 Carlos Delfino1
Carlos Delfino1 M. Cecilia Poli2,3,4
M. Cecilia Poli2,3,4 Cecilia Vial2,5
Cecilia Vial2,5 Pablo A. Vial2,5Gonzalo Martínez6Amy Riviotta1Catalina Arbat2Nicole Mac-Guire2
Pablo A. Vial2,5Gonzalo Martínez6Amy Riviotta1Catalina Arbat2Nicole Mac-Guire2 Josefina Hoppe2Cristóbal Carvajal7
Josefina Hoppe2Cristóbal Carvajal7 Paula Muñoz Venturelli1,8,9*
Paula Muñoz Venturelli1,8,9*- 1Centro de Estudios Clínicos, Instituto de Ciencias e Innovación en Medicina (ICIM), Facultad de Medicina Clínica Alemana Universidad del Desarrollo, Santiago, Chile
- 2Facultad de Medicina Clínica Alemana de Santiago, Universidad del Desarrollo, Santiago, Chile
- 3Programa de Inmunogenética e Inmunología Traslacional, Instituto de Ciencias e Innovación en Medicina, Facultad de Medicina, Santiago, Chile
- 4Unidad de Inmunología y Reumatología, Hospital Roberto del Río, Santiago, Chile
- 5Programa de Hantavirus y Zoonosis, Instituto de Ciencias e Innovación en Medicina, Facultad de Medicina, Santiago, Chile
- 6Departamento de Enfermedades Cardiovasculares, Pontificia Universidad Católica de Chile, Santiago, Chile
- 7Centro de Informática Biomédica, Instituto de Ciencias e Innovación en Medicina (ICIM), Facultad de Medicina Clínica Alemana—Universidad del Desarrollo, Santiago, Chile
- 8Servicio de Neurología, Departamento de Neurología y Psiquiatría, Clínica Alemana de Santiago, Facultad de Medicina Clínica Alemana—Universidad del Desarrollo, Santiago, Chile
- 9The George Institute for Global Health, Faculty of Medicine, University of New South Wales, Sydney, NSW, Australia
Background and aim: Post-COVID-19 condition (PCC) encompasses long-lasting symptoms in individuals with COVID-19 and is estimated to affect between 31–67% of patients, with women being more commonly affected. No definitive biomarkers have emerged in the acute stage that can help predict the onset of PCC, therefore we aimed at describing sex-disaggregated data of PCC patients from a local cohort and explore potential acute predictors of PCC and neurologic PCC.
Methods: A local cohort of consecutive patients admitted with COVID-19 diagnosis between June 2020 and July 2021 were registered, and clinical and laboratory data were recorded. Only those <65 years, discharged alive and followed up at 6 and 12 months after admission were considered in these analyses. Multivariable logistic regression analysis was performed to explore variables associated with PCC (STATA v 18.0).
Results: From 130 patients in the cohort, 104 were contacted: 30% were women, median age of 42 years. At 6 months, 71 (68%) reported PCC symptoms. Women exhibited a higher prevalence of any PCC symptom (87 vs. 60%, p = 0.007), lower ferritin (p = 0.001) and procalcitonin (p = 0.021) and higher TNF levels (p = 0.042) in the acute phase compared to men. Being women was independently associated to 7.60 (95% CI 1.27–45.18, p = 0.026) higher risk for PCC. Moreover, women had lower return to normal activities 6 and 12 months.
Conclusion: Our findings highlight the lasting impact of COVID-19, particularly in young women, emphasising the need for tailored post-COVID care. The lower ferritin levels in women are an intriguing observation, warranting further research. The study argues for comprehensive strategies that address sex-specific challenges in recovery from COVID-19.
Background
Since the declaration of the COVID-19 pandemic in March 2020, approximately 760 million individuals worldwide have been diagnosed with SARS-CoV-2 infection (1). Beyond the acute phase of the illness, some people experience ongoing symptoms, known as post-COVID-19 condition (PCC). PCC includes individuals with confirmed or probable COVID-19 who continue to have symptoms or develop new ones at least 3 months after the initial infection, lasting for at least 2 months (2). Studies suggest that a staggering 31 to 67% of patients infected with SARS-COV-2 endure these post-acute sequelae (3).
Among the published findings related to PCC, a stark disparity emerges, with women facing a significantly higher risk compared to men (63.2% vs. 36.8%) (4). It has also been proposed that the severity of the acute infection and BMI (5) may increase the risk of developing PCC, although this remains a topic of ongoing debate (6). Both systemic inflammation and neuroinflammation, as well as microvascular injury and thrombosis are critical to COVID-19 pathobiology (7, 8). Among these, the NLRP3 inflammasome plays a prominent role, triggering the release of highly inflammatory cytokines (e.g., IL-1β and IL-18) (9). Activation by SARS-CoV-2 of this complex results in the downstream production of interleukin-6 and C-reactive protein (CRP) (10). Additionally, the central nervous system can initiate an immune response through inflammasome activation (11). Moreover, a common genetic polymorphism (NLRP3 rs10754555 variant) has been reported to enhance systemic inflammation and inflammasome activity in patients with atherosclerosis, with those with the C/G and G/G genotype being at higher risk (12). This polymorphism may potentially influence the severity of COVID-19 and the neurological symptoms experienced by affected individuals. As of now, no biomarkers have emerged during acute COVID-19 that can predict the occurrence of PCC (13).
Because of the described sex predisposition to PCC, in this study, we sought to describe clinical and immunological profiles of acute COVID-19 patients, focusing on sex-specific analysis and potential predictors of PCC including comprehensive acute inflammatory and immunological response.
Methods
Study design, patients, and endpoints definitions
These analyses are based on a prospective single-centre cohort study conducted at Clínica Alemana Santiago, Chile. Patients under 65 years of age who were admitted for COVID-19 between June 2020 and July 2021 (corresponding to the two first waves of the pandemic) were consecutively enrolled. During this initial phase of the pandemic, where clinical assessments were severely restricted and there was a risk of underreporting comorbidities, we made the decision to concentrate on a younger demographic. This approach aimed to mitigate potential comorbidities that could independently contribute to poorer outcomes. During this period, the predominant circulating variants were Gamma (51.7%), Lambda (22.8%), and Alpha (6%) (14). Only patients who were discharged alive were included in the follow-up at 6 and 12 months. Detailed records of their previous medical history and acute clinical data upon admission were collected. Acute information regarding the patients was gathered during the initial 11 days of their hospitalization. The study protocol was approved by the local Ethics Committee (2022–33) and informed consent from all participants was obtained.
Baseline clinical-laboratory parameters including white blood cell count, ESR, CRP, ferritin and procalcitonin were measured at the time of acute hospital admission. In addition, acute phase samples were collected for comprehensive inflammatory response assessment including quantification of serum amyloid levels, inflammatory cytokines (IL-1β, IL-6, IL-8, IL-10, IL-12, IL-18, TNF) and chemokines (CCL2, CCL5, CCL8, CXCL9, CXCL10). Furthermore, samples were tested for the presence of the NLRP3 polymorphism (variant rs10754555), considering the C/G and G/G alleles as risk genotypes (12).
Following discharge, assessments were conducted by telephone interviews at 6 and 12 months to identify the presence of PCC symptoms using a structured questionnaire. These assessments utilized a structured questionnaire encompassing cognitive, cardiovascular, and gastrointestinal symptoms, as well as fatigue levels and return to normal activities. (Supplementary Table S1). Questions were related to current symptoms, therefore only those patients who still had symptoms at the time of the call were considered in the PCC group.
Statistical analysis
Quantitative variables are reported as means ± SD or median (IQ range) depending on the normality (K-S test) and were compared using T Test or Mann–Whitney U test. Qualitative variables are reported as absolute and % prevalence and compared using the χ2 test or Fisher’s exact test. A multivariable logistic regression analysis was performed to explore variables associated with PCC. The variables were identified by univariate logistic regression analysis, including those that correlated significantly with the symptoms at follow-up and clinically significant variables were also included. In this analysis, we considered sex, age, BMI, data of acute care clinical setting, and comorbidities. Multivariable logistic regression was done to obtain an adjusted odds ratio with a 95% confidence interval. STATA version 18.0 was used to perform the analyses.
Results
During the study period, a total of 130 patients under 65 years were discharged alive (Figure 1). At 6 months, 104 patients completed the follow up assessment. Patients had a median age of 42 years (IQR 37–56) and 30% were women (Table 1). Most of them had no comorbidities (64%), while a minority had been previously vaccinated against COVID-19 (19%), and only 11% required invasive mechanical ventilation (IMV). Regarding the acute laboratory findings and immune biomarkers obtained during acute hospitalization, it was noted that women had significantly lower ferritin values compared to men (465 vs. 1,141 ng/mL p = 0.004). No differences were found for inflammatory cytokines, chemokines or the presence of the NLRP risk variant (Table 1 and Supplementary Figures S1–S3).
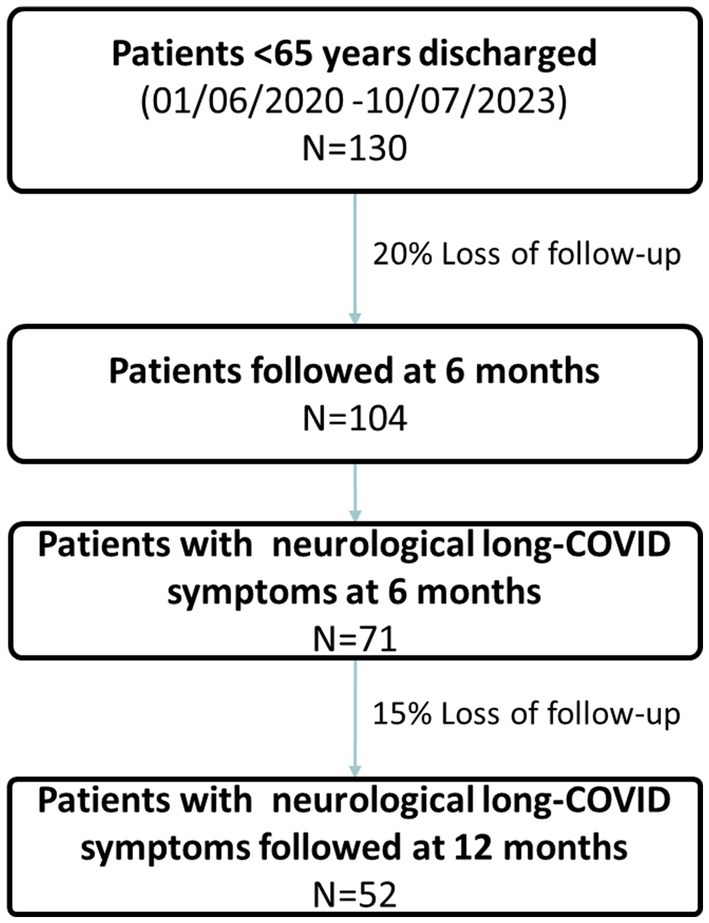
Figure 1. Study flowchart.
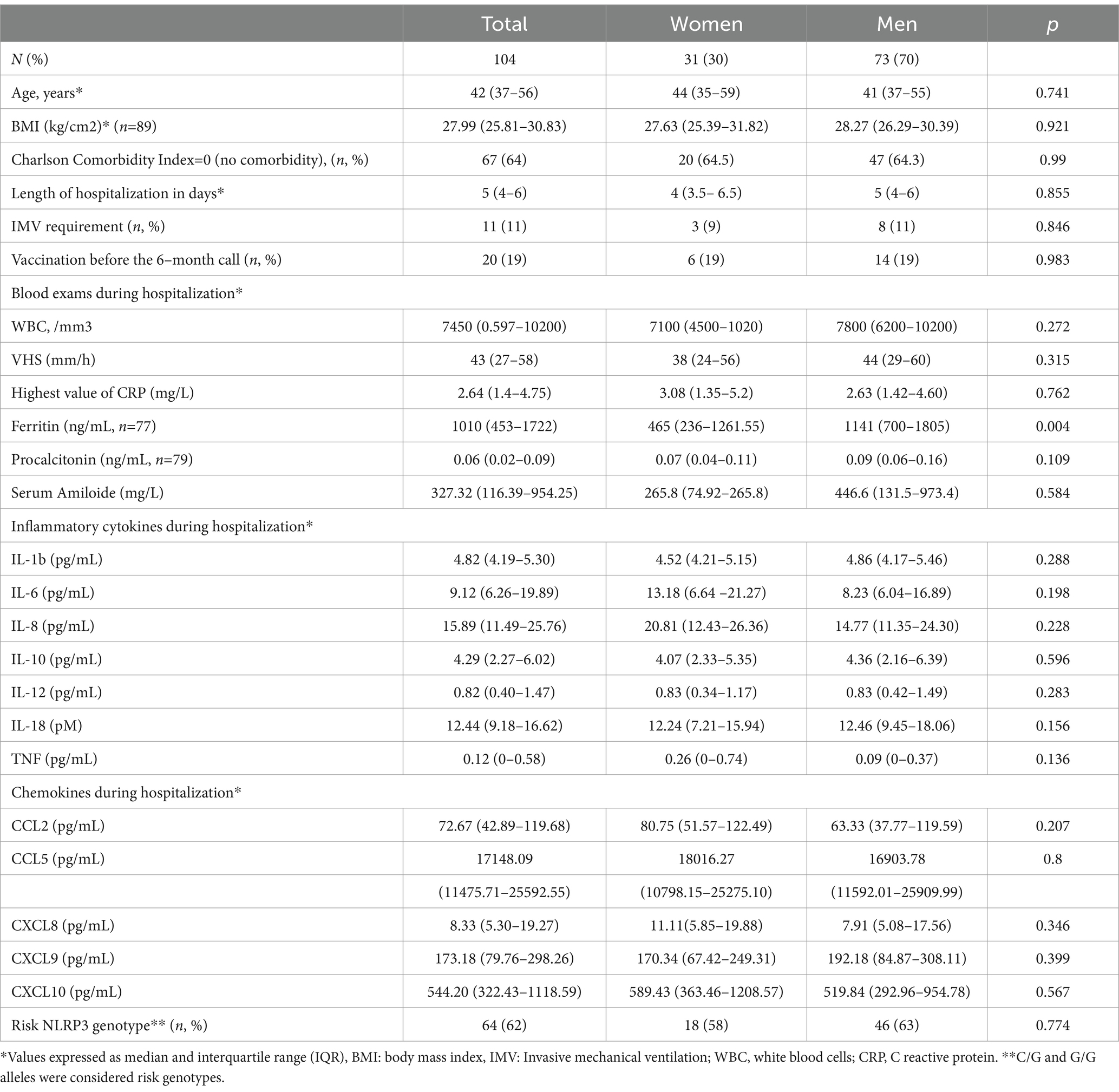
Table 1. Demographic, clinical characteristics and inflammatory parameters of study participants.
At 6 months, 71 out of 104 patients (68%) met the criteria for PCC, with a higher proportion of women (87 vs. 60%, p = 0.007) (Table 2). Of relevance, significant differences were observed between sexes. Women reported higher presence of cognitive (52 vs. 25% p = 0.007), cardiovascular (26 vs. 10% p = 0.031), and gastrointestinal (32 vs. 8% p = 0.022) symptoms compared to men. The evaluation of return to usual activities revealed a noteworthy gap: only 61% of women managed to resume their normal routines, whereas a substantial 90% of men with PCC achieved the same (p < 0.001). A comparison between those with and without PCC revealed a higher proportion of women in the former group (27 vs. 4, p = 0.007), as well as a greater requirement for IMV (11 vs. 0, p = 0.017) (Table 2). Nevertheless, no significant differences were observed in other clinical characteristics or blood test results (Table 2 and Supplementary Figures S4–S6). Moreover, 97% of individuals in the non-PCC group successfully resumed their usual activities compared to 75% within the PCC group (p = 0.006). In the group without PCC symptoms at 6 months, there were no significant differences between men (29/33) and women (4/33).
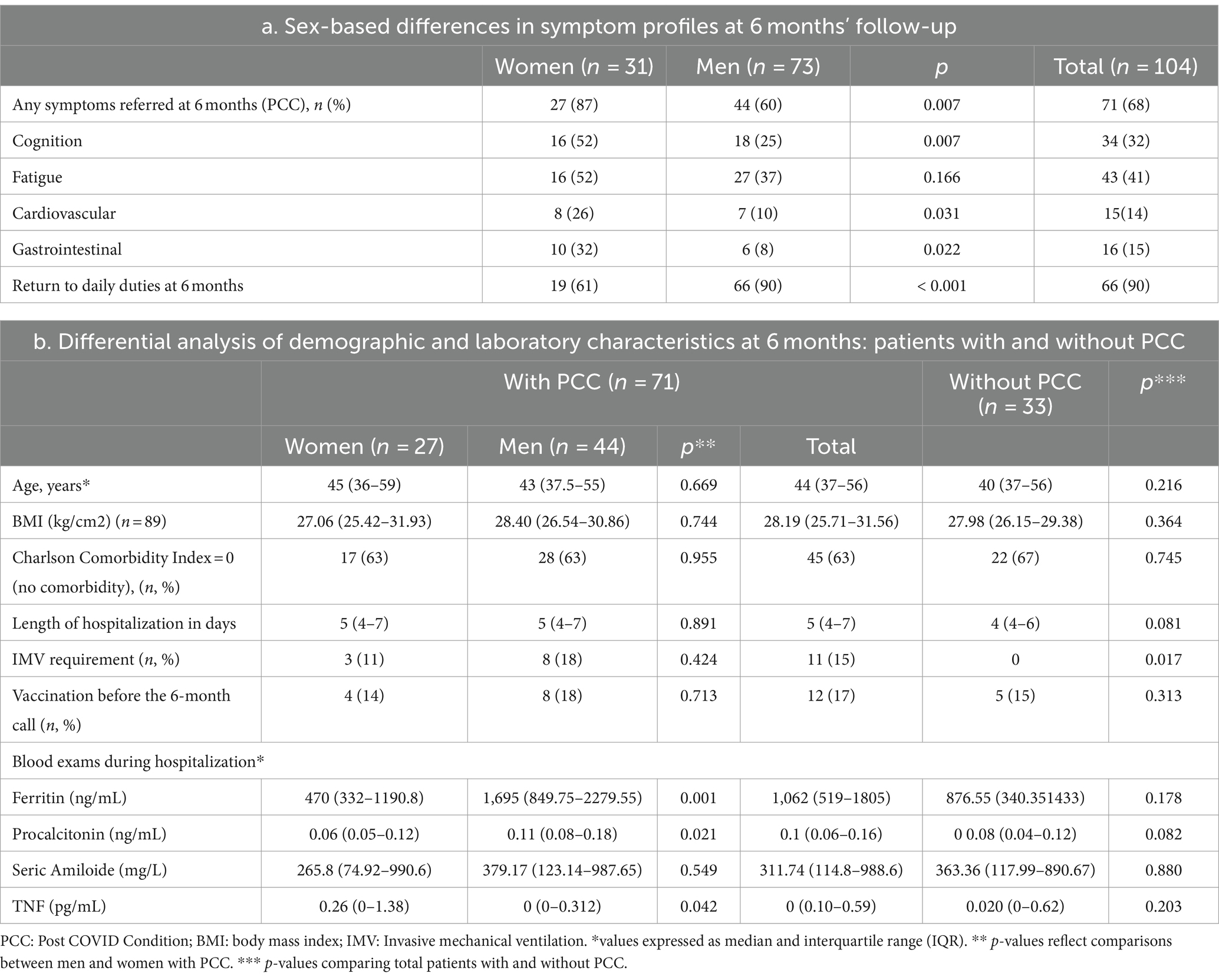
Table 2. Relevant acute phase characteristics and reported symptoms at 6 months.
In the PCC group, there were differences regarding laboratory findings during hospitalisation between sexes: women exhibited lower levels of ferritin (470 vs. 1,695 ng/mL, p = 0.001) and procalcitonin (0.06 vs. 0.11, p = 0.021), but higher TNF values (0.26 vs. 0, p = 0.042) compared to men in the acute phase (Table 2; Figure 2; Supplementary Figures S4–S6). Being women was the only independent predictor factor for PCC at 6 months, as they were 7.60 times more likely to experience it compared to men (p = 0.026, CI 1.27–45.18, Supplementary Figure S7).
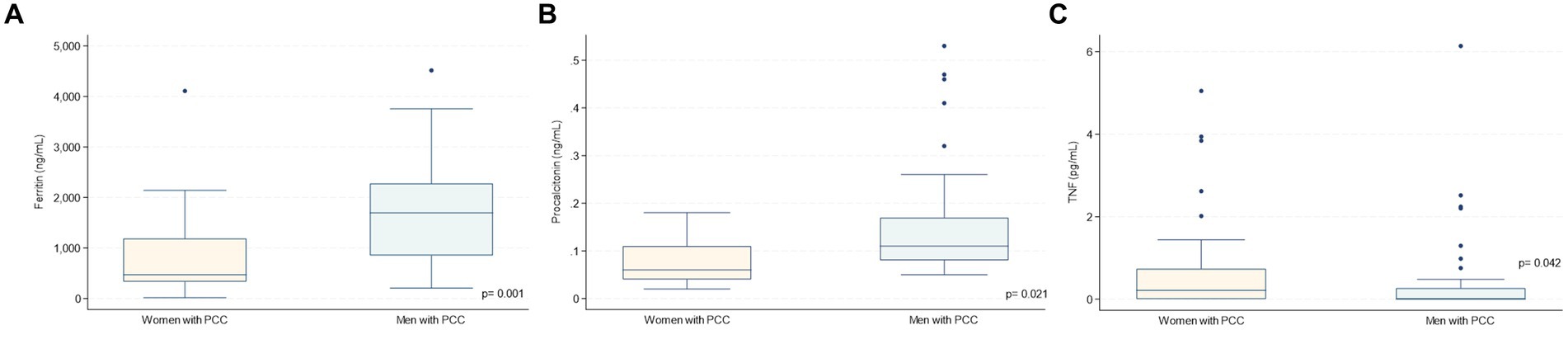
Figure 2. Acute phase biomarkers during hospitalisation according to sex in patients with PCC symtoms at 6 months. * PCC: post COVID-19 condition. (A) Ferritin, (B) Procalcitonin, (C) TNF.
At 12 months, 87% of patients with previous PCC at 6 months still had symptoms but showed no evident clinical or laboratory differences by sex (Supplementary Table S2). Importantly, in this subgroup, only 56% of women were able to return to their regular activities, as opposed to 86% of men (p = 0.004).
Discussion
The results of our study provide valuable information on the lasting impact of COVID-19 among adults under the age of 65 with non-critical disease. Despite a higher initial admission rate of men for COVID-19, PCC affected predominantly women. Specifically, they reported a higher prevalence of cognitive, cardiovascular, and gastrointestinal compromise. This is in line with previous reports (15–17), although it is noteworthy that these women did not have other concurrent comorbidities, as has been observed in other cohorts (18).
Only female sex was found to be predictive of subsequent PCC. This finding is consistent with previous research, which highlights the notable association between the risk of PCC and specific socio-demographic factors, in particular female sex (19). Although some studies have hinted at possible links with ethnicity or pre-existing conditions (such as poor mental and general health or asthma), there is a lack of consistent evidence across studies to designate these as reliable predictors of PCC (20–22). Despite this, we observed clear acute differences in ferritin and procalcitonin levels between sexes, with lower levels in women than in men. Many studies have found a link between elevated ferritin levels and increased risk of death. However, the relationship is complex, and other factors can play a role (19, 20). It should be noted that, to our knowledge, no previous research has specifically examined sex disparities in ferritin values among patients with mild COVID-19. However, the lower ferritin values observed in women could be attributed to the fact that they experience a milder acute infectious course. In addition, women showed higher TNF values than men. This is consistent with recent studies that have indicated elevated TNF levels in patients with post-COVID symptoms, suggesting its potential role as a predictor of PCC (21). This finding could be related to variations in immune response, hormonal factors, or other underlying biological mechanisms. The absence of notable disparities in inflammatory cytokines, chemokines and the NLRP3 risk variant suggests a more nuanced interaction between sex and immune response in COVID-19. At 12-month follow-up, we observed that patients with PCC had no significant clinical or laboratory differences, suggesting a possible stabilisation or stagnation of symptoms in this subgroup, possibly influenced by different factors such as the initiation of COVID-19 vaccination (20).
In terms of the return to daily activities, when comparing individuals with and without PCC, the PCC-affected group demonstrated greater difficulty resuming their usual routines (75% vs. 97%, p = 0.006). Within the PCC group, women showed significantly lower rates of resumption of usual activities compared to men, both at 6-and 12-months follow-up. This observation points to a possible impact on quality of life and highlights the specific obstacles that women may encounter during their recovery process. This may be associated with a higher prevalence of neuropsychiatric symptoms (23) and the societal expectation that males often shoulder the primary role in household support. It underlines the need for personalised care plans after COVID-19, especially adapted to female patients.
The results herein support the need to establish PCC assessment in all adults in the aftermath of COVID-19, particularly in women, as predictive factors in the acute setting remain elusive.
To the best of our knowledge, this represents the largest cohort of COVID-19 patients with a 12-month follow-up, coupled with a comprehensive evaluation of inflammatory biomarkers. This is especially significant as obtaining blood samples during the early stages of the pandemic posed considerable challenges, given the limited availability of specific laboratory reagents and the associated costs of analysis. Notably, this cohort primarily comprised individuals affected during the two initials waves of the pandemic; therefore, effects of infection can be assessed independently of vaccination, which could be confounding.
Our study has remarked limitations that deserve to be acknowledged. First, it is a single-centre investigation conducted in a relatively uniform cohort of patients with moderate COVID-19 severity, because of challenges associated to consenting acute severe patients for the study or had died at follow up. In addition, participants were under 65 years old. Therefore, larger scale studies covering a broader spectrum of patients, including those who did not require hospitalisation and with more comorbidities, are essential to validate these findings. Second, our admission information was limited to 11 days, potentially leading to loss of relevant information from the acute phase. However, the comprehensive characterisation of acute patients, including assessment of inflammatory markers and evaluation of risk genotypes, lends strength to the study results. Finally, discharge follow-up was conducted by telephone and employing a concise questionnaire with broad questions regarding PCC symptoms, which could introduce bias in the results by restricting participation to those who could answer the call and incomplete information. Throughout the pandemic, numerous studies have employed similar methodologies, demonstrating their reliability (22–24). Unlike other studies with high non-response rates or unreachable participants, our study had only a 20% dropout rate at 6 months and a 15% dropout rate at 12 months (25). Nevertheless, it is likely that our results are more representative of a younger, healthier population, whereas frail subjects are under-represented in our study.
Conclusion
In summary, our study emphasizes the significance of acknowledging and addressing sex-specific nuances among COVID-19 survivors. These findings support the need for a more individualized and comprehensive approach to post-COVID care, with particular attention to the distinct challenges encountered by female patients. Further research is essential to elucidate the underlying mechanisms contributing to these disparities and to enhance interventions for achieving the best possible recovery and rehabilitation outcomes.
Data availability statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found at: https://www.ncbi.nlm.nih.gov/clinvar/, SUB14168930.
Ethics statement
The studies involving humans were approved by Centro de bioética, Facultad de Medicina Clínica Alemana, Universidad del Desarrollo. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
CD: Data curation, Formal analysis, Validation, Writing – original draft, Investigation. MCP: Investigation, Supervision, Writing – review & editing. CV: Investigation, Methodology, Writing – review & editing. PVi: Conceptualization, Supervision, Writing – review & editing. GM: Conceptualization, Supervision, Visualization, Writing – review & editing. AR: Data curation, Investigation, Project administration, Writing – review & editing. CA: Writing – review & editing, Investigation. NM-G: Writing – review & editing, Investigation. JH: Writing – review & editing, Investigation. CC: Software, Writing – review & editing. PMV: Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Writing – original draft, Writing – review & editing.
Funding
The authors declare having received financial support for the research, authorship and/or publication of this article. This study was funded by research grants from ANID Fondecyt Regular 1221837 and Pfizer 76883481 receiving PMV. The funding agencies were not involved in the design of the study or in the analysis and interpretation of the data. MCP receives research grants from ANIDCOVID0999 and ANID Fondecyt Regular 1221802.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2024.1376030/full#supplementary-material
References
1. Coronavirus disease (COVID-19), Available at: https://www.who.int/news-room/fact-sheets/detail/coronavirus-disease-(covid-19) (Accessed September 26, 2023).
2. Soriano, JB, Murthy, S, Marshall, JC, Relan, P, and Diaz, JVWHO Clinical Case Definition Working Group on Post-COVID-19 Condition. A clinical case definition of post-COVID-19 condition by a Delphi consensus. Lancet Infect Dis. (2022) 22:e102–7. doi: 10.1016/S1473-3099(21)00703-9
3. Groff, D, Sun, A, Ssentongo, AE, Ba, DM, Parsons, N, Poudel, GR, et al. Short-term and long-term rates of Postacute sequelae of SARS-CoV-2 infection: a systematic review. JAMA Netw Open. (2021) 4:e2128568. doi: 10.1001/jamanetworkopen.2021.28568
4. Ferrari, AJ, Santomauro, DF, Aali, A, Abate, YH, Abbafati, C, Abbastabar, H, et al. Global incidence, prevalence, years lived with disability (YLDs), disability-adjusted life-years (DALYs), and healthy life expectancy (HALE) for 371 diseases and injuries in 204 countries and territories and 811 subnational locations, 1990–2021: a systematic analysis for the global burden of disease study 2021. Lancet. (2024) 403:2133–61. doi: 10.1016/S0140-6736(24)00757-8
5. Pilotto, A, Cristillo, V, Cotti Piccinelli, S, Zoppi, N, Bonzi, G, Sattin, D, et al. Long-term neurological manifestations of COVID-19: prevalence and predictive factors. Neurol Sci. (2021) 42:4903–7. doi: 10.1007/s10072-021-05586-4
6. Arjun, MC, Singh, AK, Pal, D, Das, K, Venkateshan, M, Mishra, B, et al. Characteristics and predictors of long COVID among diagnosed cases of COVID-19. PLoS One. (2022) 17:e0278825. doi: 10.1371/journal.pone.0278825
7. Low, RN, Low, RJ, and Akrami, A. A review of cytokine-based pathophysiology of long COVID symptoms. Front Med. (2023) 10:1011936. doi: 10.3389/fmed.2023.1011936
8. Heneka, MT, Golenbock, D, Latz, E, Morgan, D, and Brown, R. Immediate and long-term consequences of COVID-19 infections for the development of neurological disease. Alzheimers Res Ther. (2020) 12:69. doi: 10.1186/s13195-020-00640-3
9. Van Den Berg, DF, and Te Velde, AA. Severe COVID-19: NLRP3 Inflammasome dysregulated. Front Immunol. (2020) 11:1580. doi: 10.3389/fimmu.2020.01580
10. Zhao, N, Di, B, and Xu, L. The NLRP3 inflammasome and COVID-19: activation, pathogenesis and therapeutic strategies. Cytokine Growth Factor Rev. (2021) 61:2–15. doi: 10.1016/j.cytogfr.2021.06.002
11. Abulafia, DP, de Rivero Vaccari, JP, Lozano, JD, Lotocki, G, Keane, RW, and Dietrich, WD. Inhibition of the Inflammasome complex reduces the inflammatory response after thromboembolic stroke in mice. J Cereb Blood Flow Metab. (2009) 29:534–44. doi: 10.1038/jcbfm.2008.143
12. Schunk, SJ, Kleber, ME, März, W, Pang, S, Zewinger, S, Triem, S, et al. Genetically determined NLRP3 inflammasome activation associates with systemic inflammation and cardiovascular mortality. Eur Heart J. (2021) 42:1742–56. doi: 10.1093/eurheartj/ehab107
13. Augustin, M, Heyn, F, Ullrich, S, Sandaradura de Silva, U, Albert, MC, Linne, V, et al. Immunological fingerprint in coronavirus disease-19 convalescents with and without post-COVID syndrome. Front Med. (2023) 10:1129288. doi: 10.3389/fmed.2023.1129288
14. Möller, M, Borg, K, Janson, C, Lerm, M, Normark, J, and Niward, K. Cognitive dysfunction in post-COVID-19 condition: mechanisms, management, and rehabilitation. J Intern Med. (2023) 294:563–81. doi: 10.1111/joim.13720
15. Bai, F, Tomasoni, D, Falcinella, C, Barbanotti, D, Castoldi, R, Mulè, G, et al. Female gender is associated with long COVID syndrome: a prospective cohort study. Clin Microbiol Infect. (2022) 28:611.e9–611.e16. doi: 10.1016/j.cmi.2021.11.002
16. Hedberg, P, Granath, F, Bruchfeld, J, Askling, J, Sjöholm, D, Fored, M, et al. Post COVID-19 condition diagnosis: a population-based cohort study of occurrence, associated factors, and healthcare use by severity of acute infection. J Intern Med. (2023) 293:246–58. doi: 10.1111/joim.13584
17. Kaushal, K, Kaur, H, Sarma, P, Bhattacharyya, A, Sharma, DJ, Prajapat, M, et al. Serum ferritin as a predictive biomarker in COVID-19. A systematic review, meta-analysis and meta-regression analysis. J Crit Care. (2022) 67:172–81. doi: 10.1016/j.jcrc.2021.09.023
18. Alroomi, M, Rajan, R, Omar, AA, Alsaber, A, Pan, J, Fatemi, M, et al. Ferritin level: a predictor of severity and mortality in hospitalized COVID-19 patients. Immun Inflamm Dis. (2021) 9:1648–55. doi: 10.1002/iid3.517
19. Alonso-Domínguez, J, Gallego-Rodríguez, M, Martínez-Barros, I, Calderón-Cruz, B, Leiro-Fernández, V, Pérez-González, A, et al. High levels of IL-1β, TNF-α and MIP-1α one month after the onset of the acute SARS-CoV-2 infection, predictors of post COVID-19 in hospitalized patients. Microorganisms. (2023) 11:2396. doi: 10.3390/microorganisms11102396
20. Fatima, S, Ismail, M, Ejaz, T, Shah, Z, Fatima, S, Shahzaib, M, et al. Association between long COVID and vaccination: a 12-month follow-up study in a low-to middle-income country. PLoS One. (2023) 18:e0294780. doi: 10.1371/journal.pone.0294780
21. Sansone, D, Tassinari, A, Valentinotti, R, Kontogiannis, D, Ronchese, F, Centonze, S, et al. Persistence of symptoms 15 months since COVID-19 diagnosis: prevalence, risk factors and residual work ability. Life. (2022) 13:97. doi: 10.3390/life13010097
22. Righi, E, Mirandola, M, Mazzaferri, F, Razzaboni, E, Zaffagnini, A, Erbogasto, A, et al. Long-term patient-Centred follow-up in a prospective cohort of patients with COVID-19. Infect Dis Ther. (2021) 10:1579–90. doi: 10.1007/s40121-021-00461-3
23. Peghin, M, Palese, A, Venturini, M, de Martino, M, Gerussi, V, Graziano, E, et al. Post-COVID-19 symptoms 6 months after acute infection among hospitalized and non-hospitalized patients. Clin Microbiol Infect. (2021) 27:1507–13. doi: 10.1016/j.cmi.2021.05.033
24. Xiong, Q, Xu, M, Li, J, Liu, Y, Zhang, J, Xu, Y, et al. Clinical sequelae of COVID-19 survivors in Wuhan, China: a single-Centre longitudinal study. Clin Microbiol Infect. (2021) 27:89–95. doi: 10.1016/j.cmi.2020.09.023
Keywords: post COVID-19 condition, long COVID, COVID-19, sex-disaggregated, neurologic long-COVID-19
Citation: Delfino C, Poli MC, Vial C, Vial PA, Martínez G, Riviotta A, Arbat C, Mac-Guire N, Hoppe J, Carvajal C and Muñoz Venturelli P (2024) Post-COVID-19 condition: a sex-based analysis of clinical and laboratory trends. Front. Med. 11:1376030. doi: 10.3389/fmed.2024.1376030
Edited by:
César Fernández-de-las-Peñas, Rey Juan Carlos University, SpainReviewed by:
Martin Helán, St. Anne’s University Hospital, CzechiaElham Jamshidi, Johns Hopkins University, United States
Zaki A. Sherif, Howard University, United States
Copyright © 2024 Delfino, Poli, Vial, Vial, Martínez, Riviotta, Arbat, Mac-Guire, Hoppe, Carvajal and Muñoz Venturelli. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Paula Muñoz Venturelli, cGF1bXVub3pAdWRkLmNs