 Thomas Thibault1,2
Thomas Thibault1,2 Jean-Louis Alberini3,4Anne-Claire Billet5Hélène Greigert6,7,8
Jean-Louis Alberini3,4Anne-Claire Billet5Hélène Greigert6,7,8 André Ramon8,9Hervé Devilliers1,2Alexandre Cochet3,4
André Ramon8,9Hervé Devilliers1,2Alexandre Cochet3,4 Bernard Bonnotte6,8
Bernard Bonnotte6,8 Maxime Samson6,8*
Maxime Samson6,8*- 1Department of Internal Medicine and Systemic Disease, Dijon University Hospital, Dijon, France
- 2CHU Dijon Bourgogne, INSERM, Université de Bourgogne, CIC 1432, Module Épidémiologie Clinique, Dijon, France
- 3Centre Georges Francois Leclerc, Service de Médecine Nucléaire, Dijon, France
- 4Institut de Chimie Moléculaire de l’Université de Bourgogne, ICMUB UMR CNRS 6302, Université de Bourgogne, Dijon, France
- 5Department of Internal Medicine, Hôpital Edouard Herriot, Hospices Civils de Lyon, Lyon, France
- 6Department of Internal Medicine and Clinical Immunology, Dijon-Burgundy University Hospital, Dijon, France
- 7Department of Vascular Medicine, Dijon University Hospital, Dijon, France
- 8INSERM, EFS BFC, UMR1098, RIGHT Interactions Greffon-Hôte-Tumeur/Ingénierie Cellulaire et Génique, Université Bourgogne Franche-Comté, Dijon, France
- 9Department of Rheumatology, Dijon University Hospital, Dijon, France
PET/CT is an imaging modality that is increasingly being used to diagnose large-vessel vasculitis. In the case of giant cell arteritis, it was first used to demonstrate inflammation of the walls of large arterial trunks such as the aorta and its main branches, showing that aortic involvement is common in this vasculitis and associated with the occurrence of aortic complications such as aneurysms. More recently, with the advent of digital PET/CT, study of the cranial arteries (i.e., temporal, occipital, maxillary and vertebral arteries) has become possible, further increasing the diagnostic interest of this examination for the diagnosis of GCA. Despite these advantages, there are still limitations and questions regarding the use of PET/CT for the diagnosis and especially the follow-up of GCA. The aim of this review is to take stock of currently available data on the use of PET/CT for GCA diagnosis and follow-up.
Introduction
Giant cell arteritis (GCA) is a large-vessel vasculitis (LVV) affecting people over the age of fifty (1, 2) and especially targets the aorta and branches of the external carotid arteries. The disease can cause vascular complications, particularly vision loss or stroke at diagnosis (3, 4), or aortic aneurysm in long-term follow-up (5).
GCA diagnosis is based on the combination of clinical signs of GCA with an increase in acute phase reactants (CRP, ESR) and evidence of vasculitis. Historically, temporal artery biopsy (TAB) was the gold standard to demonstrate granulomatous vasculitis (6). However, this examination is invasive (7) and lacks sensitivity (8), which led to vascular imaging’s growing role in confirming the diagnosis of GCA. Ultrasonography has been recommended by EULAR for several years as a first-line test to assess the temporal arteries in suspected GCA (9). This is also supported by the most recent EULAR guidelines, which state that ultrasonography of the temporal and axillary arteries is the first-line imaging test to be performed in this context (10). However, GCA does not always affect temporal arteries and sometimes targets large vessels, especially the aorta and its main branches, often in the upper limbs (11), and these areas are not readily accessible by ultrasound.
Along this line, 18F-fluorodeoxyglucose positron emission tomography/computed tomography (PET/CT) has emerged as a very sensitive examination to detect LVV in GCA patients. More recently, newer generations of PET/CT have shown their good performance in demonstrating vasculitis of cranial arteries, including the temporal, occipital and maxillary arteries, allowing a more comprehensive assessment of vascular involvement (12–15), and are recognized in the new EULAR recommendations on imaging’s use in GCA (15) (Figure 1).
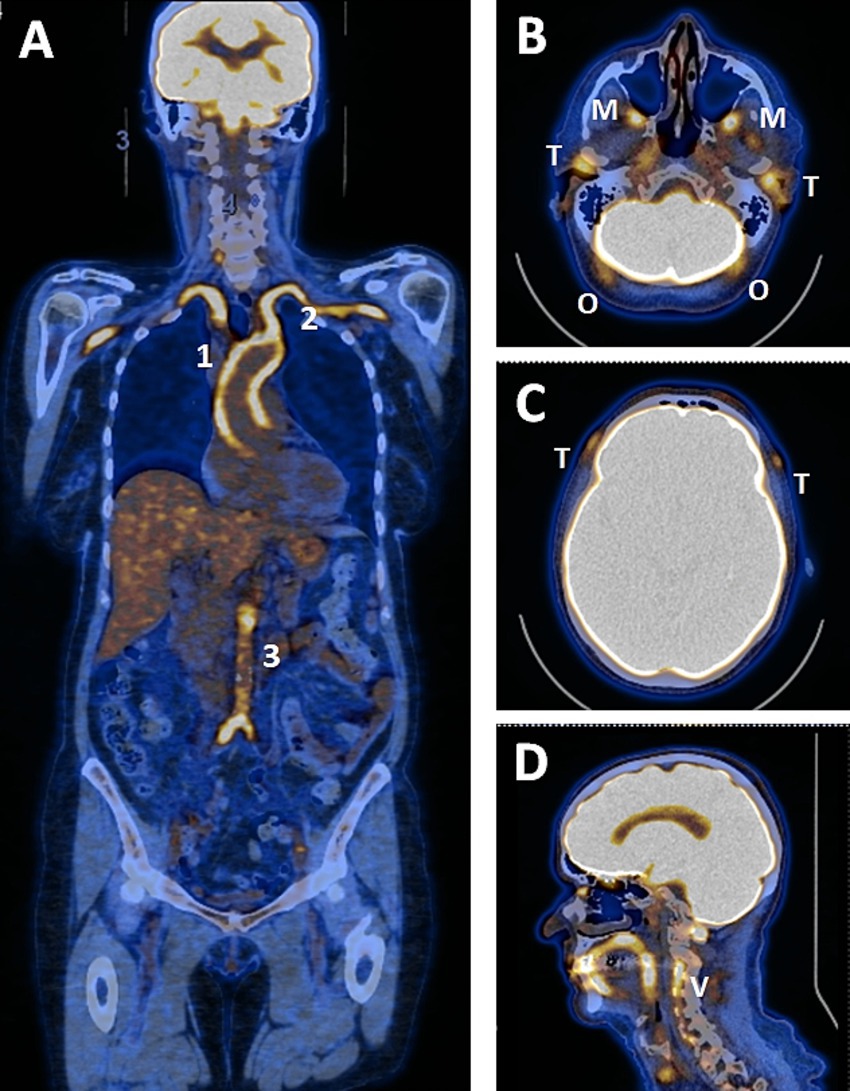
Figure 1. PET/CT study of a patient with GCA involving cephalic and large arteries. (A) study of large arteries showing grade 3 hypermetabolism of the ascending aorta (1), subclavian and axillary arteries (2) and from the abdominal aorta to the origin of the iliac arteries (3). (B–D) study of cephalic arteries showing significant hypermetabolism of the temporal (T), maxillary (M), occipital (O) and vertebral (V) arteries. (C) hypermetabolism of the frontal branch of the temporal artery (T).
PET/CT is now widely used for GCA diagnosis, but there are still limitations to its application and interpretation. Indeed, PET/CT is highly sensitive to glucocorticoids and should therefore be performed before or as soon as possible after the start of treatment. A previous study showed that the hypermetabolic signal in large arteries decreased significantly after 72 h of treatment, meaning that this limit is often used as a quality criterion for PET/CT (16). However, it has been clearly demonstrated that arterial hypermetabolism can persist for many months after treatment begins, so this rule is not absolute.
PET/CT was first used to detect LVV but has since expanded beyond that setting and been evaluated in different contexts. Therefore, in addition to the diagnosis of GCA, PET/CT has been used for disease monitoring.
This report aims to provide an update on the performance of PET/CT in the diagnosis and monitoring of GCA.
Generalities about PET/CT
The latest EULAR guidelines indicate that, in cases of high clinical suspicion and positive imaging, the diagnosis of GCA can be confirmed without additional tests, including TAB. The first-line imaging test to achieve this goal is ultrasonography of the temporal and axillary arteries. Furthermore, PET/CT remains the test of choice for evidencing LVV in extracranial arteries (aorta and proximal branches). PET/CT and MRI are also becoming an alternative to ultrasonography for the study of cranial arteries (10).
Protocol procedure
With the aim of standardising procedures and optimising diagnostic accuracy, the recommendations reiterate good practice with regard to the protocol for performing PET/CT, including the acquisition of cranial artery imaging (Table 1) (15).
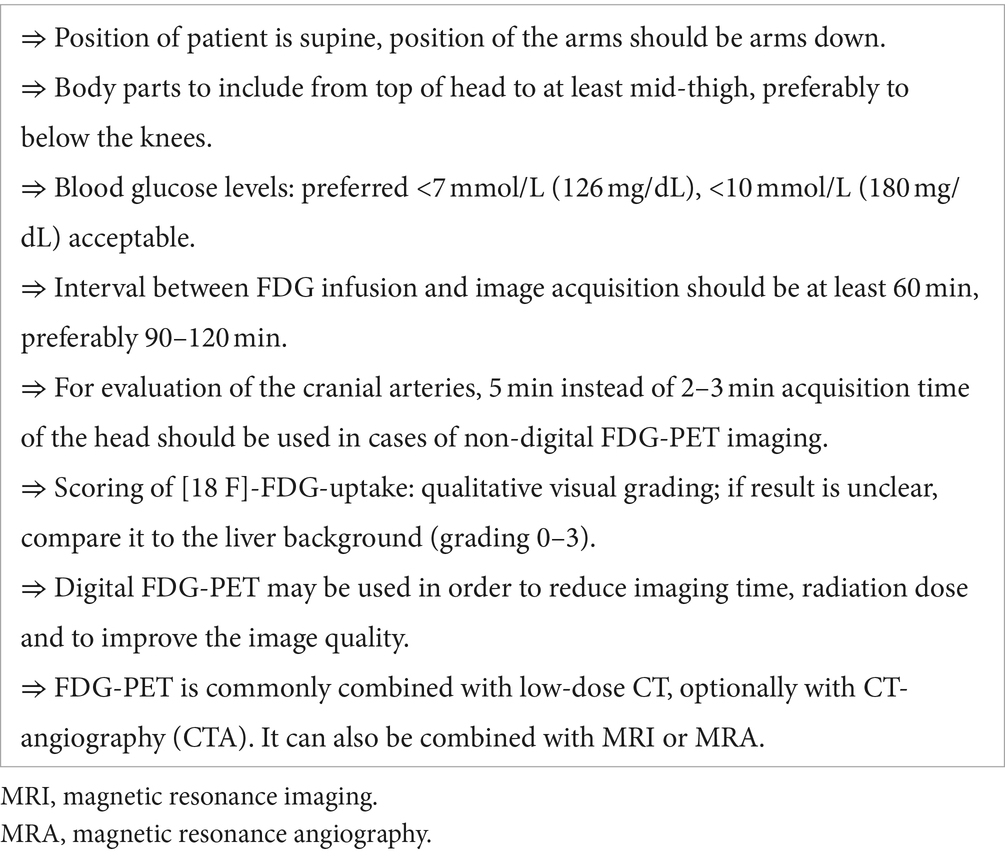
Table 1. Imaging modalities for PET/CT in LVV, according to EULAR recommendations (15).
In particular, it is specified that the time between FDG infusion and image acquisition should be at least 60 min. Most studies on PET/CT in LVV have been conducted in these conditions. Delayed imaging at 3 h may provide a more detailed image of the arterial wall, mainly due to decreased blood pool activity, according to only one small prospective study of 23 patients with suspected LVV (17). However, there is little evidence to support a possible extension of this timeframe, in contrast to the recommended delay of 2 h for assessing the metabolic activity of atherosclerosis (18). Therefore, further studies extending the time between FDG infusion and imaging are needed to determine whether performance can be optimized in the diagnosis of GCA and LVV in general.
Before PET/CT, blood glucose levels should be closely monitored, especially in diabetic patients and after the introduction of glucocorticoids, as FDG uptake is reduced when serum glucose levels exceed 7 mmol/L (126 mg/dL) (19, 20).
According to Nielsen et al., diagnostic accuracy is not significantly affected when PET/CT is performed 3 days after the start of GC therapy, whereas it is significantly reduced when PET/CT is performed 10 days later (21). Therefore, PET/CT should be performed before or within this three-day period after starting GC to ensure good performance (16). The availability of PET/CT is one of the main limitations to its use in clinical practice, as it is often inappropriate to wait for a suspected GCA diagnosis before initiating glucocorticoid therapy due to the risk of ocular complications (16).
PET/CT interpretation
There are several interpretation methods for assessing vascular hypermetabolism: the qualitative method, visual grading and semi-quantitative methods (19):
• The global qualitative method is still preferred in daily clinical practice due to the speed with which it can be initiated, as it is based on the clinician’s experience and overall visual assessment. PET/CT is defined as negative or positive according to the presence or absence of evidence of active LVV. However, particularly in the context of clinical research, standardization of interpretation and intra- and inter-observer reliability are not guaranteed with this approach.
• Qualitative visual grading is recommended in clinical practice when the result of the global qualitative method is unclear. Visual grading is based on comparing the intensity of vascular FDG uptake in each vascular segment with the background uptake in the liver. The resulting score ranges from 0 to 3: 0 = no FDG uptake (lower than the mediastinal blood pool); 1 = low-grade uptake (< liver uptake); 2 = intermediate-grade uptake (similar to liver uptake), 3 = high-grade uptake (> liver uptake). This score should be interpreted with caution due to frequent false positives related to atherosclerotic vascular uptake, particularly in the iliac and femoral arteries. According to guidelines, a score of 3 should be considered positive for active LVV and a score of 2 indicative of possible LVV (20). Lower scores are considered as negative for LVV. It should be noted that most PET/CT studies (extracranial and cranial PET/CT) use a visual grading of ≥2 to define PET/CT as positive.
• Semi-quantitative methods consist of directly measuring the SUVmax of vascular FDG uptake in each vascular segment. The target is defined by drawing a manually delineated volume of interest (VOI) that includes each vascular segment and avoids areas of atherosclerosis. Target-to-liver and target-to-blood pool ratios are calculated by dividing the SUVmax by liver or superior vena cava background, respectively. These ratios were proposed because the simple SUV metric does not seem relevant for initial diagnosis due to the high overlap between patients and controls (22), and the potential loss of specificity (23).
Scores
Scores can be calculated by adding each vessel’s visual grading (from 0 to 3 points). Two scores are mainly used: TVS (Total Vascular Score) and PETVAS (PET Vascular Activity Score). TVS is defined by the addition of the Meller score (24), which is composed of 14 arterial territories ranging from 0 to 42 points, including the carotid arteries [n = 2], subclavian arteries [n = 2], axillary arteries [n = 2], ascending thoracic aorta [n = 1], aortic arch [n = 1], descending thoracic aorta [n = 1], abdominal aorta [n = 1], and the iliac arteries [n = 2] and femoral arteries [n = 2] (23). PETVAS includes 9 arterial territories, ranging from 0 to 27 points, including the ascending thoracic aorta [n = 1], aortic arch [n = 1], descending thoracic aorta [n = 1], abdominal aorta [n = 1], brachiocephalic trunk [n = 1], carotid arteries [n = 2] and subclavian arteries [n = 2] (25). Unlike TVS, PETVAS does not include the arteries of the lower limbs, where atheroma can interfere with interpretation of the uptake (24). The scores’ value is well correlated with vasculitis activity. Therefore, TVS and PETVAS are higher at GCA diagnosis than in treated GCA (26, 27). In addition, PETVAS is able to discriminate clinically active from inactive LVV with a sensitivity of 60% and specificity of 80% for a threshold of ≥10 points (28).
Dashora et al. (29) compared PETVAS with SUV semiquantitative metrics in 52 GCA and 43 Takayasu’s arteritis patients. Intra-rater reliability showed a better intraclass correlation (ICC) for the semiquantitative method [0.99 (range 0.98–1.00)] than for the visual grading by PETVAS [0.82 (range 0.56–0.93)]. When compared to physician assessment of clinical disease activity, the target-to-liver ratio had the highest area under the receiver operating characteristic curve (AUROC). The authors suggested that visual grading (such as PETVAS or TVS) should be used in clinical practice or observational studies when ease of interpretation is preferred, and SUV metrics should be used in randomized clinical trials or translational research when precision is mandatory.
Diagnostic accuracy
Guidelines have specified that PET/CT can be used to detect mural inflammation or luminal changes affecting extracranial arteries in patients with suspected GCA (28).
Evaluating the diagnostic accuracy of PET/CT in GCA is challenging because no other available test, especially TAB, is a perfect gold standard due to lack of sensitivity (30). In some patients, only PET/CT can confirm the diagnosed GCA by showing high vascular uptake in cranial or extracranial arteries. To avoid this difficulty, recent studies have used a reference clinical diagnosis as a gold standard, i.e., a diagnosis maintained by the treating physician after 6 months of follow-up with no alternative found. These studies are compiled in the systematic review and metanalysis by Bosch et al. (31). Four studies with a low risk of bias (12, 15, 32, 33) which evaluated the diagnostic accuracy of PET/CT in suspected GCA compared with the reference clinical diagnosis were included. The four studies’ pooled results support high diagnostic accuracy (sensitivity 76% and specificity 95%). It should be noted that some of the studies include vascular FDG uptake in the cranial arteries to consider a positive PET/CT.
After evaluation of the diagnostic accuracy of PET/CT, there is a need for comparison of PET/CT with other imaging tests, particularly ultrasound of the temporal and axillary arteries. However, data about direct comparison between these two tests are lacking. Most published studies have included patients who had PET/CT or temporal ultrasound as the gold standard test (33–35). Therefore, the two tests cannot be compared. Other published trials evaluated the diagnostic accuracy of PET/CT and ultrasound using the clinical diagnosis confirmed after 6 months of follow-up as the gold standard. Unfortunately, at least one test was not performed in the whole population, which makes it difficult to draw firm conclusions in these studies (36, 37). Moreel et al. (38) published a systematic review and meta-analysis in 2023 with the aim of comparing PET/CT, ultrasound and MRI for the diagnosis of GCA. Eleven studies (including 1,578 patients) and three studies (including 149 patients) were included to evaluate ultrasound and PET/CT, respectively. The results showed a sensitivity of 86% (76–92%) and a specificity of 96% (92–98%) for cranial and large vessel ultrasound, and a sensitivity of 82% (61–93%) and a specificity of 79% (60–90%) for cranial and extracranial PET/CT. However, at the time of the meta-analysis, the authors could not identify any studies that assessed both PET/CT and ultrasound, which prevent head-to-head comparison. More recently, van Nieuwland et al. (39) included patients with suspected GCA in a nested case–control pilot study. Ultrasound, cranial and extracranial FDG-PET/CT, and cranial MRI were performed within 5 days of the initial clinical evaluation, and clinical diagnosis after 6 months of follow-up was used as gold standard. A total of 23 patients with GCA and 19 patients with suspected but undiagnosed GCA were included. The sensitivity was 69.6% (95%CI 50.4–88.8%) for ultrasound, 52.2% (95%CI 31.4–73.0%) for PET/CT and 56.5% (95%CI 35.8–77.2%) for MRI. The specificity was 100% for CDUS, FDG-PET/CT and MRI.
Another advantage of PET/CT is the ability to detect other diagnoses of interest. Firstly, PET/CT could detect neoplasms or infections that may mimic GCA. Secondly, polymyalgia rheumatica (PMR), a rheumatic disease that is often associated with GCA, can be confirmed or excluded by PET/CT. In PMR, PET/CT shows high FDG uptake in the scapula and pelvic girdles, and also in the lumbar and cervical interspinous bursae. Thirdly, PET/CT could aid the differential diagnosis of inflammatory rheumatic diseases occurring in the same age group, such as elderly-onset rheumatoid arthritis (EORA), spondyloarthropathies, crystal-induced arthropathies or remitting seronegative symmetrical synovitis with pitting oedema (RS3PE), by showing typical patterns of each disease (40).
Finally, in the case of large-vessel GCA (LV-GCA), a specific subset of GCA usually revealed by nonspecific symptoms (fatigue, fever, weight loss) and in the absence of typical signs of cranial GCA, PET/CT may be the only test that can diagnose GCA by showing vascular FDG uptake in the aorta and its main branches (39, 40).
Prognostic accuracy
FDG uptake evolution during follow-up
Some studies have focused on the evolution of vascular FDG uptake on therapy (mainly with glucocorticoids) by performing repeated PET/CT during follow-up. These studies showed that vascular FDG uptake decreases significantly, especially after 8 months of follow-up (41, 42), and this metabolic regression generally correlates with clinical and biological improvement (24, 43). However, other studies have observed persistent vascular uptake in patients in clinical and biological remission, defined by the absence of clinical signs and normal C-reactive protein (CRP) and/or erythrocyte sedimentation rate (ESR) (44). For example, about 80% of GCA patients who are in remission still have significant vascular uptake on PET-CT (45). In addition, Prieto-Pena et al. (46) reported a significant reduction in vascular FDG uptake in 30 LV-GCA patients followed for 10.8 ± 3.7 months, but less than one third achieved complete normalization of vascular uptake. Some authors have hypothesized that the persistence of low-grade vascular uptake may reflect smouldering inflammation or post-inflammatory vascular remodeling (45). Moreover, thoracic aortic histopathology from aortic surgery revealed active aortitis in most GCA patients despite clinical remission several years after GCA diagnosis, lending credence to the hypothesis of smouldering vasculitis persisting in patients in clinical and biological remission (47). Therefore, the value of follow-up PET/CT to predict the risk of relapse or the occurrence of aortic complication is questionable.
PET/CT for predicting relapse
Some studies have focused on the risk of subsequent relapse in relation to persistent FDG uptake on repeat PET/CT (Table 2). Only the study by Grayson et al. (46) suggests that the value of PETVAS can be used to predict the risk of relapse during follow-up. In this study, the authors prospectively analysed patients with Takayasu’s arteritis (n = 26) and GCA (n = 30) who underwent serial PET/CT every 6 months. A total of 170 PET/CT from 56 patients with LV-GCA were analysed. PETVAS ≥20 during follow-up was associated with an increased risk of recurrence compared to patients with PETVAS <20 (55% vs. 11% of relapse, p = 0.003). Interpreting the study may be challenging. Firstly, patients with GCA and Takayasu’s arteritis were included. Secondly, the 30 patients with GCA were enrolled 2.6 +/− 2.7 years after diagnosis. Therefore, the patients included may have been more refractory than usual patients and at higher risk of relapse. This may explain why some of them had a PETVAS ≥20 points during follow-up, which is particularly high.
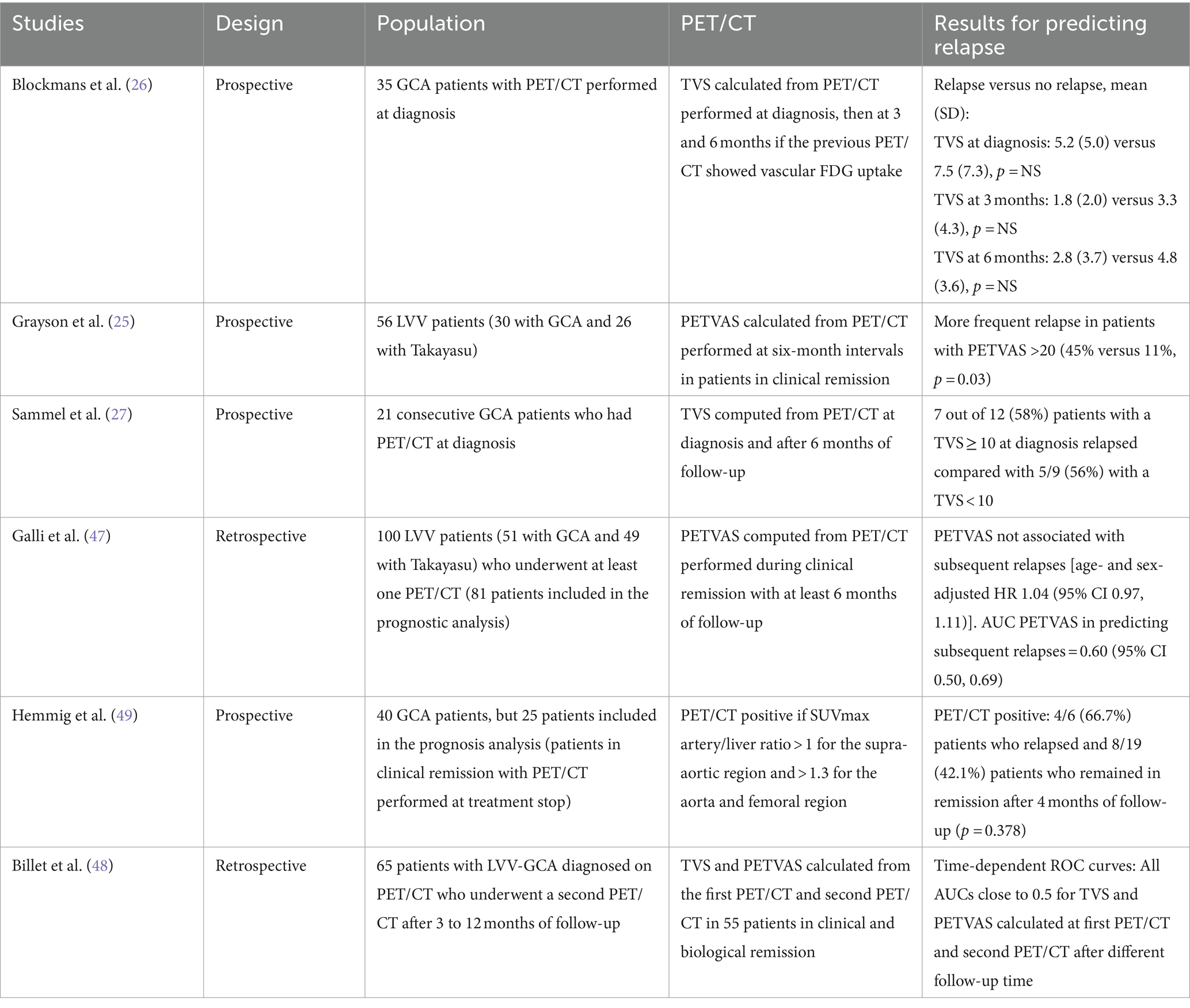
Table 2. Summary of studies assessing the prognostic value of PET/CT for subsequent relapse.
Billet et al. (48) included 55 patients with LV-GCA who underwent 2 PET/CT during the course of the disease (the first at diagnosis and the second 3–12 months later) and who were in clinical and biological remission at the time of the second PET/CT. Only 4/55 (7%) patients had a PETVAS >20 at the time of the second PET/CT. All AUROCs calculated from the time-dependent ROC curves up to 2 years after the second PET/CT were close to 0.5 for both scores (TVS and PETVAS), which means poor discriminatory power to predict relapse. However, this study also has several limitations. Firstly, patients were recruited between 2009 and 2020 in different centres with different PET/CT techniques and resolutions. Therefore, the study’s retrospective nature precluded systematic, centralized double-reading of all PET/CT images. Finally, the clinician prescribing the second PET/CT was aware of the imaging results, which may have influenced subsequent treatment decisions and relapse risk.
The study by Hemmig et al. (49) aimed to investigate the value of PET/CT and MRI in predicting relapse after stopping treatment in patients with LV-GCA (25 patients underwent PET/CT and 15 underwent MRI). A relapse occurred in 11/40 patients (27.5%) after 4 months of follow-up (time to relapse 1.9 months, IQR 1.4–3.3). Patients experiencing a relapse had no more active vasculitis on MRI and/or PET/CT (54.5% versus 58.6%, p = 1.0). These results are consistent with other studies detailed in Table 2, which often included patients with GCA and Takayasu’s arteritis and calculated TVS (26, 27), PETVAS or both (41).
In summary, PET/CT does not appear to predict relapse and may not be suitable for guiding treatment decisions in patients with LV-GCA in clinical remission.
PET/CT for predicting vascular complications
Large-vessel involvement is known to be associated with an increased risk of vascular complications, particularly aortic dilatation in GCA (43). Therefore, the guidelines specify the need to monitor for structural damage, particularly at sites of previous vascular inflammation (48). This recommendation is supported by several studies.
First, the one of Quinn et al., who reported that in 32 GCA and 28 TAK patients, 80% of vascular territories with significant FDG uptake at baseline developed stenosis or aneurysms during follow-up (50). Then Blockmans et al. (51) also showed in 46 patients with a positive GCA biopsy who underwent PET/CT at diagnosis and a CT scan of the aorta during follow-up with a delay of 46.7 (29.9) months [mean (SD)] that increased FDG uptake was associated with a significantly larger diameter of the ascending and descending aorta and a significantly larger volume of the thoracic aorta. Along this line, Muratore et al. (52) reported that aortic FDG uptake grade 3 at diagnosis was associated with an increased risk of aortic dilatation compared with aortic FDG uptake ≤2. Retrospective data from the French cohort involving 549 GCA patients confirmed the results by showing that in LV-GCA, aortic dilatation occurred in a previously inflamed segment in 94% of cases (51).
More recently, Moreel et al. (53) included 106 GCA patients who had undergone PET/CT at diagnosis, within 3 days of starting glucocorticoid therapy, and who were followed by performing annual CT scans of the aorta over a ten-year period. The TVS at diagnosis was associated with a greater annual increase in thoracic aortic diameter and volume. A positive PET/CT at diagnosis was associated with a higher risk of thoracic aortic aneurysm [adjusted hazard ratio = 10.24 (CI 95%: 1.25 to 83.3)]. The authors concluded that the intensity and extent of the initial inflammation determine the risk of subsequent aortic dilatation, as no association was observed between the development of thoracic aortic aneurysm and treatment regimen or relapse rate (53). Blockmans et al. (54) performed a post-hoc analysis of this study, including 52/106 patients who had at least one further PET/CT during follow-up. A total of 88 PET/CT were analysed during follow-up, 55 during relapse and 33 during remission. Overall, 9/10 patients with thoracic aortic aneurysms had a positive PET/CT both at diagnosis and during follow-up. However, the authors emphasize that no conclusions can be drawn about FDG uptake in remission because most patients underwent repeat PET/CT during a relapse (54). Therefore, the hypothesis that persistent aortic inflammation may contribute to the development of thoracic aortic aneurysms in GCA contrasts with the lack of association between thoracic aneurysm occurrence and treatment regimen or relapse rate shown in the first part of this study (53).
In conclusion, the results of numerous studies converge on the fact that large-vessel vascular FDG uptake at GCA diagnosis is associated with an increased risk of vascular complications (mainly dilatation and aneurysm) during follow-up. Whether persistent smouldering vascular inflammation or post-inflammatory vascular remodeling is responsible for the development of aortic aneurysms is still unclear.
Cranial PET/CT
Assessment of the cranial arteries (including temporal, occipital, maxillary and vertebral arteries) to diagnose GCA was not part of the original 2018 EULAR recommendations due to a lack of sufficient data (42). Following the publication of several studies evaluating cranial PET/CT (12–15), the updated recommendations include PET/CT alongside MRI as an alternative to ultrasonography for the examination of cranial arteries (46). Comparing these studies is challenging because different criteria were used to define a positive PET/CT and the gold standard diagnosis of GCA.
Two prospective studies by Sammel et al. (48) and Thibault et al. (15) used the clinical diagnosis as the gold standard, based on the absence of an alternative diagnosis and a favorable outcome with glucocorticoid treatment after 6 months of follow-up. Sammel et al. (48) considered the PET/CT to be positive based on a qualitative subjective evaluation of the cranial and thoracic segments. Thibault et al. (15) considered the PET/CT to be positive if at least one cranial segment had a visual grading ≥2 compared to liver FDG uptake. In the studies by Nienhuis et al. (49) and Nielsen et al. (53), patients with metastatic melanoma were used as a control group. Nienhuis et al. (55) included GCA cases with a positive TAB and Nielsen et al. (53) included GCA cases that met the ACR criteria confirmed after 6 months of follow-up. In these two case–control studies, the PET/CT was defined as positive if at least one cranial segment had a higher FDG uptake than the surrounding tissue.
The two prospective studies showed sensitivity of 71 and 73.3% and specificity of 91 and 97.2% for Sammel et al. (12) and Thibault et al. (15), respectively (54). An advantage of the study by Thibault et al. (15) was the combination of cranial PET/CT with extracranial PET/CT in a single examination. The combination of the two examinations optimized sensitivity (73.3% for cranial PET/CT, 66.7% for extracranial PET/CT and 80% for the combination) at the expense of specificity (97.2% for cranial PET/CT, 80.6% for extracranial PET/CT and 77.8% for the combination).
In conclusion, the advantage of cranial PET/CT is that it increases diagnostic sensitivity when combined with extracranial PET/CT. In addition to the temporal arteries, other cranial vessels such as the vertebral, maxillary or occipital arteries can also be studied. The correlation between the involvement of certain arterial segments and the risk of ischemic complications, for example between vertebral arteries and stroke, still requires further research. Table 3 summarises the studies’ characteristics.
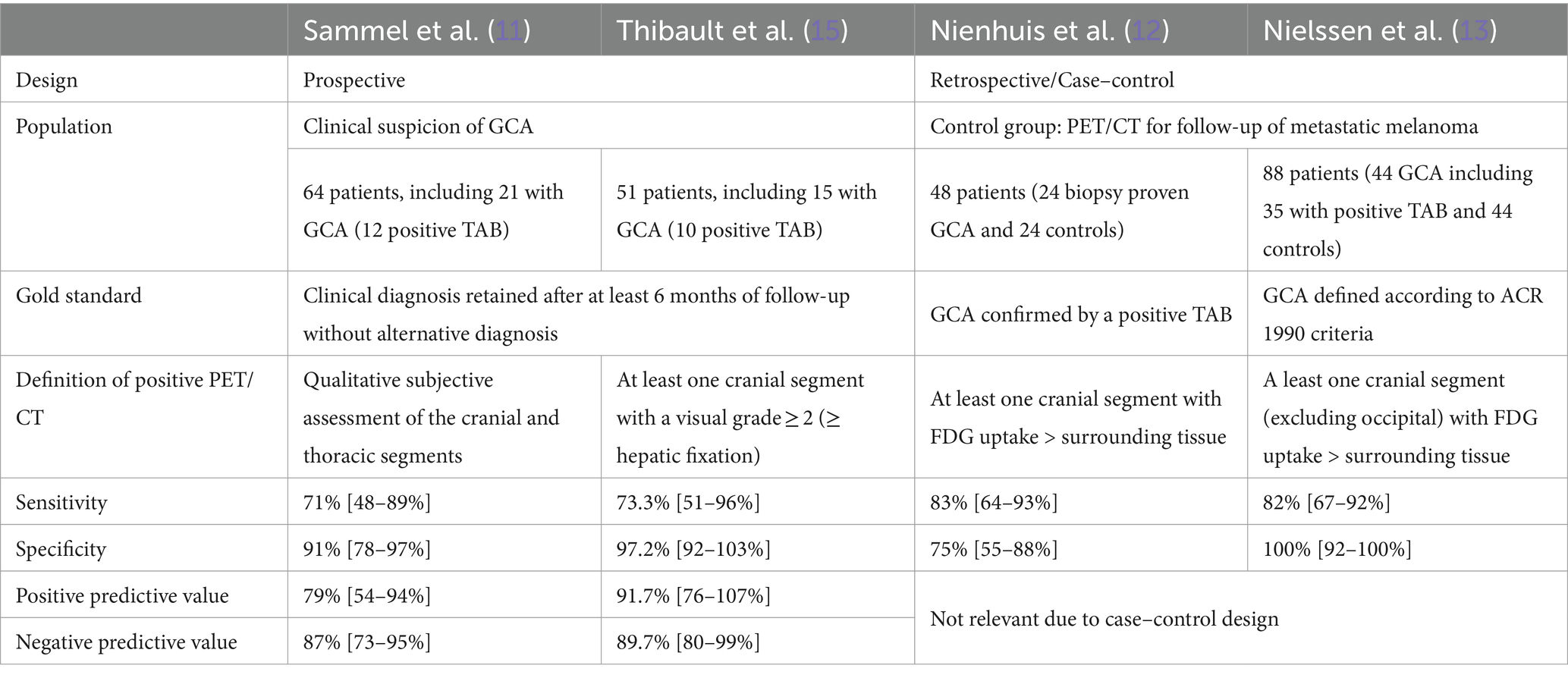
Table 3. Summary of studies assessing PET/CT for cranial arteries in GCA.
Perspectives
How PET/CT involvement and the extent of inflammation might guide treatment remains uncertain. Therefore, we believe that prospective evaluation of PET/CT in GCA is needed. This is especially true in clinical trials evaluating immunosuppressive therapy, where data on PET/CT assessment are lacking. In addition, the management of patients with GCA may benefit from the development and evaluation of new technologies. Examples include PET/MRI and new tracers that target the somatostatin receptor.
Combining FDG-PET with MRI may allow more precise anatomical localization of PET tracer uptake and better characterization of the inflamed arterial wall (56), while reducing radiation exposure (57). However, availability is poorer than with PET/CT and no prospective study has investigated the diagnostic performance of FDG-PET/MRI. Laurent et al. (58) defined three different patterns according to the positivity of MRI and/or PET in 13 retrospectively recruited patients with LVV who underwent 18 PET/MRIs at different follow-up times. The “inflammatory” pattern was defined as positive PET (visual grading = 3) and abnormal MRI (stenosis and/or wall thickening), the “fibrous” pattern as negative PET (visual grading = 1 or 2) and abnormal MRI (stenosis and/or wall thickening), and the “normal” pattern when both PET and MRI are negative. In a retrospective study, 14 patients with aortitis defined by PET/CT as the gold standard (11 GCA and 3 Takayasu patients) were compared with 14 control patients without aortitis (59). The sensitivity and specificity of PET/MRI were 85.7 and 100%, respectively. Sensitivity limitations were observed in the thoracic part of the aorta due to motion artefacts.
False-positive results from FDG PET/CT may be due to the metabolic activity of atherosclerosis, which is sometimes difficult to distinguish from persistent smoldering vascular inflammation or vascular remodeling, calling for the development of new, more specific radiotracers. Targeting the somatostatin receptor expressed by inflammatory macrophages, which play a major role in the pathophysiology of GCA, is an interesting prospect that could meet this need. Among these, somatostatin receptor PET/MRI using 68Ga-DOTATATE or 8F-FET-βAG-TOCA are candidates for more specific evaluation of large vessel vasculitis (60). In this prospective study, Ćorović et al. (60) compared 61 patients, including 27 with LVV (GCA = 13, Takayasu = 13, unspecified LVV = 1), 25 with recent atherosclerotic myocardial infarction and 9 patients with cancer. PET/MRI with 68Ga-DOTATATE and 18F-FET-bAG-TOCA discriminated active LVV from inactive LVV and active LVV from athrosclerosis with high diagnostic accuracy (AUROC = 0.89 and AUROC = 0.86, respectively).
Conclusion
PET/CT imaging has high diagnostic accuracy in GCA by demonstrating transmural vascular inflammation in large vessels. Recently, sensitivity has been improved by the ability to detect vascular FDG uptake in cranial arteries. LVV detected by PET/CT correlates with disease activity and could predict vascular complications such as aneurysms, suggesting that assessment of vascular damage by morphologic imaging during follow-up is warranted in these patients. However, PET/CT has several limitations. First, significant vascular FDG uptake may remain in some patients in remission on therapy. It is unclear whether this FDG uptake is due to persistent smouldering vascular inflammation or post-inflammatory vascular remodeling. In particular, the persistence of this FDG uptake does not appear to be predictive of future relapse and therefore should not be used to guide treatment decisions in patients in clinical remission. Secondly, the main limitation to the generalization of PET/CT is its availability in most centres less than 72 h after the introduction of glucocorticoids, after which the diagnostic accuracy decreases significantly. This limitation is very problematic because glucocorticoids must be started early after suspicions because of the risk of ophthalmological complications and blindness.
Author contributions
TT: Writing – original draft, Writing – review & editing. J-LA: Writing – review & editing. A-CB: Writing – review & editing. HG: Writing – review & editing. AR: Writing – review & editing. HD: Writing – review & editing. AC: Writing – review & editing. BB: Writing – review & editing. MS: Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
MS was employed by the AbbVie consulting, Argenx consulting, Boehringer Ingelheim consulting, GSK consulting, Novartis consulting and research grant, Roche–Chugai consulting, CSL VIFOR consulting, Fresenius consulting. BB was employed by the Roche–Chugai personal fees for consulting, Boehringer Ingelheim consulting. AR was employed by the Novartis research grant, Novartis consulting, AbbVie consulting, Boehringer Ingelheim consulting, Chugai consulting. HD declare Grants from GSK, Consultant for NOVARTIS, Consultant for GSK, Consultant for Jonhson & Jonhson.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Jennette, JC, Falk, RJ, Bacon, PA, Basu, N, Cid, MC, Ferrario, F, et al. 2012 revised international Chapel Hill consensus conference nomenclature of Vasculitides. Arthritis Rheum. (2013) 65:1–11. doi: 10.1002/art.37715
2. Borchers, AT, and Gershwin, ME. Giant cell arteritis: a review of classification, pathophysiology, geoepidemiology and treatment. Autoimmun Rev. (2012) 11:A544–54. doi: 10.1016/j.autrev.2012.01.003
3. Fein, AS, and Ko, MW. Neuro-ophthalmologic complications of Giant cell arteritis: diagnosis and treatment. Semin Neurol. (2019) 39:673–81. doi: 10.1055/s-0039-1698761
4. Samson, M, Jacquin, A, Audia, S, Daubail, B, Devilliers, H, Petrella, T, et al. Stroke associated with giant cell arteritis: a population-based study. J Neurol Neurosurg Psychiatry. (2015) 86:216–21. doi: 10.1136/jnnp-2014-307614
5. de Boysson, H, Daumas, A, Vautier, M, Parienti, J-J, Liozon, E, Lambert, M, et al. Large-vessel involvement and aortic dilation in giant-cell arteritis. A multicenter study of 549 patients. Autoimmun Rev. (2018) 17:391–8. doi: 10.1016/j.autrev.2017.11.029
6. Maz, M, Chung, SA, Abril, A, Langford, CA, Gorelik, M, Guyatt, G, et al. 2021 American College of Rheumatology/Vasculitis Foundation guideline for the Management of Giant Cell Arteritis and Takayasu Arteritis. Arthritis Rheumatol. (2021) 73:1349–65. doi: 10.1002/art.41774
7. Gunawardene, AR, and Chant, H. Facial nerve injury during temporal artery biopsy. Ann R Coll Surg Engl. (2014) 96:257–60. doi: 10.1308/003588414X13814021679438
8. Bienvenu, B, Ly, KH, Lambert, M, Agard, C, André, M, Benhamou, Y, et al. Management of giant cell arteritis: recommendations of the French study Group for Large Vessel Vasculitis (GEFA). Rev Med Interne. (2016) 37:154–65. doi: 10.1016/j.revmed.2015.12.015
9. Dejaco, C, Ramiro, S, Duftner, C, Besson, FL, Bley, TA, Blockmans, D, et al. EULAR recommendations for the use of imaging in large vessel vasculitis in clinical practice. Ann Rheum Dis. (2018) 77:636–43. doi: 10.1136/annrheumdis-2017-212649
10. Dejaco, C, Ramiro, S, Bond, M, Bosch, P, Ponte, C, Mackie, SL, et al. EULAR recommendations for the use of imaging in large vessel vasculitis in clinical practice: 2023 update. Ann Rheum Dis. (2024) 83:741–51. doi: 10.1136/ard-2023-224543
11. Dejaco, C, Duftner, C, Buttgereit, F, Matteson, EL, and Dasgupta, B. The spectrum of giant cell arteritis and polymyalgia rheumatica: revisiting the concept of the disease. Rheumatology. (2017) 56:506–15. doi: 10.1093/rheumatology/kew273
12. Sammel, AM, Hsiao, E, Schembri, G, Nguyen, K, Brewer, J, Schrieber, L, et al. Diagnostic accuracy of positron emission tomography/computed tomography of the head, neck, and chest for Giant cell arteritis: a prospective, double-blind, cross-sectional study. Arthritis Rheumatol. (2019) 71:1319–28. doi: 10.1002/art.40864
13. Nienhuis, PH, Sandovici, M, Glaudemans, AW, Slart, RH, and Brouwer, E. Visual and semiquantitative assessment of cranial artery inflammation with FDG-PET/CT in giant cell arteritis. Semin Arthritis Rheum. (2020) 50:616–23. doi: 10.1016/j.semarthrit.2020.04.002
14. Nielsen, BD, Hansen, IT, Kramer, S, Haraldsen, A, Hjorthaug, K, Bogsrud, TV, et al. Simple dichotomous assessment of cranial artery inflammation by conventional 18F-FDG PET/CT shows high accuracy for the diagnosis of giant cell arteritis: a case-control study. Eur J Nucl Med Mol Imaging. (2019) 46:184–93. doi: 10.1007/s00259-018-4106-0
15. Thibault, T, Durand-Bailloud, B, Soudry-Faure, A, Greigert, H, Drouet, C, Devilliers, H, et al. PET/CT of cranial arteries for a sensitive diagnosis of giant cell arteritis. Rheumatology. (2023) 62:1568–75. doi: 10.1093/rheumatology/keac430
16. Slart, RHJAWriting group, Reviewer group, Members of EANM Cardiovascular, Members of EANM Infection & Inflammation, Members of Committees, SNMMI Cardiovascular, Members of Council, PET Interest Group, Members of ASNC, EANM Committee Coordinator . FDG-PET/CT(a) imaging in large vessel vasculitis and polymyalgia rheumatica: joint procedural recommendation of the EANM, SNMMI, and the PET interest group (PIG), and endorsed by the ASNC. Eur J Nucl Med Mol Imaging. (2018) 45:1250–69. doi: 10.1007/s00259-018-3973-8
17. Martínez-Rodríguez, I, Martínez-Amador, N, Banzo, I, Quirce, R, Jiménez-Bonilla, J, De Arcocha-Torres, M, et al. Assessment of aortitis by semiquantitative analysis of 180-min 18F-FDG PET/CT acquisition images. Eur J Nucl Med Mol Imaging. (2014) 41:2319–24. doi: 10.1007/s00259-014-2863-y
18. Bucerius, J, Hyafil, F, Verberne, HJ, Slart, RHJA, Lindner, O, Sciagra, R, et al. Position paper of the cardiovascular Committee of the European Association of nuclear medicine (EANM) on PET imaging of atherosclerosis. Eur J Nucl Med Mol Imaging. (2016) 43:780–92. doi: 10.1007/s00259-015-3259-3
19. Rabkin, Z, Israel, O, and Keidar, Z. Do hyperglycemia and diabetes affect the incidence of false-negative 18F-FDG PET/CT studies in patients evaluated for infection or inflammation and cancer? A Comparative analysis. J Nucl Med. (2010) 51:1015–20. doi: 10.2967/jnumed.109.074294
20. Bucerius, J, Mani, V, Moncrieff, C, Machac, J, Fuster, V, Farkouh, ME, et al. Optimizing 18F-FDG PET/CT imaging of vessel wall inflammation: the impact of 18F-FDG circulation time, injected dose, uptake parameters, and fasting blood glucose levels. Eur J Nucl Med Mol Imaging. (2014) 41:369–83. doi: 10.1007/s00259-013-2569-6
21. Nielsen, BD, Gormsen, LC, Hansen, IT, Keller, KK, Therkildsen, P, and Hauge, E-M. Three days of high-dose glucocorticoid treatment attenuates large-vessel 18F-FDG uptake in large-vessel giant cell arteritis but with a limited impact on diagnostic accuracy. Eur J Nucl Med Mol Imaging. (2018) 45:1119–28. doi: 10.1007/s00259-018-4021-4
22. Besson, FL, De, BH, Parienti, JJ, Bouvard, G, Bienvenu, B, and Agostini, D. Towards an optimal semiquantitative approach in giant cell arteritis: an (18)F-FDG-PET/CT case-control study. Eur J Nucl Med Mol Imaging. (2014) 41:155–66. doi: 10.1007/s00259-013-2545-1
23. Lehmann, P, Buchtala, S, Achajew, N, Haerle, P, Ehrenstein, B, and Lighvani, H. 18F-FDG-PET as a diagnostic procedure in large vessel vasculitis-a controlled, blinded re-examination of rou tine PET scans. Clin Rheumatol. (2011) 30:37–42. doi: 10.1007/s10067-010-1598-9
24. Meller, J, Strutz, F, Siefker, U, Scheel, A, Sahlmann, CO, Lehmann, K, et al. Early diagnosis and follow-up of aortitis with [(18)F]FDG PET and MRI. Eur J Nucl Med Mol Imaging. (2003) 30:730–6. doi: 10.1007/s00259-003-1144-y
25. Grayson, PC, Alehashemi, S, Bagheri, AA, Civelek, AC, Cupps, TR, Kaplan, MJ, et al. 18 F-Fluorodeoxyglucose-positron emission tomography as an imaging biomarker in a prospective, longitudinal cohort of patients with large vessel Vasculitis. Arthritis Rheumatol. (2018) 70:439–49. doi: 10.1002/art.40379
26. Blockmans, D, de Ceuninck, L, Vanderschueren, S, Knockaert, D, Mortelmans, L, and Bobbaers, H. Repetitive 18F-fluorodeoxyglucose positron emission tomography in giant cell arteritis: a prospective study of 35 patients. Arthritis Rheum. (2006) 55:131–7. doi: 10.1002/art.21699
27. Sammel, AM, Hsiao, E, Schembri, G, Bailey, E, Nguyen, K, Brewer, J, et al. Cranial and large vessel activity on positron emission tomography scan at diagnosis and 6 months in giant cell arteritis. Int J Rheum Dis. (2020) 23:582–8. doi: 10.1111/1756-185X.13805
28. Galli, E, Muratore, F, Mancuso, P, Boiardi, L, Marvisi, C, Besutti, G, et al. The role of PET/CT in disease activity assessment in patients with large vessel vasculitis. Rheumatology. (2022) 61:4809–16. doi: 10.1093/rheumatology/keac125
29. Dashora, HR, Rosenblum, JS, Quinn, KA, Alessi, H, Novakovich, E, Saboury, B, et al. Comparing semiquantitative and qualitative methods of vascular 18F-FDG PET activity measurement in large-vessel vasculitis. J Nucl Med. (2022) 63:280–6. doi: 10.2967/jnumed.121.262326
30. Ponte, C, Martins-Martinho, J, and Luqmani, RA. Diagnosis of giant cell arteritis. Rheumatology. (2020) 59:iii5–iii16. doi: 10.1093/rheumatology/kez553
31. Bosch, P, Bond, M, Dejaco, C, Ponte, C, Mackie, SL, Falzon, L, et al. Imaging in diagnosis, monitoring and outcome prediction of large vessel vasculitis: a systematic literature review and meta-analysis informing the 2023 update of the EULAR recommendations. RMD Open. (2023) 9:e003379. doi: 10.1136/rmdopen-2023-003379
32. Lariviere, D, Benali, K, Coustet, B, Pasi, N, Hyafil, F, Klein, I, et al. Positron emission tomography and computed tomography angiography for the diagnosis of giant cell arteritis: a real-life prospective study. Medicine. (2016) 95:e4146. doi: 10.1097/MD.0000000000004146
33. Nielsen, BD, Hansen, IT, Keller, KK, Therkildsen, P, Gormsen, LC, and Hauge, E-M. Diagnostic accuracy of ultrasound for detecting large-vessel giant cell arteritis using FDG PET/CT as the reference. Rheumatology (Oxford). (2020) 59:2062–73. doi: 10.1093/rheumatology/kez568
34. Löffler, C, Hoffend, J, Benck, U, Krämer, BK, and Bergner, R. The value of ultrasound in diagnosing extracranial large-vessel vasculitis compared to FDG-PET/CT: a retrospective study. Clin Rheumatol. (2017) 36:2079–86. doi: 10.1007/s10067-017-3669-7
35. Molina-Collada, J, Castrejón, I, Monjo-Henry, I, Fernández-Fernández, E, Torres Ortiz, G, Martínez-Barrio, J, et al. Impact of ultrasound limitation to assess aortitis in patients with giant cell arteritis: comparative study with FDG-PET/CT. RMD Open. (2023) 9:e003329. doi: 10.1136/rmdopen-2023-003329
36. Molina-Collada, J, Castrejón, I, Rivera, J, Martínez-Barrio, J, Nieto-González, JC, López, K, et al. The role of ultrasound and FDG-PET/CT to detect extracranial artery involvement in patients with suspected large vessel vasculitis. Mod Rheumatol. (2023) 33:549–56. doi: 10.1093/mr/roac058
37. Hop, H, Mulder, DJ, Sandovici, M, Glaudemans, AWJM, van Roon, AM, Slart, RHJA, et al. Diagnostic value of axillary artery ultrasound in patients with suspected giant cell arteritis. Rheumatology (Oxford). (2020) 59:3676–84. doi: 10.1093/rheumatology/keaa102
38. Moreel, L, Betrains, A, Doumen, M, Molenberghs, G, Vanderschueren, S, and Blockmans, D. Diagnostic yield of combined cranial and large vessel PET/CT, ultrasound and MRI in giant cell arteritis: a systematic review and meta-analysis. Autoimmun Rev. (2023) 22:103355. doi: 10.1016/j.autrev.2023.103355
39. van Nieuwland, M, Colin, EM, Vermeer, M, Wagenaar, NRL, Vijlbrief, OD, van Zandwijk, JK, et al. A direct comparison in diagnostic performance of CDUS, FDG-PET/CT and MRI in patients suspected of giant cell arteritis. Rheumatology. (2024). doi: 10.1093/rheumatology/keae171
40. Gheysens, O, de Ponfilly, MP, Nocturne, G, Seror, R, Besson, FL, and Jamar, F. [18F]FDG-PET/CT in polymyalgia rheumatica: an update and future aspects. Semin Nucl Med. (2024) 54:371–8. doi: 10.1053/j.semnuclmed.2023.10.003
41. Quinn, KA, Dashora, H, Novakovich, E, Ahlman, MA, and Grayson, PC. Use of 18F-fluorodeoxyglucose positron emission tomography to monitor tocilizumab effect on vascular inflammation in giant cell arteritis. Rheumatology. (2021) 60:4384–9. doi: 10.1093/rheumatology/keaa894
42. Sebastian, A, Kayani, A, Prieto-Pena, D, Tomelleri, A, Whitlock, M, Mo, J, et al. Efficacy and safety of tocilizumab in giant cell arteritis: a single Centre NHS experience using imaging (ultrasound and PET-CT) as a diagnostic and monitoring tool. RMD Open. (2020) 6:e001417. doi: 10.1136/rmdopen-2020-001417
43. Schönau, V, Roth, J, Tascilar, K, Corte, G, Manger, B, Rech, J, et al. Resolution of vascular inflammation in patients with new-onset giant cell arteritis: data from the RIGA study. Rheumatology. (2021) 60:3851–61. doi: 10.1093/rheumatology/keab332
44. de Boysson, H, Liozon, E, Lambert, M, Parienti, J-J, Artigues, N, Geffray, L, et al. 18F-fluorodeoxyglucose positron emission tomography and the risk of subsequent aortic complications in giant-cell arteritis: a multicenter cohort of 130 patients. Medicine. (2016) 95:e3851. doi: 10.1097/MD.0000000000003851
45. de Boysson, H, Aide, N, Liozon, E, Lambert, M, Parienti, J-J, Monteil, J, et al. Repetitive 18F-FDG-PET/CT in patients with large-vessel giant-cell arteritis and controlled disease. Eur J Intern Med. (2017) 46:66–70. doi: 10.1016/j.ejim.2017.08.013
46. Prieto Peña, D, Martínez-Rodríguez, I, Atienza-Mateo, B, Calderón-Goercke, M, Banzo, I, González-Vela, MC, et al. Evidence for uncoupling of clinical and 18-FDG activity of PET/CT scan improvement in tocilizumab-treated patients with large-vessel giant cell arteritis. Clin Exp Rheumatol. (2021) 39:69–75. doi: 10.55563/clinexprheumatol/mjm8fr
47. Kaymakci, MS, Boire, NA, Bois, MC, Elfishawi, MM, Langenfeld, HE, Hanson, AC, et al. Persistent aortic inflammation in patients with giant cell arteritis. Autoimmun Rev. (2023) 22:103411. doi: 10.1016/j.autrev.2023.103411
48. Billet, A-C, Thibault, T, Liozon, É, De Boysson, H, Perard, L, Espitia, O, et al. Prognostic value of 18 FDG-PET at diagnosis and follow-up in giant cell arteritis: an observational restrospective study. Eur J Intern Med. (2024) 126:69–76. doi: 10.1016/j.ejim.2024.03.037
49. Hemmig, AK, Rottenburger, C, Baruti, L, Mensch, N, Aschwanden, M, Kyburz, D, et al. Imaging to predict early relapses after treatment discontinuation in patients with large vessel giant cell arteritis - a cohort study. Semin Arthritis Rheum. (2024) 66:152425. doi: 10.1016/j.semarthrit.2024.152425
50. Quinn, KA, Ahlman, MA, Alessi, HD, LaValley, MP, Neogi, T, Marko, J, et al. Association of 18 F-Fluorodeoxyglucose-positron emission tomography activity with angiographic progression of disease in large vessel Vasculitis. Arthritis Rheumatol. (2023) 75:98–107. doi: 10.1002/art.42290
51. Blockmans, D, Coudyzer, W, Vanderschueren, S, Stroobants, S, Loeckx, D, Heye, S, et al. Relationship between fluorodeoxyglucose uptake in the large vessels and late aortic diameter in giant cell arteritis. Rheumatology. (2008) 47:1179–84. doi: 10.1093/rheumatology/ken119
52. Muratore, F, Crescentini, F, Spaggiari, L, Pazzola, G, Casali, M, Boiardi, L, et al. Aortic dilatation in patients with large vessel vasculitis: a longitudinal case control study using PET/CT. Semin Arthritis Rheum. (2019) 48:1074–82. doi: 10.1016/j.semarthrit.2018.10.003
53. Moreel, L, Coudyzer, W, Boeckxstaens, L, Betrains, A, Molenberghs, G, Vanderschueren, S, et al. Association between vascular 18F-Fluorodeoxyglucose uptake at diagnosis and change in aortic dimensions in Giant cell arteritis: a cohort study. Ann Intern Med. (2023) 176:1321–9. doi: 10.7326/M23-0679
54. Blockmans, D, Moreel, L, Betrains, A, Vanderschueren, S, Coudyzer, W, Boeckxstaens, L, et al. Association between vascular FDG uptake during follow-up and the development of thoracic aortic aneurysms in giant cell arteritis. Front Med. (2024) 11:1384533. doi: 10.3389/fmed.2024.1384533
55. Hunder, GG, Bloch, DA, Michel, BA, Stevens, MB, Arend, WP, Calabrese, LH, et al. The American College of Rheumatology 1990 criteria for the classification of giant cell arteritis. Arthritis Rheum. (1990) 33:1122–8. doi: 10.1002/art.1780330810
56. van der Geest, KSM, Gheysens, O, Gormsen, LC, Glaudemans, AWJM, Tsoumpas, C, Brouwer, E, et al. Advances in PET imaging of large vessel Vasculitis: an update and future trends. Semin Nucl Med. (2024) 54:753–60. doi: 10.1053/j.semnuclmed.2024.03.001
57. Brauner, J-F, Rasul, S, Berzaczy, D, Beitzke, D, Wollenweber, T, and Beitzke, D. Hybrid PET/MRI of large vessel vasculitis: radiation dose compared to PET/CT with view on cumulative effective dose. Wien Klin Wochenschr. (2024). doi: 10.1007/s00508-024-02336-2 (Epub ahead of print).
58. Laurent, C, Ricard, L, Fain, O, Buvat, I, Adedjouma, A, Soussan, M, et al. PET/MRI in large-vessel vasculitis: clinical value for diagnosis and assessment of disease activity. Sci Rep. (2019) 9:12388. doi: 10.1038/s41598-019-48709-w
59. Einspieler, I, Henninger, M, Mergen, V, Wendorff, H, Haller, B, Eiber, M, et al. Three-dimensional fat-saturated T1-weighted Cartesian volumetric interpolated breath-hold examination (VIBE) for the diagnosis of aortitis in patients with suspected large vessel vasculitis: a comparative study with 18F-FDG PET applying fully integrated PET/MRI. Clin Radiol. (2019) 74:731.e11–9. doi: 10.1016/j.crad.2019.04.012
Keywords: giant cell arteritis, 18F-fluorodeoxyglucose positron emission tomography/computed tomography, diagnosis, monitoring, prognostic
Citation: Thibault T, Alberini J-L, Billet A-C, Greigert H, Ramon A, Devilliers H, Cochet A, Bonnotte B and Samson M (2024) An overview of 18F-fluorodeoxyglucose positron emission tomography/computed tomography in giant cell arteritis. Front. Med. 11:1469964. doi: 10.3389/fmed.2024.1469964
Edited by:
Ryusuke Yoshimi, Yokohama City University, JapanReviewed by:
Juan Molina-Collada, Gregorio Marañón Hospital, SpainChristos Koutsianas, National and Kapodistrian University of Athens, Greece
Copyright © 2024 Thibault, Alberini, Billet, Greigert, Ramon, Devilliers, Cochet, Bonnotte and Samson. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Maxime Samson, bWF4aW1lLnNhbXNvbkB1LWJvdXJnb2duZS5mcg==; bWF4aW1lLnNhbXNvbkBjaHUtZGlqb24uZnI=