
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Med., 24 July 2024
Sec. Pulmonary Medicine
Volume 11 - 2024 | https://doi.org/10.3389/fmed.2024.1337609
 Christian Rønn1*
Christian Rønn1* Andreas Dehlbæk Knudsen2
Andreas Dehlbæk Knudsen2 Nicoline Stender Arentoft2Rebekka Faber Thudium2Safura-Luise Heidari2
Nicoline Stender Arentoft2Rebekka Faber Thudium2Safura-Luise Heidari2 Pradeesh Sivapalan1,3Charlotte S. Ulrik3,4
Pradeesh Sivapalan1,3Charlotte S. Ulrik3,4 Thomas Benfield3,5
Thomas Benfield3,5 Sisse Rye Ostrowski3,6Jens Ulrik Stæhr Jensen1,3
Sisse Rye Ostrowski3,6Jens Ulrik Stæhr Jensen1,3 Susanne D. Nielsen2,3*
Susanne D. Nielsen2,3*Objectives: Endothelial injury may promote declining lung function. We aimed to investigate in well-treated persons living with HIV (PLWH) whether elevated levels of thrombomodulin (TM) and syndecan-1 (SDC1) are associated with excess lung function decline and worsening dyspnea.
Methods: A prospective cohort study comprising patients from the Copenhagen municipality. We included 698 PLWH with undetectable viral load. Biomarkers and demographics were measured at baseline, spirometry [forced expiratory volume in one second (FEV1) and forced vital capacity (FVC)] and dyspnea score both at baseline and 2-year follow-up.
Both biomarkers were dichotomized at the 3rd quartile. Decline in lung function was estimated using a linear mixed model with patient-specific random effect. Increase in dyspnea score was estimated using a general mixed logistic regression model.
Results: We did not find an association between elevated SDC1 or TM and an excess decline in neither FEV1: SDC1: 4.5 mL/year (95% CI: −3.9–12.9, p = 0.30), TM: 2.2 mL/year (95% CI: −6.0–10.4, p = 0.60) nor FVC: SDC1: 4.1 mL/year (95% CI: −6.0–14.2, p = 0.42), TM: 1.4 mL/year (95% CI: −8.3–11.1, p = 0.78). A subgroup analysis of never-smokers was consistent with the main analysis.
Likewise, we did not find any association between elevated SDC1 and TM and increase in dyspnea score: SDC1: OR 1.43 (95% CI: 0.89–2.30, p = 0.14), TM: OR 1.05 (95% CI: 0.65–1.71, p = 0.26).
Conclusion: We did not find a significant association between elevated biomarkers of endothelial injury and decline in lung function nor dyspnea.
Persons living with HIV (PLWH), even when well-treated and without detectable viral replication, experience an increased rate of decline in lung function, as measured by forced expiratory volume in one second (FEV1) and forced vital capacity (FVC), compared to controls without HIV (1, 2). As a corollary, chronic obstructive pulmonary disease (COPD) is more prevalent in PLWH (3) and, low FEV1 in PLWH is associated with impaired quality of life and an increased risk of hospitalization (4). Likewise, low FEV1 in COPD is strongly associated with level of dyspnea, overall symptom burden, risk of hospitalization, and mortality (5–8).
Endothelial dysfunction is highly prevalent in all severities of COPD (9, 10), and it is well established that the pulmonary vascular endothelium is involved in chronic lung disease (11). Furthermore, it is proposed that endothelial dysfunction is not only a consequence of damaged alveolar surfaces, but rather a driving factor behind the decline in lung function and a potential target for treatment (12, 13). Additionally, PLWH exhibits increased prevalence of risk factors for endothelial dysfunction such as smoking, dyslipidemia, and abdominal obesity. Also, HIV infection has been proposed as an independent risk factor possibly through HIV associated immune activity or by direct effect on endothelial cells (14). Recent studies have found, that PLWH have elevated plasma levels of both SDC1 and TM (15, 16).
As the endothelial surface layer is being produced and shed continuously, the most used method to investigate changes in the endothelial surface layer is by measuring shed components (17, 18). Both the membrane bound expression and shedding of surface layer components may be regulated, often in response to inflammation or under conditions of cellular stress (19–21).
Syndecans are transmembrane proteins heavily involved in cellular signaling, with syndecan-1 (SDC1) exclusively found on endothelial cells (17). Elevated levels of soluble SDC1 have been associated with increased endothelial damage and worsened outcomes in COVID-19 (22), heart failure (23), pulmonary embolism (24), and renal disease (25) among others.
Thrombomodulin (TM) is a transmembrane protein involved in the antithrombogenic pathway through its binding of thrombin and activation of Protein C (26). Soluble TM has been associated with coronary heart disease and atherosclerosis (27), endothelial damage in renal disease (27), and acute respiratory distress syndrome (28).
We hypothesize that endothelial dysfunction and injury promotes excess decline in lung function in PLWH, and thus, associates with the presence of elevated shed SDC1 and TM is. Moreover, we hypothesize that elevated SDC1 and TM are associated with increased dyspnea as expressed by the medical research council (MRC) dyspnea score.
This was a prospective cohort study comprising patients from the Copenhagen Comorbidity in HIV infection (COCOMO) study (29). For the current study a subgroup of the COCOMO study cohort were selected based on the following inclusion criteria:
• Spirometry measured at baseline and two-year follow up.
• Age ≥ 25 years at baseline.
• HIV RNA viral load <100 copies/mL at baseline and follow up.
• CD4+ count >300 cells/μL at baseline and follow up.
• Initiated antiretroviral therapy ≥6 month prior to baseline visit.
Patients were followed from baseline to first follow-up after approximately 2 years. Written informed consent was signed by all patients and the COCOMO study is approved by ethics committee (approval number H-8-2014-004, ClinicalTrials.gov: NCT02382822).
Spirometry was performed to measure pre-bronchodilator values for FEV1 and FVC. Spirometry was performed two times during the study: Once at baseline and once at 2 year follow-up using a handheld EasyOne spirometer (ndd Medical, Zürich, Switzerland). Patients were instructed by staff trained in spirometry. All spirometry results were validated, as described earlier (30).
Dyspnea was assessed using the MRC score at baseline and follow-up, with questions slightly altered (Supplementary Appendix 1).
As earlier described by Ronit et al. plasma concentrations of soluble SDC1 and TM were analyzed on thawed plasma using Luminex® Human Discovery Assays (R&D Systems, United Kingdom, Europe) in a 1:2 dilution, according to the manufacturer’s instructions, at the Department of Clinical Immunology, Copenhagen University Hospital, Rigshospitalet, Copenhagen, Denmark, as described earlier (29). Both biomarkers were dichotomized at the 3rd quartile in line with earlier studies (31).
Descriptive statistics were performed on baseline data. Comparison was performed with a χ2 test for categorical data. For continuous data, the normally distributed data were compared with a t test, while non-normally distributed data were compared with Mann–Whitney Wilcoxon test.
Change in FEV1 and FVC between baseline and follow-up were expressed as mL/year to account for slight variations in follow up time. A linear mixed model was used to compare the rate of lung function decline. An adjusted model included age (continuous), sex (M/F), BMI (underweight/normal/overweight/obese), smoking status (current/former/never), and ethnicity (African/Caucasian/Hispanic/Asian/other) as fixed effects. To account for the correlation in the repeated measurements as well as possible variance over time, we included random effects (patient-specific intercept). The endothelial injury markers were added one at a time.
Risk of rapid decliner phenotype, defined by decrease in FEV1 ≥ 40 mL/year, according to baseline endothelial injury marker was evaluated using a general mixed logistic regression model, where the dependent variable was FEV1 ≥ 40 mL/year (1/0), adjusting for age (continuous), sex (M/F), BMI (underweight/normal/overweight/obese), smoking status (current/former/never), and ethnicity (African/Caucasian/Hispanic/Asian/other). The endothelial injury markers were added one at a time.
Risk of increase in dyspnea score between baseline and follow-up was evaluated using a general mixed logistic regression model, where the dependent variable was increase in MRC dyspnea score (1/0), adjusting for FEV1 (continuous), time (continuous), age (continuous), sex (M/F), BMI (underweight/normal/overweight/obese), smoking status (current/former/never), and ethnicity (African/Caucasian/Hispanic/Asian/other). The endothelial injury markers were added one at a time.
All analyses were first done with a crude model adjusting only for age (continuous) and sex (M/F), before applying the full adjusted model as described above.
The primary endpoint of decline in FEV1 was further investigated in the following sensitivity analyses: (1) stratifying for smoking status (current/former/never), (2) only using patients with airflow limitation defined by FEV1 < 80% of predicted and FEV1/FVC ratio < 0.70 at baseline, (3) including all patients with validated spirometry performed at both baseline and follow-up regardless of HIV RNA and CD4 count.
Results are presented as change in mL/year with a 95% confidence interval (CI) for change in FEV1 and FVC and as odds ratio (OR) with a 95% CI for risk of rapid decliner phenotype and increase in dyspnea score. p values <0.05 are considered significant. All statistical analyses were completed in R 4.3.0 (R Foundation for Statistical Computing, Vienna, Austria).
A total of 1,099 patients were included in the COCOMO study. Of these, 926 patients had validated spirometry measured at both baseline and follow-up. Patients with missing markers of endothelial damage (n = 40), age < 25 years (n = 6), HIV RNA viral load >100 copies/mL at baseline and/or follow-up (n = 65), immunosuppressed with CD4 count <300 cell/μL at baseline and/or follow-up (n = 99), and been in antiretroviral therapy <6 months (n = 18) were excluded, resulting in a study population of 698 patients (see Figure 1), of whom 67 had airflow limitation.
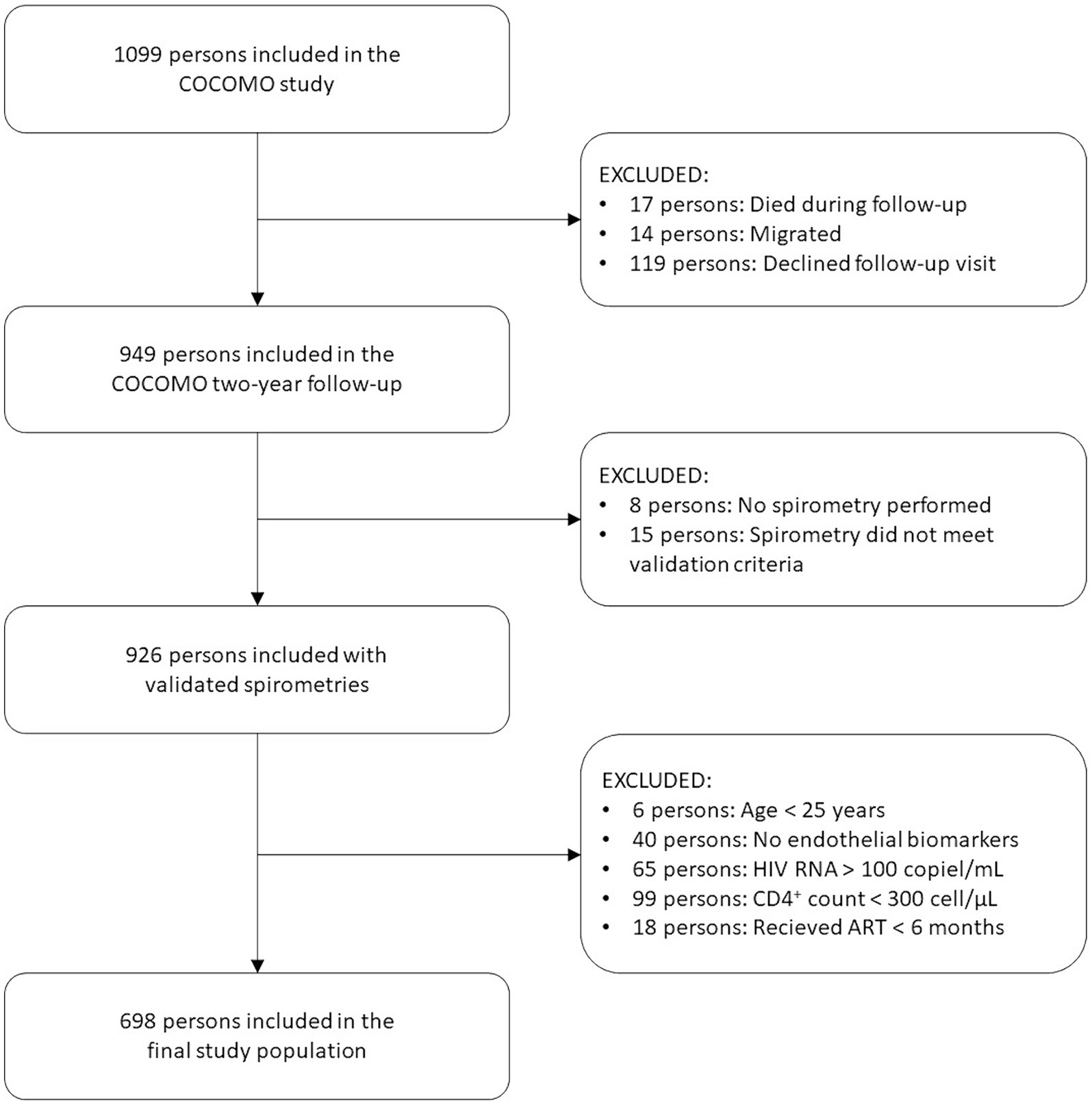
Figure 1. Study flow chart. ART: antiretroviral therapy.
Generally, the upper quartile group of both SDC1 and TM were in most aspects similar to the overall study population, however slightly older: Mean age upper quartile TM: 52.4 years, upper quartile SDC1: 51.5 years, overall study population: 50.3 years (for full baseline characteristics see Table 1, for graphical distribution of SDC1 and TM levels see Supplementary Appendix 2).
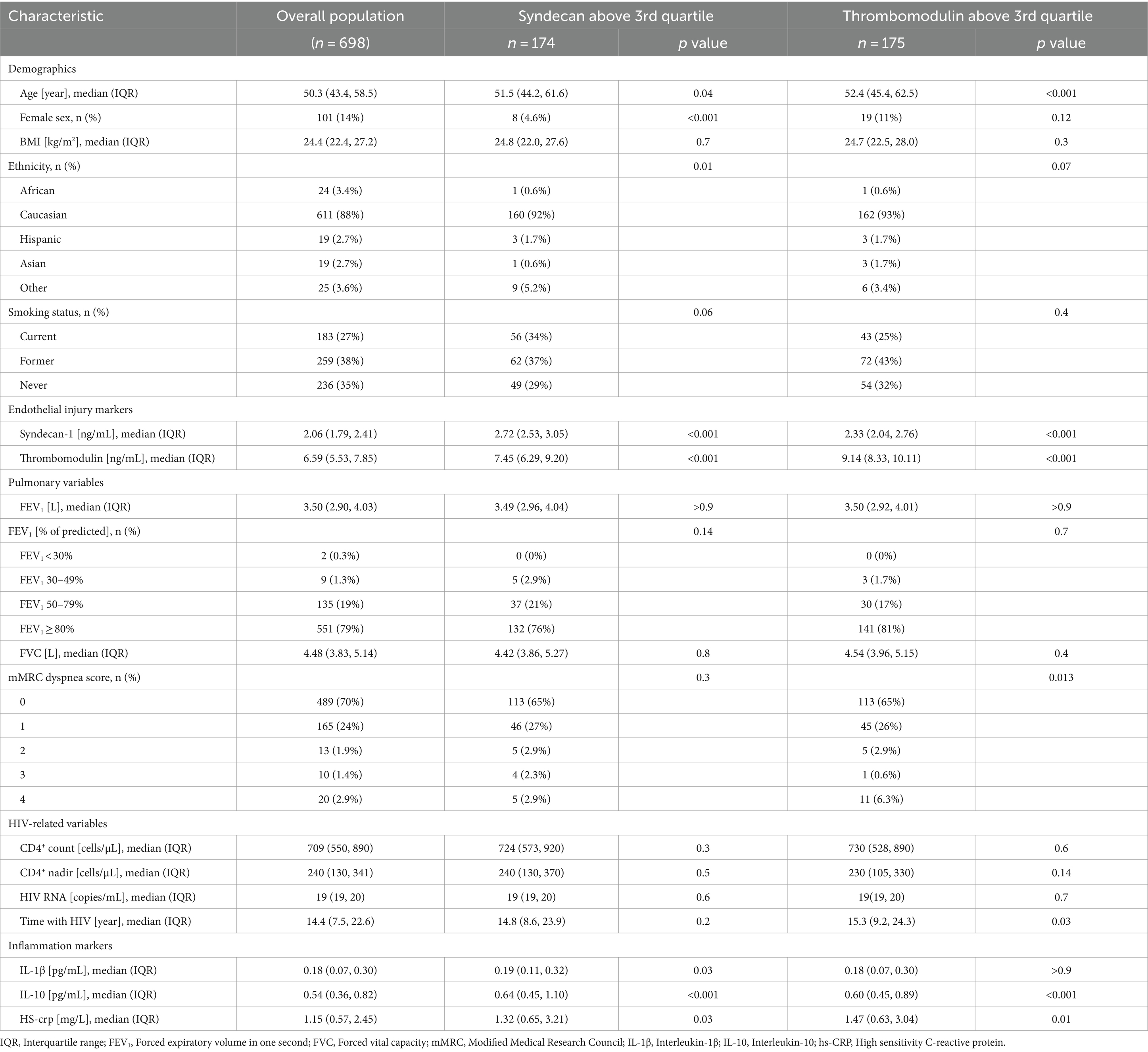
Table 1. Baseline characteristics.
Overall, we found that FEV1 declined 38.6 mL/year (95% CI: 34.8–42.4, p < 0.001). An excess, though not statistically significant, decline was found in fully adjusted models for both upper quartile SDC1: 4.5 mL/year (95% CI: −3.9–12.9, p = 0.30) and upper quartile TM: 2.2 mL/year (95% CI: −6.0–10.4, p = 0.60). The adjusted results were an attenuation of the crude analyses (for crude analyses see Table 2).
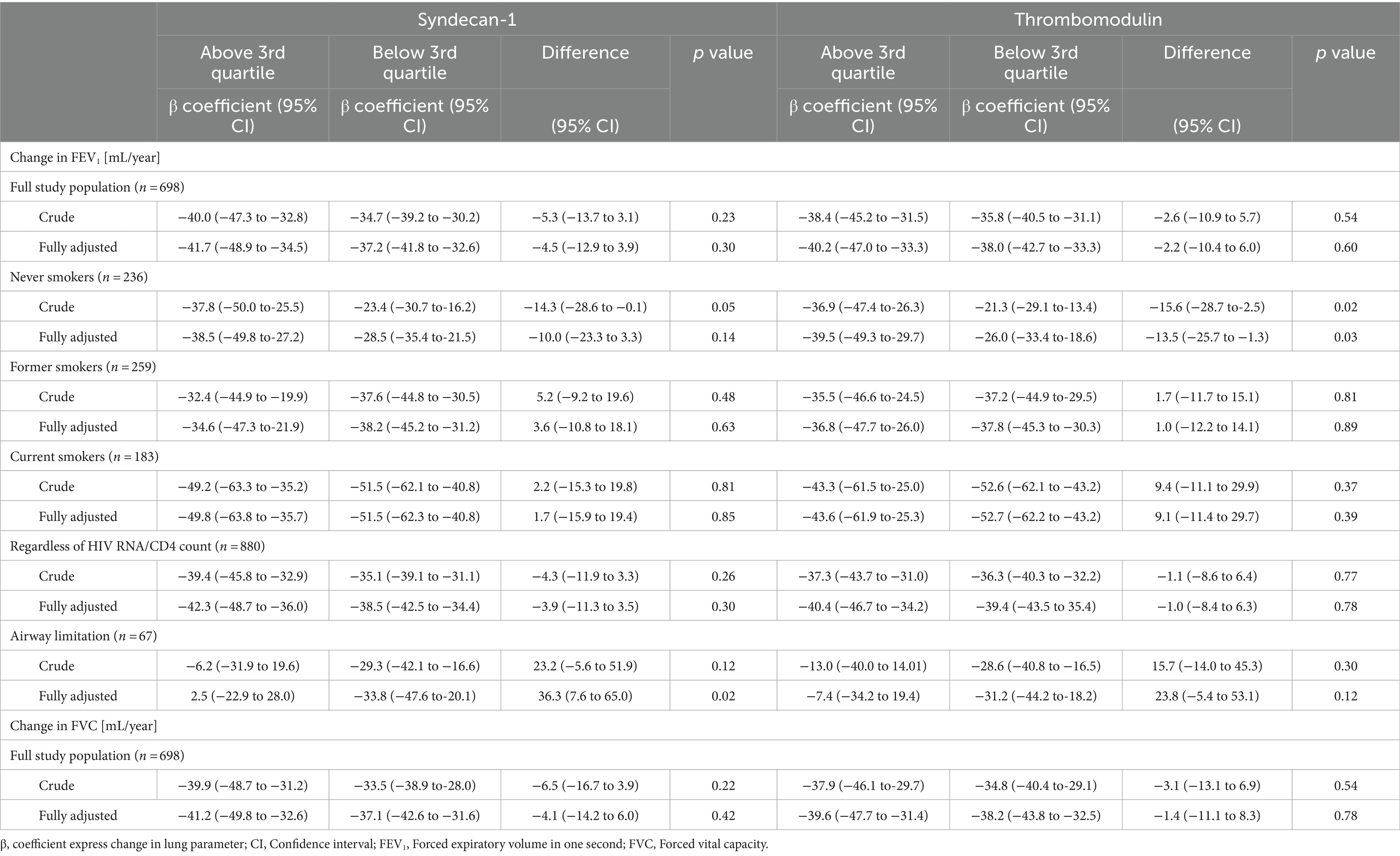
Table 2. Change in lung function according to syndecan-1 and thrombomodulin plasma levels at baseline.
In the sensitivity analysis stratifying for smoking status, a significant faster decline in the never smoking group (n = 236) was observed for both upper quartile SDC1: 14.3 mL/year (95% CI: 0.1–28.6, p = 0.05) and TM: 15.6 mL/year (95% CI: 2.5–28.7, p = 0.02). After adjustment only elevated TM remained significantly associated with a faster decline in FEV1: Upper quartile SDC1: 10.0 mL/year (95% CI: −3.3–23.3, p = 0.14) and TM: 13.5 mL/year (95% CI: 1.3–25.7, p = 0.03). For current and former smokers no significant results were observed (for analyses see Table 2).
In the subgroup analysis with airflow limitation (n = 67), upper quartile SDC1 and TM were associated with large, mostly non-significant increases in FEV1, probably due to random findings in a small subgroup (for analyses see Table 2).
In the sensitivity analysis including patients regardless of HIV RNA and CD4+ count (n = 880) no significant associations between upper quartile SDC1 or TM and decline in FEV1 were observed (for analyses see Table 2).
In general, we found that FVC declined 38.5 mL/year (95% CI: 33.8–43.2, p < 0.001). An excess, not significant, decline was found for both upper quartile SDC1: 4.1 mL/year (95% CI: −6.0–14.2 p = 0.42) and upper quartile TM: 1.4 mL/year (95% CI: −8.3–11.1, p = 0.78), both results fully adjusted. The adjusted results were an attenuation of the crude analyses (for crude analyses see Table 2).
We observed a significant reduction in the risk for rapid decline in FEV1 in the fully adjusted analysis for upper SDC1: OR 0.68 (95% CI: 0.47–0.99, p = 0.04) while upper quartile TM did not change risk for rapid decliner phenotype: OR: 1.04 (95% CI: 0.73–1.49, p = 0.83). The crude analyses were non-significant (for crude analyses see Table 3).
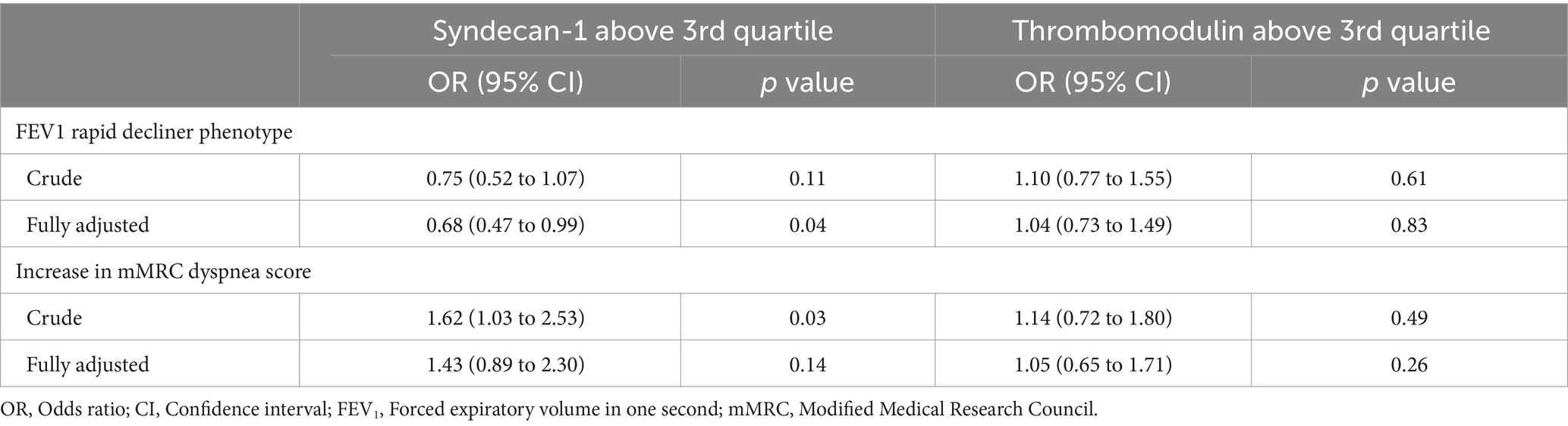
Table 3. Odds for FEV1 rapid decliner phenotype and increase in mMRC dyspnea score according to syndecan-1 and thrombomodulin plasma levels at baseline.
Neither upper quartile SDC1 or TM were associated with a risk for increased dyspnea score in the fully adjusted model: SDC1: OR 1.43 (95% CI: 0.89–2.30, p = 0.14) and TM: OR 1.05 (95% CI: 0.65–1.71, p = 0.26), however in the crude model SDC1 was significantly associated with increased dyspnea score (for crude analyses see Table 3).
We did not find an association between the investigated biomarkers of endothelial injury, TM and SDC1, and decline in lung function or dyspnea. However, in a subgroup of never-smokers (n = 236), we did find a significant association between TM and SDC1 in the crude analysis with only TM remaining significant in the fully adjusted model, although not adjusting for multiple testing.
We hypothesized that endothelial dysfunction and injury might play an important role in driving the decline in lung function. Indeed, our analysis of a never-smoking population suggested that TM and SDC1 could serve as markers of endothelial injury and predict impairment in lung function. However, smoking is a very potent driver of lung function impairment and the main cause of COPD in high income countries (32). Also, smoking is a major contributor to endothelial injury and cardiovascular disease (33, 34), as is also seen in the considerably overlap of COPD and cardiovascular diseases (35). Therefore, it is possible that smoking-related endothelial damage may be not directly related to levels of SDC1 and TM.
The equilibrium between membrane bound and soluble SDC1 and TM is complex and not only influenced by endothelial injury, but also regulated by multiple factors (16, 18). As a result of this complexity, results may be difficult to interpret. A case-cohort study by Salomaa et al. observed decreasing incidence of coronary heart disease with increasing levels of soluble TM. However, the also observed an increase in carotid atherosclerosis with increasing TM (36). Similarly, a recent study by Bundgård et al. reported an association between elevated levels of soluble TM and decreased odds for peripheral arterial disease (31). The explanations may be many, but one offered by the two aforementioned studies was, that increasing levels of soluble TM reflects increasing levels of membrane bound TM which protect the endothelium and ensure an overall anticoagulant state both at and in close proximity to the endothelium and thereby reducing the risk of disease (31, 36). Interestingly, in the present study, a subgroup analysis considering only PLWH with airway limitation (n = 67) found that both elevated TM and SDC1 were associated with protection against decline in FEV1, however the subgroup was small and the findings non-significant.
PLWH with HIV RNA viral load >100 copies and/or CD4+ count ≤300 cells/μl were excluded from the main study, as we hypothesized that uncontrolled HIV may be a confounder both influencing SDC-1 and TM levels and lung function decline thereby distorting the association. However, the sensitivity analysis considering PLWH regardless of HIV RNA viral load and CD4+ count did not find any association between markers of endothelial damage and FEV1 decline, in line with the main analysis findings.
This study was performed on a large, well-characterized population of well-treated PLWH on antiretroviral therapy. Further strengthening the study, spirometry data underwent vigorous validation. Some limitations should be considered: Most notably the follow-up was approximately 2 years which might be too short to demonstrate a significant decline in lung function parameters associated with endothelial injury biomarkers TM and SDC1. Also, TM and SDC1 are only measured once at baseline and therefore temporal alterations in biomarker levels cannot be accounted for. Additionally, TM and SDC1 are not measured locally in the respiratory tract. In future follow-up visits it would be interesting to collect sputum samples, to establish whether biomarkers of endothelial injury in sputum is correlated to lung decline. Last, 150 patients dropped out before follow-up, which may introduce attrition bias to some degree.
To conclude, in this study comprising 698 well-treated PLWH, we did not find an association between elevated biomarkers of endothelial injury, TM and SDC1, and an accelerated decline in lung function nor an increased level of dyspnea.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
This study approved by Committee on Health Research Ethics of the Capital Region of Denmark (approval number H-8-2014-004). This study was conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
CR: Conceptualization, Formal analysis, Methodology, Software, Writing – original draft. AK: Conceptualization, Methodology, Writing – review & editing. NA: Conceptualization, Methodology, Writing – review & editing. RT: Methodology, Writing – review & editing. S-LH: Methodology, Writing – review & editing. PS: Methodology, Writing – review & editing. CU: Methodology, Writing – review & editing. TB: Methodology, Writing – review & editing. SO: Methodology, Writing – review & editing. JJ: Conceptualization, Methodology, Writing – review & editing. SN: Conceptualization, Funding acquisition, Methodology, Supervision, Writing – review & editing.
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This study was supported by Rigshospitalet, the Novo Nordisk Foundation, and Gilead Sciences. The funder Gilead Sciences was not involved in the study design, collection, analysis, interpretation of data, the writing of this article, or the decision to submit it for publication.
We sincerely thank all the participants of the COCOMO study for their participation.
Outside the submitted work, AK has received grant from Gilead, speaker’s fee and travel grants from GSK. RT has received travel grants from Gilead. S-LH has received grants from Novo Nordisk Foundation and meeting and travel grants from GSK. CU reports grants from Sanofi, grants and advisory board participation from Boehringer Ingelheim, grants, consulting fees, speaker fees, and advisory board participation from AstraZeneca, grants and advisory board participation from Novartis, consulting fees and advisory board participation from Chiesi, consulting and speaker fees Orion Pharma, consulting fees and advisory board participation from GSK, consulting fees, speaker fees, and advisory board participation from TEVA. TB reports grants from Novo Nordisk Foundation, grants from Simonsen Foundation, grants from Kai Hansen Foundation, grants from Erik and Susanna Olsen’s Charitable Fund grants, consulting fees, lecture fees, and advisory board participation from GSK, grants, consulting fees, lecture fees, and advisory board participation from Pfizer, lecture fees from Boehringer Ingelheim, lecture fees from Abbvie, grants, lecture fees, and advisory board participation from Gilead, advisory board participation from MSD, grants from Lundbeck Foundation, advisory board participation for Janssen, and lecture fees and advisory board participation for AstraZeneca. SN reports grants from Novo Nordisk Foundation, grants from Sofus Carl Emil Friis and Wife Olga Doris Friis Scholarship, speakers fee and advisory board participation for Gilead, speakers fee and advisory board participation for MSD, and advisory board participation for GSK.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2024.1337609/full#supplementary-material
1. Verboeket, SO, Boyd, A, Wit, FW, Verheij, E, Schim van der Loeff, M, Kootstra, N, et al. Changes in lung function among treated HIV-positive and HIV-negative individuals: analysis of the prospective AGEhIV cohort study. Lancet Healthy Longevity. (2021) 2:e202–11. doi: 10.1016/S2666-7568(21)00033-7
2. Thudium, RF, Ronit, A, Afzal, S, Çolak, Y, Forman, JL, Mendo, F, et al. Faster lung function decline in people living with HIV despite adequate treatment: a longitudinal matched cohort study. Thorax. (2023) 78:535–42. doi: 10.1136/thorax-2022-218910
3. Bigna, JJ, Kenne, AM, Asangbeh, SL, and Sibetcheu, AT. Prevalence of chronic obstructive pulmonary disease in the global population with HIV: a systematic review and meta-analysis. Lancet Glob Health. (2018) 6:e193–202. doi: 10.1016/S2214-109X(17)30451-5
4. Raju, S, McCormack, MC, Drummond, MB, Ramamurthi, HC, Merlo, CA, Wise, RA, et al. Association of Lung Function with HIV-related quality of life and health care utilization in a high-risk cohort. JAIDS J Acquired Immune Deficiency Syndromes. (2020) 85:219–26. doi: 10.1097/QAI.0000000000002431
5. Bikov, A, Lange, P, Anderson, JA, Brook, RD, Calverley, PMA, Celli, BR, et al. FEV(1) is a stronger mortality predictor than FVC in patients with moderate COPD and with an increased risk for cardiovascular disease. Int J Chron Obstruct Pulmon Dis. (2020) 15:1135–42. doi: 10.2147/COPD.S242809
6. Jakeways, N, McKeever, T, Lewis, SA, Weiss, ST, and Britton, J. Relationship between FEV1 reduction and respiratory symptoms in the general population. Eur Respir J. (2003) 21:658–63. doi: 10.1183/09031936.03.00069603
7. Müllerova, H, Maselli, DJ, Locantore, N, Vestbo, J, Hurst, JR, Wedzicha, JA, et al. Hospitalized exacerbations of COPD: risk factors and outcomes in the ECLIPSE cohort. Chest. (2015) 147:999–1007. doi: 10.1378/chest.14-0655
8. Soriano, JB, Lamprecht, B, Ramírez, AS, Martinez-Camblor, P, Kaiser, B, Alfageme, I, et al. Mortality prediction in chronic obstructive pulmonary disease comparing the GOLD 2007 and 2011 staging systems: a pooled analysis of individual patient data. Lancet Respir Med. (2015) 3:443–50. doi: 10.1016/S2213-2600(15)00157-5
9. Theodorakopoulou, MP, Alexandrou, ME, Bakaloudi, DR, Pitsiou, G, Stanopoulos, I, Kontakiotis, T, et al. Endothelial dysfunction in chronic obstructive pulmonary disease: a systematic review and meta-analysis of studies using different functional assessment methods. ERJ Open Res. (2021) 7:00983–2020. doi: 10.1183/23120541.00983-2020
10. Peinado, VI, Barbera, JA, Ramirez, J, Gomez, FP, Roca, J, Jover, L, et al. Endothelial dysfunction in pulmonary arteries of patients with mild COPD. Am J Phys. (1998) 274:L908–13. doi: 10.1152/ajplung.1998.274.6.L908
11. Huertas, A, Guignabert, C, Barberà, JA, Bärtsch, P, Bhattacharya, J, Bhattacharya, S, et al. Pulmonary vascular endothelium: the orchestra conductor in respiratory diseases. Highlights Basic Res Therapy. (2018) 51:1700745. doi: 10.1183/13993003.00745-2017
12. Kohlbrenner, D, Clarenbach, CF, Thiel, S, Roeder, M, Kohler, M, and Sievi, NA. A few more steps lead to improvements in endothelial function in severe and very severe COPD. Respir Med. (2021) 176:106246. doi: 10.1016/j.rmed.2020.106246
13. Hisata, S, Racanelli, AC, Kermani, P, Schreiner, R, Houghton, S, Palikuqi, B, et al. Reversal of emphysema by restoration of pulmonary endothelial cells. J Exp Med. (2021) 218:e20200938. doi: 10.1084/jem.20200938
14. Gelpi, M, Afzal, S, Lundgren, J, Ronit, A, Roen, A, Mocroft, A, et al. Higher risk of abdominal obesity, elevated low-density lipoprotein cholesterol, and hypertriglyceridemia, but not of hypertension, in people living with human immunodeficiency virus (HIV): results from the Copenhagen comorbidity in HIV infection study. Clin Infect Dis. (2018) 67:579–86. doi: 10.1093/cid/ciy146
15. Meneses, GC, Cavalcante, MG, da Silva Junior, GB, Martins, AMC, Neto, RJP, Libório, AB, et al. Endothelial Glycocalyx damage and renal dysfunction in HIV patients receiving combined antiretroviral therapy. AIDS Res Hum Retrovir. (2017) 33:703–10. doi: 10.1089/aid.2016.0284
16. Leucker, TM, Weiss, RG, Schär, M, Bonanno, G, Mathews, L, Jones, SR, et al. Coronary endothelial dysfunction is associated with elevated serum PCSK9 levels in people with HIV independent of low-density lipoprotein cholesterol. J Am Heart Assoc. (2018) 7:e009996. doi: 10.1161/JAHA.118.009996
17. Weinbaum, S, Tarbell, JM, and Damiano, ER. The structure and function of the endothelial Glycocalyx layer. Annu Rev Biomed Eng. (2007) 9:121–67. doi: 10.1146/annurev.bioeng.9.060906.151959
18. Reitsma, S, Slaaf, DW, Vink, H, van Zandvoort, MAMJ, and oude Egbrink, MGA. The endothelial glycocalyx: composition, functions, and visualization. Pflugers Arch. (2007) 454:345–59. doi: 10.1007/s00424-007-0212-8
19. Bertrand, J, and Bollmann, M. Soluble syndecans: biomarkers for diseases and therapeutic options. Br J Pharmacol. (2019) 176:67–81. doi: 10.1111/bph.14397
20. Manon-Jensen, T, Itoh, Y, and Couchman, JR. Proteoglycans in health and disease: the multiple roles of syndecan shedding. FEBS J. (2010) 277:3876–89. doi: 10.1111/j.1742-4658.2010.07798.x
21. Martin, FA, Murphy, RP, and Cummins, PM. Thrombomodulin and the vascular endothelium: insights into functional, regulatory, and therapeutic aspects. Am J Physiol Heart Circ Physiol. (2013) 304:H1585–97. doi: 10.1152/ajpheart.00096.2013
22. Ghondaghsaz, E, Khalaji, A, Norouzi, M, Fraser, DD, Alilou, S, and Behnoush, AH. The utility of syndecan-1 circulating levels as a biomarker in patients with previous or active COVID-19: a systematic review and meta-analysis. BMC Infect Dis. (2023) 23:510. doi: 10.1186/s12879-023-08473-9
23. Tromp, J, van der Pol, A, Klip, IJT, de Boer, RA, Jaarsma, T, van Gilst, WH, et al. Fibrosis marker syndecan-1 and outcome in patients with heart failure with reduced and preserved ejection fraction. Circ Heart Fail. (2014) 7:457–62. doi: 10.1161/CIRCHEARTFAILURE.113.000846
24. Lehnert, P, Johansson, PI, Ostrowski, SR, Møller, CH, Bang, LE, Olsen, PS, et al. Coagulopathy in patients with acute pulmonary embolism: a pilot study of whole blood coagulation and markers of endothelial damage. Scand J Clin Lab Invest. (2017) 77:19–26. doi: 10.1080/00365513.2016.1239130
25. Padberg, JS, Wiesinger, A, di Marco, GS, Reuter, S, Grabner, A, Kentrup, D, et al. Damage of the endothelial glycocalyx in chronic kidney disease. Atherosclerosis. (2014) 234:335–43. doi: 10.1016/j.atherosclerosis.2014.03.016
26. Boffa, MC, and Karmochkine, M. Thrombomodulin: an overview and potential implications in vascular disorders. Lupus. (1998) 7:120–5. doi: 10.1177/096120339800700227
27. Dane, MJ, Khairoun, M, Lee, DH, van den Berg, BM, Eskens, BJM, Boels, MGS, et al. Association of kidney function with changes in the endothelial surface layer. Clin J Am Soc Nephrol. (2014) 9:698–704. doi: 10.2215/CJN.08160813
28. Ware, LB, Fang, X, and Matthay, MA. Protein C and thrombomodulin in human acute lung injury. Am J Phys Lung Cell Mol Phys. (2003) 285:L514–21. doi: 10.1152/ajplung.00442.2002
29. Ronit, A, Haissman, J, Kirkegaard-Klitbo, DM, Kristensen, TS, Lebech, AM, Benfield, T, et al. Copenhagen comorbidity in HIV infection (COCOMO) study: a study protocol for a longitudinal, non-interventional assessment of non-AIDS comorbidity in HIV infection in Denmark. BMC Infect Dis. (2016) 16:713. doi: 10.1186/s12879-016-2026-9
30. Løkke, A, Marott, JL, Mortensen, J, Nordestgaard, BG, Dahl, M, and Lange, P. New Danish reference values for spirometry. Clin Respir J. (2013) 7:153–67. doi: 10.1111/j.1752-699X.2012.00297.x
31. Bundgård, J, Jensen, AMR, Suarez-Zdunek, MA, Høgh, J, Gerstoft, J, Benfield, T, et al. Peripheral artery disease and markers of endothelial dysfunction and platelet activation in people with HIV. J Acquir Immune Defic Syndr. (2023) 93:237–43. doi: 10.1097/QAI.0000000000003194
32. Barnes, PJ, Burney, PGJ, Silverman, EK, Celli, BR, Vestbo, J, Wedzicha, JA, et al. Chronic obstructive pulmonary disease. Nat Rev Dis Primers. (2015) 1:15076. doi: 10.1038/nrdp.2015.76
33. Powell, JT, Edwards, RJ, Worrell, PC, Franks, PJ, Greenhalgh, RM, and Poulter, NR. Risk factors associated with the development of peripheral arterial disease in smokers: a case-control study. Atherosclerosis. (1997) 129:41–8. doi: 10.1016/S0021-9150(96)06012-1
34. Manley, AF . Cardiovascular implications of smoking: the surgeon general's point of view. J Health Care Poor Underserved. (1997) 8:303–10. doi: 10.1353/hpu.2010.0517
35. Rabe, KF, Hurst, JR, and Suissa, S. Cardiovascular disease and COPD: dangerous liaisons? Eur Respir Rev. (2018) 27:180057. doi: 10.1183/16000617.0057-2018
36. Salomaa, V, Matei, C, Aleksic, N, Sansores-Garcia, L, Folsom, AR, Juneja, H, et al. Soluble thrombomodulin as a predictor of incident coronary heart disease and symptomless carotid artery atherosclerosis in the atherosclerosis risk in communities (ARIC) study: a case-cohort study. Lancet. (1999) 353:1729–34. doi: 10.1016/S0140-6736(98)09057-6
Keywords: endothelial dysfunction, inflammation, spirometry, lung function, lung function decline, HIV
Citation: Rønn C, Knudsen AD, Arentoft NS, Thudium RF, Heidari S-L, Sivapalan P, Ulrik CS, Benfield T, Ostrowski SR, Jensen JUS and Nielsen SD (2024) Endothelial injury and decline in lung function in persons living with HIV: a prospective Danish cohort study including 698 adults. Front. Med. 11:1337609. doi: 10.3389/fmed.2024.1337609
Edited by:
Hyun Woo Lee, Seoul Metropolitan Government - Seoul National University Boramae Medical Center, Republic of KoreaReviewed by:
Konstantinos Bartziokas, Independent researcher, Trikala, GreeceCopyright © 2024 Rønn, Knudsen, Arentoft, Thudium, Heidari, Sivapalan, Ulrik, Benfield, Ostrowski, Jensen and Nielsen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Christian Rønn, Q2hyaXN0aWFuLnJvZW5uQHJlZ2lvbmguZGs=; Susanne D. Nielsen, c3VzYW5uZS5kYW0ucG91bHNlbkByZWdpb25oLmRr
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.