirkey, G. Applications of structural equation modeling (SEM) in ecological studies: an updated review. Ecol Process. (2016) 5:19. doi: 10.1186/s13717-016-0063-3
34. Kline, RB. Principles and practice of structural equation modeling. Fifth ed. New York: The Guilford Press (2023).
35. Bergen, N, and Labonte, R. “Everything is perfect, and we have no problems”: detecting and limiting social desirability bias in qualitative research. Qual Health Res. (2020) 30:783–92. doi: 10.1177/1049732319889354
Keywords: knowledge, attitude, practice, gastric cancer, patients, nutritional support, cross-sectional study
Citation: Yu H, Li L, Gu J, Wang J, Su H, Lu H, Zhou Y, Xia J, Xu Y, Liang D, Yang Y and Chen Y (2025) Knowledge, attitudes, and practices of gastric cancer patients toward nutritional therapy. Front. Med. 12:1433849. doi: 10.3389/fmed.2025.1433849
Edited by:
Ana Sanches Silva, National Institute for Agricultural and Veterinary Research (INIAV), PortugalReviewed by:
Venkatarao Epari, Institute of Medical Sciences and Sum Hospital, IndiaCopyright © 2025 Yu, Li, Gu, Wang, Su, Lu, Zhou, Xia, Xu, Liang, Yang and Chen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ying Chen, amRmeV8xODMwNjBAdmlwLnFxLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.