 Chun-yi Jia1
Chun-yi Jia1 Xin-yuan Bi
Xin-yuan Bi Yi-ning Wang
Yi-ning Wang
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Med. , 26 July 2024
Sec. Translational Medicine
Volume 11 - 2024 | https://doi.org/10.3389/fmed.2024.1420012
This article is part of the Research Topic Insights in Thrombosis and Haemostasis: From a Biological, Clinical and Genetic Perspective View all 14 articles
This review examines recent advancements in interventional treatments and nursing care for lower extremity deep vein thrombosis (DVT), highlighting significant innovations and their clinical applications. It discusses the transition to novel anticoagulants such as Direct Oral Anticoagulants, which offer a safer profile and simplified management compared to traditional therapies. Mechanical interventions, including balloon angioplasty and venous stenting, are detailed for their roles in improving immediate and long-term vascular function in acute DVT cases. Furthermore, the use of image-guided techniques is presented as essential for enhancing the accuracy and safety of DVT interventions. Additionally, this study outlines advances in nursing care strategies, emphasizing comprehensive preoperative and postoperative evaluations to optimize patient outcomes. These evaluations facilitate tailored treatment plans, crucial for managing the complex needs of DVT patients. Long-term care strategies are also discussed, with a focus on patient education to ensure adherence to treatment protocols and to prevent recurrence. The synthesis aims to inform healthcare professionals about cutting-edge practices in DVT management, promoting a deeper understanding of how these advancements can be integrated into clinical practice. It also underscores the necessity for ongoing research to address challenges such as cost-effectiveness and patient compliance, ensuring that future treatments are both accessible and effective.
Deep vein thrombosis (DVT) represents a significant medical condition characterized by the formation of blood clots within the major veins of the lower extremities (1, 2). This condition not only induces pain, swelling, and limited mobility in the affected limb but also poses a severe risk of life-threatening pulmonary embolisms should a clot dislodge and migrate to the lungs (1, 2). Given its prevalence and the severe complications associated with it, DVT is a critical public health issue demanding effective strategies for its prevention, diagnosis, and management (3).
Traditionally, the management of DVT has centered around anticoagulant therapy, the use of compression stockings, and occasionally, surgical interventions (4). While these treatments have proven beneficial, they come with notable limitations (5). Anticoagulants, for example, while effective in preventing clot progression and new clot formation, require rigorous monitoring to mitigate the risk of severe bleeding complications. Compression stockings are beneficial for reducing thrombus formation and edema but often face challenges with patient compliance (6). Furthermore, these conventional approaches do not fully address the recurrence of the condition or the long-term complications associated with DVT (6).
In response to these challenges, there has been a marked shift towards more innovative interventional treatments and care protocols in recent years (7). Advanced treatment modalities, including novel anticoagulants, mechanical thrombectomy, and image-guided minimally invasive procedures, have been developed (8, 9). These innovations offer enhanced efficacy and safety, showing particular promise in the management of severe or complex DVT cases.
The objective of this mini review is to conduct a thorough evaluation and synthesis of the current scientific and clinical advancements in the interventional treatment and management of DVT. This mini review will scrutinize the latest research findings and clinical trials, aiming to elucidate how these innovative approaches have refined patient outcomes. Moreover, it explores prospective research avenues and potential advancements in technology that could further revolutionize the treatment landscape of DVT.
This review is crucial for healthcare professionals as it not only highlights contemporary treatment methodologies but also lays down a comprehensive framework for future investigations. Such rigorous examination is essential for advancing clinical practice and enhancing patient care in the realm of DVT.
Pharmacological interventions play a pivotal role in the management of DVT, with significant advancements in both drug types and therapeutic strategies in recent years. Modern pharmacotherapy primarily involves anticoagulants and thrombolytics, which have substantially evolved to improve both efficacy and safety for patients (10–18) (Table 1).
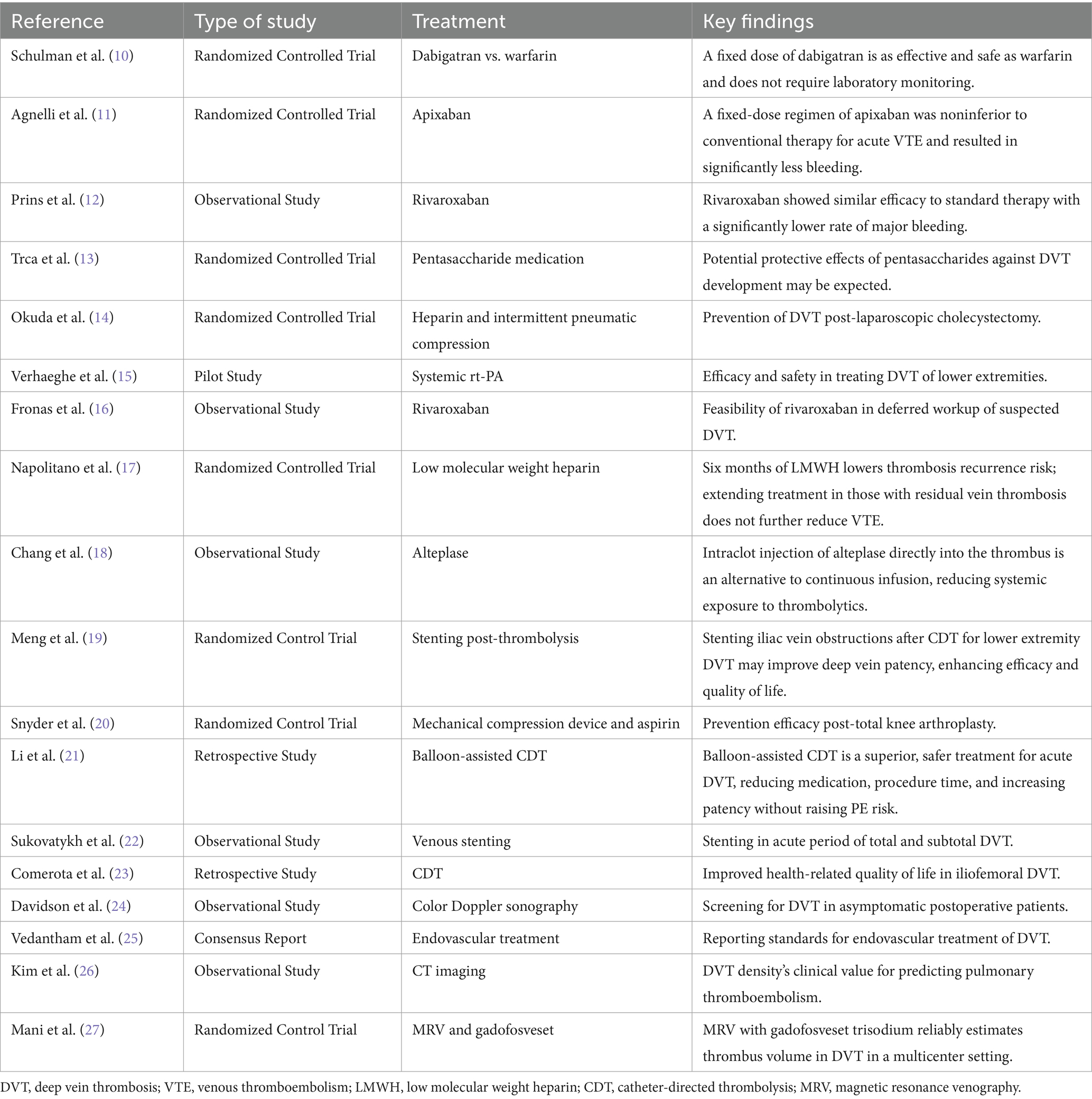
Table 1. Interventional therapy in patients with DVT in the lower extremities.
The advent of direct oral anticoagulants (DOACs), including rivaroxaban, apixaban, and dabigatran, marks a significant shift from traditional warfarin therapy (10–18) (Table 1). DOACs offer advantages such as reduced need for monitoring, fewer dietary and drug interactions, and a more stable therapeutic profile. Not requiring frequent INR monitoring, these anticoagulants simplify outpatient management and enhance patient adherence.
Clinical trials such as EINSTEIN, RE-COVER, and AMPLIFY have demonstrated the efficacy of DOACs in treating DVT with a notably lower risk of bleeding compared to traditional anticoagulants. These studies underline the role of DOACs in setting new standards for anticoagulation therapy (10–18).
Alongside established therapies, the development of anti-XI anticoagulants marks an innovative frontier in thromboprophylaxis (28). These agents specifically inhibit Factor XI, offering a targeted approach to reducing thrombosis risk while potentially minimizing bleeding complications—a common limitation of traditional anticoagulants (28, 29). Emerging clinical trials have begun to explore the efficacy and safety profiles of these anticoagulants, indicating their promise for safer therapeutic regimens in populations at high risk of bleeding (30). The introduction of anti-XI agents underscores the dynamic evolution of anticoagulant therapy, aiming to balance efficacy and safety more effectively (31).
Tissue plasminogen activator, such as alteplase, continues to be extensively utilized for acute DVT management, effectively dissolving clots and restoring venous flow (14, 15) (Table 1). Its application is crucial in managing severe thrombotic events where rapid resolution is necessary.
The ATTRACT trial, among others, has explored the role of thrombolytics in the early intervention of DVT to prevent post-thrombotic syndrome and chronic venous insufficiency. While highlighting the benefits in symptom reduction, these studies also stress the importance of careful patient selection to mitigate bleeding risks.
The development of mechanical interventional techniques has introduced novel therapeutic possibilities for DVT, especially beneficial for patients who are not ideal candidates for conventional anticoagulation (19, 20) (Table 1).
This technique involves the insertion of a catheter with an attached balloon into the thrombosed vein (21). Upon inflation, the balloon physically expands the vein, displacing the clot and restoring blood flow. This approach is particularly effective in acute cases where rapid amelioration of symptoms is critical (21) (Table 1). Balloon angioplasty is typically reserved for critical cases requiring rapid restoration of venous flow due to significant obstruction (21). This intervention is particularly crucial in severe phlegmasia dolens, where there is an immediate risk of limb ischemia.
Stenting involves the placement of a metallic mesh within the vein to maintain vascular patency and prevent future occlusions. It is particularly applicable in scenarios where venous stenosis persists post-thrombosis or when angioplasty alone does not suffice to restore normal blood flow (19, 22). The stent acts as a scaffold, ensuring long-term patency and improving overall venous return, which is crucial for reducing recurrence rates and improving long-term outcomes (19, 22). Stenting is primarily recommended for managing chronic venous insufficiency, particularly when compressive symptoms continue to persist despite the application of less invasive treatments (32).
Recent clinical data affirm that mechanical interventions like balloon angioplasty and stenting significantly enhance symptom management and quality of life (19, 22) (Table 1). However, the sustainability of treatment effects and the potential for long-term complications necessitate further research and careful patient follow-up.
Image-guided techniques have revolutionized the precision and safety of interventions for managing DVT, proving essential in both diagnosis and therapeutic application.
Color Doppler ultrasound is the frontline modality for diagnosing DVT, providing real-time, dynamic blood flow information. It is indispensable for guiding minimally invasive procedures such as catheter-directed thrombolysis, allowing for direct visualization of the thrombus and treatment effects (23–25) (Table 1).
Advancements in Ultrasound Technology: The field of ultrasound technology has seen significant advancements, notably in the development of portable, high-resolution devices (33). These improvements have expanded the reach of ultrasound beyond traditional clinical settings, facilitating its use in remote locations and potentially increasing patient access to timely diagnosis and management.
Future Directions in Ultrasound and Digital Health Integration: Looking forward, the integration of ultrasound technology with digital health applications holds promising potential for enhancing patient management (34). Innovations on the horizon include wearable devices capable of continuous monitoring of vital parameters such as heart rate, oxygen saturation, and electrocardiographic signals (34). These devices could play a crucial role in early detection of complications, such as pulmonary embolism, and enhance preventive care. Furthermore, advancements are expected in the development of smart medication adherence tools that remind patients of dosage schedules, thereby improving compliance with treatment protocols (35).
These technological advancements are poised to transform the management of DVT, enhancing both the efficacy and safety of treatments and supporting proactive patient care through continuous monitoring and timely intervention.
Computed tomography (CT) or magnetic resonance imaging (MRI) offers comprehensive imaging capabilities that extend beyond the limitations of ultrasound, especially useful in complex cases where clots are located in anatomically challenging positions (26, 27). These modalities enable detailed visualization of the vascular anatomy, facilitating precise interventions such as stenting and targeted thrombolysis, ensuring interventions are performed with the highest accuracy (26, 27) (Table 1).
Specifically, the use of CT and MRI is highly restricted and generally recommended in specialized cases such as left iliac DVT in pregnant patients (26, 27). In these patients, MRI is preferred over CT due to the absence of ionizing radiation, which poses a risk to the developing fetus (27). This ensures that both mother and fetus are safeguarded while obtaining essential diagnostic information to guide further treatment.
The integration of image-guided technology not only enhances the effectiveness of therapeutic interventions but also minimizes procedural risks, thereby improving patient safety and treatment outcomes. As imaging technology advances, future interventions are expected to become even more refined, further elevating the standard of care for patients with DVT.
Effective preoperative and postoperative care is crucial in optimizing outcomes and minimizing complications in the interventional treatment of lower extremity DVT. Advancements in medical technology have greatly enhanced the precision of nursing assessments, which now play a pivotal role in the planning and execution of treatment (Table 2).
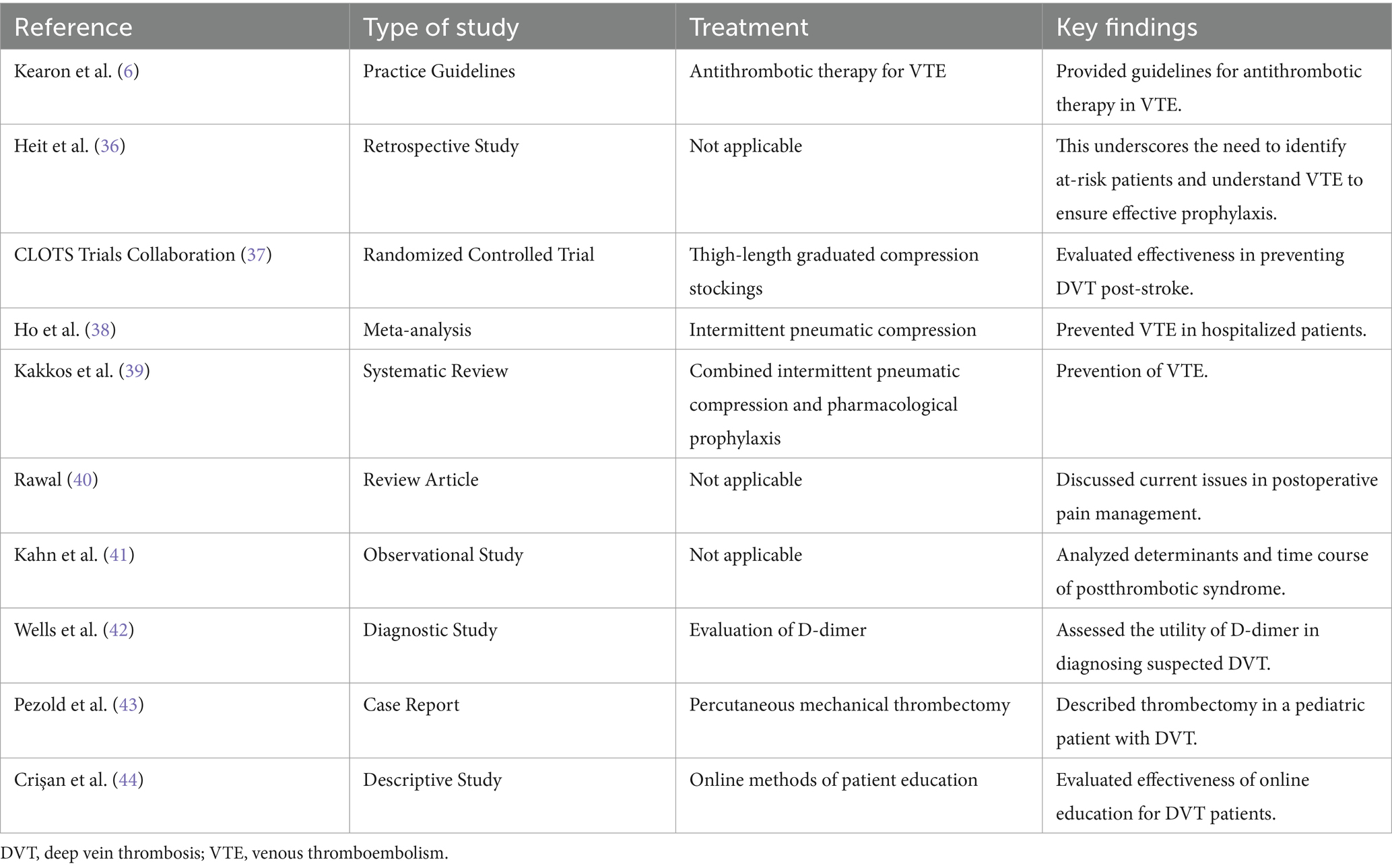
Table 2. Nursing strategies in patients with DVT in the lower extremities.
Nursing Assessments: Modern nursing practices involve comprehensive evaluations using standardized tools that assess hemorheology, limb measurements, and a patient’s overall physiological and psychological state. These evaluations help clinicians identify patient-specific risk factors and predict potential complications, allowing for the creation of tailored interventional treatment plans (6, 36). Furthermore, assessments extend to evaluating a patient’s understanding and preparedness for upcoming treatments, ensuring they are fully informed and ready both mentally and physically.
Preoperative Preparations: Key aspects of preoperative care include thorough health examinations to ascertain the patient’s baseline health status and detailed discussions to gauge their understanding and acceptance of the proposed interventions (37–39). Educating patients about what to expect during and after the procedure is critical. This education covers potential postoperative scenarios and adherence to prescribed self-care protocols.
Postoperative Management: Focuses on managing pain and overseeing wound care, essential for facilitating a swift recovery and optimizing the treatment’s success. Pain management strategies often encompass both pharmacological and non-pharmacological approaches, including physical therapy (40). Wound care involves regular monitoring and timely intervention if signs of infection arise, preventing further complications. Postoperative care also includes functional rehabilitation and ongoing psychological support, fostering a holistic recovery approach.
Implementing these refined care strategies can significantly enhance patient outcomes, reducing the risks and complications associated with the treatment of DVT (Table 2).
Managing lower extremity DVT extends beyond immediate medical intervention and encompasses long-term care and patient education, which are essential for the sustained well-being of patients (Table 2).
Home Care: After hospital discharge, home care becomes a critical aspect of a DVT patient’s routine, particularly during the recovery and maintenance phases. Patients need comprehensive instructions and continuous support for activities such as adhering to anticoagulation regimens and monitoring for adverse effects (41, 42). The ongoing anticoagulation is crucial for preventing thrombus reformation but carries an inherent risk of bleeding, necessitating patient education on managing these risks effectively (41, 42).
Lifestyle Modifications: Adjustments in daily living, such as maintaining an active lifestyle, achieving and sustaining an appropriate weight, and following a heart-healthy diet, are crucial (43). These modifications help mitigate the risk of recurrent DVT and enhance overall health.
Patient Education: This is an integral component of long-term management, empowering patients with knowledge about their condition, the importance of their treatment regimen, and the ability to recognize symptoms of potential complications (44). Education should not only provide disease and treatment-related information but also include practical advice on when and how to seek further medical assistance (44). Effective education transforms patients from passive recipients of healthcare into active participants in their health management, aiming to prevent recurrence and elevate their quality of life.
By enhancing these aspects of care, healthcare providers can ensure better management of DVT, promoting patient independence and improving outcomes in long-term disease management.
Elderly Patients: Elderly individuals undergoing DVT intervention often present with multiple comorbidities, such as cardiovascular diseases and renal insufficiency, which can affect their response to anticoagulant therapy (45). The diminished drug metabolism typical in older age further elevates the risk of adverse reactions during treatment. Hence, nursing care for elderly patients should include meticulous monitoring of drug dosages and therapeutic responses. Care plans must also consider potential cognitive impairments and the availability of family support, tailoring education and support programs to meet their specific needs. This ensures that elderly patients receive care that is both effective and sensitive to their particular health status.
Pregnant Women: DVT treatment in pregnant women requires careful consideration of both maternal and fetal health due to the teratogenic risks associated with many standard anticoagulants (46–48). The selection and timing of therapeutic interventions must prioritize safety, avoiding any potential harm to the developing fetus. Physiological changes during pregnancy can alter the risk profile for thrombus formation and modify responses to treatment, necessitating vigilant monitoring and management (46–48). Collaborative efforts with obstetric specialists are essential to tailor interventions that safeguard the health of both mother and child, ensuring that treatment protocols are precisely followed.
Patients with Chronic Diseases: Individuals with chronic conditions such as cancer, diabetes, or cardiovascular disease may face additional challenges when undergoing DVT interventions (3, 49). These conditions can influence both the choice of treatment and the overall prognosis. For instance, cancer patients are particularly susceptible to increased thrombotic risk due to the malignancy and associated treatments like chemotherapy. Nursing care strategies must be adaptive to these risks, adjusting therapeutic approaches to effectively manage and minimize the likelihood of recurrence. It is also crucial for the care team to address the comprehensive needs of these patients, including nutritional support, effective pain management, and psychological care, to enhance their overall quality of life and treatment outcomes.
In summary, effective nursing care for special populations undergoing treatment for lower extremity DVT requires a detailed understanding of each individual’s unique medical and personal circumstances. By implementing personalized and meticulously planned care strategies, healthcare providers can ensure that interventions are not only safe and effective but also aligned with the specific needs and conditions of elderly patients, pregnant women, and those with chronic diseases. This approach promotes optimal health outcomes and patient satisfaction.
Despite notable advancements in the management of lower extremity DVT through interventional treatments, several challenges persist that affect the adoption and efficacy of these approaches.
Current interventional techniques such as thrombectomy and catheter-directed thrombolysis are effective but involve complex procedures that require a high degree of technical skill (3, 50, 51). The reliance on sophisticated medical equipment also limits the application of these treatments in resource-constrained settings (3, 50, 51). Addressing these technological constraints involves simplifying procedures and developing equipment that is both cost-effective and suitable for use in a broader range of healthcare environments.
The high costs associated with interventional treatments for DVT pose significant barriers to their widespread use (41, 49–53). These costs can be prohibitive for patients and healthcare systems, especially in lower-income areas. Future research must focus on conducting thorough cost-effectiveness analyses to identify economic strategies that can reduce expenses while maintaining or enhancing clinical outcomes. Exploring generic medication options, streamlined procedural techniques, and cost-sharing models could be viable approaches.
The acceptance of new or complex interventional treatments by patients is crucial for successful outcomes (41, 54). Challenges in patient education and the communication of treatment benefits and risks are significant (41, 54). Improving educational strategies to better inform patients about their options, the procedures involved, potential risks, and expected outcomes is essential. Enhanced communication efforts should aim to build trust and understanding, facilitating informed consent and engagement in treatment decisions.
Research in the coming years may concentrate on creating simpler, more affordable interventional techniques. There is a need to innovate in patient education and care coordination to adapt to the evolving landscape of healthcare delivery. Future developments could include (55–57):
Technology Advancements: Redesigning devices and simplifying interventional procedures to make them more accessible and easier to perform.
Digital Tools: Leveraging technology to enhance patient education, treatment transparency, and engagement through digital platforms that provide accessible information and support.
Interdisciplinary Approaches: Developing collaborative care models that integrate various healthcare professionals, including doctors, nurses, physical therapists, and social workers, to deliver holistic and coordinated care.
Such innovations are expected to optimize the management of DVT, significantly improve clinical outcomes, and broaden the application of interventional treatments, making them more accessible and effective across diverse patient populations and geographic locations.
A thorough evaluation of the recent developments in interventional treatments and nursing strategies for lower extremity DVT reveals several critical insights. Firstly, technological advancements in interventional methods have notably increased the efficiency and safety of treatments for DVT. The adoption of advanced anticoagulants, mechanical thrombectomy techniques, and image-guided minimally invasive surgeries has shown exceptional effectiveness in clinical settings, particularly in managing complex or high-risk DVT cases. Furthermore, enhancements in nursing strategies, including detailed assessments before and after surgery, effective pain management, and comprehensive long-term care coupled with patient education, have substantially improved both the rehabilitation outcomes and the overall quality of life for patients.
Despite these advancements, the need for continuous research is imperative. Future investigations should delve deeper into the capabilities of emerging technologies, especially focusing on their role in minimizing complications and fostering long-term wellness for patients. Moreover, there is a critical need to focus on increasing patient compliance with treatment regimens and improving the effectiveness of interdisciplinary collaborations to streamline and execute treatment protocols more efficiently. By addressing these areas, we can further refine DVT treatment processes and enhance the quality of care provided to patients, ultimately leading to significant improvements in their quality of life.
C-yJ: Conceptualization, Data curation, Methodology, Resources, Validation, Visualization, Writing – original draft, Writing – review & editing. D-dD: Data curation, Methodology, Resources, Validation, Visualization, Writing – original draft, Writing – review & editing. X-yB: Conceptualization, Methodology, Resources, Validation, Visualization, Writing – original draft, Writing – review & editing. XZ: Resources, Validation, Visualization, Writing – original draft, Writing – review & editing. Y-nW: Conceptualization, Data curation, Investigation, Project administration, Resources, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This study was partly supported by Research Project of the Heilongjiang Health Commission (20231414050484).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Liang, W, and Moverley, JA. Deep vein thrombosis. JAAPA. (2022) 35:61–2. doi: 10.1097/01.JAA.0000819540.23572.34
2. Navarrete, S, Solar, C, Tapia, R, Pereira, J, Fuentes, E, and Palomo, I. Pathophysiology of deep vein thrombosis. Clin Exp Med. (2023) 23:645–54. doi: 10.1007/s10238-022-00829-w
3. Kearon, C, Akl, EA, Ornelas, J, Blaivas, A, Jimenez, D, Bounameaux, H, et al. Antithrombotic therapy for VTE disease: CHEST guideline and expert panel report. Chest. (2016) 149:315–52. doi: 10.1016/j.chest.2015.11.026
4. Kahn, SR, Shbaklo, H, Lamping, DL, Holcroft, CA, Shrier, I, Miron, MJ, et al. Determinants of health-related quality of life during the 2 years following deep vein thrombosis. J Thromb Haemost. (2008) 6:1105–12. doi: 10.1111/j.1538-7836.2008.03002.x
5. Watson, L, Broderick, C, and Armon, MP. Thrombolysis for acute deep vein thrombosis. Cochrane Database Syst Rev. (2016) 11:CD002783. doi: 10.1002/14651858.CD002783.pub4
6. Kearon, C, Akl, EA, Comerota, AJ, Prandoni, P, Bounameaux, H, Goldhaber, SZ, et al. Antithrombotic therapy for VTE disease: antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. (2012) 141:e419S–96S. doi: 10.1378/chest.11-2301
7. Jaff, MR, McMurtry, MS, Archer, SL, Cushman, M, Goldenberg, N, Goldhaber, SZ, et al. Management of massive and submassive pulmonary embolism, iliofemoral deep vein thrombosis, and chronic thromboembolic pulmonary hypertension: a scientific statement from the American Heart Association. Circulation. (2011) 123:1788–830. doi: 10.1161/CIR.0b013e318214914f
8. Galanaud, JP, Quenet, S, Rivron-Guillot, K, Quere, I, Sanchez Muñoz-Torrero, JF, Tolosa, C, et al. Comparison of the clinical history of symptomatic isolated distal deep-vein thrombosis vs. proximal deep-vein thrombosis in 11 086 patients. J Thromb Haemost. (2009) 7:2028–34. doi: 10.1111/j.1538-7836.2009.03629.x
9. Enden, T, Haig, Y, Kløw, NE, Slagsvold, CE, Sandvik, L, Ghanima, W, et al. Long-term outcome after additional catheter-directed thrombolysis versus standard treatment for acute iliofemoral deep vein thrombosis (the CaVenT study): a randomised controlled trial. Lancet. (2012) 379:31–8. doi: 10.1016/S0140-6736(11)61753-4
10. Schulman, S, Kearon, C, Kakkar, AK, Mismetti, P, Schellong, S, Eriksson, H, et al. Dabigatran versus warfarin in the treatment of acute venous thromboembolism. N Engl J Med. (2009) 361:2342–52. doi: 10.1056/NEJMoa0906598
11. Agnelli, G, Buller, HR, Cohen, A, Curto, M, Gallus, AS, Johnson, M, et al. Oral apixaban for the treatment of acute venous thromboembolism. N Engl J Med. (2013) 369:799–808. doi: 10.1056/NEJMoa1302507
12. Prins, MH, Lensing, AWA, Bauersachs, R, van Bellen, B, Bounameaux, H, Brighton, TA, et al. Oral rivaroxaban versus standard therapy for the treatment of symptomatic venous thromboembolism: a pooled analysis of the EINSTEIN-DVT and PE randomized studies. Thromb J. (2013) 11:21. doi: 10.1186/1477-9560-11-21
13. Trca, S, Krska, Z, Sedlár, M, Kudrnová, Z, and Dohnalová, A. Comparison of various types of pharmacological prevention of lower extremities deep vein thrombosis in patients with proximal femoral fractures. Rozhl Chir. (2007) 86:241–8.
14. Okuda, Y, Kitajima, T, Egawa, H, Hamaguchi, S, Yamaguchi, S, Yamazaki, H, et al. A combination of heparin and an intermittent pneumatic compression device may be more effective to prevent deep-vein thrombosis in the lower extremities after laparoscopic cholecystectomy. Surg Endosc. (2002) 16:781–4. doi: 10.1007/s00464-001-8191-x
15. Verhaeghe, R, Besse, P, Bounameaux, H, and Marbet, GA. Multicenter pilot study of the efficacy and safety of systemic rt-PA administration in the treatment of deep vein thrombosis of the lower extremities and/or pelvis. Thromb Res. (1989) 55:5–11. doi: 10.1016/0049-3848(89)90451-9
16. Fronas, SG, Dahm, AEA, Wik, HS, Jørgensen, CT, Gleditsch, J, Raouf, N, et al. Safety and feasibility of rivaroxaban in deferred workup of patients with suspected deep vein thrombosis. Blood Adv. (2020) 4:2468–76. doi: 10.1182/bloodadvances.2020001556
17. Napolitano, M, Saccullo, G, Malato, A, Sprini, D, Ageno, W, Imberti, D, et al. Optimal duration of low molecular weight heparin for the treatment of cancer-related deep vein thrombosis: the Cancer-DACUS study. J Clin Oncol. (2014) 32:3607–12. doi: 10.1200/JCO.2013.51.7433
18. Chang, R, Chen, CC, Kam, A, Mao, E, Shawker, TH, and Horne, MDK III. Deep vein thrombosis of lower extremity: direct Intraclot injection of Alteplase once daily with systemic anticoagulation—results of pilot study. Radiology. (2008) 246:619–29. doi: 10.1148/radiol.2461062076
19. Meng, QY, Li, XQ, Jiang, K, Qian, AM, Sang, HF, Rong, JJ, et al. Stenting of iliac vein obstruction following catheter-directed thrombolysis in lower extremity deep vein thrombosis. Chin Med J. (2013) 126:3519–22. doi: 10.3760/cma.j.issn.0366-6999.20130933
20. Snyder, MA, Sympson, AN, Scheuerman, CM, Gregg, JL, and Hussain, LR. Efficacy in deep vein thrombosis prevention with extended mechanical compression device therapy and prophylactic aspirin following Total knee arthroplasty: a randomized control trial. J Arthroplast. (2017) 32:1478–82. doi: 10.1016/j.arth.2016.12.027
21. Li, Z, Yang, C, Fan, B, Jin, Y, and Ni, C. Balloon-assisted catheter-directed thrombolysis: a novel approach for acute deep vein thrombosis in the lower extremities. J Interv Med. (2020) 3:37–40. doi: 10.1016/j.jimed.2020.01.005
22. Sukovatykh, BS, Sereditskiy, AV, Muradyan, VF, Azarov, AM, Sukovatykh, MB, Lapinas, AA, et al. Venous stenting in acute period of total and subtotal deep vein thrombosis. Khirurgiia (Mosk). (2022) 12:92–8. doi: 10.17116/hirurgia202212192
23. Comerota, AJ, Throm, RC, Mathias, SD, Haughton, S, and Mewissen, M. Catheter-directed thrombolysis for iliofemoral deep venous thrombosis improves health-related quality of life. J Vasc Surg. (2000) 32:130–7. doi: 10.1067/mva.2000.105664
24. Davidson, HC, Mazzu, D, Gage, BF, and Jeffrey, RB. Screening for deep venous thrombosis in asymptomatic postoperative orthopedic patients using color Doppler sonography: analysis of prevalence and risk factors. AJR Am J Roentgenol. (1996) 166:659–62. doi: 10.2214/ajr.166.3.8623645
25. Vedantham, S, Grassi, CJ, Ferral, H, Patel, NH, Thorpe, PE, Antonacci, VP, et al. Reporting standards for endovascular treatment of lower extremity deep vein thrombosis. J Vasc Interv Radiol. (2006) 17:417–34. doi: 10.1097/01.RVI.0000197359.26571.C2
26. Kim, DK, Jung, JH, Kim, JK, and Kim, T. Clinical value of deep vein thrombosis density on pre-contrast and post-contrast lower-extremity CT for prediction of pulmonary thromboembolism. Acta Radiol. (2023) 64:1410–7. doi: 10.1177/02841851221131250
27. Mani, V, Alie, N, Ramachandran, S, Robson, PM, Besa, C, Piazza, G, et al. A multicenter MRI protocol for the evaluation and quantification of deep vein thrombosis. J Vis Exp. (2015) 100:e52761. doi: 10.3791/52761
28. Nopp, S, Kraemmer, D, and Ay, C. Factor XI inhibitors for prevention and treatment of venous thromboembolism: a review on the rationale and update on current evidence. Front Cardiovasc Med. (2022) 9:903029. doi: 10.3389/fcvm.2022.903029
29. Presume, J, Ferreira, J, and Ribeiras, R. Factor XI inhibitors: a new horizon in anticoagulation therapy. Cardiol Ther. (2024) 13:1–16. doi: 10.1007/s40119-024-00352-x
30. Büller, HR, Bethune, C, Bhanot, S, Gailani, D, Monia, BP, Raskob, GE, et al. Factor XI antisense oligonucleotide for prevention of venous thrombosis. N Engl J Med. (2015) 372:232–40. doi: 10.1056/NEJMoa1405760
31. Vedovati, MC, Becattini, C, and Agnelli, G. A new strategy for anticoagulation: the factor XI inhibitors. Eur J Intern Med. (2023) 116:8–15. doi: 10.1016/j.ejim.2023.08.001
32. Patel, R, Mulukutla, V, Mistry, A, and Prajapati, K. Successful intravascular ultrasound-guided Thrombus removal and angioplasty for Phlegmasia Cerulea Dolens in a young male with a history of multiple lower extremity deep vein thrombosis. Cureus. (2023) 15:e39739. doi: 10.7759/cureus.39739
33. Shin, B, Jeon, S, Ryu, J, and Kwon, HJ. Elastography for portable ultrasound. Biomed Eng Lett. (2017) 8:101–16. doi: 10.1007/s13534-017-0052-1
34. Shajari, S, Kuruvinashetti, K, Komeili, A, and Sundararaj, U. The emergence of AI-based wearable sensors for digital health technology: a review. Sensors (Basel). (2023) 23:9498. doi: 10.3390/s23239498
35. Faisal, S, Samoth, D, Aslam, Y, Patel, H, Park, S, Baby, B, et al. Key features of smart medication adherence products: updated scoping review. JMIR Aging. (2023) 6:e50990. doi: 10.2196/50990
36. Heit, JA, Melton, LJ, Lohse, CM, Petterson, TM, Silverstein, MD, Mohr, DN, et al. Incidence of venous thromboembolism in hospitalized patients vs community residents. Mayo Clin Proc. (2001) 76:1102–10. doi: 10.4065/76.11.1102
37. CLOTS (Clots in Legs Or sTockings after Stroke) Trials Collaboration . Effectiveness of thigh-length graduated compression stockings to reduce the risk of deep vein thrombosis after stroke (CLOTS trial 1): a multicentre, randomised controlled trial. Lancet. (2009) 373:1958–65. doi: 10.1016/S0140-6736(09)60941-7
38. Ho, KM, and Tan, JA. Stratified meta-analysis of intermittent pneumatic compression of the lower limbs to prevent venous thromboembolism in hospitalized patients. Circulation. (2013) 128:1003–20. doi: 10.1161/CIRCULATIONAHA.113.002690
39. Kakkos, SK, Caprini, JA, Geroulakos, G, Nicolaides, AN, Stansby, G, Reddy, DJ, et al. Combined intermittent pneumatic leg compression and pharmacological prophylaxis for prevention of venous thromboembolism. Cochrane Database Syst Rev. (2016) 9:CD005258. doi: 10.1002/14651858.CD005258.pub3
40. Rawal, N . Current issues in postoperative pain management. Eur J Anaesthesiol. (2016) 33:160–71. doi: 10.1097/EJA.0000000000000366
41. Kahn, SR, Shrier, I, Julian, JA, Ducruet, T, Arsenault, L, Miron, MJ, et al. Determinants and time course of the postthrombotic syndrome after acute deep venous thrombosis. Ann Intern Med. (2008) 149:698–707. doi: 10.7326/0003-4819-149-10-200811180-00004
42. Wells, PS, Anderson, DR, Rodger, M, Forgie, M, Kearon, C, Dreyer, J, et al. Evaluation of D-dimer in the diagnosis of suspected deep-vein thrombosis. N Engl J Med. (2003) 349:1227–35. doi: 10.1056/NEJMoa023153
43. Pezold, M, Jacobowitz, GR, and Garg, K. Percutaneous mechanical thrombectomy of lower extremity deep vein thrombosis in a pediatric patient. J Vasc Surg Cases Innov Tech. (2020) 6:543–6. doi: 10.1016/j.jvscit.2020.08.032
44. Crişan, D, Crişan, S, Buzdugan, E, Vesa, S, and Pestrea, C. Deep vein thrombosis--online methods of patient education. Med Ultrason. (2010) 12:311–6.
45. Ageno, W, Gallus, AS, Wittkowsky, A, Crowther, M, Hylek, EM, and Palareti, G. Oral anticoagulant therapy: antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. (2012) 141:e44S–88S. doi: 10.1378/chest.11-2292
46. Bates, SM, Greer, IA, Middeldorp, S, Veenstra, DL, Prabulos, AM, and Vandvik, PO. VTE, thrombophilia, antithrombotic therapy, and pregnancy: antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. (2012) 141:e691S–736S. doi: 10.1378/chest.11-2300
47. Pomp, ER, Lenselink, AM, Rosendaal, FR, and Doggen, CJ. Pregnancy, the postpartum period and prothrombotic defects: risk of venous thrombosis in the MEGA study. J Thromb Haemost. (2008) 6:632–7. doi: 10.1111/j.1538-7836.2008.02921.x
48. Heit, JA, Kobbervig, CE, James, AH, Petterson, TM, Bailey, KR, and Melton, LJ III. Trends in the incidence of venous thromboembolism during pregnancy or postpartum: a 30-year population-based study. Ann Intern Med. (2005) 143:697–706. doi: 10.7326/0003-4819-143-10-200511150-00006
49. Prandoni, P, Lensing, AWA, Piccioli, A, Bernardi, E, Simioni, P, Girolami, B, et al. Recurrent venous thromboembolism and bleeding complications during anticoagulant treatment in patients with cancer and venous thrombosis. Blood. (2002) 100:3484–8. doi: 10.1182/blood-2002-01-0108
50. Meissner, MH, Gloviczki, P, Comerota, AJ, Dalsing, MC, Eklof, BG, Gillespie, DL, et al. Early thrombus removal strategies for acute deep venous thrombosis: clinical practice guidelines of the Society for Vascular Surgery and the American venous forum. J Vasc Surg. (2012) 55:1449–62. doi: 10.1016/j.jvs.2011.12.081
51. Roberts, LN, Patel, RK, and Arya, R. Venous thromboembolism and ethnicity. Br J Haematol. (2009) 146:369–83. doi: 10.1111/j.1365-2141.2009.07786.x
52. Sarode, R, Milling, TJ Jr, Refaai, MA, Mangione, A, Schneider, A, Durn, BL, et al. Efficacy and safety of a 4-factor prothrombin complex concentrate in patients on vitamin K antagonists presenting with major bleeding: a randomized, plasma-controlled, phase IIIb study. Circulation. (2013) 128:1234–43. doi: 10.1161/CIRCULATIONAHA.113.002283
53. Kahn, SR, Partsch, H, Vedantham, S, Prandoni, P, and Kearon, C. Subcommittee on control of anticoagulation of the SSC of the ISTH. Definition of post-thrombotic syndrome of the leg for use in clinical investigations: a recommendation for standardization. J Thromb Haemost. (2009) 7:879–83. doi: 10.1111/j.1538-7836.2009.03294.x
54. Galanaud, JP, Monreal, M, and Kahn, SR. Epidemiology of the post-thrombotic syndrome. Thromb Res. (2018) 164:100–9. doi: 10.1016/j.thromres.2017.07.026
55. Garcia, MJ, Lookstein, R, Malhotra, R, Amin, A, Blitz, LR, Leung, DA, et al. Endovascular management of deep vein thrombosis with rheolytic thrombectomy: final report of the prospective multicenter PEARL (peripheral use of Angio jet Rheolytic Thrombectomy with a variety of catheter lengths) registry. J Vasc Interv Radiol. (2015) 26:777–85. doi: 10.1016/j.jvir.2015.01.036
56. Lee, TH, Bodenheimer, T, Goroll, AH, Starfield, B, and Treadway, K. Perspective roundtable: redesigning primary care. N Engl J Med. (2008) 359:e24. doi: 10.1056/NEJMp0809050
Keywords: deep vein thrombosis, lower extremity, interventional therapy, anticoagulants, nursing care
Citation: Jia C-y, Dai D-d, Bi X-y, Zhang X and Wang Y-n (2024) Advancements in the interventional therapy and nursing care on deep vein thrombosis in the lower extremities. Front. Med. 11:1420012. doi: 10.3389/fmed.2024.1420012
Edited by:
Cristina Tudoran, Victor Babes University of Medicine and Pharmacy, RomaniaReviewed by:
Cristiano Bortoluzzi, Azienda Ulss 12 veneziana, ItalyCopyright © 2024 Jia, Dai, Bi, Zhang and Wang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yi-ning Wang, WWktbmluZ3dhbmcxOTkwQGhvdG1haWwuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.