
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Med. , 22 April 2024
Sec. Dermatology
Volume 11 - 2024 | https://doi.org/10.3389/fmed.2024.1353354
This article is part of the Research Topic A Year in Review: Discussions in Dermatology View all 6 articles
 Lidia Rudnicka1*
Lidia Rudnicka1* Magdalena Trzeciak2
Magdalena Trzeciak2 Erkan Alpsoy3Petr Arenberger4Sibel Alper5Nina Benáková6Svetlana Bobko7
Erkan Alpsoy3Petr Arenberger4Sibel Alper5Nina Benáková6Svetlana Bobko7 Murat Borlu8
Murat Borlu8 Magdalena Czarnecka Operacz9
Magdalena Czarnecka Operacz9 Burhan Engin10Tülin Ergun11Ilgen Ertam Sağduyu12Olga Filipovská13Aida Gadzhigoroeva14Martina Kojanová6Aleksandra Lesiak15
Burhan Engin10Tülin Ergun11Ilgen Ertam Sağduyu12Olga Filipovská13Aida Gadzhigoroeva14Martina Kojanová6Aleksandra Lesiak15 Anna Michenko7,16,17
Anna Michenko7,16,17 Nikolay Murashkin18,19,20,21
Nikolay Murashkin18,19,20,21 Nahide Onsun22Witold Owczarek23Zuzana Plzakova6
Nahide Onsun22Witold Owczarek23Zuzana Plzakova6 Adam Reich24Marie Selerová25Burcu Aybike Gürbüz26
Adam Reich24Marie Selerová25Burcu Aybike Gürbüz26Objectives: This study aims to update the understanding of Alopecia Areata (AA) in Poland, Czechia, Russia, and Türkiye, focusing on the disease burden, clinical management, and patient journey. It seeks to establish a consensus on optimal management strategies for AA in these regions.
Methods: A modified 2-round Delphi panel was conveyed with 23 Dermatologists (Russia; 4, Türkiye; 7, Poland; 6, and Czechia; 6). The Delphi questionnaire consisted of 61 statements and 43 questions designed to obtain an overall understanding of the perception and acceptance of available information regarding the care of patients with alopecia areata.
Results: The study revealed that moderate-to-severe AA significantly impacts patients’ and their families’ QoL, consistent with previous studies. AA was found to cause more substantial impairment when additional lesions appeared in visible areas besides the scalp. Work and productivity impairment were notably higher in adults with moderate-to-severe AA. Diagnostic consensus highlighted the importance of skin biopsies and trichoscopy, while the need for more practical severity scoring systems was emphasized. Current treatments, including topical therapies, corticosteroids, and systemic immune modifiers, were deemed insufficient, highlighting the unmet medical need.
Conclusion: The Delphi study underscores a significant disease burden and unmet medical needs in patients with moderate-to-severe AA. It highlights the necessity of access to novel treatments and further research to develop more effective therapies with a tolerable safety profile. The findings align with global research, emphasizing the psychosocial impact of AA and the need for standardized, effective treatment protocols.
Alopecia areata (AA) is a common hair loss disorder with a wide range of clinical presentations. Although AA affects approximately 2% of the general population with an unpredictable clinical course and sudden relapse at any given time, robust and recent epidemiology data for AA are still lacking (1, 2). Current evidence suggests that the cause of the condition is autoimmune, with a significant genetic contribution, which is further influenced by unknown environmental factors. Reported triggers include emotional or physical stress, vaccinations, viral infections, and medications (3). While some patients experience spontaneous recovery, others progress to more extensive hair loss, including alopecia totalis and alopecia universalis, with a low chance of full recovery (4).
Current treatment options for AA include topical and intralesional corticosteroids, topical immunotherapy, and oral immunomodulators. However, the efficacy of these treatments varies, and there is no clear consensus on the optimal treatment pathway for AA (3, 5). In recent years, Janus kinase inhibitors (JAK inhibitors) have shown promise in the treatment of AA, with several studies reporting positive outcomes. However, there are concerns about the potential side effects and long-term safety of these drugs (5). Furthermore, the psychological impact of AA cannot be underestimated, as it can be a disfiguring disease with no available cure or therapies to prevent disease relapse.
While data on the global burden of AA are scarce, the disease has been shown to have a substantial impact on quality of life (QoL) (1). Disease management patterns for AA vary across countries; therefore, there is a need for a more comprehensive understanding of the disease burden, clinical management, and multiple aspects of the journey of patients with AA in different countries and regions (3, 5). This study aims to update our understanding of AA in Poland, Czechia, Russia, and Türkiye by obtaining information-driven insights from expert physicians regarding the current disease burden, clinical management, and multiple aspects of patients’ journey with AA. Ultimately, this study seeks to establish a consensus on the optimal management of AA in these regions.
We used a Modified Delphi Method for executing this study. The modified Delphi Method is a research technique that aims to achieve a consensus among a group of experts on specific issues. This method involves multiple rounds of surveys and discussions, typically over several months. The Delphi method is beneficial when limited data is available or when knowledge is uncertain or incomplete. There are no set rules for selecting the appropriate number of Delphi members or rounds. Still, generally, a classic Delphi strategy involves three or more rounds, while modified versions may be completed in just two rounds (6, 7).
The modified Delphi method used in this study consisted of two rounds of online surveys conducted over 2 years (between November 26, 2020, and November 2022). During each round, panel members were able to revise their earlier answers based on the responses of others. This modified method allowed for a literature review and multiple online surveys to transform expert opinions into a consensus-based group decision. The questionnaires used in this modified Delphi method can be obtained from corresponding author upon request.
At the outset of the study, a scientific committee consisting of four experienced dermatologists was formed, with one member acting as the study coordinator and three other members selected from Czechia, Poland, Türkiye, and Russia, respectively. The study coordinator oversaw the study’s design and progress, including data analysis and manuscript execution.
To ensure the study’s topics were adequately addressed, an independent expert consultant facilitated a discussion among the scientific committee members, who then selected and approved the relevant issues based on the limited world evidence available.
To participate in the study, candidates were selected based on their specific interests and extensive experience in alopecia areata. A total of 23 Dermatology specialists from universities and public hospitals in Russia, Türkiye, Poland, and Czechia were chosen, each with at least 10 years of experience with alopecia areata. Each panelist also had a proven track record in contributing to the field of alopecia areata, either by serving as a board member of an academic association, contributing to guideline development, or publishing articles on the topic. Finally, 22 participants equally contributed to the manuscript development and validated the final version. The independent expert consultant did not get involved in the manuscript development and she did not want to be included in the authors list. Due to a health problem, one participant could not participate in the second round and the validation of the final manuscript.
Before conducting the first round of the study questionnaire, the same independent consultant mentioned in the participant identification part also conducted a comprehensive literature review. The consultant searched for relevant articles published between 2010 and 2020 in several databases, including MEDLINE, Web of Science, Google Scholar, and EMBASE. The search terms used were focused on various aspects of alopecia areata, such as its burden, pathogenesis, etiology, diagnosis, severity, treatment, and response to treatment. The literature review also identified evidence-based recommendations and care pathways as selection criteria. Additionally, relevant guidelines published between 2010 and 2020 were systematically reviewed to ensure the study questionnaire aligned with current best practices. The consultant then prepared the survey questions to avoid participation bias among panelists. Based on the main topics identified in the literature review and guidelines, a total of 133 questions were developed for the study questionnaire, covering different aspects of alopecia areata, such as disease burden, diagnosis, severity, treatment, treatment response, treatment landscape, and unmet medical needs.
The questions were designed using a 5-point Likert response scale or multiple-choice answers with an additional open-ended choice to capture the panel members’ opinions. An electronic questionnaire was used to collect the panel members’ responses, and a consensus/dominant approach was achieved when 70% of the panel members strongly agreed or agreed (or strongly disagreed or disagreed) with a statement or selected the same answer. Statements with less than 40% agreement were dropped from the second Delphi round and not repeated.
Second round of the study delayed for a year and a half due to some of the participants’ serious health problems and several other logistic issues. The questions which were identified to be asked again at the second round were checked by the independent consultant to see if there has been any new significant developments in the evidence over the last year which might affect the validity of these questions. No significant change has been observed, therefore, identified questions were repeated, either using the same question or rephrased content based on the commentaries/corrections made by the participants during the first round. Inconsistencies between different countries were recognized as a non-consensus factor. This process ensured that the study questionnaire was designed based on the latest evidence and was aligned with current best practices.
The study questionnaire comprised five distinct sections, which aimed to evaluate various aspects of alopecia areata, such as disease burden, diagnosis, disease severity, treatment, treatment response, and unmet treatment needs. The questionnaire consisted of 61 statements and 43 questions designed to obtain an overall understanding of the perception and acceptance of available information regarding the care of patients with alopecia areata in the four countries included in the study.
All participants responded to all questions in the first round; however, one could not answer the second-round survey due to health problems. The consensus was reached on 53 of the 61 statement questions. The level of agreement ranged between 79 and 100%, with the highest consensus percentages observed in the diagnosis and disease severity sections and the lowest in the treatment section. Regarding the remaining 43 questions, the most common observations, perspectives, and clinical practices were reported in the disease burden and diagnosis. Furthermore, it was observed that the clinical practices for assessing disease flare, treatment response, and treatment preferences varied significantly between countries and even within each country (Table 1).
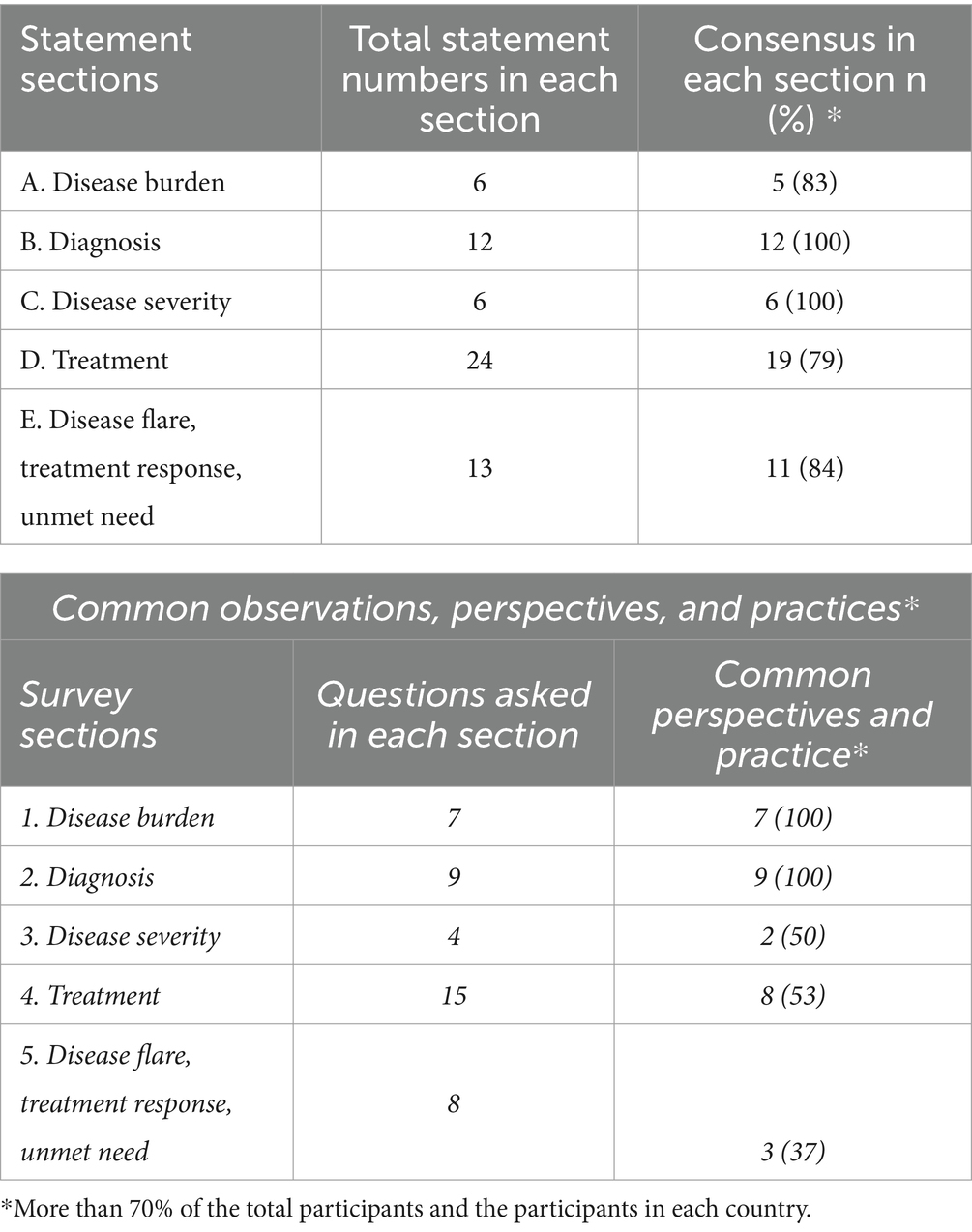
Table 1. General results.
The consensus was achieved on most of the statement items in this section. The highest consensus was the ‘Moderate-to-severe AA causes stigmatization in society.’ statement (100%). Participants agreed on the fact that all forms of AA cause considerable psychological disorders, while moderate-to-severe AA causes significant psychological disorders and results in a dramatic impact on the QoL for patients and their families (86.9, 91.2%). They also reported that additional lesions in visible areas beside the scalp (eyebrows, eyelashes, beard, etc.) impair the patient’s QoL to a greater extent (95.6%).
Despite participants agreed on that AA is perceived as an impairing and disabling disease in their societies, they also stated that AA-related impairments and disabilities are still not adequately publicized/emphasized enough in media to raise public awareness of the AA disease burden (86.9, 81.8, 78.2%). Additionally, QoL indexes and psychiatric consultations were not found to be performed as much as they should evaluate AA patients in daily practice (100, 81.8%) (Table 2).
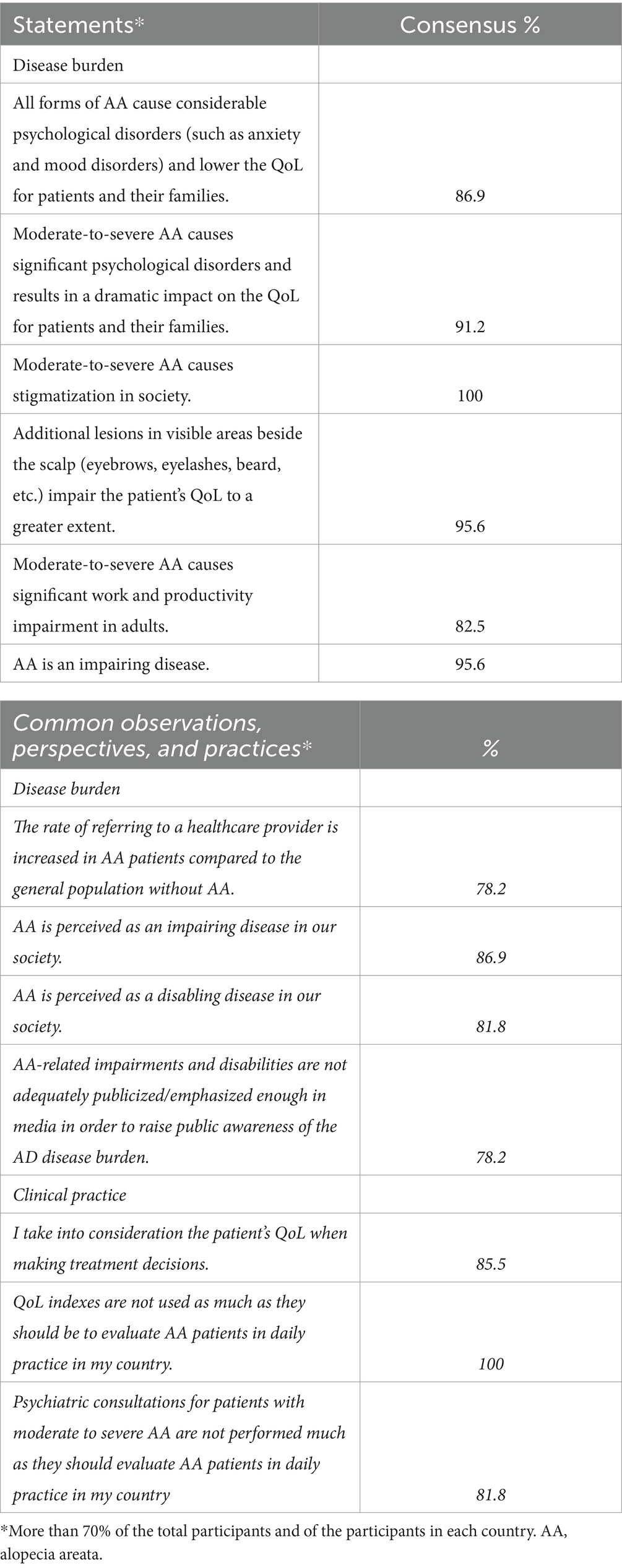
Table 2. Results regarding AA disease burden perception.
The consensus was achieved in all the statement items, and participants were also reported to be very similar regarding their observations, perspectives, and clinical practices for the diagnosis of AA (Table 3). The consensus with the highest percentages was ‘In certain situations, skin biopsies should be considered to exclude other conditions (e.g., when the cause of the hair loss is unclear),’ ‘Autoimmune comorbidities (such as vitiligo, systemic lupus erythematosus, psoriasis, inflammatory bowel disease, thyroid disorders, ocular diseases, and rheumatoid arthritis) are more common in AA patients. Compared to the general population without AA.’ (100, 95.6%).
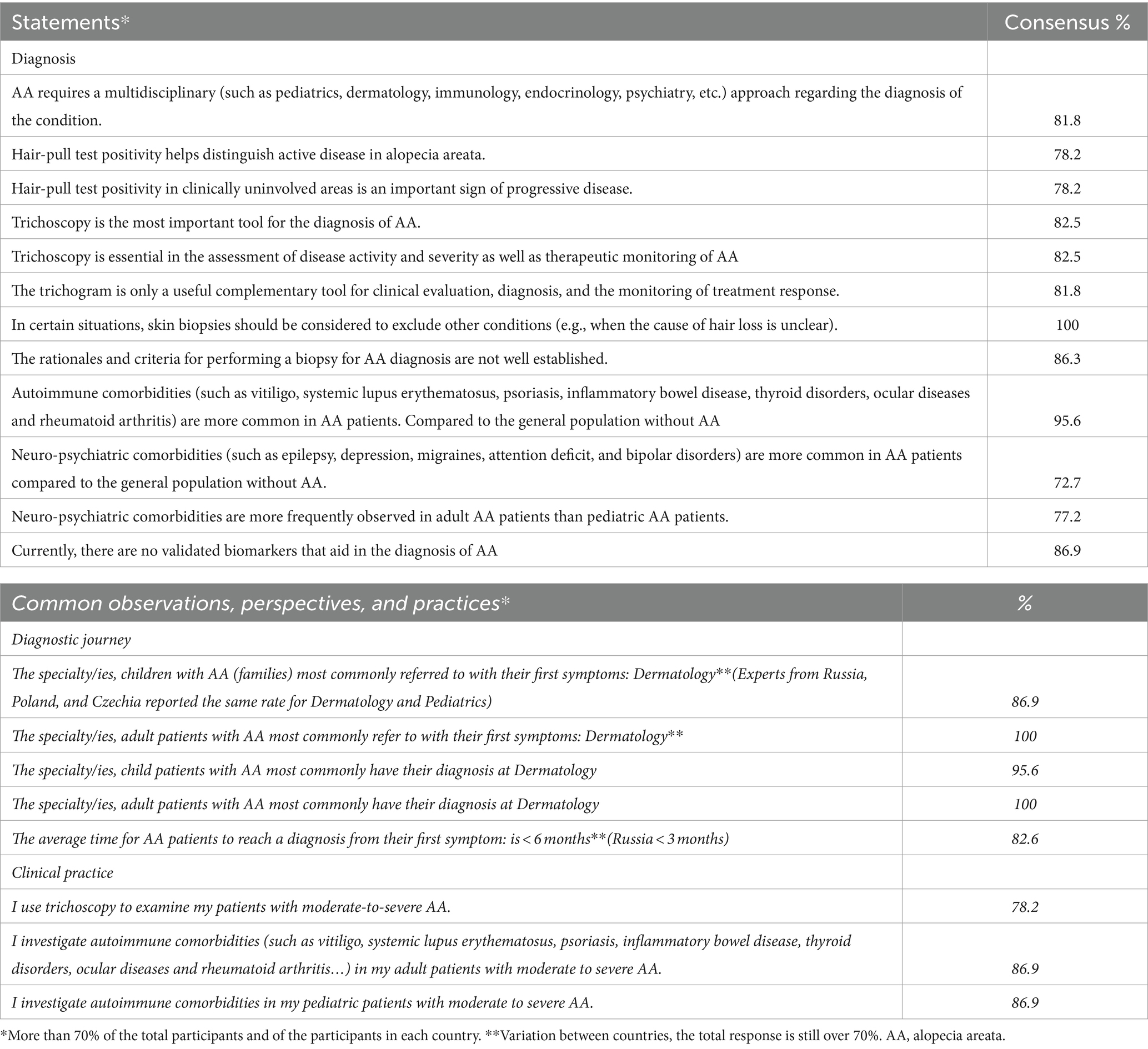
Table 3. Results regarding AD diagnostic approach and patient journey.
They agreed that trichoscopy is essential in the assessment of disease activity and severity as well as therapeutic monitoring of AA, whereas trichogram was found to be only a useful complementary tool for clinical evaluation, diagnosis, and the monitoring of treatment response (82.5, 81.8%). The vast majority of the participants stated that they use trichoscopy to examine patients with moderate-to-severe AA (78.2).
The consensus was achieved in all the statement items in this section. The highest consensus was for ‘AA patients with a hair loss of more than 50% on the scalp can be considered as severe AA.’ and ‘AA patients who have significantly impaired QoL may be considered as moderate-to-severe AA regardless of hair loss percentage on the scalp.’ (Table 4).
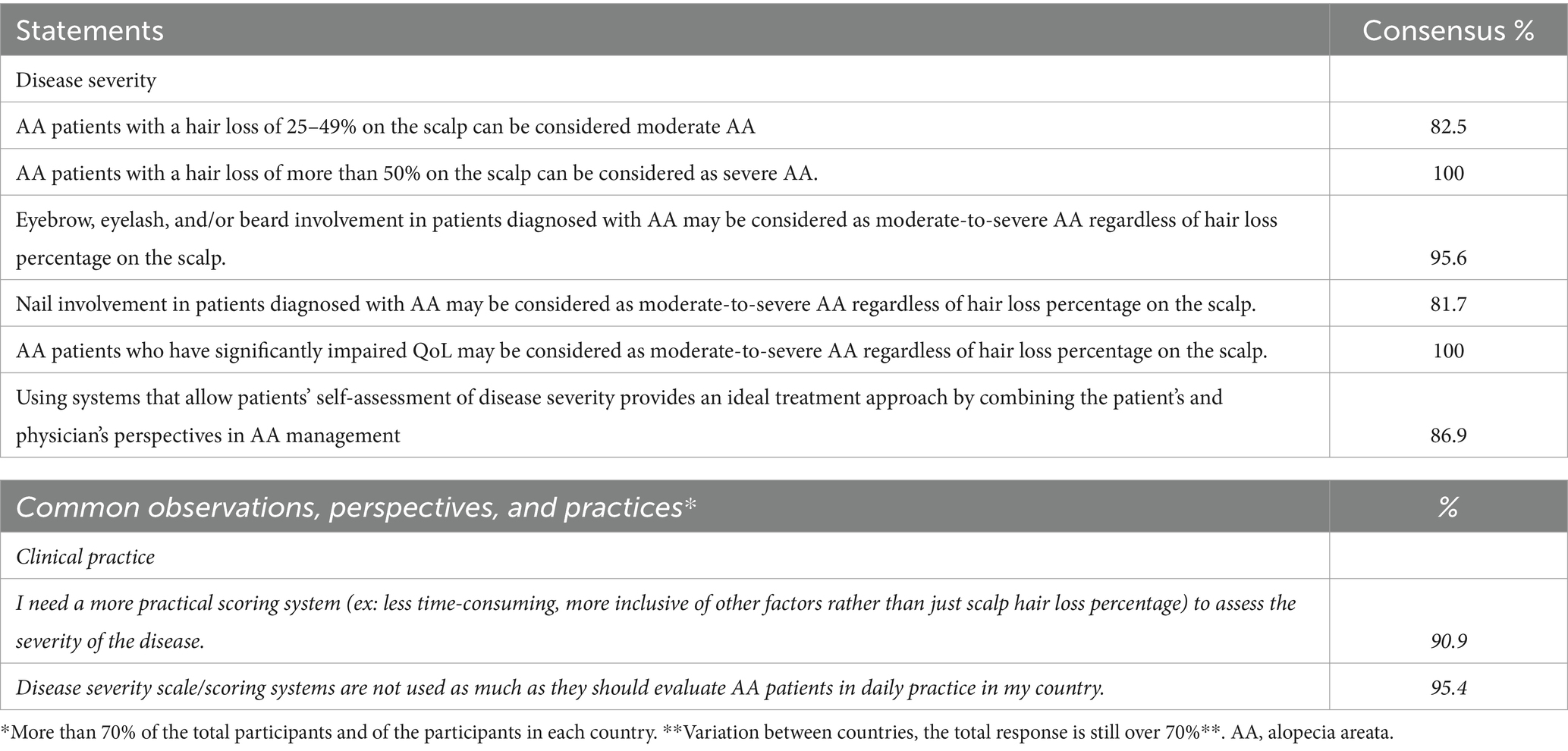
Table 4. Results regarding AA disease severity perception and assessment.
The treatment section had the lowest consensus percentage, indicating significant differences among participants, including those from the same country, in their preferred treatment approach and duration. However, there was full agreement on certain literature-based statements, such as the primary goals of stopping further hair loss and promoting hair regrowth in cases where curative treatment is not possible, as well as the use of systemic corticosteroids only for temporarily halting disease progression in patients with rapidly progressing, widespread, active disease, all of which received a 100% consensus.
Other consensuses with the highest percentages were; ‘In the event that curative treatment is impossible, improving the QoL is also a primary goal of the AA treatment.’, ‘Topical calcineurin inhibitors (TCIs) have lower efficacy than topical corticosteroids in alopecia areata.’ and ‘JAK inhibitor (with or without SCS) can be initiated as a first-line systemic treatment in children over 12 years old with moderate-to-severe AA in whom the disease could not be controlled with optimal topical/local therapies. (From a scientific perspective assuming JAK inhibitor treatment is available and reimbursed for this condition for your patients.)’ (91.3, 91.3, 90.9%) (Table 5).
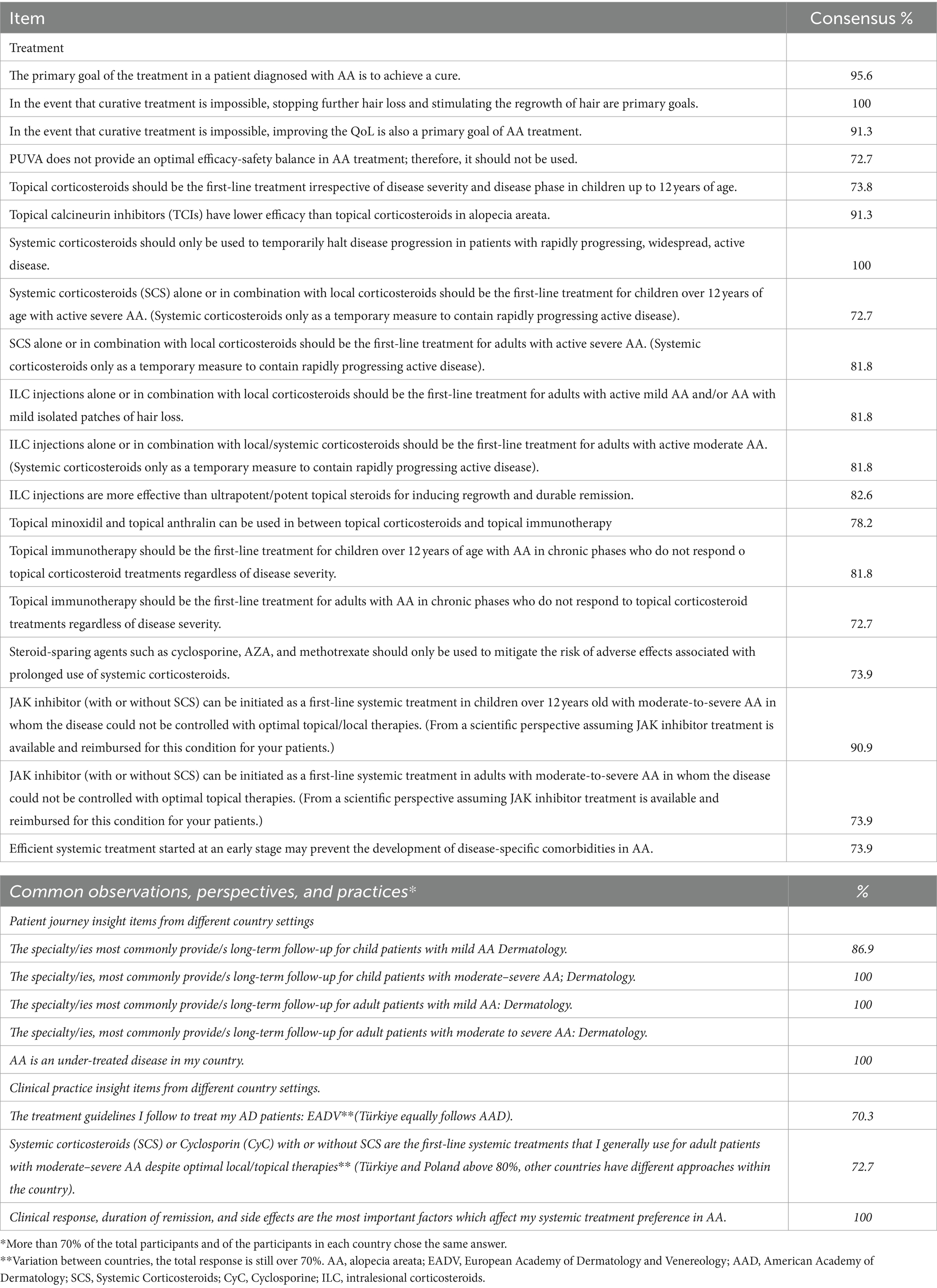
Table 5. Results regarding treatment preferences and management.
Panelists stated that defining an AA flare is a complex process, and there is a need for standardization in defining measures of long-term disease control; it should be assessed by disease severity scores (such as SALT, AA-IGA, etc.) and can be defined as an episode requiring escalation of treatment (95.6%). Panelists fully agreed that potential adverse effects associated with long-term use and the risk of relapse on dose reduction or treatment cessation limit the use of all conventional systemic therapies for AA. Panelists also agreed on multiple treatment failure definitions; the highest rated ones are as follows; Inadequate clinical improvement despite appropriate dose and duration of and adherence to a therapeutic agent and failure to achieve stable long-term disease control despite appropriate dose and duration of and adherence to a therapeutic agent (86.9%). Current topical therapies, intralesional corticosteroids, and systemic immune response modifiers were not found to be sufficient by panelists to cover the therapeutic needs of patients with moderate-to-severe AA (95.6, 86.9, 91.3%) (Table 6).
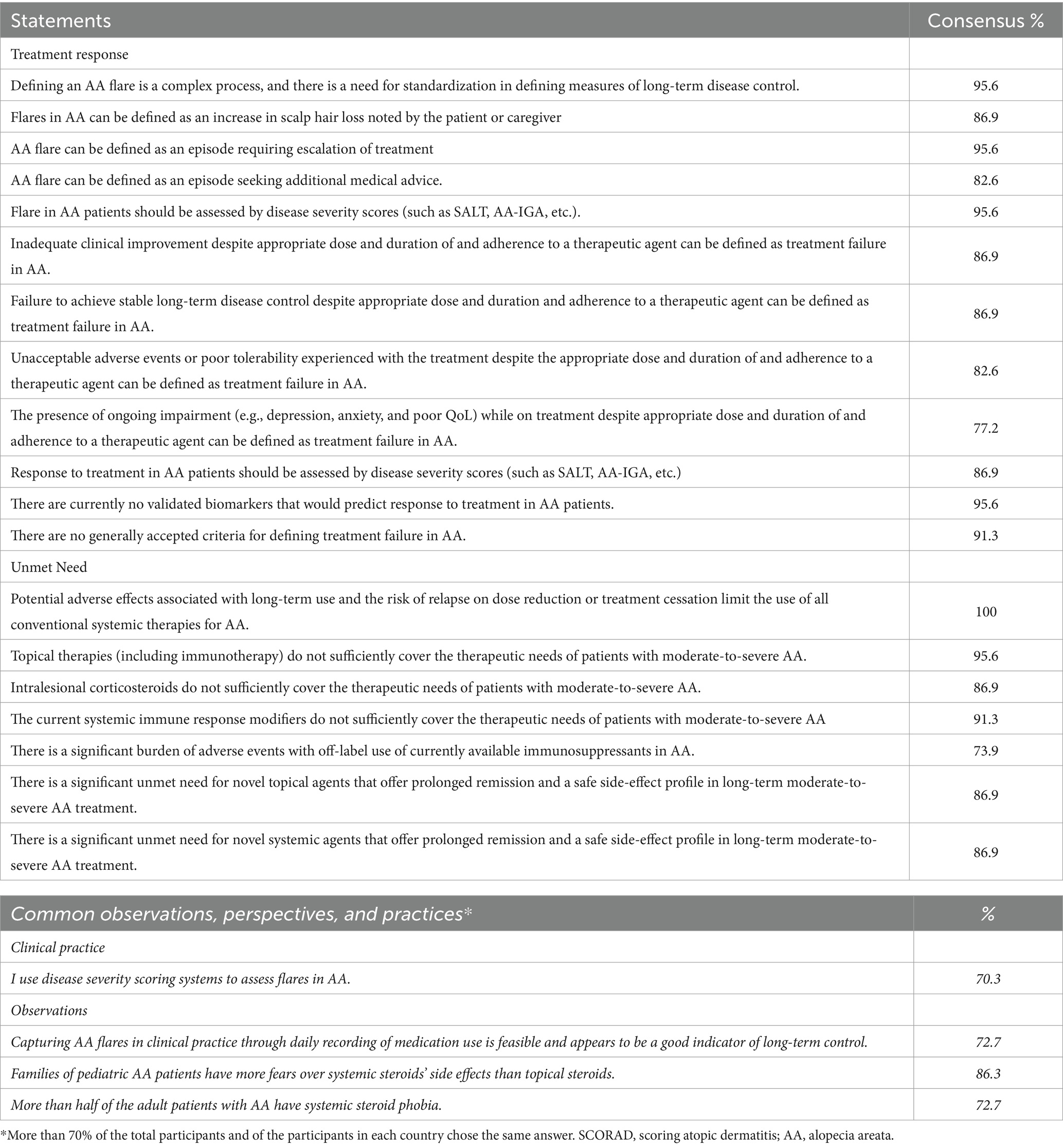
Table 6. Results regarding disease flare, treatment response, and unmet need perceptions and observations.
The results of this Delphi study revealed that moderate-to-severe AA has a significant impact on the QoL of patients and their families from physician perspectives. This finding is consistent with several patient-reported outcome studies conducted in various countries, all of which confirmed that AA patients have significantly lower QoL, significant psychosocial burden compared to those without AA and that the severity of AA was associated with poorer QoL outcomes (8–11). QoL in AA patients was also shown to be significantly worse compared to other patients with cutaneous conditions, such as androgenetic alopecia and psoriasis (12, 13). In a survey study carried out in the United States, not only did children with AA experience diminished health related QoL (HRQoL), but their parents also manifested significant impairment. The adverse influence of AA is similarly observed in the partners of affected adults. Interestingly, parents indicated a more pronounced decline in HRQoL than their AA-affected children. The emotional strain on parents was found to intensify due to the absence of clinical improvement after consulting with multiple healthcare professionals, undergoing unsuccessful treatments, and incurring financial costs (14).
Furthermore, the panelists agreed that additional AA lesions in visible areas besides the scalp cause more significant impairment in patients’ QoL. Cross-sectional research undertaken in the United States identified a correlation between the loss of eyebrows/eyelashes and ocular discomfort/functional disruptions. Meanwhile, the absence of scalp hair was linked to heightened sensitivity to temperature fluctuations and an elevated potential for sunburns. This underscores the influence on QoL, extending beyond mere self-perception and societal stigmatization (14).
The panelists also agreed that AA significantly impacts work and productivity impairment in adults with moderate-to-severe conditions. In a UK-based population study from primary healthcare environments, individuals with AA were found to receive work leave certificates at a higher rate (13.0% within a year of diagnosis) compared to matched controls (7.9%) (aHR 1.56, 95% CI 1.43–1.71; p < 0.001). Additionally, those diagnosed with AA demonstrated a higher likelihood of being recorded as unemployed in the subsequent year after their diagnosis (1.3% of cases of AA, 0.6% of matched controls; aHR 1.82, 95% CI 1.33–2.49) (15). In a cross-sectional study involving 216 USA-based AA patients (of which 132 were employed), it was observed that 45% of those employed had taken time off work due to their AA condition (16). Another assessment involving dermatologists and their adult AA patients highlighted the existence of work productivity loss (WPL) and activity disruption stemming from AA-related emotional symptoms (ES) (17). In a separate survey focusing on workplace bullying in AA patients, it was found that 21.7% (n = 146) had encountered workplace bullying. The most common manifestations of such bullying were having their views overlooked (53.8%, n = 362), being ostracized (47.7%, n = 321), and being the subject of rumors (44.0%, n = 296). Intriguingly, 75.0% (n = 120/160) of those who self-identified as victims of bullying confronted the behavior, yet in 30.8% of these instances, the bullying persisted (30.8%, n = 37) (18).
While the diagnosis of AA is primarily clinical, there are several nuances and challenges that clinicians encounter in making an exact diagnosis. One of the primary challenges in diagnosing AA lies in its resemblance to other forms of nonscarring alopecia, such as trichotillomania, traction alopecia, and telogen effluvium. Therefore, despite the characteristic clinical features of AA, there are instances where additional investigations may be warranted to confirm the diagnosis or exclude other conditions (19, 20). As per the diagnostic approach in AA, this study reported that participant physicians agree that skin biopsies should be considered to exclude other conditions when the cause of hair loss is unclear. Numerous research articles have indicated that scalp biopsies enhance diagnostic precision compared to mere examination, potentially influencing both prognosis and therapeutic decisions (19, 20). The panelists agreed that trichoscopy is an essential tool for the assessment of disease activity and severity, whereas trichogram was only found to be a useful complementary tool for clinical evaluation, diagnosis, and monitoring of treatment as well as therapeutic monitoring. These results align with prior research which highlighted the efficacy of trichoscopy in diagnosing and tracking AA. Multiple other investigations have established trichoscopy as not only a beneficial instrument for assessing hair loss but also as surpassing the trichogram in its effectiveness (21, 22).
Moreover, literature suggest that the presence of associated autoimmune conditions, such as thyroid disorders and vitiligo, should prompt further evaluation to assess for underlying autoimmune polyglandular syndromes or immune dysregulation in suspected AA patients (23). Vast majority of study participants stated that they investigate autoimmune comorbidities (such as vitiligo, systemic lupus erythematosus, psoriasis, inflammatory bowel disease, thyroid disorders, ocular diseases and rheumatoid arthritis.) in their adult and pediatric patients with moderate to severe AA (86.9%).
Negative prognostic factors associated with alopecia areata (AA) extend beyond autoimmune comorbidities, with emerging evidence suggesting correlations with atopy. Atopic dermatitis (AD), a chronic inflammatory skin condition characterized by pruritus and eczematous lesions, shares immunological pathways with AA, potentially influencing disease outcomes. Studies have reported increased prevalence of AD among AA patients, indicating a possible association between the two conditions (24). Furthermore, shared genetic susceptibility loci and dysregulated immune responses, particularly involving T-helper cell subsets and cytokine profiles, may contribute to the co-occurrence of AA and AD. Clinical observations suggest that patients with concurrent AA and AD may experience more severe disease manifestations and treatment challenges, highlighting the need for comprehensive management strategies.
AA patients with a hair loss of more than 50% on the scalp were agreed to be considered as having a severe AA. However, the practicality of existing severity indices, such as the Severity of Alopecia Tool (SALT) and Alopecia Areata Investigator Global Assessment (AA-IGA), remains questionable due to their limited sensitivity and applicability in routine clinical practice. The panelists also underlined the need for a more practical scoring system to assess the severity of AA. Existing scoring systems were not found sensitive enough to reflect AA’s complex and heterogeneous nature in other studies. Furthermore, the panelists reported that disease severity scales are not widely used in daily practice to evaluate AA patients in their countries. Indeed, studies from both the US and Europe have highlighted the inconsistent use of severity scales in daily patient evaluation, reflecting the need for more standardized and objective assessment tools (25, 26). Efforts to bridge the gap between research methodologies and clinical reality are imperative to enhance patient care. A holistic approach that integrates patient-reported outcomes, clinician assessments, and objective measures may offer a more comprehensive understanding of AA severity and treatment response in real-world settings.
The Delphi consensus study provided valuable insights into the management of AA, particularly in defining an AA flare, long-term disease control, and treatment failure definitions. Panelists agreed that defining an AA flare is complex, and there is a need for standardization in defining measures of long-term disease control. Severity indices, like SALT and AA-IGA, have been identified as effective instruments for gauging disease intensity and managing flare-ups. Research from both the US and Europe further emphasized the significance of these severity metrics in appraising AA patients and overseeing treatment outcomes, corroborating the consensus of the panelists (27, 28).
Regarding the treatment of moderate-to-severe AA, the panelists agreed that current therapies, including topical treatments, intralesional corticosteroids, and systemic immune response modifiers, are insufficient to cover patients’ therapeutic needs. Although numerous studies have demonstrated that topical minoxidil can promote new hair growth, using it as a standalone therapy yielded limited results. Specifically, hair growth was only observed in cases of mild AA, while it was ineffective for severe AA (29). On the other hand, topical immunotherapy employing diphenylcyclopropenone (DPCP) was proven to be successful in several research, promoting hair regrowth. However, there’s a considerable risk of side effects and relapse upon long-term observation (30, 31). A systematic review pinpointed systemic corticosteroids as effective in promoting hair regrowth among patients with severe AA, yet they come with substantial risks of side effects, including diabetes and osteoporosis (29). Furthermore, the scientific literature lacks a unified stance on the recommended dosage and duration for the daily use of systemic corticosteroids in AA treatments.
Moreover, the panelists acknowledged the significant burden of adverse events associated with the off-label use of currently available immunosuppressants, highlighting the importance of developing new therapies that offer a safe side-effect profile on long-term treatment. Expert opinion studies based on available evidence suggests that Cyclosporine is not a favored choice for AA due to its pronounced side-effect profile and considerable relapse rate. Such side effects encompass nephrotoxicity, immunosuppression, hypertension, and excessive body hair growth, known as hypertrichosis (32). Furthermore, the use of oral methotrexate for alopecia areata has been linked to severe adverse events, including gastrointestinal issues and liver toxicity (33). All available evidence strongly emphasizes the need for developing new therapies that promise enhanced safety and more acceptable tolerability for AA patients.
Recent studies have reported promising results in using Janus kinase inhibitors (JAK inhibitors) for the treatment of AA (34–39). A recent systematic review and meta-analysis, encompassing 7 randomized clinical trials and involving 1710 patients, demonstrated that JAK inhibitors were more efficacious in promoting hair regrowth than placebos. Notably, the effectiveness of oral JAK inhibitors appeared superior to topical applications, and there was no observed increase in treatment-related adverse events (AEs) when compared to placebos (40). Baricitinib is approved for use only in adult severe AA patients, whereas ritlecitinib is approved for the same use in people ages 12 years and older. While JAK inhibitors offer promising therapeutic benefits and now in clinical use, concerns regarding their safety profile remain. The most common adverse effects due to oral JAK inhibitors were upper respiratory tract infections, urinary infections, headache, laboratory abnormality, and acne. These side-effects are similar to those reported in previous reviews of JAK inhibitors in patients with alopecia. Laboratory abnormalities included cytopaenias, lipid abnormalities, and an increase in blood creatine phosphokinase. No cases of reactivation of tuberculosis or new malignancies were reported (41). Despite serious adverse effects being less reported in AA studies, it is important to highlight that data regarding the safety of JAK inhibitors in relation to AA is still in its infancy. Data from clinical trials have underscored the importance of careful patient selection, particularly in individuals with cardiovascular comorbidities, to mitigate potential risks associated with JAK inhibitor therapy. Moreover, proactive measures such as herpes zoster vaccination may serve to minimize the risk of opportunistic infections in patients undergoing treatment with JAK inhibitors.
The high cost of JAK inhibitors may limit their accessibility to some patients. Therapeutic challenges in alopecia areata (AA) may present unique considerations especially in Central Eastern Europe, Türkiye or Russia, reflecting regional variations in healthcare access, treatment availability, and patient preferences. While conventional treatments such as topical corticosteroids and systemic immunosuppressants are commonly used, challenges may arise due to limited access to newer therapies like Janus kinase inhibitors (JAK inhibitors). Despite both FDA approved JAK inhibitors are also approved by EMA, they are still not reimbursed in some CEE countries or available through self-funding for AA. Studies suggest that economic factors and regulatory barriers may impact the adoption of innovative treatments, potentially affecting treatment outcomes. Additionally, cultural perceptions of hair loss and dermatological conditions may influence patient attitudes toward seeking medical care and adherence to treatment regimens (42). Collaborative efforts between healthcare providers, policymakers, and patient advocacy groups are essential to address these challenges and improve the management of AA in the region.
In conclusion, the findings of this Delphi study demonstrate a significant disease burden and unmet medical need for patients with moderate-to-severe AA from the perspective of experts. These findings are consistent with previous studies conducted in different countries, highlighting the need for and importance of providing patients access to recently approved novel treatments and for further research to develop more effective therapies with tolerable safety profile for AA.
The limitations of this study are inherent in the nature of the Delphi method. One limitation is the small number of experts and differences in the representation of each country, which may not fully reflect the approaches and insights of the majority of experts at an ideal level. Additionally, the absence of AA patients on the panel limits the ability to reflect their perspectives on the disease burden and unmet treatment needs. The delay between 2 rounds might have an effect on the validity of participants’ current opinion, however none of the participants objected nor wanted to revise any claims on these outcomes. Additionally, this Delphi study also enabled a comprehensive and systematic exploration of clinical, diagnostic, and follow-up approaches in patients with AA based on the expert opinions of qualified dermatologists in Poland, Czechia, Russia, and Türkiye within a limited time frame. The findings and limitations of this study can serve as reference points to initiate and establish more focused and populated consensus studies not only in these countries but also in other developing countries.
The original contributions presented in the study are included in the article as well as in supplementary material which can be obtained from the corresponding author.
LR: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Supervision, Validation, Writing – review & editing. MT: Investigation, Validation, Writing – review & editing. EA: Validation, Writing – review & editing. PA: Validation, Writing – review & editing. SA: Validation, Writing – review & editing. NB: Validation, Writing – review & editing. SB: Validation, Writing – review & editing. MB: Validation, Writing – review & editing. MC: Validation, Writing – review & editing. BE: Validation, Writing – review & editing. TE: Validation, Writing – review & editing. IS: Validation, Writing – review & editing. OF: Validation, Writing – review & editing. AG: Validation, Writing – review & editing. MK: Validation, Writing – review & editing. AL: Validation, Writing – review & editing. AM: Validation, Writing – review & editing. NM: Validation, Writing – review & editing. NO: Validation, Writing – review & editing. WO: Validation, Writing – review & editing. ZP: Validation, Writing – review & editing. AR: Validation, Writing – review & editing. MS: Validation, Writing – review & editing. BG: Validation, Writing – review & editing.
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This study was funded by Pfizer. Project management and technical support was provided by Remedium Consulting Group and funded by Pfizer. Pfizer employees did not have any involvement in the achieved consensus nor the decision for journal submission.
Project management, interview with panelists, panel moderation and analysis of the results, medical writing, submission secretariat are provided by, Dr. Ferda Kiziltas, and Feride Ucar at Remedium Consulting Group.
PA has acted in advisory board of AbbVie, Bristol Myers Squibb, Merck Sharp Dohme, Novartis, Pfizer Pharmaceuticals, and has received speaker honorarium from Pfizer, Abbvie. MK has served as consultant, speaker, or investigator for Abbvie, Almirall, Amgen, Eli Lilly, Janssen, Leo Pharma, Novartis, Pfizer, Sanofi and UCB. MC has acted on the advisory board of Novartis, Pfizer Pharmaceuticals, and Bristol Myers Squibb and has received a speaker honorarium from Pfizer, Abbvie, OF has acted in advisory board of Novartis, Lilly, LeoPharma, Almirall and in clinical studies Pfizer, Janssen, Lilly, Amgen, Abbvie, Novartis, Regeneron. AM has acted in advisory board of Novartis, Pfizer Pharmaceuticals, and Bristol Myers Squibb and has received speaker honorarium from L’Oreal, La Roche Posay. MT has been a speaker and/or consultant an/or investigator and/or participant of Advisory Board of Abbvie, BauschHealth, Bioderma, Eli Lilly, La Roche, Leo pharma, Novartis, Pfizer, Pierre-Fabre, Sanofi Genzyme. ZP has acted in advisory board of Novartis, Pfizer Pharmaceuticals, and Bristol Myers Squibb and has received speaker honorarium from Pfizer, Abbvie. IS has acted in advisory board of Novartis, Pfizer Pharmaceuticals, and Bristol Myers Squibb and has received speaker honorarium from Pfizer, Abbvie. WO received honorarium for lectures and clinical research from AbbVie, Aflofarm Farmacja, Alfasigma, Almirall, Amgen, Apotex Polska Astellas Pharma, AstraZeneca, Bausch Health Poland, Berlin Chemie Menarini, Boehringer Ingelheim, Bristol Myers Squibb, EGIS, Eli Lilly, Galderma, Janssen-Cilag, LEO Pharma, Medac GmbH, Merck, Mylan Healthcare, Novartis, Pfizer, Pierre Fabre Medicamente, TZF Polfa S.A., Roche Diagnostics, Sandoz, Sanofi-Aventis, SUN-FARM, Teva Pharmaceuticals, UCB Pharma. AL has acted in advisory board of Novartis, Pfizer Pharmaceuticals, Abbvie, Sanofie, Sandoz, Lilly, Janssen, Almiral and has received speaker honorarium from Pfizer, Abbvie, Novartis, Pfizer Pharmaceuticals, Abbvie, Sanofie, Sandoz, Lilly, Almiral, UCB. AG has received speaker honorarium from Pfizer. NM reports grants and personal fees from Jansen, grants from Eli Lilly, grants and personal fees from Novartis, personal fees from Galderma, personal fees from Pierre Fabre, personal fees from Bayer, personal fees from Leofarma, grants and personal fees from Pfizer, grants and personal fees from AbbVie, grants from Amryt Pharma, personal fees and non-financial support from Viatris, outside the submitted work. NB declare to have acted as member of Advisory Board of Pfizer Pharmaceuticals and has received speaker honorarium from Pfizer. SB has received speaker honorarium from Pfizer, LEO PHARMAEB has acted in advisory board of Novartis and Pfizer Pharmaceuticals has received speaker honorarium from Pfizer, Abbvie. SA has acted in advisory board of Novartis, Pfizer and Bristol Myers Squibb, and has received honorarium from Pfizer and Abbvie. AR has worked as a consultant or speaker for AbbVie, Bioderma, Celgene, Chema Elektromet, Eli Lilly, Galderma, Janssen, Leo Pharma, Medac, Menlo Therapeutics, Novartis, Pierre-Fabre, Sandoz and Trevi and has participated as principal investigator in clinical trials sponsored by AbbVie, Almirall, Amgen, Anaptys, Argenx, Biogen, Biothera, BMS, Celltrion, Dermira, Dice, Evelo, Galderma, Genentech, Horizon Therapeutics, Incyte, Janssen, Kymab Ltd., Leo Pharma, Eli Lilly, Menlo Therapeutics, MetrioPharm, MSD, Novartis, Pfizer, Regeneron, Sanofi, Takeda, Trevi, and UCB. BG is an employee of Pfizer.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Villasante Fricke, AC, and Miteva, M. Epidemiology and burden of alopecia areata: a systematic review. Clin Cosmet Investig Dermatol. (2015) 8:397–403. doi: 10.2147/CCID.S53985
2. Lee, HH, Gwillim, E, Patel, KR, Hua, T, Rastogi, S, Ibler, E, et al. Epidemiology of alopecia areata, ophiasis, totalis, and universalis: a systematic review and meta-analysis. J Am Acad Dermatol. (2020) 82:675–82. doi: 10.1016/j.jaad.2019.08.032
3. Strazzulla, LC, Wang, EHC, Avila, L, Lo Sicco, K, Brinster, N, Christiano, AM, et al. Alopecia areata: disease characteristics, clinical evaluation, and new perspectives on pathogenesis. J Am Acad Dermatol. (2018) 78:1–12. doi: 10.1016/j.jaad.2017.04.1141
4. Alkhalifah, A, Alsantali, A, Wang, E, McElwee, KJ, and Shapiro, J. Alopecia areata update: part I. Clinical picture, histopathology, and pathogenesis. J Am Acad Dermatol. (2010) 62:177–88. doi: 10.1016/j.jaad.2009.10.032
5. Malhotra, K, and Madke, B. An updated review on current treatment of alopecia areata and newer therapeutic options. Int J Trichology. (2023) 15:3–12. doi: 10.4103/ijt.ijt_28_21
6. Keeney, S, McKenna, H, and Hasson, F. The delphi technique in nursing and health research. Int J Nurs Stud. (2011) 38:195–200.
7. Hsu, C-C, and Sandford, BA. The Delphi technique: making sense of consensus. Pract Assess Res Eval. (2007) 12:1–8.
8. Ito, T, Kamei, K, Yuasa, A, Matsumoto, F, Hoshi, Y, Okada, M, et al. Health-related quality of life in patients with alopecia areata: results of a Japanese survey with norm-based comparisons. J Dermatol. (2022) 49:584–93. doi: 10.1111/1346-8138.16364
9. Masmoudi, J, Sellami, R, Ouali, U, Mnif, L, Feki, I, Amouri, M, et al. Quality of life in alopecia areata: a sample of Tunisian patients. Dermatol Res Pract. (2013) 2013:983804:1–5. doi: 10.1155/2013/983804
10. Shi, Q, Duvic, M, Osei, JS, Hordinsky, MK, Norris, DA, Price, VH, et al. Health-related quality of life (HRQoL) in alopecia areata patients—a secondary analysis of the national alopecia areata registry data. J Investig Dermatol Symp Proc. (2013) 16:S49–50. doi: 10.1038/jidsymp.2013.18
11. Qi, S, Xu, F, Sheng, Y, and Yang, Q. Assessing quality of life in alopecia areata patients in China. Psychol Health Med. (2015) 20:97–102. doi: 10.1080/13548506.2014.894641
12. Jun, M, Keum, DI, Lee, S, Kim, BJ, and Lee, W-S. Quality of life with alopecia areata versus androgenetic alopecia assessed using hair specific skindex-29. Ann Dermatol. (2018) 30:388–91. doi: 10.5021/ad.2018.30.3.388
13. Karia, SB, De Sousa, A, Shah, N, Sonavane, S, and Bharati, A. Psychiatric morbidity and quality of life in skin diseases: a comparison of alopecia areata and psoriasis. Indust Psychiatr J. (2015) 24:125. doi: 10.4103/0972-6748.181724
14. Liu, LY, King, BA, and Craiglow, BG. Alopecia areata is associated with impaired health-related quality of life: a survey of affected adults and children and their families. J Am Acad Dermatol. (2018) 79:556–558.e1. doi: 10.1016/j.jaad.2018.01.048
15. Macbeth, AE, Holmes, S, Harries, M, Chiu, WS, Tziotzios, C, de Lusignan, S, et al. The associated burden of mental health conditions in alopecia areata: a population-based study in UK primary care. Br J Dermatol. (2022) 187:73–81. doi: 10.1111/bjd.21055
16. Mesinkovska, N, King, B, Mirmirani, P, Ko, J, and Cassella, J. Burden of illness in alopecia areata: a cross-sectional online survey study. J Investig Dermatol Symp Proc. (2020) 20:S62–8. doi: 10.1016/j.jisp.2020.05.007
17. Gandhi, K, Shy, ME, Ray, M, Fridman, M, Vaghela, S, and Mostaghimi, A. The association of alopecia areata-related emotional symptoms with work productivity and daily activity among patients with alopecia Areata. Dermatol Ther. (2023) 13:285–98. doi: 10.1007/s13555-022-00864-1
18. Li, SJ, Reyes-Hadsall, S, Drake, L, Huang, K, and Mostaghimi, A. Experiencing workplace bullying in patients with alopecia areata: a cross-sectional survey study. Skin Appendage Disord. (2023) 9:258–61. doi: 10.1159/000529924
19. Douglas, A, Romisher, A, Cohen, A, Zaya, R, Wang, J, Suriano, J, et al. Scalp biopsy influences diagnostic accuracy and treatment in black women with alopecia: a retrospective study. J Am Acad Dermatol. (2023) 88:1375–6. doi: 10.1016/j.jaad.2023.01.022
20. Marwah, M, Nadkarni, N, and Patil, S. 'Ho-ver'ing over alopecia areata: histopathological study of 50 cases. Int J Trichology. (2014) 6:13–8. doi: 10.4103/0974-7753.136749
21. Galliker, NA, and Trüeb, RM. Value of trichoscopy versus trichogram for diagnosis of female androgenetic alopecia. Int J Trichology. (2012) 4:19–22. doi: 10.4103/0974-7753.96080
22. Bhamla, SA, Dhurat, RS, and Saraogi, PP. Is trichoscopy a reliable tool to diagnose early female pattern hair loss? Int J Trichology. (2013) 5:121–5. doi: 10.4103/0974-7753.125603
23. Yuan, J, Sun, C, Jiang, S, Lu, Y, Zhang, Y, Gao, XH, et al. The prevalence of thyroid disorders in patients with vitiligo: a systematic review and meta-analysis. Front Endocrinol. (2019) 9:803. doi: 10.3389/fendo.2018.00803
24. Sun, R, and Kong, D. Bilateral association between atopic dermatitis and alopecia Areata: a systematic review and meta-analysis. Dermatitis. (2023). doi: 10.1089/derm.2023.0114
25. King, BA, Senna, MM, Ohyama, M, Tosti, A, Sinclair, RD, Ball, S, et al. Defining severity in alopecia Areata: current perspectives and a multidimensional framework. Dermatol Ther. (2022) 12:825–34. doi: 10.1007/s13555-022-00711-3
26. Reid, EE, Haley, AC, Borovicka, JH, Rademaker, A, West, DP, Colavincenzo, M, et al. Clinical severity does not reliably predict quality of life in women with alopecia areata, telogen effluvium, or androgenic alopecia. J Am Acad Dermatol. (2012) 66:e97–e102. doi: 10.1016/j.jaad.2010.11.042
27. Olsen, E, Roberts, J, Sperling, L, Tosti, A, Shapiro, J, McMichael, A, et al. Objective outcome measures: collecting meaningful data on alopecia Areata. J Am Acad Dermatol. (2017) 79:470–478.e3. doi: 10.1016/j.jaad.2017.10.048
28. Lintzeri, DA, Constantinou, A, Hillmann, K, Ghoreschi, K, Vogt, A, and Blume-Peytavi, U. Alopecia areata – current understanding and management. JDDG. J Dtsch Dermatol Ges. (2022) 20:59–90. doi: 10.1111/ddg.14689
29. Strazzulla, LC, Wang, EHC, Avila, L, Lo Sicco, K, Brinster, N, Christiano, AM, et al. Alopecia areata: an appraisal of new treatment approaches and overview of current therapies. J Am Acad Dermatol. (2018) 78:15–24. doi: 10.1016/j.jaad.2017.04.1142
30. Van der Steen, PHM, Boezeman, JBM, and Happle, R. Topical immunotherapy for alopecia areata: re-evaluation of 139 cases after an additional follow-up of 19 months. Dermatology. (1992) 184:198–201. doi: 10.1159/000247540
31. Wiseman, MC, Shapiro, J, McDonald, N, and Lui, H. Predictive model for immunotherapy of alopecia areata with diphencyprone. Arch Dermatol. (2001) 137:1063–8.
32. Alkhalifah, A, Alsantali, A, Wang, E, McElwee, KJ, and Shapiro, J. Alopecia areata update: part II. Treatment J Am Acad Dermatol. (2010) 62:191–202. doi: 10.1016/j.jaad.2009.10.031
33. Ramírez-Marín, HA, and Tosti, A. Emerging drugs for the treatment of alopecia areata. Expert Opin Emerg Drugs. (2022) 27:379–87. doi: 10.1080/14728214.2022.2149735
34. King, B, Guttman-Yassky, E, Peeva, E, Banerjee, A, Sinclair, R, Pavel, AB, et al. A phase 2a randomized, placebo-controlled study to evaluate the efficacy and safety of the oral Janus kinase inhibitors ritlecitinib and brepocitinib in alopecia areata: 24-week results. J Am Acad Dermatol. (2021) 85:379–87. doi: 10.1016/j.jaad.2021.03.050
35. Olsen, EA, Kornacki, D, Sun, K, and Hordinsky, MK. Ruxolitinib cream for the treatment of patients with alopecia areata: a 2-part, double-blind, randomized, vehicle-controlled phase 2 study. J Am Acad Dermatol. (2020) 82:412–9. doi: 10.1016/j.jaad.2019.10.016
36. Mikhaylov, D, Glickman, JW, del Duca, E, Nia, J, Hashim, P, Singer, GK, et al. A phase 2a randomized vehicle-controlled multi-center study of the safety and efficacy of delgocitinib in subjects with moderate-to-severe alopecia areata. Arch Dermatol Res. (2023) 315:181–9. doi: 10.1007/s00403-022-02336-0
37. King, B, Mesinkovska, N, Mirmirani, P, Bruce, S, Kempers, S, Guttman-Yassky, E, et al. Phase 2 randomized, dose-ranging trial of CTP-543, a selective Janus kinase inhibitor, in moderate-to-severe alopecia areata. J Am Acad Dermatol. (2022) 87:306–13. doi: 10.1016/j.jaad.2022.03.045
38. King, B, Ko, J, Forman, S, Ohyama, M, Mesinkovska, N, Yu, G, et al. Efficacy and safety of the oral Janus kinase inhibitor baricitinib in the treatment of adults with alopecia areata: phase 2 results from a randomized controlled study. J Am Acad Dermatol. (2021) 85:847–53. doi: 10.1016/j.jaad.2021.05.050
39. King, B, Ohyama, M, Kwon, O, et al. Two phase 3 trials of baricitinib for alopecia areata. N Engl J Med. (2022) 386:1687–99. doi: 10.1056/NEJMoa2110343
40. Liu, M, Gao, Y, Yuan, Y, Yang, K, Shen, C, Wang, J, et al. Janus kinase inhibitors for alopecia Areata: a systematic review and meta-analysis. JAMA Netw Open. (2023) 6:e2320351. doi: 10.1001/jamanetworkopen.2023.20351
41. Phan, K, and Sebaratnam, DF. JAK inhibitors for alopecia areata: a systematic review and meta-analysis. J Eur Acad Dermatol Venereol. (2019) 33:850–6. doi: 10.1111/jdv.15489
Keywords: alopecia areata, disease burden, diagnosis, treatment, clinical management
Citation: Rudnicka L, Trzeciak M, Alpsoy E, Arenberger P, Alper S, Benáková N, Bobko S, Borlu M, Czarnecka Operacz M, Engin B, Ergun T, Sağduyu IE, Filipovská O, Gadzhigoroeva A, Kojanová M, Lesiak A, Michenko A, Murashkin N, Onsun N, Owczarek W, Plzakova Z, Reich A, Selerová M and Gürbüz BA (2024) Disease burden, clinical management and unmet treatment need of patients with moderate to severe alopecia areata; consensus statements, insights, and practices from CERTAAE (Central/Eastern EU, Russia, Türkiye AA experts) Delphi panel. Front. Med. 11:1353354. doi: 10.3389/fmed.2024.1353354
Edited by:
Ralf J. Ludwig, University of Lübeck, GermanyReviewed by:
Alvise Sernicola, University of Padua, ItalyCopyright © 2024 Rudnicka, Trzeciak, Alpsoy, Arenberger, Alper, Benáková, Bobko, Borlu, Czarnecka Operacz, Engin, Ergun, Sağduyu, Filipovská, Gadzhigoroeva, Kojanová, Lesiak, Michenko, Murashkin, Onsun, Owczarek, Plzakova, Reich, Selerová and Gürbüz. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lidia Rudnicka, bGlkaWFydWRuaWNrYUBnbWFpbC5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.