 Domitille Renard1*
Domitille Renard1* Mikael Verdalle-Cazes2Perrine Leprêtre1,3
Mikael Verdalle-Cazes2Perrine Leprêtre1,3 Jérémy Bellien3,4Valery Brunel5Sylvanie Renet3Fabienne Tamion3,6
Jérémy Bellien3,4Valery Brunel5Sylvanie Renet3Fabienne Tamion3,6 Emmanuel Besnier1,3
Emmanuel Besnier1,3 Thomas Clavier1,3
Thomas Clavier1,3- 1Department of Anesthesiology and Critical Care, CHU Rouen, Rouen, France
- 2Department of Radiology, CHU Rouen, Rouen, France
- 3INSERM EnVI UMR 1096, University of Rouen Normandie, Rouen, France
- 4Department of Pharmacology, CHU Rouen, Rouen, France
- 5Department of General Biochemistry, CHU Rouen, Rouen, France
- 6Medical Intensive Care Unit, CHU Rouen, Rouen, France
Introduction: Links have been established between SARS-CoV-2 and endoplasmic reticulum stress (ERS). However, the relationships between inflammation, ERS, and the volume of organ damage are not well known in humans. The aim of this study was to explore whether ERS explains lung damage volume (LDV) among COVID-19 patients admitted to the intensive care unit (ICU).
Materials and methods: We conducted a single-center retrospective study (ancillary analysis of a prospective cohort) including severe COVID-19 ICU patients who had a chest computed tomography (CT) scan 24 h before/after admission to assess LDV. We performed two multivariate linear regression models to identify factors associated with plasma levels of 78 kDa-Glucose-Regulated Protein (GRP78; ERS marker) and Interleukin-6 (IL-6; inflammation marker) at admission.
Results: Among 63 patients analyzed, GRP78 plasma level was associated with LDV in both multivariate models (β = 22.23 [4.08;40.38]; p = 0.0179, β = 20.47 [0.74;40.20]; p = 0.0423) but not with organ failure (Sequential Organ Failure Assessment (SOFA) score) at admission (r = 0.03 [−0.22;0.28]; p = 0.2559). GRP78 plasma level was lower among ICU survivors (1539.4 [1139.2;1941.1] vs. 1714.2 [1555.2;2579.1] pg./mL. respectively; p = 0.0297). IL-6 plasma level was associated with SOFA score at admission in both multivariate models (β = 136.60 [65.50;207.70]; p = 0.0003, β = 193.70 [116.60;270.90]; p < 0.0001) but not with LDV (r = 0.13 [−0.14;0.39]; p = 0.3219). IL-6 plasma level was not different between ICU survivors and non-survivors (12.2 [6.0;43.7] vs. 30.4 [12.9;69.7] pg./mL. respectively; p = 0.1857). There was no correlation between GRP78 and IL-6 plasma levels (r = 0.13 [−0.13;0.37]; p = 0.3106).
Conclusion: Among severe COVID-19 patients, ERS was associated with LDV but not with systemic inflammation, while systemic inflammation was associated with organ failure but not with LDV.
1 Introduction
The emergence of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) disease (COVID-19) at the end of 2019 has affected 689 million people worldwide and has been responsible for 6.9 million deaths (data from 28 March 2023) (1). This virus mainly induces pulmonary damages that can lead to acute respiratory distress syndrome (ARDS) through cell apoptosis and inflammatory storm (2, 3). This inflammatory stress is linked to pro-inflammatory cytokines, notably interleukin-6 (IL-6), which is associated with organ failure among COVID-19 patients (4, 5). The volume of these pulmonary lesions induced by SARS-CoV-2 is assessed by chest computed tomography (CT), which is now the reference exam for COVID-19 patients. The extent of SARS-CoV-2 lesions on CT is known to be predictive of severity, regardless of analytical methods used (scoring, ventilation imaging, etc.) (6, 7).
Endoplasmic reticulum (ER) stress (ERS) and its adaptive response, the unfolded protein response (UPR), represent an archetypal example of adaptive stress response. The ER plays a crucial role in protein folding, notably regulated by specific proteins known as chaperones, such as the 78 kDa Glucose-Regulated Protein (GRP78) which stimulates the correct folding of polypeptide to functional protein complexes (8). Multiple disturbances observed during infection or trauma can result in a dysfunction of the ER, leading to the accumulation of unfolded proteins within the lumen of the ER, known as ERS (9, 10). One of the roles of the UPR is to lead the synthesis of new chaperones to allow protein folding (e.g., GRP78, the final effector of UPR). However, if the ERS is severe and prolonged, UPR can lead to cell death by apoptosis (11). Several studies have shown that GRP78 and UPR mediators are enhanced in ARDS patients, suggesting that ERS may be a central component of lung inflammatory diseases. In comparison to healthy individuals, COVID-19 patients had higher plasma levels of GRP78, higher expression of GRP78 within pneumocytes and alveolar macrophages (12–14). It was also mentioned an increase in GRP78 expression on the surface of leukocytes in severe COVID-19 patients, a correlation between circulating GRP78 and COVID-19 severity among COVID-19 patients and amelioration of the lung hyperinflammatory response by the modulation of ERS in a mouse COVID-19 ARDS model (15). Some data suggested that GRP78 acts as a pro-viral protein during SARS-CoV-2 infection (16). However, we recently found no association between GRP78 plasma level and clinical worsening from a “severe” toward a “critical” condition in ICU patients (17).
ERS is classically linked to systemic inflammation and organ failure (18, 19). However, a recent study questioned the causal relationship between inflammation, organ injury and ERS during sepsis. Thus, in a model of surgical peritoneal sepsis [cecal ligation-puncture (CLP)], peritoneal infection predominantly triggered inflammatory responses, while damages induced by surgical stress were predominant triggers of the ERS/UPR response (20). These data, showing that inflammation was little associated with tissue trauma (but driven by infection) while ERS/UPR were essentially driven by tissue trauma more than by infection or systemic inflammation, raise the question of the relationship between ERS, inflammation and volume of organ damage (cellular necrosis/tissue degradation).
To our knowledge, while several works reported links between organ failure, inflammation and ERS among humans, there is no study which directly assessed the link between the volume of organ damage and ERS expression. Therefore, the aim of this study was to investigate whether circulating GRP78 explains the volume of pulmonary damage among patients with severe COVID-19 admitted in ICU.
2 Materials and methods
2.1 Study design
We conducted a single-center retrospective study using a previously prospectively collected data set. The present study is an ancillary analysis of the COVID-THELIUM cohort, that was described in a previous publication (21). This cohort concerned severe COVID-19 patients hospitalized in three intensive care units (ICU) of a tertiary care hospital between May and November 2020. This cohort was approved by an ethics committee (Comité de Protection des Personnes Est-III, approval number 2020-A00885-34). According to the French law, verbal approval was required from the patient or their relatives (22). The study was conducted in accordance with the principles of the Declaration of Helsinki related to human research. The elaboration of the manuscript was in accordance with the STROBE statement.
To put things briefly, patients were eligible for inclusion if they presented a “severe” condition related to a documented infection by SARS-CoV-2 (determined by polymerase chain reaction assay), defined as the need for ICU admission because of acute respiratory failure. Non-inclusion criteria were pregnancy, a documented bacterial co-infection, known limitations in life support because of patient choice or important comorbidities and an expected death within 24 h. For the present study, we also excluded patients who did not receive a lung scan within 24 h before or after ICU admission and patients already on mechanical ventilation at ICU admission.
Clinical data were collected at admission and during ICU stay, including conventional characteristics, Sequential Organ Failure Assessment (SOFA) score, conventional biological characteristics (blood count, creatinine, C-reactive protein (CRP), aspartate aminotransferase (AST), lactatemia, high-sensitivity troponin T). Patients were followed for up to 28 days or until death.
2.2 Endpoints
Our primary endpoint was to investigate whether circulating GRP78 plasma level explain lung damage volume (expressed in percentage of total lung volume) evaluated by chest CT.
Our secondary endpoints were to investigate an association between:
• GRP78 plasma level and organ failure and inflammation;
• IL-6 plasma level and organ failure, tissue damage and inflammation;
• GRP78 and IL-6 plasma levels and length of ICU/hospital stay and mortality.
2.3 CT scan
Chest CT scans were re-analyzed in DICOM format by Thoracic VCAR software (GE Healthcare, Chicago, Illinois, United States) for every patient (23). This new analysis was performed by a single radiologist, blinded to the patients’ condition and biological results. Soft tissue reconstruction was used before this analysis. This software allows an automatic segmentation of the two lungs. On this segmentation, a thresholding by binarization was applied, assuming the darkest voxels correspond to air (healthy alveoli, bronchial and bronchiolar lumens) and the lightest voxels to the damaged territory (ground glass hyperdensity, alveolar condensations). The threshold used for binarization was −522UH, which seems to have the best diagnostic value for COVID-19 (24). The software displayed the volume and percentage of involvement for each lung. The volume of damage was then expressed as a percentage of total lung volume for each patient.
2.4 Blood sample and assays
Whole blood was collected on ethylenediaminetetraacetic acid (EDTA) tubes within the first 24 h after ICU admission, using a venous or arterial catheter. Tubes were immediately centrifugated for 15 min (2000 G, 4°C) and plasma was frozen at −20°C for a maximum of 2 weeks before being frozen at −80°C until final assays.
Assays were performed using an Enzyme-Linked Immunosorbent Assay for GRP78 (Enzo Life Sciences, Villeurbanne, France), and using an Electro-Chemiluminescence Immunoassay for IL-6 (Roche Diagnostics, Meylan, France).
2.5 Data and statistical analysis
Because of the non-normal distribution of data, as observed using a Shapiro–Wilk test, results are expressed as medians with interquartile ranges (IQR) for quantitative data and as absolute numbers and percentages (n, %) for qualitative data. Analysis was performed using Spearman correlation test or Mann–Whitney test according to the type of variable. In cases of missing data, no value was imputed.
We conducted univariate analyses to investigate which factors were associated with GRP78 and IL-6 plasma levels in our study. We then established two multivariate linear regression models with GRP78 and IL-6 plasma levels as associated factors with the endpoints studied:
• The first one took into account factors associated with GRP78 or IL-6 plasma levels in univariate analysis. The significance level to include a parameter in the model was 0.1 (a posteriori model);
• The second was an a priori theoretical model including factors that were clinically relevant or frequently found associated with GRP78 and/or IL-6 plasma levels in medical literature (15, 25–28). We included in this a priori theoretical model: demographic characteristics (age, body mass index (BMI)), medical history (hypertension, diabetes), volume of lung damaged by SARS-CoV-2 (% of total lung volume), inflammatory markers used in daily practice (neutrophils, CRP) and quantification of organ failure (SOFA score, lactates).
Statistical significance was assessed using an alpha level of 0.05. The statistical analyses were performed by means of the statistical software GRAPHPAD PRISM (9.5.1).
3 Results
3.1 Patient’s characteristics
A total of 98 patients were included in the initial COVID-THELIUM cohort, 35 were excluded (timing of chest CT unknown or more than 24 h before/after ICU admission and/or already under mechanical ventilation at admission) leading to 63 patients analyzed. Their main clinical and biological characteristics at ICU admission are shown in Table 1.

Table 1. Characteristics of the population analyzed.
3.2 Endoplasmic reticulum stress marker
Quantitative parameters associated with GRP78 plasma level in univariate analysis are shown in Figure 1. Detailed results with 95% confidence interval are given in Supplementary material 1. Pulmonary embolism on chest CT was associated with higher GRP78 plasma level (1949.0 [1865.0;2083.0] vs. 1507.6 [1139.2;1877.8] pg./mL; p = 0.0298) but we found no association between GRP78 plasma level and gender, and history of diabetes or hypertension.
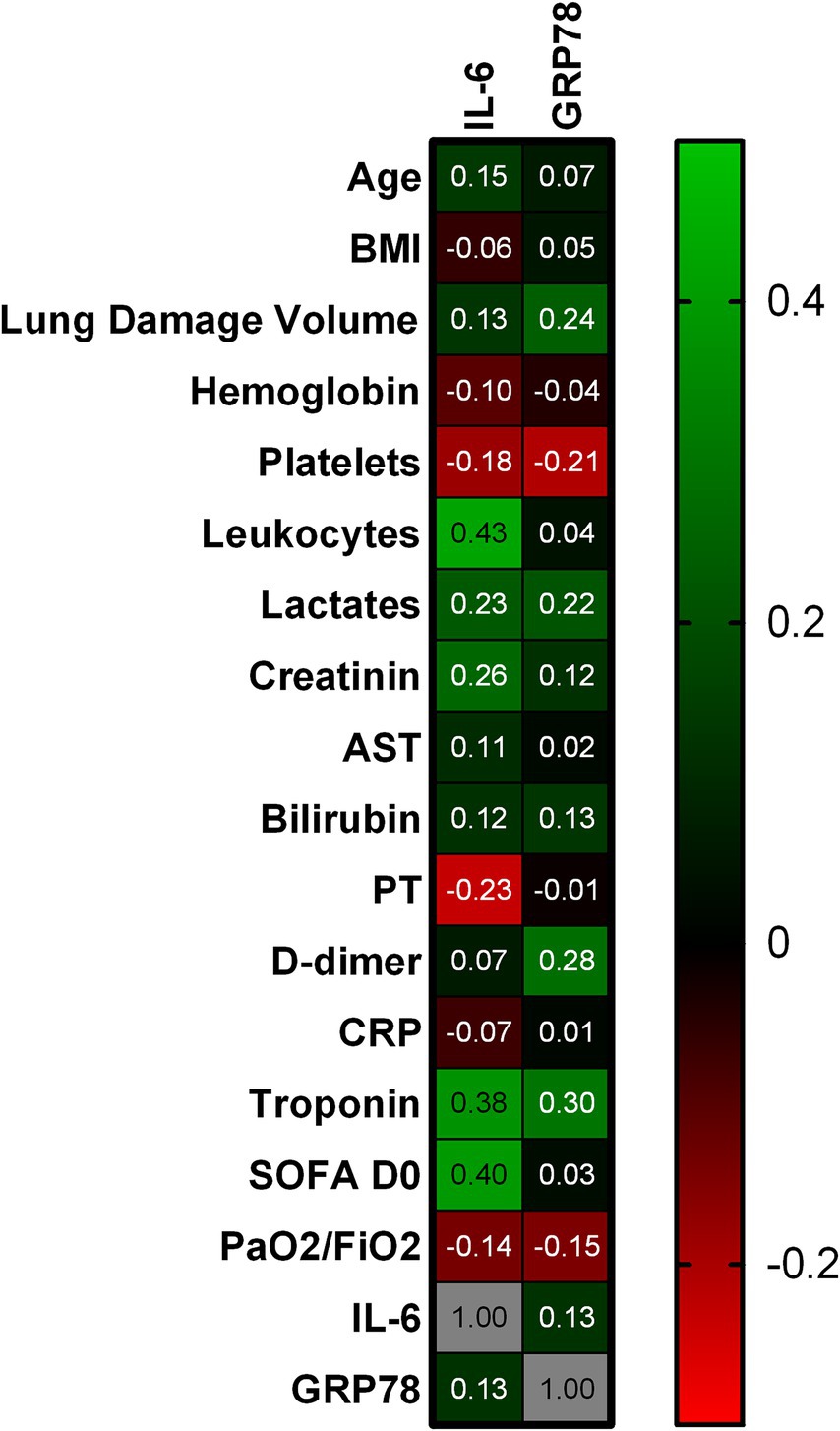
Figure 1. Correlation between characteristics at ICU admission and GRP78/IL-6 plasma levels. This figure presents the Spearman r correlation coefficient between quantitative parameters and GRP78/IL6 plasma levels at admission. Green represents a positive correlation with intensity increasing according to the lightness of the green, black represents no correlation, and red represents a negative correlation, with intensity increasing according to the lightness of the red. BMI, Body Mass Index; AST, Aspartate Aminotransferase; PT, Prothrombin Time; CRP, C-Reactive Protein; SOFA D0 score, Sequential Organ Failure Assessment day 0 score; IL-6, Interleukin-6; GRP78, 78 kDa Glucose-Regulated Protein.
The multivariate regression model based on univariate analyses results, including platelets, lactates, D-dimer, troponin, pulmonary embolism and lung damage volume, only found an association between lung damage volume percentage and GRP78 plasma level (Table 2). The multivariate regression model based on clinically relevant or frequently described factors also found an association between lung damage volume percentage and GRP78 plasma level (Table 2).
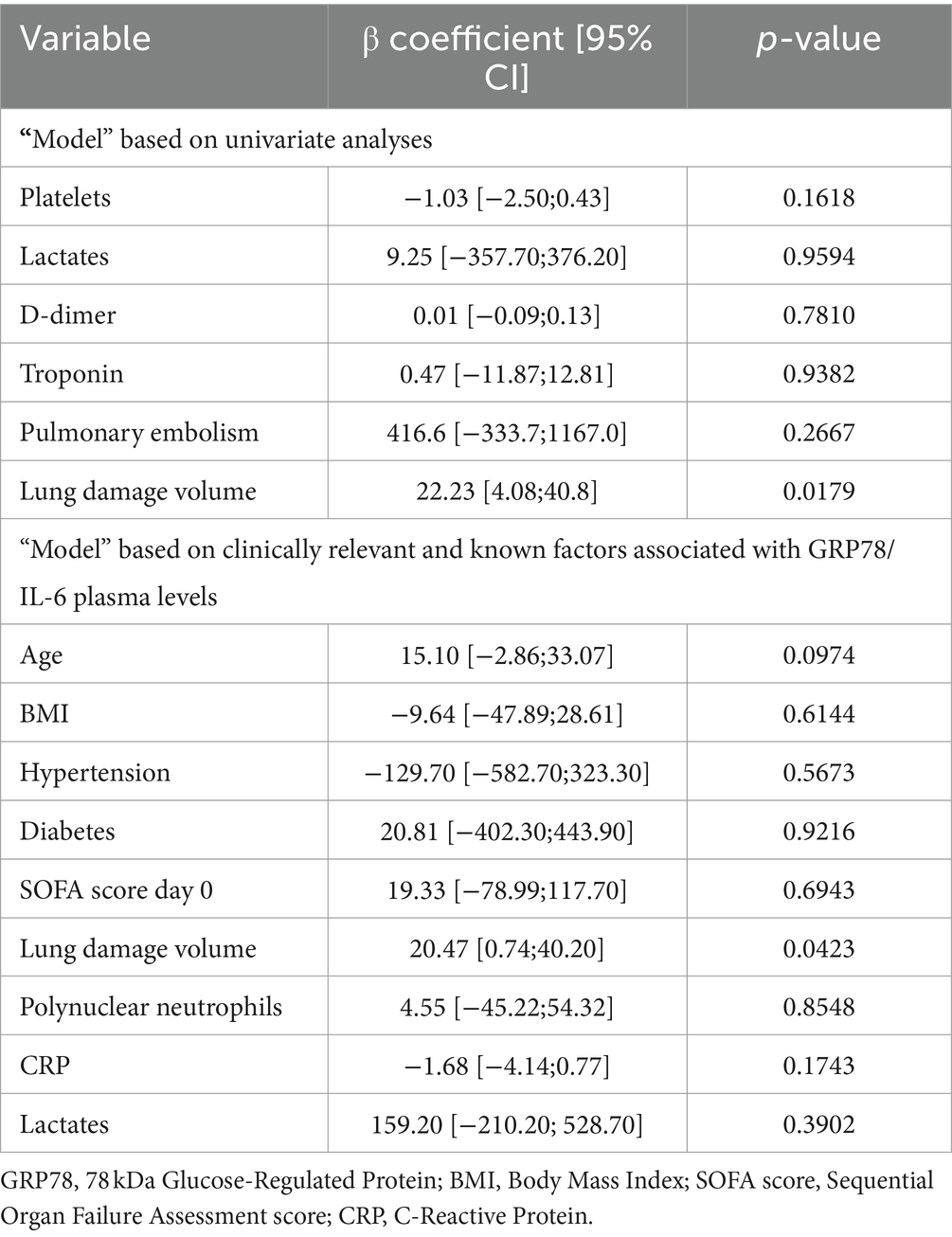
Table 2. Linear regression models (factors associated with GRP78 plasma level).
3.3 Inflammatory marker
Quantitative parameters associated with IL-6 plasma level in univariate analysis are shown in Figure 1. Detailed results with 95% confidence interval are given in Supplementary material 2. We found no association between IL-6 plasma level and pulmonary embolism, gender, history of diabetes or hypertension.
The multivariate regression model based on univariate analyses, including leukocytes, lactates, creatinine, prothrombin time, troponin and SOFA score at day 0, only found an association between SOFA score at day 0 and IL-6 plasma level (Table 3). The multivariate regression model based on clinically relevant or frequently described factors also found an association between SOFA score at day 0 and IL-6 plasma level (Table 3).
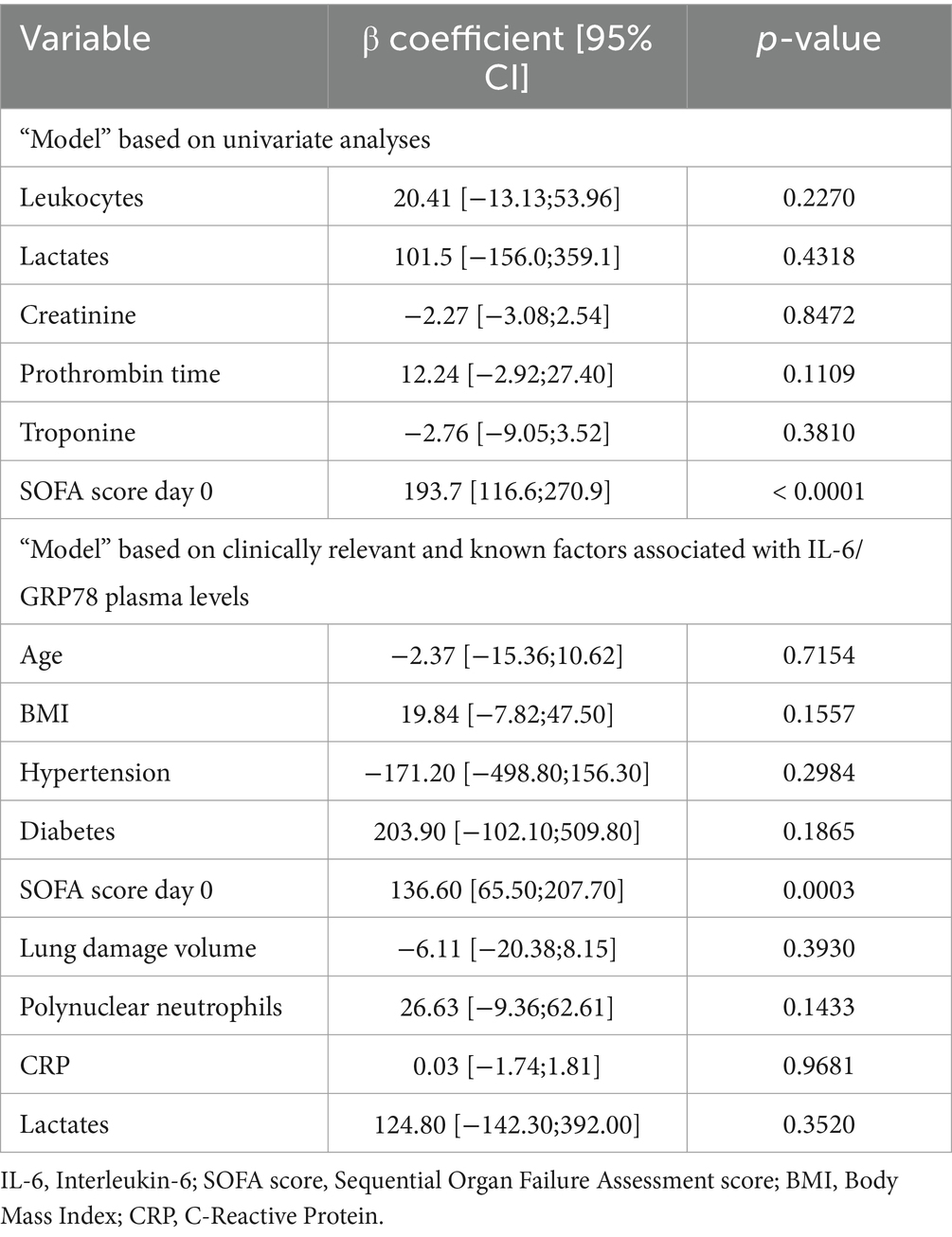
Table 3. Linear regression models (factors associated with IL-6 plasma level).
3.4 GRP78/IL-6 plasma levels and clinical evolution
There was no correlation between IL-6 plasma level (reflecting systemic inflammation) and GRP78 plasma level (reflecting intensity of ERS expression; r = 0.13 [−0.13;0.37]; p = 0.3106).
We found an association between IL-6 plasma level and length of ICU stay (r = 0.55 [0.34;0.70] p < 0.0001), length of hospital stay (r = 0.36 [0.11;0.56]; p = 0.0045), and SOFA score at day 7 (r = 0.60 [0.40;0.74]; p < 0.0001), but no association between these parameters and GRP78 plasma level.
Regarding the association between GRP78/IL-6 plasma levels and qualitative variables, we found an association between GRP78 plasma level and death, and between IL-6 plasma level and the need for intubation, prone positioning, and catecholamine administration (Table 4).
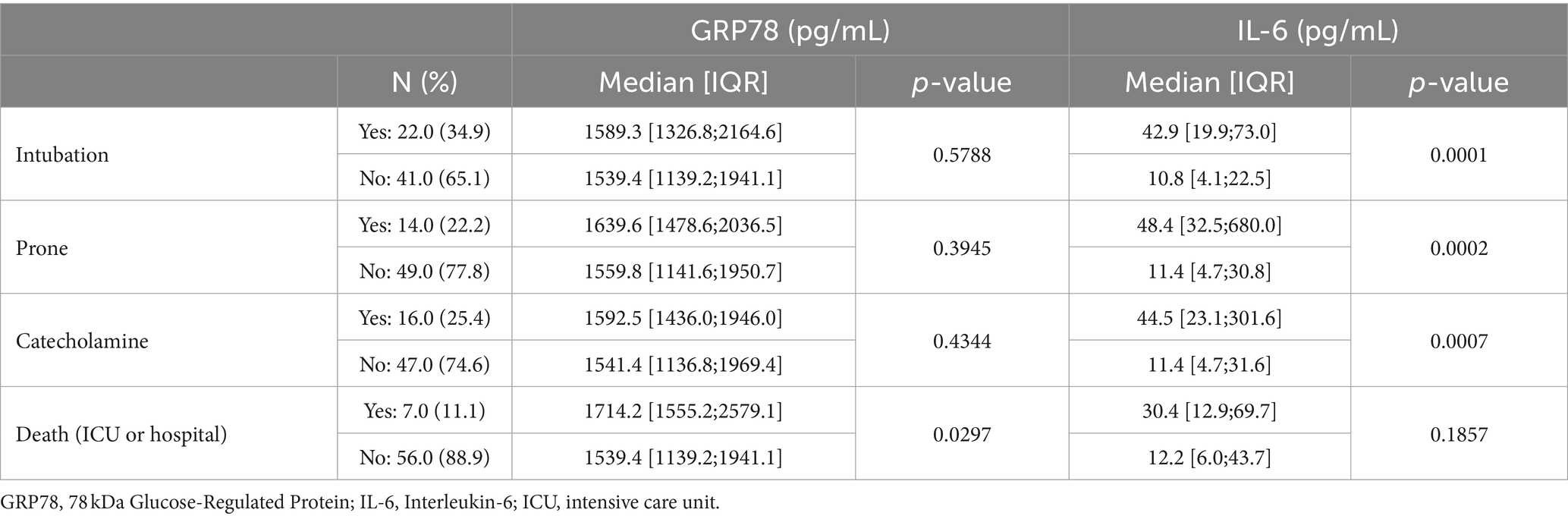
Table 4. Association between GRP78 and IL-6 plasma levels with morbidity and mortality criteria.
4 Discussion
Our results suggest that ERS and its response, UPR, could be independently associated with the volume of lung damage in severe COVID-19 patients and explain it. We did not find any association between GRP78 plasma level and inflammation or systemic organ failure. IL-6 plasma level seemed independently associated with systemic organ failure but not with tissue injury. Finally, IL-6 plasma level was more correlated with short-term severity while GRP78 plasma level was associated with short-term mortality. We developed two models of multivariate analysis for GRP78 and IL-6 plasma levels. One with strictly associated parameters in univariate analyses, the second one taking into account relevant factors found in the literature. The aim was to take into account as many confounding factors as possible, including those not found in our study and to strengthen the value of our findings with a “double methodology.” We distinguish between lung lesion volume, which represents a volume of tissue damage without presuming its functionality, and organ failure, represented by the SOFA score, which objectively reflects organ dysfunction.
Our objective was to study a “clinical model” of infectious injury associated with systemic inflammation in humans, involving a single organ whose volume of injured tissue could be easily quantified in vivo with a reliable and validated method. Studying a population of patients with severe COVID-19 allowed us to have a population with a pathology meeting these criteria. Indeed, SARS-CoV-2 has an essentially lung tropism responsible for an isolated respiratory failure and whose organ damages are easy to quantify in vivo by validated CT methods, with nevertheless an important systemic inflammation (2, 5, 29). We used a dedicated software used by a single radiologist to estimate lung damage through binarization. The analysis was then automatic, allowing us to avoid the human factor: the radiologist did not interpret the CT scans but only used the software. We arbitrarily chose a 24-h window between CT and the measurement of GRP78 plasma level. Our objective being to study the link between pulmonary damage and ERS and the kinetics of circulating GRP78 being a few hours, this 24-h window with a new systematic analysis by a blinded operator of previously performed chest CT seemed relevant (30).
Upregulation of circulating GRP78 is specific to ERS response and is considered to be a sensitive marker of ERS intensity (8). Furthermore, elevated blood and lung GRP78 levels had already been found among COVID-19 patients (13, 14). In our cohort, the lowest GRP78 plasma level was 406.3 pg./mL with a median at 1564.1 [1162.2;1969.4] pg./mL, which is well above the thresholds found in studies investigating the diagnostic values of GRP78 plasma level. Recently a threshold of GRP78 plasma level at 157.3 pg./mL was thus suggested for sepsis diagnosis (sensitivity 75.0%; specificity 73.1%) (31). A recent work studying inflammation and ERS among COVID-19 patients suggested that any SARS-CoV-2 positive patient who showed a GRP78 plasma level superior to 300 pg./mL in serum at the beginning of the infection had a 100% probability of developing pneumonia (15). The same study suggested that the plasma level of GRP78 among COVID-19 patients was associated with organ failure and severity of infection while we did not find an association between organ failure and GRP78 plasma level (15). It appears in agreement with our previous results in this cohort, which found no association between GRP78 plasma level at admission and clinical worsening in ICU (17). However, our patients had much higher plasma levels of GRP78 than the vast majority of this previous cohort, suggesting that this association could be influenced by the infection severity. As the GRP78 plasma level at admission was higher in deceased patients’ plasma than in survivors’, our results are however compatible with the link between ERS expression and short-term prognosis among COVID-19 patients. High plasma levels of IL-6 are known to be associated with adverse clinical outcomes, including ICU admission, ARDS, mechanical ventilation and death among COVID-19 patients (4, 32). We found an association between IL-6 plasma level and organ failure as previously described, showing that our population is similar to previous cohorts of COVID-19 patients admitted in ICU.
In our cohort, GRP78 plasma level was associated with lung damage volume but not with inflammation or organ failure, while IL-6 plasma level was associated with organ failure but not with lung damage volume or ERS. To respond to ERS, cells activate an adaptive pathway, the UPR, to synthesize chaperones (including GRP78) and restore normal ER function. While a strong UPR appears necessary in the acute stress phase, excessively prolonged ERS responses promote cell death as a result of an imbalance in favor of pro-apoptotic pathways rather than anti-apoptotic pathways (11). The fact that ERS and then UPR may promote apoptosis could be an explanation for the link between high GRP78 plasma levels and macroscopic volume of damaged organ. It is known that organ and/or tissue damage without infection can lead to ERS expression in humans and we previously described that among humans with surgical stress, there was no correlation between GRP78 and IL-6 or CRP levels (30, 33, 34). However, it is also often presumed in animal models that inflammation triggers ERS response (and vice versa). Our findings are in concordance with the recent animal study by Müllebner et al. showing that peritoneal infection induced by CLP predominantly triggered inflammatory response, while damages caused by surgery were predominant triggers of the ERS/UPR response (20). They hypothesized that ERS/UPR and inflammatory response in vivo during sepsis may be triggered by different mechanisms and that secondary tissue injury influences the severity of ERS more than the intensity of local and systemic inflammation. The association found between GRP78 plasma level and lung damage volume in our cohort combined with a non-correlation between ERS and systemic inflammation (IL-6) strengthen their hypothesis and describe for the first time this potential link among infected humans. This hypothesis is also comforted by recent studies in mouse models showing that important mechanical volume induced lung injury was the predominant trigger of ERS, preceding and contributing to lung inflammation (35, 36). As it is known that ERS expression after tissue injury last longer than systemic inflammation in humans, and given its association with damaged lung volume, it would be interesting to study the link between ERS expression and long-term prognosis among COVID-19 patients (fibrosis, bronchiectasis, chronic dyspnea,…) (33). Given these recent data, it also probably appears relevant in animal models of septic shock exploring ERS expression, to take into account the existence or not of tissue damage in the model to better interpret the intensity of ERS and UPR.
Regarding inflammation in our patients, we must emphasize that our patients exhibited inflammation with a median CRP of 114 mg/L and median neutrophil count of 6.5 G/L. There is no defined norm to describe a state of hyperinflammation; our patients seem to display an inflammatory state that could be considered moderate. We must also note that although interleukin-6 is a well-recognized and studied marker of inflammation, it also has functions outside of inflammation, such as in hematopoiesis, liver and neuronal regeneration, embryonal development, and fertility (4, 5, 37).
Finally, this dichotomy between ERS on one hand and tissue lesion volume (without presuming organ dysfunction) and on the other hand inflammation and organ failure allows for a different perspective. While inflammation is commonly associated with severity, as we find in the short term in our study, this severity and inflammation do not seem to be correlated with or responsible for the volume of tissue injury. Thus, we can infer that the response to ERS reflects direct viral tissue damage rather than excessive inflammation. ERS intensity could therefore be used as a proxy and marker of tissue lesions during pathology, allowing for the monitoring of lesion evolution.
Despite interesting results, our study has several limitations. Firstly, it was a monocenter retrospective study, including a limited number of patients, even though we had few missing data given the prospective design of the initial cohort. Secondly, some factors that we did not take into account could have impacted the plasma levels of GRP78 and/or IL-6. For example, it has been established in animal models that caloric restriction influences GRP78 production, which is a frequent situation within 24 h of arrival in ICU (38). Thirdly, the maximum lung parenchymal damage is known to occur 11 days after the onset of symptoms in COVID-19 patients, which is also the timing corresponding to their clinical worsening (8–12 days) (7, 26). The median time from symptoms to ICU admission in our population was 8.0 [5.7;10.0] days. We chose to include only patients with a chest CT performed in a 24-h window before/after ICU admission to account for GRP78 plasma level sample timing, but we probably missed the maximum of lung damage and could perhaps have shown a different association by changing this 24-h window. Fourthly, unlike many previous analyses, we did not find an association between IL-6 and CRP plasma levels. Nevertheless, IL-6 plasma level remained correlated with leukocytes, as did CRP. We thus hypothesize that the de-correlation between IL-6 plasma level and CRP could be due to a lack of statistical power. In addition, it appears that there may be some de-correlation between CRP and IL-6 plasma level in the most severe patients, CRP increasing little with a spike at 72 h in contrast to IL-6 plasma level, which increases a lot in a few hours (39). We took this point into account by including CRP in our a priori linear regression model. Fifthly, given our methodology, our results do not presume any causality link between ERS and lung tissue damage in humans. While some animal studies described that ERS expression is induced by tissue damage rather than by inflammation or infection, we cannot here confirm this hypothesis among infected humans. Sixth, our samples were taken at only one-time point (ICU admission) and we did not explore the kinetics or ERS/UPR and its links to the evolution of lung lesions during ICU stay. Further studies are needed to understand the kinetics of GRP78 plasma level during infections and sepsis among humans, and its association with organ damage and organ failure. Finally, our models include a large number of variables. However, we also performed the analyses with fewer variables but still keeping lung lesion volume and GRP78 levels, and the associations were still present, allowing us to think that our models are not affected by overfitting.
5 Conclusion
Our results suggest that, among severe COVID-19 patients, ERS is associated with the volume of lung damage but not with systemic inflammation, while systemic inflammation is associated with organ failure but not with lung damage. Given the ERS association with organ damage, it would be interesting to study its relationship with long-term functional outcome among COVID-19 patients.
Data availability statement
The data analyzed in this study is subject to the following licenses/restrictions: Data would be available depending of the reason. Requests to access these datasets should be directed to DR, ZG10LnJlbmFyZEBnbWFpbC5jb20=.
Ethics statement
The studies involving humans were approved by Comité de Protection des Personnes Est-III, approval number 2020-A00885-34. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin because according to the French law, verbal approval was required from the patient or their relatives. A written informed consent was not required for this study. Written informed consent was not obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article because according to the French law, verbal approval was required from the patient or their relatives, a written informed consent for publication was not required.
Author contributions
DR: Writing – original draft, Writing – review & editing. MV-C: Writing – review & editing. PL: Writing – review & editing. JB: Writing – review & editing. VB: Writing – review & editing. SR: Writing – review & editing. FT: Writing – review & editing. EB: Writing – review & editing. TC: Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2024.1368031/full#supplementary-material
Abbreviations
ARDS, Acute Respiratory Distress Syndrome; AST, Aspartate Aminotransferase; BMI, Body Mass Index; CLP, Cecal Ligation-Puncture; CRP, C-Reactive Protein; CT, Computer Tomography; ER, Endoplasmic Reticulum; ERS, Endoplasmic Reticulum Stress; IQR, Interquartile Range; GRP78, 78 kDa Glucose-Regulated Protein; ICU, Intensive Unit Care; IL-6, Interleukin-6; LDV, Lung Damage Volume; SOFA score, Sequential Organ Failure Assessment score; UPR, Unfolded Protein Response.
References
1. Our World in Data . (2022). COVID-19 data explorer. Available at: https://ourworldindata.org/explorers/coronavirus-data-explorer
2. Mason, RJ . Pathogenesis of COVID-19 from a cell biologic perspective. Eur Respir J. (2020) 55:2000607. doi: 10.1183/13993003.00607-2020
3. Parasher, A . COVID-19: current understanding of its pathophysiology, clinical presentation and treatment. Postgrad Med J. (2021) 97:312–20. doi: 10.1136/postgradmedj-2020-138577
4. Coomes, EA, and Haghbayan, H. Interleukin-6 in Covid-19: a systematic review and meta-analysis. Rev Med Virol. (2020) 30:1–9. doi: 10.1002/rmv.2141
5. Montazersaheb, S, Hosseiniyan Khatibi, SM, Hejazi, MS, Tarhriz, V, Farjami, A, Ghasemian Sorbeni, F, et al. COVID-19 infection: an overview on cytokine storm and related interventions. Virol J. (2022) 19:92. doi: 10.1186/s12985-022-01814-1
6. Peng, S, Chen, J, Zhang, W, Zhang, B, Liu, Z, Liu, L, et al. The role of chest CT quantitative pulmonary inflammatory index in the evaluation of the course and treatment outcome of COVID-19 pneumonia. Sci Rep. (2021) 11:7752. doi: 10.1038/s41598-021-87430-5
7. Wang, C, Huang, L, Xiao, S, Li, Z, Ye, C, Xia, L, et al. Early prediction of lung lesion progression in COVID-19 patients with extended CT ventilation imaging. Eur J Nucl Med Mol Imaging. (2021) 48:4339–49. doi: 10.1007/s00259-021-05435-8
8. Ibrahim, IM, Abdelmalek, DH, and Elfiky, AA. GRP78: a cell’s response to stress. Life Sci. (2019) 226:156–63. doi: 10.1016/j.lfs.2019.04.022
9. Kaufman, RJ . Orchestrating the unfolded protein response in health and disease. J Clin Invest. (2002) 110:1389–98. doi: 10.1172/JCI0216886
10. Khan, MM, Yang, WL, and Wang, P. Endoplasmic reticulum stress in Sepsis. Shock Augusta Ga. (2015) 44:294–304. doi: 10.1097/SHK.0000000000000425
11. Walter, P, and Ron, D. The unfolded protein response: from stress pathway to homeostatic regulation. Science. (2011) 334:1081–6. doi: 10.1126/science.1209038
12. Köseler, A, Sabirli, R, Gören, T, Türkçüer, İ, and Kurt, Ö. Endoplasmic reticulum stress markers in SARS-COV-2 infection and pneumonia: case-control study. In Vivo. (2020) 34:1645–50. doi: 10.21873/invivo.11956
13. Sabirli, R, Koseler, A, Goren, T, Turkcuer, I, and Kurt, O. High GRP78 levels in Covid-19 infection: a case-control study. Life Sci. (2021) 265:118781. doi: 10.1016/j.lfs.2020.118781
14. Puzyrenko, A, Jacobs, ER, Sun, Y, Felix, JC, Sheinin, Y, Ge, L, et al. Pneumocytes are distinguished by highly elevated expression of the ER stress biomarker GRP78, a co-receptor for SARS-CoV-2, in COVID-19 autopsies. Cell Stress Chaperones. (2021) 26:859–68. doi: 10.1007/s12192-021-01230-4
15. Rico-Llanos, G, Porras-Perales, Ó, Escalante, S, Vázquez-Calero, DB, Valiente, L, Castillo, MI, et al. Cellular stress modulates severity of the inflammatory response in lungs via cell surface BiP. Front Immunol. (2022) 13:1054962. doi: 10.3389/fimmu.2022.1054962
16. Shin, WJ, Ha, DP, Machida, K, and Lee, AS. The stress-inducible ER chaperone GRP78/BiP is upregulated during SARS-CoV-2 infection and acts as a pro-viral protein. Nat Commun. (2022) 13:6551. doi: 10.1038/s41467-022-34065-3
17. Besnier, E, Brunel, V, Thill, C, Leprêtre, P, Bellien, J, Demailly, Z, et al. Soluble RAGE as a prognostic marker of worsening in patients admitted to the ICU for COVID-19 pneumonia: a prospective cohort study. J Clin Med. (2022) 11:4571. doi: 10.3390/jcm11154571
18. Li, L, Peng, X, Guo, L, Zhao, Y, and Cheng, Q. Sepsis causes heart injury through endoplasmic reticulum stress-mediated apoptosis signaling pathway. Int J Clin Exp Pathol. (2020) 13:964–71.
19. Qian, WJ, and Cheng, QH. Endoplasmic reticulum stress-mediated apoptosis signal pathway is involved in sepsis-induced liver injury. Int J Clin Exp Pathol. (2017) 10:9990–7.
20. Müllebner, A, Herminghaus, A, Miller, I, Kames, M, Luís, A, Picker, O, et al. Tissue damage, not infection, triggers hepatic unfolded protein response in an experimental rat peritonitis model. Front Med. (2022) 9:785285. doi: 10.3389/fmed.2022.785285
21. Billoir, P, Leprêtre, P, Thill, C, Bellien, J, Le Cam, DV, Selim, J, et al. Routine and advanced laboratory tests for hemostasis disorders in COVID-19 patients: a prospective cohort study. J Clin Med. (2022) 11:1383. doi: 10.3390/jcm11051383
22. Toulouse, E, Granier, S, Nicolas-Robin, A, Bahans, C, Milman, A, Andrieu, VR, et al. The French clinical research in the European Community regulation era. Anaesth Crit Care Pain Med. (2023) 42:101192. doi: 10.1016/j.accpm.2022.101192
23. Grassi, R, Belfiore, MP, Montanelli, A, Patelli, G, Urraro, F, Giacobbe, G, et al. COVID-19 pneumonia: computer-aided quantification of healthy lung parenchyma, emphysema, ground glass and consolidation on chest computed tomography (CT). Radiol Med. (2021) 126:553–60. doi: 10.1007/s11547-020-01305-9
24. Negroni, D, Zagaria, D, Paladini, A, Falaschi, Z, Arcoraci, A, Barini, M, et al. COVID-19 CT scan lung segmentation: how we do it. J Digit Imaging. (2022) 35:424–31. doi: 10.1007/s10278-022-00593-z
25. Gao, Y-d, Ding, M, Dong, X, Zhang, J-j, Kursat Azkur, A, Azkur, D, et al. Risk factors for severe and critically ill COVID-19 patients: a review. Allergy. (2021) 76:428–55. doi: 10.1111/all.14657
26. Zhou, F, Yu, T, Du, R, Fan, G, Liu, Y, Liu, Z, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. (2020) 395:1054–62. doi: 10.1016/S0140-6736(20)30566-3
27. Lazar, M, Barbu, EC, Chitu, CE, Anghel, AMJ, Niculae, CM, Manea, ED, et al. Mortality predictors in severe SARS-CoV-2 infection. Med Kaunas Lith. (2022) 58:945. doi: 10.3390/medicina58070945
28. Canovi, S, Besutti, G, Bonelli, E, Iotti, V, Ottone, M, Albertazzi, L, et al. The association between clinical laboratory data and chest CT findings explains disease severity in a large Italian cohort of COVID-19 patients. BMC Infect Dis. (2021) 21:157. doi: 10.1186/s12879-021-05855-9
29. Fang, Y, Zhang, H, Xie, J, Lin, M, Ying, L, Pang, P, et al. Sensitivity of chest CT for COVID-19: comparison to RT-PCR. Radiology. (2020) 296:E115–7. doi: 10.1148/radiol.2020200432
30. Clavier, T, Demailly, Z, Semaille, X, Thill, C, Selim, J, Veber, B, et al. A weak response to endoplasmic reticulum stress is associated with postoperative organ failure in patients undergoing cardiac surgery with cardiopulmonary bypass. Front Med. (2020) 7:613518. doi: 10.3389/fmed.2020.613518
31. Doerflinger, M, Reljic, B, Menassa, J, Nedeva, C, Jose, I, Faou, P, et al. Circulating BiP/Grp78 is a novel prognostic marker for sepsis-mediated immune cell death. FEBS J. (2021) 288:1809–21. doi: 10.1111/febs.15552
32. Zhou, J, He, W, Liang, J, Wang, L, Yu, X, Bao, M, et al. Association of Interleukin-6 levels with morbidity and mortality in patients with coronavirus disease 2019 (COVID-19). Jpn J Infect Dis. (2021) 74:293–8. doi: 10.7883/yoken.JJID.2020.463
33. Song, J, Finnerty, CC, Herndon, DN, Boehning, D, and Jeschke, MG. Severe burn-induced endoplasmic reticulum stress and hepatic damage in mice. Mol Med Camb Mass. (2009) 15:316–20. doi: 10.2119/molmed.2009.00048
34. Yoshino, J, Almeda-Valdes, P, Moseley, AC, Mittendorfer, B, and Klein, S. Percutaneous muscle biopsy-induced tissue injury causes local endoplasmic reticulum stress. Physiol Rep. (2018) 6:e13679. doi: 10.14814/phy2.13679
35. Yang, C, Guo, J, Ni, K, Wen, K, Qin, Y, Gu, R, et al. Mechanical ventilation-related high stretch mainly induces endoplasmic reticulum stress and thus mediates inflammation response in cultured human primary airway smooth muscle cells. Int J Mol Sci. (2023) 24:3811. doi: 10.3390/ijms24043811
36. Ye, L, Zeng, Q, Dai, H, Zhang, W, Wang, X, Ma, R, et al. Endoplasmic reticulum stress is involved in ventilator-induced lung injury in mice via the IRE1α-TRAF2-NF-κB pathway. Int Immunopharmacol. (2020) 78:106069. doi: 10.1016/j.intimp.2019.106069
37. Heinrich, PC, Behrmann, I, Haan, S, Hermanns, HM, Müller-Newen, G, and Schaper, F. Principles of interleukin (IL)-6-type cytokine signalling and its regulation. Biochem J. (2003) 374:1–20. doi: 10.1042/bj20030407
38. Mote, PL, Tillman, JB, and Spindler, SR. Glucose regulation of GRP78 gene expression. Mech Ageing Dev. (1998) 104:149–58. doi: 10.1016/S0047-6374(98)00064-5
Keywords: COVID-19, endoplasmic reticulum stress, inflammation, interleukin-6, acute respiratory distress syndrome, organ failure, humans, intensive care unit
Citation: Renard D, Verdalle-Cazes M, Leprêtre P, Bellien J, Brunel V, Renet S, Tamion F, Besnier E and Clavier T (2024) Association between volume of lung damage and endoplasmic reticulum stress expression among severe COVID-19 ICU patients. Front. Med. 11:1368031. doi: 10.3389/fmed.2024.1368031
Edited by:
Denise Battaglini, San Martino Hospital (IRCCS), ItalyReviewed by:
Yalim Dikmen, Istanbul University Cerrahpasa, TürkiyeNozomi Takahashi, University of British Columbia, Canada
Leland Shapiro, University of Colorado Anschutz Medical Campus, United States
Copyright © 2024 Renard, Verdalle-Cazes, Leprêtre, Bellien, Brunel, Renet, Tamion, Besnier and Clavier. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Domitille Renard, ZG9taXRpbGxlLnJlbmFyZEBjaHUtcm91ZW4uZnI=