 Xiaohui Fang1,2†Yuhang Yin1,3†Haonan Zhao1,2†Cai’e Wang1,2†Hui Li1,2Yiyang Shang1,2Jiayu Li4Yue Gao5
Xiaohui Fang1,2†Yuhang Yin1,3†Haonan Zhao1,2†Cai’e Wang1,2†Hui Li1,2Yiyang Shang1,2Jiayu Li4Yue Gao5 Nahum Méndez-Sánchez6*
Nahum Méndez-Sánchez6* Xingshun Qi1,2,3*
Xingshun Qi1,2,3*- 1Department of Gastroenterology, The General Hospital of Northern Theater Command (Teaching Hospital of Shenyang Pharmaceutical University), Shenyang, China
- 2Department of Life Sciences and Biopharmaceutics, Shenyang Pharmaceutical University, Shenyang, China
- 3Postgraduate College, China Medical University, Shenyang, China
- 4Department of Laboratory Medicine, The General Hospital of Northern Theater Command, Shenyang, China
- 5Department of Ultrasound, The General Hospital of Northern Theater Command, Shenyang, China
- 6Liver Research Unit, Medica Sur Clinic and Foundation, National Autonomous University of Mexico, Mexico City, Mexico
Purpose: Chronic hepatitis B (CHB) and fatty liver disease (FLD) are common chronic liver diseases, both of which can progress to advanced liver diseases with poor outcome. However, it remains controversial whether the presence of FLD aggravates the disease severity of CHB patients.
Patients and methods: All consecutive outpatients who were diagnosed with CHB at our department between March 1, 2021 and September 30, 2023 were retrospectively screened. They were divided into FLD and non-FLD groups. Liver function parameters and non-invasive indicators of liver fibrosis, including liver stiffness measurement (LSM) value, fibrosis-4 index (FIB-4) score, and aspartate aminotransferase to platelet ratio index (APRI) score, were compared between the two groups. Subgroups analyses were performed in HBeAg-positive, HBeAb-positive, HBV DNA > 10 IU/mL, mild FLD, and moderate/severe FLD patients.
Results: Overall, 201 CHB patients were included, of whom 76 (37.81%) had FLD. In the overall analyses, CHB patients with FLD had a significantly higher alanine aminotransferase (ALT) (47.04 ± 53.28 vs. 32.95 ± 35.10, p = 0.003) than those without FLD, but there was no significant difference in the LSM value (7.79 ± 5.16 vs. 8.19 ± 4.99, p = 0.508), FIB-4 score (1.13 ± 0.75 vs. 1.28 ± 0.99, p = 0.679), and APRI score (0.41 ± 0.46 vs. 0.36 ± 0.47, p = 0.535) between CHB patients with and without FLD. The above-mentioned statistical results in all subgroup analyses were nearly consistent with those in the overall analyses.
Conclusion: FLD may intensify abnormal liver function reflected by increased ALT level in CHB patients, but not influence the progression of liver fibrosis.
1 Introduction
Chronic hepatitis B (CHB) is a chronic liver disease caused by long-term infection with hepatitis B virus (HBV), affecting an estimated 316 million people, which poses a significant global health challenge (1). In CHB patients, fibrosis can be secondary to persistent inflammation with subsequent scar formation (2). Approximately 20% of them will progress from fibrosis to cirrhosis and hepatocellular carcinoma (HCC), in spite of widespread use of HBV vaccines and effective antiviral therapy in recent years (3, 4).
Fatty liver disease (FLD), a condition characterized by excessive fat accumulation in the liver, is mainly divided into alcohol-related and metabolic dysfunction-associated fatty liver disease (MAFLD) (5, 6). MAFLD is closely related to overweight/obesity, type 2 diabetes, and metabolic dysregulation, and it is the prominent cause of FLD and becomes the most common cause of chronic liver diseases in some regions (7–9). According to the recent findings from a large National Health and Nutrition Examination Surveys (NHANES) study, the estimated prevalence of MAFLD among the American adults significantly increased from 22% to 36% during the past three decades (10). Lifestyle modifications are the only approved interventions for the treatment of FLD (11). Once MAFLD patients developed fibrosis, the risk of liver-related mortality would be significantly increased (12).
Generally, CHB and FLD are common chronic liver diseases, both of which can progress to advanced liver diseases with poor prognosis. The coexistence of FLD with CHB is also common, especially in Asia (13, 14). Recently, some studies have shown that concomitant FLD may exacerbate the progression of CHB with a higher incidence of liver fibrosis and abnormal liver function, increasing the risk of cirrhosis, HCC, and death (13, 15, 16). However, others suggested that FLD might be beneficial to the disease course of CHB by decreasing the levels of HBV DNA and HBsAg, and compromising the development of liver fibrosis (17, 18). Considering this controversy in this topic, a retrospective study has been performed to explore the impact of FLD on liver function and fibrosis in patients with CHB.
2 Methods
2.1 Study design
We retrospectively reviewed the medical records of 201 outpatients with CHB who were treated by one physician (XQ) at the Department of Gastroenterology of the General Hospital of Northern Theater Command between March 1, 2021 and September 30, 2023. This study has been approved by the Medical Ethical Committee of the General Hospital of Northern Theater Command with an approval number [NO. Y (2024) 082]. It was performed according to the 1975 Declaration of Helsinki. Patients’ written informed consents were waived by the Medical Ethical Committee of our hospital due to the retrospective nature of this study.
Exclusion criteria were as follows: (i) repeated visits of the same patient; (ii) patients diagnosed with liver cirrhosis; (iii) patients diagnosed with HCC; and (iv) absence of imaging examinations, such as ultrasound, computed tomography (CT), or magnetic resonance imaging (MRI).
2.2 Laboratory test
Total bilirubin [(TBIL, reference range: 0–21 μmol/L, reagent CH0101003), direct bilirubin (DBIL, reference range: 0–8 μmol/L, reagent CH0101004), alanine aminotransferase (ALT, reference range: 7–40 U/L, reagent AUZ2390), aspartate aminotransferase (AST, reference range: 13–35 U/L, reagent AUZ2197), alkaline phosphatase (AKP, reference range: 50–135 U/L, reagent AUZ1959), gamma-glutamyl transferase (GGT, reference range: 7–45 U/L, reagent GS9051G), total bile acid (TBA, reference range: 0–10 μmol/L, reagent CH0101005)] were analyzed with reagents from Mike Laboratories (Mike, Sichuan, China) on a AUS800 automatic biochemical analyzer (Beckman Coulter, Suzhou, China); platelet count [PLT, reference range: 125–350 (×109/L), reagent DS] were analyzed with reagents from Mindray Laboratories (Mindray, Shenzhen, China) on a BC-6800PLUS instrument (Mindray, Shenzhen, China); and alpha-fetoprotein (AFP, reference range: 0–7 ng/mL, reagent 105-002524-00) were analyzed with reagents from Mindray Laboratories (Mindray, Shenzhen, China) on a CL-6000i instrument (Mindray, Shenzhen, China) at the Department of Laboratory Medicine. Virological indicators [hepatitis B surface antigen (HBsAg, reagent IM4403001), hepatitis B surface antibody (HBsAb, reagent IM4403002), hepatitis B e antigen (HBeAg, reagent IM4403003), hepatitis B e antibody (HBeAb, reagent IM4403004), hepatitis B core antibody (HBcAb, reagent IM4403005)] were analyzed with reagents from Mike Laboratories (Mike, Sichuan, China) on a i3000B instrument (Mike, Sichuan, China) at the Department of Laboratory Medicine. Hepatitis B virus deoxyribonucleic acid (HBV DNA, reagent 20230403B) was analyzed with reagents from Northeast Pharmaceutical (Northeast Pharmaceutical, Shanghai, China) on a Gentier 9EB instrument (Northeast Pharmaceutical, Shanghai, China) by real-time fluorescence quantitative polymerase chain reaction at the Department of Laboratory Medicine.
2.3 Imaging
Hepatobiliary imaging examination (ultrasound, CT, or MRI) was performed at the Department of Ultrasound and Department of Radiology, when the patients should be fasting. The liver stiffness measurement (LSM) and controlled attenuation parameter (CAP) value were measured by the Hepatus 6 CS liver ultrasound diagnostic instrument (Mindray, Shenzhen, China) at the Department of Gastroenterology, when the patients should be fasting for at least 2 h (19).
2.4 Scores
Body mass index (BMI), fibrosis-4 index for liver fibrosis (FIB-4), and aspartate aminotransferase to platelet ratio index (APRI) were also calculated.
2.5 Diagnosis and group
CHB was diagnosed with positive HBsAg for a duration of more than 6 months, and antiviral therapy is recommended when HBV DNA level is positive (i.e., HBV DNA level is more than 10 IU/mL at our hospital) in CHB patients without cirrhosis according to the recommendations of current Chinese guideline on the prevention and treatment of chronic hepatitis B (20). Notably, HBV DNA screening should be further conducted when HBsAg is positive.
FLD was diagnosed under hepatobiliary ultrasound, CT, and/or MRI according to the recommendations of Chinese guideline on diagnosis and treatment for FLD (5). FLD was classified as mild (240–265 db/m), moderate (265–295 db/m), and severe (above 295 db/m) according to the CAP value. CHB patients were divided into FLD and non-FLD groups.
2.6 Statistical analyses
All statistical analyses were performed by using SPSS version 25.0 statistical software (IBM Corp, Armonk, NY, USA). Continuous variables were expressed as mean ± standard deviation and median (range), and compared by the independent sample t-tests for normal distribution, and those without normal distribution by nonparametric Mann–Whitney U tests. The Chi-square test was used for categorical variables to analyze the difference between groups. Subgroups analyses were performed in HBeAg-positive patients, HBeAb-positive patients, patients with HBV DNA > 10 IU/mL, and patients with mild and moderate/severe FLD. A two-tailed p < 0.05 was considered statistically significant.
3 Results
3.1 Patient selection
A total of 201 CHB patients were included (Figure 1), of whom 76 (37.81%) had FLD. Patient characteristics are summarized in Table 1.
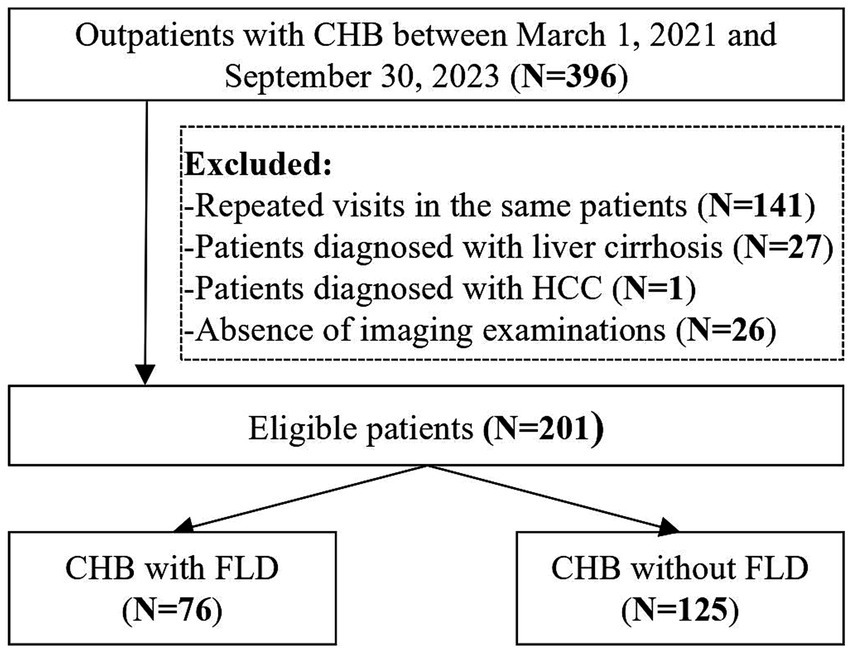
Figure 1. Flowchart of patients’ screening and grouping. CHB, chronic hepatitis B; FLD, fatty liver disease; HCC, hepatocellular carcinoma.
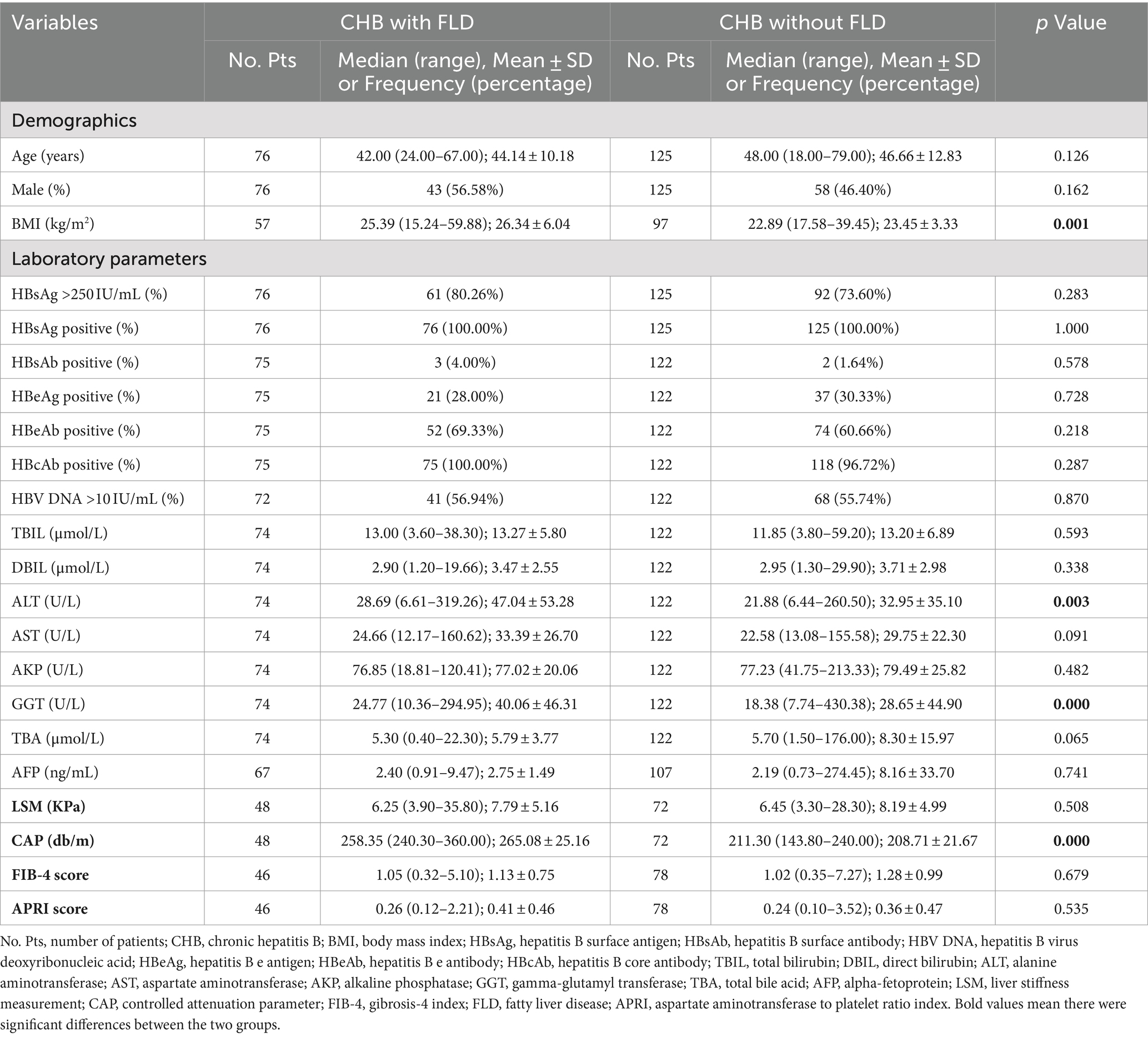
Table 1. Baseline characteristics of CHB patients with versus without FLD.
3.2 Overall analysis
CHB patients with FLD had significantly higher BMI (26.34 ± 6.04 vs. 23.45 ± 3.33, p = 0.001), ALT (47.04 ± 53.28 vs. 32.95 ± 35.10, p = 0.003), and GGT (40.06 ± 46.31 vs. 28.65 ± 44.90, p = 0.000) than those without FLD, but there was no significant difference in the proportions of HBsAg-positive >250 IU/mL (80.26% vs. 73.60%, p = 0.283), HBeAg-positive (28.00% vs. 30.33%, p = 0.728), HBeAb-positive (69.33% vs. 60.66%, p = 0.218), HBcAb-positive (100.00% vs. 96.72%, p = 0.287), and HBV DNA > 10 IU/mL (56.94% vs. 55.74%, p = 0.870), AST (33.39 ± 26.70 vs. 29.75 ± 22.30, p = 0.091), AFP (2.75 ± 1.49 vs. 8.16 ± 33.70, p = 0.741), LSM value (7.79 ± 5.16 vs. 8.19 ± 4.99, p = 0.508), FIB-4 score (1.13 ± 0.75 vs. 1.28 ± 0.99, p = 0.679), and APRI score (0.41 ± 0.46 vs. 0.36 ± 0.47, p = 0.535) between CHB patients with and without FLD (Table 1).
3.3 Subgroup analyses
3.3.1 HBeAg-positive patients
In HBeAg-positive patients, the proportion of male (80.95% vs. 45.95%, p = 0.005) was significantly higher in CHB with FLD than those without FLD, but age (37.43 ± 7.41 vs. 41.19 ± 12.35, p = 0.153), BMI (24.49 ± 3.25 vs. 22.83 ± 3.32, p = 0.108), ALT (79.03 ± 85.33 vs. 53.61 ± 50.29, p = 0.394), AST (45.70 ± 41.28 vs. 43.71 ± 33.51, p = 0.973), GGT (34.44 ± 21.16 vs. 40.63 ± 68.66, p = 0.170), AFP (2.48 ± 1.29 vs. 21.51 ± 62.19, p = 0.135), LSM value (10.01 ± 7.61 vs. 9.52 ± 5.81, p = 0.899), FIB-4 score (0.86 ± 0.41 vs. 1.54 ± 1.57, p = 0.223), and APRI score (0.61 ± 0.73 vs. 0.62 ± 0.84, p = 0.530) were not significantly different between them (Table 2).
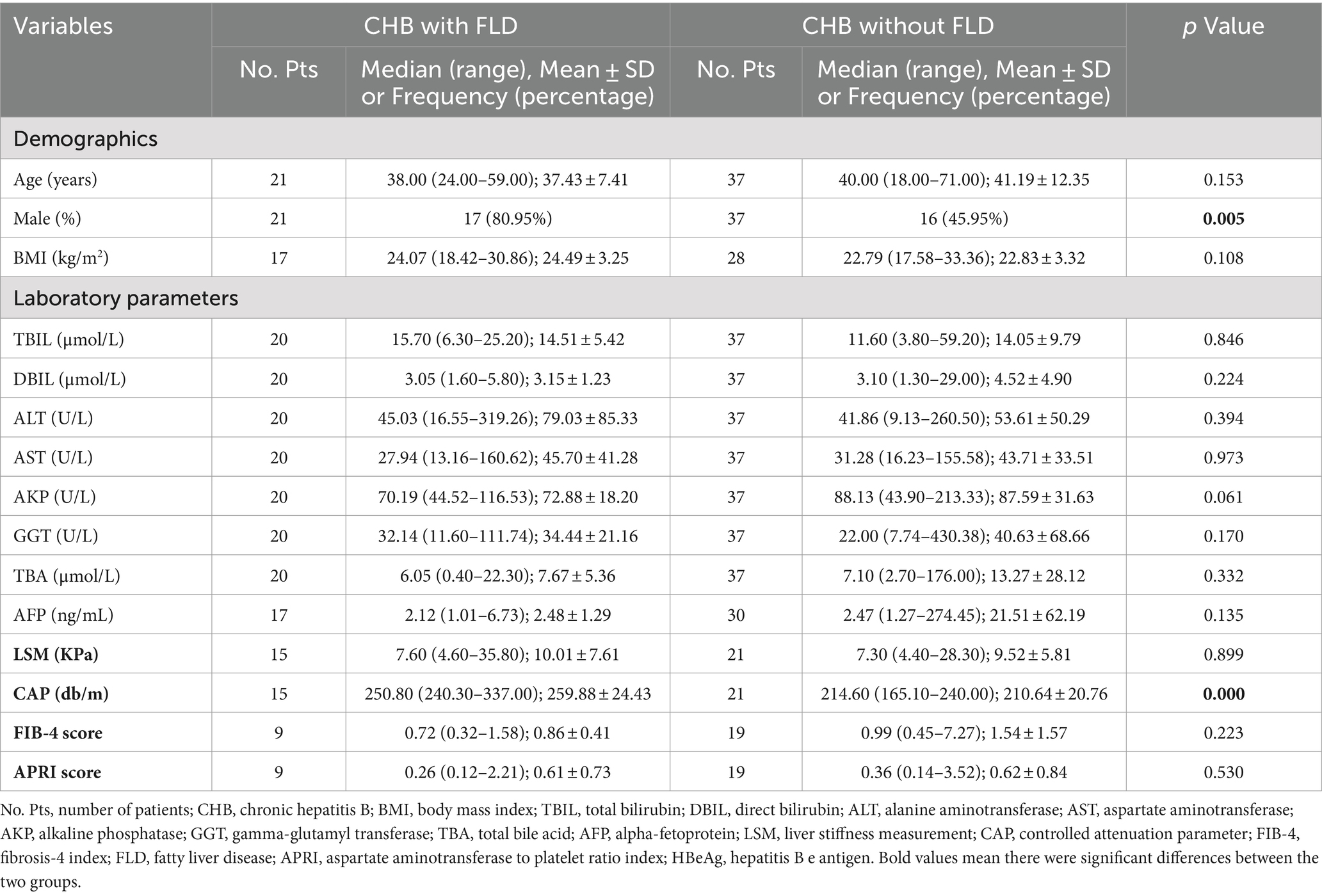
Table 2. Subgroups analyses of HBeAg-positive patients with versus without FLD.
3.3.2 HBeAb-positive patients
In HBeAb-positive patients, BMI (27.12 ± 6.96 vs. 23.80 ± 3.58, p = 0.009), ALT (33.03 ± 22.87 vs. 24.35 ± 21.76, p = 0.004), AST (28.37 ± 16.91 vs. 23.91 ± 11.14, p = 0.039), and GGT (40.70 ± 53.26 vs. 23.25 ± 29.63, p = 0.002) were significantly higher in CHB patients with FLD than those without FLD, but the proportion of male (44.23% vs. 48.65%, p = 0.625), age (47.02 ± 10.04 vs. 48.82 ± 12.49, p = 0.553), AFP (2.81 ± 1.56 vs. 3.00 ± 3.35, p = 0.189), LSM value (6.78 ± 3.32 vs. 7.19 ± 4.25, p = 0.622), FIB-4 score (1.21 ± 0.81 vs. 1.21 ± 0.73, p = 0.996), and APRI score (0.36 ± 0.36 vs. 0.29 ± 0.21, p = 0.296) were not significantly different between them (Table 3).
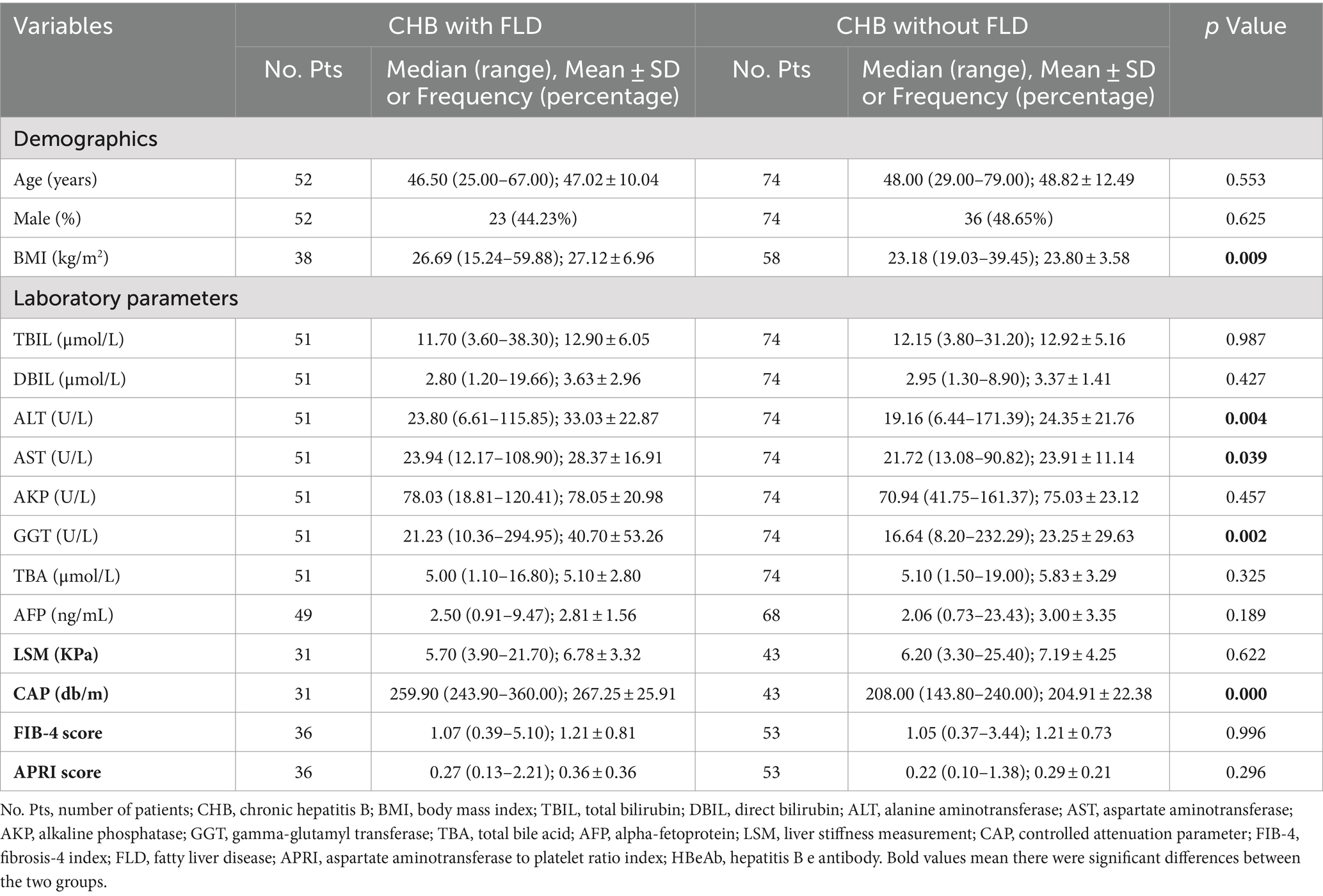
Table 3. Subgroups analyses of HBeAb-positive patients with versus without FLD.
3.3.3 HBV DNA > 10 IU/mL patients
In HBV DNA > 10 IU/mL patients, BMI (25.22 ± 3.54 vs. 23.10 ± 3.43, p = 0.009), ALT (62.47 ± 66.30 vs. 40.63 ± 43.99, p = 0.004), AST (41.02 ± 33.09 vs. 34.75 ± 28.33, p = 0.026), and GGT (38.13 ± 27.99 vs. 30.57 ± 51.87, p = 0.004) were significantly higher in CHB patients with FLD than those without FLD, but DBIL (3.04 ± 1.12 vs. 4.08 ± 3.73, p = 0.036) was significantly lower in CHB with FLD than those without FLD. The proportion of male (60.98% vs. 45.59%, p = 0.119), age (41.73 ± 9.77 vs. 45.51 ± 14.08, p = 0.283), AFP (2.63 ± 1.27 vs. 12.55 ± 46.20, p = 0.936), LSM value (8.74 ± 6.80 vs. 8.01 ± 5.05, p = 0.883), FIB-4 score (1.26 ± 0.98 vs. 1.34 ± 1.18, p = 0.995), and APRI score (0.56 ± 0.61 vs. 0.43 ± 0.61, p = 0.189) were not significantly different between them (Table 4).
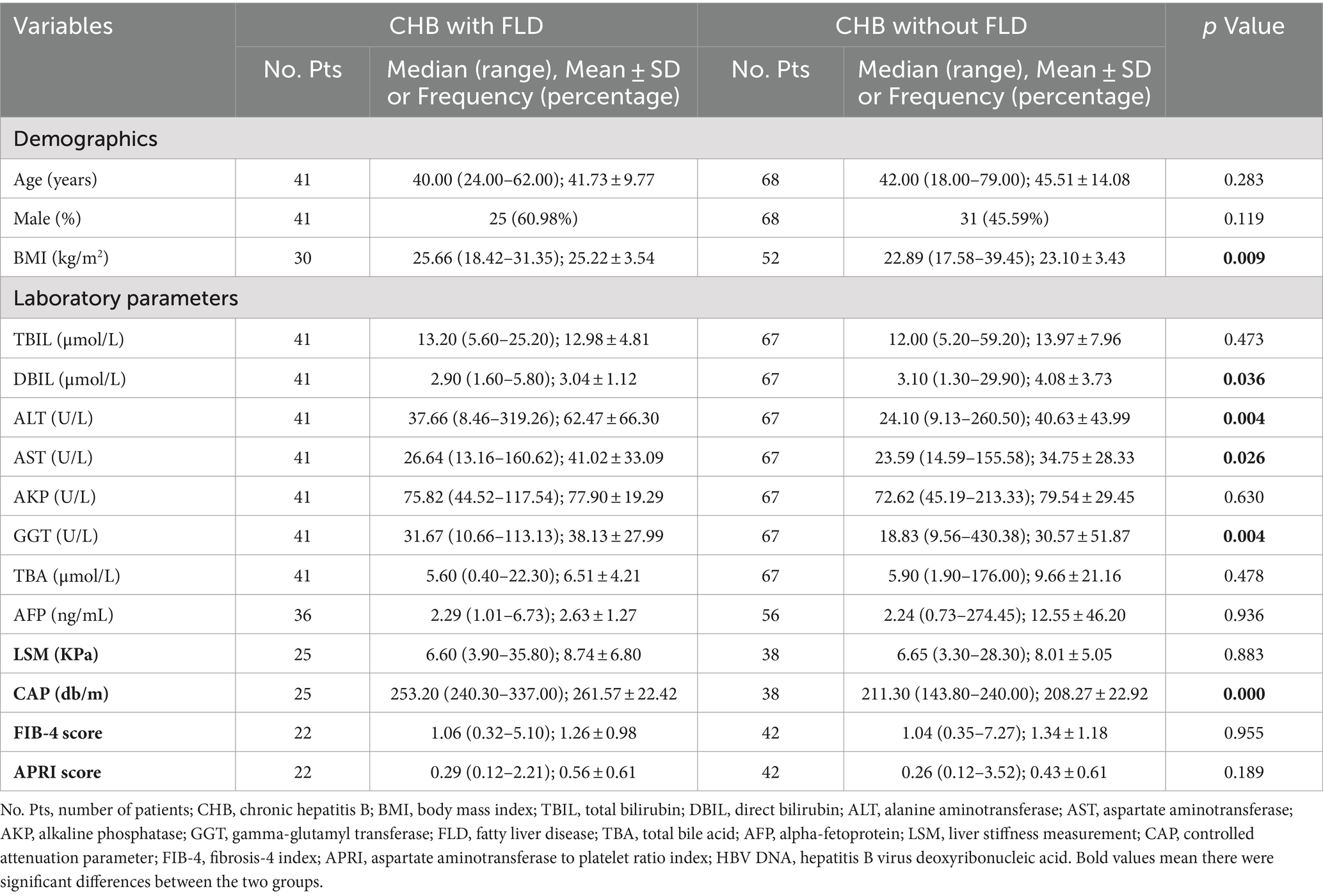
Table 4. Subgroups analyses of HBV DNA > 10 IU/mL patients with versus without FLD.
3.3.4 Mild FLD
In CHB patients, BMI (25.53 ± 3.78 vs. 23.45 ± 3.33, p = 0.005), and GGT (30.36 ± 25.07 vs. 28.65 ± 44.90, p = 0.049) were significantly higher in CHB patients with mild FLD than those without FLD, but the proportions of male (57.14% vs. 46.40%, p = 0.261), HBsAg-positive >250 IU/mL (80.00% vs. 73.60%, p = 0.440), HBeAg-positive (31.43% vs. 30.33%, p = 0.901), HBeAb-positive (65.71% vs. 60.66%, p = 0.587), HBcAb-positive (100.00% vs. 96.72%, p = 0.576), and HBV DNA > 10 IU/mL (54.55% vs. 55.74%, p = 0.903), age (44.60 ± 11.36 vs. 46.66 ± 12.83, p = 0.390), ALT (43.56 ± 52.54 vs. 32.95 ± 35.10, p = 0.101), AST (31.69 ± 26.24 vs. 29.75 ± 22.30, p = 0.229), AFP (2.90 ± 1.91 vs. 8.16 ± 33.70, p = 0.989), LSM value (8.27 ± 5.88 vs. 8.19 ± 4.99, p = 0.803), FIB-4 score (1.13 ± 0.43 vs. 1.28 ± 0.99, p = 0.854), and APRI score (0.40 ± 0.48 vs. 0.36 ± 0.47, p = 0.676) were not significantly different between them (Table 5).
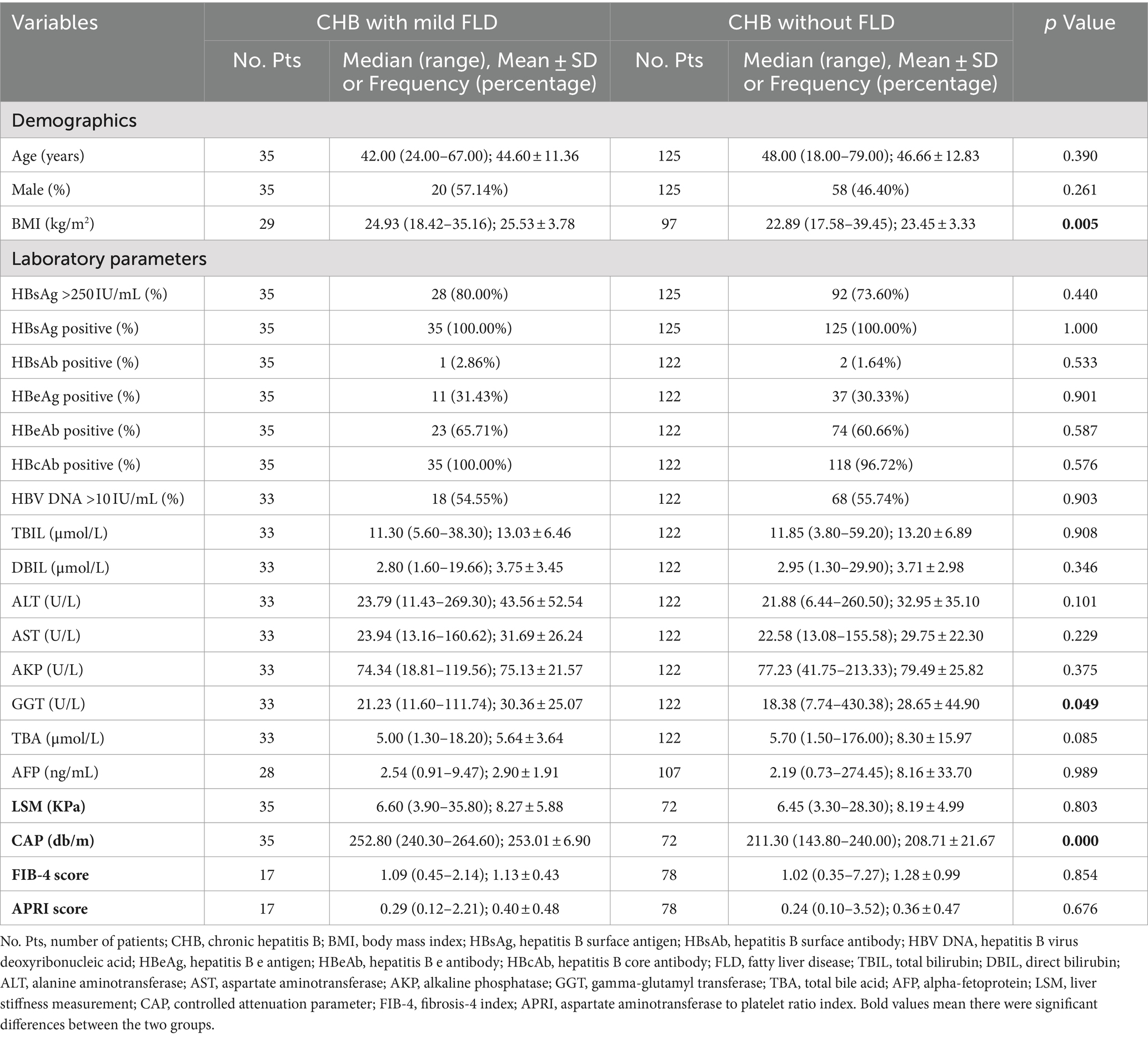
Table 5. Subgroup analyses of CHB patients with mild FLD versus without FLD.
3.3.5 Moderate/severe FLD
In CHB patients, the proportions of male (53.85% vs. 46.40%, p = 0.609), HBsAg-positive >250 IU/mL (76.92% vs. 73.60%, p = 1.000), HBeAg-positive (30.77% vs. 30.33%, p = 1.000), HBeAb-positive (61.54% vs. 60.66%, p = 0.951), HBcAb-positive (100.00% vs. 96.72%, p = 1.000), and HBV DNA > 10 IU/mL (53.85% vs. 55.74%, p = 0.896), age (42.15 ± 11.16 vs. 46.66 ± 12.83, p = 0.225), ALT (37.06 ± 25.24 vs. 32.95 ± 35.10, p = 0.136), AST (25.81 ± 7.74 vs. 29.75 ± 22.30, p = 0.612), GGT (31.57 ± 20.28 vs. 28.65 ± 44.90, p = 0.200), AFP (2.47 ± 0.80 vs. 8.16 ± 33.70, p = 0.859), LSM value (6.50 ± 1.91 vs. 8.19 ± 4.99, p = 0.294), FIB-4 score (0.79 ± 0.41 vs. 1.28 ± 0.99, p = 0.066), and APRI score (0.23 ± 0.05 vs. 0.36 ± 0.47, p = 0.322) were not significantly different between them (Table 6).
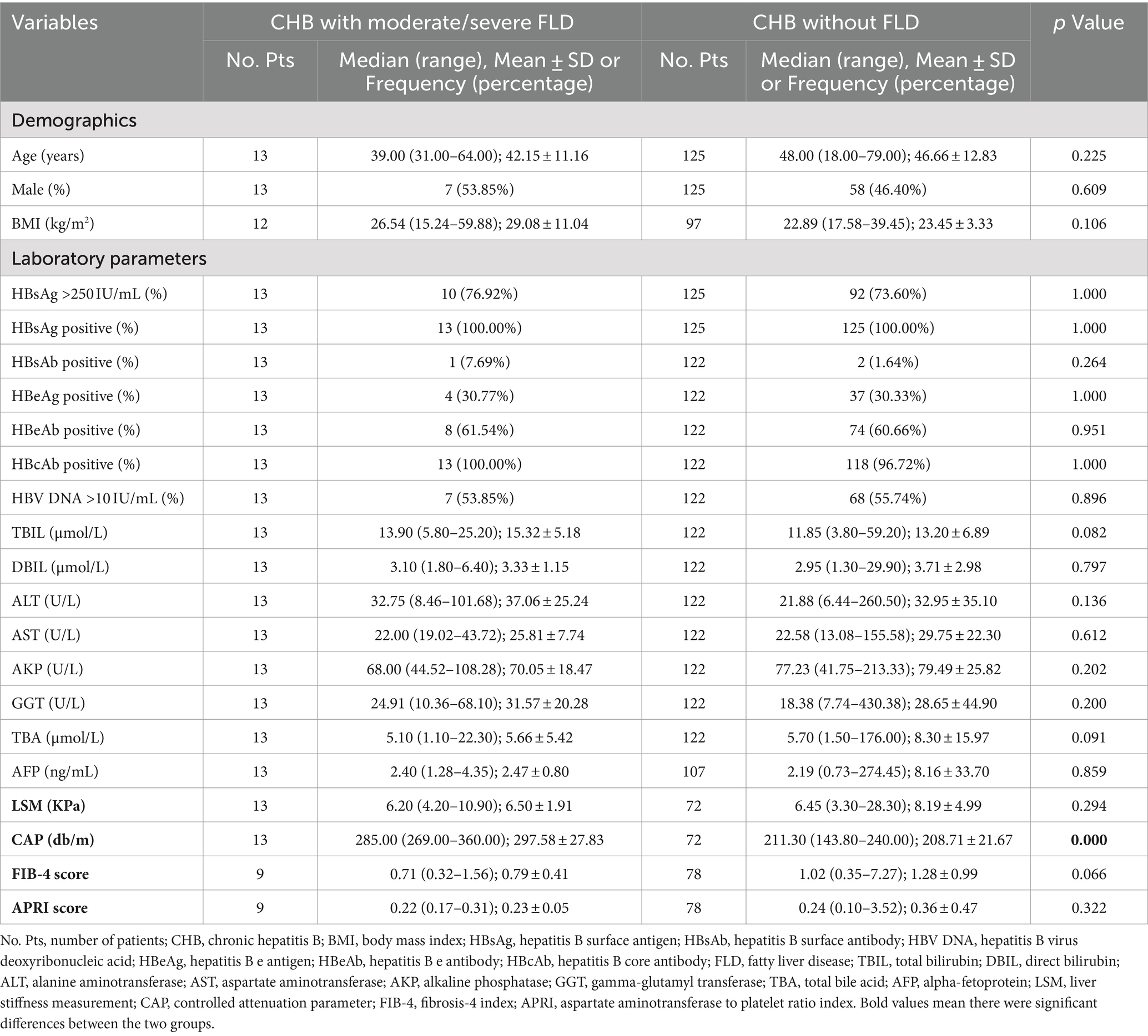
Table 6. Subgroup analyses of CHB patients with moderate/severe FLD versus without FLD.
4 Discussion
The first finding of our study should be that approximately 38% of CHB patients had FLD, which is close to the reported prevalence in three previous studies performed in China (36.5–41.8%), but a bit higher than the reported prevalence worldwide (34.9%) (13, 14, 21, 22). Despite so, a majority (35/48) of our patients who had measured CAP values had mild FLD, which is also consistent with previous studies (21, 22).
ALT, an enzyme mainly located in the cytoplasm of hepatocytes, is responsible for catalyzing the conversion of α-amino alanine to pyruvic acid (23). When liver tissue is damaged, ALT will leak into the systemic circulation from hepatocyte, causing an increase of ALT level in serum (23). Traditionally, ALT level is one of the important parameters for initiating antiviral therapy in HBsAg-positive patients (24, 25). It has been reported that increased ALT levels can be attributed to FLD in one fourth of the CHB patients (26). Our study also demonstrated that CHB patients with FLD had significantly higher ALT levels than those without, which was consistent with previous studies (15, 27, 28). Therefore, FLD might worsen liver damage in CHB patients.
Liver fibrosis, which refers to excessive accumulation of extracellular matrix proteins in the liver, is the consequence of chronic injury and inflammation of hepatocyte due to various pathogenic factors, such as HBV, hepatitis C virus, and other causes (29). As well known, liver biopsy is the gold standard for the assessment of liver fibrosis. However, it is often unacceptable due to its invasiveness and poor reproducibility (30). Thus, non-invasive methods for assessment of liver fibrosis have been frequently employed in clinical practice (31, 32). Several commonly used indicators have been recommended for the assessment of liver fibrosis by the European Association for the Study of the Liver (EASL) guidelines (33). Among them, LSM, FIB-4, and APRI are clinically significant markers for liver fibrosis among MAFLD patients (34–37). Our study demonstrated that the severity of liver fibrosis reflected by LSM, FIB-4, and APRI was not significantly influenced by the presence of FLD at both HBeAg-positive and HBeAb-positive stages, which was also supported by previous studies (38–41). This could be attributed to the fact that the majority of these patients from previous studies and ours had only mild FLD, which might hardly affect the development and progression of liver fibrosis (21, 22, 29).
The strength of our study is that all patients were treated by the same physician, potentially minimizing the heterogeneity in diagnosis and treatment selection among practitioners. However, our study also has some limitations. First, due to a relatively small sample size, the statistical results should be cautiously interpreted. Second, because our study population were outpatients and the nature of our study was retrospective, some information was not collected, such as history of alcohol abuse and metabolic variables (i.e., glucose, uric acid, and lipids). Thus, it was not possible to distinguish whether FLD was related to metabolic disorders in our patients. Third, due to the cross-sectional design of our study, the follow-up outcome was not evaluated.
5 Conclusion
FLD is common in CHB patients, and can intensify liver damage, particularly ALT level, but may not influence the progression of liver fibrosis. Large-scale cohort studies are imperative to further investigate the impact of FLD on virological markers and long-term outcome in CHB patients.
Data availability statement
The datasets presented in this article are not readily available because our data is not open to the public. Requests to access the datasets should be directed to Xingshun Qi, eGluZ3NodW5xaUAxMjYuY29t.
Ethics statement
The studies involving humans were approved by the Medical Ethical Committee of the General Hospital of Northern Theater Command. The studies were conducted in accordance with the local legislation and institutional requirements. The Ethics Committee/Institutional Review Board waived the requirement of written informed consent for participation from the participants or the participants’ legal guardians/next of kin because patients’ written informed consents were waived by the Medical Ethical Committee of our hospital due to the retrospective nature of this study.
Author contributions
XF: Writing – original draft, Validation, Methodology, Formal analysis, Data curation. YY: Writing – review & editing, Methodology, Formal analysis. HZ: Writing – review & editing, Methodology, Formal analysis, Data curation. CW: Writing – review & editing, Methodology, Formal analysis, Data curation. HL: Writing – review & editing, Data curation. YS: Writing – review & editing, Data curation. JL: Writing – review & editing, Methodology. YG: Writing – review & editing, Methodology, Formal analysis. NM-S: Writing – review & editing, Validation, Supervision, Methodology, Formal analysis. XQ: Writing – review & editing, Supervision, Methodology, Conceptualization.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The present study was partially supported by the National Key R&D Program of China (2023YFC2507500), Outstanding Youth Foundation of Liaoning Province (2022-YQ-07), and Science and Technology Plan Project of Liaoning Province (2022JH2/101500032).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Collaborators, GHB. Global, regional, and national burden of hepatitis B, 1990-2019: a systematic analysis for the global burden of disease study 2019. Lancet Gastroenterol Hepatol. (2022) 7:796–829. doi: 10.1016/S2468-1253(22)00124-8
2. Bera, C, Hamdan-Perez, N, and Patel, K. Non-invasive assessment of liver fibrosis in hepatitis B patients. J Clin Med. (2024) 13:1046. doi: 10.3390/jcm13041046
3. Ganem, D, and Prince, AM. Hepatitis B virus infection — natural history and clinical consequences. N Engl J Med. (2004) 350:1118–29. doi: 10.1056/NEJMra031087
4. Broquetas, T, and Carrión, JA. Past, present, and future of long-term treatment for hepatitis B virus. World J Gastroenterol. (2023) 29:3964–83. doi: 10.3748/wjg.v29.i25.3964
5. Committee of Hepatology CRHA, Fatty Liver Expert Committee, Chinese Medical Doctor Association, National Workshop on Fatty Liver and Alcoholic Liver Disease, Chinese Society of Hepatology; National Workshop on Liver and Metabolism, Chinese Society of Endocrinology, Chinese Medical Association. Expert recommendations on standardized diagnosis and treatment for fatty liver disease in China (2019 revised edition). Zhonghua Gan Zang Bing Za Zhi. (2019) 27:748–53. doi: 10.3760/cma.j.issn.1007-3418.2019.10.003
6. Testino, G, and Pellicano, R. Corrected and republished from: metabolic associated liver disease. Panminerva Med. (2023) 65:391–9. doi: 10.23736/S0031-0808.23.04850-4
7. Wang, C, Kanaan, G, Shang, Y, Chai, L, Li, H, and Qi, X. Silymarin for treatment of adults with nonalcoholic fatty liver disease. Cochrane Database Syst Rev. (2023) 2023:CD015524. doi: 10.1002/14651858.CD015524
8. Eslam, M, Newsome, PN, Sarin, SK, Anstee, QM, Targher, G, Romero-Gomez, M, et al. A new definition for metabolic dysfunction-associated fatty liver disease: an international expert consensus statement. J Hepatol. (2020) 73:202–9. doi: 10.1016/j.jhep.2020.03.039
9. Méndez-Sánchez, N, Bugianesi, E, Gish, RG, Lammert, F, Tilg, H, Nguyen, MH, et al. Global multi-stakeholder endorsement of the MAFLD definition. Lancet Gastroenterol Hepatol. (2022) 7:388–90. doi: 10.1016/S2468-1253(22)00062-0
10. Xie, ZQ, Li, HX, Wang, BK, Yang, ZM, Zhang, ZY, Tan, WL, et al. Trends in prevalence and all-cause mortality of metabolic dysfunction-associated fatty liver disease among adults in the past three decades: results from the NHANES study. Eur J Intern Med. (2023) 110:62–70. doi: 10.1016/j.ejim.2023.01.029
11. Rinella, ME, Neuschwander-Tetri, BA, Siddiqui, MS, Abdelmalek, MF, Caldwell, S, Barb, D, et al. AASLD practice guidance on the clinical assessment and management of nonalcoholic fatty liver disease. Hepatology. (2023) 77:1797–835. doi: 10.1097/HEP.0000000000000323
12. Ng, CH, Lim, WH, Hui Lim, GE, Hao Tan, DJ, Syn, N, Muthiah, MD, et al. Mortality outcomes by fibrosis stage in nonalcoholic fatty liver disease: a systematic review and Meta-analysis. Clin Gastroenterol Hepatol. (2023) 21:931–9.e5. doi: 10.1016/j.cgh.2022.04.014
13. Zhou, R, Yang, L, Zhang, B, Gu, Y, Kong, T, Zhang, W, et al. Clinical impact of hepatic steatosis on chronic hepatitis B patients in Asia: a systematic review and meta-analysis. J Viral Hepat. (2023) 30:793–802. doi: 10.1111/jvh.13872
14. Jiang, D, Chen, C, Liu, X, Huang, C, Yan, D, Zhang, X, et al. Concurrence and impact of hepatic steatosis on chronic hepatitis B patients: a systematic review and meta-analysis. Ann Transl Med. (2021) 9:1718. doi: 10.21037/atm-21-3052
15. Choi, HSJ, Brouwer, WP, Zanjir, WMR, de Man, RA, Feld, JJ, Hansen, BE, et al. Nonalcoholic steatohepatitis is associated with liver-related outcomes and all-cause mortality in chronic hepatitis B. Hepatology. (2020) 71:539–48. doi: 10.1002/hep.30857
16. Chan, AW, Wong, GL, Chan, HY, Tong, JH, Yu, YH, Choi, PC, et al. Concurrent fatty liver increases risk of hepatocellular carcinoma among patients with chronic hepatitis B. J Gastroenterol Hepatol. (2017) 32:667–76. doi: 10.1111/jgh.13536
17. Zhang, M, Chen, S, Wu, X, Zhou, J, Wang, T, Liu, H, et al. Persistent steatosis correlates with decreased fibrosis regression during anti-HBV treatment in patients with chronic HBV infection. J Med Virol. (2023) 95:e29156. doi: 10.1002/jmv.29156
18. Yi, S, Ren, G, Zhu, Y, and Cong, Q. Correlation analysis of hepatic steatosis and hepatitis B virus: a cross-sectional study. Virol J. (2024) 21:22. doi: 10.1186/s12985-023-02277-8
19. Dietrich, CF, Bamber, J, Berzigotti, A, Bota, S, Cantisani, V, Castera, L, et al. EFSUMB guidelines and recommendations on the clinical use of liver ultrasound Elastography, update 2017 (long version). Ultraschall in der Medizin. (2017) 38:e48. doi: 10.1055/a-0641-0076
20. Chinese Society of Hepatology CMA, Chinese Society of Infectious Diseases, Chinese Medical Association. Guidelines for the prevention and treatment of chronic hepatitis B (version 2022). Zhonghua Gan Zang Bing Za Zhi. (2022) 30:1309–31. doi: 10.3760/cma.j.cn501113-20221204-00607
21. Mi, YQ, Shi, QY, Xu, L, Shi, RF, Liu, YG, Li, P, et al. Controlled attenuation parameter for noninvasive assessment of hepatic steatosis using Fibroscan®: validation in chronic hepatitis B. Dig Dis Sci. (2015) 60:243–51. doi: 10.1007/s10620-014-3341-x
22. Kang, NL, Zhang, JM, Liu, YR, Lin, S, Dong, J, Jiang, JJ, et al. Novel predictive models using serum ceruloplasmin levels for hepatic steatosis in patients with chronic hepatitis B infection. Clin Res Hepatol Gastroenterol. (2020) 44:57–65. doi: 10.1016/j.clinre.2019.04.001
23. Nguyen, LH, Chao, D, Lim, JK, Ayoub, W, and Nguyen, MH. Histologic changes in liver tissue from patients with chronic hepatitis B and minimal increases in levels of alanine aminotransferase: a meta-analysis and systematic review. Clin Gastroenterol Hepatol. (2014) 12:1262–6. doi: 10.1016/j.cgh.2013.11.038
24. Terrault, NA, Lok, ASF, McMahon, BJ, Chang, KM, Hwang, JP, Jonas, MM, et al. Update on prevention, diagnosis, and treatment of chronic hepatitis B: AASLD 2018 hepatitis B guidance. Hepatology. (2018) 67:1560–99. doi: 10.1002/hep.29800
25. Liver EAftSot. EASL 2017 clinical practice guidelines on the management of hepatitis B virus infection. J Hepatol. (2017) 67:370–98. doi: 10.1016/j.jhep.2017.03.021
26. Spradling, PR, Bulkow, L, Teshale, EH, Negus, S, Homan, C, Simons, B, et al. Prevalence and causes of elevated serum aminotransferase levels in a population-based cohort of persons with chronic hepatitis B virus infection. J Hepatol. (2014) 61:785–91. doi: 10.1016/j.jhep.2014.05.045
27. Prati, D, Taioli, E, Zanella, A, Della Torre, E, Butelli, S, Del Vecchio, E, et al. Updated definitions of healthy ranges for serum alanine aminotransferase levels. Ann Intern Med. (2002) 137:1–10. doi: 10.7326/0003-4819-137-1-200207020-00006
28. Hui, RWH, Seto, WK, Cheung, KS, Mak, LY, Liu, KSH, Fung, J, et al. Inverse relationship between hepatic steatosis and hepatitis B viremia: results of a large case-control study. J Viral Hepat. (2018) 25:97–104. doi: 10.1111/jvh.12766
29. Hammerich, L, and Tacke, F. Hepatic inflammatory responses in liver fibrosis. Nat Rev Gastroenterol Hepatol. (2023) 20:633–46. doi: 10.1038/s41575-023-00807-x
30. Sanyal, AJ, Castera, L, and Wong, VW. Noninvasive assessment of liver fibrosis in NAFLD. Clin Gastroenterol Hepatol. (2023) 21:2026–39. doi: 10.1016/j.cgh.2023.03.042
31. Ooi, GJ, Mgaieth, S, Eslick, GD, Burton, PR, Kemp, WW, Roberts, SK, et al. Systematic review and meta-analysis: non-invasive detection of non-alcoholic fatty liver disease related fibrosis in the obese. Obes Rev. (2018) 19:281–94. doi: 10.1111/obr.12628
32. Dulai, PS, Singh, S, Patel, J, Soni, M, Prokop, LJ, Younossi, Z, et al. Increased risk of mortality by fibrosis stage in nonalcoholic fatty liver disease: systematic review and meta-analysis. Hepatology. (2017) 65:1557–65. doi: 10.1002/hep.29085
33. Archer, AJ, Belfield, KJ, Orr, JG, Gordon, FH, and Abeysekera, KW. EASL clinical practice guidelines: non-invasive liver tests for evaluation of liver disease severity and prognosis. Front Gastroenterol. (2022) 13:436–9. doi: 10.1136/flgastro-2021-102064
34. Ciardullo, S, Muraca, E, Zerbini, F, and Perseghin, G. Liver stiffness is associated with all-cause mortality in patients with NAFLD: a systematic review and meta-analysis. Liver Int. (2023) 43:2604–10. doi: 10.1111/liv.15742
35. Yoshioka, K, Hashimoto, S, and Kawabe, N. Measurement of liver stiffness as a non-invasive method for diagnosis of non-alcoholic fatty liver disease. Hepatol Res. (2015) 45:142–51. doi: 10.1111/hepr.12388
36. Han, S, Choi, M, Lee, B, Lee, HW, Kang, SH, Cho, Y, et al. Accuracy of noninvasive scoring Systems in Assessing Liver Fibrosis in patients with nonalcoholic fatty liver disease: a systematic review and Meta-analysis. Gut Liver. (2022) 16:952–63. doi: 10.5009/gnl210391
37. Ismaiel, A, Leucuta, DC, Popa, SL, Fagoonee, S, Pellicano, R, Abenavoli, L, et al. Noninvasive biomarkers in predicting nonalcoholic steatohepatitis and assessing liver fibrosis: systematic review and meta-analysis. Panminerva Med. (2021) 63:508–18. doi: 10.23736/S0031-0808.20.04171-3
38. Yun, JW, Cho, YK, Park, JH, Kim, HJ, Park, DI, Sohn, CI, et al. Hepatic steatosis and fibrosis in young men with treatment-naïve chronic hepatitis B. Liver Int. (2009) 29:878–83. doi: 10.1111/j.1478-3231.2009.01976.x
39. Yilmaz, B, Koklu, S, Buyukbayram, H, Yalçin, K, Korkmaz, U, Posul, E, et al. Chronic hepatitis B associated with hepatic steatosis, insulin resistance, necroinflammation and fibrosis. Afr Health Sci. (2015) 15:714–8. doi: 10.4314/ahs.v15i3.3
40. Zheng, RD, Xu, CR, Jiang, L, Dou, AX, Zhou, K, and Lu, LG. Predictors of hepatic steatosis in HBeAg-negative chronic hepatitis B patients and their diagnostic values in hepatic fibrosis. Int J Med Sci. (2010) 7:272–7. doi: 10.7150/ijms.7.272
41. Huang, Y, Gan, Q, Lai, R, Wang, W, Guo, S, Sheng, Z, et al. Application of fatty liver inhibition of progression algorithm and steatosis, activity, and fibrosis score to assess the impact of non-alcoholic fatty liver on untreated chronic hepatitis B patients. Front Cell Infect Microbiol. (2021) 11:733348. doi: 10.3389/fcimb.2021.733348
Keywords: fatty liver disease, chronic hepatitis B, fibrosis, effect, prevalence
Citation: Fang X, Yin Y, Zhao H, Wang C, Li H, Shang Y, Li J, Gao Y, Méndez-Sánchez N and Qi X (2024) Effect of fatty liver disease on liver function and fibrosis in patients with chronic hepatitis B: a cross-sectional study. Front. Med. 11:1481051. doi: 10.3389/fmed.2024.1481051
Edited by:
Krzysztof Tomasiewicz, Medical University of Lublin, Poland, PolandReviewed by:
Dong Ji, Peking University, ChinaDorota Dybowska, Nicolaus Copernicus University in Toruń, Poland
Copyright © 2024 Fang, Yin, Zhao, Wang, Li, Shang, Li, Gao, Méndez-Sánchez and Qi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xingshun Qi, eGluZ3NodW5xaUAxMjYuY29t; Nahum Méndez-Sánchez, bm1lbmRlekBtZWRpY2FzdXIub3JnLm14
†These authors have contributed equally to this work