 Zhiyang Zhang1,2
Zhiyang Zhang1,2 Heling Zhao
Heling Zhao
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Med. , 21 May 2024
Sec. Intensive Care Medicine and Anesthesiology
Volume 11 - 2024 | https://doi.org/10.3389/fmed.2024.1379019
Background: This study aims to systematically assess the risk factors, the overall strength of association, and evidence quality related to sepsis-associated encephalopathy.
Methods: A systematic search was conducted in the Cochrane Library, PubMed, Web of Science, and Embase for cohort or case-control studies published up to August 2023 on risk factors associated with sepsis-related encephalopathy. The selected studies were screened, data were extracted, and the quality was evaluated using the Newcastle–Ottawa Scale. Meta-analysis was performed using RevMan 5.3 software. The certainty of the evidence was assessed using the GRADE criteria.
Results: A total of 13 studies involving 1,906 participants were included in the analysis. Among these studies, 12 were of high quality, and one was of moderate quality. Our meta-analysis identified six risk factors significantly associated with Serious Adverse Events (SAE). These included APACHE II, SOFA, age, tau protein, and IL-6, which were found to be risk factors with significant effects (standard mean difference SMD: 1.24–2.30), and albumin, which was a risk factor with moderate effects (SMD: −0.55). However, the certainty of evidence for the risk factors identified in this meta-analysis ranged from low to medium.
Conclusion: This systematic review and meta-analysis identified several risk factors with moderate to significant effects. APACHE II, SOFA, age, tau protein, IL-6, and albumin were associated with sepsis-related encephalopathy and were supported by medium- to high-quality evidence. These findings provide healthcare professionals with an evidence-based foundation for managing and treating hospitalized adult patients with sepsis-related encephalopathy.
Sepsis is a life-threatening disease caused by a dysregulation of the body’s response to infection (1). To distinguish sepsis-induced brain dysfunction from intracranial infection, sepsis-associated encephalopathy (SAE) was introduced and defined as diffuse brain dysfunction caused by a systemic immune-inflammatory response to a disease without clinical or laboratory evidence of direct brain infection (2). Sepsis-associated encephalopathy (SAE) and sepsis-associated delirium (SAD) are closely related neurological manifestations of sepsis. SAD, a subtype of SAE, explicitly denotes the acute and fluctuating cognitive impairments that occur in the context of sepsis. While all patients with SAD have SAE, not all SAE patients exhibit the characteristic confusion and reduced awareness seen in delirium. SAE usually presents as an acute deterioration in mental status, manifested by cognitive confusion, impaired consciousness, disorientation, agitation, rigidity, and coma (3). The pathophysiologic basis of SAE is very complex and involves multiple mechanisms that lead to brain dysfunction and injury (4). One of its main mechanisms is the release of pro-inflammatory cytokines, which leads to the breakdown of the blood-brain barrier (BBB), causing the influx of immune cells and inflammatory mediators into the brain (5).
SAE is considered the most common cause of encephalopathy in the intensive care unit (ICU) (6). Sepsis has a variety of complications, among which sepsis-associated encephalopathy (SAE) is one of the critical clinical manifestations, and severe SAE can occur in about 30 to 70% of patients with sepsis (7). In a landmark study of 50 non-sedated ICU sepsis patients, SAE was observed in 54% of patients (8). The incidence reported in a specific French multicenter cohort of ICUs was 53 percent (9). SAE prevalence is up to 68% in US MIMIC-IV and eICU databases (10). The diagnostic criteria for sepsis have evolved from Sepsis 1.0 to Sepsis 3.0 (11–13). There are no standardized criteria for the diagnosis of SAE, and the following diagnostic criteria are currently in use: (1) cognitive and neuropsychiatric disorders documented by healthcare professionals (doctors and nurses); (2) manifestations of Delirium (diagnosed by assessment methods such as CAM-ICU); and (3) Glasgow Coma Score (GCS) <15 (6, 14–16). Numerous studies have shown that SAEs are associated with increased short-term mortality, prolonged hospitalization, or over-expenditure of healthcare resources and have the potential to cause permanent neurological sequelae (17–19).
This systematic review aimed to identify key risk factors for sepsis-associated encephalopathy. Historically, there have been several problems with research reviews on SAE, such as confusing diagnoses of SAE, different study sample sizes, and different clinical populations. Identifying risk factors for SAE will help develop and implement prevention strategies for patients with sepsis.
It is a systematic review and meta-analysis assessing risk factors for sepsis-associated encephalopathy. Before the study started, a proposal was developed and registered in PROSPERO (CRD42023483721) (see Supplementary Table S1 for PROSPERO protocol). This study followed the Preferred Reporting Items for Systematic Reviews and Meta-Analysis guidelines (20).
We based search terms on Medical Subject Headings (MeSH) and other standard (controlled vocabulary) terms. A concept-based approach was used, including terms related to “Sepsis,” “Encephalopathy,” “Delirium,” “Risk Factors,” and others. Supplementary Table S2 details the entire search strategy. Two reviewers (ZZ and LJ) independently searched the Web of Science, Cochrane Library, Embase, and PubMed databases from inception to August 10, 2023. Our research team then searched the references of relevant studies to identify possible additional eligible studies. We used Endnote documentation software as a literature screening tool. Our research team repeated this process until we found no new relevant papers. Any discrepancies or differences were resolved through discussion or consultation with a third reviewer to reach a consensus.
We included studies involving human subjects aged 18 and above.
Each study must include at least five cases of sepsis-associated encephalopathy (SAE), ensuring a representative dataset and statistical robustness.
Included studies must utilize industry-recognized diagnostic or assessment tools for SAE to ensure consistency and accuracy in case diagnosis and evaluation (6, 14–16).
Only studies assessing risk factors for the onset of SAE were included. Specifically, we focused on cohort, case-control, and cross-sectional studies as these designs are suitable for identifying associations between risk factors and disease occurrence.
Studies must be peer-reviewed, published in scientific journals, and provide full-text articles for comprehensive quality assessment and data extraction.
We excluded studies involving intracranial infections as their pathology and treatment could significantly differ from those of standard SAE patients, potentially skewing the results.
We excluded case reports and case series involving four or fewer patients due to their insufficient data volume to support broad scientific conclusions. Similarly, literature reviews were excluded as they often rely on secondary data, which may not provide original data or detailed methods.
Only studies published in English were included to ensure accurate understanding and analysis of the data by our research team.
Data extraction was independently and systematically conducted by two reviewers (ZZ and LG) using a pre-specified data extraction form; any disputes were resolved through consensus or adjudicated by a third reviewer (HZ) until the disagreement was resolved. Data collection included study characteristics: first author, publication year, study design, total number of patients, age, gender, incidence of SAE, sepsis diagnostic criteria, and SAE diagnostic criteria. The baseline characteristics of the included studies are illustrated in Table 1.
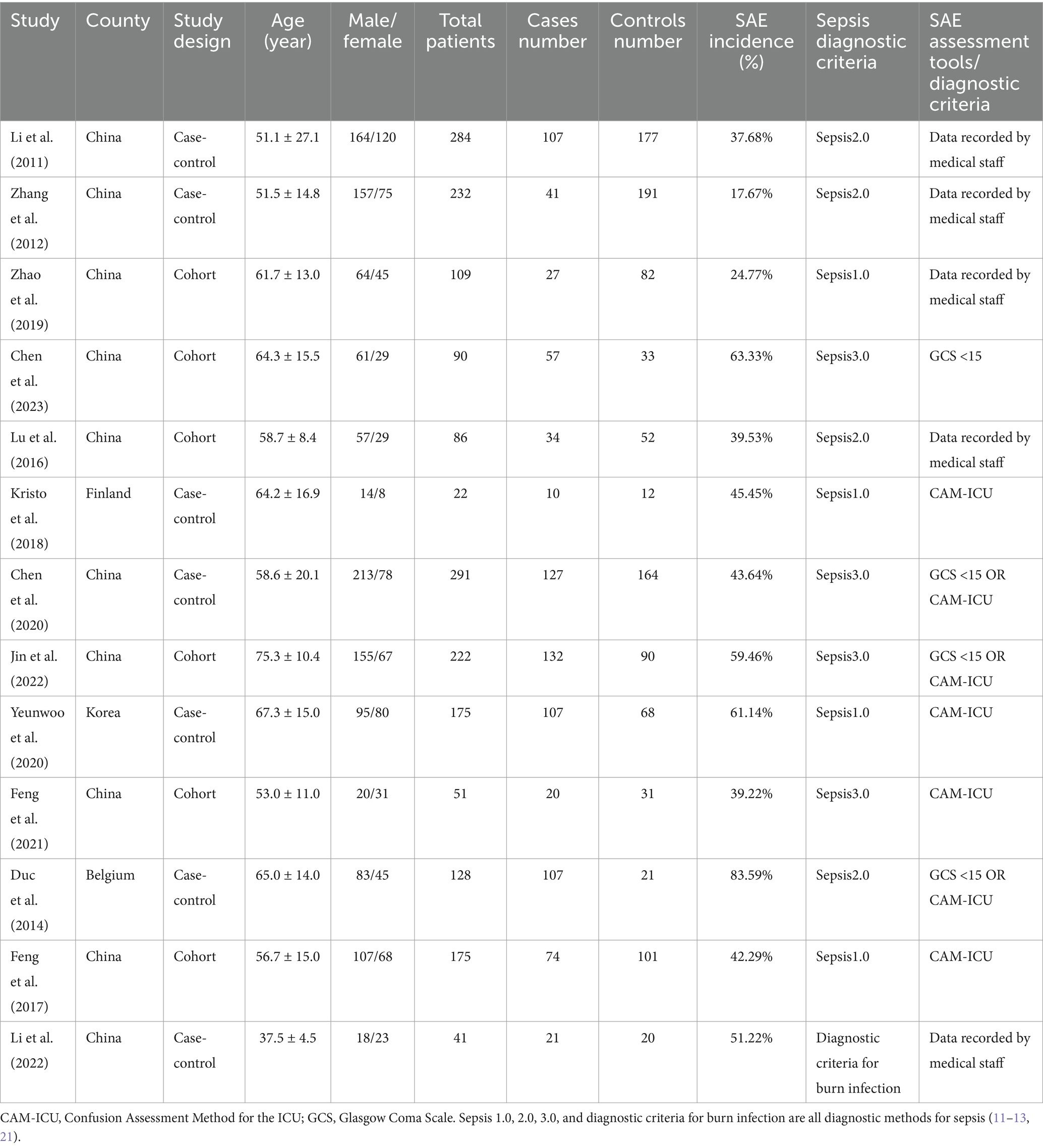
Table 1. Characteristics of the 13 studies.
When only 1 study provided data on the association between a potential risk factor and SAE, we reported the estimate extracted from the original article in the table (i.e., no meta-analysis was performed). When two or more studies provided data on the association between a potential risk factor and SAE, we calculated a meta-analyzed estimate of that possible association. When encountering studies that provided unadjusted and adjusted estimates, we preferred to use adjusted effect estimates because they represent effect estimates closer to the actual value (i.e., less biased). If forecasts from different overlapping cohorts were available, we used data from the report with the largest sample size to avoid duplicating data in the meta-analysis.
The diagnostic criteria for sepsis are constantly being updated. There are also no uniform diagnostic criteria for sepsis-associated encephalopathy. In each study we included, the diagnosis of both conditions varied. If it does not violate general principles, we respect the diagnostic criteria for sepsis and sepsis-associated encephalopathy used by researchers in each study and directly extract patient information from the data published in each study. The primary outcome of this study was the risk factors of sepsis-associated encephalopathy.
We will group the studies included based on the type of study design (case-control studies or cohort studies). Additionally, due to the lack of uniform diagnostic criteria for sepsis-associated encephalopathy, we will also group the studies based on whether the diagnosis in the included studies was made using objective scoring (GCS <15 or CAM-ICU) or based on the subjective evaluation of medical personnel. If heterogeneity analysis is required, we will determine the source of heterogeneity by employing a study-by-study exclusion approach for the included studies.
Two independent authors assessed the included studies’ methodological strength and risk of bias using the Newcastle–Ottawa Scale (NOS) (22). We used this assessment tool to evaluate the design quality of nonrandomized case-control and cohort studies. Scores were assigned based on selection criteria, comparability, and outcome (cohort studies) or exposure (case-control studies). The maximum score of 9 reflects the highest quality.
We used the Grades of Recommendations, Assessment, Development, and Evaluation (GRADE) evidence rating system to assess the credibility of the available evidence for the relevant factors associated with this meta-analysis (23, 24). We initially regarded observational studies as being of poor quality. Depending on the GRADE criteria, the level of credibility may be reduced (with five domains, including the risk of bias, inconsistency, circumstantial evidence, uncertainty, or publication bias) or increased (with three fields, including larger effect sizes, dose-response relationships, or confounders). We ultimately categorized the credibility of the evidence as high, moderate, low, or very low.
We used Review Manager (version 5.3; Nordic Cochrane Centre, The Cochrane Collaboration, Copenhagen, Denmark) (25) to perform meta-analysis. Continuous variables were pooled using standard mean difference (SMD), and We calculated a 95% confidence interval (CI). In contrast, binary variables were pooled using odds ratio (OR), and a 95% confidence interval (CI) was calculated. A fixed effects model was used when statistical heterogeneity was low (I2 ≤ 50%). When statistical heterogeneity was high (I2 > 50%), meta-analysis was performed using a random-effects model, and sensitivity and subgroup analyses were performed to investigate potential sources of heterogeneity (26). p < 0.05 was considered statistically significant.
A flow diagram for study selection is shown in Figure 1. Through database searching from inception to August 10, 2023, the date of our final search, we identified 2,041 original literature records. After the removal of duplicates, 1,718 records remained. Of these, 1,645 were excluded after screening titles and abstracts as they met our exclusion criteria. Excluding one article that could not be retrieved, we assessed the full texts of the remaining 72 articles. Ultimately, a total of 13 studies met the eligibility criteria for a full-text review (27–39).
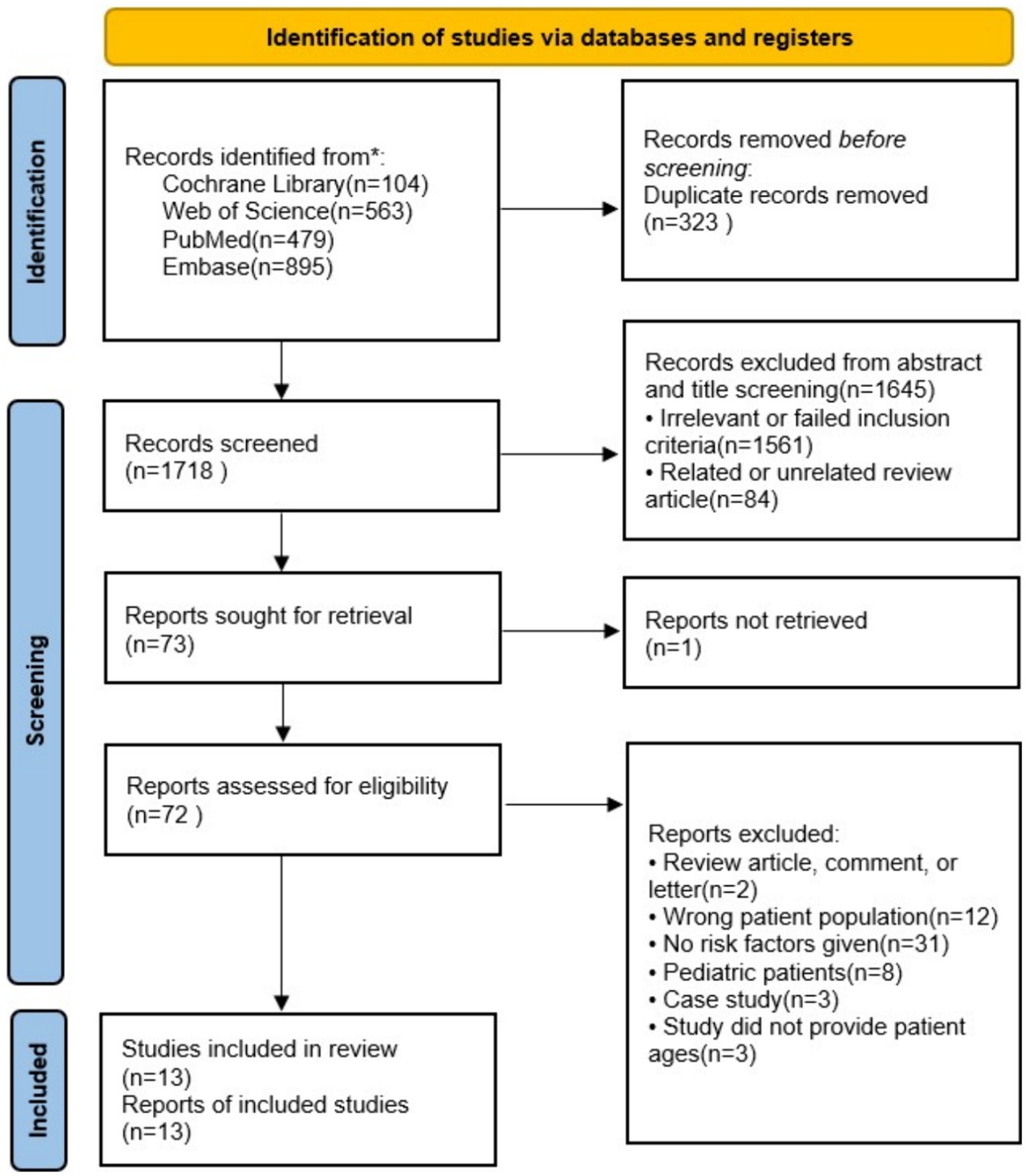
Figure 1. Flow diagram of the literature and selection in the meta-analysis.
Of the 13 studies included, there were six cohort studies and seven case-control studies. All these studies were published in English. The total sample size of these studies was 1906, with a cumulative case group of 864 and a control group of 1,042. The prevalence of SAE ranged from 17.67 to 83.59%. The studies were published between 2011 and 2023. The included studies were conducted in multiple countries, including China (n = 10), South Korea (n = 1), Finland (n = 1), and Belgium (n = 1). Thirteen studies were conducted in single-center settings. One study exclusively utilized the Glasgow Coma Scale (GCS) criteria for assessing SAE. Four studies solely employed the Confusion Assessment Method for the Intensive Care Unit (CAM-ICU) criteria for evaluating SAE. Three studies incorporated both GCS and CAM-ICU criteria for the assessment of SAE. Additionally, five studies assessed SAE through clinical records maintained by healthcare professionals (more details are seen in Table 1).
According to the NOS scores, 12 were high-quality studies, and one was of moderate quality (Supplementary Table S3). When performing multivariate analyses, explanations of the factors that accounted for most of the lost points were made more evident.
In our study, observational cohort studies were initially considered low quality. However, there was no high-quality evidence for any of the risk factors regarding deterministic assessment. Only APACHE II, SOFA, age, dependent activities, high care needs, low level of consciousness, and ALT showed moderate-quality evidence (Table 2). For all other risk factors, the certainty of evidence was categorized as low. The reduced quality of evidence for some risk factors was attributed to variations in study results and imprecision.
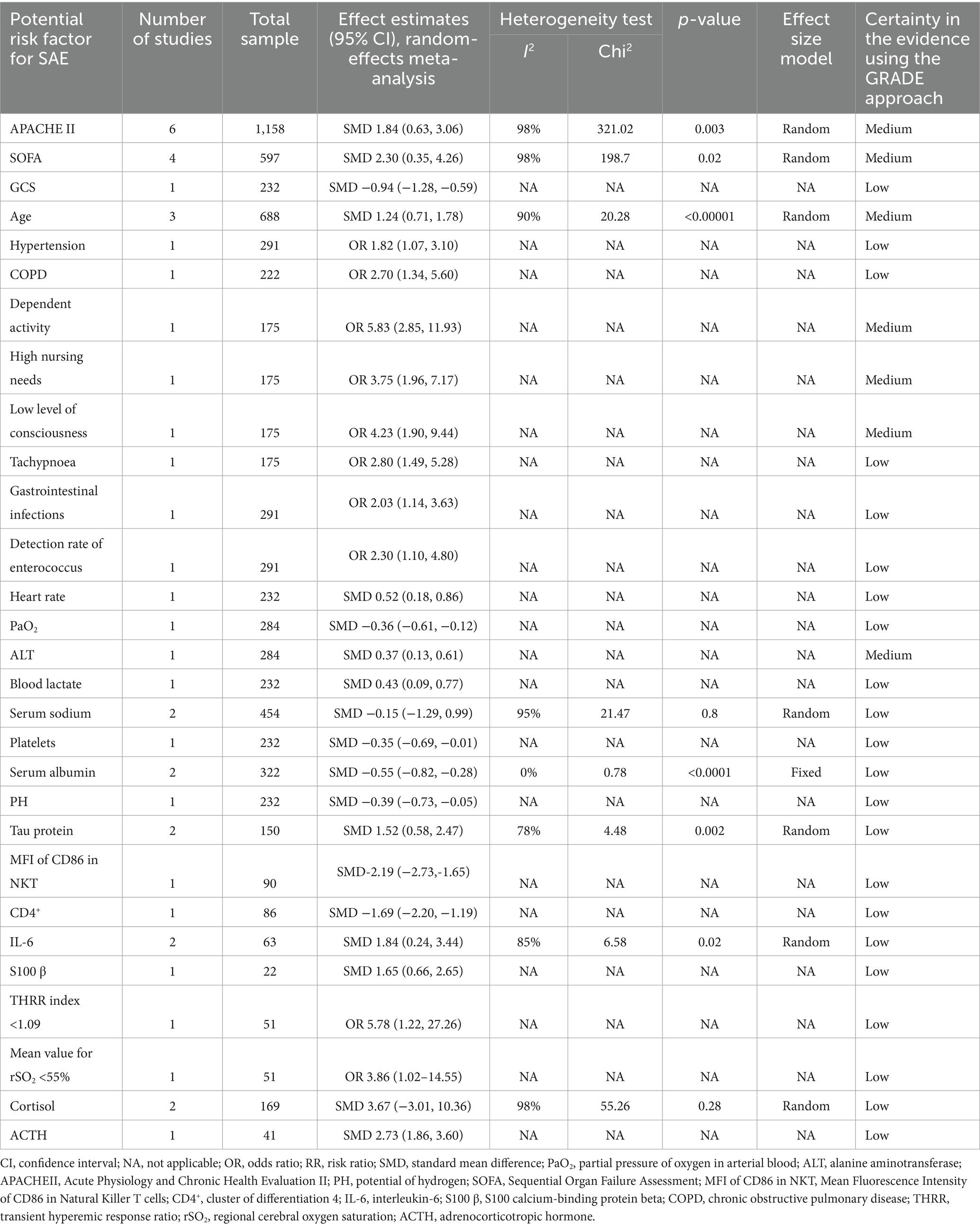
Table 2. Potential risk factors for SAE and its effect estimates.
We conducted a meta-analysis of data from 6 studies (27, 28, 30, 31, 33, 38) examining the relationship between APACHE II and SAE, with 440 cases in the SAE group and 718 cases in the non-SAE group. The results showed a statistically positive effect between the two {[SMD = 1.84, 95% CI (0.63, 3.06)], p = 0.003} (Table 2 and Figure 2). However, there was a high degree of heterogeneity between studies (I2 = 98%, p < 0.00001), and the source of the heterogeneity could not be determined despite a study-by-study exclusion maneuver. Subgroup analyses were performed based on differences in study design and diagnostic criteria for encephalopathy between studies (Supplementary Figures S1, S2).
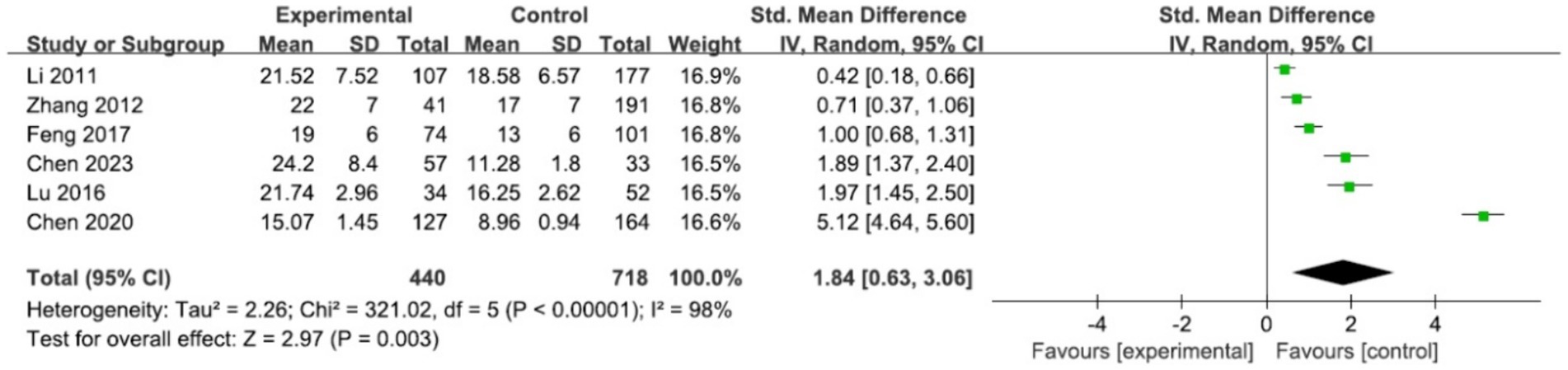
Figure 2. Forest plot of the studies in APACHEII.
The effect of SOFA on SAE was examined in four studies (29, 32, 33, 38). There were 238 cases in the SAE group and 359 cases in the non-SAE group. The results demonstrated a statistically significant positive association between the two variables, as evidenced by a standard mean difference (SMD) of 2.3 with a 95% confidence interval (CI) ranging from 0.35 to 4.26 (p = 0.02) (Table 2 and Figure 3). Notably, the studies had substantial heterogeneity (I2 = 98%, p < 0.00001). Despite conducting a thorough exclusion analysis for each study, the root cause of this heterogeneity remained elusive. Consequently, subgroup analyses were undertaken to explore the potential effects of variations in study designs across the studies (Supplementary Figure S3).
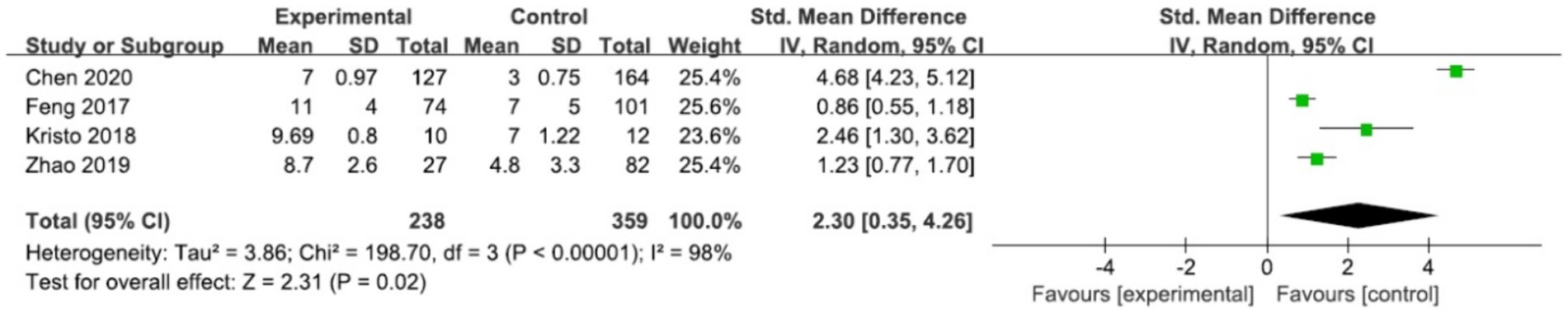
Figure 3. Forest plot of the studies in SOFA.
In three studies, the impact of age on sepsis-associated encephalopathy (SAE) was examined, and a meta-analysis was conducted (33, 34, 38). The SAE group comprised 368 cases, while the non-SAE group included 322 cases. The results showed a statistically positive effect between the two {[SMD = 1.24, 95% CI (0.71, 1.78)], p < 0.00001} (Table 2 and Figure 4). However, there was a high degree of between-study heterogeneity (I2 = 90%, p < 0.0001), and despite a study-by-study exclusion maneuver, the source of the heterogeneity could not be determined. Subgroup analyses were then performed based on differences in study design between studies (Supplementary Figure S4).

Figure 4. Forest plot of the studies in age.
We conducted a meta-analysis of data from 2 studies (28, 30) examining the relationship between albumin and SAE, with 98 cases in the SAE group and 224 cases in the non-SAE group. The results showed a statistically negative effect between the two {[SMD = −0.55, 95% CI (−0.82, −0.28)], p < 0.0001} and low heterogeneity in the meta-analysis. In our meta-analysis (28, 34), sodium was not found to be a significant risk factor in the occurrence of SAE (p = 0.8) (Table 2 and Supplementary Figures S5, S6).
The effect of tau protein on SAE was examined in 2 studies (29, 39). The results showed a statistically positive effect between the two {[SMD = 1.52, 95% CI (0.58, 2.47)], p = 0.002}, with high heterogeneity in the meta-analysis (I2 = 78%, p = 0.03). The effect of IL-6 on SAE was examined in 2 studies (32, 39). The results showed a statistically positive effect between the two {[SMD = 1.84, 95% CI (0.24, 3.44)], p = 0.02}, with high heterogeneity in the meta-analysis (I2 = 85%, p = 0.01). In our meta-analysis (37, 39), cortisol was not found to be a significant risk factor in SAE (p = 0.28) (Table 2 and Supplementary Figures S7–S9).
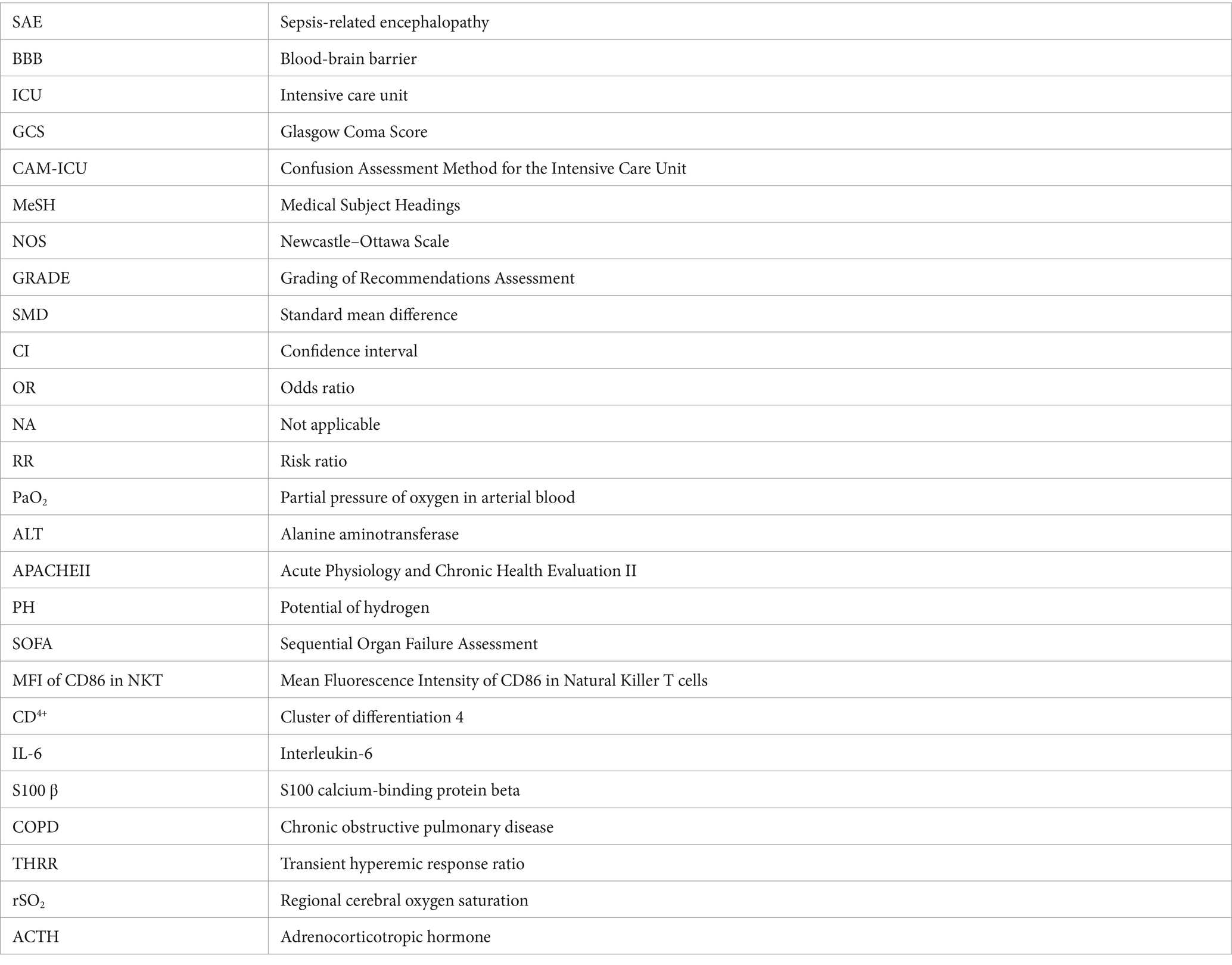
In our study, multiple regression analysis identified 21 potential risk factors for developing encephalopathy in patients with sepsis. These factors include GCS, hypertension, COPD, dependent activity, high nursing needs, low level of consciousness, tachypnoea, gastrointestinal infections, detection rate of enterococcus, heart rate, PaO2, ALT, blood lactate, platelets, pH, MFI of CD86 in NKT cells, CD4+, S100 β, THRR index <1.09, mean value for rSO2 <55%, and ACTH. However, as these risk factors were only reported in a single study and insufficient data from multiple studies for a meta-analysis, they were omitted in our meta-analysis (more details seen in Table 2).
Six risk factors significantly associated with SAE were identified in this meta-analysis of 13 studies involving 1,906 patients hospitalized with sepsis. Among these, APACHE II, SOFA, age, tau protein, and IL-6 were found to be risk factors with significant effects (SMD: 1.24–2.30), and albumin was a risk factor with moderate effects (SMD: −0.55). However, for the risk factors identified in this meta-analysis, the certainty of evidence was low to moderate.
According to our results, the incidence of APACHE II and SOFA in SAE was statistically a risk factor for more significant effects, but considerable heterogeneity was seen between studies. We could not determine the heterogeneity source even after sensitivity analyses.
We performed subgroup analyses based on some subgroups that may affect heterogeneity, such as differences in study design and diagnostic criteria for encephalopathy. Despite these subgroups, there was still more significant heterogeneity in the within-group analyses of APACHE II and SOFA, suggesting that the significant inconsistency in the study results was not caused by differences in study design and diagnostic criteria for encephalopathy and that further exploration of the sources of heterogeneity is needed. Both APACHE II and SOFA scores are important indicators of the severity of a patient’s condition and have been widely used to evaluate critically ill patients (8, 40). Encephalopathy is seen as an indicator of a poor prognosis for patients suffering from sepsis; the severity of encephalopathy is closely related to the severity of the systemic disease and requires prompt and aggressive treatment. According to our study, both APACHE II and SOFA scores were risk factors for a more significant effect of SAE, with advantages in assessing the severity and prognosis of encephalopathy, consistent with previous reports (41). Compared to non-SAE patients, SAE patients are more severely ill, as evidenced by higher costs, prolonged hospitalization, and higher duration of mechanical ventilation (17–19). Also, patients with SAE had a higher hospital mortality rate, suggesting that once SAE occurs in septic patients, the mortality rate is significantly higher. In the studies included in our meta-analysis, the incidence of SAE in septic patients may be as high as 83.59% (37). The high incidence of SAE may explain why sepsis is still fatal today. It is important to note that GCS scores <15 were used to diagnose patients with SAE; however, GCS scores are a component of SOFA and APACHE II scores. Patients with higher SOFA and APACHE II scores were likelier to have SAE, which may have biased the conclusions (34).
In our study, age incidence in SAE was also statistically a risk factor for more significant effects, but considerable heterogeneity was seen between studies. Sensitivity analyses could not identify the source of the heterogeneity. Because only three studies were included, we did not perform subgroup analyses, and the small sample size made the results we obtained less reliable. There was a significant publication bias and other circumstances. Elderly patients are at higher risk of developing sepsis, and critically ill patients with underlying disease usually have a more rapid progression and a poorer prognosis. Especially if the underlying illness is hypertension COPD, these patients may be more likely to develop central nervous system complications (9, 42–44). In addition, hospitalization of elderly patients is often associated with an increase in the need for nursing care due to dependence on daily activities and poor self-care ability, which further aggravates their condition (45, 46). This finding is consistent with some of the SAE-associated risk factors identified in our META analysis, including Age, COPD, and others.
Laboratory parameters such as tau protein, IL-6, and albumin in our study, although risk factors for predicting a medium to significant effect for the occurrence of SAEs, were included in a limited number of studies with small sample sizes and were only supported by low-quality evidence. In our meta-analysis, we applied the GRADE system to ensure the scientific validity of our findings. Despite many studies initially rated as low quality, careful reassessment allowed for upgrades based on study design and execution. We recognize heterogeneity due to geographical and ethnic variations, which introduces some uncertainty in interpretation. Also, potential biases and unmeasured confounders in primary studies could affect the generalizability of our results. Our findings, while insightful, should be applied cautiously in clinical practice, integrating high-quality evidence, clinical experience, and patient values. They provide a basis for guidelines but require adaptation to local contexts. Future research should aim to enhance study design quality, increase sample sizes, and broaden demographic coverage to improve evidence quality and extend its applicability.
Further inflammation is needed in the future through more extensive studies supported by higher levels of evidence. However, IL-6 and albumin are conveniently available and cost-effective biomarkers during hospitalization because they can be calculated from standard peripheral blood tests without additional effort or expense. Monitoring changes in IL-6 and albumin levels can be a useful clinical tool for assessing the risk of SAE and developing appropriate medical interventions. This meta-analysis needed to have identified specific thresholds for predicting SAE due to the limited sample size and potential heterogeneity of baseline values in different studies. Future prospective studies are required to establish validated entries for predicting SAE. We confidently use IL-6 and Albumin as clinical tools for predicting SAE risk.
The main strength of this study is that it is the first meta-analysis of risk factors for SAE, where multiple factors affecting SAE were analyzed separately. However, like all studies, this study has some limitations. First, the diagnostic criteria for sepsis and sepsis-associated encephalopathy differed between studies. The diagnostic criteria for sepsis 1.0 have high sensitivity but low specificity, which may lead to overdiagnosis while missing some immunosuppressed patients. Sepsis 2.0 is a transitional criterion. However, the latest definition of sepsis 3.0 remains controversial. When a patient’s SOFA score changes by ≥2 points, the patient’s condition is exacerbated, caused by an infection that may adversely affect the early recognition and treatment of sepsis and lead to a delayed diagnosis of the disease. In addition, non-infectious conditions in critically ill patients may also lead to organ damage that can achieve a SOFA score of ≥2, leading to overdiagnosis. The diagnostic criteria for burn infection are expressly limited to burn patients (21). All four diagnostic criteria for sepsis are deficient. Among the currently used diagnostic criteria for SAE, GCS <15 and CAM-ICU are relatively objective diagnostic methods. At the same time, data recorded by medical staff is somewhat subjective; all three diagnostic procedures are based on consistent clinical symptoms of SAE. Second, only English-language databases were searched, possibly excluding relevant studies published in other languages. Third, only a few studies were included for certain factors such as tau protein, IL-6, and albumin, resulting in small sample sizes for these studies. Fourth, the exclusion of minors under the age of 18 limits the generalizability of the results. In addition, most of the studies were conducted in Asia and Europe, limiting the applicability of generalizing the results to other parts of the world.
Therefore, future research needs to address these limitations and provide a more comprehensive investigation of the risk factors associated with SAE. Efforts should include studies from different geographic regions and populations, consider a broader range of languages, and use standardized assessment methods. By overcoming these limitations, we can further advance our understanding of SAE and provide more substantial evidence for clinical practice.
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
ZZ: Writing – original draft. LG: Writing – review & editing. LJ: Writing – review & editing. HD: Writing – review & editing. LS: Writing – review & editing. HZ: Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2024.1379019/full#supplementary-material
1. Slooter, AJC, Otte, WM, Devlin, JW, Arora, RC, Bleck, TP, Claassen, J, et al. Updated nomenclature of delirium and acute encephalopathy: statement of ten societies. Intensive Care Med. (2020) 46:1020–2. doi: 10.1007/s00134-019-05907-4
2. Wilson, JX, and Young, GB. Progress in clinical neurosciences: sepsis-associated encephalopathy: evolving concepts. Can J Neurol Sci. (2003) 30:98–105. doi: 10.1017/S031716710005335X
3. Iacobone, E, Bailly-Salin, J, Polito, A, Friedman, D, Stevens, RD, and Sharshar, T. Sepsis-associated encephalopathy and its differential diagnosis. Crit Care Med. (2009) 37:S331–6. doi: 10.1097/CCM.0b013e3181b6ed58
4. Heming, N, Mazeraud, A, Verdonk, F, Bozza, FA, Chrétien, F, and Sharshar, T. Neuroanatomy of sepsis-associated encephalopathy. Crit Care. (2017) 21:65. doi: 10.1186/s13054-017-1643-z
5. Sharshar, T, Annane, D, de la Grandmaison, GL, Brouland, JP, Hopkinson, NS, and Françoise, G. The neuropathology of septic shock. Brain Pathol. (2004) 14:21–33. doi: 10.1111/j.1750-3639.2004.tb00494.x
6. Bleck, TP, Smith, MC, Pierre-Louis, SJ, Jares, JJ, Murray, J, and Hansen, CA. Neurologic complications of critical medical illnesses. Crit Care Med. (1993) 21:98–103. doi: 10.1097/00003246-199301000-00019
7. Czempik, PF, Pluta, MP, and Krzych, ŁJ. Sepsis-associated brain dysfunction: a review of current literature. Int J Environ Res Public Health. (2020) 17:5852. doi: 10.3390/ijerph17165852
8. Eidelman, LA, Putterman, D, Putterman, C, and Sprung, CL. The spectrum of septic encephalopathy. Definitions, etiologies, and mortalities. JAMA. (1996) 275:470–3. doi: 10.1001/jama.1996.03530300054040
9. Sonneville, R, de Montmollin, E, Poujade, J, Garrouste-Orgeas, M, Souweine, B, Darmon, M, et al. Potentially modifiable factors contributing to sepsis-associated encephalopathy. Intensive Care Med. (2017) 43:1075–84. doi: 10.1007/s00134-017-4807-z
10. Lu, X, Qin, M, Walline, JH, Gao, Y, Yu, S, Ge, Z, et al. Clinical phenotypes of SEPSIS-associated encephalopathy: a retrospective cohort study. Shock. (2023) 59:583–90. doi: 10.1097/SHK.0000000000002092
11. Dellinger, RP, Levy, MM, Rhodes, A, Annane, D, Gerlach, H, Opal, SM, et al. Surviving sepsis campaign: international guidelines for management of severe sepsis and septic shock: 2012. Crit Care Med. (2013) 41:580–637. doi: 10.1097/CCM.0b013e31827e83af
12. Dellinger, RP, Levy, MM, Carlet, JM, Bion, J, Parker, MM, Jaeschke, R, et al. Surviving sepsis campaign: international guidelines for management of severe sepsis and septic shock: 2008. Intensive Care Med. (2008) 34:17–60. doi: 10.1007/s00134-007-0934-2
13. Rhodes, A, Evans, LE, Alhazzani, W, Levy, MM, Antonelli, M, Ferrer, R, et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock: 2016. Intensive Care Med. (2017) 43:304–77. doi: 10.1007/s00134-017-4683-6
14. Young, GB, Bolton, CF, Austin, TW, Archibald, YM, Gonder, J, and Wells, GA. The encephalopathy associated with septic illness. Clin Invest Med. (1990) 13:297–304.
15. Eggers, V, Schilling, A, Kox, WJ, and Spies, C. Septic encephalopathy. Diagnosis und therapy. Anaesthesist. (2003) 52:294–303. doi: 10.1007/s00101-003-0496-9
16. Chelazzi, C, Consales, G, and De Gaudio, A. Sepsis associated encephalopathy. Curr Anaesth Crit Care. (2008) 19:15–21. doi: 10.1016/j.cacc.2007.07.009
17. Ren, C, Yao, RQ, Zhang, H, Feng, YW, and Yao, YM. Sepsis-associated encephalopathy: a vicious cycle of immunosuppression. J Neuroinflammation. (2020) 17:14. doi: 10.1186/s12974-020-1701-3
18. Kikuchi, DS, Campos, ACP, Qu, H, Forrester, SJ, Pagano, RL, Lassègue, B, et al. Poldip2 mediates blood-brain barrier disruption in a model of sepsis-associated encephalopathy. J Neuroinflammation. (2019) 16:241. doi: 10.1186/s12974-019-1575-4
19. Sonneville, R, Benghanem, S, Jeantin, L, de Montmollin, E, Doman, M, Gaudemer, A, et al. The spectrum of sepsis-associated encephalopathy: a clinical perspective. Crit Care. (2023) 27:386. doi: 10.1186/s13054-023-04655-8
20. Moher, D, Liberati, A, Tetzlaff, J, and Altman, DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. (2009) 6:e1000097. doi: 10.1371/journal.pmed.1000097
21. Peng, YZ, Yuan, ZQ, Li, XL, Luo, GX, and Wu, J. Guidelines for the diagnosis and treatment of burn infection (2012 edition). Chin J Burns. (2012) 28:401–3. doi: 10.3760/cma.j.issn.1009-2587
22. Wells, GA, Wells, G, Shea, B, Shea, B, O’Connell, D, Peterson, J, et al. (Eds). The Newcastle-Ottawa scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. (2014). Available at: https://www.ohri.ca/programs/clinical_epidemiology/oxford.asp
23. Balshem, H, Helfand, M, Schünemann, HJ, Oxman, AD, Kunz, R, Brozek, J, et al. GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol. (2011) 64:401–6. doi: 10.1016/j.jclinepi.2010.07.015
24. Foroutan, F, Guyatt, G, Zuk, V, Vandvik, PO, Alba, AC, Mustafa, R, et al. GRADE guidelines 28: use of GRADE for the assessment of evidence about prognostic factors: rating certainty in identification of groups of patients with different absolute risks. J Clin Epidemiol. (2020) 121:62–70. doi: 10.1016/j.jclinepi.2019.12.023
25. DerSimonian, R, and Laird, N. Meta-analysis in clinical trials revisited. Contemp Clin Trials. (2015) 45:139–45. doi: 10.1016/j.cct.2015.09.002
26. Higgins, JP, Thompson, SG, Deeks, JJ, and Altman, DG. Measuring inconsistency in meta-analyses. BMJ. (2003) 327:557–60. doi: 10.1136/bmj.327.7414.557
27. Li, J, Li, A, Weng, Y, Zhang, S, and Duan, M. Risk factors for sepsis-associated encephalopathy. Neural Regen Res. (2011) 6:309–12. doi: 10.3969/j.issn.1673-5374
28. Zhang, LN, Wang, XT, Ai, YH, Guo, QL, Huang, L, Liu, ZY, et al. Epidemiological features and risk factors of sepsis-associated encephalopathy in intensive care unit patients: 2008–2011. Chin Med J. (2012) 125:828–31. doi: 10.3760/cma.j.issn.0366-6999.2012.05.018
29. Zhao, T, Xia, Y, Wang, D, and Pang, L. Association between elevated serum tau protein level and sepsis-associated encephalopathy in patients with severe sepsis. Can J Infect Dis Med Microbiol. (2019) 2019:1–6. doi: 10.1155/2019/1876174
30. Chen, SL, Liu, XY, Huang, JH, Xian, LH, Li, XS, Wang, KR, et al. The expression of CD86 in CD3+ CD56+ NKT cells is associated with the occurrence and prognosis of sepsis-associated encephalopathy in sepsis patients: a prospective observational cohort study. Immunol Res. (2023) 71:929–40. doi: 10.1007/s12026-023-09405-0
31. Lu, CX, Qiu, T, Tong, HS, Liu, ZF, Su, L, and Cheng, B. Peripheral T-lymphocyte and natural killer cell population imbalance is associated with septic encephalopathy in patients with severe sepsis. Exp Ther Med. (2016) 11:1077–84. doi: 10.3892/etm.2016.3000
32. Erikson, K, Ala-Kokko, TI, Koskenkari, J, Liisanantti, JH, Kamakura, R, Herzig, KH, et al. Elevated serum S-100β in patients with septic shock is associated with delirium. Acta Anaesthesiol Scand. (2019) 63:69–73. doi: 10.1111/aas.13228
33. Chen, J, Shi, X, Diao, M, Jin, G, Zhu, Y, Hu, W, et al. A retrospective study of sepsis-associated encephalopathy: epidemiology, clinical features and adverse outcomes. BMC Emerg Med. (2020) 20:77. doi: 10.1186/s12873-020-00374-3
34. Jin, G, Wang, S, Chen, J, Hu, W, Zhu, Y, and Xi, S. Identification of sepsis-associated encephalopathy risk factors in elderly patients: a retrospective observational cohort study. Turk J Med Sci. (2022) 52:1513–22. doi: 10.55730/1300-0144.5491
35. Kim, Y, Jin, Y, Jin, T, and Lee, SM. Risk factors and outcomes of sepsis-associated delirium in intensive care unit patients: a secondary data analysis. Intensive Crit Care Nurs. (2020) 59:102844. doi: 10.1016/j.iccn.2020.102844
36. Feng, Q, Ai, M, Huang, L, Peng, Q, Ai, Y, and Zhang, L. Relationship between cerebral hemodynamics, tissue oxygen saturation, and delirium in patients with septic shock: a pilot observational cohort study. Front Med. (2021) 8:641104. doi: 10.3389/fmed.2021.641104
37. Nguyen, DN, Huyghens, L, Zhang, H, Schiettecatte, J, Smitz, J, and Vincent, JL. Cortisol is an associated-risk factor of brain dysfunction in patients with severe sepsis and septic shock. Biomed Res Int. (2014) 2014:712742:1–7. doi: 10.1155/2014/712742
38. Feng, Q, Ai, YH, Gong, H, Wu, L, Ai, ML, Deng, SY, et al. Characterization of sepsis and sepsis-associated encephalopathy. J Intensive Care Med. (2019) 34:938–45. doi: 10.1177/0885066617719750
39. Li, XL, Xie, JF, Ye, XY, Li, Y, Li, YG, Feng, K, et al. Value of cerebral hypoxic-ischemic injury markers in the early diagnosis of sepsis associated encephalopathy in burn patients with sepsis. Zhonghua Shao Shang Yu Chuang Mian Xiu Fu Za Zhi. (2022) 38:21–8. doi: 10.3760/cma.j.cn501120-20211006-00346
40. Sprung, CL, Peduzzi, PN, Shatney, CH, Schein, RM, Wilson, MF, Sheagren, JN, et al. Impact of encephalopathy on mortality in the sepsis syndrome. The Veterans Administration Systemic Sepsis Cooperative Study Group. Crit Care Med. (1990) 18:801–6. doi: 10.1097/00003246-199008000-00001
41. Taylor, SL, Morgan, DL, Denson, KD, Lane, MM, and Pennington, LR. A comparison of the Ranson, Glasgow, and APACHE II scoring systems to a multiple organ system score in predicting patient outcome in pancreatitis. Am J Surg. (2005) 189:219–22. doi: 10.1016/j.amjsurg.2004.11.010
42. Hajjar, I, Keown, M, and Frost, B. Antihypertensive agents for aging patients who are at risk for cognitive dysfunction. Curr Hypertens Rep. (2005) 7:466–73. doi: 10.1007/s11906-005-0043-y
43. Sonneville, R, Vanhorebeek, I, den Hertog, HM, Chrétien, F, Annane, D, Sharshar, T, et al. Critical illness-induced dysglycemia and the brain. Intensive Care Med. (2015) 41:192–202. doi: 10.1007/s00134-014-3577-0
44. Siew, ED, Fissell, WH, Tripp, CM, Blume, JD, Wilson, MD, Clark, AJ, et al. Acute kidney injury as a risk factor for delirium and coma during critical illness. Am J Respir Crit Care Med. (2017) 195:1597–607. doi: 10.1164/rccm.201603-0476OC
45. Pandharipande, PP, Girard, TD, Jackson, JC, Morandi, A, Thompson, JL, Pun, BT, et al. Long-term cognitive impairment after critical illness. N Engl J Med. (2013) 369:1306–16. doi: 10.1056/NEJMoa1301372
46. Brummel, NE, Jackson, JC, Pandharipande, PP, Thompson, JL, Shintani, AK, Dittus, RS, et al. Delirium in the ICU and subsequent long-term disability among survivors of mechanical ventilation. Crit Care Med. (2014) 42:369–77. doi: 10.1097/CCM.0b013e3182a645bd
Keywords: sepsis, encephalopathy, delirium, risk factors, meta-analysis
Citation: Zhang Z, Guo L, Jia L, Duo H, Shen L and Zhao H (2024) Factors contributing to sepsis-associated encephalopathy: a comprehensive systematic review and meta-analysis. Front. Med. 11:1379019. doi: 10.3389/fmed.2024.1379019
Edited by:
Dirk M. Hermann, University of Duisburg-Essen, GermanyReviewed by:
Andrea Glotta, Ospedale Regionale di Lugano, SwitzerlandCopyright © 2024 Zhang, Guo, Jia, Duo, Shen and Zhao. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Heling Zhao, aGx6aGJnaEAxNjMuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.