 Berit D. Nielsen1,2,3*†
Berit D. Nielsen1,2,3*† Salome Kristensen4,5†Agnete Donskov2,3
Salome Kristensen4,5†Agnete Donskov2,3 Lene Terslev6,7†Lene Wohlfahrt Dreyer4,5†Ada Colic8†Merete Lund Hetland6,7†Pil Højgaard9†
Lene Terslev6,7†Lene Wohlfahrt Dreyer4,5†Ada Colic8†Merete Lund Hetland6,7†Pil Højgaard9† Torkell Ellingsen10†Ellen-Margrethe Hauge2,3†
Torkell Ellingsen10†Ellen-Margrethe Hauge2,3† Stavros Chrysidis11†Kresten K. Keller2,3†
Stavros Chrysidis11†Kresten K. Keller2,3†- 1Department of Medicine, The Regional Hospital in Horsens, Horsens, Denmark
- 2Department of Rheumatology, Aarhus University Hospital, Aarhus, Denmark
- 3Department of Clinical Medicine, Aarhus University, Aarhus, Denmark
- 4Center of Rheumatic Research Aalborg (CERRA), Department of Rheumatology, Aalborg University Hospital, Aalborg, Denmark
- 5Department of Clinical Medicine, Aalborg University, Aalborg, Denmark
- 6DANBIO and Copenhagen Center for Arthritis Research (COPECARE), Center for Rheumatology and Spine Diseases, Centre for Head and Orthopedics, Rigshospitalet, Glostrup, Denmark
- 7Department of Clinical Medicine, Faculty of Health and Medical Sciences, University of Copenhagen, Copenhagen, Denmark
- 8Department of Rheumatology, Zealand University Hospital, Køge, Denmark
- 9Department of Medicine (2), Holbæk Hospital, Holbæk, Denmark
- 10Department of Rheumatology, Odense University Hospital, Odense, Denmark
- 11Department of Rheumatology, University Hospital of Southern Denmark, Esbjerg, Denmark
The DANIsh VASculitis cohort study, DANIVAS, is an observational national multicenter study with the overall aim to prospectively collect protocolized clinical data and biobank material from patients with polymyalgia rheumatica (PMR) and giant cell arteritis (GCA) diagnosed and/or followed at Danish rheumatology departments. A long-term key objective is to investigate whether the use of new clinically implemented diagnostic imaging modalities facilitates disease stratification in the GCA-PMR disease spectrum. In particular, we aim to evaluate treatment requirements in GCA patients with and without large-vessel involvement, treatment needs in PMR patients with and without subclinical giant cell arteritis, and the prognostic role of imaging with respect to aneurysm development. Hence, in GCA and PMR, imaging stratification is hypothesized to be able to guide management strategies. With an established infrastructure within rheumatology for clinical studies in Denmark, the infrastructure of the Danish Rheumatologic Biobank, and the possibility to cross-link data with valid nationwide registries, the DANIVAS project holds an exceptional possibility to collect comprehensive real-world data on diagnosis, disease severity, disease duration, treatment effect, complications, and adverse events. In this paper, we present the research protocol for the DANIVAS study.
Clinical trial registration: https://clinicaltrials.gov/, identifier NCT05935709.
Introduction
In recent years, research advancements in giant cell arteritis (GCA) and polymyalgia rheumatica (PMR) have improved diagnosis and treatment approaches. Imaging tests have become integral in diagnosing GCA, improving diagnostic reliability, promoting fast diagnosis, and expediting treatment initiation, thereby reducing complications (1–10). Vascular ultrasound has high diagnostic accuracy, is a cheap and non-invasive procedure, and can be performed bedside. Therefore, vascular ultrasound of temporal and axillary arteries is recommended as a first-line diagnostic tool in patients suspected of GCA. A whole-body 18F FDG PET/CT and a cranial MR have comparable diagnostic properties and can be used as alternatives or in unresolved patients (9, 10). Few studies exploring the potential value of imaging in PMR have been performed (11–15), but recent reports suggest an overall benefit of early referral and specialist care of PMR patients (16–20). Additionally, new glucocorticoid-sparing treatment options for GCA and PMR have emerged, and several clinical trials are ongoing (18, 21).
Despite these improvements in GCA and PMR management, several unmet needs call for systematic prospective observational and long-term follow-up studies in real-world settings.
GCA and PMR have different initial glucocorticoid requirements, but a long-term glucocorticoid -tapering regime over 1–2 years is the treatment target for both diseases (6, 22, 23). However, relapses are frequent, and longer treatment is often required carrying a high risk of glucocorticoid adverse events (24–29). In addition, the risk of complications and the lack of valid clinical tools to assess activity imply a high risk of over-treatment. Specific indications for initiation and optimal timing of tapering or discontinuation of IL-6 inhibitor treatment remain unresolved (30–37). To select patients who gain the most from early add-on steroid sparring therapy and to guide treatment strategy, baseline stratification tools and disease activity biomarkers are highly needed.
Despite the diagnostic value of imaging and its sensitivity to change after the institution of glucocorticoids, its prognostic value and ability to discriminate remission and relapse in clinical routine care remain less clear (7, 9, 25, 38–41). Imaging facilitates new insight into disease distribution and severity that may have prognostic potential, as, for example, discriminating large-vessel and cranial vessel involvement in GCA or by identification of subclinical GCA in phenotypic PMR (42).
Epidemiologic studies and smaller cohort studies consistently report an increased risk of vascular complications such as aortic aneurysms and dissection later in the disease course of GCA (43–46). Although the development of aortic aneurysm and dissection can be fatal, incidence rates are still low and progression rates vary (46). Current guidelines only recommend screening for aortic complications on an individual basis but do not provide any guidance for the identification of patients at risk (6, 10, 47).
In Denmark, the optimal conditions for the establishment of a national GCA and PMR research collaboration exist. The highest incidences of GCA and PMR are found in the Scandinavian countries (24), and all GCA patients and many PMR patients are evaluated and diagnosed by a rheumatologist. In addition, within the Danish Rheumatology Society, established experience and infrastructure for clinical cohort studies in GCA and PMR and the Danish Rheumatologic Biobank are present (2, 8, 48, 49). In line with Danish and European guidelines, imaging has been gradually implemented, allowing imaging-based disease characterization. Furthermore, linkage to Danish nationwide administrative registries with data on, e.g., diagnosis, prescriptions, laboratory and pathology results, time, and cause of death is available and provide important complementary data (50). Alignment with similar European cohorts has been strived for when selecting data variables for the study and developing the DANIVAS data collection instrument. Taken together, the DANIVAS cohort study will include crucial data providing new insight into GCA/PMR management and disease course, with a particular emphasis on the prognostic value of imaging-based disease stratification. Even more, DANIVAS enables data comparison across cohorts and supports future international research collaboration.
In this paper, we present the protocol for the DANIVAS study.
Study design
A national multicenter prospective observational study of incident and prevalent patients with PMR and GCA diagnosed and/or followed at Danish rheumatology departments.
Descriptive clinical data are collected in a web-based, clinician-driven database, and blood samples are collected through the infrastructure of the Danish Rheumatologic Biobank. Complementary data are obtained from national administrative registries.
Study objectives
The overall aim of the DANIVAS cohort study is to improve disease control and reduce disease- and treatment-related damage in GCA and PMR. The study objective is to investigate the use of new diagnostic imaging modalities for facilitating disease stratification that can potentially predict treatment requirements and complications and hence guide management strategies. Specific primary, key secondary, secondary, and exploratory objectives are listed in Table 1.
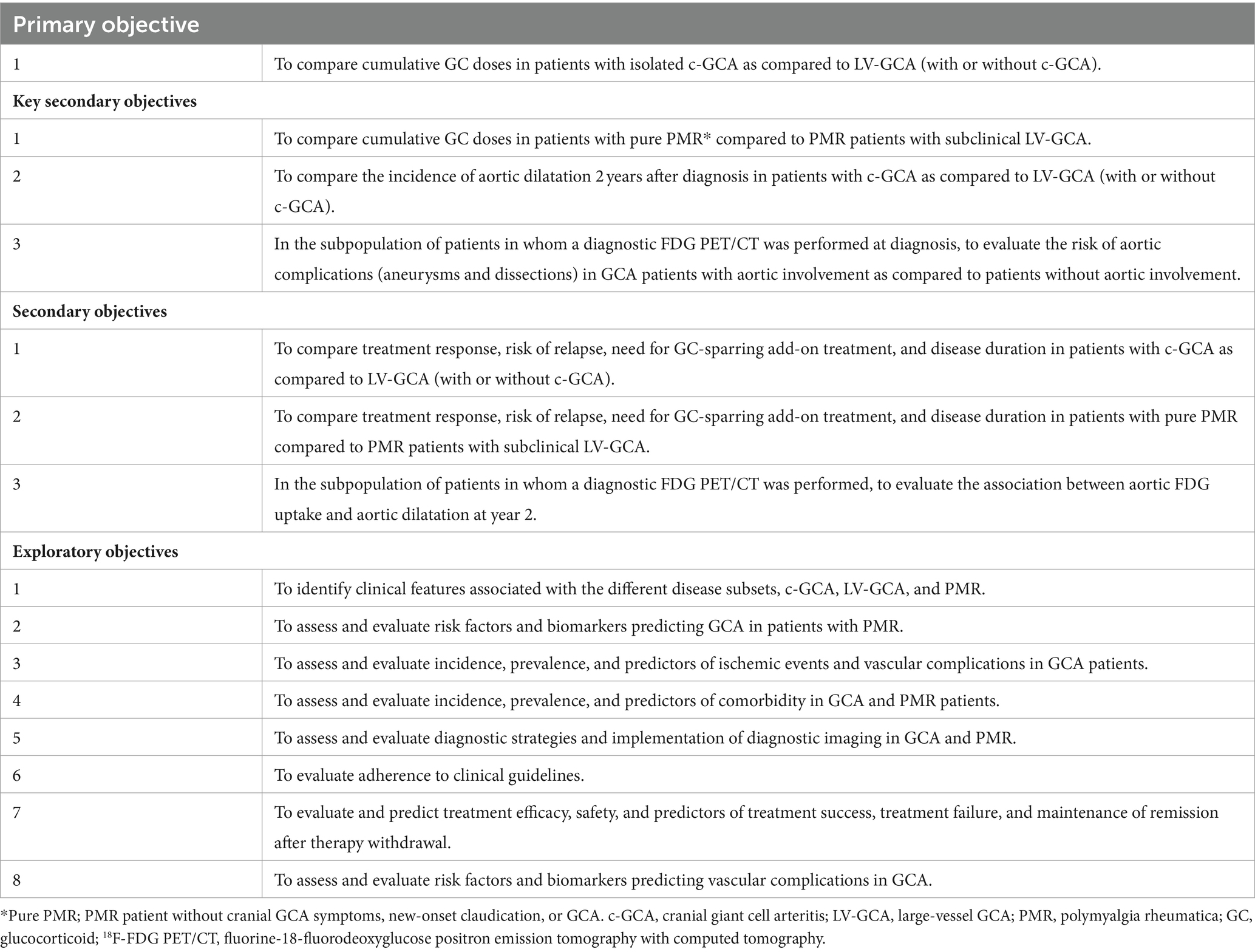
Table 1. Catalog of study objectives.
On top of the specific research objectives, the systematic collection of prospective clinical data and biobank blood samples provides a fundamental basis for future research projects and a scientific framework for Danish GCA/PMR researchers and for international research collaborations.
Methods and analysis
Data collection and setting
Clinical data (including imaging, blood tests, and histology), demographics, patient-reported outcomes, and biobank samples will be collected at baseline and during follow-up for as long as patients are seen in the rheumatology departments. For an angiographic sub-study, structural damage of the aorta will be assessed in a subset of GCA patients 2 years after diagnosis. Data on long-term complications, comorbidity, death and migration, and time and amount of retrieved glucocorticoid prescriptions will be collected through Danish registries.
Patients will be treated according to the Danish national treatment guideline for GCA and PMR, which adhere to current European recommendations (6, 22, 23).
The study was registered in ClinicalTrials.gov (NCT05935709) on 28 June 2023.
Recruitment
Patients will be recruited from Danish rheumatology departments at routine visits either at the time of diagnosis or during the disease course.
Enrollment was initiated on 1 November 2023 from two centers in order to test the feasibility of study organization and data collection. Within the next year, all rheumatology departments at Danish hospitals will be invited to participate in the study. The last patient’s first visit is expected by the end of 2039.
The potential for recruitment from Danish rheumatology departments is excellent. High referral rates can be expected according to the Danish national GCA and PMR management guidelines that encourage PMR evaluation by rheumatologists and recommend that all patients suspected of GCA are referred for prompt diagnostic evaluation by a rheumatologist, the latter including diagnostic imaging performed in a hospital setting.
Study population
Sample size
In-depth disease characterization by the time of inclusion, including reporting on vessel involvement according to imaging results, allows for both incident and prevalent GCA and PMR patients to contribute to the primary and secondary outcomes. A sample size calculation was made based on the primary outcome reaching a total number of 3,000 GCA patients to be included. Assuming a pooled standard deviation of 8,500 mg (24, 51), and an equal distribution between the groups (c-GCA and LV-GCA), each group requires 1,519 samples to achieve 90% power and a 5% significance level (two-sided) for detecting a true difference in mean cumulated glucocorticoid dose of 1,000 mg between the two groups. Based on incidence rates and the proportion of referrals, we expect to be able to include the same number of PMR patients (16, 18). Expecting subclinical GCA in 20% of PMR patients and assuming a similar pooled standard deviation (52, 53), 1,370 PMR patients are needed to achieve 90% power and a 5% significance level (two-sided) for detecting a true difference in mean cumulated glucocorticoid dose of 2000 mg between the two groups (PMR with and without subclinical GCA).
Eligibility
Patients can be included at any time during the disease course. By the time of inclusion, patients will be registered as either incident (newly diagnosed within the last 3 months) or prevalent (included during routine follow-up >3 months after and ≤ 5 years after diagnosis) cases. Inclusion criteria are as follows:
• GCA and/or PMR diagnosis established or confirmed by a rheumatologist (clinical expert opinion), and
• Speak and understand Danish, and
• Are able to give signed and dated informed consent.
Patients diagnosed with other systemic autoimmune diseases that out-rule the diagnosis of GCA or PMR and patients diagnosed >5 years ago will not be included.
For participation in the angiography sub-study, patients included more than 2 years after diagnosis or with contraindications for the angiography (claustrophobia, body weight > 150 kg, pacemaker, metallic foreign body, and eGFR<30) will not be included.
Visits
The study visit schedule is adapted to standard programs for managing PMR and GCA patients in routine clinical care. In routine rheumatology care in Denmark, GCA patients are typically followed up 2–12 months after treatment discontinuation, while the follow-up schedule for PMR patients varies. The study design is illustrated in Figure 1. The following study visits will be conducted:
• Enrollment visit: First visit to obtain informed consent and collect master data regarding diagnostic subgroup classification and demography.
• Response visit: Second visit 2 months after diagnosis (only incident patients).
• Routine study visits: Six months after diagnosis (incident patients and prevalent patients included <4 months after diagnosis) and subsequently every year as long as patients are seen at the rheumatology department.
• Aortic screening visit: Two years after diagnosis, screening for aortic complications will be performed
• Withdrawal visit: Visit to complete study participation due to stable drug-free remission or dismission from rheumatology care, patients’ request, or in the event of death, migration, non-compliance, or if GCA/PMR diagnosis is dismissed.
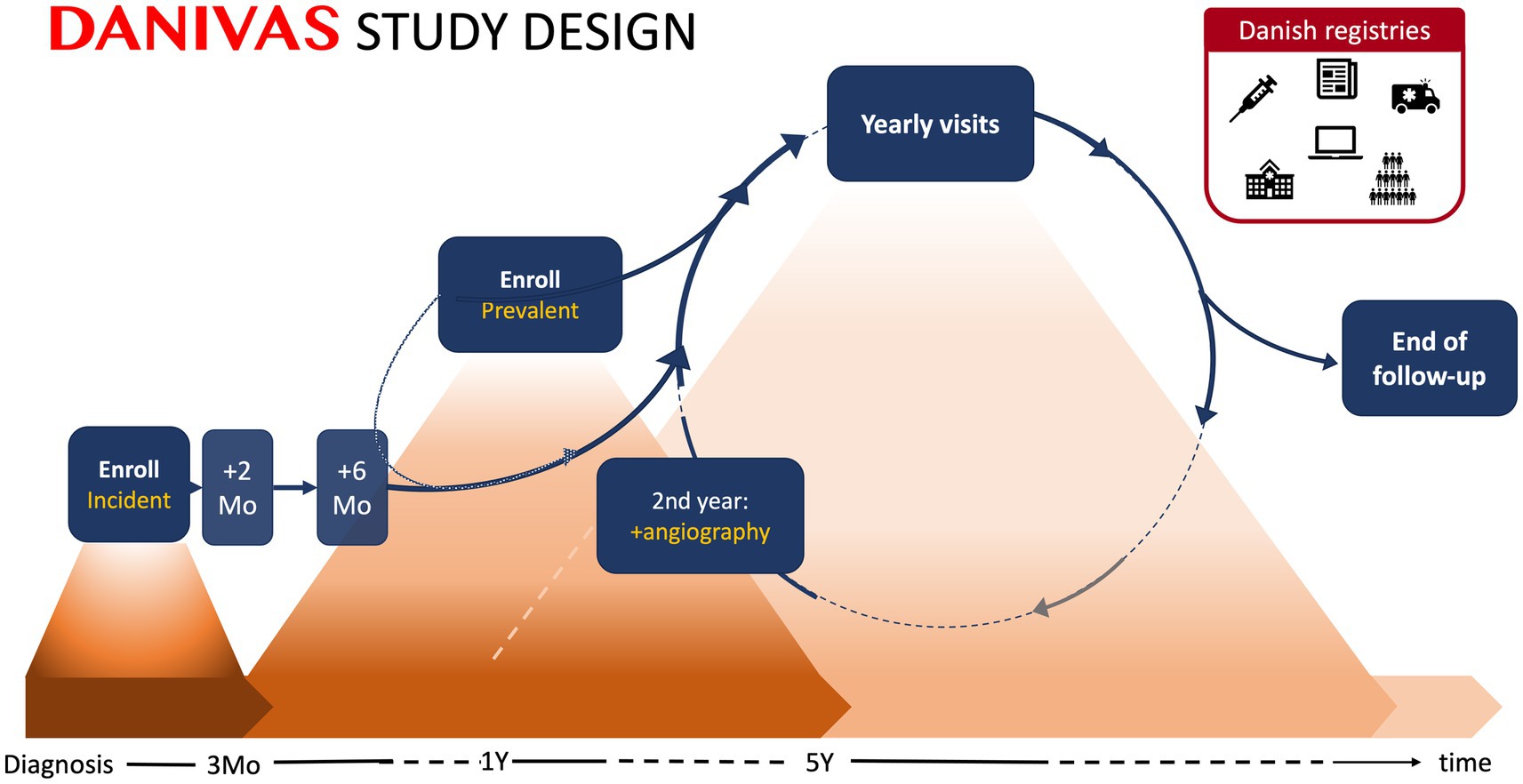
Figure 1. DANIVAS study design. Patients are enrolled at any time during their disease course (≤5 years disease duration) and will be registered as either incident (within 3 months of diagnosis) or prevalent. Study visits will be performed 2 (response visit) and 6 months after diagnosis (incident patients and prevalent patients included <4 months after diagnosis) and subsequently every year (all patients). At the 2-year follow-up, aortic angiography will be performed in a subset of GCA patients. Data collection for the enrollment visits and other study visits (2-month response visit, 6 months visit, and annual visits) are described in more detail in the ‘Data collection’ section and Table 2. Clinical follow-up is terminated by the time of stable drug-free remission or dismission from rheumatology care, on patient’s request or in the event of death, migration, non-compliance, or if the diagnosis is dismissed. Linkage of data across nationwide medical and administrative registries at the individual level will be performed to enrich outcome and covariate data. Mo, month; Y, year.

Table 2. Schedule of procedures and assessments at baseline, follow-up, and withdrawal.
Data collection
An overview of the data collection at each study visit is presented in Table 2. All procedures, but the 2-year angiography, are performed on clinical indication according to clinical guidelines as part of routine care. As not all routine care visits are necessarily performed as study visits, the data collection at each study visit also serves the purpose of summarizing disease-related medical events in the interim period.
Diagnostic information and referral history
Diagnostic information regarding symptom onset, presentation, referral history, diagnostic work-up, time and type of clinical diagnosis (GCA and/or PMR as considered by the treating physician), and initial treatment will be recorded by the time of enrollment.
For patients with a clinical diagnosis of GCA, it will be recorded if a diagnostic test, that is temporal artery biopsy, vascular ultrasonography, 18F FDG PET/CT, MR, or CT-angiography, was conducted or not, and if so, whether the result was positive, inconclusive, or negative for GCA diagnosis.
For patients with a clinical diagnosis of PMR, it will be recorded if the following diagnostic tests either supporting PMR or excluding differential diagnosis was performed: musculoskeletal hip and shoulder ultrasonography, 18F FDG PET/CT, negative vascular ultrasonography, computed tomography of chest, abdomen, and pelvis, or other investigation to evaluate potential malignancy. Assessment of the variables included in the 2022 ACR/EULAR classification criteria for GCA and/or 2012 EULAR classification criteria for PMR will be registered.
Definition of imaging-based disease stratification groups
The Danish Society of Rheumatology endorses adherence to EULAR recommendations regarding the diagnostic evaluation of patients suspected of GCA and/or PMR (6, 10, 23). Consequently, we expect GCA patients to have at least one vascular imaging procedure performed, and in case of negative or inconclusive results. That additional tests to confirm diagnosis will be made. Vascular ultrasonography, including the assessment of temporal and axillary arteries as a minimum, is performed by trained rheumatologists, and recommended technical and procedural requirements are met (10, 54). Diagnostic conclusions are made according to OMERACT definitions (55). Recording of other imaging and pathology results relies on the radiology/pathology report and is interpreted according to procedural recommendations and accepted diagnostic criteria (56, 57).
GCA patients with a positive imaging test or histology will be categorized according to vessel involvement as ‘c-GCA’ and/or ‘LV-GCA’. C-GCA is defined as the involvement of cranial arteries including, but not limited to temporal, facial, occipital, maxillary, and vertebral arteries, whereas LV-GCA is defined as the involvement of extracranial large arteries including but not limited to aorta and/or its primary branches (e.g., carotid, subclavian, axillary, and femoral arteries). If applicable, the presence or absence of aortitis will be recorded.
In patients with concomitant GCA and PMR, it will be recorded if GCA is subclinical, that is vasculitis is diagnosed by imaging or histology in the absence of cranial or claudication symptoms attributed to GCA (12).
Diagnosis and disease stratification will continuously be revised according to diagnostic test results available (at study visits and retrospectively).
Demography
Age, gender, height, weight, and history of smoking and alcohol consumption will be recorded at enrollment.
Clinical evaluation
New or persistent symptoms and findings of GCA and (58) will be recorded at each visit if present. Cranial symptoms and findings recorded include headache, scalp tenderness, jaw or tongue claudication, visual disturbances (sight loss, amaurosis fugax, and double vision), abnormal temporal artery (tender, swollen, and pulseless), scalp necrosis, transient ischemic attack, or stroke. Large-vessel symptoms include arm or leg claudication, carotidynia, brachial blood pressure difference > 10 mmHg, pulselessness, or large-vessel bruits. PMR symptoms and findings recorded include symmetric shoulder pain and stiffness, symmetric hip pain and stiffness, mobility of upper arms, PMR activity score (58), RS3PE (remitting seronegative symmetrical synovitis with pitting edema), and peripheral arthritis. Constitutional symptoms include fever, weight loss, night sweats, and malaise. New symptoms are defined as new onset or worsening within 4 weeks, whereas symptoms lasting without worsening for >4 weeks are considered persistent. The physician’s assessment of disease activity based on clinical evaluation (physician NRS and physician disease activity category; remission, potential relapse without treatment escalation, relapse (treatment escalation), and refractory disease) will be recorded. Relapses will be categorized as minor or major according to EULAR definitions (10). Any relapse that leads to treatment intensification since the last study visit will also be recorded.
Medical history and adverse events
At each visit, the current dose of glucocorticoid, tsDMARD, and/or bDMARD treatment and changes since the last visit are recorded. Date of start, change, and discontinuation of immunosuppressive therapy and reasons (start or increase: risk of disease complications, refractory disease, repeated relapses, relapse on unacceptable high glucocorticoid doses, adverse effects from other immunosuppressive therapy, and comorbidity. Discontinuation or decrease: remission, adverse events, or no effect) for these will be recorded.
Complications
At each visit, potential disease-related complications, including visual impairment and vascular complications including aortic dilatation and aortic dissection, and the time of the event will be recorded.
Comorbidity
Comorbidity including cardiovascular disease, hypertension, hypercholesterolemia, diabetes, chronic kidney disease, osteoporosis, chronic lung disease, infections, or malignancies will be recorded at the baseline visit. Routine clinical monitoring of HbA1c levels and results of DXA scans will be recorded continuously.
Patient-reported outcome measures (PROMs)
At each visit, patients will be asked to report their global disease activity [Numerical Rating Scale (NRS), 0–10] and the duration of morning stiffness (minutes) will be recorded.
Laboratory tests and biobank
Routine blood analysis, including C-reactive protein and glycated hemoglobin (HbA1c), will be performed as a standard of care. Additionally, biobank blood samples for future research purposes are collected by the infrastructure of the clinical biobank Danish Rheumatologic Biobank under the interregional Bio- and Genome Bank Denmark. Biobank blood samples will be collected at each study visit.
Aortic screening visit
In a subpopulation of GCA patients, an aortic angiography will be scheduled 2 years after diagnosis to screen for aortic dilatation and aneurysms. The angiography can be performed as either CT or MR angiography and will be performed according to local set-up and imaging acquisition protocols. Subsequent aortic imaging will be performed on clinical indications at an individual basis at the discretion of the treating physician.
Linkage with registries
Danish residents receive a unique 10-digit civil registration number by the time of birth or immigration that ensures the linkage of data across nationwide health and administrative registries at the individual level (Table 3). This linkage will ensure the collection of data on events, and treatment occurring after consultations in rheumatology departments has been terminated as well as the follow-up time.
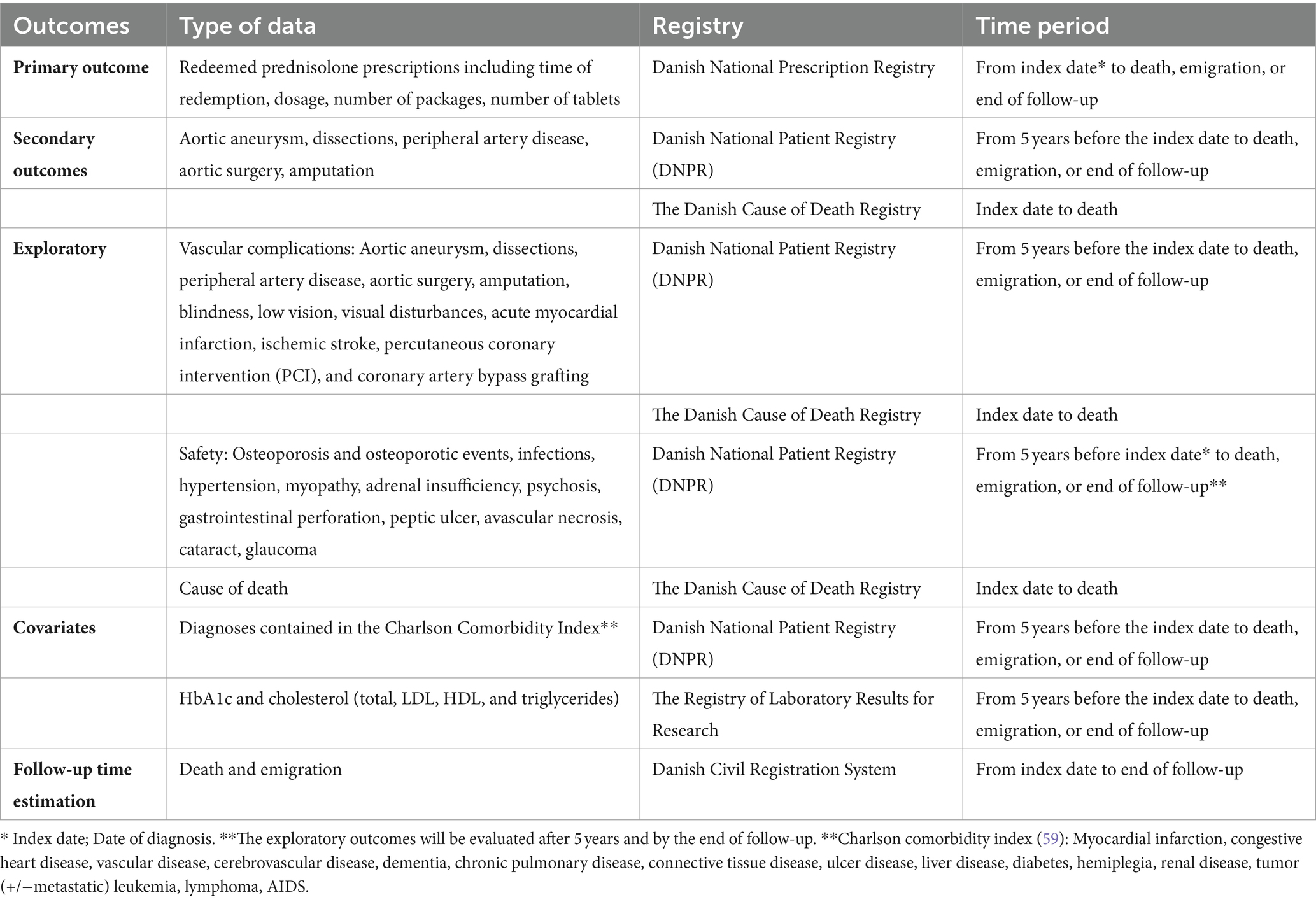
Table 3. Data from national registries.
The cumulated dose of glucocorticoid, time of glucocorticoid treatment, and potential treatment-free remission will be estimated based on redeemed prednisolone prescriptions obtained through the Danish National Prescription Registry (DPR).
Linkage with the Danish National Patient Registry (DNPR), the Danish Cause of Death Registry, The Registry of Laboratory Results for Research (LABKA), and the Danish Civil Registration System is performed to enrich data regarding vascular complications, treatment-related complications, potential confounding diseases, time to event, death, immigration, or censoring.
Outcomes and data analysis plan
Primary outcome
1. Cumulative glucocorticoid doses will be calculated based on redeemed prescriptions from the time of diagnosis to the end of follow-up (date of data extraction, death, or emigration). The difference between LV-GCA (with and without c-GCA) and isolated c-GCA, as characterized in the DANIVAS database will be compared by Student’s t-test or Wilcoxon Mann–Whitney U-test.
Key secondary outcomes
1. Cumulative glucocorticoid doses will be calculated based on redeemed prescriptions from the time of diagnosis to the end of follow-up (date of data extraction, death, or emigration). The difference between patients with pure PMR compared to PMR patients with subclinical LV-GCA will be compared by Student’s t-test or Wilcoxon Mann–Whitney U-test.
2. The incidence of aortic dilatation 2 years after diagnosis in patients with isolated c-GCA as compared to LV-GCA (with or without c-GCA) will be compared by chi-square test. Incidences will be calculated as proportions, that is events per patient at risk, and as incidence rates, that is number of events divided by the sum of the person-time of the at-risk population. Associated 95% binomial confidence intervals will be calculated.
3. The risk of aortic complications (aneurysms and dissections) in GCA patients with aortic involvement as compared to patients without aortic involvement (in the subpopulation of patients diagnosed by PET/CT) will be compared by chi-square test and the association between baseline aortic FDG uptake intensity and aortic diameter at year 2 will be evaluated by linear regression or Spearman correlation.
For the primary and key secondary outcome 2, subgroup analysis will be performed on patients diagnosed with PET/CT and ultrasound, respectively. In addition, an analysis comparing cumulative glucocorticoid doses in isolated LV-GCA as compared to patients with c-GCA (with or without LV-GCA) will be performed.
Study organization, collaboration, and patient involvement
DANIVAS is led by a steering committee who has the overall scientific, organizational, and economic responsibility for DANIVAS. A DANIVAS research collaboration network of researchers within the field of GCA and PMR is built and will facilitate new research projects building upon the infrastructure of, and the teamwork within, DANIVAS.
Two patient research partners will be part of the steering committee. Patient research partners will be included in the research project according to” the European League Against Rheumatism recommendations for the inclusion of patient representatives in scientific projects” (60). In the selection of potential patient partners, communication skills, motivation, and constructive assertiveness in a team will be taken into account. Patient partners will prospectively ensure patients’ perspective on the relevance, feasibility, and added value of research initiatives as well as contribute to any needed adjustment of the study organization.
Through international research networks within the field of GCA and PMR, alignment of data collection with related European prospective GCA/PMR cohorts that are currently being developed was strived for in order to facilitate data comparison and future collaboration.
Data collection and management
Data collection is documented in the individual electronic Case Report Form. To ensure high data completeness, the data manager at the Department of Rheumatology, Aarhus University Hospital, monitors data completeness and a built-in notifications system automatically sends alerts to the site investigators in case of missing visits and, if unsolved, ultimately to the data manager.
Discussion
Although the implementation of diagnostic imaging has increased the awareness of the impact of disease extent and severity and led to the interpretation of GCA and PMR as overlapping diseases with a spectrum of disease manifestations and treatment requirements, the clinical impact on management and the therapeutic consequences remains mainly unsolved (42, 47).
Higher relapse rates or longer treatment needed for LV-GCA as compared to c-GCA has been reported in some studies (61–66), but not in all (67–70). In general, many of these studies are small, retrospective, and prone to selection or misclassification bias. Therefore, data to fully support early initiation of glucocorticoid-sparring therapy based on stratification by vessel involvement are still lacking.
Subclinical GCA occurs in approximately 20% of PMR patients (52, 53). However, many of these studies were performed in selected cohorts, questioning the true incidence. Nevertheless, a recent study reported higher relapse rates for PMR patients with subclinical GCA as compared to pure PMR patients (13) and smaller studies indicated a noteworthy risk of ischemic complications in this subgroup (71, 72). Accordingly, the routine diagnostic approach for patients with suspected PMR and the standard of care needed for patients with subclinical GCA need further evaluation (13).
Prospective long-term observational data of larger cohorts that allow for the evaluation of risk factors and prognostic biomarkers to identify patients at risk of aortic aneurysms and dissection and to reduce numbers needed to screen are lacking. Screening for aortic aneurysm would allow for timely surgical intervention to prevent aortic rupture. Although the relative risk for aortic rupture in GCA is high, the overall incidence rate is still low and time to event uncertain, challenging the development of screening algorithms (22, 46). Recent studies have indicated a positive association between the presence of vessel inflammation and subsequent vessel damage and a potential prognostic role of the presence of large-vessel involvement and the risk of aortic aneurysms (39, 45, 73, 74).
With systematic disease characterization including diagnostic imaging, which is highly implemented in the clinical care of GCA and PMR in Denmark, the DANIVAS cohort study provides essential data to address these needs.
Important differences between the results of real-world observational studies and RCT or single-center expert studies in GCA and PMR have been found and call for high-quality real-life data (2, 31, 75). Moreover, the potential drawbacks of smaller single-center cohort studies such as selection bias, lack of statistic power, and limited external validity can be overcome by a protocolized prospective national cohort study including GCA and PMR patients from both secondary and tertiary hospitals. The linkage of clinical data, including comprehensive disease characteristics, and registry data on an individual level provides unique insight into GCA and PMR disease courses. Hence, the DANIVAS cohort study holds the potential to improve diagnostic strategies and identify biomarkers of disease activity and prognosis, possibly providing tools to be implemented in daily clinical practice to personalize treatment strategies and hence improve effectiveness and safety. Moreover, translation and validation of the newly developed GCA-PRO and steroid-PRO to Danish versions are currently being performed. Incorporating these into DANIVAS in the future will gain supplementary information reflecting the impact of disease and its treatment on health-related quality of life (HRQoL) from the patient’s perspective (76, 77).
As a nationwide study aiming for inclusion and registration in everyday clinical care of patients with GCA and PMR in hospitality settings both with and without research experience within the field, the study comes with potential limitations. First, inclusion and data collection rely upon the clinician’s effort and may compete with other clinical obligations. Consequently, we cannot ensure all GCA and PMR patients are enrolled in the study. Careful pragmatic selection of data variables to be collected has been performed in order to ensure feasibility in a clinical context. However, this may also exclude appreciated but non-essential characteristics or confounders or outcomes. For instance, we did not find it possible to prioritize the collection of detailed vascular ultrasound data including the newly developed OGUS score or the complete set of variables included in the glucocorticoid toxicity index. For the latter, selected items can be obtained through the linkage with registries. Clinical data collection feasibility is currently being tested by clinicians, and data collection instruments and variables are adjusted if needed.
Although the majority of patients diagnosed with GCA are seen in hospital settings, and current guidelines endorse rheumatologic diagnostic evaluation of PMR patients also, not all patients with PMR are seen or followed in secondary care and the PMR cohort may be prone to selection bias toward more complicated cases.
Although imaging is recommended to establish GCA diagnosis and supplementary tests should be performed in patients with negative or inconclusive results, a smaller proportion of patients with a clinical diagnosis of GCA may not have a positive diagnostic test that allows stratification into defined disease subsets. Our primary outcome will be analyzed in patients that can be categorized based on diagnostic tests as described. A sensitivity analysis including patients with negative diagnostic tests will be performed stratifying these patients according to clinical symptoms.
Routine diagnostic imaging for GCA includes both cranial and large-vessel assessment. However, only evaluation of selected cranial and large vessels is needed to establish a diagnosis, potentially misclassifying some patients. However, it is well established that including axillary artery assessment, which is currently part of routine vascular ultrasonography examination in GCA, increases overall sensitivity (9) and also that axillary ultrasound depicts the majority of LV-GCA patients when PET/CT is used as a reference diagnosis(8). Screening for subclinical GCA in PMR is a matter of debate and may not need to be assessed in all PMR patients. However, diagnostic imaging is increasingly implemented in Denmark and cranial and large-vessel diagnostic imaging is performed in the majority of GCA patients and is increasingly used to assess for vessel involvement in PMR.
The timing of aortic damage evaluation was decided to address that the risk of aortic damage appears to be present from the time of diagnosis (39, 74, 78), with the cumulative incidence rising almost linearly over time (46) and to minimize death as a competing risk. Finally, it was considered feasible, to plan a 2-year follow-up imaging visit within the time frame of routine rheumatology care, minimizing loss to follow-up. Nevertheless, the timing also implies a risk of missing damage that is not yet detectable.
In September 2023, DANIVAS held its first annual DANIVAS research symposium to officially launch the DANIVAS cohort study to a broader audience of researchers and clinicians of the Danish rheumatology community and several rheumatology departments nationwide have committed to being part of the DANIVAS study. In November 2023, the first GCA and PMR patients were enrolled in the DANIVAS study. Within the next year, more Danish centers will be enrolled. On a longer perspective, the DANIVAS study is designed to improve the care and outcomes for patients with GCA and PMR.
Ethics statement
The study has been conducted in full conformance with the principles of the Declaration of Helsinki. The Central Denmark Region Committees on Health Research Ethics (reference number 1–10–72-174-22) have approved the DANIVAS study protocol. The DANIVAS study is registered in the Danish Central Region internal list of research projects (reference number 1–16–02-470-22). All patients included in the study gave their written informed consent.
Author contributions
BN: Conceptualization, Funding acquisition, Investigation, Methodology, Project administration, Writing – original draft, Writing – review & editing. SK: Conceptualization, Investigation, Methodology, Project administration, Writing – review & editing, Validation. AD: Investigation, Methodology, Project administration, Writing – review & editing. LT: Conceptualization, Investigation, Methodology, Project administration, Writing – review & editing. LD: Conceptualization, Investigation, Methodology, Project administration, Writing – review & editing. AC: Conceptualization, Investigation, Methodology, Project administration, Writing – review & editing. MH: Conceptualization, Investigation, Methodology, Project administration, Writing – review & editing. PH: Conceptualization, Investigation, Methodology, Project administration, Writing – review & editing. TE: Conceptualization, Investigation, Methodology, Project administration, Writing – review & editing. E-MH: Conceptualization, Funding acquisition, Investigation, Methodology, Project administration, Writing – review & editing. SC: Investigation, Methodology, Project administration, Writing – review & editing, Conceptualization. KK: Funding acquisition, Investigation, Methodology, Project administration, Writing – review & editing, Conceptualization.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. The study has received grants for the establishment and implementation of the database from AbbVie (Agr-2021-731-16898) and The Danish Rheumatism Association (R214-A8127). The funders were not involved in the study design, data collection or analysis plan, the writing of this article, or the decision to submit it for publication.
Conflict of interest
BN has received speaker’s fees from Novartis and AbbVie. AC has received research grants from Novartis, Janssen, GSK, Syneos, and personal fees from UCB. LT has received speaker’s fees from Janssen, Pfizer, and Novartis. LD has received a research grant (paid to the institution) from BMS and AbbVie outside the present work; travel expenses from Janssen, UCB, and Boehringer Ingelheim. MH has received a research grant (paid to Institution) from AbbVie, BMS, Eli Lilly, MSD, Pfizer, Sandoz, and Novartis; speaker’s fee (paid to Institution) from Medac, Pfizer, Sandoz, and speaker’s fee (personal) from Novartis. E-MH has received fees for speaking and/or consulting from Novo, Novartis, and SynAct Pharma; research funding to Aarhus University Hospital from Novo Nordic Foundation, Galapagos, AbbVie; travel expenses from Pfizer, Sobi, and AbbVie. SC received speaker’s fee from Pfizer, Novartis, and Roche.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Nielsen, BD, Hansen, IT, Kramer, S, Haraldsen, A, Hjorthaug, K, Bogsrud, TV, et al. Simple dichotomous assessment of cranial artery inflammation by conventional 18F-FDG PET/CT shows high accuracy for the diagnosis of giant cell arteritis: a case-control study. Eur J Nucl Med Mol Imaging. (2019) 46:184–93. doi: 10.1007/s00259-018-4106-0
2. Chrysidis, S, Døhn, UM, Terslev, L, Fredberg, U, Lorenzen, T, Christensen, R, et al. Diagnostic accuracy of vascular ultrasound in patients with suspected giant cell arteritis (EUREKA): a prospective, multicentre, non-interventional, cohort study. Lancet Rheumatol. (2021) 3:e865–73. doi: 10.1016/S2665-9913(21)00246-0
3. Patil, P, Williams, M, Maw, WW, Achilleos, K, Elsideeg, S, Dejaco, C, et al. Fast track pathway reduces sight loss in giant cell arteritis: results of a longitudinal observational cohort study. Clin Exp Rheumatol. (2015) 53:i5–6. doi: 10.1093/rheumatology/keu191
4. Diamantopoulos, AP, Haugeberg, G, Lindland, A, and Myklebust, G. The fast-track ultrasound clinic for early diagnosis of giant cell arteritis significantly reduces permanent visual impairment: towards a more effective strategy to improve clinical outcome in giant cell arteritis? Rheumatology (Oxford). (2016) 55:66–70. doi: 10.1093/rheumatology/kev289
5. Smith, SCM, Al-Hashimi, MR, Jones, CD, and Mukhtyar, CB. Frequency of visual involvement in a 10-year interdisciplinary cohort of patients with giant cell arteritis. Clin Med (Lond). (2023) 23:206–12. doi: 10.7861/clinmed.2022-0415
6. Hellmich, B, Agueda, A, Monti, S, Buttgereit, F, De Boysson, H, Brouwer, E, et al. Update of the EULAR recommendations for the management of large vessel vasculitis. Ann Rheum Dis. (2018) 79:19–130. doi: 10.1136/annrheumdis-2019-215672
7. Nielsen, BD, Gormsen, LC, Hansen, IT, Keller, KK, Therkildsen, P, and Hauge, E-M. Three days of high-dose glucocorticoid treatment attenuates large-vessel 18F-FDG uptake in large-vessel giant cell arteritis but with a limited impact on diagnostic accuracy. Eur J Nucl Med Mol Imaging. (2018) 45:1119–28. doi: 10.1007/s00259-018-4021-4
8. Nielsen, BD, Hansen, IT, Keller, KK, Therkildsen, P, Gormsen, LC, and Hauge, E. Diagnostic accuracy of ultrasound for detecting large-vessel giant cell arteritis using FDG PET / CT as the reference. Rheumatology (Oxford). (2019) 59:2062–73. doi: 10.1093/rheumatology/kez568
9. Bosch, P, Bond, M, Dejaco, C, Ponte, C, MacKie, SL, Falzon, L, et al. Imaging in diagnosis, monitoring and outcome prediction of large vessel vasculitis: a systematic literature review and meta-analysis informing the 2023 update of the EULAR recommendations. RMD Open. (2023):e003379. doi: 10.1136/rmdopen-2023-003379
10. Dejaco, C, Ramiro, S, Bond, M, Bosch, P, Ponte, C, Mackie, SL, et al. EULAR recommendations for the use of imaging in large vessel vasculitis in clinical practice: 2023 update. Ann Rheum Dis. (2023) 83:741–751. doi: 10.1136/ard-2023-224543
11. van der Geest, KSM, Treglia, G, Glaudemans, AWJM, Brouwer, E, Jamar, F, Slart, RHJA, et al. Diagnostic value of [18F]FDG-PET/CT in polymyalgia rheumatica: a systematic review and meta-analysis. Eur J Nucl Med Mol Imaging. (2021) 48:1876–89. doi: 10.1007/s00259-020-05162-6
12. De Miguel, E, Macchioni, P, Conticini, E, Campochiaro, C, Karalilova, R, Monti, S, et al. Prevalence and characteristics of subclinical giant cell arteritis in polymyalgia rheumatica. Rheumatology. (2023) 63:158–64. doi: 10.1093/rheumatology/kead189
13. De Miguel, E, Karalilova, R, Macchioni, P, Ponte, C, Conticini, E, Cowley, S, et al. Subclinical giant cell arteritis increases the risk of relapse in polymyalgia rheumatica. Ann Rheum Dis. (2023) 83:335–41. doi: 10.1136/ard-2023-224768
14. Owen, CE, Poon, AMT, Liu, B, Liew, DFL, Yap, LP, Yang, V, et al. Characterising polymyalgia rheumatica on whole-body 18 F-FDG PET/CT: an atlas.
15. Camellino, D, Duftner, C, and Dejaco, C. New insights into the role of imaging in polymyalgia rheumatica. Rheumatology. (2021) 60, 60:1016–33. doi: 10.1093/rheumatology/keaa646
16. Donskov, AO, Mackie, SL, Hauge, EM, Toro-Gutiérrez, CE, Hansen, IT, Hemmig, AK, et al. An international survey of current management practices for polymyalgia rheumatica by general practitioners and rheumatologists. Rheumatology. (2023) 62:2797–805. doi: 10.1093/rheumatology/keac713
17. Frølund, LL, Våben, C, Dam, M, Kjær, SG, Nielsen, BD, Østgård, RD, et al. Fast track clinic for early diagnosis of polymyalgia rheumatica: impact on symptom duration and prednisolone initiation. Joint Bone Spine. (2021) 88:105185. doi: 10.1016/j.jbspin.2021.105185
18. Espígol-Frigolé, G, Dejaco, C, Mackie, SL, Salvarani, C, Matteson, EL, and Cid, MC. Polymyalgia rheumatica. Lancet. (2023) 402:1459–72. doi: 10.1016/S0140-6736(23)01310-7
19. Krarup Keller, K, Mukhtyar, CB, Wiggers Nielsen, A, Katharina Hemmig, A, Louise Mackie, S, Eduardo Sattui, S, et al. Recommendations for early referral of individuals with suspected polymyalgia rheumatica: an initiative from the international giant cell arteritis and polymyalgia rheumatica study group. Ann Rheum Dis. (2023) 1–7. doi: 10.1136/ard-2023-225134 [Online ahead of print].
20. Chrysidis, S, Lage-Hansen, PR, Svendsen, N, and Diamantopoulos, AP. The fast-track outpatient clinic significantly decreases hospitalisation rates among polymyalgia rheumatica patients. BMC Rheumatol. (2021) 5:4–11. doi: 10.1186/s41927-021-00210-6
21. Nepal, D, Putman, M, and Unizony, S. Giant cell arteritis and polymyalgia Rheumatica: treatment approaches and new targets. Rheumatic disease. Clin North America. (2023) 49:505–21. doi: 10.1016/j.rdc.2023.03.005
22. MacKie, SL, Dejaco, C, Appenzeller, S, Camellino, D, Duftner, C, Gonzalez-Chiappe, S, et al. British Society for Rheumatology guideline on diagnosis and treatment of giant cell arteritis. Rheumatology. (2020) 59:e1–e23. doi: 10.1093/rheumatology/kez672
23. Dejaco, C, Singh, YP, Perel, P, Hutchings, A, Camellino, D, Mackie, S, et al. Recommendations for the management of polymyalgia rheumatica: a European league against rheumatism/American College of Rheumatology collaborative initiative. Ann Rheum Dis. (2015) 2015:1799–807. doi: 10.1136/annrheumdis-2015-207492
24. Therkildsen, P, de Thurah, A, Hansen, IT, Nørgaard, M, Nielsen, BD, and Hauge, EM. Giant cell arteritis: a nationwide, population-based cohort study on incidence, diagnostic imaging, and glucocorticoid treatment. Semin Arthritis Rheum. (2021) 51:360–6. doi: 10.1016/j.semarthrit.2021.01.007
25. Moreel, L, Betrains, A, Molenberghs, G, Vanderschueren, S, and Blockmans, D. Epidemiology and predictors of relapse in giant cell arteritis: a systematic review and meta-analysis. Joint Bone Spine. (2023) 90:105494. doi: 10.1016/j.jbspin.2022.105494
26. Therkildsen, P, Nielsen, BD, De Thurah, A, Hansen, IT, Nørgaard, M, and Hauge, EM. All-cause and cause-specific mortality in patients with giant cell arteritis: a nationwide, population-based cohort study. Rheumatology (United Kingdom). (2022) 61:1195–203. doi: 10.1093/rheumatology/keab507
27. Best, JH, Kong, AM, Unizony, S, Tran, O, and Michalska, M. Risk of potential glucocorticoid-related adverse events in patients with Giant cell arteritis: results from a USA-based electronic health records database. Rheumatol Ther. (2019) 6:599–610. doi: 10.1007/s40744-019-00180-9
28. Mahr, A, Hachulla, E, de Boysson, H, Guerroui, N, Héron, E, Vinzio, S, et al. Presentation and real-world Management of Giant Cell Arteritis (Artemis study). Front Med (Lausanne). (2021) 8:1–9. doi: 10.3389/fmed.2021.732934
29. Therkildsen, P, de Thurah, A, Nielsen, BD, Faurschou, M, Baslund, B, Hansen, IT, et al. The one-year infection risk among patients diagnosed with giant cell arteritis: use of antibiotics and hospitalisations. Rheumatology. (2024). doi: 10.1093/rheumatology/keae107
30. Samec, MJ, Rakholiya, J, Langenfeld, H, Crowson, CS, Abril, A, Wang, B, et al. Relapse risk and safety of long-term Tocilizumab use among patients with Giant cell arteritis: a single-enterprise cohort study. J Rheumatol. (2023) 50:1310. doi: 10.3899/jrheum.2022-1214
31. Calderón-Goercke, M, Castañeda, S, Aldasoro, V, Villa, I, Prieto-Peña, D, Atienza-Mateo, B, et al. Tocilizumab in giant cell arteritis: differences between the GiACTA trial and a multicentre series of patients from the clinical practice. Clin Exp Rheumatol. (2020) 124:112–119.
32. Calderón-Goercke, M, Loricera, J, Moriano, C, Castañeda, S, Narváez, J, Aldasoro, V, et al. Optimisation of tocilizumab therapy in giant cell arteritis. A multicentre real-life study of 471 patients. Clin Exp Rheumatol. (2023) 41:829–36. doi: 10.55563/clinexprheumatol/oqs8u9
33. de Boysson, H, De, BM, Blaison, F, Daumas, A, Jarrot, P, Perrin, F, et al. Assessment of the efficacy and safety of tocilizumab in patients over 80 years health and care evidence, from health education England. Arthritis Res Ther. (2021) 23:1–7. doi: 10.1186/s13075-021-02529-4
34. Regola, F, Cerudelli, E, Bosio, G, Andreoli, L, Tincani, A, Franceschini, F, et al. Long-term treatment with tocilizumab in giant cell arteritis: efficacy and safety in a monocentric cohort of patients. Rheumatol Adv Pract. (2020) 4:1–9. doi: 10.1093/rap/rkaa017
35. Spiera, RF, Unizony, S, Warrington, KJ, Sloane, J, Giannelou, A, Nivens, MC, et al. Sarilumab for relapse of polymyalgia Rheumatica during glucocorticoid taper. N Engl J Med [Internet]. (2023) 389:1263–72. doi: 10.1056/NEJMoa2303452
36. Devauchelle-Pensec, V, Carvajal-Alegria, G, Dernis, E, Richez, C, Truchetet, ME, Wendling, D, et al. Effect of tocilizumab on disease activity in patients with active polymyalgia rheumatica receiving glucocorticoid therapy: a randomized clinical trial. JAMA. (2022) 328:1053. doi: 10.1001/jama.2022.15459
37. Bonelli, M, Radner, H, Kerschbaumer, A, Mrak, D, Durechova, M, Stieger, J, et al. Tocilizumab in patients with new onset polymyalgia rheumatica (PMR-SPARE): a phase 2/3 randomised controlled trial. Ann Rheum Dis. (2022) 81:838–44. doi: 10.1136/annrheumdis-2021-221126
38. Nielsen, BD, Therkildsen, P, Keller, KK, Gormsen, LC, Hansen, IT, and Hauge, E-M. Ultrasonography in the assessment of disease activity in cranial and large-vessel giant cell arteritis: a prospective follow-up study. Rheumatology. (2023) 62:3084–94. doi: 10.1093/rheumatology/kead028
39. Moreel, L, Coudyzer, W, Boeckxstaens, L, Betrains, A, Molenberghs, G, Vanderschueren, S, et al. Association between vascular 18F-Fluorodeoxyglucose uptake at diagnosis and change in aortic dimensions in Giant cell arteritis. Ann Intern Med. (2023) 17:1321–9. doi: 10.7326/M23-0679,
40. Billet, AC, Thibault, T, Liozon, É, De Boysson, H, Perard, L, Espitia, O, et al. Prognostic value of 18 FDG-PET at diagnosis and follow-up in giant cell arteritis: an observational restrospective study. Eur J Intern Med. (2024) 7:S0953-6205(24)00145-6. doi: 10.1016/j.ejim.2024.03.037
41. Molina-Collada, J, Monjo-Henry, I, Fernández-Fernández, E, María Álvaro-Gracia, J, De Miguel, E, and Molina Collada, J. The OMERACT giant cell arteritis ultrasonography score: a potential predictive outcome to assess the risk of relapse during follow-up. Rheumatology. (2024) 8:keae260. doi: 10.1093/rheumatology/keae260
42. Tomelleri, A, van der Geest, KSM, Khurshid, MA, Sebastian, A, Coath, F, Robbins, D, et al. Disease stratification in GCA and PMR: state of the art and future perspectives. Nat Rev Rheumatol. (2023) 19:446–59. doi: 10.1038/s41584-023-00976-8
43. Robson, JC, Kiran, A, Maskell, J, Hutchings, A, Arden, N, Dasgupta, B, et al. The relative risk of aortic aneurysm in patients with giant cell arteritis compared with the general population of the UK. Ann Rheum Dis. (2015) 74:129–35. doi: 10.1136/annrheumdis-2013-204113
44. Jud, P, Verheyen, N, Dejaco, C, Haas, E, Szolar, D, Meinitzer, A, et al. Prevalence and prognostic factors for aortic dilatation in giant cell arteritis – a longitudinal study. Semin Arthritis Rheum. (2021) 51:911–8. doi: 10.1016/j.semarthrit.2020.11.003
45. Muratore, F, Crescentini, F, Spaggiari, L, Pazzola, G, Casali, M, Boiardi, L, et al. Aortic dilatation in patients with large vessel vasculitis: a longitudinal case control study using PET/CT. Semin Arthritis Rheum. (2019) 48:1074–82. doi: 10.1016/j.semarthrit.2018.10.003
46. Therkildsen, P, de Thurah, AL, Nielsen, BD, Hansen, IT, Eldrup, N, Nørgaard, M, et al. Increased risk of thoracic aortic complications among patients with giant cell arteritis: a nationwide, population-based cohort study. Rheumatology (Oxford). (2021) 61:2931–41. doi: 10.1093/rheumatology/keab871
47. Dejaco, C, Kerschbaumer, A, Aletaha, D, Bond, M, Hysa, E, Camellino, D, et al. Treat-to-target recommendations in giant cell arteritis and polymyalgia rheumatica. Ann Rheum Dis. (2023) 83:48–57. doi: 10.1136/ard-2022-223429
48. Kringelbach, TM, Glintborg, B, Hogdall, EV, Johansen, JS, and Hetland, ML. Identification of new biomarkers to promote personalised treatment of patients with inflammatory rheumatic disease: protocol for an open cohort study. BMJ Open. (2018) 8:e019325. doi: 10.1136/bmjopen-2017-019325
49. Nielsen, AW, Hansen, IT, Berit Nielsen, D, Søren Kjaer, G, Nielsen, BD, Kjær, SG, et al. The effect of prednisolone and a short-term prednisolone discontinuation for the diagnostic accuracy of FDG-PET/CT in polymyalgia rheumatica-a prospective study of 101 patients. Eur J Nucl Med Mol Imaging. doi: 10.1007/s00259-024-06697-8
50. Schmidt, M, Pedersen, L, and Sørensen, HT. The Danish civil registration system as a tool in epidemiology. Eur J Epidemiol. (2014) 29:541–9. doi: 10.1007/s10654-014-9930-3
51. Wan, X, Wang, W, Liu, J, and Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med Res Methodol. (2014) 14:135. doi: 10.1186/1471-2288-14-135
52. Nielsen, AW, Frølund, LL, Våben, C, Bonde, AR, Gormsen, LC, de Thurah, AL, et al. Concurrent baseline diagnosis of giant cell arteritis and polymyalgia rheumatica – a systematic review and meta-analysis. 56, Sem Arthritis Rheumatism. (2022):152069, doi: 10.1016/j.semarthrit.2022.152069
53. Hemmig, AK, Gozzoli, D, Werlen, L, Ewald, H, Aschwanden, M, Blockmans, D, et al. Subclinical giant cell arteritis in new onset polymyalgia rheumatica a systematic review and meta-analysis of individual patient data. Semin Arthritis Rheum. (2022) 55:152017. doi: 10.1016/j.semarthrit.2022.152017
54. Terslev, L, Diamantopoulos, AP, Døhn, UM, Schmidt, WA, and Torp-Pedersen, S. Settings and artefacts relevant for Doppler ultrasound in large vessel vasculitis. Arthritis Res Ther. (2017) 19:167. doi: 10.1186/s13075-017-1374-1
55. Chrysidis, S, Duftner, C, Dejaco, C, Schäfer, VS, Ramiro, S, Carrara, G, et al. Definitions and reliability assessment of elementary ultrasound lesions in giant cell arteritis: a study from the OMERACT large vessel vasculitis ultrasound working group. RMD Open. (2018) 4:e000598. doi: 10.1136/rmdopen-2017-000598
56. Slart RHJA, Writing group W, Reviewer group R, Members of EANM Cardiovascular M of E, Members of EANM Infection & Inflammation M of EI&, Members of Committees, et al. FDG-PET/CT(a) imaging in large vessel vasculitis and polymyalgia rheumatica: joint procedural recommendation of the EANM, SNMMI, and the PET interest group (PIG), and endorsed by the ASNC. Eur J Nucl Med Mol Imaging. (2018) 45:1250–1269. doi: 10.1007/s00259-018-3973-8
57. Nair, V, Fishbein, GA, Padera, R, Seidman, MA, Castonguay, M, Leduc, C, et al. Consensus statement on the processing, interpretation and reporting of temporal artery biopsy for arteritis. Cardiovasc Pathol. (2023) 67:107574. Available from:. doi: 10.1016/j.carpath.2023.107574
58. Leeb, B, and Bird, H. A disease activity score for polymyalgia rheumatica. Ann Rheum Dis. (2004) 63:1279–83. doi: 10.1136/ard.2003.011379
59. Thygesen, SK, Christiansen, CF, Christensen, S, Lash, TL, and Sørensen, HT. The predictive value of ICD-10 diagnostic coding used to assess Charlson comorbidity index conditions in the population-based Danish National Registry of patients, vol. 11 (2011).
60. De Wit, MPT, Berlo, SE, Aanerud, GJ, Aletaha, D, Bijlsma, JW, Croucher, L, et al. European league against rheumatism recommendations for the inclusion of patient representatives in scientific projects. Ann Rheum Dis. (2011) 70:722–6. doi: 10.1136/ard.2010.135129
61. Genin, V, Alexandra, JF, de Boysson, H, Sailler, L, Samson, M, Granel, B, et al. Prognostic factors in giant cell arteritis associated aortitis with PET/CT and CT angiography at diagnosis. Semin Arthritis Rheum. (2023) 152172. doi: 10.1016/j.semarthrit.2023.152172
62. de Mornac, D, Espitia, O, Néel, A, Connault, J, Masseau, A, Espitia-Thibault, A, et al. Large-vessel involvement is predictive of multiple relapses in giant cell arteritis. Ther Adv Musculoskelet Dis. (2021) 13:1759720X2110090. doi: 10.1177/1759720X211009029
63. Muratore, F, Kermani, TA, Crowson, CS, Green, AB, Salvarani, C, Matteson, EL, et al. Large-vessel giant cell arteritis: a cohort study. Rheumatology (Oxford). (2015) 54:463–70. doi: 10.1093/rheumatology/keu329
64. Dumont, A, Parienti, JJ, Delmas, C, Boutemy, J, Maigné, G, Silva, NM, et al. Factors associated with relapse and dependence on glucocorticoids in giant cell arteritis. J Rheumatol. (2020) 47:108–16. doi: 10.3899/jrheum.181127
65. Sugihara, T, Hasegawa, H, Uchida, HA, Yoshifuji, H, Watanabe, Y, Amiya, E, et al. Associated factors of poor treatment outcomes in patients with giant cell arteritis: clinical implication of large vessel lesions. Arthritis Res Ther. (2020) 22:72. doi: 10.1186/s13075-020-02171-6
66. Bosch, P, Dejaco, C, Schmidt, WA, Schlüter, KD, Pregartner, G, and Schäfer, VS. Association of ultrasound-confirmed axillary artery vasculitis and clinical outcomes in giant cell arteritis. Semin Arthritis Rheum. (2022) 56:152051. doi: 10.1016/j.semarthrit.2022.152051
67. Schmidt, WA, Moll, A, Seifert, A, Schicke, B, Gromnica-Ihle, E, and Krause, A. Prognosis of large-vessel giant cell arteritis. Rheumatology. (2008) 47:1406–8. doi: 10.1093/rheumatology/ken258
68. Tomelleri, A, Campochiaro, C, Sartorelli, S, Farina, N, Baldissera, E, and Dagna, L. Presenting features and outcomes of cranial-limited and large-vessel giant cell arteritis: a retrospective cohort study. Scand J Rheumatol. (2022) 51:59–66. doi: 10.1080/03009742.2021.1889025
69. de Boysson, H, Liozon, E, Lambert, M, Dumont, A, Boutemy, J, Maigné, G, et al. Giant-cell arteritis: do we treat patients with large-vessel involvement differently? Am J Med. (2017) 130:992–5. doi: 10.1016/j.amjmed.2017.03.054
70. Esperança Almeida, D, Smith, K, Sarker, BA, Barr, A, Wakefield, RJ, and Mackie, SL. Does the halo count on temporal and axillary ultrasound predict time to relapse in giant cell arteritis? Rheumatology (United Kingdom). (2023) 62:3710–3714.
71. Narváez, J, Estrada, P, López-Vives, L, Ricse, M, Zacarías, A, Heredia, S, et al. Prevalence of ischemic complications in patients with giant cell arteritis presenting with apparently isolated polymyalgia rheumatica. Semin Arthritis Rheum. (2015) 45:328–33. doi: 10.1016/j.semarthrit.2015.06.009
72. Hernández-Rodríguez, J, Font, C, García-Martínez, A, Espígol-Frigolé, G, Sanmartí, R, Cañete, JD, et al. Development of ischemic complications in patients with Giant cell arteritis presenting with apparently isolated polymyalgia Rheumatica. Medicine. (2007) 86:233–41. doi: 10.1097/MD.0b013e318145275c
73. Quinn, KA, Ahlman, MA, Alessi, HD, LaValley, MP, Neogi, T, Marko, J, et al. Association of 18F-Fluorodeoxyglucose–positron emission tomography activity with angiographic progression of disease in large vessel Vasculitis. Arthritis Rheumatol. (2023) 75:98–107. doi: 10.1002/art.42290
74. de Boysson, H, Daumas, A, Vautier, M, Parienti, J-J, Liozon, E, Lambert, M, et al. Large-vessel involvement and aortic dilation in giant-cell arteritis. A multicenter study of 549 patients. Autoimmun Rev. (2018) 17:391–8. doi: 10.1016/j.autrev.2017.11.029
75. Luqmani, R, Lee, E, Singh, S, Gillett, M, Schmidt, WA, Bradburn, M, et al. The role of ultrasound compared to biopsy of temporal arteries in the diagnosis and treatment of giant cell arteritis (TABUL): a diagnostic accuracy and cost-effectiveness study. Health Technol Assess. (2016) 20:1–238. doi: 10.3310/hta20900
76. Bridgewater, S, Shepherd, MA, Dawson, J, Richards, P, Silverthorne, C, Ndosi, M, et al. Measuring the impact of steroid therapy on health-related quality of life in patients with rheumatic diseases: international development of a glucocorticoid treatment-specific patient-reported outcome measure. Rheumat (Oxford). (2023) 62:3565–3575. doi: 10.1093/rheumatology/kead081
77. Ndosi, M, Almeida, C, Dawson, J, Dures, E, Greenwood, R, Bromhead, A, et al. Validation of a patient-reported outcome measure for giant cell arteritis. Rheumatology. (2024) 63:181–189. doi: 10.1093/rheumatology/kead201
Keywords: giant cell arteritis, polymyalgia rheumatica, imaging, prognosis, cohort study (or longitudinal study), prospective observational study
Citation: Nielsen BD, Kristensen S, Donskov A, Terslev L, Dreyer LW, Colic A, Hetland ML, Højgaard P, Ellingsen T, Hauge E-M, Chrysidis S and Keller KK (2024) The DANIsh VASculitis cohort study: protocol for a national multicenter prospective study including incident and prevalent patients with giant cell arteritis and polymyalgia rheumatica. Front. Med. 11:1415076. doi: 10.3389/fmed.2024.1415076
Edited by:
Eugenio De Miguel, Hospital Universitario La Paz, SpainReviewed by:
Roberto Padoan, University of Padua, ItalyAlojzija Hocevar, University Medical Centre Ljubljana, Slovenia
Elisa Fernández, La Paz Regional Hospital, Spain
Copyright © 2024 Nielsen, Kristensen, Donskov, Terslev, Dreyer, Colic, Hetland, Højgaard, Ellingsen, Hauge, Chrysidis and Keller. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Berit D. Nielsen, YmVybmlsQHJtLmRr
†ORCID: Berit D. Nielsen, https://orcid.org/0000-0001-6291-157X
Salome Kristensen, https://orcid.org/0000-0001-5812-5234
Lene Terslev, https://orcid.org/0000-0001-8193-9471
Lene Wohlfahrt Dreyer, https://orcid.org/0000-0002-5156-2922
Ada Colic, https://orcid.org/0009-0008-7788-1797
Merete Lund Hetland, https://orcid.org/0000-0003-4229-6818
Pil Højgaard, https://orcid.org/0000-0002-8046-263X
Torkell Ellingsen, https://orcid.org/0000-0003-0426-4962
Ellen-Margrethe Hauge, https://orcid.org/0000-0003-2562-9174
Stavros Chrysidis, https://orcid.org/0000-0001-8583-6517
Kresten Keller, https://orcid.org/0000-0003-2474-3389