 Magnus Akerstrom
Magnus Akerstrom Jens Wahlström
Jens Wahlström Agneta Lindegård1,2
Agneta Lindegård1,2
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Med., 17 January 2025
Sec. Healthcare Professions Education
Volume 11 - 2024 | https://doi.org/10.3389/fmed.2024.1509023
This article is part of the Research TopicBurnout, Wellbeing and Resilience of Healthcare Workers in the Post-COVID WorldView all 16 articles
Introduction: The healthcare sector is globally experiencing increasing demands and workplace interventions on an organisational level is sought to create healthy workplaces. The aim of this study was to provide an overview of Nordic research on the work environment and health of healthcare professionals, with a focus on identifying organisational-level risk and health-promoting factors.
Methods: This systematic search and review was based on an analysis of studies published in peer-reviewed journals between 1 January 2016 and 3 January 2023. The selected studies investigate the relationships between organisational-level risk and health-promoting factors and measures of health and well-being among healthcare professionals during ordinary operations. To increase applicability, this systematic search and review was limited to the Nordic countries as they share the same context with a publicly-funded widely accessible healthcare system. A total of 2,677 articles were initially identified, with 95 original studies meeting the criteria for relevance and quality.
Results: Identified organisational risk and health-promoting factors were categorised into five categories: work schedule distribution, operations design and work methods, ergonomic conditions, working conditions and personnel policies, and the organisation’s ethical environment. In addition, two themes across the categories emerged, providing further insight into the implications for practice. The first theme emphasises risk and health-promoting factors in the actions that employers take to fulfil the organisation’s goals. The second theme emphasises risk and health-promoting factors in connection with the ability of employees to do their jobs at a level of quality they deem acceptable.
Conclusion: Several organisational-level risk and health-promoting factors were identified, and the results indicate that the actions that employers take to fulfil the health-care organisation’s goals and promote the ability of employees to provide high-quality care are important for the health and wellbeing of healthcare employees.
High-quality healthcare is essential for social welfare, and attention to the health and wellbeing of healthcare workers is a crucial aspect of this effort. Reduced health in healthcare workers can have adverse effects on the individual healthcare workers. In addition, it may also lead to reduced quality in patient care, the risk of accidents, and challenges attracting and retaining a skilled workforce. Maintaining healthcare workers´ health is especially important since the competition for healthcare professionals is increasing due to an aging population in many societies (1–6). Despite this, healthcare in Europe is recognised as a high-risk sector from an employee wellbeing perspective (7), and healthcare workers report the highest levels of work-related stress compared to other professionals (8). They also experience poor wellbeing (9, 10) and physical symptoms (11).
Challenges within the healthcare sector arise from demands connected to healthcare work, which include contact with distressed and ill patients, work overload, up-to-date learning, and high-quality standards of performance (8). In addition, ongoing medical developments have resulted in growing demands for speed, complexity, and responsibility; an increased administrative burden, and reduced autonomy among healthcare workers (12, 13). In order to maintain healthy workplaces, job demands need to be manageable, and workers need to have access to sufficient resources to balance these demands (14). This challenging situation is not unique to Europe, and the World Health Organization (WHO) estimates that within the healthcare sector alone, there will be a shortfall of 10 million employees globally by 2030 (15).
Creating healthy workplaces requires organisational approaches that aim to improve working conditions and the organisation of work, rather than individual approaches that aim to improve workers’ competencies, knowledge, and coping capacity (16–18). In addition, instead of simply preventing harm, an approach that focuses on promoting employee wellbeing has been recommended as a way to improve working conditions within the healthcare sector (19). Such organisational-level interventions require not just in-depth knowledge of the healthcare sector (i.e., challenges, structure, and processes imbedded in that system and culture) but also knowledge on risk and health-promoting factors (i.e., working conditions that increase the likelihood of illness among employees or reduce the likelihood of health, and increase the likelihood of health among employees or reduce the risk of illness, respectively) that may be targeted (20, 21).
At present, the knowledge of the impact of risk and health-promoting factors on the workplace level within the healthcare sector is extensive, as a wide range of systematic reviews have been performed. These systematic reviews have provided evidence of the associations between burnout and a high workload, time constraints, value incongruence, low level of control, insufficient support from colleagues and managers, lack of collaboration, inadequate rewards, insufficient staffing, shifts exceeding 12 h, limited scheduling flexibility and uncertain employment conditions (22–25); musculoskeletal disorders and pain due to awkward working postures, a large number of patients, administrative work, vibration, and repetitive work (26, 27); and job satisfaction with workload and income, responsibility, recognition, autonomy and collaboration (28, 29).
However, there is still limited knowledge of the underlying causes of the presence or absence of these risk and health-promoting factors (i.e., risk and health-promoting factors on a higher organisational level). Following the principles of the hierarchy of controls for occupational safety and health (30, 31), risks to health and wellbeing should be reduced or eliminated by targeting the organisational level rather than the workplace or individual level. Thus, there is an urgent need to increase knowledge on organisational-level risk and health-promoting factors that may be used to improve the health of employees within the healthcare sector. To increase applicability to practice, this systematic review was limited to the Nordic context (Denmark, Finland, Iceland, Norway and Sweden), where all countries have a publicly-funded, widely accessible healthcare system (32).
The aim of this study was to provide an overview of Nordic research on the work environment and health of healthcare professionals, with a focus on identifying organisational-level risk and health-promoting factors.
Due to the multifaceted nature of organisational-level risk and health-promotive factors, in combination with the absence of earlier systematic reviews that could be used to guide the search, a broad scope that incorporates multiple study types rather than focusing on a single preferred study design had to be used. Thus, this study was carried out as a systematic search and review with a narrative summary (33) and reported according to the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) 2020 statement (34); see supporting information on-line Supplementary material (Prisma 2020 checklist). This study has not been reviewed by the Swedish Ethical Review Authority. This is not required for this type of study according to the Swedish Ethical Review Act. Informed consent to participate was not applicable in this study. No protocol exists for this review, since it was first commissioned as a part of a government assignment to the Swedish Agency for Work Environment Expertise and the absence of ethical review requirements.
Studies investigating health-related risk and health-promoting factors for healthcare professionals in the Nordic countries that were published in peer-reviewed journals between 1 January 2016 and 3 January 2023 were included. The start date of the searches was a pragmatic choice used to increase the relevance of the included studies by reflecting the current context and normal operations. The search strategy was structured according to SPIDER (sample, phenomenon of interest, design, evaluation, and type of research) as we expected a wide range of study designs, including quantitative, qualitative, and mixed method designs (35). Studies were included if they examined the relationship between health and illness in relation to risk and health-promoting factors at the organisational level, or employees’ experiences of these factors. Descriptive studies that described relationships without examine the relationship between health and illness in relation to risk and health-promoting factors at the organisational level were excluded. Outcomes that cannot be directly seen as an aspect of health or illness have also been excluded, although they may be an outcome of a risk or health-promoting factor and related to health or illness. For example, various performance-related outcomes, such as patient satisfaction, quality of care, or incidents, have been excluded since such outcomes do not directly reflect worker health. Outcomes related to employee turnover, such as the desire to leave or remain in the workplace or organisation, have also been excluded. Finally, studies conducted under non-ordinary or non-generalisable conditions, such as pandemics or crises, have been excluded. Complete inclusion and exclusion criteria can be found in Table 1.
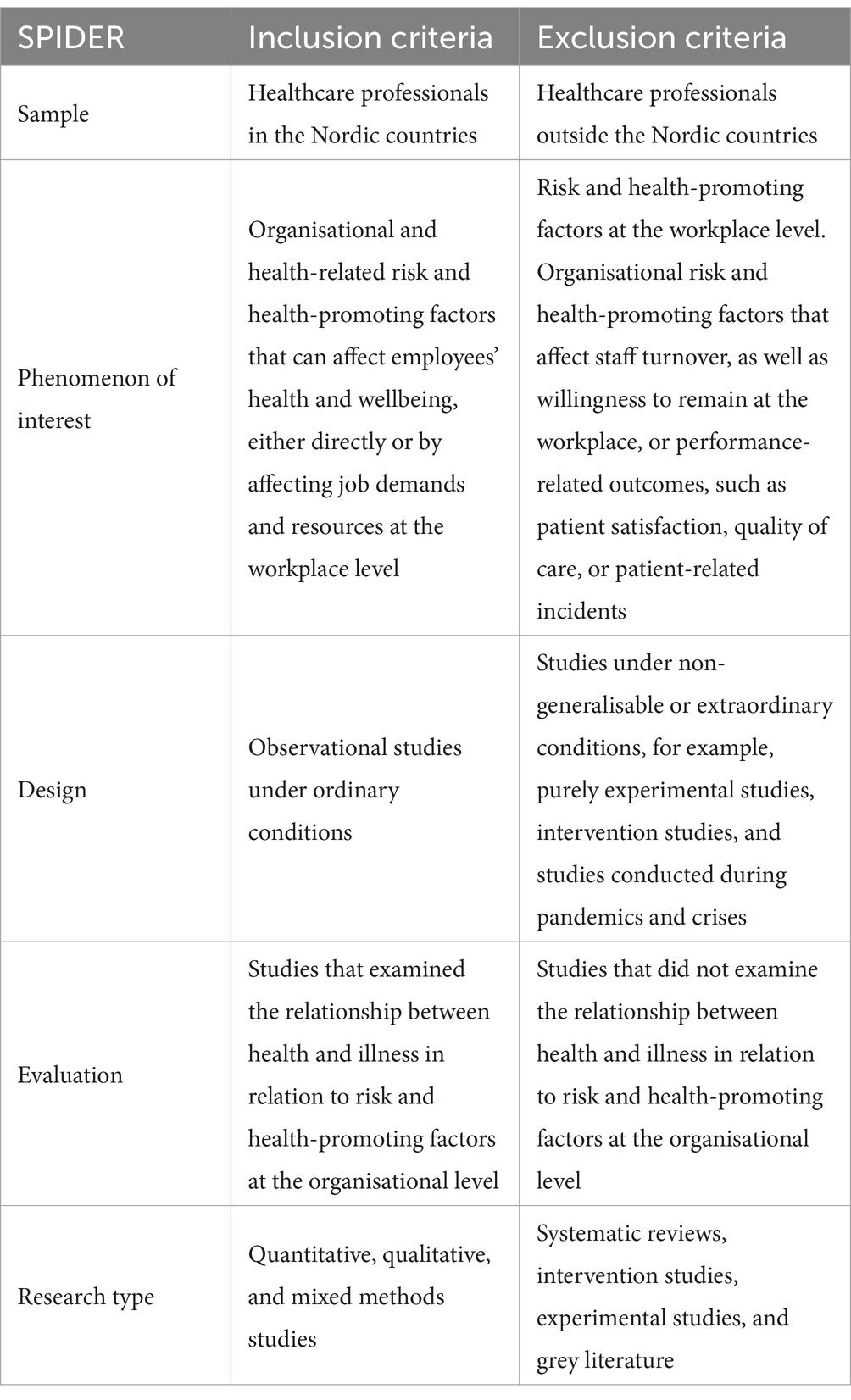
Table 1. Inclusion and exclusion criteria structured according to SPIDER (sample, phenomenon of interest, design, evaluation, and type of research).
Literature searches were developed and conducted by librarians/information specialists to reflect the concept outlined by the project team. A set of key articles were identified before the search process, which were used to generate search terms (MeSH and free-text terms) and test the effectiveness of the strategies in each database. A combination of three different thematic search terms (blocks) were used: (1) population (e.g., “healthcare worker*,” “healthcare personnel*,” “health professional*,” etc.), (2) the phenomenon of interest (e.g., “occupational health*,” “workplace health*,” “employee health*,” etc.), and (3) the context (e.g., “Sweden,” “Norway,” Denmark,” “Finland,”” Iceland.”). The complete list of search terms is presented in the on-line Supplementary material (Search terms). To cover a wide range of disciplines such as healthcare, psychology, and occupational health research, the search was performed using four different databases (Pubmed, Scopus, Cindahl, and PsycINFO) 3 January 2023.
Records found during the search phase were exported to a reference management software (EndNote) to identify and remove duplicates. To ensure adequate understanding and consistency in the application of inclusion and exclusion criteria, a calibration exercise was carried out within the project team prior to the formal screening. In this calibration exercise, the project team met to discuss inclusion and exclusion decisions on randomly selected records until adequate consensus and consistency was assessed to be reached within the group. The records were then screened based on the inclusion and exclusion criteria using Covidence, a web-based application for systematic reviews. The initial screening on the title/abstract level and the full-text assessments of each record were done independently by two of the authors (MA, JW, ALA, and/or ACFS). Cohen’s Kappa showed an agreement between 0.33 and 0.60 between the different evaluators. To increase the agreement between evaluators, the project team met up to discuss inclusion and exclusion decisions until adequate consensus and consistency was assessed to be reached. Disagreements were resolved by discussion until consensus was reached.
The methodological quality of each included study was assessed by two of the authors (MA and JW). To provide a nuanced view of study quality across multiple research designs, in line with the methodology of this systematic search and review, the 2018 Mixed Methods Appraisal Tool (MMAT) was used. MMAT is designed to review the quality of studies with different designs and varying methods (36). When using the MMAT, no scores or overall assessments, such as low/medium/high quality, are calculated; rather, the MMAT provides an in-depth picture of the quality of the studies. The quality review was conducted in two stages. In the first stage, each study was evaluated based on two screening questions (whether there were clear research questions and whether these questions could be investigated using the available data in the study). The assessment of these questions (yes, no, or cannot tell) determined whether the study should be included or excluded due to a lack of methodological quality. In the second stage, the included studies were evaluated using five additional and specific study design questions (with response alternatives: yes, no, or cannot tell), to provide an in-depth picture of the quality of the study. In this stage, the templates for qualitative studies, randomised controlled trials, non-randomised trials, and mixed methods studies were used. Any disagreement during the quality appraisal were resolved by discussion until consensus was reached.
Data extraction was performed by the authors (MA, JW, ALA, and ACFS) and cross-checked to ensure accuracy and consistency in the extracted data by another author (MA or ACFS). To include both information on the identified organisational-level risk or health-promoting factors and contextual and methodological information that may be used to support the analysis, a matrix, including: (A) country representing the context of the study, (B) study aim, (C) study design, (D) study period, (E) study population, (F) Size of the study population (G) outcomes, and (H) identified organisational-level risk or health-promoting factors was used and is provided in the on-line Supplementary material (Data extraction matrix). Any disagreements during data extraction were resolved by discussion until consensus was reached.
Since a large heterogenicity was expected in the included studies, the data synthesis was conducted with a narrative summary based on which aspects of the organisation of health care had been examined. This categorisation was done jointly by the authors (MA, JW, ALA, IA, ACFS) and was reported together with the more descriptive compilation of the included studies. Finally, overarching themes were also identified across these categories (i.e., meaningful patterns that contribute to a better understanding) (37). An example of the qualitative data synthesis process, including the identification of the categorisation and identification of overarching themes can be seen in Table 2.

Table 2. Example of the qualitative data synthesis process.
The database searches identified 4,461 records, and 2,677 record were screened on the title/abstract level after removal of duplicates. Of these, 375 full-text articles were reviewed, and 95 were included for analysis (Supplementary Table S1). A flow diagram of the review process is shown in Figure 1. A list of excluded full-text articles are provided in the on-line Supplementary material (Excluded full-text articles).
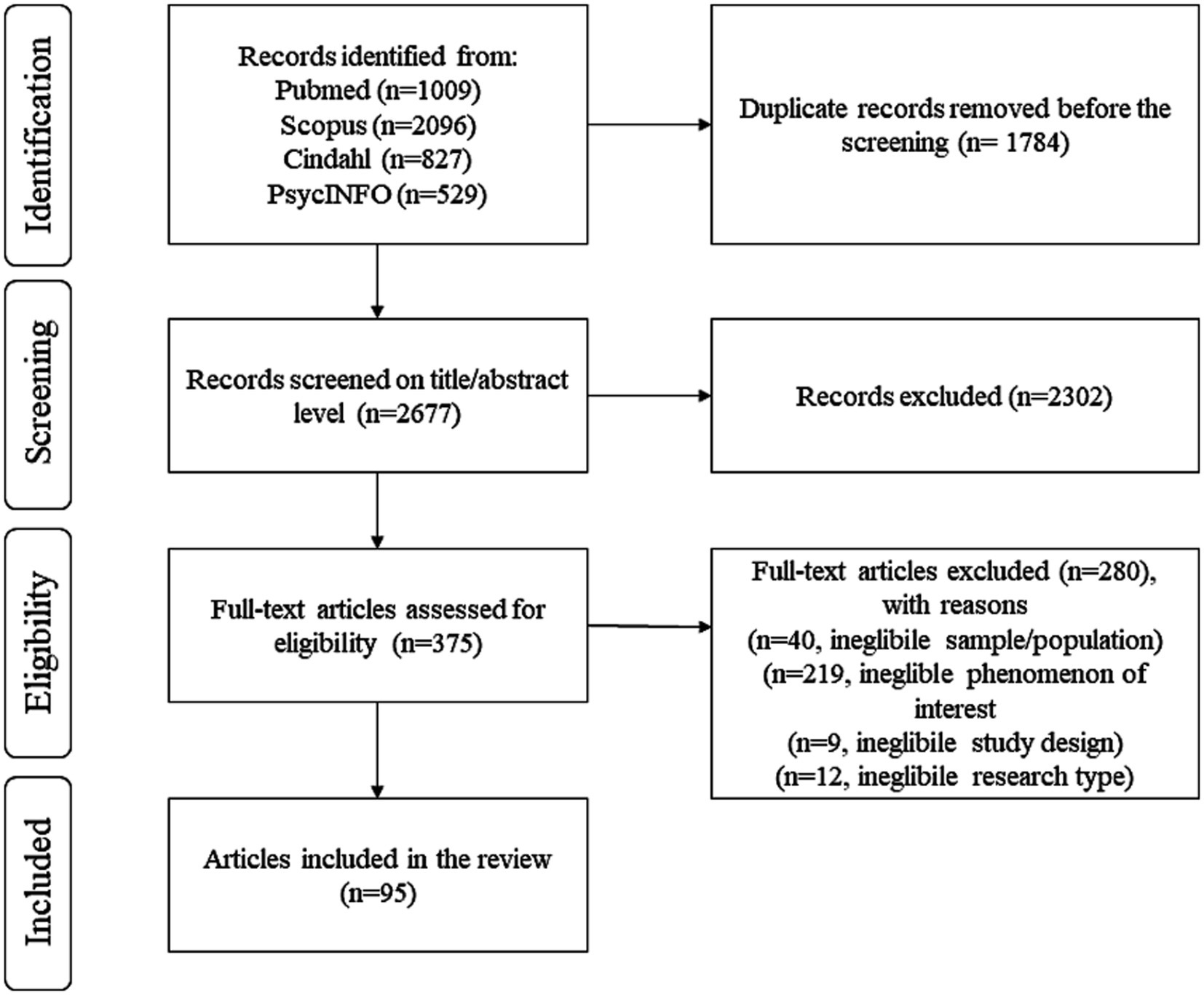
Figure 1. PRISMA 2020 flow diagram of review process.
Most of the included studies had a cross-sectional design (n = 34, 36%) or a longitudinal cohort design (n = 34, 36%). A total of 20 studies (21%) were qualitative, and two studies (2%) used a mixed methods design. The remaining five studies (5%) used a case–control design or examined the importance of organisational risk and health-promoting factors in connection with natural experiments under normal operations (quasi-experimental intervention or randomised field experiments) (Supplementary Table S1).
Two out of five studies (n = 38, 40%) included healthcare professionals from different professional groups, without examining the groups separately or specifying the groups in greater detail. The other studies (n = 57, 60%) focused on specific professional groups, including registered nurses (n = 37, 39%), physicians (n = 9, 9%), healthcare managers (n = 5, 5%), midwives (n = 4, 4%), dental hygienists and other dental professionals (n = 2, 2%), and psychotherapists (n = 1, 1%) (Supplementary Table S1).
There was an even distribution of studies from the Nordic countries, with 27 studies (28%) from Finland, 25 (26%) from Sweden, 22 (23%) from Norway and 22 (23%) from Denmark. Iceland was the exception with only one study (1%) (Supplementary Table S1). No overall differences in the identified factors could be seen between the Nordic countries.
A majority of the included studies studied organisational risk factors (n = 67, 71%) connected to a wide range of outcomes with a focus on both mental and physical illness and disease (Supplementary Table S1). The remaining studies (n = 28, 29%) focused on health-promoting factors connected to outcomes such as job satisfaction, motivation, engagement, etc. (Supplementary Table S1).
All reviewed studies were assessed to be of sufficient methodological quality and were included in the systematic review. In the in-depth assessments of the methodological quality of the included studies, most of the qualitative and mixed method studies were found to lack information on whether the authors had quality assured the article using a checklist for reporting the study (such as the “Consolidated criteria for reporting qualitative research” [COREQ] or similar resource). For the quantitative studies (17 out of 75 studies), questions were raised regarding whether the participants were representative of the intended study population due to low response rates and/or a non-random sample of the study population. The checklist for the evaluation of methodological quality is provided in the on-line Supplementary material (Quality assessment).
To obtain an overview of the results, all studies were categorised based on which aspects of the organisation of health care had been examined (Supplementary Table S1). Results identified risk and health-promoting factors in the organisation of health care in terms of the distribution of working time schedules (n = 39, 36%), design of operations and working methods (n = 28, 26%), ergonomic conditions (n = 18, 17%), terms of employment and personnel policy (n = 13, 12%), and the organisation’s ethical environment (n = 10, 9%), Table 3. These categories are described in detail below. In some cases, a single study contained risk and health-promoting factors associated with more than one of these categories, bringing the total number of studies in the above summary to more than 95.
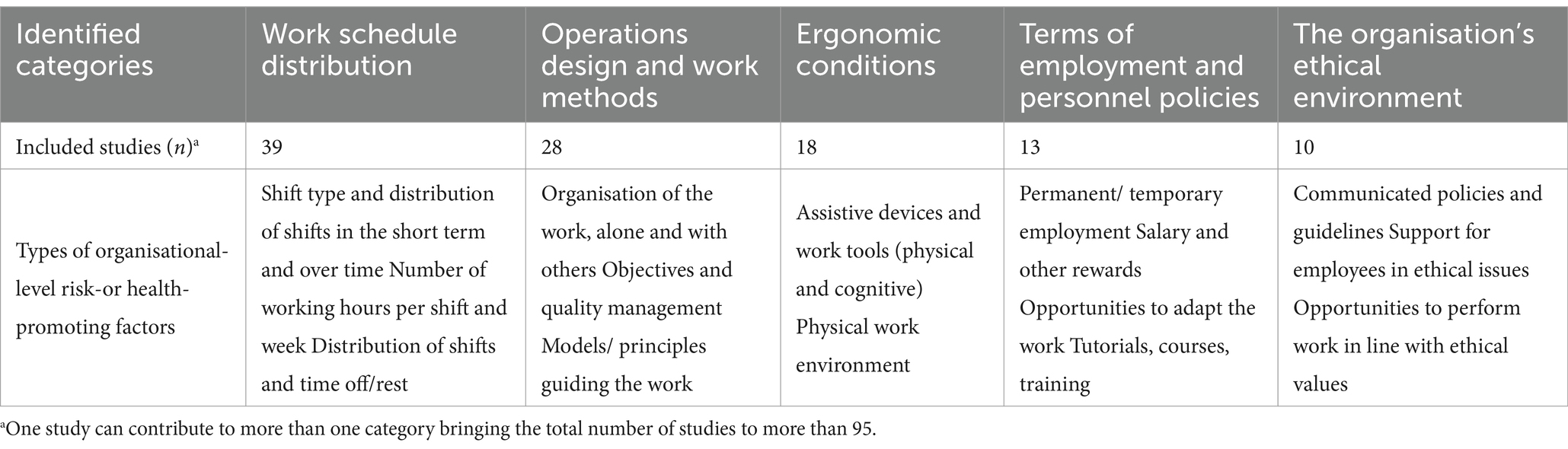
Table 3. Summary of the five identified categories of organisational-level risk-and health-promoting factors, and the types of factors associated with each of these categories.
A relatively large group of studies (n = 39) investigated employees health related to the distribution of working time schedules, that is, how shifts and working hours were distributed among existing staff. Shift work can refer to both fixed night shifts and rotating shifts. Shifts can rotate regularly or irregularly, and their duration may vary. For many healthcare organisations that must be staffed around the clock, the need for evening and night work is unavoidable. Still, the distribution of these shifts and working hours among available staff is a changeable factor at an organisational level.
Schedules that largely included night shifts and shift work, especially over several years, were found to be an organisational-level risk factor. An association was found between night work and cerebrovascular disease and stroke (38), sleep disturbances and severe fatigue (39), exhaustion (40), heart disease (41), diabetes (42), sick leave (43) and work-related accidents (44). Working several night shifts in a row increased the risk of exhaustion (45), sick leave (46, 47), and premature birth (48). Working night shifts for more than six years increased the risk of dementia (49, 50), and multiple night shifts over more than five years increased the risk of telomere shortening, which, in turn, increases the risk of breast cancer (51). However, the findings were not completely unanimous, and some studies found no association between night work and health (52, 53) or sick leave (44), or only for specific subgroups (54–56). Evening shifts were also found to be a risk factor and were associated with diabetes (42), long-term sick leave (46), and the incidence of accidents during these shifts (57, 58). Some studies found that both evening and night shifts increase the risk of both mental illness (50, 59) and mortality (60), while other studies conclude that the increased risk of mental illness was greater for people who work night shifts than evening shifts (61, 62). Shift and night work was also associated with sleep problems and insufficient recovery (63).
The distribution of working time schedules over the day and week was also found to be a risk factor. Long shifts of more than eight hours and long weeks of more than 40 h increased the risk of sick leave (46, 47, 64), work-related accidents (65), and work-related injuries (66). A schedule with fewer but longer shifts on weekends (12-h shifts instead of 8-h shifts) did not affect job satisfaction among registered nurses, but the effect of this schedule on health depended on the nurses’ general health and family situation (67). The number of 24-h on-call shifts was positively associated with burnout among surgeons (68).
Another identified risk factor was quick returns (i.e., a short duration between shifts), which was associated with perceived stress (69, 70), sleep disturbances and severe fatigue (39, 139), exhaustion (45), heart disease (41), cerebrovascular disease and stroke (38), sick leave (46, 64, 70), premature birth (48), and work-related accidents (43, 44, 58, 65).
The importance of these risk factors was also seen in studies that examined the impact of reducing shift work, quick returns, and working hours. Night workers’ symptoms of mental illness improved when they stopped working night shifts (71), and their sleep disturbances and severe fatigue decreased when they reduced the number of quick returns, discontinued night work, or reduced the number of night shifts (39). A reduction in the number of quick returns also reduced the risk of work-related injuries among registered nurses (72). When working hours were reduced from eight to six hours (with the same salary), assistant nurses and registered nurses felt that they had more energy, both on the job and outside of work (72, 137).
A health-promoting factor was identified in the ability to influence the schedules, working hours, and holidays, which was perceived as a reward (73) and increased job satisfaction (74) among registered nurses. Another study found that participation in the planning of working hours resulted in increased control, but not increased well-being, compared to traditional planning among healthcare workers (138).
The second largest category (n = 28) comprises studies focusing on how the organisation and its work are designed and what working methods prevail and are rewarded within the organisation. This includes different ways in which tasks and responsibilities have been distributed and how the organisation has chosen to structure the work, measure quality, provide feedback, offer rewards, and manage goals. Although all studies in this category address the design of operations and working methods, this is a broad field, and the identified articles mostly examine different aspects, in different contexts, for different groups, making it difficult to draw overall conclusions.
Some studies identified risk and health-promoting factors in the social aspect of how work was designed in terms of collaborations and hierarchies. Associations were identified between working alone and increased perceived anxiety (75) and musculoskeletal disorders and pain (76), but also with increased job satisfaction (77). Non-hierarchical collaboration was associated with motivation among primary care staff (78), and collaboration within the organisation and with policymakers and support (administratively and organisationally) increased well-being among healthcare managers (79). Working in self-organising teams (80) and having the ability to self-manage (81) were positively associated with job satisfaction.
Other studies identified both risk and health-promoting factors in how the tasks were designed and distributed. Physicians who were required to perform illegitimate tasks had increased presenteeism (82). The risk of exhaustion increased for physicians within primary care when they were forced to take over tasks from specialist care providers and when documentation and administration increased and became more complex (83). For general practitioners in Norway, the number of consultations per day had no association with stress, but the number of consultations containing elements of conflict did (84). Among registered nurses, the manner in which responsibility for patients was distributed was both positively and negatively associated with various aspects of stress (85). Among healthcare workers in Denmark, job satisfaction increased when clinical tasks were delegated from the physician to other health professions (86). The dissatisfaction of general practitioners with their work situation decreased when the time per patient consultation increased from less than 10 min to more than 20 min (77). When the work of midwives was organised to ensure that patients could have one midwife throughout their pregnancy, this resulted in lower rates of burnout (87) and increased job satisfaction, as the midwives felt important and appreciated (88). The more primary care units relied on a lean-based working method, the lower the levels of fatigue among staff, who also reported a greater sense of well-being (89). Operational designs that resulted in short-term planning and uncertainty about the future and finances were a risk factor for poor health among healthcare managers (79). Work that involves standing still was not associated with pain among healthcare workers (90).
Risk and health-promoting factors were also identified in the way organisations set up and managed their goals and how they chose to measure quality and performance. Clear goals and systematic quality work were associated with increased motivation among primary care staff (78), while the use of inadequate quality measures was associated with reduced job satisfaction among registered nurses (91). A focus on cost-effectiveness within an organisation sparks frustration among home care staff, who feel that they are not able to work as effectively as they would like (92). Accreditation of the enterprise was negatively associated with physicians’ job satisfaction if it was perceived as a means of control, but increased job satisfaction if it was considered to improve quality (93). Healthcare workers who were exposed to demands connected to financial constraints, administration, and productivity by their senior management had increased sickness absence compared to other healthcare workers (94). When registered nurses were rewarded based on performance goals, it sometimes resulted in increased stress (73). Registered nurses reported feeling more motivated and that collaboration improved when tasks were visually presented and could be discussed and ticked off after completion by using activity boards (95).
Finally, this category also included studies of risk and health-promoting factors linked to whether senior management had the necessary conditions to acknowledge and understand the needs of their employees. The perception that the management of a healthcare organisation focuses and acts based on the needs and desires of employees is positively linked to job satisfaction and engagement among registered nurses (96). Registered nurses reported that being seen and receiving recognition and feedback from senior management increased motivation (73, 74). A senior management team that supported patient safety and inter-unit teamwork was associated with lower levels of burnout among registered nurses (97). Registered nurses and midwives perceived that managers promoted health when they had the opportunity to take a hands-on approach, whereas a lack of instructions and procedures was perceived as a risk factor (98). Registered nurses experienced greater job satisfaction when their line manager had a moderate number of employees, thus enabling them to take on a more active leadership role (99). In another study, the number of subordinate registered nurses had no correlation with the neck and back pain of unit managers (100).
In this category, 18 studies had investigated the results of actions at the organisational level to eliminate ergonomic risk factors and optimise ergonomic conditions, including electronic information and communication systems (e.g., electronic medical record systems or registers), with the purpose of simplify or facilitating work.
Risk and health-promoting factors were seen in measures that reduced strain in individual work tasks at the organisational level and measures that provided and enabled the use of various aids to reduce the workload and the risk of injury. When working in clients’ private homes, difficulty in using adequate aids or equipment poses a risk of injury (63). The inability to use assistive devices when moving patients from one place to another was associated with ill-health among healthcare workers (63, 101, 102). Access to adapted assistive devices in the form of prism glasses reduced the risk of neck pain and injury among dental professionals by limiting neck strain (103). The design of medical equipment did not affect pain among dialysis registered nurses (104), but a closer analysis identified risks associated with repetitive tasks and the design of the workplace and various tools (76).
Other risk and health-promoting factors were found in the physical work environment. A work environment that was perceived as pleasant and allowed for social interaction increased job satisfaction among healthcare workers in long-term dementia care homes (105). Access to daylight was perceived to be important for well-being and working ability (106). The inability to see the outside world (e.g., through a window) over the course of an entire shift, as well as the long-term use of surgical equipment that requires darkness, contributed to stress and exhaustion (106). Acceptable indoor air quality was identified as an important factor for decreasing hoarseness among healthcare workers (107, 108). However, the use of blue lights in healthcare facilities had no effect on either the mood or stress levels of healthcare workers compared to normal lighting (109).
Lastly, IT systems were perceived as a health-promoting factor, if they reduced documentation requirements, improved access to information, and gave staff a sense of security (110, 111). However, they were identified as a risk factor if their use was found to be an obstacle to the ability of staff to do their work or were fraught with technical problems (112–114). The perceived stress caused by electronic tools was reduced for registered nurses if they were perceived to be user-friendly (115). This was also the case for healthcare managers, if they had access to sufficient IT support (111). Daily use of multiple IT systems was associated with a higher level of stress compared to using only one system (115, 116). Physicians who already experienced time constraints reported more IT-related stress, and physicians in primary care experienced more stress related to IT than physicians in hospitals (113).
This category includes 13 somewhat diverse studies, which in various ways examined the conditions under which their organisation employs staff and how they take care of and support these staff.
Risk and health-promoting factors were identified in job security (73, 92), salary, and other monetary rewards (73, 79, 117), which were associated with higher levels of engagement and job satisfaction. Short-term work contracts, combined with shift work with variable shift lengths, irregular rest periods, and weekend shifts, increase the risk of sick leave (118). At the same time, a study found that temporarily employed registered nurses rated their health as better than permanent registered nurses (119). In the period preceding downsizing, staff absenteeism due to illness decreased, mainly among employees with temporary contracts (120). Requirements for employees to switch units against their will negatively affected job satisfaction (74).
Risk and health-promoting factors were also identified in the organisation’s systematic work to create conditions to increase the individual’s capacity to manage their own work and development. Two studies examine access to supervision among psychotherapists with different results: group clinical supervision was associated with lower stress (121), but no association could be confirmed between participation in clinical supervision and burnout (122). Another study investigated whether the opportunity to attend courses during working hours can be a health-promoting factor but found no correlation with job satisfaction (123). Physical exercise at work reduced pain and pain sensitivity more than exercise at home (124). Registered nurses reported that inadequate adaptation of work for pregnant workers and those with health problems was a reason for sickness absence (125).
The category of studies that addressed the ethical environment of organisations includes relatively few studies (n = 10). However, they are generally homogeneous and examine the ability of employees to perform their work in accordance with their own fundamental values of what constitutes good care, as well as the values of their profession. The ethical environment also encompasses the extent to which the organisation encourages ethical discussions in the workplace and ensures that employees are supported in ethical issues and dilemmas.
Risk and health-promoting factors were identified in the ability of employees to act in accordance with their values and receive support in dealing with ethical issues, as this was seen as important for job satisfaction and engagement. When an organisation shares the values of its staff and ensures that there are resources and conditions for employees to be able to deal with ethical issues and act in accordance with their values, it is a health-promoting factor (126). Motivation and engagement increase when employees feel that they have adequate time (95) and sufficient staff (92, 98). Furthermore, when the number of employees in a unit increases or functions are outsourced, the risk of long-term sick leave decreases (127). Conversely, healthcare workers in home care services who are forced to “count the minutes” feel frustrated and unable to work as effectively (92), and inadequate staffing poses a health risk that entails extra stress, pressure, and responsibility (63).
For managers, the inability to implement decisions that were made higher up in the organisation or the obligation to implement decisions with which they personally disagree constitute a risk factor for future illness (128). Another risk factor for reduced job satisfaction arises when an individual’s values conflict with the values of the organisation. This demonstrates the importance of management understanding the ethical challenges related to the profession (91). Conversely, a health-promoting factor for job satisfaction was identified in the organisation’s encouragement of ethical discussions and support in grappling with ethical issues (129).
Although there was a wide variety within and between the categories in terms of the risk and health-promoting factors on which the studies focused, there were also similarities. Within each category, the studies demonstrated that what the organisation does to control and manage the work to meet its goals has an impact on employee health. This applies, for example, to how the organisation allocates working hours and staffs its operations, manages its objectives, and provides aids and support. In addition, there were studies in all categories that pointed to the importance of the organisation’s culture and values and what it communicates to its employees, including through priorities that affect both the work environment and the opportunities for employees to work effectively.
This review presents knowledge from recent Nordic research on organisational risk and health-promoting factors in the healthcare sector. It takes a relatively new approach to risk and health-promoting factors, insofar as it focuses on the organisational level, that is, the structure, choice of principles, and values of the organisations. When work-related illness and well-being are discussed, workplace and individual factors are usually the dominant theme (18, 130, 131).
Our findings indicate that organisational-level risk and health-promoting factors can be divided into five categories: distribution of working time schedules; design of operations and working methods; ergonomic conditions; terms of employment and personnel policy; and the organisation’s ethical environment. In terms of their effect on the health of healthcare workers, these categories are well known. It is common knowledge that the scheduling of shifts (duration, number, and frequency, as well as time for recovery between shifts) can be both a risk factor for physical and mental illness, for example, exhaustion and cancer (22, 23, 132–134), and a health-promoting factor that increases job satisfaction (133). Furthermore, Aust et al. (16) recently showed the importance of job and task modification, flexible work and scheduling, and changes in the physical work environment in improving healthcare workers mental health and wellbeing. The HR practices of organisations have been associated with nurse absenteeism (135), and ethical value conflicts in healthcare have been associated with the health of nurses (2, 136). However, what this systematic review adds is a deeper understanding of how these risk and health-promoting factors can be created at the organisational level – and hence a better understanding of how to address risks at their roots and create a hotbed for a healthy and attractive work environment through the active engagement of the top management. It also identifies similarities between categories, highlighting the importance of including multiple perspectives within the employer’s occupational safety and health management, since both the actions that employers take to fulfil the healthcare organisation’s goals and the ability of employees to provide good quality care were found to be important for the health and wellbeing of healthcare employees. Consequently, employee health and wellbeing can and should be managed at the organisational level, not only at the workplace or individual level by first-line managers, according to the principles of the hierarchy of controls for occupational safety and health (30, 31) and recommendations from peers (16, 18).
This review also shows that there is a lack of knowledge on measures to promote well-being and health compared to knowledge of measures to counteract illness and disease. This is highlighted by the fact that most of the studies investigated risk factors rather than health-promoting factors. The definition of health-promoting factors differed substantially between the included studies, and in some studies, measures that sought to address risk factors rather than add something positive were also defined as health-promoting factors (e.g., reducing quick returns or alleviating strain/workload through well-adapted aids). Such factors may reduce the risk of illness but likely do not promote health or well-being, since they simply mean that a risk factor has been addressed. The utilisation of health-promoting factors within the occupational health and safety management of organisations may be particularly important if the healthcare sector (19) is to remain attractive to professions that are both demanding for the individual and essential for a well-functioning society.
Some limitations need to be considered when interpreting the results of this review. The current study is limited to healthcare professions in the Nordic, countries and the findings cannot automatically be generalised to other professions or countries. Given the complex characteristics of healthcare organisations (20), future research would benefit from performing similar reviews for other contexts, rather than broadening the search criteria to include other professions and countries. Future research could also build on these findings to enable systematic reviews that include meta-analyses for individual categories of organisational-level risk-and health-promoting factors. The present review only considered studies published on or before 3 January 2023. We did not update the search further because we did not want to include studies that reflected the extraordinary circumstances following the COVID-19 pandemic, which currently influences research in this area. As a result, many studies published from 2021 an onwards were excluded during the study selection of this review.
A very broad approach was used to provide an overview of Nordic research on the work environment and health of healthcare professionals, with a focus on identifying organisational-level risk and health-promoting factors. This resulted in a wide range of study types across different healthcare professionals and settings, targeting a variety of outcomes. Although this heterogenicity did not allow for firm conclusions, it showed the large variety of studies within the area. Dividing these studies in five categories of organisational-level risk and health-promoting factors provided a better understanding of areas of interest when investigating potential risk factors within an organisation. However, due to this heterogenicity, it was not possible to perform a meta-analysis of the findings within each category.
It should also be pointed out that a large proportion of the included studies used a longitudinal cohort design. This means that they followed participants over time and investigated how factors related to health, illness, and the organisation of work changed in relation to each other. This is useful when pinpointing the risk and health-promoting factors in the work environment. A relatively large number of qualitative studies were identified. This helps to provide a deeper understanding of employees’ perceptions of risk and health-promoting factors. Two out of five studies included more than one occupational profession. This increases the generalisability of the results but at the expense of being able to comment on individual occupational groups. Many of the studies that reported results for individual occupational groups focused on registered nurses.
This review offers valuable information on how leaders within healthcare organisations can promote employee wellbeing through strategies that target the way work is organised, designed, and managed. Our results call for action on the strategic level within the occupational health and safety management in healthcare organisations, since it is at the organisational level that opportunities arise to not only manage but eliminate risks in the work environment, and it is also here that there is an opportunity to promote health in the workplace (16, 18).
In addition, our analysis of overall themes can also give an indication of which perspectives on the organisation of work in health care are important for both employer and employees, regardless of which specific areas are considered. To ensure a sustainable, safe, and healthy working life, the effect of actions that employers take to meet the health care organisation’s goals and provide employees with the ability to provide high-quality care must be given equal priority. Management must ensure that its staffing, distribution of working time schedules, and choice of working methods are adequate to meet society’s needs for healthcare and that their operations are designed in a way that ensures the organisation can fulfil its mission. Yet it is equally important that management prevents employees from being exposed to the risk of illness and provides them with the opportunity to conduct their work in accordance with their fundamental values regarding what constitutes good care. The organisation must ensure that working methods, aids, and the physical work environment enable employees to perform their work in a manner that is satisfactory to both patients and employees. The terms of employment and work must be adapted to the organisation’s need for flexibility and simultaneously provide sufficient security to meet the employees’ needs for security and rewards. The organisation’s ethical environment must consider not only care priorities, but also how these affect employees.
Overall, the main contribution of this review is threefold. Firstly, our results indicate that organisational-level risk and health-promoting factors can be found within an organisations’ work schedule distribution, operations design and work methods, ergonomic conditions, terms of employment and personnel policies, and within the organisation’s ethical environment. Secondly, by addressing organisational-level factors within healthcare organisations, risks in the work environment may be eliminated rather than simply managed at the workplace level. Thus, our findings emphasise that the underlying causes of adverse working conditions within the healthcare sector must be identified and managed at the organisational and structural level. Lastly, two themes emerged across the categories, providing further insight into implications for practice. The first theme concerns how risk and health-promoting factors are present in the actions that are taken to fulfil the organisation’s goals, and the second theme concerns how these factors affect the ability of employees to perform their jobs at a level of quality that they consider reasonable. Thus, a successful approach to occupational health and safety management needs to consider both aspects when taking measures to improve working conditions, as well as the organisation of work within the healthcare sector. Integrating organisational-level factors in the occupational health and safety management could potentially result in a retention of skilled professionals within healthcare organisations’ both in the Nordic countries and globally.
MA: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Validation, Visualization, Writing – original draft, Writing – review & editing. JW: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Validation, Visualization, Writing – original draft, Writing – review & editing. AL: Conceptualization, Formal analysis, Investigation, Validation, Writing – original draft, Writing – review & editing. IA: Conceptualization, Software, Validation, Writing – original draft, Writing – review & editing. A-CF: Conceptualization, Formal analysis, Investigation, Methodology, Validation, Visualization, Writing – original draft, Writing – review & editing.
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This research was funded by the Swedish Agency for Work Environment Expertise (Dnr 21/00176: MA). The funding body had no role in designing the study; the collection, analysis, and interpretation of data; or in writing the manuscript.
We would like to thank Marlene Franzén and Maria von Essen, librarians/information specialists at Mid Sweden University for support in developing and conducting the literature search strategy.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors declare that no Gen AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2024.1509023/full#supplementary-material
1. Jun, J, Ojemeni, MM, Kalamani, R, Tong, J, and Crecelius, ML. Relationship between nurse burnout, patient and organizational outcomes: systematic review. Int J Nurs Stud. (2021) 119:103933. doi: 10.1016/j.ijnurstu.2021.103933
2. Larsman, P, Pousette, A, Skyvell Nilsson, M, Gadolin, C, and Törner, M. Ethical value conflicts in healthcare and their effects on nurses’ health, turnover intent, team effectiveness, and patient safety: a longitudinal questionnaire study. Scand J Work Environ Health. (2024) 50:113–21. doi: 10.5271/sjweh.4138
3. Salyers, MP, Bonfils, KA, Luther, L, Firmin, RL, White, DA, Adams, EL, et al. The relationship between professional burnout and quality and safety in healthcare: a Meta-analysis. J Gen Intern Med. (2017) 32:475–82. doi: 10.1007/s11606-016-3886-9
4. Wallace, JE. Burnout, coping and suicidal ideation: an application and extension of the job demand-control-support model. J Work Behav Health. (2017) 32:99–118. doi: 10.1080/15555240.2017.1329628
5. Wei, H, Sewell, KA, Woody, G, and Rose, MA. The state of the science of nurse work environments in the United States: a systematic review. Int J Nurs Sci. (2018) 5:287–300. doi: 10.1016/j.ijnss.2018.04.010
6. West, CP, Dyrbye, LN, and Shanafelt, TD. Physician burnout: contributors, consequences and solutions. J Intern Med. (2018) 283:516–29. doi: 10.1111/joim.12752
7. EU-OHSA. (2023). Psychosocial risk management in the health and social sector. Discussion paper. Available online at: https://osha.europa.eu/en/publications/psychosocial-risks-health-and-social-care-sector_risk_management_social_care_en_.pdf (Accessed September 6, 2024)
9. Johnson, J, Hall, LH, Berzins, K, Baker, J, Melling, K, and Thompson, C. Mental healthcare staff well-being and burnout: a narrative review of trends, causes, implications, and recommendations for future interventions. Int J Ment Health Nurs. (2018) 27:20–32. doi: 10.1111/inm.12416
10. Rodrigues, H, Cobucci, R, Oliveira, A, Cabral, JV, Medeiros, L, Gurgel, K, et al. Burnout syndrome among medical residents: a systematic review and meta-analysis. PloS One. (2018) 13:e0206840. doi: 10.1371/journal.pone.0206840
11. Pekkarinen, L, Elovainio, M, Sinervo, T, Heponiemi, T, Aalto, AM, Noro, A, et al. Job demands and musculoskeletal symptoms among female geriatric nurses: the moderating role of psychosocial resources. J Occup Health Psychol. (2013) 18:211–9. doi: 10.1037/a0031801
12. Adriaenssens, J, De Gucht, V, and Maes, S. Determinants and prevalence of burnout in emergency nurses: a systematic review of 25 years of research. Int J Nurs Stud. (2015) 52:649–61. doi: 10.1016/j.ijnurstu.2014.11.004
13. Harvey, SB, Epstein, RM, Glozier, N, Petrie, K, Strudwick, J, Gayed, A, et al. Mental illness and suicide among physicians. Lancet. (2021) 398:920–30. doi: 10.1016/S0140-6736(21)01596-8
14. Bakker, AB, and Demerouti, E. Job demands-resources theory: taking stock and looking forward. J Occup Health Psychol. (2017) 22:273–85. doi: 10.1037/ocp0000056
15. WHO. (2024) Health workforce. Avalible at: https://www.who.int/health-topics/health-workforce#tab=tab_1 (Accessed September 6, 2024)
16. Aust, B, Leduc, C, Cresswell-Smith, J, O'Brien, C, Rugulies, R, Leduc, M, et al. The effects of different types of organisational workplace mental health interventions on mental health and wellbeing in healthcare workers: a systematic review. Int Arch Occup Environ Health. (2024) 97:485–522. doi: 10.1007/s00420-024-02065-z
17. LaMontagne, AD, Shann, C, and Martin, A. Developing an integrated approach to workplace mental health: a hypothetical conversation with a small business owner. Ann Work Exposures Health. (2018) 62:S93–s100. doi: 10.1093/annweh/wxy039
18. Rugulies, R, Aust, B, Greiner, B, Arensman, E, Kawakami, N, LaMontagne, A, et al. Work-related causes of mental health conditions and interventions for their improvement in workplaces. Lancet. (2023) 402:1368–81. doi: 10.1016/S0140-6736(23)00869-3
19. Teoh, K, Dhensa-Kahlon, R, Christensen, M, Frost, F, Hatton, E, and Nielsen, K. Organizational wellbeing interventions: Case studies from the NHS. London: University of London (2023).
20. Giusino, D, De Angelis, M, Mazzetti, G, Faiulo, IR, Innstrand, ST, Christensen, M, et al. Mentally healthy healthcare: main findings and lessons learned from a needs assessment exercise at multiple workplace levels In: CA Bowers, DC Beidel, MR Marks, K Horan, and J Cannon-Bowers, editors. Mental health and wellness in healthcare workers: Identifying risks, prevention, and treatment IGI global. Hershey, PA: Information Resources Management Association (2022). 143–71.
21. von Thiele, SU, Nielsen, K, Edwards, K, Hasson, H, Ipsen, C, Savage, C, et al. How to design, implement and evaluate organizational interventions for maximum impact: the Sigtuna principles. Eur J Work Organ Psychol. (2021) 30:415–27. doi: 10.1080/1359432X.2020.1803960
22. Alabi, RO, Hietanen, P, Elmusrati, M, Youssef, O, Almangush, A, and Mäkitie, AA. Mitigating burnout in an oncological unit: a scoping review. Front Public Health. (2021) 9:9. doi: 10.3389/fpubh.2021.677915
23. Dall'Ora, C, Ball, J, Reinius, M, and Griffiths, P. Burnout in nursing: a theoretical review. Hum Resour. Health. (2020) 18:469. doi: 10.1186/s12960-020-00469-9
24. McCormack, HM, Mac Intyre, TE, O'Shea, D, Herring, MP, and Campbell, MJ. The prevalence and cause (s) of burnout among applied psychologists: a systematic review. Front Psychol. (2018) 9:1897. doi: 10.3389/fpsyg.2018.01897
25. O'Connor, K, Muller Neff, D, and Pitman, S. Burnout in mental health professionals: a systematic review and meta-analysis of prevalence and determinants. Eur Psychiatry. (2018) 53:74–99. doi: 10.1016/j.eurpsy.2018.06.003
26. Jacquier-Bret, J, and Gorce, P. Prevalence of body area work-related musculoskeletal disorders among healthcare professionals: a systematic review. Int J Environ Res Public Health. (2023) 20:841. doi: 10.3390/ijerph20010841
27. Lietz, J, Kozak, A, and Nienhaus, A. Prevalence and occupational risk factors of musculoskeletal diseases and pain among dental professionals in Western countries: a systematic literature review and meta-analysis. PloS One. (2018) 13:e0208628. doi: 10.1371/journal.pone.0208628
28. Le Floch, B, Bastiaens, H, Le Reste, JY, Lingner, H, Hoffman, RD, Czachowski, S, et al. Which positive factors determine the GP satisfaction in clinical practice? A systematic literature review. BMC Fam Pract. (2016) 17:133. doi: 10.1186/s12875-016-0524-x
29. Zangaro, GA, and Soeken, KL. A meta-analysis of studies of nurses' job satisfaction. Res Nurs Health. (2007) 30:445–58. doi: 10.1002/nur.20202
30. Ajslev, JZN, Møller, JL, Andersen, MF, Pirzadeh, P, and Lingard, H. The hierarchy of controls as an approach to visualize the impact of occupational safety and health coordination. Int J Environ Res Public Health. (2022) 19:2731. doi: 10.3390/ijerph19052731
31. Montano, D, Hoven, H, and Siegrist, J. Effects of organisational-level interventions at work on employees' health: a systematic review. BMC Public Health. (2014) 14:135. doi: 10.1186/1471-2458-14-135
32. Laugesen, K, Ludvigsson, JF, Schmidt, M, Gissler, M, Valdimarsdottir, UA, Lunde, A, et al. Nordic health registry-based research: a review of health care systems and key registries. Clin Epidemiol. (2021) 13:533–54. doi: 10.2147/CLEP.S314959
33. Grant, MJ, and Booth, A. A typology of reviews: an analysis of 14 review types and associated methodologies. Health Inf Libr J. (2009) 26:91–108. doi: 10.1111/j.1471-1842.2009.00848.x
34. Page, MJ, McKenzie, JE, Bossuyt, PM, Boutron, I, Hoffmann, TC, Mulrow, CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. (2021) 372:n71. doi: 10.1136/bmj.n71
35. Cooke, A, Smith, D, and Booth, A. Beyond PICO: the SPIDER tool for qualitative evidence synthesis. Qual Health Res. (2012) 22:1435–43. doi: 10.1177/1049732312452938
36. Hong, QN, Gonzalez-Reyes, A, and Pluye, P. Improving the usefulness of a tool for appraising the quality of qualitative, quantitative and mixed methods studies, the mixed methods appraisal tool (MMAT). J Eval Clin Pract. (2018) 24:459–67. doi: 10.1111/jep.12884
37. Braun, V, and Clarke, V. Using thematic analysis in psychology. Qual Res Psychol. (2006) 3:77–101. doi: 10.1191/1478088706qp063oa
38. Bigert, C, Kader, M, Andersson, T, Selander, J, Bodin, T, Gustavsson, P, et al. Night and shift work and incidence of cerebrovascular disease – a prospective cohort study of healthcare employees in Stockholm. Scand J Work Environ Health. (2022) 48:31–40. doi: 10.5271/sjweh.3986
39. Waage, S, Pallesen, S, Moen, BE, Vedaa, Ø, Thun, E, Vikanes Buchvold, H, et al. Changes in work schedule affect the prevalence of shift work disorder among Norwegian nurses—a two year follow-up study. Chronobiol Int. (2021) 38:924–32. doi: 10.1080/07420528.2021.1896535
40. Härmä, M, Karhula, K, Puttonen, S, Ropponen, A, Koskinen, A, Ojajärvi, A, et al. Shift work with and without night work as a risk factor for fatigue and changes in sleep length: a cohort study with linkage to records on daily working hours. J Sleep Res. (2019) 28:e12658. doi: 10.1111/jsr.12658
41. Kader, M, Selander, J, Andersson, T, Albin, M, Bodin, T, Härmä, M, et al. Night and shift work characteristics and incident ischemic heart disease and atrial fibrillation among healthcare employees – a prospective cohort study. Scand J Work Environ Health. (2022) 48:520–9. doi: 10.5271/sjweh.4045
42. Hansen, AB, Stayner, L, Hansen, J, and Andersen, ZJ. Night shift work and incidence of diabetes in the Danish nurse cohort. Occup Environ Med. (2016) 73:262–8. doi: 10.1136/oemed-2015-103342
43. Bernstrøm, VH, and Houkes, I. Shift work and sickness absence at a Norwegian hospital: a longitudinal multilevel study. Occup Environ Med. (2020) 77:555–63. doi: 10.1136/oemed-2019-106240
44. Vedaa, Ø, Harris, A, Erevik, EK, Waage, S, Bjorvatn, B, Sivertsen, B, et al. Short rest between shifts (quick returns) and night work is associated with work-related accidents. Int Arch Occup Environ Health. (2019) 92:829–35. doi: 10.1007/s00420-019-01421-8
45. Härmä, M, Karhula, K, Ropponen, A, Puttonen, S, Koskinen, A, Ojajärvi, A, et al. Association of changes in work shifts and shift intensity with change in fatigue and disturbed sleep: a within-subject study. Scand J Work Environ Health. (2018) 44:394–402. doi: 10.5271/sjweh.3730
46. Larsen, AD, Ropponen, A, Hansen, J, Hansen, ÅM, Kolstad, HA, Koskinen, A, et al. Working time characteristics and long-term sickness absence among Danish and Finnish nurses: a register-based study. Int J Nurs Stud. (2020) 112:103639. doi: 10.1016/j.ijnurstu.2020.103639
47. Ropponen, A, Koskinen, A, Puttonen, S, and Härmä, M. Exposure to working-hour characteristics and short sickness absence in hospital workers: a case-crossover study using objective data. Int J Nurs Stud. (2019) 91:14–21. doi: 10.1016/j.ijnurstu.2018.11.002
48. Kader, M, Bigert, C, Andersson, T, Selander, J, Bodin, T, Skröder, H, et al. Shift and night work during pregnancy and preterm birth – a cohort study of Swedish health care employees. Int J Epidemiol. (2021) 50:1864–74. doi: 10.1093/ije/dyab135
49. Jørgensen, JT, Hansen, J, Westendorp, RGJ, Nabe-Nielsen, K, Stayner, LT, Simonsen, MK, et al. Shift work and incidence of dementia: a Danish nurse cohort study. Alzheimers Dement. (2020) 16:1268–79. doi: 10.1002/alz.12126
50. Jørgensen, JT, Schernhammer, E, Papantoniou, K, Hansen, J, Westendorp, RGJ, Stayner, L, et al. Night work and incidence of Parkinson's disease in the Danish nurse cohort. Occup Environ Med. (2021) 78:419–25. doi: 10.1136/oemed-2020-107067
51. Erdem, JS, Notø, HØ, Skare, Ø, Lie, JAS, Petersen-øverleir, M, Reszka, E, et al. Mechanisms of breast cancer risk in shift workers: association of telomere shortening with the duration and intensity of night work. Cancer Med. (2017) 6:1988–97. doi: 10.1002/cam4.1135
52. Hammer, P, Hageman, I, Garde, A, Begtrup, L, Flachs, E, Hansen, J, et al. Night work and postpartum depression: a national register-based cohort study. Scand J Work Environ Health. (2019) 45:577–87. doi: 10.5271/sjweh.3831
53. Persson, SS, Lindström, PN, Pettersson, P, and Andersson, I. Workplace relationships impact self-rated health: a survey of Swedish municipal health care employees. Work J Prevent Assess Rehabil. (2018) 60:85–94. doi: 10.3233/WOR-182721
54. Cheng, W-J, Puttonen, S, Vanttola, P, Koskinen, A, Kivimäki, M, and Härmä, M. Association of shift work with mood disorders and sleep problems according to chronotype: a 17-year cohort study. Chronobiol Int. (2021) 38:518–25. doi: 10.1080/07420528.2021.1885431
55. Henriksen, L, and Lukasse, M. Burnout among Norwegian midwives and the contribution of personal and work-related factors: a cross-sectional study. Sex Reprod Healthc. (2016) 9:42–7. doi: 10.1016/j.srhc.2016.08.001
56. Ropponen, A, Koskinen, A, Puttonen, S, and Härmä, M. A case-crossover study of age group differences in objective working-hour characteristics and short sickness absence. J Nurs Manag. (2020) 28:787–96. doi: 10.1111/jonm.12992
57. Nielsen, HB, Dyreborg, J, Hansen, ÅM, Hansen, J, Kolstad, HA, Larsen, AD, et al. Shift work and risk of occupational, transport and leisure-time injury. A register-based case-crossover study of Danish hospital workers. Saf Sci. (2019) 120:728–34. doi: 10.1016/j.ssci.2019.07.006
58. Nielsen, HB, Hansen, ÅM, Conway, SH, Dyreborg, J, Hansen, J, Kolstad, HA, et al. Short time between shifts and risk of injury among danish hospital workers: a register-based cohort study. Scand J Work Environ Health. (2019) 45:166–73. doi: 10.5271/sjweh.3770
59. Jørgensen, JT, Rozing, MP, Westendorp, RGJ, Hansen, J, Stayner, LT, Simonsen, MK, et al. Shift work and incidence of psychiatric disorders: the Danish nurse cohort study. J Psychiatr Res. (2021) 139:132–8. doi: 10.1016/j.jpsychires.2021.05.045
60. Jørgensen, JT, Karlsen, S, Stayner, L, Hansen, J, and Andersen, ZJ. Shift work and overall and cause-specific mortality in the Danish nurse cohort. Scand J Work Environ Health. (2017) 43:117–26. doi: 10.5271/sjweh.3612
61. Jensen, HI, Larsen, JW, and Thomsen, TD. The impact of shift work on intensive care nurses’ lives outside work: a cross-sectional study. J Clin Nurs. (2018) 27:e703–9. doi: 10.1111/jocn.14197
62. Karhula, K, Hakola, T, Koskinen, A, Ojajärvi, A, Kivimäki, M, and Härmä, M. Permanent night workers´ sleep and psychosocial factors in hospital work. A comparison to day and shift work. Chronobiol Int. (2018) 35:785–94. doi: 10.1080/07420528.2018.1466792
63. Grasmo, SG, Liaset, IF, and Redzovic, SE. Home care workers’ experiences of work conditions related to their occupational health: a qualitative study. BMC Health Serv Res. (2021) 21:962. doi: 10.1186/s12913-021-06941-z
64. Ropponen, A, Koskinen, A, Puttonen, S, Ervasti, J, Kivimäki, M, Oksanen, T, et al. Association of working hour characteristics and on-call work with risk of short sickness absence among hospital physicians: a longitudinal cohort study. Chronobiol Int. (2022) 39:233–40. doi: 10.1080/07420528.2021.1993238
65. Ropponen, A, Gluschkoff, K, Ervasti, J, Kivimäki, M, Koskinen, A, Krutova, O, et al. Working hour patterns and risk of occupational accidents. An optimal matching analysis in a hospital employee cohort. Saf Sci. (2023) 159:106004. doi: 10.1016/j.ssci.2022.106004
66. Härmä, M, Koskinen, A, Sallinen, M, Kubo, T, Ropponen, A, and Lombardi, DA. Characteristics of working hours and the risk of occupational injuries among hospital employees: a case-crossover study. Scand J Work Environ Health. (2020) 46:570–8. doi: 10.5271/sjweh.3905
67. Ose, SO, Tjønnås, MS, Kaspersen, SL, and Færevik, H. One-year trial of 12-hour shifts in a non-intensive care unit and an intensive care unit in a public hospital: a qualitative study of 24 nurses' experiences. BMJ Open. (2019) 9:e024292. doi: 10.1136/bmjopen-2018-024292
68. Møller, CM, Clausen, T, Aust, B, and Eiberg, JP. A cross-sectional national study of burnout and psychosocial work environment in vascular surgery in Denmark. J Vasc Surg. (2022) 75:1750–9.e3. doi: 10.1016/j.jvs.2021.11.042
69. Dahlgren, A, Tucker, P, Bujacz, A, Frögéli, E, Rudman, A, and Gustavsson, P. Intensive longitudinal study of newly graduated nurses’ quick returns and self-rated stress. Scand J Work Environ Health. (2021) 47:404–7. doi: 10.5271/sjweh.3962
70. Vedaa, Ø, Pallesen, S, Waage, S, Bjorvatn, B, Sivertsen, B, Erevik, E, et al. Short rest between shift intervals increases the risk of sick leave: a prospective registry study. Occup Environ Med. (2017) 74:496–501. doi: 10.1136/oemed-2016-103920
71. Beltagy, MS, Pentti, J, Vahtera, J, and Kivimäki, M. Night work and risk of common mental disorders: analyzing observational data as a non-randomized pseudo trial. Scand J Work Environ Health. (2018) 44:512–20. doi: 10.5271/sjweh.3733
72. Vedaa, Ø, Harris, A, Waage, S, Bjorvatn, B, Thun, E, Buchvold, HV, et al. A longitudinal study on the association between quick returns and occupational accidents. Scand J Work Environ Health. (2020) 46:645–9. doi: 10.5271/sjweh.3906
73. Seitovirta, J, Vehviläinen-Julkunen, K, Mitronen, L, De Gieter, S, and Kvist, T. Attention to nurses’ rewarding—an interview study of registered nurses working in primary and private healthcare in Finland. J Clin Nurs. (2017) 26:1042–52. doi: 10.1111/jocn.13459
74. Loft, MI, and Jensen, CS. What makes experienced nurses stay in their position? A qualitative interview study. J Nurs Manag. (2020) 28:1305–16. doi: 10.1111/jonm.13082
75. Ruotsalainen, S, Jantunen, S, and Sinervo, T. Which factors are related to Finnish home care workers' job satisfaction, stress, psychological distress and perceived quality of care?- a mixed method study. BMC Health Serv Res. (2020) 20:896. doi: 10.1186/s12913-020-05733-1
76. Westergren, E, and Lindberg, M. Work-related musculoskeletal complaints among haemodialysis nurses: an exploratory study of the work situation from an ergonomic perspective. Work. (2022) 72:875–84. doi: 10.3233/WOR-205241
77. Cohidon, C, Wild, P, and Senn, N. Practice organization characteristics related to job satisfaction among general practitioners in 11 countries. Ann Fam Med. (2019) 17:510–7. doi: 10.1370/afm.2449
78. Kjellström, S, Avby, G, Areskoug-Josefsson, K, Andersson Gäre, B, and Andersson, BM. Work motivation among healthcare professionals: a study of well-functioning primary healthcare centers in Sweden. J Health Organ Manage. (2017) 31:487–502. doi: 10.1108/JHOM-04-2017-0074
79. Herttuala, N, Kokkinen, L, and Konu, A. Social-and healthcare managers' work wellbeing—literature review and key informant interviews. Int J Workplace Health Manag. (2020) 13:633–48. doi: 10.1108/IJWHM-05-2019-0077
80. Ruotsalainen, S, Elovainio, M, Jantunen, S, and Sinervo, T. The mediating effect of psychosocial factors in the relationship between self-organizing teams and employee wellbeing: a cross-sectional observational study. Int J Nurs Stud. (2023) 138:104415. doi: 10.1016/j.ijnurstu.2022.104415
81. Gamskjaer, T, Werlauff, U, and Handberg, C. Investigating job satisfaction in palliative rehabilitation: reflections and perspectives of health professionals working with amyotrophic lateral sclerosis. J Eval Clin Pract. (2022) 28:108–19. doi: 10.1111/jep.13599
82. Thun, S, Halsteinli, V, and Løvseth, L. A study of unreasonable illegitimate tasks, administrative tasks, and sickness presenteeism amongst Norwegian physicians: an everyday struggle? BMC Health Serv Res. (2018) 18:407. doi: 10.1186/s12913-018-3229-0
83. Svedahl, ER, Pape, K, Toch-Marquardt, M, Skarshaug, LJ, Kaspersen, S-L, Bjørngaard, JH, et al. Increasing workload in Norwegian general practice – a qualitative study. BMC Fam Pract. (2019) 20:1–10. doi: 10.1186/s12875-019-0952-5
84. Johnsen, TM, Norberg, BL, Krogh, FH, Vonen, HD, Getz, O, and Austad, B. The impact of clinical experience on working tasks and job-related stress: a survey among 1032 Norwegian GPs. BMC Primary Care. (2022) 23:1–10. doi: 10.1186/s12875-022-01810-y
85. Rantanen, A, Pitkänen, A, Paimensalo-Karell, I, Elovainio, M, and Aalto, P. Two models of nursing practice: a comparative study of motivational characteristics, work satisfaction and stress. J Nurs Manag. (2016) 24:261–70. doi: 10.1111/jonm.12313
86. Riisgaard, H, Søndergaard, J, Munch, M, Le, JV, Ledderer, L, Pedersen, LB, et al. Associations between degrees of task delegation and job satisfaction of general practitioners and their staff: a cross-sectional study. BMC Health Serv Res. (2017) 17:44. doi: 10.1186/s12913-017-1984-y
87. Jepsen, I, Juul, S, Foureur, M, Sørensen, EE, and Nøhr, EA. Is caseload midwifery a healthy work-form? – a survey of burnout among midwives in Denmark. Sex Reprod Healthc. (2017) 11:102–6. doi: 10.1016/j.srhc.2016.12.001
88. Jepsen, I, Mark, E, Aagaard Nøhr, E, Foureur, M, and Elgaard, SE. A qualitative study of how caseload midwifery is constituted and experienced by Danish midwives. Midwifery. (2016) 36:61–9. doi: 10.1016/j.midw.2016.03.002
89. Kaltenbrunner, M, Bengtsson, L, Mathiassen, SE, Högberg, H, and Engström, M. Staff perception of lean, care-giving, thriving and exhaustion: a longitudinal study in primary care. BMC Health Serv Res. (2019) 19:652. doi: 10.1186/s12913-019-4502-6
90. Lunde, L-K, Merkus, S, Koch, M, Knardahl, S, Wærsted, M, and Veiersted, KB. Associations of objectively measured total duration and maximum bout length of standing at work with lower-extremity pain intensity: a 2-year follow-up of construction and healthcare workers. BMC Musculoskelet Disord. (2021) 22:1–11. doi: 10.1186/s12891-020-03868-0
91. Olsen, E, Bjaalid, G, and Mikkelsen, A. Work climate and the mediating role of workplace bullying related to job performance, job satisfaction, and work ability: a study among hospital nurses. J Adv Nurs. (2017) 73:2709–19. doi: 10.1111/jan.13337
92. Nielsen, MS, and Jørgensen, F. Meaning creation and employee engagement in home health caregivers. Scand J Caring Sci. (2016) 30:57–64. doi: 10.1111/scs.12221
93. Pedersen, LB, Allen, T, Waldorff, FB, and Andersen, MKK. Does accreditation affect the job satisfaction of general practitioners? A combined panel data survey and cluster randomised field experiment. Health Policy. (2020) 124:849–55. doi: 10.1016/j.healthpol.2020.04.002
94. Fallman, SL, Dellve, L, and Kullén, EA. Managerial approaches for maintaining low levels of sick leave: a qualitative study. J Nurs Manage. (2022) 30:3546–52. doi: 10.1111/jonm.13678
95. Ahlstedt, C, Eriksson Lindvall, C, Holmström, IK, and Muntlin, AÅ. What makes registered nurses remain in work? An ethnographic study. Int J Nurs Stud. (2019) 89:32–8. doi: 10.1016/j.ijnurstu.2018.09.008
96. Slåtten, T, Lien, G, and Mutonyi, BR. Precursors and outcomes of work engagement among nursing professionals—a cross-sectional study. BMC Health Serv Res. (2022) 22:21. doi: 10.1186/s12913-021-07405-0
97. Vifladt, A, Simonsen, BO, Lydersen, S, and Farup, PG. The association between patient safety culture and burnout and sense of coherence: a cross-sectional study in restructured and not restructured intensive care units. Intensive Crit Care Nurs. (2016) 36:26–34. doi: 10.1016/j.iccn.2016.03.004
98. Thapa, DR, Ekström-Bergström, A, Krettek, A, and Areskoug-Josefsson, K. Support and resources to promote and sustain health among nurses and midwives in the workplace: a qualitative study. Nordic J Nurs Res. (2021) 41:166–74. doi: 10.1177/2057158520988452
99. Jacobsen, CB, Hansen, AKL, and Pedersen, LD. Not too narrow, not too broad: linking span of control, leadership behavior, and employee job satisfaction in public organizations. Public Adm Rev. (2022) 83:775–92. doi: 10.1111/puar.13566
100. Sigursteinsdóttir, H, Skúladóttir, H, Agnarsdóttir, T, and Halldórsdóttir, S. Stressful factors in the working environment, lack of adequate sleep, and musculoskeletal pain among nursing unit managers. Int J Environ Res Public Health. (2020) 17:673. doi: 10.3390/ijerph17020673
101. Andersen, LL, Vinstrup, J, Villadsen, E, Jay, K, and Jakobsen, MD. Physical and psychosocial work environmental risk factors for back injury among healthcare workers: prospective cohort study. Int J Environ Res Public Health. (2019) 16:4528. doi: 10.3390/ijerph16224528
102. Vinstrup, J, Jakobsen, MD, Madeleine, P, and Andersen, LL. Physical exposure during patient transfer and risk of back injury & low-back pain: prospective cohort study. BMC Musculoskelet Disord. (2020) 21:715. doi: 10.1186/s12891-020-03731-2
103. Lindegård, A, Nordander, C, Jacobsson, H, and Arvidsson, I. Opting to wear prismatic spectacles was associated with reduced neck pain in dental personnel: a longitudinal cohort study. BMC Musculoskelet Disord. (2016) 17:347. doi: 10.1186/s12891-016-1145-1
104. Westergren, E, Ludvigsen, MS, and Lindberg, M. Associations between materials used and work-related musculoskeletal hand complaints among haemodialysis nurses. J Ren Care. (2020) 46:185–92. doi: 10.1111/jorc.12317
105. Lee, SY, Hung, L, Chaudhury, H, and Morelli, A. Staff perspectives on the role of physical environment in long-term care facilities on dementia care in Canada and Sweden. Dementia. (2021) 20:2558–72. doi: 10.1177/14713012211003994
106. Golvani, J, Roos, L, and Henricson, M. Operating room nurses’ experiences of limited access to daylight in the workplace – a qualitative interview study. BMC Nurs. (2021) 20:227. doi: 10.1186/s12912-021-00751-8
107. Vilén, L, Atosuo, J, and Putus, T. Prevalence of hoarseness in primary health care and hospitals—associations with different work tasks and environmental factors among nurses. J Voice. (2022) 38:1253.e29–1253.e34. doi: 10.1016/j.jvoice.2022.02.024
108. Vilén, L, and Putus, T. Hoarseness among nurses. J Voice. (2021) 37:798.e15–798.e18. doi: 10.1016/j.jvoice.2021.03.030
109. Kjørstad, K, Faaland, PM, Sivertsen, B, Kallestad, H, Langsrud, K, Vethe, D, et al. Sleep and work functioning in nurses undertaking inpatient shifts in a blue-depleted light environment. BMC Nurs. (2022) 21:1–10. doi: 10.1186/s12912-022-00973-4
110. Golay, D, Salminen Karlsson, M, and Cajander, Å. Effortlessness and security: Nurses' positive experiences with work-related information technology use. CIN Comput Informatics Nurs. (2022) 40:589–97. doi: 10.1097/CIN.0000000000000917
111. Stadin, M, Nordin, M, Fransson, EI, and Broström, A. Healthcare managers' experiences of technostress and the actions they take to handle it – a critical incident analysis. BMC Med Informatics Decis Mak. (2020) 20:244. doi: 10.1186/s12911-020-01261-4
112. Golay, D, Salminen Karlsson, M, and Cajander, Å. Negative emotions induced by work-related information technology use in hospital nursing. CIN Comput Informatics Nurs. (2022) 40:113–20. doi: 10.1097/CIN.0000000000000800
113. Heponiemi, T, Hyppönen, H, Vehko, T, Kujala, S, Aalto, A-M, Vänskä, J, et al. Finnish physicians' stress related to information systems keeps increasing: a longitudinal three-wave survey study. BMC Med Informatics Decision Making. (2017) 17:1–8. doi: 10.1186/s12911-017-0545-y
114. Vainiomäki, S, Heponiemi, T, Vänskä, J, and Hyppönen, H. Tailoring ehrs for specific working environments improves work well-being of physicians. Int J Environ Res Public Health. (2020) 17:1–10. doi: 10.3390/ijerph17134715
115. Heponiemi, T, Kaihlanen, AM, Gluschkoff, K, Saranto, K, Nissinen, S, Laukka, E, et al. The association between using a mobile version of an electronic health record and the well-being of nurses: cross-sectional survey study. JMIR Med Inform. (2021) 9:e28729. doi: 10.2196/28729
116. Heponiemi, T, Kujala, S, Vainiomäki, S, Vehko, T, Lääveri, T, Vänskä, J, et al. Usability factors associated with physicians' distress and information system-related stress: cross-sectional survey. JMIR Med Inform. (2019) 7:e13466. doi: 10.2196/13466
117. Holmberg, C, Sobis, I, and Carlström, E. Job satisfaction among Swedish mental health nursing staff: a cross-sectional survey. Int J Public Adm. (2016) 39:429–36. doi: 10.1080/01900692.2015.1018432
118. Rosenström, T, Härmä, M, Kivimäki, M, Ervasti, J, Virtanen, M, Hakola, T, et al. Patterns of working hour characteristics and risk of sickness absence among shift-working hospital employees: a data-mining cohort study. Scand J Work Environ Health. (2021) 47:395–403. doi: 10.5271/sjweh.3957
119. Hult, M, Halminen, O, Mattila-Holappa, P, and Kangasniemi, M. Health and work well-being associated with employment precariousness among permanent and temporary nurses: a cross-sectional survey. Nordic J Nurs Res. (2022) 42:140–6. doi: 10.1177/20571585211070376
120. Grønstad, A, Kjekshus, LE, Tjerbo, T, and Bernstrøm, VH. Work-related moderators of the relationship between organizational change and sickness absence: a longitudinal multilevel study. BMC Public Health. (2020) 20:1218. doi: 10.1186/s12889-020-09325-w
121. Blomberg, K, Isaksson, AK, Allvin, R, Bisholt, B, Ewertsson, M, Kullén Engström, A, et al. Work stress among newly graduated nurses in relation to workplace and clinical group supervision. J Nurs Manage. (2016) 24:80–7. doi: 10.1111/jonm.12274
122. Spännargård, Å, Fagernäs, S, and Alfonsson, S. Self-perceived clinical competence, gender and workplace setting predict burnout among psychotherapists. Couns Psychother Res. (2022) 23:469–77. doi: 10.1002/capr.12532
123. Liss, A, Alian, AY, Wennström, JL, and Abrahamsson, KH. Professional competencies and work-related support in relation to periodontal therapy and work satisfaction: a questionnaire study among Swedish dental hygienists. Int J Dent Hyg. (2018) 16:349–56. doi: 10.1111/idh.12324
124. Jakobsen, MD, Sundstrup, E, Brandt, M, and Andersen, LL. Effect of physical exercise on musculoskeletal pain in multiple body regions among healthcare workers: secondary analysis of a cluster randomized controlled trial. Musculoskelet Sci Pract. (2018) 34:89–96. doi: 10.1016/j.msksp.2018.01.006
125. Ose, SO, Færevik, H, Håpnes, T, and Øyum, L. Perceived causes of work-related sick leave among hospital nurses in Norway: a Prepandemic study. Saf Health Work. (2022) 13:350–6. doi: 10.1016/j.shaw.2022.04.002
126. Mauno, S, Ruokolainen, M, Kinnunen, U, and De Bloom, J. Emotional labour and work engagement among nurses: examining perceived compassion, leadership and work ethic as stress buffers. J Adv Nurs. (2016) 72:1169–81. doi: 10.1111/jan.12906
127. Grønstad, A, Kjekshus, LE, Tjerbo, T, and Bernstrøm, VH. Organizational change and the risk of sickness absence: a longitudinal multilevel analysis of organizational unit-level change in hospitals. BMC Health Serv Res. (2019) 19:895. doi: 10.1186/s12913-019-4745-2
128. Fallman, SL, Jutengren, G, and Dellve, L. The impact of restricted decision-making autonomy on health care managers’ health and work performance. J Nurs Manag. (2019) 27:706–14. doi: 10.1111/jonm.12741
129. Poikkeus, T, Suhonen, R, Katajisto, J, and Leino-Kilpi, H. Relationships between organizational and individual support, nurses' ethical competence, ethical safety, and work satisfaction. Health Care Manag Rev. (2020) 45:83–93. doi: 10.1097/HMR.0000000000000195
130. Burgess, MG, Brough, P, Biggs, A, and Hawkes, AJ. Why interventions fail: a systematic review of occupational health psychology interventions. Int J Stress Manag. (2020) 27:195–207. doi: 10.1037/str0000144
131. Karanika-Murray, M, Biron, C, and Saksvik, P. Organizational health interventions: advances in evaluation methodology. Stress Health. (2016) 32:255–7. doi: 10.1002/smi.2708
132. Kecklund, G, and Axelsson, J. Health consequences of shift work and insufficient sleep. BMJ. (2016) 355:i 5210. doi: 10.1136/bmj.i5210
133. Rosa, D, Terzoni, S, Dellafiore, F, and Destrebecq, A. Systematic review of shift work and nurses' health. Occup Med. (2019) 69:237–43. doi: 10.1093/occmed/kqz063
134. Schneider, A, and Weigl, M. Associations between psychosocial work factors and provider mental well-being in emergency departments: a systematic review. PloS One. (2018) 13:e0197375. doi: 10.1371/journal.pone.0197375
135. Daouk-Öyry, L, Anouze, AL, Otaki, F, Dumit, NY, and Osman, I. The JOINT model of nurse absenteeism and turnover: a systematic review. Int J Nurs Stud. (2014) 51:93–110. doi: 10.1016/j.ijnurstu.2013.06.018
136. Oh, Y, and Gastmans, C. Moral distress experienced by nurses: a quantitative literature review. Nurs Ethics. (2015) 22:15–31. doi: 10.1177/0969733013502803
137. Gyllensten, K, Andersson, G, and Muller, H. Experiences of reduced work hours for nurses and assistant nurses at a surgical department: A qualitaive study. BMC Nurs. (2017) 16. doi: 10.1186/s12912-017-0210-x
138. Karhula, K, Turunen, J, Hakola, T, Ojajärvi, A, Puttonen, S, Ropponen, A, et al. The effects of using participatory working time scheduling software on working hour characteristics and wellbeing: A quasi-experimental study of irregular shift work. Int J Nurs Stud. (2020) 112:9. doi: 10.1016/j.ijnurstu.2020.103696
Keywords: risk factors, health-promoting factors, healthcare, organisational-level, occupational health and safety management, prevention
Citation: Akerstrom M, Wahlström J, Lindegård A, Arvidsson I and Fagerlind Ståhl A-C (2025) Organisational-level risk and health-promoting factors within the healthcare sector—a systematic search and review. Front. Med. 11:1509023. doi: 10.3389/fmed.2024.1509023
Edited by:
Kim Walker, University of Aberdeen, United KingdomReviewed by:
Shah Imran Ahmed, Shah Abdul Latif University, PakistanCopyright © 2025 Akerstrom, Wahlström, Lindegård, Arvidsson and Fagerlind Ståhl. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Magnus Akerstrom, bWFnbnVzLmFrZXJzdHJvbUB2Z3JlZ2lvbi5zZQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.