 Fan-dong Bu
Fan-dong Bu Shang-kun Si
Shang-kun Si Dong-bin Zhang5*
Dong-bin Zhang5*
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Med., 13 January 2025
Sec. Intensive Care Medicine and Anesthesiology
Volume 11 - 2024 | https://doi.org/10.3389/fmed.2024.1502619
This article is part of the Research TopicMechanisms and Interventions for Post-Operative Neurocognitive Disorder and Sleep DisruptionsView all 13 articles
Background: The process of waking up from general anesthesia is still not well understood, and recovery issues such as delayed awakening, agitation, postoperative cognitive dysfunction, continue to be a challenge for anesthesiologists. Currently, the treatment of these complications is mainly achieved through the antagonistic action of specific drugs, but sometimes the antagonistic drugs are not as effective as they should be and can add to the financial burden of the patient. Acupuncture, a common treatment in Traditional Chinese Medicine, is widely used around surgery. However, there is no enough evidence to show it improves recovery after anesthesia. To explore this, we reviewed relevant randomized trials and conducted a meta-analysis.
Objective: This systematic review was conducted to explore the effect of perioperative application of invasive acupuncture on the quality of postoperative awakening after general anesthesia.
Methods: By searching PubMed, Embase, Cochrane Clinical Trials Center, China Knowledge Network (CNKI), China Biomedical Database (CBM), Wanfang Medical Database, Weipu Database, to include randomized controlled trials of invasive acupuncture applied perioperatively. Search is limited from the build-up of the database to March 2022. The statistical analysis was conducted using RevMan 5.3. Quality assessment of the included research literature using Cochrane-recommended risk of bias assessment tool.
Results: 18 randomized controlled trials were included with 1,127 patients. 565 patients in invasive acupuncture intervention group, 562 patients in control group. Results showed that invasive acupuncture group had a shorter eye opening time than control group (MD = −6.42, 95% CI [−8.17, −4.66], p < 0.001), shorter extubation times (MD = -5.84, 95% CI [−8.12, −3.56], p < 0.001), lower MAP at extubation (MD = −18.54, 95% CI [−22.69, −14.39], p < 0.001), lower HR at extubation (MD = −14.85, 95% CI [−23.90, −5.81], p < 0.001). No statistical difference in the occurrence of POCD (OR = 0.56, 95% CI [0.28, 1.11], p = 0.10) and postoperative agitation (OR = 0.42, 95% CI [0.11, 1.65], p = 0.21).
Systematic review registration:
The period of awakening after general anesthesia is both crucial and potentially hazardous (1). Complications such as delayed awakening, emergence agitation (EA), and cardiovascular issues can increase the risk of patient harm. Reports indicate that approximately 19% of adults experience EA following non-cardiac surgeries (2), EA is typically characterized by irritability, purposeless movements, and heightened arousal during the early recovery phase from anesthesia (3). Unlike postoperative delirium (POD), EA involves aggressive behaviors that can pose significant risks to healthcare professionals (4). The process of awakening includes the removal of the tracheal tube, which can activate the sympathetic catecholamine system, leading to increased oxygen consumption and the potential for brain damage (1). Current strategies for managing adverse reactions during this period primarily involve drug antagonism and enhanced analgesia. However, the administration of antagonistic drugs may result in additional complications, such as increased sedation during surgery in patients with EA, which could cause delays in awakening.
Invasive acupuncture, which includes techniques such as hand-twisting and electroacupuncture, is rooted in traditional Chinese medicine. It is thought to regulate the balance between the sympathetic and parasympathetic nervous systems and has demonstrated anti-inflammatory effects through various signaling pathways (5, 6). Owing to its safety, convenience, and fewer side effects, invasive acupuncture is commonly used in clinical settings (7–9).
While invasive acupuncture is commonly employed, there is still a considerable gap in meta-analyses examining its effects on the quality of recovery from general anesthesia. Thus, this study aims to perform a meta-analysis of randomized controlled trials (RCTs) to investigate if invasive acupuncture can affect the quality of awakening. The ultimate goal is to provide an evidence-based framework for clinical decision-making aimed at improving recovery quality during the awakening phase and providing higher-quality evidence.
In this research, invasive acupuncture is defined as including both electroacupuncture and traditional acupuncture, with the intervention group receiving one of these treatments. The time to eye opening is defined as the period from the end of the procedure until the patient opens their eyes, while the time to extubation is defined as the interval from the end of the procedure until the endotracheal tube is removed. Postoperative cognitive dysfunction (POCD) was defined as a decrease of one standard deviation in the Mini-Mental State Examination (MMSE) score at 3 days postoperatively compared to the baseline score obtained 1 day preoperatively. The control group was given either a blank control or a sham intervention.
The aim of this study was to assess the impact of the application of invasive acupuncture on the quality of awakening in postoperative patients undergoing general anesthesia.
(1) Study type: RCT including the effect of invasive acupuncture (Electroacupuncture, acupuncture) on the quality of postoperative awakening after general anesthesia; language is not limited. (2) Study population: The study included patients who underwent surgery under general anesthesia and received either invasive acupuncture or blank/sham stimulation during the perioperative period. No limitations were placed on age, gender, or nationality. (3) Interventions: Invasive acupuncture group received electroacupuncture, or acupuncture. The control group was not subjected to acupuncture stimulation, nor did they receive stimulation at non-meridian or non-acupuncture points.
(1) Studies involving patients undergoing surgeries without general anesthesia or receiving other interventions were included in the analysis. (2) Original text was inaccessible or if the outcome indicators were incomplete. (3) Studies from non-RCTs, systematic evaluations or reviews, mechanistic studies, conferences and animal trials.
BF and SS searched Chinese and English databases on 2022/03/24, included PubMed, Embase, Cochrane Clinical Trials Center, Chinese National Knowledge Infrastructure (CNKI), Wei-pu Database (VIP), Chinese Biomedical Database (CBM), Wan-fang Database, and article were searched from the time of database creation to March 2022.
The Chinese search terms included: “general anesthesia,” “awakening,” “recovery of consciousness,” “open eyes,” “extubation,” “post-anesthesia monitoring treatment room,” “acupoint “, “acupuncture,” “electroacupuncture,” “needle acupuncture,” “randomized controlled trial.” English search terms included: “general anesthesia,” “awakening,” “emergence,” “recovery,” “eye-opening,” “extubation,” “PACU,” “acupoint,” “acupuncture,” “electroacupuncture,” “randomized controlled trial.” The formula can be viewed in the Supplementary material S1.
After de-duplication, two people initially screened by looking at titles and abstracts, and then they reviewed the full article. Key data, such as author names, publication years, sample sizes, interventions, and outcome indicators, were extracted from the final set of screened studies for analysis. If there was any disagreement, the corresponding author was consulted for resolution.
The data of the study was extracted by two independent persons (BF, SS) and the extracted data was saved in an Excel sheet. When there were doubts about the data in the study, they negotiated to resolve them. If data were not available for the outcome of interest, we contacted the authors of the data for information. The names and definitions of the extracted data are given in Supplementary material S2.
Two researchers independently assessed the quality of the studies included in the review using a specific tool and criteria recommended by the Cochrane systematic review manual. The assessment focused on key elements including randomization, blinding, incomplete outcome data, and other potential sources of bias. The findings were classified into three categories: “low risk”, “high risk”, or “unclear”. Methodological and qualitative evaluation of the included literature was as follows. If a study lacks relevant information, the two individuals will contact the corresponding author of the relevant study to enquire. GRADE was also applied to assess the quality of evidence.
Time to open eyes, Time to extubation, MAP immediately after extubation, HR immediately after extubation is a continuous variable are continuous variables, statistical description and effect sizes were combined using Mean difference (MD), along with their corresponding 95% confidence interval (CI). Incidence of POCD and Agitation are dichotomous variables, statistical description and effect sizes were combined using Odds ratio (OR), along with their corresponding 95% confidence interval (CI).
Review Manager 5.3 was applied for data analysis. All outcomes were analyzed using an intention-to-treat analysis. We evaluated the results using MD, OR values, and their 95% CI. A p-value of less than 0.05 was regarded as indicative of a statistically significant difference. Heterogeneity was evaluated using the chi-square test with a significance threshold of α = 0.1, and the extent of heterogeneity was quantified by the I2 statistic. When heterogeneity is obvious (I2 ≥ 50%), random effects model is used. When heterogeneity is low (I2 < 50%), using fixed effects model. The results of each synthesis are presented in the form of a forest plot. Funnel plots were used to evaluate publication bias when a sufficient number (n ≥ 10) of studies were available for analysis. A balanced distribution of points on the center line was considered a low level of publication bias. Egger’s test was employed to evaluate the presence of publication bias when there was a lack of sufficient study (n < 10). p < 0.05 suggests a publication bias.
Based on age classification, we performed subgroup analyses of eye-opening time. One group is age >60, another group is age ≤ 60. Based on the type of surgery, we performed subgroup analyses of time to extubation. One group is minor surgery and one group is major surgery.
When I2 ≥ 50%, a sensitivity analysis of the literature was performed, the sensitivity analysis was done by excluding studies where the MD deviated more from the center in the forest plot produced by Review manager 5.3. A larger deviation means that more heterogeneity is likely to be produced. Re-perform sensitivity analysis until I2 is stable.
A total of 2,043 relevant literature was obtained from the search, 784 duplicates were excluded, 1,004 were excluded based on the title and abstract, After the full-text assessment, 18 studies meeting the study requirements were included, involved a total of 1,127 patients, 565 cases in invasive acupuncture group and 562 cases in control group. Figure 1 illustrates the literature screening process, Tables 1, 2 display the study characteristics and interventions details of the included studies. Good results in quality grading of evidence from included studies (see Supplementary material S3 GRADE).
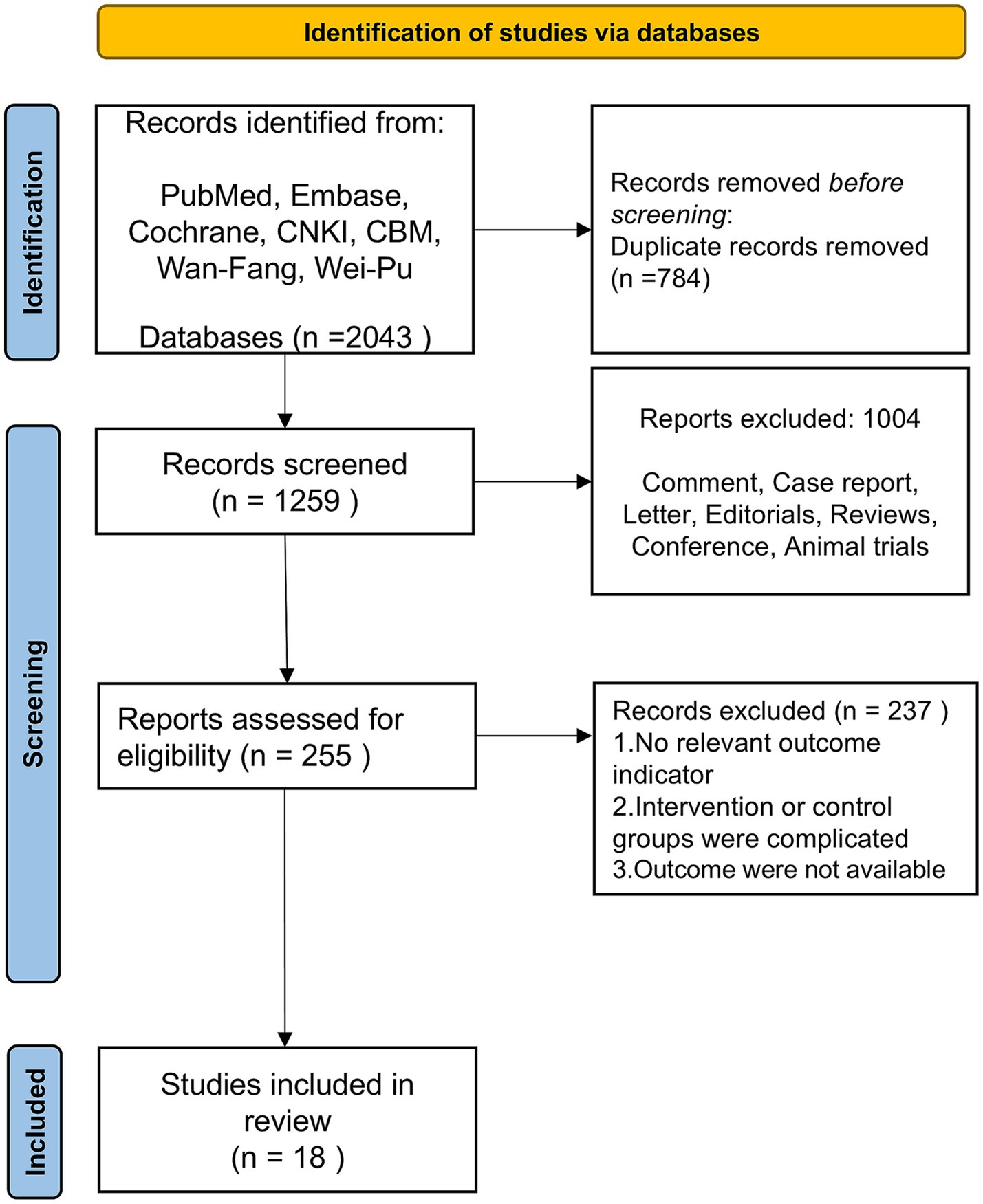
Figure 1. Flow chart of literature screening.
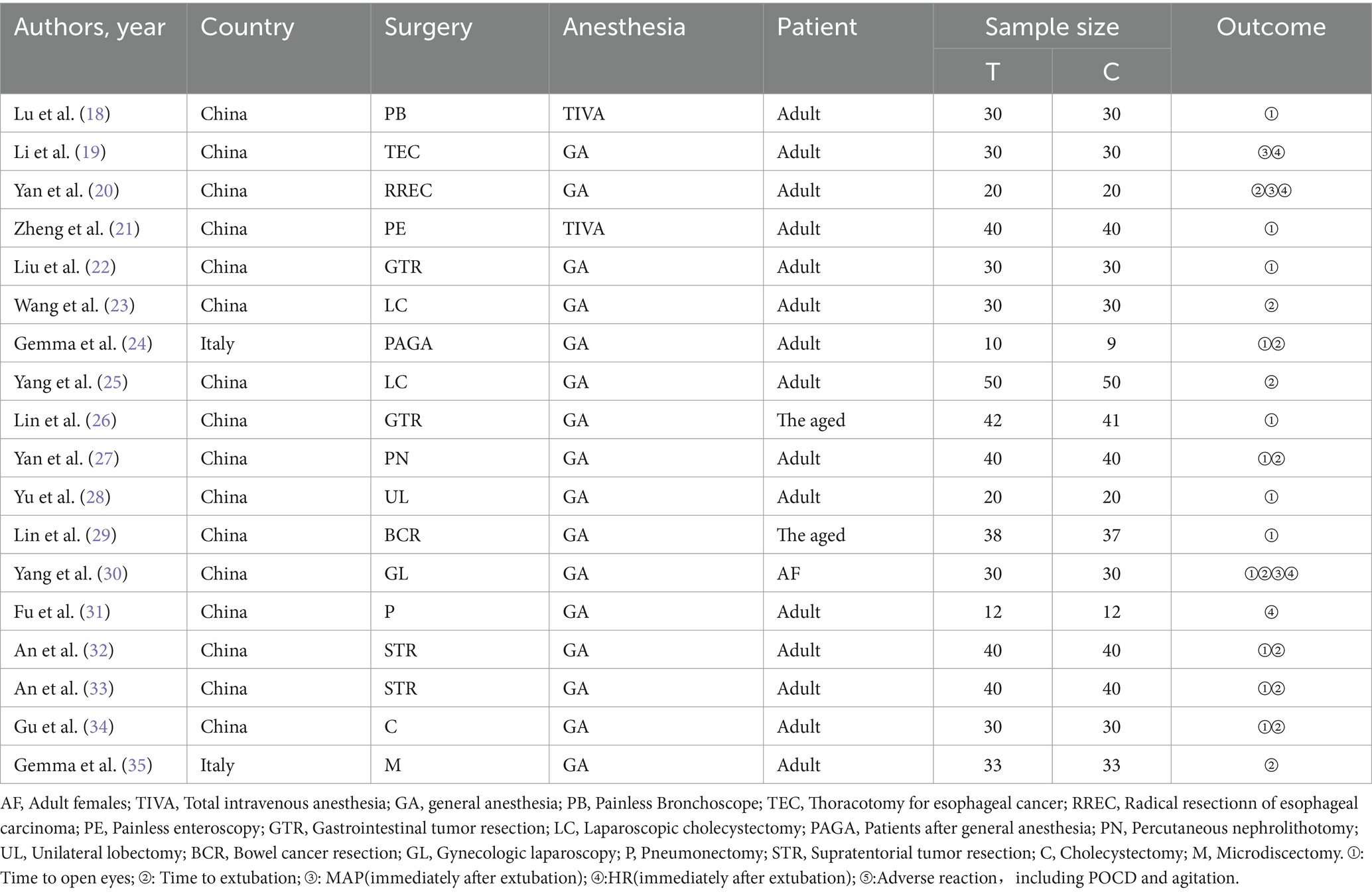
Table 1. Study characteristics.
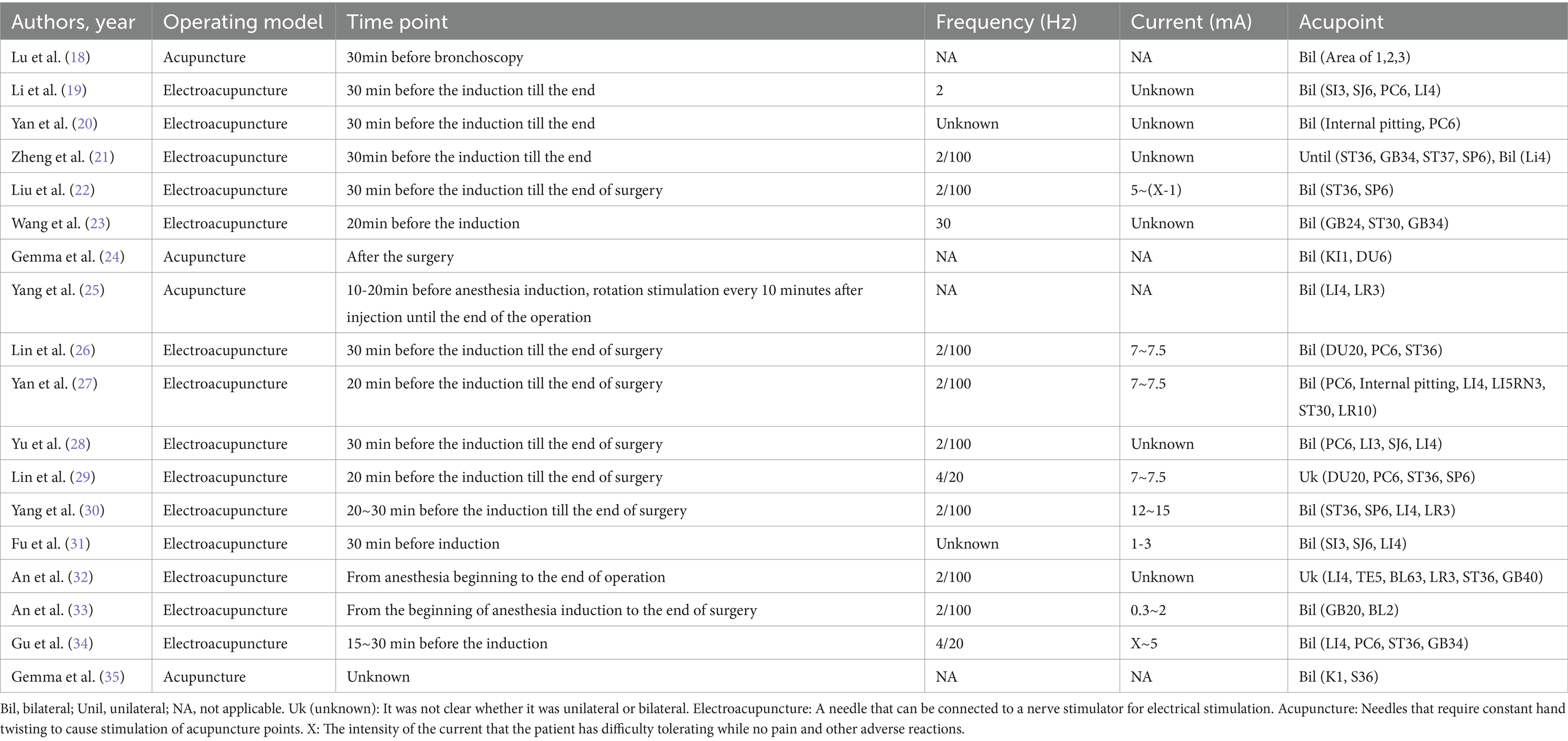
Table 2. Details of interventions.
The assessment of bias for the included studies is shown in Figure 2. The overall risk of bias of the included studies showed good. Results of publication bias test in Supplementary material S4.
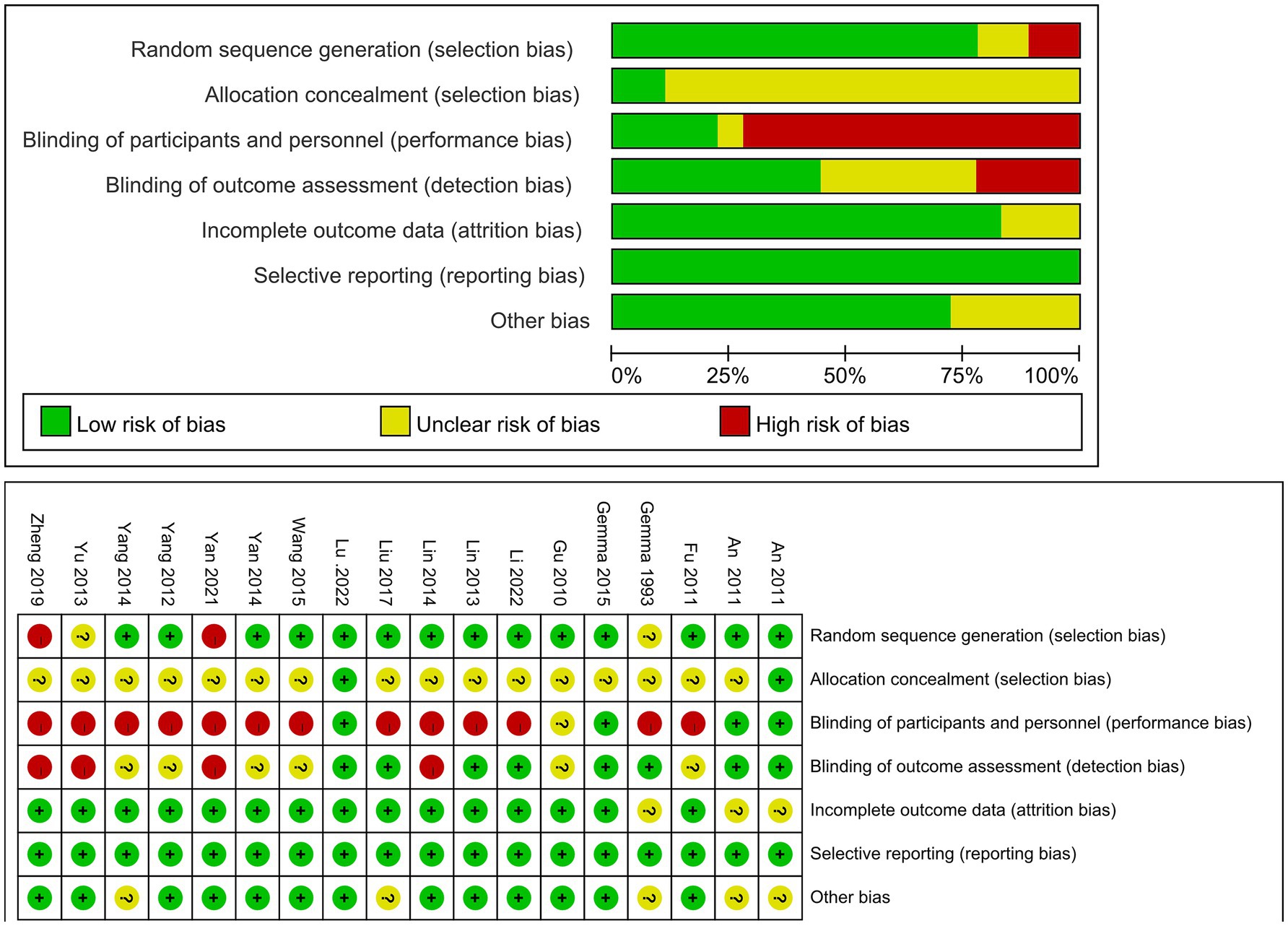
Figure 2. Risk of bias graph and risk of bias summary.
10 studies mentioned time to open eyes. Included 677 patients, 340 in invasive acupuncture group, 337 in control group. Heterogeneity test I2 = 90% and random effects model was used to synthesize the data. Result shows that invasive acupuncture group had a shorter eye-opening time than control group (MD = −6.42, 95% CI [−8.17, −4.66], p < 0.001), as shown in Figure 3.
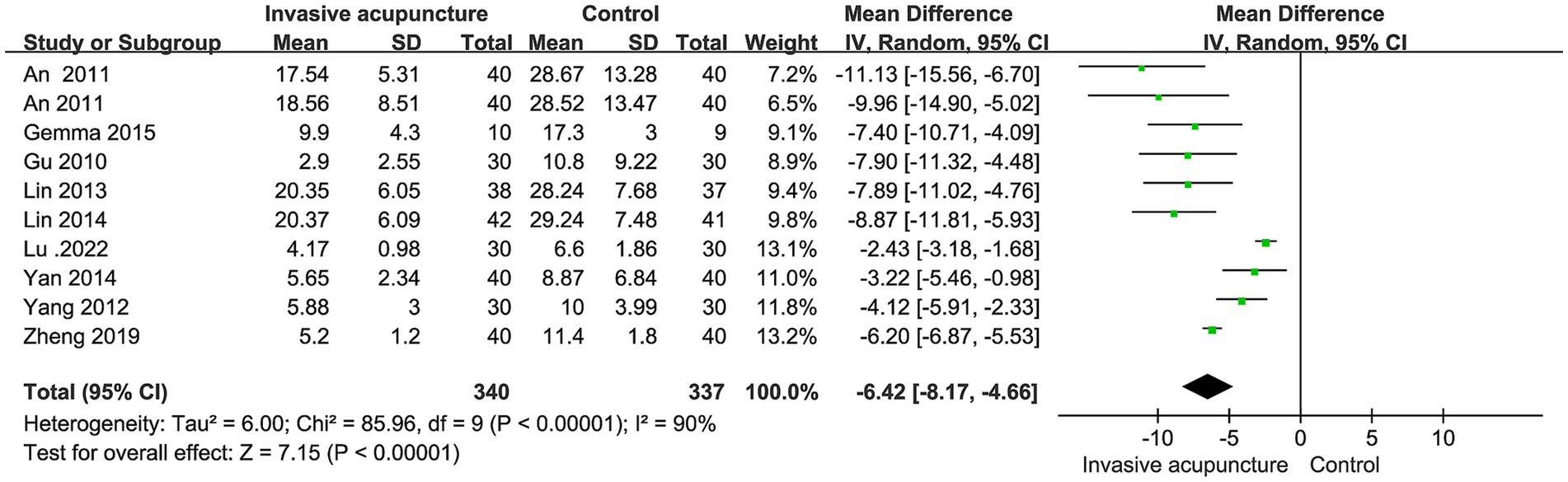
Figure 3. Synthesized results of eye-opening time.
12 studies mentioned the time to extubation. Included 745 patients, 373 in invasive acupuncture group, 372 in control group. I2 = 93%, with high heterogeneity, random effects model data synthesis results show that invasive acupuncture group has a shorter extubation time compared to control group (MD = -5.84, 95% CI [−8.12, −3.56], p < 0.001), as illustrated in Figure 4.
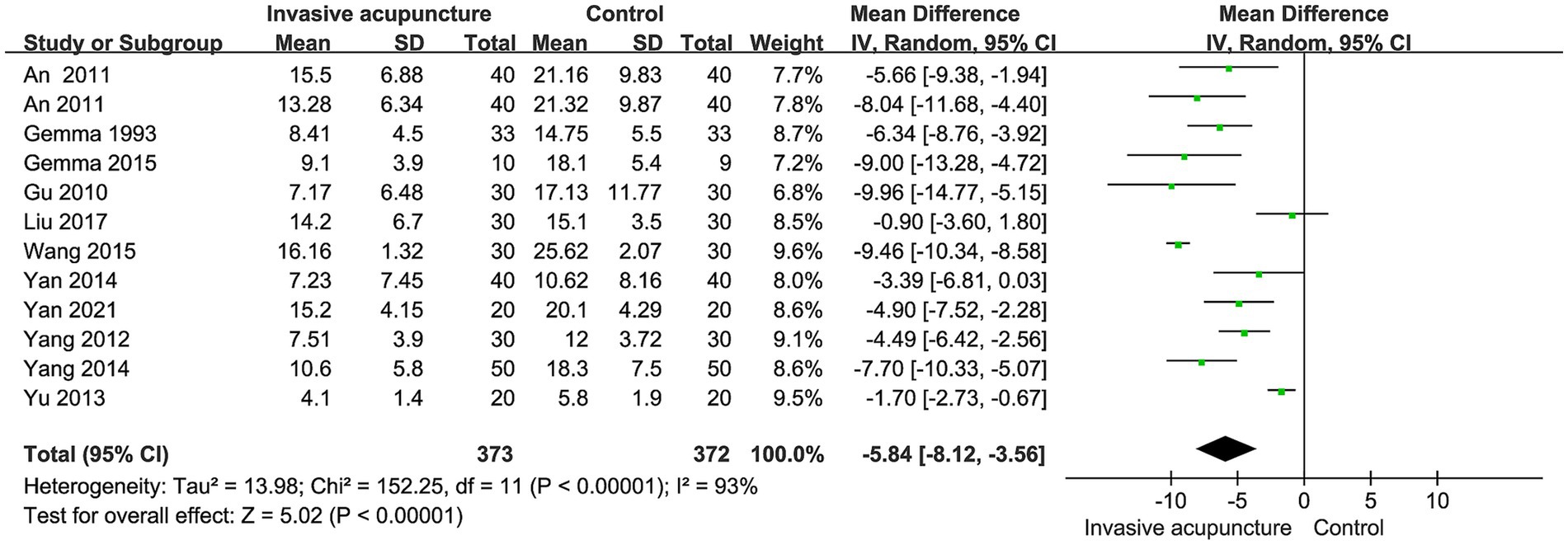
Figure 4. Synthesized results of extubation time.
3 studies mentioned the mean arterial pressure (MAP) immediately following extubation. 160 patients in total, 80 in invasive acupuncture group, 80 in control group. Heterogeneity test I2 = 56%, using random effects model for combining effect sizes. The MAP was lower in invasive acupuncture group than in the control group (MD = −18.54, 95% CI [−22.69, −14.39], p < 0.001), as shown in Figure 5.

Figure 5. Synthesized results of MAP.
4 studies mentioned heart rate (HR) at extubation. The synthesis included 184 patients, with 92 in the invasive acupuncture group and 92 in the control group. A heterogeneity test showed an I2 value of 91%, and the results were analyzed using a random effects model. Showed that HR was lower in invasive acupuncture group at the moment of extubation (MD = −14.85, 95% CI [−23.90, −5.81], p < 0.001), forest plot in Figure 6.

Figure 6. Synthesized results of HR.
2 studies reported about the incidence of postoperative cognitive dysfunction (POCD). Included 158 patients, 80 in invasive acupuncture group while 78 patients in the control group. I2 = 0%, a fixed-effects model was used, the result showed that no statistical difference between invasive acupuncture group and control group on incidence of POCD (OR = 0.56, 95% CI [0.28, 1.11], p = 0.10), forest plot in Figure 7.

Figure 7. Synthesized results of POCD.
Three studies mentioned the incidence of postoperative agitation. 220 patients involved, 110 in invasive acupuncture group, 110 in control group. Heterogeneity was low (I2 = 18%), according to fixed effects model and effect size analysis no statistical difference was found on postoperative agitation (OR = 0.42, 95% CI [0.11, 1.65], p = 0.21), forest plot in Figure 8.
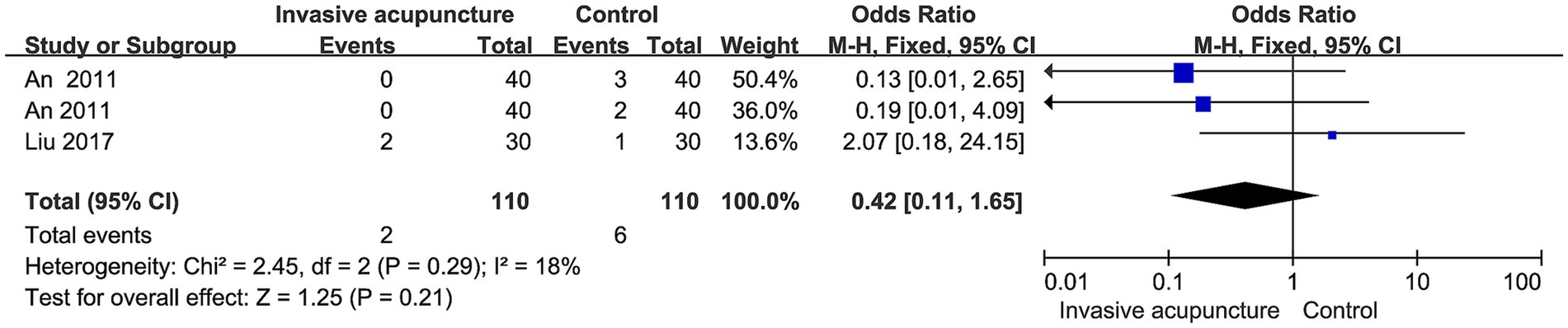
Figure 8. Synthesized results of agitation.
Based on age classification, we performed subgroup analyses of eye-opening time. One group is age >60, another group is age ≤ 60. Results suggests that heterogeneity may come from group age ≤ 60 (I2 = 91%). We performed subgroup analyses of time to extubation stratified by type of surgery (minor or major). The findings from these analyses suggest that the type of surgery does not appear to be a significant source of heterogeneity in the synthesized results for time to extubation, as shown in Figures 9, 10.
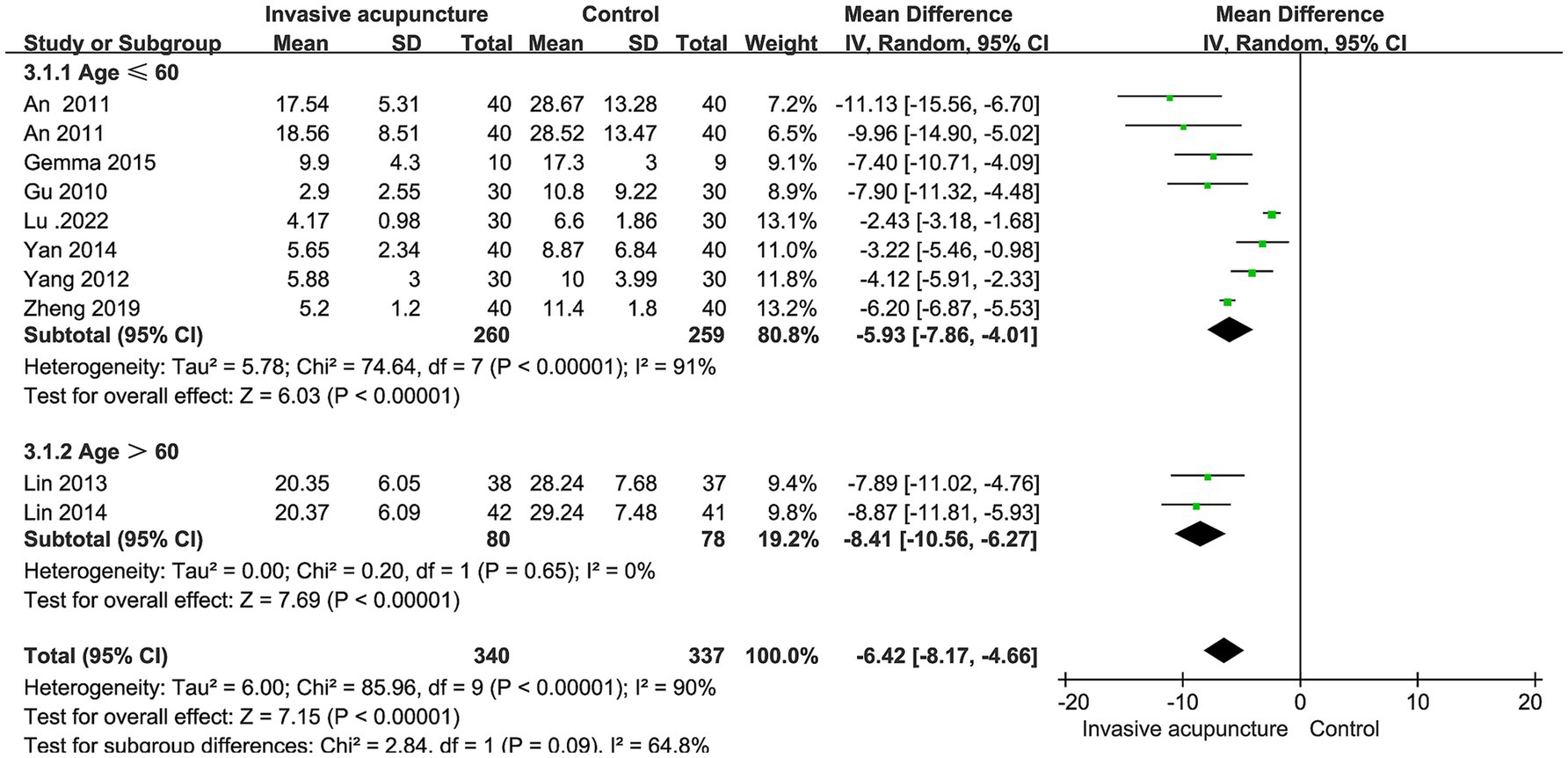
Figure 9. Subgroup analysis results of eye-opening time.
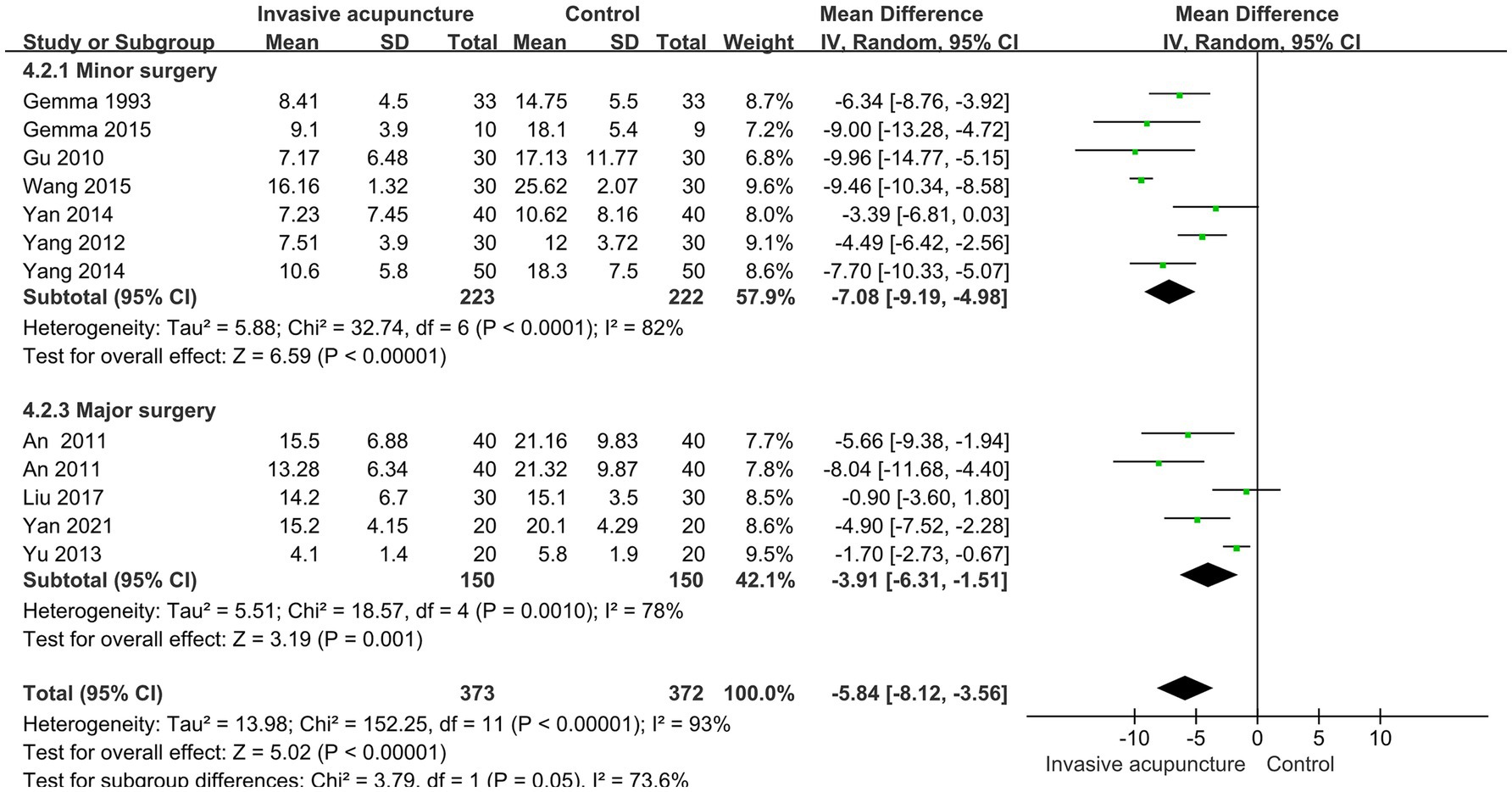
Figure 10. Subgroup analysis results of extubation time.
For single studies with large heterogeneity, excluding any one evidence in Revman 5.3 had no effect on the overall effect. This suggests that the results of our study are robust and reliable. In the synthesized analysis of immediate heart rate at extubation, we observed that Yan 2021 has a great heterogeneity.
All synthesized results show that perioperative application of invasive acupuncture accelerates awakening from general anesthesia and improves the quality of awakening. Both electroacupuncture and acupuncture require acupuncture needles to be inserted into the skin and their interventions are similar in nature, so the interventions included in this study were both of them. It is noteworthy that in both electroacupuncture and acupuncture they intervened 20–30 min before the start of surgery. This coincides with the timing of perioperative acupuncture application in recent years. For the selection of acupuncture points, most of the studies took PC6. This may suggest that stimulation of PC6 promotes the patient’s awakening after general anesthesia.
Electroacupuncture, a technique that applies electrical stimulation through acupuncture needles, can activate different neurotransmitters in the brain based on the frequency of stimulation. Specifically, electroacupuncture administered at a frequency of 2/100 Hz can stimulate the release of three substances—endorphins, enkephalins, and prednisolone—in the spinal cord (10). This may also explain why the frequency of electroacupuncture in the literature included in this study is mostly 2/100 Hz.
For both papers involving POCD, postoperative MMSE scores declined in both the intervention and control groups compared to their preoperative levels, with the difference being apparent on the third postoperative day. The invasive acupuncture group had higher scores than control group. However, the impact of cognitive scores over a longer postoperative period is lacking and more high-quality, large sample size clinical studies are needed to add to the evidence.
It is important to acknowledge the potential side effects associated with acupuncture, considering its invasive nature. While bleeding stands as the most commonly reported adverse reaction, rare occurrences of pneumothorax (11), hemothorax (12), and even cases like the one documented by Abe Daishiro (13), involving vertebral artery perforation due to fractured and displaced silver needles, emphasize the significance of proper training for acupuncture practitioners. The scarcity of experienced acupuncturists remains a notable concern raised by critics in surveys gauging the sentiments of healthcare professionals towards acupuncture in Australia (14).
Nevertheless, patients’ enthusiasm for perioperative acupuncture remains undiminished. In a preoperative assessment survey conducted at the Mayo Clinic (15), a remarkable 68.4% of participants expressed keen interest in receiving acupuncture during the perioperative period. Notably, the approval rate for complimentary acupuncture services reached an impressive 86.7%, underscoring the substantial potential for the perioperative application of acupuncture in the Western world. This view was confirmed across the pond in European. Acupuncture is widely available and promoted in Switzerland and France. Switzerland’s insurance is the most supportive of acupuncture in all of European, with reimbursement rates of up to 70–80%, and if the acupuncturist is a licensed Western medical practitioner, the patient can receive an even higher reimbursement rate. In France, due to the large number of acupuncture clinics, the competition between clinics has led directly to lower prices for acupuncture. It is easy to see how the low cost could greatly increase the acceptance of acupuncture by patients in the European and American countries.
Owing to linguistic barriers and other pertinent factors, the comprehensive adoption of traditional Chinese acupuncture in the Western world poses considerable challenges. Consequently, a process of localization has emerged, wherein dry needling therapy and battlefield acupuncture (16, 17) offer expedient and efficient means of attaining analgesic effects. As a result, these approaches find extensive utilization in the realms of combatting opioid abuse and managing pain in military settings.
At the same time the subject of this literature is the awakening process after general anesthesia, and patients with non-general anesthesia do not exclude. The two papers included in this study had TIVA anesthesia although there was an anesthetic awakening process, but there was no use of inhalational anesthetics, which may increase the heterogeneity of the study when compared to anesthesia with a combination of sedation and suction and the difference in the type of intervention.
Of the types of surgeries included in these 18 articles in the literature, 7 were on the digestive system, which accounted for the largest proportion. Thoracic surgeries were next in importance with 5 articles. However, urological surgeries gynecological surgeries orthopedic surgeries neurological surgeries accounted for a lesser percentage. The patient population for these surgeries were all adults, so the findings of this study cannot be extended to the minor patient population.
There was variation in the neurostimulation instrumentation utilized within the electroacupuncture group, further contributing to heterogeneity. The absence of allocation concealment methods presents a direct risk to the research due to inadequate attention. Additionally, only some of the studies reported using blinding methods, which increases the risk of measurement bias. The absence of allocation concealment methods poses a direct risk to the research due to lack of attention.
The combined analysis of time to open eyes, time to extubation, and immediate heart rate at extubation demonstrated significant heterogeneity. To explore potential sources of this heterogeneity, we performed subgroup analyses for time to open eyes and time to extubation, along with sensitivity analyses for immediate heart rate at extubation. For the time to open eyes, subgroup stratification was based on age (≤60 years and >60 years), while for time to extubation, stratification was based on the type of surgery (minor or major). The findings revealed that heterogeneity for time to open eyes was 91% in the ≤60 years group and 0% in the >60 years group, suggesting that the younger age group (≤60 years) was likely responsible for the observed heterogeneity.
Extubation time was analyzed by categorizing surgeries into minor and major groups based on duration, with minor surgeries defined as lasting ≤2 h and major surgeries as lasting >2 h. The synthesized results demonstrated significant heterogeneity between the two groups, suggesting that surgery duration was not a contributing factor to the observed heterogeneity in extubation time. While subgroup analyses of time to open eyes and extubation time revealed considerable heterogeneity, the direction of the effect size was consistent across all groups. This consistency indicates that invasive acupuncture facilitates postoperative awakening and extubation in both minor and major surgeries, regardless of age group (≤60 years or >60 years).
Subgroup analyses demonstrated a reduction in heterogeneity across all subgroups, indicating that subgroup characteristics may contribute as a potential risk factor for the observed heterogeneity. However, this suggests that subgroup information alone is not the sole determinant of heterogeneity.
In the synthesized analysis of immediate heart rate at extubation, we observed that excluding one study (Yan, 2021) reduced the heterogeneity among the remaining three studies to 0%. This finding suggests that the Yan (2021) study contributed significantly to the observed heterogeneity. This may be explained by the fact that, in Yan’s (2021) study, epidural analgesia was administered intraoperatively, effectively reducing the patients’ pain response during the immediate extubation period. Since pain is a significant contributor to increased heart rate in the postoperative period, this intervention likely influenced the observed outcomes. Additionally, epidural anesthesia can slow heart rate if the level of anesthesia is excessively high (above T4), as it may block the cardiac sympathetic nerves.
The conclusions of the study should be viewed with caution due to the possible heterogeneity of the synthesized results. Future clinical studies of acupuncture should aim for multicenter, long follow-up periods, and standardized treatment protocols.
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found in the article/Supplementary material.
F-dB: Conceptualization, Data curation, Formal analysis, Investigation, Validation, Writing – original draft. S-kS: Conceptualization, Data curation, Supervision, Writing – original draft, Writing – review & editing. D-bZ: Project administration, Supervision, Writing – review & editing. Y-lC: Project administration, Supervision, Writing – review & editing.
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. Funded by Shandong Province Chinese Medicine Science and Technology Program (Grant number: Z-2022048).
Thanks to our colleagues for creating a great writing environment.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declare that no Gen AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2024.1502619/full#supplementary-material
1. Fàbregas, N, and Bruder, N. Recovery and neurological evaluation. Best Pract Res Clin Anaesthesiol. (2007) 21:431–47. doi: 10.1016/j.bpa.2007.06.006
2. Tolly, B, Waly, A, Peterson, G, Erbes, CR, Prielipp, RC, and Apostolidou, I. Adult emergence agitation: a veteran-focused narrative review. Anesth Analg. (2021) 132:353–64. doi: 10.1213/ANE.0000000000005211
3. Seo, I-S, Seong, C-R, Jung, G, Park, S-J, Kim, SY, and Kim, MM. The effect of sub-tenon lidocaine injection on emergence agitation after general anaesthesia in paediatric strabismus surgery. Eur J Anaesthesiol. (2011) 28:334–9. doi: 10.1097/EJA.0b013e3283426ed6
4. McGuire, JM. The incidence of and risk factors for emergence delirium in U.S. military combat veterans. J Perianesth Nurs. (2012) 27:236–45. doi: 10.1016/j.jopan.2012.05.004
5. Chen, T, Zhang, WW, Chu, Y-X, and Wang, Y-Q. Acupuncture for pain management: molecular mechanisms of action. Am J Chin Med. (2020) 48:793–811. doi: 10.1142/S0192415X20500408
6. Yang, N-N, Yang, J-W, Ye, Y, Huang, J, Wang, L, Wang, Y, et al. Electroacupuncture ameliorates intestinal inflammation by activating Α7nachr-mediated Jak2/Stat3 signaling pathway in postoperative ileus. Theranostics. (2021) 11:4078–89. doi: 10.7150/thno.52574
7. Garland, SN, Xie, SX, DuHamel, K, Bao, T, Li, Q, Barg, FK, et al. Acupuncture versus cognitive behavioral therapy for insomnia in cancer survivors: a randomized clinical trial. JNCI J Natl Cancer Inst. (2019) 111:1323–31. doi: 10.1093/jnci/djz050
8. Hinman, RS, McCrory, P, Pirotta, M, Relf, I, Forbes, A, Crossley, KM, et al. Acupuncture for chronic knee pain: a randomized clinical trial. JAMA. (2014) 312:1313–22. doi: 10.1001/jama.2014.12660
9. Liao, H-Y, Satyanarayanan, SK, Lin, Y-W, and Su, K-P. Clinical efficacy and immune effects of acupuncture in patients with comorbid chronic pain and major depression disorder: a double-blinded, randomized controlled crossover study. Brain Behav Immun. (2023) 110:339–47. doi: 10.1016/j.bbi.2023.03.016
10. Jisheng, H. New evidence to substantiate the frequency specificity of acupuncture-induced analgesia. Acupunct Res. (2001) 26:224–7. doi: 10.3969/j.issn.1000-0607.2001.03.045
11. Th’ng, F, Rao, KA, and Huang, PY. Case series: acupuncture-related pneumothorax. International. J Emerg Med. (2022) 15:1–4. doi: 10.1186/s12245-022-00455-z
12. Hanabusa, Y, Kubo, T, Watadani, T, Nagano, M, Nakajima, J, and Abe, O. Successful transcatheter arterial embolization for a massive hemothorax caused by acupuncture. Radiol Case Rep. (2022) 17:3107–10. doi: 10.1016/j.radcr.2022.05.040
13. Abe, D, Hanaoka, Y, Kobayashi, K, Kiuchi, T, Watanabe, T, Kobayashi, S, et al. Surgical removal of an intracranially migrated acupuncture needle: a case report and literature review. Nagoya J Med Sci. (2022) 84:890–9. doi: 10.18999/nagjms.84.4.890
14. Zhang, NM, Daly, D, Terblanche, M, Joshi, S, Mark Tacey, M, Vesty, G, et al. Doctors’ and nurses’ attitudes of acupuncture and acupressure use in perioperative care: an Australian National Survey. Pain Manag Nurs. (2022) 23:800–10. doi: 10.1016/j.pmn.2022.08.008
15. Harbell, MW, Barendrick, LN, Mi, L, Quillen, J, and Millstine, DM. Patient attitudes toward acupuncture in the perioperative setting. J Integrat Comp Med. (2022) 28:349–54. doi: 10.1089/jicm.2021.0311
16. Chen, S-Z, and Gong, C-Z. Localization of Chinese acupuncture-moxibustion in the United States: the openness of modern acupuncture-moxibustion system. Zhongguo Zhen Jiu. (2020) 40:85–8. doi: 10.13703/j.0255-2930.20181214-0006
17. Kim, H, Ronald, RM, and Burtson, K. Battlefield acupuncture appears to be an effective therapy for pain management. Acupunct Med. (2022) 40:43–9. doi: 10.1177/09645284211050648
18. Zhi-xia, L, Li, Y, Min-xiao, L, Wei, H, and Zeng-jie, L. Reducing dosage of propofol in painless undergoing bronchoscopy of elderly patients by wrist-ankle acupuncture: a randomised controlled trail. CJITWM. (2022) 42:317–21. doi: 10.7661/j.cjim.20211119.224
19. Maojun, L, Qiuxia, D, Xiaodong, Z, Huawen, P, Binxiu, W, Daping, T, et al. Application and safety of Electroacupuncture combined with Tci target controlled infusion in anesthesia for one lung ventilation esophagectomy for esophageal cancer. Modern Tradtion Chin Med Materia Med World Sci Tech. (2022) 24:1660–6. doi: 10.11842/wst.20210111011
20. Xiang-biao, Y, Xue-chang, H, Qun-zhi, X, Yu, L, Xu, D, You, W, et al. Comparative study between electroacupuncture at neima point and neiguan (pc 6) and epidural nerve block for preemptive analgesia in patients undergoing thoracic surgery. Chin Acupunct Moxibust. (2021) 41:59–64. doi: 10.13703/j.0255-2930.20200121-k0001
21. Junfei, Z, Ye, L, Zhiyong, C, Dan, W, Jiamin, Z, and Meihua, Z. Clinical efficacy of electroacupuncture combined with propofol in painless enteroscopy. J Clin Anesth. (2019) 35:874–7. doi: 10.12089/jca.2019.09.010
22. Yang, L, Zeguo, F, Guokai, L, Jie, Z, Jingwei, Z, and Enlu, Z. Effects of electroacupuncture on general anesthesia recovery of elderly patients undergoing gastrointestinal surgery. Acad J Chin PLA Med Sch. (2017) 38:1051–4. doi: 10.3969/j.issn.2095-5227.2017.11.014
23. Yidong, W, Jia, Z, Gang, H, Xiancheng, K, Yu, C, and Hangjun, G. The application of needle-medicine compound anaesthesia in laparoscopic cholecystectomy clinical efficacy observation. J Basic Chin Med. (2015) 21:728–30. doi: 10.19945/j.cnki.issn.1006-3250.2015.06.040
24. Gemma, M, Nicelli, E, Gioia, L, Moizo, E, Beretta, L, and Calvi, MR. Acupuncture accelerates recovery after general anesthesia: a prospective randomized controlled trial. J Integr Med. (2015) 13:99–104. doi: 10.1016/S2095-4964(15)60159-5
25. Xiaochu, Y, Huimin, X, Yalan, W, Meiyuan, H, Yan, L, and Liehu, J. Clinical study of acupuncture-assisted general anaesthesia for laparoscopic cholecystectomy. CJITWM. (2014) 34:883–6. doi: 10.7661/CJM201407.0883
26. Shun-yan, L, Zheng-lu, Y, Ju, G, Luo-jing, Z, and Xin, C. Effect of acupuncture-anesthetic composite anesthesia on the incidence of Pocd and Tnf-Α,Il-1β,Il-6 in elderly patients. CJITWM. (2014) 34:795–9. doi: 10.7661/CJIM.2014.07.0795
27. Jiang, Y, Cui-qin, L, Cheng-zhang, Z, Jin-yan, O, Fu-rong, L, Shao-lin, Z, et al. Effects of assisted-Electroacupuncture on recovery of fast tracking anesthesia in Mpcnl. Chin Acupunct Moxibust. (2014) 34:385–8. doi: 10.13703/j.0255-2930.2014.04.023
28. Zhang-Jie, Y, Wen-Yuan, Y, Jian-Gang, S, and Xiang-Rui, W. Effects of acupuncture combined with ultrasound-guided ParaverteBral block on perioperative analgesia in patients undergoing ThoracotOmy surger. Chin J Pain Med. (2013) 19:71–4. doi: 10.3969/j.issn.1006-9852.2013.02.003
29. Shun-yan, L, Zheng-lu, Y, Ju, G, Hai-ming, W, and Luo-jing, Z. Influence of acupuncture anesthesia on postoperative cognitive dysfunction and S-100β protein level of the elderly patients of colorectal cancer resection. Chin Acupunct Moxibust. (2013) 33:63–6. doi: 10.13703/j.0255-2930.2013.01.024
30. Qiong-hui, Y, Wu-hua, M, and Yu-hui, L. Comparison of effects of acupuncture-asisted anesthesia with different acupoint combination in gynecologic laparoscopy operation. Chin Acupunct Moxibust. (2012) 32:59–64. doi: 10.13703/j.0255-2930.2012.01.024
31. Guo-qiang, F, Jia, Z, Qiu-yu, T, Yu-ming, Z, Wen, M, Hong, Z, et al. Observation on the anti-stress effect of acupuncture-assisted anesthesia for Pul Monary Lobecto my patients. Acupunct Res. (2011) 36:361–5. doi: 10.13702/j.1000-0607.2011.05.010
32. Li-xin, A, Ying, H, Xiu-jun, R, Shu-qin, L, Ru-quan, H, and Bao-guo, W. Effect of electroacupuncture on sevoflurane anesthesia in patients undergoing resection of Supratentorial tumor. Acupunct Anesth. (2011) 21:36–42.
33. Li-xin, A, Yong, J, Li-li, W, Xiu-jun, R, Yun-ning, L, and Bao-guo, W. The application of electro-acupuncture combined with sevoflurane anesthesia in neurosurgery. CJITWM. (2011) 31:1181–6.
34. Chenyi, G, and Yunbiao, C. Application of combined acupuncture and Intratracheal anesthesia in cholecystectomy under LaParoscopy. Chin Acupunct Moxibust. (2010) 21:231–3. doi: 10.13703/j.0255-2930.2010.08.022
Keywords: invasive acupuncture, general anesthesia, awakening, systematic review, meta-analysis
Citation: Bu F-d, Si S-k, Zhang D-b and Chi Y-l (2025) Effect of invasive acupuncture on awakening quality after general anesthesia: systematic review and meta-analysis. Front. Med. 11:1502619. doi: 10.3389/fmed.2024.1502619
Edited by:
Zhaolan Hu, Central South University, ChinaReviewed by:
Xi-Xi Tang, Chongqing University, ChinaCopyright © 2025 Bu, Si, Zhang and Chi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yong-liang Chi, MTU1NTMxNTY1ODhAMTYzLmNvbQ==; Dong-bin Zhang, emhhbmdkYnp1bnlpQDE2My5jb20=
†These authors share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.