
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Med. , 03 October 2024
Sec. Pulmonary Medicine
Volume 11 - 2024 | https://doi.org/10.3389/fmed.2024.1405840
 Maria Tereza Campos Vidigal1
Maria Tereza Campos Vidigal1 Guilherme Henrique Borges1
Guilherme Henrique Borges1 Diogo Henrique Rabelo1
Diogo Henrique Rabelo1 Walbert de Andrade Vieira2
Walbert de Andrade Vieira2 Gustavo G. Nascimento3,4
Gustavo G. Nascimento3,4 Rafael Rodrigues Lima5
Rafael Rodrigues Lima5 Márcio Magno Costa6
Márcio Magno Costa6 Álex Moreira Herval7*
Álex Moreira Herval7* Luiz Renato Paranhos7
Luiz Renato Paranhos7Background: To compare, through a systematic literature review, the cost-effectiveness ratio of home care compared to hospital care for following up patients with chronic obstructive pulmonary disease (COPD).
Methods: This review was registered in PROSPERO, and the bibliographic search was performed in six primary databases [MedLine (via PubMed), Scopus, LILACS, SciELO, Web of Science, and Embase], two dedicated databases for economic studies (NHS Economic Evaluation Database (NHS EED) and Cost-Effectiveness Analysis (CEA) Registry), and two databases for partially searching the “gray literature” (DansEasy and ProQuest). This review only included studies that compared home and hospital care for patients diagnosed with COPD, regardless of publication year or language. Two reviewers selected the studies, extracted the data, and assessed the risk of bias independently. A JBI tool was used for risk of bias assessment.
Results and discussion: 7,279 studies were found, of which 14 met the eligibility criteria. Only one study adequately met all items of the risk of bias assessment. Thirteen studies found lower costs and higher effectiveness for home care. Home care showed a better cost-effectiveness ratio than hospital care for COPD patients. Regarding effectiveness, there is no possibility of choosing a more effective care for COPD patients, given the incipience of the data presented on eligible studies. However, considering the analyzed data refer only to high-income countries, caution is required when extrapolating this conclusion to low- and low-middle-income countries.
Systematic review registration: https://www.crd.york.ac.uk/prospero/, identifier CRD42022319488.
Chronic obstructive pulmonary disease (COPD) affects the airways and other lung structures, and it is known for manifesting persistent respiratory symptoms and lung capacity limitations (1). It develops gradually and is related to a combination of different risk factors, such as exposure to active or passive smoking, chronic respiratory exposure to harmful products, recurrent respiratory infections, premature birth with interferences in lung growth, and even a genetic condition called alpha-1 antitrypsin deficiency (1, 2).
It is a highly prevalent condition, affecting 14% of men and almost 7% of women between 30 and 79 years old worldwide (3). Although COPD is treatable, it has high morbidity and mortality rates (2), and it was the third cause of global deaths in 2019, with more than three million deaths (1). Moreover, COPD patients are more vulnerable to developing mental disorders, such as depression and anxiety, as well as suicidal behaviors such as suicide ideation and attempts (4).
The treatment for COPD patients involves intensive care and recurrent or even continuous hospitalizations (5). Treatment also includes medication therapies and non-pharmacological interventions, such as pulmonary rehabilitation and oxygen therapy (6), added to expensive supplies, medications, and professionals (6, 7). Home care is an alternative form of health assistance for COPD patients (8, 9) and it is characterized by a set of prevention actions, disease treatments, rehabilitation, palliative care, and health promotion provided at home to ensure care continuity (10). This modality of care proposes to decrease the demand for hospital assistance (11), reduce the length of stay of hospitalized users (12), and optimize financial and structural resources (8).
Home care has shown good cost-effectiveness for following up individuals with other chronic diseases, such as cancer (13), chronic heart failure (14), coronary disease (15), chronic tuberculosis (16), and diabetes mellitus type 1 (17) and type 2 (15). Also, primary studies on COPD show that home care may be more inexpensive and effective than hospital care (8, 9, 18). Despite the existing studies assessing the healthcare cost-effectiveness ratio in COPD patients, robust evidence still lacks to support the decision-making of healthcare systems. Therefore, this systematic review evaluated the cost-effectiveness of home care compared to hospital care for following up COPD patients.
All methods were carried out in accordance with relevant guidelines and regulations. The protocol of this systematic review followed the PRISMA-P (Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols) guidelines (19) and was registered in the PROSPERO database1 (CRD42022319488). There were no changes or departures from the protocol when performing the review. The PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyzes) guidelines (20) and the JBI Manual for Evidence Synthesis (21) were used to report and conduct the method of this systematic review. Data were not collected from human participants for this systematic review. Ethical considerations of the primary studies included in this systematic review are presented in the results section.
This systematic review aimed to answer the guiding question, designed according to the PICO acronym (Population, Intervention, Comparator, and Outcome): For the treatment of COPD patients (P), is home care (I) more cost-effective (O) than hospital care (C)?
Inclusion criteria
• Population: Patients diagnosed with COPD, regardless of age, nationality, or disease stage
• Intervention: Follow-up through home care
• Comparator: Follow-up through hospital care
• Outcome: Cost-effectiveness assessment at an individual level, regardless of the time horizon. The studies should report at least one finding related to the economic evaluation (healthcare costs, indirect medical costs, and costs outside healthcare) and intervention effectiveness (risk of death, readmissions, pulmonary functions, and quality of life)
• Study design: Randomized and non-randomized clinical trials.
Exclusion criteria
• Literature reviews, letters to the editor/editorials, personal opinions, books/book chapters, case reports/case series, pilot studies, preprint studies not yet submitted for peer reviewing, congress abstracts, and patents
• Studies that did not clearly define the comparison group
• Studies with oversampling (the most recent study that best described the methodology and results was considered in this case).
Electronic searches were performed up to February 2022 in the Embase, LILACS, MedLine (via PubMed), SciELO, Scopus, and Web of Science databases. Dedicated databases for economic studies–NHS Economic Evaluation Database (NHS EED) and Cost-Effectiveness (CEA) Registry–were also used. The DansEasy and ProQuest databases were searched to partially capture the “gray literature” and reduce the risk of publication bias. A search update was performed between February 2022 and August 2024. There were no restrictions on language or year of publication. The MeSH (Medical Subject Headings), DeCS (Health Sciences Descriptors), and Emtree (Embase Subject Headings) resources were used to select the search descriptors accordingly. Moreover, synonyms and free words composed the search. The Boolean operators “AND” and “OR” were used to improve the research strategy with several combinations. The search strategies in each database were made according to their respective syntax rules (Table 1). The results obtained in the primary databases were initially exported to the EndNote Web™ software (Thomson Reuters, Toronto, Canada) for cataloging and removing duplicates. The “gray literature” results were exported to Microsoft Word (Microsoft™, Ltd, Washington, USA) for excluding duplicates manually.
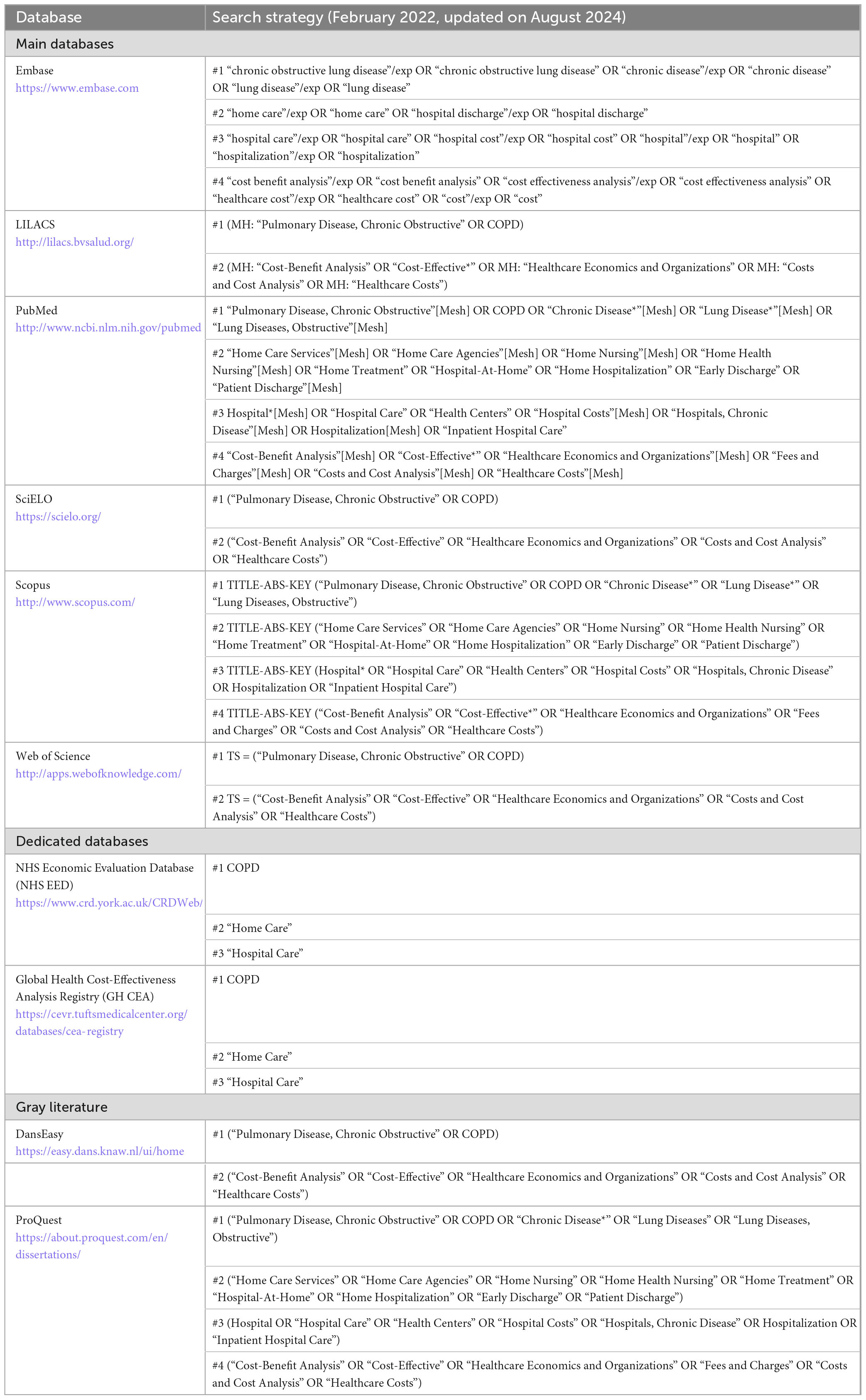
Table 1. Strategies for database search.
After removing duplicates, the results were exported to Rayyan QCRI software (Qatar Computing Research Institute, Doha, Qatar) (22). Study titles were methodically analyzed (first phase) and those unrelated to the topic excluded. In the second phase, the abstracts of the studies were assessed with the initial application of the eligibility criteria. Titles that met the study objectives but without available abstracts were fully analyzed in the next phase. Subsequently, the eligible studies had their texts fully read to verify whether they met the eligibility criteria. If the full texts were not found, a bibliographic request was performed to the library database (COMUT), and an e-mail was sent to the corresponding authors to obtain the articles. Full texts published in languages other than English or Portuguese were translated to allow the application of the eligibility criteria. Two reviewers (MTCV and GHB), after previous calibration (Kappa = 0.87), independently performed all phases, and in case of doubt or disagreement, a third reviewer (LRP) was consulted to make a final decision.
Before data extraction, to ensure consistency between the reviewers (MTCV and GHB), they performed a calibration exercise in which the data from one eligible study were extracted jointly. A third reviewer (LRP) conducted the calibration phase. Next, the full texts of the selected studies were reviewed, and the data were systematically extracted, including information on study identification (author, year, country, and location), sample characteristics (the number of participants included in each analysis group), collection and processing characteristics (description of home and hospital care methodologies, currency, and effectiveness variable), and main findings (specific costs from each group and effectiveness quantification). In case of incomplete or insufficient information, the corresponding author was contacted via e-mail.
An author (MTCV) extracted all the previous data and a second reviewer (GHB) performed a cross-examination to confirm the agreement among the extracted data. Any disagreement between the reviewers was solved by discussing it with a third reviewer (LRP).
Two authors (WAV and MTCV) independently assessed the risk of individual bias of the eligible studies with the JBI Critical Appraisal Tools for use in the JBI Critical Appraisal Checklist for Economic Evaluations (23). Each question could be answered as follows: “Yes” if the study did not have biases for the domain assessed in the question, “No” if the study had biases for the domain assessed in the question, “Uncertain” if the study did not provide sufficient information to assess the question biases, or “Not Applicable” if the question did not fit in the study. A third reviewer (LRP) was consulted in case of divergences between the evaluators.
Considering the high heterogeneity of outcomes, measurement periods and methods, and health settings, the collected data were organized and described in a structured narrative synthesis according to the findings from each eligible study.
In the first phase of study selection, 7,279 results were found distributed in ten electronic databases, including the economy-specific and “gray-literature” ones. After removing duplicates, 6,286 results remained for analysis. A careful reading of the titles excluded 5,459 results. Seven hundred and sixty-nine studies remained for abstract reading. Of these, 402 studies were excluded after applying the eligibility criteria, and 22 were not located even after applying different means of locating bibliographic records. The remaining 138 articles were fully read, of which 124 were excluded (Supplementary Appendix 1). Fourteen studies (8, 9, 11, 12, 18, 24–32) were included in the qualitative synthesis. Figure 1 displays the details of the search, identification, inclusion, and exclusion of studies.
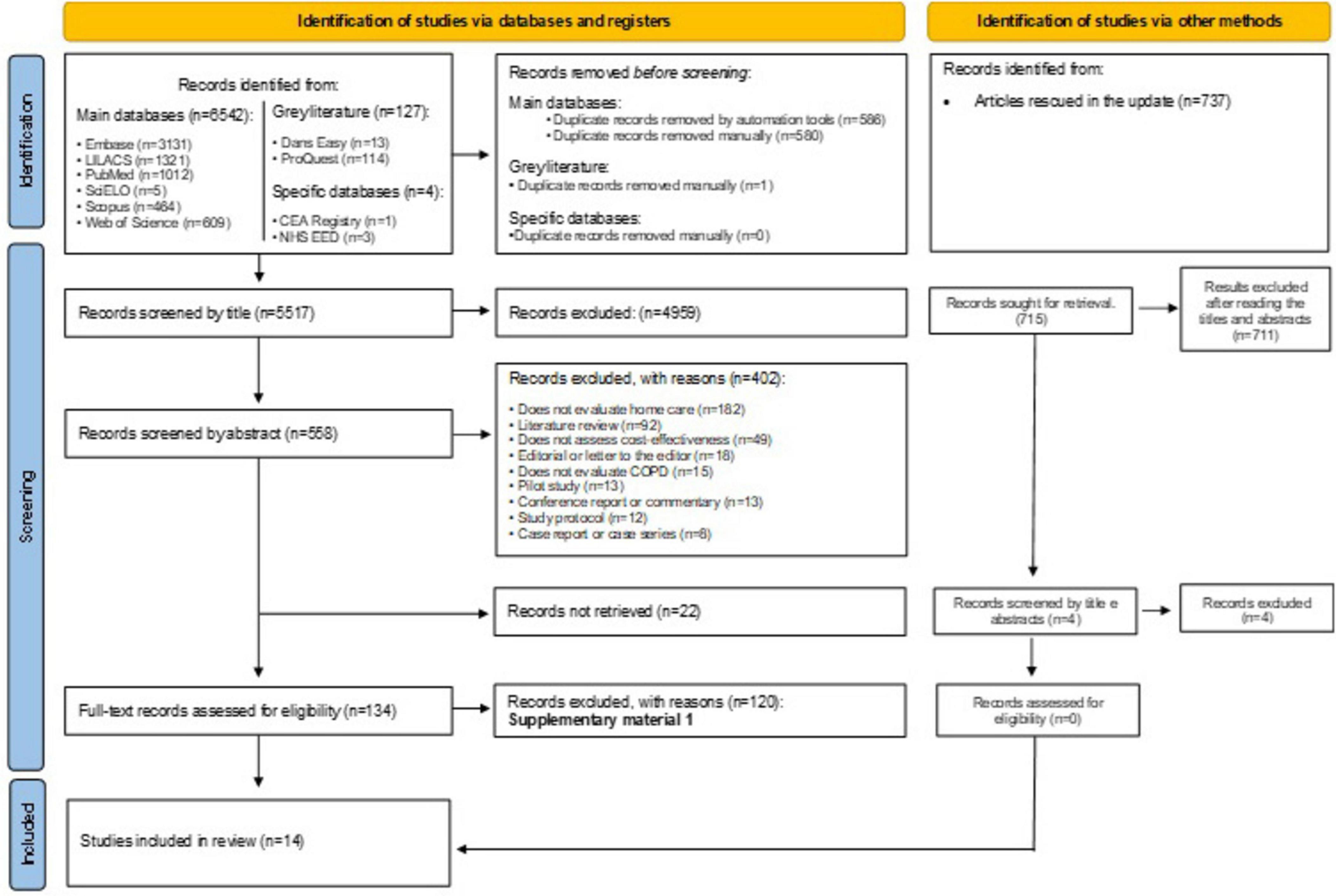
Figure 1. PRISMA flowchart.
The studies were published between 1988 and 2021 and performed in nine countries, with nine studies in Europe (8, 12, 18, 25, 27–29, 31, 32), two in Asia (9, 11), two in America (24, 30) and one in Oceania (26). Six studies (8, 12, 24, 30–32) did not mention to follow ethical criteria to conduct the research.
The total sample included 1,565 individuals with COPD subjected to home care and 7,932 under hospital care. Among the studies that reported the mean age of their sample, there was a variation between 63.6 (32) and 84.0 (29) years for the home care group and a variation between 61.2 (11) and 83.4 (30) years for the hospital care group. Regarding sex, there was a predominance of males (60.1 and 64.2%) among the studies that reported the sex of the participants for the home care and hospital care groups, respectively. Regarding the disease stage of the patients followed up through home care, six studies (12, 18, 26–28, 32) assessed patients in disease exacerbation (acute phase) and the remaining eight (8, 9, 11, 24, 25, 29–31) did not identify the disease stage and only informed it was a follow-up. The initial forced expiratory volume of the patients included in the studies ranged between 33.3 and 43% for patients under home care and 32.2 and 47% for those under hospital care. The application of both care options, such as follow-up time and the professional in charge and the tele-assistance technologies available to patients to contact the follow-up staff varied among studies (Table 2).
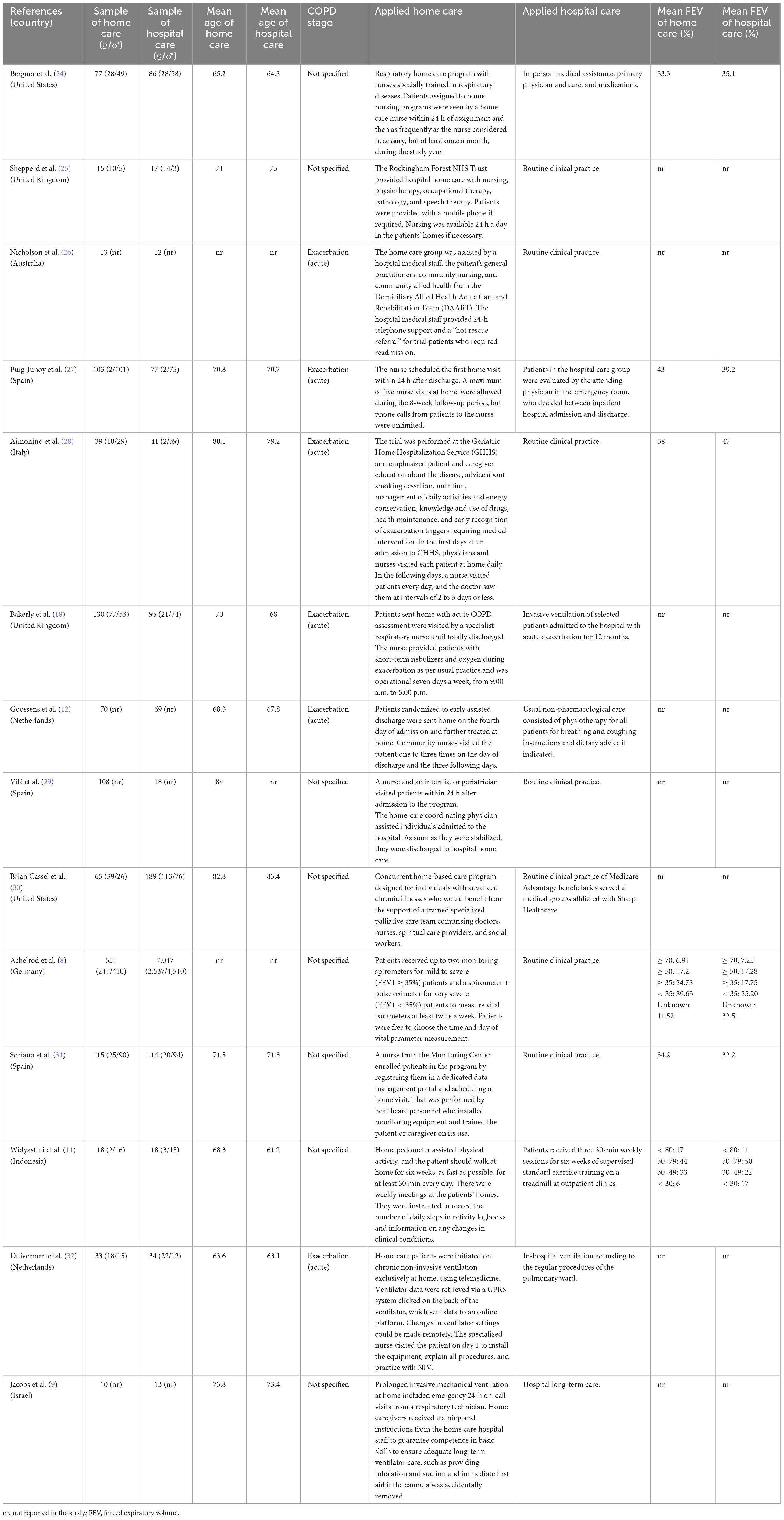
Table 2. Summary of the main characteristics of the eligible studies.
As for cost analysis, the currencies used in the studies were US dollar (24, 26, 28, 30), euro (8, 11, 12, 27, 29, 32), sterling pound (18, 25), and Israeli shekel (9). Moreover, different economic evaluation perspectives were addressed, between them societal perspective (12, 24, 25, 32), patient perspective (18, 25, 28), healthcare and services perspective (9, 11, 12, 26, 29–31), public insurer perspective (27), and sickness fund perspective (8).
Regarding the effectiveness analysis, the following factors composed the indicators: hospital readmission rates, exacerbation rates, the number of visits to the hospital emergency sector, and the number of deaths. One study (11) assessed home care follow-up related to respiratory exercises. In that case, effectiveness was analyzed with body mass and exercise indices and airflow obstruction and dyspnea rates.
Only one study (8) presented positive answers to all tool items. Question 4 (Has clinical effectiveness been established?) received only five positive responses because most eligible studies did not specify clinical efficacy or the origin of efficacy estimation. That might increase the risk of bias because there was no confirmation of a solid evidence base supporting the assumptions about the direction and magnitude of the efficacy measurement. Question 5 (Are costs and outcomes measured accurately?) received six unclear answers, indicating that cost and outcome measurement precision was incorrectly reported. Questions 9 (Were sensitivity analyses conducted to investigate uncertainty in estimates of cost or consequences?) and 11 (Are the results generalizable to the setting of interest in the review?) received only three positive answers because numerous studies did not perform a sensitivity analysis to investigate the uncertainty in cost estimates and did not obtain results generalizable to other environments, respectively. Figure 2 provides detailed information on the risk of bias in the eligible studies.

Figure 2. Risk of bias assessed with the Joanna Briggs Institute Critical Appraisal Tools for use in the JBI Critical Appraisal Checklist for economic evaluations.
Only one study (25) reported the discount rate percentage, and two others (8, 28) informed applying the discount but not the rate. Total costs varied, and this variation referred to the type and services included in the provided home care. Home care costs were lower in the follow-up cases of patients with COPD exacerbation, which is the acute phase of the condition (12, 18, 26–28, 32). For investigations that did not specify the COPD phase, costs were also lower for home care, except for the study by Bergner et al. (24), which showed charges of 8,085 dollars for standard home care and 9,767 dollars for specialized home care for respiratory diseases, while hospital care cost 5,051 dollars (Figure 3). Only five studies (8, 11, 12, 18, 27) calculated incremental costs. Table 3 shows the cost analysis information of the included studies.
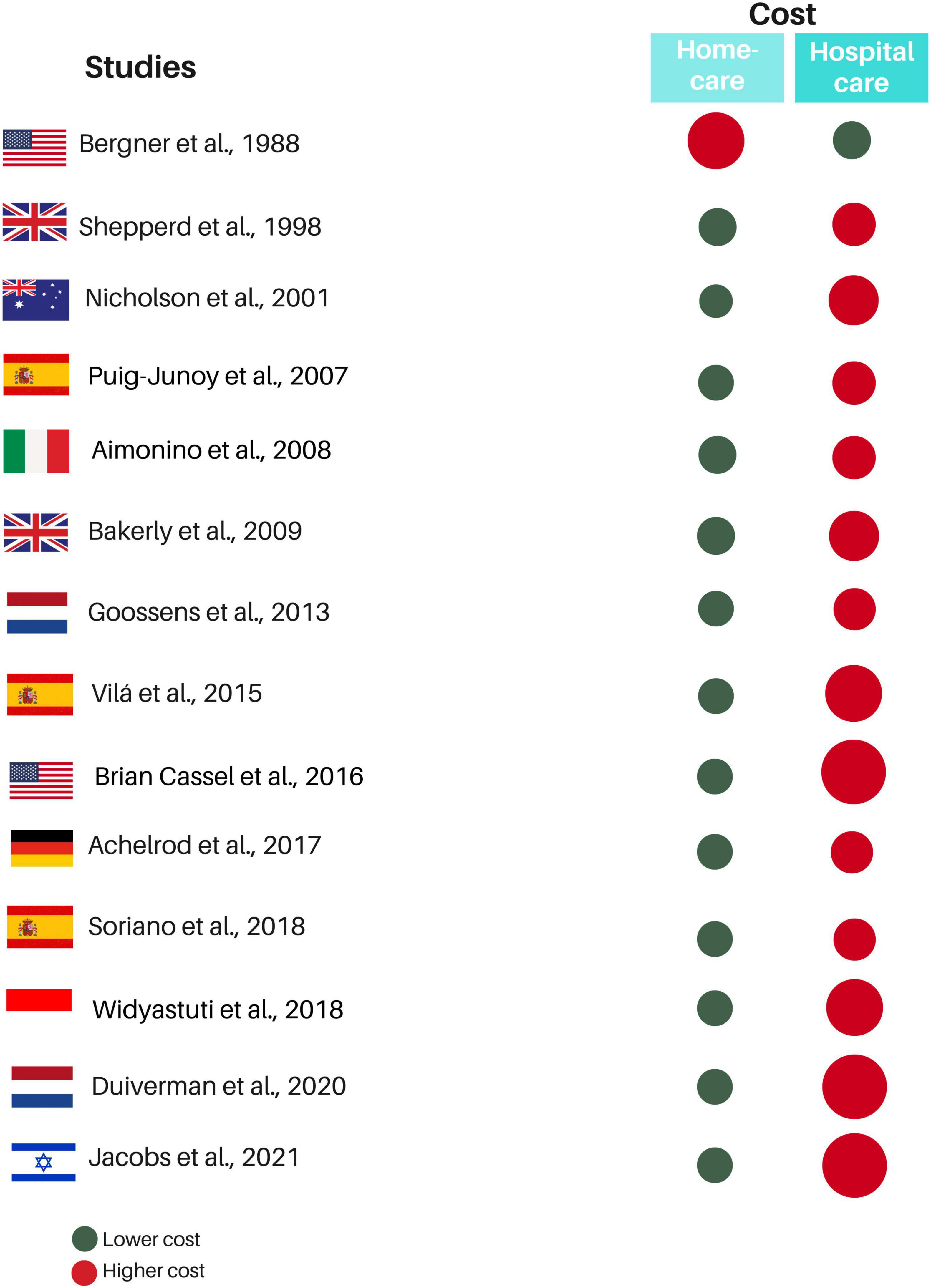
Figure 3. Summary of quantitative results in eligible studies. Red circles represent the treatment with the highest cost, while the green circle represents the treatment with the lowest cost. The size difference between the red and green circles within the same study indicates the proportional cost difference between the treatments. The greater the cost difference, the larger the red circle.
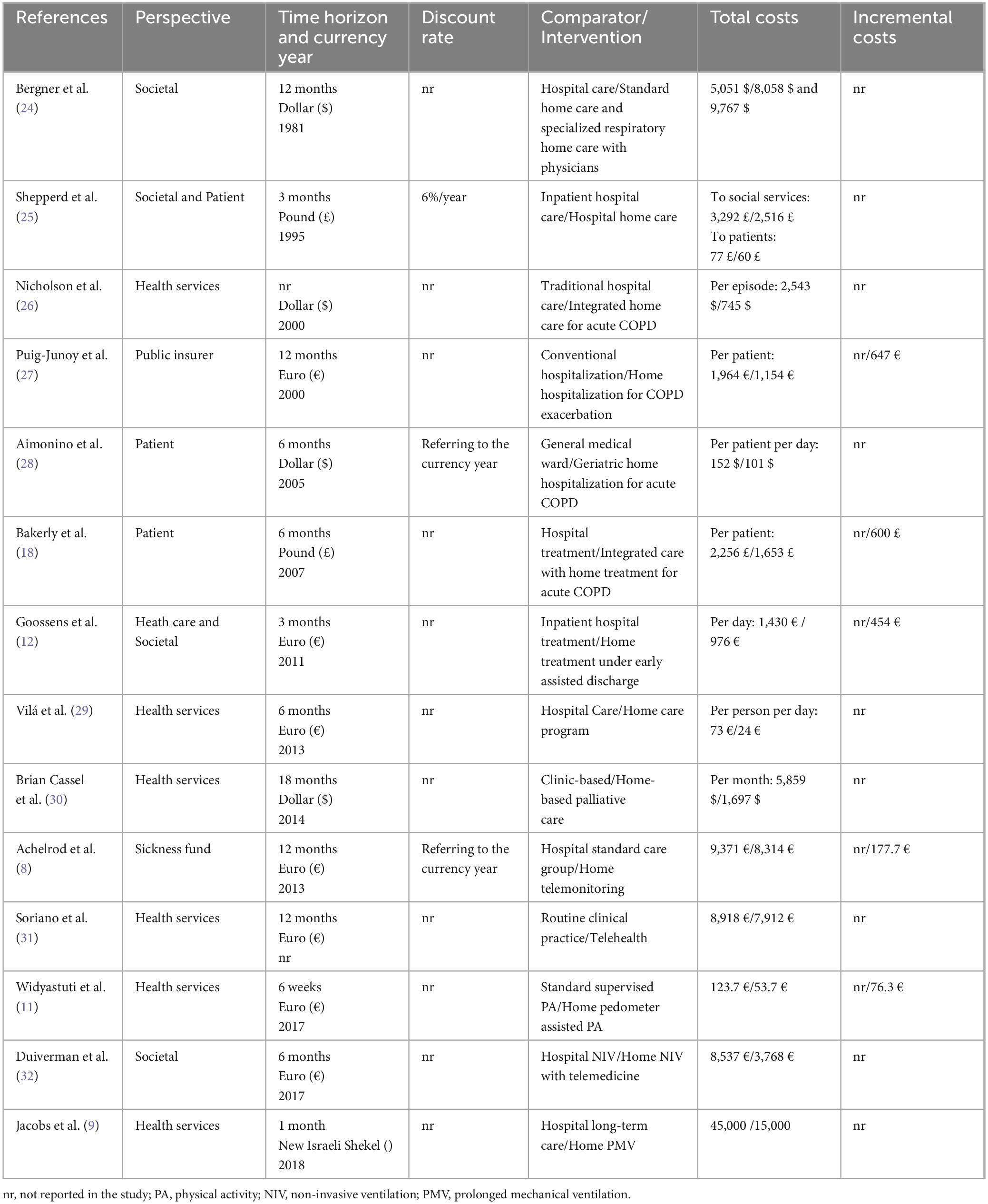
Table 3. Main results and outcomes of the eligible studies regarding cost analysis.
Among the few studies that reported indicators to assess effectiveness, the following were applied: QALY (quality-adjusted life years) (12) and YLL (years of life lost) (8) (Table 4). The readmission rate in the emergency sector was lower for patients followed up at home (28, 30). Finally, three studies (8, 12, 25) performed sensitivity analyses, ranging from two to six analysis scenarios.
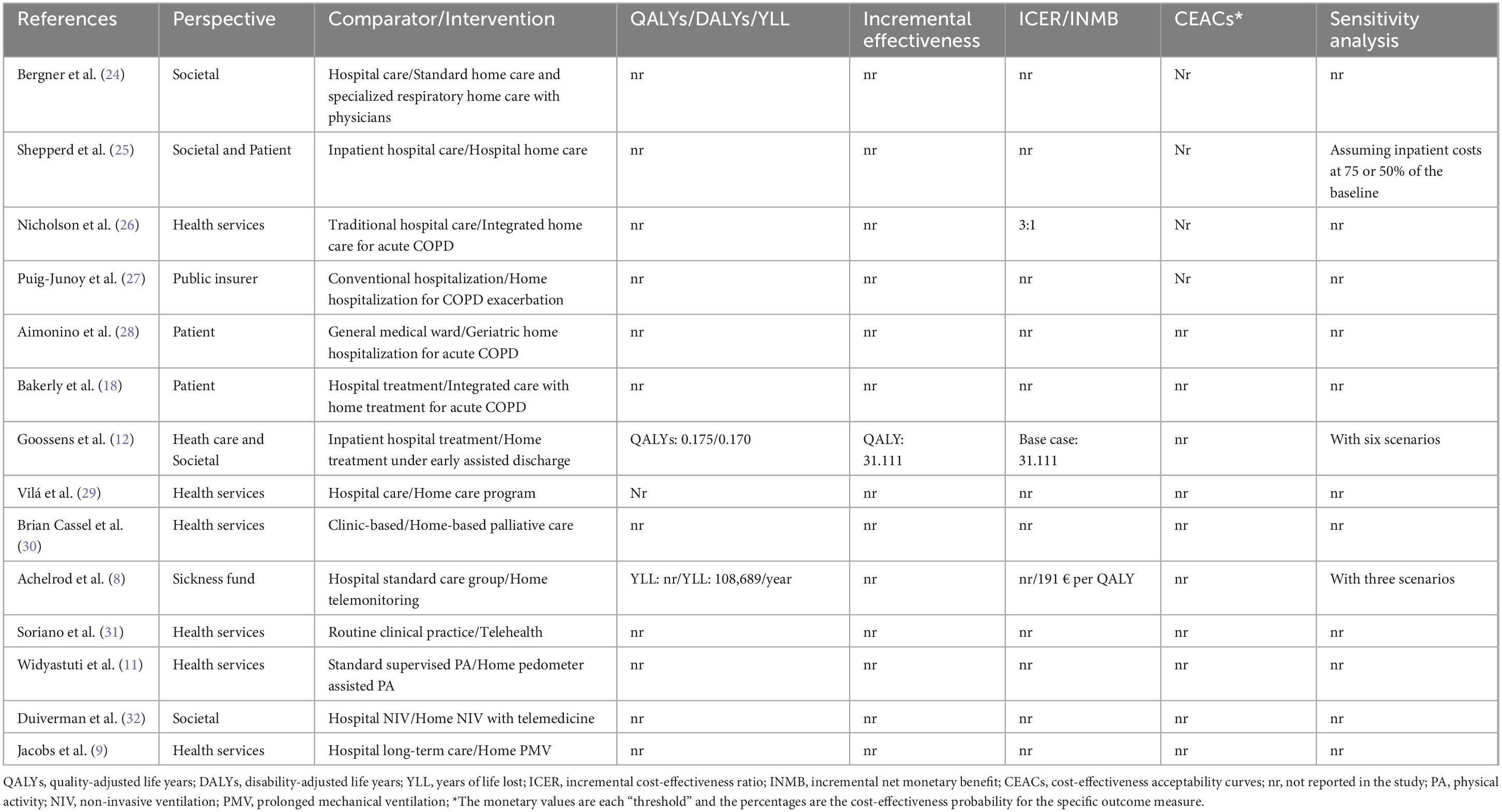
Table 4. Main results and outcomes of the eligible studies regarding the effectiveness analysis.
This systematic review investigated the scientific literature to assess whether home care has a better cost-effectiveness ratio for following up COPD patients than hospital care. The synthesis showed that home care usually has lower costs and higher effectiveness for following up on COPD patients.
Among the main challenges of health systems, adequate management of resources to optimize the processes involving healthcare coverage and access for the population stand out. Patients who require intensive care and recurrent or even continuous hospitalizations, such as COPD patients, may bear higher costs with supplies, medications, and professionals (5). In pandemic times, such as COVID-19 or other disease outbreaks, the search for hospital beds in outpatient or intensive care increased abruptly (33, 34). Moreover, overcrowding has also contributed to a higher risk of hospital contamination or infections (34), especially concerning immunocompromised individuals, such as COPD patients under long-term pharmacological treatment with immunosuppressants (35). Hence, home care represents a relevant alternative to the healthcare of COPD patients.
Home care for following up COPD patients may be applied differently, with potential variations in the service time, expertise of professionals in charge of follow-up, and tele-assistance technologies available to patients to contact the staff. The data of the eligible studies regarding these factors confirm these variations, but regardless of them, it was almost unanimous that home care reduced costs. Only Bergner et al. (24) reported a higher charge for home care than hospital care. This difference from the other eligible studies may be due to the incipient technological development and the high cost of information and communication media at the time of the study, considering that patients were followed up with the help of tele-assistance in the late 80s, when such a technology was more restricted and, consequently, expensive.
Regarding the effectiveness analysis among eligible studies, one fact drew attention: even though they claimed to have performed cost-effectiveness analyses, the cost data were generally more complete, while the data regarding effectiveness were mostly incipient. Only two studies (8, 12) applied effectiveness analysis indicators and provided results on this analysis, and these results did not present a statistically significant difference. Even though they performed narrative descriptions of some effectiveness factors, such as hospital readmissions and lung functions, an effectiveness analysis with known and widely used indicators is extremely important to reveal more valuable effectiveness results. Therefore, it is not feasible to indicate better results for one of the groups.
Besides the variations in the type of home care used, COPD has heterogeneous clinical characteristics manifested with different symptom severity levels at each disease stage (36, 37). Considering this assumption, only six eligible studies reported including only COPD patients in exacerbation, which is an acute phase of the disease (12, 18, 26–28, 32). Acute COPD patients usually manifest exacerbated symptomatology (27), which may interfere with the required care and costs. The other studies did not specify the COPD stage or the clinical condition of patients when performing the analyses. Considering that COPD is a complex disease, it would be crucial to analyze these differences in further studies to obtain homogeneous evidence according to the clinical condition of patients.
In this review, all studies were performed in high-income countries. However, the availability of specialized professionals and funding and the offer of tele-assistance technology differs between high- and low-middle-income countries (38), and discrepancies are even higher compared to underdeveloped countries (39). Moreover, national health systems show high diversity regarding the characteristics of healthcare funding, coverage, management, and models. Hence, a significant limitation of the present review is the impossibility of generalizing the findings to the reality of low-middle-income countries. Therefore, further studies must be performed in these countries to collect representative data on the impact of home care on financially vulnerable countries.
Some countries do not have universal healthcare (such as the United States and Switzerland), some offer healthcare through partnerships with private institutions (such as Australia), and in other countries, citizens are obliged to acquire health insurance (such as Germany, the Netherlands, and Israel). Also, countries like Brazil guarantee access to comprehensive treatment for the population, including home care (40). New economies must consider the characteristics of national health systems, especially the budget source and scope of hospital and home care coverage.
The limitations of this study predominantly refer to the lack of standardization of the methodological designs of the eligible studies. Ideally, treatments would be compared using a meta-analysis, but the heterogeneity of the included studies (lack of standardization in disease stages, different cost perspectives, and diverse care approaches applied to home care) made the grouping of results impossible.
Regarding the methodology of primary studies, despite the guidelines with best practice recommendations to conduct and report cost-effectiveness in economic evaluations (41, 42), most studies did not perform them. Hence, researchers should use these guidelines and journals should promote them for standardizing economic evaluations. Although the methodological quality of the included studies was satisfactory overall, there were still considerable flaws. Moreover, the present review covers only outcomes from developed countries, whereas a global scope would be optimal, including the weaknesses and strengths of each system.
The data of the qualitative synthesis allow concluding that home care presents lower costs than hospital care for COPD patients. Regarding effectiveness, there is no possibility of choosing a more effective care for COPD patients, given the incipience of the data presented on eligible studies. Home care for COPD patients could be considered an alternative when managing healthcare systems, but effectiveness assessments must be carried out with vigor in future studies and evaluations. Furthermore, considering the analyzed data refer only to high-income countries, caution is required when extrapolating this conclusion to low- and low-middle-income countries.
The original contributions presented in this study are included in this article/Supplementary material, further inquiries can be directed to the corresponding author.
MV: Conceptualization, Data curation, Formal analysis, Investigation, Writing – original draft. GB: Formal analysis, Methodology, Validation, Writing – original draft. DR: Conceptualization, Data curation, Investigation, Writing – original draft. WA: Conceptualization, Data curation, Formal analysis, Methodology, Writing – original draft. GN: Data curation, Formal analysis, Methodology, Writing – original draft. RL: Formal analysis, Methodology, Writing – original draft. MC: Conceptualization, Formal analysis, Supervision, Validation, Writing – review & editing. ÁH: Conceptualization, Formal analysis, Methodology, Supervision, Validation, Writing – original draft, Writing – review & editing. LP: Conceptualization, Formal analysis, Methodology, Project administration, Supervision, Validation, Writing – original draft, Writing – review & editing.
The authors declare that financial support was received for the research, authorship, and/or publication of this article. This study received financial support from CNPq (Conselho Nacional de Desenvolvimento Científico e Tecnológico) and Decit/SCTIE/MS (Departamento de Ciência e Tecnologia da Secretaria de Ciência, Tecnologia, Inovação e Insumos Estratégicos em Saúde do Ministério da Saúde) of Brazil. This study was also partially financed CAPES (Coordenação de Aperfeiçoamento de Pessoal de Nível Superior) and FAPEMIG (Fundação de Amparo á Pesquisa do Estado de Minas Gerais).
We are thankful for the support of CAPES (Coordenação de Aperfeiçoamento de Pessoal de Nível Superior) and FAPEMIG (Fundação de Amparo á Pesquisa do Estado de Minas Gerais).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2024.1405840/full#supplementary-material
1. World Health Organization [WHO]. Chronic obstructive pulmonary disease (COPD). Geneva: World Health Organization [WHO] (2022).
2. Zhu B, Wang Y, Ming J, Chen W, Zhang L. Disease burden of COPD in China: A systematic review. Int J Chron Obstruct Pulmon Dis. (2018) 13:1353–64. doi: 10.2147/COPD.S161555
3. Adeloye D, Song P, Zhu Y, Campbell H, Sheikh A, Rudan I, et al. Global, regional, and national prevalence of, and risk factors for, chronic obstructive pulmonary disease (COPD) in 2019: A systematic review and modelling analysis. Lancet Respir Med. (2022) 10:447–58. doi: 10.1016/S2213-2600(21)00511-7
4. Sampaio M, Vieira W, Bernardino ÍM, Herval ÁM, Flores-Mir C, Paranhos LR. Chronic obstructive pulmonary disease as a risk factor for suicide: A systematic review and meta-analysis. Respir Med. (2019) 151:11–8. doi: 10.1016/j.rmed.2019.03.018
5. Varmaghani M, Dehghani M, Heidari E, Sharifi F, Moghaddam S, Farzadfar F. Global prevalence of chronic obstructive pulmonary disease: Systematic review and meta-analysis. East Mediterr Health J. (2019) 25:47–57. doi: 10.26719/emhj.18.014
6. Liu S, Zhao Q, Li W, Zhao X, Li K. The cost-effectiveness of pulmonary rehabilitation for copd in different settings: A systematic review. Appl Health Econ Health Policy. (2021) 19:313–24. doi: 10.1007/s40258-020-00613-5
7. Gutiérrez Villegas C, Paz-Zulueta M, Herrero-Montes M, Parás-Bravo P, Madrazo Pérez M. Cost analysis of chronic obstructive pulmonary disease (COPD): A systematic review. Health Econ Rev. (2021) 11:31. doi: 10.1186/s13561-021-00329-9
8. Achelrod D, Schreyögg J, Stargardt T. Health-economic evaluation of home telemonitoring for COPD in Germany: Evidence from a large population-based cohort. Eur J Health Econ. (2017) 18:869–82. doi: 10.1007/s10198-016-0834-x
9. Jacobs JM, Marcus EL, Stessman J. Prolonged mechanical ventilation: A comparison of patients treated at home compared with hospital long-term care. J Am Med Dir Assoc. (2021) 22:418–24. doi: 10.1016/j.jamda.2020.06.038
10. Helgheim BI, Sandbaek B. Who is doing what in home care services? Int J Environ Res Public Health. (2021) 18:10504. doi: 10.3390/ijerph181910504
11. Widyastuti K, Makhabah D, Setijadi A, Sutanto Y, Ambrosino N. Benefits and costs of home pedometer assisted physical activity in patients with COPD. A preliminary randomized controlled trial. Pulmonology. (2018) 24:211–8. doi: 10.1016/j.pulmoe.2018.01.006
12. Goossens L, Utens C, Smeenk F, van Schayck O, van Vliet M, van Litsenburg W, et al. Cost-effectiveness of early assisted discharge for COPD exacerbations in The Netherlands. Value Health. (2013) 16:517–28. doi: 10.1016/j.jval.2013.01.010
13. Gallagher A, Shersher V, Mortimer D, Truby H, Haines T. The cost-effectiveness of adjunctive lifestyle interventions for the management of cancer: A systematic review. Appl Health Econ Health Policy. (2022) 21:225–42. doi: 10.1007/s40258-022-00759-4
14. Grustam A, Severens J, De Massari D, Buyukkaramikli N, Koymans R, Vrijhoef H. Cost-effectiveness analysis in telehealth: A comparison between home telemonitoring, nurse telephone support, and usual care in chronic heart failure management. Value Health. (2018) 21:772–82. doi: 10.1016/j.jval.2017.11.011
15. Oksman E, Linna M, Hörhammer I, Lammintakanen J, Talja M. Cost-effectiveness analysis for a tele-based health coaching program for chronic disease in primary care. BMC Health Serv Res. (2017) 17:138. doi: 10.1186/s12913-017-2088-4
16. Moalosi G, Floyd K, Phatshwane J, Moeti T, Binkin N, Kenyon T. Cost-effectiveness of home-based care versus hospital care for chronically ill tuberculosis patients, Francistown, Botswana. Int J Tuberc Lung Dis. (2003) 7:S80–5.
17. McCarroll Z, Townson J, Pickles T, Gregory J, Playle R, Robling M, et al. Cost-effectiveness of home versus hospital management of children at onset of type 1 diabetes: The DECIDE randomised controlled trial. BMJ Open. (2021) 11:e043523. doi: 10.1136/bmjopen-2020-043523
18. Bakerly N, Davies C, Dyer M, Dhillon P. Cost analysis of an integrated care model in the management of acute exacerbations of chronic obstructive pulmonary disease. Chron Respir Dis. (2009) 6:201–8. doi: 10.1177/1479972309104279
19. Shamseer L, Moher D, Clarke M, Ghersi D, Liberati A, Petticrew M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: Elaboration and explanation. BMJ. (2015) 350:g7647. doi: 10.1136/bmj.g7647
20. Page M, McKenzie J, Bossuyt P, Boutron I, Hoffmann T, Mulrow C, et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ. (2021) 372:n71. doi: 10.1136/bmj.n71
21. Aromataris E, Munn Z. JBI manual for evidence synthesis. JBI (2020). Available online at: https://jbi-global-wiki.refined.site/space/MANUAL (accessed March 12, 2024).
22. Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan-a web and mobile app for systematic reviews. Syst Rev. (2016) 5:210. doi: 10.1186/s13643-016-0384-4
23. Gomersall J, Jadotte Y, Xue Y, Lockwood S, Riddle D, Preda A. Conducting systematic reviews of economic evaluations. Int J Evid Based Healthc. (2015) 13:170–8. doi: 10.1097/XEB.0000000000000063
24. Bergner M, Hudson L, Conrad D, Patmont C, McDonald G, Perrin E, et al. The cost and efficacy of home care for patients with chronic lung disease. Med Care. (1988) 26:566–79. doi: 10.1097/00005650-198806000-00005
25. Shepperd S, Harwood D, Gray A, Vessey M, Morgan P. Randomised controlled trial comparing hospital at home care with inpatient hospital care. II: Cost minimisation analysis. BMJ. (1998) 316:1791–6. doi: 10.1136/bmj.316.7147.1791
26. Nicholson C, Bowler S, Jackson C, Schollay D, Tweeddale M, O’Rourke P. Cost comparison of hospital- and home-based treatment models for acute chronic obstructive pulmonary disease. Aust Health Rev. (2001) 24:181–7. doi: 10.1071/ah010181
27. Puig-Junoy J, Casas A, Font-Planells J, Escarrabill J, Hernández C, Alonso J, et al. The impact of home hospitalization on healthcare costs of exacerbations in COPD patients. Eur J Health Econ. (2007) 8:325–32. doi: 10.1007/s10198-006-0029-y
28. Aimonino N, Tibaldi V, Leff B, Scarafiotti C, Marinello R, Zanocchi M, et al. Substitutive “hospital at home” versus inpatient care for elderly patients with exacerbations of chronic obstructive pulmonary disease: A prospective randomized, controlled trial. J Am Geriatr Soc. (2008) 56:493–500. doi: 10.1111/j.1532-5415.2007.01562.x
29. Vilà A, Villegas E, Cruanyes J, Delgado R, Sabaté R, Ortega J, et al. Cost-effectiveness of a Barcelona home care program for individuals with multimorbidity. J Am Geriatr Soc. (2015) 63:1017–24. doi: 10.1111/jgs.13396
30. Brian Cassel J, Kerr K, McClish D, Skoro N, Johnson S, Wanke C, et al. Effect of a home-based palliative care program on healthcare use and costs. J Am Geriatr Soc. (2016) 64:2288–95. doi: 10.1111/jgs.14354
31. Soriano J, García-Río F, Vázquez-Espinosa E, Conforto J, Hernando-Sanz A, López-Yepes L, et al. A multicentre, randomized controlled trial of telehealth for the management of COPD. Respir Med. (2018) 144:74–81. doi: 10.1016/j.rmed.2018.10.008
32. Duiverman M, Vonk J, Bladder G, van Melle J, Nieuwenhuis J, Hazenberg A, et al. Home initiation of chronic non-invasive ventilation in COPD patients with chronic hypercapnic respiratory failure: A randomised controlled trial. Thorax. (2020) 75:244–52. doi: 10.1136/thoraxjnl-2019-213303
33. Centers for Disease Control and Prevention [CDC]. COVID data tracker. Atlanta, GA: Centers for Disease Control and Prevention [CDC] (2022).
34. Sandhu P, Shah A, Ahmad F, Kerr J, Demeke H, Graeden E, et al. Emergency department and intensive care unit overcrowding and ventilator shortages in us hospitals during the COVID-19 pandemic, 2020-2021. Public Health Rep. (2022) 137:796–802. doi: 10.1177/00333549221091781
35. Munjal S, Munjal S, Gao J, Venketaraman V. Exploring potential COPD immunosuppression pathways causing increased susceptibility for MAC infections among COPD patients. Clin Pract. (2021) 11:619–30. doi: 10.3390/clinpract11030077
36. Pinto L, Alghamdi M, Benedetti A, Zaihra T, Landry T, Bourbeau J. Derivation and validation of clinical phenotypes for COPD: A systematic review. Respir Res. (2015) 16:50. doi: 10.1186/s12931-015-0208-4
37. Esteban C, Arostegui I, Aburto M, Moraza J, Quintana J, García-Loizaga A, et al. Chronic obstructive pulmonary disease subtypes. Transitions over time. PLoS One. (2016) 11:e0161710. doi: 10.1371/journal.pone.0161710
38. Naresh B, Reddy BS. Challenges and opportunity of e-learning in developed and developing countries- a review. Int J Emerg Res Manag Tech. (2015) 4:259–62.
39. Frost LJ, Reich MR. Creating access to health technologies in poor countries. Health Affairs. (2009) 28:962–73.
40. Ministério da Saúde. Departamento de Atenção Básica. Caderno de atenção domiciliar. Ministério da Saúde, Secretaria de Atenção à Saúde, Departamento de Atenção Básica. Brasília: Ministério da Saúde (2012).
41. Evers S, Goossens M, de Vet H, van Tulder M, Ament A. Criteria list for assessment of methodological quality of economic evaluations: Consensus on health economic criteria. Int J Technol Assess Health Care. (2005) 21:240–5.
Keywords: pulmonary disease, chronic obstructive, hospitals, Home Care Services, Hospital-Based Home Care Services, cost-effectiveness analysis
Citation: Vidigal MTC, Borges GH, Rabelo DH, de Andrade Vieira W, Nascimento GG, Lima RR, Costa MM, Herval ÁM and Paranhos LR (2024) Cost-effectiveness of home care compared to hospital care in patients with chronic obstructive pulmonary disease (COPD): a systematic review. Front. Med. 11:1405840. doi: 10.3389/fmed.2024.1405840
Received: 23 March 2024; Accepted: 17 September 2024;
Published: 03 October 2024.
Edited by:
Paschalis Steiropoulos, Democritus University of Thrace, GreeceReviewed by:
Giorgio Reggiardo, Consorzio per Valutazioni Biologiche e Farmacologiche, ItalyCopyright © 2024 Vidigal, Borges, Rabelo, de Andrade Vieira, Nascimento, Lima, Costa, Herval and Paranhos. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Álex Moreira Herval, YWxleG1oZXJ2YWxAdWZ1LmJy
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.