 Jie Chen
Jie Chen Tao Bai
Tao Bai Jinsong Liu
Jinsong Liu Lishou Xiong2
Lishou Xiong2 Huahong Wang
Huahong Wang Xiaohua Hou
Xiaohua Hou
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Med. , 10 April 2024
Sec. Healthcare Professions Education
Volume 11 - 2024 | https://doi.org/10.3389/fmed.2024.1338206
Aims: This cohort study aimed to explore the effect of a one-day online continuing medical education (CME) on the improvement of physicians’ knowledge and clinical practice on functional dyspepsia (FD).
Methods: Physicians were invited to participate in this CME via medical education applications. FD training videos made in advance were sent to participants via a weblink. Before and after training, participants were required to finish the FD knowledge test and provide case information of FD patients. McNemar test, Wilcoxon rank-sum test, Freidman test, Chi-square test, quantile regression, and generalized estimating equations (GEE) were used to perform statistical analysis.
Results: There were 397 of 430 (92.33%) physicians finished this CME program. The total score of the FD knowledge test after training was significantly higher compared with before training [488.3 (468.3–510.0) vs. 391.7 (341.7–450.0), p < 0.001]. Particularly, physicians from primary hospitals show more increase in total scores than physicians from secondary and tertiary hospitals. According to the GEE model, receiving this online training was an independent predictor of physicians’ choice of upper gastrointestinal endoscopy in patients with FD [OR 1.73, 95%CI (1.09–2.73), p = 0.020], especially in PDS. Also, it was an independent predictor of physicians’ choice of acid-suppressive drugs in patients with FD [OR 1.30, 95%CI (1.03–1.63), p = 0.026], especially in EPS and PDS overlapping EPS.
Conclusion: This one-day online CME program effectively and conveniently improved physicians’ knowledge and clinical practice, providing new ideas for future CME and facilitating precise clinical management of FD patients with different subtypes especially in primary hospitals.
Functional dyspepsia (FD) is one of the most common gastrointestinal complaints with a worldwide prevalence of 5 to 40% (1, 2). Moreover, the diagnosis of FD accounts for around 20% of all outpatients in the gastrointestinal medical clinics (3).
It is thought that insufficient understanding of symptoms, uncertain diagnosis, inappropriate examination, and treatment selection, together contribute to unsatisfied patient management (4, 5). As a result, patients would visit the outpatient clinic repeatedly, which brought a heavy burden on health care services (6, 7). Therefore, it is of vital importance to improve physicians’ knowledge and clinical practice in FD patients.
At present, the most accepted diagnostic criteria for FD are the Rome criteria. With the development of research and the accumulation of knowledge, Rome criteria have been updated for many times in the past 20 years (8, 9). Finally, Rome IV (10) was formed in 2016, which had been developed into a knowledge system including definition, diagnostic criteria, treatment options, etc. Previous study found that most patients were not able to understand the related symptoms of dyspepsia accurately. Especially for early satiety and postprandial satiety, two easily confused symptoms, the proportions of patients who could precisely understand the connotation of these two concepts were 37.7 and 52.27%, respectively (11). Misunderstanding of the symptom would inevitably affect the treatment plan and efficacy of FD patients. Therefore, how to transfer the latest knowledge opportunely, effectively, and conveniently to clinicians for the first-line practice is of great significance.
Continuing medical education (CME) is thought to be an essential part and effective method for health care professionals (12–17). However, it is difficult for physicians to take part in continuing education due to their busy clinical work. Differed from the traditional on-the-spot mode, the convenience of smartphones and the Internet brings the CME more choices. As for online training, physicians can complete the training project whenever it is convenient. Besides, for the training of single disease knowledge, it is very practicable to promote a short-term but effective training program.
Therefore, we conducted this cohort study to explore the effect of a one-day online CME about FD on the improvement of physicians’ knowledge and clinical practice.
This online CME was open for access from March to August 2019. Physicians in different levels of hospital, with different positional titles, were invited to participate in this CME program via professional medical education application (APP), including Medhorizon1 and DXY.2 Professional certificated clinicians who have more than 15 daily outpatient visits, were included in this study. This study was performed in accordance with the Declaration of Helsinki. Informed consent was obtained online from participants before they can be included in this study.
FD training videos made in advance were designed by experts of functional gastrointestinal diseases collaborative group of Chinese medical association, based on Rome IV Functional Gastrointestinal Disorders – Disorders of Gut-Brain Interaction (Fourth Edition). These training videos included three parts: interpretation of symptoms of FD, interpretation of Rome IV diagnostic criteria for FD, and standardized treatment and of FD, to provide participants with a comprehensive understanding of the latest management recommendations of FD. Each video contained 30 min approximately. Those training videos were sent to all participants through the weblink, and the entire course can be finished in a single day. Participants can watch training videos over and over again if they want to learn some knowledge points repeatedly.
The 25-question FD knowledge test was used to evaluate the level of knowledge of physicians, which was designed based on Rome IV (The specific questions of the test can be found in Supplementary Table S1). It contains six aspects, including FD symptoms, diagnostic criteria for FD, diagnostic criteria for Postprandial Distress Syndrome (PDS), diagnostic criteria for Epigastric Pain Syndrome (EPS), examination choices for FD, and treatment choices for FD. Each aspect of the knowledge test has a score of 100 and the total score is 600. The test was a closed-book exam and was sent to participants through a weblink before they started the training and after they finished watching all training videos. Participants were required to finish the FD knowledge test twice at least, before and after training, respectively. In these two tests, the same questions were reorganized with different sequences. They can choose to answer the knowledge test again every time after view the training videos. And the scores of each time would be recorded. For each participant, the score of the FD knowledge test before training, the score at first answer after training and the highest score among all answering times were compared and analyzed to evaluate the improvement of physicians’ knowledge.
Meanwhile, we required participants to submit case information, such as examinations and prescriptions, of FD patients who visited their outpatient’s clinic and treated by them before and after training. The change of physicians’ clinical practice was evaluated through the comparison and analysis of management that physician gave for different FD patients before and after training.
Participants who completed all the online training and finished the FD knowledge test before and after training were included in the final analysis. Missing data would be excluded from the final analysis. The main contrast was performed between before training and after training. Statistical differences in the categorical variable for paired and unpaired designs were tested by the McNemar test and the Chi-square test, respectively. Continuous variables without normal distribution were displayed as median (interquartile range), and paired Wilcoxon rank-sum test or Freidman test (with Bonferroni correction) were conducted to detect statistical significance. Quantile regressions at the 5th, 25th, 50th, 75th, and 95th percentiles of the increase in total score were performed to eliminate the effect of confounders. As the examination and treatment options for FD were more influenced by the subjective perception of the individual physician, cases submitted by one physician were seen as a cluster, which was analyzed using generalized estimating equations (GEE) to explore possible interfering factors. All statistical analyses were performed by R 4.0.3.3 A p-value less than 0.05 was considered statistically significant. And this study was reported using the STROBE cohort reporting guidelines (18).
Four hundred and thirty physicians signed up for the program. Before training, 414 participants (96.28%) completed the FD knowledge test. Then, 402 participants (93.49%) completed all online video training. Finally, a total of 397 participants (92.33%) completed the FD knowledge test again after the training and finished this CME program. Among them, 180 (45.34%) participants were gastroenterologists, and 217 (54.66%) were general practitioners. The numbers of participants with junior, intermediate, and senior positional titles were 60 (15.11%), 178 (44.84%), and 159 (40.05%), respectively. There were 124 (31.23%) participants from primary hospitals, 114 (28.72%) from secondary hospitals, and 159 (40.05%) from tertiary hospitals. After training, 47.61% (189/397) of participants took the FD knowledge test only once, and 52.39% (208/397) of participants took the FD knowledge test several times.
A total of 7032 cases information of the FD patients diagnosed and treated by participants before and after training were collected from those who finished this CME program. There were 814 (11.58%) cases collected before training and 6218 (88.42%) after training. Cases diagnosed with PDS by participants took a proportion of 52.01% (3657), whereas the proportions of cases diagnosed with EPS and PDS overlapping EPS were 29.49% (2074) and 18.50% (1301), respectively. Among these cases, there were 2517 (35.79%) cases including examination information and 5402 (76.82%) cases including prescription and drug information.
Before training, the total scores on the FD knowledge test among participants were 391.7 (341.7–450.0), which means the understanding rate of FD knowledge was about 65% (391.7/600). The highest scores after training were 488.3 (468.3–510.0), which means the understanding rate of FD knowledge was raised to 81% (488.3/600). Compared with before training, total scores at the first answer after training were significantly improved [450.0 (406.6–484.9), p < 0.001]. And the highest score on the FD knowledge test after training was also significantly higher than that of the first answer after training (p < 0.001) (Figure 1A). As for the spending time on the knowledge test, there was no statistical difference (p = 0.985, p = 0.266) (Figure 1B).
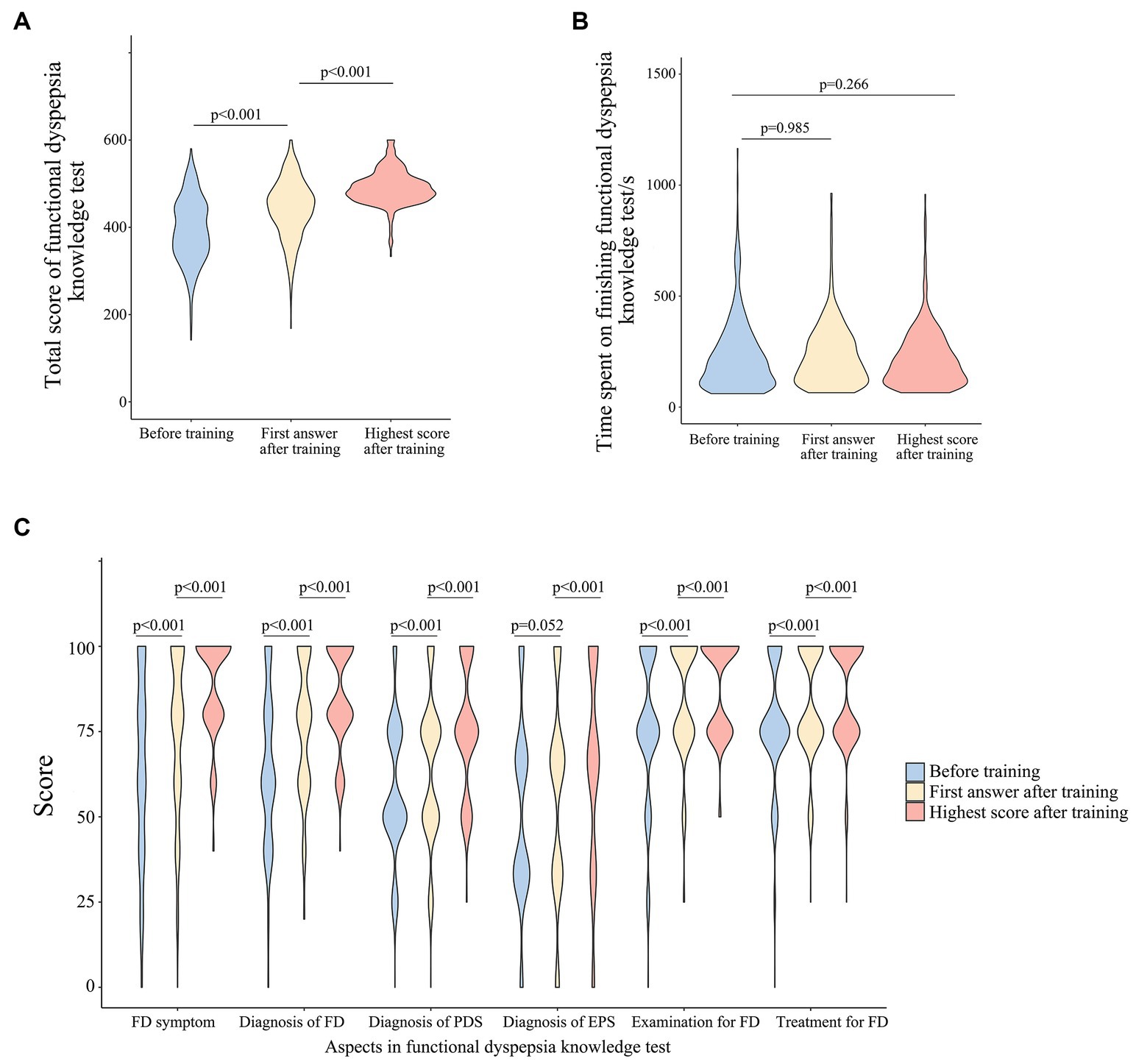
Figure 1. (A) Total scores of FD knowledge test before and after training; (B) time spent on FD knowledge test before and after training; (C) scores of six aspects in FD knowledge test before and after training.
In contrast to before training, the scores after training were higher with statistical significance in all six aspects of the knowledge test (p < 0.001) (Figure 1C). Scores of FD symptom understanding, diagnosis of FD, diagnosis of PDS, selection of examination, and selection of treatment were improved at the first answer after training, compared with before training (p < 0.001). And the highest scores after training on the above five aspects were also higher than that of the first answer after training (p < 0.001). As for the diagnosis of EPS, there was no statistical difference between scores before training and at the first answer after training (p = 0.052), but the highest score after training was improved significantly compared with the first answer after training (p < 0.001). Correct rates for each question of the knowledge test before training and at the highest score after training were shown in Supplementary Table S1. For most of the questions in the FD knowledge test, correct rates after training were higher than that of before training with statistical significance.
Gastroenterologists scored higher than general practitioners before training, but there was almost no difference in their scores after training. And similarly, physicians in the tertiary hospital scored higher before training than those who were in primary hospital. But their scores after training were almost the same (Table 1). Compared with before training, the highest scores of physicians after training increased significantly (p < 0.001), regardless of their major, positional titles, and levels of hospital (Table 1). To test the influence factors of the improvement in FD knowledge test, quantile regressions were performed according to physicians’ characteristics (Figure 2). There were no statistical differences between gastroenterologists and general practitioners, as well as among physicians with junior, intermediate, and senior titles. However, compared with physicians in primary hospitals, physicians from tertiary hospitals showed less increase in the total score at the 5th (p = 0.002), 75th (p = 0.004), and 95th (p = 0.002) percentiles, and physicians from secondary hospitals showed less increase in the total score at the 75th (p = 0.005), and 95th (p < 0.001) percentiles. Physicians who answered the FD knowledge test twice or more times after training displayed more increase in total score than those who answered the FD knowledge test only once at the 5th (p < 0.001), 25th (p < 0.001), 50th (p < 0.001), 75 (p = 0.007), and 95 (p = 0.002) percentiles.
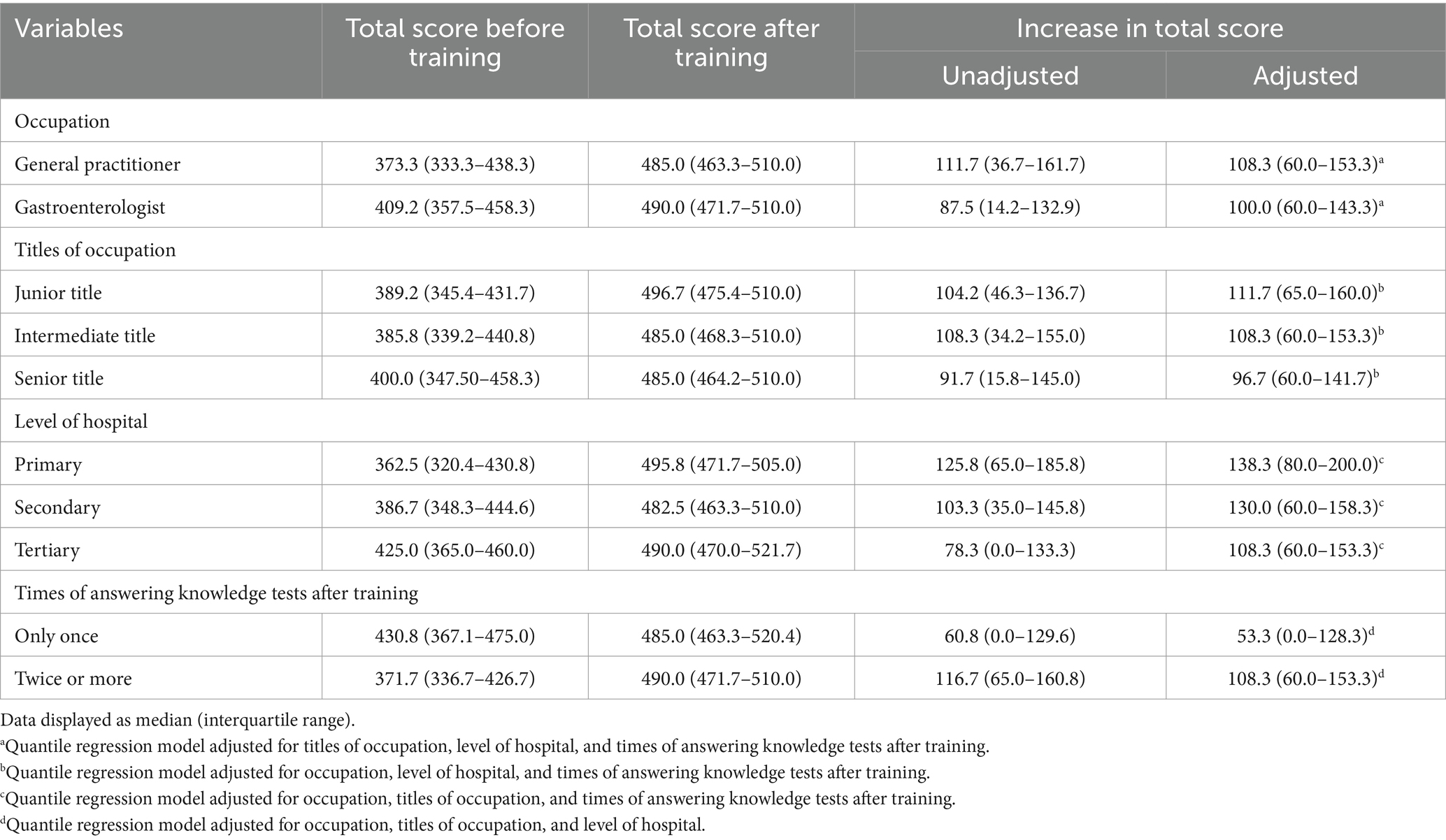
Table 1. Total score increases among different groups of physicians.
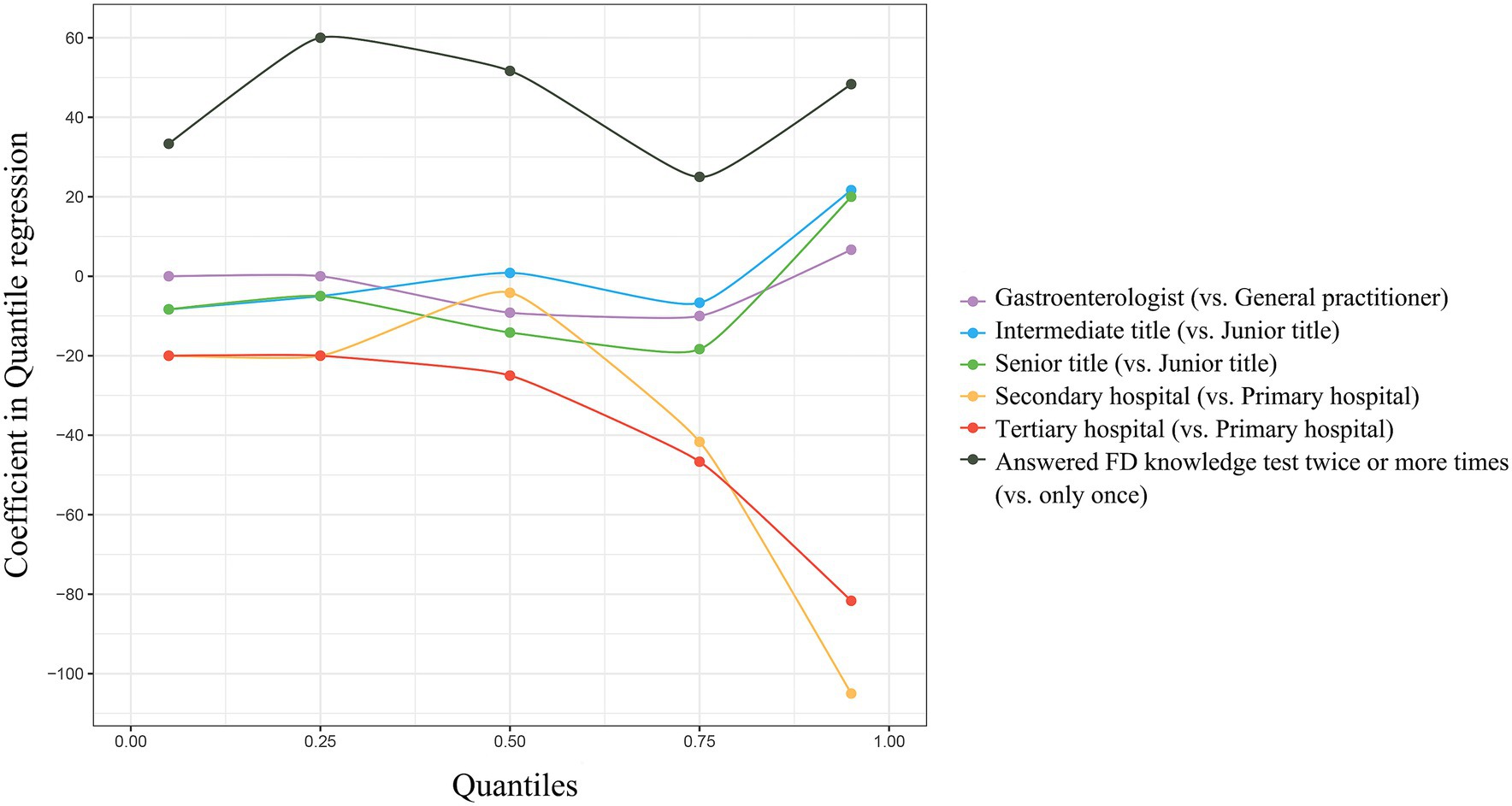
Figure 2. Quantile regressions on different percentiles of the increase in total scores of FD knowledge test.
After training, physicians’ selection rate of upper gastrointestinal endoscopy was significantly higher than before training in FD [62.99% (1384/2197) vs. 46.56% (149/320), p < 0.001], PDS [64.08% (769/1200) vs. 47.62% (70/147), p < 0.001], and EPS [60.59% (369/609) vs. 39.78% (37/93), p < 0.001] patients (Figure 3A). In patients diagnosed with PDS overlapping EPS, physicians’ selection rate of endoscopy improved after training without statistical significance [63.40% (246/388) vs. 52.50% (42/80), p = 0.089]. According to GEE estimating model (Figure 3B), receiving this online training was an independent predictor of physicians’ choice of upper gastrointestinal endoscopy in patients with FD [OR 1.73, 95%CI (1.09–2.73), p = 0.020], especially in patients with a subtype of PDS [OR 1.82, 95%CI (1.06–3.14), p = 0.031] (Supplementary Table S2).
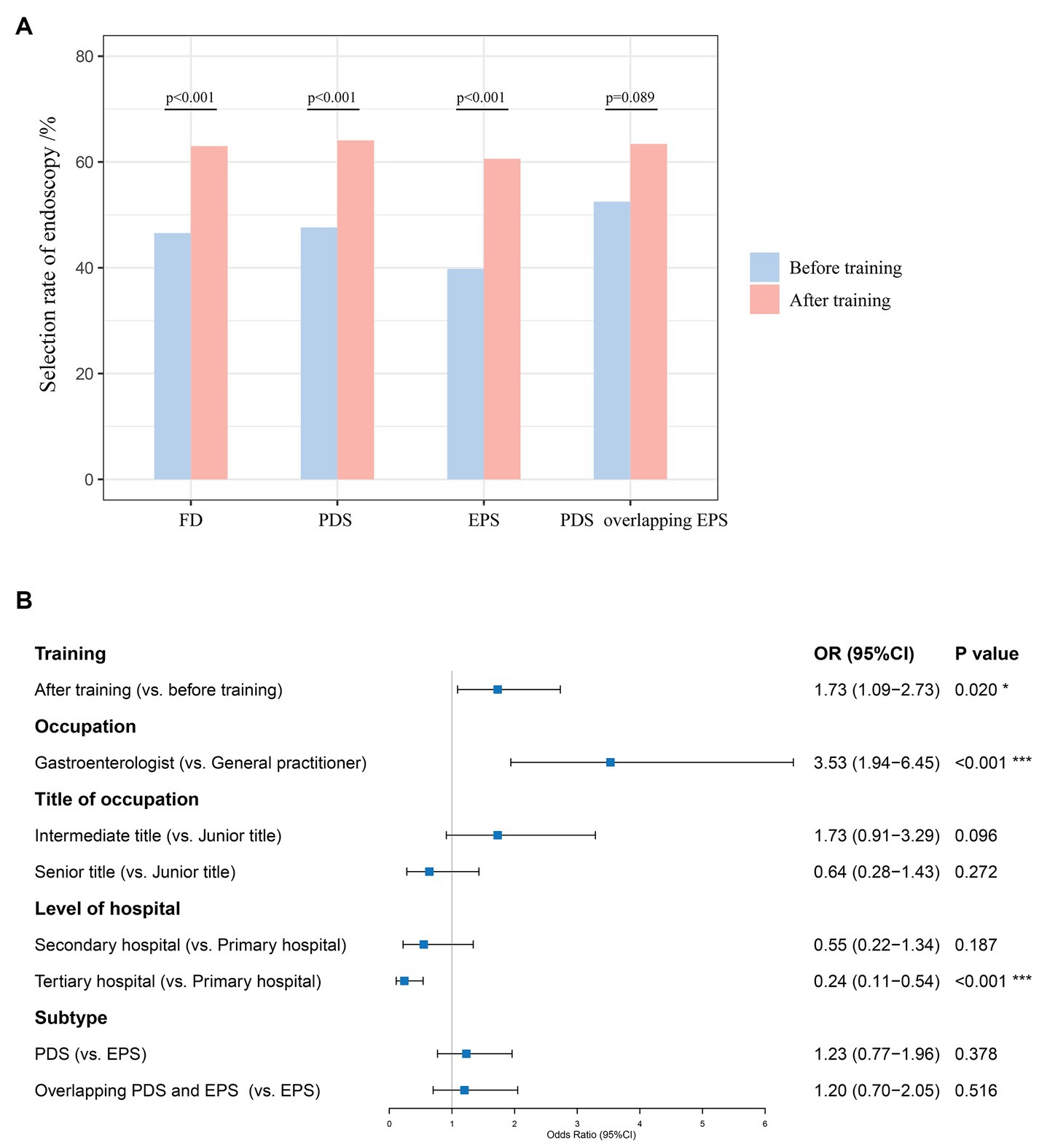
Figure 3. (A) Physicians’ selection rate of upper gastrointestinal endoscopy before and after training; (B) GEE estimating model for independent predictors of physicians’ choice of upper gastrointestinal endoscopy in patients with FD.
In general, physicians’ selection rate of prokinetic drugs among FD patients was at a high level after and before training [91.51% (4411/4820) vs. 90.72% (528/582), p = 0.571] (Figure 4A). After training, physicians’ selection rate of prokinetic drugs was slightly improved in PDS patients [96.86% (2464/2544) vs. 93.91% (262/279), p = 0.017]. Physicians’ selection rate of prokinetic drugs decreased after training without statistical differences in patients diagnosed with EPS [86.18% (1247/1447) vs. 90.21% (129/143), p = 0.223] and PDS overlapping EPS [84.44% (700/829) vs. 85.63% (137/160), p = 0.794]. According to GEE estimating model (Figure 4B), receiving this online training barely changed physicians’ choice of prokinetic drugs in patients with FD [OR 1.00, 95%CI (0.71–1.41), p = 0.989], regardless of subtypes (Supplementary Table S3) [OR 1.47, 95%CI (0.91–2.37), p = 0.114 for PDS patients; OR 0.66, 95%CI (0.35–1.27), p = 0.211 for EPS patients; OR 1.10, 95%CI (0.53–2.27), p = 0.797 for patients diagnosed with PDS overlapping EPS].
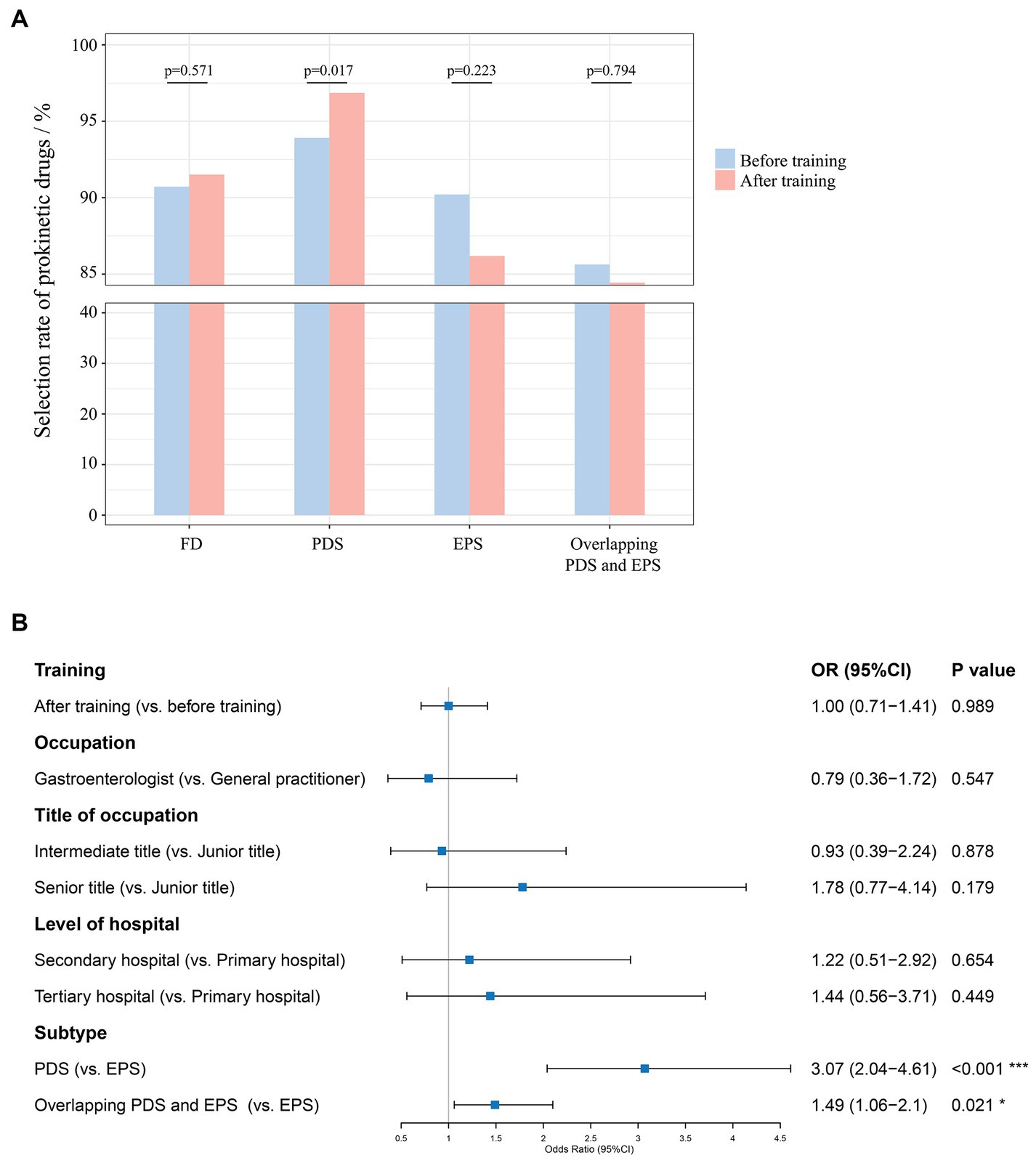
Figure 4. (A) Physicians’ selection rate of prokinetic drugs before and after training; (B) GEE estimating model for independent predictors of physicians’ choice of prokinetic drugs in patients with FD.
Overall, there was no significant difference in physicians’ selection rate of acid-suppressive drugs after training and before training among all FD patients [29.88% (1440/4820) vs. 25.95% (151/582), p = 0.055] (Figure 5A). Physicians’ selection rate of acid-suppressive drugs significantly improved after training in patients diagnosed with EPS [42.85% (620/1447) vs. 27.27% (39/143), p < 0.001] and PDS overlapping EPS [51.99% (431/829) vs. 34.38% (55/160), p < 0.001], whereas it decreased in PDS patients [15.29% (389/2544) vs. 20.43% (57/279), p = 0.032]. According to GEE estimating model (Figure 5B), receiving this online training was an independent predictor of physicians’ choice of acid-suppressive drugs in patients with FD [OR 1.30, 95%CI (1.03–1.63), p = 0.026], especially in patients with a subtype of EPS [OR 1.76, 95%CI (1.18–2.63), p = 0.006] and PDS overlapping EPS [OR 1.80, 95%CI (1.26–2.56), p = 0.001] (Supplementary Table S4).
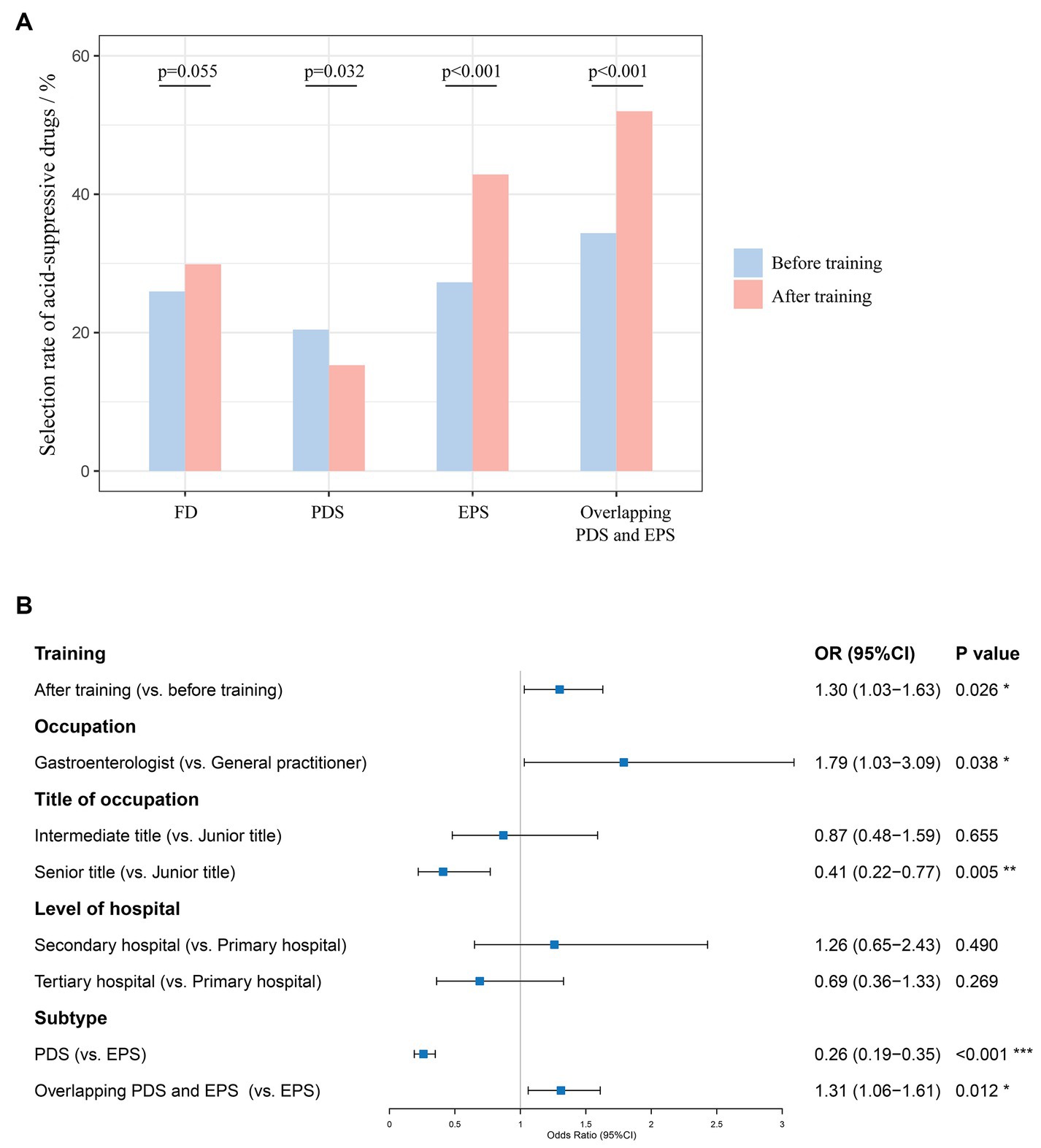
Figure 5. (A) Physicians’ selection rate of acid-suppressive drugs before and after training; (B) GEE estimating model for independent predictors of physicians’ choice of acid-suppressive drugs in patients with FD.
This one-day online CME program was successfully practiced, with significant improvement in physicians’ knowledge of FD. Physicians in primary hospitals had a greater improvement in FD knowledge than physicians in secondary and tertiary hospitals. Physicians’ inappropriate clinical practice during diagnosing and treating FD patients were partially corrected after training. There were satisfying increases in the selection rate of upper gastrointestinal endoscopy in FD patients and the selection rate of acid-suppressive drugs in patients diagnosed with EPS and PDS overlapping EPS.
With the development of medical science, physicians’ knowledge acquired during undergraduate and pre-employment training has already been outdated (12, 19). It is known that physicians need to update their clinical knowledge and maintain a lifelong learning attitude (12, 13, 19). Under this circumstance, CME is an important and effective way for all physicians to learn the latest medical knowledge. Despite several reported practices of online CME (20, 21), to our knowledge, there is no report on the application of one-day, online CME in FD. This opportune CME program of FD significantly improved doctors’ knowledge and clinical practice, which brings inspiration to continuing education on functional dyspepsia and further on other gut-brain disorders.
Furthermore, the system of medical education varies in different countries and regions. Even in the same country, there were substantially diverse education systems. Medical students in China graduated with degree programs ranging from 3 to 8 years (22–24), which caused great variability in physicians’ clinical capabilities, and in turn, led to differences in patient outcomes (17, 25, 26). This study showed the online CME program of FD can effectively improve physicians’ knowledge and clinical practice, regardless of their major, positional titles, and levels of hospital. These results indicate a promising prospect in the field of continuing medical education.
Besides, physicians in primary hospitals have less access to traditional lecture-based CME due to the busy clinical work and remote geographical location (19). As a result, updating of knowledge was limited under this situation (26, 27). With the application and popularization of the internet and smartphone, social media has become a more and more popular platform for spreading knowledge, which also facilitates more and more people, including doctors (20, 21). In China, a vast country, medical exchanges between different regions were not an easy task. If there was no way to online CME, doctors in primary hospitals need to schedule specific times and travel long distances to access the latest and systematic diagnostic and treatment guidelines. Considering that offline lectures would greatly reduce the participation rate of doctors in primary hospital, we ultimately adopted online CME in this study. In addition, online learning supports participants to repeatedly watch training videos, learn multiple times, and consolidate their knowledge. According to our study, this one-day online CME benefited doctors in primary hospitals more than doctors in secondary and tertiary hospitals with great significance. After training, the knowledge level of physicians in primary hospitals was almost the same as that of physicians in secondary or tertiary hospitals. This phenomenon proves the value and significance of online CME program in homogenization of doctors. The CME pattern developed in this study provides a convenient approach for physicians in primary hospitals to acquire up-to-date clinical knowledge.
Previous study showed that online CME was as effective as traditional onsite course in the improvement of professionals’ clinical skills (21). Other study displayed a similar knowledge gain of participants between online plus face-to-face learning group and only face-to-face learning group (28). In a survey of physiotherapists’ satisfaction towards online CME, most participants believed that online CME promoted their knowledge level and more than half of the participant agreed that online CME was more flexible and satisfactory compared to conventional face-to-face CMEs (29). Practice had proven that online learning had changed the traditional pattern of CME and was becoming increasingly popular among medical professionals.
There were also some limitations in this study. Firstly, the study population is generated by convenient sampling, which may cause selection bias. Secondly, testing bias was also likely to occur, although it is widely accepted to use the same questions with different sequences before and after training (30–32). Another point to note is that this study only investigated the effect of CME on physicians’ short-term behaviors. More evidence is needed to see whether this online CME could improve physicians’ long-term clinical performance.
In summary, this one-day online CME program could opportunely, effectively, and conveniently transform the latest knowledge into first-line clinical practice, leading to the improvement of physicians’ knowledge and clinical practice. This successful practice demonstrated the effectiveness of the online CME program, providing new ideas for future CPD and facilitating precise clinical management of FD patients with different subtypes especially in primary hospitals. Further exploration and optimization are needed for the content and methods of online teaching, such as the impact of teaching methods (participatory teaching, clinical case-based teaching, … etc.) on teaching effectiveness. We will continue to promote specialized online CMEs for functional gastrointestinal diseases, carefully selecting appropriate teaching content to enhance the understanding of gastrointestinal symptoms and patient management by primary care doctors.
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
Ethical approval was not required for the studies involving humans because this study was performed in accordance with the Declaration of Helsinki and approval of the Ethics Committee was not required for a CME program since there was no risk for participants and any private information of doctors or patients would not be collected. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
JC: Writing – review & editing, Writing – original draft, Visualization, Software, Investigation, Formal analysis. TB: Writing – review & editing, Supervision, Resources, Methodology, Investigation, Data curation. JL: Writing – review & editing, Resources, Methodology, Investigation, Conceptualization. LX: Writing – review & editing, Resources, Investigation. WW: Writing – review & editing, Resources, Investigation. HW: Writing – review & editing, Resources, Investigation. RW: Writing – review & editing, Resources, Investigation. XH: Writing – review & editing, Validation, Supervision, Project administration, Methodology, Funding acquisition, Conceptualization.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This study was supported by Beijing Medical Award Foundation.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2024.1338206/full#supplementary-material
CME, Continuing medical education; EPS, Epigastric pain syndrome; FD, Functional dyspepsia; GEE, Generalized estimating equations; PDS, Postprandial distress syndrome.
1. Enck, P, Azpiroz, F, Boeckxstaens, G, Elsenbruch, S, Feinle-Bisset, C, Holtmann, G, et al. Functional dyspepsia. Nat Rev Dis Primers. (2017) 3:17081. doi: 10.1038/nrdp.2017.81
2. Mahadeva, S, and Ford, AC. Clinical and epidemiological differences in functional dyspepsia between the east and the west. Neurogastroenterol Motil. (2016) 28:167–74. doi: 10.1111/nmo.12657
3. Wang, A, Liao, X, Xiong, L, Peng, S, Xiao, Y, Liu, S, et al. The clinical overlap between functional dyspepsia and irritable bowel syndrome based on Rome III criteria. BMC Gastroenterol. (2008) 8:43. doi: 10.1186/1471-230X-8-43
4. Fang, X, Francisconi, CF, Fukudo, S, Gerson, MJ, Kang, JY, Schmulson, WMJ, et al. Multicultural aspects in functional gastrointestinal disorders (FGIDs). Gastroenterology. (2016) 150:1344–1354.e2. doi: 10.1053/j.gastro.2016.02.013
5. Camilleri, M, and Stanghellini, V. Current management strategies and emerging treatments for functional dyspepsia. Nat Rev Gastroenterol Hepatol. (2013) 10:187–94. doi: 10.1038/nrgastro.2013.11
6. Lacy, BE, Weiser, KT, Kennedy, AT, Crowell, MD, and Talley, NJ. Functional dyspepsia: the economic impact to patients. Aliment Pharmacol Ther. (2013) 38:170–7. doi: 10.1111/apt.12355
7. Moayyedi, P, Lacy, BE, Andrews, CN, Enns, RA, Howden, CW, and Vakil, N. ACG and CAG clinical guideline: Management of Dyspepsia. Am J Gastroenterol. (2017) 112:988–1013. doi: 10.1038/ajg.2017.154
8. Talley, NJ, Stanghellini, V, Heading, RC, Koch, KL, Malagelada, JR, and Tytgat, GN. Functional gastroduodenal disorders. Gut. (1999) 45:II37–42. doi: 10.1136/gut.45.2008.ii37
9. Tack, J, Talley, NJ, Camilleri, M, Holtmann, G, Hu, P, Malagelada, JR, et al. Functional gastroduodenal disorders. Gastroenterology. (2006) 130:1466–79. doi: 10.1053/j.gastro.2005.11.059
10. Stanghellini, V, Chan, FK, Hasler, WL, Malagelada, JR, Suzuki, H, Tack, J, et al. Gastroduodenal Disorders. Gastroenterology. (2016) 150:1380–92. doi: 10.1053/j.gastro.2016.02.011
11. Lin, R, Wang, W, and Hou, X. The self-evaluation of upper-gastrointestinal symptoms in Chinese patients with digestive disease: a multicenter questionnaire survey. J Gastroenterol Hepatol. (2016) 31:87–92. doi: 10.1111/jgh.13064
12. McMahon, GT. Advancing continuing medical education. JAMA. (2015) 314:561–2. doi: 10.1001/jama.2015.7094
13. Kearney, P, Simoons, M, Ryden, L, Kirchhof, P, Pries, A, O'Morain, C, et al. The medical profession, industry, and continuing medical education: finding the balance That's right for patients. Am J Med. (2019) 132:921–5. doi: 10.1016/j.amjmed.2019.02.026
14. Davis, D, O'Brien, MA, Freemantle, N, Wolf, FM, Mazmanian, P, and Taylor-Vaisey, A. Impact of formal continuing medical education: do conferences, workshops, rounds, and other traditional continuing education activities change physician behavior or health care outcomes? JAMA. (1999) 282:867–74. doi: 10.1001/jama.282.9.867
15. Davis, D, and Galbraith, R. American College of Chest Physicians Health and Science Policy Committee. Continuing medical education effect on practice performance: effectiveness of continuing medical education: American college of chest physicians evidence-based educational guidelines. Chest. (2009) 135:42S–8S. doi: 10.1378/chest.08-2517
16. Brennan, N, and Mattick, K. A systematic review of educational interventions to change behaviour of prescribers in hospital settings, with a particular emphasis on new prescribers. Br J Clin Pharmacol. (2013) 75:359–72. doi: 10.1111/j.1365-2125.2012.04397.x
17. Cervero, RM, and Gaines, JK. The impact of CME on physician performance and patient health outcomes: an updated synthesis of systematic reviews. J Contin Educ Heal Prof. (2015) 35:131–8. doi: 10.1002/chp.21290
18. Von Elm, E, Altman, DG, Egger, M, Pocock, SJ, Gøtzsche, PC, Vandenbroucke, JP, et al. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. Epidemiology. (2007) 18:800–4. doi: 10.1097/EDE.0b013e3181577654
19. Nissen, SE. Reforming the continuing medical education system. JAMA. (2015) 313:1813–4. doi: 10.1001/jama.2015.4138
20. Thamman, R, Gulati, M, Narang, A, Utengen, A, Mamas, MA, and Bhatt, DL. Twitter-based learning for continuing medical education? Eur Heart J. (2020) 41:4376–9. doi: 10.1093/eurheartj/ehaa346
21. Llambí, L, Esteves, E, Martinez, E, Forster, T, García, S, Miranda, N, et al. Teaching tobacco cessation skills to Uruguayan physicians using information and communication technologies. J Contin Educ Heal Prof. (2011) 31:43–8. doi: 10.1002/chp.20100
22. Hou, J, Michaud, C, Li, Z, Dong, Z, Sun, B, Zhang, J, et al. Transformation of the education of health professionals in China: progress and challenges. Lancet. (2014) 384:819–27. doi: 10.1016/S0140-6736(14)61307-6
23. Anand, S, Fan, VY, Zhang, J, Zhang, L, Ke, Y, Dong, Z, et al. China's human resources for health: quantity, quality, and distribution. Lancet. (2008) 372:1774–81. doi: 10.1016/S0140-6736(08)61363-X
24. Hsieh, CR, and Tang, C. The multi-tiered medical education system and its influence on the health care market-China's Flexner report. Hum Resour Health. (2019) 17:50. doi: 10.1186/s12960-019-0382-4
25. Currie, J, and MacLeod, WB. Diagnosing expertise: human capital, decision making, and performance among physicians. J Labor Econ. (2017) 35:18977. doi: 10.3386/w18977
26. Sylvia, S, Shi, Y, Xue, H, Tian, X, Wang, H, Liu, Q, et al. Survey using incognito standardized patients shows poor quality care in China's rural clinics. Health Policy Plan. (2015) 30:322–33. doi: 10.1093/heapol/czu014
27. Wang, C, Rao, K, Wu, S, and Liu, Q. Health care in China: improvement, challenges, and reform. Chest. (2013) 143:524–31. doi: 10.1378/chest.12-1839
28. Uzzaman, MN, Jackson, T, Uddin, A, Rowa-Dewar, N, Chisti, MJ, Habib, GMM, et al. Continuing professional education for general practitioners on chronic obstructive pulmonary disease: feasibility of a blended learning approach in Bangladesh. BMC Fam Pract. (2020) 21:203. doi: 10.1186/s12875-020-01270-2
29. Shalabi, KM, and Almurdi, MM. Satisfaction and attitudes towards online continuous medical education and its impact on clinical practice among physiotherapists. BMC Med Educ. (2024) 24:70. doi: 10.1186/s12909-024-05049-2
30. Sears, KE, Cohen, JE, and Drope, J. Comprehensive evaluation of an online tobacco control continuing education course in Canada. J Contin Educ Heal Prof. (2008) 28:235–40. doi: 10.1002/chp.190
31. Canchihuaman, FA, Garcia, PJ, Gloyd, SS, and Holmes, KK. An interactive internet-based continuing education course on sexually transmitted diseases for physicians and midwives in Peru. PLoS One. (2011) 6:e19318. doi: 10.1371/journal.pone.0019318
Keywords: continuing medical education, functional dyspepsia, knowledge level, clinical practice, primary hospital
Citation: Chen J, Bai T, Liu J, Xiong L, Wang W, Wang H, Wang R and Hou X (2024) Significant improvement of physicians’ knowledge and clinical practice: an opportune, effective, and convenient continuing medical education program on functional dyspepsia. Front. Med. 11:1338206. doi: 10.3389/fmed.2024.1338206
Edited by:
Sumant Inamdar, University of Arkansas System, United StatesReviewed by:
Jiande Chen, University of Michigan, United StatesCopyright © 2024 Chen, Bai, Liu, Xiong, Wang, Wang, Wang and Hou. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xiaohua Hou, aG91eGhAaHVzdC5lZHUuY24=
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.