 Charlene Desaintjean1
Charlene Desaintjean1 Kaïs Ahmad1Julie Traclet1Mathieu Gerfaud-Valentin2†Cecile-Audrey Durel2†Jean-Charles Glerant3
Kaïs Ahmad1Julie Traclet1Mathieu Gerfaud-Valentin2†Cecile-Audrey Durel2†Jean-Charles Glerant3 Arnaud Hot4François Lestelle1Sabine Mainbourg5,6†
Arnaud Hot4François Lestelle1Sabine Mainbourg5,6† Mouhamad Nasser1†
Mouhamad Nasser1† Pascal Seve7,8Ségolène Turquier3†Gilles Devouassoux9,10,11†
Pascal Seve7,8Ségolène Turquier3†Gilles Devouassoux9,10,11† Vincent Cottin1,12*†
Vincent Cottin1,12*†- 1Department of Respiratory Medicine, National Reference Centre for Rare Pulmonary Diseases, Member of ERN-LUNG, Louis Pradel Hospital, Hospices Civils de Lyon, Lyon, France
- 2Department of Internal Medicine, Hôpital Saint-Joseph Saint-Luc, Lyon, France
- 3Pulmonary Function Tests Department, Louis Pradel Hospital, Hospices Civils de Lyon, Lyon, France
- 4Department of Internal Medicine, Edouard Herriot Hospital, Hospices Civils de Lyon, Lyon, France
- 5Department of Internal Medicine and Vascular Medicine, Lyon Sud Hospital, and Lyon Immunopathology Federation (LIFe), Hospices Civils de Lyon, Lyon, France
- 6UMR 5558, Laboratoire de Biométrie et Biologie Evolutive, Claude Bernard University Lyon 1, Lyon, France
- 7Department of Internal Medicine, Hôpital de la Croix Rousse, Hospices Civils de Lyon, Lyon, France
- 8Research on Healthcare Performance (RESHAPE), INSERM U1290, Claude Bernard University Lyon 1, Lyon, France
- 9Department of Respiratory Medicine, CIERA, Hôpital de la Croix Rousse, Hospices Civils de Lyon, Lyon, France
- 10CRISALIS INSERM, F-CRIN Network, Toulouse, France
- 11VirPath, INSERM U1111-CNRS UMR 5308-ENS de Lyon, Université Claude Bernard Lyon 1, Lyon, France
- 12UMR 754, INRAE, Claude Bernard University Lyon 1, Lyon, France
Introduction: Asthma associated with eosinophilic granulomatosis with polyangiitis (EGPA) is often severe and corticosteroid-dependent, leading to significant morbidity. Mepolizumab and benralizumab are humanized monoclonal antibodies targeting interleukin 5 (IL-5) and its receptor, respectively. They have been shown to be effective in steroid-sparing in patients with severe eosinophilic asthma.
Objective: Our aim was to evaluate the efficacy and safety of mepolizumab and benralizumab prescribed for severe asthma in patients with EGPA under “real-world” conditions.
Methods: This was a retrospective analysis of patients with EGPA and persistent asthma who received either mepolizumab 100 or 300 mg administered every 4 weeks, or benralizumab 30 mg administered every 4 weeks for the initial 3 injections and followed by an injection every 8 weeks thereafter, whilst combined with oral glucocorticoids. The follow-up every 6 ± 3 months included an assessment of clinical manifestations, pulmonary function tests and eosinophil cell count. The primary outcome was the proportion of patients at 12 months receiving a daily oral dose of prednisone or equivalent of 4 mg or less with a BVAS of 0.
Results: Twenty-six patients were included. After 12 months of treatment with mepolizumab or benralizumab, 32% of patients met the primary outcome and were receiving less than 4 mg of prednisone per day with a BVAS of 0. The median dose of prednisone was 10 mg per day at baseline, 9 mg at 6 months, and 5 mg at 12 months (p ≤ 0.01). At 12 months, 23% of patients were weaned off corticosteroids, while an increase or no change in dose was observed in 27% of patients. The median eosinophil count was significantly reduced from 365 cells/mm3 to 55 cells/mm3 at 6 months and 70 cells/mm3 at 12 months, respectively. No significant change was observed in FEV1. After 12 months of treatment, 14% of patients had had an average of 1 exacerbation of asthma, compared with 52% of patients before baseline. The tolerability profile was favorable.
Conclusion: In this real-world study in patients with severe asthma and a history of EGPA asthma, mepolizumab and benralizumab had a significant steroid-sparing effect and reduced asthma exacerbation, but no significant effect on lung function.
Introduction
Eosinophilic granulomatosis with polyangiitis (EGPA) belongs to the spectrum of anti-neutrophil cytoplasmic antibody (ANCA)-associated vasculitides predominantly affecting small to medium vessels (1). It is characterised by an association with asthma, ear, nose and throat (ENT) involvement, blood and tissue eosinophilia and systemic vasculitis manifestations (2).
Asthma is almost always present in EGPA. It is often severe and usually precedes systemic manifestations by several years (3). The treatment of EGPA is based on systemic glucocorticoids, and immunosuppressive agents in severe cases (4, 5). However, a long-term treatment with low-dose glucocorticoids is often necessary to prevent asthma flares and relapses of vasculitis and leads to significant morbidity (3, 6–9). Reducing treatment-related morbidity is a priority of novel treatment approaches (10).
Mepolizumab, a humanized anti-interleukin-5 (IL-5) monoclonal antibody, reduces blood eosinophil counts and has demonstrated benefit at a dose of 100 mg subcutaneously every 4 weeks in patients with severe eosinophilic asthma (11, 12). In the phase 3, randomised controlled trial MIRRA, which enrolled patients with relapsing or refractory EGPA, a regimen of mepolizumab 300 mg every 4 weeks increased the duration of remission and resulted in a higher proportion of participants in remission than placebo did (13). Mepolizumab treatment was also associated with a greater proportion of patients with a daily dose of glucocorticoids of less than 4 mg per day during weeks 48 through 52, suggesting a steroid-sparing effect (13), consistent with observational data (14). Mepolizumab use was approved by the Food and Drug Administration (FDA) and by the European Medicine Agency (EMA) to treat relapsing or refractory EGPA.
Benralizumab is a monoclonal antibody targeting the IL-5 receptor-alpha. Using a regimen of 30 mg every 8 weeks after the first 3 injections every 4 weeks, benralizumab reduces blood eosinophil counts, and significantly reduces annual asthma exacerbation rates in patients with severe, uncontrolled asthma with blood eosinophils 300 cells/mm3 or greater (15, 16). A steroid-sparing effect of benralizumab was reported in small-size, retrospective cohorts (17) and prospective studies of patients with EGPA and severe asthma (18, 19). Comparable results were reported in a pilot study using reslizumab, another monoclonal antibody bindings to the alpha chain of the IL-5 receptor (20). However, few studies were conducted in patients with severe asthma and a history of EGPA.
In this retrospective study, we assessed the benefit of mepolizumab and benralizumab on the use of oral glucocorticoids, respiratory manifestations and lung function, and their tolerability by patients with asthma following EGPA, in real-life settings.
Patients and methods
Study design and patients
We conducted a retrospective monocentric study in a large tertiary care institution (Hospices Civils in Lyon). Cases enrolled in the study were admitted to one of the six departments of pulmonology or internal medicine of the institution between 1995 and July 2021, who were prescribed mepolizumab and/or benralizumab for severe persistent asthma, had a history of EGPA, and had been followed-up at least 12 months after the initiation of treatment. Patients who were prescribed mepolizumab or benralizumab were identified using the electronic patient files and the database of the hospital pharmacy (reslizumab was not available), and patient charts were reviewed manually. Patients had a clinical diagnosis of EGPA which satisfied either the inclusion criteria used in the MIRRA study (13) or the 1990 American College of Rheumatology (21) or the 2022 American College of Rheumatology / European Alliance of Associations for Rheumatology classification criteria (22), namely: (1) asthma; (2) peripheral blood eosinophilia >1,000/mm3 or 10% and (3) the presence of two or more criteria that are typical of EGPA. Patients who had granulomatosis with polyangiitis, microscopic polyangiitis, hypereosinophilic syndrome, or idiopathic chronic or acute eosinophilic pneumonia, eosinophilia related to parasite infections or malignant tumors, were excluded, as well as pregnant or breastfeeding women.
Procedures and data collection
Data was collected at the diagnosis of EGPA, at the initiation of mepolizumab or benralizumab, and at 6-month and 12-month follow-up visits. The treatment was left to the discretion of the attending physician including for tapering oral glucocorticoids. Data was collected during each visit by the caring physician using a standardised case-report form. Assessments included demographics, clinical manifestations, and biological data including blood and alveolar eosinophil counts, presence of ANCA. Lung function tests were performed following international guidelines and with standardised protocols. We assessed forced expiratory volume in 1 s (FEV1), forced vital capacity (FVC) and the FEV1/FVC ratio before bronchodilators and then 10 min after the inhalation of a short-acting beta-2 agonist. All values were expressed as percentage of predicted values, except for the FEV1/FVC ratio which was expressed as an absolute percentage and mean standard deviation. Reversibility was defined by an improvement of FEV1 with short-acting beta-2 agonist of 200 millilitres or more with 12% improvement or greater compared to the pre-bronchodilator FEV1.
Vasculitis activity was assessed using the Birmingham Vasculitis Activity Score (BVAS) from 2003 (0 → 63). Medications taken by the patient were extracted from electronic patients’ files and prescriptions, including daily prednisone dose and concomitant therapy. Severe asthma exacerbations were assessed per 6 month-periods, as well as any significant event including respiratory infections. Severe asthma exacerbations were defined as the worsening of respiratory symptoms (dyspnea, wheezing, cough) necessitating the initiation or increase of systemic glucocorticoids, visit to the emergency department, or non-elective hospitalisation. In order to monitor safety, adverse effects were assessed at every visit.
Outcome
The primary efficacy outcome was the proportion of patients who had a daily prednisone dose reduced to 4 mg or less at 12 months, and a BVAS score of 0, as per the MIRRA trial (13). Secondary efficacy outcomes were the proportion of patients who had a daily prednisone dose reduced to 4 mg or less at 6 months; the proportion of patients with a decrease of the median corticosteroid dose of 50% or more at 6 months and at 12 months; a significant decrease in the oral corticosteroid dose at 6 and 12 months; the percentage of patients weaned of oral glucocorticoids; a decrease in eosinophil blood count; and the improvement of lung function (FEV1 before bronchodilators, FEV1/FVC). We also evaluated the tolerability and safety of biologics over 12 months.
Statistical analysis
Descriptive results are expressed as median (interquartile) for quantitative variables and as number (percentage) for qualitative variables. Baseline measures were compared to those at 6 and 12 months after the initiation of mepolizumab or benralizumab, using chi-squared or the Fischer’s exact test for the qualitative variables. The Wilcoxon signed-rank test was applied to compare pre- and post-treatment lung function, and the Mann–Whitney U test was used to compare measures between groups. All tests were two sided, and statistical significance was set at p < 0.05 (two-tailed). IBM SPSS Statistics for Windows, Version 25.0 (IBM Corp., Armonk, NY) was used for statistical analyses. Graphs were created using GraphPad Prism.
Ethics
This study was conducted with respect to the Declaration of Helsinki. It was approved by the ethics committee of the Hospices Civils de Lyon and was registered with the national data protection agency (Commission Nationale de l’Informatique et des Libertés, number 21-5484). According to the legislation in place at the time of the study, informed consent signature was waived, but each patient was informed by a written letter and could object to the use of their personal data.
Results
Study population at EGPA diagnosis
A total of 26 patients were included (14 women and 12 men) with a median age of 49.5 years at EGPA diagnosis.
Clinical manifestations at the time of EGPA diagnosis are showed in Table 1. The median blood eosinophil count was 41% or 5,970 cells/mm3. Apart from asthma, the most frequent manifestations were sinonasal abnormalities (including chronic rhinitis, sinusitis, polyposis, and nasal obstruction) (76.9% of patients), myocarditis defined by elevated troponine levels with suggestive echocardiography or cardiac magnetic resonance imaging (38.5%), mononeuritis multiplex (30.8%), pericardial effusion at echocardiography (30.8%), fever (30.8%), weight loss (26.9%), and skin involvement (23.1%). Eosinophilic pneumonia with non-fixed pulmonary infiltrates and ground-glass attenuation was present in 84.6% of patients on computed-tomography (CT) scan. The median alveolar eosinophil count was 52%.
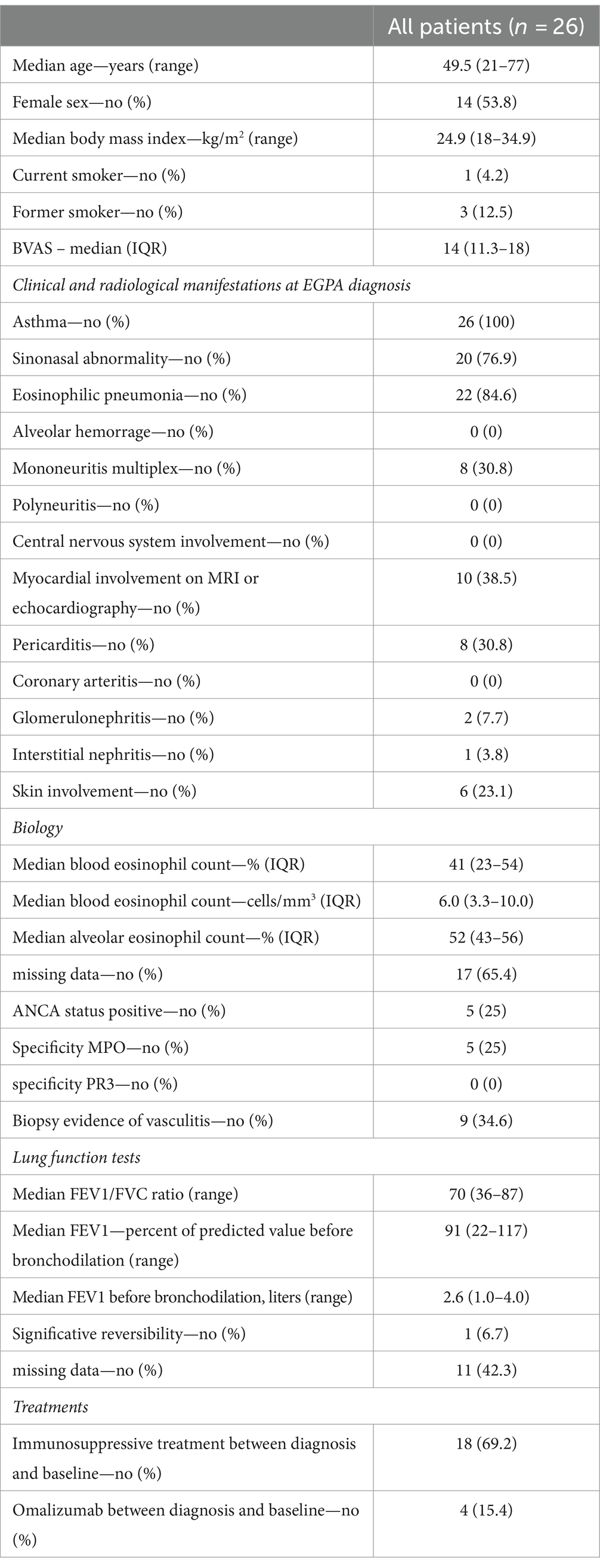
Table 1. Main characteristics at EGPA diagnosis.
All patients had persistent asthma despite daily oral glucocorticoids, inhaled corticosteroids, and long-acting bronchodilators. Thirteen patients had an obstructive ventilatory defect (FEV1/FVC ratio <0.70). The median FEV1/FVC ratio was 0.70. The median FEV1 was 2.59 L (91% of predicted value) before bronchodilation. The FEV1 was reversible in only one patient. Three patients were former smokers, one was a current smoker, and the others had never smoked.
Perinuclear ANCAs were found in 5 patients (19.2%), all with myeloperoxidase specificity. The vasculitis had been confirmed by biopsy in 34.6% of patients: skin (n = 3), pulmonary (n = 2), nasal cavity, muscle, gall bladder, renal (n = 1 each). Eighteen patients (69.2%) had received an immunosuppressive therapy (Supplementary Table S1).
Characteristics at initiation of IL5/IL5R therapy
At the time of initiation of anti-IL5/IL5R therapy (thereafter referred to as baseline), the median age was 58 years (range 22–78) 12 months. The median BVAS was 1 (range 0–2). All the patients had a symptomatology of severe asthma, and 52% had at least one severe asthma exacerbation per 6 months. Twelve patients (46%) had sinonasal abnormalities; 4 (17%) had migrating pulmonary infiltrates. None of the patients had neurological, cardiac, renal, skin, or gastrointestinal involvements at baseline. The median blood eosinophil count was 4.5% or 365 cells/mm3.
At baseline, 17 patients (68%) had airflow obstruction. The median FEV1/FVC ratio was 0.65, and the median FEV1 before bronchodilation was 85% of predicted. There was a significant reversibility of FEV1 in 5 patients (33%). All patients were receiving 4 mg or more of oral prednisone, with a median daily dosage of 10 mg (interquartile range 7.6–20 mg). All patients were also receiving long-acting bronchodilators and inhaled corticosteroids. Seven patients (27%) were still receiving immunosuppressive treatment (5 receiving azathioprine, and 2 rituximab).
Treatment
Mepolizumab/benralizumab treatment was introduced after a median duration of 5.5 years after the EGPA diagnosis. Fifteen patients were treated with subcutaneous injections of mepolizumab 100 mg every 4 weeks, 1 patient received mepolizumab 300 mg every 4 weeks, and 10 patients were treated with subcutaneous injections of benralizumab 30 mg administered at baseline, week 4, week 8, then every 8 weeks. Treatment with benralizumab was discontinued after 9 months in one patient who became pregnant.
Outcome
The median duration of follow-up was 12 months for efficacy and 721 days for safety. At 12 ± 3 months, 32% of patients (7/22) had reached the primary endpoint and had reduced the daily prednisone dosage to 4 mg or less (Figure 1) with a BVAS score of 0. For the second efficacy outcomes, 15% of patients (4/26) had reduced the daily prednisone dosage to 4 mg or less at 6 ± 3 months (Supplementary Figure S1). The median prednisone daily dosage significantly decreased from 10 mg at baseline to 9 mg at 6 ± 3 months (p = 0.0032) and further to 5 mg at 12 ± 3 months (p = 0.0052) (Table 2; Supplementary Table S2). At 12 months, 5 patients (23%) had discontinued oral glucocorticoid therapy. The daily dose of oral glucocorticoids was reduced by 50% or more in 31% of the patients at 6 months (n = 8) and in 55% at 12 months (n = 12), but was unchanged or increased in 6 patients (27%) at 12 months (Supplementary Table S3).
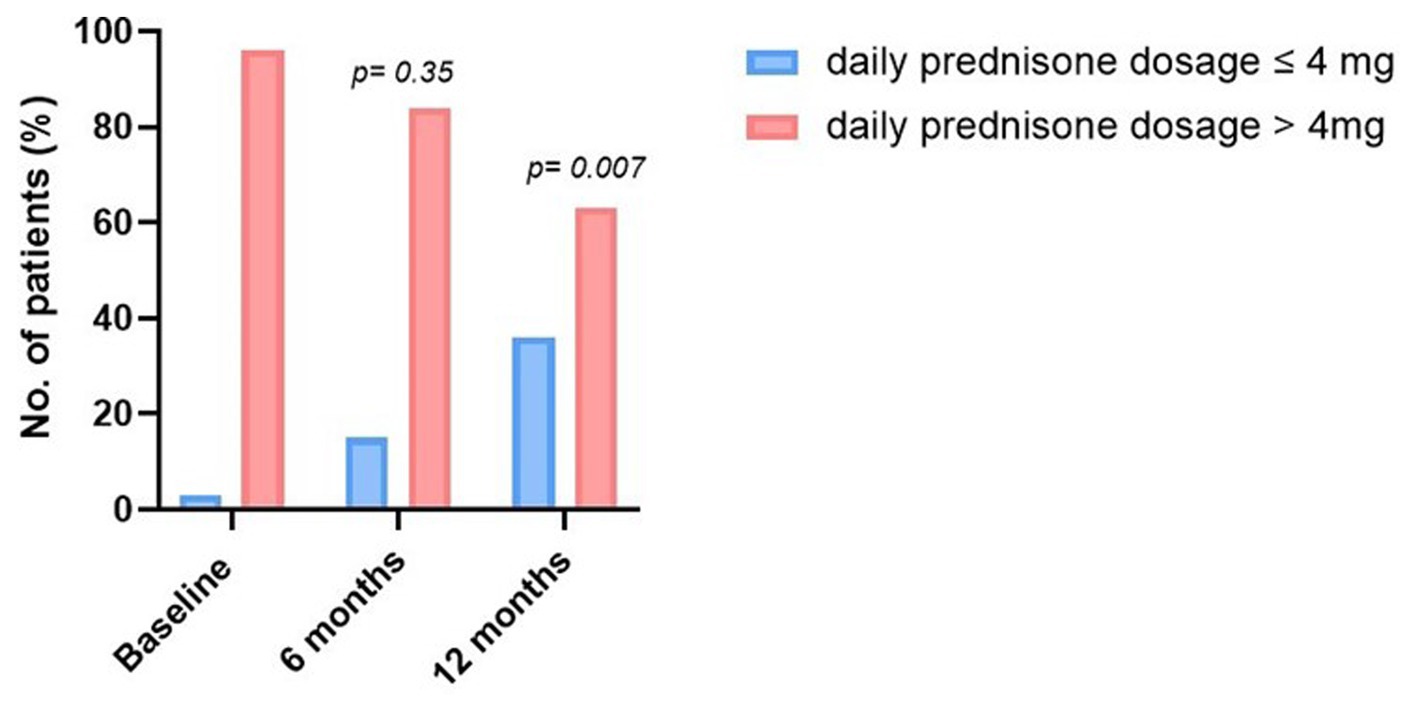
Figure 1. Evolution of the proportion of patients according to the daily dosage of oral glucocorticoids during the follow-up.
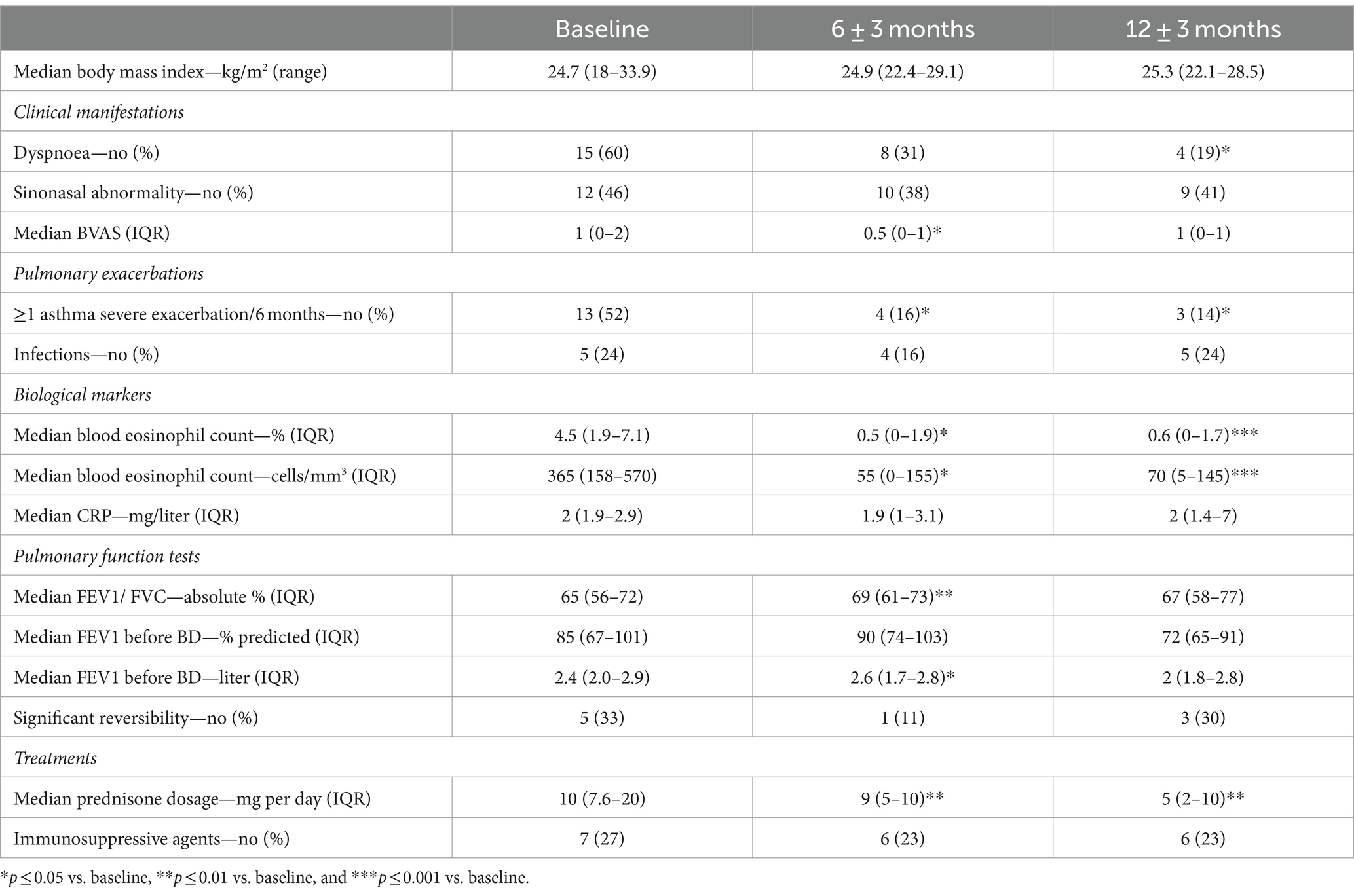
Table 2. Main outcome variables (n = 26).
The median blood eosinophil count significantly decreased during the follow-up, from 365 cells/mm3 at baseline to 55 cells/mm3 at 6 ± 3 months, and 70 cells/mm3 at 12 months (p = 0.00033) (Figure 2A). Asthma exacerbations were less frequent (14% versus 52%). No significant changes were observed in the rate of exertional dyspnea, sinonasal manifestations, FEV1, or use of immunosuppressive agents.
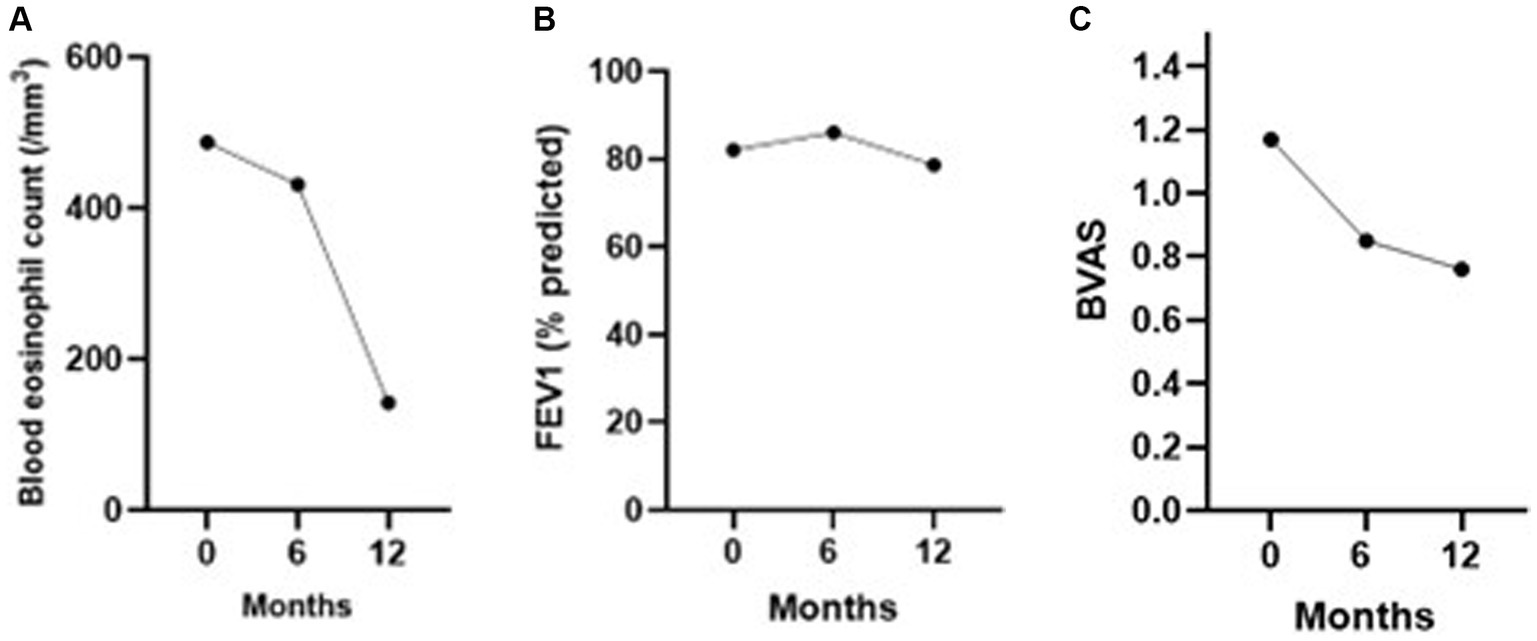
Figure 2. (A) Mean blood eosinophil count, (B) mean FEV1 (% predicted), and (C) mean BVAS during the 12 months of follow-up after anti-IL5/IL5(R) initiation.
Seven patients (26.9%) discontinued prematurely anti-IL-5/Rα therapy, after a mean of 16.6 months: mepolizumab 100 mg (n = 4), mepolizumab 300 mg (n = 1), benralizumab 30 mg (n = 2). The reasons were: a perceived lack of efficacy (n = 5), a vasculitis flare (n = 1 with polyarthritis), and acute eosinophilic pneumonia (n = 1). The lack of efficacy was defined as a worsening of asthma (n = 3) or sinusitis (n = 1), or persistent blood eosinophilia with no change in the need of oral glucocorticoids. Four patients with response considered insufficient to mepolizumab switched to benralizumab, and one switched from benralizumab to mepolizumab.
Comparison of the efficacy of anti-IL-5/Rα biologics was limited by the small sample size. At 12 months, 4/13 patients (30.8%) receiving mepolizumab and 4/9 patients (44.4%) on benralizumab had 4 mg or less of oral glucocorticoids per day, respectively (Supplementary Figure S2). The median prednisone dosage at 12 months was 5 mg for each group. The median blood eosinophil count was 80 cells/mm3 in mepolizumab group and 0 cells/mm3 in benralizumab group at 12 months.
Safety
The tolerability of anti-IL5/Rα biologics was unremarkable. No serious adverse event and no anaphylaxis were reported (Supplementary Table S4). The most frequent adverse effects were headache (15.4%) with mepolizumab (n = 3) or benralizumab (n = 1). While he was treated by mepolizumab and had been weaned off oral glucocorticoids, a patient developed an acute eosinophilic pneumonia, and was switched to benralizumab.
Discussion
In this real-life study of patients with severe eosinophilic asthma and a history of EGPA, we found that treatment with mepolizumab or benralizumab was associated with a reduction in the daily dose of oral glucocorticoids, asthma flares, and in blood eosinophil cell counts, without safety alerts. No significant change in lung function was observed at 12 months.
Optimising the management of EGPA is a real therapeutic challenge since long-term glucocorticoids lead to significant morbidity, even when using “low” doses (23), including osteoporosis, cardiovascular and metabolic manifestations (24, 25). At 12 months, 36% of the patients were receiving 4 mg of prednisone per day or less; 55% had reduced their daily dose of glucocorticoids by 50% or more, and 23% had discontinued oral glucocorticoids. The median prednisone daily dose decreased from 10 mg at baseline to 9 mg at 6 months and 5 mg at 12 months. Our findings support the results of clinical trials demonstrating a glucocorticoid-sparing effect of mepolizumab and benralizumab in the setting of EGPA (13) and of severe eosinophilic asthma (11, 16). Comparable results were reported in a prospective open-label pilot study of benralizumab in 10 patients with eosinophilic asthma and a history of EGPA (18), with a reduction of the median glucocorticoid daily dose from 15 mg to 2 mg. Preliminary results from the MANDARA trial demonstrated the non-inferiority of benralizumab 30 mg every 4 weeks compared with mepolizumab 300 mg every 4 weeks, and suggested a greater glucocorticoid-sparing effect with benralizumab,1 as suggested by our cohort. A steroid-sparing effect of mepolizumab or benralizumab was also suggested in several multicenter retrospective studies (14, 26–28). Two patients had persisting eosinophilia despite biologics, raising the question of compliance to treatment.
However, it should be noted that 27% of our patients had an increase or no change in the dose of prednisone. In the MIRRA trial, 47% of participants receiving mepolizumab did not achieve complete remission (13). Predictors of response to anti-IL5/Rα biologics have not been identified in EGPA. In addition, no significant improvement in FEV1 was observed. Consistently, in the study by Nair et al. (16) in severe asthma, no significant effect of benralizumab on FEV1 was found. It is to be noted that only 5 patients (33%) had a significant reversibility at baseline, consistent with previous findings from our center in EGPA (6).
The doses of anti-IL-5/Rα biologics used in our study were those used in severe eosinophilic asthma (16, 23), and only one patient received mepolizumab 300 mg, the approved and recommended regimen to treat relapsing or active, non-severe EGPA (4), or the hypereosinophilic syndrome (29). In a European observational study of 191 patients with EGPA, mepolizumab 100 mg and 300 mg had a comparable efficacy (14), however the two regimens have not been compared prospectively. Our findings suggest that mepolizumab 100 mg every 4 weeks could be an acceptable regimen in patients with asthma in the setting of EGPA (3, 14, 30–35). Consistently, a recent guideline stated that an initial dosage of mepolizumab 100 mg every 4 weeks can be used for remission maintenance in EGPA; this dosage can subsequently be titrated up to 300 mg every 4 weeks in patients with an unsatisfactory response to treatment (36).
Only 25% of our patients had ANCAs at diagnosis of EGPA, compared to 30%–40% in the literature (37, 38). This is consistent with our patients being predominantly referred to departments of respiratory medicine with an ANCA-negative, “eosinophilic-driven” phenotype of EGPA, and the use of anti-IL-5/Rα biologics in severe asthma. Conceivably, treatment strategies might be adapted to the EGPA phenotype (39). The potential role of mepolizumab as a first-line treatment of EGPA, and the benefit of benralizumab versus mepolizumab, are currently being evaluated (NCT05030155, NCT04157348).
While anti-IL-5 /Rα biologics were generally well tolerated, headache was the most frequently reported adverse event, consistent with previous findings (11).
The strength of this real-world study is to include a relatively large number of consecutive patients from a single institution. The limitations of the study are inherent to the retrospective design. However, patients were followed-up regularly, with a single electronic chart system, facilitating data extraction and review, and limiting the amount of missing data. Quality of life questionnaire or clinical assessment scores were not available, and the decrease in the dosage of glucocorticoids was not standardised. However, most patients were followed in a respiratory department, which explains the large number of pulmonary function tests available and the particular emphasis placed on asthma control and steroid-sparing.
In conclusion, this real-life observational study supports the efficacy of mepolizumab and benralizumab as steroid-sparing agents in patients with EGPA and severe asthma, with a favorable tolerability profile.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Ethics Committee of the Hospices Civils de Lyon, registered with the national data protection agency (Commission Nationale de l’Informatique et des Libertés, number 21-5484). The studies were conducted in accordance with the local legislation and institutional requirements. The ethics committee/institutional review board waived the requirement of written informed consent for participation from the participants or the participants’ legal guardians/next of kin because this was in line with the legislation in France on retrospective studies on existing data.
Author contributions
CD: Data curation, Formal analysis, Investigation, Writing – original draft. KA: Validation, Writing – review & editing. JT: Validation, Writing – review & editing. MG-V: Validation, Writing – review & editing. C-AD: Validation, Writing – review & editing. J-CG: Validation, Writing – review & editing. AH: Validation, Writing – review & editing. FL: Validation, Writing – review & editing. SM: Validation, Writing – review & editing. MN: Validation, Writing – review & editing. PS: Validation, Writing – review & editing. ST: Validation, Writing – review & editing. GD: Validation, Writing – review & editing. VC: Conceptualization, Methodology, Supervision, Validation, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
GD and VC received speaking fees from GSK and Astra Zeneca, not related with the present manuscript.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2024.1341310/full#supplementary-material
Footnotes
1. ^ https://www.astrazeneca.com/media-centre/press-releases/2023/fasenra-phase-iii-egpa-trial-met-primary-endpoint.html
References
1. Jennette, JC, Falk, RJ, Bacon, PA, Basu, N, Cid, MC, Ferrario, F, et al. 2012 revised International Chapel Hill Consensus Conference Nomenclature of Vasculitides. Arthritis Rheum. (2013) 65:1–11. doi: 10.1002/art.37715
2. Trivioli, G, Terrier, B, and Vaglio, A. Eosinophilic granulomatosis with polyangiitis: understanding the disease and its management. Rheumatology. (2020) 59:iii84–94. doi: 10.1093/rheumatology/kez570
3. Cottin, V, Bel, E, Bottero, P, Dalhoff, K, Humbert, M, Lazor, R, et al. Respiratory manifestations of eosinophilic granulomatosis with polyangiitis (Churg–Strauss). Eur Respir J. (2016) 48:1429–41. doi: 10.1183/13993003.00097-2016
4. Chung, SA, Langford, CA, Maz, M, Abril, A, Gorelik, M, Guyatt, G, et al. 2021 American College of Rheumatology/Vasculitis Foundation Guideline for the management of antineutrophil cytoplasmic antibody-associated vasculitis. Arthritis Rheumatol. (2021) 73:1366–83. doi: 10.1002/art.41773
5. Groh, M, Pagnoux, C, Baldini, C, Bel, E, Bottero, P, Cottin, V, et al. Eosinophilic granulomatosis with polyangiitis (Churg–Strauss) (EGPA) Consensus Task Force recommendations for evaluation and management. Eur J Intern Med. (2015) 26:545–53. doi: 10.1016/j.ejim.2015.04.022
6. Cottin, V, Khouatra, C, Dubost, R, Glerant, JC, and Cordier, JF. Persistent airflow obstruction in asthma of patients with Churg–Strauss syndrome and long-term follow-up. Allergy. (2009) 64:589–95. doi: 10.1111/j.1398-9995.2008.01854.x
7. Szczeklik, W, Sokolowska, BM, Zuk, J, Mastalerz, L, Szczeklik, A, and Musial, J. The course of asthma in Churg–Strauss syndrome. J Asthma. (2011) 48:183–7. doi: 10.3109/02770903.2010.551796
8. Berti, A, Cornec, D, Casal Moura, M, Smyth, RJ, Dagna, L, Specks, U, et al. Eosinophilic granulomatosis with polyangiitis: clinical predictors of long-term asthma severity. Chest. (2020) 157:1086–99. doi: 10.1016/j.chest.2019.11.045
9. Durel, CA, Berthiller, J, Caboni, S, Jayne, D, Ninet, J, and Hot, A. Long-term followup of a multicenter cohort of 101 patients with eosinophilic granulomatosis with polyangiitis (Churg–Strauss). Arthritis Care Res. (2016) 68:374–87. doi: 10.1002/acr.22686
10. Floyd, L, Morris, A, Joshi, M, and Dhaygude, A. Glucocorticoid therapy in ANCA Vasculitis: using the glucocorticoid toxicity index as an outcome measure. Kidney360. (2021) 2:1002–10. doi: 10.34067/KID.0000502021
11. Ortega, HG, Liu, MC, Pavord, ID, Brusselle, GG, FitzGerald, JM, Chetta, A, et al. Mepolizumab treatment in patients with severe eosinophilic asthma. N Engl J Med. (2014) 371:1198–207. doi: 10.1056/NEJMoa1403290
12. Bel, EH, Wenzel, SE, Thompson, PJ, Prazma, CM, Keene, ON, Yancey, SW, et al. Oral glucocorticoid-sparing effect of mepolizumab in eosinophilic asthma. N Engl J Med. (2014) 371:1189–97. doi: 10.1056/NEJMoa1403291
13. Wechsler, ME, Akuthota, P, Jayne, D, Khoury, P, Klion, A, Langford, CA, et al. Mepolizumab or placebo for eosinophilic granulomatosis with polyangiitis. N Engl J Med. (2017) 376:1921–32. doi: 10.1056/NEJMoa1702079
14. Bettiol, A, Urban, ML, Dagna, L, Cottin, V, Franceschini, F, Del Giacco, S, et al. Mepolizumab for eosinophilic granulomatosis with polyangiitis: a European multicenter observational study. Arthritis Rheumatol. (2022) 74:295–306. doi: 10.1002/art.41943
15. FitzGerald, JM, Bleecker, ER, Nair, P, Korn, S, Ohta, K, Lommatzsch, M, et al. Benralizumab, an anti-interleukin-5 receptor alpha monoclonal antibody, as add-on treatment for patients with severe, uncontrolled, eosinophilic asthma (CALIMA): a randomised, double-blind, placebo-controlled phase 3 trial. Lancet. (2016) 388:2128–41. doi: 10.1016/S0140-6736(16)31322-8
16. Nair, P, Wenzel, S, Rabe, KF, Bourdin, A, Lugogo, NL, Kuna, P, et al. Oral glucocorticoid-sparing effect of benralizumab in severe asthma. N Engl J Med. (2017) 376:2448–58. doi: 10.1056/NEJMoa1703501
17. Nanzer, AM, Dhariwal, J, Kavanagh, J, Hearn, A, Fernandes, M, Thomson, L, et al. Steroid-sparing effects of benralizumab in patients with eosinophilic granulomatosis with polyangiitis. ERJ Open Res. (2020):00451-2020. doi: 10.1183/23120541.00451-2020
18. Guntur, VP, Manka, LA, Denson, JL, Dunn, RM, Dollin, YT, Gill, M, et al. Benralizumab as a steroid-sparing treatment option in eosinophilic granulomatosis with polyangiitis. J Allergy Clin Immunol Pract. (2021) 9:1186–1193.e1. doi: 10.1016/j.jaip.2020.09.054
19. Padoan, R, Chieco Bianchi, F, Marchi, MR, Cazzador, D, Felicetti, M, Emanuelli, E, et al. Benralizumab as a glucocorticoid-sparing treatment option for severe asthma in eosinophilic granulomatosis with polyangiitis. J Allergy Clin Immunol Pract. (2020) 8:3225–3227.e2. doi: 10.1016/j.jaip.2020.05.033
20. Manka, LA, Guntur, VP, Denson, JL, Dunn, RM, Dollin, YT, Strand, MJ, et al. Efficacy and safety of reslizumab in the treatment of eosinophilic granulomatosis with polyangiitis. Ann Allergy Asthma Immunol. (2021) 126:696–701.e1. doi: 10.1016/j.anai.2021.01.035
21. Masi, AT, Hunder, GG, Lie, JT, Michel, BA, Bloch, DA, Arend, WP, et al. The American College of Rheumatology 1990 criteria for the classification of Churg–Strauss syndrome (allergic granulomatosis and angiitis). Arthritis Rheum. (1990) 33:1094–100. doi: 10.1002/art.1780330806
22. Grayson, PC, Ponte, C, Suppiah, R, Robson, JC, Craven, A, Judge, A, et al. 2022 American College of Rheumatology/European Alliance of Associations for rheumatology classification criteria for eosinophilic granulomatosis with polyangiitis. Ann Rheum Dis. (2022) 81:309–14. doi: 10.1136/annrheumdis-2021-221794
23. Volmer, T, Effenberger, T, Trautner, C, and Buhl, R. Consequences of long-term oral corticosteroid therapy and its side-effects in severe asthma in adults: a focused review of the impact data in the literature. Eur Respir J. (2018) 52:1800703. doi: 10.1183/13993003.00703-2018
24. Rice, JB, White, AG, Scarpati, LM, Wan, G, and Nelson, WW. Long-term systemic corticosteroid exposure: a systematic literature review. Clin Ther. (2017) 39:2216–29. doi: 10.1016/j.clinthera.2017.09.011
25. Daugherty, J, Lin, X, Baxter, R, Suruki, R, and Bradford, E. The impact of long-term systemic glucocorticoid use in severe asthma: a UK retrospective cohort analysis. J Asthma. (2018) 55:651–8. doi: 10.1080/02770903.2017.1353612
26. Canzian, A, Venhoff, N, Urban, ML, Sartorelli, S, Ruppert, AM, Groh, M, et al. Use of biologics to treat relapsing and/or refractory eosinophilic granulomatosis with polyangiitis: data from a European collaborative study. Arthritis Rheumatol. (2021) 73:498–503. doi: 10.1002/art.41534
27. Nolasco, S, Portacci, A, Campisi, R, Buonamico, E, Pelaia, C, Benfante, A, et al. Effectiveness and safety of anti-IL-5/Rα biologics in eosinophilic granulomatosis with polyangiitis: a two-year multicenter observational study. Front Immunol. (2023) 14:1204444. doi: 10.3389/fimmu.2023.1204444
28. Cottu, A, Groh, M, Desaintjean, C, Marchand-Adam, S, Guillevin, L, Puechal, X, et al. Benralizumab for eosinophilic granulomatosis with polyangiitis. Ann Rheum Dis. (2023) 82:1580–6. doi: 10.1136/ard-2023-224624
29. Roufosse, F, Kahn, JE, Rothenberg, ME, Wardlaw, AJ, Klion, AD, Kirby, SY, et al. Efficacy and safety of mepolizumab in hypereosinophilic syndrome: a phase III, randomized, placebo-controlled trial. J Allergy Clin Immunol. (2020) 146:1397–405. doi: 10.1016/j.jaci.2020.08.037
30. Vergles, M, Matković, Z, Lalić, K, Trkanjec, JT, and Tudorić, N. Mepolizumab as a glucocorticoid-sparing agent in eosinophilic granulomatosis with polyangiitis (EGPA): is a lower dose sufficient? J Asthma. (2021) 58:1675–9. doi: 10.1080/02770903.2020.1827417
31. Vultaggio, A, Nencini, F, Bormioli, S, Vivarelli, E, Dies, L, Rossi, O, et al. Low-dose mepolizumab effectiveness in patients suffering from eosinophilic granulomatosis with polyangiitis. Allergy Asthma Immunol Res. (2020) 12:885–93. doi: 10.4168/aair.2020.12.5.885
32. Detoraki, A, Tremante, E, Poto, R, Morelli, E, Quaremba, G, Granata, F, et al. Real-life evidence of low-dose mepolizumab efficacy in EGPA: a case series. Respir Res. (2021) 22:185. doi: 10.1186/s12931-021-01775-z
33. Caminati, M, Crisafulli, E, Lunardi, C, Micheletto, C, Festi, G, Maule, M, et al. Mepolizumab 100 mg in severe asthmatic patients with EGPA in remission phase. J Allergy Clin Immunol Pract. (2021) 9:1386–8. doi: 10.1016/j.jaip.2020.09.025
34. Özdel Öztürk, B, Yavuz, Z, Aydın, Ö, Mungan, D, Sin, BA, Demirel, YS, et al. Effectiveness of low-dose mepolizumab in the treatment of eosinophilic granulomatosis with polyangiitis (EGPA): a real-life experience. Int Arch Allergy Immunol. (2022) 183:1281–90. doi: 10.1159/000526410
35. Portacci, A, Campisi, R, Buonamico, E, Nolasco, S, Pelaia, C, Crimi, N, et al. Real-world characteristics of “super-responders” to mepolizumab and benralizumab in severe eosinophilic asthma and eosinophilic granulomatosis with polyangiitis. ERJ Open Res. (2023) 9:00419-2023. doi: 10.1183/23120541.00419-2023
36. Emmi, G, Bettiol, A, Gelain, E, Bajema, IM, Berti, A, Burns, S, et al. Evidence-based guideline for the diagnosis and management of eosinophilic granulomatosis with polyangiitis. Nat Rev Rheumatol. (2023) 19:378–93. doi: 10.1038/s41584-023-00958-w
37. Sinico, RA, Di Toma, L, Maggiore, U, Bottero, P, Radice, A, Tosoni, C, et al. Prevalence and clinical significance of antineutrophil cytoplasmic antibodies in Churg–Strauss syndrome. Arthritis Rheum. (2005) 52:2926–35. doi: 10.1002/art.21250
38. Comarmond, C, Pagnoux, C, Khellaf, M, Cordier, JF, Hamidou, M, Viallard, JF, et al. Eosinophilic granulomatosis with polyangiitis (Churg–Strauss): clinical characteristics and long-term followup of the 383 patients enrolled in the French Vasculitis Study Group cohort. Arthritis Rheum. (2013) 65:270–81. doi: 10.1002/art.37721
39. Cottin, V, Bel, E, Bottero, P, Dalhoff, K, Humbert, M, Lazor, R, et al. Revisiting the systemic vasculitis in eosinophilic granulomatosis with polyangiitis (Churg–Strauss): a study of 157 patients by the Groupe d’Etudes et de Recherche Sur les maladies Orphelines Pulmonaires and the European Respiratory Society taskforce on eosinophilic granulomatosis with polyangiitis (Churg–Strauss). Autoimmun Rev. (2017) 16:1–9. doi: 10.1016/j.autrev.2016.09.018
Keywords: Interleukin-5, vasculitis, eosinophil, asthma, corticosteroids, granulomatosis
Citation: Desaintjean C, Ahmad K, Traclet J, Gerfaud-Valentin M, Durel C-A, Glerant J-C, Hot A, Lestelle F, Mainbourg S, Nasser M, Seve P, Turquier S, Devouassoux G and Cottin V (2024) Mepolizumab and benralizumab in patients with severe asthma and a history of eosinophilic granulomatosis with polyangiitis. Front. Med. 11:1341310. doi: 10.3389/fmed.2024.1341310
Edited by:
Hsiao-Chi Chuang, Taipei Medical University, TaiwanReviewed by:
Corrado Pelaia, University of Magna Graecia, ItalyRoberto Padoan, University of Padua, Italy
Copyright © 2024 Desaintjean, Ahmad, Traclet, Gerfaud-Valentin, Durel, Glerant, Hot, Lestelle, Mainbourg, Nasser, Seve, Turquier, Devouassoux and Cottin. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Vincent Cottin, dmluY2VudC5jb3R0aW5AY2h1LWx5b24uZnI=
†ORCID: Mathieu Gerfaud-Valentin, orcid.org/0000-0003-4245-8039
Cecile-Audrey Durel, orcid.org/0000-0003-2878-5017
Sabine Mainbourg, orcid.org/0000-0003-4564-2931
Mouhamad Nasser, orcid.org/0000-0001-8373-8032
Ségolène Turquier, orcid.org/0000-0001-5894-4491
Gilles Devouassoux, orcid.org/0000-0002-1335-6562
Vincent Cottin, orcid.org/0000-0002-5591-0955