
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Med., 23 January 2024
Sec. Dermatology
Volume 11 - 2024 | https://doi.org/10.3389/fmed.2024.1328488
This article is part of the Research TopicThe Impact of the COVID-19 Pandemic on Dermatology Patients: Diagnosis, Treatment, and PrognosisView all 8 articles
 Adina Patricia Apostu1,2
Adina Patricia Apostu1,2 Ștefan Cristian Vesa3*Simona Frățilă4,5Gabriela Iancu6,7Nona Bejinariu8Maximilian Muntean9Simona C. Șenilă1,10Oana Alexandra Baba2Cristina Pop Secășan10
Ștefan Cristian Vesa3*Simona Frățilă4,5Gabriela Iancu6,7Nona Bejinariu8Maximilian Muntean9Simona C. Șenilă1,10Oana Alexandra Baba2Cristina Pop Secășan10 Loredana Ungureanu1,10
Loredana Ungureanu1,10Background: The COVID-19 pandemic disrupted the healthcare system and negatively affected the diagnosis and management of melanoma worldwide. The purpose of this study is to investigate the long-term effects of the COVID-19 pandemic on the diagnosis and prognosis of melanoma.
Materials and methods: This retrospective cohort study included histopathologically confirmed melanoma cases from March 2019 to February 2023 in Cluj and Bihor counties. Data from the post-COVID-19 period (March 2021 to February 2023) were compared to the pre-COVID-19 period (March 2019 to February 2020) and the COVID-19 period (March 2020 to February 2021). Patient characteristics, monthly diagnostics, histological subtypes, and key histological features were analyzed using statistical tests.
Results: The number of melanoma cases diagnosed annually decreased by 31.37 and 23.75% in the first and second post-pandemic years, respectively, compared to pre-pandemic numbers. Diagnostic rates also decreased by 14.9 and 5.4% in the first and second post-pandemic years, respectively, compared to the pandemic period. Prognostic factors worsened in the post-pandemic period, with higher Breslow index and mitotic rate, and increased ulceration and thick melanomas compared to the pre-pandemic period.
Conclusion: The COVID-19 pandemic had a long-lasting impact on the diagnosis of melanoma in Romania, resulting in advanced stages and unfavorable prognostic factors. Larger global studies are needed to comprehensively understand the pandemic’s long-term effects on the diagnosis of melanoma.
Melanoma, one of the most aggressive types of skin cancers, is a global rising health issue, with a significantly increasing incidence worldwide (1, 2).
The rising incidence might be explained by the frequent exposure to sunlight, increasing number of public screening campaigns and the wide adoption of dermoscopy. Several studies have shown that high sun exposure and indoor ultraviolet (UV) tanning significantly increase the risk of melanoma, while a study conducted in the United States of America (United States) highlighted that the preventive measures are not regularly followed: most of the subjects reported one or more sunburns in the previous year (3–5). Dermoscopy improves the accuracy of diagnosis of melanoma compared to naked eye examination and is widely used in almost all dermatological services. Together with increased patient awareness and frequent public screening campaigns, it allows the detection of melanoma at an earlier stage (6). Even if melanoma is less common than other skin cancers, it remains the most deadly, causing death in all age groups, including adolescents, if diagnosed too late (1, 2).
The survival rate for melanoma varies depending on factors such as the stage of the disease when diagnosed, the Breslow index, the mitotic rate, the presence of tumor ulceration, perineural and lymphatic invasion, the patients’ overall health and the treatment received. For localized melanoma (stage 0-stage I), the 5-year survival rate is around 97%. However, for stage IV melanoma, the five-year survival rate drops to 4% (7, 8). Detecting melanoma in its early stages is crucial for its survival rate as it allows timely intervention and treatment, significantly improving the chances of successful outcome and reducing the risk of severe complications (7, 8).
Threrefore, the early melanoma diagnosis is considered an important task by the healthcare providers worldwide, but the significant rise in melanoma incidence with no increase in mortality might be interpreted as overdiagnosis. Even if the incidence of both invasive and in situ melanoma is rising,for in situ melanoma it does so exponentially. One possible explanation is that tumors which had previously been diagnosed as “dysplastic nevi” are now labelled as melanoma in situ, yet evidence suggests a low probability of progression to invasive melanoma. Another explanation is the rising use of dermoscopy which improves the accuracy of diagnosis (6, 9–11).
The question which arises is whether the overdiagnosis of melanoma has a negative impact on the patient physical and mental health. While most of the patients get a small scar after a wide excision, with almost zero morbidity, the negative emotional and economic effects of overdiagnosis support the efforts to reduce it (12, 13). Nazzaro et al. proposed five dermoscopic predictors of small diameter melanoma to decrease the rate of overdiagnosis and the unnecessary biopsies, but further research on larger datasets is needed to validate the results (14).
Betz-Stablein et al. recommend combining clinical information, total body photography, sequential dermoscopy images and whole slide pathology images associated by artificial intelligence (AI) to increase diagnostic accuracy and decrease the rate of overdiagnosis (9). To date, no healthcare provider should ever take the risk of not excising a lesion just because of the fear of overdiagnosis, as long as the available evidence is insufficient to predict the outcome of the tumor (9, 15).
The most recent and important global pandemic of the last decades, Coronavirus Disease 2019 (COVID-19), caused by the SARS-CoV2 virus, came as a substantial healthcare system challenge. Since the World Health Organization declared the COVID-19 pandemic a global health issue in March 2020, healthcare services had to redirect resources for the management of the COVID-19 patients and most of the countries around the globe imposed harsh restrictions in order to reduce the high infection rates. The restrictions implemented to stop transmission led to drastic reductions in non-urgent medical visits, hindering the management of other conditions (16–18).
The interruption of the healthcare system negatively affected the diagnosis and management of melanoma worldwide. Many studies reported a reduction in the diagnosis of melanoma and an increase in the more advanced stages diagnosed during the COVID-19 pandemic when comparing to the pre-pandemic period (19–23). On the other hand, assessing the cases following the lockdown, they displayed a higher level of progression (24).
Therefore, this study aims to investigate the long-term effects of the COVID-19 pandemic on the diagnosis and prognosis of melanoma in two academic medical centers in Romania (Cluj-Napoca and Oradea).
This was an observational, retrospective, cohort study carried out in Cluj and Bihor counties, in the North-Western Region of Romania. We included all the histopathologically confirmed cases of melanoma from 1 March 2019 to 28 February 2023 from all histopathological centers from the two counties (Santomar, Radusan, Emergency County Hospital Cluj, Emergency County Hospital Oradea, Prof. Dr. I. Chiricuta Institute of Oncology Cluj). We compared the results from 1 March 2021 to 28 February 2022 and from 1 March 2022 to 28 February 2023 (the first and second year of the post COVID-19 period) to the pre COVID-19 period (1 March 2019–29 February 2020) and the COVID-19 period (1 March 2020–28 February 2021). We excluded the cases with incomplete data or with a histopathologic diagnosis of melanoma metastasis. This study was approved by the Ethics Committee (No.4249/30.01.2023). Patient characteristics (age and gender), the monthly numbers of melanomas diagnosed, histological subtypes (superficial spreading melanoma (SSM), lentigo maligna melanoma (LMM), nodular melanoma (NM), acral lentiginous melanoma (ALM), and others), and the following histological features (Breslow index, presence of mitosis, ulceration, vascular and neural invasion, and tumor stage [TNM edition]) were collected (25).
Statistical analysis was performed using the MedCalc® Statistical Software version 20.014 (MedCalc Software Ltd., Ostend, Belgium; https://www.medcalc.org. Numerical variables were expressed as median and 25th–75th percentiles. Categorical data were presented as frequency and percentage. The Mann–Whitney U test was used to determine differences in age, Breslow index, mitotic count and the chi-square test was used for gender, histological subtype, ulceration, vascular/lymphatic invasion, neural invasion, staging. A p value <0.05 was considered statistically significant.
During the study period, 1,284 patients were diagnosed with melanoma (658 females, 626 males). A total of 1,100 patients (341 in the pre-COVID period, 275 in the COVID period and 494 in the post COVID period, 234 between March 2021 and February 2022 and 260 between March 2022 and February 2023) were included in the study. A number of 184 patients were excluded due to missing data. There were no significant differences in patient characteristics in the three cohorts regarding gender. There was a statistically significant difference in the average age for diagnosis: 59 before the pandemic, 63 during the pandemic and 59 after the pandemic.
The total number of melanoma cases diagnosed in the first year of the post COVID19 period decreased by 31.37% and by 23.75% in the second year respectively, when compared to the pre COVID-19 period. The Breslow index and the mitotic rate were statistically significantly higher in the post-COVID-19- first year period (p < 0.001) and in the post-COVID19- second year period (p = 0.004) when compared to the pre-COVID-19 period. Ulceration was significantly more frequent in the post-COVID-19- first year group (p < 0.05). There was also a statistically significantly higher number of thick melanomas in the post-COVID-19 period. (65.0% vs. 49.6% in the first year and 60.0% vs. 49.6% in the second year); p < 0.001 and p < 0.05, respectively. The most common histological subtype was SSM in the three periods. A larger number of NMs were diagnosed during the post-COVID-19 period (26.9 and 21.9% vs. 17.6%) (Tables 1, 2).
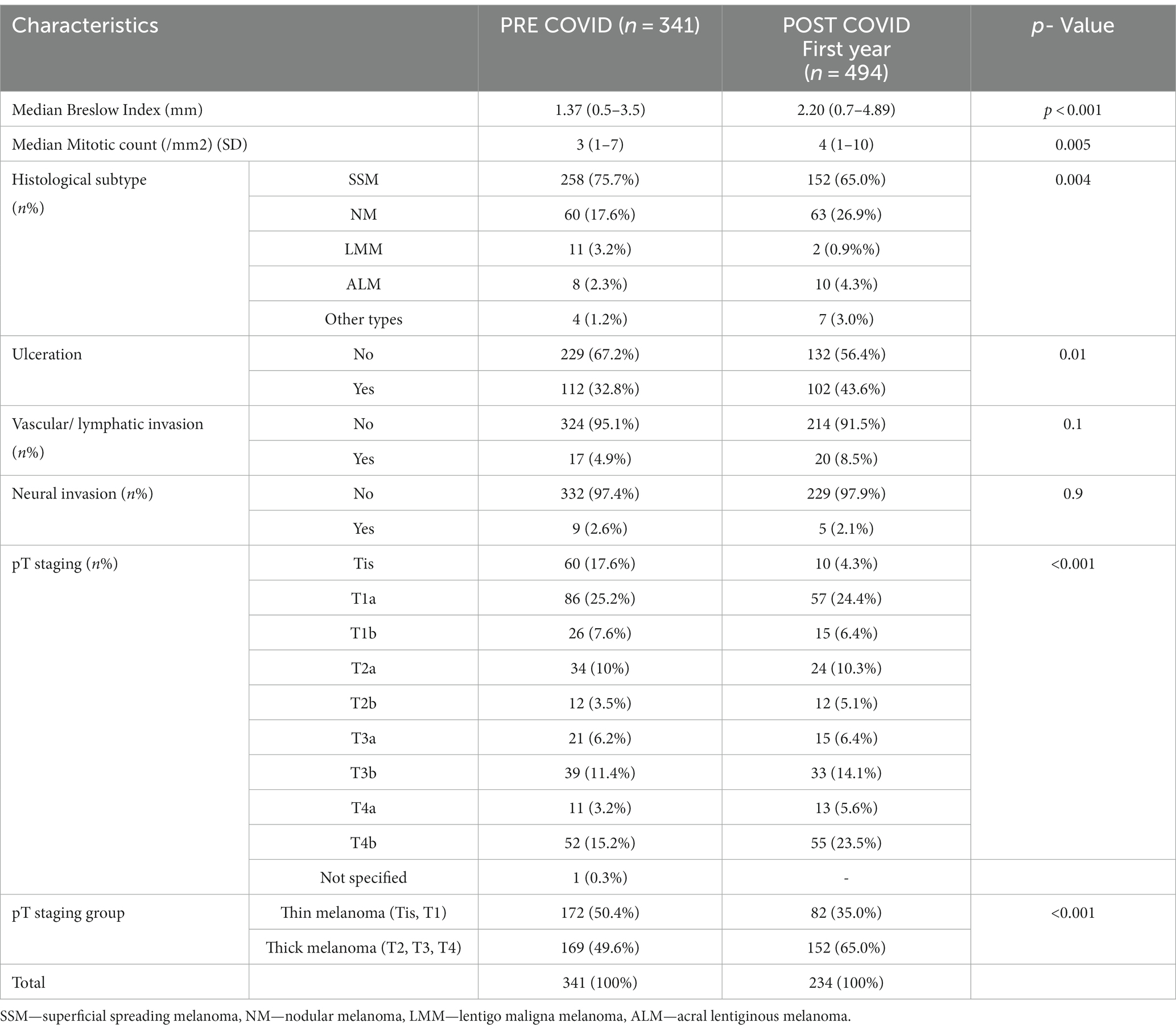
Table 1. Tumor characteristics in the pre-COVID-19 and post-COVID-19- first year period.
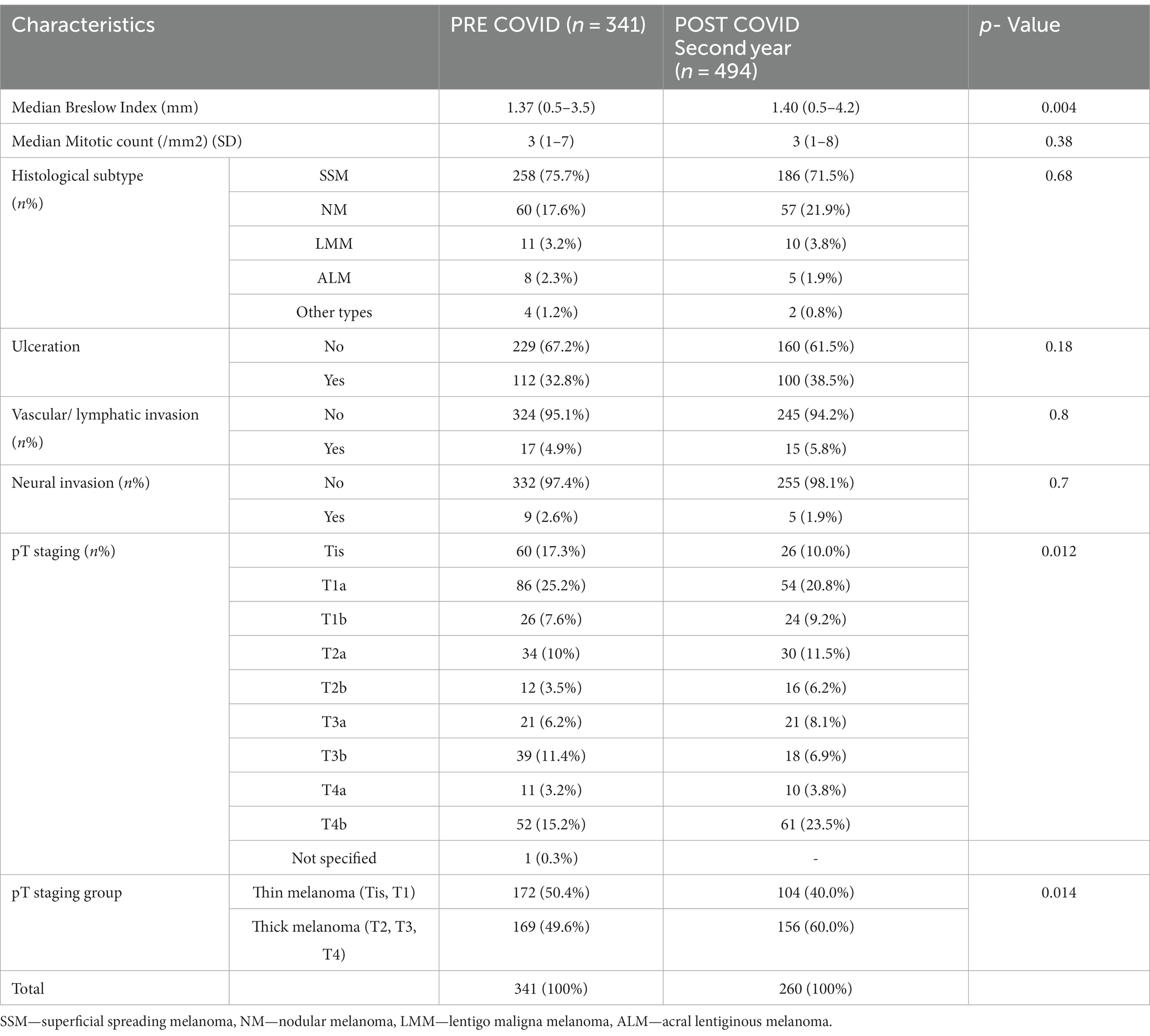
Table 2. Tumor characteristics in the pre-COVID-19 and post-COVID-19- s year period.
The total number of melanoma cases diagnosed in the first year of the post-COVID-19 period decreased by 14.9% and by 5.45% in the second year, respectively, when compared to the COVID-19 period. The Breslow index, the mitotic rate, the percentage of NMs were similar in the post-COVID-19 first year period when compared to the COVID-19 period. The Breslow index and the percentage of NMs were lower in the post-COVID-19 s year when compared to the COVID-19 period, but they do not reach statistical significance. The mitotic rate in the post-COVID-19 s year period was statistically significant lower then in the COVID-19 period (p < 0.05). Also, we did not observe a statistically significantly difference in the presence of ulceration, the vascular/ lymphatic invasion, the neural invasion in the post-COVID-19 period (both years) compared to the COVID-19 period. The percentage of thick melanomas was higher in the post-COVID-19 period (both years), but it did not reach statistical significance. However, we observed a statistically significantly difference in melanoma staging between the two periods, more invasive melanomas being diagnosed during the post-COVID-19 period- first year (p = 0.007) (Tables 3, 4).
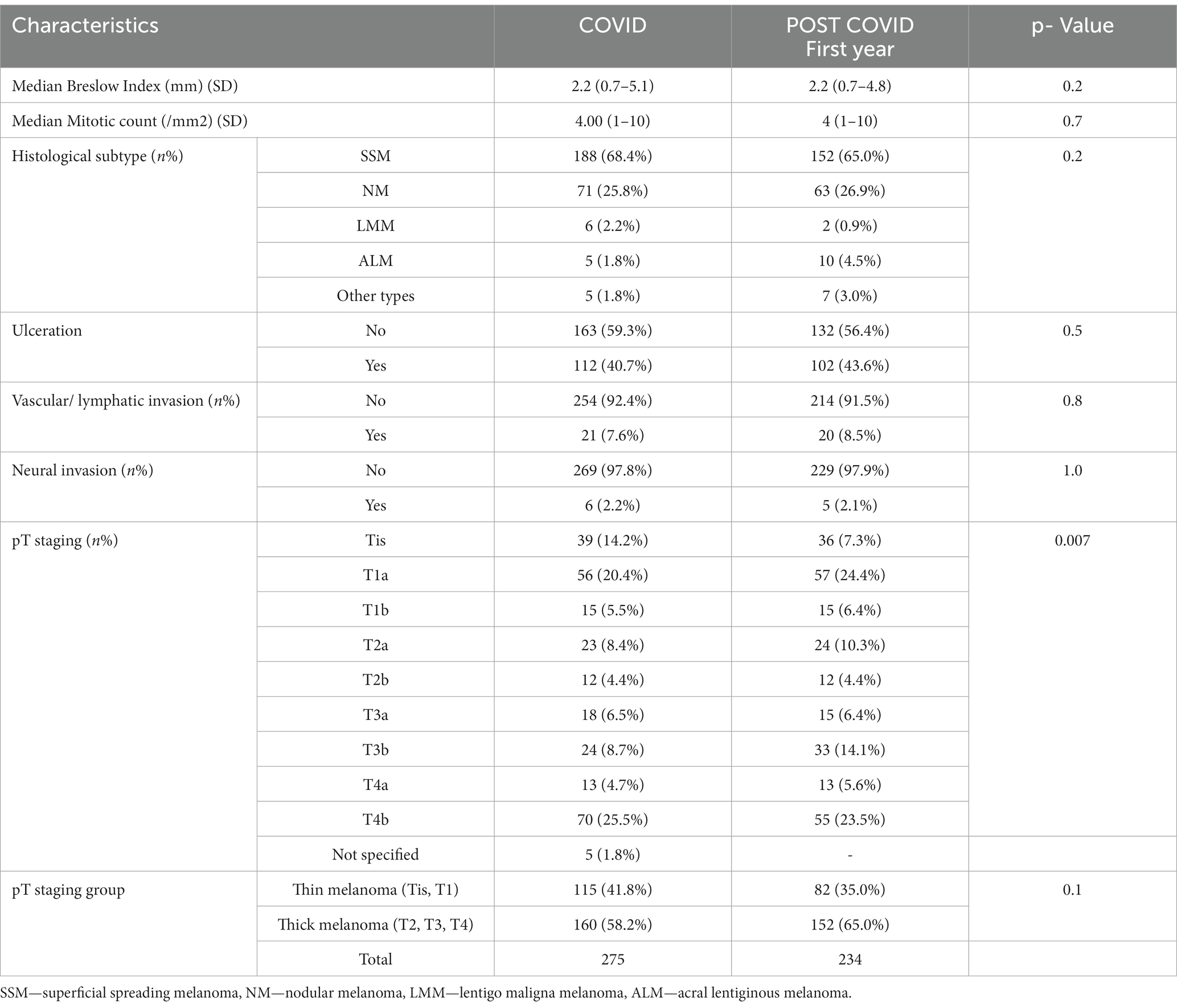
Table 3. Tumor characteristics in the COVID-19 and post-COVID-19 first year period.

Table 4. Tumor characteristics in the COVID-19 and post-COVID-19 s year period.
We report the results of the effects of the COVID-19 pandemic on the diagnosis of melanoma in two academic medical centers in Romania 2 years after the pandemic. We found a decrease in the diagnosis of new melanoma of 31.37% in the first year of the post-COVID-19 period and a decrease by 23.75% in the second year, when compared to the pre-COVID-19 period. When compared to the COVID-19 period, we found a 14.9% decrease in the first year and a 5.4% decrease in the second year.
Several studies showed a significant reduction in the diagnosis of new melanomas since the development of the COVID-19 pandemic, which lead to an increase in melanoma diagnosis post-lockdown (19–22). A possible explanation for this finding can be due to the patients’ fear of contacting the disease while exposed to close contact from their face-to-face medical visits, temporary suspension of cancer screening programs and the substitution of face-to-face visits with telemedicine (23). Moreover, operating rooms were used sparingly during the pandemic to limit the transmission of the virus. A study conducted in Italy reported that surgical procedures were longer to allow for proper sanitizing after each patient and therefore, the number of surgeries was lower (20). On the other hand, a study in USA reported that during the pandemic patients experienced longer waiting times from the initial appointment until the diagnostic biopsy when compared to the pre-pandemic patients, but shorter waiting times from the biopsy until the operation (26). During the COVID-19 pandemic, an institution in Canada cancelled all elective surgeries for benign lesions, prioritizing the oncologic surgeries, and found no differences in overall wait time from the consult to the wide local excision surgery in melanoma patients, when compared to the pre-pandemic period (27). In our region we were able to continue dermo-oncologic surgery throughout the entire lockdown and pandemic period, but similar to the study by Gauldi et al. (20), surgical procedures were longer and the number of surgeries was reduced. Furthermore, we noted that many patients spontaneously cancelled their appointments for fear of getting infected.
Interestingly, our study shows that fewer cases were diagnosed each year after the COVID-19 pandemic. Even if a trend towards normality was observed between the first and the second year of the post COVID-19 period (a 10% increase of newly diagnosed melanoma cases), the diagnostic rates have not yet fully resumed. However, other studies support our findings. The study conducted by Jeremic et al. reported lower melanoma diagnosis rates in 2021 and 2022 when compared to the pre-pandemic years (28). Another Serbian study found 65 melanoma patients registered in 2018, 31 in 2019, 16 in 2020, 30 in 2021, 47 in 2022 and 10 in the first three months of 2023 (29). In Romania, a study by Aabed et al. reported a 17% reduction in melanoma cases 24 months after the outbreak of the COVID19 pandemic when compared to the 24 months before the pandemic, which means that even in the pandemic recovery phase, patients are still reluctant to ask for medical care (30). Also, the decrease in the number of cases after the pandemic in our study might be explained by the fact that during the pandemic there were much fewer skin cancer prevention, screening and awareness campaigns and by the tendency of patients to ask for medical care only in severe situations.
The delay in the diagnosis of melanoma resulted in worse prognostic factors. Compared to the pre-COVID period, the Breslow index was significantly higher during the post-COVID-19 period. In the first year after the COVID-19 pandemic, the mitotic rate was significantly higher and the presence of ulceration was more frequent, which subsequently led to an increase in the number of thick melanomas. Fewer patients presented with in situ disease post-COVID-19, 4.3% in the first year and 10.0% in the second year vs. 17.3% pre-COVID-19 and a higher proportion presented with thick melanomas 65.0% in the first year and 60.0% in the second year vs. 49.6%. Compared to the COVID-19 period, the Breslow index did not reach statistical significance in the post COVID-19 period (both years) and there was no statistically significant difference in the presence of ulceration, vascular/ lymphatic invasion, and neural invasion between the three periods. NMs, the histological subtype with the worst survival rates, increased in the post-COVID-19- first year period when compared to the pre-COVID-19 period and remained constant when compared to the post-COVID-19- s year and COVID-19 period (31).
The shift to more invasive melanomas was documented by other studies (32–34). Gualdi et al. evaluated melanomas excised within two months after the end of the lockdown and found poorer prognostic factors of the disease such as: a higher Breslow index, a higher number of mitoses and a higher number of ulcerated melanomas (20). Another study carried out in Spain compared the melanoma diagnosed one year before the lockdown and one year after the lockdown and found an increase in Breslow thickness, as well as an increase in the number of mitoses and in the percentage of ulcerated melanomas (35). A systematic review carried out by Toma AO et al. analyzing the epidemiology of melanoma 2 years after the COVID-19 pandemic found that the percentage of thick melanomas was higher during 2020–2021 then before the pandemic (36.25% vs 25.88%). They also found a decrease in the proportion of in situ melanoma diagnoses, reported by most of the studies included in the review (36).
On the other hand, an Austrian study reported statistically significant differences in the presence of ulceration in the year after the lockdown, but there were no differences in the Breslow index (19). A nationwide study developed in the Netherlands revealed only a minor shift towards more advanced melanoma stages during the first lockdown and no impact afterwards (37). Klepfisch et al. found no clinical or histopathological differences in the number of melanomas diagnosed after the lockdown compared to the pre-lockdown period and reported a minimal impact of COVID-19 lockdown on the diagnosis of melanoma, however, other studies reported the contrary (38). One possible explanation for the difference between data reported in different countries could be the different magnitude of the pandemic throughout the world (21, 24, 39).
Unfortunately, the effects of the COVID-19 pandemic affect not only those who presented in the months following the lockdown. As was feared, a trend towards a higher cancer stage at presentation still remains for patients in the post-COVID-19 period.
Melanoma represents one of the most aggressive forms of the routinely monitored cancers. More precisely, the doubling time for melanoma is 94 days compared to 936 days for colorectal adenocarcinoma (40, 41). Thus, early diagnosis is crucial for melanoma-associated survival as the risk of metastases increases with a higher Breslow index, mitotic rate and presence of ulceration (42). The COVID-19 pandemic postponed most cancer diagnosis in the corresponding period and therefore postponed treatment. Tejera et al. published a rate of growth model and calculated a 2% loss in 5-year survival for melanoma patients diagnosed with a delay of up to 3 months (43). Another study found that melanoma patients who are diagnosed with a 3-month delay experience a reduction in five-year survival rates of 1.9%, and ten-year survival of 2.4%. Moreover, it has been estimated that melanoma patients diagnosed after March 2020 have a 7% reduction in their survival rates (44). Our study found a higher Breslow index and a greater percent of thick melanomas in the post-COVID period. If melanomas were indeed growing as fast as previously reported, this effect would have been observed only in the period immediately after lockdown. This might suggest that melanomas may grow slower than previously assumed or only the slow-growing tumors were delayed in terms of being diagnosed (37).
Furthermore, patients diagnosed before and after the pandemic were younger than those diagnosed during the pandemic (59 vs. 63 years old), suggesting that elderly patients did not underestimate the severity of their disease. On the other hand, Hurley et al. reported that the mean age was statistically significantly higher pre-COVID-19 compared to the COVID-19 period (68 vs. 63 years), and Martinez- Lopez et al. described a median age of 77 years in the pre-pandemic period compared to 53 years during 2020 and 2021, which might mean that the elderly are more concerned about contacting the COVID-19 (35, 45). A study conducted by Asai et al. reported no difference in the median age of the cohort, both before and during the pandemic (46).
Regarding cancer in general, a study carried out in Catalonia saw a substantial reduction in cancers over two pandemic years (until January 2022), with an estimated 13,000 undetected cancers, compared with the preceding year. Although a trend towards normality was observed in 2021, the diagnostic rates have not yet fully recovered. Also, they found that the pandemic affected women less than men. When it comes to our study, there was no statistically significant difference between the two genders and other studies support our findings (47–49).
Most of the countries worldwide adopted harsh measures in order to prevent the spreading of the COVID-19 and meetings and crowded places had to be avoided until complete virus extinction. Therefore, melanoma screening campaigns, where usually a lot of people took part in, were cancelled. Even if the restrictions were lifted and the screening programs restarted, these delays in screening created a “bottleneck effect” and large numbers of melanomas are still undiagnosed (48). Dermatology specialists, oncology specialists and primary care providers should encourage patients to go back to the doctor and resume their screening programs (49). Moreover, healthcare providers should work together in order to promote and organize more screening campaigns. These may include public awareness campaigns, promoting whole-body self-examination, patient education about sun protection, media campaigns and in person screening programs (50).
To our knowledge, this is the first study that reports the effects of the COVID-19 pandemic on the diagnosis of melanoma 2 years after the pandemic. The strengths of this study lie in the collection of homogeneous data and the long time frames. The limitations of our study consist of it being a retrospective study, the data was not collected from patients seen during the three periods. In addition, it is a double center-study and the sample is limited.
Our study suggests that the COVID-19 pandemic negatively affected the diagnosis of melanoma 2 years after the COVID-19 pandemic in Romania, leading to the detection of the tumor at more advanced stages and worse prognostic factors, which require more diagnostic procedures and more aggressive treatments, resulting in greater healthcare costs and worse survival rates for these patients. Even if the normal clinical activity was restored after the COVID-19 lockdown, our study shows that the diagnostic rates of melanoma have not yet fully recovered. Health care professionals should work together in order to encourage patients to resume their normal medical visits. We believe that larger worldwide studies are needed in order to better define the long-term effects of the COVID-19 pandemic on the diagnosis of melanoma.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by Ethics Committee of the Emergency County Hospital Cluj. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants' legal guardians/next of kin in accordance with the national legislation and institutional requirements.
AA: Conceptualization, Data curation, Investigation, Methodology, Writing – original draft. ȘV: Methodology, Software, Writing – review & editing. SF: Data curation, Formal analysis, Writing – original draft. GI: Data curation, Formal analysis, Writing – original draft. NB: Data curation, Formal analysis, Writing – original draft. MM: Data curation, Formal analysis, Writing – original draft. SȘ: Data curation, Formal analysis, Investigation, Writing – original draft. OB: Data curation, Formal analysis, Writing – original draft. CS: Data curation, Formal analysis, Writing – original draft. LU: Conceptualization, Methodology, Supervision, Validation, Visualization, Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Alessia, V, Gabriella, F, Claudia, C, and Massimiliano, S. Melanoma screening days during the coronavirus disease 2019 (COVID-19) pandemic: strategies to adopt (2020) 10:525–7.
2. Marianne, B, and Charles, W. The current epidemiology of cutaneous malignant melanoma (2006) 11:1244–125. doi: 10.2741/1877,
3. Gandini, S, Sera, F, Cattaruzza, MS, Pasquini, P, Picconi, O, Boyle, P, et al. Meta-analysis of risk factors for cutaneous melanoma: II. Sun exposure Eur J Cancer. (2005) 41:45–60. doi: 10.1016/j.ejca.2004.10.016
4. Boniol, M, Autier, P, Boyle, P, and Gandini, S. Cutaneous melanoma attributable to sunbed use: systematic review and meta- analysis. BMJ. (2012) 345:e4757. doi: 10.1136/bmj.e4757
5. Centers for Disease Control and Prevention . Youth risk be- havior surveillance system: 1991–2013 high school youth risk behavior survey data
6. Kittler, H, Pehamberger, H, Wolff, K, and Binder, M. Diagnostic accuracy of dermoscopy. Lancet Oncol. (2002) 3:159–65. doi: 10.1016/S1470-2045(02)00679-4
7. Balch, CM, Gershenwald, JE, Soong, SJ, Thompson, JF, Atkins, MB, Byrd, DR, et al. Final version of 2009 AJCC melanoma staging and classification. J Clin Oncol. (2009) 27:6199–206. doi: 10.1200/JCO.2009.23.4799
8. Noone, AM, Howlader, N, Krapcho, M, Miller, D, Brest, A, Yu, M, et al. eds. SEER Cancer statistics review, 1975–2015. Bethesda, MD: National Cancer Institute (2018).
9. Betz-Stablein, B, and Soyer, HP. Overdiagnosis in melanoma screening: is it a real problem? Dermatol Pract Concept. (2023) 13:e2023247. doi: 10.5826/dpc.1304a247
10. Welch, HG, Mazer, BL, and Adamson, AS. The rapid rise in cutaneous melanoma diagnoses. N Engl J Med. (2021) 384:72–9. doi: 10.1056/NEJMsb2019760
11. Semsarian, CR, Ma, T, Nickel, B, Scolyer, RA, Ferguson, PM, Soyer, HP, et al. Do we need to rethink the diagnoses melanoma in situ and severely dysplastic naevus? Br J Dermatol. (2022) 186:1030–2. doi: 10.1111/bjd.21010
12. Navarrete-Dechent, C, and Lallas, A. Overdiagnosis of melanoma: is it a real problem? Dermatol Pract Concept. (2023) 13:e2023246. doi: 10.5826/dpc.1304a246
13. Swetter, SM, Tsao, H, Bichakjian, CK, Curiel-Lewandrowski, C, Elder, DE, Gershenwald, JE, et al. Guidelines of care for the management of primary cutaneous melanoma. J Am Acad Dermatol. (2019) 80:208–50. doi: 10.1016/j.jaad.2018.08.055
14. Nazzaro, G, Maronese, CA, Casazza, G, Giacalone, S, Spigariolo, CB, Roccuzzo, G, et al. Dermoscopic predictors of melanoma in small diameter melanocytic lesions (mini-melanoma): a retrospective multicentric study of 269 cases. Int J Dermatol. (2023) 62:1040–9. doi: 10.1111/ijd.16710
15. Zalaudek, I . Over-diagnosis, overtreatment or Oversurveillance of melanoma: is there a way out? Dermatol Pract Concept. (2023) 13:e2023250. doi: 10.5826/dpc.1304a250
16. Patrinely, JR, and Johnson, DB. Pandemic medicine: the management of advanced melanoma during COVID-19. Melanoma Manag. (2020) 7:MMT45. doi: 10.2217/mmt-2020-0012
17. Hanna, TP, King, WD, Thibodeau, S, Jalink, M, Paulin, GA, Harvey-Jones, E, et al. Mortality due to cancer treatment delay: systematic review and meta-analysis. BMJ. (2020) 371:m4087. doi: 10.1136/bmj.m4087
18. Seretis, K, Bounas, N, Gaitanis, G, and Bassukas, I. A Meta-analysis on the impact of the COVID-19 pandemic on cutaneous melanoma diagnosis in Europe. Cancers (Basel). (2022) 14:6085. doi: 10.3390/cancers14246085
19. Hoellwerth, M, Kaiser, A, Emberger, M, Brandlmaier, M, Laimer, M, Egger, A, et al. COVID-19-induced reduction in primary melanoma diagnoses: experience from a Dermatopathology referral center. J Clin Med. (2021) 10:4059. doi: 10.3390/jcm10184059
20. Gualdi, G, Porreca, A, Amoruso, GF, Atzori, L, Calzavara-Pinton, P, De Tursi, M, et al. The effect of the COVID-19 lockdown on melanoma diagnosis in Italy. Clin Dermatol. (2021) 39:911–9. doi: 10.1016/j.clindermatol.2021.05.015
21. Molinier, R, Roger, A, Genet, B, Blom, A, Longvert, C, Chaplain, L, et al. Impact of the French COVID-19 pandemic lockdown on newly diagnosed melanoma delay and severity. Journal of the European Academy of Dermatology and Venereology: JEADV. (2022) 36:e164–6. doi: 10.1111/jdv.17802
22. Scharf, C, Brancaccio, G, Di Stefani, A, Fargnoli, MC, Kittler, H, Kyrgidis, A, et al. The association between COVID-19 lockdowns and melanoma diagnosis and thickness: a multicenter retrospective study from Europe. J Am Acad Dermatol. (2022) 87:648–9. doi: 10.1016/j.jaad.2022.05.018
23. Tejera-Vaquerizo, A, Paradela, S, Toll, A, Santos-Juanes, J, Jaka, A, López, A, et al. Effects of COVID-19 lockdown on tumour burden of melanoma and cutaneous squamous cell carcinoma. Acta Derm Venereol. (2021) 101:adv00525. doi: 10.2340/00015555-3890
24. Davis, CH, Ho, J, Greco, SH, Koshenkov, VP, Vidri, RJ, Farma, JM, et al. COVID-19 is affecting the presentation and treatment of melanoma patients in the northeastern United States. Ann Surg Oncol. (2022) 29:1629–35. doi: 10.1245/s10434-021-11086-8
25. Gershenwald, JE, Scolyer, RA, Hess, KR, Sondak, VK, Long, GV, Ross, MI, et al. Melanoma staging: evidence-based changes in the American joint committee on Cancer eighth edition cancer staging manual. CA Cancer J Clin. (2017) 67:472–92. doi: 10.3322/caac.21409
26. Lamm, R, Lyons, W, So, W, and Willis, AI. Advanced-stage melanoma at presentation following the peak of the pandemic: a COVID-19 Cancer canary in a coal mine. World J Surg. (2022) 46:1820–5. doi: 10.1007/s00268-022-06623-9
27. Aw, K, Lau, R, and Nessim, C. Prioritizing melanoma surgeries to prevent wait time delays and upstaging of melanoma during the COVID-19 pandemic. Curr Oncol. (2023) 30:8328–37. doi: 10.3390/curroncol30090604
28. Jeremić, J, Suđecki, B, Radenović, K, Mihaljević, J, Radosavljević, I, Jovanović, M, et al. Impact of the COVID-19 pandemic on melanoma diagnosis: increased Breslow thickness in primary melanomas-a single center experience. Int J Environ Res Public Health. (2022) 19:16806. doi: 10.3390/ijerph192416806
29. Mladenovic, S, Kovacevic, P, Visnjic, A, and Apostolovic, MA. Surigcal Management of Cutaneous Melanoma in the era of COVID-19 pandemic: a single center experience. Acta Medica Medianae. (2023) 62:95–102. doi: 10.5633/amm.2023.0314
30. Aabed, H, Bloanca, V, Crainiceanu, Z, Bratosin, F, Citu, C, Diaconu, MM, et al. The impact of SARS-CoV-2 pandemic on patients with malignant melanoma at a Romanian academic center: a four-year retrospective analysis. Int J Environ Res Public Health. (2022) 19:8499. doi: 10.3390/ijerph19148499
31. Lattanzi, M, Lee, Y, Simpson, D, Moran, U, Darvishian, F, Kim, RH, et al. Primary melanoma histologic subtype: impact on survival and response to therapy. J Natl Cancer Inst. (2021) 111:180–8.
32. Fernandez Canedo, MI, de Troya Martin, M, and Rivas Ruiz, F. Impact of the SARS-CoV-2 pandemic on the early diagnosis of melanoma. Med Clin. (2021) 156:356–7. doi: 10.1016/j.medcli.2020.12.011
33. Sarriugarte Aldecoa-Otalora, J, Loidi Pascual, L, Cordoba Iturriagagoitia, A, and Yanguas Bayona, JI. How has the COVID- 19 pandemic and lockdown affected Breslow thickness in cutaneous melanoma? Actas Dermosifiliogr. (2021) 113:107–9.
34. van Not, OJ, van Breeschoten, J, van den Eertwegh, AJM, Hilarius, DL, De Meza, MM, Haanen, JB, et al. The unfavorable effects of COVID-19 on Dutch advanced melanoma care. Int J Cancer. (2022) 150:816–24. doi: 10.1002/ijc.33833
35. Martinez-Lopez, A, Diaz-Calvillo, P, Cuenca-Barrales, C, Montero-Vilchez, T, Sanchez-Diaz, M, and Buendia-Eisman, A. Arias-Santiag,. Impact of the COVID-19 pandemic on the diagnosis and prognosis of melanoma. J Clin Med. (2022) 11:4181. doi: 10.3390/jcm11144181
36. Toma, AO, Prodan, M, Reddyreddy, AR, Seclaman, E, Crainiceanu, Z, Bloanca, V, et al. The epidemiology of malignant melanoma during the first two years of the COVID-19 pandemic: a systematic review. Int J Environ Res Public Health. (2022) 20:305. doi: 10.3390/ijerph20010305
37. Sangers, T.E; Wakkee, M., Kramer-Noels, E.C., Nijsten, T., Louwman, M.W.J., Jaspars, E.H., and Hollestein, L.M. Limited impact of COVID-19-related diagnostic delay on cutaneous melanoma and squamous cell carcinoma tumour characteristics: a nationwide pathology registry analysis. Br J Dermatol (2022);187:196–202, doi: 10.1111/bjd.21050
38. Klepfisch, L, Carbonnelle-Puscian, A, Faisant, M, Godeneche, J, Provencal, N, Lacoste, C, et al. Impact of the COVID-19 lockdown on the severity of newly-diagnosed primary cutaneous melanoma: a retrospective regional study in France. Ann Dermatol Venereol. (2023) 150:49–51. doi: 10.1016/j.annder.2022.09.002
39. Ricci, F, Fania, L, Paradisi, A, Di Lella, G, Pallotta, S, Sobrino, L, et al. Delayed melanoma diagnosis in the COVID-19 era: increased breslow thickness in primary melanomas seen after the COVID-19 lockdown. J European Academy of Dermatology and Venereol: JEADV. (2020) 34:e778–9. doi: 10.1111/jdv.16874
40. Carlson, JA . Tumor doubling time of cutaneous melanoma and its metastasis. Am J Dermatopathol. (2003) 25:291–9. doi: 10.1097/00000372-200308000-00003
41. Matsui, T, Yao, T, and Iwashita, A. Natural history of early colorectal cancer. World J Surg. (2000) 24:1022–8. doi: 10.1007/s002680010153
42. Gershenwald, JE, and Scolyer, RA. Melanoma staging: American joint committee on cancer (AJCC) 8th edition and beyond. Ann Surg Oncol. (2018) 25:2105–10. doi: 10.1245/s10434-018-6513-7
43. Tejera-Vaquerizo, A, and Nagore, E. Estimated effect of COVID-19 lockdown on melanoma thickness and prognosis: a rate of growth model. J Eur Acad Dermatol Venereol. (2020) 34:e351–3. doi: 10.1111/jdv.16555
44. Guven, DC, Sahin, TK, Yildirim, HC, Cesmeci, E, Incesu, FGG, Tahillioglu, Y, et al. Newly diagnosed cancer and the COVID-19 pandemic: tumour stage migration and higher early mortality. BMJ Support Palliat Care. (2021):003301. doi: 10.1136/bmjspcare-2021-003301
45. Hurley, CM, Wrafter, L, Dhannoon, A, Regan, H, and Regan, PJ. Optimising the Management of Malignant Melanoma during COVID-19. JPRAS Open. (2022) 31:72–5. doi: 10.1016/j.jpra.2021.09.004
46. Asai, Y, Nguyen, P, and Hanna, TP. Impact of the COVID-19 pandemic on skin cancer diagnosis: a population-based study. PLoS One. (2021) 16:e0248492. doi: 10.1371/journal.pone.0248492
47. Ribes, J, Pareja, L, Sanz, X, Mosteiro, S, Escribà, JM, Esteban, L, et al. Cancer diagnosis in Catalonia (Spain) after two years of COVID-19 pandemic: an incomplete recovery. ESMO Open. (2022) 7:100486. doi: 10.1016/j.esmoop.2022.100486
48. Amit, M, Tam, S, Bader, T, Sorkin, A, and Benov, A. Pausing cancer screening during the severe acute respiratory syndrome coron- avirus pandemic: should we revisit the recommendations? Eur J Cancer. (2020) 134:86–9. doi: 10.1016/j.ejca.2020.04.016
49. Vose, JM . Delay in cancer screening and diagnosis during the COVID-19 pandemic: what is the cost? Oncology (Williston Park). (2020) 34:343. doi: 10.46883/ONC.2020.3409.0343
Keywords: melanoma, COVID-19 pandemic, prognosis, diagnosis, delay
Citation: Apostu AP, Vesa &C, Frățilă S, Iancu G, Bejinariu N, Muntean M, Șenilă SC, Baba OA, Secășan CP and Ungureanu L (2024) The effects of the COVID-19 pandemic on the diagnosis and prognosis of melanoma 2 years after the pandemic in two Romanian counties. Front. Med. 11:1328488. doi: 10.3389/fmed.2024.1328488
Edited by:
Guangtong Deng, Central South University, ChinaReviewed by:
Mara Madalina Mihai, ‘Carol Davila’ University of Medicine and Pharmacy, RomaniaCopyright © 2024 Apostu, Vesa, Frățilă, Iancu, Bejinariu, Muntean, Șenilă, Baba, Secășan and Ungureanu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ștefan Cristian Vesa, c3RlZmFudmVzYUBnbWFpbC5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.