 Carlos Pineda
Carlos Pineda Hugo Sandoval1††
Hugo Sandoval1†† Iván Pérez-Neri
Iván Pérez-Neri Fabián Carranza-Enríquez
Fabián Carranza-Enríquez- 1Instituto Nacional de Rehabilitación Luis Guillermo Ibarra Ibarra, Mexico City, Mexico
- 2Evidence Synthesis Unit, Instituto Nacional de Rehabilitación Luis Guillermo Ibarra Ibarra, Mexico City, Mexico
- 3Department of Rheumatology, Instituto Nacional de Rehabilitación Luis Guillermo Ibarra Ibarra, Mexico City, Mexico
CPPD disease can affect patients’ quality of life through its various clinical presentations. This mini-review discusses the evolution of CPPD from its discovery to current knowledge of its pathogenesis, genetic associations, diagnostics, and treatment options. Despite extensive research, the exact mechanisms of CPPD are not well understood, and there is a notable lack of knowledge about psychosocial impacts and patient experiences. This study aims to present a CPPD Disease Timeline identifying gaps in current knowledge and potential directions for future research. These findings contribute to a broader understanding of CPPD disease and emphasize the importance of continued research and innovation in this field.
Introduction
Calcium Pyrophosphate Deposition (CPPD) Disease occurs when calcium pyrophosphate dihydrate (CPP) crystals are deposited in the articular cartilage and periarticular tissues. This condition is of concern in rheumatology because of its potential impact on a patient’s quality of life (1). CPPD disease is a clinically heterogeneous condition that can present in several forms, including acute calcium pyrophosphate (CPP) crystal arthritis, osteoarthritis (OA) with CPPD disease, chronic CPP crystal inflammatory arthritis, and crowned dens syndrome. The most commonly cartilage calcification associated with CPPD and detected by imaging or histology is referred to as chondrocalcinosis (CC) (2). It affects various anatomical sites, including but not limited to the knee, wrist, hip, spine, and temporomandibular joint (2–4).
Radiographic identification and terminology began to be developed in the 1920s. Familial forms were introduced in the late 1950s. The relationship with calcium pyrophosphate crystals was finally established in the 1960s, leading to the term CPPD, which encompasses all cases of calcium pyrophosphate crystals (CPP) in joints and periarticular tissues.
Consequently, advances in imaging techniques, genetic discoveries, and ongoing insights into novel treatment and management strategies have marked the late 20th and early 21st centuries. This mini-review highlights both the historical background and recent milestones in CPPD disease, including innovative imaging modalities and genetic associations with this entity, such as the ANKH gene, focusing on potential gaps and perspectives.
Figure 1 shows the number of published documents related to CPPD disease recorded per year in the Scopus database from 1975 to 2023. There has been a gradual increase in this number over the years, particularly in the last decade, albeit with some fluctuations; resulting in well-defined peaks and troughs, indicating higher and lower periods of research activity or publication frequency. Since 2014, there has been a noticeable increase in this trend, resulting in a steeper slope. The highest peak occurred in 2021, indicating the maximum number of documents registered. This year was followed by a decrease in 2022 and a partial recovery in 2023.
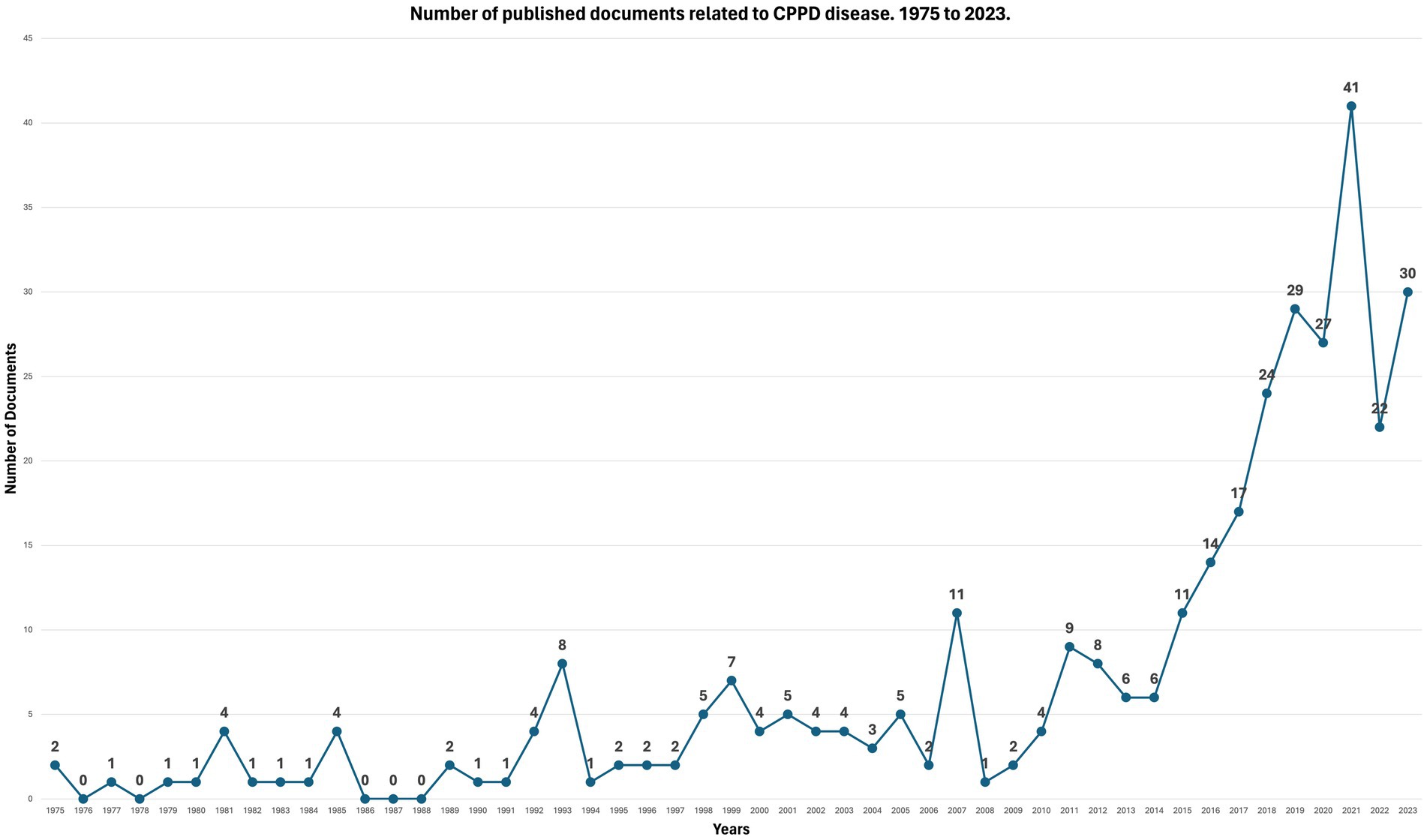
Figure 1. Number of published documents related to CPPD disease 1975–2023 (Source: Scopus).
Although research on CPPD disease began several decades ago and was mainly held by Italian and Anglo-Saxon authors, in recent years an extensive collaborative group has been integrated with participation of many centers throughout the globe.
CPPD disease timeline
19th century
1842. Roderick McLeod identified a white powdery substance on the surfaces of articular cartilage during autopsies, probably representing the first observation of chondrocalcinosis (5, 6).
1873. Robert Adams published a detailed description of chondrocalcinosis in a patient with chronic rheumatic disease. At autopsy, he observed calcification of the fibrocartilage of the knee meniscus. His description provides valuable insights into the pathogenesis and clinical manifestations of this condition (7).
Early 20th century
In its early stages, CPPD disease was often misdiagnosed as rheumatoid arthritis or osteoarthritis because of overlapping clinical features. However, radiographic techniques made it possible to visualize calcium deposits within the cartilage.
1922. Jacques Calvé and Marcel Galland documented the observation of calcification in intervertebral discs that were visible on radiographs (8).
1927. Felix Mandl describes articular cartilage calcifications seen radiographically (9).
1960–62. Dusan Zitnan and Stefan Sitaj coined the term “chondrocalcinosis articularis,” which was followed in 1962, by a detailed description of radiographic calcification of the articular cartilage of members of several Slovak families with chronic oligoarthritis. This was the first report of a familial cluster of chondrocalcinosis (10, 11).
Late 20th century
1962. Daniel McCarty and colleagues found non-urate crystals in the affected joints of two patients (12). In one case, the typical clinical features of acute gouty arthritis were present, but the serum urate level was normal. Following this observation, the researchers then examined under the microscope many samples of synovial fluid removed from so-called arthritic joints under the microscope. They were able to identify non-urate crystals in six additional cases (13).
Additionally, McCarty’s group identified and characterized the presence of calcium pyrophosphate crystals in the synovial fluid of patients with acute synovitis using polarized light microscopy. They established the crystal structure of CPPD and definitively distinguished this clinical entity from other joint diseases based on the nature of the crystals. The authors named the disease as “pseudo-gout” due to its close resemblance to an acute gouty attack (14).
1969. The term “pyrophosphate arthropathy” was introduced to accurately describe the structural joint changes that occur in CPPD disease (15, 16).
1975. The term “calcium pyrophosphate deposition disease” was formally introduced for the first time by various groups of investigators (17, 18). Further descriptions of deposition in diverse anatomical structures were made in subsequent years (3).
1979. Original diagnostic criteria for CPPD disease were proposed by Ryan and McCarty (19).
1989. Magnetic resonance imaging emerged as an innovative method for assessing calcium deposition in periarticular tissues, beginning with the description of two separate case reports with involvement of cervical vertebrae (20, 21).
1995. First description of sonographic findings of CPPD in the knee joints of 28 patients with documented CC (22). Ultrasonography showed linear hyperechoic features in the condylar cartilage, parallel to the bone surface, which were interpreted as calcifications because of their agreement with conventional radiography.
1997. A clinical trial demonstrated improvement in pain with the use of hydroxychloroquine in patients with chronic CPPD (23).
Early 21st century
2001–2002. Advances in molecular genetics led to the discovery of ANKH, the first gene associated with the CPPD disease phenotype. The ANKH protein has been implicated in pyrophosphate metabolism, specifically in the transport of pyrophosphate from the intracellular to the extracellular compartment (19–21).
2000s. Multiple studies have been carried out revealing the prevalence and incidence of chondrocalcinosis in different age groups and specific population groups. However, epidemiological studies of this entity are yet to be carried out in the general population (24–31).
2006. Using an “in vivo” rat model, CPP crystals are shown to cleave the caspase-1-activating NALP3 inflammasome, which in turn stimulates production of active IL-1B and IL-18 (32).
2008. Clinical studies increasingly began to focus on the potential use of anakinra, an IL-1 receptor antagonist. In the treatment of CPPD disease (33).
2009. Use of highly sensitive methods, such as Raman spectroscopy, for the identification of CPP crystals (34–37).
2010s–present
2011. European League Against Rheumatism recommendations for CPPD terminology, diagnosis, and management, mainly focusing on symptom management through pharmacological interventions including NSAIDs and corticosteroids (2, 38).
2011. Ultrasound (US) was identified as a highly accurate tool for detecting CPP crystal deposition in musculoskeletal structures, with both high sensitivity and specificity (39).
2014. A randomized controlled trial failed to prove a substantial benefit of methotrexate for treating CPDD disease (40–42); however, observational studies showing more positive results leave an open question on the role of this drug for the treatment of CPPD disease.
2018. A gain-of-function mutation in TNFRSF11B encoding osteoprotegerin was found to cause familial CPPD disease, suggesting a bone pathology contribution (43).
2018. Preliminary studies on targeted therapies aimed at modulating pyrophosphate metabolism as a treatment modality (44).
2018. The OMERACT group published the new sonographic definitions of elementary lesions in CPPD disease (45). Likewise, the good intra- and inter-observer reliability of US by using these definitions was proven (46).
2019. Development of novel imaging techniques, such as dual-energy CT scans, continue to favor a better understanding of the disease, improve diagnosis and distinguish CPPD among other forms of microcrystalline deposits (47).
2020. A systematic literature review supports the use of anakinra as a therapeutic option for patients with CPPD disease, especially in cases of acute refractory CPPD or when standard treatments are contraindicated (48).
2020. Publication of results of the first clinical trials employing biologic drugs for the treatment of CPPD (49, 50), including tocilizumab in symptomatic patients.
2021. Development of Machine Learning approaches and Electronic Health Record Data algorithms for the identification of CPPD (51).
2022. Classifying Pseudogout using Machine Learning Approaches with Electronic Health Record Data. An approach to the identification of acute subtype of CPPD disease patients using electronic health record data with a positive predictive value of 81% was developed (52).
2022. The first Consensus-based definitions of imaging features characteristic of CPPD on CR, CT, DECT, US and MRI served as a reference for future clinical research studies and diagnostic criteria (53).
2023. Publication of the ACR/EULAR CPPD disease classification criteria, which showed very good diagnostic performance and provided guidance for future research (54).
2023. A clinical trial demonstrates equivalence between colchicine and prednisone for the treatment of acute calcium pyrophosphate crystal arthritis (55).
2023. Development and validation by the OMERACT group of a scoring system to determine the extent of CPPD by US (56). Figure 2 shows a synthetized timeline highlighting the most relevant events listed in the past section.

Figure 2. CPPD timeline.
Identified gaps
Epidemiology and demographics
Although there is a considerable amount of data on the prevalence and incidence of CPPD and chondrocalcinosis, particularly in older populations, there appears to be a gap in detailed epidemiological studies focusing on specific demographics such as younger populations or specific ethnic groups. Understanding the prevalence and characteristics of these diseases in different populations could provide valuable insights into the genetic and environmental risk factors.
Pathogenesis and molecular mechanisms
The exact mechanisms underlying CPPD and chondrocalcinosis are not fully understood. Research into the cellular and molecular pathways involved in crystal formation and deposition may lead to a better understanding of the potential therapeutic targets. Studies into the role of ANKH mutations and their influence on CPPD are particularly promising.
Diagnostic tools and biomarkers
There is ongoing research to improve the diagnostic methods for CPPD and chondrocalcinosis; however, there is still a need for more accurate, non-invasive, and early detection tools. Identification of specific biomarkers associated with these conditions could improve diagnostic accuracy and help monitor disease progression.
Treatment and management
Although there are available treatments to manage the symptoms and complications of CPPD and chondrocalcinosis, of specific therapies targeting the underlying causes of these diseases are lacking. Research into new pharmacological agents or therapeutic approaches that may alter course of the disease or prevent crystal deposition is a potential key intervention that remains unresolved. Similarly, although some small clinical trials have shown treatment benefits with drugs such as hydroxychloroquine, anakinra, or tocilizumab for chronic management or colchicine or prednisone for acute management, an update of new treatment guidelines is needed.
Genetic studies and familial patterns
While familial patterns and genetic links have been identified, particularly with the ANKH gene, more comprehensive genetic studies could provide deeper insights into the hereditary aspects of these diseases. This could lead to a better risk assessment and targeted interventions for individuals with a family history of CPPD or Chondrocalcinosis.
Longitudinal studies
Long-term studies of patients with CPPD and chondrocalcinosis could provide valuable data on the natural history, progression, and long-term outcomes of these diseases. This could improve our understanding of the disease course and improve the management strategies.
Comorbidity and multimorbidity research
Exploring the relationship between CPPD, chondrocalcinosis, and other comorbid conditions (such as osteoarthritis, cardiovascular diseases, and additional associated metabolic disorders) could provide important insights into the broader health impact of these conditions.
Patient-centered research
There is a need for more research focusing on patient experiences, quality of life, and psychosocial aspects of living with CPPD and chondrocalcinosis. This includes understanding the impact on daily activities, mental health, and the effectiveness of different support systems.
Discussion
In conclusion, major advances have been made in the field of CPPD disease since its first description almost two centuries ago, beginning with its first categorization as a separate crystal arthropathy from gout more than six decades ago. Specific areas to be highlighted because of their direct current impact on clinical practice are the development of alternative imaging tools (with a greater diagnostic accuracy than conventional radiography), the first validated classification criteria with international endorsement and an ongoing exhaustive research activity on the underlying pathogenetic mechanisms that trigger and maintain calcium deposition among tissues.
Other fields, like the description of several therapeutic strategies in chronic and acute presentations of CPPD disease, or the discovery of new genetic mutations directly linked to it, though still far from having considerable impact over its natural history, hold promising for further improving how we understand disease pathogenesis in the oncoming years; future research must be directed toward improving long-term clinical outcomes.
Author contributions
CP: Conceptualization, Data curation, Investigation, Methodology, Writing – original draft, Writing – review & editing. HS: Conceptualization, Data curation, Investigation, Methodology, Writing – original draft, Writing – review & editing. IP-N: Conceptualization, Data curation, Investigation, Writing – original draft, Writing – review & editing. CS-F: Conceptualization, Data curation, Investigation, Writing – original draft, Writing – review & editing. FC-E: Conceptualization, Data curation, Investigation, Methodology, Writing – original draft, Writing – review & editing.
Funding
The author (s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
We used Grammarly (https://www.grammarly.com) for a correct application of the English language at the time of writing and editing the present manuscript.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Fuller, A, Cai, K, Filippou, G, Pascart, T, Diaz-Torne, C, Hensey, O, et al. Experience and impact of crystal pyrophosphate deposition (CPPD) from a patient and caregiver perspective: a qualitative exploration from the OMERACT CPPD working group. Semin Arthritis Rheum. (2021) 51:655–60. doi: 10.1016/j.semarthrit.2021.04.010
2. Zhang, W, Doherty, M, Bardin, T, Barskova, V, Guerne, PA, Jansen, TL, et al. European league against rheumatism recommendations for calcium pyrophosphate deposition. Part I: terminology and diagnosis. Ann Rheum Dis. (2011) 70:563–70. doi: 10.1136/ard.2010.139105
3. Resnick, D, and Pineda, C. Vertebral involvement in calcium pyrophosphate dihydrate crystal deposition disease radiographic-pathological correlation. Radiology. (1984) 153:55–60. doi: 10.1148/radiology.153.1.6089266
4. Hutton, CW, Doherty, M, and Dieppe, PA. Acute pseudogout of the temporomandibular joint: a report of three cases and review of the literature. Rheumatology. (1987) 26:51–2. doi: 10.1093/rheumatology/26.1.51
6. Marson, P, and Pasero, G. Some historical remarks on microcrystalline arthritis (gout and chondrocalcinosis). Reumatismo. (2012) 63:199–206. doi: 10.4081/reumatismo.2011.199
8. Calvé, J, and Galland, M. Sur une affection particulière de la colonne vertrebale simulant le mal de Pott (calcification de nucleus pulposus). J Radiol Electrol Med Nucl. (1922) 6:21–3.
9. Mandl, F . Zur Pathologie und Therapie der Zwischenknorpelerkrankungen des kniegelenkes. Arch Klin Chir. (1927) 146:149–214.
10. Zitnan, D, and Sitaj, S. Chondrocalcinosis polyarticularis (familiaris): roentgenological and clinical analysis. Cesk Rentgenol. (1960) 14:27–34.
11. Sitaj, S, Zitnan, D, Trnavska, Z, and Valsik, J. Study on familial outbreaks of alkaptonuria and articular chondrocalcinosis. Bratisl Lek Listy. (1962) 42:129–35.
12. McCarty, DJ, and Hollander, JL. Identification of urate crystals in gouty synovial fluid. Ann Intern Med. (1961) 54:452. doi: 10.7326/0003-4819-54-3-452
13. McCarty, DJ, Kohn, NN, and Faires, JS. The significance of calcium phosphate crystals in the synovial fluid of arthritic patients: the “Pseudogout syndrome.” I. Clinical aspects. Ann Intern Med. (1962) 56:711. doi: 10.7326/0003-4819-56-5-711
14. Kohn, N, Hughes, RE, Jr, MCDJ, and Faires, JS. The significance of calcium phosphate crystals in the synovial fluid of arthritic patients: the “Pseudogout syndrome”. II. Identification of crystals. Ann Intern Med. (1962) 56:738–45. doi: 10.7326/0003-4819-56-5-738
15. Martel, W, Champion, CK, Thompson, GR, and Carter, TL. A roentgenologically distinctive arthropathy in some patients with the pseudogout syndrome. Am J Roentgenol. (1970) 109:587–605. doi: 10.2214/ajr.109.3.587
16. Resnick, D, Niwayama, G, Goergen, TG, Utsinger, PD, Shapiro, RF, Haselwood, DH, et al. Clinical, radiographic and pathologic abnormalities in calcium pyrophosphate Dihydrate deposition disease (CPPD): Pseudogout. Radiology. (1977) 122:1–15. doi: 10.1148/122.1.1
17. Utsinger, PD, Resnick, D, and Zvaifler, NJ. Wrist arthropathy in calcium pyrophosphate dihydrate deposition disease. Arthritis Rheum. (1975) 18:485–91. doi: 10.1002/art.1780180509
18. McCarty, D . Calcium pyrophosphate dihydrate crystal deposition disease −1975. Arthritis Rheum. (1976) 19:275–85. doi: 10.1002/1529-0131(197605/06)19:3+<275::AID-ART1780190702>3.0.CO;2-0
19. McCarty, DJ . Calcium pyrophosphate dihydrate crystal deposition disease: Pseudogout: articular chondrocalcinosis In: D Mccarty , editor. Arthritis and allied conditions. 9th ed. Philadelphia, PA: Lea & Febiger (1979). 1276–99.
20. Ciricillo, SF, and Weinstein, PR. Foramen magnum syndrome from pseudogout of the atlanto-occipital ligament. Case report. J Neurosurg. (1989) 71:141–3. doi: 10.3171/jns.1989.71.1.0141
21. Gomez, H, and Chou, SM. Myeloradiculopathy secondary to pseudogout in the cervical ligamentum flavum. Neurosurgery. (1989) 298:298. doi: 10.1097/00006123-198908000-00024
22. Coari, G, Iagnocco, A, and Zoppini, A. Chondrocalcinosis sonographic study of the knee. Clin Rheumatol. (1995) 14:511–4. doi: 10.1007/BF02208146
23. Rothschild, B, and Yakubov, LE. Prospective 6-month, double-blind trial of hydroxychloroquine treatment of CPDD. Compr Ther. (1997) 23:327–31.
24. De la Garza-Montaño, P, Pineda, C, Lozada-Pérez, CA, Camargo-Ibarias, K, González-Hernández, MF, Avila-Luna, A, et al. Prevalence of chondrocalcinosis in a Mexican tertiary care institution of musculoskeletal disorders. Clin Rheumatol. (2019) 38:2595–602. doi: 10.1007/s10067-019-04614-1
25. Abhishek, A, Doherty, S, Maciewicz, R, Muir, K, Zhang, W, and Doherty, M. Chondrocalcinosis is common in the absence of knee involvement. Arthritis Res Ther. (2012) 14:R205. doi: 10.1186/ar4043
26. Zhang, Y, Terkeltaub, R, Nevitt, M, Xu, L, Neogi, T, Aliabadi, P, et al. Lower prevalence of chondrocalcinosis in Chinese subjects in Beijing than in white subjects in the United States: the Beijing osteoarthritis study. Arthritis Rheum. (2006) 54:3508–12. doi: 10.1002/art.22189
27. Ryu, K, Iriuchishima, T, Oshida, M, Kato, Y, Saito, A, Imada, M, et al. The prevalence of and factors related to calcium pyrophosphate dihydrate crystal deposition in the knee joint. Osteoarthr Cartil. (2014) 22:975–9. doi: 10.1016/j.joca.2014.04.022
28. Neame, RL, Carr, AJ, Muir, K, and Doherty, M. UK community prevalence of knee chondrocalcinosis: evidence that correlation with osteoarthritis is through a shared association with osteophyte. Ann Rheum Dis. (2003) 62:513–8. doi: 10.1136/ard.62.6.513
29. Ramonda, R, Musacchio, E, Perissinotto, E, Sartori, L, Punzi, L, Corti, MC, et al. Prevalence of chondrocalcinosis in Italian subjects from northeastern Italy. The pro. V.A. (PROgetto Veneto Anziani) study. Clin Exp Rheumatol. (2009) 27:981–4.
30. Hameed, M, Turkiewicz, A, Englund, M, Jacobsson, L, and Kapetanovic, MC. Prevalence and incidence of non-gout crystal arthropathy in southern Sweden. Arthritis Res Ther. (2019) 21:291. doi: 10.1186/s13075-019-2077-6
31. Hawellek, T, Hubert, J, Hischke, S, Krause, M, Bertrand, J, Schmidt, BC, et al. Calcification of the acetabular labrum of the hip: prevalence in the general population and relation to hip articular cartilage and fibrocartilage degeneration. Arthritis Res Ther. (2018) 20:104. doi: 10.1186/s13075-018-1595-y
32. Martinon, F, Pétrilli, V, Mayor, A, Tardivel, A, and Tschopp, J. Gout-associated uric acid crystals activate the NALP3 inflammasome. Nature. (2006) 440:237–41. doi: 10.1038/nature04516
33. McGonagle, D, Tan, AL, Madden, J, Emery, P, and McDermott, MF. Successful treatment of resistant pseudogout with anakinra. Arthritis Rheum. (2008) 58:631–3. doi: 10.1002/art.23119
34. Cheng, X, Haggins, DG, York, RH, Yeni, YN, and Akkus, O. Analysis of crystals leading to joint Arthropathies by Raman spectroscopy: comparison with compensated polarized imaging. Appl Spectrosc. (2009) 63:381–6. doi: 10.1366/000370209787944280
35. Fuerst, M, Lammers, L, Schäfer, F, Niggemeyer, O, Steinhagen, J, Lohmann, CH, et al. Investigation of calcium crystals in OA knees. Rheumatol Int. (2010) 30:623–31. doi: 10.1007/s00296-009-1032-2
36. Li, B, Yang, S, and Akkus, O. A customized Raman system for point-of-care detection of arthropathic crystals in the synovial fluid. Analyst. (2014) 139:823–30. doi: 10.1039/c3an02062b
37. Li, B, Singer, NG, Yeni, YN, Haggins, DG, Barnboym, E, Oravec, D, et al. A point-of-care Raman spectroscopy–based device for the diagnosis of gout and Pseudogout: comparison with the clinical standard microscopy. Arthritis Rheumatol. (2016) 68:1751–7. doi: 10.1002/art.39638
38. Zhang, W, Doherty, M, Pascual, E, Barskova, V, Guerne, PA, Jansen, TL, et al. EULAR recommendations for calcium pyrophosphate deposition. Part II: Management Ann Rheum Dis. (2011) 70:571–5. doi: 10.1136/ard.2010.139360
39. Wu, Y, Chen, K, and Terkeltaub, R. Systematic review and quality analysis of emerging diagnostic measures for calcium pyrophosphate crystal deposition disease. RMD Open. (2016) 2:e000339. doi: 10.1136/rmdopen-2016-000339
40. Chollet-Janin, A, Finckh, A, Dudler, J, and Guerne, PA. Methotrexate as an alternative therapy for chronic calcium pyrophosphate deposition disease: an exploratory analysis. Arthritis Rheum. (2007) 56:688–92. doi: 10.1002/art.22389
41. Andres, M, Sivera, F, and Pascual, E. Methotrexate is an option for patients with refractory calcium pyrophosphate crystal arthritis. J Clin Rheumatol. (2012) 18:234–6. doi: 10.1097/RHU.0b013e3182611471
42. Finckh, A, Mc Carthy, GM, Madigan, A, Van Linthoudt, D, Weber, M, Neto, D, et al. Methotrexate in chronic-recurrent calcium pyrophosphate deposition disease: no significant effect in a randomized crossover trial. Arthritis Res Ther. (2014) 16:458. doi: 10.1186/s13075-014-0458-4
43. Williams, CJ, Qazi, U, Bernstein, M, Charniak, A, Gohr, C, Mitton-Fitzgerald, E, et al. Mutations in osteoprotegerin account for the CCAL1 locus in calcium pyrophosphate deposition disease. Osteoarthr Cartil. (2018) 26:797–806. doi: 10.1016/j.joca.2018.03.005
44. Danino, O, Svetitsky, S, Kenigsberg, S, Levin, A, Journo, S, Gold, A, et al. Inhibition of nucleotide pyrophosphatase/phosphodiesterase 1: implications for developing a calcium pyrophosphate deposition disease modifying drug. Rheumatology. (2018) 57:1472–80. doi: 10.1093/rheumatology/key092
45. Filippou, G, Scirè, CA, Damjanov, N, Adinolfi, A, Carrara, G, Picerno, V, et al. Definition and reliability assessment of elementary Ultrasonographic findings in calcium pyrophosphate deposition disease: a study by the OMERACT calcium pyrophosphate deposition disease ultrasound subtask force. J Rheumatol. (2017) 44:1744–9. doi: 10.3899/jrheum.161057
46. Filippou, G, Scirè, CA, Adinolfi, A, Damjanov, NS, Carrara, G, Bruyn, GAW, et al. Identification of calcium pyrophosphate deposition disease (CPPD) by ultrasound: reliability of the OMERACT definitions in an extended set of joints—an international multiobserver study by the OMERACT calcium pyrophosphate deposition disease ultrasound subtask force. Ann Rheum Dis. (2018) 77:annrheumdis-2017-212542–1199. doi: 10.1136/annrheumdis-2017-212542
47. Pascart, T, Norberciak, L, Legrand, J, Becce, F, and Budzik, JF. Dual-energy computed tomography in calcium pyrophosphate deposition: initial clinical experience. Osteoarthr Cartil. (2019) 27:1309–14. doi: 10.1016/j.joca.2019.05.007
48. Cipolletta, E, Di Matteo, A, Scanu, A, Isidori, M, Di Battista, J, Punzi, L, et al. Biologics in the treatment of calcium pyrophosphate deposition disease: a systematic literature review. Clin Exp Rheumatol. (2020) 79:447–8. doi: 10.1136/annrheumdis-2020-eular.1080
49. Dumusc, A, Pazar Maldonado, B, Benaim, C, Zufferey, P, Aubry-Rozier, B, and So, A. Anakinra compared to prednisone in the treatment of acute CPPD crystal arthritis: a randomized controlled double-blinded pilot study. Joint Bone Spine. (2021) 88:105088. doi: 10.1016/j.jbspin.2020.105088
50. Latourte, A, Ea, HK, Frazier, A, Blanchard, A, Lioté, F, Marotte, H, et al. Tocilizumab in symptomatic calcium pyrophosphate deposition disease: a pilot study. Ann Rheum Dis. (2020) 79:1126–8. doi: 10.1136/annrheumdis-2020-217188
51. Yang, S, Varghese, P, Stephenson, E, Tu, K, and Gronsbell, J. Machine learning approaches for electronic health records phenotyping: a methodical review. J Am Med Inform Assoc. (2023) 30:367–81. doi: 10.1093/jamia/ocac216
52. Tedeschi, SK, Cai, T, He, Z, Ahuja, Y, Hong, C, Yates, KA, et al. Classifying Pseudogout using machine learning approaches with electronic health record data. Arthritis Care Res. (2021) 73:442–8. doi: 10.1002/acr.24132
53. Tedeschi, SK, Becce, F, Pascart, T, Guermazi, A, Budzik, JF, Dalbeth, N, et al. Imaging features of calcium pyrophosphate deposition disease: consensus definitions from an international multidisciplinary working group. Arthritis Care Res. (2023) 75:825–34. doi: 10.1002/acr.24898
54. Abhishek, A, Tedeschi, SK, Pascart, T, Latourte, A, Dalbeth, N, Neogi, T, et al. The 2023 ACR/EULAR classification criteria for calcium pyrophosphate deposition disease. Arthritis Rheumatol. (2023) 75:1703–13. doi: 10.1002/art.42619
55. Pascart, T, Robinet, P, Ottaviani, S, Leroy, R, Segaud, N, Pacaud, A, et al. Evaluating the safety and short-term equivalence of colchicine versus prednisone in older patients with acute calcium pyrophosphate crystal arthritis (COLCHICORT): an open-label, multicentre, randomised trial. Lancet Rheumatol. (2023) 5:e523–31. doi: 10.1016/S2665-9913(23)00165-0
56. Sirotti, S, Terslev, L, Filippucci, E, Iagnocco, A, Moller, I, Naredo, E, et al. Development and validation of an OMERACT ultrasound scoring system for the extent of calcium pyrophosphate crystal deposition at the joint level and patient level. Lancet Rheumatol. (2023) 5:e474–82. doi: 10.1016/S2665-9913(23)00136-4
Keywords: chondrocalcinosis, Pseudogout, calcium pyrophosphate, crystal arthropathies, CPPD
Citation: Pineda C, Sandoval H, Pérez-Neri I, Soto-Fajardo C and Carranza-Enríquez F (2024) Calcium pyrophosphate deposition disease: historical overview and potential gaps. Front. Med. 11:1380135. doi: 10.3389/fmed.2024.1380135
Edited by:
Georgios Filippou, IRCCS Istituto Ortopedico Galeazzi, ItalyReviewed by:
Francesca Oliviero, University of Padua, ItalyCopyright © 2024 Pineda, Sandoval, Pérez-Neri, Soto-Fajardo and Carranza-Enríquez. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Fabián Carranza-Enríquez, ZmFiY2FlbjkwQGdtYWlsLmNvbQ==
†ORCID: Carlos Pineda, orcid.org/0000-0003-0544-7461
Hugo Sandoval, orcid.org/0000-0002-9622-1558
Iván Pérez-Neri, orcid.org/0000-0003-0190-7272
Carina Soto-Fajardo, orcid.org/0000-0001-6148-7789
Fabián Carranza-Enríquez, orcid.org/0000-0002-2515-8280
†These authors have contributed equally to this work and share first authorship