
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Med. , 28 June 2024
Sec. Infectious Diseases: Pathogenesis and Therapy
Volume 11 - 2024 | https://doi.org/10.3389/fmed.2024.1363899
 Kokab Jabeen1
Kokab Jabeen1 Sameen Bint Ali2Zainab Tufail1Sana Mustafa1Mahnoor Chaudhry1
Sameen Bint Ali2Zainab Tufail1Sana Mustafa1Mahnoor Chaudhry1 Muhammad J. Tahir3
Muhammad J. Tahir3 Muhammad Sohaib Asghar4*
Muhammad Sohaib Asghar4* Ali Ahmed5
Ali Ahmed5Introduction: Salmonella typhi, a gram-negative bacterium responsible for typhoid fever, can infect the inner lining or valves of the heart and cause endocarditis. This systematic review aimed to report cases of S. typhi-associated endocarditis and its clinical features.
Methods: This systematic review was reported as per the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) checklist. Only case reports and case series of endocarditis caused by S. typhi, irrespective of age, gender, and demographics, were considered eligible for inclusion. To identify relevant studies, a literature search was conducted using relevant keywords on PubMed, Google Scholar, and the Cochrane Library from inception to 31 December 2023. After selecting the studies, the relevant data were extracted and pooled in terms of frequencies and percentages. A quality assessment was performed using the Joanna Briggs Institute Critical Appraisal Checklist for Case Reports.
Results: This review included seven case reports, comprising 22.2% female and 77.8% male patients. The mean age of patients was 27.9 + 12.0 years. Regarding past medical history, 33.3% (3/9) of patients had a previous cardiac pathology. Fever remained the most common complaint, occurring in 88.9% of cases. Transthoracic and transesophageal echocardiography were used to diagnose all cases, with 33.3% identifying vegetation on the mitral, aortic, and tricuspid valves. Ceftriaxone, with or without gentamycin, remained the choice of antibiotic for 88.9% of cases, and all patients responded to the offered treatment.
Conclusion: S. typhi-associated endocarditis, though rare, presents unique challenges and requires timely diagnosis. This systematic review of seven cases highlights a predominantly male population affected, with a mean age in the third decade, suggesting a higher invasiveness than other causes. The findings from this study underscore the importance of early recognition and appropriate management, primarily with antibiotic therapy. Further research with larger cohorts is crucial to refine understanding and guide policymaking for this rare but life-threatening condition.
Salmonella bacteria can be classified based on their serotype, determined by two bacterial surface antigens, O and H. They are categorized as either typhoidal (causing typhoid and paratyphoid fever) or non-typhoidal (causing gastroenteritis). To date, over 2,500 different serotypes, or serovars, have been identified. Serotypes of Salmonella known to cause disease in humans include both non-typhoidal strains, such as Enteritidis, Typhimurium, Newport, and Javiana, and typhoidal strains, such as Typhi (causing typhoid fever), as well as Paratyphi A, B, and C (causing paratyphoid fever). Additionally, Salmonella is further categorized into two species based on phenotype: Salmonella enterica and Salmonella bongori, with S. enterica further divided into six subspecies: arizonae, diarizonae, houtenae, salamae, indica, and enterica (1, 2).
Salmonella typhi, a gram-negative bacterium belonging to the S. enterica subspecies, primarily spreads via the consumption of contaminated food and water (3, 4). Globally, typhoid fever accounts for 11–21 million cases and 200,000 deaths annually (5). Owing to poor hygiene, sanitation, lack of safe drinking water, and overcrowding, the condition is more prevalent in low-to-middle-income parts of the world, whereas the history of international travel and immigration are among the significant risk factors observed in high-income regions (4, 5).
The infectious dose varies from 10,000 to 1 million organisms and is modulated by multiple factors such as geographic location and immunity status (6). Following ingestion, an incubation period of 1–2 weeks is observed, and later, the patient may present with typical step ladder fever, chills, a dull headache, nausea, malaise, anorexia, abdominal discomfort, diarrhea, or constipation. Additionally, patients may also demonstrate rose spots, a coated tongue, hepatomegaly, splenomegaly, and bradycardia (6). While most cases resolve without medical treatment or with minimal outpatient management, approximately 10–15% of patients may develop complications, with gastrointestinal bleeding being the most common. Other complications reported include intestinal perforation, cholecystitis, pneumonia, miscarriage in pregnant individuals, encephalopathy, endocarditis, and myocarditis (6). Among complications, cardiovascular involvement is rare, but cases of myocarditis, myocardial abscess, pericarditis, and aortic aneurysm have been reported (7).
Infective endocarditis (IE), a condition marked by inflammation of the endocardium, heart valves, or indwelling cardiac devices, shares an annual incidence of almost 3–10 for every 100,000 individuals (8). With a monthly mortality rate of 30%, the in-hospital mortality rate stands at 23% for patients with native valves and 29% for prosthetic valve patients (9). Staphylococcus aureus remains the most common causative agent, accounting for 26.6% of cases, followed by Streptococcus viridians, other Streptococcus groups, and Enterococci in reducing order of frequency (10). Rare cases of S. typhi-associated IE have also been reported in the literature (7). The reported prevalence of Salmonella-caused endocarditis varies from 0.01 to 2.9%, of which multiple cases result from infection with Salmonella paratyphi, Typhimurium, etc. (7). Owing to significant short- and long-term morbidity and mortality, appropriate treatment must be offered at the earliest. While most cases of Salmonella-related endocarditis are caused by non-typhoidal species, rare incidences of S. typhi-associated endocarditis have been reported in the literature. This may be attributable to a higher incidence of infections by non-typhoidal species (2, 11). This systematic review aimed to comprehensively evaluate the literature for clinical presentation, examination findings, investigations, management offered, and outcomes across published cases of S. typhi-associated endocarditis and contribute to a better understanding of these rare incidences.
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) guidelines (12), and a protocol was registered at PROSPERO before the literature search (CRD42023470910).
To identify all eligible studies, a literature search was conducted using PubMed, Google Scholar, and Cochrane Library from inception to 31 December 2023. The Medical Subject Heading (MeSH) browser was used to determine relevant keywords, and the search string comprised the following terms: “endocarditis,” “infective endocarditis,” “S. typhi,” “S. enterica Typhi,” “S. typhi,” “S. enterica serovar Typhi,” and “Typhoid.” To obtain comprehensive literature search results, spelling variants and synonyms were also used. Furthermore, gray literature, references of included articles, and relevant reviews were also screened to identify any missed articles.
Only studies that met the predefined inclusion criteria were included (Table 1). Case reports and case series reporting endocarditis caused by S. typhi, irrespective of age, gender, and demographics, were deemed eligible for inclusion. Moreover, only articles published in the English language were considered. In contrast, studies reporting endocarditis caused by other Salmonella enterica subspecies, such as S. typhi murium and Paratyphi, were excluded. Similarly, cross-sectional studies, cohorts, randomized controlled trials (RCTs), narrative reviews, systematic reviews, comments, editorials, and articles published in languages other than English were not considered.
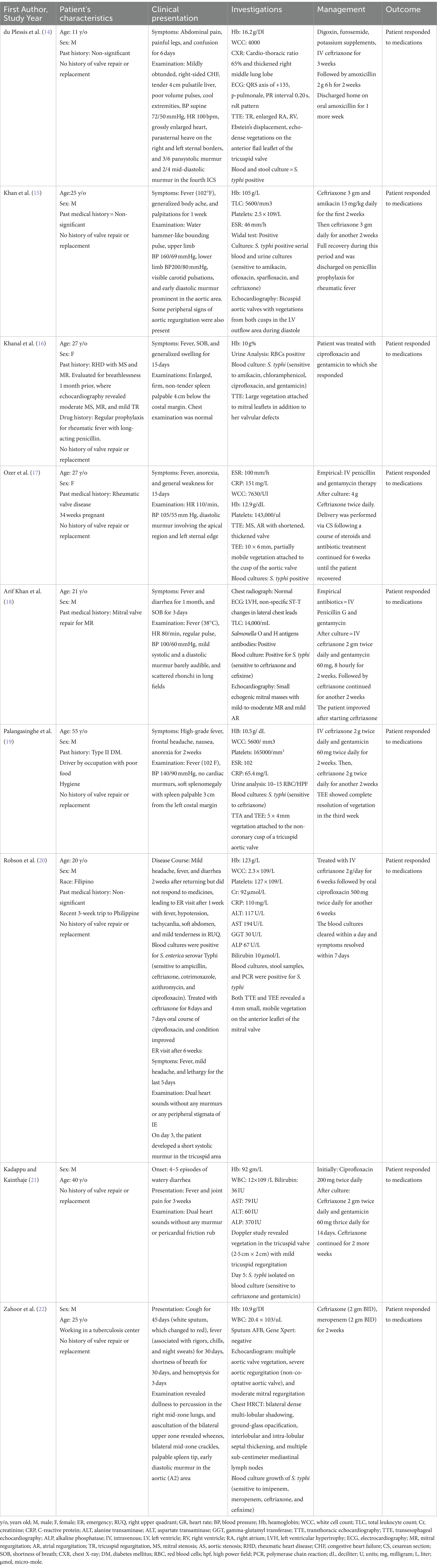
Table 1. Summary of included case reports.
Following a thorough literature search, two authors (KJ and SBA) independently screened all the search results via title and abstract. Recruited articles were then examined at full length to determine adherence to the inclusion criteria. Only articles meeting the above-mentioned inclusion criteria were included.
After the study selection process, two independent authors (KJ and SBA) extracted the following data from all included case reports: first author’s last name, year of publication, patient age, gender, past medical history, any other relevant baseline features, the clinical course of the disease, presenting complaints, examination findings, investigations ordered, drugs offered, management course, and outcome into an excel spreadsheet.
Excluding age, which was expressed as the mean age of included participants, all other parameters were reported as frequencies and percentages. To assess the quality of each included study, the Joanna Briggs Institute Critical Appraisal Checklist for Case Reports (13) was used, which scrutinizes each included study based on the reported patient’s demographics, clinical history, presentation, examination findings, diagnostic investigations, interventions offered, post-intervention impact, adverse events reported, and take-home messages.
Our initial literature search revealed 5,830 articles: 93 records from PubMed, 5,730 from Google Scholar, and 7 articles from the Cochrane Library. Following duplicate removal and screening via title and abstract, 27 case reports were considered for full-length review. Ultimately, only nine studies met the predefined inclusion criteria and were included in this systematic review (14–22). The results of the literature search are summarized in Figure 1.
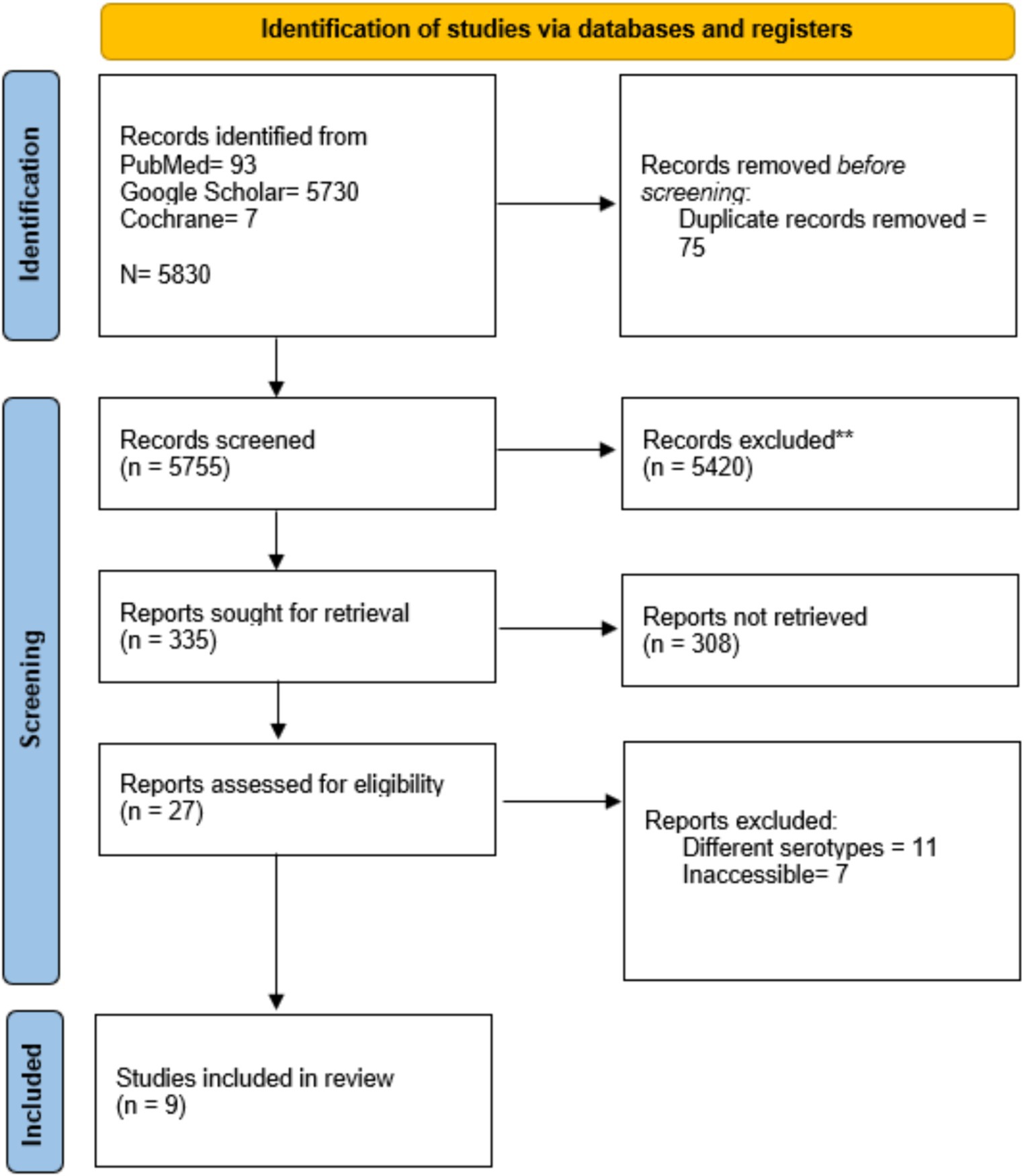
Figure 1. Preferred reporting items for systematic review and meta-analysis (PRISMA) flowchart.
The included case reports comprised data from nine patients, and their baseline characteristics, clinical presentation, laboratory investigations, and management offered are summarized in Table 1. Of the included population, 22.2% (2/9) (16, 17) were female patients, and the remaining 77.8% (7/9) (14, 15, 18–22) were male patients. The participants’ ages ranged from 11 to 55 years, with a mean age of 27.9 + 12.0 years. Regarding past medical history, 33.3% (3/9) (16–18) of patients had a previous cardiac pathology, with 22.2% (2/9) (16, 17) being diagnosed with rheumatic heart disease (RHD). In contrast, 55.6% (5/9) (14, 15, 20–22) had a non-significant past medical history and 11.1% (1/9) (19) had type II diabetes mellitus.
At the time of emergency presentation, fever was the most common complaint, present in 88.9% (8/9) (15–22) of patients. Gastrointestinal complaints were present in only 33.3% (3/9) (14, 18, 21) of individuals, with 22.2% (2/9) (18, 21) having diarrhea and the remaining 11.1% having abdominal pain (14). Cardiac symptoms were present in 44.4% (4/9) (15, 16, 18, 22) of patients: shortness of breath in 33.3% (3/9) (16, 18, 22) and palpitations in 11.1% (1/9) (15) of participants. Other presenting complaints included headaches (22.2%) (19, 20), bone and joint pain (2.2%) (14, 21), generalized pain (11.1%) (15), confusion (11.1%) (14), weakness and lethargy (22.2%) (17, 20), generalized swelling (11.1%) (16), anorexia (22.2%) (17, 19), cough (11.1%) (22), hemoptysis (11.1%) (22), and nausea (11.1%) (19).
Upon examination, murmurs were the most common finding, being present in 55.6% (5/9) of cases (14, 15, 17, 18, 22). Blood pressure and pulse abnormalities were found in 33.3% (3/9) of patients (14, 15, 17). Similarly, splenomegaly was determined in 33.3% (3/9) (16, 19, 22) of cases. Other findings reported include peripheral signs of aortic regurgitation (11.1%) (15), hepatomegaly (11.1%) (14), gross cardiomegaly (11.1%) (14), right-sided congestive heart failure (11.1%) (14), and dual heart sounds (22.2%) (20, 21). The clinical presentation and examination findings are summarized in Table 1.
Transthoracic and transesophageal echocardiography remained the mainstay of diagnosis in all cases, with identified vegetation involving the mitral (16, 18, 20), aortic (15, 17, 22), and tricuspid valves (14, 19, 21), each in 33.3% (3/9) of individuals. Other findings identified included right atrial and ventricular enlargement, bicuspid aortic valve, left ventricular hypertrophy, mitral stenosis, mitral regurgitation, and aortic regurgitation. A blood culture was ordered in all nine cases, and each tested positive for S. typhi. Other investigations ordered include a complete blood count (CBC), erythrocyte sedimentation rate (ESR), urine analysis, electrocardiography (ECG), chest radiograph, liver function test (LFT), and Widal test.
Following antibiotic sensitivity analysis, ceftriaxone remained the choice of antibiotic for 88.9% (8/9) (14, 15, 17–22) of cases. Ceftriaxone alone was initially given to 33.3% (3/9) of individuals (14, 17, 20), followed by ceftriaxone and gentamycin in 33.3% (3/9) (18, 19, 21), ceftriaxone and amikacin in 11.1% (1/7) (15), and ceftriaxone and meropenem in 11.1% (22) of individuals. The duration of treatment varied from 4 weeks to 12 weeks, and all nine patients responded to the offered intervention and recovered. No mortality was observed across any of the included studies.
Our quality appraisal using the JBI appraisal tool revealed an overall low risk of bias across included studies except for reporting of adverse or unanticipated events, which were marked unclear for all studies due to a lack of clarity on whether any adverse event occurred. Additionally, the take-home message was adequately specified in only 66.7% (6/9) of studies (15, 18–22), being unclear or not mentioned in the remaining 3. Other than this, the patient’s demographics, history, and current presentation were discussed across all included studies. The results of the quality assessment are summarized in Table 2.
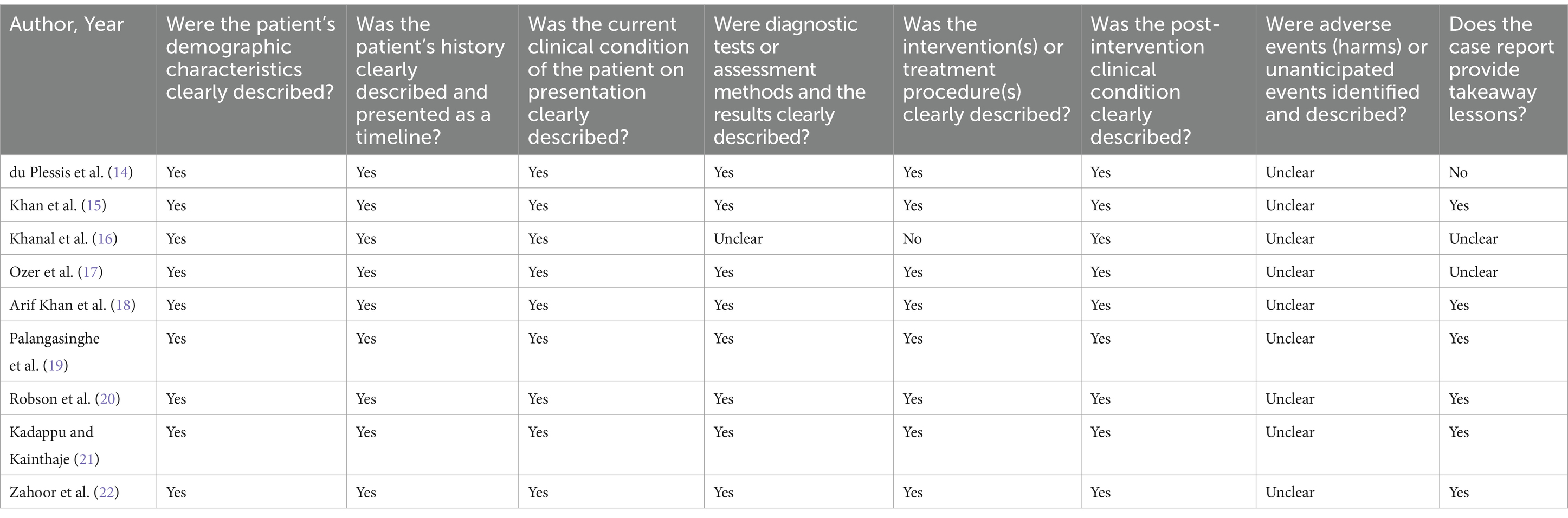
Table 2. Results of quality assessment.
This systematic review comprehensively assesses the literature for case reports and case series reporting rare incidences of endocarditis caused by S. typhi and includes data from nine published cases. The condition demonstrated a male predominance, majorly affecting individuals in their 20s. Although the clinical presentation varied among studies, fever, lethargy, and cardiac and gastrointestinal symptoms were frequently reported. In terms of valve involvement, mitral, aortic, and tricuspid valves were equally involved. Antimicrobial therapy, particularly ceftriaxone with or without gentamycin, remained the mainstay of management, and all patients responded positively to the offered treatment.
The mean age of presentation and gender distribution vary across different studies. According to Cheng et al. (7), Salmonella endocarditis showed female predominance, with a mean age of presentation estimated at 40 years. Contrary to the above finding, our systematic review revealed a male preponderance and presentation in the third decade. This difference may be attributable to the diverse studies covered in the review by Cheng et al., which included a majority of cases caused by non-typhoid Salmonella subspecies.
While RHD is the most common risk factor for IE among adults, accounting for 55% of affected individuals and 44.7% of affected children having a positive history of congenital cardiac pathologies (23), our findings indicate a lower incidence, with any prior cardiac pathology present in less than half of participants and RHD in less than a third. Similar findings were reported by Cheng et al., where a younger mean age and a relative absence of pre-existing cardiac diseases were found in S. typhi and Paratyphi-related cases, indicating a higher invasiveness compared to non-typhoid Salmonella-associated cases (7).
In accordance with our results, a recent prospective study by Habib et al. also reported fever as the most common symptom in patients with IE (24). Moreover, preceding abdominal complaints were observed in one-third of the cases reported. A similar proportion of gastrointestinal symptoms was reported in the review by Cheng et al. Other clinical features observed in the included cases, such as body aches, murmurs, splenomegaly, and shortness of breath, have also been commonly reported in the literature (20, 21).
Furthermore, in accordance with the hospital guidelines, echocardiography remained the mainstay of diagnosis across all nine included studies (22, 23). The blood cultures were positive for the causative organisms in all nine cases, as compared to 79% in a recent prospective cohort (24). Generally, IE more commonly affects left-sided valves, with the mitral valve being involved in most cases (52.2%), followed by an aortic valve (34.8%) (25). Similarly, in a review including Salmonella-associated endocarditis cases, the mitral valve was most frequently involved, affecting approximately 33.3% of patients (7). In congruence with the above findings, our review also found the mitral valve to be most affected, but the aortic and tricuspid valves also demonstrated similar involvement.
In accordance with the guidelines published in the Journal of American Medical Association, antibiotic therapy remained the mainstay of management, and the choice of drug was guided primarily by the organism’s sensitivity (26). However, in none of the included cases was a surgical approach offered, despite literature reports of lower mortality rates in patients offered combined medical and surgical interventions (15%) compared to those treated with medical therapy only (27.2%) (5, 27). Owing to better diagnostic techniques and prompt management, the overall prognosis of Salmonella endocarditis has improved over the last three decades, with the mortality rate reducing from 69.0 to 13.3% (5, 27, 28).
Excluding endocarditis, other cardiovascular complications such as Salmonella pericarditis, mycotic aneurysms, and infection of the arteriovenous fistula have also been reported in the literature (29, 30, 31). Hence, timely identification of high-risk patients and prompt management are necessary to avoid any preventable mortality.
This study has certain limitations. First, it encompasses a limited number of studies. Second, this systematic review exclusively encompasses case reports featuring small sample sizes and individual patient-level data. Consequently, extrapolating the findings of this study to a broader population becomes difficult. Finally, the absence of control subjects in the studies included may introduce potential biases in the study’s results. Hence, large group studies must be conducted to determine differences among risk factors, clinical presentation, desired investigations, and management for S. typhi endocarditis relative to other causative agents. Finally, in our systematic review of case reports, we recognize the potential for publication bias, wherein positive or exceptional cases may be preferentially published, possibly influencing the overall findings.
This systematic review scrutinized seven case reports of S. typhi-associated endocarditis, elaborating on unique clinical presentations, diagnostic investigations, and management approaches. Notably, a predominantly male and relatively younger population was affected compared to endocarditis of other origins, indicating a higher invasiveness. Fever remained the most common presenting feature, with abdominal pain, headache, body aches, palpitations, splenomegaly, murmurs, and others also reported. Echocardiography and positive blood cultures were pivotal in the diagnosis, with the mitral valve frequently affected. Antibiotic therapy remained the primary treatment, yielding promising outcomes, although surgical interventions were notably absent.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
KJ: Conceptualization, Data curation, Writing – original draft, Writing – review & editing. SB: Formal analysis, Writing – original draft, Writing – review & editing. ZT: Investigation, Software, Writing – original draft, Writing – review & editing. SM: Methodology, Resources, Writing – original draft, Writing – review & editing. MC: Data curation, Resources, Writing – original draft, Writing – review & editing. MT: Project administration, Supervision, Writing – original draft, Writing – review & editing. MA: Project administration, Supervision, Writing – original draft, Writing – review & editing. AA: Validation, Visualization, Writing – original draft, Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
MA was employed by AdventHealth.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Chattaway, MA, Langridge, GC, and Wain, J. Salmonella nomenclature in the genomic era: a time for change. Sci Rep. (2021) 11:7494. doi: 10.1038/s41598-021-86243-w
2. Information for Healthcare Professionals | Salmonella | CDC [Internet]. (2023). Available at: https://www.cdc.gov/salmonella/general/technical.html (Accessed May 5, 2024).
3. Masuet-Aumatell, C, and Atouguia, J. Typhoid fever infection - antibiotic resistance and vaccination strategies: a narrative review. Travel Med Infect Dis. (2021) 40:101946. doi: 10.1016/j.tmaid.2020.101946
4. Dougan, G, and Baker, S. Salmonella enterica serovar Typhi and the pathogenesis of typhoid fever. Ann Rev Microbiol. (2014) 68:317–36. doi: 10.1146/annurev-micro-091313-103739
5. Information for Healthcare Professionals | Typhoid fever | CDC [Internet] (2023). Available at: https://www.cdc.gov/typhoid-fever/health-professional.html (Accessed October 16, 2023).
6. Parry, CM, Hien, TT, Dougan, G, White, NJ, and Farrar, JJ. Typhoid fever. N Engl J Med. (2002) 347:1770–82. doi: 10.1056/NEJMra020201
7. Cheng, WL, Li, CW, Li, MC, Lee, NY, Lee, CC, and Ko, WC. Salmonella infective endocarditis. J Microbiol Immunol Infect. (2016) 49:313–20. doi: 10.1016/j.jmii.2015.02.659
8. Cahill, TJ, and Prendergast, BD. Infective endocarditis. Lancet Lond Engl. (2016) 387:882–93. doi: 10.1016/S0140-6736(15)00067-7
9. Cresti, A, Chiavarelli, M, Scalese, M, Nencioni, C, Valentini, S, Guerrini, F, et al. Epidemiological and mortality trends in infective endocarditis, a 17-year population-based prospective study. Cardiovasc Diagn Ther. (2017) 7:27–35. doi: 10.21037/cdt.2016.08.09
10. Rajani, R, and Klein, JL. Infective endocarditis: a contemporary update. Clin Med. (2020) 20:31–5. doi: 10.7861/clinmed.cme.20.1.1
11. Lamichhane, B, Mawad, AMM, Saleh, M, Kelley, WG, Harrington, PJ, Lovestad, CW, et al. Salmonellosis: an overview of epidemiology, pathogenesis, and innovative approaches to mitigate the antimicrobial resistant infections. Antibiotics. (2024) 13:76. doi: 10.3390/antibiotics13010076
12. Page, MJ, McKenzie, JE, Bossuyt, PM, Boutron, I, Hoffmann, TC, Mulrow, CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. (2021) 29:n71. doi: 10.1136/bmj.n71
13. Martin, J . © Joanna Briggs Institute 2017 Critical appraisal checklist for case reports. (2017).
14. du Plessis, JP, Govendrageloo, K, and Levin, SE. Right-sided endocarditis due to Salmonella typhi. Pediatr Cardiol. (1997) 18:443–4. doi: 10.1007/s002469900226
15. Khan, GQ, Kadri, SM, Hassan, G, Shahid, IT, Gazanfar, A, Kak, M, et al. Salmonella typhi endocarditis: a case report. J Clin Pathol. (2003) 56:801–2. doi: 10.1136/jcp.56.10.801
16. Khanal, B, Sharma, SK, and Deb, M. Infective endocarditis due to Salmonella typhi. J Nepal Med Assoc. (2004) 43 Available at: https://www.jnma.com.np/jnma/index.php/jnma/article/view/435
17. Ozer, O, Sari, I, Davutoglu, V, and Cebesoy, FB. A case of Salmonella typhi endocarditis in pregnancy. Am J Med Sci. (2009) 337:210–1. doi: 10.1097/MAJ.0b013e31818128a3
18. Khan, JA, Ali, B, Masood, T, Ahmed, F, Sial, JA, and Balooch, ZH. Salmonella typhi infection: a rare cause of endocarditis. J Coll Physicians Surg Pak. (2011) 21:559–60.
19. Palangasinghe, DR, Weeratunga, P, Wijeyaratne, A, and Jayasinghe, S. Endocarditis of a native cardiac valve due to Salmonella typhi - a case report. Prensa Med [Internet]. (2015) 101:6. doi: 10.4172/lpma.1000192
20. Robson, C, O’Sullivan, MVN, and Sivagnanam, S. Salmonella enterica Serovar Typhi: an unusual cause of infective endocarditis. Trop Med Infect Dis. (2018) 3:35. doi: 10.3390/tropicalmed3010035
21. R Coll Physicians Edinb . (2006) 36:304–305. https://www.rcpe.ac.uk/college/journal/tricuspid-valve-endocarditis-due-salmonella-typhi
22. Zahoor, M, Ahmad, K, Kakakhel, M, Yousaf, A, Saleh, M, Sayyar, M, et al. Multidrug-resistant Salmonella endocarditis of a native valve: a rare case presentation. Cureus. (2023) 15:e48396. doi: 10.7759/cureus.48396
23. Noubiap, JJ, Nkeck, JR, Kwondom, BS, and Nyaga, UF. Epidemiology of infective endocarditis in Africa: a systematic review and meta-analysis. Lancet Glob Health. (2022) 10:e77–86. doi: 10.1016/S2214-109X(21)00400-9
24. Habib, G, Erba, PA, Iung, B, Donal, E, Cosyns, B, Laroche, C, et al. Clinical presentation, aetiology and outcome of infective endocarditis. Results of the ESC-EORP EURO-ENDO (European infective endocarditis) registry: a prospective cohort study. Eur Heart J. (2019) 40:3222–32. doi: 10.1093/eurheartj/ehz620
25. Al-Makhamreh, HK, Al Bakri, FG, Shafei, M, Mokheemer, E, Alqudah, S, Nofal, A, et al. Epidemiology, microbiology, and outcomes of infective endocarditis in a tertiary center in Jordan. Wien Med Wochenschr. (2023) 1946:1–7. doi: 10.1007/s10354-023-01004-w
26. JAMA Network Open . Guidelines for Diagnosis and Management of Infective Endocarditis in Adults: A WikiGuidelines Group Consensus Statement | Infectious diseases | JAMA network open | JAMA network [Internet]. Available at: https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2807791 (Accessed October 28, 2023).
27. Furrer, H, and Malinverni, R. Clinical aspects and diagnosis of infectious endocarditis. Praxis. (1994) 83:1309–15.
28. Bea, C, Vela, S, García-Blas, S, Perez-Rivera, JA, Díez-Villanueva, P, de Gracia, AI, et al. Infective endocarditis in the elderly: challenges and strategies. J Cardiovasc Dev Dis. (2022) 9:192. doi: 10.3390/jcdd9060192
29. Fernández Guerrero, ML, Aguado, JM, Arribas, A, Lumbreras, C, and de Gorgolas, M. The spectrum of cardiovascular infections due to Salmonella enterica: a review of clinical features and factors determining outcome. Medicine (Baltimore). (2004) 83:123–38. doi: 10.1097/01.md.0000125652.75260.cf
30. Baddour, LM, Wilson, WR, Bayer, AS, Fowler, VG, Tleyjeh, IM, Rybak, MJ, et al. Infective endocarditis in adults: diagnosis, antimicrobial therapy, and management of complications: a scientific statement for healthcare professionals from the American Heart Association. Circulation. 132:1435–86. doi: 10.1161/CIR.0000000000000296
Keywords: infective endocarditis, endocarditis, Salmonella typhi, Salmonella, typhoid
Citation: Jabeen K, Bint Ali S, Tufail Z, Mustafa S, Chaudhry M, Tahir MJ, Asghar MS and Ahmed A (2024) Salmonellatyphi and endocarditis: a systematic review of case reports. Front. Med. 11:1363899. doi: 10.3389/fmed.2024.1363899
Edited by:
Max Maurin, Centre Hospitalier Universitaire de Grenoble, FranceReviewed by:
Jyotshna Sapkota, Foundation for Innovative New Diagnostics, SwitzerlandCopyright © 2024 Jabeen, Bint Ali, Tufail, Mustafa, Chaudhry, Tahir, Asghar and Ahmed. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Muhammad Sohaib Asghar, c29oYWliX2FzZ2hhcjEyM0Bob3RtYWlsLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.