
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Med. , 25 July 2024
Sec. Geriatric Medicine
Volume 11 - 2024 | https://doi.org/10.3389/fmed.2024.1390057
 Camila Rabelo Monteiro de Andrade1*†
Camila Rabelo Monteiro de Andrade1*† Fernanda Silva Trindade Luz2†Neimy Ramos de Oliveira3†Luciane Kopittke4,5†
Fernanda Silva Trindade Luz2†Neimy Ramos de Oliveira3†Luciane Kopittke4,5† Luiza Marinho Motta Santa Rosa6†Angelica Gomides dos Reis Gomes7†
Luiza Marinho Motta Santa Rosa6†Angelica Gomides dos Reis Gomes7† Frederico Bartolazzi8†Saionara Cristina Francisco9†
Frederico Bartolazzi8†Saionara Cristina Francisco9† Felicio Roberto da Costa2†Alzira de Oliveira Jorge10†
Felicio Roberto da Costa2†Alzira de Oliveira Jorge10† Christiane Corrêa Rodrigues Cimini11†
Christiane Corrêa Rodrigues Cimini11† Marcelo Carneiro12†Karen Brasil Ruschel13,14†
Marcelo Carneiro12†Karen Brasil Ruschel13,14† Alexandre Vargas Schwarzbold15†
Alexandre Vargas Schwarzbold15† Daniela Ponce16†
Daniela Ponce16† Maria Angélica Pires Ferreira17†Milton Henriques Guimarães Júnior18†Daniel Vitório Silveira19†Fernando Graça Aranha20†
Maria Angélica Pires Ferreira17†Milton Henriques Guimarães Júnior18†Daniel Vitório Silveira19†Fernando Graça Aranha20† Rafael Lima Rodrigues de Carvalho21,22†Mariana Frizzo de Godoy23†Lucas Macedo Pereira Viana24†Vânia Naomi Hirakata4†
Rafael Lima Rodrigues de Carvalho21,22†Mariana Frizzo de Godoy23†Lucas Macedo Pereira Viana24†Vânia Naomi Hirakata4† Maria Aparecida Camargos Bicalho25,26,27,28†
Maria Aparecida Camargos Bicalho25,26,27,28† Milena Soriano Marcolino27,29†
Milena Soriano Marcolino27,29†Context: COVID-19 induces complex distress across physical, psychological, and social realms and palliative care (PC) has the potential to mitigate this suffering significantly.
Objectives: To describe the clinical characteristics and outcomes of COVID-19 patients with an indication of PC, compared to patients who had no indication, in different pandemic waves.
Methods: This retrospective multicenter observational cohort included patients from 40 hospitals, admitted from March 2020 to August 2022. Patients who had an indication of palliative care (PC) described in their medical records were included in the palliative care group (PCG), while those who had no such indication in their medical records were allocated to the non-palliative care group (NPCG).
Results: Out of 21,158 patients, only 6.7% had indication for PC registered in their medical records. The PCG was older, had a higher frequency of comorbidities, exhibited higher frailty, and had a higher prevalence of clinical complications and mortality (81.4% vs. 17.7%, p < 0.001), when compared to the NPCG. Regarding artificial life support, the PCG had a higher frequency of dialysis (20.4% vs. 10.1%, p < 0.001), invasive mechanical ventilation (48.2% vs. 26.0%, p < 0.001) and admission to the intensive care unit (53.6% vs. 35.4%, p < 0.001). These differences were consistent across all three waves.
Conclusion: A low proportion of patients received PC. Patients in PCG were more fragile, had more clinical complications, and had a higher mortality. On the contrary to our expectations, they received more artificial life support in all three waves. Taken together, these findings suggest that decisions regarding PC indication were made too late, within a context of end-of-life and therapeutic failure.
The COVID-19 pandemic has had a significant impact on healthcare systems worldwide, with over 772 million cases and almost 7 million deaths globally (1). This unprecedented situation has led to several hospitalizations, stemming from either the direct impact of the infection or the exacerbation of pre-existing health conditions (2, 3).
Individuals afflicted by COVID-19, along with their families, endured multifaceted distress arising from severe physical symptoms related to the disease and its complications, and major psychological and social repercussions stemming from social isolation and other pandemic-related factors. In this context, palliative care (PC), a healthcare approach focused on alleviating suffering, is essential for providing better care (4).
Palliative care plays a crucial role in managing prevalent symptoms in COVID-19-infected patients, such as breathlessness and agitation, and involves empathetic communication with patients and families, whether in-person or through virtual platforms (5). Palliative care also aids clinicians in aligning the treatments provided with patients’ values and goals (6), and supports families in bereavement (7). Importantly, PC should not be contingent on the patient’s prognosis (8) because it is designed to integrate seamlessly with curative treatments (9).
Despite the clear benefits of PC, it was estimated that before COVID-19, less than 15% of people in need received it (10). The pandemic exacerbated the demand for health resources, including PC consultation, leading to a lower proportion of patients obtaining this care (11, 12), a situation particularly dire in low and middle-income countries, where health systems are generally less robust and have fewer resources compared to high-income countries (4).
During the pandemic, the demand for life support measures, such as invasive mechanical ventilation, dialysis, and ICU admissions, increased exponentially (13, 14). These interventions, while critical for some patients, may not align with the goals of care for those who are severely ill and have limited chances of recovery (15, 16). This discrepancy highlights the importance of early PC interventions to ensure that treatments are consistent with the patients’ wishes and overall health status (9, 16–19). By integrating PC early in the treatment course, healthcare providers can better manage symptoms, reduce unnecessary interventions, and improve the quality of life for patients and their families (7, 8, 11, 19). In this scenario, the pandemic highlighted the urgent need to optimize PC referrals and implement systematic protocols to ensure timely care (16, 20–22).
Studies assessing COVID-19 patients eligible for PC, considering their underlying diseases, clinical complications during hospitalization, and use of artificial life support, are scarce, particularly in developing countries outside Asia. Therefore, this study aims to describe the clinical characteristics and outcomes of COVID-19 in this population compared to patients who were not indicated for PC across the three different pandemic waves. The sample was collected in Brazil, a country severely hit by the COVID-19 pandemic (23).
Our initial hypothesis posited that patients in the PCG would be less likely to receive life support measures, given their lower likelihood of benefiting from them compared to patients in the non-palliative care group (NPCG), especially in a scenario of limited health resources.
This is a substudy of the Brazilian COVID-19 Registry, a retrospective multicenter observational cohort that includes 40 Brazilian hospitals, funded by both public and private sources, located in 18 different cities, across six Brazilian states (Bahia, Minas Gerais, Pernambuco, Rio Grande do Sul, Santa Catarina, and São Paulo). The Brazilian COVID-19 Registry has been described in detail previously (24).
The study followed a predefined protocol (24). It adheres to the Strengthening the Reporting of Observational Studies in Epidemiology guidelines (25) and to the Helsinki Declaration. It has been approved by the Brazilian National Committee for Research Ethics (Comissão Nacional de Ética em Pesquisa, CONEP, CAAE: 30350820.5.1001.0008). The study was exempt from the individual free and informed consent term, considering its retrospective nature, the pandemic context, and the use of unidentified data.
Consecutive patients aged 18 or older with laboratory-confirmed COVID-19 according to the World Health Organization guidance (26), admitted to one of the participating hospitals between March 2020 and August 2022, were included. Those who manifested COVID-19 symptoms during their hospital stay, who were transferred to other non-participant hospitals, or had missing value in the variable concerning PC indication were excluded. This study utilized a convenience sample, and a priori sample size calculation was not performed.
For the current analysis, we categorized patients into two distinct groups: (i) those with documented indications for PC in their medical records, referred to henceforth as the palliative care group (PCG); and (ii) those without any recorded indication for PC, denoted as the non-palliative care group (NPCG).
The primary outcomes were the consumption of artificial life support measures, which included invasive mechanical ventilation (IMV) support and kidney replacement therapy (KRT). Secondary outcomes included admission to the intensive care unit (ICU), hospital length of stay, length of stay in the ICU, nosocomial infection, sepsis, thromboembolic events, and mortality.
Demographic data, underlying comorbidities, clinical characteristics, laboratory and imaging exams, treatment, and outcomes were collected by previously trained personnel from the medical records (Supplementary material 1).
For frailty analysis, the Clinical Frailty Scale (CFS) was used as a reference (27), but the strata were regrouped into 6 groups: (i) fit (includes very fit, well, and managing well); (ii) vulnerable or mild frailty; (iii) moderate frailty; (iv) severe frailty (includes severely frail and very severely frail); (v) terminal illness (life expectancy <6 months); (vi) participants with no information described on medical reports. Patients were classified at hospital admission based on their pre-admission characteristics.
Collected data were included in specific forms on the Research Electronic Data Capture (REDCap) platform (28, 29), hosted in the Telehealth Center from the Universidade Federal de Minas Gerais (30). The data underwent periodic auditing to identify outliers and unexpected values. In instances where such discrepancies were detected, the data was returned to each local coordinator for double-checking, aiming to minimize errors and ensure data quality.
For the descriptive analysis, demographic, clinical characteristics, and outcomes were represented by frequency distribution, using mean and standard deviations, as the sample size was large, while categorical data were described as absolute numbers and proportions.
Clinical characteristics and outcomes of PCG and NPCG were assessed during the whole period of data collection and stratified by COVID-19 waves. The first wave comprised the period from March 10th, 2020, to November 14th, 2020; the second wave was from November 15th, 2020, to December 25th, 2021, and the third wave was from December 26th, 2021, to March 8th, 2022 (31). The PCG was compared to NPCG using the t-test for continuous variables and Fisher’s exact test for categorical variables. In addition, patients’ characteristics were compared within each group, considering the three different waves, with the aim of identifying changes over the course of the pandemic. The significance level was set at a two-tailed p-value ≤ 0.05.
Since frailty assessments were conducted only during the second and third waves, participants from the first wave were excluded from the analysis of this variable. The same applies to vaccination data, which was available only from the second wave onward, as Brazil did not have access to vaccinations during the first wave.
Statistical analyses were conducted using IBM SPSS Statistics (IBM SPSS Statistics for Macintosh, Version 26.0 Armonk, NY: IBM Corp.RRID:SCR_019096).
Among 21,158 patients, 1,425 (6.7%) had a documented indication for PC in their medical records, with a higher frequency observed during the first wave (8%, 615/7,677), followed by the third (6.8%, 157/2,299), and the second wave (5.8%, 653/11,182). Patients in the PCG were older in both overall analysis (74 ± 14 vs. 58 ± 16 years) and stratified per wave analysis. There was a higher proportion of women (50.7% vs. 46.9%) compared to the NPCG in the overall analysis. This sex difference was observed in the first wave but not in the other waves (Table 1). Women were older in the overall analyses when compared to men, but this difference was not clinically relevant: 59 ± 17 vs. 58 ± 16 years (data not shown).

Table 1. Baseline demographics, underlying comorbidities and clinical characteristics at hospital presentation of COVID-19 patients with and without a palliative care indication registered in their medical records, including an overall comparison and a stratified analysis by COVID-19 waves.
Overall, the PCG exhibited a higher burden of comorbidities and a lower proportion of patients without comorbidities when compared to the NPCG (16.4% vs. 32.4%, p < 0.001, in the overall analysis). This was also observed in the stratified comparisons (Table 1). The overall prevalence of various comorbidities was higher in the PCG, except for asthma (4.0% vs. 5.7%, p = 0.006) and obesity (10.0% vs. 17.7%, p < 0.001), which were more frequent in the NPCG. While this difference persisted in the first and second waves, it became nonsignificant for several comorbidities in the third wave, such as cirrhosis, chronic kidney disease, chronic obstructive pulmonary disease, and heart failure. Cancer, stroke, and dementia were consistently more prevalent in the PCG across all three waves.
There was a high proportion of missing data concerning COVID-19 vaccination among the patient records (72.2% of cases during the second wave and 53.8% during the third wave). There was no significant difference in vaccination between groups in overall or stratified analyses (Table 1).
There was also a high proportion of missing data (38.9%) for frailty assessment during the period this data was collected (second and third waves). Among those, the PCG demonstrated greater frailty, with a higher proportion of vulnerable or frail patients, in both overall and stratified analyses. Conversely, the PCG had a lower proportion of fit individuals in overall analyses (36.3% vs. 84.4%, p < 0.001), as well as during the second (43.8% vs. 87.8%, p < 0.001) and third (11.9% vs. 59.6%, p < 0.001) waves (Table 1). Throughout the course of the pandemic, there was a significant reduction in the proportion of fit patients in both groups. In the NPCG, the proportion dropped from 87.8% in the second wave to 59.6% in the third, while in the PCG, it fell from 43.8 to 11.9% (data not shown). The proportion of patients with a life expectancy <6 months was significantly higher in the PCG (1.5% [8/538] vs. 0.1% [5/7,889], p < 0.001) in both overall and stratified analyses (Table 1).
Upon hospital presentation, dyspnea was the most prevalent symptom (Supplementary Table S1) in both groups and afflicted a significantly higher proportion of patients in the PCG during the first and third waves, but not in the second wave or in the overall analysis when compared to the NPCG. Impaired consciousness (Glasgow Coma Scale <15) at hospital presentation were more common in the PCG, when compared to the NPCG, in the overall (32.7% vs. 7.7%, p < 0.001), and in stratified analysis (Supplementary Table S1). Patients in PCG needed greater support upon hospital presentation, with higher use of IMV and vasoactive amines, in the overall comparison (8% vs. 3.1%, p < 0.001 and 7.1% vs. 2.6%, p < 0.001, respectively) and during the first and second waves. There was no significant difference between groups in the third wave (Table 1).
Regarding artificial life support during the entire period of hospitalization, when compared to the NPCG, the PCG received more KRT overall (20.4% vs. 10.1%, p < 0.001) and in the stratified analysis, with the following proportions: first wave (19.1% vs. 10.9%, p < 0.001), second wave (24.2% vs. 10.4%, p < 0.001), and third wave (9.6% vs. 5.7%, p < 0.001). The PCG group also required IMV more often: 48.2% vs. 26.0%, p < 0.001 in the overall analysis; 49.0% vs. 28.1%, p < 0.001 in the first wave; 51.6% vs. 27.3%, p < 0.001 in the second; and 31.4% vs. 12.9%, p < 0.001 in the third wave (Table 2). There was a significant reduction in the use of KRT and IMV in both groups during the third wave in comparison to the other waves (Supplementary Table S2).
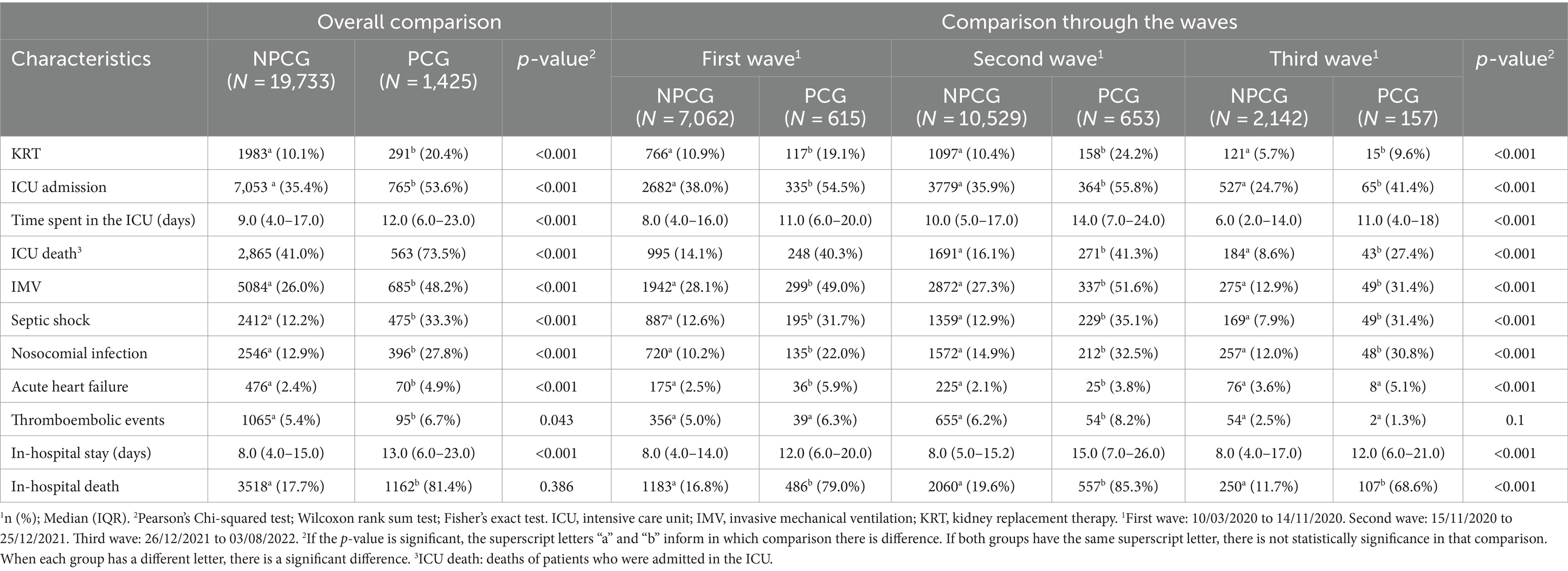
Table 2. Outcomes of COVID-19 patients with palliative care indication in their medical records and those without the indication for palliative care, overall comparison and stratified analysis by COVID-19 waves.
Patients in the PCG were more frequently admitted to the ICU (53.6% vs. 35.4%, p < 0.001) when compared to the NPCG, and this difference was sustained across all three waves (Table 2). In the PCG, there was a significant reduction in the ICU beds used in the third wave (41.4%) when compared to the first (54.5%) and second (55.8%) waves (p=0.004). A similar trend was observed in the NPCG, with ICU admissions peaking in the first wave, showing intermediate values in the second wave, and reaching its lowest point in the third wave (Supplementary Table S2). Concerning clinical complications during hospitalization (Table 2), the PCG had a higher incidence of septic shock (33.3% vs. 12.2%, p < 0.001), nosocomial infection (27.8% vs. 12.9%, p < 0.001), and acute heart failure when compared to the NPCG (4.9% vs. 2.4%, p < 0.001) in overall analyses. In the stratified analysis, this difference remained significant for septic shock and nosocomial infection but not for acute heart failure in the third wave. In the analysis within the PCG, comparing the waves, there was no difference in the incidence of septic shock or acute heart failure. However, there was a higher incidence, within this group, of nosocomial infection in the second wave compared to the first wave (32.5% vs. 22%, p < 0.001; Supplementary Table S2). There was no significant difference in the incidence of thromboembolic events between groups in the overall analysis, but the PCG had a higher incidence of this event when compared to the NPCG in the second wave (Table 2).
Patients in the PCG had a longer hospital stay (13 [6–23] vs. 8 [4–15] days, p < 0.001) and spent more days in the ICU (12 [6–23] vs. 9 [4–17] days, p < 0.001) in overall and stratified analyses (Table 2), and there was no significant difference within the PCG in the wave comparison (Supplementary Table S2). This group also had a higher overall mortality rate (81.4% vs. 17.7%, p < 0.001), which was consistent in stratified analyses for the different waves (first 79% vs. 16.8%, p < 0.001; second 85.3% vs. 19.6%, p < 0.001; and third 68.6% vs. 11.7%, p < 0.001; Table 2). Comparing each group across the waves, mortality was significantly higher in the second wave when compared to the third wave for both groups (Supplementary Table S2). A higher proportion of patients who were admitted to the ICU died in this setting in the PCG, when compared to the NPCG (73.5% vs. 41%, p < 0.001) in the overall and stratified analyses (Table 2). And there was no significant difference in this outcome among the PCG across the waves (Supplementary Table S2).
Within this large cohort of COVID-19 hospitalized patients, we identified a notably small proportion of patients with indication for PC (less than 7%) based on medical records. Patients in the PCG were older, had more comorbidities, a higher frequency of frailty and clinical complications, and had a higher in-hospital mortality rate when compared to the NPCG, as anticipated. However, unexpectedly, this group received a greater extent of artificial life support measures, such as IMV and KRT, experienced an extended hospital stay, a heightened rate of ICU admissions, as well as a longer period in the ICU.
The shockingly low proportion of patients with an indication for PC in our cohort may be partially attributed to challenges associated with prognosticating an acute and largely unknown infectious disease (11). However, it could also stem from a lack of awareness regarding PC, its association with end-of-life care (32), and a sense of defeat among healthcare professionals primarily trained for curative purposes (33). The underutilization of PC services during the pandemic had been reported in other studies, but not to the extent that our findings suggest (11, 12, 18, 34–36). In a retrospective cohort conducted in the United States, it was revealed that less than 40% of critically ill patients admitted to the ICU with severe COVID-19 received a PC consultation (11). A Brazilian cohort study from two of the largest COVID-19 treatment centers in São Paulo (35) showed that 17% of COVID-19 patients had PC indication, which is significantly lower than previously reported by American data but is still nearly 2.5 times higher than our findings.
We have not collected data to ascertain how many patients with PC eligibility did not receive this care pathway. However, the substantial presence of patients grappling with conditions such as heart failure, active cancer, and dementia and afflicted with serious clinical complications such as septic shock in the NPCG leads us to surmise that a significant number of individuals may have been overlooked in terms of receiving compassionate care. This underutilization is likely influenced by several factors, including a limited understanding of this care pathway among the Brazilian general population, healthcare professionals, and policymakers (36) and the low availability of specialized teams, which are unequally distributed across the country and lacking integration (37, 38). In Brazil, the provision of PC is primarily concentrated in hospitals, but the majority of them do not have a PC team (37).
Based on a higher utilization of artificial life support and ICU beds, higher proportion of ICU deaths, longer hospital and longer ICU stay among patients in the PCG compared to the NPCG, we posit that PC was likely contemplated after the implementation of invasive measures or only after therapeutic failure and near death. These findings are in line with previous publications (11, 18, 34, 35) and may indicate that health professionals were more likely to recommend palliative care for patients with more severe COVID-19.
Data on frailty were collected from the second wave on, and it was noteworthy the high rate of missing data. We found a relevant prevalence of fit individuals in PCG, especially during the second wave, and very low rates of patients classified in the last strata of frailty, meaning a life expectancy of less than 6 months. The significant numbers of fit individuals in the PCG support our hypothesis that many patients had the indication for PC only after therapeutic failure. And the low proportion of patients classified as terminally ill, especially in an aging world where non-communicable diseases associated with frailty are leading causes of death (10), along with the high rate of missing data, may indicate a lack of professional preparedness in assessing frailty and valuing this parameter in the decision-making process.
The rapid and unpredictable progression of COVID-19 has led many patients to lose their ability to make decisions (8), making it even more challenging to construct a realistic care plan aligned with a patient’s preferences. We identified certain factors that could have impeded communication between patients and the healthcare team in the PCG right from hospital admission. While both groups exhibited high rates of dyspnea, the PCG had a higher prevalence of neurological manifestations and the use of mechanical ventilation. These factors may have hindered the identification of a patient’s pre-existing comorbidities, functional status, values, and wishes, which are essential elements for crafting an individualized care plan (39).
As predicted, patients in the PCG exhibited a heightened mortality rate. However, we observed a decline in this outcome during the third wave, coupled with reductions in ICU admissions, KRT usage, and Substitute for IMV administration. These positive trends were evident in both groups and may be linked to the widespread vaccination efforts and the prevalence of variants with lower lethality (40). We observed comparable vaccination rates in both groups, a finding that could have been influenced by the considerable amount of missing data. Vaccination status, akin to frailty, may have been undervalued, given the limited documentation of this information in the medical records, even in a setting of high comorbid rates.
It is important to emphasize that our study did not measure specialized delivery of PC, because this variable was not collected. Our study gathered data from medical records and included patients in PCG when any mention of this type of care was registered. This strategy aimed to analyze when the frontline healthcare professional considered PC. During the pandemic, the primary guiding document for PC in Brazil was the 41st resolution issued by the Brazilian Ministry of Health in 2018 (41). It provides guidelines for the organization of PC, in light of integrated continuous care, within the Brazilian Unified Health System Sistema Único de Saúde (SUS). This resolution specifies that care should be provided to individuals who are facing a life-threatening illness and, within a hospital setting, should aim to alleviate symptoms that cannot be managed through other means. Consequently, it implies that a significant proportion of COVID-19 patients requiring hospitalization should be included in this care provision, especially those admitted to an ICU.
Our analysis highlights a notably deficient identification of PC needs, which was considered mainly in the context of end-of-life and probably therapeutic failure and not as a way to provide comfort to frail patients with major comorbidities. PC is not about limiting life support, but about making the best, proportionate choice for each individual, considering technical parameters, patients` values, and goals of care. Therefore, its implementation could have mitigated considerable suffering and likely steered toward a more sustainable allocation of healthcare investments. We contend that our study offers a profound basis for reflection on the challenges of a recent past, aiming to better equip us for a future that effectively addresses human suffering arising from illness.
This study compared two groups based on PC indication from medical records data. However, as previously mentioned, the data collection did not assess the disparity between patients eligible for PC and those who ultimately received it, nor did it evaluate the quality of the care provided. Consequently, some patients may have received a palliative approach that was not documented in their medical records. Additionally, a significant percentage of patients lacked information about functionality, a crucial parameter for determining appropriate treatments.
To the best of our acknowledgement, this is the largest study to investigate PC delivery in COVID-19 patients in Brazil and South American countries. Additionally, the inclusion of diverse centers from different regions enhances its applicability to a continental country marked by significant inequalities.
Future research endeavors should delve into the reasons behind defining PC, the availability of specialized care and education on PC, and the quality of care provided. This last dimension can be analyzed by considering data on symptom management, conflicts regarding goals of care, time elapsed between the indication of PC and death, and the time between patient admission to the hospital or ICU and the initiation of palliative care.
Our cohort comprised a substantial number of patients from 40 public and private centers distributed across three macro-regions of Brazil. Only a small group of patients had an indication for PC based on medical reports. The PCG exhibited characteristics such as older age, increased frailty, and a higher prevalence of comorbidities, clinical complications, and mortality compared to the NPCG. They also had higher usage of artificial life support, which contradicted our initial predictions, considering that patients were frailer and had a higher number of comorbidities, making them seemingly less likely to benefit from such measures. Additionally, we observed a low emphasis on functional assessment, leading us to speculate that this parameter was given minimal consideration in the decision-making process.
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
This study was approved by the Brazilian National Committee for Research Ethics (Comissão Nacional de Ética em Pesquisa, CONEP, CAAE: 30350820.5.1001.0008). It was exempt from the individual free and informed consent term, considering its retrospective nature, the pandemic context, and the use of unidentified data.
CA: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Supervision, Writing – original draft, Writing – review & editing. FL: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Supervision, Writing – original draft, Writing – review & editing. NO: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Supervision, Writing – original draft, Writing – review & editing. LK: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Supervision, Writing – original draft, Writing – review & editing. LSR: Conceptualization, Data curation, Methodology, Writing – original draft, Writing – review & editing. AG: Data curation, Writing – review & editing. FB: Data curation, Writing – review & editing. SF: Data curation, Writing – review & editing. FC: Data curation, Writing – review & editing. AJ: Data curation, Writing – review & editing. CC: Data curation, Writing – review & editing. MC: Data curation, Writing – review & editing. KR: Data curation, Writing – review & editing. AS: Data curation, Writing – review & editing. DP: Data curation, Writing – review & editing. MF: Data curation, Writing – review & editing. MGJ: Data curation, Writing – review & editing. DS: Data curation, Writing – review & editing. FA: Data curation, Writing – review & editing. RC: Data curation, Writing – review & editing. MG: Data curation, Writing – review & editing. MB: Data curation, Writing – review & editing, Conceptualization, Investigation, Methodology, Project administration, Supervision, Writing – original draft. MM: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. LV: Data curation, Writing – review & editing. VH: Formal analysis, Writing – review & editing.
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This study was supported in part by the Minas Gerais State Agency for Research and Development (Fundação de Amparo à Pesquisa do Estado de Minas Gerais—FAPEMIG) [grant number APQ-01154-21], the National Institute of Science and Technology for Health Technology Assessment (Instituto de Avaliação de Tecnologias em Saúde—IATS)/ National Council for Scientific and Technological Development (Conselho Nacional de Desenvolvimento Científico e Tecnológico—CNPq) [grant number 465518/2014–1]. MM was supported in part by CNPq [grant number 310561/2021–3].
We would like to thank the hospitals that participated in this project. Furthermore, we also thank the clinical staff at those hospitals, who cared for the patients, and all collaborators who helped with data collection.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2024.1390057/full#supplementary-material
1. World Health Organization. WHO COVID-19 dashboard; (2023). Available from: https://covid19.who.int/?bot=1. Accessed May 2, 2024
2. Rey, JR, Caro-Codón, J, Rosillo, SO, Iniesta, AM, Castrejón-Castrejón, S, Marco-Clement, I, et al. Heart failure in COVID-19 patients: prevalence, incidence and prognostic implications. Eur J Heart Fail. (2020) 22:2205–15. doi: 10.1002/ejhf.1990
3. Dufour, JF, Marjot, T, Becchetti, C, and Tilg, H. COVID-19 and liver disease. Gut. (2022) 71:2350–62. doi: 10.1136/gutjnl-2021-326792
4. Bhadelia, A, Grant, L, De Lima, L, Knaul, F, and Pettus, K. How pandemics affect health systems and resource allocation: impact on palliative care In: L Lima, K Pettus, J Downing, S Connor, and J Marston, editors. Palliative care and COVID19 series–briefing notes compilation. Houston: IAHPC Press (2020). 5–7.
5. Leong, YY, Bakar, FA, Siow, YC, Racp, R, and Lim, BL. Characteristics, symptom management and outcomes in Covid-19 patients referred to palliative care in a tertiary hospital. Mcgill J Med. (2022) 77:454–461.
6. Yen, YF, Hu, HY, Chou, YC, Chen, CC, and Ho, CY. Utilization of palliative care screening tool to early identify patients with COVID-19 needing palliative care: A cohort study. Int J Environ Res Public Health. (2022) 19:18. doi: 10.3390/ijerph19031054
7. Lobb, E, Maccallum, F, Phillips, JL, Agar, M, Hosie, A, Breen, LJ, et al. The COVID-19 pandemic: bereavement outcomes between hospital and home deaths in palliative care. J Pain Symptom Manag. (2023) 67:147–56. doi: 10.1016/j.jpainsymman.2023.10.025
8. Ting, R, Edmonds, P, Higginson, IJ, and Sleeman, KE. Palliative care for patients with severe covid-19. BMJ. (2020) 14:m2710. doi: 10.1136/bmj.m2710
9. World Health Organization. COVID-19 clinical management: living guidance. (2021). Available from: https://www.who.int/publications/i/item/WHO-2019-nCoV-clinical-2021-2. Accessed Jan 18, 2024.
10. Global Atlas of Palliative Care. 2nd Edition Global Atlas of Palliative Care at the End of Life Global Atlas of Palliative Care 2nd Edition. (2014). Available from: https://cdn.who.int/media/docs/default-source/integrated-health-services-(ihs)/csy/palliative-care/whpca_global_atlas_p5_digital_final.pdf?sfvrsn=1b54423a_3. Accessed May 18, 2024.
11. Sheehan, J, Ho, KS, Poon, J, Sarosky, K, and Fung, JY. Palliative care in critically ill COVID-19 patients: the early new York City experience. BMJ Support Palliat Care. (2023) 13:107–11. doi: 10.1136/bmjspcare-2020-002677
12. Frydman, JL, Aldridge, M, Moreno, J, Singer, J, Zeng, L, Chai, E, et al. Access to palliative care consultation for hospitalized adults with COVID-19 in an urban health system: were there disparities at the peak of the pandemic? J Palliat Med. (2022) 25:124–9. doi: 10.1089/jpm.2021.0313
13. Truog, RD, Mitchell, C, and Daley, GQ. The toughest triage — allocating ventilators in a pandemic. N Engl J Med. (2020) 382:1973–5. doi: 10.1056/NEJMp2005689
14. Emanuel, EJ, Persad, G, Upshur, R, Thome, B, Parker, M, Glickman, A, et al. Fair allocation of scarce medical resources in the time of Covid-19. N Engl J Med. (2020) 382:2049–55. doi: 10.1056/NEJMsb2005114
15. Arya, A, Buchman, S, Gagnon, B, and Downar, J. Pandemic palliative care: beyond ventilators and saving lives. Can Med Assoc J. (2020) 192:E400–4. doi: 10.1503/cmaj.200465
16. Schoenherr, LA, Cook, A, Peck, S, Humphreys, J, Goto, Y, Saks, NT, et al. Proactive identification of palliative care needs among patients with COVID-19 in the ICU. J Pain Symptom Manag. (2020) 60:e17–21. doi: 10.1016/j.jpainsymman.2020.06.008
17. Managing COVID-19 symptoms (including at the end of life) in the community: summary of NICE guidelines. BMJ. National Institute for Health and Care Excellence (NICE), NHS England, NHS Improvement. (2020) 369:m1461. doi: 10.1136/bmj.m1461
18. Garg, I, Gangu, K, Zabel, KM, Shuja, H, Sohail, AH, Nasrullah, A, et al. Trends in utilisation of palliative care services in COVID-19 patients and their impact on hospital resources in the USA: insights from the national inpatient sample. BMJ Support Palliat Care. (2023):spcare-2023-004621. doi: 10.1136/spcare-2023-004621
19. Shankar, KN, Dugas, J, Jaiprasert, S, Nentwich, L, Caruso, L, Dobie, A, et al. Evaluation of an emergency department-based palliative care extender program on hospital and patient outcomes. West J Emerg Med. (2023) 24:637–43. doi: 10.5811/westjem.56015
20. Kaya, E, Lewin, W, Frost, D, Hannon, B, and Zimmermann, C. Scalable model for delivery of inpatient palliative care during a pandemic. Am J Hosp Palliat Med. (2021) 38:877–82. doi: 10.1177/10499091211005701
21. Burke, RV, Rome, R, Constanza, K, Amedee, M, Santos, C, and Leigh, A. Addressing palliative care needs of COVID-19 patients in New Orleans, LA: A team-based reflective analysis. Palliative Med Reports. (2020) 1:124–8. doi: 10.1089/pmr.2020.0057
22. CKA, A, Woodrell, CD, Meier, DE, Morrison, RS, and Chai, E. A Beacon for dark times: palliative care support during the coronavirus pandemic. NEJM Catalyst Innov Care Delivery. (2020) 1. doi: 10.1056/CAT.20.0204
23. Naghavi, M, Ong, KL, Aali, A, Ababneh, HS, Abate, YH, Abbafati, C, et al. Global burden of 288 causes of death and life expectancy decomposition in 204 countries and territories and 811 subnational locations, 1990–2021: a systematic analysis for the global burden of disease study 2021. Lancet. (2024) 403:2100–32. doi: 10.1016/S0140-6736(24)00367-2
24. Marcolino, MS, Ziegelmann, PK, Souza-Silva, MVR, Nascimento, IJB, Oliveira, LM, Monteiro, LS, et al. Clinical characteristics and outcomes of patients hospitalized with COVID-19 in Brazil: results from the Brazilian COVID-19 registry. Int J Infect Dis. (2021) 107:300–10. doi: 10.1016/j.ijid.2021.01.019
25. von Elm, E, Altman, DG, Egger, M, Pocock, SJ, Gøtzsche, PC, Vandenbroucke, JP, et al. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet. (2007) 370:1453–7. doi: 10.1016/S0140-6736(07)61602-X
26. World Health Organization. Diagnostic testing for SARS-CoV-2: interim guidance, (2020). Available from: https://iris.who.int/handle/10665/334254. Accessed Jan 23, 2024.
27. Rockwood, K, Song, X, MacKnight, C, Bergman, H, Hogan, DB, McDowell, I, et al. A global clinical measure of fitness and frailty in elderly people. CMAJ. (2005) 173:489–95. doi: 10.1503/cmaj.050051
28. Harris, PA, Taylor, R, Thielke, R, Payne, J, Gonzalez, N, and Conde, JG. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. (2009) 42:377–81. doi: 10.1016/j.jbi.2008.08.010
29. Harris, PA, Taylor, R, Minor, BL, Elliott, V, Fernandez, M, O’Neal, L, et al. The REDCap consortium: building an international community of software platform partners. J Biomed Inform. (2019) 95:103208. doi: 10.1016/j.jbi.2019.103208
30. Soriano Marcolino, M, Minelli Figueira, R, Pereira Afonso dos Santos, J, Silva Cardoso, C, Luiz Ribeiro, A, and Alkmim, MB. The experience of a sustainable large scale Brazilian telehealth network. Telemed J E Health. (2016) 22:899–908. doi: 10.1089/tmj.2015.0234
31. Moura, EC, Cortez-Escalante, J, Cavalcante, FV, Barreto, ICHC, Sanchez, MN, and Santos, LMP. Covid-19: evolução temporal e imunização nas três ondas epidemiológicas, Brasil, 2020–2022. Rev Saúde Pública. (2022) 56:105. doi: 10.11606/s1518-8787.2022056004907
32. Kaasa, S, Loge, JH, Aapro, M, Albreht, T, Anderson, R, Bruera, E, et al. Integration of oncology and palliative care: a lancet oncology commission. Lancet Oncol. (2018) 19:e588–653. doi: 10.1016/S1470-2045(18)30415-7
33. Sallnow, L, Smith, R, Ahmedzai, SH, Bhadelia, A, Chamberlain, C, Cong, Y, et al. Report of the lancet commission on the value of death: bringing death back into life. Lancet. (2022) 399:837–84. doi: 10.1016/S0140-6736(21)02314-X
34. Haydar, A, Lo, KB, Goyal, A, Gul, F, Peterson, E, Bhargav, R, et al. Palliative care utilization among patients with COVID-19 in an underserved population: A single-center retrospective study. J Pain Symptom Manag. (2020) 60:e18–21. doi: 10.1016/j.jpainsymman.2020.05.022
35. Almeida, LKR, Avelino-Silva, TJ, Silva DC, DLE, Campos, BA, Varela, G, CMB, F, et al. Palliative care in hospitalized middle-aged and older adults with COVID-19. J Pain Symptom Manag. (2022) 63:680–8. doi: 10.1016/j.jpainsymman.2022.01.004
36. Rodrigues, LF, Da, SJFM, and Cabrera, M. Cuidados paliativos: percurso na atenção básica no Brasil. Cadernos de Saúde Pública. (2022) 38:e00130222. doi: 10.1590/0102-311XPT130222
37. Dos Santos, AF, Ferreira, EA, and Guirro, ÚBP. Atlas dos cuidados paliativos no Brasil 2019. Academia Nacional de Cuidados Paliativos (2022). 55p. [cited 2024 Jan 15]. Available from: https://paliativo.org.br/wp-content/uploads/2020/05/ATLAS_2019_final_compressed.pdf
38. Guirro, ÚBD, Kappel, RC, and Crispim, D. Atlas dos cuidados paliativos no Brasil 2022. Academia Nacional de Cuidados Paliativos. (2023). 64p. [cited 2024 Jan 15]. Available from: https://drive.google.com/file/d/1iWP5UArc82kn3Wrcvc0YgAs90N7JCEq6/view
39. Bender, M, Huang, KN, and Raetz, J. Advance care planning during the COVID-19 pandemic. J Am Board Fam Med. (2021) 34:S16–20. doi: 10.3122/jabfm.2021.S1.200233
40. Link-Gelles, R, Weber, ZA, Reese, SE, Payne, AB, Gaglani, M, Adams, K, et al. Estimates of bivalent mRNA vaccine durability in preventing COVID-19–associated hospitalization and critical illness among adults with and without immunocompromising conditions—VISION network, 2023. MMWR Morb Mortal Wkly Rep. (2023) 72:579–88. doi: 10.15585/mmwr.mm7221a3
41. Office of the Minister/Tripartite Intermanager Commission. Resolution No. 41, October 31, 2018. Provides guidelines for the organization of palliative care, in light of integrated continuous care, within the Unified Health System (SUS). Official Gazette of the Union: edition 225, section 1, page 276, Brasília, DF, October 31, 2018. Available at: https://bvsms.saude.gov.br/bvs/saudelegis/cit/2018/res0041_23_11_2018.html. Accessed on June 2, 2024.)
Keywords: palliative care, COVID-19, clinical characteristics, frailty, hospitalization, outcomes assessment
Citation: Andrade CRM, Luz FST, Oliveira NR, Kopittke L, Santa Rosa LMM, Gomes AGR, Bartolazzi F, Francisco SC, Costa FR, Jorge AO, Cimini CCR, Carneiro M, Ruschel KB, Schwarzbold AV, Ponce D, Ferreira MAP, Guimarães Júnior MH, Silveira DV, Aranha FG, Carvalho RLR, Godoy MF, Viana LMP, Hirakata VN, Bicalho MAC and Marcolino MS (2024) Palliative care and COVID-19: acknowledging past mistakes to forge a better future. Front. Med. 11:1390057. doi: 10.3389/fmed.2024.1390057
Edited by:
Robbert Gobbens, Inholland University of Applied Sciences, NetherlandsReviewed by:
Akram Parandeh, Baqiyatallah University of Medical Sciences, IranCopyright © 2024 Andrade, Luz, Oliveira, Kopittke, Santa Rosa, Gomes, Bartolazzi, Francisco, Costa, Jorge, Cimini, Carneiro, Ruschel, Schwarzbold, Ponce, Ferreira, Guimarães Júnior, Silveira, Aranha, Carvalho, Godoy, Viana, Hirakata, Bicalho and Marcolino. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Camila Rabelo Monteiro de Andrade, Y2FtaWxhcGVwQGdtYWlsLmNvbQ==
†ORCID: Camila Rabelo Monteiro de Andrade, http://orcid.org/0009-0005-6869-1076
Fernanda Silva Trindade Luz, http://orcid.org/0000-0003-4309-9998
Neimy Ramos de Oliveira, http://orcid.org/0000-0001-5408-9459
Luciane Kopittke, http://orcid.org/0000-0002-6606-7756
Luiza Marinho Motta Santa Rosa, http://orcid.org/0000-0002-4741-4871
Angelica Gomides dos Reis Gomes, http://orcid.org/0000-0002-4568-0738
Frederico Bartolazzi, http://orcid.org/0000-0002-9696-4685
Saionara Cristina Francisco, http://orcid.org/0000-0002-9655-6294
Felicio Roberto da Costa, http://orcid.org/0000-0001-9923-236X
Alzira de Oliveira Jorge, http://orcid.org/0000-0003-1366-1732
Christiane Corrêa Rodrigues Cimini, http://orcid.org/0000-0002-1973-1343
Marcelo Carneiro, http://orcid.org/0000-0003-3603-1987
Karen Brasil Ruschel, http://orcid.org/0000-0002-0812-920X
Alexandre Vargas Schwarzbold, http://orcid.org/0000-0002-5535-6288
Daniela Ponce, http://orcid.org/0000-0002-6178-6938
Maria Angélica Pires Ferreira, http://orcid.org/0000-0003-0961-524X
Milton Henriques Guimarães Júnior, http://orcid.org/0000-0002-2127-8015
Daniel Vitório Silveira, http://orcid.org/0000-0002-7381-1651
Fernando Graça Aranha, http://orcid.org/0000-0001-9173-8892
Rafael Lima Rodrigues de Carvalho, http://orcid.org/0000-0003-3576-3748
Mariana Frizzo de Godoy, http://orcid.org/0000-0002-6631-8826
Lucas Macedo Pereira Viana, http://orcid.org/0000-0002-8457-0531
Vânia Naomi Hirakata, http://orcid.org/0000-0003-4645-2080
Maria Aparecida Camargos Bicalho, http://orcid.org/0000-0001-6298-9377
Milena Soriano Marcolino, http://orcid.org/0000-0003-4278-3771
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.