 Yue Wen
Yue Wen Yang Yu
Yang Yu
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Med. , 11 July 2024
Sec. Nephrology
Volume 11 - 2024 | https://doi.org/10.3389/fmed.2024.1366362
Aims: The health management of end-stage renal disease patients is a complicated process, and mobile health management technology provides a new choice for the health management of end-stage renal disease patients. The scope of clinical studies on mobile health management for patients with end-stage renal disease was reviewed, and found that about mobile health management problems existing in the literature were identified to provide ideas for subsequent mobile health management research.
Methods: The databases Web of Science, PubMed, The Cochrane Library, Embase, CNKI, Wan Fang Data, BMJ, and VIP were systematically searched for studies on Mobile health management among end-stage renal disease in adult and adolescent patients or children undergoing kidney replacement therapy. The search covered the period from the inception of the databases to June 20, 2023. Two independent reviewers conducted the literature screening process. Following eligibility screening, a total of 38 papers were included for data extraction and descriptive analysis.
Results: A total of 38 studies from 14 countries were finally included. The majority of which were interventional trials. The platforms used in these studies included remote monitoring systems, apps, websites, mobile phones or tablets, and social platforms. These platforms provided patients with a wide range of services, including disease management, behavioral intervention, social support, and follow-up care. Most studies focused on patient clinical indicators, patient experience, quality of life, and healthcare costs.
Conclusion: Our findings that mobile health management has been widely used in disease management of end-stage renal disease patients, with rich management content and many evaluation indicators. Future studies should strengthen the evaluation of patients’ mental health, quality of life, and healthcare costs. Additionally, developing a clinical decision support system would enable mobile health management to play a more effective role in end-stage renal disease patients.
As the global population ages at an unprecedented rate, the incidence of chronic diseases is soaring, and chronic kidney disease (CKD) is no exception (1). The more patients suffer from CKD, the more develop end-stage renal disease (ESRD) (2). ESRD is diagnosed when kidney function is insufficient to sustain life without kidney transplantation or dialysis (3), and its prevalence is also rising (4). The treatment of ESRD is complex and demanding, requiring long-term dialysis therapy (hemodialysis or peritoneal dialysis), kidney transplantation, and drug management (5). Patients with ESRD also face a variety of health management challenges, including cardiovascular disease (6) and skin disorders (7), etc.
In contrast to traditional medical models, which require patients go to a hospital for treatment, peritoneal dialysis can now be performed at home, while hemodialysis is typically conducted at a dialysis center via an arteriovenous fistula (which requires months to mature before use), an arteriovenous graft (which can be used in as little as 24 h, depending on the graft material), or a central venous catheter (which can be used immediately, but poses the highest risk of infection). Vascular access is essential for both hemodialysis and peritoneal dialysis, but kidney transplantation remains the preferred treatment for ESRD patients (5).
Mobile health (MHealth) management technology has emerged as a promising method in modern medicine, offering patients more convenient and effective ways to manage their health (8). MHealth leverages mobile devices and other technologies to improve patient engagement, monitoring, outreach, and healthcare services. It is accelerating the modernization of medicine and has been widely adopted for the management of various chronic diseases (9), including diabetes (10), hypertension (11), cancer (12), and others. In this context, MHealth management technology provides a new and innovative approach to the health management of ESRD patients.
However, the health management of ESRD patients is a complex and challenging endeavor, requiring close collaboration between medical institutions, patients (13) and IT services. It’s not just about data protection and data safety, it’s also about how much project funding or budget there is, and bureaucracy is also an obstacle. MHealth management technology, interventions that provide health-related information through telecommunications or other wireless technologies, such as smartphones, tablets (14, 15) telemedicine, can provide patients with more convenient and personalized healthcare solutions, enabling them to better monitor their health status and improve their overall health and quality of life (16). A scope review is an ideal tool to determine the scope or coverage of the body of literature on a given topic and to specify the amount of literature and research available as well as an overview (17). Previous studies that reviewed the scope of lifestyle interventions provided by eHealth in chronic kidney disease found that there is currently insufficient evidence to recommend the implementation of specific lifestyle e-health interventions in the clinical care of people with chronic kidney disease (18), funding or budget problems which gives researchers the direction and focus of future research in chronic kidney disease. Therefore, a scope review on MHealth management for ESRD patients is warranted to better manage ESRD patients.
This study aims to review the scope of mobile health management for patients with end-stage renal disease and to synthesize and analyze relevant domestic and international literature. The application landscape, advantages and disadvantages, development trends, and future prospects of mobile health management technology in ESRD patient management were comprehensively studied and analyzed to provide a reference for the practice of mobile health management for ESRD patients. We envision that mobile health management technology for ESRD patients will continue to develop and improve in the future, providing patients with more convenient and personalized health management services. Simultaneously, we hope that medical institutions and researchers will pay greater attention to the health management of ESRD patients and provide more comprehensive and in-depth support for research and application in this area.
In this study, according to PRISMA Extension for Scoping Reviews (PRISMA-SCR) (19) (see Supplementary file 1) and the Arksey and O’Malley (20) framework of mobile health management in patients with end-stage renal disease in the scope of review. All data can be made available upon reasonable request.
Inclusion criteria ① Subjects: laboratory confirmed patients with end-stage renal disease, regardless of sex, age. ② Study types: randomized controlled trial, non-randomized controlled trial, cohort study, case–control study. ③ Literature sources: journal papers published in peer-reviewed journals and dissertations.
Exclusion criteria ① Repeated publication, full text is not available.
A systematic paper search was conducted in PubMed, Cochrane Library, CNKI, VIP, Web of Science, EMBASE, BMJ, and Wan fang digital journal full-text database, we included all papers which were listed in the different searching tools until day June 20, 2023. The search strategy was: (end-stage renal disease OR ESRD) AND (telemedicine OR telehealth OR eHealth OR mobile health OR MHealth).
Two researchers (WY and RY) rigorously adhered to the inclusion and exclusion criteria for literature screening. First, they reviewed the titles and abstracts of all identified studies, and then carefully read the full text of any studies that potentially met the inclusion criteria. Any disagreements were resolved through discussion or consultation with a third reviewer. Data were extracted from the included studies, including author, publication year, country, study type, sample size, MHealth management interventions, and evaluation indicators, etc.
A total of 676 papers were retrieved from all databases. After 67 duplicate records were removed, among the remaining 609 relevant studies, 523 were excluded due to being object mismatch, thematic incompatibility, comments, minutes of meeting, book or document. The full text of the remaining 86 studies were read and 48 studies were removed after reading the full text due to object mismatch. The remaining 38 papers were extracted from the corresponding data according to the data extraction requirements. The papers screening process is shown in Figure 1.
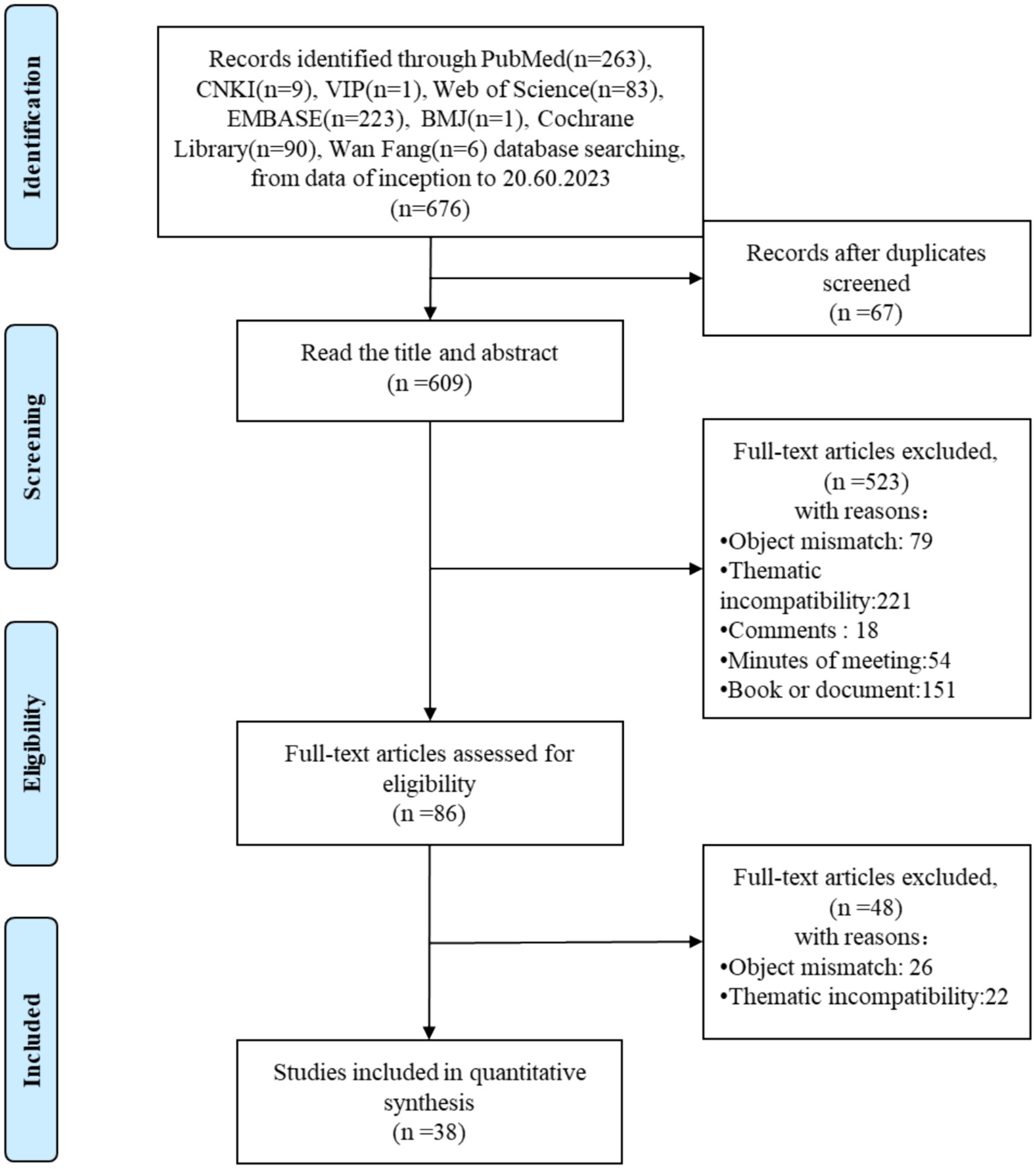
Figure 1. Papers screening process.
The 38 included articles were published between 2003 and 2023, originating from 14 countries, with the United States contributing the most (14 articles, 36.84%), followed by China (7 articles, 18.42%) and Denmark (3 articles, 7.89%). In terms of literature types, 16 were randomized controlled trials, 8 were cohort studies, 11 were qualitative studies, and 3 were meta-analyses/systematic reviews, primarily examining ESRD telecare. According to the treatment methods, 11 studies focused on hemodialysis, 9 on peritoneal dialysis, 11 on kidney transplantation, and 7 on unspecified or multiple dialysis methods (Tables 1, 2).
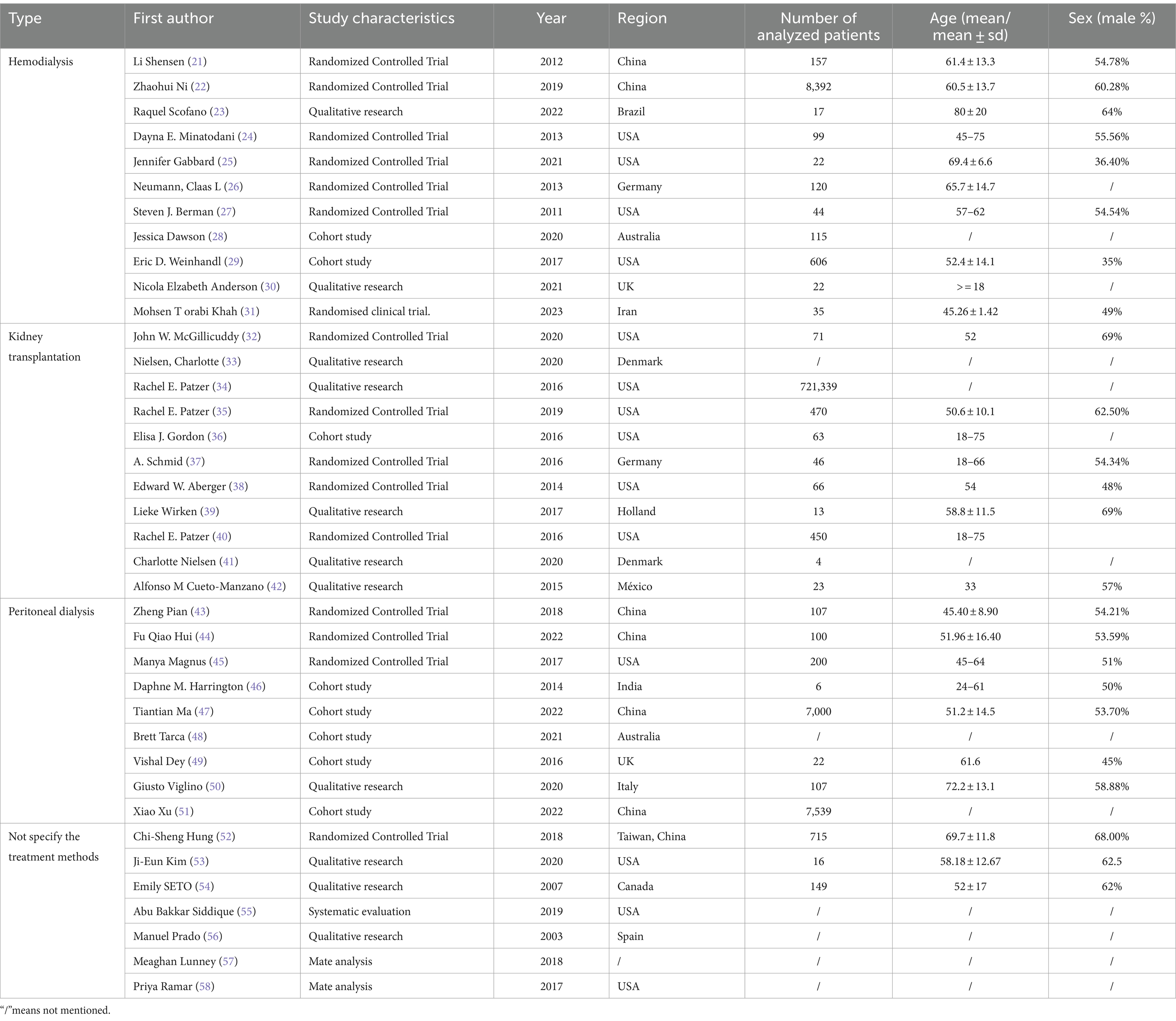
Table 1. Basic information of literature.
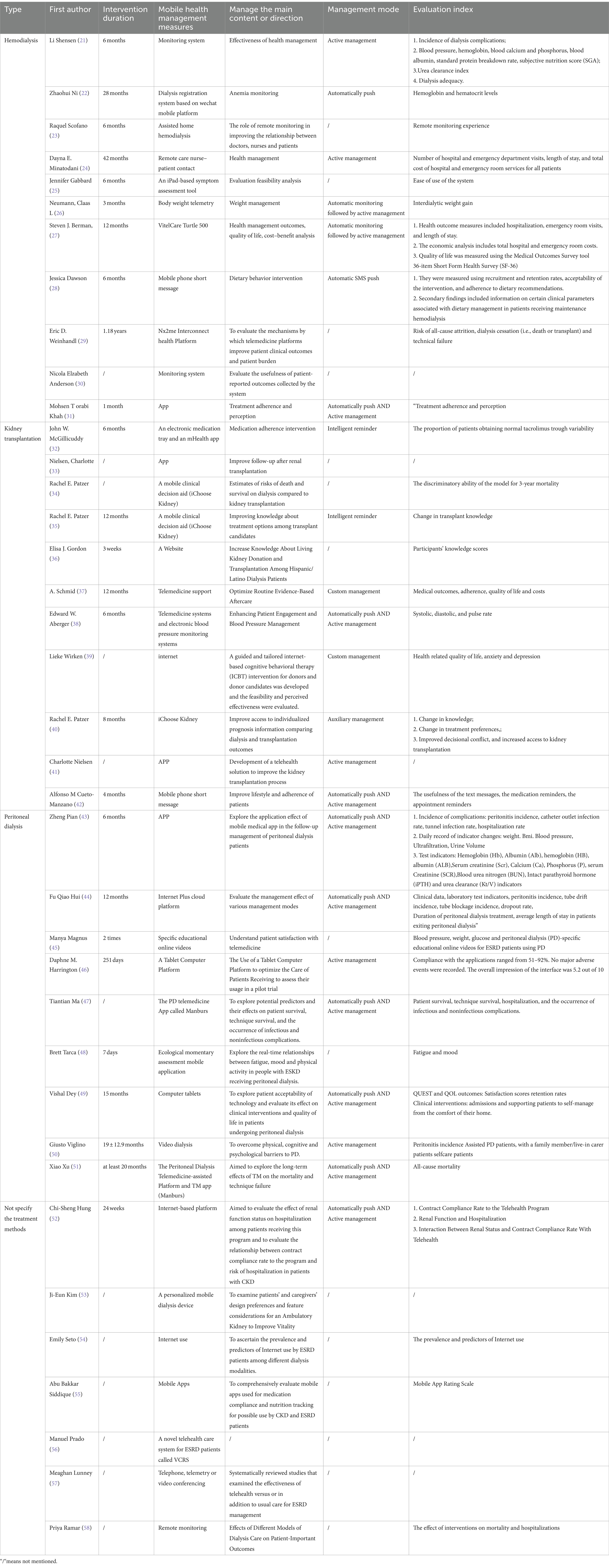
Table 2. Characteristics of study interventions and evaluation index.
Of the 38 studies included in the review, 13 (34.21%) mentioned remote monitoring systems. The following is a description of these systems by treatment method:
• Hemodialysis: there were a total of 7 literature, four of which assessed the effectiveness of remote monitoring for health management, i.e., the use of a remote monitoring system to track patients’ vital signs, such as blood pressure and weight. Secondly, the monitoring content includes quality of life detection, mainly focusing on the quality of life and mental health of patients; and monitoring the patient’s medical burden, such as medical costs. And two of the studies examined the potential of remote monitoring to improve doctor-patient relationships and the patient-reported outcomes collected through this modality. One of the study just focused on remote weight monitoring.
• Peritoneal dialysis: one study evaluated the management effectiveness of various peritoneal dialysis modalities.
• Kidney transplantation: two studies focused on kidney transplantation, with one focusing on optimizing routine evidence-based aftercare and the other on enhancing patient engagement and blood pressure management.
• Unspecified treatment methods: three studies did not specify the treatment methods used. One study evaluated the impact of hospitalization on patients receiving telemedicine and the relationship between compliance and hospitalization risk. The second study explored the impact of different dialysis nursing modes on patient outcomes.
Of the 38 studies included in the review, 9 (23.68%) mentioned mobile app. These studies were categorized by treatment method as follows:
• Hemodialysis: the study focused on changes in patients’ treatment adherence and perception though app and face-to-face training, and the result showed that such improvements were detected much more in the patients trained with APP based on the micro-learning method than face-to- face training.
• Kidney transplantation: three studies focused on kidney transplantation, with one assessing medication adherence and two examining improved follow-up after kidney transplantation.
• Peritoneal dialysis: four studies focused on peritoneal dialysis. Two of these studies, named “Manburs,” explored potential predictors of peritoneal dialysis patients and their effects on patient survival, technical survival, infectious disease occurrence, non-infectious complications, and long-term mortality. The other two studies examined the effectiveness of follow-up management in peritoneal dialysis patients and the real-time relationship between fatigue, mood, and physical activity in ESRD patients undergoing peritoneal dialysis.
• Unspecified treatment methods: one review systematically evaluated the impact of mobile apps on medication adherence and nutrition tracking.
Among the 38 literatures, a total of 6 (15.78%) mentioned the use of mobile phones or tablet for health management, as follows:
• Hemodialysis: there were two studies, and one of which, adopted mobile phone short message to intervene eating behavior regularly. Another one analyzed the feasibility of data collected by iPad.
• Kidney transplantation: there was one used mobile phone text messages, regular text messages to improve the patient’s lifestyle and persistence
• Peritoneal dialysis: there were 2 papers used a tablet computer, which mainly focused on the satisfaction and retention rate.
• Unspecified treatment methods: there was one study to adopted mobile phone short message to intervene eating behavior regularly.
• Peritoneal dialysis: one web-based study assessed patient satisfaction with telemedicine.
• Kidney transplantation: five studies used this approach, including one web-based study that disseminated kidney transplantation knowledge and one qualitative study that explored the evaluation of interventions for kidney donors and donor candidates. Three studies used a mobile clinical decision aid called “iChoose Kidney,” which helped patients discuss treatment plans at the onset of ESRD and improved their knowledge of kidney transplantation, which could influence their decision-making.
• Unspecified treatment methods: one study analyzed patients’ internet use.
For hemodialysis, there has a collection system based on WeChat to monitor anemia.
One article described the use of video dialysis to train peritoneal dialysis patients, providing them with essential information about PD and improving the quality of their training. Another article reported on the design of a personalized mobile dialysis device to enhance the vitality of dialysis devices.
The overwhelming majority of studies (28 articles, 73.68%) used electronic archives to ascertain baseline information, including age, sex, and geographic region. Further data monitoring and management were conducted based on electronic records.
Disease management is primarily reflected in the monitoring of objective indicators, including clinical and physical parameters. Physical parameters include blood pressure, weight, and so on; clinical indicators include laboratory and clinical findings. Specific examples are as follows:
• Hemodialysis: three studies reported on real-time guidance and personalized intervention through disease monitoring. For example, in studies Li Shensen (21) and Minatodani (24), Berman (27), data uploaded to the network in real time through the remote monitoring system were monitored, analyzed, and evaluated by medical staff, who then provided personalized feedback and guidance to patients.
• Peritoneal dialysis: five studies described timely intervention and treatment by medical staff after automatic monitoring.
• Kidney transplantation: seven studies reported on personalized guidance and management by doctors. For example, Nielsen’s (33), Schmid’s (37) and Aberger’s (38) studies proposed allowing consultations via telephone, video, or online, or introducing training courses for patients.
• Unspecified treatment methods: Hung’s (52) study exemplified the automatic monitoring push and personalized guidance of disease management.
Behavioral intervention is primarily reflected in health behaviors, such as medication adherence and dietary compliance. Nine studies reported on behavioral intervention.
• Hemodialysis: two studies focused on healthy behaviors, including weight management monitoring to guide patients in weight control and dietary advice.
• Peritoneal dialysis: three studies mentioned behavioral intervention, such as diet advice and weight management (43, 44, 49).
• Kidney transplantation: three studies evaluated interventions to improve compliance. For example, two studies (32, 42) reported improved medication adherence through remote intervention management, and one study (37) showed a reduction in non-compliance through remote monitoring.
• Unspecified treatment methods: Huang’s study (52) exemplified behavioral intervention, with nurse case managers communicating with patients daily over the phone as needed to ensure medication and medical instruction adherence.
Social support encompasses patient-clinician communication and question-and-answer sessions, as well as the support provided by clinicians to patients through remote monitoring and behavioral interventions. Notably, Viglino’s study (50) found that video dialysis enhanced patients’ confidence in peritoneal dialysis (PD).
Here are 10 articles on follow-up management, and they are distributed across different treatment modalities. For hemodialysis, there are three studies mentioned follow-up management (21, 24, 27), for peritoneal dialysis, there are four studies mentioned follow-up management (43, 44, 47, 51), for kidney transplantation, follow-up management was mentioned in two studies (38, 40), for unspecified treatment methods, One study mentioned follow-up management (52). Follow-up management and reminders primarily involve the regular monitoring and communication with patients to assess their overall self-management behavior, provide medication reminders, dietary guidance, and exercise guidance, and schedule follow-up appointments. Ten studies reported using the internet, mini-programs, phone calls, or text messages for follow-up management and reminders.
A diverse range of studies have investigated the clinical indicators associated with m-health management. The main indicators include:
• Dialysis indicators: dialysis adequacy
• Complication indicators: complication rate
• Daily recording indicators: body weight, BMI, blood pressure, ultrafiltration, urine volume
• Assay parameters: hemoglobin, albumin, calcium, phosphorus, serum creatinine, blood urea nitrogen, intact parathyroid hormone (iPTH), urea clearance
• Medical indicators: length of hospital stay, average length of hospital stay, number of emergency department visits, treatment duration
• Survival situation indexes: survival rate, survival time, life expectancy.
Two studies assessed the impact of MHealth management on quality of life.
In hemodialysis, Berman (27) used the 36-item Short Form Health Survey (SF-36) to measure quality of life. In peritoneal dialysis, Dey (49) assessed quality of life before and after a MHealth management intervention.
For hemodialysis, Berman (27) Economic analysis of total hospital and emergency room costs; for kidney transplantation, Schmid (37) involved the reduction of nursing cost.
Among the included studies, 7 (18.42%) assessed patient experience and satisfaction, including the availability of remote monitoring systems, apps, or professional websites, and the feasibility of MHealth management measures.
• Hemodialysis: one study (55) evaluated the patient experience of remote monitoring, one study (25) assessed the system’s usability, and one study (30) evaluated the system’s role in collecting patient reports.
• Peritoneal dialysis: one study (45) analyzed the satisfaction of nurses with remote monitoring, one study (46) assessed the satisfaction with the interface, and one study (49) evaluated the satisfaction with remote assistive technology.
• Unspecified treatment methods: one study (53) found that research is conducive to improving the efficiency, effectiveness, and user satisfaction of AKTIV prototypes and products.
For example, four studies (35, 36, 39, 42) assessed the acquisition of transplanted knowledge, and one study (48) investigated the real-time relationships between fatigue, mood, and physical activity in people with ESRD receiving peritoneal dialysis.
The scope review commences with an examination of MHealth management types, MHealth management content, MHealth management evaluation indices, and other relevant aspects. The studies included in this review utilized various platforms such as remote monitoring systems, apps, websites, mobile phones or tablets, and social platforms to offer patients a wide array of services encompassing disease management, behavioral intervention, social support, and follow-up care. These studies primarily focused on patient clinical indicators, patient experience, quality of life improvements, and healthcare cost. It is discussed from the following aspects.
This study found that the volume of literature on MHealth management for ESRD has steadily increased since 2003, reflecting the growing convergence of mobile internet technology and medicine. In the early stages, patient management was primarily conducted via phone, text messages, and other simple modalities. However, in recent years, research has focused on developing app-and mini-program-based interventions that leverage the internet and monitoring systems to facilitate personalized interventions based on automatically uploaded health data and automated push or early warning notifications. This study demonstrates that MHealth management has been widely adopted in kidney disease management, with a diverse range of applications. Similarly to the review (18), both demonstrate the breadth of e-health interventions used to provide lifestyle interventions in the CKD population.
Overall, MHealth offers several advantages for ESRD patients, enabling comprehensive multi-platform management from the dissemination of relevant knowledge to the monitoring of physiological parameters and disease intervention. MHealth also facilitates effective doctor-patient communication. We analyzed different treatment methods separately. From the perspective of mobile management carrier types, hemodialysis research is relatively comprehensive. In terms of research content, the peritoneal dialysis system in China, a telemedicine-assisted platform and telemedicine app (47, 51), has demonstrated promising results in a large-sample cohort study, which was real-world associations between telemedicine use and reduced survival and technology survival in peritoneal dialysis patients. Among kidney transplantation methods, iChoose Kidney (34, 35, 40) from the United States is a prominent mobile health management platform that not only provides transplant-related knowledge, but also predicts the mortality risk of dialysis and transplantation, and aids decision-making for kidney transplantation. Notably, iChoose Kidney offers outstanding functional features, but lacks follow-up management after kidney transplantation, while other MHealth management functions are relatively basic, focusing on the dissemination of transplant knowledge. From the perspective of evaluation indicators, most studies focus on clinical and patient experience indicators. We observed that most studies paid more attention to the physical health status of patients, with vital signs and kidney function being the primary monitoring indicators and evaluation outcomes. Additionally, we found that most studies monitored the health data of ESRD patients through mobile health management, and background medical staff analyzed and evaluated the data, providing further interventions for patients with abnormal conditions, such as adjusting medication or recommending outpatient clinic visits.
The application of peritoneal dialysis and kidney transplantation lacks research on social media platforms, which are commonly used and familiar to us. Strengthening the interaction with social media platforms could enhance effective communication between medical staff and patients, improve patient engagement, and boost management efficiency.
Single-sample management studies are still present in hemodialysis, such as those that monitor and manage only weight (26) or anemia (22).
Further research is needed to determine whether mobile health management can improve patients’ quality of life and reduce costs.
ESRD can seriously affect patients’ quality of life (59). It involves a variety of physical and emotional challenges, including frequent medical interventions, dialysis treatments, dietary restrictions, and limitations in daily activities. In this context, MHealth applications can play a key role in providing personalized care, symptom management and support. By integrating these technologies into the healthcare ecosystem, patients can better self-manage, reduce hospital admissions, and improve overall well-being. ESRD and its associated treatments, such as dialysis and transplantation, can be a financial burden on individuals and healthcare systems (60). Given the long-term nature of ESRD management, cost-effectiveness is an important issue. MHealth applications have the potential to optimize the allocation of medical resources, streamline care processes, and reduce unnecessary expenses. By allowing patients to actively participate in the medical process, these technologies enable more efficient use of resources, resulting in cost savings for patients and providers.
Depression is the most common psychiatric disorder in patients with ESRD, with a prevalence of 22.8 to 39.3% in the dialysis population (61). However, in this study, few people paid attention to mental health, and we found that the psychological management of mobile health management is becoming more and more abundant. For example, Chou’s research (62) found that chatbots can promote the mental health of the elderly and reduce depressive symptoms. Therefore, integrating it into mobile health management and offering enhanced psychological support represents a key future direction for mobile health management in ESRD patients.
These interventions are rarely based on big data decision support systems, lack accurate evidence-based feedback, and lack clinical decision support. However, sometimes data security and privacy concerns affect the development of decision support systems (63). Clinical decision support refers to the integration of electronic medical records and other clinical information through computer technology, automatic processing of patient data, and intelligent medical and nursing recommendations to provide the best plan to help patients make the best clinical decision (64). Clinical decision support is used in the management of many chronic diseases, such as hypertension (65) and advanced heart failure (66). In this study, only the “iChoose Kidney” tool in the kidney transplantation domain exhibited decision-making capabilities. There are studies of biomedical based remote diagnosis of kidney disease, for example, electrochemical creatinine (Bio) sensors for point-of-care diagnosis of renal malfunction and CKD (67). Studies have also been conducted through the development and validation of mixed Brillouin-Raman spectroscopy for non-contact assessment of the mechanochemical properties of urinary proteins as biomarkers for kidney disease (68). Therefore, developing a mobile management decision support system with diversified functions to provide optimal clinical decision support to patients is a key area for future development, and based on biomedical remote instant of ESRD disease diagnosis is also worth exploring, In the context of ESRD, clinical decision support systems can help healthcare providers make timely and informed decisions about treatment choices, medication management, and care planning. By integrating patient-specific data from mobile health apps, clinical decision support systems can enhance clinical decision making, improve treatment outcomes, and potentially reduce the occurrence of medical errors. And how to develop and adopt a standardized set of evaluation metrics and evaluation methods to compare different MHealth applications and platforms. This may include validation based on assessments of enablement and functionality, user satisfaction surveys, and clinical trials.
At the same time, there is a lack of relevant research on MHealth management for special ESRD population, especially applicability and accessibility of MHealth applications. This may include specific features and interface designs for these patients to ensure they can easily use these apps. Also can consider exploring how assistive technologies and technical support can be used to help these patients overcome barriers to use. And, how the elderly (digital newbies) or individuals from low-income backgrounds can access and benefit from MHealth treatments is also a question. This entails providing technical training and support, enhancing digital engagement capabilities, and improving accessibility to devices and networks. Simultaneously, there is a need to increase public policies and initiatives to ensure that individuals from low-income backgrounds have equitable access to necessary medical treatment and support.
Following the scoping review reporting framework of Arksey and O’Malley (20), this study reviewed relevant studies on MHealth management for ESRD patients to synthesize the types, contents, and evaluation indicators of MHealth management. The findings revealed that MHealth management has been widely adopted in the disease management of ESRD patients, encompassing a diverse range of management content and numerous evaluation indicators. Future research should focus on enhancing the evaluation of patients’ mental health, quality of life, and costs, as well as developing a clinical decision support system to better realize the potential of MHealth management in ESRD patients.
There was a suggestion at the June 2019 Consensus meeting on Improving Global Results in Kidney Disease (KDIGO) to use “kidney failure” and appropriately describe whether symptoms, signs and treatments are present, rather than “end-stage kidney disease, “but since it is limited to English (nuances can be difficult to translate) (69), Therefore, “end-stage renal disease” was still used for the search in this review, resulted in 38 number of papers in this scope review. Additionally, this scope review starts from types of MHealth management, content of mobile health management, evaluation index of health management, and Others four aspects have been reported, lack of the responsibility of the government to establish modern medicine, including MHealth products and other aspects of sorting. Lastly, quality assessment of included studies is not a primary component of a scoping review (18), therefore critical appraisal is not provided.
YW: Writing – original draft, Writing – review & editing. YR: Writing – original draft, Writing – review & editing. YY: Writing – original draft, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This research were funded by the National Natural Science Foundation of China (Grant No. 82200837), the Sichuan Province Science and Technology Program (Grant No. 2021YFS0163).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2024.1366362/full#supplementary-material
ESRD, End-stage renal disease; MHealth, Mobile health; CKD, Chronic kidney disease; PRISMA-SCR, Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews.; eHealth, Electronic health; PD, Peritoneal dialysis; iPTH, Intact parathyroid hormone; SF-36, The 36-item Short Form Health Survey; AKTIV, Ambulatory Kidney to Improve Vitality; BMI, Body mass index.
1. Matter, MA-O, Probst, S, Läuchli, S, and Herrmann, IK. Uniting drug and delivery: Metal oxide hybrid Nanotherapeutics for skin wound care. Pharmaceutics. (2020) 12:780. doi: 10.3390/Pharmaceutics12080780
2. Aitbaev, KA, Murkamilov, IT, and Fomin, VV. Hypolipidemic Therapy and Chronic Kidney Disease: Effects on Cardiovascular Risks and Renal Dysfunction. Kardiologiia. (2019) 59:79–87. doi: 10.18087/cardio.2019.2.10231
4. O'Connor, NR, and Corcoran, AM. End-stage renal disease: Symptom management and advance care planning. Am Fam Physician. (2012) 85:705–10.
6. Ahmadmehrabi, S, and Tang, WHW. Hemodialysis-induced cardiovascular disease. Semin Dial. (2018) 31:258–67. doi: 10.1111/sdi.12694
7. Galperin, TA, Cronin Aj Fau-Leslie, KS, and Leslie, KS. Cutaneous manifestations of Esrd. Clin J Am Soc Nephrol. (2014) 9:201–18. doi: 10.2215/CJN.05900513
8. Sauchelli, S, Pickles, T, Voinescu, A, Choi, H, Sherlock, B, Zhang, J, et al. Public attitudes towards the use of novel Technologies in Their Future Healthcare: a Uk survey. BMC Med Inform Decis Mak. (2023) 23:38. doi: 10.1186/s12911-023-02118-2
9. MacKinnon, GE, and Brittain, EL. Mobile health Technologies in Cardiopulmonary Disease. Chest. (2020) 157:654–64. doi: 10.1016/j.chest.2019.10.015
10. Duke, DC, Barry, S, Wagner, DV, Speight, J, Choudhary, P, and Harris, MA. Distal technologies and type 1 diabetes management. Lancet Diabetes Endocrinol. (2018) 6:143–56. doi: 10.1016/S2213-8587(17)30260-7
11. Artinian, NT . Telehealth as a tool for enhancing Care for Patients with cardiovascular disease. J Cardiovasc Nurs. (2007) 22:25–31. doi: 10.1097/00005082-200701000-00004
12. Vercell, AA-O, Taylor, SA-O, Yorke, JA-O, and Dowding, DA-O. Assessing the acceptability of home blood monitoring for patients with Cancer who are receiving systemic anticancer therapy from a patient, caregiver, and clinician perspective: focus group and interview study. Jmir Nurs. (2023) 6:e39815. doi: 10.2196/39815
13. Martínez-Ramírez, HR, Cortés-Sanabria, L, Rojas-Campos, E, Hernández-Herrera, A, and Cueto-Manzano, AM. Multidisciplinary strategies in the Management of Early Chronic Kidney Disease. Arch Med Res. (2013) 44:611–5. doi: 10.1016/j.arcmed.2013.10.013
14. Jakob, R, Harperink, S, Rudolf, AM, Fleisch, E, Haug, S, Mair, JL, et al. Factors influencing adherence to Mhealth apps for prevention or Management of Noncommunicable Diseases: systematic review. J Med Internet Res. (2022) 24:e35371. doi: 10.2196/35371
15. Ruco, A, Dossa, F, Tinmouth, J, Llovet, D, Jacobson, J, Kishibe, T, et al. Social media and Mhealth Technology for Cancer Screening: systematic review and Meta-analysis. J Med Internet Res. (2021) 23:e26759. doi: 10.2196/26759
16. Jacob, CA-O, Sanchez-Vazquez, AA-O, and Ivory, CA-O. Social, organizational, and technological factors impacting Clinicians' adoption of Mobile health tools: systematic literature review. JMU. (2020) 8:e15935. doi: 10.2196/15935
17. Munn, ZA-O, Peters, MDJ, Stern, C, Tufanaru, C, McArthur, A, and Aromataris, E. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. Medical Res Methodol. (2018) 18:143. doi: 10.1186/s12874-018-0611-x
18. Curtis, F, Burton, JO, Butt, A, Dhaliwal, HK, Graham-Brown, MMP, Lightfoot, CJ, et al. Lifestyle interventions delivered by Ehealth in chronic kidney disease: a scoping review. PLoS One. (2024) 19:e0297107. doi: 10.1371/journal.pone.0297107
19. Tricco, AC, Lillie, E, Zarin, W, O'Brien, KK, Colquhoun, H, Levac, D, et al. Prisma extension for scoping reviews (Prisma-Scr): checklist and explanation. Ann Intern Med. (2018) 169:467–73. doi: 10.7326/M18-0850
20. Arksey, H, and O'Malley, L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. (2005) 8:19–32. doi: 10.1080/1364557032000119616
21. Shensen, L . The establishment and evaluation of electronic information management Systemin hemodialysis center, Shanghai: Fudan University (2012) Available at: https://d.wanfangdata.com.cn/thesis/ChJUaGVzaXNOZXdTMjAyMzA5MDESCFkyODY0MTM3Ggg0dmJpZXprag%3D%3D
22. Ni, ZA-O, Jin, HA-O, Jiang, GA-O, Wang, NA-O, Peng, AA-O, Guo, ZA-O, et al. A telemedicine-based registration system for the Management of Renal Anemia in patients on maintenance hemodialysis: multicenter study. J Med Internet Res. (2019) 21:e13168. doi: 10.2196/13168
23. Scofano, RA-O, Monteiro, AA-O, and Motta, LA-O. Evaluation of the experience with the use of telemedicine in a home Dialysis program-a qualitative and quantitative study. BMC Nephrol. (2022) 23:190. doi: 10.1186/s12882-022-02824-5
24. Minatodani, DE, and Berman, SJ. Home telehealth in high-risk Dialysis patients: a 3-year study. Telemed J E Health. (2013) 19:520–2. doi: 10.1089/tmj.2012.0196
25. Gabbard, JA-O, McLouth, CJ, Brenes, G, Claudel, S, Ongchuan, S, Burkart, J, et al. Rapid electronic capturing of patient-reported outcome measures in older adults with end-stage renal disease: a feasibility study. Am J Hosp Palliat Care. (2021) 38:432–40. doi: 10.1177/1049909120954805
26. Neumann, CL, Wagner, F, Menne, J, Brockes, C, Schmidt-Weitmann, S, Rieken, EM, et al. Body weight telemetry is useful to reduce Interdialytic weight gain in patients with end-stage renal failure on hemodialysis. Telemed J E Health. (2013) 19:480–6. doi: 10.1089/tmj.2012.0188
27. Berman, SJ, Wada, C, Minatodani, D, Halliday, T, Miyamoto, R, Lindo, J, et al. Home-based preventative Care in High-Risk Dialysis Patients: a pilot study. Telemed J E Health. (2011) 17:283–7. doi: 10.1089/tmj.2010.0169
28. Dawson, J, Campbell, KL, Craig, JC, Tong, A, Teixeira-Pinto, A, Brown, MA, et al. A text messaging intervention for dietary behaviors for people receiving maintenance hemodialysis: a feasibility study of Kidneytext. Am J Kidney Dis. (2021) 78:85–95.e1. doi: 10.1053/j.ajkd.2020.11.015
29. Weinhandl, ED, and Collins, AJ. Relative risk of home hemodialysis attrition in patients using a telehealth platform. Hemodial Int. (2018) 22:318–27. doi: 10.1111/hdi.12621
30. Anderson, NA-O, McMullan, CA-O, Calvert, MA-OX, Dutton, M, Cockwell, P, Aiyegbusi, OL, et al. Using patient-reported outcome measures during the Management of Patients with end-stage kidney disease requiring treatment with Haemodialysis (prom-Hd): a qualitative study. BMJ Open. (2021) 11:2044–6055. doi: 10.1136/bmjopen-2021-052629
31. Torabi Khah, M, Farsi, Z, and Sajadi, SA. Comparing the effects of Mhealth application based on Micro-learning method and face-to-face training on treatment adherence and perception in Haemodialysis patients: a randomised clinical trial. BMJ Open. (2023) 13:e071982. doi: 10.1136/bmjopen-2023-071982
32. McGillicuddy, JW, Chandler, JA-OX, Sox, LR, and Taber, DJ. Exploratory analysis of the impact of an Mhealth medication adherence intervention on tacrolimus trough concentration variability: post hoc results of a randomized controlled trial. Ann Pharmacother. (2020) 54:1185–93. doi: 10.1177/1060028020931806
33. Nielsen, CA-O, Agerskov, H, Bistrup, C, and Clemensen, J. Evaluation of a telehealth solution developed to improve follow-up after kidney transplantation. J Clin Nurs. (2020) 29:1053–63. doi: 10.1111/jocn.15178
34. Patzer, RE, Basu, M, Larsen, CP, Pastan, SO, Mohan, S, Patzer, M, et al. Ichoose kidney: a clinical decision aid for kidney transplantation versus Dialysis treatment. Transplantation. (2016) 100:630–9. doi: 10.1097/TP.0000000000001019
35. Patzer, RA-O, McPherson, LA-O, Basu, M, Mohan, SA-O, Wolf, M, Chiles, M, et al. Effect of the Ichoose kidney decision aid in improving knowledge about treatment options among transplant candidates: a randomized controlled trial. Am J Transplant. (2018) 18:1954–65. doi: 10.1111/ajt.14693
36. Gordon, EJ, Feinglass, J, Carney, P, Vera, K, Olivero, M, Black, A, et al. A website intervention to increase knowledge about living kidney donation and transplantation among Hispanic/Latino Dialysis patients. Prog Transplant. (2016) 26:82–91. doi: 10.1177/1526924816632124
37. Schmid, A, Hils, S, Kramer-Zucker, A, Bogatyreva, L, Hauschke, D, De Geest, S, et al. Telemedically supported case Management of Living-Donor Renal Transplant Recipients to optimize routine evidence-based aftercare: a single-center randomized controlled trial. Am J Transplant. (2017) 17:1594–605. doi: 10.1111/ajt.14138
38. Aberger, EW, Migliozzi, D, Follick, MJ, Malick, T, and Ahern, DK. Enhancing patient engagement and blood pressure Management for Renal Transplant Recipients via Home Electronic Monitoring and web-Enabled Collaborative Care. Telemed J E Health. (2014) 20:850–4. doi: 10.1089/tmj.2013.0317
39. Wirken, LA-O, van Middendorp, H, Hooghof, CW, Bremer, TE, Hopman, SPF, van der Pant, K, et al. Development and feasibility of a guided and tailored internet-based cognitive-Behavioural intervention for kidney donors and kidney donor candidates. BMJ Open. (2018) 8:e020906. doi: 10.1136/bmjopen-2017-020906
40. Patzer, RE, Basu, M, Mohan, S, Smith, KD, Wolf, M, Ladner, D, et al. A randomized controlled trial of a Mobile clinical decision aid to improve access to kidney transplantation: Ichoose kidney. Kidney Int Rep. (2016) 1:34–42. doi: 10.1016/j.ekir.2016.04.001
41. Nielsen, CA-O, Agerskov, H, Bistrup, C, and Clemensen, J. User involvement in the development of a telehealth solution to improve the kidney transplantation process: a participatory design study. Health Informatics J. (2020) 26:1237–52. doi: 10.1177/1460458219876188
42. Cueto-Manzano, AM, Gallardo-Rincón, H, Martínez-Ramírez, HR, Cortés-Sanabria, L, Rojas-Campos, E, Tapia-Conyer, R, et al. A pilot study of a Mobile phone application to improve lifestyle and adherence of patients with kidney disease. J Telemed Telecare. (2015) 21:119–20.(1758-1109. doi: 10.1177/1357633X14566591
43. Zheng, P. Application of mobile medical APP in follow-up management of peritoneal dialysis patients [D]. Yangtze University, (2018). Available at: https://d.wanfangdata.com.cn/thesis/ChJUaGVzaXNOZXdTMjAyMzA5MDESCUQwMjM2MzI2NhoIcGJwMXV3M2o%3D
44. Fu, QiAhui . Evaluation on quality and effect of single center in different peritoneal dialysis management models [D]. Chengdu Medical College, (2022). Available at: https://d.wanfangdata.com.cn/thesis/ChJUaGVzaXNOZXdTMjAyMzA5MDESCUQwMjgwMTYwORoIdjQ4azdjNWY%3D
45. Magnus, M, Sikka, N, Cherian, T, and Lew, SQ. Satisfaction and improvements in peritoneal Dialysis outcomes associated with telehealth. Inform. (2017) 8:214–25. doi: 10.4338/ACI-2016-09-RA-0154
46. Harrington, DM, Myers, L, Eisenman, K, Bhise, V, Nayak, KS, and Rosner, MH. The use of a tablet computer platform to optimize the Care of Patients Receiving Peritoneal Dialysis: a pilot study. Blood Purif. (2014) 37:311–5. doi: 10.1159/000365440
47. Ma, TA-O, Yang, Z, Li, S, Pei, H, Zhao, J, Li, YA-O, et al. The peritoneal Dialysis telemedicine-assisted platform cohort (Pdtap) study: design and methods. Perit Dial Int. (2022) 42:75–82. doi: 10.1177/0896860820962901
48. Tarca, BA-O, Jesudason, S, Le Leu, R, Ovenden, M, Borlace, M, Meade, A, et al. Ecological momentary assessment to explore fatigue, mood and physical activity levels in people receiving peritoneal Dialysis: a study protocol. Perit Dial Int. (2021) 41:502–8. doi: 10.1177/0896860821992243
49. Dey, V, Jones, A, and Spalding, EM. Telehealth: acceptability, clinical interventions and quality of life in peritoneal Dialysis. SAGE Open Med. (2016) 4:2050312116670188. doi: 10.1177/2050312116670188
50. Viglino, G, Neri, L, Barbieri, S, and Tortone, C. Videodialysis: a pilot experience of telecare for assisted peritoneal Dialysis. J Nephrol. (2020) 33:177–82. doi: 10.1007/s40620-019-00647-6
51. Xu, X, Ma, T, Tian, X, Li, S, Pei, H, Zhao, J, et al. Telemedicine and clinical outcomes in peritoneal Dialysis: a propensity-matched study. Am J Nephrol. (2022) 53:663–74. doi: 10.1159/000525917
52. Hung, CA-O, Lee, JA-OX, Chen, YA-O, Huang, CA-O, Wu, VA-O, Wu, HA-OX, et al. Effect of contract compliance rate to a fourth-generation telehealth program on the risk of hospitalization in patients with chronic kidney disease: retrospective cohort study. J Med Internet Res. (2018) 20:e23. doi: 10.2196/jmir.8914
53. Kim, J-E, Kessler, L, McCauley, Z, Niiyama, I, and Boyle, LN. Human factors considerations in designing a personalized Mobile Dialysis device: an interview study. Appl Ergon. (2020) 85:103003. doi: 10.1016/j.apergo.2019.103003
54. Seto, E, Cafazzo, JA, Rizo, C, Bonert, M, Fong, E, and Chan, CT. Internet use by end-stage renal disease patients. Hemodial Int. (2007) 11:328–32. doi: 10.1111/j.1542-4758.2007.00188.x
55. Siddique, AA-O, Krebs, MA-O, Alvarez, SA-O, Greenspan, IA-O, Patel, AA-O, Kinsolving, JA-O, et al. Mobile apps for the Care Management of Chronic Kidney and end-Stage Renal Diseases: systematic search in app stores and evaluation. JMIR Mhealth Uhealth. (2019) 7:e12604. doi: 10.2196/12604
56. Prado, M, Roa, L, Reina-Tosina, J, Palma, A, and Milán, JA. Renal Telehealthcare system based on a patient physiological image: a novel hybrid approach in telemedicine. Telemed J E Health. (2003) 9:149–65. doi: 10.1089/153056203766437499
57. Lunney, M, Lee, R, Tang, K, Wiebe, N, Bello, AK, Thomas, C, et al. Impact of telehealth interventions on processes and quality of Care for Patients with Esrd. Am J Kidney Dis. (2018) 72:592–600. doi: 10.1053/j.ajkd.2018.02.353
58. Ramar, P, Ahmed, AT, Wang, Z, Chawla, SS, Suarez, MLG, Hickson, LTJ, et al. Effects of different models of Dialysis care on patient-important outcomes: a systematic review and Meta-analysis. Popul Health Manag. (2017) 20:495–505. doi: 10.1089/pop.2016.0157
59. Ravindran, A, Sunny, A, Kunnath, RP, and Divakaran, B. Assessment of quality of life among end-stage renal disease patients undergoing maintenance hemodialysis. Indian J Palliat Care. (2020) 26:47–53. doi: 10.4103/ijpc.Ijpc_141_19
60. Société Francophone de Néphrologie Dialyse Et T . Report on chronic Dialysis in France in 2016. Nephrol Ther. (2017) 13:105–26. doi: 10.1016/j.nephro.2016.06.008
61. King-Wing Ma, T , Kam-Tao, Li P . Depression in dialysis patients. Nephrology (Carlton). (2016) 21:639–46. doi: 10.1111/nep.12742
62. Chou, YH, Lin, C, Lee, SH, Chang Chien, YW, and Cheng, LC. Potential Mobile health applications for improving the mental health of the elderly: a systematic review. Clin Interv Aging. (2023) 18:1523–34. doi: 10.2147/cia.S410396
63. Albarrak, AM . Determining a trustworthy application for medical data visualizations through a knowledge-based fuzzy expert system. Diagnostics. (2023) 13:1916. doi: 10.3390/diagnostics13111916
64. Sadeghi-Ghyassi, F, Damanabi, SA-O, Kalankesh, LR, van de Velde, S, Feizi-Derakhshi, MR, and Hajebrahimi, S. How are ontologies implemented to represent clinical practice guidelines in clinical decision support systems: protocol for a systematic review. Syst Rev. (2022) 11:183. doi: 10.1186/s13643-022-02063-7
65. Kharbanda, EO, Asche, SE, Sinaiko, AR, Ekstrom, HL, Nordin, JD, Sherwood, NE, et al. Clinical decision support for recognition and Management of Hypertension: A randomized trial. Pediatrics. (2018) 141:e20172954. doi: 10.1542/Peds.2017-2954
66. Evans, RS, Kfoury, AG, Horne, BD, Lloyd, JF, Benuzillo, J, Rasmusson, KD, et al. Clinical decision support to efficiently identify patients eligible for advanced heart failure therapies. J Card Fail. (2017) 23:719–26. doi: 10.1016/j.cardfail.2017.08.449
67. Saddique, Z, Faheem, M, Habib, AA-O, UlHasan, IA-O, Mujahid, AA-O, and Afzal, AA-O. Electrochemical creatinine (bio)sensors for point-of-care diagnosis of renal malfunction and chronic kidney disorders. Diagnostics. (2023) 13:1737. doi: 10.3390/diagnostics13101737
68. Gaipov, AA-O, Utegulov, Z, Bukasov, R, Turebekov, D, Tarlykov, P, Markhametova, Z, et al. Development and validation of hybrid Brillouin-Raman spectroscopy for non-contact assessment of Mechano-chemical properties of urine proteins as biomarkers of kidney diseases. BMC Nephrol. (2020) 21:229. doi: 10.1186/s12882-020-01890-x
Keywords: end-stage renal disease, mobile health management, MHealth management, ESRD, MHealth
Citation: Wen Y, Ruan Y and Yu Y (2024) Mobile health management among end stage renal disease patients: a scoping review. Front. Med. 11:1366362. doi: 10.3389/fmed.2024.1366362
Edited by:
Yi-Chun Tsai, Kaohsiung Medical University Hospital, TaiwanReviewed by:
William C. Cho, Queen Elizabeth Hospital (QEH), Hong Kong SAR, ChinaCopyright © 2024 Wen, Ruan and Yu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yang Yu, eXV5YW5nY2hlbmdkdUAxNjMuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.