
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Med. , 19 June 2024
Sec. Geriatric Medicine
Volume 11 - 2024 | https://doi.org/10.3389/fmed.2024.1394640
This article is part of the Research Topic Pathophysiology, Treatment and Rehabilitation of Neurodegenerative Diseases in Geriatric Population View all 20 articles
 Marco Antonio Barrero-Mejias1
Marco Antonio Barrero-Mejias1 Sandra Gómez-Martínez2
Sandra Gómez-Martínez2 Jesús González-Moreno2
Jesús González-Moreno2 María Rueda-Extremera1Eva Izquierdo-Sotorrio1
María Rueda-Extremera1Eva Izquierdo-Sotorrio1 María Cantero García1*
María Cantero García1*Introduction: The phenomenon of aging is distinguished by profound life transformations, with the most dependent group being constituted by elderly individuals. The responsibility for their care primarily falls on the figure of the informal caregiver. The scarcity of time, the stress associated with caregiving, the financial, work-related, and personal difficulties it entails, make it a collective with high probabilities of experiencing various psychological disorders. Interventions that have shown the best results are those of multiple components, composed of various techniques that seek to adapt to the reality of the informal caregiver.
Method: The purpose of this study is a systematic review of effective interventions on depressive symptoms, emotional wellbeing, burden, or quality of life in informal caregivers of non-institutionalized dependents from 2018 to the present. A search was conducted in November 2023, on Pubmed, Pubmed Central, Proquest, and Scielo. The final review was conducted on 11 articles.
Results: The results indicate that multiple component interventions including cognitive behavioral techniques and psychoeducation in combination with stress coping techniques and social support are more effective on depressive symptoms, burden, quality of life, and increasing the social support network.
Discussion: Results on web-based programs demonstrate their efficacy and effectiveness, but require a greater number of trials to adjust their methodological quality and content to the idiosyncrasies of the informal caregiver.
Dependency refers to the chronic condition in which individuals, due to a variety of factors (such as age, illness, disability, etc.), have lost part or all of their physical, mental, and intellectual capacity and require assistance or care from others to perform all daily activities (1). There are several mechanisms to ensure adequate care for dependent individuals, but the burden of care still mainly falls within the family. This type of care, commonly referred to as informal care (IC), is characterized by being unpaid work, taking place in the home itself with limited resources, and involving a kinship relationship (2–4). IC for a dependent person causes a higher level of stress and anxiety than that of other chronic illnesses, being present in more than 75% of caregivers (5). More than 50% of informal caregivers (ICGs) exhibit depressive symptoms (DS) at a significant level, and as the caregiving time progresses, they may show higher probabilities of developing major depressive disorder (6–9). They must cope with more daily problems, suffer economic complications, lack leisure time, have limited social relationships, and express a greater sense of overall discomfort in their lives (7, 10–16). The characteristics of the dependent person’s illness correlate with the health of the ICG, their level of anxiety, and their quality of life (QoL), constituting one of the predictive variables for the development of DS (7, 16–19).
The “Caregiver Syndrome” is the most used concept to explain all the risk factors that affect the health of ICGs, in psychological, physical, social, and economic aspects, due to the care of dependent individuals, generating a high level of stress over a long period of time (20–22). Overload is the most studied concept in relation to the discomfort and deterioration of the QoL experienced by ICGs (23), with the variables that constitute it being related to the stressful situations faced by ICGs, dedication time, age, educational level, social status, socioeconomic factors, social support network (SSN), their own coping strategies, and the relationship and type of dependency of the care recipient (24–28), showing that, the higher the overload, the higher the risk of anxiety, depression, lower social support (SS), and longer caregiving time (3, 6, 14, 23, 25, 29–31). Therefore, the caregiver syndrome is not a simple concept to define due to its multidimensionality (32) and, consequently, to evaluate (28). Regarding the profile of the ICG, it is mostly women, middle-aged, married, with a low educational level, and closely related to the care recipient, usually daughter or spouse, with a caregiving time exceeding 8 h per day (3, 14, 30, 31, 33–35).
In line with this multidimensional model of IC, numerous interventions have been developed to mitigate the negative effects of this type of care, supported by numerous research studies that have shown significantly high results, among which psychoeducational interventions (PEIs), cognitive-behavioral interventions (CBT), multiple component interventions (MCIs), group support (GS), stress coping (SC), problem-solving (PS), and some third-generation therapies, such as behavioral activation therapy (BAT) and acceptance and commitment therapy (ACT), stand out. It has been evidenced that MCIs and CBTs are the ones that maintain the best results, especially in variables such as depression, and secondarily affecting variables such as burden, stress, and anxiety, improving the QoL and emotional wellbeing (EWB) of ICGs, thereby enhancing care (36–43). Interventions carried out in different modalities, especially by phone (IT) and online (IOL), show significant results, although with less efficacy than the interventions mentioned above, but they encourage further research on their effectiveness (44–47). The aim of this document is to conduct a review of the most recent studies on the effectiveness of interventions in reducing DS, burden, and improving the QoL of dependent individuals’ ICGs. It is hypothesized that MCIs, with techniques derived from CBT, are the most suitable for eliminating or reducing the DS of dependent individuals’ ICGs. A second hypothesis is proposed in which MCIs, with techniques based on psychoeducation and SS, improve QoL, reduce burden, and increase SSN.
A systematic review of articles, in both English and Spanish, published between the years 2018 and 2023 has been conducted, following the guidelines established by the PRISMA protocol (48).
For the search and selection of studies, the PICO(s) strategy has been employed (Table 1). The inclusion criteria for the selection of research have been as follows: (a) the intervention targets caregivers of elderly individuals who do not reside in specialized centers, (b) they must assess the EWB, burden, QoL, and DS of the ICG, (c) the evaluation must be conducted at least at two time points, (d) the intervention has a control group, and (e) participation in each intervention group must be controlled and randomized. The exclusion criteria for trials have been as follows: (a) the dependent individual is institutionalized, (b) the dependent individual is under 60 years old, (c) the intervention focuses on the dependent older adult, and (d) the intervention focuses on other psychological and medical aspects of the caregiver (Table 2).
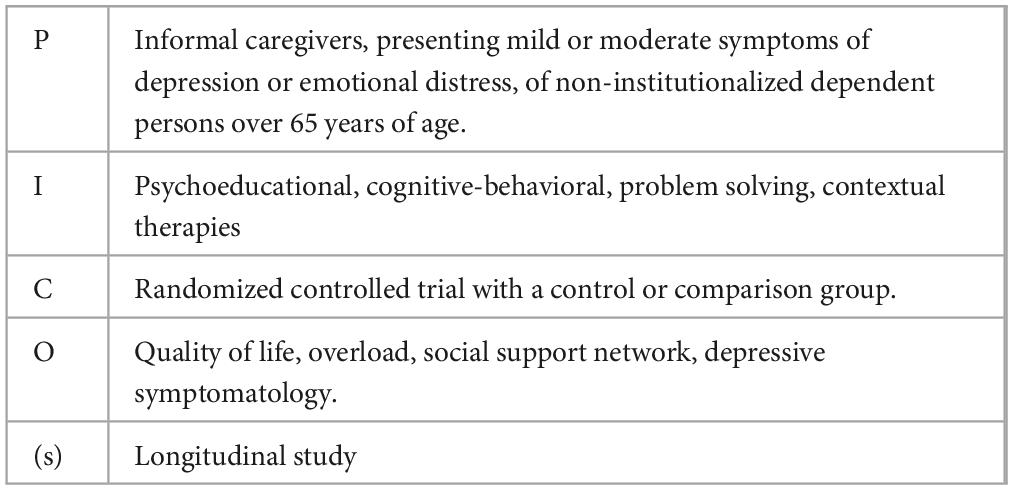
Table 1. Process description PICO(s).
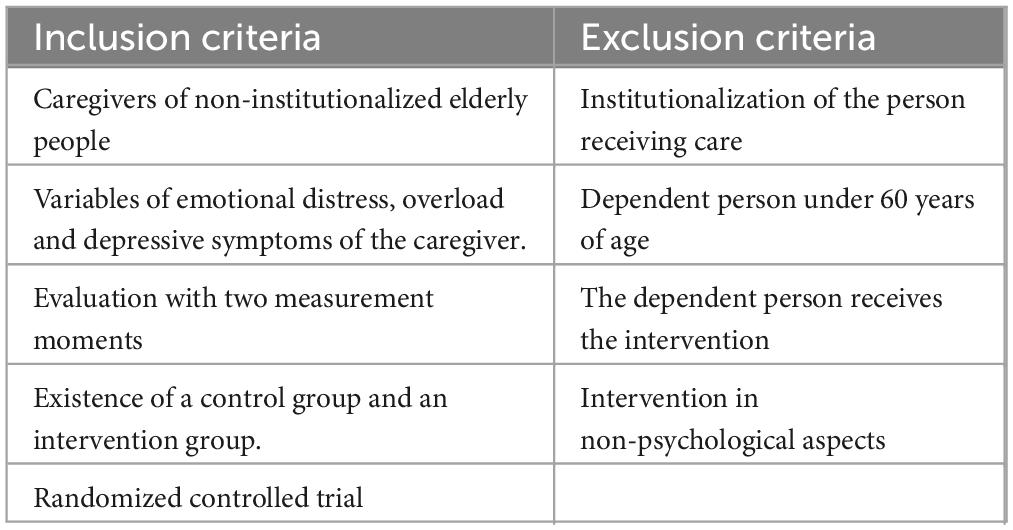
Table 2. Selection criteria.
A search was conducted in the databases of “Proquest,” “Pubmed,” “Pubmed Central,” and “Scielo.” This search ended on 14 November 2023, with articles published after that date not considered. The following search terms were established both in Spanish (Intervención, cuidadores, Dementia, depressión, Alzheimer) and in English (Intervention, caregiver, dependent, Alzheimer, Dementia, quality of life, depression), using the Boolean operators “AND,” “NOT,” and “OR” (Table 3).
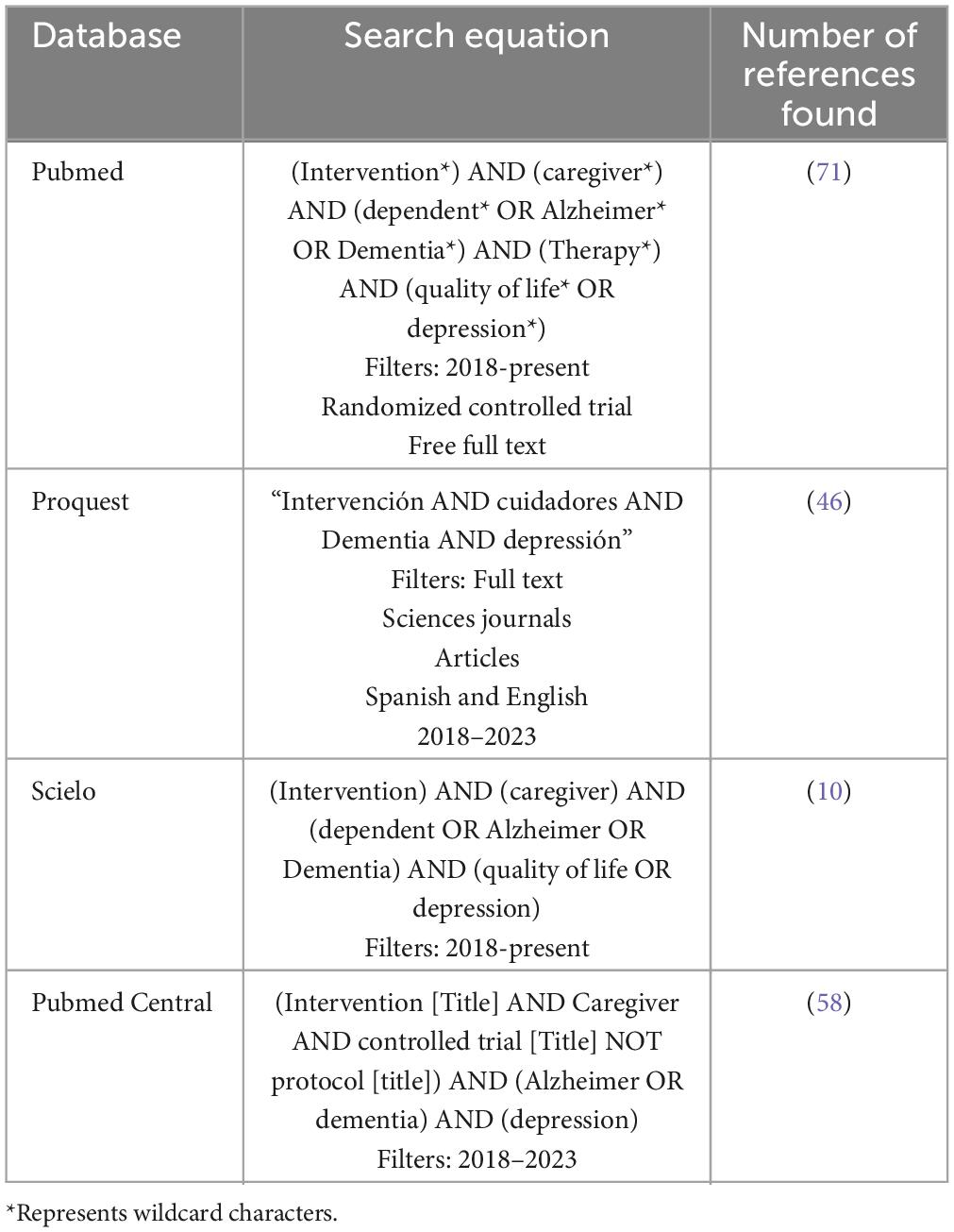
Table 3. Information sources and search strategies.
Applying the information search strategy and once filters were applied using automatic tools from the meta-search engines (randomized controlled trial, open access, full text) and based on the criteria established previously, 184 articles were selected (N = 184) (Figure 1) (49). After reading the title and abstract, 23 articles were selected (N = 23). Once this set of articles was retrieved, they were read and analyzed accordingly, discarding those that did not meet the inclusion criteria (N = 12). For the final analysis of this review, 11 articles were included (N = 11).
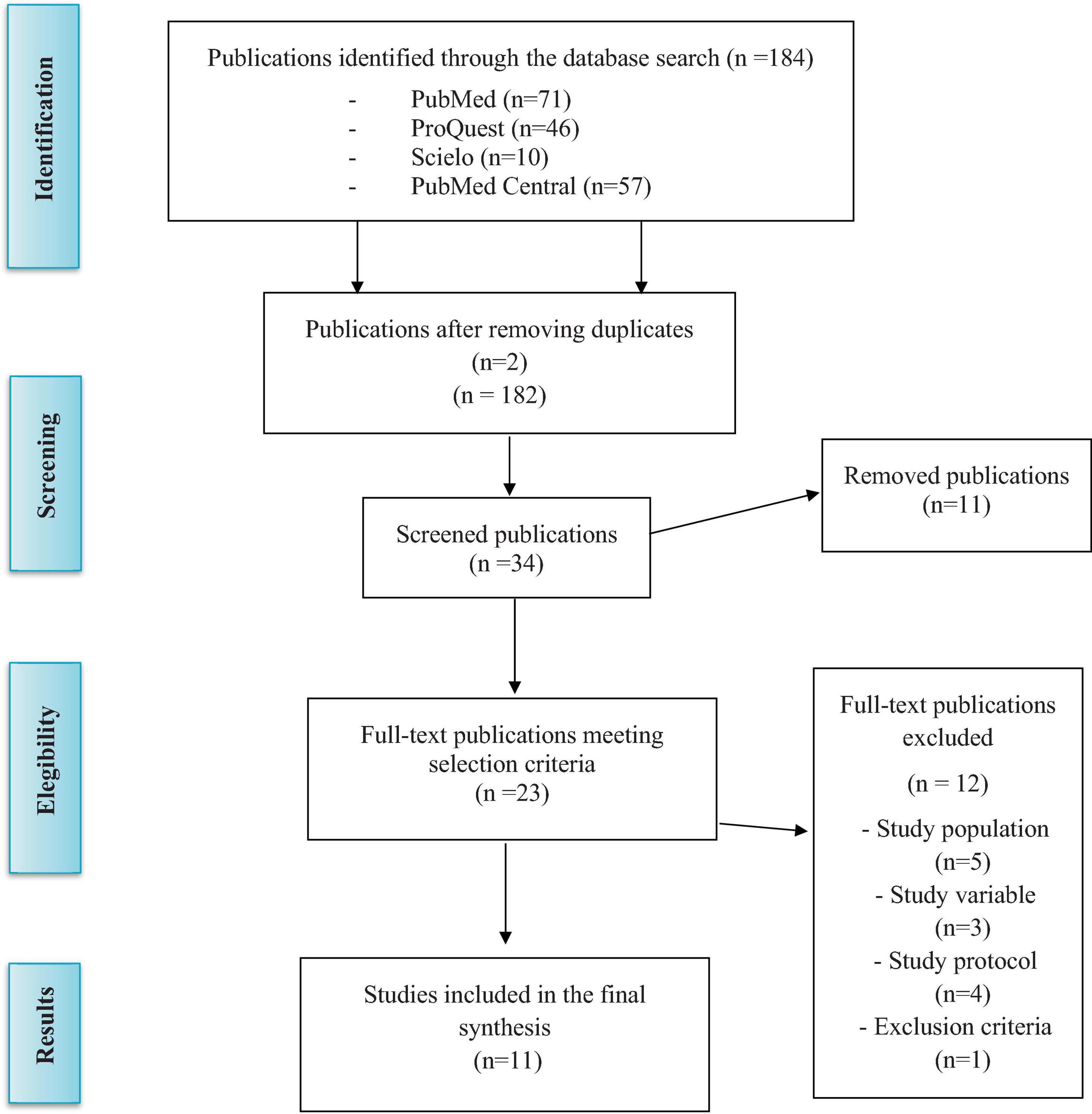
Figure 1. Flowchart based in Moher et al. (49).
To analyze the results of the selected primary studies, the following variables have been considered: (1) Sample size, age, educational level, and caregiving time to contrast results with other studies. (2) Evaluated variables such as DS, burden, QoL, and EWB. (3) Assessment instruments used to measure the aforementioned variables. (4) Type of intervention applied, both in the experimental group (EG) and in the control group (CG). (5) Analysis of methodological quality, analyzing those studies with inclusion and exclusion criteria, type of clinical trial, and if they had a CG. The analysis of methodological quality was carried out using the PEDro scale that evaluates internal validity through 10 criteria, leaving the first criterion out of the calculation as it is related to the external validity of the trial. (6) Intervention results and effects, analyzing statistically significant changes from EG compared to CG for the evaluated variables. (7) To assess the risk of bias presented by the selected studies with the aim of providing good evidence, the Cochrane Risk of Bias Assessment Tool proposed in the Cochrane Handbook for Systematic Reviews (2011) was used.
All selected studies are randomized controlled trials (RCTs), with random allocation to one or more EGs and one CG. The most evaluated variables in all RCTs are DS (N = 6), burden (N = 7), EWB (N = 5), QoL (N = 6), and SSN (N = 4), whose baseline measures, obtained through relevant assessment instruments, indicated acceptance of the sample for the proposed intervention in each of the trials (Table 4).
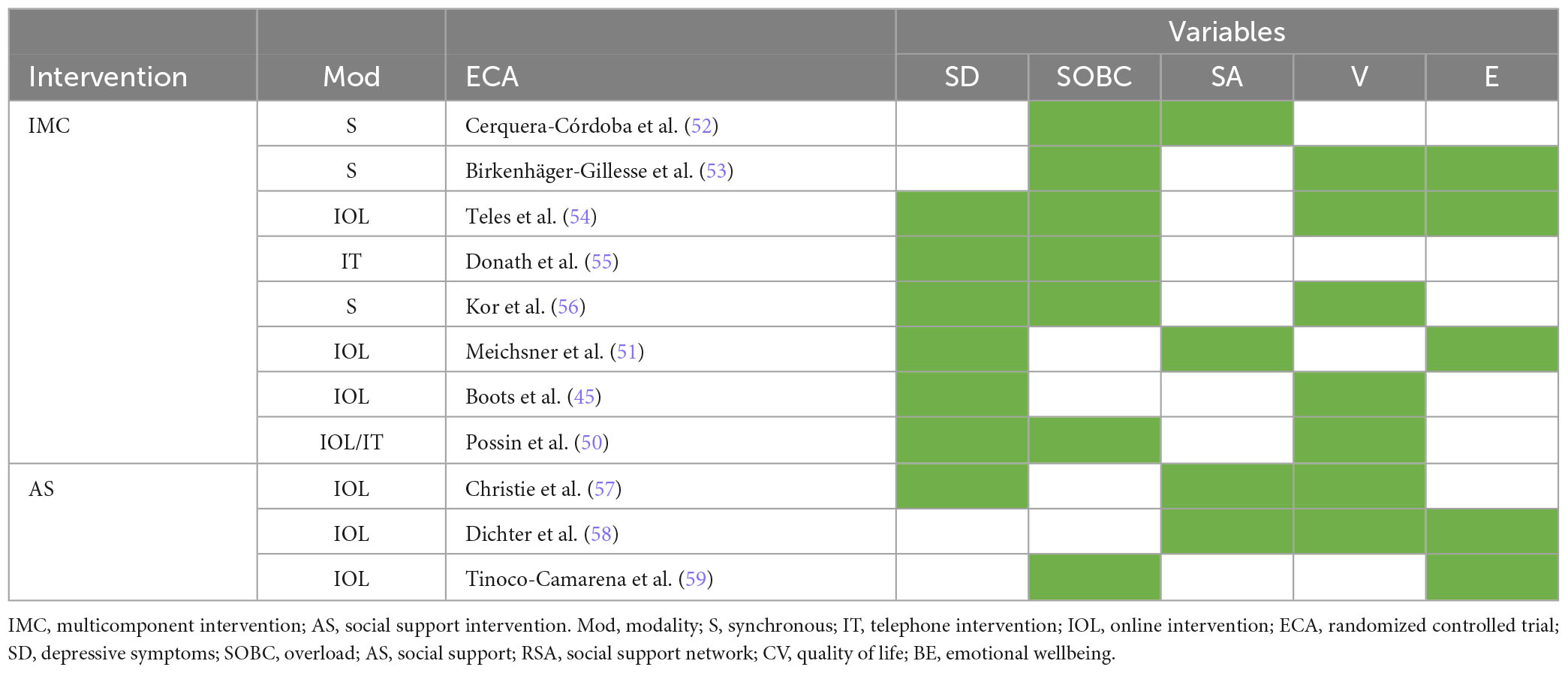
Table 4. Classification of interventions and study variables.
Combining all selected studies, 1,743 participants constitute the total sample, of which 1,242 participants (72%) are female, with an average age of 60 years. In most studies, and for which data are provided, it is the daughter or son (55%) or spouse (40%) who is the primary ICG, with an average of 3.46 years of continuous caregiving. The sample size varies greatly among articles, with the largest sample size in the study by Possin et al. (50), with a sample of 780 participants, and the smallest in the study by Meichsner et al. (51), with a total of 37 participants. The educational level of the constituent sample varies from one study to another, highlighting that 54% of the sample has secondary education, followed by 35% with higher or tertiary education. The basic level is below 35% of the total.
All RCTs are characterized by aiming to intervene on the effects of caregiving in ICGs of dependent individuals, but they differ in the study variables, from reducing DS to improving QoL or increasing SSN, and therefore, they differ in the type of intervention applied. Hence, studies are classified according to the type of intervention and specify whether they were applied in online or telephone modalities (Table 4).
In the study by Cerquera-Córdoba et al. (52), the multicomponent program designed aims to decrease burden and increase SSN for the caregiver. It includes components of psychoeducation, systemic communication and physiotherapy, assertive communication, mental health, subjective wellbeing, caregiving skills, and SSN enhancement, both professional and functional. It is designed with a methodology composed of three intervention groups: Group A receives the MCI, Group B receives a respite program, and Group C or CG is on a waiting list. In the study by Birkenhäger-Gillesse et al. (53) titled “More at home with dementia,” the objective is to improve QoL, analyzing secondary outcomes such as burden and EWB (53). The multicomponent program includes educational components and CBT that address psychological and educational issues related to emotional, relational, practical, financial, and social changes associated with living with someone with dementia, as well as group work techniques, modeling, and role-playing delivered in group sessions. The CG receives a care relief intervention. Teles et al. (54) present in their study the online and self-guided program “iSupport,” a pilot test carried out in Portugal that requires cultural adaptation, with the aim of reducing burden, DS, anxiety, increasing positive caregiving aspects and self-efficacy, and improving QoL. Its components include education on caring for the dependent person and SS for caregivers using techniques such as PS, CBT, SC, or BAT. It is presented as a self-guided online application with five modules and 23 lessons. The CG receives an educational program.
Donath et al. (55) developed a psychoeducational telephone intervention (TI) on dementia and stress coping (ACE) tailored to the needs of caregivers with the aim of reducing caregiver burden and DS and improving QoL. The control group (CG) receives no intervention. They also intervene with people with dementia to verify if the effects of the intervention are related to the cognitive decline of the care recipient. Kor et al. (56) relied on CBT combined with Mindfulness to develop their intervention with the aim of reducing perceived stress as the primary outcome and burden, QoL, depression, and anxiety as secondary outcomes. The program included psychoeducation on stress and caregiving for the dependent person and mindfulness activities with components such as meditation and mindful eating, understanding unpleasant feelings, and awareness of difficult feelings, thoughts, and sensations related to caregiving. The CG receives standard care plus an educational session on dementia caregiving. The online program “Partner in Balance (PiB)” with face-to-face support, described in the study by Boots et al. (45), includes components such as acceptance, communication with family and social environment, and stress management techniques, focusing on the positive, insecurities, reflections, self-awareness, social relationships, and support. Its aim is to improve self-efficacy and mastery of ICGs in early stages of caregiving and also to evaluate its impact on DS, QoL, anxiety, and stress. The CG is on a waiting list.
Possin et al. (50) present an Internet-based intervention combined with TI called “Care Ecosystem,” composed of supportive care for dementia caregivers with the aim of reducing burden and DS and thereby improving the QoL of the care recipient. The team first addresses the immediate needs of ICGs, then identifies common problems and provides personalized support and education, following a standardized care plan. Both the care recipient and the caregiver are the recipients of the program. Outside the program, a team handles medical needs, problematic behavioral symptoms, legal or financial circumstances. The CG receives general articles related to dementia.
The study by Meichsner et al. (51) describes a trial using an Internet-based intervention, the Tele.TAnDem program, which customizes the intervention according to the specific needs of each caregiver, employing mixed techniques of Acceptance and Commitment Therapy (ACT) and CBT. It was conducted online with the aim of supporting ICGs in a more flexible manner. It consists of 10 modules aimed at reducing caregiver DS and enhancing their psychosocial resources and improving their EWB. At the beginning of the intervention, platform users set their personal goals, and the intervention is designed based on the assessment of those goals. The control group (CG) is on a waiting list.
The online program “Inlife,” described in Christie et al. (57), aims to provide SS and encourage the development of positive interactions with loved ones, friends, and other significant members of their support network, analyzing secondarily its effect on loneliness, psychological distress, and QoL.
Dichter et al. (58) developed the Internet-based intervention “Talking Time.” This intervention is based on support groups where the exchange and reciprocal learning are important and how these can influence emotional wellbeing, QoL, and other psychological variables. The CG remains on a waiting list.
Tinoco-Camarena et al. (59) present an online program called “Dialog Circles” to reduce burden and improve positive mental health, conducted by a team of nurses, with a duration of 90 min and a frequency of 15 days in which SS is provided by creating safe spaces that allow participants, organized in groups, to express problems, difficulties, and feelings about their role as caregivers.
All studies have had at least two measurement points. Here, T0 will be defined as the pre-test or initial evaluation moment, T1 as the post-test moment, T2 as the follow-up, and T3 as a third moment or a second follow-up, if any. Thus, in the selected trials, we find that all have a T0 and T1, with an average time of 3 months from the start of the study. Nine of the studies have a T2 with an average of 6.2 months from the start of the trial. The RCTs by Boots et al. (45) and Dichter et al. (58) are the only ones that do not have a T2.
The results of methodological quality measured through the PEDro Scale (Table 5) show that only one study reaches excellent methodological quality with 10 points (56). The rest of the studies demonstrate good methodological quality with scores ranging from 6 to 8 points (45, 50, 51, 53–59). In the RCTs where subjects and therapists could not be blinded, it is specified that blinding could not be achieved due to the type of intervention applied, mostly because it was a web-based or telephone-based intervention. Overall, methodological quality is good in the selected studies.
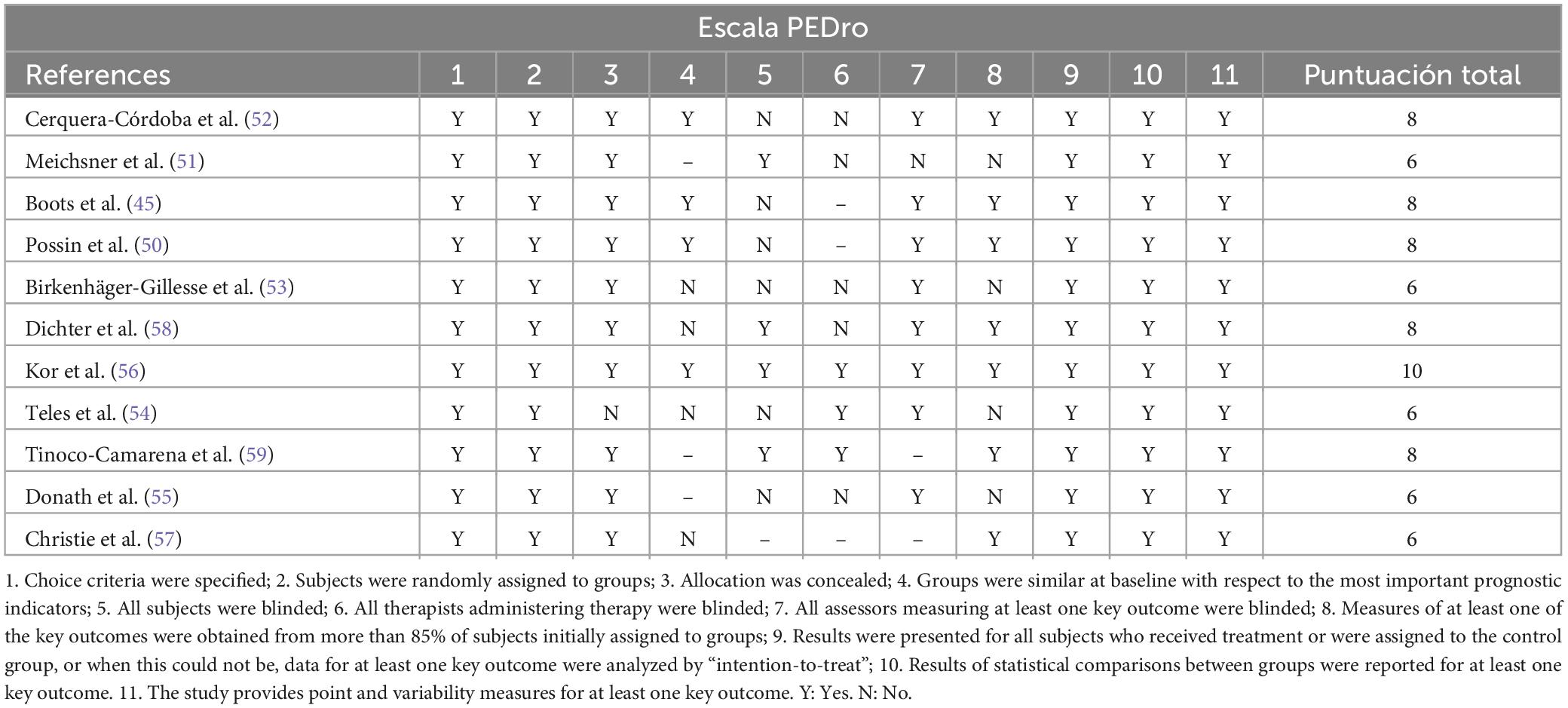
Table 5. Methodological quality results.
Table 5 presents the results of the Cochrane bias risk assessment, and each of the evaluated items is described below. All selected RCTs show a low risk in random sequence generation. The methods used include computer generation, block allocation, allocation by hour and date of submission, and random selection.
All RCTs show a low risk in this criterion. All subjects were recruited through various means, including mailing lists, social networks, advertising, community centers, associations, etc., for subsequent evaluation and random group allocation, preventing prediction of group assignment.
Only two studies (56, 59) demonstrated adequate blinding of participants and personnel, presenting a low risk of bias. In the remaining articles, except for Birkenhäger-Gillesse et al. (53) and Christie et al. (57), where masking is not clear, there is a high risk of bias due to no concealment of the type of intervention carried out for both participants and personnel. In all cases, the recipient of the intervention knows which group they belong to, mainly due to the type of intervention received.
All RCTs show a low risk of bias in outcome assessment, as they include trials in which the assessors were blinded at all measurement points, either due to unawareness of group allocation or through the design of computerized self-assessment. Only four RCTs show a low risk of bias in this criterion (51, 52, 55, 59). In these trials, results regarding participant dropout or attrition are analyzed, demonstrating a low dropout rate that does not affect the displayed results, and effects are analyzed based on initial measurements. In the remaining studies, methods such as intention-to-treat analysis or protocol approaches are employed to address missing data in the study. In the trials by Tinoco-Camarena et al. (59) and Christie et al. (57), the provided data are insufficient to identify the risk of bias in the displayed programs.
All RCTs have study protocols or rely on previous studies with minimal or no changes, presenting results based on them and reporting expected and anticipated outcomes. Despite Donath et al.’s (55) trial having a protocol, it is the only one that presents a high risk of bias, as it focused solely on results that were significant in the primary analysis.
The variability in the scales and measurement instruments used in each study and the disparity in their content, along with the particular characteristics of the sample, can also represent a bias risk to consider.
The results presented below are categorized according to the therapeutic objective of the intervention (Table 6), considering significant differences between groups at the time of measurement (p < 0.05) and the intervention effect size (if data are provided).
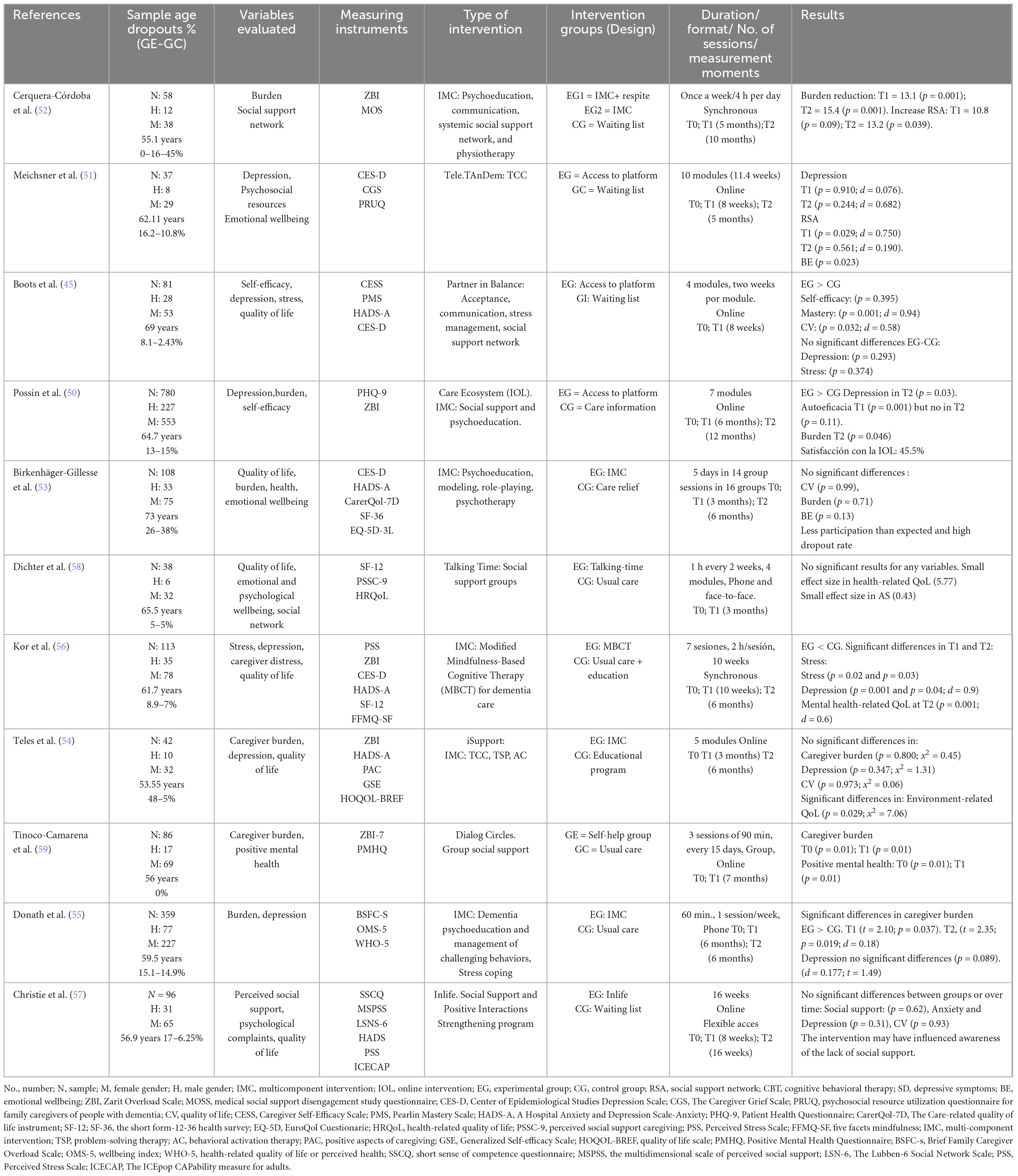
Table 6. Results of the interventions.
Meichsner et al. (51) demonstrated that the IOL “Tele.TAnDem,” based on CBT, did not have significant effect sizes on depressive symptoms (d = 0.076), nor were there significant differences between group experimental (GE) and group control (GC) (p = 0.910) at T1. However, in the measurements at T2, the intervention had a medium effect size, although there were no significant differences between GC and GE (d = 0.682; p = 0.244), with GE showing a decrease in symptom scores over time, while in GC they had slightly increased, concluding that the intervention effect was somewhat insignificant. In the “Partner in Balance (PiB)” program by Boots et al. (45), depressive symptoms did not show a significant effect (f = 1.13), and there were no differences between GC and GE (p = 0.293). There was a difference in the self-efficacy domain (p = 0.395), and it was expected that increasing self-efficacy (attention management, service utilization, care mastery) would decrease depressive symptoms and burden, but this was not observed in the results. One possible explanation provided by the authors is that the program targeted a population of caregivers in the early stages of care, characterized by less stressful situations. Possin et al. (50), in their combined IOL with IT, a multicomponent type, “Care Ecosystem,” showed significant results for GE in depressive symptoms at T2 (p = 0.03). The treatment effect at T1 was also statistically significant (p = 0.001). Furthermore, in the GE, the number of caregivers with high depression scores decreased from 49 to 29 participants by the end of T2 (p = 0.004), while in the GC, it slightly increased from 16 to 22 individuals (p = 0.22). These positive results were a result of individualized attention to caregivers along with addressing their most immediate needs, in addition to more individualized specialist phone contacts. Kor et al. (56), in their combined TCC and Mindfulness program, showed significant differences between GE and GC in depressive symptoms in favor of the treatment group (T1: p = 0.001; T2: p = 0.04), with a large effect size (d = 0.90). The combination of both techniques seems to have had a positive effect on re-evaluating negative thoughts, influencing a decrease in depressive symptoms. Teles et al. (54) presented the multicomponent intervention “iSupport,” with no significant differences for depressive symptoms (p = 0.347), although there were for anxiety. Donath et al. (55), in their telephone-based multicomponent intervention, with psychoeducational and ACE components, report that, for depressive symptoms, there are no significant differences between GE and GC over time (p = 0.089). During the intervention, depressive symptoms decreased but increased at T2. The results show that there is an effect on depressive symptoms during the intervention period, but these effects do not persist over time. Finally, the “Inlife” study developed by Christie et al. (57), on social support, in online mode, one of the secondary outcomes evaluated was depression, with a somewhat insignificant difference between groups (p = 0.31) at T2. The intervention had no effect on depressive symptoms. Its main components were aimed at improving caregivers’ social support, and there was no significant interaction between this variable and depressive symptoms.
In the study by Cerquera-Córdoba et al. (52), significant differences at T1 and T2 regarding burden (p = 0.001) were attributed to psychosocial support aimed at providing strategies for the empowerment of the primary caregiver and group interventions aimed at improving self-care and, consequently, the care of the dependent person. The GE, in its initial evaluation, showed higher results in the burden variable, so the effect size calculation considered that initial measurement rather than the comparison between groups. The multicomponent intervention proposed by Birkenhäger-Guillese et al. (53) does not show improvement in burden (p = 0.71), although it does show significant differences in the subscale assessing physical and emotional function using the SF-36 scale (p = 0.01). In the trial by Possin et al. (50), burden decreased more in the GE than in the GC at T1 (p = 0.008) and T2 (p = 0.046). These results were attributed to the psychoeducational component, which reduced the need for external attention (visits to health centers, emergencies, hospitalizations, etc.), thus reducing the burden of care as caregivers had more information and support. In the trial by Teles et al. (54), there were no effects on burden (x2 = 0.45) or significant differences between GC and GC (p = 0.80). These results were difficult to assess in the intervention context, as during the pandemic lockdown, platform participants could not leave their homes, increasing caregiver stress. The authors consider these variables for future large-scale program trials. Tinoco-Camarena et al. (59), in the online self-help group intervention, show statistically significant results in burden at both T1 and T2 (p = 0.01). The support received through the intervention, as well as the information provided by the self-help group, combined with very high participation and no dropout rate, showed that the intervention influenced lower burden and, furthermore, correlated with self-care and improvement in the care received by the dependent person. In the trial presented by Kor et al. (56), stress decreased (p = 0.03), but not physical burden at T2 (p = 0.39). On the other hand, in the trial by Donath et al. (55), burden did not show a significant difference for both groups (p = 0.126), with a small effect size (d = 0.20). However, regarding time, the GE showed an improvement in burden compared to the GC (T1, p = 0.037; T2, p = 0.019). In general, all presented trials show an improvement in the burden variable, especially in multicomponent interventions that include specific techniques to reduce primary caregiver burden, based on psychoeducation and social support.
In the study by Cerquera-Córdoba et al. (52), social support availability (SSA) is increased by the intervention in the GE, with a statistically significant difference between initial and post-treatment measures (p = 0.09), maintaining its effect over time (p = 0.039). Having time, during which care was provided by another person for certain hours, as well as obtaining self-help strategies, allowed primary caregivers to establish new social relationships and more time to participate in the intervention program. The study by Meichesner et al. (51) evaluated the impact of the intervention on the use of psychosocial resources, finding no significant differences between groups at T1 (p = 0.781; d = 0.22) or at T2 (p = 0.750; d = 0.12). However, there were differences and intervention effects on the use of resources for emotional wellbeing (EWB) only at T1 (p = 0.023; d = 0.190). The telephone-based social support program “Talking-Time,” described in the study by Dichter et al. (58), had no significant effect on the social support variable between groups (p = 0.12), with a small effect size (d = 0.43). Similarly, the article by Christie et al. (57) presents an online intervention aimed at providing and enhancing social support, finding no significant difference in favor of the intervention between groups (p = 0.11). The authors suggest that the results were influenced by the limited number of interactions on the platform.
The study by Boots et al. (45) assessed the intervention’s effect on the QoL of the GE, finding a significant difference (p = 0.032), with a moderate effect size (d = 0.58). The trial by Birkenhäger-Gillese et al. (53) did not show significant differences in the QoL of the caregiver for the effects of the intervention (p = 0.99), measured through the CarerQol-7D scale. In the study by Kor et al. (56), a significantly greater improvement in mental health-related QoL was demonstrated at T2 compared to the GC (p = 0.001), with a large effect size (d = 0.6), not so for QoL related to physical health (p = 0.30). Teles et al. (54) did not show a significant difference between groups in overall QoL (p = 0.973), with a small effect size (x2 = 0.06) but did so in QoL related to the environment (p = 0.029) with a large effect size (x = 7.06). In the study by Christie et al. (57), it is detailed that there is no significant difference in the GE compared to the GC or over time. The study by Teles et al. (54) evaluated the overall QoL and environmental QoL of the groups, finding no significant differences in the former (p = 0.973) with a small effect (x2 = 0.06), but did so in the latter (p = 0.029) with a large effect (x = 7.06). Only the interventions show positive results on QoL, except for the trial by Birkenhäger-Guillesse et al. (53), where participants’ age and educational level could correlate with the results obtained, showing that younger participants and those with a higher educational level benefited more from this type of intervention, but needed it less compared to participants with a lower educational level and older average age.
The variable BE only showed significant differences in two programs: the multicomponent program by Meichsner et al. (51) and the AS program by Tinoco-Camarena et al. (59). In the first program, the component of writing down feelings and emotions of the caregivers through the platform, along with therapist guidance and feedback, increased the BE (p = 0.023). In the second program, the perceived support and self-help from the group led to an increase in BE (p = 0.001). You may insert up to 5 heading levels into your manuscript as can be seen in “Styles” tab of this template. These formatting styles are meant as a guide, as long as the heading levels are clear, Frontiers style will be applied during typesetting.
Following the conducted review, it can be observed that, across all studies, the gender of the informal caregivers (ICs) remains predominantly female, middle-aged, daughters (> 50%) or spouses (> 40%), with varying educational levels from one study to another, indicating an increasingly higher level of education among ICs. Due to differences in the sociodemographic characteristics of the population across studies, it’s important to consider the context for conducting a detailed analysis from a gender perspective (60). The analysis confirms that interventions with multiple components (IMCs) are the most utilized within the established timeframe (2018–2023), albeit with differences in the intervened variables. Except for five trials (52, 53, 57–59), all aim to evaluate the effectiveness of interventions in reducing depressive symptoms (DS). The most common components in all these trials are psychoeducational, ACE, cognitive behavioral therapy (CBT), and social support (SS) interventions, which, in turn, have the most significant effect on the variable of caregiver burden and improvement of quality of life (QoL). These results are supported by other studies where psychoeducation and the application of ACE and SS techniques have a positive effect on caregiver burden and the stress associated with caregiving, improving the QoL of the IC (39, 61–63).
However, upon analyzing the components of each program, those utilizing CBT techniques show greater effectiveness and a significant difference in the intervention effect on the IC group in terms of depression and emotional wellbeing (BE). This is even more pronounced when combined with third-generation therapies like Mindfulness (56). or Acceptance and Commitment Therapy (ACT) Cheng et al. (64) concluded that psychoeducational programs along with mindfulness-based interventions were more effective in reducing DS than other IMCs, but younger individuals benefit more from mindfulness techniques, necessitating their combination with other techniques to address caregiver issues. Given that these are multicomponent programs, the combination of all their components has a positive effect on all evaluated variables. This conclusion suggests that caregiver burden is a multidimensional concept (32, 65), hence requiring an intervention adapted to each specific variable to be addressed. Kwon et al. (66) concluded that an effective tool for reducing DS lies in CBT. The same authors detailed that multicomponent programs including psychoeducation, SS, and CBT have positive effects on the studied sample. Similarly, Bustillo et al. (67) and Gallagher-Thompson and Coon (38) concluded that CBT-based interventions in combination with SS techniques and coping strategies or a combination of at least two theoretical approaches (41) show the best results, in line with Kor et al.’s trial (56), which combines CBT with Mindfulness, showing a large effect on DS, similar to the results of other reviews (68). A special mention to the “iSupport” program (54), which adapts to the cultural context of the intervention, obtaining good results in QoL, though not in DS, according to the authors themselves, due to the timing of the intervention, coinciding with the COVID pandemic.
Therefore, multicomponent programs combining psychoeducation with CBT-based techniques or contextual therapies like ACT or Mindfulness show better results in improving the BE and psychological wellbeing of ICs, enhancing their QoL. However, programs including psychoeducation along with SS techniques achieve greater benefit in obtaining social resources and reducing caregiver burden, as had been shown by previous studies (36–38, 69, 70). As observed in the results of the study by Meichsner et al. (51), CBT alone has a significant effect when intervening in the BE of the IC, with a significant effect over time, supported by other conducted studies, whose results were very similar (18, 26, 37, 40). However, unlike the aforementioned cited studies, the trial by Meichsner et al. (51) does not show significant efficacy on DS, mainly influenced by the content included in the platform, which mainly focused on emotional wellbeing related to anticipatory grief, rather than intervening in DS. Additionally, the intervention did not provide a structured approach by therapists that was similar for all participants, as flexibility was attempted to be provided in platform usage, along with the few exchanges within it between users and therapists.
Among the analyzed randomized controlled trials (RCTs), only the study by Tinoco-Camarena et al. (59) shows high efficacy of an intervention based on SS and self-help groups in variables such as caregiver burden and SS, while the studies by Christie et al. (57) and Dichter et al. (58) provide insignificant results on the same variables. These results are inconsistent with other studies, concluding that perceived SS of the caregiver increases thanks to self-help groups and interventions based on providing psychosocial support through professionals and shared experiences with other caregivers (71, 72). In the study by Christie et al. (57), it is noted that low involvement and commitment in the use of the IOL could explain the low efficacy both in the perceived SS and in the increase of the appraisal of social support (RSA). Furthermore, it is concluded.
The number of trials, while not limited, is insufficient to fully grasp the effectiveness of the interventions due to the multitude of variables that must be considered, hence, it is recommended to conduct more comprehensive and separate studies to better understand intervention efficacy. Additionally, the number of randomized controlled trials (RCTs) found is scarce, given the broad search for effective interventions in informal caregivers (ICs) of dependent individuals. It would be interesting to carry out a more focused search on the effectiveness of more specific interventions. Lastly, the selected trials were conducted within the last 5 years, limiting the results. Therefore, it is recommended to consider different existing protocols for future reviews.
This work also has strengths. The inclusion of web-based programs provides interesting data to establish a new line of research that enhances program content for efficacy, effectiveness, and methodological quality improvement. Additionally, this review demonstrates that interventions with multiple components (IMCs) are the most applied in recent years based on studies conducted in the selected population, so continuing along this path could be positive for establishing solid interventions with greater efficacy in addressing the issues of ICs.
– IMCs combining psychoeducation and SS increase psychosocial resources and decrease caregiver burden.
– IMCs combining cognitive behavioral therapy (CBT) with other techniques are more effective in reducing Depressive Symptoms (DS) and increasing emotional wellbeing (BE).
– Internet-based interventions can improve the quality of life (QoL) and BE of ICs if they include various components combining different intervention models and tailored to the beneficiaries’ specificities.
More studies on the effectiveness and efficacy of Internet-based interventions are needed, as well as a more thorough study on the quality of interventions based on this modality.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
MB-J: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review and editing. SG-M: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review and editing. JG-M: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review and editing. MR-E: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review and editing. EI-S: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review and editing. MC: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review and editing.
The authors declare that no financial support was received for the research, authorship, and/or publication of this article.
This is a short text to acknowledge the contributions of specific colleagues, institutions, or agencies that aided the efforts of the authors. The authors thank the Universidad a Distancia de Madrid (UDIMA) for its support of research.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Agencia Estatal Boletín Oficial del Estado. Ley 39/2006, de 14 de diciembre, de promoción de la autonomía personal y atención a las personas en situación de dependencia (SAAD). Marid: Boletín Oficial del Estado (2006). p. 299.
2. García-Calvente MDM, Mateo-Rodríguez I, Eguiguren AP. El sistema informal de cuidados en clave de desigualdad. Gac Sanit. (2004) 18:132–9.
3. Cerquera Córdoba AM, Galvis Aparicio MJ. Efectos de cuidar personas con Alzheimer: Un estudio sobre cuidadores formales e informales. Pensam Psicol. (2014) 12:144. doi: 10.11144/javerianacali.ppsi12-1.ecpa
4. Theng B, Tran JT, Serag H, Raji M, Tzeng H-M, Shih M, et al. Understanding caregiver challenges: A comprehensive exploration of available resources to alleviate caregiving burdens. Cureus. (2023) 15:e43052. doi: 10.7759/cureus.43052
5. Villarejo Galende A, Eimil Ortiz M, Llamas Velasco S, Llanero Luque M, López de Silanes de Miguel C, Prieto Jurczynska C. Informe de la fundación del cerebro. Impacto social de la enfermedad de alzheimer y otras demencias. Neurologia. (2021) 36:39–49. doi: 10.1016/j.nrl.2017.10.005
6. Covinsky KE, Newcomer R, Fox P, Wood J, Sands L, Dane K, et al. Patient and caregiver characteristics associated with depression in caregivers of patients with dementia. J Gen Intern Med. (2003) 18:1006–14. doi: 10.1111/j.1525-1497.2003.30103.x
7. Mahoney R, Regan C, Katona C, Livingston G. Anxiety and depression in family caregivers of people with Alzheimer disease: The LASER-AD study. Am J Geriatr Psychiatry. (2005) 13:795–801. doi: 10.1097/00019442-200509000-00008
8. Torres Á, Blanco V, Vázquez FL, Díaz O, Otero P, Hermida E. Prevalence of major depressive episodes in non-professional caregivers. Psychiatry Res. (2015) 226:333–9. doi: 10.1016/j.psychres.2014.12.066
9. Pinyopornpanish K, Soontornpun A, Wongpakaran T, Wongpakaran N, Tanprawate S, Pinyopornpanish K, et al. Impact of behavioral and psychological symptoms of Alzheimer’s disease on caregiver outcomes. Sci Rep. (2022) 12:1–9. doi: 10.1038/s41598-022-18470-8
10. Vitaliano PP, Zhang J, Scanlan JM. Is caregiving hazardous to one’s physical health? A meta-analysis. Psychol Bull. (2003) 129:946–72. doi: 10.1037/0033-2909.129.6.946
11. Instituto de Mayores y Servicios Sociales. Cuidados a las personas mayores en los hogares españoles. Madrid: El entorno familiar (2005).
12. Pinquart M, Sörensen S. Helping caregivers of persons with dementia: Which interventions work and how large are their effects? Int Psychogeriatr. (2006) 18:577–95. doi: 10.1017/s1041610206003462
13. Deborah Majerovitz S. Predictors of burden and depression among nursing home family caregivers. Aging Ment Health. (2007) 11:323–9. doi: 10.1080/13607860600963380
14. Flores GE, Rivas RE, Seguel PF. Nivel DE sobrecarga en El desempeño Del Rol Del cuidador familiar DE adulto mayor con dependencia Severa. Cienc Enferm. (2012) 18:29–41. doi: 10.4067/s0717-95532012000100004
15. Espín Andrade AM. Factores de riesgo de carga en cuidadores informales de adultos mayores con demencia. Rev Cubana Salud Publica. (2012) 38:393–402.
16. Watson B, Tatangelo G, McCabe M. Depression and anxiety among partner and offspring carers of people with dementia: A systematic review. Gerontologist. (2018) 59:e597–610. doi: 10.1093/geront/gny049
17. Pérez Peñaranda A, García Ortiz L, Rodríguez Sánchez E, Losada Baltar A, Porras Santos N, Gómez Marcos MÁ. Función familiar y salud mental del cuidador de familiares con dependencia. Aten Prim. (2009) 41:621–8. doi: 10.1016/j.aprim.2009.03.005
18. Rodriguez-Sanchez E, Patino-Alonso MC, Mora-Simón S, Gómez-Marcos MA, Pérez-Peñaranda A, Losada-Baltar A, et al. Effects of a psychological intervention in a primary health care center for caregivers of dependent relatives: A randomized trial. Gerontologist. (2013) 53:397–406. doi: 10.1093/geront/gns086
19. Isik AT, Soysal P, Solmi M, Veronese N. Bidirectional relationship between caregiver burden and neuropsychiatric symptoms in patients with Alzheimer’s disease: A narrative review. Int J Geriatr Psychiatry. (2019) 34:1326–34. doi: 10.1002/gps.4965
20. Zarit SH, Reever KE, Bach-Peterson J. Relatives of the impaired elderly: Correlates of feelings of burden. Gerontologist. (1980) 20:649–55. doi: 10.1093/geront/20.6.649
21. Narváes Bravo ML, Martínez Martínez D. Caracterización del síndrome de sobrecarga del cuidador en familiares de pacientes institucionalizados y no institucionalizados con diagnóstico de enfermedad de Alzheimer mediante la escala Zarit (Characterization of caregiver burden syndrome). Incl Desarro. (2015) 3:101–7. doi: 10.26620/uniminuto.inclusion.3.1.2016.101-107
22. Aguilar Gutiérrez AE, Jiménez Reyes J, Álvarez Aguirre A, Sánchez Perales M, Ortega Jiménez M. Sobrecarga del cuidador principal del adulto mayor con enfermedad alzheimer. Epistemus. (2016) 10:30–6. doi: 10.36790/epistemus.v10i21.31
23. Galvis MJ, Cerquera Córdoba AM. Relationship between depression and burden in caregivers of alzheimer disease patients. Psicol Desde Caribe. (2016) 33:83–103. doi: 10.14482/psdc.33.2.6307
24. Pearlin LI, Mullan JT, Semple SJ, Skaff MM. Caregiving and the stress process: An overview of concepts and their measures. Gerontologist. (1990) 30:583–94. doi: 10.1093/geront/30.5.583
25. Savage S, Bailey S. The impact of caring on caregivers’ mental health: A review of the literature. Aust Health Rev. (2004) 27:111. doi: 10.1071/ah042710111
26. Losada A, Montorio I, Izal M, Márquez M. Estudio e intervención sobre el malestar psicológico de los cuidadores de personas con demencia. El papel de los pensamientos disfuncionales. Madrid: IMSERSO (2005).
27. Turró O, Soler O, Garre J, López S, Vilalta J, Monserrat S. Distribución factorial de la carga en cuidadores de pacientes con enfermedad de Alzheimer. Rev Neurol. (2008) 46:582–8.
28. Crespo M, Rivas MT. La evaluación de la carga del cuidador: Una revisión más allá de la escala de Zarit. Clin Salud. (2015) 26:9–16. doi: 10.1016/j.clysa.2014.07.002
29. Artaso B, Goñi A, Biurrun A. Cuidados informales en la demencia: Predicción de sobrecarga en cuidadoras familiares. Rev Esp Geriatr Gerontol. (2003) 38:212–8. doi: 10.1016/s0211-139x(03)74886-0
30. Blanco V, Guisande MA, Sánchez MT, Otero P, López L, Vázquez FLS. Índrome de carga del cuidador y factores asociados en cuidadores familiares gallegos. Rev Esp Geriatr Gerontol. (2019) 54:19–26. doi: 10.1016/j.regg.2018.03.005
31. Bertel De la Hoz AM. Riesgo a enfermar y sobrecarga del cuidador principal del anciano dependiente. Rev Cienc Bioméd. (2020) 3:77–85. doi: 10.32997/rcb-2012-3170
32. Fundacio Pere Tarrés. Proyectes Socials. La calidad de vida de las cuidadoras informales: Bases para un sistema de valoración. Informe II: El impacto del cuidado en la calidad de vida de las cuidadoras informales. Madrid: Ministerio de trabajo e inmigración, Secretaria de Estado de Seguridad Social (2024).
33. Ramón-Arbués E, Martínez-Abadía B, Martín-Gómez S. Factores determinantes de la sobrecarga del cuidador. Estudio de las diferencias de género. Aten Prim. (2017) 49:308–9. doi: 10.1016/j.aprim.2016.07.003
34. Embracing Carers. Informe sobre el bienestar de los cuidadores 2020. Quién cuida a los que cuidan? Así afectan la Covid-19 y la falta de apoyo a los cuidadores no profesionales. Madrid: Merck (2021).
35. Instituto Nacional de Estadística. Encuesta de discapacidad, autonomía personal y situaciones de dependencia 2020. Cuidadores y cuidados. Cifras absolutas. Madrid: Instituto Nacional de Estadística (2022).
36. Belle SH. Enhancing the quality of life of dementia caregivers from different ethnic or racial groups: A randomized, controlled trial. Ann Intern Med. (2006) 145:727. doi: 10.7326/0003-4819-145-10-200611210-00005
37. Márquez-González M, Losada A, Izal M, Pérez-Rojo G, Montorio I. Modification of dysfunctional thoughts about caregiving in dementia family caregivers: Description and outcomes of an intervention programme. Aging Ment Health. (2007) 11:616–25. doi: 10.1080/13607860701368455
38. Gallagher-Thompson D, Coon DW. Evidence-based psychological treatments for distress in family caregivers of older adults. Psychol Aging. (2007) 22:37–51. doi: 10.1037/0882-7974.22.1.37
39. Saavedra Macías FJ, Bascón Díaz MJ, Árias Sánchez S, García Calderón M, Mora Moreno D. Cuidadoras de familiares dependientes y salud: Influencia de la participación en un taller de control de estrés. Clin Salud. (2013) 24:85–93. doi: 10.5093/cl2013a10
40. Arango-Lasprilla JC, Panyavin I, Merchán EJH, Perrin PB, Arroyo-Anlló EM, Snipes DJ, et al. Evaluation of a group cognitive–behavioral dementia caregiver intervention in Latin America. Am J Alzheimers Dis Other Dement. (2014) 29:548–55. doi: 10.1177/1533317514523668
41. Losada A, Márquez-González M, Romero-Moreno R. Mechanisms of action of a psychological intervention for dementia caregivers: Effects of behavioral activation and modification of dysfunctional thoughts. Int J Geriatr Psychiatry. (2011) 26:1119–27. doi: 10.1002/gps.2648
42. Losada A, Márquez-González M, Romero-Moreno R, Mausbach BT, López J, Fernández-Fernández V, et al. Cognitive–behavioral therapy (CBT) versus acceptance and commitment therapy (ACT) for dementia family caregivers with significant depressive symptoms: Results of a randomized clinical trial. J Consult Clin Psychol. (2015) 83:760–72. doi: 10.1037/ccp0000028
43. Otero P, Vázquez FL, Ferraces MJ, Blanco V, Torres Á. Prevención de la depresión en cuidadoras no profesionales: Relación entre habilidades de solución de problemas y síntomas depresivos. Clin Salud. (2015) 26:1–7. doi: 10.1016/j.clysa.2014.07.001
44. Lewis ML, Hobday JV, Hepburn KW. Internet-based program for dementia caregivers. Am J Alzheimers Dis Other Dement. (2010) 25:674–9. doi: 10.1177/1533317510385812
45. Boots LMM, de Vugt ME, Kempen GI, Verhey FRJ. Effectiveness of a blended care self-management program for caregivers of people with early-stage dementia (partner in balance): Randomized controlled trial. J Med Internet Res. (2018) 20:e10017. doi: 10.2196/10017
46. Cristancho-Lacroix V, Wrobel J, Cantegreil-Kallen I, Dub T, Rouquette A, Rigaud A-SA. web-based psychoeducational program for informal caregivers of patients with Alzheimer’s disease: A pilot randomized controlled trial. J Med Internet Res. (2015) 17:e117. doi: 10.2196/jmir.3717
47. Steffen AM, Gant JRA. Telehealth behavioral coaching intervention for neurocognitive disorder family carers. Int J Geriatr Psychiatry. (2016) 31:195–203. doi: 10.1002/gps.4312
48. Yepes-Nuñeza JJ, Urrútiac G, Romero-Garcíae M, Alonso-Fernándeze S. Declaración PRISMA 2020: Una guía actualizada para la publicación de revisiones sistemáticas. Rev Esp Cardiol. (2021) 74:790–9. doi: 10.1016/j.recesp.2021.06.016
49. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. (2009) 6:e1000097. doi: 10.1371/journal.pmed.1000097
50. Possin KL, Merrilees JJ, Dulaney S, Bonasera SJ, Chiong W, Lee K, et al. Effect of collaborative dementia care via telephone and internet on quality of life, caregiver well-being, and health care use: The care ecosystem randomized clinical trial. JAMA Intern Med. (2019) 179:1658. doi: 10.1001/jamainternmed.2019.4101
51. Meichsner F, Theurer C, Wilz G. Acceptance and treatment effects of an internet-delivered cognitive-behavioral intervention for family caregivers of people with dementia: A randomized-controlled trial. J Clin Psychol. (2019) 75:594–613. doi: 10.1002/jclp.22739
52. Cerquera-Córdoba AM, Tiga-Loza DC, Álvarez-Anaya WA, Dugarte-Peña E, Jaimes-Espíndola LR, Plata-Osma LJ. Ensayo controlado aleatorizado de un programa multicomponente para cuidadores informales de pacientes con Alzheimer. Rev Cuid. (2021) 12:e2002. doi: 10.15649/cuidarte.2002
53. Birkenhäger-Gillesse EG, Achterberg WP, Janus SIM, Kollen BJ, Zuidema SU. Effects of caregiver dementia training in caregiver-patient dyads: A randomized controlled study. Int J Geriatr Psychiatry. (2020) 35:1376–84. doi: 10.1002/gps.5378
54. Teles S, Ferreira A, Paúl C. Feasibility of an online training and support program for dementia carers: Results from a mixed-methods pilot randomized controlled trial. BMC Geriatr. (2022) 22:173. doi: 10.1186/s12877-022-02831-z
55. Donath C, Luttenberger K, Graessel E, Scheel J, Pendergrass A, Behrndt E-M. Can brief telephone interventions reduce caregiver burden and depression in caregivers of people with cognitive impairment? – Long-term results of the German day-care study (RCT). BMC Geriatr. (2019) 19:196. doi: 10.1186/s12877-019-1207-y
56. Kor PPK, Liu JYW, Chien WT. Effects of a modified mindfulness-based cognitive therapy for family caregivers of people with dementia: A randomized clinical trial. Gerontologist. (2021) 61:977–90. doi: 10.1093/geront/gnaa125
57. Christie HL, Dam AEH, van Boxtel M, Köhler S, Verhey F, de Vugt ME. Lessons learned from an effectiveness evaluation of in life, a web-based social support intervention for caregivers of people with dementia: Randomized controlled trial. JMIR Aging. (2022) 5:e38656. doi: 10.2196/38656
58. Dichter MN, Albers B, Trutschel D, Ströbel AM, Seismann-Petersen S, Wermke K, et al. TALKING TIME: A pilot randomized controlled trial investigating social support for informal caregivers via the telephone. BMC Health Serv Res. (2020) 20:788. doi: 10.1186/s12913-020-05523-9
59. Tinoco-Camarena JM, Puig-Llobet M, Lluch-Canut MT, Roldan-Merino J, Moreno-Arroyo MC, Moreno-Poyato A, et al. Effectiveness of the online “dialogue circles” nursing intervention to increase positive mental health and reduce the burden of caregivers of patients with complex chronic conditions. Randomized clinical trial. Int J Environ Res Public Health. (2022) 20:644. doi: 10.3390/ijerph20010644
60. Sanjuán-Quiles A, Alcañiz-Garrán MM, Montejano-Lozoya R, Ramos-Pichardo JD, García-Sanjuán S. La perspectiva de las personas cuidadoras desde un análisis de género. Rev Esp Salud Publica. (2023) 97:e202307062.
61. Losada A, Izal M, Montorio I, Márquez M, Pérez G. Eficacia diferencial de dos intervenciones psicoeducativas para cuidadores de familiares con demencia. Rev Neurol. (2004) 38:701–8.
62. Losada A, Moreno-Rodríguez R, Cigarán M, Peñacoba C, Montorio I. Análisis de programas de intervención psicosocial en cuidadores de pacientes con demencia. Inform Psiquiatr. (2006) 184:173–86.
63. Kajiyama B, Thompson LW, Eto-Iwase T, Yamashita M, Di Mario J, Marian Tzuang Y, et al. Exploring the effectiveness of an Internet-based program for reducing caregiver distress using the iCare stress management e-training program. Aging Ment Health. (2013) 17:544–54. doi: 10.1080/13607863.2013.775641
64. Cheng S-T, Li K-K, Losada A, Zhang F, Au A, Thompson LW, et al. The effectiveness of nonpharmacological interventions for informal dementia caregivers: An updated systematic review and meta-analysis. Psychol Aging. (2020) 35:55–77. doi: 10.1037/pag0000401
65. Acton GJ, Kang J. Interventions to reduce the burden of caregiving for an adult with dementia: A meta-analysis§. Res Nurs Health. (2001) 24:349–60. doi: 10.1002/nur.1036
66. Kwon O-Y, Ahn HS, Kim HJ, Park K-W. Effectiveness of cognitive behavioral therapy for caregivers of people with dementia: A systematic review and meta-analysis. J Clin Neurol. (2017) 13:394. doi: 10.3988/jcn.2017.13.4.394
67. Bustillo ML, Gómez-Gutiérrez M, Guillén AI. Los cuidadores informales de personas mayores dependientes: Una revisión de las intervenciones psicológicas de los últimos diez años. Clin Salud. (2018) 29:89–100. doi: 10.5093/clysa2018a13
68. Collins RN, Kishita N. The effectiveness of mindfulness- and acceptance-based interventions for informal caregivers of people with dementia: A meta-analysis. Gerontologist. (2019) 59:e363–79. doi: 10.1093/geront/gny024
69. Livingston G, Barber J, Rapaport P, Knapp M, Griffin M, King D, et al. Clinical effectiveness of a manual based coping strategy programme (START, STrAtegies for RelaTives) in promoting the mental health of carers of family members with dementia: Pragmatic randomised controlled trial. BMJ. (2013) 347:f6276–6276. doi: 10.1136/bmj.f6276
70. Wilz G, Soellner R. Evaluation of a short-term telephone-based cognitive behavioral intervention for dementia family caregivers. Clin Gerontol. (2016) 39:25–47. doi: 10.1080/07317115.2015.1101631
71. Drentea P, Clay OJ, Roth DL, Mittelman MS. Predictors of improvement in social support: Five-year effects of a structured intervention for caregivers of spouses with Alzheimer’s disease. Soc Sci Med. (2006) 63:957–67. doi: 10.1016/j.socscimed.2006.02.020
Keywords: informal caregiver, depression, burden, quality of life, multiple component intervention
Citation: Barrero-Mejias MA, Gómez-Martínez S, González-Moreno J, Rueda-Extremera M, Izquierdo-Sotorrio E and Cantero García M (2024) Effectiveness of psychological interventions for reducing depressive symptomatology and overload and improving quality of life in informal caregivers of non-institutionalized dependent elderly: a systematic review. Front. Med. 11:1394640. doi: 10.3389/fmed.2024.1394640
Received: 01 March 2024; Accepted: 03 May 2024;
Published: 19 June 2024.
Edited by:
Roger Adams, University of Canberra, AustraliaReviewed by:
Irma Ruslina Defi, Padjadjaran University, IndonesiaCopyright © 2024 Barrero-Mejias, Gómez-Martínez, González-Moreno, Rueda-Extremera, Izquierdo-Sotorrio and Cantero García. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: María Cantero García, bWFyaWEuY2FudGVyb2dhckBnbWFpbC5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.