 Giovanna Vieira Giannecchini*
Giovanna Vieira Giannecchini* Jessé Lopes da SilvaGustavo de Oliveira BretasAlexssandra Lima Siqueira dos SantosLais Fernandes Rodrigues BaltarAndreia Cristina de Melo
Jessé Lopes da SilvaGustavo de Oliveira BretasAlexssandra Lima Siqueira dos SantosLais Fernandes Rodrigues BaltarAndreia Cristina de Melo- Oncoclínicas&Co – Medica Scientia Innovation Research (MEDSIR), Sao Paulo, Brazil
By presenting a comprehensive analysis of low-grade serous carcinomas (LGSCs), a subset of epithelial ovarian cancers, this review delves into their distinct molecular characteristics, clinicopathological features and systemic therapy options, emphasizing their differences from high-grade serous carcinomas (HGSCs). Notably, LGSCs exhibit prevalent RAS/RAF/MEK/MAPK pathway activation, KRAS and BRAF mutations, and infrequent p53 mutations. While chemotherapy is commonly employed, LGSCs display lower responsiveness compared to HGSCs. Hormone therapy, particularly endocrine maintenance therapy, is explored due to the higher estrogen receptor expression. Novel therapeutic approaches involving CDK4/6 inhibitors, MEK inhibitors, and antiangiogenic agents like bevacizumab are also investigated. Ongoing clinical trials are striving to enhance LGSC treatment strategies, offering valuable insights for future therapeutic advancements in this challenging ovarian cancer subtype.
1 Introduction
Ovarian cancer (OC) is the seventh most common cancer in women worldwide (1). In 2020, approximately 314,000 women were diagnosed with this neoplasm and 207,000 died from the disease (2).
Based on the component from which OC originates, it can be classified into epithelial carcinoma, germ cell tumor and sex cord-stromal tumor. The most common are the epithelial carcinomas, which accounts for about 90% of ovarian tumors (1).
Previously regarded as a singular entity, epithelial ovarian cancers (EOCs) are now increasingly acknowledged as a diverse collection of tumors encompassing various histologic subcategories. These subtypes are characterized by their unique immunohistochemical, histopathological, and molecular attributes (3). The main classification of EOCs encompasses five distinct subtypes, namely high-grade serous carcinomas (HGSCs), endometrioid carcinomas, clear-cell carcinomas, mucinous carcinomas, and low-grade serous carcinomas (LGSCs) (4). In contrast to HGSCs, which constitute approximately 70–80% of all malignant ovarian tumors, LGSCs are infrequent and account for less than 5% of cases (5–7). It is important to note that the exact prevalence of LGSC is subject to significant variability due to historical inconsistencies in defining this subgroup (8).
Low-grade serous carcinomas exhibit particularities in clinical behavior, chemo responsiveness and molecular profile (9). As a rare subtype, it is difficult to compare the efficacy of different systemic therapies since there are few randomized trials to establish an evidence-based standard treatment. Consequently, there is no uniform approach and uncertainties regarding the use of current treatments are faced (10).
The aim of this study is to comprehensively examine the landscape of systemic therapy for LGSC, recognizing its distinctive clinicopathological features, molecular profile, and clinical behavioral patterns compared to other ovarian tumor subtypes. In addition to gaining an in-depth understanding of this specific context, the investigation also sought to uncover novel insights that could guide future therapeutic strategies. To accomplish this, a search for relevant literature was conducted utilizing MEDLINE databases, renowned for their comprehensive coverage of healthcare and medical research information. A search on ClinicalTrials.gov to pull up ongoing studies in the field was also performed.
2 Pathology
The existing delineation of ovarian serous carcinoma into high-grade or low-grade subgroups relies on the 2004 proposition made by Malpica et al. and the MD Anderson Cancer Center (MDACC) employing a two-tier system (11). This proposes that the classification primarily hinges on nuclear atypia, supplemented by the secondary characteristic of the mitotic rate. Under this binary framework, tumors displaying mild to moderate nuclear atypia and a mitotic index of up to 12 mitoses per 10 high-powered fields are categorized as LGSCs. Subsequent studies have further validated and solidified this binary classification, demonstrating its enhanced reproducibility and prognostic value compared to the previously suggested three-tier grading system, thereby fostering its widespread adoption globally (12–15).
Low-grade serous carcinomas typically present as a uniform population of cuboidal or low-columnar cells, occasionally demonstrating a flattened morphology, and showcasing an amphophilic or lightly eosinophilic cytoplasm (11). Immunohistochemical staining assumes pivotal importance in the pathological assessment. PAX-2 is markedly expressed in 50% of LGSC cases, contrasting with its absence in HGSCs (16). Estrogen receptors (ER) show frequent expression, and in certain cases, progesterone receptors (ProR) and E-cadherin may also exhibit expression (17). Approximately 28% of patients display Her-2/neu expression, while c-kit is positive in 4.5% of cases (18).
Low-grade serous carcinoma can emerge either de novo or as a progression from a serous borderline tumor (SBT). The pathogenesis follows a sequential and gradual development, starting from a serous cystadenoma or adenofibroma, progressing to a SBT with invasive or noninvasive implants, and eventually culminating in the formation of LGSC (15). However, there is ongoing controversy regarding the cells’ origin for LGSC. Some researchers propose that LGSC originates from the fallopian tube rather than the ovary (19). According to this theory, the epithelial inclusion glands are more likely of tubal origin due to the invagination of the ovarian surface epithelium with metaplasia (20). The tubal epithelia near the fimbriated end attach to the ovarian surface, facilitated by chronic inflammation, ovulation, and nonovulation-induced disruption of the ovarian surface. The adherent tubal epithelia have the potential to invaginate into the ovarian cortex, forming ovarian epithelial inclusions, which could be the precursor lesions for serous cystadenoma, SBT, and ultimately LGSC. Additionally, a tubal pathway of pathogenesis has been proposed, suggesting that papillary tubal hyperplasia (PTH) serves as the origin for SBT, noninvasive implants, and endosalpingiosis (20). Finally, a non-PTH tubal pathway may also contribute to the development of these lesions, where normal tubal epithelium exfoliates and implants on the peritoneum or ovary (19).
3 Molecular fingerprint
In the evolving landscape of oncology, precision and targeted approaches are becoming increasingly vital. Beyond the traditional reliance on histological classification, a thorough understanding of the molecular characteristics of LGSCs is essential for accurate diagnosis and holds significant prognostic and therapeutic relevance (21). Herein, the focus is to describe the molecular alterations in LGSCs and point out their differences from HGSCs. All this knowledge comprehends targetable therapeutic opportunities for clinical studies.
Low-grade serous carcinomas are more likely to have constitutive activation of the RAS/RAF/MEK/MAPK pathway, while HGSC is more likely to have constitutive activation of the PI3K/AKT/mTOR pathway (22–25).
Molecular alterations in the RAS/RAF/MEK/MAPK pathway are highly prevalent in LGSCs. About two-thirds of LGSCs have some molecular alteration in this pathway, and about 50% harbor KRAS mutations (26).
KRAS mutations in LGSCs vary from 18 to 54% and are the most common genetic alterations in those tumors. These mutations lead to constitutive activation of the RAS pathway, which promotes uncontrolled growth and proliferation (24, 27, 28). However, the prognostic value of KRAS mutations seems to be less elucidated than BRAF mutations (29).
The mitogen-activated protein kinase (MAPK) pathway is important for some vital cellular functions, such as differentiation, proliferation, survival, autophagy, and apoptosis. BRAF mutations result in constitutive activation of this pathway and a downstream activation of kinases, resulting in uncontrolled cellular growth and carcinogenesis (30). In LGSCs, the frequency of these genetic mutations ranges from 2 to 35% and is infrequent in HGSCs. There has been an indication that BRAF mutations, particularly the V600E type, are associated to a favorable outcome in surgically treated patients and are seldom observed in LGSC patients necessitating systemic therapy. Assessing the presence of BRAF mutation in newly diagnosed patients with LGSC histology may aid in identifying those unlikely to progress to a more aggressive histology or advanced disease. Nevertheless, further prospective studies are needed to elucidate the clinical utility of this test (23, 24, 28, 31–33).
In contrast to HGSCs, p53 mutations are uncommon in LGSCs (34, 35). While mutations in BRCA1, BRCA2, and other genes associated with homologous DNA repair are closely linked to HGSCs, they do not appear to play a central role in LGSCs (36).
Figure 1 presents a comprehensive portrayal of the PI3K/AKT/mTOR and RAS/RAF/MEK signaling pathways.
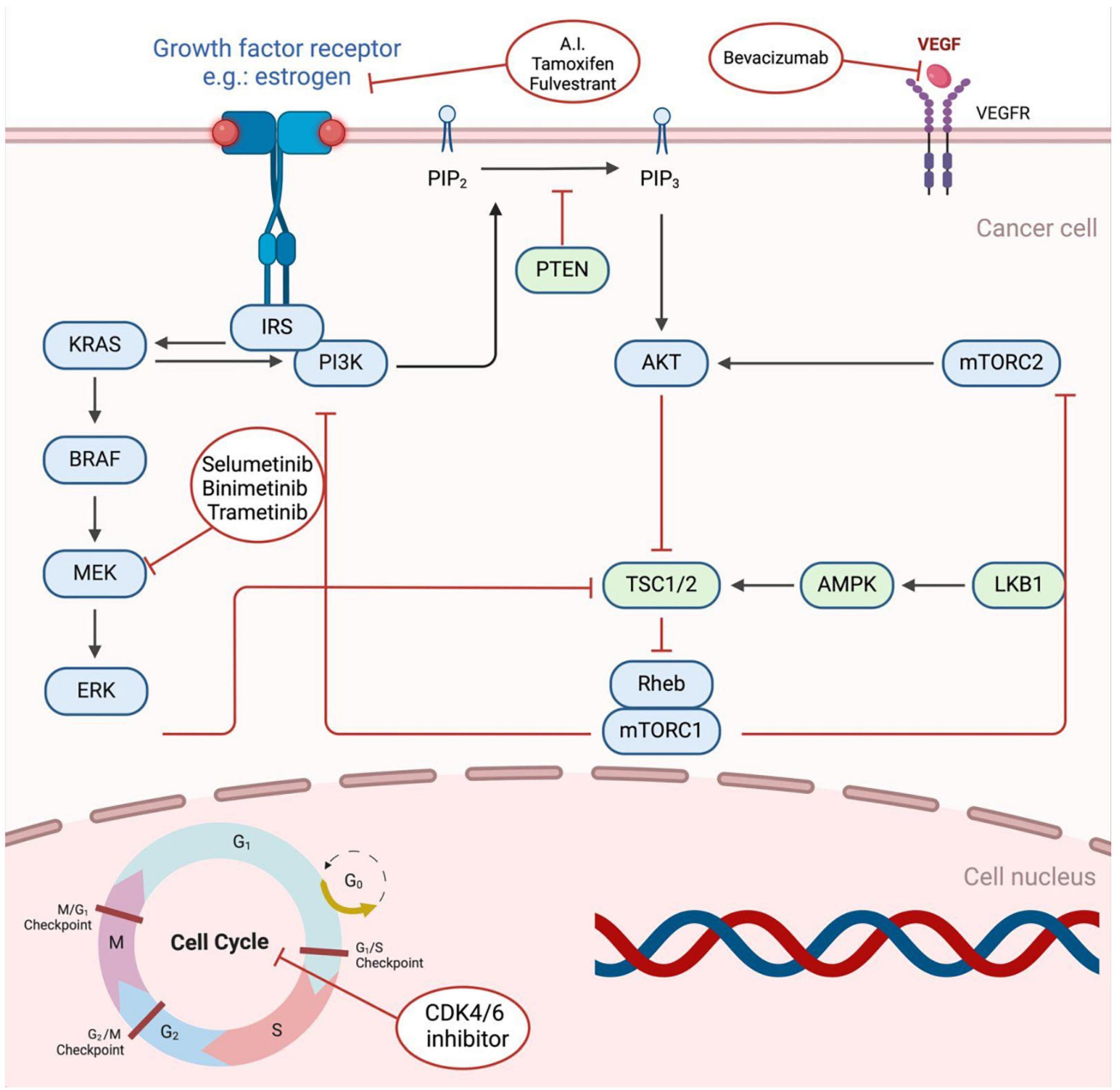
Figure 1. Critical components of the VEGF, Pl3K/AKT/mTOR, and RAS/RAF/MEK signal transduction pathways, as well as the therapeutic interventions employed to target these pathways. Upon ligand binding, the receptors initiate a cascade of signaling events, which are hyperactive in cancerous cells. The diagram provides a visual representation of the key factors involved in these pathways and highlights the therapeutic agents used to intervene in their aberrant activation. Created with BioRender.com.
4 Surgery
The cornerstone treatment for LGSCs is primary cytoreductive surgery (PCS) (37). An additional examination of the GOG 182 trial, involving 189 patients with FIGO stage III-IV LGSC, demonstrated that achieving optimal cytoreduction (defined as residual disease with a maximal diameter of less than 1.0 cm) was linked to improved median progression-free survival (PFS) and overall survival (OS) in comparison to suboptimal cytoreduction (more than 1.0 cm residual disease): 14.7 months versus 14.1 months for PFS and 44.5 months versus 42.0 months for OS (PFS, p < 0.001; OS, p < 0.001) (38). While the primary objective is to attain complete gross resection, given the low chemosensitivity of this disease, PCS is advised, even in cases where complete resection may not be attainable (39).
In the context of recurrence, consideration should be given to secondary cytoreductive surgery (SCS). An analysis of 41 patients with recurrent LGSC in a single-institution retrospective study revealed that individuals who directly underwent SCS at the time of progression or recurrence had a longer median OS of 83.3 months, in comparison to 33.2 months for those who initially received systemic therapy (p = 0.09) (40). Optimal cytoreduction remains the primary objective for SCS. A systematic review by Goldberg et al. indicated prolonged PFS and OS in patients who underwent complete cytoreduction, and to a lesser extent, optimal cytoreduction, compared to those with suboptimal cytoreduction (41).
5 Systemic chemotherapy
Systemic therapy plays a crucial role in the management of LGSC, particularly in cases where the disease has spread beyond the ovaries. Two primary approaches for systemic treatment are chemotherapy and hormone therapy. While these treatments aim to control the progression of cancer and improve outcomes, the choice of the treatment regimen depends on various factors, including the stage, patient characteristics, and individualized treatment plans (42–44).
There is no consensus about the standard adjuvant therapy for stage I LGSC. Routinely, observation is recommended for stage IA disease, whereas stage IB and IC has no universally recognized standardized approach, especially for patients with complete surgical staging (45, 46). Chemotherapy with carboplatin alone for six cycles or carboplatin/paclitaxel for a minimum of three cycles or six cycles if FIGO stage IC, as well as endocrine therapy, are plausible options to be discussed individually with the patients (39).
Following cytoreductive surgery for advanced stages (stage II-IV), patients often receive systemic therapy, which commonly consists of a taxane/platinum regimen (43). This treatment regimen is typically administered every 3 weeks for six cycles and may be succeeded by maintenance endocrine therapy. Intraperitoneal chemotherapy or dose-dense paclitaxel/carboplatin chemotherapy have not demonstrated any established advantages over standard chemotherapy (47, 48).
Despite the widespread use of adjuvant chemotherapy in these patients, studies consistently show the relatively lower responsiveness of this subtype to taxane/platinum chemotherapy compared to HGSCs, with reported response rates ranging from 4 to 23% in newly diagnosed women with stage II to IV LGSCs (49).
For patients with metastatic disease at diagnosis and who are not suitable for surgery, primary systemic therapy with cytotoxic chemotherapy is a feasible option, particularly in those with visceral disease. In such cases, conducting an imaging assessment after three cycles of therapy to identify patients who may benefit from interval cytoreductive surgery is recommended (50, 51).
Regarding neoadjuvant chemotherapy (NACT) for stages III-IV, a retrospective cohort study and systematic literature review with meta-analysis involving less common EOCs was conducted in the United States. 1156 patients with LGSC were included and the use of NACT increased from 7.7 to 14.2% during the study period (p = 0.007 for trend) but it was associated with decreased OS compared with PCS (4-year rates, 56.4% versus 81.0%; Hazard Ratio (HR) 2.12; 95% CI, 1.55–2.90) (52).
In a retrospective analysis at Gustave Roussy Institut including 34 patients with LGSC stage IIIb-IV, NACT was administered in 16 patients (47.1%), and complete response (CR) never occurred, which emphasizes the chemoresistance of this disease and the importance of maximum surgical effort (53).
A recently published single-center cohort evaluated 50 patients with LGSC. 58% of the 12 patients with suboptimal residual disease achieved objective responses - 5 partial responses (PRs) and 2 CRs. Only 9% of the 11 patients who had NACT achieved a PR. Overall response rates (ORRs) for platinum-based chemotherapy were 22% in the second line (2 of 9) and 10% in the third line (1 of 10). Primary platinum-based chemotherapy showed moderate activity in LGSC and minimal activity in the recurrent setting, suggesting a need to reconsider platinum sensitivity definitions in LGSC (54).
These findings have highlighted the medical unmet need and the urgency for the development of more efficacious therapeutic approaches for the management of LGSC.
Table 1 provides an overview of published trials on LGSC. Table 2 details the current clinical trials involving LGSC, excluding phase 1 trials and observational studies.
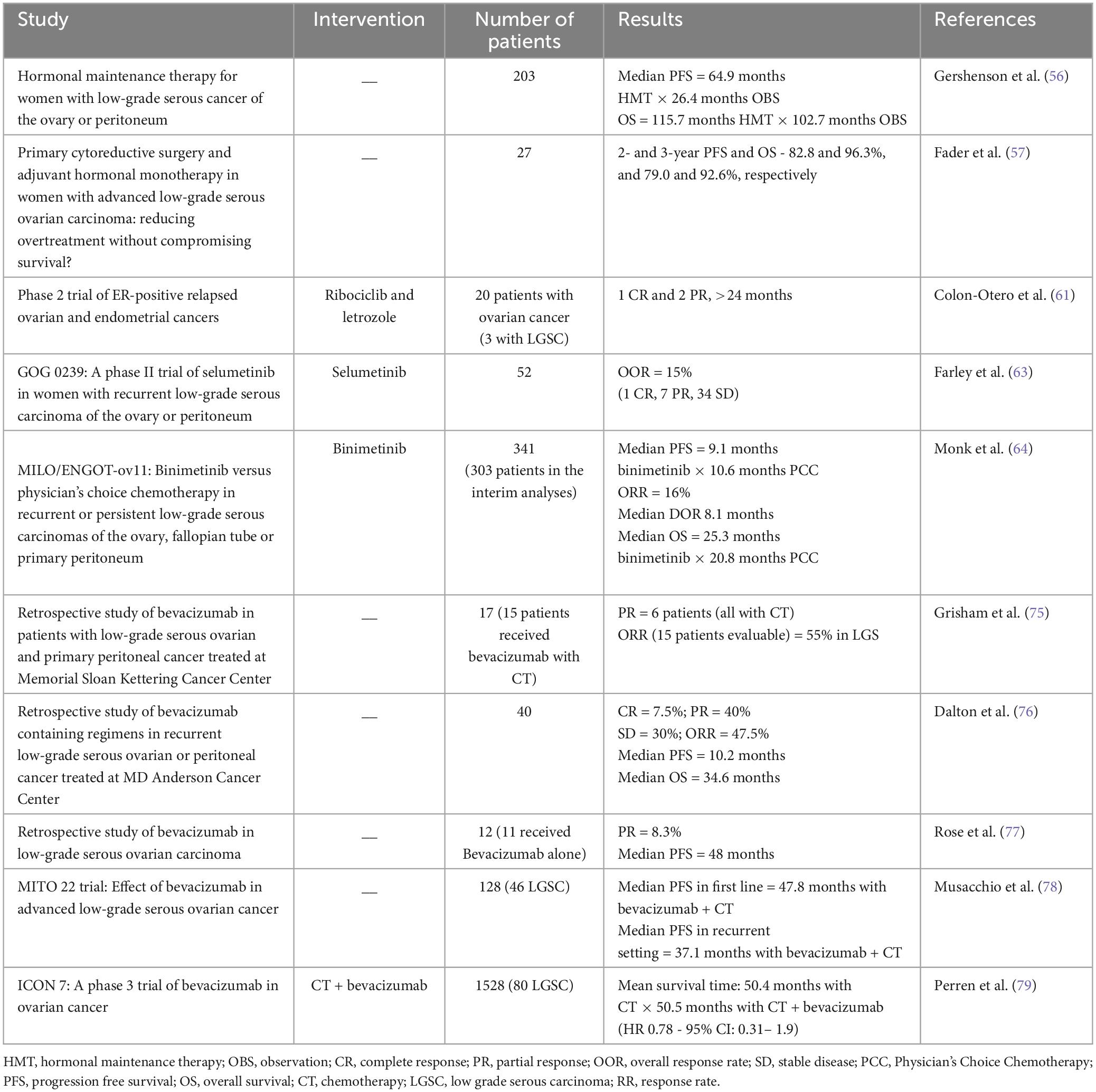
Table 1. Published trials in low-grade serous ovarian carcinoma.
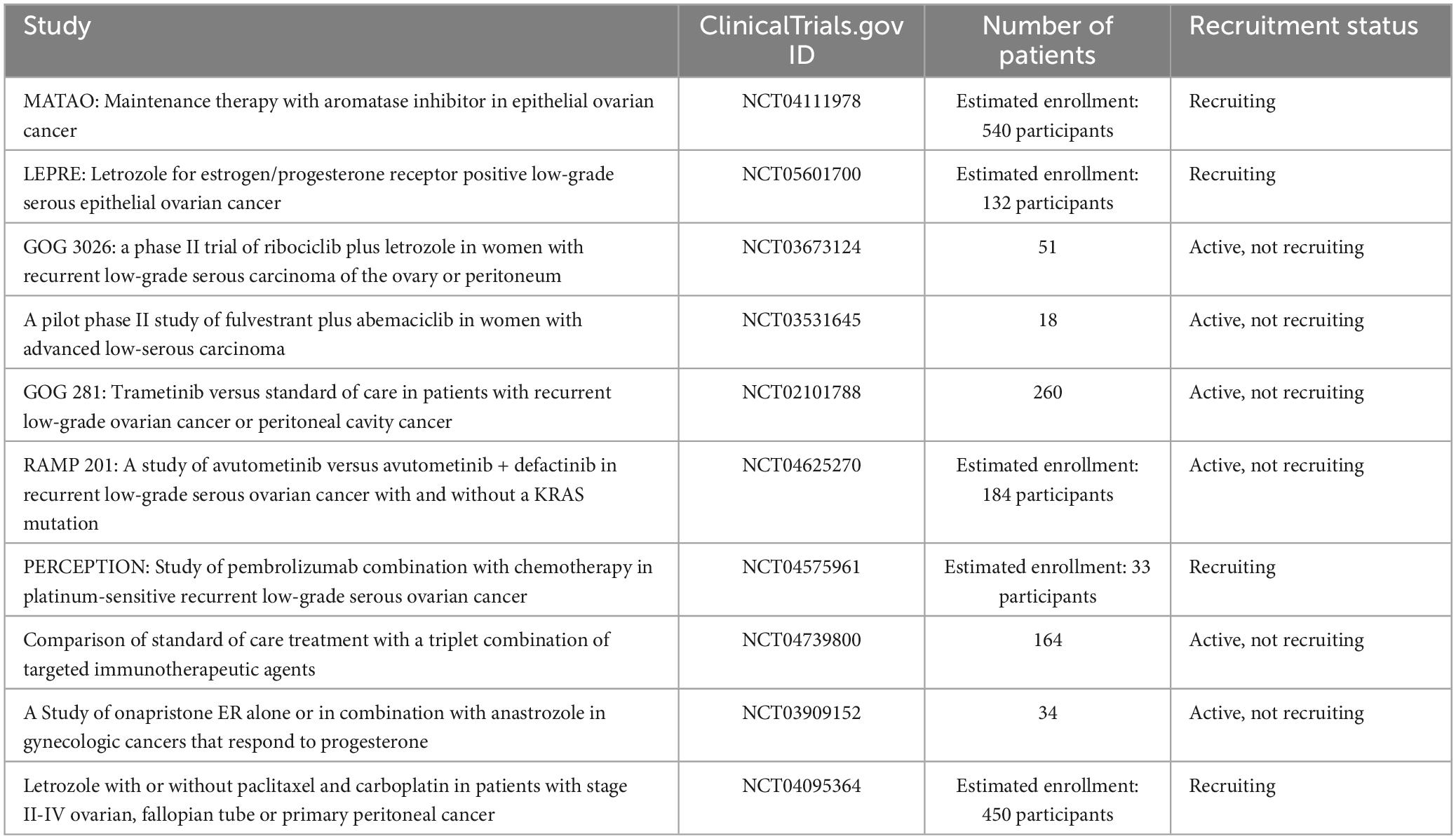
Table 2. Ongoing clinical trials in low-grade serous ovarian carcinoma (excluded phase I and observational trials).
6 Hormone therapy in sequencing systemic treatment
As demonstrated, a very high proportion of LGSCs demonstrate expression of the ER (55). In this scenario, anti-estrogen therapies such as aromatase inhibitors, tamoxifen and fulvestrant are potential treatments.
Therefore, in patients undergoing adjuvant chemotherapy, there might be a potential advantage in utilizing maintenance endocrine therapy, although prospective evidence is required. Gershenson et al. demonstrated in a retrospective study with women diagnosed with stage II to IV LGSCs, that endocrine maintenance therapy after completing primary chemotherapy improved median PFS compared to those who underwent observation alone – 64.9 months (95% CI, 43.5–86.3) versus 26.4 months (95% CI, 21.8–31.0), p < 0.001. There was no significant difference in OS, median of 115.7 months versus 102.7 months; p = 0.42 (56).
Another approach currently being explored is adjuvant endocrine therapy as a substitute for adjuvant chemotherapy. In a retrospective study, Fader et al. analyzed 27 women with LGSC stage II-IV that underwent cytoreductive surgery followed by endocrine monotherapy, without receiving any adjuvant chemotherapy. Optimal cytoreduction, resulting in the absence of visible residual disease, was achieved in 85.2% of patients. Following a median follow-up period of 41 months, 2- and 3-year PFS and OS were 82.8 and 96.3%, and 79.0 and 92.6%, respectively (57).
There are some ongoing international phase 3 clinical trials evaluating endocrine therapy in women with LGSCs. The MATAO trial (NCT04111978) is recruiting participants to investigate the efficacy of the addition of letrozole in maintenance therapy in women with ER-positive high- and low-grade epithelial ovarian cancer after standard surgery and chemotherapy. LEPRE trial (NCT05601700) is a phase 3 study that is recruiting women with advanced ER- and/or ProR-positive low-grade serous epithelial ovarian cancer to compare letrozole with standard chemotherapy (carboplatin plus paclitaxel). NRG-GY-019 (NCT04095364) is currently enrolling participants and aims to compare the effectiveness of platinum/taxane chemotherapy followed by letrozole maintenance therapy with letrozole monotherapy in women diagnosed with stage II-IV ovarian, fallopian tube or primary peritoneal cancer (including LGSC) who have undergone PCS.
7 Cyclin-dependent kinases 4/6 inhibitors
Cyclin-dependent kinases 4/6 (CDK 4/6) play an essential role in regulating cell cycle progression. They bind to the ER-regulated cyclin D1 and mediate the cellular transition from G1 to S phase (58).
In metastatic luminal breast cancer, the role of CDK 4/6 inhibitors in combination with endocrine therapy is well established, with phase 3 studies demonstrating significant improvements in PFS and OS (59). As LGSC presents similarities to hormone receptor-positive breast cancer (60), studies are being developed to evaluate the efficacy of this combination in this scenario.
A phase 2 clinical trial with 40 patients investigated the combination of the CDK4/6 inhibitor ribociclib and the aromatase inhibitor letrozole in the treatment of relapsed ER-positive ovarian and endometrial cancer. Three patients with LGSCs were included and all three obtained durable responses, one CR and two PRs lasting over 2 years (61).
The GOG 3026 (NCT03673124) is a phase 2 trial that evaluated the combination of ribociclib and letrozole in patients with recurrent LGSC. None of the included patients had received prior letrozole or a CDK4/6 inhibitor. The ORR was 23%, with a median duration of response (DOR) of 19.1 months, and 64% of patients experienced a reduction in target lesions. The median PFS was 19.1 months. Such results are promising in a scenario of limited therapeutic options (62).
NCT03531645 is also a phase 2 trial evaluating the role of fulvestrant in combination with abemaciclib in women with advanced LGSCs. This study is still active and will provide important information on the potential of this combination.
8 MEK inhibitors
Targeting the MAPK pathway has shown to be a therapeutic opportunity and MEK inhibitors have been evaluated in LGSCs.
Selumetinib, an inhibitor of MEK 1/2, was investigated in a phase 2 study in which 52 women with recurrent LGSC or peritoneal carcinoma were treated until disease progression. The ORR was 15%, with one CR, seven PRs and 34 patients with stable disease (SD) (63).
Other MEK inhibitors have also been evaluated. The MILO/ENGOT-ov11 study was a phase 3 trial that compared binimetinib versus physician’s choice chemotherapy (pegylated liposomal doxorubicin, paclitaxel, or topotecan) in patients with persistent or recurrent LGSC of the ovary, fallopian tube, or primary peritoneum. Median PFS was 9.1 months for binimetinib and 10.6 months for chemotherapy, which resulted in early study closure; however, the MEK inhibitor showed activity in LGSC, with ORR of 16%, median DOR of 8.1 months and median OS of 25.3 months. Patients with KRAS mutations had better responses to binimetinib (64).
The GOG 281 is a phase 2/3 trial where patients with recurrent LGSC who had received at least one platinum-based regimen were randomly assigned to receive the oral MEK inhibitor trametinib or the physician’s choice of standard of care therapy (weekly paclitaxel, pegylated liposomal doxorubicin, topotecan, letrozole or tamoxifen). The median PFS was 13 months for trametinib versus 7.2 months for standard of care (HR 0.48; 95% CI 0.36–0.64; p < 0.0001). The ORR for the trametinib group was 26%, and a median DOR of 13.6 months versus an ORR of 6% and a median DOR of 5.9 months for standard therapy. Median OS was 37.6 months in the trametinib group and 29.2 months in the standard treatment group, with a HR for death of 0.76 (95% CI 0.51–1.12; p 0.056), but the trial allowed cross-over to trametinib after disease progression. Regarding the mutational status, KRAS, BRAF and NRAS mutations were not predictive for PFS. ORR was better for trametinib than the standard of care in mutation-positive than in mutation-negative tumors but not reaching statistical significance (65).
In a multicentre retrospective study in the United Kingdom that included 28 patients with recurrent LGSC treated with trametinib, the median duration of treatment was 5.0 months, with PR, SD, and disease progression (DP) in 21, 32, and 36% of patients, respectively. These real-world response rates were similar to that reported in GOG 281, confirming the effectiveness of these MEK inhibitor in LGSC (66).
9 Antiangiogenic agents
Angiogenesis plays a significant role in tumor growth and metastasis, being considered one of the hallmarks of cancer (67). Bevacizumab is a humanized anti-VEGF-A monoclonal antibody and works as an anti-angiogenic drug that is approved in many countries for the treatment of ovarian (mostly high-grade) and other cancers. While bevacizumab has shown benefits in HGSC, its use in LGSC is still a topic of ongoing research and clinical evaluation. Most available evidence comes from subgroup analyses, small retrospective studies, and several case reports (68–74).
The Memorial Sloan Kettering Cancer Center published a series describing patients with recurrent LGSC or serous borderline treated with bevacizumab between 2005 and 2012. Only 17 patients were reported, and most received bevacizumab plus chemotherapy agents. The mean number of prior cytotoxic therapies was 3.4 (range 1–9; median 2). The median duration of bevacizumab administration in evaluable patients was 23 weeks (mean 32.2 weeks; range 6–79.4). There were no CRs, and PRs were observed in 6 patients (5 received concurrent paclitaxel, and 1 received concurrent gemcitabine). The ORR was 40%, with a response rate of 55% amongst the subgroup of patients with LGSCs (75).
The MD Anderson Cancer Center also published their retrospective experience with bevacizumab in recurrent LGSC of the ovary. A total of 40 patients were reported, and the median number of prior regimens was 4 (range 1–15). The average duration of bevacizumab treatment was 4 months, with a range of 0.8–25.4 months. CRs were seen in 7.5% of patients, 40.0% had PRs, while 30.0% achieved SD. DP occurred in 22.5%, and clinical benefit was achieved in 77.5% of patients (76).
The Cleveland Clinic or MetroHealth Medical Center in Cleveland retrospectively published their data on the use of bevacizumab in LGSC. Twelve patients were reported, and 11 of those received bevacizumab alone. The ORR was only 8.3%, but the median PFS was 48 months (range 5–123). The median OS was not reached at a median follow-up of 32 months, with only 1 of the 12 patients dying of disease (77).
In a retrospective observational multicenter study, the authors explored the efficacy of bevacizumab on survival outcomes in women with LGSC both in first-line and recurrent settings, comparing the results with those presented by patients who did not receive bevacizumab. A total of 46 out of 128 patients who received bevacizumab in a first-line setting or at the time of first recurrence were identified. In the first-line, 30 patients received bevacizumab plus chemotherapy and 65 chemotherapy alone, and the median PFS was 47.8 months [95% CI 31.48 to not reached (NR)] and 22.6 months (95% CI 15–39.24), p = 0.0392, respectively. In the recurrent setting, 16 patients who received bevacizumab plus chemotherapy were compared to 33 women treated with platinum-based chemotherapy. Median PFS was 37.1 months (95% CI 13.42–40.56) and 11.2 months (95% CI 8.26–15.63), p = 0.013, respectively, suggesting that bevacizumab might be an effective drug both in diagnosis and in relapse (78).
In the ICON7 study (79), which investigated the benefits of adding bevacizumab in the first-line setting, only 80 patients with LGSC were included. The addition of bevacizumab resulted in a non-significant HR of 0.78 (95% CI 0.31–1.97; p = 0.07) in the sub-analysis (80).
10 Conclusion
In conclusion, this thorough review underscores the evolving understanding of LGSCs within the broader context of ovarian cancers. Since it is a rare disease, with few randomized studies, this narrative review was representative in including data on real-world experience, with descriptions of retrospective cohort studies, series of cases, and experience from single centers.
Investigating the distinctive molecular profile, histopathological characteristics, and clinical behavior of LGSC has revealed its unique nature in contrast to HGSC. The higher prevalence of RAS/RAF/MEK/MAPK pathway activation, KRAS and BRAF mutations, and limited p53 involvement provide a foundation for targeted therapies. The challenges in chemotherapy response emphasize the need for innovative treatment strategies. Hormone therapy, mainly endocrine maintenance therapy, offers a promising avenue due to the higher ER expression. Moreover, the investigation into CDK4/6 inhibitors, MEK inhibitors, and antiangiogenic agents unveils potential therapeutic directions for LGSC management. Ongoing clinical trials further highlight these prospects and encourage continued research. Throughout the execution of these studies, the creation of a biorepository for collection and storage of human biological material is essential for ethical purposes and to standardize protocols aiming reliable and reproducible research data.
Finally, the present study humbly underlines the imperative of a multidisciplinary approach to tackle the challenges posed by LGSCs. By dissecting the intricate interplay of molecular characteristics and therapeutic options, this review highlights that the way for more targeted, effective, and personalized treatments should be prioritized in order to improve the prognosis and quality of life for patients with this unique ovarian cancer subtype.
Author contributions
GG: Investigation, Writing – original draft, Project administration, Writing – review and editing. JS: Writing – review and editing, Investigation, Writing – original draft. GO: Investigation, Writing – original draft, Writing – review and editing. AS: Investigation, Writing – original draft, Writing – review and editing. LB: Investigation, Writing – original draft, Writing – review and editing. AM: Conceptualization, Supervision, Writing – review and editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
The authors would like to recognize the contributions of the researchers whose studies, accessible via PubMed, have paved the way for innovative therapeutic strategies for low-grade ovarian tumors. Their research has served as a cornerstone for the discussions and recommendations presented within this review.
Conflict of interest
GG, JS, GO, AS, LB, and AM were employed by company Oncoclínicas&Co – Medica Scientia Innovation Research (MEDSIR).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Gaona-Luviano P, Medina-Gaona LA, Magaña-Pérez K. Epidemiology of ovarian cancer. Chin Clin Oncol. (2020) 9:47. doi: 10.21037/cco-20-34
2. Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. (2021) 71:209–49. doi: 10.3322/caac.21660
3. Tavassoli FA, Devilee P. World health organization classification of tumours. Pathology and genetics of tumours of the breast and female genital organs. Lyon: IARC Press (2003). p. 117–39.
4. Köbel M, Kang EY. The evolution of ovarian carcinoma subclassification. Cancers (Basel). (2022) 14:416. doi: 10.3390/cancers14020416
5. Gershenson DM, Sun CC, Lu KH, Coleman RL, Sood AK, Malpica A, et al. Clinical behavior of stage II-IV low-grade serous carcinoma of the ovary. Obstet Gynecol. (2006) 108:361–8. doi: 10.1097/01.AOG.0000227787.24587.d1
6. Köbel M, Kalloger SE, Huntsman DG, Santos JL, Swenerton KD, Seidman JD, et al. Differences in tumor type in low-stage versus high-stage ovarian carcinomas. Int J Gynecol Pathol. (2010) 29:203–11. doi: 10.1097/PGP.0b013e3181c042b6
7. Matsuo K, Machida H, Grubbs BH, Sood AK, Gershenson DM. Trends of low-grade serous ovarian carcinoma in the United States. J Gynecol Oncol. (2018) 29:e15. doi: 10.3802/jgo.2018.29.e15
8. Seidman JD, Horkayne-Szakaly I, Haiba M, Boice CR, Kurman RJ, Ronnett BM. The histologic type and stage distribution of ovarian carcinomas of surface epithelial origin. Int J Gynecol Pathol. (2004) 23:41–4. doi: 10.1097/01.pgp.0000101080.35393.16
9. Leary AF, Quinn M, Fujiwara K, Coleman RL, Kohn E, Sugiyama T, et al. Fifth ovarian cancer consensus conference of the gynecologic cancer InterGroup (GCIG): Clinical trial design for rare ovarian tumours. Ann Oncol. (2017) 28:718–26. doi: 10.1093/annonc/mdw662
10. Scott SA, Llaurado Fernandez M, Kim H, Elit L, Nourmoussavi M, Glaze S, et al. Low-grade serous carcinoma (LGSC): A Canadian multicenter review of practice patterns and patient outcomes. Gynecol Oncol. (2020) 157:36–45. doi: 10.1016/j.ygyno.2020.01.021
11. Malpica A, Deavers MT, Lu K, Bodurka DC, Atkinson EN, Gershenson DM, et al. Grading ovarian serous carcinoma using a two-tier system. Am J Surg Pathol. (2004) 28:496–504. doi: 10.1097/00000478-200404000-00009
12. Seidman JD, Horkayne-Szakaly I, Cosin JA, Ryu HS, Haiba M, Boice CR, et al. Testing of two binary grading systems for FIGO stage III serous carcinoma of the ovary and peritoneum. Gynecol Oncol. (2006) 103:703–8. doi: 10.1016/j.ygyno.2006.05.030
13. Bodurka DC, Deavers MT, Tian C, Sun CC, Malpica A, Coleman RL, et al. Reclassification of serous ovarian carcinoma by a 2-tier system: A gynecologic oncology group study. Cancer. (2012) 118:3087–94. doi: 10.1002/cncr.26618
14. Fader AN, Java J, Krivak TC, Bristow RE, Tergas AI, Bookman MA, et al. The prognostic significance of pre- and post-treatment CA-125 in grade 1 serous ovarian carcinoma: A gynecologic Oncology Group study. Gynecol Oncol. (2014) 132:560–5. doi: 10.1016/j.ygyno.2013.11.016
15. Kurman RJ, Shih IM. The dualistic model of ovarian carcinogenesis: Revisited, revised, and expanded. Am J Pathol. (2016) 186:733–47. doi: 10.1016/j.ajpath.2015.11.011
16. Tung CS, Mok SC, Tsang YTM, Zu Z, Song H, Liu J, et al. PAX2 expression in low malignant potential ovarian tumors and low-grade ovarian serous carcinomas. Mod Pathol. (2009) 22:1243–50. doi: 10.1038/modpathol.2009.92
17. Llaurado Fernandez M, Dawson A, Kim H, Lam N, Russell H, Bruce M, et al. Hormone receptor expression and outcomes in low-grade serous ovarian carcinoma. Gynecol Oncol. (2020) 157:12–20. doi: 10.1016/j.ygyno.2019.11.029
18. Wong KK, Lu KH, Malpica A, Bodurka DC, Shvartsman HS, Schmandt RE, et al. Significantly greater expression of ER, PR, and ECAD in advanced-stage low-grade ovarian serous carcinoma as revealed by immunohistochemical analysis. Int J Gynecol Pathol. (2007) 26:404–9. doi: 10.1097/pgp.0b013e31803025cd
19. Wang Y, Hong S, Mu J, Wang Y, Lea J, Kong B, et al. Tubal origin of “ovarian” low-grade serous carcinoma: A gene expression profile study. J Oncol. (2019) 2019:8659754. doi: 10.1155/2019/8659754
20. Vang R, Shih IM, Kurman RJ. Fallopian tube precursors of ovarian low– and high-grade serous neoplasms. Histopathology. (2013) 62:44–58. doi: 10.1111/his.12046
21. Shih IM, Kurman RJ. Ovarian tumorigenesis: A proposed model based on morphological and molecular genetic analysis. Am J Pathol. (2004) 164:1511–8. doi: 10.1016/s0002-9440(10)63708-x
22. Cheaib B, Auguste A, Leary A. The PI3K/Akt/mTOR pathway in ovarian cancer: Therapeutic opportunities and challenges. Chin J Cancer. (2015) 34:4–16. doi: 10.5732/cjc.014.10289
23. Jones S, Wang TL, Kurman RJ, Nakayama K, Velculescu VE, Vogelstein B, et al. Low-grade serous carcinomas of the ovary contain very few point mutations. J Pathol. (2012) 226:413–20. doi: 10.1002/path.3967
24. Singer G, Oldt R III, Cohen Y, Wang BG, Sidransky D, Kurman RJ, et al. Mutations in BRAF and KRAS characterize the development of low-grade ovarian serous carcinoma. J Natl Cancer Inst. (2003) 95:484–6. doi: 10.1093/jnci/95.6.484
25. Therachiyil L, Anand A, Azmi A, Bhat A, Korashy HM, Uddin S. Role of RAS signaling in ovarian cancer. F1000Research. (2022) 11:1253. doi: 10.12688/f1000research.126337.1
26. Zarei S, Wang Y, Jenkins SM, Voss JS, Kerr SE, Bell DA. Clinicopathologic, immunohistochemical, and molecular characteristics of ovarian serous carcinoma with mixed morphologic features of high-grade and low-grade serous carcinoma. Am J Surg Pathol. (2020) 44:316–28. doi: 10.1097/PAS.0000000000001419
27. Singer G, Kurman RJ, Chang HW, Cho SK, Shih IM. Diverse tumorigenic pathways in ovarian serous carcinoma. Am J Pathol. (2002) 160:1223–8. doi: 10.1016/s0002-9440(10)62549-7
28. Wong KK, Bateman NW, Ng CW, Tsang YTM, Sun CS, Celestino J, et al. Integrated multi-omic analysis of low-grade ovarian serous carcinoma collected from short and long-term survivors. J Transl Med. (2022) 20:606. doi: 10.1186/s12967-022-03820-x
29. Gershenson DM, Sun CC, Wong KK. Impact of mutational status on survival in low-grade serous carcinoma of the ovary or peritoneum. Br J Cancer. (2015) 113:1254–8. doi: 10.1038/bjc.2015.364
30. Shan KS, Rehman TU, Ivanov S, Domingo G, Raez LE. Molecular targeting of the BRAF proto-oncogene/mitogen-activated protein kinase (MAPK) pathway across cancers. Int J Mol Sci. (2024) 25:624. doi: 10.3390/ijms25010624
31. Campos MP, Cohen M, Von Euw E, Velculescu V, Kujak JL, Conklin D, et al. BRAF mutations occur infrequently in ovarian cancer but suggest responsiveness to BRAF and MEK inhibition. JCO Precis Oncol. (2018) 2:O.18.00025. doi: 10.1200/PO.18.00025
32. Grisham RN, Iyer G, Garg K, Delair D, Hyman DM, Zhou Q, et al. BRAF mutation is associated with early stage disease and improved outcome in patients with low-grade serous ovarian cancer. Cancer. (2013) 119:548–54. doi: 10.1002/cncr.27782
33. Wong KK, Tsang YTM, Deavers MT, Mok SC, Zu Z, Sun C, et al. BRAF mutation is rare in advanced-stage low-grade ovarian serous carcinomas. Am J Pathol. (2010) 177:1611–7. doi: 10.2353/ajpath.2010.100212
34. Singer G, Stöhr R, Cope L, Dehari R, Hartmann A, Cao DF, et al. Patterns of p53 mutations separate ovarian serous borderline tumors and low- and high-grade carcinomas and provide support for a new model of ovarian carcinogenesis: A mutational analysis with immunohistochemical correlation. Am J Surg Pathol. (2005) 29:218–24. doi: 10.1097/01.pas.0000146025.91953.8d
35. Altman AD, Nelson GS, Ghatage P, McIntyre JB, Capper D, Chu P, et al. The diagnostic utility of TP53 and CDKN2A to distinguish ovarian high-grade serous carcinoma from low-grade serous ovarian tumors. Mod Pathol. (2013) 26:1255–63. doi: 10.1038/modpathol.2013.55
36. Vineyard MA, Daniels MS, Urbauer DL, Deavers MT, Sun CC, Boerwinkle E, et al. Is low-grade serous ovarian cancer part of the tumor spectrum of hereditary breast and ovarian cancer? Gynecol Oncol. (2011) 120:229–32. doi: 10.1016/j.ygyno.2010.10.033
37. Grisham RN, Slomovitz BM, Andrews N, Banerjee S, Brown J, Carey MS, et al. Low-grade serous ovarian cancer: Expert consensus report on the state of the science. Int J Gynecol Cancer. (2023) 33:1331–44. doi: 10.1136/ijgc-2023-004610
38. Nickles Fader A, Java J, Ueda S, Bristow RE, Armstrong DK, Bookman MA, et al. Survival in women with grade 1 serous ovarian carcinoma. Obstet Gynecol. (2013) 122:225–32. doi: 10.1097/AOG.0b013e31829ce7ec
39. González-Martín A, Harter P, Leary A, Lorusso D, Miller RE, Pothuri B, et al. Newly diagnosed and relapsed epithelial ovarian cancer: ESMO clinical practice guideline for diagnosis, treatment and follow-up. Ann Oncol. (2023) 34:833–48. doi: 10.1016/j.annonc.2023.07.011
40. Crane EK, Sun CC, Ramirez PT, Schmeler KM, Malpica A, Gershenson DM. The role of secondary cytoreduction in low-grade serous ovarian cancer or peritoneal cancer. Gynecol Oncol. (2015) 136:25–9. doi: 10.1016/j.ygyno.2014.11.005
41. Goldberg RM, Kim SR, Fazelzad R, Li X, Brown TJ, May T. Secondary cytoreductive surgery for recurrent low-grade serous ovarian carcinoma: A systematic review and meta-analysis. Gynecol Oncol. (2022) 164:212–20. doi: 10.1016/j.ygyno.2021.10.080
42. Grabowski JP, Harter P, Heitz F, Pujade-Lauraine E, Reuss A, Kristensen G, et al. Operability and chemotherapy responsiveness in advanced low-grade serous ovarian cancer. An analysis of the AGO study group metadatabase. Gynecol Oncol. (2016) 140:457–62. doi: 10.1016/j.ygyno.2016.01.022
43. Romero I, Sun CC, Wong KK, Bast RC Jr., Gershenson DM. Low-grade serous carcinoma: New concepts and emerging therapies. Gynecol Oncol. (2013) 130:660–6. doi: 10.1016/j.ygyno.2013.05.021
44. Schmeler KM, Sun CC, Malpica A, Deavers MT, Bodurka DC, Gershenson DM. Low-grade serous primary peritoneal carcinoma. Gynecol Oncol. (2011) 121:482–6. doi: 10.1016/j.ygyno.2011.02.017
45. Colombo N, Sessa C, du Bois A, Ledermann J, McCluggage WG, McNeish I, et al. ESMO-ESGO consensus conference recommendations on ovarian cancer: Pathology and molecular biology, early and advanced stages, borderline tumours and recurrent disease†. Ann Oncol. (2019) 30:672–705. doi: 10.1093/annonc/mdz062
46. Di Lorenzo P, Conteduca V, Scarpi E, Adorni M, Multinu F, Garbi A, et al. Advanced low grade serous ovarian cancer: A retrospective analysis of surgical and chemotherapeutic management in two high volume oncological centers. Front Oncol. (2022) 12:970918. doi: 10.3389/fonc.2022.970918
47. Markman M, Bundy BN, Alberts DS, Fowler JM, Clark-Pearson DL, Carson LF, et al. Phase III trial of standard-dose intravenous cisplatin plus paclitaxel versus moderately high-dose carboplatin followed by intravenous paclitaxel and intraperitoneal cisplatin in small-volume stage III ovarian carcinoma: An intergroup study of the Gynecologic Oncology Group, Southwestern Oncology Group, and Eastern Cooperative Oncology Group. J Clin Oncol. (2001) 19:1001–7. doi: 10.1200/JCO.2001.19.4.1001
48. Jaaback K, Johnson N, Lawrie TA. Intraperitoneal chemotherapy for the initial management of primary epithelial ovarian cancer. Cochrane Database Syst Rev. (2016) 2016:CD005340. doi: 10.1002/14651858.CD005340.pub4
49. Gockley A, Melamed A, Bregar AJ, Clemmer JT, Birrer M, Schorge JO, et al. Outcomes of women with high-grade and low-grade advanced-stage serous epithelial ovarian cancer. Obstet Gynecol. (2017) 129:439–47. doi: 10.1097/AOG.0000000000001867
50. Schmeler KM, Sun CC, Bodurka DC, Deavers MT, Malpica A, Coleman RL, et al. Neoadjuvant chemotherapy for low-grade serous carcinoma of the ovary or peritoneum. Gynecol Oncol. (2008) 108:510–4. doi: 10.1016/j.ygyno.2007.11.013
51. Gershenson DM, Sun CC, Bodurka D, Coleman RL, Lu KH, Sood AK, et al. Recurrent low-grade serous ovarian carcinoma is relatively chemoresistant. Gynecol Oncol. (2009) 114:48–52. doi: 10.1016/j.ygyno.2009.03.001
52. Matsuo K, Matsuzaki S, Maeda M, Rau AR, Yoshihara K, Tamura R, et al. Uptake and outcomes of neoadjuvant chemotherapy among US patients with less common epithelial ovarian carcinomas. JAMA Netw Open. (2023) 6:e2318602. doi: 10.1001/jamanetworkopen.2023.18602
53. Zaccarini F, Roosen A, Sanson C, Maulard A, Scherier S, Pautier P, et al. Carcinome séreux de bas grade ovarien à un stade avancé: Étude rétrospective sur 34 patientes en résection complète [Low-grade serous ovarian carcinoma: A retrospective study on 34 complete cytoreductive surgeries]. Gynecol Obstet Fertil Senol. (2021) 49:750–5. doi: 10.1016/j.gofs.2021.04.009
54. Manning-Geist BL, Kahn RM, Nemirovsky D, Girshman J, Laibangyang A, Gordhandas S, et al. Chemotherapy response in low-grade serous ovarian carcinoma at a comprehensive cancer center: Readdressing the roles of platinum and cytotoxic therapies. Cancer. (2023) 129:2004–12. doi: 10.1002/cncr.34753
55. Escobar J, Klimowicz AC, Dean M, Chu P, Nation JG, Nelson GS, et al. Quantification of ER/PR expression in ovarian low-grade serous carcinoma. Gynecol Oncol. (2013) 128:371–6. doi: 10.1016/j.ygyno.2012.10.013
56. Gershenson DM, Bodurka DC, Coleman RL, Lu KH, Malpica A, Sun CC. Hormonal maintenance therapy for women with low-grade serous cancer of the ovary or peritoneum. J Clin Oncol. (2017) 35:1103–11. doi: 10.1200/JCO.2016.71.0632
57. Fader AN, Bergstrom J, Jernigan A, Tanner EJ III, Roche KL, Stone RL, et al. Primary cytoreductive surgery and adjuvant hormonal monotherapy in women with advanced low-grade serous ovarian carcinoma: Reducing overtreatment without compromising survival? Gynecol Oncol. (2017) 147:85–91. doi: 10.1016/j.ygyno.2017.07.127
58. Goel S, Bergholz JS, Zhao JJ. Targeting CDK4 and CDK6 in cancer. Nat Rev Cancer. (2022) 22:356–72. doi: 10.1038/s41568-022-00456-3
59. Moujaber T, Balleine RL, Gao B, Madsen I, Harnett PR, DeFazio A. New therapeutic opportunities for women with low-grade serous ovarian cancer. Endocr Relat Cancer. (2021) 29:R1–16. doi: 10.1530/ERC-21-0191
60. Cobb L, Gershenson D. Novel therapeutics in low-grade serous ovarian cancer. Int J Gynecol Cancer. (2023) 33:377–84. doi: 10.1136/ijgc-2022-003677
61. Colon-Otero G, Zanfagnin V, Hou X, Foster NR, Asmus EJ, Wahner Hendrickson A, et al. Phase II trial of ribociclib and letrozole in patients with relapsed oestrogen receptor-positive ovarian or endometrial cancers. ESMO Open. (2020) 5:e000926. doi: 10.1136/esmoopen-2020-000926
62. GOG Foundation. GOG 3026 press release. (2023). Available online at: https://www.gog.org/news/gog-3026-press-release/ (accessed June 11, 2023).
63. Farley J, Brady WE, Vathipadiekal V, Lankes HA, Coleman R, Morgan MA, et al. Selumetinib in women with recurrent low-grade serous carcinoma of the ovary or peritoneum: An open-label, single-arm, phase 2 study. Lancet Oncol. (2013) 14:134–40. doi: 10.1016/S1470-2045(12)70572-7
64. Monk BJ, Grisham RN, Banerjee S, Kalbacher E, Mirza MR, Romero I, et al. MILO/ENGOT-ov11: Binimetinib versus physician’s choice chemotherapy in recurrent or persistent low-grade serous carcinomas of the ovary, fallopian tube, or primary peritoneum. J Clin Oncol. (2020) 38:3753–62. doi: 10.1200/JCO.20.01164
65. Gershenson DM, Miller A, Brady WE, Paul J, Carty K, Rodgers W, et al. Trametinib versus standard of care in patients with recurrent low-grade serous ovarian cancer (GOG 281/LOGS): An international, randomised, open-label, multicentre, phase 2/3 trial. Lancet. (2022) 399:541–53. doi: 10.1016/S0140-6736(21)02175-9
66. Shotton R, Ren X, Randhawa M, Tilby M, Vazquez I, Williams S, et al. 743P Real-world outcomes in patients treated with trametinib for low grade serous ovarian carcinoma. Annals of Oncology. (2021) 32:S740. doi: 10.1016/j.annonc.2021.08.1185
67. Hanahan D. Hallmarks of cancer: New dimensions. Cancer Discov. (2022) 12:31–46. doi: 10.1158/2159-8290.CD-21-1059
68. Burger RA, Sill MW, Monk BJ, Greer BE, Sorosky JI. Phase II trial of bevacizumab in persistent or recurrent epithelial ovarian cancer or primary peritoneal cancer: A gynecologic oncology group study. J Clin Oncol. (2007) 25:5165–71. doi: 10.1200/JCO.2007.11.5345
69. Cannistra SA, Matulonis UA, Penson RT, Hambleton J, Dupont J, Mackey H, et al. Phase II study of bevacizumab in patients with platinum-resistant ovarian cancer or peritoneal serous cancer. J Clin Oncol. (2007) 25:5180–6. doi: 10.1200/JCO.2007.12.0782
70. Garcia AA, Hirte H, Fleming G, Yang D, Tsao-Wei DD, Roman L, et al. Phase II clinical trial of bevacizumab and low-dose metronomic oral cyclophosphamide in recurrent ovarian cancer: A trial of the California, Chicago, and princess margaret hospital phase II consortia. J Clin Oncol. (2008) 26:76–82. doi: 10.1200/JCO.2007.12.1939
71. Aghajanian C, Blank SV, Goff BA, Judson PL, Teneriello MG, Husain A, et al. OCEANS: A randomized, double-blind, placebo-controlled phase III trial of chemotherapy with or without bevacizumab in patients with platinum-sensitive recurrent epithelial ovarian, primary peritoneal, or fallopian tube cancer. J Clin Oncol. (2012) 30:2039–45. doi: 10.1200/JCO.2012.42.0505
72. Stark D, Nankivell M, Pujade-Lauraine E, Kristensen G, Elit L, Stockler M, et al. Standard chemotherapy with or without bevacizumab in advanced ovarian cancer: Quality-of-life outcomes from the international collaboration on ovarian neoplasms (ICON7) phase 3 randomised trial. Lancet Oncol. (2013) 14:236–43. doi: 10.1016/S1470-2045(12)70567-3
73. Chan JK, Brady MF, Penson RT, Huang H, Birrer MJ, Walker JL, et al. Weekly vs. every-3-week paclitaxel and carboplatin for ovarian cancer. N Engl J Med. (2016) 374:738–48. doi: 10.1056/NEJMoa1505067
74. Tewari KS, Burger RA, Enserro D, Norquist BM, Swisher EM, Brady MF, et al. Final overall survival of a randomized trial of bevacizumab for primary treatment of ovarian cancer. J Clin Oncol. (2019) 37:2317–28. doi: 10.1200/JCO.19.01009
75. Grisham RN, Iyer G, Sala E, Zhou Q, Iasonos A, DeLair D, et al. Bevacizumab shows activity in patients with low-grade serous ovarian and primary peritoneal cancer. Int J Gynecol Cancer. (2014) 24:1010–4. doi: 10.1097/IGC.0000000000000190
76. Dalton HJ, Fleming ND, Sun CC, Bhosale P, Schmeler KM, Gershenson DM. Activity of bevacizumab-containing regimens in recurrent low-grade serous ovarian or peritoneal cancer: A single institution experience. Gynecol Oncol. (2017) 145:37–40. doi: 10.1016/j.ygyno.2017.01.027
77. Rose PG, Mahdi H, Jernigan A, Yang B. Activity of bevacizumab in patients with low-grade serous ovarian carcinoma. Int J Gynecol Cancer. (2016) 26:1048–52. doi: 10.1097/IGC.0000000000000742
78. Musacchio L, Turinetto M, Arenare L, Bartoletti M, Califano D, Tuninetti V, et al. Effect of bevacizumab in advanced low grade serous ovarian cancer: Data from the MITO 22 trial. Gynecol Oncol. (2023) 172:72–7. doi: 10.1016/j.ygyno.2023.03.011
79. Perren TJ, Swart AM, Pfisterer J, Ledermann JA, Pujade-Lauraine E, Kristensen G, et al. A phase 3 trial of bevacizumab in ovarian cancer. N Engl J Med. (2011) 365:2484–96. doi: 10.1056/NEJMoa1103799
80. Oza AM, Cook AD, Pfisterer J, Embleton A, Ledermann JA, Pujade-Lauraine E, et al. Standard chemotherapy with or without bevacizumab for women with newly diagnosed ovarian cancer (ICON7): Overall survival results of a phase 3 randomised trial. Lancet Oncol. (2015) 16:928–36. doi: 10.1016/S1470-2045(15)00086-8
Keywords: ovarian cancer, low-grade serous carcinoma, molecular features, systemic treatment, novel therapeutic options
Citation: Giannecchini GV, da Silva JL, de Oliveira Bretas G, dos Santos ALS, Baltar LFR and de Melo AC (2024) Exploring novel approaches in the systemic therapy of low-grade serous carcinoma of the ovary: a literature review. Front. Med. 11:1366603. doi: 10.3389/fmed.2024.1366603
Received: 06 January 2024; Accepted: 26 April 2024;
Published: 21 May 2024.
Edited by:
A. Seval Ozgu-Erdinc, Ankara City Hospital, TürkiyeReviewed by:
Zhaochu Wang, The Affiliated People’s Hospital of Fujian University of Traditional Chinese Medicine, ChinaCristiano de Pádua Souza, Barretos Cancer Hospital, Brazil
Copyright © 2024 Giannecchini, da Silva, de Oliveira Bretas, dos Santos, Baltar and de Melo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Giovanna Vieira Giannecchini, Z2lvdmFubmF2Zy45MkBnbWFpbC5jb20=