
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Med. , 20 September 2024
Sec. Infectious Diseases: Pathogenesis and Therapy
Volume 11 - 2024 | https://doi.org/10.3389/fmed.2024.1457501
 Willy Le Roi Togna Pabo1,2,3*
Willy Le Roi Togna Pabo1,2,3* Aurelie Minelle Kengni Ngueko4,5
Aurelie Minelle Kengni Ngueko4,5 Alex Durand Nka1,4,6*
Alex Durand Nka1,4,6* Maria Mercedes Santoro4
Maria Mercedes Santoro4 Yagai Bouba1,4
Yagai Bouba1,4 Collins Ambe Chenwi1
Collins Ambe Chenwi1 Ezéchiel Ngoufack Jagni Semengue1,4,6Désiré Takou1Georges Teto1Beatrice Dambaya1Raymond Babila Nyasa2Michel Carlos Tommo Tchouaket1,5Grace Angong Beloumou1Sandrine Claire Djupsa Ndjeyep1
Ezéchiel Ngoufack Jagni Semengue1,4,6Désiré Takou1Georges Teto1Beatrice Dambaya1Raymond Babila Nyasa2Michel Carlos Tommo Tchouaket1,5Grace Angong Beloumou1Sandrine Claire Djupsa Ndjeyep1 Aude Christelle Ka’e1Tatiana Anim Keng Tekoh1Derrick Tambe Ayuk Ngwese1Naomi-Karell Etame1Rachel Audrey Nayang Mundo1Rachel Simo Kamgaing1Samuel Martin Sosso1Roland Ndip Ndip2Vittorio Colizzi1,4,6
Aude Christelle Ka’e1Tatiana Anim Keng Tekoh1Derrick Tambe Ayuk Ngwese1Naomi-Karell Etame1Rachel Audrey Nayang Mundo1Rachel Simo Kamgaing1Samuel Martin Sosso1Roland Ndip Ndip2Vittorio Colizzi1,4,6 Francesca Cecchereni-Silberstein4Alexis Ndjolo1
Francesca Cecchereni-Silberstein4Alexis Ndjolo1 Joseph Fokam1,5,7,8,9*
Joseph Fokam1,5,7,8,9*Background: The elevated rate of AIDS-related mortality in Sub-Saharan Africa among adolescents living with HIV (ALHIV) is influenced by various factors, notably immunosuppression, within a framework of limited therapeutic alternatives. We aimed to enhance the management of pediatric HIV by assessing the immune response and associated factors in perinatally-infected ALHIV on antiretroviral therapy (ART) in Cameroon.
Methods: A cohort study was conducted from 2018–2020 among 271 ART-experienced ALHIV in Cameroon. Sociodemographic data, immunological (CD4), and virological (plasma viral load, PVL) responses were measured at enrolment (T0), 6-months (T1), and 12-months (T2) using PIMA CD4 (Abbott/Pantech (Pty) Ltd) and Abbott Applied Biosystem platform (Real-Time PCR m2000RT) respectively. Immunological failure (IF) was defined as absolute CD4 < 250 cells/mm3, and Virological failure (VF) as PVL ≥ 1,000 copies/ml. A linear mixed-effects model with R version 4.4.1 was used to estimate both fixed and random effects, with significance set at p < 0.05.
Results: Of the 271 perinatally-infected ALHIV enrolled over three phases, females were predominant (55.7, 55.1, and 56.0%); median age was 14 (IQR: 12–17); majority of the participants were followed-up in urban areas (77.5, 74.5, and 78.6%); and the age distribution favored older adolescents (48.7, 61.2, and 58.5%). Most participants achieved clinical success (93.1, 89.7, 88.9%), predominantly on first-line ART (80.8, 66.2, and 53.0%), with good adherence (64.2, 58.9, and 64.5%). Most participants had secondary education (67.2, 70.1, and 67.5%). Median CD4+ counts fluctuated overtime, with values of 563 (IQR: 249.0–845.0), 502 (IQR: 319.0–783.5), and 628 (IQR: 427.5–817.5), respectively. Of note, being male was linked to a reduction in CD4+ count compared to females, [−200.63 (−379.32 to −21.95), p = 0.028]. Similarly, late adolescence was associated with lower CD4+ counts compared to early adolescence, [−181.08 (−301.08 to −61.09), p = 0.003]. Moreover, participants experiencing VF showed significantly lower CD4+ counts compared to those with undetectable viral loads, [−353.08 (−465.81 to −240.36), p < 0.001]. Additionally, there was a marginally significant interaction between male gender and secondary educational level, [209.78 (−6.94–426.51), p = 0.058].
Conclusion: Among perinatally-infected ALHIV, age, gender, educational level, and virological status are key factors influencing their immune health and treatment outcomes. Prioritizing targeted interventions and close monitoring within these subgroups is crucial for optimal management, employing holistic care strategies that consider not only medical interventions but also psychosocial support and education.
Sub-Saharan Africa (SSA) bears the highest global burden of HIV, encompassing 54.6% of the 38.0 million infections and 43.7% of the 690,000 [500,000–970,000] AIDS-related deaths (1). Adolescents, constituting a vulnerable demographic, contribute to approximately 49.3% of new infections in this region (1). Cameroon, one of the 15 countries severely affected by HIV among adolescents, contributes 2% to the global HIV prevalence in this population (2). Despite a decline in AIDS-related mortality attributed to expanded antiretroviral therapy (ART), adolescent mortality has risen by approximately 50%, primarily due to opportunistic infections (3). Adolescents with HIV pose a significant health concern with limited routine management data, especially in SSA where surveillance strategies remain suboptimal without robust clinical evidence (4–6).
Historically, the CD4 cell count served as the primary marker for immune suppression assessment and ART initiation timing in HIV/AIDS patients (7, 8). However, the 2015 World Health Organization (WHO) recommendation advocates for ART initiation irrespective of CD4 count, symptoms, or clinical conditions (9). Some subsequent studies propose reduced or discontinued CD4 monitoring post-ART initiation when viral load tests are available and show viral load suppression (10, 11). The paradigm shifts toward treatment for all, viral load implementation, and suggestions to curtail CD4 testing post-treatment initiation prompt a re-evaluation of the significance of CD4 testing. Intriguingly, the 2017 WHO guideline strongly advocates for a comprehensive care package, including close monitoring of viral load and CD4, for patients with advanced HIV disease (CD4 count below 200 cells/mm3) (12).
Beyond the CD4 T cell count, viral load significantly influences treatment outcomes (13). Elevated baseline viral loads indicate heightened HIV replication and increased immune system strain, possibly necessitating more aggressive treatment strategies for viral suppression (14). It is crucial to acknowledge that while baseline immune status strongly predicts treatment outcomes, it is not the sole determinant (14). Factors like treatment adherence, drug resistance, and comorbidities also impact treatment response. Hence, a holistic approach considering multiple factors becomes imperative to optimize treatment outcomes for ALHIV (15). The immunological status of ALHIV undergoing ART plays a pivotal role in predicting treatment outcomes. Elevated baseline CD4+ T cell counts are linked to more favorable treatment responses and enhanced long-term results. Conversely, diminished CD4+ T cell counts and heightened viral loads at baseline signify an increased risk of complications, necessitating more rigorous monitoring and intervention (16). However, it is imperative to take into account other factors influencing treatment response to formulate a comprehensive approach for managing HIV infection in this adolescent population. Given the paucity of information on immuno-virological monitoring in pediatric populations, especially in developing countries, this study aimed to evaluate the prevalence of adolescents living with HIV (ALHIV) requiring immune monitoring and investigate the association between immunological markers and virological failure (VF) in this population.
A prospective cohort study was carried out from 2018 to 2020 among 271 ALHIV undergoing ART at designated health facilities within the “Resistance Evolution among Adolescents in Yaoundé and its surroundings” (READY-study) in the Centre region of Cameroon. Participants were enrolled through consecutive sampling methods, and follow-ups occurred at enrolment (T0), 6 months (T1), and 12 months (T2).
The study sites were selected from both urban and rural settings within the Centre region of Cameroon, and were classified as follows:
Urban settings: Two health facilities specialized in pediatric care, located in Yaoundé: the Mother–Child Centre of the Chantal Biya Foundation (MCC-FCB) and the National Social Welfare Hospital (NSWH);
Rural settings: Two health facilities situated 30–50 km from the urban area: the Mbalmayo District Hospital (HDMB) in Mbalmayo and the Mfou District Hospital (HDMF) in Mfou. Additionally, the Nkomo Integrated Health Centre (NIHC) and the Bikop Catholic Health Centre (BCHC) served as satellite sites in the Centre region of Cameroon.
The site selection for the study was based on several key criteria. Facilities were required to have at least three years of experience in managing pediatric ART, ensuring a robust background in treatment. Additionally, clinics needed to provide both first-and second-line ART regimens at their pharmacies and adhere to national ART guidelines, demonstrating compliance with established national standards. The availability of ART registers, patient medical files, or a database was also necessary to facilitate comprehensive data management. Each selected site had to cater to a minimum of 15 adolescents on ART to ensure a sufficient sample size. Lastly, to ensure a diverse representation, facilities were chosen from both urban and rural areas. An exhaustive and non-randomized sampling method was used for participant enrolment, following eligibility criteria.
Participants were enrolled from the selected study sites. Inclusion criteria encompassed adolescents perinatally infected with HIV (APHI) within the age range of 10 to 19 years, possessing documented infection routes, and undergoing a standard antiretroviral therapy (ART) regimen based on either a first-line reverse transcriptase inhibitor (RTI) or a second-line regimen comprising a Ritonavir-boosted protease inhibitor (PI/r) for a minimum of 6 months. Additionally, compliance with the criteria involved providing written assent and securing informed consent from their legal guardian(s). Non-inclusion criteria involved individuals not formally enrolled in any ART monitoring system, reported as ART-naïve, on a drug regimen not aligned with national guidelines, or experiencing treatment interruption. Exclusion criteria encompassed participants who voluntarily withdrew from the study or transferred out of a study site before reaching mid-or endpoint evaluations.
Following enrolment, ten mL of whole blood were collected from each participant and transported on icepacks within 6 h to the virology laboratory of the Chantal Biya International Reference Centre (CIRCB) in Yaounde, Cameroon. A 200 μL whole blood aliquot for CD4 enumeration was obtained. Subsequently, plasma aliquots for Viral Load (PVL) and HIV genotypic resistance testing (GRT) were extracted after centrifugation at 1,600 rpm for 10 min and then stored at −80°C for further analyses. CD4 cell count was conducted using the Pima CD4 (Abbott/Pantech (Pty) Ltd., Westville, South Africa) automatic test, following the manufacturer’s instructions (17). The Pima test consists of a disposable Pima test cartridge, containing dried reagents, and the Pima Analyzer. A low sample volume of approximately 25 microliters (μL) of whole blood is collected into the test cartridge, which is then capped. The Pima test cartridge is inserted into the Pima Analyzer and the sample sealed within the cartridge is processed. During the course of test processing, data is recorded, analyzed and interpreted using software embedded in the Pima Analyzer. Upon completion of the test the cartridge is removed from the Pima Analyzer and a test result is displayed.
PVL measurement utilized the Abbott Applied Biosystem platform (Real-Time PCR AB m2000RT), adhering to the manufacturer’s instructions (Abbott Laboratories, USA) (18), with a detection threshold of 40 copies/mL (lower) and 10,000,000 copies/mL (upper). Viral RNA was extracted from 600 μL Plasma samples and carefully prepared (remove inhibitors that can interfere with the PCR reaction) for analysis. After then, 25 μL of elution buffer and 65 μL of nuclease free water was add on extracted RNA; 50 μL of eluted RNA was homogenised with Master mix (50 μL per reaction) containing reagents, primers, probes, and enzymes. The m2000RT system analyses the real-time fluorescence data and calculates the viral load in copies/mL of plasma.
To enhance polymerase chain reaction (PCR) amplification sensitivity, HIV-1 RNA extraction was performed from 1,000 μL of plasma aliquots, involving an initial 2-h refrigerated centrifugation step at 14,000 rpm to concentrate viral RNA (19). Manual extraction of HIV-1 RNA was carried out from 140 μL of plasma using the QIAGEN protocol (QIAamp® DNA Minikit; QIAGEN, Courtaboeuf, France) (20) which after the Lysis step done by adding 200 μL of Lyzol, a phase separation is done by adding 200 μL of chloroform and the RNA isolated is carefully transferred to a new 1.5 mL Eppendorf which purification with ethanol at 70% and wash solutions brought with the Kit then follows. It is finally eluted with 50 μL of elution buffer (AVE Buffer) which is now ready for the RT-PCR.
The socio-demographic, clinical and biological data of each participant was stored in a database with access restricted to authorized persons, and each participant was assigned an identification number which was used throughout the data analysis process. CIRCB is a government institute of the Ministry of Public Health, in charge of research and reference clinical monitoring of HIV-infected patients, with participation in external quality assurance programs for HIV screening/diagnosis, viral load measurements, CD4 count, as well as biochemistry and hematological analysis.1
Young adolescents referred to participants aged between 10–14 years, and old adolescents referred to participants aged between 15–19 years. Virological failure (VF) was defined as PVL ≥1,000 RNA copies/mL; Virological suppression (VS) referred to PVL between 50–999 copies/mL and undetectable viremia referred to PVL < 50 copies/mL (21); immunological failure was defined as CD4+ cell count <250 cells/mm3, and adequate immune response as CD4+ cell ≥250 cells/mm3 (22). The primary outcome for immune monitoring was defined as CD4+ cell count >250 cells/mm3 as recommended by WHO (23).
Data were initially recorded in an Excel spreadsheet and subjected to a rigorous double-checking process to ensure accuracy. Subsequently, the meticulously cleaned dataset underwent analysis using SPSS and RStudio version 2023.09.1 + 494, with a predetermined statistical significance level set at p < 0.05. Data for continuous variables were presented as mean and standard deviation (SD) for normally distributed, or median and interquartile range (IQR) for non-normally distributed variables. Data for categorical variables were presented as frequencies and percentages, and the data were succinctly summarized using tables and figures. Chi-square and Fisher’s exact tests were employed to discern associations between categorical variables, as deemed appropriate. Additionally, the Spearman correlation and the Post Hoc test of Tukey were implemented to ascertain the impact of different categories within variables on the outcome. Linear regression was used to explore factors associated with immunological response in participants with complete data on the outcome and covariates. The outcome of the model was absolute CD4+ count; model selection was done by best subset selection approach with Akaike Information Criterion (AIC) (24). “The Akaike” Information Criterion (AIC) is a statistical tool used to assess the relative quality of different models by balancing model fit and complexity. It evaluates both the likelihood of the model and the number of parameters, with lower AIC values indicating a more favorable trade-off between goodness of fit and simplicity. Thus, models with lower AIC scores are generally preferred for their more efficient representation of the data. Possible clinically meaningful interactions between variables were investigated. To account for the correlation between participants in the same study site, we expanded the multivariate linear model to a linear mixed-effect model with study site as a random effect and age ranges, gender, educational level, age at HIV diagnosis, ART line, adherence, clinical stages, and viral load ranges as fixed effects. The significance of the random effect was tested by the log-likelihood ratio test. Assumptions of the final linear regression model (linearity, normality, homoscedasticity, and outliers) were examined based on graphical examination. All statistical tests in this report were performed with a complete case analysis approach.
In total, 271 adolescents living with HIV (ALHIV) were initially enrolled during the first phase (T1), with subsequent follow-up of 263 participants at the 6-month mark (T2), and 234 ALHIV at the 12-month mark (T3). From enrolment (T1) to 12-month assessment (T3), the majority of ALHIV were followed up in urban areas, with proportions of 210 (77.5%), 196 (74.5%), and 184 (78.6%) respectively (Table 1). Regarding the age distribution, from T1 to T3, 139 (51.3%) ALHIV were aged 10–14 years, while 161 (61.2%), and 137 (58.5%) fell into the older age category, respectively (Table 1). The median age at diagnosis was 5 years (IQR: 2–10), and the median duration on treatment was 36 months (IQR: 21–81) at T1, 30 months (IQR: 10–55) at T2, and 23 months (IQR: 9–54) at T3. In terms of gender distribution, at all-time points, there were more female participants than males, 151 (55.7%), 145 (55.1%), and 131 (56.0%) from T1 – T3, respectively (Table 1). Regarding educational level, the majority of participants had secondary education across all time points. At T1, 182 (67.2%) were in secondary school, while at T2, the number increased to 184 (70.1%). At T3, 158 (67.5%) participants had secondary education (Table 1).
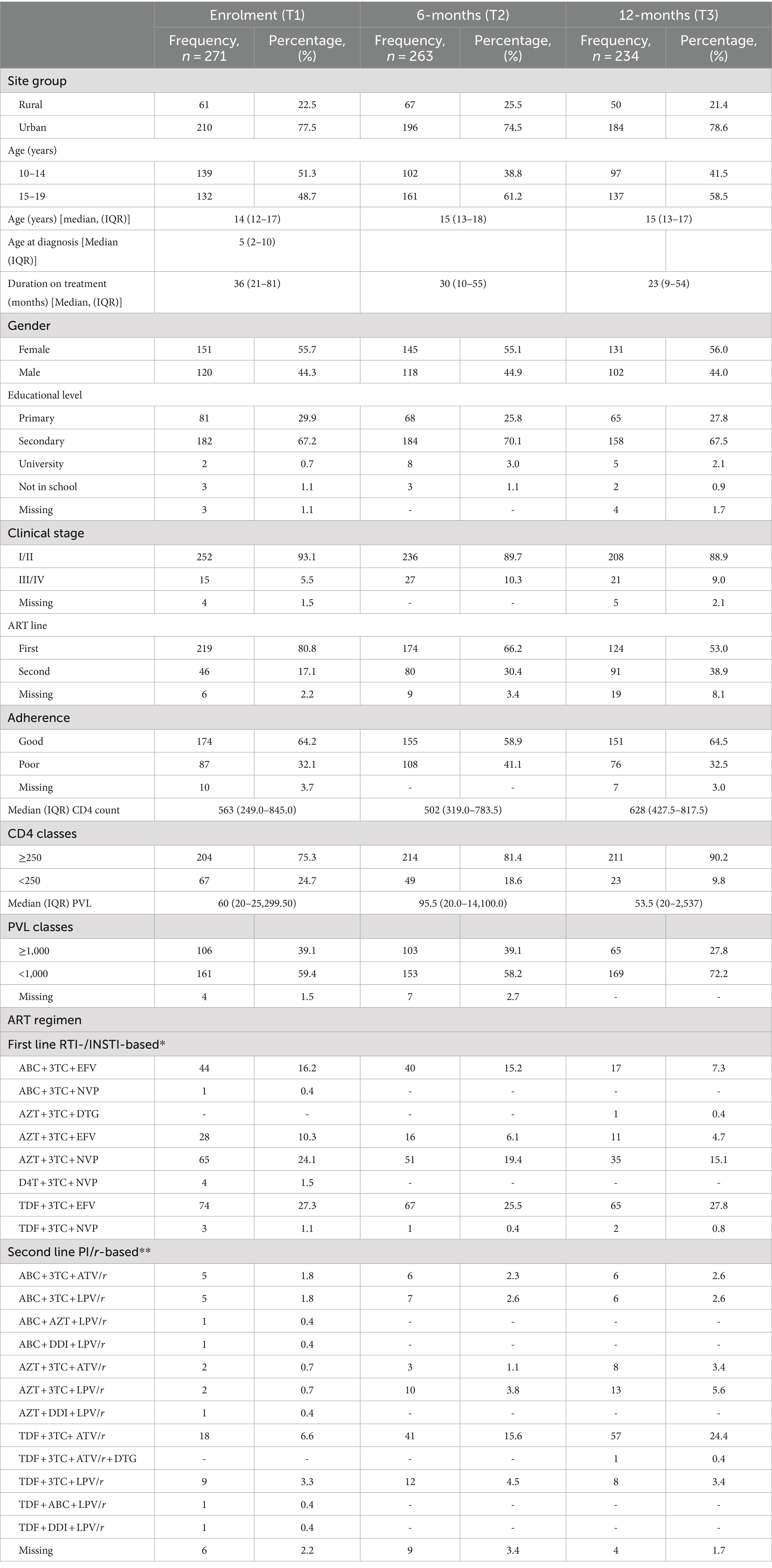
Table 1. Sociodemographic, biological, and clinical characteristics of the study population.
Overall, the majority of participants achieved clinical success, classified in clinical stages I/II, with 252 (93.1%), 236 (89.7%), and 208 (88.9%) participants, respectively. In terms of ART lines, the majority of participants were on the first line, with frequencies of 219 (80.8%), 174 (66.2%), and 124 (53.0%) at each respective time point (Table 1). Regarding adherence levels, the majority of participants reported good adherence, with frequencies of 174 (64.2%), 155 (58.9%), and 151 (64.5%) across the three time points. Furthermore, the median CD4+ count fluctuated over time, with values of 563 (IQR: 249.0–845.0) at T1, 502 (IQR: 319.0–783.5) at T2, and 628 (IQR: 427.5–817.5) at T3. Similarly, the median PVL also varied across time points, with values of 60 (IQR: 20–25,299.50) at T1, 95.5 (IQR: 20.0–14,100.0) at T2, and 53.5 (IQR: 20–2,537) at T3 (Table 1). The ART regimen data showed diverse combinations of first and second-line treatments, with some variations observed over the follow-up periods (Table 1).
In our analysis, we observed several key findings regarding CD4+ count among ALHIV. First, we found a comparable median absolute CD4+ count between male and female adolescents (Figure 1), and this remained consistent across the study duration, with no statistically significant differences detected (p > 0.05) (Table 2). Additionally, comparing absolute CD4+ counts between participants followed up in urban and rural sites across different phases of the study rendered non-significant outcomes (Figure 1; Table 2). Conversely, assessing the effect of longitudinal follow-up phases on immunological responses, we observed a statistically significant difference in CD4+ count across various follow-up phases of the longitudinal study (p = 0.021) (Figure 2; Table 3). Regarding educational level, we observed varying median CD4+ counts, with highest values among participants with primary education, followed by secondary education, and the lowest values among participants with university education (Figure 1; Table 2).
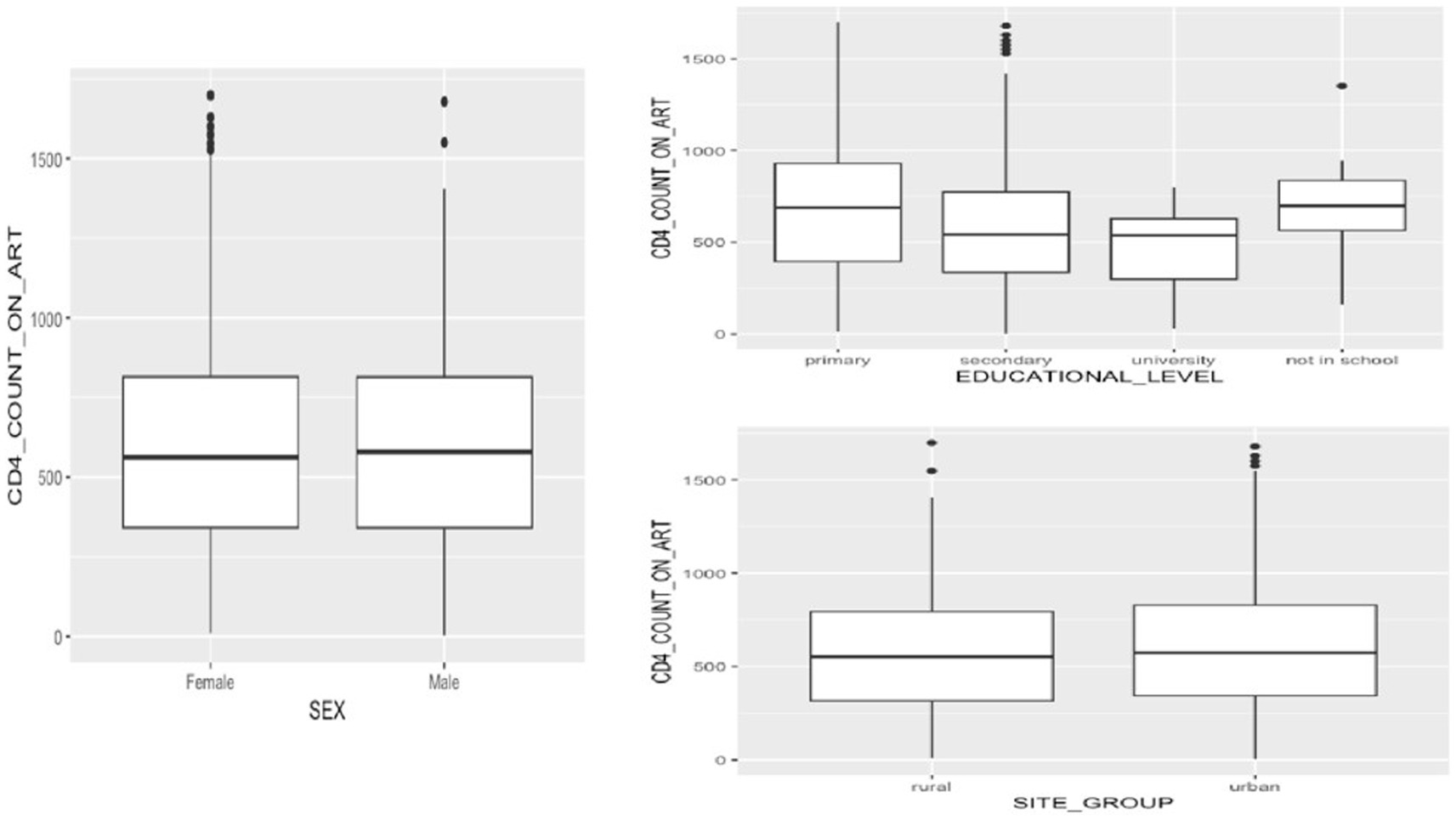
Figure 1. Exploratory analysis of CD4+ count dynamics in adolescents living with HIV: impact of gender (sex), educational level, and study site characteristics.
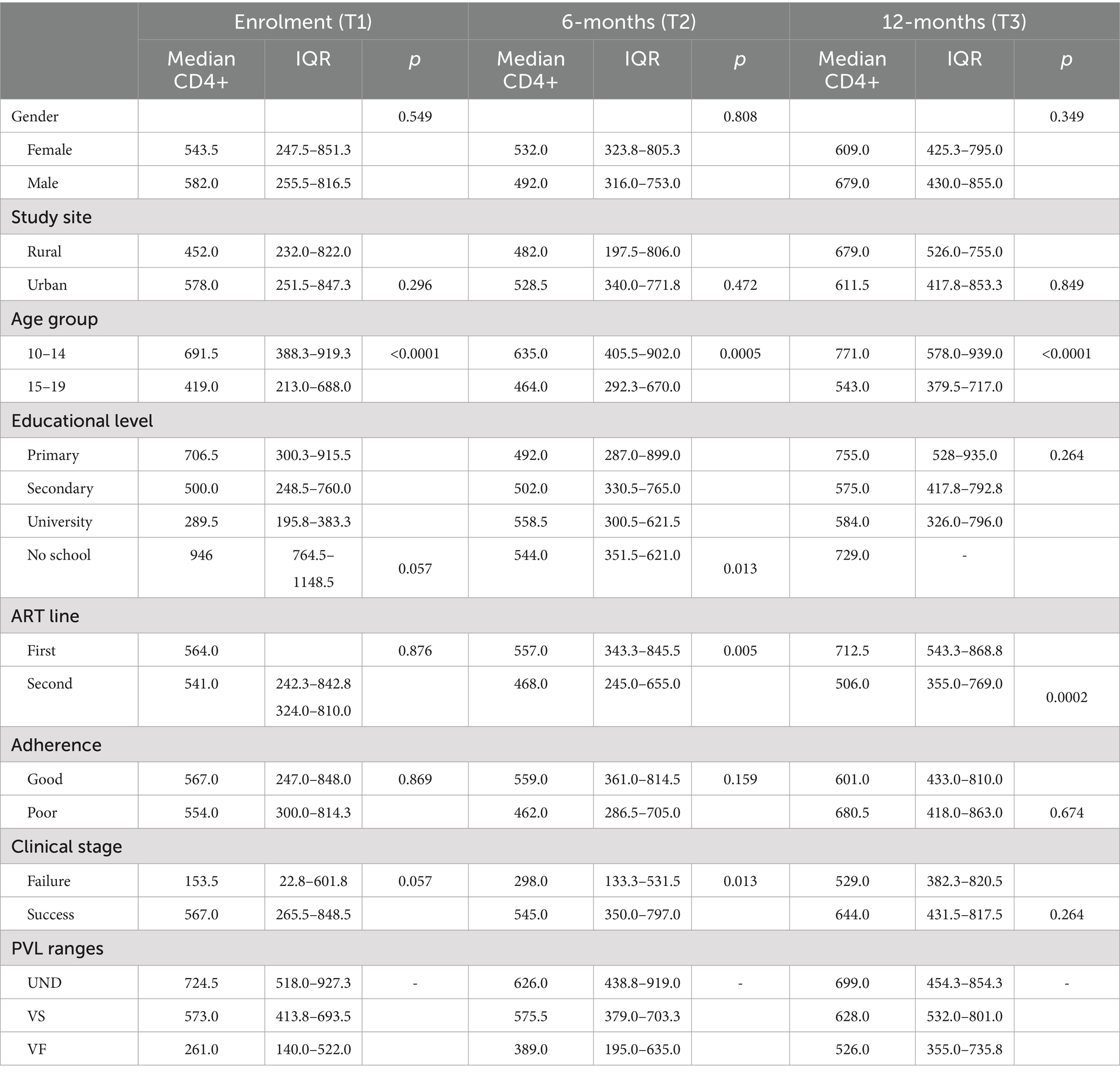
Table 2. Median CD4+ count across study population characteristics.
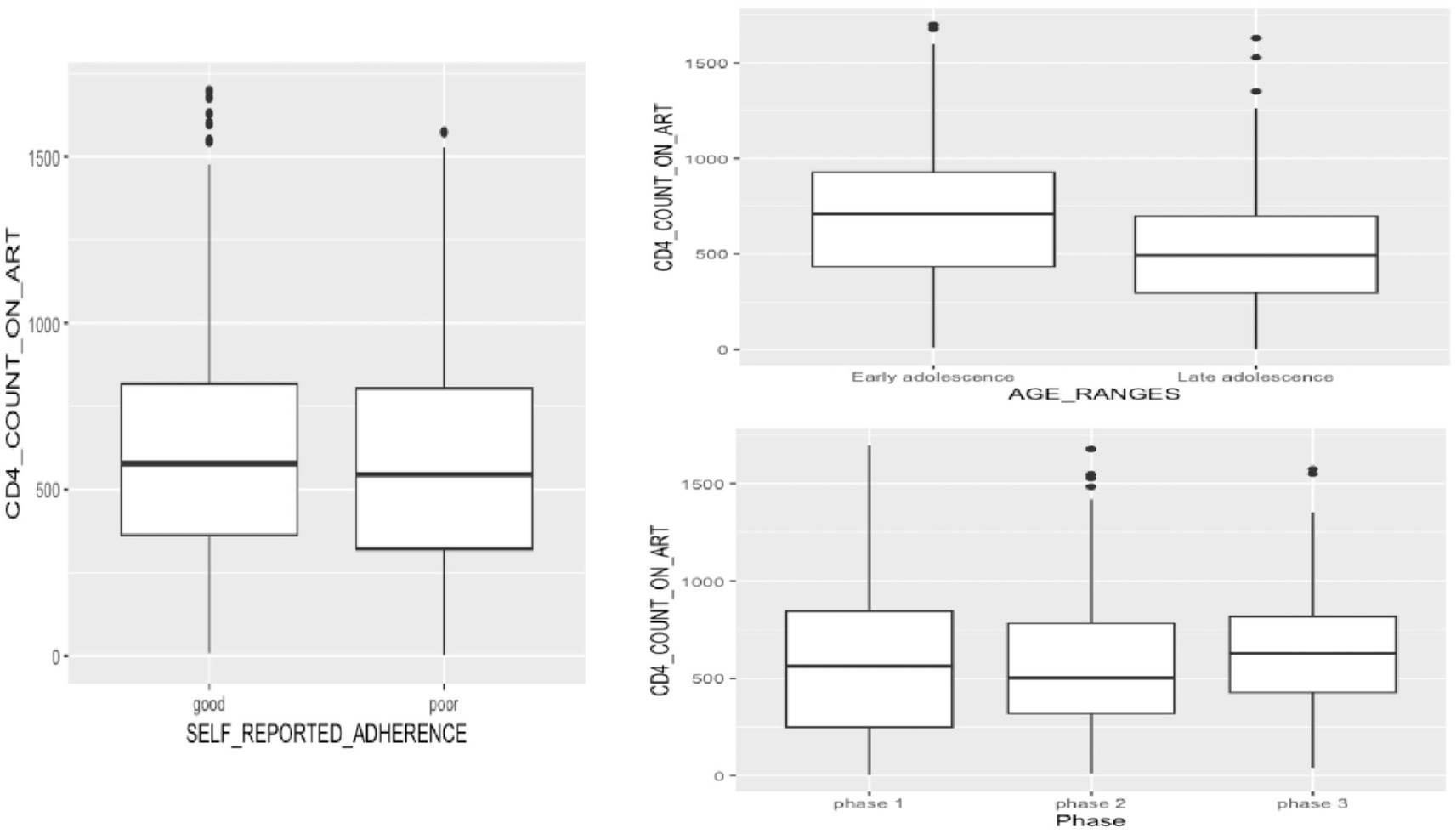
Figure 2. CD4+ count patterns among adolescents living with HIV: influence of self-reported adherence, adolescence age ranges, and follow-up period.
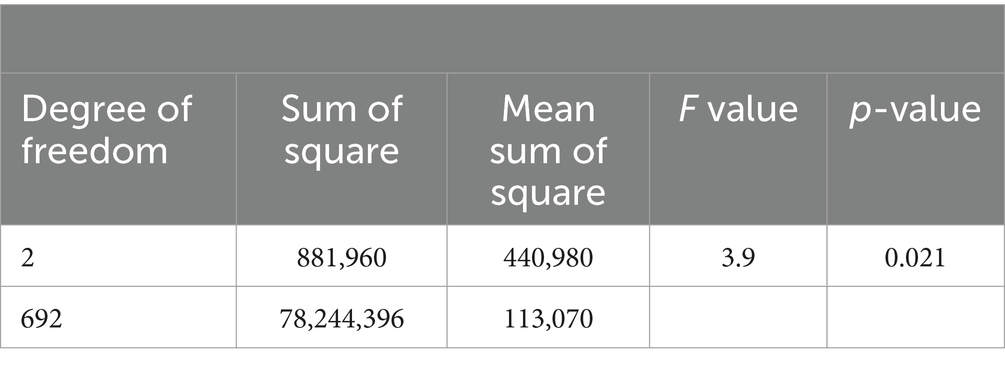
Table 3. Results of two-way ANOVA analysis.
Furthermore, statistical analysis comparing CD4+ counts between participants on first-line ART and those on second-line ART revealed notable differences across the study’s phases. At enrolment, the comparison yielded a non-significant p-value of 0.876, suggesting no substantial distinction in CD4+ counts between the two treatment groups. However, as the study progressed into 6-month and 12-month follow-ups, the p-values decreased significantly to 0.005 and 0.0002, respectively (Figure 3; Table 2). Investigating CD4+ counts between early and late adolescence cohorts revealed significant differences across study phases. At enrolment, a low p-value (p < 0.0001) indicated significant variation, with early-age adolescents having higher median CD4+ counts compared to older adolescents. Similar trends persisted at 6-month (p = 0.0005) and 12-month (p < 0.0001) follow-up, underlining persistent disparities between early and late adolescence groups (Figure 2; Table 2). Moreover, participants with good adherence to ART exhibited higher median CD4 counts compared to those with poor adherence (Figure 2). However, these differences were non-significant across all three phases of the study (Table 2).
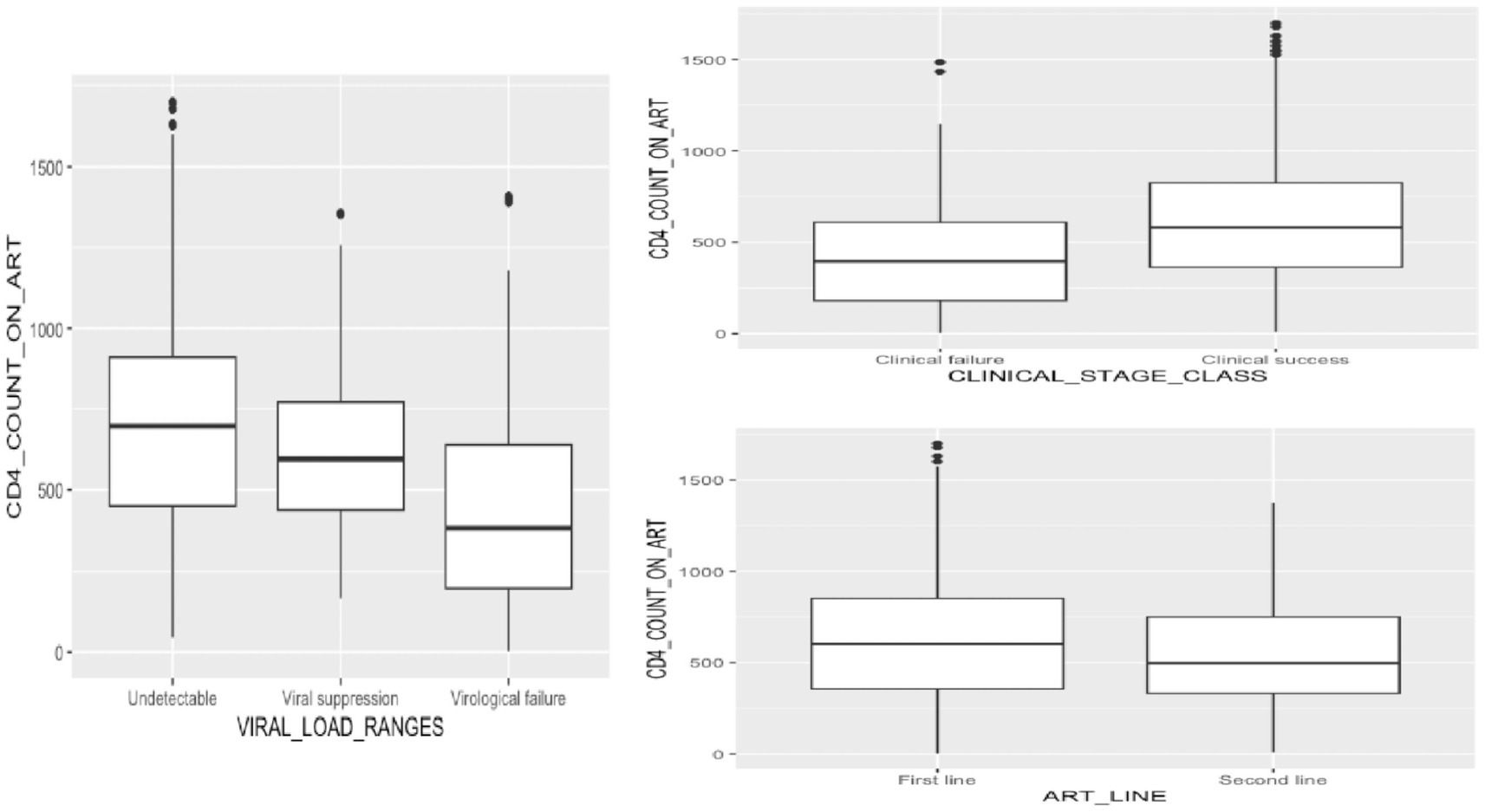
Figure 3. CD4+ count dynamics in adolescents living with HIV: effect of clinical, virological, and antiretroviral treatment regimen characteristics.
Comparing CD4+ count among ALHIV classified based on their clinical status revealed varying levels of significance (Figure 3). In phase 1, a potential difference in CD4 count between ALHIV classified as clinically successful versus those classified as clinically failed was suggested, however, this analysis had only a borderline significance (p = 0.0572). Phase 2 yielded a more significant result, with a p-value of 0.0125, but in phase 3, the comparison showed non-significant results, with a p-value of 0.2637, suggesting no significant difference in CD4+ count based on clinical outcomes success (Table 2). Finally, assessing the impact of plasma viral load (PVL) ranges on CD4+ count demonstrated a statistically significant effect [F(2, 692) = 58.89, p < 0.001] (Table 4). Further assessment across the three levels of PVL (viral suppression, virological failure, and undetectable viremia) revealed statistically significant variations in CD4+ count across these groups (Figure 3). The p-values obtained from the post hoc test were 0.0119, <0.001, and < 0.001, corresponding to the pairwise comparisons between viral suppression and undetectable viremia, virological failure and undetectable viremia, and virological failure and viral suppression, respectively (Table 5).
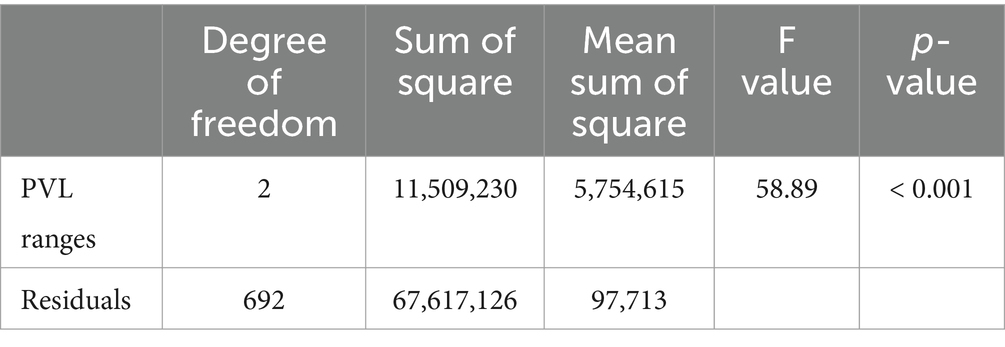
Table 4. Results of repeated measures two-way ANOVA analysis.

Table 5. Results of Tukey HSD tests.
Assessing the relationship between age and CD4+ count among ALHIV revealed that there was a statistically significant moderate negative correlation between absolute CD4+ count on antiretroviral therapy and adolescence age (correlation coefficient, r = −0.28, confidence interval = −0.35 to −0.21, p-value <0.0001) (Figure 4). Conversely, there was a statistically significant weak positive correlation between CD4+ count on ART and duration of treatment (r = 0.15, CI = 0.07–0.23, p = 0.0001) (Figure 4). A correlation test between CD4+ count and age at HIV diagnosis yielded a weak negative correlation between CD4+ count on antiretroviral therapy and increasing age at HIV diagnosis, but this correlation was not statistically significant (r = −0.11, CI = −0.25 – 0.04, p = 0.143) (Figure 4).
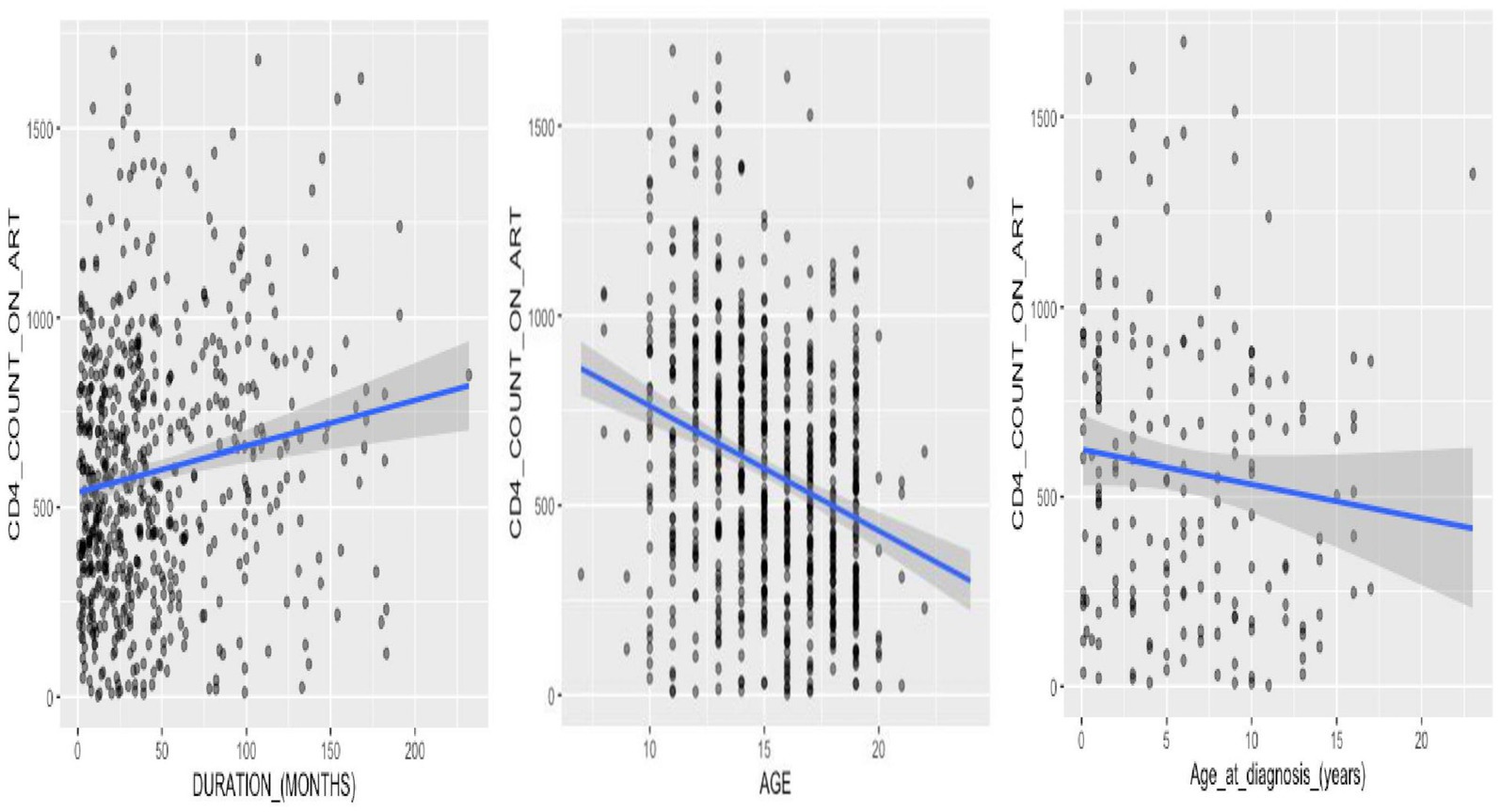
Figure 4. Correlation analysis of CD4+ count dynamics in adolescent HIV patients: assessing associations with age at HIV diagnosis, age, and duration of treatment.
The results of the final multivariable linear regression model with and without study site (as random effect) were presented in Table 6. Details about the model selection were presented in the Supplementary Table S1. Supplementary Figure S1 illustrates the validation of model assumptions, confirming linearity, normality, homoscedasticity, and the absence of outliers through graphical examination. A linear regression model was applied to analyze the relationship between CD4+ count on ART and various predictors including site group, gender, age ranges, educational level, age at diagnosis, ART line, duration on treatment, self-reported adherence, clinical stage class, viral load ranges, and the interaction between sex and educational level (Table 6). Among the predictors, males exhibited a decrease in CD4+ count on ART compared to females [Estimate: −198.07 (95% CI: −376.81 to −19.32), p < 0.001]. Similarly, participants in the late adolescence age range had lower CD4+ counts compared to those in early adolescence [−185.93 (−306.30 to −65.56), p = 0.003]. Notably, participants with virological failure had significantly lower CD4+ counts compared to those with undetectable viral loads [−354.21 (−466.96–241.47), p < 0.0001] (Table 6). Moreover, the interaction between gender and educational level showed marginal significance, suggesting that there may be some interaction effect between being male and having a secondary educational level [206.29 (−0.01–0.01), p = 0.062]. However, this interaction effect was not statistically significant (Table 6).
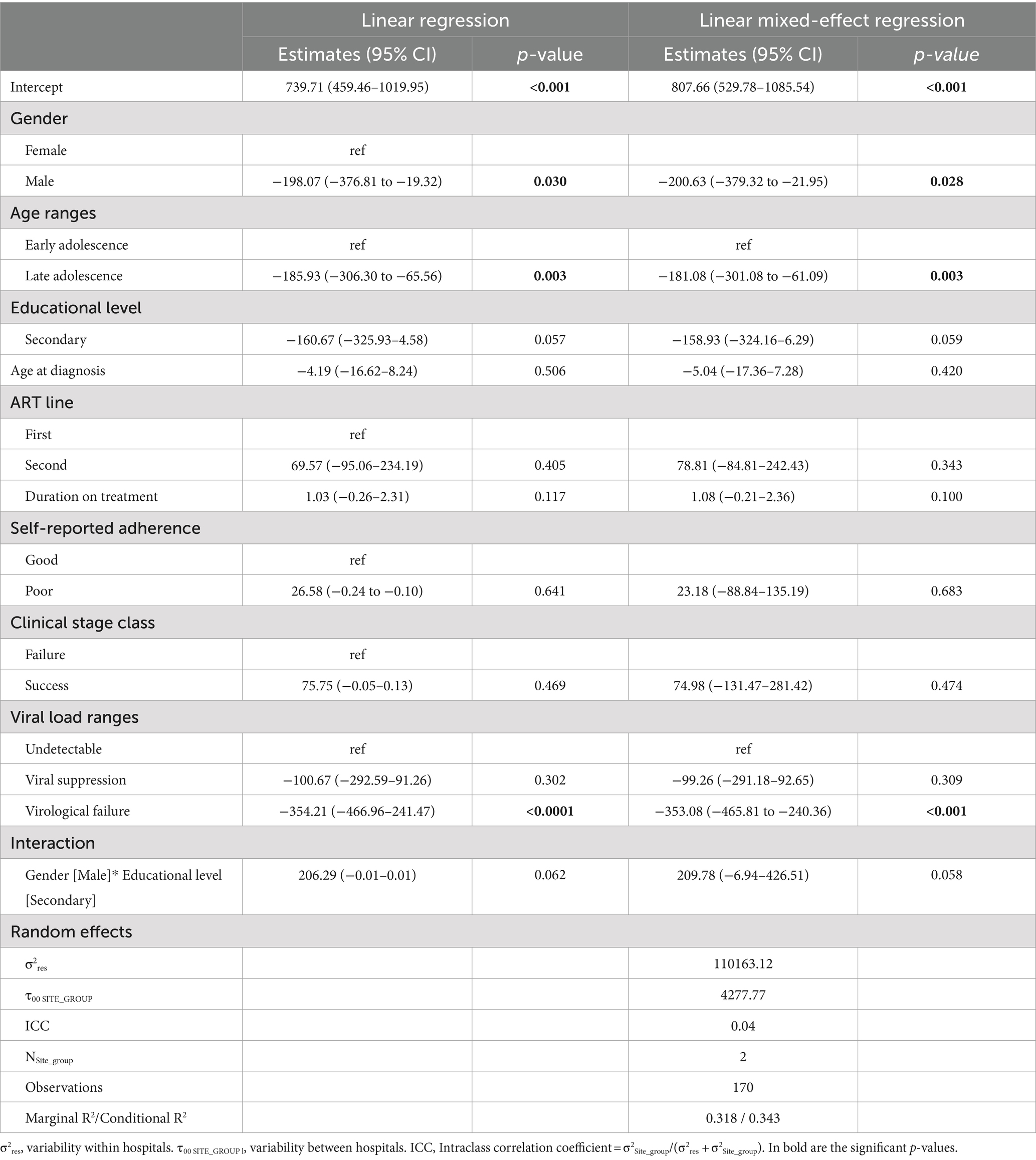
Table 6. Multivariate linear regression for CD4+ count with and without study site as random effect.
The linear regression model was extended to a linear mixed-effects regression model with random intercepts specified for each participant’s site group to account for variability between study sites (Table 6). The summary of the model revealed several significant fixed effects. Being male was associated with a decrease in CD4+ count compared to females, [−200.63 (−379.32 to −21.95), p = 0.028]. Similarly, individuals in the late adolescence age range [−181.08 (−301.08 to −61.09), p = 0.003] and those with virological failure [−353.08 (−465.81 to −240.36), p < 0.001] exhibited lower CD4+ counts compared to their respective reference categories. Furthermore, the interaction between gender and educational level showed a marginally significant effect, suggesting that the association between male gender and CD4+ count may vary depending on whether individuals have attained a secondary education level [209.78 (−6.94–426.51), p = 0.058] (Table 6).
Overall, the model demonstrated moderate explanatory power, with a marginal R-squared value of 0.318, indicating that approximately 31.8% of the variance in CD4+ count on ART was explained by the predictors included in the model (Table 6). The conditional R-squared value was 0.343 (34.3%), suggesting that the model’s explanatory power remains robust after adjusting for the number of predictors. The F-statistic was highly significant (p < 0.001), indicating that the overall model was statistically significant in predicting CD4+ count on ART. In addition, the random effects analysis revealed significant variability between study sites, with a variance of 4277.77. This underscored the importance of accounting for site-level differences when analyzing CD4+ count data in this context.
Our study identified important factors that influence CD4+ counts among perinatally-infected adolescents living with HIV (ALHIV) and the importance of considering demographic, clinical, and contextual factors in HIV care and management. Our findings suggest that tailored interventions addressing gender disparities, age at diagnosis, educational attainment, and healthcare delivery systems are crucial for optimizing health outcomes and improving the well-being of ALHIV.
Most of the study participants hailed from urban areas, possibly linked to improved access to healthcare services, including ART clinics and support systems, compared to their counterparts in rural areas. This observation aligns with findings from previous studies conducted in Cameroon (25, 26) but contrasts with those reported in Kenya (27). Urban settings typically have more developed healthcare infrastructure and resources, which may contribute to higher retention rates among ALHIV (27). However, the shifting demographic trends observed in our study, with an increasing proportion of older adolescents’ overtime, suggest evolving dynamics that warrant careful consideration. Older adolescents may encounter distinct challenges related to HIV management, treatment adherence, or psychosocial support needs compared to their younger counterparts (28, 29). Understanding of these age-specific nuances is essential for tailoring interventions and support ART services effectively to meet the diverse needs of ALHIV across different age groups (30) a finding similar to other studies in Cameroon (27, 31).
Furthermore, our results reveal consistent patterns in the participants’ demographic and educational characteristics over time. The median age of five years at HIV diagnosis among perinatally infected adolescents raises concerns about missed opportunities for early treatment, underscoring the importance of enhancing HIV testing and prevention efforts, particularly among at-risk populations like perinatally infected adolescents as seen in other countries (27, 32). Moreover, the greater representation of female participants compared to males may indicate gender-specific disparities in healthcare-seeking behaviors or HIV prevalence among ALHIV, consistent with national data (33–36). This contrasts with the predominance of males reported in a European study (37). The predominance of participants at the secondary educational level, and the marginally significant interaction between male gender and attainment of this level of education regarding CD4+ count suggest that educational attainment may influence healthcare access, ART adherence, or other factors affecting immunological responses, which may vary between males and females. Further research is needed to fully understand this association.
In terms of clinical outcomes, most participants achieved clinical success, with the majority on first-line RTI-based ART regimens and reporting good adherence. However, this raises concerns about prolonged exposure to suboptimal regimens with low barriers to drug resistance, a significant consideration in HIV treatment (38–40). Consistent with findings from similar settings (31, 38, 41). Moreover, the fluctuations observed in CD4+ counts suggest dynamic changes in immune response and treatment effectiveness over the follow-up periods. Analysis of the ART regimens administered revealed a variety of first-and second-line treatment combinations, consistent with findings from similar settings (39, 42). This diversity emphasizes the significance of a personalized therapy approach tailored to factors like HIV drug resistance, side effects, and patient response, all crucial for enhancing treatment outcomes. These findings highlight the dynamic nature of HIV care, emphasizing the importance of continuous monitoring of CD4+ cell counts, viral loads, and treatment plans to ensure optimal clinical outcomes for ALHIV receiving ART (43, 44).
Analyzing median CD4+ counts across different study population characteristics revealed several key findings. The absence of a significant difference in the median CD4+ counts between males and females suggests that gender may not have a significant impact on CD4+ fluctuations over time (45), contrasting with studies indicating women’s susceptibility to immunological failure and virological failure (45–49). Furthermore, the lack of significant disparity in CD4+ counts between urban and rural study sites implies that location may not influence CD4+ counts among ALHIV, potentially due to effective adherence counseling provided at both sites. Unlike findings reported in Zimbabwe where CD4+ counts were higher in urban settings (50).
The variation in median CD4+ counts across educational levels, with the highest values observed among participants in primary education, followed by secondary education, and the lowest among those with university education, prompts intriguing considerations. One plausible explanation is that adolescents at the primary education level may benefit from enhanced parental/guardian oversight, contributing to better adherence and health management. Meanwhile, older adolescents pursuing higher education may encounter heightened social stigma and challenges associated with disclosing their HIV status, potentially impacting their psychological well-being and treatment adherence (51, 52).
Investigating CD4+ counts between early and late adolescence cohorts demonstrated a statistically significant difference overtime (40, 53–55). This could be due to physiological changes, variations in treatment adherence, healthcare access, and psychosocial factors like stress, stigma, and mental health issues. Therefore, it is important to consider age-related factors when assessing immune health and treatment response among ALHIV to identify and tackle the unique needs and challenges faced by different adolescent age groups.
Our study findings suggested that plasma viral load (PVL) levels had a significant impact on CD4+ counts among ALHIV. Participants with viral suppression had different CD4+ counts compared to those with undetectable viremia or virological failure. The pairwise comparisons further emphasized these differences, indicating that maintaining viral suppression is crucial for preserving immune health and optimizing treatment outcomes. Effective management of PVL through ART is essential to achieve and sustain viral suppression, which in turn helps to maintain or improve CD4+ counts. Therefore, strategies aimed at achieving and maintaining viral suppression should be prioritized in HIV treatment and care protocols to ensure better health outcomes for ALHIV (13, 56–58).
Further analysis revealed several significant fixed effects on immune responses. Being male was associated with a decrease in CD4+ count compared to females which aligns with studies in other African countries (45, 59, 60). This could be attributed to females generally mounting stronger immune responses to infections, including HIV, as well as potential differences in healthcare-seeking behavior or treatment adherence (61, 62). Similarly, the lower CD4+ counts among ALHIV in the late adolescence age range could be attributed to various factors. These include a longer duration of HIV infection leading to more advanced disease progression (63, 64), increased social and emotional stress, and potential decline in treatment adherence as adolescents transition into adulthood. Additionally, ALHIV experiencing virological failure exhibited lower CD4+ counts which may be linked to poor ART adherence, drug resistance, suboptimal treatment regimens, or challenges in accessing healthcare services (33, 38, 65).
More still, the interaction between gender and educational level showed a marginally significant effect, suggesting that the relationship between male gender and CD4+ count may vary depending on whether individuals have attained a secondary education level. This could be due to socioeconomic factors associated with education, such as access to healthcare services, or lifestyle factors. However, further research is needed to fully understand the underlying mechanisms driving this interaction (37).
The results highlight the importance of prioritizing close immune monitoring in the perinatal ALHIV population, advocating for frequent CD4+ count tests to optimize strategies for rapid immune recovery, as recommended by WHO in 2017 (66, 67). While viral load (VL) testing is considered the gold standard for monitoring treatment response, it is crucial for countries to maintain their CD4+ cell count testing capacity, alongside efforts to provide quality VL testing to support comprehensive and effective HIV care and management (8).
In our longitudinal study, missing laboratory data and participant loss to follow-up presented challenges, as methods like multiple imputation and sensitivity analysis were not used to evaluate the impact of missing data. This limitation may have affected data quality and the applicability of findings to the target population. However, the study’s strengths included a multi-time point follow-up, personalized monitoring, and repeated assessments, ensuring robust within-program comparisons of immunovirological responses and minimizing potential confounders. Despite these strengths, relying on complete case analysis may have introduced bias, highlighting the need for more advanced methods to handle missing data.
In a nutshell, these findings emphasize the importance of prioritizing close immune monitoring for ALHIV, particularly those in the older adolescent age category, of male gender, and those experiencing virological failure. It is imperative that the care strategy, as recommended by WHO, for such cases includes CD4+ count assessment, given its significance as the most relevant immunological parameter correlated with virological response in this population.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by National Ethical Committee for Human Health Research of Cameroon (CNERSH/No: 2018/01/981/CE/CNERSH/SP). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
WT: Conceptualization, Data curation, Methodology, Writing – original draft, Writing – review & editing. AMK: Writing – original draft, Writing – review & editing. ADN: Writing – original draft, Writing – review & editing. MS: Conceptualization, Project administration, Writing – original draft, Writing – review & editing. YB: Writing – review & editing. CC: Writing – review & editing. EN: Writing – review & editing, Writing – original draft. DT: Writing – review & editing. GT: Writing – review & editing. BD: Writing – review & editing. RBN: Writing – review & editing. MT: Writing – original draft, Writing – review & editing. GB: Writing – review & editing. SD: Methodology, Writing – review & editing. ACK: Methodology, Writing – review & editing. TT: Writing – review & editing. DA: Writing – review & editing. N-KE: Writing – review & editing. RM: Writing – review & editing. RK: Writing – review & editing. SS: Supervision, Writing – review & editing. RNN: Supervision, Writing – review & editing. VC: Supervision, Validation, Visualization, Writing – review & editing. FC-S: Supervision, Validation, Writing – review & editing. AN: Funding acquisition, Supervision, Validation, Writing – review & editing. JF: Funding acquisition, Investigation, Methodology, Visualization, Writing – original draft, Writing – review & editing.
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. The study was financially supported by the EDCTP2, the European and Developing Countries Clinical Trial Partnership, CDF-TMA 1027.
We thank the staff of the study sites for assisting in the data collection and in the enrolment of participants.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2024.1457501/full#supplementary-material
ALHIV, Adolescent living with HIV; ART, Antiretroviral therapy; CIRCB, Chantal Biya International Reference Center for Research on HIV/AIDS Prevention and Management; EDTA, Ethylene diamine tetra acetic acid; HIV, Human immunodeficiency virus; VL, Viral load; VS, Virological suppression; VF, Virological failure; UNAIDS, United Nation’s programme on HIV/AIDS; WHO, World Health Organization.
1. UNAIDS . (n.d.) Statistiques mondiales sur le VIH. Available online at: https://www.unaids.org/sites/default/files/media_asset/UNAIDS_FactSheet_en.pdf (Accessed September 23, 2020)
2. Slogrove, AL, Mahy, M, Armstrong, A, and Davies, M-A. Living and dying to be counted: what we know about the epidemiology of the global adolescent HIV epidemic. J Int AIDS Soc. (2017) 20:21520. doi: 10.7448/IAS.20.4.21520
4. Bekker, L-G, and Hosek, S. HIV and adolescents: focus on young key populations. J Int AIDS Soc. 18:20076. doi: 10.7448/IAS.18.2.20076
5. Fish, R, Judd, A, Jungmann, E, O'Leary, C, and Foster, CHIV Young Persons Network (HYPNet). Mortality in perinatally HIV-infected young people in England following transition to adult care: an HIV young persons network (HYPNet) audit. HIV Med. (2014) 15:239–44. doi: 10.1111/hiv.12091
6. WHO . (2023) Consolidated guidelines on the use of antiretroviral drugs for treating and preventing HIV infection. WHO. Available online at: https://www.who.int/hiv/pub/guidelines/arv2013/en/ (Accessed September 23, 2020)
7. Author . Scaling up antiretroviral therapy in resource-limited settings: guidelines for a public health approach. Executive summary. IAPAC Mon. (2002) 8:168–75.
8. WHO . (2013) The use of antiretroviral drugs for treating and preventing HIV infection. Available online at: https://apps.who.int/iris/bitstream/handle/10665/85322/WHO_HIV_2013.7_eng.pdf (Accessed September 25, 2020)
9. WHO . (2015) Guidelines on when to start antiretroviral therapy and pre-exposure prophylaxis for HIV. Available online at: https://www.who.int/hiv/pub/arv/chapter4.pdf?ua=1 (Accessed September 25, 2020)
10. Ahn, JY, Boettiger, D, Law, M, Kumarasamy, N, Yunihastuti, E, Chaiwarith, R, et al. Effects of CD4 monitoring frequency on clinical endpoints in clinically stable HIV-infected patients with viral suppression. J Acquir Immune Defic Syndr. (1999) 2015:e85–92. doi: 10.1097/QAI.0000000000000634
11. HIV . (2022) Plasma HIV-1 RNA (Viral Load) and CD4 Count Monitoring | Laboratory Testing | Adult and Adolescent ARV. Available online at: https://clinicalinfo.hiv.gov/en/guidelines/adult-and-adolescent-arv/plasma-hiv-1-rna-viral-load-and-cd4-count-monitoring?view=full (Accessed September 25, 2020)
12. World Health Organization . (2017) Guidelines for managing advanced HIV disease and rapid initiation of antiretroviral therapy. Available online at: http://www.ncbi.nlm.nih.gov/books/NBK475977/ (Accessed September 25, 2020)
13. Smurzynski, M, Wu, K, Benson, CA, Bosch, RJ, Collier, AC, Koletar, SL, et al. Relationship between CD4+ T-cell counts/HIV-1 RNA plasma viral load and AIDS defining events among persons followed in the ACTG longitudinal linked randomized trials (ALLRT) study. J Acquir Immune Defic Syndr. (1999) 2010:117–27. doi: 10.1097/QAI.0b013e3181e8c129
14. Nou, E, Lo, J, and Grinspoon, SK. Inflammation, immune activation, and cardiovascular disease in HIV. AIDS Lond Engl. (2016) 30:1495–509. doi: 10.1097/QAD.0000000000001109
15. Schaecher, KL . The importance of treatment adherence in HIV. Am J Manag Care. (2013) 19:s231–7.
16. McKinnon, LR, Kimani, M, Wachihi, C, Nagelkerke, NJ, Muriuki, FK, Kariri, A, et al. Effect of baseline HIV disease parameters on CD4+ T cell recovery after antiretroviral therapy initiation in Kenyan women. PLoS One. (2010) 5:e11434. doi: 10.1371/journal.pone.0011434
17. WHO . (2022) AWHO Prequalification of Diagnostics Programme PUBLIC REPORT. Available online at: https://extranet.who.int/prequal/sites/default/files/whopr_files/PQDx_0099-032-00_PimaCD4-Test_v6.0.pdf (Accessed August 10, 2024)
18. Abbott . (2011) RealTime HIV-1 Viral Load Assay | Abbott Molecular. Available online at: https://www.molecular.abbott/us/en/products/infectious-disease/realtime-hiv-1-viral-load (Accessed August 10, 2024)
19. Fokam, J, Salpini, R, Santoro, M, Cento, V, D'Arrigo, R, Gori, C, et al. Performance evaluation of an in-house human immunodeficiency virus type-1 protease-reverse transcriptase genotyping assay in Cameroon. Arch Virol. (2011) 156:1235–43. doi: 10.1007/s00705-011-0982-3
20. Qiagen . (2013) QIAmp DNA Kits | Genomic DNA Isolation | QIAGEN. Available online at: https://www.qiagen.com/us/products/discovery-and-translational-research/dna-rna-purification/dna-purification/genomic-dna/qiaamp-dna-kits (Accessed August 10, 2024)
21. Taieb, F, Madec, Y, Cournil, A, and Delaporte, E. Virological success after 12 and 24 months of antiretroviral therapy in sub-Saharan Africa: comparing results of trials, cohorts and cross-sectional studies using a systematic review and meta-analysis. PLoS One. (2017) 12:e0174767. doi: 10.1371/journal.pone.0174767
22. World Health Organization . (2007). WHO case definitions of HIV for surveillance and revised clinical staging and immunological classification of HIV-related disease in adults and children. World health Organization. Available online at: https://apps.who.int/iris/handle/10665/43699 (Accessed September 28, 2020)
23. World Health Organization . (2017) What’s new in treatment monitoring: viral load and CD4 testing July 2017. Available online at: https://apps.who.int/iris/bitstream/handle/10665/255891/WHO-HIV-2017.22-eng.pdf?sequence=1 (Accessed September 25, 2020)
24. Wiley . (2018) Variable selection – A review and recommendations for the practicing statistician – Heinze −2018- Biometrical Journal-Wiley Online Library. Available online at: https://onlinelibrary.wiley.com/doi/full/10.1002/bimj.201700067 (Accessed April 8, 2024)
25. Dobseu Soudebto, RS, Fokam, J, Kamgaing, N, Fainguem, N, Semengue, ENJ, Tchouaket, MCT, et al. Determinants of Immunovirological response among children and adolescents living with HIV-1 in the central region of Cameroon. Trop Med Infect Dis. (2024) 9:48. doi: 10.3390/tropicalmed9020048
26. Tendongfor, N, Fokam, J, Chenwi, CA, Nwabo, FLT, Nangmo, A, Debimeh, N, et al. Determinants of survival of adolescents receiving antiretroviral therapy in the Centre region of Cameroon: a multi-centered cohort-analysis. AIDS Res Ther. 20:584. doi: 10.1186/s12981-023-00584-2
27. Kose, J, Tiam, A, Siamba, S, Lenz, C, Okoth, E, Wolters, T, et al. Clinical outcomes among adolescents living with HIV in Kenya following initiation on antiretroviral treatment. PLOS Glob Public Health. (2022) 2:e0000094. doi: 10.1371/journal.pgph.0000094
28. Audi, C, Jahanpour, O, Antelman, G, Guay, L, Rutaihwa, M, van de Ven, R, et al. Facilitators and barriers to antiretroviral therapy adherence among HIV-positive adolescents living in Tanzania. BMC Public Health. (2021) 21:2274. doi: 10.1186/s12889-021-12323-1
29. Gitahi, N, Camlin, C, Mwania, V, Ngure, K, Auerswald, C, Bukusi, E, et al. Psychosocial needs among older perinatally infected adolescents living with HIV and transitioning to adult care in Kenya. PLoS One. 15:233451. doi: 10.1371/journal.pone.0233451
30. Adams, C, Kiruki, M, Karuga, R, Otiso, L, Graham, SM, and Beima-Sofie, KM. “Your status cannot hinder you”: the importance of resilience among adolescents engaged in HIV care in Kenya. BMC Public Health. (2022) 22:1272. doi: 10.1186/s12889-022-13677-w
31. Wlrt, P, Njume, D, Ndip, RN, Takou, D, Santoro, M-M, Chenwi, C, et al. Genotypic resistance testing improves antiretroviral treatment outcomes in a cohort of adolescents in Cameroon: implications in the dolutegravir-era. J Public Health Afr. (2023) 14:2612. doi: 10.4081/jphia.2023.2612
32. Ang, LW, Toh, MPHS, Boudville, IC, Wong, CS, Archuleta, S, Lee, V, et al. Epidemiological factors associated with the absence of previous HIV testing among HIV-positive persons in Singapore, 2012–2017. BMJ Open. (2021) 11:e050133. doi: 10.1136/bmjopen-2021-050133
33. Fokam, J, Takou, D, Njume, D, Pabo, W, Santoro, MM, Njom Nlend, AE, et al. Alarming rates of virological failure and HIV-1 drug resistance amongst adolescents living with perinatal HIV in both urban and rural settings: evidence from the EDCTP READY-study in Cameroon. HIV Med. (2021) 22:567–80. doi: 10.1111/hiv.13095
34. Fokam, J, Billong, SC, Jogue, F, Ndiang, SMT, Motaze, ACN, Paul, KN, et al. Immuno-virological response and associated factors amongst HIV-1 vertically infected adolescents in Yaoundé-Cameroon. PLoS One. (2017) 12:e0187566. doi: 10.1371/journal.pone.0187566
35. HIV and Women . (2023) Be in the KNOW. Available online at: https://www.beintheknow.org/understanding-hiv-epidemic/community/hiv-and-women (Accessed March 27, 2024)
36. Abba, A, Fokam, J, Kamgaing, RS, Yimga, JF, Ka'e, AC, Nka, AD, et al. Correlation between the immuno-virological response and the nutritional profile of treatment-experienced HIV-infected patients in the east region of Cameroon. PLoS One. (2021) 16:e0229550. doi: 10.1371/journal.pone.0229550
37. Novelli, S, Delobel, P, Bouchaud, O, Avettand-Fenoel, V, Fialaire, P, Cabié, A, et al. Enhanced immunovirological response in women compared to men after antiretroviral therapy initiation during acute and early HIV-1 infection: results from a longitudinal study in the French ANRS primo cohort. J Int AIDS Soc. (2020) 23:e25485. doi: 10.1002/jia2.25485
38. Djiyou, ABD, Penda, CI, Madec, Y, Ngondi, GD, Moukoko, A, Varloteaux, M, et al. Viral load suppression in HIV-infected adolescents in Cameroon: towards achieving the UNAIDS 95% viral suppression target. BMC Pediatr. (2023) 23:119. doi: 10.1186/s12887-023-03943-0
39. Buh, A, Deonandan, R, Gomes, J, Krentel, A, Oladimeji, O, Yaya, S, et al. Prevalence and factors associated with HIV treatment non-adherence among people living with HIV in three regions of Cameroon: a cross-sectional study. PLoS One. (2023) 18:e0283991. doi: 10.1371/journal.pone.0283991
40. Togna Pabo, WLR, Fokam, J, Njume, D, Takou, D, Santoro, M-M, Nyasa, RB, et al. HIV-1 subtype diversity and immuno-virological outcomes among adolescents failing antiretroviral therapy in Cameroon: a cohort study. PLoS One. (2023) 18:e0293326. doi: 10.1371/journal.pone.0293326
41. Villiera, JB, Katsabola, H, Bvumbwe, M, Mhango, J, Khosa, J, Silverstein, A, et al. Factors associated with antiretroviral therapy adherence among adolescents living with HIV in the era of isoniazid preventive therapy as part of HIV care. PLoS Glob Public Health. (2022) 2:e0000418. doi: 10.1371/journal.pgph.0000418
42. van Zyl, G, Bale, MJ, and Kearney, MF. HIV evolution and diversity in ART-treated patients. Retrovirology. (2018) 15:14. doi: 10.1186/s12977-018-0395-4
43. Leeme, Tshepo B., Mine, Madisa, Lechiile, Kwana, Mulenga, Fredah, Mosepele, Mosepele, and Mphoyakgosi, Thongbotho. (2020) Utility of CD4 Count Testing in the Era of Universal ART: An Analysis of Routine Laboratory Data in Botswana-PMC. Available online at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7736557/ (Accessed March 28, 2024)
44. HIV . (n.d.) Plasma HIV-1 RNA (Viral Load) and CD4 Count Monitoring. Available online at: https://clinicalinfo.hiv.gov/en/guidelines/hiv-clinical-guidelines-adult-and-adolescent-arv/plasma-hiv-1-rna-cd4-monitoring (Accessed March 28, 2024)
45. Maskew, M, Brennan, AT, Westreich, D, McNamara, L, MacPhail, AP, Fox, MP, et al. Gender differences in mortality and CD4 count response among virally suppressed HIV-positive patients. J Women's Health. (2013) 22:113–20. doi: 10.1089/jwh.2012.3585
46. Braitstein, P, Boulle, A, Nash, D, et al. Gender and the use of antiretroviral treatment in resource-constrained settings: findings from a multicenter collaboration. J Women's Health. (2002) 2008:47–55. doi: 10.1089/jwh.2007.0353
47. Kagee, A, and Nel, A. Assessing the association between self-report items for HIV pill adherence and biological measures. AIDS Care. (2012) 24:1448–52. doi: 10.1080/09540121.2012.687816
48. Jesson, J, Crichton, S, Quartagno, M, et al. Growth and CD4 patterns of adolescents living with perinatally acquired HIV worldwide, a CIPHER cohort collaboration analysis. J Int AIDS Soc. (2022) 25:e25871. doi: 10.1002/jia2.25871
49. Lemly, DC, Shepherd, BE, Hulgan, T, Rebeiro, P, Stinnette, S, Blackwell, RB, et al. Race and sex differences in antiretroviral therapy use and mortality among HIV-infected persons in care. J Infect Dis. (2009) 199:991–8. doi: 10.1086/597124
50. Vogt, F, Tayler-Smith, K, Bernasconi, A, Makondo, E, Taziwa, F, Moyo, B, et al. Access to CD4 testing for rural HIV patients: findings from a cohort study in Zimbabwe. PLoS One. (2015) 10:e0129166. doi: 10.1371/journal.pone.0129166
51. Sithole, Z, Mbizvo, E, Chonzi, P, Mungati, M, Juru, TP, Shambira, G, et al. Virological failure among adolescents on ART, Harare City, 2017-a case-control study. BMC Infect Dis. (2018) 18:469. doi: 10.1186/s12879-018-3372-6
52. Nabunya, P, Byansi, W, Sensoy Bahar, O, McKay, M, Ssewamala, FM, Damulira, C, et al. Factors associated with HIV disclosure and HIV-related stigma among adolescents living with HIV in southwestern Uganda. Front Psych. (2020) 11:772. doi: 10.3389/fpsyt.2020.00772
53. Okonji, EF, van Wyk, B, Mukumbang, FC, and Hughes, GD. Determinants of viral suppression among adolescents on antiretroviral treatment in Ehlanzeni district, South Africa: a cross-sectional analysis. AIDS Res Ther. (2021) 18:66. doi: 10.1186/s12981-021-00391-7
54. CDC . (2024) CD4 cell counts | aidsmap. Available online at: https://www.aidsmap.com/about-hiv/cd4-cell-counts (Accessed March 28, 2024)
55. Montarroyos, UR, Miranda-Filho, DB, César, CC, Souza, WV, Lacerda, HR, Albuquerque, M d FPM, et al. Factors related to changes in CD4+ T-cell counts over time in patients living with HIV/AIDS: a multilevel analysis. PLoS One. 9:84276. doi: 10.1371/journal.pone.0084276
56. CDC . (2014) About Your Viral Load and CD4 Cell Count. Available online at: https://www.cdc.gov/hiv/effective-interventions/library/every-dose-every-day/marketing-materials/cdc-hiv-ei-e2d2-about-your-viral-load-and-cd4.pdf (Accessed March 28, 2024)
57. Gaifer, Z, and Boulassel, M-R. Low-level viremia predicts Virological failure in HIV-infected Omani patients receiving antiretroviral therapy. J Int Assoc Provid AIDS Care. (2020) 19:2325958220979817. doi: 10.1177/2325958220979817
58. Fokam, J, Nka, AD, Dzukam, FYM, Gabisa, JE, Bouba, Y, Tchouaket, MCT, et al. Viral suppression in the era of transition to dolutegravir-based therapy in Cameroon: children at high risk of virological failure due to the lowly transition in pediatrics. Medicine (Baltimore). 102:737. doi: 10.1097/MD.0000000000033737
59. Ruel, TD, Zanoni, BC, Ssewanyana, I, Cao, H, Havlir, DV, Kamya, M, et al. Sex differences in HIV RNA level and CD4 cell percentage during childhood. Clin Infect Dis. (2011) 53:592–9. doi: 10.1093/cid/cir484
60. Means, AR, Risher, KA, Ujeneza, EL, Maposa, I, Nondi, J, Bellan, SE, et al. Impact of age and sex on CD4+ cell count trajectories following treatment initiation: an analysis of the Tanzanian HIV treatment database. PLoS One. (2016) 11:e0164148. doi: 10.1371/journal.pone.0164148
61. Klein, SL, and Morgan, R. The impact of sex and gender on immunotherapy outcomes. Biol Sex Differ. (2020) 11:24. doi: 10.1186/s13293-020-00301-y
62. Thompson, AE, Anisimowicz, Y, Miedema, B, Hogg, W, Wodchis, WP, Aubrey-Bassler, K, et al. The influence of gender and other patient characteristics on health care-seeking behaviour: a QUALICOPC study. BMC Fam Pract. (2016) 17:38. doi: 10.1186/s12875-016-0440-0
63. Yusuf, H, and Agwu, A. Adolescents and young adults with early acquired HIV infection in the United States: unique challenges in treatment and secondary prevention. Expert Rev Anti-Infect Ther. (2021) 19:457–71. doi: 10.1080/14787210.2021.1829473
64. Medscape . (2023). Pediatric HIV infection: practice essentials, background, Pathophysiology. Available at: https://emedicine.medscape.com/article/965086-overview?form=fpf#a2 (Accessed April 7, 2024)
65. Mbébi Enoné, PJ, Penda, CI, Ngondi, G, Fokam, J, Ebong, SB, Ndongo, JM, et al. High risk of virologic failure among HIV-infected children and adolescents routinely followed-up in Littoral region of Cameroon. PLoS One. (2023) 18:e0289426. doi: 10.1371/journal.pone.0289426
66. Ford, N, Meintjes, G, Vitoria, M, Greene, G, and Chiller, T. The evolving role of CD4 cell counts in HIV care. Curr Opin HIV AIDS. (2017) 12:123–8. doi: 10.1097/COH.0000000000000348
67. WHO . (2023) What’s new in treatment monitoring: viral load and cd4 testing. Available online at: https://iris.who.int/bitstream/handle/10665/255891/WHO-HIV-2017.22-eng.pdf?sequence=1 (Accessed March 27, 2024)
Keywords: HIV, immune monitoring, CD4 cell count, adolescents, Cameroon
Citation: Togna Pabo WLR, Kengni Ngueko AM, Nka AD, Santoro MM, Bouba Y, Chenwi CA, Ngoufack Jagni Semengue E, Takou D, Teto G, Dambaya B, Nyasa RB, Tommo Tchouaket MC, Beloumou GA, Djupsa Ndjeyep SC, Ka’e AC, Tekoh TAK, Ayuk Ngwese DT, Etame N-K, Mundo RAN, Kamgaing RS, Sosso SM, Ndip RN, Colizzi V, Cecchereni-Silberstein F, Ndjolo A and Fokam J (2024) Empowering adolescents living with perinatally-acquired HIV: tailored CD4+ count assessment for optimized care, the EDCTP READY-study. Front. Med. 11:1457501. doi: 10.3389/fmed.2024.1457501
Edited by:
Elena Criscuolo, Vita-Salute San Raffaele University, ItalyReviewed by:
Getu Girmay, University of Gondar, EthiopiaCopyright © 2024 Togna Pabo, Kengni Ngueko, Nka, Santoro, Bouba, Chenwi, Ngoufack Jagni Semengue, Takou, Teto, Dambaya, Nyasa, Tommo Tchouaket, Beloumou, Djupsa Ndjeyep, Ka’e, Tekoh, Ayuk Ngwese, Etame, Mundo, Kamgaing, Sosso, Ndip, Colizzi, Cecchereni-Silberstein, Ndjolo and Fokam. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Joseph Fokam, am9zZXBoZm9rYW1AZ21haWwuY29t; Alex Durand Nka, bmthYWxleGR1cmFuZEB5YWhvby5jb20=; Willy Le Roi Togna Pabo, d2lsbHlwYWJvQHlhaG9vLmZy
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.